immune checkpoint inhibitors of the pd-1/pd-l1-axis in non ...–rebro läns...
TRANSCRIPT
Full Terms & Conditions of access and use can be found athttps://www.tandfonline.com/action/journalInformation?journalCode=iclb20
Scandinavian Journal of Clinical and LaboratoryInvestigation
ISSN: 0036-5513 (Print) 1502-7686 (Online) Journal homepage: https://www.tandfonline.com/loi/iclb20
Immune checkpoint inhibitors of the PD-1/PD-L1-axis in non-small cell lung cancer: promise,controversies and ambiguities in the noveltreatment paradigm
Lars H. Breimer, Petros Nousios, Louise Olsson & Hans Brunnström
To cite this article: Lars H. Breimer, Petros Nousios, Louise Olsson & Hans Brunnström (2020):Immune checkpoint inhibitors of the PD-1/PD-L1-axis in non-small cell lung cancer: promise,controversies and ambiguities in the novel treatment paradigm, Scandinavian Journal of Clinicaland Laboratory Investigation, DOI: 10.1080/00365513.2020.1742369
To link to this article: https://doi.org/10.1080/00365513.2020.1742369
Published online: 02 Apr 2020.
Submit your article to this journal
View related articles
View Crossmark data

REVIEW ARTICLE
Immune checkpoint inhibitors of the PD-1/PD-L1-axis in non-small cell lungcancer: promise, controversies and ambiguities in the novel treatment paradigm
Lars H. Breimera,b, Petros Nousiosa, Louise Olssona and Hans Brunnstr€omc
aCentre for Assessment of Medical Technology in €Orebro, School of Health and Medical Sciences, €Orebro University, €Orebro UniversityHospital, €Orebro, Sweden; bDepartment of Laboratory Medicine, Clinical Chemistry Division, €Orebro University Hospital, €Orebro, Sweden;cDepartment of Clinical Sciences, Division of Oncology and Pathology, Lund University, Lund, Sweden
ABSTRACTImmune checkpoint inhibitors (ICIs) have received much attention not least for melanoma since theaward of the Nobel prize in 2018. Here, we review the current state of knowledge about the use ofthese monoclonal antibodies (mAbs) in non-small cell lung cancer (NSCLC). These drugs have generallybeen conditionally approved on limited early data and there are few long-term follow-up data fromrandomized clinical trials. The effect observed for NSCLC thus far is, on average, moderately betterthan that obtained with chemotherapy. Severe side-effects are more common than might have beenexpected. The drugs themselves are expensive and are associated with time-consuming histopatho-logic testing even though the predictive value of these tests can be discussed. In addition, monitoringfor side-effects involves increased workload and budgetary expense for clinical chemistry laboratories.Here, we review and summarize the current knowledge, controversies and ambiguities of ICIs for thetreatment of NSCLC.
ARTICLE HISTORYReceived 6 December 2019Revised 2 March 2020Accepted 10 March 2020
KEYWORDSNon-small-cell lungcarcinoma; biomarkers;immune checkpointinhibition; PD-1/PD-L1;pharmaceutical economics
Background
The non-surgical, non-radiological, non-endocrinologicaltreatment of cancer has developed by leaps and bounds. Anumber of increasingly powerful but also toxic chemothera-peutic agents like the taxanes and platinums have beenavailable for more than 25 years. About 20 years ago, themonoclonal antibody (mAbs) rituximab and trastuzumabchanged the treatment of lymphoma and breast cancer.Today a whole host of mAbs is on the market. The firstimmune checkpoint inhibitor (ICI) ipilimumab wasapproved in 2011 for metastatic melanoma and since then,the ICIs have opened up a new field of treatment options.Some of the expected benefits at that time, in addition tobetter survival, were less acute toxicity and no mutagenicside-effects as with chemotherapy.
The ICIs essentially fall into 2 classes: inhibitors of cyto-toxic T-lymphocyte–associated protein 4 (CTLA-4) andinhibitors of the PD-1/PD-L1-axis, which in turn can targetprogrammed cell death receptor 1 (PD-1) or programmedcell death ligand 1 (PD-L1) [1–4]. All ICIs work by prevent-ing immune evasion by cancer cells. Ipilimumab is still theonly CTLA-4-inhibitor approved. There now are 3 PD-1-inhibitors – pembrolizumab (Keytruda), nivolumab(Opdivo), and cemiplimab (Libtayo) as well as 3 PD-L1inhibitors – atezolizumab (Tecentriq), avelumab (Bavencio)and durvalumab (Imfinzi). In all, they have been approvedfor 14 indications during the last five years. Melanoma hasreceived most attention as this seems to be the disease in
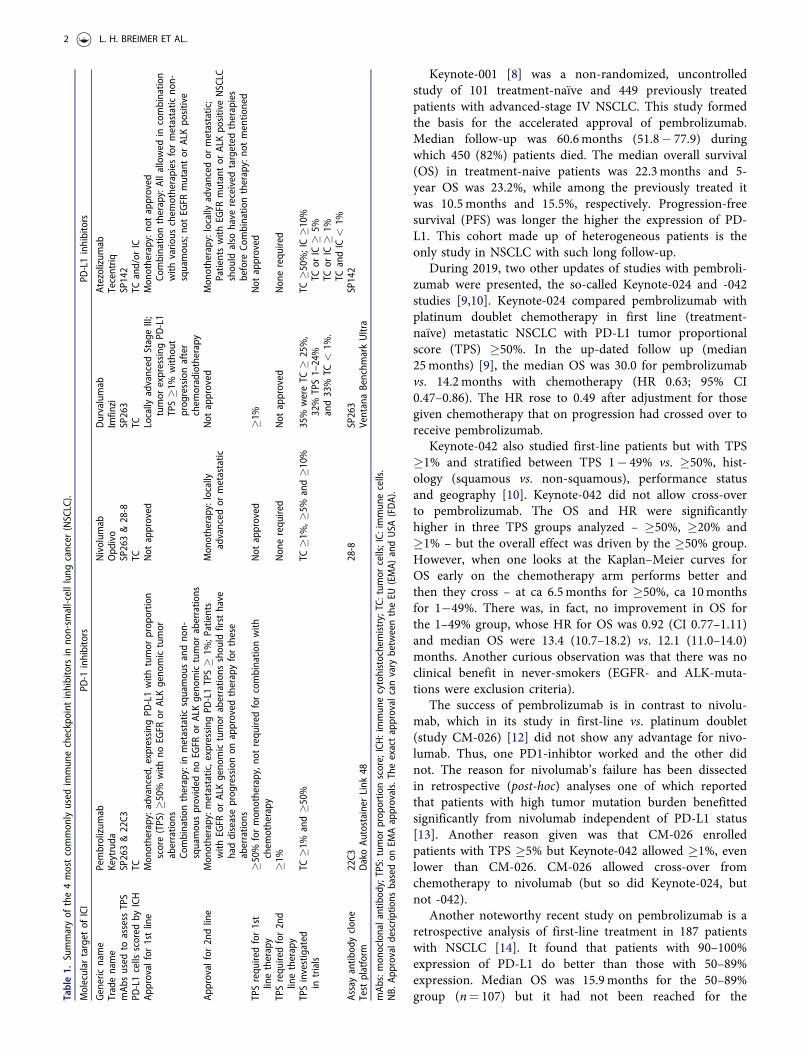
which the ICIs work the best and for which most ICIs areapproved. The 4 PD-1/PD-L1-inhibitors that have been onthe market the longest are summarized in Table 1. Thesefour (pembrolizumab, nivolumab, atezolizumab and durva-lumab) are all approved for non-small-cell lung can-cer (NSCLC).
Lung cancer has a global mortality rate of 18.6/100,000and this is by far the highest worldwide [5]. The pattern issimilar in Sweden [6]. In this review, we focus on (NSCLC),which embraces about 80% of all lung cancer and includesboth adenocarcinoma and squamous cell carcinoma. The 5-year age-standardized net survival in high-income countriesin 2010–2014 was about 20%, almost double compared tothe 1990s [7]. In the UK, it increased from 7% toalmost 15%.
Effect of ICIs in NSCLC according to recentlypublished studies
A major problem in assessing how well ICIs work inNSCLC is that there are precious few results from matureclinical trials. Nearly all data are from interim follow-ups,and the time period is often quite short. The exceptions area 5-year follow-up that has recently been published for astudy of pembrolizumab (Keynote-001) [8]. There have alsobeen extended follow-up of Keynote-024 [9] and Keynote-042 studies (2 years) [10], and also a recent 2-year follow-upfor nivolumab [11].
CONTACT Lars H. Breimer [email protected] Department of Laboratory Medicine, Clinical Chemistry Division, €Orebro University Hospital,SE-701 85 €Orebro, Sweden� 2020 Medisinsk Fysiologisk Forenings Forlag (MFFF)
SCANDINAVIAN JOURNAL OF CLINICAL AND LABORATORY INVESTIGATIONhttps://doi.org/10.1080/00365513.2020.1742369
Keynote-001 [8] was a non-randomized, uncontrolledstudy of 101 treatment-naïve and 449 previously treatedpatients with advanced-stage IV NSCLC. This study formedthe basis for the accelerated approval of pembrolizumab.Median follow-up was 60.6months (51.8� 77.9) duringwhich 450 (82%) patients died. The median overall survival(OS) in treatment-naive patients was 22.3months and 5-year OS was 23.2%, while among the previously treated itwas 10.5months and 15.5%, respectively. Progression-freesurvival (PFS) was longer the higher the expression of PD-L1. This cohort made up of heterogeneous patients is theonly study in NSCLC with such long follow-up.
During 2019, two other updates of studies with pembroli-zumab were presented, the so-called Keynote-024 and -042studies [9,10]. Keynote-024 compared pembrolizumab withplatinum doublet chemotherapy in first line (treatment-naïve) metastatic NSCLC with PD-L1 tumor proportionalscore (TPS) �50%. In the up-dated follow up (median25months) [9], the median OS was 30.0 for pembrolizumabvs. 14.2months with chemotherapy (HR 0.63; 95% CI0.47–0.86). The HR rose to 0.49 after adjustment for thosegiven chemotherapy that on progression had crossed over toreceive pembrolizumab.
Keynote-042 also studied first-line patients but with TPS�1% and stratified between TPS 1� 49% vs. �50%, hist-ology (squamous vs. non-squamous), performance statusand geography [10]. Keynote-042 did not allow cross-overto pembrolizumab. The OS and HR were significantlyhigher in three TPS groups analyzed – �50%, �20% and�1% – but the overall effect was driven by the �50% group.However, when one looks at the Kaplan–Meier curves forOS early on the chemotherapy arm performs better andthen they cross – at ca 6.5months for �50%, ca 10monthsfor 1�49%. There was, in fact, no improvement in OS forthe 1–49% group, whose HR for OS was 0.92 (CI 0.77–1.11)and median OS were 13.4 (10.7–18.2) vs. 12.1 (11.0–14.0)months. Another curious observation was that there was noclinical benefit in never-smokers (EGFR- and ALK-muta-tions were exclusion criteria).
The success of pembrolizumab is in contrast to nivolu-mab, which in its study in first-line vs. platinum doublet(study CM-026) [12] did not show any advantage for nivo-lumab. Thus, one PD1-inhibtor worked and the other didnot. The reason for nivolumab’s failure has been dissectedin retrospective (post-hoc) analyses one of which reportedthat patients with high tumor mutation burden benefittedsignificantly from nivolumab independent of PD-L1 status[13]. Another reason given was that CM-026 enrolledpatients with TPS �5% but Keynote-042 allowed �1%, evenlower than CM-026. CM-026 allowed cross-over fromchemotherapy to nivolumab (but so did Keynote-024, butnot -042).
Another noteworthy recent study on pembrolizumab is aretrospective analysis of first-line treatment in 187 patientswith NSCLC [14]. It found that patients with 90–100%expression of PD-L1 do better than those with 50–89%expression. Median OS was 15.9months for the 50–89%group (n¼ 107) but it had not been reached for theTa
ble1.
Summaryof
the4mostcommon
lyused
immun
echeckpoint
inhibitors
inno
n-sm
all-celllun
gcancer
(NSCLC).
Molecular
target
ofICI
PD-1
inhibitors
PD-L1inhibitors
Genericname
Pembrolizum
abNivolum
abDurvalumab
Atezolizum
abTradename
Keytruda
Opd
ivo
Imfin
ziTecentriq
mAb
sused
toassess
TPS
SP263&22C3
SP263&28-8
SP263
SP142
PD-L1cells
scored
byICH
TCTC
TCTC
and/or
ICAp
proval
for1stline
Mon
otherapy:advanced,
expressing
PD-L1with
tumor
prop
ortio
nscore(TPS)�5
0%with
noEG
FRor
ALKgeno
mictumor
aberratio
nsCo
mbinatio
ntherapy:in
metastatic
squamou
sandno
n-squamou
sprovided
noEG
FRor
ALKgeno
mictumor
aberratio
ns
Not
approved
Locally
advanced
StageIII;
tumor
expressing
PD-L1
TPS�1
%with
out
prog
ressionafter
chem
oradiotherapy
Mon
otherapy:n
otapproved
Combinatio
ntherapy:Allallowed
incombinatio
nwith
vario
uschem
otherapies
formetastatic
non-
squamou
s;no
tEG
FRmutantor
ALKpo
sitive
Approval
for2ndline
Mon
otherapy:m
etastatic,expressingPD
-L1TPS�
1%;P
atients
with
EGFR
orALKgeno
mictumor
aberratio
nsshou
ldfirst
have
haddiseaseprog
ressionon
approved
therapyforthese
aberratio
ns
Mon
otherapy:locally
advanced
ormetastatic
Not
approved
Mon
otherapy:locallyadvanced
ormetastatic;
Patientswith
EGFR
mutantor
ALKpo
sitiveNSCLC
shou
ldalso
have
received
targeted
therapies
before
Combinatio
ntherapy:no
tmentio
ned
TPSrequ
iredfor1st
linetherapy
�50%
formon
otherapy,n
otrequ
iredforcombinatio
nwith
chem
otherapy
Not
approved
�1%
Not
approved
TPSrequ
iredfor2nd
linetherapy
�1%
Non
erequ
ired
Not
approved
Non
erequ
ired
TPSinvestigated
intrials
TC�1
%and�5
0%TC
�1%,�
5%and�1
0%35%
wereTC
�25%,
32%
TPS1–24%
and33%
TC<
1%.
TC�5
0%;IC�1
0%TC
orIC
�5%
TCor
IC�
1%TC
andIC
<1%
Assayantib
odyclon
e22C3
28-8
SP263
SP142
Test
platform
DakoAu
tostainerLink
48VentanaBenchm
arkUltra
mAb
s:mon
oclonalantibod
y;TPS:tumor
prop
ortio
nscore;ICH:immun
ecytohistochemistry;TC:tum
orcells;IC:
immun
ecells.
NB.
Approval
descrip
tions
basedon
EMAapprovals.Theexactapproval
canvary
betweentheEU
(EMA)
andUSA
(FDA).
2 L. H. BREIMER ET AL.

90–100% group (n¼ 80) (p¼ .002). Thus, this indicates thatpembrolizumab monotherapy may be preferable to chemo-therapy-based regimens in patients with tumors showing avery high expression of PD-L1. The authors note that therewas a similar finding in a study of avelumab, a PD-L1-inhibitor, compared to docetaxel in previously treatedNSCLC, that is the clinical response to ICI seemed toimprove with higher PD-L1 cut-off �1%, �50% and �80%,but in the end, there was no benefit of OS [15].
Nivolumab has been investigated in an interesting studyadopting a complex design. A preliminary analysis based ontumor mutational burden (TMB) was reported in 2018 [13],and a larger analysis with 2-year follow-up data was publishedin 2019 [11]. The main analysis concerns the combination ofthe CTLA4-inhibitor ipilimumab with nivolumab comparedwith chemotherapy but data on the single-agent nivolumab wasmainly found in a 42-page appendix. The study populationincluded patients with advanced-stage IV or recurrent NSCLCbut they must not have received any previous treatment forthis disease, and no relevant EGFR- or ALK-mutations must bepresent in their tumor specimen. The most interesting sum-mary of the study results is found in an inconspicuous figure,which showed that patients with PD-L1 TPS <1% did betterthan patients TPS �50%, and much better than patients in thegroup 1–49%. This applied to all patients, and also those withhigh TMB. In the overall analysis for patients with TPS �1%,OS for nivolumabþ ipilimumab was 17.1 vs. 14.9months forchemotherapy (p¼ .007), a difference of 2.2months (66d). Forthose with TPS <1% it was 17.2 vs. 12.2months but no p valuewas reported. This is in contrast to the results for pembrolizu-mab which also targets PD-1 (see above).
Outcome of ICIs in NSCLC according to recentsystematic reviews
During 2019, so far three systematic reviews with meta-anal-yses and slightly different designs have been published[16–18] with a focus on ICIs with or without chemotherapyin first-line treatment of NSCLC. All three concluded thatadding ICIs significantly improved the treatment of NSCLCbut cautioned that longer follow-up and more mature datawere required for firm conclusions.
Modeling efficacy of ICI treatment
In the absence of mature data, a few investigators haveattempted to handle the situation by modeling based ontheir systematic review with meta-analysis. Three very recentpublications were found and the authors did not restrictthemselves to NSCLC.
Shen and Zhao [19] questioned the need for testing forexpression of PD-L1 by immunohistochemistry (IHC) priorto ICI treatment. In their systematic review of publisheddata from eight randomized controlled trials, they concludedthat, based on the overall response rate, although 34% ofPD-L1 positive tumors responded to ICI treatment, also20% of PD-L1 negative tumors responded as well. Theirthreshold for PD-L1 positivity or negativity was that PD-L1
stained cell accounted for 1% of tumor cells, or tumor andimmune cells (IC), assayed by IHC staining methods.
Haslam and Prasad used a different approach, previouslyadopted when they assessed the benefit of genetic treatments[20–22]. Statistics from the American Cancer Society wereused to estimate the number of patients with advanced can-cer who would be eligible for treatment with ICIs. Theresearchers then did a year-by-year comparison with theICIs with their indications as approved by the FDA andfrom this modeling, they concluded that less than 13% ofthose treatable would benefit from ICIs, while almost 44%were eligible for the treatment. They also contended that thepercentage of patients with modeled benefit had peaked in2014 and then decreased. The conclusion was that morerecent indications diluted the strength of any treatmentbenefit since then.
A French group performed an inventive meta-analysiswith modeling of Phase 3 studies, first presented in 2018and then published in 2019 [23]. Because there were no5-year follow-up data, they defined ‘durable response’ as thepercentage of patients with more than either 3 times themedian PFS and/or 2 times the median OS. There were11,640 patients distributed between 26 study arms treatedwith ICIs and 16 without. A statistically significant benefitin favor of ICI treatment was found for all tumors, includ-ing NSCLC, both in terms of PFS and OS. In their modelingbased on OS, both in all indications and in NSCLC specific-ally, ICI treatment achieved 30% compared to 23% withoutICI, while their comparison of the PD-1/PD-L1 class withCTLA-4 it was 31 vs. 29%.
It is interesting in this context to note that two groups[24,25] have independently concluded that so-called realworld data (RWD) validate efficacy-based outcomes fromRCTs. One group found that in the USA only about 15% ofstudies could be replicated using data from insurance claimsand/or electronic health records [24].
Side-effects; how toxic are the ICI agents?
In general, about 10–20% of patients treated with ICIs getsevere (grade 3 & 4) side-effects and even deaths (grade 5)have been described. CTLA-4 inhibitors appear to be associ-ated with an increased rate of and more difficult side-effectsthan PD-1/PD-L1-inhibitors. It also seems that inhibitors ofPD-L1 are slightly less toxic than PD-1. All bodily systemscan be affected by a form of ‘inflammation’ (they are ICIsafter all). An overall term, immune-related adverse events(irAE), has been coined. This involves the skin – mainlyrash; the GI-tract – diarrhea and colitis; the thyroid –mostly hypo – but also hyperthyroidism; pneumonitis, aspecial problem in patients with NSCLC; type1 dia-betes (T1D).
Pillai et al. [26] looked at 3284 patients treated with PD-1 inhibitors and 2460 who received a PD-L1 inhibitor(Table 2). They found a statistically significant differenceonly for pneumonitis (4% for PD-1 inhibitor vs. 2% for PD-L1 inhibitor; p¼ .01). Hypothyroidism (at 7 vs. 4%) almostachieved significant difference (p¼ .07). For other main
SCANDINAVIAN JOURNAL OF CLINICAL AND LABORATORY INVESTIGATION 3
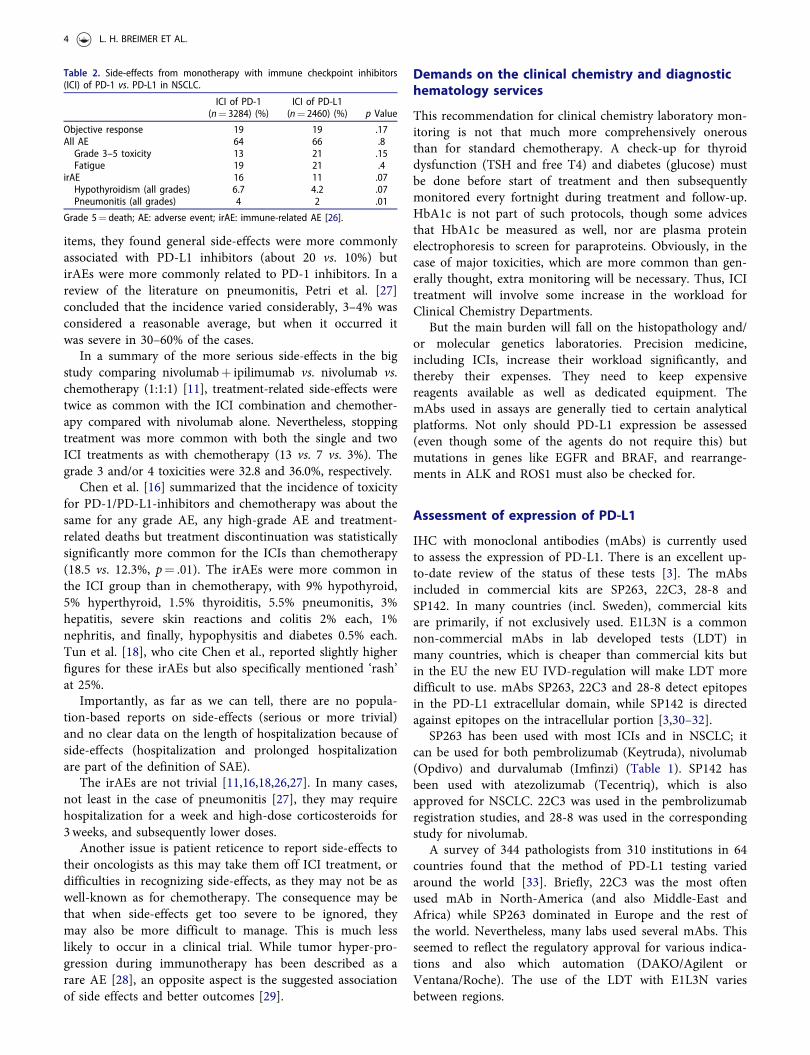
items, they found general side-effects were more commonlyassociated with PD-L1 inhibitors (about 20 vs. 10%) butirAEs were more commonly related to PD-1 inhibitors. In areview of the literature on pneumonitis, Petri et al. [27]concluded that the incidence varied considerably, 3–4% wasconsidered a reasonable average, but when it occurred itwas severe in 30–60% of the cases.
In a summary of the more serious side-effects in the bigstudy comparing nivolumabþ ipilimumab vs. nivolumab vs.chemotherapy (1:1:1) [11], treatment-related side-effects weretwice as common with the ICI combination and chemother-apy compared with nivolumab alone. Nevertheless, stoppingtreatment was more common with both the single and twoICI treatments as with chemotherapy (13 vs. 7 vs. 3%). Thegrade 3 and/or 4 toxicities were 32.8 and 36.0%, respectively.
Chen et al. [16] summarized that the incidence of toxicityfor PD-1/PD-L1-inhibitors and chemotherapy was about thesame for any grade AE, any high-grade AE and treatment-related deaths but treatment discontinuation was statisticallysignificantly more common for the ICIs than chemotherapy(18.5 vs. 12.3%, p¼ .01). The irAEs were more common inthe ICI group than in chemotherapy, with 9% hypothyroid,5% hyperthyroid, 1.5% thyroiditis, 5.5% pneumonitis, 3%hepatitis, severe skin reactions and colitis 2% each, 1%nephritis, and finally, hypophysitis and diabetes 0.5% each.Tun et al. [18], who cite Chen et al., reported slightly higherfigures for these irAEs but also specifically mentioned ‘rash’at 25%.
Importantly, as far as we can tell, there are no popula-tion-based reports on side-effects (serious or more trivial)and no clear data on the length of hospitalization because ofside-effects (hospitalization and prolonged hospitalizationare part of the definition of SAE).
The irAEs are not trivial [11,16,18,26,27]. In many cases,not least in the case of pneumonitis [27], they may requirehospitalization for a week and high-dose corticosteroids for3weeks, and subsequently lower doses.
Another issue is patient reticence to report side-effects totheir oncologists as this may take them off ICI treatment, ordifficulties in recognizing side-effects, as they may not be aswell-known as for chemotherapy. The consequence may bethat when side-effects get too severe to be ignored, theymay also be more difficult to manage. This is much lesslikely to occur in a clinical trial. While tumor hyper-pro-gression during immunotherapy has been described as arare AE [28], an opposite aspect is the suggested associationof side effects and better outcomes [29].
Demands on the clinical chemistry and diagnostichematology services
This recommendation for clinical chemistry laboratory mon-itoring is not that much more comprehensively onerousthan for standard chemotherapy. A check-up for thyroiddysfunction (TSH and free T4) and diabetes (glucose) mustbe done before start of treatment and then subsequentlymonitored every fortnight during treatment and follow-up.HbA1c is not part of such protocols, though some advicesthat HbA1c be measured as well, nor are plasma proteinelectrophoresis to screen for paraproteins. Obviously, in thecase of major toxicities, which are more common than gen-erally thought, extra monitoring will be necessary. Thus, ICItreatment will involve some increase in the workload forClinical Chemistry Departments.
But the main burden will fall on the histopathology and/or molecular genetics laboratories. Precision medicine,including ICIs, increase their workload significantly, andthereby their expenses. They need to keep expensivereagents available as well as dedicated equipment. ThemAbs used in assays are generally tied to certain analyticalplatforms. Not only should PD-L1 expression be assessed(even though some of the agents do not require this) butmutations in genes like EGFR and BRAF, and rearrange-ments in ALK and ROS1 must also be checked for.
Assessment of expression of PD-L1
IHC with monoclonal antibodies (mAbs) is currently usedto assess the expression of PD-L1. There is an excellent up-to-date review of the status of these tests [3]. The mAbsincluded in commercial kits are SP263, 22C3, 28-8 andSP142. In many countries (incl. Sweden), commercial kitsare primarily, if not exclusively used. E1L3N is a commonnon-commercial mAbs in lab developed tests (LDT) inmany countries, which is cheaper than commercial kits butin the EU the new EU IVD-regulation will make LDT moredifficult to use. mAbs SP263, 22C3 and 28-8 detect epitopesin the PD-L1 extracellular domain, while SP142 is directedagainst epitopes on the intracellular portion [3,30–32].
SP263 has been used with most ICIs and in NSCLC; itcan be used for both pembrolizumab (Keytruda), nivolumab(Opdivo) and durvalumab (Imfinzi) (Table 1). SP142 hasbeen used with atezolizumab (Tecentriq), which is alsoapproved for NSCLC. 22C3 was used in the pembrolizumabregistration studies, and 28-8 was used in the correspondingstudy for nivolumab.
A survey of 344 pathologists from 310 institutions in 64countries found that the method of PD-L1 testing variedaround the world [33]. Briefly, 22C3 was the most oftenused mAb in North-America (and also Middle-East andAfrica) while SP263 dominated in Europe and the rest ofthe world. Nevertheless, many labs used several mAbs. Thisseemed to reflect the regulatory approval for various indica-tions and also which automation (DAKO/Agilent orVentana/Roche). The use of the LDT with E1L3N variesbetween regions.
Table 2. Side-effects from monotherapy with immune checkpoint inhibitors(ICI) of PD-1 vs. PD-L1 in NSCLC.
ICI of PD-1(n¼ 3284) (%)
ICI of PD-L1(n¼ 2460) (%) p Value
Objective response 19 19 .17All AE 64 66 .8Grade 3–5 toxicity 13 21 .15Fatigue 19 21 .4
irAE 16 11 .07Hypothyroidism (all grades) 6.7 4.2 .07Pneumonitis (all grades) 4 2 .01
Grade 5¼ death; AE: adverse event; irAE: immune-related AE [26].
4 L. H. BREIMER ET AL.
SP142 gives a significantly lower signal at IHC thanSP263, 22C3 and 28-8 but it is not known how to interpretthis difference, while SP263, 22C3 and 28-8 are overall con-sidered to result in similar staining [2–4,30,31,34–43],though not all observers agree [32]. There is also generalagreement that there is poor concordance between themAbs for PD-L1 expression on IC. Each commercial anti-body is used with the platform of that company, i.e.Ventana (Roche, Basel, Switzerland) for Ventana’s MabsSP263 and SP142 and Dako (Agilent, Santa Clara, CA) forDako’s 22C3 and 22-8. The platform-specificity increasescosts because it means that labs must run both platforms, ifthey are to cover all mAbs.
In an unusual study Munari et al. [44] investigated 198NSCLC mainly early stage cases to compare 22C3 on itsDako platform with 22C3 on a Ventana platform and alsowith SP263 (Ventana) scored by 2 pathologists. In theirhands, SP263 was the most reliable assay to interpret. Theynoted that the pathologist trained on 22C3 consistentlyscored more positive cases than the one trained on SP263both at the 1 and 50% cut-offs. There was less differencebetween 22C3 run on the two platforms than between 22C3and SP263. This is further supported by Ilie et al. [45]where the results for 223C were almost identical for Dakoand Ventana platforms. Hendry et al. [46] evaluated all 4mAbs in 355 cases of NSCLC using 1 single pathologisttrained on 22C3. Like others, they found lower scores withSP142 and poor concordance of ICs. They also found thatSP263 scored more positive than 22C3 and 28-8, both at the1 and 50% level, but concluded there was better concord-ance between 22C3 and 28-8. Brunnstr€om et al. [35] had 7pathologists look at 55 samples stained with all 4 mAbs andfound a significantly better agreement between pathologistswhen using �50% as cutoff. They concluded that the con-cordance between the PD-L1 antibodies 22C3, 28-8 andSP263 was relatively good (for lung cancers) and any one ofthese assays was sufficient for decision on treatment withnivolumab, pembrolizumab and durvalumab, but that thescoring of the pathologist presents an intrinsic source oferror that should be considered especially at low PD-L1 scores.
The Blueprint 1 study [38] is sometimes quoted as argu-ing against the interchangeability of testing mAbs. Thisstudy used commercial (i.e. not real world) samples andcompared 22C3� 1% vs. 28-8� 1% vs. SP263� 25% whileBlueprint 2 [42] made a real world comparison. In theBlueprint 2 study [42] by the same researchers, they statethe ‘three PD-L1 assays (22C3, 28-8 and SP263) showedcomparable analytical performances on TCs but SP142stained fewer’, whereas IC staining was in poor concord-ance. In Blueprint 2, which compared the same 4 mAbsplus a new mAb 73-10 developed for avelumab, theyreported highly comparable TC staining with 22C3, 28-8and SP263, less with SP142, and more with 73-10; and poorcorrelation for IC. Some of these authors in an overview[32] nevertheless question the equivalence of the differentdiagnostic mAbs.
In countries where LDT with E1L3N are used, screeningmight be done with this antibody [31]. It should, however,be noted that in the USA, the FDA assignations of‘companion’ test may result in US clinicians keeping faithwith the mAb as assigned by the FDA, based on the clinicaltrials. In large practices, all mAbs may be used in the histo-pathology department anyway, in which they might as wellbe used as they were in the clinical trials that led toapproval of the treatment. It is worth noting though, that inthe survey [33], 25% of respondents from North-Americaand 15% from Central/South America outsourced their sam-ples (no figures given for the EU or the ROW).
The variations in staining and its assessment are probablyowed to a mixture of reasons, such as variation in the pro-portion of adenocarcinoma vs. squamous cell carcinoma,frequency of smokers, or ex-smokers among patients andother factors. Also, it seems easier to determine if there isno staining (<1%) or if staining is strong (�50%) while thegroup of 1–49% staining seems harder to adjudicate, thoughstudies disagree on this matter [47]. There may also be het-erogeneity of the expression throughout a tumor, and aquite variable concordance in PD-L1 expression betweenmatched biopsies and resected tumors has beenobserved [48–50].
Though there have been calls for TPS for PD-L1 to bereported in a continuous manner from 0 to 100% and letthe requesting physician categorize the level, only somenational pathology societies do this while many these daysoften report in the cut-off values (<1%, 1–49%,�50%) [3,51,52].
Both in the USA and Europe, the clinically interestingvalues are still 1% þ and 50% þ as there are requirementsfor pembrolizumab as monotherapy in second and first line,respectively. Atezolizumab and nivolumab may be used evenin the case of negative PD-L1 (both in the second line, aze-tolizumab also in first line when in combination), but some(though not all) national guidelines advise only give nivolu-mab at PD-L1 1% þ. There is also a consensus that allNSCLC should be PD-L1 tested. In Europe (but not theUnited States), there is also a requirement for PD-L1� 1%for durvalumab as ‘maintenance therapy’ after curative che-moradiotherapy. Thus, the requirement of the pathologist isto (at least) report <1%, 1–49% or �50%.
Sweden has a national consensus and quality document/care program that states that (if possible) we should reporton the scale <1%, 1–4%, 5–9%, 10–24%, 25–49%, 50–74%and �75% [51]. Other countries/departments have differentscales (e.g. Denmark recommends reporting exact percen-tages) but there is no international consensus and there arecertainly many countries without national consensus.
Regarding inclusion in clinical trials, things have lookeddifferent. Most have not had a TPS requirement for PD-L1,but patients have been included regardless and then one hastried to obtain PD-L1 analysis (on current or archived biop-sies or – to a lesser extent – resections) in as many cases aspossible. Subsequently, PD-L1 levels have been analyzed inrelation to treatment response/survival. For example,
SCANDINAVIAN JOURNAL OF CLINICAL AND LABORATORY INVESTIGATION 5

pembrolizumab in the first line was inclusion criterion PD-L1� 50% (Keynote-024) [53].
Health economics
Health economic evaluations have assessed the cost-effect-iveness and budget impact of PD-L1-guided therapy forNSCLC in diverse country settings with mixed results[54–63]. Findings of treatment cost-effectiveness in Brazil,France, Hong Kong and the USA [54–56,59,60,62] havebeen questioned by opposing findings in Australia, China,Switzerland, the UK and the USA [57,58,61,63,64]. Analyseshave been marked by high treatment costs. As evidenced inTable 3, in Sweden such costs have been calculated in excessof SEK 60,000 per month and have been associated withvariable but positive quality-adjusted life-year (QALY) gains.Authorities have assessed the severity of NSCLC as veryhigh thereby indicating a willingness to accept ICERs inexcess of SEK 500,000, the generally accepted cut-off limit.
The modeling of the costs of PD-L1 testing has varied toreflect company preferences as well as the treatment indica-tion(s) achieved. In the UK submission for pembrolizumab,PD-L1 testing was modeled with a unit cost of £40.50 (2019SEK 546)1 [65]. The analysis assumed that in order to iden-tify one patient eligible for treatment, 8.39 patients wouldneed to be tested thereby giving rise to a cost of £337.51(2019 SEK 4566) per patient. In the submission for atezoli-zumab, PD-L1 testing costs were not included in the atezoli-zumab treatment arm due to the license achieved thatincluded all patients irrespective of PD-L1 expression [66].In Sweden, the cost of PD-L1 testing has been calculated inthe durvalumab submission at SEK 2323 exercising modestimpact on overall treatment cost-effectiveness [67]. Why theSwedish cost-estimate should be almost half the Englishone, is an interesting question that speaks to the transfer-ability challenges of health economic analysis across nationalborders.
Existing economic evaluations of PD-L1-dependent treat-ment strategies have incorporated adverse event (AE) infor-mation from the underlying clinical trials with anemia,fatigue, nausea, thromboembolism, pneumonitis and otherirAEs, and peripheral neuropathy comprising the mostexpensive event categories [65,66,68–71]. Reimbursementsubmissions in Sweden have indicated that the impact ofsuch events may be marginal in the determination of treat-ment cost-effectiveness [67,72–74]. This finding contrastswith evidence that existing evaluations of antineoplasticdrugs, and of NSCLC drugs in particular, tend to underesti-mate AE incidence and the associated costs and effects thatmay arise [75,76]. AE selection, the simultaneous experience
of multiple AEs, dose modifications and the actual qualityof life impact on NSCLC patients and their caregivers [77]comprise factors whose complexity may not have beenadequately captured thereby injecting uncertainty in existingcost-effectiveness estimates.
The benefits of NSCLC treatment selection and patientresponse are challenged by the budgetary consequences aris-ing from the use of PD-L1 assays and test platforms withspecific therapeutic agents as shown in Table 1. Studies havehighlighted that while molecular testing may enable bettertreatment selection and savings in the longer term, it is alsoassociated with significant impact on hospital laboratorybudgets [78]. As indicated by Sheppard et al. [79] utilizationof PD-L1 testing decreased treatment costs by 47% but alsoincreased diagnostic costs by e354,783 (2019 SEK 4,4 mil-lion)2. Chabrol et al. [55] analyzed the budgetary impact ofPD-L1 testing in second-line therapy for NSCLC from aBrazilian private payer perspective. Although the analysisindicated considerable treatment cost savings, any assess-ment of study findings needs to take into account the factthat study testing costs were fully subsidized by manufac-turers thereby limiting the generalizability or transferabilityof results into other country settings. In Sweden, PD-L1testing would involve an addition to existing diagnosticcosts whose magnitude would be determined by the fre-quency of the test’s utilization in the national care pathway[51]. According to treatment guidelines, PD-L1 testingshould be performed at the time of initial diagnosis andthen repeated at progress, relapse or metastasis for the initi-ation of immunotherapy subject to the indication of admin-istered treatment(s), the presence (or not) of mutations anddisease stage. It should be noted that the field is undergoingchange making an extension of ICI indications to first-linetreatment not unlikely. This would in turn involve an adap-tation of clinical practice and require additional resourcesfor the delivery of the required testing in the not-toodistant future.
New compounds and principles in development
Not surprisingly given the success of the ICIs launched sofar, there is a lot of activity in developing more agents act-ing on targets other than the PD-1/PD-L1-axis [80,81].Most of these are mAbs but there are also binding-proteinsand fusion-proteins. There is also a drive to develop dual-target compounds that is a single compound that attackstwo pathways. The two compounds most advanced targetlymphocyte-associated gene 3 (LAG3) and TIM3 judging bythe number of Phase 2 and even Phase 3 studies.
Table 3. Monthly treatment costs and cost-effectiveness of ICIs for NSCLC, Sweden 2019.
Treatment Treatment cost (SEK, per month) QALY gain ICER (SEK/QALY) Source
Atezolizumab 63,000 0.52 880,000 [73]Durvalumab 96,000 1.09 857,440 [67]Nivolumab 62,000 0.6 890,136 [74]Pembrolizumab 66,320 1.15 745,585 [72]
QALY: quality-adjusted life-year; ICER: incremental cost-effectiveness ratio.
6 L. H. BREIMER ET AL.

LAG3 is a transmembrane protein, which binds themajor histocompatibility complex (MHC) class II [81].LAG3 has mainly been found on tumor infiltrating regula-tory T-cells (Tregs). LAG3 is cleaved for optimal function ofT-cells. This releases soluble LAG3 (sLAG3). In animalmodels, dual blockade with anti- LAG3 and -PD-1 morethan doubled the tumor clearance. A large number of com-pounds targeting LAG3 are being studied in Phase 1�3 butonly 2 studies specifically mentioned NSCLC.
Another advanced target is antibodies against TIM3(T-cell immunoglobulin and mucin domain-3) stimulatesimmune attack on cancer cells by a dual blockade [80].These mAbs block both the Tregs from down regulating theT-cells that attack cancer cells and also the cancer cells frominhibiting the T-cells. There are at least 10 ongoing Phase Itrials with compounds directed at TIM3.
The ICIs in use have in common that they encouragekiller T-cells to attack cancer cells but only about 20% havelasting clinical benefit [82]. Three articles in Nature thisyear (2020) have shown that B-cells in tertiary lymphoidstructure (TLS) are associated with favorable responses toICIs, at least in myeloma, sarcoma and renal cell [83–85].TLS are collections of B and T cells induced by immuno-logical stimulation. They nurture B-cells. The studiesshowed that TLS was frequently more marked and con-spicuous in those that responded than did not. One problemfor future studies is that because TLS-formation is not seenin animals like rodents (they are a feature of humans) thereare no good experimental models.
Closing remarks
The ICIs have generally been approved through the condi-tional (accelerated) pathway and then expanded into otherdiseases. Institutions like NICE in England and othernational bodies have unusually speedily agreed to recom-mend funding of these treatments. Prasad’s group [21] hasshown that, though 8 ICI indications granted AcceleratedApproval proved to improve OS in confirmatory trials, theFDA has allowed 5 agents that were granted AcceleratedApproval to remain on the market in spite of subsequenttrials failing to show statistically significant improved OS inconfirmatory trials.
Now an intense development and extension of new indi-cations are ongoing. Although ICIs have been approved foruse with as low TPS as �1% or without any positive tumorcells (atezolizumab), it could be argued that till further dataare available, treatment should be restricted to patients withhigh TPS �50% or even higher. Therefore, national oncol-ogy societies must keep detailed registers of patients treatedin the real world setting so that a more complete picturecan be painted.
Reviews of the current status of IHC testing for PD-L1[3,4,31,32,86,87] seem somewhat contradictory and it is dif-ficult to recommend a common strategy for antibody test-ing. Treatment decisions based on SP142 analysis appear toneed separate consideration and should not be the standardtest for NSCLC today, while screening with SP263 (or 22C3)
may be a reasonable strategy though sending samples to labwith appropriate analyses set-up might be just as simple.
Given the moderate predictive value of current testing,there is a need to develop methods beyond IHC to deter-mine PD-L1 expression, such as mRNA, microarray andmassive parallel sequencing analysis [88–91]. Better predict-ive markers are urgently needed to identify patients that arelikely to respond and, importantly, patients unlikely torespond must also be identified. The ethical balance betweenthe risk of AE vs. effect of treatment must be clarified.
The concept of ‘pseudoprogression’ has become part of thetreatment with ICI. Essentially, this is a concern that whatlooks like progression on imaging (e.g. on a CT scan), may bean inflammatory reaction to treatment. It is an approach thatcame in from the use of temozolomide and bevacizumab inglioblastoma. Instead of declaring progression, treatment con-tinues for another couple of cycles to be certain. Althoughregulatory approvals recommend treatment continuation forclinically stable patients with initial evidence of disease pro-gression until disease progression is confirmed, it is desirablethat pseudoprogression is kept also under review and eval-uated to see if it truly matters for long-term survival.
The multiplicity of commercially available test platformsas well as the variability in staining protocols and test refer-ence points indicate the technical and other challenges thatneed to be overcome to make these health technologies suc-cessfully and sustainably integrated into national reimburse-ment schedules and clinical praxis [86,92–94].
Although it is easy to be critical about how the ICI hasbeen introduced and used, nevertheless the studies with pem-brolizumab can be seen as consistent with a not insignificantbenefit. The longest, 5-year follow-up is only from the non-randomized, non-controlled study (Keynote-001) but bothKeynote-024 and -042 have had some time to mature.
Conclusion
There is currently a lack of long-term follow-up data asregulatory approval of ICI for NSCLC has generally beenconditional and based on early, immature data. The needfor population-based, real-world data on the effects, inci-dence of AEs, severe AEs and associated health economicanalyses of ICI treatment in NSCLC cannot be overstated.The long-term benefit in NSCLC remains to be established;the jury is still out.
Notes
1. Inflation and conversion to 2019 SEK prices based onCCEMG – EPPI-Centre Cost Converter’ (v.1.6 last update:29 April 2019) 13.5 SEK/£available at https://eppi.ioe.ac.uk/costconversion/ (accessed 2019-10-30)
2. Inflation and conversion to 2019 SEK prices based onCCEMG – EPPI-Centre Cost Converter’ (v.1.6 last update:29 April 2019) 12.45 SEK/eavailable at https://eppi.ioe.ac.uk/costconversion/ (accessed 2019-10-30)
SCANDINAVIAN JOURNAL OF CLINICAL AND LABORATORY INVESTIGATION 7
Disclosure statement
The authors report no conflicts of interest. The authors alone areresponsible for the content and writing of the article. This work waswritten independently; no company or institution supported theauthors financially or by providing a professional writer.
References
[1] Brody R, Zhang Y, Ballas M, et al. PD-L1 expression inadvanced NSCLC: insights into risk stratification and treatmentselection from a systematic literature review. Lung Cancer.2017;112:200–215.
[2] Buttner R, Gosney JR, Skov BG, et al. Programmed death-lig-and 1 immunohistochemistry testing: a review of analyticalassays and clinical implementation in non-small-cell lung can-cer. J Clin Oncol. 2017;35(34):3867–3876.
[3] Lantuejoul S, Sound-Tsao M, Cooper WA, et al. Perspectivefrom the IASLC pathology committee. J Thorac Oncol. 2019.doi:10.1016/j.jtho.2019.12.107 [Online ahead of print]
[4] Teixido C, Vilarino N, Reyes R, et al. PD-L1 expression testingin non-small cell lung cancer. Ther Adv Med Oncol. 2018;10:1758835918763493.
[5] World Health Organization. Global cancer observatory: inter-national agency for research on cancer. 2018. [cited 2019 Nov13]. Available from: http://gco.iarc.fr/today/data/factsheets/pop-ulations/900-world-fact-sheets.pdf
[6] Socialstyrelsen. Cancer i siffror 2018 Stockholm: socialstyrelsen.2018. [cited 2020 Feb 19]. Available from: https://static-files.cancerfonden.se/Cancer_i_siffror_2018online_webb.pdf
[7] Arnold M, Rutherford MJ, Bardot A, et al. Progress in cancersurvival, mortality, and incidence in seven high-income coun-tries 1995–2014 (ICBP SURVMARK-2): a population-basedstudy. Lancet Oncol. 2019;20(11):1493–1505.
[8] Garon EB, Hellmann MD, Rizvi NA, et al. Five-year overallsurvival for patients with advanced nonsmall-cell lung cancertreated with pembrolizumab: results from the phase IKEYNOTE-001 Study. J Clin Oncol. 2019;37(28):2518–2527.
[9] Reck M, Rodriguez-Abreu D, Robinson AG, et al. Updated ana-lysis of KEYNOTE-024: pembrolizumab versus platinum-basedchemotherapy for advanced non-small-cell lung cancer withPD-L1 tumor proportion score of 50% or greater. J Clin Oncol.2019;37(7):537–546.
[10] Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versuschemotherapy for previously untreated, PD-L1-expressing,locally advanced or metastatic non-small-cell lung cancer(KEYNOTE-042): a randomised, open-label, controlled, phase 3trial. Lancet. 2019;393(10183):1819–1830.
[11] Hellmann MD, Paz-Ares L, Bernabe Caro R, et al. Nivolumabplus ipilimumab in advanced non-small-cell lung cancer. NEngl J Med. 2019;381(21):2020–2031.
[12] Carbone DP, Reck M, Paz-Ares L, et al. First-line nivolumab instage IV or recurrent non-small-cell lung cancer. N Engl JMed. 2017;376(25):2415–2426.
[13] Hellmann MD, Ciuleanu TE, Pluzanski A, et al. Nivolumabplus ipilimumab in lung cancer with a high tumor mutationalburden. N Engl J Med. 2018;378(22):2093–2104.
[14] Aguilar EJ, Ricciuti B, Gainor JF, et al. Outcomes to first-linepembrolizumab in patients with non-small cell lung cancer andvery high PD-L1 expression. Ann Oncol. 2019;30(10):1653–1659.
[15] Barlesi F, Vansteenkiste J, Spigel D, et al. Avelumab versusdocetaxel in patients with platinum-treated advanced non-small-cell lung cancer (JAVELIN Lung 200): an open-label,randomised, phase 3 study. Lancet Oncol. 2018;19(11):1468–1479.
[16] Chen R, Hou X, Yang L, et al. Comparative efficacy and safetyof first-line treatments for advanced non-small cell lung cancer
with immune checkpoint inhibitors: a systematic review andmeta-analysis. Thorac Cancer. 2019;10(4):607–623.
[17] Dafni U, Tsourti Z, Vervita K, et al. Immune checkpoint inhib-itors, alone or in combination with chemotherapy, as first-linetreatment for advanced non-small cell lung cancer. A system-atic review and network meta-analysis. Lung Cancer. 2019;134:127–140.
[18] Tun AM, Thein KZ, Thein WL, et al. Checkpoint inhibitorsplus chemotherapy for first-line treatment of advanced non-small cell lung cancer: a systematic review and meta-analysis ofrandomized controlled trials. Future Sci OA. 2019;5(9):FSO421.
[19] Shen X, Zhao B. Efficacy of PD-1 or PD-L1 inhibitors and PD-L1 expression status in cancer: meta-analysis. BMJ. 2018;362:k3529.
[20] Catenacci DVT, Hochster H, Klempner SJ. Keeping checkpointinhibitors in check. JAMA Netw Open. 2019;2(5):e192546–e192546.
[21] Gill J, Prasad V. A reality check of the accelerated approval ofimmune-checkpoint inhibitors. Nat Rev Clin Oncol. 2019;16(11):656–658.
[22] Haslam A, Prasad V. Estimation of the percentage of USpatients with cancer who are eligible for and respond to check-point inhibitor immunotherapy drugs. JAMA Netw Open.2019;2(5):e192535–e192535.
[23] Pons-Tostivint E, Latouche A, Vaflard P, et al. Comparativeanalysis of durable responses on immune checkpoint inhibitorsversus other systemic therapies: a pooled analysis of phase IIItrials. JCO Precis Oncol. 2019;(3):1–10. doi:10.1200/PO.18.00114
[24] Bartlett VL, Dhruva SS, Shah ND, et al. Feasibility of usingreal-world data to replicate clinical trial evidence. JAMA NetwOpen. 2019;2(10):e1912869.
[25] Moran M, Nickens D, Adcock K, et al. Augmenting therandomized controlled trial with real-world data to aid clinicaldecision making in metastatic renal cell carcinoma: a systematicreview and meta-analysis. Future Oncol. 2019;15(34):3987–4001.
[26] Pillai RN, Behera M, Owonikoko TK, et al. Comparison of thetoxicity profile of PD-1 versus PD-L1 inhibitors in non-smallcell lung cancer: a systematic analysis of the literature. Cancer.2018;124(2):271–277.
[27] Petri CR, Patell R, Batalini F, et al. Severe pulmonary toxicityfrom immune checkpoint inhibitor treated successfully withintravenous immunoglobulin: case report and review of the lit-erature. Resp Med Case Rep. 2019;27:100834.
[28] Zhang D, Zhang Y, Huang Y, et al. Hyper-progressive diseasein a patient with advanced non-small cell lung cancer onimmune checkpoint inhibitor therapy: a case report and litera-ture review. Lung Cancer. 2020;139:18–21.
[29] Lisberg A, Tucker DA, Goldman JW, et al. Treatment-relatedadverse events predict improved clinical outcome in NSCLCpatients on KEYNOTE-001 at a single center. Cancer ImmunolRes. 2018;6(3):288–294.
[30] Lantuejoul S, Adam J, Girard N, et al. PD-L1 testing in non-small cell lung carcinoma: guidelines from the PATTERNgroup of thoracic pathologists. Annal Pathol. 2018;38(2):110–125.
[31] Sica GL, Ramalingam SS. Assays for PD-L1 expression: do allroads lead to Rome? JAMA Oncol. 2017;3(8):1058–1059.
[32] Torlakovic E, Lim HJ, Adam J, et al. Interchangeability of PD-L1 immunohistochemistry assays: a meta-analysis of diagnosticaccuracy. Mod Pathol. 2020;33(1):4–17.
[33] Mino-Kenudsen M, Lantuejoul S. Global survey for pathologistson PD-L1 testing: moving towards standardization. 2019. [cited2020 Feb 20]. Available from: Lungcancernews.org
[34] Batenchuk C, Albitar M, Zerba K, et al. A real-world, compara-tive study of FDA-approved diagnostic assays PD-L1 IHC 28-8and 22C3 in lung cancer and other malignancies. J Clin Pathol.2018;71(12):1078–1083.
8 L. H. BREIMER ET AL.
[35] Brunnstrom H, Johansson A, Westbom-Fremer S, et al. PD-L1immunohistochemistry in clinical diagnostics of lung cancer:inter-pathologist variability is higher than assay variability.Mod Pathol. 2017;30(10):1411–1421.
[36] Casadevall D, Clave S, Taus A, et al. Heterogeneity of tumorand immune cell PD-L1 expression and lymphocyte counts insurgical NSCLC samples. Clin Lung Cancer. 2017;18(6):682–691.e5.
[37] Chan AWH, Tong JHM, Kwan JSH, et al. Assessment of pro-grammed cell death ligand-1 expression by 4 diagnostic assaysand its clinicopathological correlation in a large cohort of sur-gical resected non-small cell lung carcinoma. Mod Pathol. 2018;31(9):1381–1390.
[38] Hirsch FR, McElhinny A, Stanforth D, et al. PD-L1 immuno-histochemistry assays for lung cancer: results from phase 1 ofthe blueprint PD-L1 IHC assay comparison project. J ThoracOncol. 2017;12(2):208–222.
[39] Marchetti A, Barberis M, Franco R, et al. Multicenter compari-son of 22C3 pharmDx (agilent) and SP263 (ventana) assays toTest PD-L1 expression for NSCLC patients to be treated withimmune checkpoint inhibitors. J Thorac Oncol. 2017;12(11):1654–1663.
[40] Rimm DL, Han G, Taube JM, et al. A Prospective, multi-insti-tutional, pathologist-based assessment of 4 immunohistochem-istry assays for PD-L1 expression in non-small cell lung cancer.JAMA Oncol. 2017;3(8):1051–1058.
[41] Scheel AH, Baenfer G, Baretton G, et al. Interlaboratory con-cordance of PD-L1 immunohistochemistry for non-small-celllung cancer. Histopathology. 2018;72(3):449–459.
[42] Tsao MS, Kerr KM, Kockx M, et al. PD-L1 immunohistochem-istry comparability study in real-life clinical samples: results ofblueprint phase 2 project. J Thorac Oncol. 2018;13(9):1302–1311.
[43] Yeo MK, Choi SY, Seong IO, et al. Association of PD-L1expression and PD-L1 gene polymorphism with poor prognosisin lung adenocarcinoma and squamous cell carcinoma. HumPathol. 2017;68:103–111.
[44] Munari E, Zamboni G, Lunardi G, et al. PD-L1 expression innon-small cell lung cancer: evaluation of the diagnostic accur-acy of a laboratory-developed test using clone E1L3N in com-parison with 22C3 and SP263 assays. Hum Pathol. 2019;90:54–59.
[45] Ilie M, Khambata-Ford S, Copie-Bergman C, et al. Use of the22C3 anti-PD-L1 antibody to determine PD-L1 expression inmultiple automated immunohistochemistry platforms. PLoSOne. 2017;12(8):e0183023.
[46] Hendry S, Byrne DJ, Wright GM, et al. Comparison of fourPD-L1 immunohistochemical assays in lung cancer. J ThoracOncol. 2018;13(3):367–376.
[47] Williams GH, Nicholson AG, Snead DRJ, et al. Interobserverreliability of programmed cell death ligand-1 scoring using theVENTANA PD-L1 (SP263) assay in NSCLC. J Thorac Oncol.2019. doi: 1016/j.jtho.2019.11.010 2019 Nov 25 [Online aheadof print]
[48] Elfving H, Mattsson JSM, Lindskog C, et al. Programmed celldeath ligand 1 immunohistochemistry: a concordance studybetween surgical specimen, biopsy, and tissue microarray. ClinLung Cancer. 2019;20(4):258–262 e1.
[49] Ilie M, Long-Mira E, Bence C, et al. Comparative study of thePD-L1 status between surgically resected specimens andmatched biopsies of NSCLC patients reveal major discordances:a potential issue for anti-PD-L1 therapeutic strategies. AnnOncol. 2016;27(1):147–153.
[50] Kitazono S, Fujiwara Y, Tsuta K, et al. Reliability of smallbiopsy samples compared with resected specimens for thedetermination of programmed death-ligand 1 expression innon–small-cell lung cancer. Clin Lung Cancer. 2015;16(5):385–390.
[51] Regionala Cancercentrum i Samverkan. Lungcancer nationelltvårdprogram. 2019. [cited 2020 Feb 20]. Available from:
https://kunskapsbanken.cancercentrum.se/diagnoser/lungcancer/vardprogram/
[52] Robinson M, James J, Thomas G, et al. Quality assurance guid-ance for scoring and reporting for pathologists and laboratoriesundertaking clinical trial work. J Pathol Clin Res. 2019;5(2):91–99.
[53] Reck M, Rodriguez-Abreu D, Robinson AG, et al.Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833.
[54] Aguiar PN, Jr., Perry LA, Penny-Dimri J, et al. The effect ofPD-L1 testing on the cost-effectiveness and economic impact ofimmune checkpoint inhibitors for the second-line treatment ofNSCLC. Ann Oncol. 2017;28(9):2256–2263.
[55] Chabrol Haas L, Coutinho MB, Peixoto RB, et al. Use of PD-L1 biomarker in second line therapy for non-small cell lungcancer: budget impact analysis from a private payer perspectivein Brazil. Value Health. 2018;21:S23.
[56] Chouaid C, Bensimon L, Clay E, et al. Cost-effectiveness ana-lysis of pembrolizumab versus standard-of-care chemotherapyfor first-line treatment of PD-L1 positive (>50%) metastaticsquamous and non-squamous non-small cell lung cancer inFrance. Lung Cancer. 2019;127:44–52.
[57] Criss SD, Mooradian MJ, Watson TR, et al. Cost-effectivenessof atezolizumab combination therapy for first-line treatment ofmetastatic nonsquamous non-small cell lung cancer in theUnited States. JAMA Netw Open. 2019;2(9):e1911952.
[58] Gao L, Li SC. Modelled economic evaluation of nivolumab forthe treatment of second-line advanced or metastatic squamousnon-small-cell lung cancer in Australia using both partitionsurvival and markov models. Appl Health Econ Health Policy.2019;17(3):371–380.
[59] Georgieva M, da Silveira Nogueira Lima JP, Aguiar P Jr, et al.Cost-effectiveness of pembrolizumab as first-line therapy foradvanced non-small cell lung cancer. Lung Cancer. 2018;124:248–254.
[60] Loong HH, Wong CKH, Leung LKS, et al. Cost effectiveness ofPD-L1-based test-and-treat strategy with pembrolizumab as thefirst-line treatment for metastatic NSCLC in Hong Kong.Pharmacoecon Open. 2019. doi:10.1007/s41669-019-00178-7[Online ahead of print].
[61] Matter-Walstra K, Schwenkglenks M, Aebi S, et al. A cost-effectiveness analysis of nivolumab versus docetaxel foradvanced nonsquamous NSCLC including PD-L1 testing. JThorac Oncol. 2016;11(11):1846–1855.
[62] She L, Hu H, Liao M, et al. Cost-effectiveness analysis of pem-brolizumab versus chemotherapy as first-line treatment inlocally advanced or metastatic non-small cell lung cancer withPD-L1 tumor proportion score 1% or greater. Lung Cancer.2019;138:88–94.
[63] Zhou K, Jiang C, Li Q. Cost-effectiveness analysis of pembroli-zumab monotherapy and chemotherapy in the non-small-celllung cancer with different PD-L1 tumor proportion scores.Lung Cancer. 2019;136:98–101.
[64] Agilent Technologies Inc. PD-L1 IHC 22C3 pharmDx inter-pretation manual - NSCLC. Santa Clara (CA): AgilentTechnologies Inc; 2018.
[65] National Institute for Health and Care Excellence (NICE).Single technology appraisal: pembrolizumab for treating PD-L1-positive non-small-cell lung cancer after platinumbasedchemotherapy [ID840] – committee papers. London: NationalInstitute for Health and Care Excellence (NICE); 2016.
[66] National Institute for Health and Care Excellence (NICE).Single technology appraisal: atezolizumab for treating non-small-cell lung cancer after platinum-based chemotherapy[ID970] – committee papers. London: National Institute forHealth and Care Excellence (NICE); 2018.
[67] Imfinzi (durvalumab) Stockholm: tandvårds- ochl€akemedelsf€ormånsverket (TLV). 2018. [cited 2020 Feb 20].Available from: https://www.tlv.se/download/18.13634819166e2df86244c71e/1541598097880/bes_underlag181106_imfinzi.pdf
SCANDINAVIAN JOURNAL OF CLINICAL AND LABORATORY INVESTIGATION 9
[68] National Institute for Health and Care Excellence (NICE).Nivolumab for previously treated squamous non-small cell lungcancer technology appraisal guidance [TA483]. London:National Institute for Health and Care Excellence (NICE);2017.
[69] National Institute for Health and Care Excellence (NICE). Finalappraisal determination Nivolumab for previously treated non-squamous non-small-cell lung cancer. London: NationalInstitute for Health and Care Excellence (NICE); 2017.
[70] National Institute for Health and Care Excellence (NICE).Pembrolizumab for untreated PD-L1 positive metastatic non-small-cell lung cancer (CDF review of TA447) [ID1349].London: National Institute for Health and Care Excellence(NICE); 2018.
[71] National Institute for Health and Care Excellence (NICE).Atezolizumab for treating locally advanced or metastatic non-small-cell lung cancer after chemotherapy. London: NationalInstitute for Health and Care Excellence (NICE); 2018.
[72] Tandvårds- och l€akemedelsf€ormånsverket (TLV). Keytruda (pem-brolizumab) Stockholm: tandvårds- och l€akemedelsf€ormånsverket(TLV). 2017. [cited 2020 Feb 20]. Available from: https://www.tlv.se/download/18.467926b615d084471ac338ea/1510316399554/Kunskapsunderlag_keytruda_forsta_linjen_icke_smacellig_lungcancer.pdf
[73] Tandvårds- och L€akemedelsf€ormånsverket (TLV). Tecentriq (atezoli-zumab) Stockholm: tandvårds- och l€akemedelsf€ormånsverket (TLV).2018. [cited 2020 Feb 20]. Available from: https://www.tlv.se/down-load/18.564d7770164e1dcb5d6a230c/1533290942740/bes180123_underlag_tecentriq.pdf
[74] Tandvårds- och l€akemedelsf€ormånsverket (TLV). Opdivo (nivo-lumab) Stockholm: tandvårds- och l€akemedelsf€ormånsverket(TLV). 2015. [cited 2020 Feb 20]. Available from: https://www.tlv.se/download/18.467926b615d084471ac33ab9/1510316360481/Kunskapsunderlag_opdivo_lungcancer.pdf
[75] Linden S, Redig J, Banos Hernaez A, et al. Comorbidities andrelevant outcomes, commonly associated with cancer, ofpatients newly diagnosed with advanced non-small-cell lungcancer in Sweden. Eur J Cancer Care (Engl). 2019;29:e13171.
[76] Pearce A, Haas M, Viney R. Are the true impacts of adverseevents considered in economic models of antineoplastic drugs?A systematic review. Appl Health Econ Health Policy. 2013;11(6):619–637.
[77] Wood R, Taylor-Stokes G, Smith F, et al. The humanistic bur-den of advanced non-small cell lung cancer (NSCLC) inEurope: a real-world survey linking patient clinical factors topatient and caregiver burden. Qual Life Res. 2019;28(7):1849–1861.
[78] Restelli U, Artale S, Pacelli V, et al. Financial consequences ofthe performance of A Pd-L1 test to select patients receivingsecond and third line treatments for non-small cell lung cancerin Italy. Value Health. 2017;20(9):A424.
[79] Sheppard B, Ahlsten M, Paolini D, et al. The budget impact ofintroducing A PD-L1 assay to select patients with metastaticnsclc who are potential candidates for treatment with immunecheckpoint inhibitors. Value Health. 2017;20(9):A576.
[80] Friedlaender A, Addeo A, Banna G. New emerging targets incancer immunotherapy: the role of TIM3. ESMO Open. 2019;4(3):e000497.
[81] Puhr HC, Ilhan-Mutlu A. New emerging targets in cancerimmunotherapy: the role of LAG3. ESMO Open. 2019;4(2):e000482.
[82] Bruno TC. New predictors for immunotherapy responsessharpen our view of the tumour microenvironment. Nature.2020;577(7791):474–476.
[83] Cabrita R, Lauss M, Sanna A, et al. Tertiary lymphoid struc-tures improve immunotherapy and survival in melanoma.Nature. 2020;577(7791):561–565.
[84] Helmink BA, Reddy SM, Gao J, et al. B cells and tertiarylymphoid structures promote immunotherapy response. Nature.2020;577(7791):549–555.
[85] Petitprez F, de Reynies A, Keung EZ, et al. B cells are associ-ated with survival and immunotherapy response in sarcoma.Nature. 2020;577(7791):556–560.
[86] Kim H, Chung JH. PD-L1 testing in non-small cell lung cancer:past, present, and future. J Pathol Transl Med. 2019;53(4):199–206.
[87] Koomen BM, Badrising SK, van den Heuvel MM, et al.Comparability of PD-L1 immunohistochemistry assays for non-small cell lung cancer: a systematic review. Histopathology.2019. doi: 10.1111/HIS.14040 2019 Dec 2 [Online ahead ofprint].
[88] Erber R, Stohr R, Herlein S, et al. Comparison of PD-L1mRNA expression measured with the checkpoint typerVR assaywith PD-L1 protein expression assessed with immunohisto-chemistry in non-small cell lung cancer. Anticancer Res. 2017;37(12):6771–6778.
[89] Gafeer MM, Hosny Mohammed K, Ormenisan-Gherasim C,et al. Diagnostic utility of PD-L1 expression in lung adenocar-cinoma: immunohistochemistry and RNA in situ hybridization.Appl Immunohistochem Mol Morphol. 2018;26(8):e86–e90.
[90] Goodman AM, Piccioni D, Kato S, et al. Prevalence of PDL1amplification and preliminary response to immune checkpointblockade in solid tumors. JAMA Oncol. 2018;4(9):1237–1244.
[91] Li C, Huang C, Mok TS, et al. Comparison of 22C3 PD-L1expression between surgically resected specimens and pairedtissue microarrays in non-small cell lung cancer. J ThoracOncol. 2017;12(10):1536–1543.
[92] Faulkner E, Annemans L, Garrison L, et al. Challenges in thedevelopment and reimbursement of personalized medicine-payer and manufacturer perspectives and implications forhealth economics and outcomes research: a report of theISPOR personalized medicine special interest group. ValueHealth. 2012;15(8):1162–1171.
[93] Garfield S, Polisena J, D SS, et al. Health technology assessmentfor molecular diagnostics: practices, challenges, and recommen-dations from the medical devices and diagnostics special inter-est group. Value Health. 2016;19(5):577–587.
[94] Garinet S, Laurent-Puig P, Blons H, et al. Current and futuremolecular testing in NSCLC, what can we expect from newsequencing technologies? J Clin Med. 2018;7(6):144.
10 L. H. BREIMER ET AL.