
REGULAR ARTICLE
Clinical and biological parameters in 166 boys, adolescents and adults withnonmosaic Klinefelter syndrome: a Copenhagen experienceLise Aksglæde ([email protected]), Niels E Skakkebæk, Kristian Almstrup, Anders JuulUniversity Department of Growth and Reproduction, Rigshospitalet, Copenhagen, Denmark
KeywordsGrowth, Klinefelter syndrome, Reproduction
CorrespondenceLise Aksglæde, Department of Growth and Repro-duction, Rigshospitalet, Section 5064, Blegdamsvej9, DK-2100 Copenhagen Ø, Denmark.Tel: +45 3545 5085 |Fax: +45 3545 6054 |Email: [email protected]
Received22 November 2010; revised 5 February 2011;accepted 24 February 2011.
DOI:10.1111/j.1651-2227.2011.02246.x
ABSTRACTAim: Klinefelter syndrome (KS) is the most frequent sex chromosome disorder in
males, but the phenotype varies greatly and is therefore highly under-diagnosed. We aimed
at describing the phenotypic characteristics throughout life from clinical follow-up of our
large cohort of patients with KS.Methods: A retrospective observational study of 166 males with nonmosaic 47,XXY
KS aged 0.3–80.3 years. Data on phenotype, growth, body composition, bone mineral
density, sex hormones, lipids, glycosylated haemoglobin (HbA1C) and prostate-specific
antigen were recorded. In addition, histological examination of testicular biopsies from 29
patients was performed.Results: Patients with Klinefelter were taller already in childhood. All patients had
smaller testicular volume and elevated luteinizing hormone (LH) and follicle-stimulating
hormone levels in adulthood. Cryptorchidism was reported in 14%, gynaecomastia in
44%, and 36% required speech therapy or educational support. The abnormal biochemi-
cal parameters became evident after onset of puberty and correlated with histological find-
ings of a gradual deterioration of seminiferous tubules and massive Leydig cell hyperplasia
in adults.Conclusion: Our patients presented with a wide spectrum of the classical Klinefelter
symptoms. In adulthood, two features were consistently present in every patient: small tes-
tes and high LH ⁄ testosterone ratio, often despite normal testosterone levels. Such bio-
chemical parameters combined with small testes should lead to a suspicion of KS.
INTRODUCTIONKlinefelter syndrome (KS) is the most frequent sex chromo-some disorder in the male affecting 1:660 newborn boys (1).The majority of affected males carry an additional X chro-mosome, 47,XXY, while the remaining have higher-gradeaneuploidies (e.g. 48,XXXY) or mosaic forms. The rareKlinefelter variant, the SRY-positive 46,XX-male, occurswith a prevalence of one in 20 000–25 000 males (2).
Adolescent and adult patients with KS are characterizedby the constellation of tall stature with eunuchoid body pro-portions, small, firm testes and androgen deficiency,whereas no specific clinical or physical hallmarks have beenidentified at birth or during infancy and childhood.
However, the adult phenotype varies greatly, and the symp-toms of KS are not exclusive, and possibly therefore, thesyndrome is highly under-diagnosed. In Denmark, <10% ofthe expected number of boys is diagnosed before puberty,and only approximately 25% of adult males with KS arediagnosed (1).
The clinical workup for patients with KS varies greatlyfrom country to country and even within countries. Thereare so far e.g. no international guidelines for clinical workupor for hormone replacement therapy. The aim of this studywas to revisit information obtained by follow-up of the pop-ulation of patients with KS in our endocrine outpatientclinic and to generate specific characteristics of patientswith KS to facilitate the diagnosis of this relative common,but frequently overlooked, syndrome at a younger age tofacilitate earlier preventive interventions.
METHODSStudy populationA total of 196 patients with KS (nonmosaic 47,XXY,mosaic, 48,XXXY, 48,XXYY and SRY-positive 46,XX-male)
Abbreviations
E2, estradiol; FSH, follicle-stimulating hormone; HbA1C, glycosy-lated haemoglobin; HDL, high-density lipoprotein; KS, Klinefel-ter syndrome; LDL, low-density lipoprotein; LH, luteinizinghormone; PSA, prostate-specific antigen; SDS, standard deviationscore; SHBG, sex hormone-binding globulin; T, testosterone; TG,triglyceride.
Acta Pædiatrica ISSN 0803–5253
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806 793

aged 0–80.3 years were followed in our endocrine outpa-tient clinic during the years 1990–2010. The distribution ofpatients according to karyotype and reason for diagnosis isshown in Table 1. Only patients with nonmosaic 47,XXYKS (n = 166) were included in this retrospective, observa-tional study.
Chromosome analysis was performed on peripheral bloodlymphocytes in each case, and a prenatal karyotype was con-firmed on a postnatal blood sample. Karyotypes were estab-lished on 30 metaphases from each patient. All XX-maleswere SRY-positive (detected by polymerase chain reaction).
Clinical examinationAll patients were followed regularly from the time of diag-nosis. If possible, the child was seen at the age of 3 monthsduring the infantile mini-puberty, and thereafter the chil-dren were seen yearly until the time of expected puberty.From the age of 9–12 years, the clinical visits were more fre-quent with quarterly clinical and biochemical evaluation. Inadulthood, patients were seen at yearly visits.
The clinical examination included height, weight andpubertal staging according to Tanner at every visit duringchildhood and adolescence, and at the first visit in adult-hood. Testicular volume was estimated by Prader’s orchi-dometer. If the sizes of the two testes were not identical, thelarger was chosen to determine testicular volume. Onset ofpuberty was defined as a testicular volume ‡4 mL.
Dual energy X-ray absorptiometry (DEXA) scansAs part of clinical practice, many patients underwent regu-lar DEXA scans. Whole body scans were performed in chil-dren and adolescents using a Hologic 1000 ⁄ W scanner(Hologic, Inc., Waltham, MA, USA) as previously described(3), but not presented here. In adults, bone mineral density(BMD) at the level of the hip and spine was evaluated byDEXA scans (XR-46; Norland Medical Systems, Inc., FortAtkinson, WI, USA, or Lunar Prodegy GE Medical Systems,Madison, WI, USA).
Laboratory analysisNonfasting blood samples were drawn from an antecubitalvein, clotted and centrifuged. Serum follicle-stimulating hor-mone (FSH) and luteinizing hormone (LH) were measuredby time-resolved immunofluorometric assays (Delfia; Perk-inElmer, Boston, MA, USA) with detection limits of 0.05and 0.06 IU ⁄ L for FSH and LH, respectively. Intra- and in-terassay Coefficient of variation (CVs) were <5% in bothassays. Testosterone (T) was measured with the DPC Coat-A-Count radioimmuno assay kit (Diagnostic Products, LosAngeles, CA, USA). The detection limit was 0.23 nmol ⁄ L,and the intra- and interassay CVs were 7.6% and 8.6%,respectively. Estradiol (E2) was measured by radioimmunoassay (Pantex, Santa Monica, CA, USA). The detection limitwas 18 pmol ⁄ L; the intra- and interassay CVs were <8% and13%, respectively. Sex hormone-binding globulin (SHBG)was determined by a time-resolved immunofluorescenceassay (Delfia; Wallac Oy, Turku, Finland) with a detectionlimit of 0.20 nmol ⁄ L. Intra- and interassay CVs were 5.8%and 6.4%, respectively. Serum inhibin B was measured by aspecific ELISA kit (Oxford Bio Innovation, Oxford, UK)with detection limit of 20 pg ⁄ mL. Intra- and interassay CVswere <13% and 19%, respectively.
Cholesterol, low-density lipoprotein (LDL), high-densitylipoprotein (HDL), triglyceride (TG) and glucose were mea-sured by Modular Analytics Clinical Chemistry System(Roche Diagnostics, Mannheim, Germany). Glycosylatedhaemoglobin (HbA1C) was measured by liquid chromatog-raphy absorption photometry. Prostate-specific antigen(PSA) was measured by sandwich electrochemilumines-cence immunoassay (ECLIA).
Testicular histologyTesticular biopsies from 29 patients with KS at differentages were available in the archives of our histology labora-tory and were re-evaluated. Some of these data have previ-ously been published (4,5). Various histochemical stainswere applied to sections of fixed biopsies and included
Table 1 Number of patients and reason for diagnosis
Non-mosaic 47,XXYn = 166*
Mosaicn = 10**
48,XXXY and 48,XXYYn = 5***
SRY-positive XX-malen = 15****
Prenatal 30 (20%) 3 (38%) None 3 (21%)
Childhood ⁄ adolescence 52 (35%) 3 (38%) 2 (50%) 5 (36%)
Abnormal growth 3 – 1 2
Phenotype 11 – – –
Delayed puberty 5 1 – –
Gynecomastia 7 – – –
Other 26 2 1 3
Adulthood 68 (45%) 2 (25%) 2 (50%) 6 (43%)
Infertility 46 2 – 5
Phenotype 6 – – –
Gynecomastia 5 – – –
Osteoporosis 1 – – –
Other 10 – 2 1
Data on reason for diagnosis available in *150 (90%), **8 (80%),***4 (80%), ****14 (93%) subjects.
Klinefelter syndrome throughout life Aksglæde et al.
794 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806

haematoxylin and eosin (H&E), periodic acid-Schiff (PAS),Masson Trichrom and martius–scarlet–blue (MSB). Testicu-lar histology was evaluated by three independent trainedobservers (NES, KA, AJ). Only nonmosaic 47,XXY karyo-types was evaluated here.
Normal pubertal and childhood samples were obtainedfrom archives of testicular tissue from boys who were trea-ted for ALL and therefore were routinely screened for lym-phoblastic infiltration (6). Foetal samples were obtainedfrom archives of testicular tissue from spontaneous abor-tions ⁄ miscarriages and adult samples from archives of tes-ticular tissue from men in infertility workup but withnormal spermatogenesis.
EthicsAll Klinefelter subjects and their parents (when the patientwas <18 years of age) gave informed consent for clinicaland biochemical follow-up. Data from routine clinical visitswere obtained from patient files and used for this study.Registration of clinical data was approved by the DanishData Protection Agency (2005-41-5479).
StatisticsClinical and biochemical characteristics are provided asunadjusted median and range if not otherwise indicated.Comparison between untreated and treated patients withKS was made with a Mann–Whitney U-test. BMD T-scoreswere statistically compared with zero using the one-samplet-test. Associations between sex hormones and BMD weretested with Spearman’s rank correlation coefficient. All sta-tistical analyses were carried out using the statistical soft-ware SPSS (version 18; SPSS, Inc., Chicago, IL, USA).
RESULTSStudy populationA total of 166 patients had a nonmosaic 47,XXY karyotype,whereas the remaining 30 had higher-grade aneuploidies ormosaicisms (Table 1); 20% of the nonmosaic 47,XXYpatients were diagnosed prenatally. The majority of the non-mosaic 47,XXY patients were diagnosed in adulthood aspart of the clinical workup for infertility (Table 1). Medianage at diagnosis in adulthood was 29 years (range 18–57 years) and in childhood ⁄ adolescence 14 years (range0.25–17 years) [data available in 115 (95.8%) of the postna-tally diagnosed patients].
Comorbidities were reported in 57 patients (Table 2). Thepatient with achondroplasia (heterozygous for the classical1138G>A mutation in the fibroblast growth factor receptor3 (FGFR3) gene) was excluded from the analysis because ofan atypical presentation with motile sperms in the ejaculateand reproductive hormones within the normal range as pre-viously described (7).
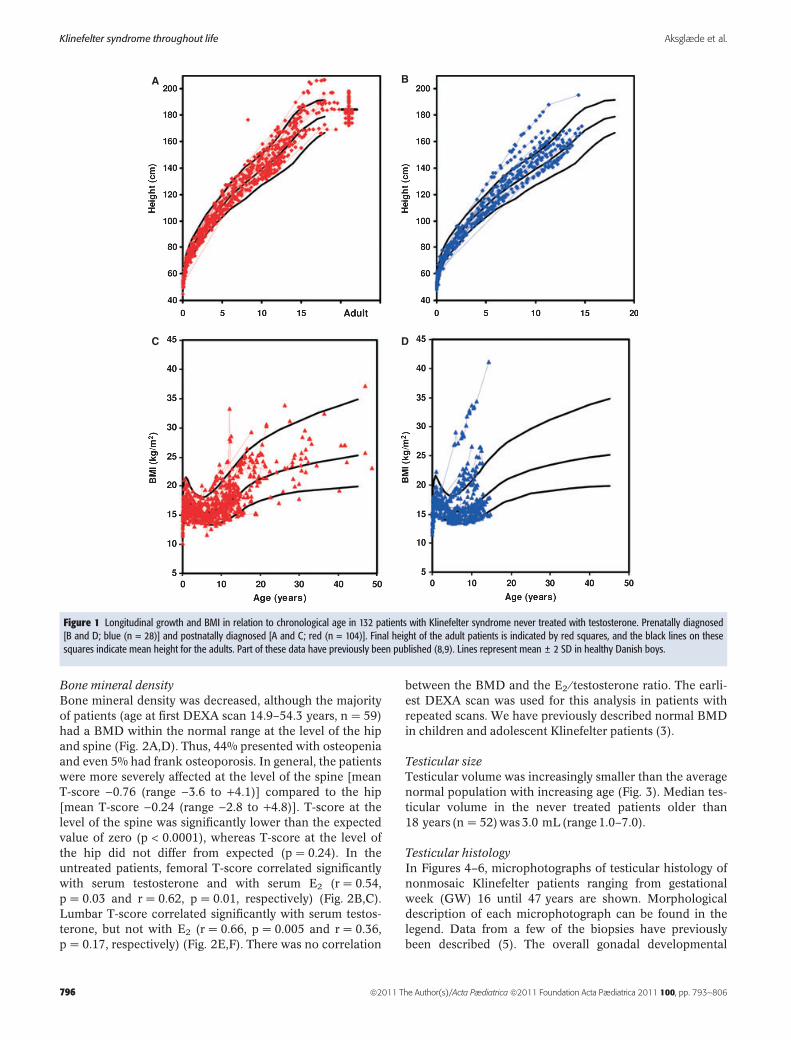
PhenotypeGrowthThe majority of patients exhibited accelerated growthalready from early childhood (Fig. 1A,B). This phenomenon
was present both in pre- and postnatally diagnosed patients(Fig. 1A,B). Mean height in patients older than 20 yearswas 184.7 cm (Fig. 1A). Final height (measured after theage of 18 years) tended to be higher in patients who wereinitiated on testosterone therapy after the age of 18 years(n = 65) [184.3 cm (range 168.4 to 207.0)] as comparedwith patients treated with testosterone from the time ofpuberty (T started £15 years) (n = 17) [median height181.2 cm (range 173.7 to 201.0)], although the differencewas not statistically significant (p = 0.27) (Table 3). Medianages at initiation of testosterone substitution in the two sub-groups were 29.7 years (range 18.9–57.3) and 13.3 years(range 10.9–15.0), respectively. Part of the data on heightand weight have previously been published (8,9).
Body compositionBMI was within the normal reference range of healthymales in the majority of patients irrespective of age and irre-spective of time of diagnosis (pre- or postnatally)(Fig. 1C,D). Accordingly, and as previously published, thechildren and adolescent patients had a normal BMI despitean unfavourable muscle ⁄ fat ratio (increased body fat % anddecreased muscle fat mass as measured by whole bodyDEXA scan) (3).
Table 2 Registered co-morbidities in non-mosaic 47,XXY
Diagnosis N
Congenital
Cleft palate 1
Cryptorchidism (unilateral) 9
Cryptorchidism (bilateral) 12
Fragile X syndrome 1
Acondroplasia 1
Endocrine
Precocious puberty 1
Cushing’s syndrome 1
Type II diabetes 2
CNS
Neurosfibromatosis 1
Mentally retarded 2
Epilepsy 2
Orthopaedic
Scoliosis 1
Femural fracture 1
Cancer
Lung cancer 1
Acute Lymphblastic Leukemia 1
Malignant melanoma 1
Tumors
Leydig cell tumor 1
Infectious
HIV 1
Psychiatric disorders
Depression (medically treated) 8
Psychosis 2
Anxiety (medically treated) 2
Asperger syndrome 2
Autism 1
Attention Deficit Hyperactivity Disorder (medically treated) 2
Aksglæde et al. Klinefelter syndrome throughout life
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806 795
Bone mineral densityBone mineral density was decreased, although the majorityof patients (age at first DEXA scan 14.9–54.3 years, n = 59)had a BMD within the normal range at the level of the hipand spine (Fig. 2A,D). Thus, 44% presented with osteopeniaand even 5% had frank osteoporosis. In general, the patientswere more severely affected at the level of the spine [meanT-score )0.76 (range )3.6 to +4.1)] compared to the hip[mean T-score )0.24 (range )2.8 to +4.8)]. T-score at thelevel of the spine was significantly lower than the expectedvalue of zero (p < 0.0001), whereas T-score at the level ofthe hip did not differ from expected (p = 0.24). In theuntreated patients, femoral T-score correlated significantlywith serum testosterone and with serum E2 (r = 0.54,p = 0.03 and r = 0.62, p = 0.01, respectively) (Fig. 2B,C).Lumbar T-score correlated significantly with serum testos-terone, but not with E2 (r = 0.66, p = 0.005 and r = 0.36,p = 0.17, respectively) (Fig. 2E,F). There was no correlation
between the BMD and the E2 ⁄ testosterone ratio. The earli-est DEXA scan was used for this analysis in patients withrepeated scans. We have previously described normal BMDin children and adolescent Klinefelter patients (3).
Testicular sizeTesticular volume was increasingly smaller than the averagenormal population with increasing age (Fig. 3). Median tes-ticular volume in the never treated patients older than18 years (n = 52) was 3.0 mL (range 1.0–7.0).
Testicular histologyIn Figures 4–6, microphotographs of testicular histology ofnonmosaic Klinefelter patients ranging from gestationalweek (GW) 16 until 47 years are shown. Morphologicaldescription of each microphotograph can be found in thelegend. Data from a few of the biopsies have previouslybeen described (5). The overall gonadal developmental
A B
C D
Figure 1 Longitudinal growth and BMI in relation to chronological age in 132 patients with Klinefelter syndrome never treated with testosterone. Prenatally diagnosed[B and D; blue (n = 28)] and postnatally diagnosed [A and C; red (n = 104)]. Final height of the adult patients is indicated by red squares, and the black lines on thesesquares indicate mean height for the adults. Part of these data have previously been published (8,9). Lines represent mean ± 2 SD in healthy Danish boys.
Klinefelter syndrome throughout life Aksglæde et al.
796 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806

pattern of patients with KS is prenatal, apparently, rathernormal histological pattern including the presence of foetalgerm cells (Fig. 5A,B). During childhood, the histology stillremains rather normal, but a gradually degeneration ofgerm cells is observed with increasing age (Fig. 5C–I).
During puberty, only sporadic germ cells and few areas withspermatogenesis are observed. Hyperplasia of undifferenti-ated Sertoli cell is often observed, while the amount of Ley-dig cells still seem normal (Fig. 5J,K). Later in puberty,most of the (germ-cell-less) seminiferous tubules become
Table 3 Phenotypic characteristics according to age at initiation of testosterone supplementation
Age at treatment Adolescence <15.0 years N Adulthood >18.0 years N p-value
Final height (cm) 181.2 (173.7 to 201.0) 17 184.3 (168.4 to 207.0) 65 0.27
Gynecomastia 47% (16 ⁄ 34) 34 40% (31 ⁄ 78) 78 0.47
Lumbar T-score* )1.04 ()3.62 to +2.04) 12 )0.80 ()0.31 to +4.07) 47 0.55
Femur T-score* +0.16 ()2.34 to +1.40) 12 )0.76 ()2.82 to +4.80) 47 0.40
Lumbar T-score** )0.29 ()2.39 to +3.90) 11 )0.80 ()2.59 to +2.00) 30 0.61
Femur T-score** +0.22 ()0.66 to +2.86) 11 )1.15 ()2.40 to +2.50) 30 0.016
Age (years) at diagnosis 0 (0 to 14) 34 29 (15 to 57) 72 <0.0001
Data are presented as median and (range).
*Data obtained from the first DEXA scan if repeated scans are performed in the same individual.
**Data obtained in individuals treated with testosterone for one or more years at the time of DEXA scan.
AB
D E F
C
Figure 2 Bone mineral density (BMD) at the level of the hip (A) and spine (D) in relation to chronological age. Orange dots indicate untreated patients, whereas bluedots indicate patients on testosterone substitution. Repeated scans in the same patient are connected by a line. BMD correlated significantly with serum testosterone atthe level of the hip (B) and spine (E), whereas serum estradiol correlated significantly with BMD at the level of the hip (C), but not at the level of the spine (F). The dottedlines represent the limit for osteopenia (T-score <)1) and for osteoporosis (T-score <)2.5). The shaded area indicates the normal reference range in healthy males(mean ± 2 SD).
Aksglæde et al. Klinefelter syndrome throughout life
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806 797

totally hyalinized (Fig. 6A,B). During adolescence and inadults, very few tubules with spermatogenesis survive andthe Leydig cells proliferate and often yield very large areaswith Leydig cell hyperplasia (Fig. 6C–I). Both differentiated(type A) and undifferentiated (type B) Sertoli cells areobserved (10).
CryptorchidismData on cryptorchidism were available in 150 (90.4%) ofthe patients. Twenty-one patients had a history of cryptor-chidism (14.0%), out of whom 12 were bilateral (Table 2).
GynecomastiaData on gynecomastia were available in 123 (81.5%) of thepatients older than 10 years of age. Gynecomastia wasreported in 56 (43.8%) of these patients at any time point offollow-up. There was no difference in E2 ⁄ T-ratio betweenuntreated patients with gynecomastia (n = 34) anduntreated patients without gynecomastia (n = 37) (medianE2 ⁄ T-ratio 6.35 versus 6.40, respectively, p = 0.57). And thesame was the case with E2 (median 68 pmol ⁄ L versus56 pmol ⁄ L, respectively, p = 0.06) and with testosterone(median 10.1 nmol ⁄ L versus 7.24 nmol ⁄ L, respectively,p = 0.10).
Reproductive hormones and semen qualityThe serum concentration of testosterone was within normallimits during childhood and until the expected time of pub-erty. Thereafter, serum testosterone remained in the lowerhalf of the normal range in the majority of patients,although a few patients presented with testosterone con-centrations in the high normal range (Fig. 7A). Accordingly,
serum LH concentrations were extremely high (>+2 SD) inthe majority of patients (Fig. 7B). E2 concentrations were inthe lower half of the normal range in the majority (Fig. 7C),whereas FSH was above +2 SD in the majority of adultpatients (Fig. 7D). Inhibin B concentrations were normalduring childhood, but after puberty, a dramatic decline wasobserved, and inhibin B was unmeasurable in all but threeadult patients (Fig. 7E). In the bivariate LH-testosteroneanalysis, all adult patients (>18 years of age) were outsidethe normal limits for healthy males (Fig. 7F). Forty adultpatients delivered a semen sample, of which 38 showedazoospermia. Thirteen of these patients were adolescents(15–19 years), but none of these had motile sperms in theejaculate (11). Two KS subjects aged 29 years had spermconcentrations of 0.5 and 1.6 mill ⁄ mL, but did not differfrom the azoospermic patients with respect to phenotype orbiochemical parameters.
Cholesterol and triglyceridesTotal cholesterol, HDL, LDL and TG were measured in arandom nonfasting blood sample in 15 untreated and 56treated patients older than 18 years (Fig. 8). Total choles-terol, HDL, LDL and TG were outside the normal range in7 (47%), 1 (7%), 9 (60%) and 6 (40%) of untreated patientsrespectively, and in 20 (36%), 13 (23%), 22 (39%) and 21(38%) of the treated patients, respectively. There was no dif-ference between the concentrations of cholesterol and TGsbetween the two groups except between HDL, which wassignificantly lower in the treated patients (p = 0.037).
HbA1C and glucoseHbA1C and glucose were measured in a random nonfastingblood sample in 12 untreated and in 24 treated patientsolder than 18 years (Fig. 9A,B). HbA1C was elevated(>6.5%) in two treated patients, whereas serum glucose waselevated in four treated and one untreated patients indica-tive of diabetes. There was no difference between glucoseconcentrations and HbA1C between the two groups.
Prostate specific antigenProstate-specific antigen was measured in 20 untreated and62 treated patients older than 18 years (Fig. 9C). Mean PSAlevel was 0.7 lg ⁄ L in the untreated and 0.8 lg ⁄ L in the trea-ted patients (mean PSA 0.8 lg ⁄ L irrespective of treatment).There was no difference in PSA levels between treated anduntreated patients, but PSA was above the normal limit of4 lg ⁄ L in one treated but in no untreated patients.
Learning disabilitiesA need for speech therapy was reported in 13 of 37 (35%)patients followed during childhood, and 45 of 125 (36%)patients who had reached school age reported a need foreducational support services in primary school especially inreading and writing.
Psychiatric disordersPsychiatric disorders were reported (Table 2); eight adultpatients being medically treated for depression, two treated
Figure 3 Longitudinal measures (by palpation) of testicular size in relation tochronological age in 79 patients never treated with testosterone. A line connectsrepeated measurements in each patient. Testicular volume in adult patients olderthan 18 years are indicated in the right side of the figure, and the black line indi-cates mean volume in these adult patients. Black lines represent mean ± 2 SD inhealthy Danish boys (13). Part of these data have previously been published(11).
Klinefelter syndrome throughout life Aksglæde et al.
798 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806

for anxiety and two for psychotic conditions. In childhood,two cases of Asperger syndrome, two cases of attention defi-cit disorder and one case with atypical autism were noted.
DISCUSSIONIn this retrospective observational study, we describe theclinical and biochemical characteristics of 166 patients withnonmosaic 47,XXY KS followed in our endocrine outpa-tient clinic during the years 1990–2010. We also report onhistological findings in 29 testicular biopsies of patients with47,XXY KS at ages ranging from foetal life (gestational week16) to adult life (47 years of age). Our patients exhibited awide spectrum of the classical symptoms as previouslydescribed in KS. Importantly, two findings were presentconsistently in all postpubertal patients, namely small testesand a bivariate testosterone ⁄ LH evaluation outside the nor-mal reference range. Cryptorchidism was reported in 14%,gynaecomastia in 44% of the patients, and 36% requiredspeech therapy or educational support. The abnormal bio-chemical parameters became evident after onset of puberty
and correlated with histological findings of a gradual deteri-oration of seminiferous tubules and massive Leydig cellhyperplasia in adults.
The syndrome was first identified in 1942 by Klinefelter(12), who described nine cases with gynaecomastia, smalltestes, azoospermia with normal to moderately reducedLeydig cell function and increased excretion of urinaryFSH. The components of the disorder remain as originallydescribed by Klinefelter (12), although the diversity of thesymptoms ranging from a normal phenotype to the classi-cally described phenotype was recognized subsequently.
In our study, the patients, as a group, exhibited increasedgrowth already before puberty, and final height in thenever-treated adult patients was significantly aboveexpected. This pattern was also evident in the group of pre-natally diagnosed patients. Importantly, the majority of thepatients presented with a height within the normal range,and therefore tall stature cannot be considered a consistentfinding in KS. By contrast, a small testicular volumeappeared to be the only consistent clinical feature identifiedin the present study. Mean testicular volume in adult males
Figure 4 Comparisons of microphotographs of testicular specimens from of various ages. Left: individuals with normal testicular function and right: individuals withKlinefelter syndrome (KS). Note that the testicular architecture of specimens from normals and KS seem similar from foetal life until puberty, except that the number ofgerm cells is severely reduced in the prepubertal KS sample. During puberty, gross morphological changes appear. Normally spermatogenesis is initiated, but the seminif-erous tubules in the KS individual shows widespread degeneration and hyalinization. In an adult Klinefelter, few degenerated tubules may contain germ cells, but mostof the testicular tissue is composed of clumps of Leydig cells. Arrows indicate gonocytes. Bars represent 100 lm.
Aksglæde et al. Klinefelter syndrome throughout life
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806 799

was 3 mL, as compared with 22 mL in healthy Danish men(13). Abnormal reproductive hormones were found in themajority, but not all patients. Especially, a normal testoster-one concentration may confuse the clinician, and thereforethe combined evaluation of testosterone and LH is neces-sary for proper evaluation of Leydig cell function. Indeed,
the LH ⁄ testosterone ratio turned out to be outside the nor-mal range in all patients in our study (Fig. 7F).
Deterioration of germ cells and subsequently seminifer-ous tubules, which is accelerated in puberty, and subse-quently Leydig cell hyperplasia are reflected byunmeasurable inhibin B levels and increased FSH and LH
A B C
D E F
G H I
J K L
Figure 5 Klinefelter syndrome and testicular specimens. Note progressive loss of germ cells from foetal period to puberty, where widespread hyalinization of seminifer-ous tubules occurs and Leydig cells aggregate in clumps. All are H&E stains except C–E and J, which is stained with periodic acid-Schiff. (A, B) Gestational week 16 and 21foetuses. Note the uniform pattern of numerous Leydig cells in the abundant interstitial space between the seminiferous tubules. Arrows point to gonocytes within theseminiferous tubules. (C) Four-year-old boy. Note the relatively normal number of spermatogonia (arrows). (D) Nine-year-old boy: area showing seminiferous tubuleswith a few atypical germ cells (arrows). (E) Same as D but with an area with seminiferous tubules without germ cells. (F) Ten-year-old boy. Note that seminiferous tubulesare without germ cells and adult type Leydig cells are just visible (arrows). (G) Eleven-years-old boy: area without germ cells. Note that several adult type Leydig cells arevisible in interstitial space (arrows). (H) Same as G. Note large microlith in seminiferous tubule, no germ cells are visible. (I) Same as G. Note mitosis (arrow), which mostlikely is a Sertoli cell division. (J) Thirteen-year (12 years 11 months)-old boy. Note hyperplasia of undifferentiated Sertoli cells. (K) Fourteen-year-old boy. Note lack ofgerm cells, adult type Leydig cells (arrows) and undifferentiated seminiferous tubules with hyperplasia of Sertoli cells. (L) Same as K. Note heterogeneous pattern withlarge seminiferous tubule with start of spermatogenesis (right) and smaller undifferentiated tubules without germ cells (left). The bar in L denotes 100 lm, and the samemagnification is used in all pictures except in I, where the bar denotes 50 lm.
Klinefelter syndrome throughout life Aksglæde et al.
800 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806

A
B D
E F H
G I
C
Figure 6 (A) Fourteen-year (14 years 6 months)-old boy. Area with complete hyalinization of seminiferous tubules. Note the tubules appear as ‘ghost tubules’ withoutgerm cells and Sertoli cells and are marked with green lines. (B) Fifteen-year-old boy. Note tubule containing fully differentiated Sertoli cells only, next to an area withmany ‘ghost tubules’ marked with green dotted lines. (C) Eighteen-year-old male. Heterogeneous, adult type pattern with tubules with spermatogenesis (left), and a fewSertoli cell only tubules (right) mixed with completely hyalinized tubules and Leydig cell hyperplasia. (D) Nineteen-year-old male. Heterogeneous adult type pattern withcontaining differentiated Sertoli cells, type A (left) and incompletely differentiated Sertoli cells (type B) (right), fibrosis and Leydig cell hyperplasia (E) Twenty-five-year-old male. Heterogeneous adult pattern showing type A (top) and B (middel) Sertoli cells. (F) Twenty-nine-year (28 years 7 months)-old male. Adult pattern showing largeLeydig cell clumps, a few Sertoli cell only tubules and ghost tubules marked with L. (G) Thirty-year-old male. Adult pattern. Note the tubules with spermatogenesisembedded in large Leydig cell clumps denoted by L. (H) Thirty-one-year (30 years 7 months)-old male. Martius ⁄ scarlet ⁄ blue (MSB) staining. Adult pattern with impairedspermatogenesis embedded in Leydig cells and hyalinized tubules (arrows). (I) Forty-seven-year-old male. Adult pattern with scattered Sertoli cell only tubules (S)embedded in large Leydig cell clumps. All bars are 100 lm except F, G and I where it denotes 250 lm. All staining are H&E except A and H, which are periodic acid-Schiffand MSB, respectively.
Aksglæde et al. Klinefelter syndrome throughout life
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806 801

A
C
E F
D
B
Figure 7 Longitudinal measures of reproductive hormones in untreated patients with nonmosaic 47,XXY in relation to chronological age. Lines represent mean ± 2 SDin health males (35). Part of data have previously been published (3,8,36,37).
A B C D
Figure 8 Nonfasting total cholesterol, high-density lipoprotein, low-density lipoprotein and triglyceride in treated (blue squares) and untreated (orange squares) patientsolder than 18 years. Shaded area indicates the normal range as provided by the manufacturer.
Klinefelter syndrome throughout life Aksglæde et al.
802 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806

concentrations. Although some of the histological changese.g. Sertoli cell only tubules and microliths (10,14) may the-oretically be secondary to cryptorchidism often seen inpatients with KS, our experience is that Klinefelter patientswith cryptochidism have similar testicular function as theKlinefelter patients without cryptorchidism.
Gynecomastia was a clinical hallmark in the originaldescription of the syndrome (12). However, in accordancewith previous studies (15–20), we only found gynecomastiain 43.8% of the patients older than 10 years. Gynecomastiacan therefore be considered a frequent but inconsistentfinding in KS. Accordingly, one study found no difference inthe incidence of gynecomastia in patients with KS as com-pared with normally karyotyped subfertile men (17). Inter-estingly, the prevalence of gynecomastia was notsignificantly different in prenatally diagnosed patients, buthigher in postnatally diagnosed patients with KS comparedto the general population in another study (21). Theincreased prevalence of gynecomastia in KS has beenrelated to an increased E2 ⁄ testosterone ratio (16). We foundthe same tendency, although no statistically significant dif-ferences in E2 ⁄ testosterone ratio between patients with andwithout gynecomastia were present.
We found decreased BMD at the level of the spine, butnot in the hip, in accordance with previous findings (22);44% presented with osteopenia and even 5% had frankosteoporosis. Lower levels of E2 could partly explain thelower BMD, but indeed genes on the X chromosome mayalso be involved. In one study, a negative associationbetween the length of the CAG repeat polymorphism in theandrogen receptor gene and bone density was found (23),although this was not confirmed in another study (22). Inaddition, lifestyle factors such as lack of exercise, smokingand nutrition may also play a role.
We found dyslipidemia and elevated HbA1C in some ofour patients. In accordance, a nationwide register-basedepidemiological study demonstrated an almost fourfold
increased risk of type 2 diabetes [HR 3.71 (2.14–6.40)] com-pared to the background population (24), and a fivefoldincreased risk of developing the metabolic syndrome inadults with KS compared to age-matched controls wasfound in a recent study (25). Plasma LDL and cholesterolwere increased, whereas HDL was decreased (25), a lipidpattern similar to that presented in our study and in patientswith type 2 diabetes. In the study by Bojesen et al. (25), thestrongest predictor for the metabolic syndrome was adipos-ity, especially truncal adiposity. In the present study, wefound normal BMI, but as previously described, our patientswith KS had increased total body fat mass despite normalBMI and lean body mass during childhood and adoles-cence, indicating that these patients may have an unfavour-able body composition (3).
Normal levels of PSA during puberty and in adulthoodhave previously been reported in untreated patients with KS(17,18,26–28). PSA is strongly androgen dependent. Inaccordance, one study reported a significant increase in PSAconcentrations following 3 months of testosterone treat-ment (28). PSA levels were significantly and positively cor-related with the prostate volume both before and aftertreatment in that study. In contrast, we and others found noeffect of androgen replacement therapy on serum PSA con-centrations (27). A low rate of prostate adenocarcinoma ascompared with healthy males has been reported in KS (29),as well as in eunuchs, in patients with hypogonadism of anyaetiology, and in patients with 5a-reductase deficiency (30).This has lead to ‘the protective hypothesis of hypogona-dism’. However, it has been hypothesized that long-term tes-tosterone therapy may remove this relative protection fromprostate cancer afforded by hypogonadism and therebyincrease the risk of developing prostate cancer in KS (31).One of our treated patients had a PSA above the limit of4 lg ⁄ L, but no cases of prostate cancer were registered.
Klinefelter syndrome is associated with learning disabili-ties with depressed verbal IQ relative to performance IQ,
A B C
Figure 9 Nonfasting glycosylated haemoglobin, glucose and prostate-specific antigen in treated (blue squares) and untreated (orange squares) patients older than18 years. Shaded area indicates the normal range.
Aksglæde et al. Klinefelter syndrome throughout life
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806 803

often accompanied by moderate to severe problems withreading, spelling, writing and arithmetic both in childrenand in adults (32–34). In our cohort, a need for speech ther-apy was reported in 35% of the children, and a need for edu-cational support in primary school was reported in 36% ofthe patients who had reached school age. However, espe-cially the latter number may be highly underestimated,because the adult patients were not systematically askedabout learning difficulties especially in the first years of thestudy period, where the awareness of this problem was notso pronounced.
Many of the frequently observed phenotypical character-istics in our patients with KS could theoretically be, at leastin part, ascribed to the associated hypogonadism and there-fore prevented by early androgen therapy. We found ten-dencies towards reduced height and higher BMD inpatients who were initiated with testosterone treatmentalready in puberty and who had received therapy fore morethan a year. However, our patients were not randomized toearly versus late treatment disabling us from any firm con-clusions because of the inherent selection bias. Thus, a ran-domized controlled trial of the possible beneficial effects ofearly androgen treatment in KS adolescents is needed.
The uniqueness of the present study is the access to clini-cal information on 166 males with nonmosaic KS from birthto late adulthood. The nature of our combined paediatricand andrology outpatient clinic allows us to follow thepatients from birth through adulthood. In addition, the clin-ical examinations have been limited to a small group oftrained paediatric endocrinologists and ⁄ or andrologistsallowing for a standardized evaluation and workup pro-gramme during the years of follow-up.
On the other hand, the retrospective observational natureof the present study adds some limitations, which need tobe addressed. First, our data are recorded from the stan-dardized patient record files, but we do not have a propercontrol group for all our parameters. Second, the majorityof patients (80%) were diagnosed postnatally for variousreasons with the inherent risk of ascertainment bias. It hasbeen shown that the physical development may not differbetween boys with pre- and postnatally diagnosed KS,whereas the presence of gynecomastia and school delay wassignificantly more frequent in postnatally diagnosed boys ascompared with the general population (21). In addition,only approximately 25% of patients with KS are ever diag-nosed (1), and we can therefore only speculate on who theremaining 75% are and how they are performing physicallyas well as psychosocially. Observations on KS thereforehave to be regarded with caution. The clinical picturedescribed in most studies on KS may be biased, showingonly the best functioning cases (ascertained through infertil-ity) and the most extreme cases (referred because of pheno-typic characteristics, behavioural problems, etc.). Indeed,patients with KS exclusively ascertained prenatally wouldform the ideal cohort to study all the aspects of the syn-drome. However, such study would require a neonatalscreening programme for a whole birth cohort, which hasnot yet been performed in any country.
In conclusion, our patients presented with a wide spec-trum of the classical symptoms of KS. However, especiallyin infancy and childhood, the symptoms were nonspecific,whereas in adulthood, two features were present consis-tently in every patient, small testes and a bivariate testoster-one ⁄ LH evaluation outside the normal reference range. KSis highly under-diagnosed, and to improve the medicalneeds for this patient group, the awareness of the syndromein primary care and among school health professionalsshould be improved. Indeed, routine examinations of testessize should be performed in all schoolboys from the time ofexpected puberty.
References
1. Bojesen A, Juul S, Gravholt CH. Prenatal and postnatal preva-lence of Klinefelter syndrome: a national registry study. J ClinEndocrinol Metab 2003; 88: 622–6.
2. de la Chapelle A. Analytic review: nature and origin of maleswith XX sex chromosomes. Am J Hum Genet 1972; 24:71–105.
3. Aksglaede L, Molgaard C, Skakkebaek NE, Juul A. Normalbone mineral content but unfavourable muscle ⁄ fat ratio inKlinefelter syndrome. Arch Dis Child 2008; 93: 30–4.
4. Muller J, Skakkebaek NE, Ratcliffe SG. Quantified testicularhistology in boys with sex chromosome abnormalities. Int JAndrol 1995; 18: 57–62.
5. Aksglaede L, Wikstrom AM, Rajpert-De ME, Dunkel L,Skakkebaek NE, Juul A. Natural history of seminiferous tubuledegeneration in Klinefelter syndrome. Hum Reprod Update2006; 12: 39–48.
6. Andersson AM, Muller J, Skakkebaek NE. Different roles ofprepubertal and postpubertal germ cells and Sertoli cells in theregulation of serum inhibin B levels. J Clin Endocrinol Metab1998; 83: 4451–8.
7. Juul A, Aksglaede L, Lund AM, Duno M, Skakkebaek NE, Raj-pert-De Meyts E. Preserved fertility in a non-mosaic Klinefelterpatient with a mutation in the fibroblast growth factor receptor3 gene: case report. Hum Reprod 2007; 22: 1907–11.
8. Aksglaede L, Skakkebaek NE, Juul A. Abnormal sex chromo-some constitution and longitudinal growth: serum levels ofinsulin-like growth factor (IGF)-I, IGF binding protein-3,luteinizing hormone, and testosterone in 109 males with47,XXY, 47,XYY, or sex-determining region of the Y chromo-some (SRY)-positive 46,XX karyotypes. J Clin EndocrinolMetab 2008; 93: 169–76.
9. Ottesen AM, Aksglaede L, Garn I, Tartaglia N, Tassone F,Gravholt CH, et al. Increased number of sex chromosomesaffects height in a non linear fashion: a study of 305 patientswith sex chromosome aneuploidy. Am J Med Genet A 2010;152A: 1206–12.
10. Skakkebaek NE. Two types of tubules containing only Sertolicells in adults with Klinefelter’s syndrome. Nature 1969; 223:643–5.
11. Aksglaede L, Jorgensen N, Skakkebaek NE, Juul A. Low semenvolume in 47 adolescents and adults with 47,XXY Klinefelter or46,XX male syndrome. Int J Androl 2009; 32: 376–84.
12. Klinefelter HF. Syndrome characterized by gynecomastia,aspermatogenesis without A-Leydigism, and increased excre-tion of follicle-stimulating hormone. J Clin Endocr Metab 1942;2: 615–27.
13. Sorensen K, Aksglaede L, Petersen JH, Juul A. Recent changesin pubertal timing in healthy Danish boys: associations withbody mass index. J Clin Endocrinol Metab 2010; 95: 263–70.
Klinefelter syndrome throughout life Aksglæde et al.
804 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806
14. Skakkebaek NE, Philip J, Hammen R. Meiotic chromosomes inKlinefelter’s syndrome. Nature 1969; 221: 1075–6.
15. Zeger MP, Zinn AR, Lahlou N, Ramos P, Kowal K, Samango-Sprouse C, et al. Effect of ascertainment and genetic featureson the phenotype of Klinefelter syndrome. J Pediatr 2008; 152:716–22.
16. Salbenblatt JA, Bender BG, Puck MH, Robinson A, Faiman C,Winter JS. Pituitary–gonadal function in Klinefelter syndromebefore and during puberty. Pediatr Res 1985; 19: 82–6.
17. Kamischke A, Baumgardt A, Horst J, Nieschlag E. Clinical anddiagnostic features of patients with suspected Klinefelter syn-drome. J Androl 2003; 24: 41–8.
18. Vorona E, Zitzmann M, Gromoll J, Schuring AN, Nieschlag E.Clinical, endocrinological, and epigenetic features of the 46,XXmale syndrome, compared with 47,XXY Klinefelter patients. JClin Endocrinol Metab 2007; 92: 3458–65.
19. Lanfranco F, Kamischke A, Zitzmann M, Nieschlag E. Klinefel-ter’s syndrome. Lancet 2004; 364: 273–83.
20. Paulsen CA, Gordon DL, Carpenter RW, Gandy HM, DruckerWD. Klinefelter’s syndrome and its variants: a hormonal andchromosomal study. Recent Prog Horm Res 1968; 24: 321–63.
21. Girardin CM, Lemyre E, Alos N, Deal C, Huot C, Van Vliet G.Comparison of adolescents with Klinefelter syndrome accord-ing to the circumstances of diagnosis: amniocentesis versusclinical signs. Horm Res 2009; 72: 98–105.
22. Ferlin A, Schipilliti M, Vinanzi C, Garolla A, Di Mambro A, Se-lice R, et al. Bone mass in subjects with klinefelter syndrome:role of testosterone levels and androgen receptor gene CAGpolymorphism. J Clin Endocrinol Metab 2011, [Epub ahead ofprint].
23. Zitzmann M, Depenbusch M, Gromoll J, Nieschlag E. X-chro-mosome inactivation patterns and androgen receptor function-ality influence phenotype and social characteristics as well aspharmacogenetics of testosterone therapy in Klinefelterpatients. J Clin Endocrinol Metab 2004; 89: 6208–17.
24. Bojesen A, Juul S, Birkebaek NH, Gravholt CH. Morbidity inKlinefelter syndrome: a Danish register study based on hospitaldischarge diagnoses. J Clin Endocrinol Metab 2006; 91: 1254–60.
25. Bojesen A, Kristensen K, Birkebaek NH, Fedder J, Mosekilde L,Bennett P, et al. The metabolic syndrome is frequent in Kline-felter’s syndrome and is associated with abdominal obesity andhypogonadism. Diabetes Care 2006; 29: 1591–8.
26. Wikstrom AM, Dunkel L, Wickman S, Norjavaara E, Ankar-berg-Lindgren C, Raivio T. Are adolescent boys with Klinefeltersyndrome androgen deficient? A longitudinal study of Finnish47,XXY boys. Pediatr Res 2006; 59: 854–9.
27. Shibasaki T, Sasagawa I, Suzuki Y, Yazawa H, Ichiyanagi O,Matsuki S, et al. Effect of testosterone replacement therapy onserum PSA in patients with Klinefelter syndrome. Arch Androl2001; 47: 173–6.
28. Ozata M, Bulur M, Beyhan Z, Sengul A, Saglam M, Turan M,et al. Effects of gonadotropin and testosterone treatments onprostate volume and serum prostate specific antigen levels inmale hypogonadism. Endocr J 1997; 44: 719–24.
29. Swerdlow AJ, Higgins CD, Schoemaker MJ, Wright AF, JacobsPA. Mortality in patients with Klinefelter syndrome in Britain: acohort study. J Clin Endocrinol Metab 2005; 90: 6516–22.
30. Slater S, Oliver RT. Testosterone: its role in development ofprostate cancer and potential risk from use as hormone replace-ment therapy. Drugs Aging 2000; 17: 431–9.
31. Bydder SA, Joseph DJ, Weinstein S, Stuckey BG. Prostate can-cer following testosterone replacement in Klinefelter syndrome.ANZ J Surg 2007; 77: 93–4.
32. Ross JL, Zeger MP, Kushner H, Zinn AR, Roeltgen DP. Anextra X or Y chromosome: contrasting the cognitive and motor
phenotypes in childhood in boys with 47,XYY syndrome or47,XXY Klinefelter syndrome. Dev Disabil Res Rev 2009; 15:309–17.
33. Walzer S, Bashir AS, Silbert AR. Cognitive and behavioral fac-tors in the learning disabilities of 47,XXY and 47,XYY boys.Birth Defects Orig Artic Ser 1990; 26: 45–58.
34. Rovet J, Netley C, Bailey J, Keenan M, Stewart D. Intelligenceand achievement in children with extra X aneuploidy: a longi-tudinal perspective. Am J Med Genet 1995; 60: 356–63.
35. Andersson AM, Toppari J, Haavisto AM, Petersen JH, Simell T,Simell O, et al. Longitudinal reproductive hormone profiles ininfants: peak of inhibin B levels in infant boys exceeds levels inadult men. J Clin Endocrinol Metab 1998; 83: 675–81.
36. Aksglaede L, Petersen JH, Main KM, Skakkebaek NE, Juul A.High normal testosterone levels in infants with non-mosaicKlinefelter’s syndrome. Eur J Endocrinol 2007; 157: 345–50.
37. Aksglaede L, Andersson AM, Jorgensen N, Jensen TK, CarlsenE, McLachlan RI, et al. Primary testicular failure in Klinefel-ter’s syndrome: the use of bivariate luteinizing hormone-testosterone reference charts. Clin Endocrinol (Oxf) 2007; 66:276–81.
APPENDIX: DISCUSSION FOLLOWING LISE AKSGLÆDE AND ANDERSJUUL PRESENTATIONSGrowth, bone density and body composition in childhoodand adolescencePituitary-gonadal axis in adult Klinefelter syndrome
Claus Gravholt (Copenhagen, Denmark):It is important to consider patients with Klinefelter syn-drome (KS) as they progress from puberty to adulthood.Adult endocrinologists see adult patients who manifest thewhole hypogonadal phenotype with increased body fatmass and reduced muscle mass. We require a randomizedcontrol trial to treat late-teenage KS patients with testos-terone (T) or placebo in an attempt to improve the adultstatus.
Anders Juul:I agree.
Fred Wu (Manchester, UK):Can you correlate testosterone levels or LH: testosteroneratio, to any particular KS phenotype such as bone structureor sexual function in order to assess useful indications tostart hormone therapy?
Anders Juul:We have found that the simple LH:T ratio in untreatedpatients with KS is not better correlated with BMD thanserum measurement of T or oestrogen by themselves. It isnot clear whether the LH:T ratio, or increased LH by itself,is a compensatory mechanism or a sign that the body lacksT. A study of patients with cancer in the UK receiving che-motherapy showed a mild abnormality in the LH:T ratio,which was considered to be compensated mild Leydig cellinsufficiency: they were treated with androgens, but therewas no pronounced effect. We still do not know whetherpatients with elevated LH and low T are prone to developosteoporosis.
Aksglæde et al. Klinefelter syndrome throughout life
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806 805

Christina Wang (Los Angeles, USA):Oestrogen (E) levels in your patients with KS are relativelynormal, but the E:T ratio will be high because of the low Tlevels in KS.
Anders Juul:The ratio of total T to E in our patients was the same as in thenormal population. Androgens and oestrogens are both low.
Alberto Ferlin (Padova, Italy):Have you measured other parameters of androgen activitysuch as prostate volume and PSA? The PSA is extremely Tdependent and may possibly reflect the true state of hypog-onadism.
Anders Juul:PSA level is a very useful marker of T activity on the pros-tate, and we have measured this in our normal pubertal con-trol population. We have not systematically evaluated PSAin all of our patients with KS, but I suspect it will be verylow.
Claus Gravholt (Aarhus, Denmark):The 70 patients with KS in our study had normal or lownormal levels of E2 comparable to the controls, but a rela-tive increase in relation to T levels causing a raised E2:Tratio.
Najiba Lahlou (Paris, France):E2 levels are normal in infants with KS. Clinically, anti-mullerian hormone (AMH) is a marker of testicular matura-tion, and levels decrease physiologically as T increases.Inhibin B may be a better marker.
Robert McLachlan (Melbourne, Australia):Part of the KS phenotype might be due to androgen defi-ciency, but I was not aware that androgen levels were dem-onstratably lower in 5–10-year-old patients. What objectivemeasurements of androgen insufficiency did you make, andwhat are the levels of androgens and SHBG in your patientpopulation across adolescence?
Lise Aksglæde:We found normal levels throughout childhood in ourpatients with KS and no difference between KS boys andnormal boys. However, we were using insensitive assaymethods, and the hormone levels were below our detectionlevels. We require more sensitive methods to make compar-isons at low levels, and this might explain differences inbody composition.
Fred Wu (Manchester, UK):When you measured BMD in boys with KS, were theymatched for height with the control boys? You measuredareal bone density, but it is probably important to measurevolumetric bone density because of differences due to stat-ure.
Lise Aksglæde:All measurements including bone area were corrected forheight.
Fred Wu:That indicates that the tendency to develop osteopeniaoccurs sometime during adulthood.
Lise Aksglæde:That is the case in our cohort.
Carole Samango-Sprouse (Washington, USA):Did you look at familial height and head circumference inyour KS subjects?
Lise Aksglæde:Parental height was measured for most of our patients inthe SHOX study, but not in our first studies. KS children aresignificantly taller than their target height. We did not mea-sure head circumference.
Gary Butler (London, UK):Please clarify a question about the dosage of SHOX geneand the mechanism of growth. There is a triple dose of theSHOX gene in both XXY and XYY boys, but these twogroups have different growth patterns with much morerapid growth throughout childhood in XXY boys, whereasXYY boys continue to grow into adolescence. Is this due toa different chromosome of origin in the SHOX gene itself,or do genes in the Y chromosomes have a moderating effecton SHOX action? Would you expect a different effect ofSHOX depending on whether it is of X or Y chromosomalorigin?
Lise Aksglæde:There are different mechanisms involved because XYY boyshave normal endocrine function, do not develop hypogona-dism, do not develop gynaecomastia and have a differentgrowth pattern resulting in normal proportions in contra-distinction to boys with KS. It is difficult to assess whetherthe abnormal growth in KS is due to genes or hormones.The chromosome of origin, whether X or Y, may have aneffect but other factors are also involved.
Alan Rogol (Charlottesville, USA):KS individuals are always described as being eunochoid, butthe legs are always relatively much longer than the arms.Did you find this disproportion with long legs and relativelynormal arm length for stature, and is there an explanation?
Lise Aksglæde:We did not measure arm length. In the original descriptionby Klinefelter, the arm span exceeded height indicating longarms also, but he did not describe body proportions.
Klinefelter syndrome throughout life Aksglæde et al.
806 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 793–806







