genital lesions in dermatopathology - pathcme.com · • erosive lp is the most common cause of...
TRANSCRIPT
Genital Lesions in Dermatopathology
Janis M. Taube, MDDirector of Dermatopathology
Associate Professor of Dermatology and PathologyJohns Hopkins University SOM
OverviewVulvovaginal lesions
• Non-Neoplastic– Spongiotic and psorasiform dermatitis– Lichenoid pattern
• lichen sclerosus• lichen amyloid• lichen planus• Zoon’s mucositis/dermatitis
– Verruciform xanthoma• Neoplastic lesions
– Two types of VIN and squamous cell carcinoma• Podophylin-treatment reaction• C0-existing nigh-grade VIN and condyloma
– BCCs of the vulva
Scrotal lesions

Spongiotic and PsorasiformPattern on Vulva
• Contact dermatitis• Psoriasis• Lichen simplex chronicus• Vulvovaginal candidiasis• Tinea infection• Extramammary Paget’s disease
Spongiotic and PsorasiformPattern on Vulva
• Contact dermatitis• Psoriasis• Lichen simplex chronicus• Vulvovaginal candidiasis• Tinea infection• Extramammary Paget’s disease
PAS stains
Contact Dermatitis
• Common condition, increasing with chronicity• Irritant (exposure to chemical or physical
agents) *most common• Allergic (cell-mediated following sensitization)
– Medications– Preservatives and fragrances in products– Nickel or rubber
• acute, subacute and chronic phases
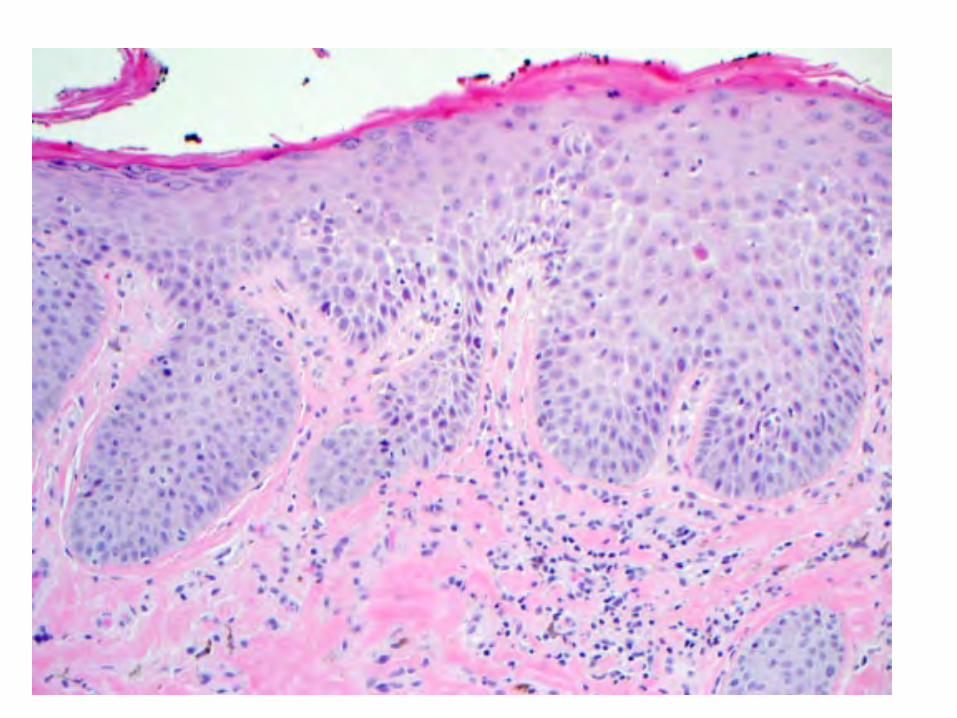
•need strong clinical input to secure diagnosis of psoriasis at this site•Features on bx are often obscured due to LSC or secondary infection•biopsy is not necessary if clinically diagnosed unless lesion is treatment-resistant
• 5% of women with vulvar symptoms• Chronic, relapsing condition• Multiple forms:
– Classic and pustular forms, either generalized or localized to vulva
– Inverse psoraisis
• Cutaneous (rather than mucosal) vulva in all forms
Vulvar psoriasis


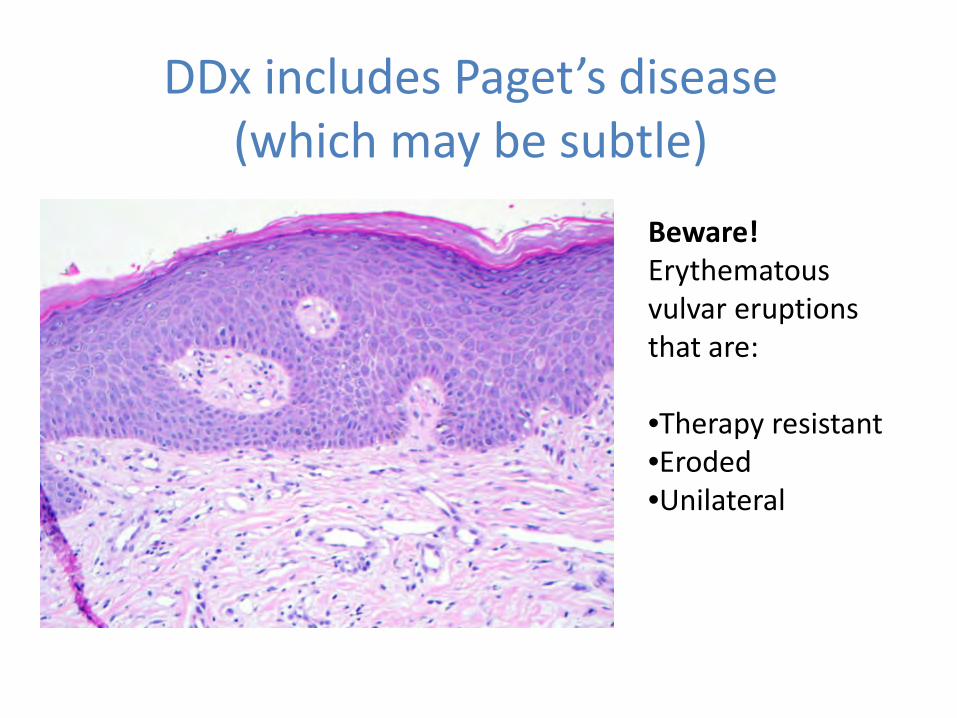
DDx includes Paget’s disease (which may be subtle)
Beware!Erythematousvulvar eruptions that are:
•Therapy resistant•Eroded•Unilateral
CK7
Overview
Vulvovaginal lesions
• Non-Neoplastic– Spongiotic and psorasiform dermatitis– Lichenoid pattern
• lichen sclerosus• lichen amyloid• lichen planus• Zoon’s mucositis/dermatitis
– Verruciform xanthoma• Neoplastic lesions
– Two types of VIN and squamous cell carcinoma– BCCs of the vulva– Paget’s disease
Scrotal lesions
Lichen Sclerosus• Chronic fibrosing disease of the anogenital
skin– Labia majora is most common site– Relapsing and remitting course– Obliteration and stenosis over time
• Bimodal age peak at pre-menarche and post-menopause
• Lesions start as ivory white papules and macules that coalesce
• Increased risk for developing non-HPV-related SCC (2-5%)
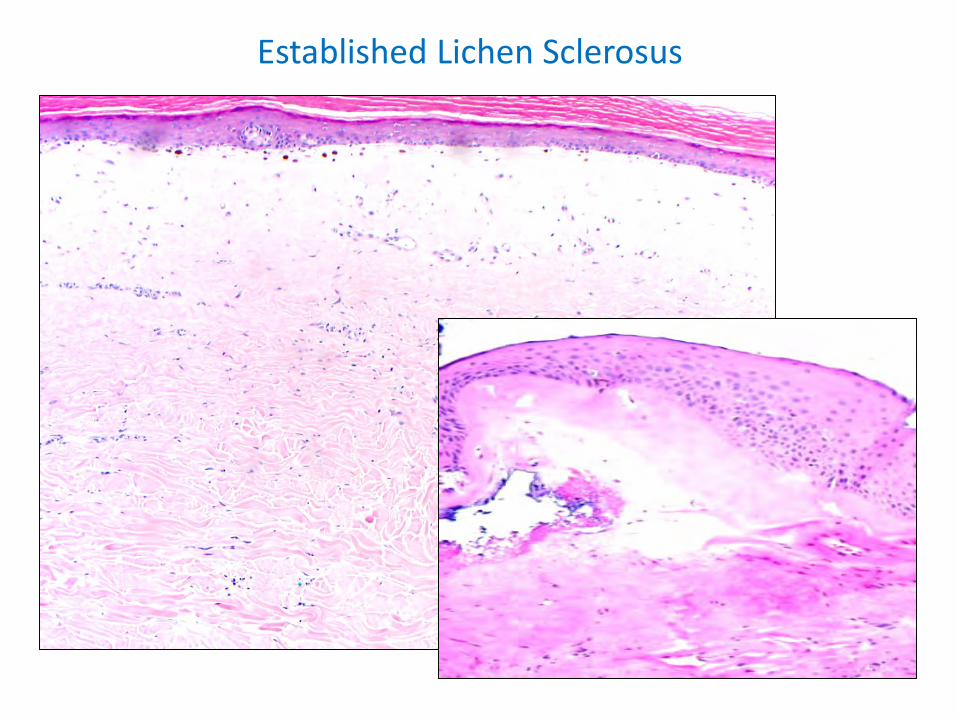
Established Lichen Sclerosus
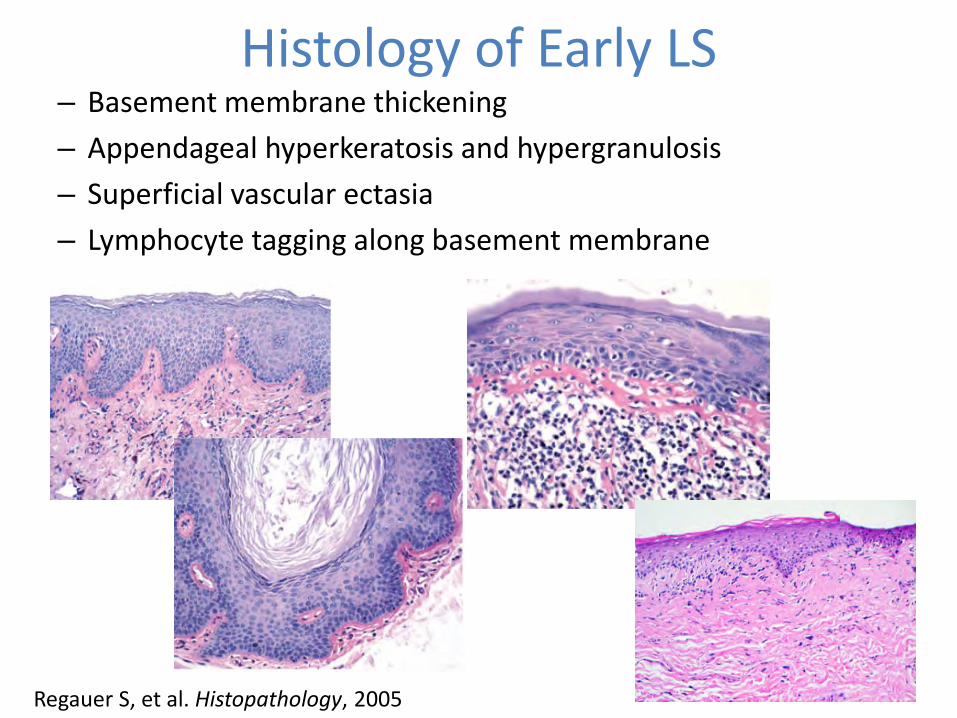
Histology of Early LS– Basement membrane thickening– Appendageal hyperkeratosis and hypergranulosis– Superficial vascular ectasia– Lymphocyte tagging along basement membrane
Regauer S, et al. Histopathology, 2005

CK5/6
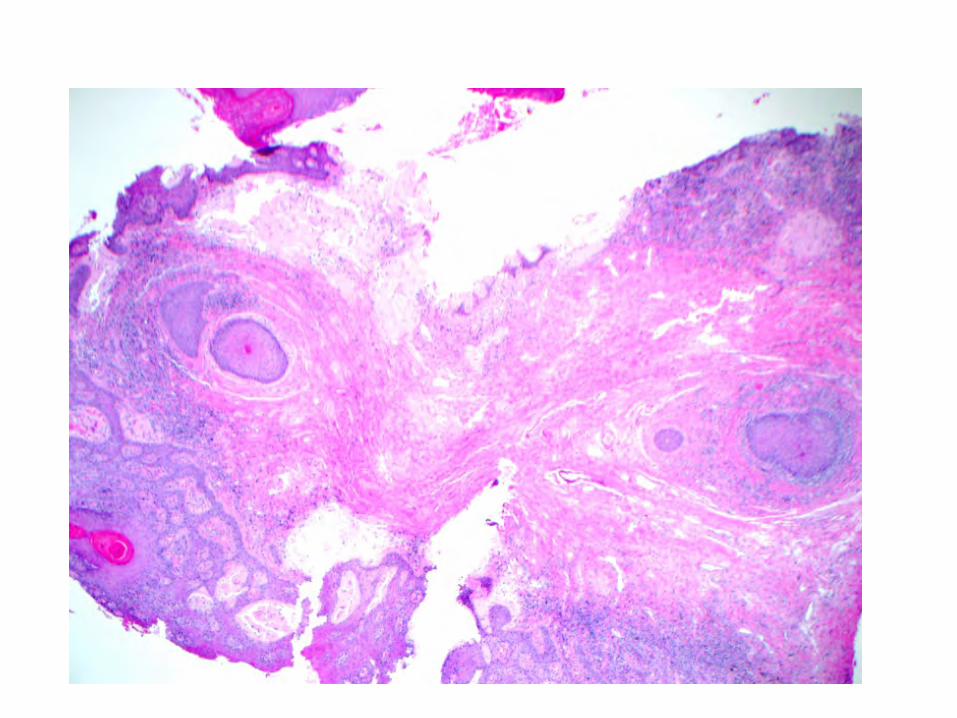
Diagnosis?
Lichen Amyloidosis
• Most common form of primary localized cutaneous amyloidosis
• Typically seen on the shins• Papules may coalesce into thickened plaques• Often shows associated LSC-type changes
Genital Lichen Planus
Genital lichen planus
• 50% of women who have lichen planus have genital involvement
• Very commonly associated with oral lesions• Erosive LP is the most common cause of non-
infectious erosive vulvar disease• DDx: early lichen sclerosus, lichenoid drug
eruption

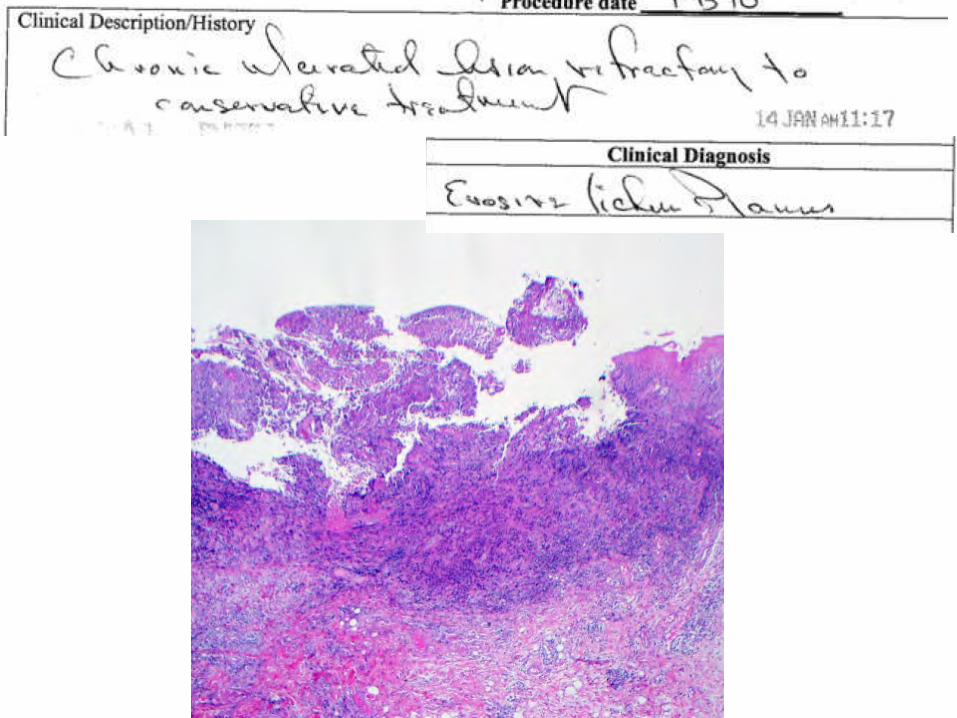
Erosive* (most common)
papulosquamous hypertrophic
Anatomic site Mucosal surface Hair-bearing skin (labia majora)
Perineal and perianal regions
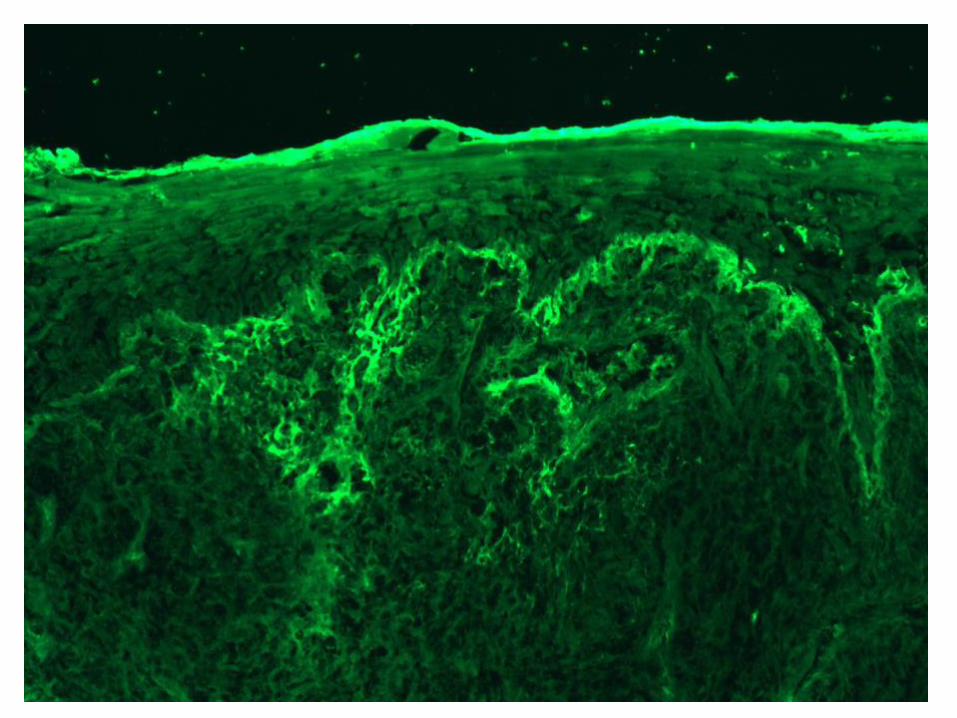
Histology Often non-specific ulceration*
Like classic cutaneous LP
Like classic hypertrophic LP
*Suggest additional sampling adjacent, inflamed, but non-ulcerated areas. If present, sample white reticulated areas.-DIF may also be of use
Vulvar Lichen Planus

Reported association of erosive LP and SCC is 2-3% of cases.
CK903
Plasma cell vulvitis (Zoon’s vulvitis)
1952– Zoon first made his histologic description in the foreskin
1957—Garnier described a rare condition of erythematous plaques on the vulva in post-menopausal women
“vulvitis circumscripta plasmacellularis”“idiopathic lymphoplasmacellular mucositis-
dermatitis”
Plasma cell vulvitis (Zoon’s vulvitis)
Plasma cell vulvitis (Zoon’s vulvitis)
• Rare, chronic inflammatory condition in classically in post-menopausal women
• Vestibule and labia minora• Single erythematous plaque: glistening, red-
orange-brown, and resembling purpura• Vulvar soreness, pruritic, burning, discharge,
and bleeding• Clinical DDx: VIN, Paget’s disease, Fixed drug
eruption
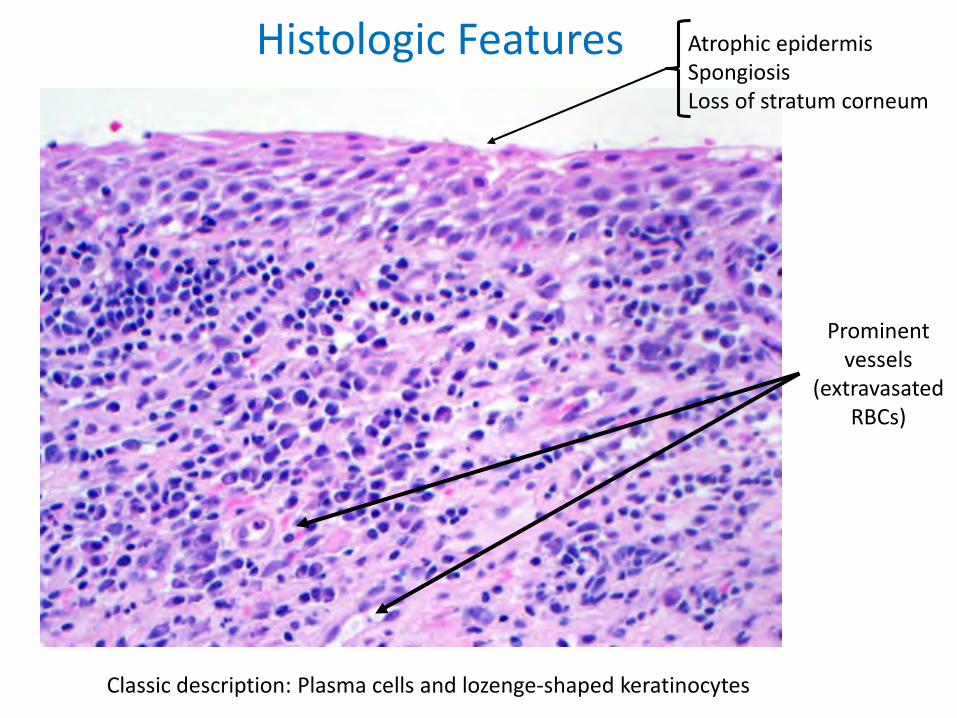
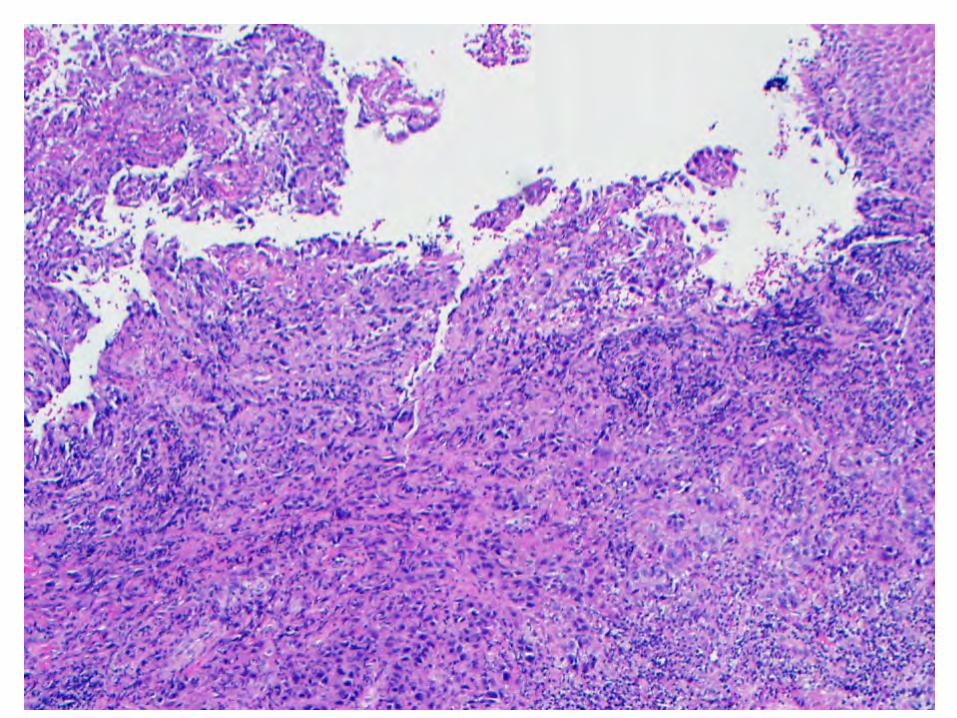
Atrophic epidermisSpongiosisLoss of stratum corneum
Prominentvessels
(extravasatedRBCs)
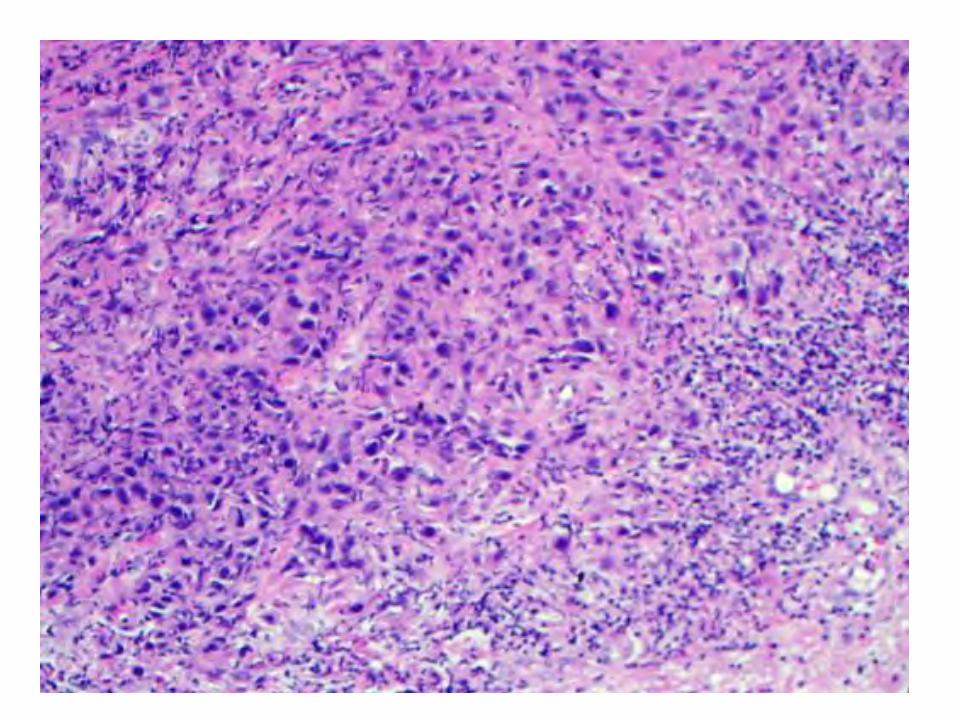
Classic description: Plasma cells and lozenge-shaped keratinocytes
Histologic Features
• Lichenoid infiltrate with plasma cells:– >50% of plasma cells or– 25-50% plasma cells with epithelial atrophy and
hemosiderin deposition– <25% may be attributed to mucosal site
• “lozenge-shaped” keratinocytes were rarely observed
Retrospective histopathologic re-evaluation of 18 cases of plasma cell vulvitis
Virgili A, et al. J Reprod Med, 2005
• Lichenoid infiltrate with plasma cells:– >50% of plasma cells or– 25-50% plasma cells with epithelial atrophy and
hemosiderin deposition– <25% may be attributed to mucosal site
• “lozenge-shaped” keratinocytes were rarely observed
Retrospective histopathologic re-evaluation of 18 cases of plasma cell vulvitis
Virgili A, et al. J Reprod Med, 2005
Identified 16/18 patients in retrospective study

Overview
Vulvovaginal lesions
• Non-Neoplastic– Spongiotic and psorasiform dermatitis– Lichenoid pattern
• lichen sclerosus• lichen amyloid• lichen planus• Zoon’s mucositis/dermatitis
– Verruciform xanthoma• Neoplastic lesions
– Two types of VIN and squamous cell carcinoma• Podophylin-treatment reaction• C0-existing nigh-grade VIN and condyloma
– BCCs of the vulva
Scrotal lesions
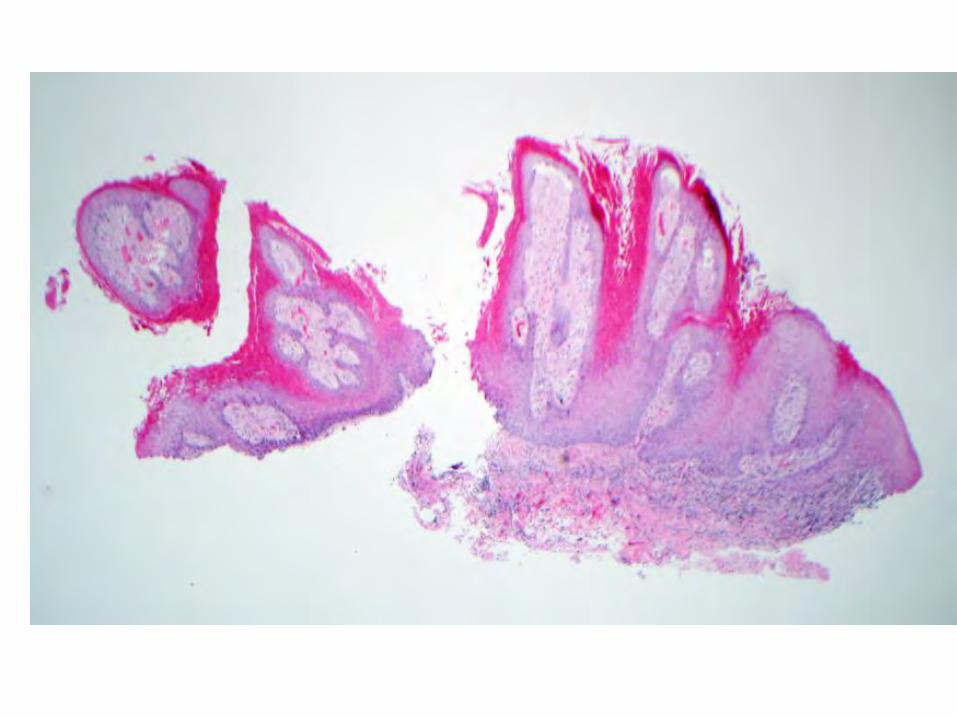
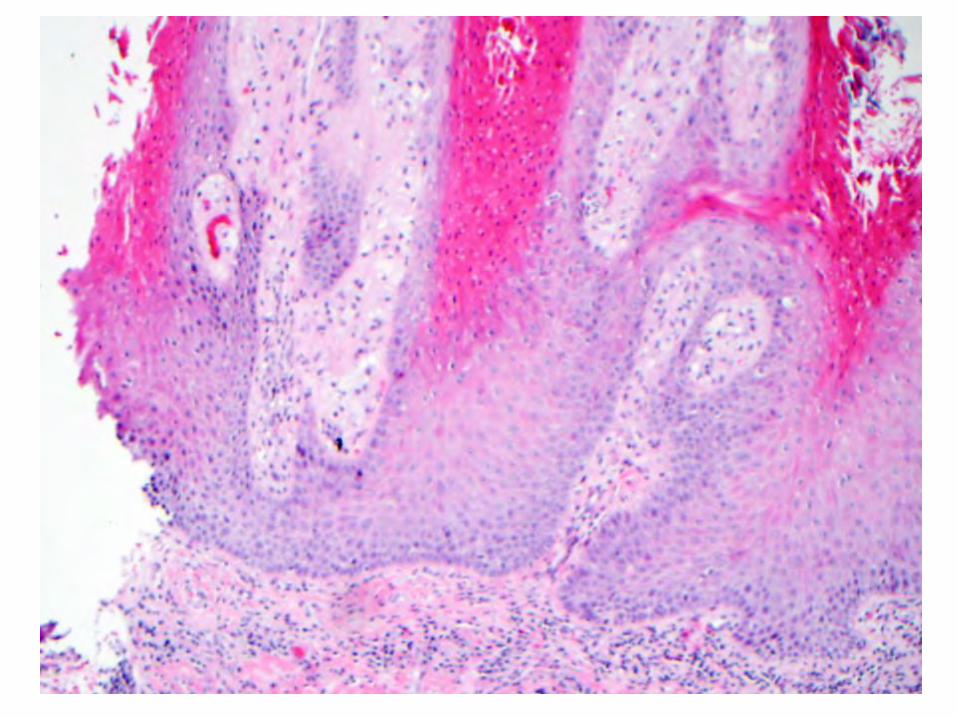
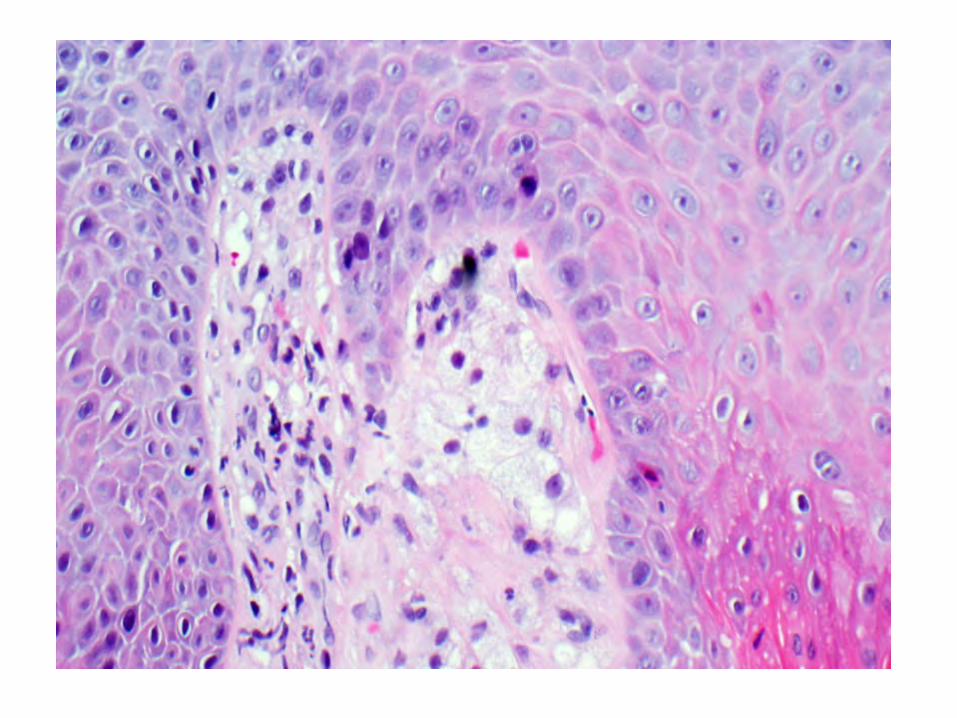
Verruciform Xanthoma
• Slow-growing, painless, solitary exophytictumors
• 0.5 to 2.0 cm in size• HPV has not been detected
OverviewVulvovaginal lesions
• Non-Neoplastic– Spongiotic and psorasiform dermatitis– Lichenoid pattern
• lichen sclerosus• lichen amyloid• lichen planus• Zoon’s mucositis/dermatitis
– Verruciform xanthoma• Neoplastic lesions
– Two types of VIN and squamous cell carcinoma• Podophylin-treatment reaction• C0-existing nigh-grade VIN and condyloma
– BCCs of the vulva
Scrotal lesions
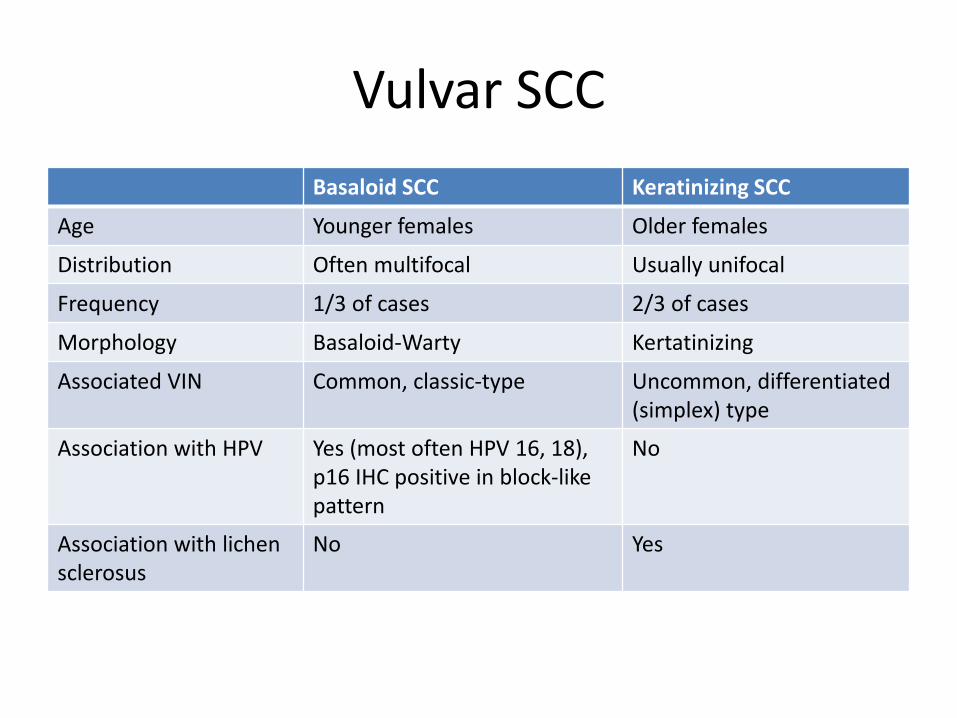
Vulvar SCCBasaloid SCC Keratinizing SCC
Age Younger females Older females
Distribution Often multifocal Usually unifocal
Frequency 1/3 of cases 2/3 of cases
Morphology Basaloid-Warty Kertatinizing
Associated VIN Common, classic-type Uncommon, differentiated (simplex) type
Association with HPV Yes (most often HPV 16, 18), p16 IHC positive in block-like pattern
No
Association with lichen sclerosus
No Yes
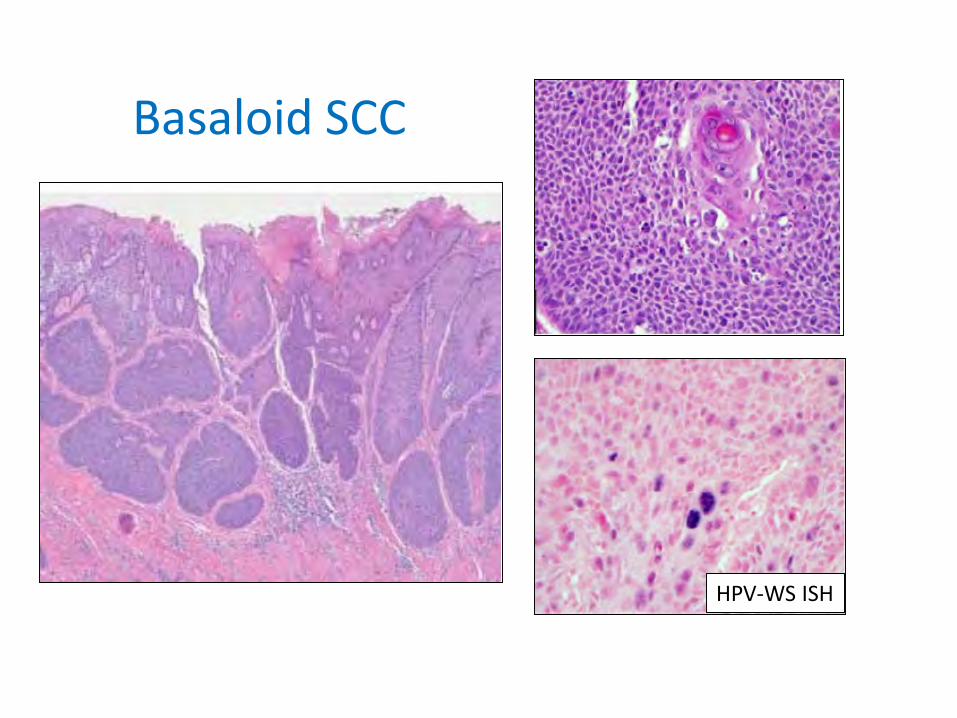
Basaloid SCC
HPV-WS ISH
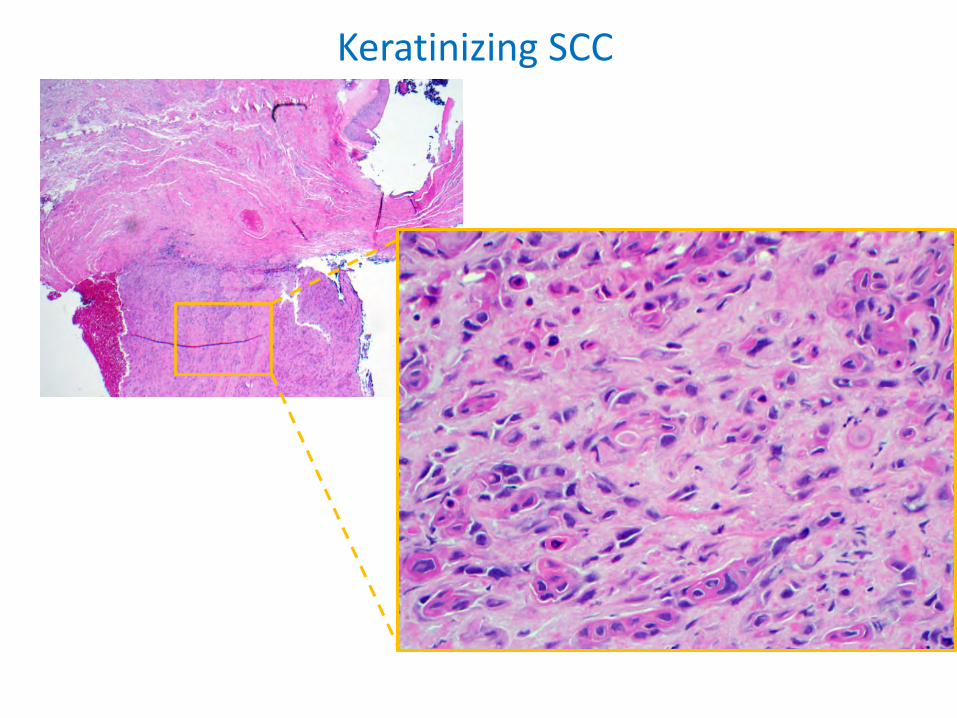
Keratinizing SCC

P16 IHC as a surrogate marker of high-risk HPV infection
• 175 archival vulvar lesions, stained with p16 IHC• Positive predictive value of diffuse, block-like pattern is 95-
97% Modified from Riethdorf S, et al. Hum Pathol 2004
Homogeneousnuclear and cytoplasmic
Uneven staining (combined strongly staining and
weak/no staining)
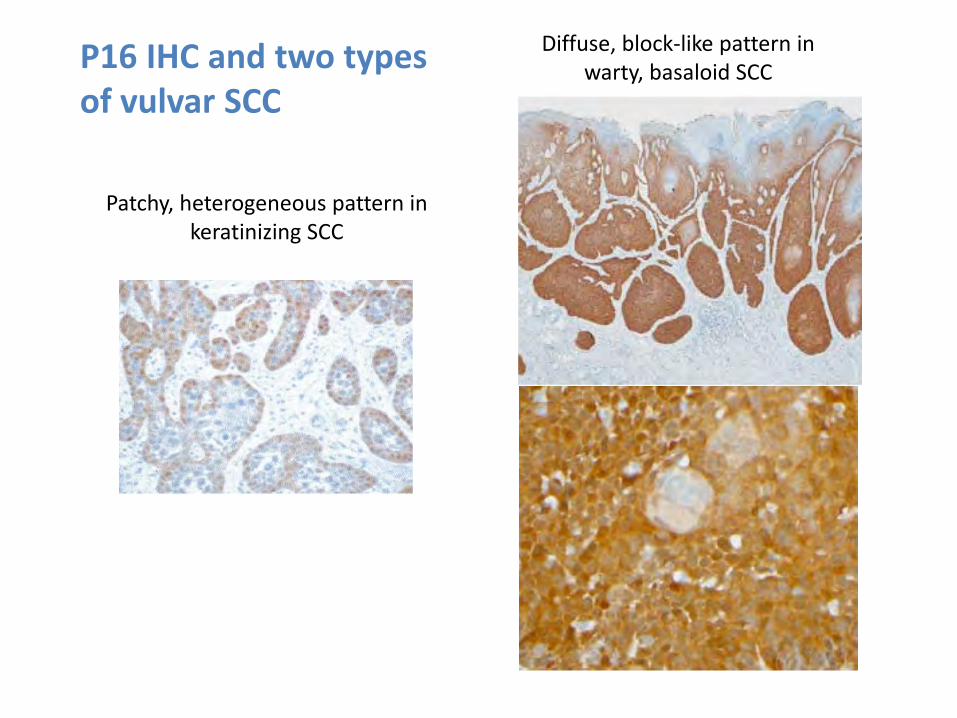
Diffuse, block-like pattern in warty, basaloid SCC
Patchy, heterogeneous pattern in keratinizing SCC
P16 IHC and two types of vulvar SCC
Differentiated (simplex) VIN
• Rarely diagnosed in its pure form• Usually identified adjacent to non-HPV SCC• Older women, often background Lichen
Sclerosus• ?prognostic significance—keratinizing SCC
thought to have a worse prognosis than basaloid variants
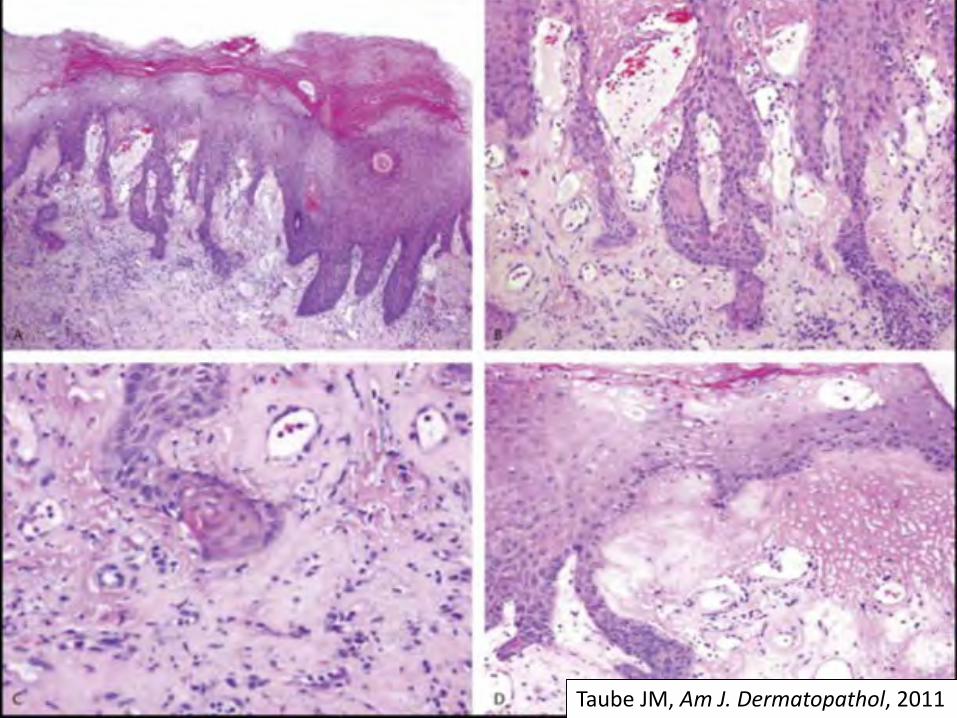
Taube JM, Am J. Dermatopathol, 2011
OverviewVulvovaginal lesions
• Non-Neoplastic– Spongiotic and psorasiform dermatitis– Lichenoid pattern
• lichen sclerosus• lichen amyloid• lichen planus• Zoon’s mucositis/dermatitis
– Verruciform xanthoma• Neoplastic lesions
– Two types of VIN and squamous cell carcinoma• Podophylin-treatment reaction• C0-existing nigh-grade VIN and condyloma
– BCCs of the vulva
Scrotal lesions
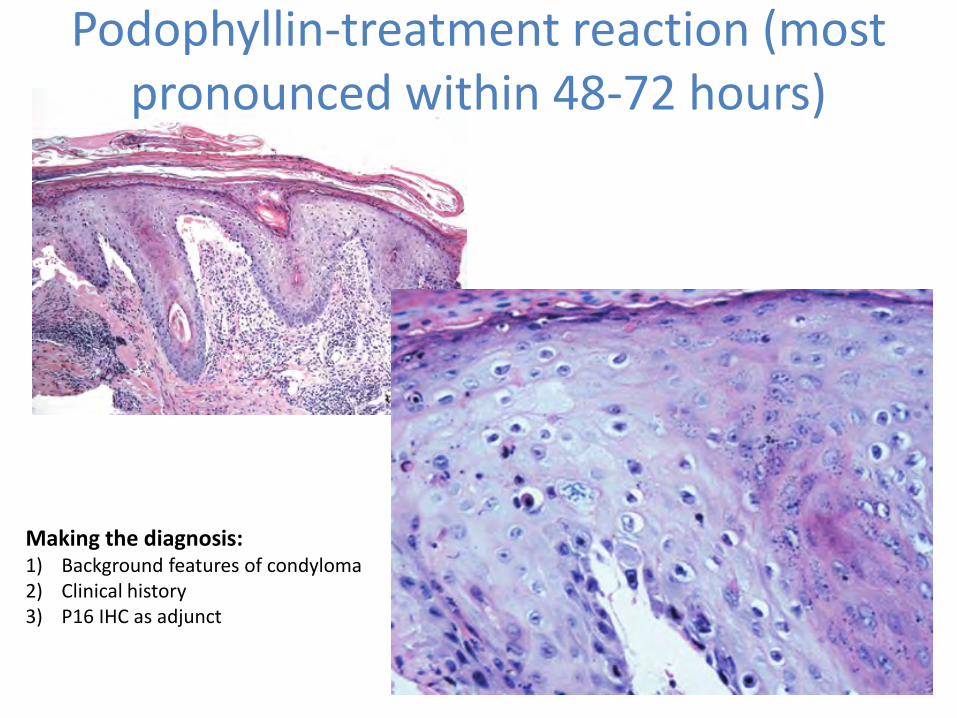
Podophyllin-treatment reaction (most pronounced within 48-72 hours)
Making the diagnosis:1) Background features of condyloma2) Clinical history3) P16 IHC as adjunct
14/14 patients were immunocompromised: 13 had HIV and 1 was transplant patient
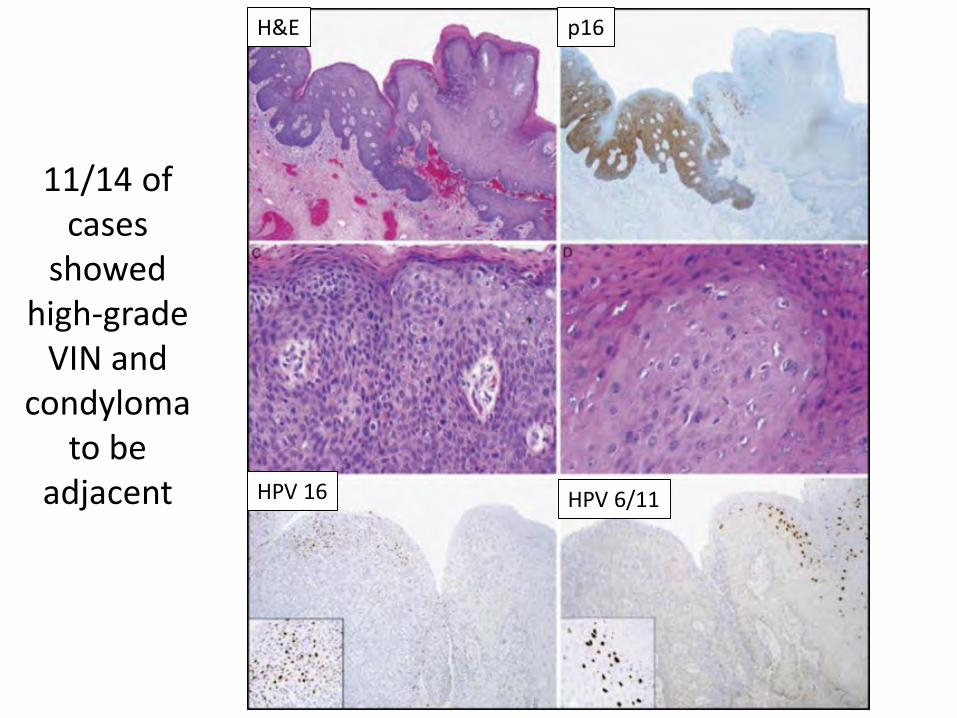
11/14 of cases
showed high-grade
VIN and condyloma
to be adjacent
H&E p16
HPV 6/11HPV 16
H&E p16
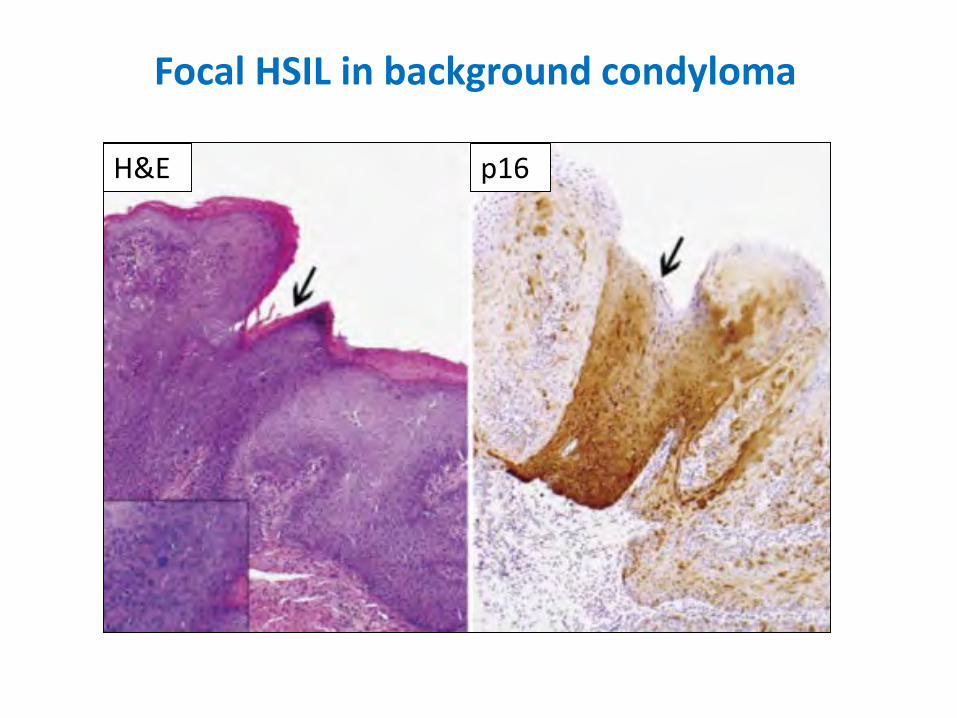
Focal HSIL in background condyloma

HPV-6/11
HPV-16
Focal HSIL in background condyloma
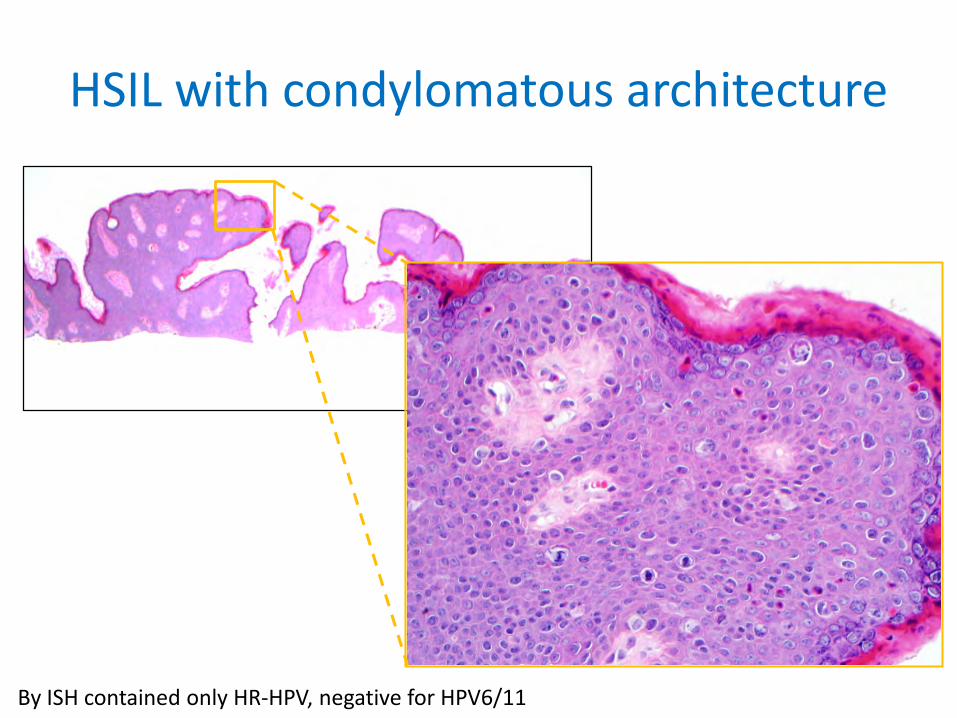
HSIL with condylomatous architecture
By ISH contained only HR-HPV, negative for HPV6/11

Vulvar BCC
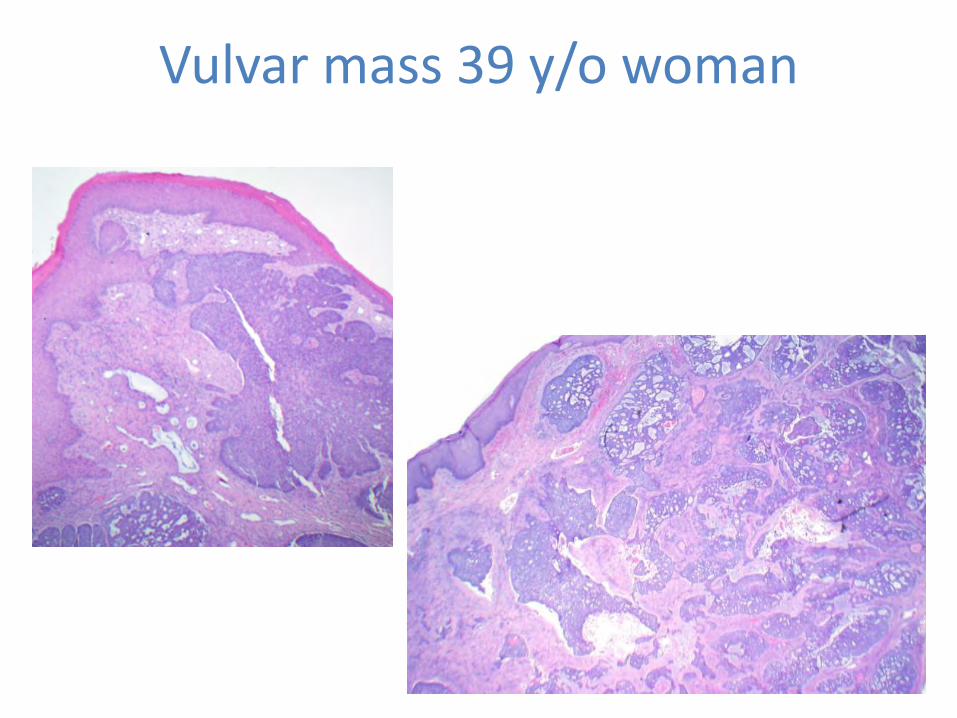
Vulvar mass 39 y/o woman
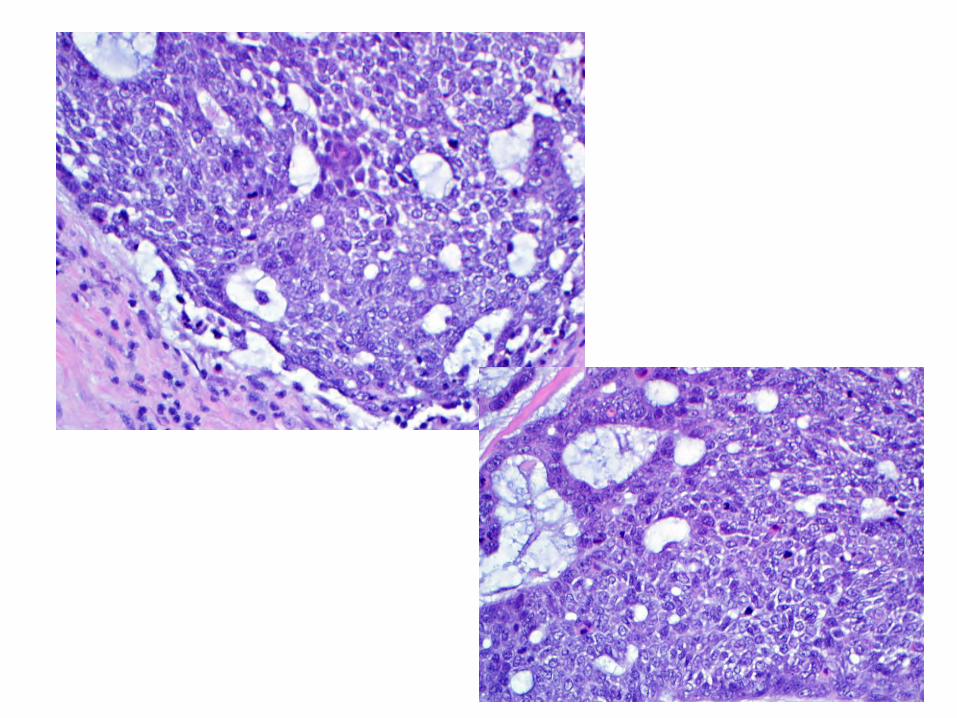
Vulvar BCC
• 3-5% of vulvar malignancies• Not associated with VIN or HPV• May have squamoid areas, and is likely to be
confused with more common HPV-related basaloid SCC
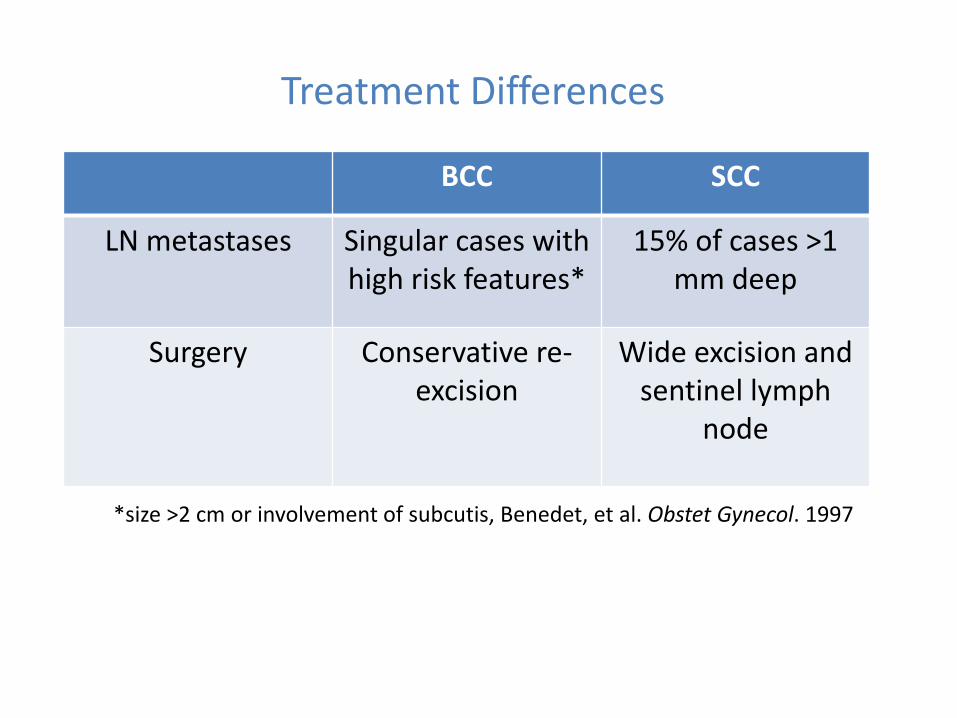
BCC SCC
LN metastases Singular cases with high risk features*
15% of cases >1 mm deep
Surgery Conservative re-excision
Wide excision and sentinel lymph
node
Treatment Differences
*size >2 cm or involvement of subcutis, Benedet, et al. Obstet Gynecol. 1997
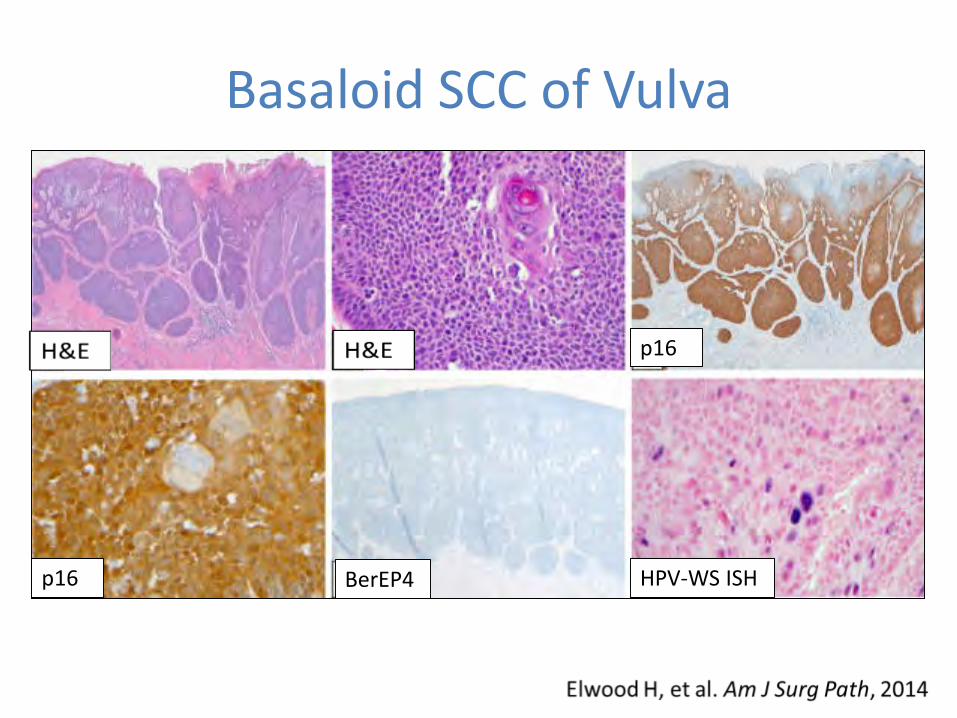
Basaloid SCC of Vulva
p16
p16 BerEP4 HPV-WS ISH
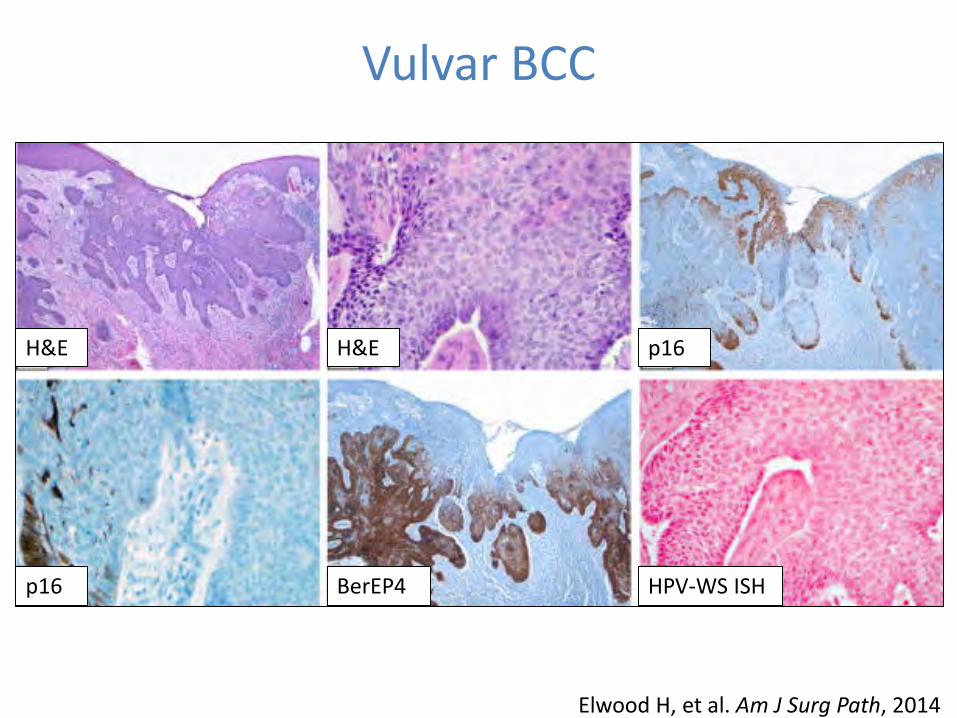
Vulvar BCC
H&E
BerEP4p16
p16H&E
HPV-WS ISH
Elwood H, et al. Am J Surg Path, 2014
OverviewVulvovaginal lesions
• Non-Neoplastic– Spongiotic and psorasiform dermatitis– Lichenoid pattern
• lichen sclerosus• lichen amyloid• lichen planus• Zoon’s mucositis/dermatitis
– Verruciform xanthoma• Neoplastic lesions
– Two types of VIN and squamous cell carcinoma• Podophylin-treatment reaction• C0-existing nigh-grade VIN and condyloma
– BCCs of the vulva
Scrotal lesions
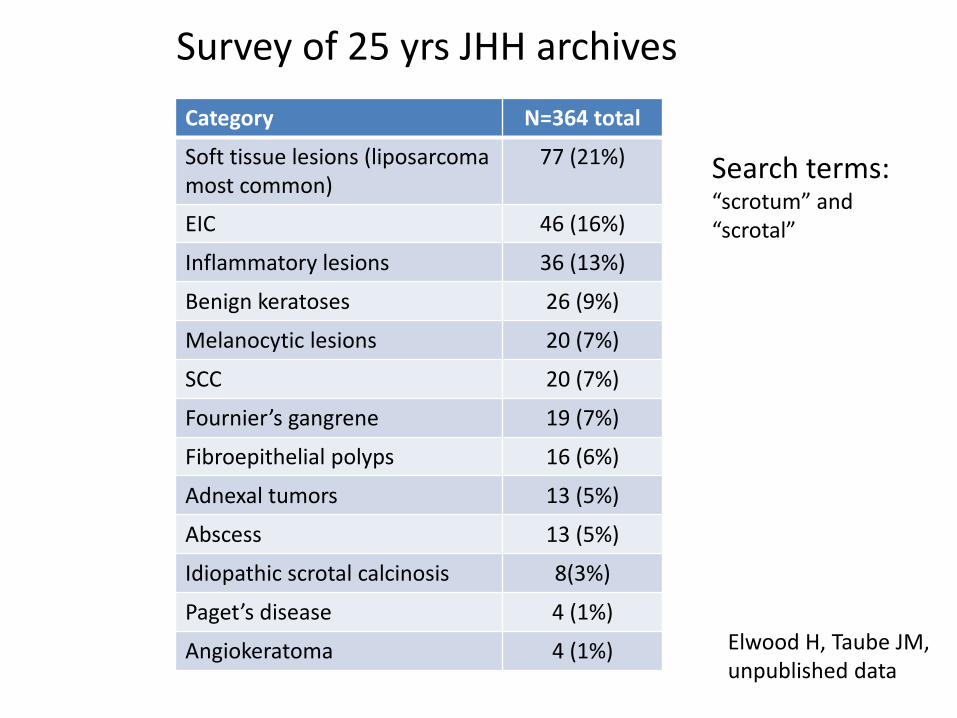
Survey of 25 yrs JHH archivesCategory N=364 total
Soft tissue lesions (liposarcoma most common)
77 (21%)
EIC 46 (16%)
Inflammatory lesions 36 (13%)
Benign keratoses 26 (9%)
Melanocytic lesions 20 (7%)
SCC 20 (7%)
Fournier’s gangrene 19 (7%)
Fibroepithelial polyps 16 (6%)
Adnexal tumors 13 (5%)
Abscess 13 (5%)
Idiopathic scrotal calcinosis 8(3%)
Paget’s disease 4 (1%)
Angiokeratoma 4 (1%)
Search terms: “scrotum” and “scrotal”
Elwood H, Taube JM, unpublished data
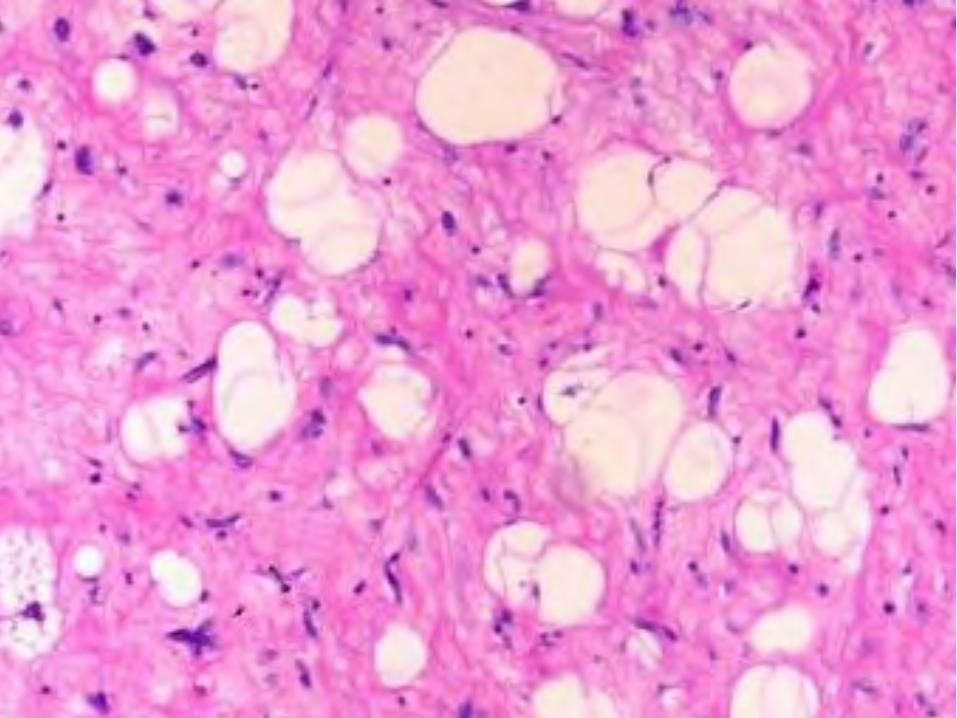
• Majority arise in the spermatic cord and testicular tunics
• Mean age 63 years• Tumors range in size from 3-30 cm• 2/3 are atypical lipomatous tumor/WDL • 1/3 de-differentiated or myxoid/round
cell variant
Liposarcoma
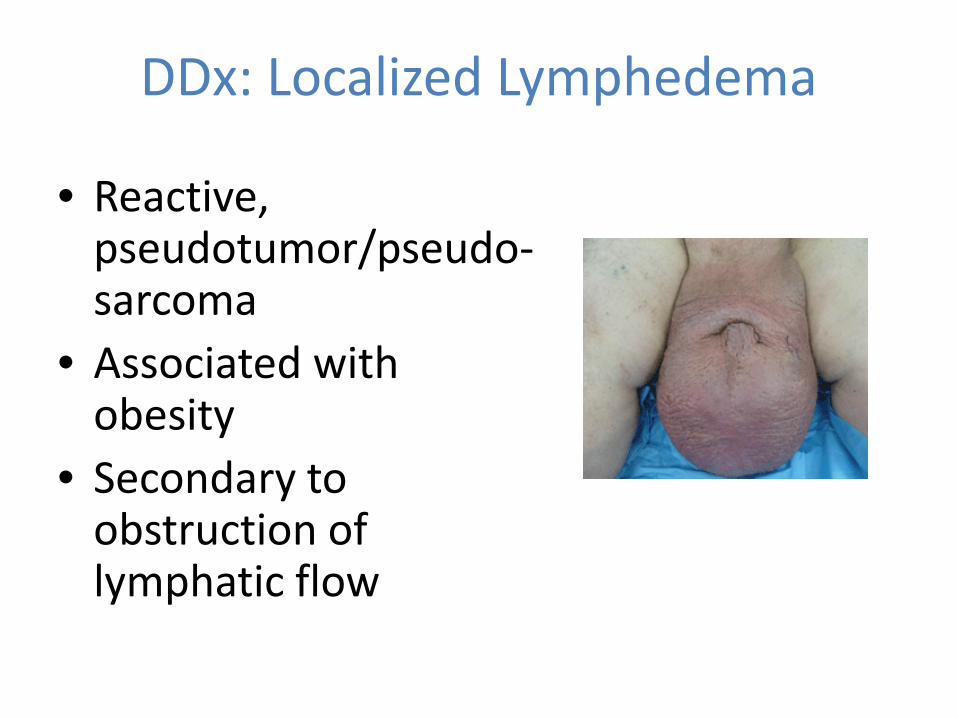
DDx: Localized Lymphedema
• Reactive, pseudotumor/pseudo-sarcoma
• Associated with obesity
• Secondary to obstruction of lymphatic flow

Questions ?
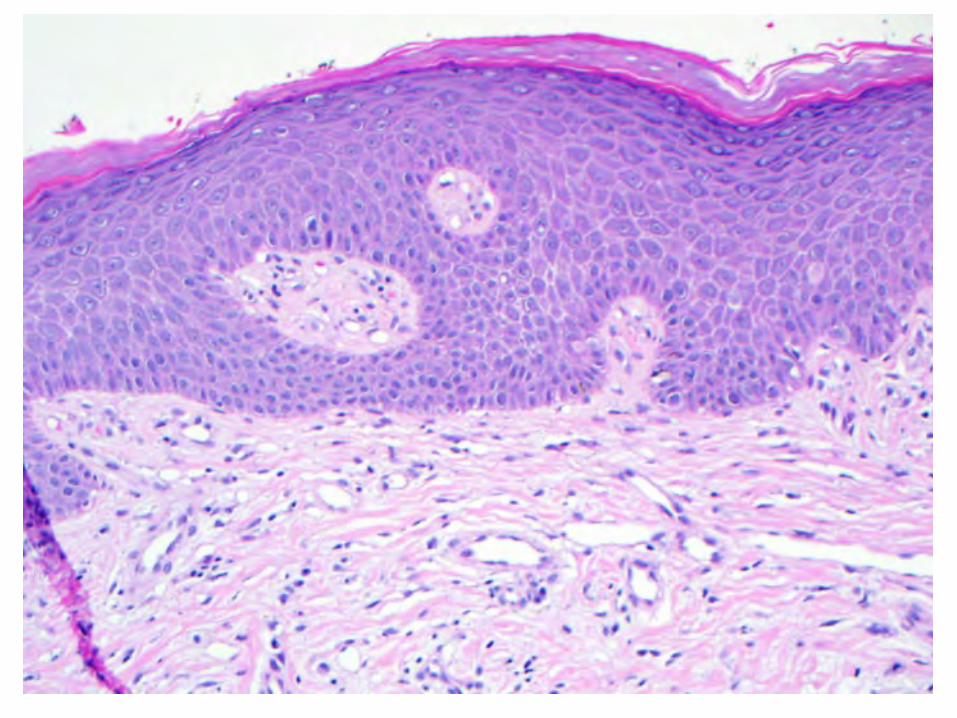
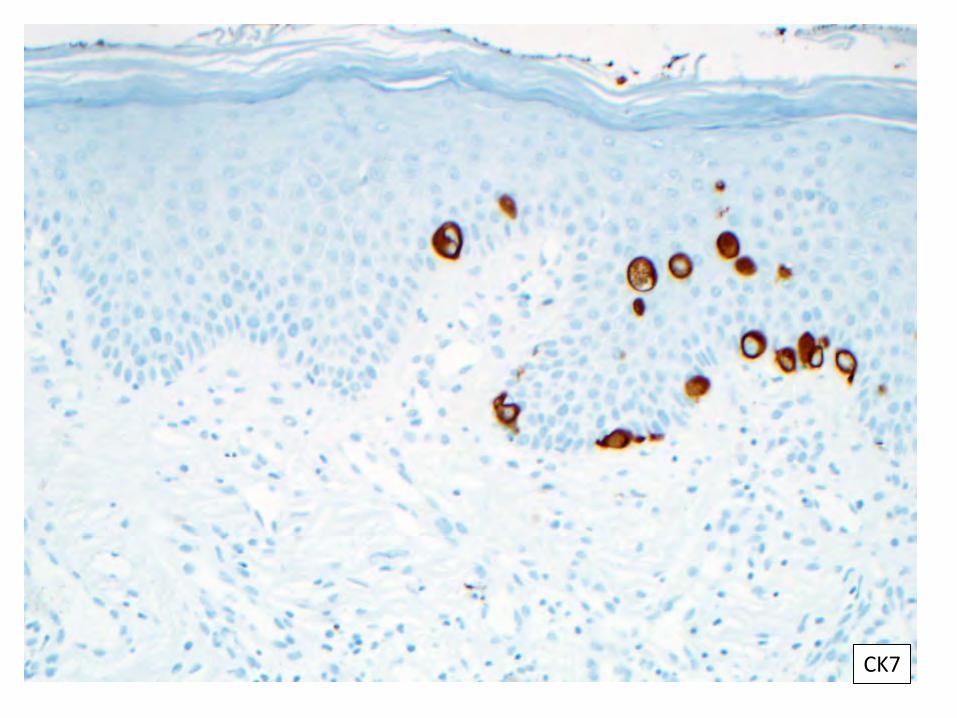
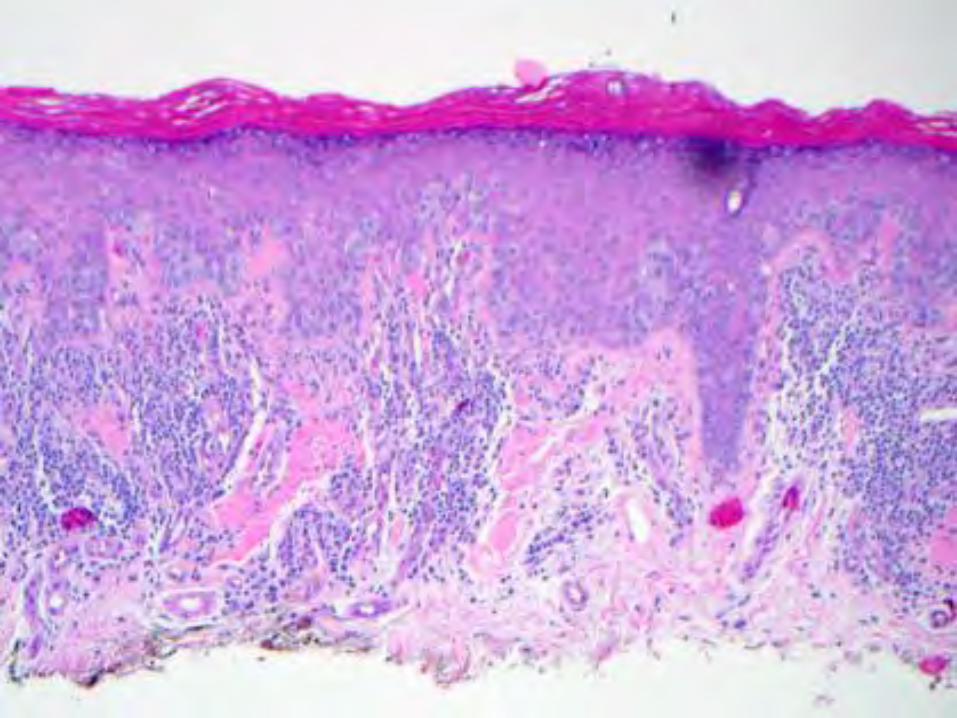
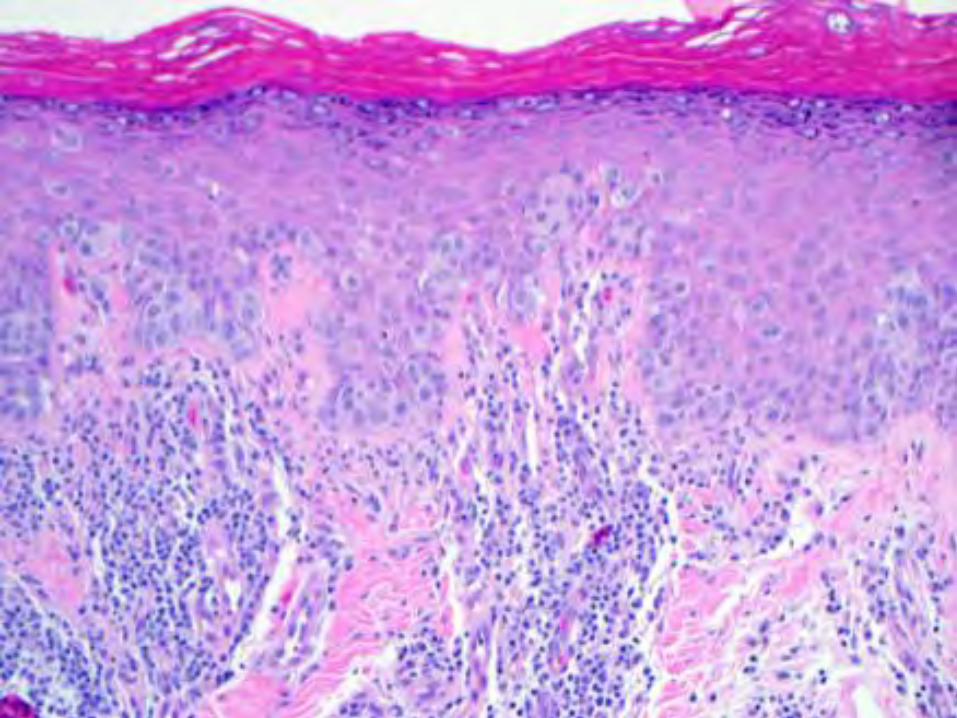
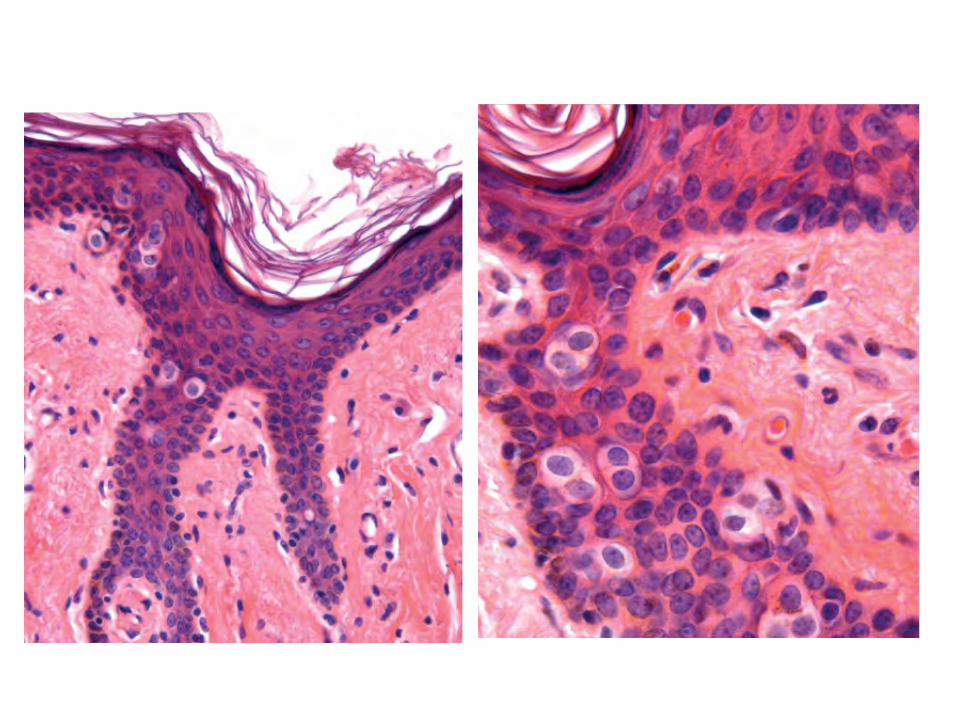
Paget’s disease of the Vulva
• Intraepidermal adenocarcinoma with tumor cells involving the epidermis and sometimes underlying skin adnexal structures
Typically CK7+, CEA+ and Cam5.2+
• The minority are secondary to a carcinoma of the cervix, rectum, or bladder
Immunophenotype reflects underlying primary carcinoma
Primary EMPD Vulva
• 7th decade• Labia majora>labia minora>clitoris• Primary disease is slowly progressive and
rarely metastasizes• Approx 30% of cases have dermal invasion,
prognostic significance unknown
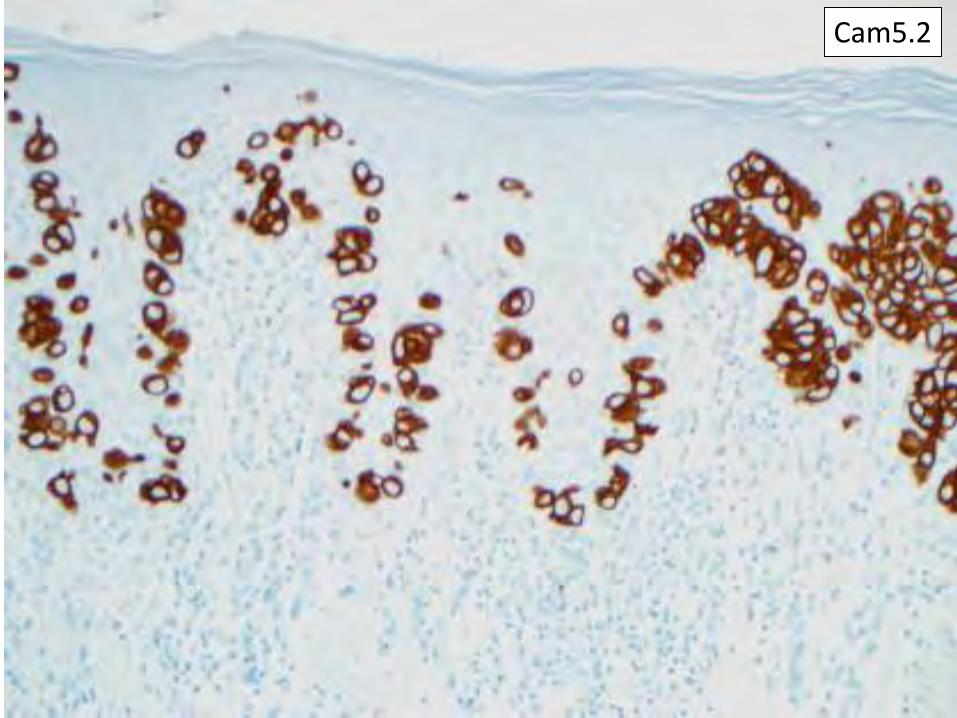
Cam5.2

CK903
OverviewVulvovaginal pathology
• Inflammatory– Spongiotic and psorasiform dermatitis– Lichenoid pattern
• lichen sclerosus• lichen amyloid• lichen planus• Zoon’s mucositis/dermatitis
• In situ and invasive carcinoma – Two types of VIN and squamous cell carcinoma– BCCs of the vulva– Paget’s disease
• Lesions of anogenital mammary-like glands• Miscellaneous
– Verruciform xanthoma
Scrotal lesionsPaget’s disease of the breast

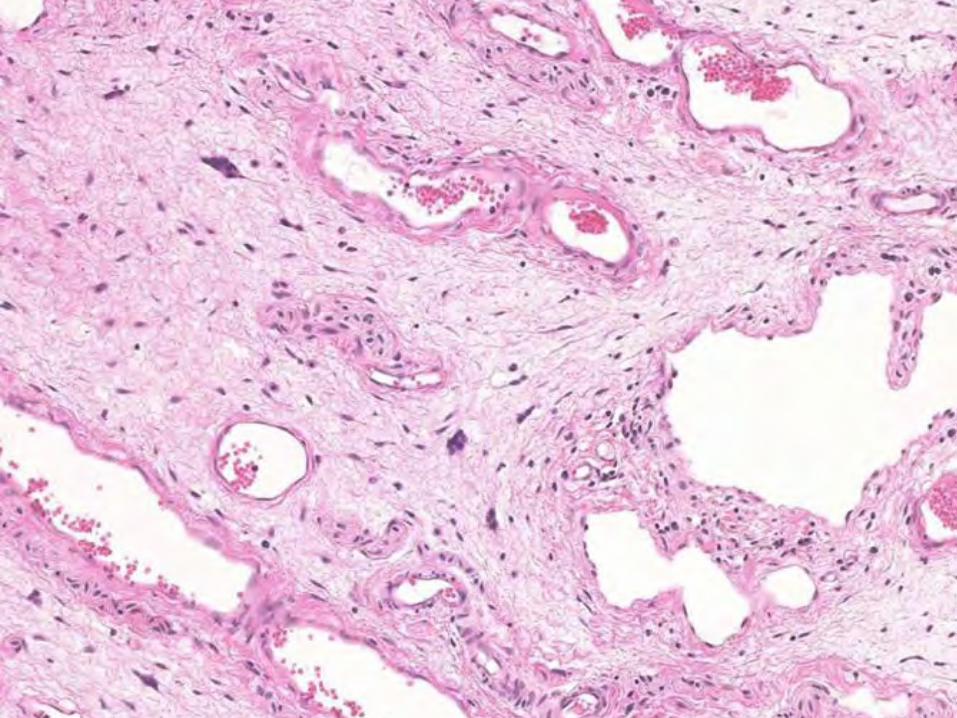
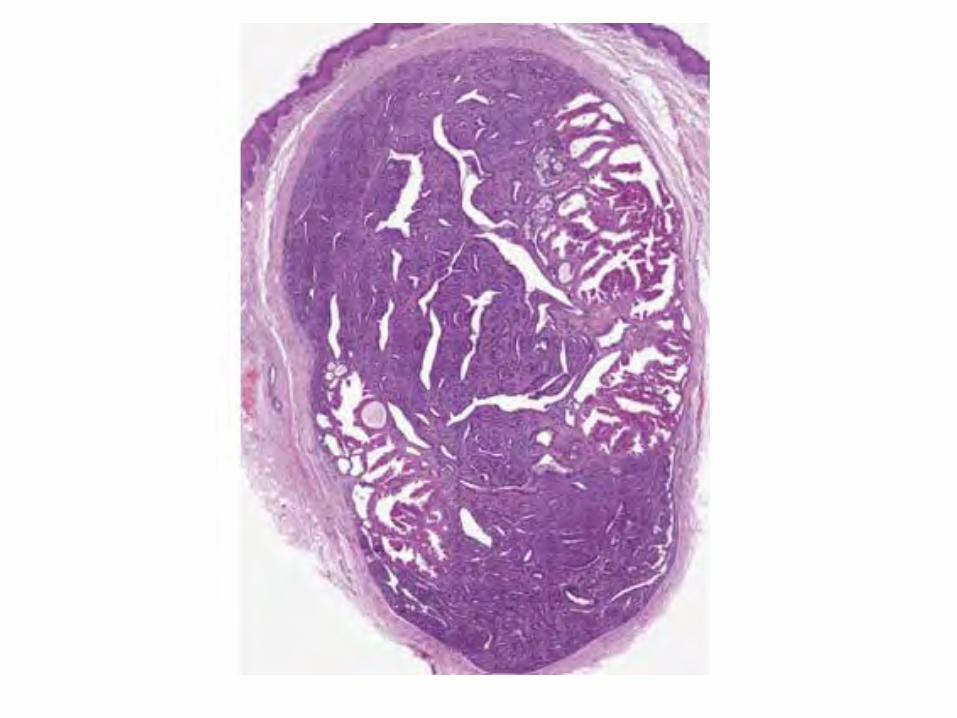
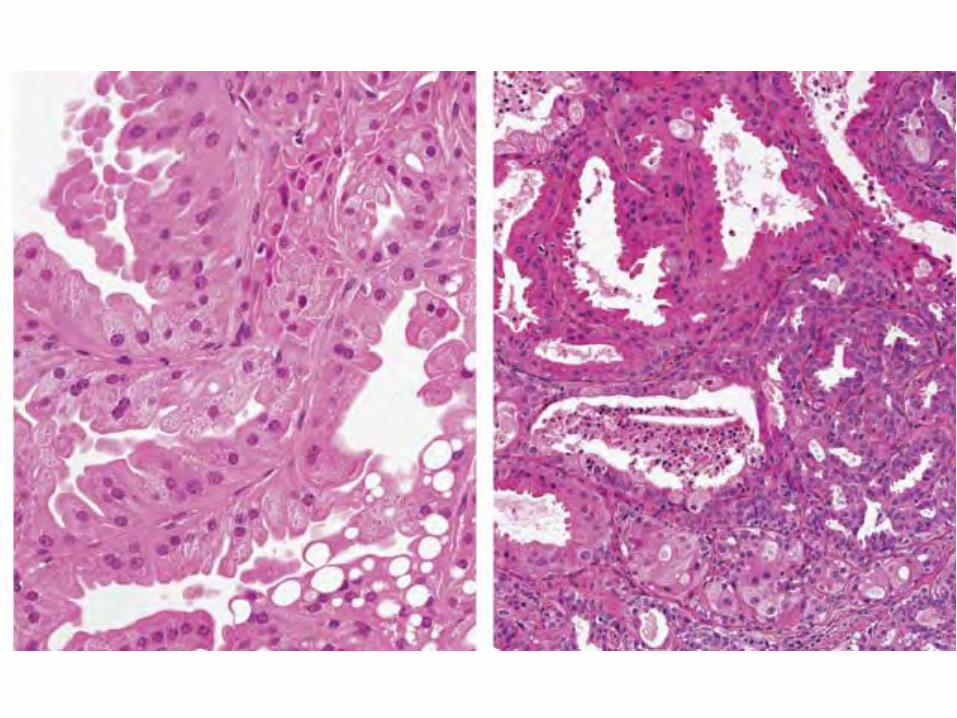
Anogenital mammary-like glands
• Located in sulcus between labia minora and majora
• Normal histology ranges from simple glandular structures to complex lobular units
• Demonstrate changes of sclerosingadenosis, columnar cell change, UDH, ADH, lactating adenoma
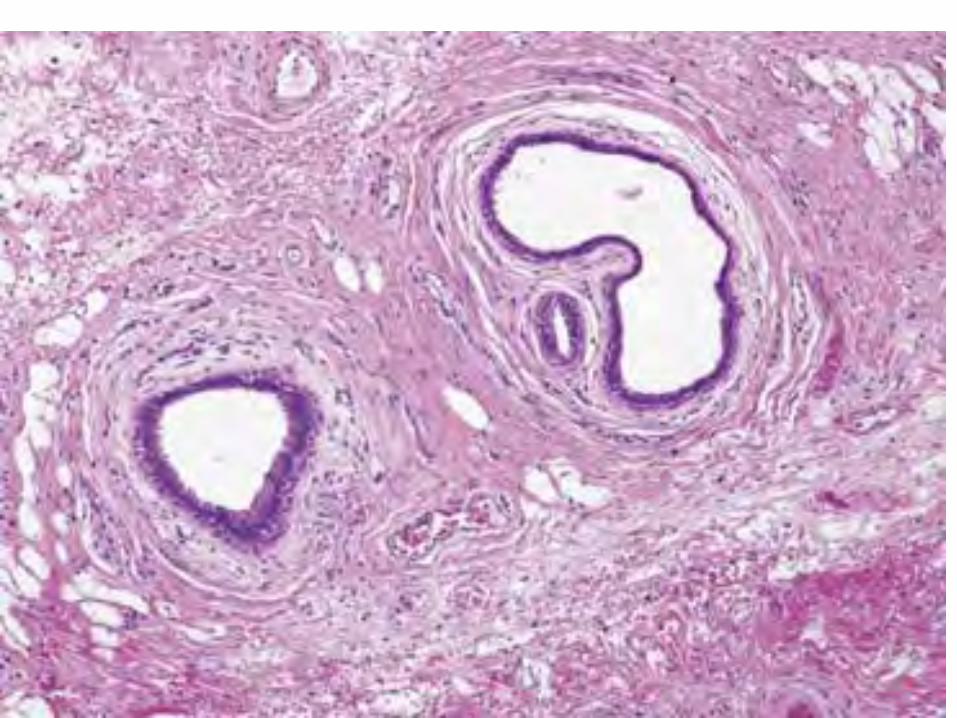
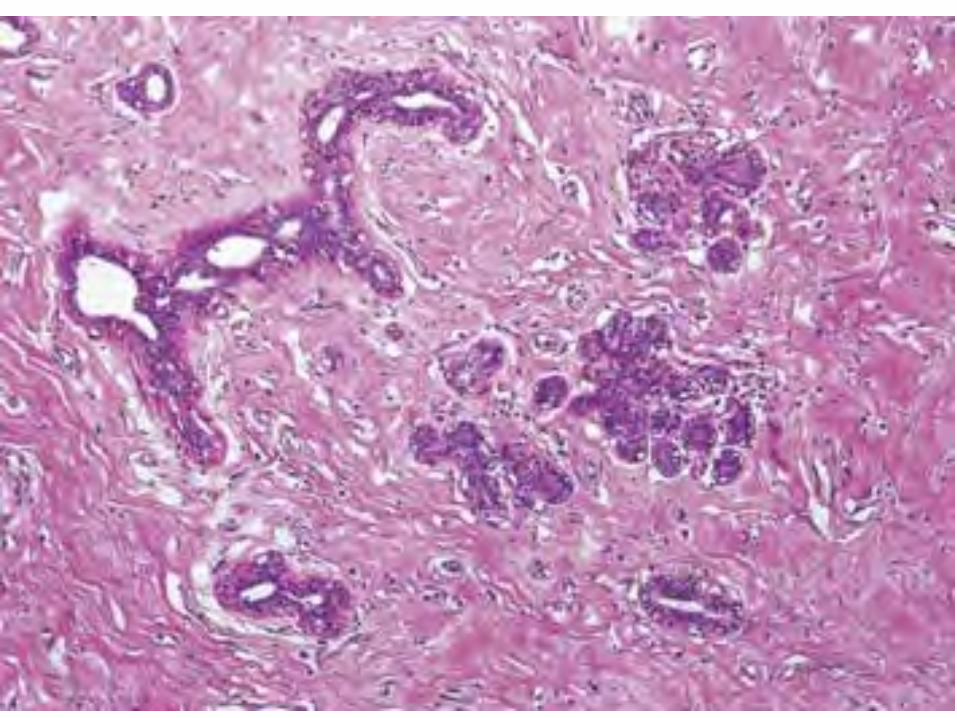
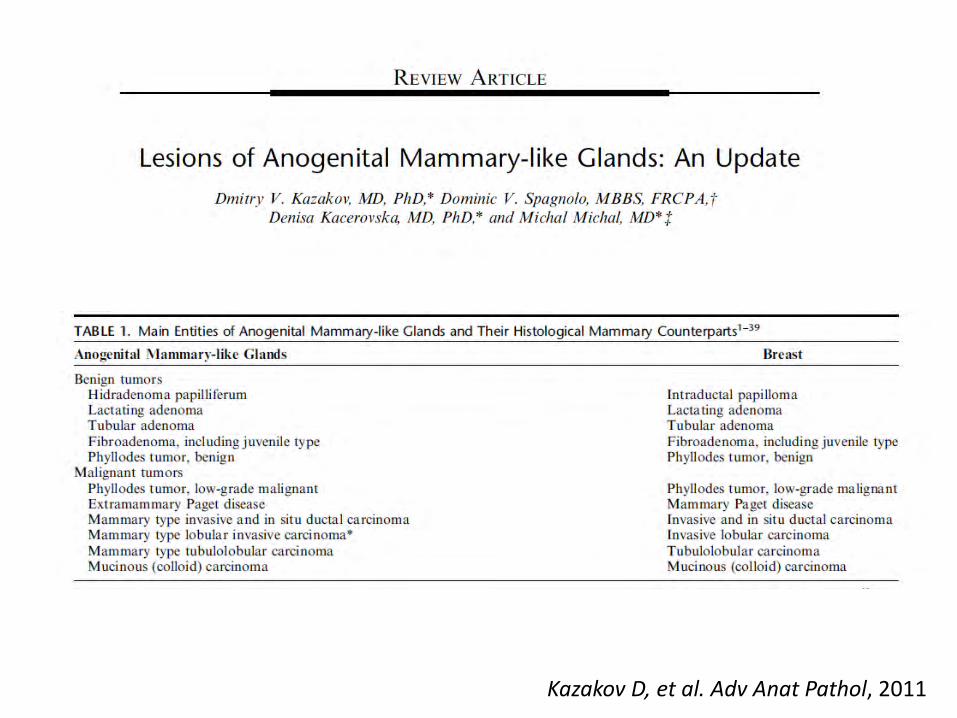
Kazakov D, et al. Adv Anat Pathol, 2011
OverviewVulvovaginal pathology
• Inflammatory– Spongiotic and psorasiform dermatitis– Lichenoid pattern
• lichen sclerosus• lichen amyloid• lichen planus• Zoon’s mucositis/dermatitis
• In situ and invasive carcinoma – Two types of VIN and squamous cell carcinoma– BCCs of the vulva– Paget’s disease
• Lesions of anogenital mammary-like glands• Miscellaneous
– Verruciform xanthoma
Scrotal lesionsPaget’s disease of the breast
OverviewVulvovaginal pathology
• Inflammatory– Spongiotic and psorasiform dermatitis– Lichenoid pattern
• lichen sclerosus• lichen amyloid• lichen planus• Zoon’s mucositis/dermatitis
• In situ and invasive carcinoma – Two types of VIN and squamous cell carcinoma– BCCs of the vulva– Paget’s disease
• Lesions of anogenital mammary-like glands• Miscellaneous
– Verruciform xanthoma
Scrotal lesionsPaget’s disease of the breast
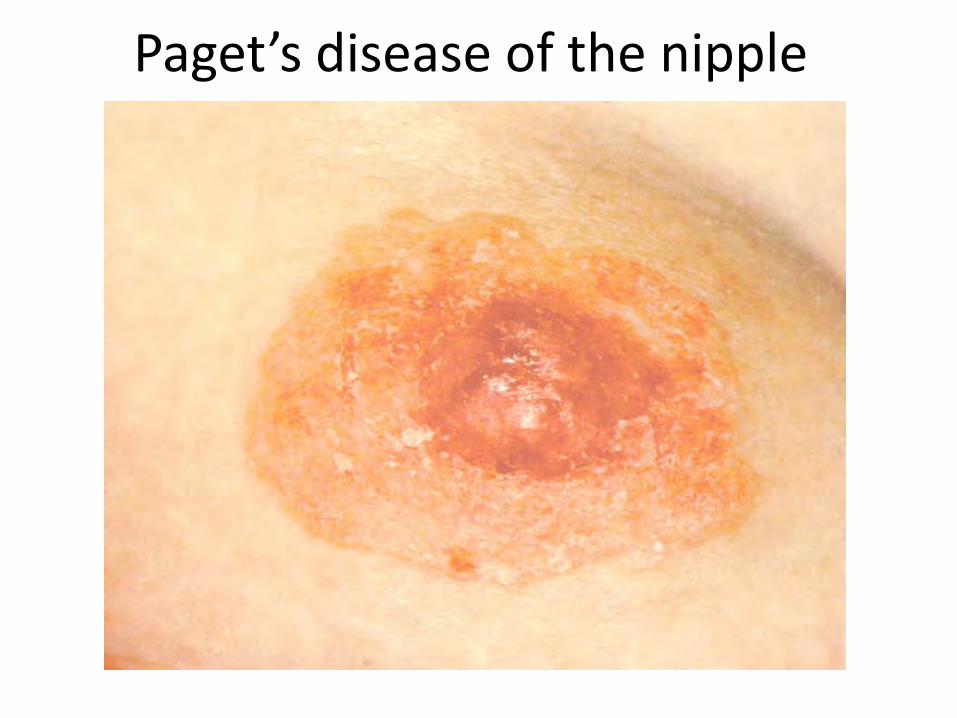
Paget’s disease of the nipple
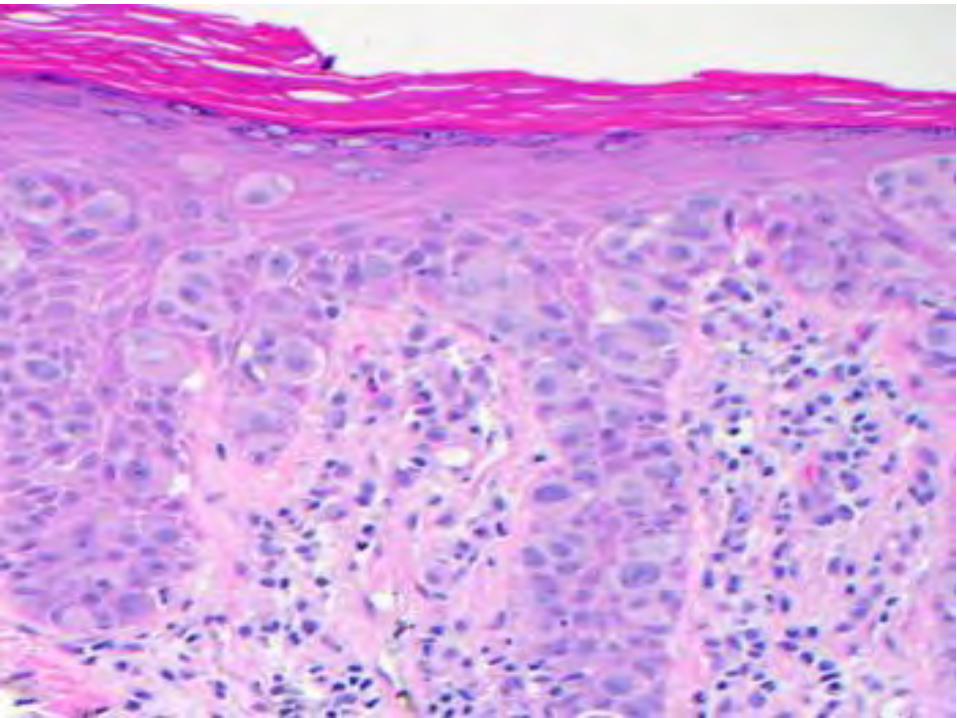
• Approx 5% of Paget’s cases have dermal invasion• No correlation with increasing tumor stage of underlying breast carcinoma• Depth of invasion measured from DEJ• Clinical significance is unclear, thus patients are managed according to the
underlying carcinoma
Am J Surg Path, 2014
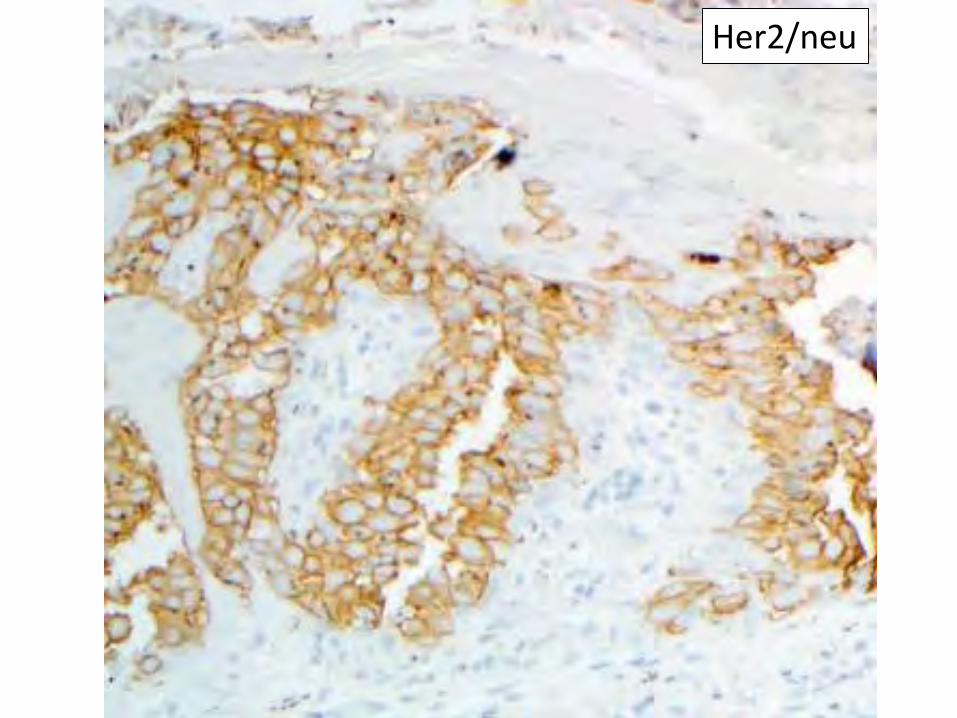
Her2/neu
• Found in normal epidermis of nipple (seen in 10% of patients on routine stains, 80% of patients with CK7).
• Usually found at opening of lactiferous ducts.• Bland cells with condensed chromatin. Lack
prominent nucleoli. • HER2/neu negative.
DDx: Toker cell hyperplasia
Garijo, MF, et al. Histol Histopathol, 2009
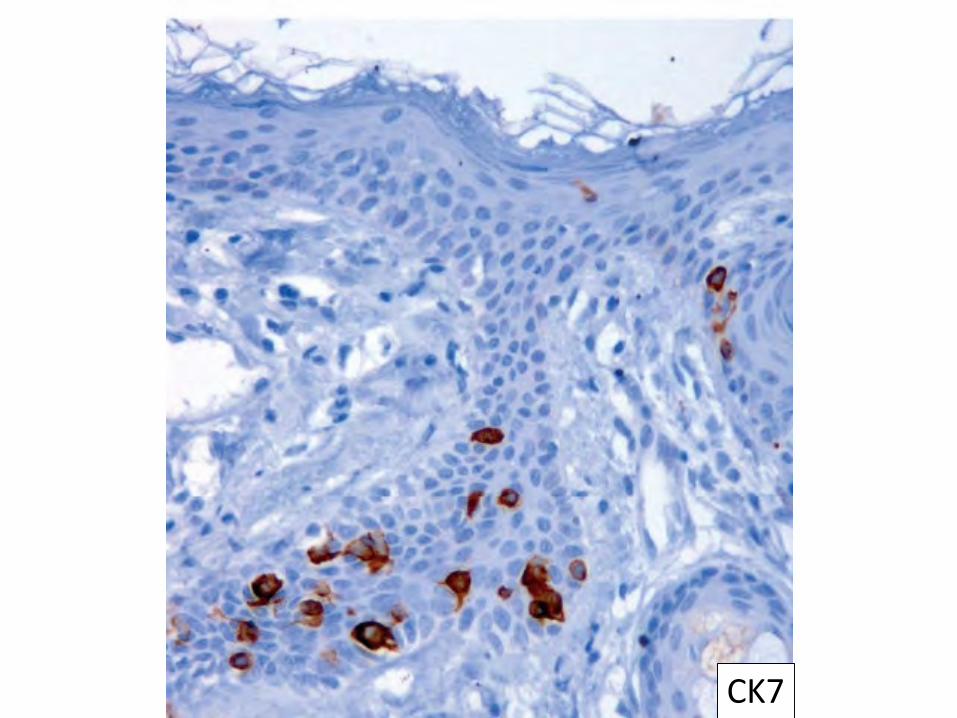
CK7
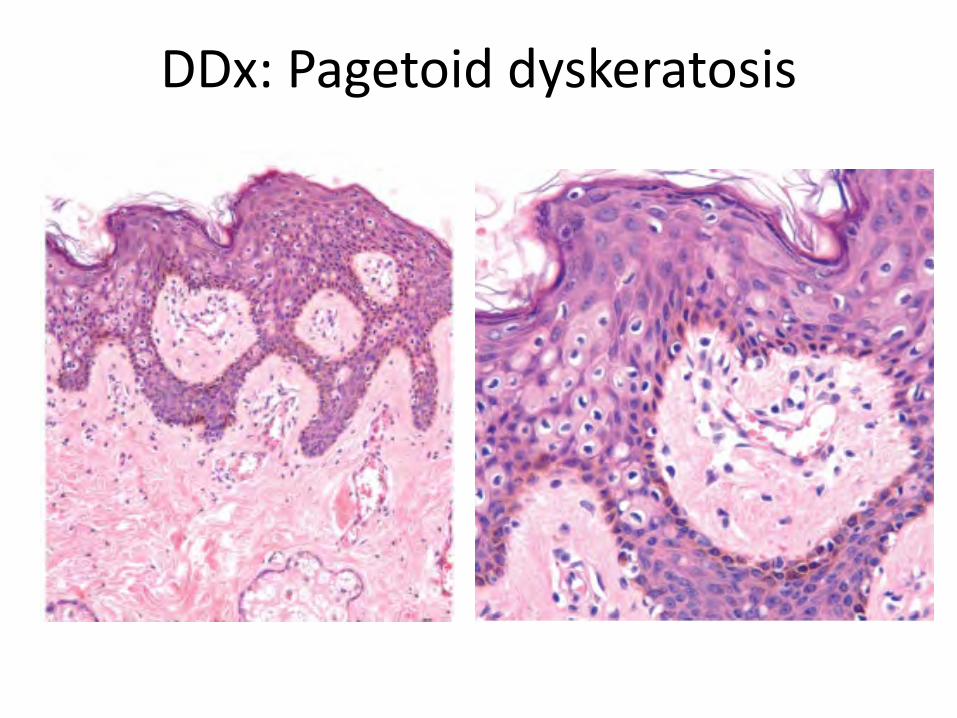
DDx: Pagetoid dyskeratosis
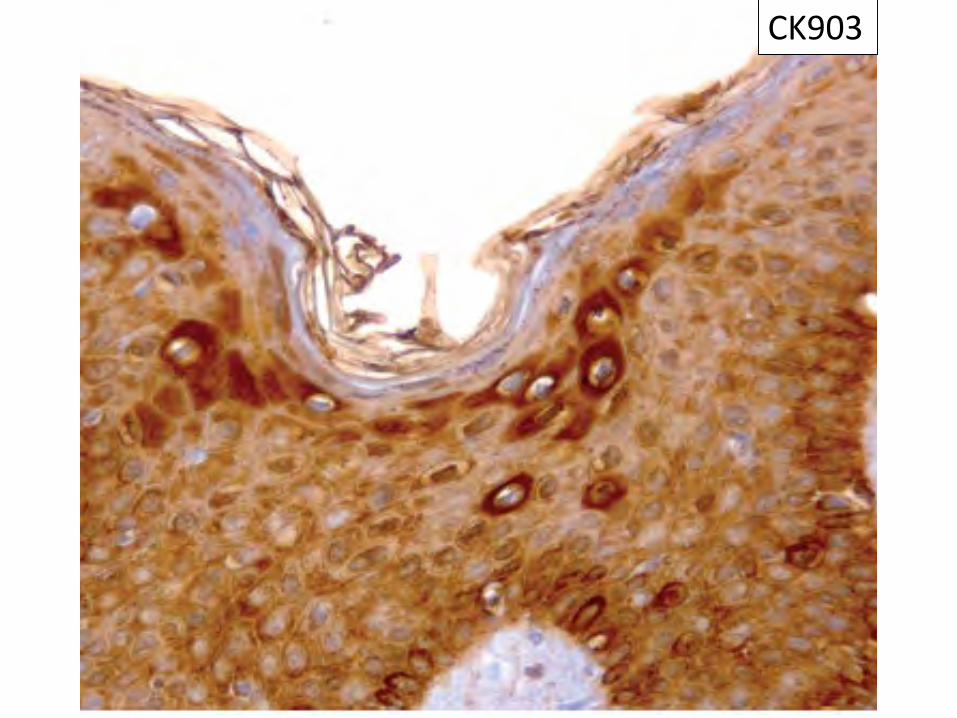
CK903
Proposal for reclassification of VIN
• DVIN-not graded• Current WHO: Classic VIN is graded I, II, and III
(like CIN)– CINI > CINIII– VIN1<VINIII
• ISSVD proposed VIN I category dropped, and combining VINII and VINIII– VINI is not reproducible, natural history unknown– VINII and VINIII no treatment difference