vascular delay and intermittent stimulation: keys to successful latissimus dorsi muscle stimulation
TRANSCRIPT

2001;71:1866-1873 Ann Thorac Surgand A. David Slater
Abul Kashem, William P. Santamore, Benjamin Chiang, Lauren Unger, Ahsan T. Ali muscle stimulation
Vascular delay and intermittent stimulation: keys to successful latissimus dorsi
http://ats.ctsnetjournals.org/cgi/content/full/71/6/1866on the World Wide Web at:
The online version of this article, along with updated information and services, is located
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2001 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 10, 2013 ats.ctsnetjournals.orgDownloaded from
Vascular Delay and Intermittent Stimulation: Keysto Successful Latissimus Dorsi Muscle StimulationAbul Kashem, MD, PhD, William P. Santamore, PhD, Benjamin Chiang, MD,Lauren Unger, PhD, Ahsan T. Ali, MD, and A. David Slater, MDDivision of Cardiovascular Research, Cardiology Section, Temple University, Philadelphia, Pennyslvania, and Division ofCardiothoracic Surgery, Department of Surgery, University of Louisville, Louisville, Kentucky
Background. The goal of this study was to obtainphysiologically significant increases in peak left ventric-ular (LV) systolic pressure and stroke volume with latis-simus dorsi muscle (LDM) stimulation in cardiomyo-plasty (CMP). We hypothesized that preserving LDMintegrity by vascular delay and intermittent stimulationwould significantly increase LDM cardiac assistance.
Methods. In 4 control dogs and 12 dogs that hadundergone a vascular delay (VD) procedure, LV dysfunc-tion was induced by intracoronary microsphere injec-tions. Cardiomyoplasty surgery was performed 14 dayslater, followed by progressive LDM conditioning. In thecontrol dogs and in 6 of the VD dogs, the LDM wasstimulated 24 hours per day (VD plus constant stimula-tion [CS]). In the other 6 VD dogs, LDMs were stimulatedon a daily schedule of 10 hours on and 14 hours off (VDplus interrupted stimulation [IS]). Latissimus dorsi mus-cle stimulated beats were compared with nonstimulatedbeats 9 weeks later.
Results. In the control dogs, LDM stimulation had
minimal effects. In VD 1 CS and VD 1 IS, LDMstimulation increased peak LV pressure, stroke volume,stroke work, and stroke power (p < 0.05). However, thesechanges were greater in the VD 1 IS group, in whichLDM stimulation increased peak aortic pressure by17.6 6 1.7 mm Hg, peak LV pressure by 19.7 61.1 mm Hg, peak positive LV dp/dt by 398 6 144 mm Hgper second, stroke volume by 5.1 6 0.7 mL, stroke workby 10.9 6 0.9 gm z m, and stroke power by 122.7 6 11.6gm z m per second (p < 0.05 compared with VD 1 CS).Quantitative morphometric analysis showed minimalLDM degeneration in the VD 1 IS group (7.5% 6 1.1%),and VD 1 CS group (10.5% 6 4.5%) compared with thecontrol group (29.5% 6 4.5%, p < 0.05).
Conclusions. VD and IS considerably increased the LVassistance with LDM stimulation. Further studies of thiscombined approach to CMP should be planned.
(Ann Thorac Surg 2001;71:1866–73)© 2001 by The Society of Thoracic Surgeons
C ardiomyoplasty has been shown to inhibit progres-sive LV enlargement [1–3]. However, in experimen-
tal and clinical studies, systolic augmentation of LVfunction by the LDM has not been routinely observed;LV ejection fraction and peak systolic pressure remainalmost identical in presence versus absence of electricalstimulation [4].
Acute mobilization and wrapping of the LDM aroundthe heart causes LDM ischemia [5, 6]. Furthermore,incessant stimulation is detrimental to the LDM. Insheep, LDM stimulation applied 24 hours per day causedmore than 40% fiber atrophy and loss of most contractilefunction, whereas stimulation limited to 10 hours per daycaused only minimal fiber atrophy, fatty infiltration, andfibrosis [7]. In goats, Ianuzzo and colleagues [8] foundthat, compared with continuous stimulation, LDM stimula-tion limited to 12 hours per day preserved muscle architec-ture and was associated with less muscle degeneration,larger fiber areas, and lower density of connective tissue.
The goal of the present study was to obtain physiolog-ically significant increases in peak LV systolic pressure
and stroke volume with LDM stimulation in an experi-mental model of LV dysfunction. We hypothesized that atwo-stage vascular delay procedure followed by intermit-tent stimulation would preserve LDM integrity, leadingto increased LDM cardiac assistance.
Material and Methods
Mongrel dogs weighing 22 to 27 kg were assigned to acontrol CMP group (n 5 4), a group that underwent avascular delay procedure followed by continuous stimu-lation (VD 1 CS; n 5 6), and a group that underwent avascular delay procedure followed by stimulation inter-mittently interrupted for 14 hours per day (VD 1 IS; n 56). All study procedures were performed in compliancewith the “Principles of Laboratory Animal Care” formu-lated by the National Society for Medical Research andthe “Guide for the Care and Use of Laboratory Animals”prepared by the National Academy of Sciences andpublished by the National Institutes of Health (NIHpublication 85-23, revised 1985).
Vascular DelayAfter an overnight fast, the animals received intravenous(IV) sodium thiopental, 15 to 25 mg/kg, and intramuscu-lar atropine, 0.01 mg/kg, and were intubated and venti-
Accepted for publication Feb 21, 2001.
Address reprints requests to Dr Kashem, Temple University School ofMedicine, Medical Research Bldg, Room 800A, 3420 N Broad St, Phila-delphia, PA 19140; e-mail: [email protected].
© 2001 by The Society of Thoracic Surgeons 0003-4975/01/$20.00Published by Elsevier Science Inc PII S0003-4975(01)02571-1
by on June 10, 2013 ats.ctsnetjournals.orgDownloaded from

lated (Quantiflex, VMC Anesthesia Machine, OrchardPark, NY). Anesthesia was maintained with 2% isoflurane(Isoflurane Vaporizer, Oharda, Isotec 3, Aushell, GA),0.5% to 1.0% nitrous oxide, and oxygen. Surface electro-cardiogram (Hewlett Packard Model No. 78346A) andoxygen saturation were monitored continuously. Cefazo-lin sodium, 500 mg IV (Marsam Pharmaceutical Inc,Cherry Hill, NJ), 75 mg of gentamicin, and 75 mg intra-muscular (Gentocin, Ayerst Laboratories Inc, RousesPoint, NY) were administered preoperatively. LactatedRinger’s solution, 250 mL to 350 mL per hour IV wasinfused perioperatively. In the vascular delay groups(VD 1 CS and VD 1 IS), a 15 to 20 cm long obliquecutaneous incision was made under sterile surgical con-dition from the left axillary region toward the posterioriliac crest. The anterior border of the left LDM wasidentified and all perforating collateral branches supply-ing the muscle were ligated and severed [9–11]. Thespinal border of the muscle was identified and partiallymobilized. The wounds were closed in layers usingabsorbable sutures.
LV DysfunctionIn all animals (controls, VD 1 CS, and VD 1 IS), leftventricular dysfunction was induced by intracoronaryinjection of microspheres [12]. The left femoral artery wascannulated percutaneously with a 7 French cathetersheath, through which a 6 French left coronary AmplatzNo. 1 catheter was advanced into the left main coronaryartery under fluoroscopy. Contrast material (Renografin276, Bristol-Myers-Squibb Co, Princeton, NJ) was in-jected to verify the catheter position. Latex microspheres(3.0 to 6.0 3 106, 90 6 2 m diameter; Polyscience Inc,Warrington, PA), mixed in 10 mL of normal saline, wereinjected into the coronary artery in fractionated dosesuntil left venticular end-diastolic pressure had increasedby 50% to 80%, and peak left ventricular pressure andaortic pressure decreased by 20%. The catheter andsheath were removed. The femoral artery was com-pressed externally for 20 to 30 minutes until hemostasis.All animals survived the intracoronary microsphere in-jections and were treated with IV injections of furo-semide, 0.75 mg/kg, and rapid infusions of 500 L Ringer’slactated saline solution. Postoperatively, sedation withAcepromazine, 0.5 mg IV, and analgesia with Buprenexhydrochloride, 0.3 mg IV, were administered as needed.A 2-week period was allowed for recovery and vascularremodeling.
CMP ProcedureA standard CMP procedure was performed on all ani-mals as described in previous articles [11, 13–15]. Undergeneral anesthesia, with the animal in the right lateralposition, a left lateral incision was performed in themidaxillary line. The LDM was dissected out and mobi-lized from the surrounding tissues and its distal inser-tions, preserving the thoraco-dorsal neurovascular bun-dle proximally. The tendon of the LDM was carefullyisolated and severed. Two epimysial leads (ModelYY38403403 Medtronic Inc, Minneapolis, MN) were im-
planted on the pedicle with nylon sutures. The cathodewas placed proximally on the muscle and the anode 6 to8 cm distally. The stimulation threshold was measuredwith a Pacing System Analyzer (PSA 5311, Medtronic Inc,Minneapolis MN).
A 4 to 5 cm section of the anterior portion of the leftthird rib, including its periosteum, was resected to allowthe translocation of the LDM flap into the left pleuralspace. The proximal parts of a sensing myocardial leadand an aortic flow probe (20 mm) were introduced intothe chest for later implantation onto the right ventricularanterior wall and ascending aorta, respectively. Theepimysial and myocardial leads were tunneled subcuta-neously and connected to a dual chamber synchronouscardiomyostimulator (SP 1005, Medtronic Inc, Minneap-olis, MN) implanted in a subcutaneous pocket fashionedon the left side. The LDM flap was fixed to the perios-teum of the second rib by polybraided 3-0 dexan suturingmaterial to prevent tension on the muscle, and thewound was closed in layers.
The heart was exposed through a median sternotomywith the animals in the supine position. After pericar-diotomy, the ascending aorta was mobilized and an aorticflow probe (A-series 20-mm, Transonic Systems Inc,Ithaca, NY) was placed around the ascending aorta witha merocel sponge positioned between the flow probe andthe aorta, and the distal end of the flow probe positionedsubcutaneously. A posterior myocardial wrap was per-formed in a clockwise fashion with fixation to the peri-cardium. Bilateral chest tubes were inserted and con-nected to a water-seal drainage system. The sternum wasclosed using 4 or 5 parasternal wire sutures. All woundswere closed in layers.
The animals were extubated. Postoperative analgesicsand sedation with Buprenorphine hydrochloride, 0.3 to0.6 mg IV, and acepromazine maleate, 0.25 to 0.5 mgintramuscular, were systematically administered, and theanimals were positioned onto the right side overnight.Chest tubes were removed on the first postoperative day.Cefazolin 500 mg IV and gentamicin 75 mg IV every 12hours, were administered for 72 hours postoperatively.
Stimulation ProtocolsCardiomyoplasty stimulation began with postoperativeweek 2. The LDM was progressively conditioned startingat 2 Hz, gradually increasing up to 33 Hz, at a pulse widthof 180 ms, interpulse interval of 25 ms, and burst dura-tions of 180 to 210 ms, until postoperative week 9. TheLDM was stimulated on every other cardiac cycle. In thecontrol and the VD 1 CS groups, the cardiomyostimula-tor was turned on 24 hours per day. In the VD 1 IS group,cardiomyostimulation was limited to 10 hours continu-ously per day.
Hemodynamic EvaluationAt 9 weeks after surgery, the dogs were reanesthetizedwith sodium pentothal, 10 to 15 mg/kg IV, followed by 2%isoflurane and 1% to 2% nitrous oxide, and ventilatedthrough an endotracheal tube with a positive-pressurerespirator. Analgesia with buprenorphine hydrochloride,
1867Ann Thorac Surg KASHEM ET AL2001;71:1866–73 VASCULAR DELAY AND INTERMITTENT LDM STIMULATION
by on June 10, 2013 ats.ctsnetjournals.orgDownloaded from

0.3 to 0.6 mg IV, was administered before intubation,avoiding atropine. A 7 French catheter sheath was intro-duced into the right carotid artery for measurements ofaortic pressure. A 6 French pigtail micromanometertipped catheter with lumen (Model SPC 464D, MILLARInstruments Inc, Houston, TX) was advanced through thecatheter sheath, and placed in the ascending aorta. An-other 7 French catheter sheath was introduced into theright femoral artery for placement under fluroscopicguidance of a 6 French pigtail micromanometer tippedcatheter with lumen (Model SPC 464D MILLAR Instru-ments Inc, Houston, TX) into the left ventricle. Analogsignals from the pressure transducers were amplified(PM-1000, CWE Inc, Admore, PA). The epimysial leadswere disconnected from the SP1005 pacemaker and con-nected to an external muscle stimulator (Model 8800,Grass Systems Inc, Quincy, MA). A cardiotachometerdetected the QRS waveform from the analog electrocar-diographic signal and triggered the muscle stimulator.This resulted in synchronized LDM stimulation with theR wave. The aortic flow probe lead was dissected outfrom its subcutaneous position and connected to a flowmeter (Model No. 206T, Transonic Systems Inc, Ithaca,NY) to measure aortic flow.
Data were recorded simultaneously on a chart recorder(Model TA-11, Gould Instrument Systems Inc, Cleveland,OH) and on a computer (Micron computer, Micron Inc,Model No. M55PLUS2-P200-MT). The pressure, flow,and electrocardiographic signals were digitized by anA/D circuit board (Model AT-MIO 16.0E-10, Labview,National Instruments, low-pass and antialiasing filters,National Instruments, Austin, TX). The data were ac-quired with LABVIEW, version 4.0 software (Houston,TX). The stimulator pulse train duration was adjustedbetween 150 and 190 ms, pulse duration set at 0.5 ms,pulse frequency at 50 Hz, with an interpulse interval of 15to 20 ms, and pulse train delay set at 20 to 80 ms after theR wave. The LDM was stimulated on every third orfourth beat. Three consecutive data sets were obtained.Each data set was 30 seconds long with the ventilatorswitched off during data acquisition to avoid respiratoryvariations. After the procedure, the animals were sacri-ficed by IV injection of 20 mL of potassium chloride.
Morphometric MeasurementsTo determine the magnitude of LDM degeneration, theheart with the LDM still attached was removed and cutinto 1-cm thick cross-sections. These sections were incu-bated in the dark in 0.05% nitroblue tetrazolium dyesolution at 22°C for 40 minutes [16]. The viable areas werestained in blue and the nonviable areas remained purple.Digital pictures of the cross sections were obtained andtracings were obtained by area manometry of the Opti-mus software (Optimus, Paint, Eden Prairie, MN). Thepercentages of viable LDM along with weighted averageswere calculated.
Data AnalysisUsing software developed in Visual Basic for Excel (Mi-crosoft Excel 7.0, Microsoft Inc, Redwood, WA), hemody-
namic variables were extracted from a digitally storeddata file. Ectopic and postectopic cycles were excludedfrom the analysis. For each cardiac cycle, end-diastolicpressure, peak ventricular systolic pressure, peak posi-tive and negative first derivative of the left ventricularpressure (1dp/dt, 2dp/dt), peak and end-diastolic aorticpressures were determined, and stroke volume, strokework, and stroke power were calculated. The stimulatedbeats were compared with the immediate precedingnonstimulated beats. Both the absolute magnitudes ofthe changes and percent changes caused by LDM stim-ulation were calculated.
Data are expressed as mean 6 standard error of themean. Within each group, the hemodynamic variables ofstimulated beats were compared with the immediatepreceding nonstimulated beats by paired Student’s t test.Two-way analysis of variance was used for comparisonand significance among the 3 groups, followed by un-paired Student’s t test with Bonferroni correction factorfor multiple comparisons. A p value less than 0.05 wasconsidered significant.
Results
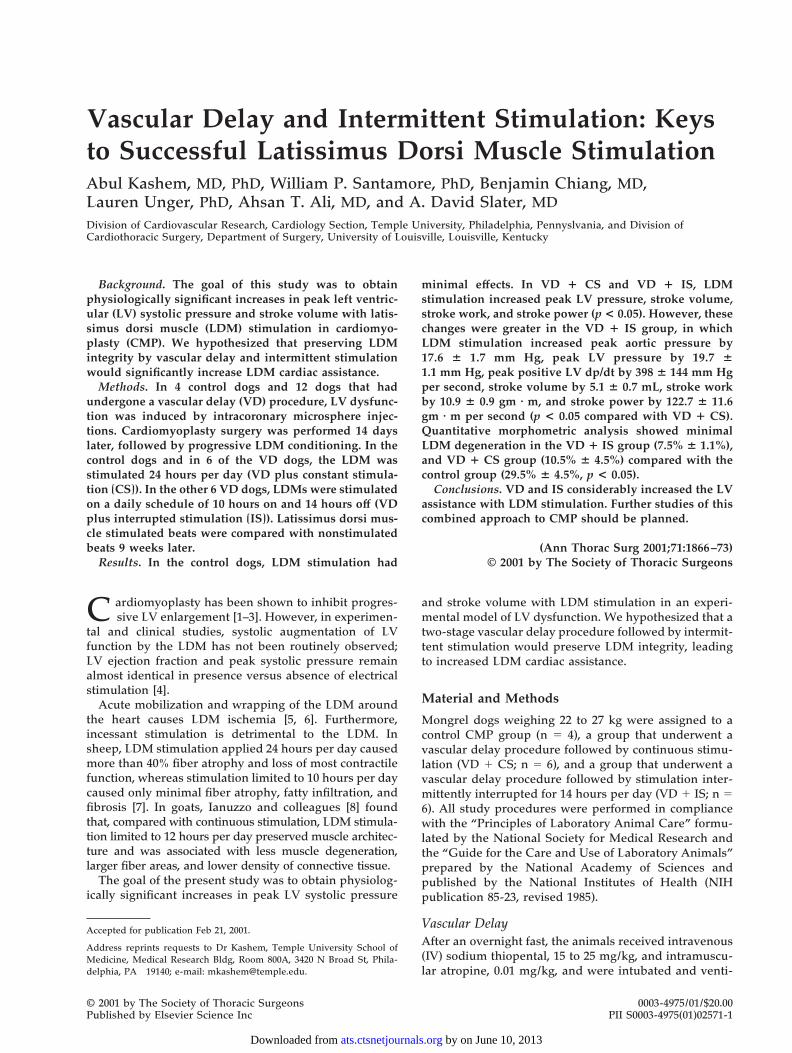
Figure 1 shows the hemodynamic data before and afterintracoronary microsphere injections in the control, VD 1CS, and VD 1 IS groups. In all groups, the hemodynamicimpairment was similar: increased left ventricular end-diastolic pressure, decreased peak systolic left ventricularpressure, peak aortic pressure, stroke volume, and strokework. Likewise, at final evaluation, there were no significantdifferences in left ventricular end-diastolic pressure, peakleft ventricular pressure, and LV 1dp/dt between the 3groups for the nonstimulated beats.
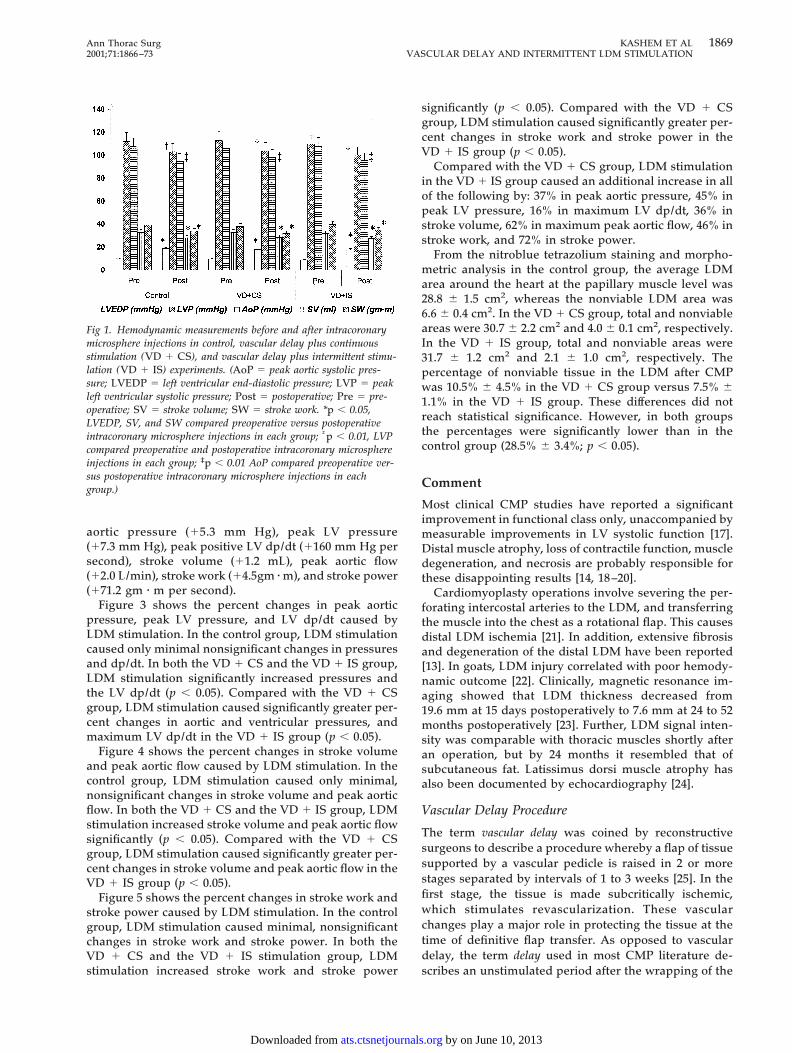
Figures 2A, 2B, and 2C show representative data froma control animal, a VD 1 CS, and a VD 1 IS LDMstimulation experiment, respectively. Aortic flow, aorticand left ventricular pressures, left ventricular dp/dt, andelectrocardiogram are shown. The LDM was stimulatedon every third or fourth beat as seen on the electrocar-diogram. In the control experiment, LDM stimulationcaused minimal increases in aortic flow, pressures, andleft ventricular dp/dt (Fig 2A). In the VD 1 CS experi-ment, LDM stimulation increased aortic flow, pressures,and left ventricular dp/dt (Fig 2B). In the VD 1 IS LDMstimulation experiment (Fig 2C), LDM stimulationcaused very large increases in aortic flow, pressures, andleft ventricular dp/dt.
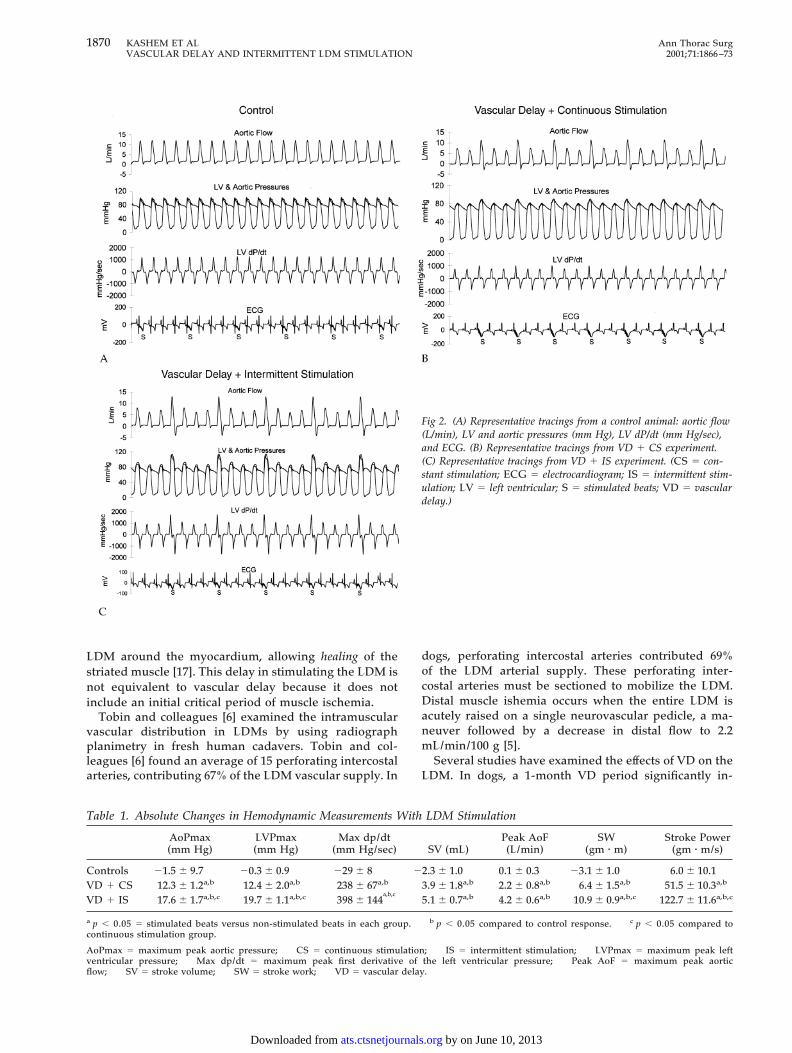
Table 1 summarizes the absolute changes in hemody-namic measurements with LDM stimulation. In the con-trol group, LDM stimulation caused minimal, nonsignif-icant changes. In both the VD 1 CS and the VD 1 ISstimulation groups, LDM stimulation significantly in-creased peak aortic systolic and LV systolic pressures,peak positive LV dp/dt, stroke volume, peak aortic flow,stroke work, and stroke power. The differences betweenthe control group and either the VD 1 CS or the VD 1 ISgroup were statistically significant (p , 0.05). Comparedwith the VD 1 CS group, LDM stimulation in the VD 1IS group caused significantly greater increases in peak
1868 KASHEM ET AL Ann Thorac SurgVASCULAR DELAY AND INTERMITTENT LDM STIMULATION 2001;71:1866–73
by on June 10, 2013 ats.ctsnetjournals.orgDownloaded from
aortic pressure (15.3 mm Hg), peak LV pressure(17.3 mm Hg), peak positive LV dp/dt (1160 mm Hg persecond), stroke volume (11.2 mL), peak aortic flow(12.0 L/min), stroke work (14.5gm z m), and stroke power(171.2 gm z m per second).
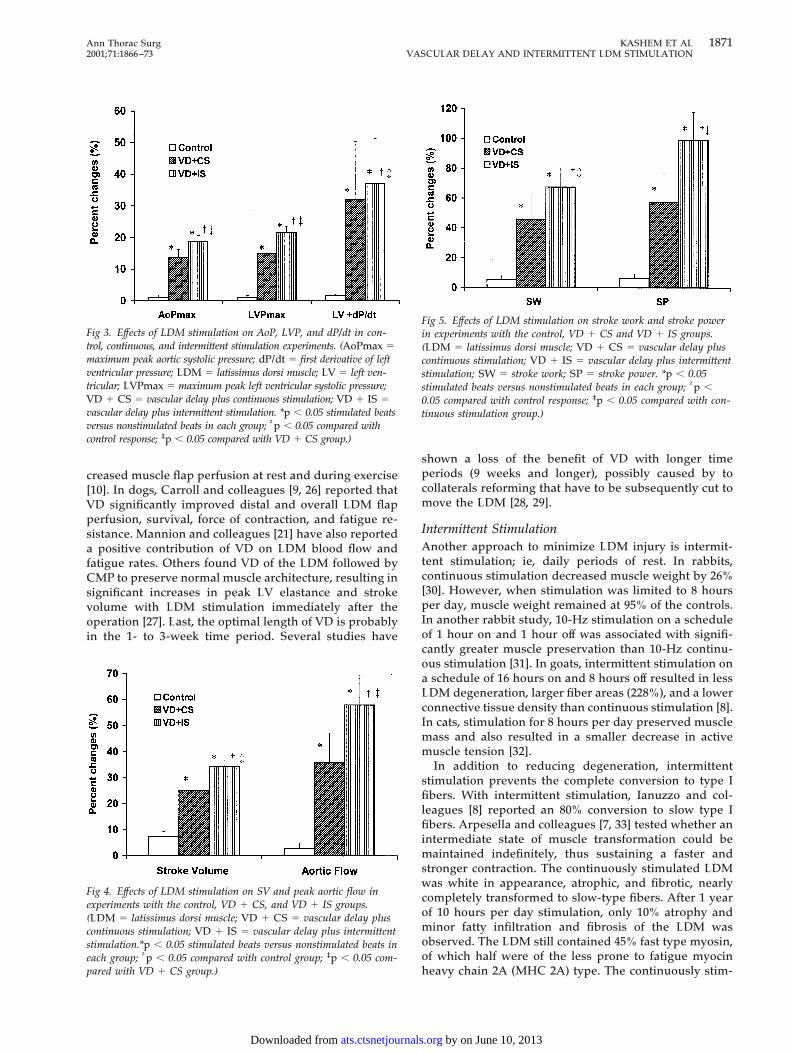
Figure 3 shows the percent changes in peak aorticpressure, peak LV pressure, and LV dp/dt caused byLDM stimulation. In the control group, LDM stimulationcaused only minimal nonsignificant changes in pressuresand dp/dt. In both the VD 1 CS and the VD 1 IS group,LDM stimulation significantly increased pressures andthe LV dp/dt (p , 0.05). Compared with the VD 1 CSgroup, LDM stimulation caused significantly greater per-cent changes in aortic and ventricular pressures, andmaximum LV dp/dt in the VD 1 IS group (p , 0.05).
Figure 4 shows the percent changes in stroke volumeand peak aortic flow caused by LDM stimulation. In thecontrol group, LDM stimulation caused only minimal,nonsignificant changes in stroke volume and peak aorticflow. In both the VD 1 CS and the VD 1 IS group, LDMstimulation increased stroke volume and peak aortic flowsignificantly (p , 0.05). Compared with the VD 1 CSgroup, LDM stimulation caused significantly greater per-cent changes in stroke volume and peak aortic flow in theVD 1 IS group (p , 0.05).
Figure 5 shows the percent changes in stroke work andstroke power caused by LDM stimulation. In the controlgroup, LDM stimulation caused minimal, nonsignificantchanges in stroke work and stroke power. In both theVD 1 CS and the VD 1 IS stimulation group, LDMstimulation increased stroke work and stroke power
significantly (p , 0.05). Compared with the VD 1 CSgroup, LDM stimulation caused significantly greater per-cent changes in stroke work and stroke power in theVD 1 IS group (p , 0.05).
Compared with the VD 1 CS group, LDM stimulationin the VD 1 IS group caused an additional increase in allof the following by: 37% in peak aortic pressure, 45% inpeak LV pressure, 16% in maximum LV dp/dt, 36% instroke volume, 62% in maximum peak aortic flow, 46% instroke work, and 72% in stroke power.
From the nitroblue tetrazolium staining and morpho-metric analysis in the control group, the average LDMarea around the heart at the papillary muscle level was28.8 6 1.5 cm2, whereas the nonviable LDM area was6.6 6 0.4 cm2. In the VD 1 CS group, total and nonviableareas were 30.7 6 2.2 cm2 and 4.0 6 0.1 cm2, respectively.In the VD 1 IS group, total and nonviable areas were31.7 6 1.2 cm2 and 2.1 6 1.0 cm2, respectively. Thepercentage of nonviable tissue in the LDM after CMPwas 10.5% 6 4.5% in the VD 1 CS group versus 7.5% 61.1% in the VD 1 IS group. These differences did notreach statistical significance. However, in both groupsthe percentages were significantly lower than in thecontrol group (28.5% 6 3.4%; p , 0.05).
Comment
Most clinical CMP studies have reported a significantimprovement in functional class only, unaccompanied bymeasurable improvements in LV systolic function [17].Distal muscle atrophy, loss of contractile function, muscledegeneration, and necrosis are probably responsible forthese disappointing results [14, 18–20].
Cardiomyoplasty operations involve severing the per-forating intercostal arteries to the LDM, and transferringthe muscle into the chest as a rotational flap. This causesdistal LDM ischemia [21]. In addition, extensive fibrosisand degeneration of the distal LDM have been reported[13]. In goats, LDM injury correlated with poor hemody-namic outcome [22]. Clinically, magnetic resonance im-aging showed that LDM thickness decreased from19.6 mm at 15 days postoperatively to 7.6 mm at 24 to 52months postoperatively [23]. Further, LDM signal inten-sity was comparable with thoracic muscles shortly afteran operation, but by 24 months it resembled that ofsubcutaneous fat. Latissimus dorsi muscle atrophy hasalso been documented by echocardiography [24].
Vascular Delay Procedure
The term vascular delay was coined by reconstructivesurgeons to describe a procedure whereby a flap of tissuesupported by a vascular pedicle is raised in 2 or morestages separated by intervals of 1 to 3 weeks [25]. In thefirst stage, the tissue is made subcritically ischemic,which stimulates revascularization. These vascularchanges play a major role in protecting the tissue at thetime of definitive flap transfer. As opposed to vasculardelay, the term delay used in most CMP literature de-scribes an unstimulated period after the wrapping of the
Fig 1. Hemodynamic measurements before and after intracoronarymicrosphere injections in control, vascular delay plus continuousstimulation ( VD 1 CS), and vascular delay plus intermittent stimu-lation ( VD 1 IS) experiments. (AoP 5 peak aortic systolic pres-sure; LVEDP 5 left ventricular end-diastolic pressure; LVP 5 peakleft ventricular systolic pressure; Post 5 postoperative; Pre 5 pre-operative; SV 5 stroke volume; SW 5 stroke work. *p , 0.05,LVEDP, SV, and SW compared preoperative versus postoperativeintracoronary microsphere injections in each group; †p , 0.01, LVPcompared preoperative and postoperative intracoronary microsphereinjections in each group; ‡p , 0.01 AoP compared preoperative ver-sus postoperative intracoronary microsphere injections in eachgroup.)
1869Ann Thorac Surg KASHEM ET AL2001;71:1866–73 VASCULAR DELAY AND INTERMITTENT LDM STIMULATION
by on June 10, 2013 ats.ctsnetjournals.orgDownloaded from
LDM around the myocardium, allowing healing of thestriated muscle [17]. This delay in stimulating the LDM isnot equivalent to vascular delay because it does notinclude an initial critical period of muscle ischemia.
Tobin and colleagues [6] examined the intramuscularvascular distribution in LDMs by using radiographplanimetry in fresh human cadavers. Tobin and col-leagues [6] found an average of 15 perforating intercostalarteries, contributing 67% of the LDM vascular supply. In
dogs, perforating intercostal arteries contributed 69%of the LDM arterial supply. These perforating inter-costal arteries must be sectioned to mobilize the LDM.Distal muscle ishemia occurs when the entire LDM isacutely raised on a single neurovascular pedicle, a ma-neuver followed by a decrease in distal flow to 2.2mL/min/100 g [5].
Several studies have examined the effects of VD on theLDM. In dogs, a 1-month VD period significantly in-
Fig 2. (A) Representative tracings from a control animal: aortic flow(L/min), LV and aortic pressures (mm Hg), LV dP/dt (mm Hg/sec),and ECG. (B) Representative tracings from VD 1 CS experiment.(C) Representative tracings from VD 1 IS experiment. (CS 5 con-stant stimulation; ECG 5 electrocardiogram; IS 5 intermittent stim-ulation; LV 5 left ventricular; S 5 stimulated beats; VD 5 vasculardelay.)
Table 1. Absolute Changes in Hemodynamic Measurements With LDM Stimulation
AoPmax(mm Hg)
LVPmax(mm Hg)
Max dp/dt(mm Hg/sec) SV (mL)
Peak AoF(L/min)
SW(gm z m)
Stroke Power(gm z m/s)
Controls 21.5 6 9.7 20.3 6 0.9 229 6 8 22.3 6 1.0 0.1 6 0.3 23.1 6 1.0 6.0 6 10.1VD 1 CS 12.3 6 1.2a,b 12.4 6 2.0a,b 238 6 67a,b 3.9 6 1.8a,b 2.2 6 0.8a,b 6.4 6 1.5a,b 51.5 6 10.3a,b
VD 1 IS 17.6 6 1.7a,b,c 19.7 6 1.1a,b,c 398 6 144a,b,c
5.1 6 0.7a,b 4.2 6 0.6a,b 10.9 6 0.9a,b,c 122.7 6 11.6a,b,c
a p , 0.05 5 stimulated beats versus non-stimulated beats in each group. b p , 0.05 compared to control response. c p , 0.05 compared tocontinuous stimulation group.
AoPmax 5 maximum peak aortic pressure; CS 5 continuous stimulation; IS 5 intermittent stimulation; LVPmax 5 maximum peak leftventricular pressure; Max dp/dt 5 maximum peak first derivative of the left ventricular pressure; Peak AoF 5 maximum peak aorticflow; SV 5 stroke volume; SW 5 stroke work; VD 5 vascular delay.
1870 KASHEM ET AL Ann Thorac SurgVASCULAR DELAY AND INTERMITTENT LDM STIMULATION 2001;71:1866–73
by on June 10, 2013 ats.ctsnetjournals.orgDownloaded from
creased muscle flap perfusion at rest and during exercise[10]. In dogs, Carroll and colleagues [9, 26] reported thatVD significantly improved distal and overall LDM flapperfusion, survival, force of contraction, and fatigue re-sistance. Mannion and colleagues [21] have also reporteda positive contribution of VD on LDM blood flow andfatigue rates. Others found VD of the LDM followed byCMP to preserve normal muscle architecture, resulting insignificant increases in peak LV elastance and strokevolume with LDM stimulation immediately after theoperation [27]. Last, the optimal length of VD is probablyin the 1- to 3-week time period. Several studies have
shown a loss of the benefit of VD with longer timeperiods (9 weeks and longer), possibly caused by tocollaterals reforming that have to be subsequently cut tomove the LDM [28, 29].
Intermittent StimulationAnother approach to minimize LDM injury is intermit-tent stimulation; ie, daily periods of rest. In rabbits,continuous stimulation decreased muscle weight by 26%[30]. However, when stimulation was limited to 8 hoursper day, muscle weight remained at 95% of the controls.In another rabbit study, 10-Hz stimulation on a scheduleof 1 hour on and 1 hour off was associated with signifi-cantly greater muscle preservation than 10-Hz continu-ous stimulation [31]. In goats, intermittent stimulation ona schedule of 16 hours on and 8 hours off resulted in lessLDM degeneration, larger fiber areas (228%), and a lowerconnective tissue density than continuous stimulation [8].In cats, stimulation for 8 hours per day preserved musclemass and also resulted in a smaller decrease in activemuscle tension [32].
In addition to reducing degeneration, intermittentstimulation prevents the complete conversion to type Ifibers. With intermittent stimulation, Ianuzzo and col-leagues [8] reported an 80% conversion to slow type Ifibers. Arpesella and colleagues [7, 33] tested whether anintermediate state of muscle transformation could bemaintained indefinitely, thus sustaining a faster andstronger contraction. The continuously stimulated LDMwas white in appearance, atrophic, and fibrotic, nearlycompletely transformed to slow-type fibers. After 1 yearof 10 hours per day stimulation, only 10% atrophy andminor fatty infiltration and fibrosis of the LDM wasobserved. The LDM still contained 45% fast type myosin,of which half were of the less prone to fatigue myocinheavy chain 2A (MHC 2A) type. The continuously stim-
Fig 3. Effects of LDM stimulation on AoP, LVP, and dP/dt in con-trol, continuous, and intermittent stimulation experiments. (AoPmax 5maximum peak aortic systolic pressure; dP/dt 5 first derivative of leftventricular pressure; LDM 5 latissimus dorsi muscle; LV 5 left ven-tricular; LVPmax 5 maximum peak left ventricular systolic pressure;VD 1 CS 5 vascular delay plus continuous stimulation; VD 1 IS 5vascular delay plus intermittent stimulation. *p , 0.05 stimulated beatsversus nonstimulated beats in each group; †p , 0.05 compared withcontrol response; ‡p , 0.05 compared with VD 1 CS group.)
Fig 4. Effects of LDM stimulation on SV and peak aortic flow inexperiments with the control, VD 1 CS, and VD 1 IS groups.(LDM 5 latissimus dorsi muscle; VD 1 CS 5 vascular delay pluscontinuous stimulation; VD 1 IS 5 vascular delay plus intermittentstimulation.*p , 0.05 stimulated beats versus nonstimulated beats ineach group; †p , 0.05 compared with control group; ‡p , 0.05 com-pared with VD 1 CS group.)
Fig 5. Effects of LDM stimulation on stroke work and stroke powerin experiments with the control, VD 1 CS and VD 1 IS groups.(LDM 5 latissimus dorsi muscle; VD 1 CS 5 vascular delay pluscontinuous stimulation; VD 1 IS 5 vascular delay plus intermittentstimulation; SW 5 stroke work; SP 5 stroke power. *p , 0.05stimulated beats versus nonstimulated beats in each group; †p ,0.05 compared with control response; ‡p , 0.05 compared with con-tinuous stimulation group.)
1871Ann Thorac Surg KASHEM ET AL2001;71:1866–73 VASCULAR DELAY AND INTERMITTENT LDM STIMULATION
by on June 10, 2013 ats.ctsnetjournals.orgDownloaded from

ulated LDM generated only 0.5 W of external power,while the 10 hours per day LDM generated 2 W ofexternal power without fatigue. Comparing long-termcontinuous versus intermittent stimulation, Duan andcolleagues [34] found that intermittent stimulation pre-vented power loss in fatigue-resistant muscles.
Literature ComparisonIn a review article, we summarized the results of 6chronic animal CMP studies [35]. In these chronic CMPstudies, LDM stimulation caused only small and physio-logically insignificant increases in LV pressure (4%),stroke volume (8%), and stroke work (8%). These resultsare very similar to the results from the control group inthe present study: LDM stimulation increased LV pres-sure by 1%, stroke volume by 7%, and stroke work by 5%.
Over the last several years, the goal of our laboratorywas to obtain physiologically significant increases inpeak LV systolic pressure and stroke volume with LDMstimulation. In an initial study, we measured the effects ofLDM stimulation 2 weeks after a CMP operation, a timeat which LDM stimulation is usually initiated in humans[14]. In 4 of 11 experiments, LDM stimulation had noeffect on LV function, and in the remaining experiments,LDM stimulation caused only a small increase in LVpressure, stroke work, and LV dp/dt. Thus, withoutpreconditioning most of the potential LDM assistancewas already lost by 2 weeks.
We have found VD essential to obtain large, consistentimprovements in hemodynamic measurements withLDM stimulation [11, 15]. In the next study, half theanimals underwent a VD procedure 2 weeks before aCMP operation [11]. Again, the effects of LDM stimula-tion were measured 2 weeks after a CMP operation. WithVD, LDM stimulation caused large increases in peak LDsystolic pressure (20%), stroke volume (45%), and strokework (64%) [11]. These data confirm the efficacy andindispensable nature of the VD procedure in CMP,without which LDM stimulation lost most of its hemody-namics effects within 2 weeks after the initial operation.
These data, however, were obtained 2 weeks after theCMP operation, before chronic LDM conditioning.Therefore, the present study determined whether the VDwould remain beneficial after LDM training. At 9 weeksafter CMP, in the group that was stimulated 24 hours perday (the current clinical practice), LDM simulation in-creased peak LV pressure by 15%, stroke volume by 25%,and stroke work by 46%. These increases are consider-ably larger than previously reported in chronic experi-mental studies [35]. However, these increases are consid-erably smaller than our previous results obtained 2weeks after CMP operation.
These results suggest that other simulation modes areneeded to maintain the long-term LDM contribution toLV systolic performance. Intermittent stimulation wastested in the present study. Now, LDM stimulation re-sulted in significantly larger increases in peak LV pres-sure (22%), stroke volume (34%), and stroke work (67%)than continuous stimulation. In total, these studies indi-cate that the combination of VD and IS are essential to
obtain physiologically important increases in LV pres-sure, stroke volume, and stroke work with LDMstimulation.
ImplicationsThe assistance of every cardiac cycle by the LDM may bean unattainable goal. Instead, LDM assistance to cardiacfunction may be best offered at times of increased de-mands. The measurement of daily physical activity inyoung, healthy volunteers by accelerometer showed thatonly 4.2% of the day (about 1 hour per day) was spent inphysical activities requiring $ 4 METS [36]. Thus, a fewhours of support would markedly improve the quality oflife of a patient with heart failure. This would allow thepatient to engage in more activities and recreation, in-cluding golf, gardening, or light swimming.
ConclusionsIn conclusion, combining VD with IS allowed large in-creases in LV pressure and stroke volume with LDMstimulation. Additional experiments are needed to con-firm these results over longer periods of observation. Ifthey are confirmed, however, changes in techniques ofCMP for the treatment of patients with congestive heartfailure should be strongly considered.
This study was supported in part by NIH grant No. HL-60084and a grant of the Jewish Hospital for Heart and LungFoundation.
Our thanks to Dr James Sharp, Dr Karla Stevens, Nancy Hughes,Edwin Ford, Dorothy Wilson, and Tracey Girard for their dedi-cated care of the animals in the preoperative and postoperativeperiod.
The authors express their gratitude to Medtronic, Inc (Minne-apolis, MN) for providing technical support.
References
1. Nakajima H, Niinami H, Hooper TL, et al. Cardiomyoplasty:probable mechanism of effectiveness using the pressure-volume relationship. Ann Thorac Surg 1994;57:407–15.
2. Capouya ER, Gerber RS, Drinkwater DC Jr, et al. Girdlingeffect of nonstimulated cardiomyoplasty on left ventricularfunction. Ann Thorac Surg 1993;56:867–71.
3. Patel HJ, Lankford EB, Polidori DJ, et al. Dynamic cardiomy-oplasty: its chronic and acute effects on the failing heart.J Thorac Cardiovasc Surg 1997;114:169–78.
4. Hagege AA, Desnos M, Fernandez F, et al. Clinical study ofthe effects of latissimus dorsi muscle flap stimulation aftercardiomyoplasty. Circulation 1995;92:II-210–5.
5. Cruz MP, Michele JJ, Mannion JD, Magno M, George DT,Santamore WP. Cardiomyoplasty: latissimus dorsi musclefunction and blood flow during isolation. ASAIO J 1997;43:338–44.
6. Tobin G, Gu JM, Tobin AE, et al. The anatomic basis forlatissimus dorsi cardiomyoplasty flap loss. AAMI, Proc Car-diovasc Sci Tech Conf 1991;69B.
7. Arpesella G, Carraro U, Mikus PM, et al. Activity-reststimulation of latissimus dorsi for cardiomyoplasty: 1-yearresults in sheep. Ann Thorac Surg 1998;66:1983–90.
8. Ianuzzo CD, Ianuzzo SE, Carson N, et al. Cardiomyoplasty:degeneration of the assisting skeletal muscle. J Appl Physiol1996;80:1205–13.
9. Carroll SM, Carroll CM, Stremel RW, Heilman SJ, Tobin GR,
1872 KASHEM ET AL Ann Thorac SurgVASCULAR DELAY AND INTERMITTENT LDM STIMULATION 2001;71:1866–73
by on June 10, 2013 ats.ctsnetjournals.orgDownloaded from
Barker JH. Vascular delay of the latissimus dorsi muscle: anessential component of cardiomyoplasty. Ann Thorac Surg1997;63:1034–40.
10. Isoda S, Yano Y, Jin Y, Walters HL, III, Kondo J, MatsumotoA. Influence of a delay on latissimus dorsi muscle flap bloodflow. Ann Thorac Surg 1995;59:632–8.
11. Ali AT, Santamore WP, Chiang BY, Dowling RD, Tobin GR,Slater AD. Vascular delay of the latissimus dorsi provides anearly hemodynamic benefit in dynamic cardiomyoplasty.Ann Thorac Surg 1999;67:1304–11.
12. Lavine SJ, Prcevski P, Held AC, Johnson V. Experimentalmodel of chronic global left ventricular dysfunction second-ary to left coronary microembolization. J Am Coll Cardiol1991;18:1794–803.
13. Cheng W, Michelle J, Spinale FG, Sink JD, Santamore WP.Effects of cardiomyoplasty on biventricular function in ca-nine chronic heart failure. Ann Thorac Surg 1993;55:893–901.
14. Chiang BB, Ali AT, Storey J, et al. Variable effects of cardio-myoplasty on left ventricular function. Artif Organs 1997;21:1277–83.
15. Chiang BB, Ali A, Kashem A, et al. Two step cardiomyo-plasty with vascular delay: effect of stimulation of latissimusdorsi muscle on diastolic function. ASAIO J 1999;45:350–5.
16. Pang CY, Yang RZ, Zhong A, Xu N, Boyd B, Forrest CR.Acute ischaemic preconditioning protects against skeletalmuscle infarction in the pig. Cardiovasc Res 1995;29:782–8.
17. Chachques JC, Grandjean PA, Carpentier A. Patient man-agement and clinical follow-up after cardiomyoplasty. J CardSurg 1991;6(Suppl 1):89–99.
18. Furnary AP, Chachques JC, Moreira LF, et al. Long-termoutcome, survival analysis, and risk stratification of dynamiccardiomyoplasty. J Thorac Cardiovasc Surg 1996;112:1640–50.
19. El Oakley RM, Jarvis JC. Cardiomyoplasty: a critical reviewof experimental and clinical results. Circulation 1994;90:2085–90.
20. Magovern GJ, Sr, Simpson KA. Clinical cardiomyoplasty:review of ten-year United States experience. Ann ThoracSurg 1996;61:413–9.
21. Mannion JD, Velchik M, Hammond RL, et al. Effects ofcollateral blood vessel ligation and electrical conditioning onblood flow in dog latissimus dorsi muscle. J Surg Res 1989;47:332–40.
22. Lucas CM, Van der Veen FH, Cheriex EC, et al. Long-termfollow up (12 to 35 weeks) after dynamic cardiomyoplasty.J Am Coll Cardiol 1993;22:758–67.
23. Kalil-Filho R, Bocchi E, Weiss RG, et al. Magnetic resonanceimaging evaluation of chronic changes in latissimus dorsicardiomyoplasty. Circulation 1994;90:II-102–6.
24. Yoshiya T, Tsukube T, Okada M, Mukai T, Kashem MA.Echocardiographic evaluation of latissimus dorsi muscle flapin cardiomyoplasty [Abstract]. Chest 1996;110:4–22S.
25. Cormack GC, Lamberty BG. The arterial anatomy of skinflaps. London: Churchill Livingstone 1986:43–44.
26. Carroll, SM, Carroll CM, Stremel RW, et al. Vascular delayand administration of basic fibroblast growth factor augmentlatissimus dorsi muscle flap perfusion and function. PlastReconstr Surg 2000;105:964–71.
27. You J, Landymore RW, Fris J. Effect of cardiomyoplasty onsystolic and diastolic function. Eur J Cardiothorac Surg 1995;9:672–7.
28. Mannion JD, Acker MA, Hammond RL, Faltemeyer W,Duckett S, Stephenson LW. Power output of skeletal muscleventricles in circulation: shot-term studies. Circulation 1987;76:155–62.
29. Mannion JD, Hammond RL, Stephenson LW. Hydraulicpouches of canine latissimus dorsi: potential for left ventric-ular assistance. J Thorac Cardiovasc Surg 1986;91:534–44.
30. Pette D, Muller W, Leisner E, Vrbova G. Time dependenteffects on contractile properties, fiber population, myosinlight chains and enzymes of energy metabolism in intermit-tently and continuously stimulated fast twitch muscles of therabbit. Pflugers Arch 1976;364:103–12.
31. Lexell J, Jarvis J, Downham D, Salmons S. Stimulation-induced damage in rabbit fast-twitch skeletal muscles: aquantitative morphological study of the influence of patternand frequency. Cell Tissue Res 1993;273:357–62.
32. Ferguson AS, Stone HE, Roessmann U, Burke M, Tisdale E,Mortimer JT. Muscle plasticity: comparison of a 30-Hz burstwith 10-Hz continuous stimulation. J Appl Physiol 1989;66:1143–51.
33. Arpesella G, Mikus PM, Pierluca L, et al. Activity-restregimen of latissimus dorsi stimulation for cardiomyoplasty:anatomy, isomyosins and sustained power of sheep LD up toone year. Basic Applied Myology (http://www bio unipdit/bam/bam html) 1997;7:45–53.
34. Duan C, Trumble DR, Scalise D, Magovern JA. Intermittentstimulation enhances function of conditioned muscle. Am JPhysiol 1999;276:R1534–40.
35. Santamore WP, Ali A, Stremel R, et al. Strategies for pre-serving muscle function for improved systolic assist indynamic cardiomyoplasty. Basic Applied Myology 1998;8:51–8.
36. Matthews CE, Freedson PS. Field trial of a three-dimensional activity monitor: comparison with self report.Med Sci Sports Exerc 1995;27:1071–8.
1873Ann Thorac Surg KASHEM ET AL2001;71:1866–73 VASCULAR DELAY AND INTERMITTENT LDM STIMULATION
by on June 10, 2013 ats.ctsnetjournals.orgDownloaded from

2001;71:1866-1873 Ann Thorac Surgand A. David Slater
Abul Kashem, William P. Santamore, Benjamin Chiang, Lauren Unger, Ahsan T. Ali muscle stimulation
Vascular delay and intermittent stimulation: keys to successful latissimus dorsi
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/71/6/1866including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/71/6/1866#BIBL
This article cites 30 articles, 17 of which you can access for free at:
Citationshttp://ats.ctsnetjournals.org/cgi/content/full/71/6/1866#otherarticlesThis article has been cited by 1 HighWire-hosted articles:
Subspecialty Collections
assistancehttp://ats.ctsnetjournals.org/cgi/collection/mechanical_circulatory_
Mechanical Circulatory Assistancefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 10, 2013 ats.ctsnetjournals.orgDownloaded from