tanzania medical journal - special issue - idrc digital library
TRANSCRIPT
TA ftL2 A NIA MEDICA L JO URNA L SPECIAL ISSUE
6
Proceedings of the International Conference on Traditional Medicine Held in
Arusha 6th— 8th October, 1986
Published by the Tanzania Medical Journal.
The Official Mouth Organ of Medical Association of Tanzania.
ACKNOWLEDGMENTS We are indebted to the International Development
Research Centre of Canada (IDRC) for supporting the research on which the conference was based, sponsoring the conference and eventual publication of the proceedings. Special thanks should go to the Director General of Muhim- bili Medical Centre for allowing us to use the Centre's Ser- vices and Ministry of Health in Tanzania for encouragement and allowing the research to take place. We also thank Mr. E.M. Mshiu, Dr. LA.J. Semali, Mr. D. Do Amsi and Dr. E.P. Muhondwa for theirorganisational and editorial services. Last but not least we are idebted to Mrs. Mugashi for her sec- retarial services.
Charles S. Mgone M.D. Editor December, 1987
TABLE OF CONTENTS
Page
Welcome Address
ByMr.E.N.Mshiu 1
Miristers Opening Address
By Dr. A. Chiduo 2 Role of Traditional Medicine in Health care Delivery Systems By Olayiwola Akerele 3
Traditional Medicine Practice in Tanzania History and Development By Dr. E.N. Mshiu 7
Traditional Medicine To—morrow
ByDr.MurrayLast 10
Use of Non—Factual Questions in a Survey: Respondent's or interviewer's opinion By Dr. C.K. Makwaya 14
Attendant at Birth as a risk factor in child survival By Dr. E.D.'Mwaikambo and D.M. Do Amsi 15
Traditional Medicine in Tharaka Kenya By Dr. G. Giarelli 18
Knowledge of Malaria and some aspects of its Control in Tanga Tanzania
By Dr. M. Fivawo 21
Traditional Beliefs and Treatment, in measles
By Dr. F.H. Mrisho 22
The Pattern of illness and the utilization of available Health Service in two regions in Tanzania
By Mr. J.Z. Kilewo 25
The Impact of Traditional Health beliefs and
practices on health care utilization Pattens
By Dr. J.J. Nguma 30
INTERNATIONAL CONFERENCE ON TRADITIONAL MEDICINE WELCOME
ADDRESS BY MSHIU, E.N.
DIRECTOR OF TRADITIONAL MEDICINE RESEARCH UNIT
MUHIMBILI MEDICAL CENTRE 6TH OCTOBER, 1986
The Honourable Dr. Aaron Chiduo, Minister for Health and Social Welfare, Distinguished Party and Government officials, our Honourable Guests and Participants, Ladies and Gentlemen.
Itis a great honour and a special priviledge for me to wel- cme you, Sir, as our Guest of Hounour to this First Interna- tional Conference on Traditional Medicine in Tanzania which I will presently request you to open officially. I am sure all participants to this conference will joir me in expressing special appreciation to you for having spared the time in your extremely busy and demanding schedule to grace this occa- sion with your presence.
Hounourable Minister, the role of traditional medicine in the achievement of health for all by the year 2000 is currently a topic of discussion in a number of local and international forums. It is the feeling of many, that traditional medicine could be an alternative source of health care as more than 100 countries signed the Alma-Ata declaration which suggests that traditional medicine be incorporated in the delivery of primary health care, a suggestion which should now be considered seriously in Tanzania.
In some countries like China and India, traditional medicine has been institutionalized and there are formal training centres and libraries. Such institutionalization puts them in a better position to lntergrate traditional medicine in the delivery of primary health care.
In Tanzania and other parts of Africa there are some limited forms of institutionalizations. These clude ritual dancing groups, religious therapy groups and herapy groups. However these are self selective small groups, addressing themselves to particular small localities and are thus usually not uniform for the whole country.
In Tanzania, some researchers have observed the need of involving traditional healers in the delivery of health care. This need arises from the limitation of inputs required for provision of health facilities to every village in Tanzania. Thus traditional medicine is an alternative source for health care to many rural dwellers. It has for instance been observed that about 75% of all deliveries are conducted by traditional birth attendants.
It is thus obvious that traditional birth attendants tTBAs) cannot and should not be ignored. For instance in Senegal' and Sudan it has been observed that training or incorporat- ing of traditional birth attendants into the official health care
system has improved the coverage and acceptance of health care services.
A survey done on some health professionals in Tanzania
indicated that many of those interviewed appreciated the competence of traditional healers in some of their practices. Some indicated that these traditional healers were a poten- tial source of health care manpower and means of educating them on some aspects of-modern medicine be considered. One may argue that in the above mentioned survey the responding health workers may have not necesarily been representative of the health workers population in Tanzania, but positive developments in other countries like Sudan, Nigeria and Ghana should counter this. In these countrie's collaboration at small scale level has proved very fruitful. Further researches should also be done to study the attitudes of traditional healers towards modern health care, utilization of traditional medicine and attitudes of the community towards traditional medicine in Tanzania.
In Oar es Salaam, it is estimated that about 8,000 people consulted traditionaithealers daily for various health prob- lems, in 1974. This implies that the presence of modern health facilities may not necessarily affect the utilization of traditional medicine. We have no doubt that the same trend may be observed in the rural sector of Tanzania.
It is because of the foregoing reasons, Traditional Medicine Research Unit in collaboration with departments of Behavioural Science, and Biostatistics and Epidemiology prepared and submitted a proposal to International Develop- ment Research Centre, Canada (D.R.C.) to fund a project which would enable us to determine the attitude and knowl- edge of traditional healers and birth attendants on modern health care an&to determine the utilization pattern of tradi- tional medicine by the rural population of Tanzania. This information is important in the planning of health care deliv- ery if the goal of health for all by the year 2000 is to be met. This information would also be helpful in the intergration and institutionalization of traditional medicine in the coun- try. Following IDRC, release of funds to the project, the col- laborating institutions decided to carry the study in two reg- ions of Tanzania Mainland namely, Iringa and Arusha reg- ions.
In Arusha region, Hanang and Babati districts were sur-
veyed. Fifty villages in 4 divisions were involved and 1999
people interviewed. These included 169 traditional healers and 105 traditional birth attendants. In Iringa Region, 56 vil-
lagés in 9 divisions were involved and 2,617 people including 159 traditional healers and 208 traditional birth attendants interviewed. The study was carried out between March, 1985 1
and February, 1986 at an estimated cost of Canadian dollars 121,260 which was equivalent to Tanzania shillings 1,091,340, at that time. For this we are grateful indeed to IDRC.
Honourable Minister, before I request you to open this conference, I would like to inform you that.the participants to the conference are from Canada, United Kingdom, Kenya, Italy, Zimbabwe, Uganda, Swaziland and Tanzania.
I now have The honour to call upon you, Sir, to address participants and declare the conference open.
E. N. Mshiu, Director, Traditional Medicine Research Unit, Muhirnbili Medical Centre, P.O. Box 65000, Oar es Salaam.
I

OPENING ADDRESS BY THE MINISTER FOR HEALTH AND SOCIAL WELFARE HON. DR.
A. D. CHIDUO (MP) TO TRADITIONAL MEDICINE SEMINAR OCTOBER 6, 1986
Mr. Chairman, Distinguished Guests, Ladies and Gentlemen.
May I start by expressing my sincere gratitude for the honour bestowed on me to officially open this seminar, on this wide ranging and interesting subject of Traditional Medicine.
Evidently, in recent years there has grown tremendous interest in this subject, despite enormous and almost unparalled advances in orthodox medicine. The main reason behind this overwhelming interest in traditional medicine is the failure of modern medicine to come up with sufficient answers to all health problems especially in Third Wor.ld countries and the fact that traditional medicine is the only source of care for many people in the Third World. It is esti- mated that approximately 50% of the population receive health care from traditional sources.
Your presence in this seminar, of people of high academic and professional standing, is a vivid example of the general interest shown in traditional medicine.
Traditional medicine has been practiced for as long as we can care to remember. Through trial and error, human beings have discovered ways of relieving pain and sickness and living in harmony with nature. Many societies regard health as a state of equilibrium both internal and external to the human body. Health has been defined as a state of har- mony between man and his internal and external environ- ment; biological, physical, social,economic and cultural. Life is defined as the union of the body, senses, mind and soul. Positive health is therefore the right mix of physical, mental, social and spiritual welfare. Moral and spiritual aspects are
important because they give an extremely important dimen- sion in the resultant health sum total of all knowledge and
practices (whether they can be explained or not) used in the prevention, diagnosis and elimination of physical, mental or social imbalances and relying exclusively on practical experience handed down from generation to generation whether orally or ri writing.
One of the most striking features of traditional medicine is that it touches on so many other domains other than medicine proper. It takes a holistic approach; and thus fos- ters a broader view of the sickrnan as an individual with phys- i'al, social, psychological, moral and spiritual aberration or disturbance. The main problem of some of the procedures and practices in traditional medicine is that, they do not lend themselves easily to logical or scientific scrutiny. For some practices for instance acupuncture, it is hard to grasp the fact, that a needle prick at some point will improve the functioning of a certain organ. To the orthodox practictioner, the argu- ment is that it cannot happen. The main flaw in this argument is that it is immediately disproved by reality, for things do
happen that cannot be easily explained. For most comrtrnn ailments herbs are usually used. The
plant kingdom is a big storehouse for medicine. Many tradi-
2
tional healers use plant derrved concoctions or a mixture of plaftt derived substances with animal or mineral derived arti- cles. Because of the widespread use of plants and their local
availability particularly in developing countries it is of cardi- nal importance that they should be scientifically assessed to exclude those that might be toxic. The therapeutic properties of several medicinal plants and popular traditional, medical practices should be instigated and validated. The scientific. validation of any therapeutic result claimed in traditional medicine requires a carefully structured research design. In order to substantiate the claims of cures made by healers accurate scientific diagnosis should first be established and as many details as possible acquired from the traditional healers regarding the mode of preparation of the decoction or medicament, the specific design regimen however crude, the part or parts of plants used and any additional details per- taining to treatment. Medicinal plants of proven value cannot only meet important health needs and reduce national drugs importation bills, they can also under suitable climatic condi- tions be cultivated and exported so as to bring substantial foreign exchange earnings.
One area of controversy in traditional medicine is the role of the spirit healers. The attitudes towards them among orthodox medical practitioners has never been favourable. In many cultures mental or physical illness represents a dis- turbance of the relationship between the individual, his ancestral spirits and society. Under the circumstances human beings in their normal life activities sometimes offend their ancestral spirits unknowingly. The consequence of offending one's ancestral spirits is illness. Healing of such an illness is based on the stablishment and maintenance of satisfactory relationship between individuals, their ances- tors and the spirit world. It is the spirit healer who comes into
play to effect the wanted relationship and determine which laws have been transgressed. The spirit healer hands out amulets against the 'evil-eye' or prescribes induction of trances and magic dances and other rituals. The healer is at one and the same time a religious leader in touch with the ancestors and the spirit world and doctor who concerns him- self whith the sick and disabled. Modern trained doctors may regard magic-eye ceremonies as charlatancy but a closer scrutiny may reveal that this may be a means of preparing the patient for real medical treatment. Short term effects are almost always striking. Acute psychoses are calmed, family disputes resolved and hysterical phenomena disappear.
Traditional Birth Attendants (Midwives) constitute a
special category in the whole structure of traditional medicine. They form the main body of primary health care workers in maternal care and child delivery. With the training of a substantial number of professional midwives and scien- tific advances made in obstetrics, one would have simply wished traditional birth attendants away. However, we know, and it is an established fact that in most developing countries, many deliveries occur not in hospitals but in homes, and it is the traditional, midwives who deliver the babies. It is estimated that approximately 60% of the deliveries in this country are done by traditional midwives. Traditional Birth Attendants exist and they are here to stay. It is therefore, pertinent that efforts should be made to integ- rate them into the general system for delivery of health care.
They have a very useful role to play. The psychological and
physical support they give to expectant mothers throughout the maternity period and the prompt response they give to any call for assistance should be reinforced and help should
Dr. A. D. Chiduo (M.P.) Minister of Health and Social Welfare, Ministry of Health, P.O. Box 9083, Dar es Salaam.
be given to them to ensure that harmful practices are tacti- fully avoided.
Since traditional medicine is still widely practiced to good effect, should it not be officially recognised, encour- aged improved upon, and integrated into contemporary nan- tional health care system? The definite answer to this ques-. tion is yes. Traditional medical practices are part of our herit- age. Tradition is the sum of attitudes, opinions, beliefs, habits and customs handed down from generation to gener- ation in a given society. As such traditional medicine cannot be ignored. What is called for urgently is research into ways and means of incorporating useful traditional practices into the national health care system. We also need to intergrate traditional healers into health service. The idea of mobilizing the manpower component of traditional medicine for pur- pose of primary health care, particularly in rural areas has been gaining ground in many countries. However, we should not only consider the manpower component of traditional medicine. We should look at "Traditional medicine and its role in the development of health services in Africa." This calls for the promotion of traditional medicine and indigen- ous systems of medicine. To do this we have to foster a realistic approachto traditional medicine in order to improve health care. We have to evaluate traditional medicine in the light of modern science so as to maximize useful and effec- tive practices and discourage harmful ones and we have to promote the integration of proven valuable knowledge and skills in traditional and modern orthodox medicine. Tradi- tional medicine practices vary widely in different countries in keeping with their social and cultural traditions. What is needed is to promote such traditional medical practices in a self-reliant way. We have to identify ways and means in which traditional practitioners and traditional birth atten- dants can be trained and mobilized to play their proper role in the general health system without destroying their indi- viduality.
On the other hand I know that there is a lot of lip-service when it comes to real action. We keep talking of our pious intention of integrating traditional medicine into modern medicine; of training and mobilizing traditional healers and Traditional Birth Attendants. But are we serious? There is the interest but it is not matched by funds for action program- mes. In this country there has scarcely been any substantial budgetary provision for the promotion of traditional medicine as a system of health care in its own right. This I am sure is the position in the other countries in our region.
If indeginous practitioners are to be integrated into the countries' health services, much more need to be known about their numbers, where they are, how they practice and whom they serve. We need to establish a rapport with tradi- tional practitioners. We must break down the barrier of com- munication between the traditional practitioner and the modern trained orthodox health workers. But this will require political will and the need to allocate more funds to support traditional medicine -
We have an institution in this country for carrying out -research in ethnopharmacology and traditional systems of medical practice. The success of research in traditional medicine depends on how we first acquire knowledge from the traditiaonal healer himself; try out his methods clinically and subjectthem to scientific analysis. The aim should not be only to find cures wherewestern medicine has failed but also to find substitutes br imported- drugs and practices accept- able to the community. Research should also seek to identify
potent herbal drugs for such purposes as fertility regulation and treatment of chronic non-communicable diseases espe- cially cardiovascular diseases, diabetes, mental diseases test and the best and safe ways of using them. -
In conclusion, the contribution of traditional medicineS for the new universally accepted goal of health for all is potentially great. Ministries of Health, however, require gui- dance as well aS firm political decision and direction to com- mit them to pursue the objective of incorporating traditional medicine into the general health system. In this national gov- ernments can cooperate by way of exchanging experience and information. Where there is the will there is a way. Semi- nars like this will go a long way to stimulate action. It is action that we want not words.
With these few remarks, I wish you a successful and con- structive seminar. May I now take this opportunity to offi- cially declare your seminar open.
INTERNATIONAL CONFERENCE OF TRADITIONAL MEDICINE
ROLE OF TRADITIONAL MEDICINE IN HEALTH CARE DELIVERY SYSTEMS
by Olayiwola Akerele, M.D.
Traditional Medicine Programme World Health Organization
Geneva
First, I wish to thank my old friend Mr Mshiu, Director, Traditional Medicine Research Unit and the other organizers of this International Conference on Traditional Medicine, for the opportunity to speak to you today.
-
I thought it would be useful to utilize this occasion to cover some aspects of WHO's workin the field of traditional medicine.
The very international nature of this conference is a tes- timony to the success of the traditional medicine movement and a worthy measure of the work of the Traditional Medicine Research Unit of the Muhimbili Medical Centre, Dares Salaam.
This presentation has been adapted from the texts of two addresses delivered to the "Fourth Scientific Seminar", Aligarh, India, February 1985 and to the "World Symposium on Traditional Medicine, 1985", an International Conferen- on World Medicine, Up-date Traditional and Indigenous Sys tems of Medicine, March 1985, New York, USA. And an arti- cle entitled "Best of Both Worlds: bringing traditional medicine to date" (In Press) to appear in a forthcoming issue of Social Sciences and Medicine. Ladies and Gentlemen, I used to be a confortable WHO Doc- tor. Now I am an apprentice WHICH DOCTOR. Why am I an apprentice WHICH DOCTOR?
Partly bad luck and partly because of my previous Involvements in other WHO programmes.
To those of you who think I can't spell, I went to a night school and therefore I can't spell during the day. However, my adopted spelling has the advantage of separating my apprenticeship from those practices that are based on super- natural and spiritual considerations.
3
Role of Traditional Medicine in Health Care Delivery Sys- tems.
What do we consider as traditional medicine? One definition that we like to use considers traditional
medicine as comprising those practices based on beliefs that were in existence, often for hundreds of years; before the development and spread of modern scientific medicine and which are still in use today. They vary widely in different countries in keeping with their social and cultural heritage and traditions.
While no definition could be entirely satisfactory, the above has the advantage of simplicity while at the same time it excludes practices of more recent origin, thereby keeping the area of study discrete.
If there is to be any real improvement in the health of the underserved populations of the world, there will have to be a
full utilization of all available resources, human and material. This is fundamental to the primary health care approach — the strategy adopted by WHO Member States for attaining the collective goal of Health for All by the Year 2000.
However, traditional medicine has been separated from the mainstream of modern medicine. A basic approach, therefore, has been to promote the bringing-of modern sci- entific medicine with the proven, useful traditional practices within the framework of the local health system, where pos- sible, as called for by the different resolutions of the govern- ing bodies of WHO.
World Health Organization's Role
The last decade has seen a resurgence of interest in the study and use of traditional systems of medicine in different cultural settings. Most of the work in this domain have been done outside the aegis of WHO. While these efforts are acknowledged and encouraged, one might justifiably ask —
what is the role of an international organization such as WHO has a constitutional responsibility for international health work.1 Therefore, it should encourage countries to re- examine their traditional systems of medicine with a view to the utilization of safe and positive elements in national care delivery systems.
One of the early objectives of WHO's traditional medicine programme was to foster a realistic approach to the subject. The realism with which countries around the world, both developed and developing, are examining their own traditional practices suggests that good progress is being made towards this goal.
WHO is not a boyscout organization. It is not a charitable institution either, it is an inter-governmental organization. The countries themselves constitute the governing bodies of WHO — they decide collectively how the organization hould proceed and what should be the policies that would best create a general awareness of the fact that there are useful elements of traditional medicine that could be incorporated into national health systems.
Key Features of WHO Resolutions
Being an intergovernmental organization most things
begin with resolutions. Now let us examine some key resolu-
tions in support of traditiotal medicine programme. It all began in 1976 with resolution WHA 29.72 which
draw attention to the manpower reserve constituted by prac- titioners of traditional medicine. The majority of the world's population depend on traditional medicine for their primary
4
health care needs and therefore this resolution makes good sense. In 1977, WHA 30.49 urged Member States to utilize their traditional systems of medicine. Again, this is econom- ically sound because traditional medicine is the people's medicine and is always readily available to them at a price that they could afford. However, recent developments if not controlled could negate this statement. In 1978, resolution WHA 3133 highlighted the importance of medicinal plants in the health care systems of many developing countries. In
addition, there are also resolutions of the Executive Board and Regional Committees of WHO, all of which called for the intensification of efforts in the development of national trad- itional medicine programme.
In 1978, the Alma Ata Declaration2, that milestone in public health history, recommended to give high priority to the utilization of traditional medicine practitioners and birth attendants. It also recommended incorporating proved trad- itional remedies into national drug policies and regulations and called for further research, as new problems are con- stantly emerging. This was the first time that an international body made special mention of the potentiality of the use in the health services of traditional remedies, qspecially natu- ral products derived from medicinal plants, through formula- tion of policies and regulations.
In spite of the universal call for traditiaonal medicine to play an important role in the development of primary health care, there are still many countries where only lip service is being paid to this principle. Other countris have initiated programmes that have had to be abandoned because they were introduced without the necessary preparatory policy formulation and implementation steps.
— Where, then, do we stand today? — What are the main thrusts of WHO Programme in
traditional medicine? — What progress has been achieved and what are the
prospects for the future? The field is vast. The traditional medicine programme,
which started some eleven years ago, has therefore focussed on three important aspects, namely:
— Evaluation — Traditional medicine as part of national health care
system — Training This morning, I would like to share with you some
thoughts on the development and implementation of the WHO programme.
Evaluation
Evaluation is the most difficult and yet the most needed field of endevour. If a generalization may be permitted, one might say that traditional medicine has the support of the population and the opposition of the health professions.
Tbe most important task for WHO, therefore, is to con- tinue to promote informed opinion on the subject so that traditional medicine is neither blindly endorsed nor rejected by health authorities but is examined carefully and with an open mind.
Countries where traditional medicine is widely practiced are therefore being encouraged to re-examine their tradi- tional medicine practices and systems by undertaking multi-
disciplinary studies into the safety and efficacy of traditional remedies. Some people have drawn an erroneous analogy between multi-disciplinary research and the proverbial three blind men exposed to an elephant for the first time. It is
wrong to describe an elephant as a rope when all you can feel • is a piece of its tail. Only by working together can the whole image emerge.
Such an examination, of course, is much easier in sys- tems of medicine for which the philosophy and educational content are well documented than in the case of traditional remedies handed down from generation to generation by word of mouth.
However, in spite of the difficulties encountered, the examination of all these systems shows that they hold great promise of a rich harvestthat can benefit mankind, especially in the field of ethno-pharmacology.
Medicinal plants constitute a most important element in traditional medicine. In most developing countries the flora remains virtually unexplored from the point of view of practi- cal utilization, yet past experience shows that many valuable drugs have been derived from plants. Information that a plant is utilized in traditional medicine is often an indication that it is worth scientific study3.
WHO will continue to play a role in sketching the main lines of action needed for the indentification and introduc- tion of traditional medicinal plant remedies into national pri- mary health care programmes. Further success will, of course, depend heavily on the resources channeled to these
endavour by Member States. However, there is virtually no interest in exploring plants as sources of new drugs by phar- maceutical in developed countries.One wonders why?4.
Since only a fraction of the world's plant has been studied, just think of the major changes in the practice of - medicine that was brought about by examples of the discov- ery of only three drugs drom plants. Consider the impact of curare of th act of surgery. The importance of penicillin on morbidity and mortality of communicable disease. And the effect of reserpine on high blood pressure. These three drugs alone have dramatically altered our life expectancy and indeed the quality of life on earth5
Briefly, the aim of the evaluation component of WHO programme is to put traditional medicine on a scientific basis by:
could be utilized in national health services, especially at the primary health care level.
Other national research centres are being identified as reference centres with the view to develop collaborative activities, linking institutions with each other, as part of inter- country and inter-regional networks on the basis of culture and subject specificity.
Integration into National Health Care system
All of this is not a short-term undertaking but one that will take many years. In the meantime, we move towards the integration of traditional medicine into national health care' systems, incorporating only those aspects which have been shown to be beneficial and desirable.
The first step is the formulation and implementation of relevant policies and legislation on the utilization of proven traditional medicine in national health system.
The next is to promote the incorporation of traditional medicine into general health systems through operational research, utilization of traditional medicine practitioners vill- ing to collaborate, etc.
Where traditional medicine is well established and seen as a valuable asset for health promotion, traditional prac- titioners should be involved in the process which strengthens links between traditional medicine and th gen- eral health delivery system. They should help in the identifi- cation of the problems associated with the establishment of linkages at the local level. They should be involved in the planning, implementation and evaluation of community health activities so as to enhance working relationship between themselves and other members of the healthtearn.
First and foremost, of course, the apractitioners should be involved in the evaluation of their own practices, so as to facilitate the ready acceptance by their peers of suggestions for change, including the assumption of new responsibilities in, for example, the field of health education What this implies for WHO is; 1. Support for the elaboration and implementation of appropriate national policies and a legal framework for the •practices of traditional medicine;
2. Development of a practical coordinating mechanism between health institutions, related social sectors and community agencies, including operational research into the utilization of traditional medicine practices and practitioners in health services. A key role for WHO is therefore to disseminate widely
the results of national efforts to incorporate safe and useful tion. ,traditional medicine practices in their respective national Fundamental approach has been to strengthen national P health systems. Specifically, information oti national
efforts for traditional medicine research within an overall policies, legislation, traditional medicine practices, research national research strategy. Through the study and research experiences and training programmes continueto be shared of traditional medicine, a more accurate and complete through various avenues including an International Tradi- knowledge of useful and effective traditional practices, as tional Medicine Newsletter published by the Collaborating welt as potentially harmful ones, is being developed. Centre in Chicago, three times a year, and distributed free of
Nátiónal research capacities are strengthened through charge to researchers from developing countries. research manpower development and institutional Technical cooperation among countries sharing com- strengthening. In those countries where little has been done, mon interests is being promoted to encourage a more rapid intial efforts are being concentrated on making an inventory and effective development of the programme within coiin4 of traditiaonal practices. tries, in areas such as provision of information on assess-
ment of standards, toxicity/safety, stability, pharmacology, and other aspects of traditional medicine remedies. An example is the Inter-Regional Seminar in China6 that gave those responsible for health policy at the national level an opportunity of studying the utilization of traditional Chinese
(1) Critical examination of traditional Materia Medica and
(2)
(3)
practices; Accurate identification of the plants and other natural products used; Identification of useful remedies and practices an'd sup- pression of those that are patently ineffective or unsafe; and Promotion of further research and exchange of informa- (4)
Encouragement and suport are being given to localS) studies on traditional medicinal plants as means of reducing drug budgets and promoting self-reliance. Countries will continue to be supported in their efforts to prepare an inven- tory of effective traditional practices and techniques that
5
medicine in primary health care and of discussing and exa- mining the possibilities of adopting comparable approaches in the provision of health services in their own countries.
Training
The promotion of suitable policies is thus an essential 4ftrst step. Once policy is established, the next step is to 'develop knowledge and skills and to favourably influence the attitude of both traditional practitioners and scientific health wokers.
On the one hand, specific training programmes need to be elaborated for traditional medicine practitioners. On the other hand, elements of traditional mediáine need to be introduced into the already established curricula of training programmes for other health workers.
These actions should promote greater acceptance of the unsefulness of traditional medicine and lead to a wider adop- tion of local practices. They should als6 facilitate the transfer of inforMation on foreign traditional medicine practices from other part of the world.
All health staff, but particularly medical and nursing stu- dents, need to be made aware of the place of traditional medicine in their culture, its strengths apd its weaknesses, and of the use that may be made of it.
As an example of a training activity, an Inter-Regional Workshop on the Selection and Use of Traditional Remedies in National Primary Health Care Programme was organized by DANIDA and WHO and was held in Thailand in 1 985. The
Workshop was the first of a series intended to address some of-the problems of safety and efficacy of traditional remedies used in primary health care, including related issues of stan- dards, stability and dosage formulation. The .participants comprised three from Indonesia, three from Malaysia, three from Nepal, two from the Philippines, six participants and
twenty observers from Thailand. All participants are directly involved in the planning and conducting of clinical and labo-
ratory studies of traditional remedies. In addition, there were
lecturers and resource persons from the Department of Med- ical Sciences of the Thai Ministry of Public Health, and the collaboration of faculty members from the University of Illinois at Chicago, USA, Chulkalongkorn and Mahidol Uni- versities, Bangkok, and the World Health Organization. Similarly, traditional practitioners need to be approached with understanding and recognition of their skills so as to encourage them to share their knowledge and to play a part in the national health service, usually after a short period of special training.
The programme is collaborating with countries hi iden-
tifying ways in which tradtional practitioners can be trained in order to ensure safety of their practices and, where possi- ble, to mobilized them to play an effective role in the general health system without destroying their individuality. WHO
- will continue to collaborate with countries in upgrading the skills and knowledge of traditional practitioners.
Studies are being undertaken in a number of countries to identify those elements of traditional medicine practices that could be utilized by other health workers as well as the type of training that traditionalpractitioners should receive in cer- tain aspects of modern medicine.
WHO Collaborating Centres
In getting this important programme started, WHO has
felt that the first essential step was to secure the interest and
6
involvement of those alreadyworking in traditional medicine around the world and to build up a network of specialized institutions and individuals possessing the required exper- tise, motivation and enthusiasm to contribute to programme development.
This has been done by establishing a number of Col-
laborating Centres in the different disciplines that constitite traditional medicine. At present, 21 such Centres have been
designated. There are five in Africa, three in the Americas, two in Europe, one in the Eastern Mediterranean, eight in the Western Pacific and two in the South-East Asia.
This type of association between WHO and the scientific community is mutually beneficial, serving to give interna- tional recognition to the individual institutions designated and to make available to WHO their expertise, on which the
organization can call on behalf of Member States. Such
assistance covers a whole range of activities, for example: (1) Situation analysis of the potential role of traditional •
practices and practitioners in national primary health care programmes;
(2) Development.of policies and legislation for the incorpo- ration of traditional medicine into health system;
(3) Support to multi-disciplinary investigations and sur- veys of local traditional medicine practices, and the use of plants of medicinal value;
(4) Collection, analysis and dissemination of information from countries and regions on successful activities, pro- jects and programmes on traditional medicine. The network of Collaborating Centres forms the back-
bone of the Organazation's programme in traditional medicine.
Guiding Pinciples
In developing the programme certain guiding principles have emerged which may be of help not only for WHO and its Member States but also to international and donor agencies working in this area. These principles are as follows:- (1) There is no single or simple approach to the problem of
how to involve traditional practitioners in national health systems, especially at the primary health care level. Dedicated and sincere action onthepartof all con- cerned will be required to foster a collective effort to generate and implement policies best suited to any given country.
(2) The first step could be the establishment of a national council for traditional medicine, that could be charged with responsibility for preparing a national strategy and laying down a broad plan of action to be followed by government. The council should be multi-disciphnry and multi-sectoral in nature, with appropriate represen- tation of the different types of traditional practitioner involved.
(3) Major policy issues, including asa minimum all those described in the preceding section, need to be identified, priorities determined and mechanisms established to propose the various options and courses of action open to government, with ad-hoc groups being formed to tackle specific issues.
(4) Adequate finance should be assured under the govern- ment's regular budget for the support and promotion of traditional medicine activities. External finance should be considered as only supplementary to the govern- ment's main effort.

(5) In parallel, it will be necessary to undertake a survey of the national situation of the practitioner, the popula- tion's preferences and needs, resources, special prob- lems, etc.. Based on this sound national health plan reflectingthe thleoftrditional medicin may b'formu- lated. Practitioners of traditional medicine should be engaged
in these activities and the results should be made widely known to general publit as well as to the health professions.
Concusion
There is no longer any doubt about the value of incor- porating traditional medicine into modern health care. It is happening — it is part of today's reality. It is happening for manydifferent reasons but, fundamentally, because people believe that traditional practices have values that they are Willing to subscribe to.
Wht is'stitl un clear is how the articulation of the two systems will be brought about in different settings. Will it happen man atmosphere of goodwill or of hostility? Will it be pursued purposefully orwill ft be acknowledged reluctantly? Will government and medical practitioners play a leading role or will they be mere spectators?
WHO's primary concern is to encourage countries to utilize those elements of traditional medicine which are of value in their national health services. In this modern age, the rich heritage of traditional medicine should not remain the exclusive or esoteric interest of only a few. Let me end by quoting the Dirctor-General of WHO.
"For too long, traditional and "modern" medicine have followed their own separate paths in mutual antipathy. But their aims are surely identical: the improvement of human health and, hence, improvemnt of the quality of life."
Halfdan Mahler, M.D.
References
1. World Health Organization, Basic Documents. 34th Edi- tion, Geneva, 1984.
2. World Health Organization, Primary Health Care, Alma- Ata,USSR, 6-12 September 1978. Health for all Series No.1,1978, Geneva.
3. Akerele 0. WHO's Traditional Medicine Programme: progress and perspective. WHO Chron. 1984; 38: 78-81.
4. Farsworth NR, Akerele, 0., Bingel AS, et al, Medicinal Plants in Therapy. Bull. WHO 1985; 63: 965-81.
5. Malone MH. The Pharmacological Evaluation of Natural Products — General and Specific Approaches to Screen- ing Ethnopharmaceuticals. Journal of Ethnopharmacol- ogy. 1983; 8: 127-47.
6. Report of the Inter-Regional Seminar on the Role of Trad- itional Medicine in Primary Health Care in Chine, 9-12 October, 1985. WHO Geneva (In Press).
7. The Selection and Use of Traditional Medicine in Primary Health Care, Report of an Inter-Regional Workshop Bangkok, Thailand, 25 November-4 December, 1985 WHO Document TRMI86. 1.
TRADITIONAL MEDICINE PRACTICE IN TANZANIA HISTORY AND
DEVELOPMENTS
Dr. J. Z. J. Kilewo 1
I.A.J. Semalj2., R. Msuya, E. N. Mshiu,2 D. M. Do Amsi C. K. Makwaya,E.p.y. Muhondwa
HISTORICAL BACKGROUND
The history of traditional medicine in Tanzania goes, back far beyond the establishment of Western cortacts. In Northern Eastern Tanzania; the boa! religions and healing traditions of the well watetd1nterioz highlands were already interacting with the Afro-lslathic Coast in the period of intense slave and ivory tradä which preceded theColonial intrusion of the 1890s'.
Before the Colonial conguest, healers and political lead- ers with whom they were allied had a muith wide range of control over the social conditions of healtfr than they have had ever since. In a study carried out by Fierman2 on a Sham- baa Kingdom found in the 18th Century in Tanga Region, and which survived until the German conquest of the 1890s, the Kingdom healers in cooperation with the Chiefs and local elders controlled a wide range of basic health conditions, such as, cleaning and irrigation of ditches and distribution of water. Diviners advised local people to choose villge sites in high location in order to keep them free of insect pest and dis- eases. Healers together with local elders and minor Chiefs insisted on isolating individuals born under an ill omen, lep- ers and those infected with contagious diseases, such as small pox. Some specialists such as those who could treat wide spread epidemics and those who could make war charms were required to work only at the Chief's court.
The German conquest in 1980s eliminated all forms Of collective control by healers over the conditions of health except for those few weak elements of collective control which could be hidden. Healers in the country were perse- cuted because an African authority over collective action was taken as a threat to German sovereignity. This was partly prompted by the role of cult leadership in the Great Maji Maji rebelion of 1905, the action of Missionaries and because of cultural emperialism. After the intial period of persecution
Traditional Medicine Research Unit Muhimbili Medical Centre P.O. Box 65001 DAR ES SALAAM.
3Department ci Epidemiology 2Department of Epidemiology Muhimbili Medical Centre
ESSALA.AM 1Department o Biostattstics
3Department of Biostatistics Muhimbili Medical Centre P.O. Box 65001 OAR ES SALAAM.
4Department of Behavioural Sciences Muhimbili Medical Centre P.O. Box 65001 OAR ES SALA.AM.
the Germans closely regulated medical treatment so as to exclude any practice capable of mobilizing people ata collec- tive level In 1909 the traditional healers were issued with cer- tificates specifying illness they could treat, prices they could charge and the localities in which they could practice Even though healers were under severe attack and although they lost rruch of their authority over communal affairs, the local healing traditions survived through the entire German colo- nial rule, for most people, local practitioners were the only healers to whom they had access. A staff surgeon in the Ger- man Protective force, Weck revealed his respect for African traditional medicine when he wrote on the Wahehe tradi- tional doctors and their science, at a time heaters were hardly taken seriously. He stated that the doctors were not practic- ing magic but they were concerned with healing of the sick He cited about 50 diseases and their pathological symptoms which he found correct in the majority of cases It is worth noting that by 1910 there were only 43 German medical offic ers mostly army doctors, who were stationed at various administrative centres throughout the country, and 6 prIvate doctors During the entire German colonial period only 12 general hospitals and 3 special hospitals were built These had a total number of 1200 beds.
Diiring the British Colonial rule (1919 — 1961) the authority of the pre colonial healers was never restored, inspite of the fact that minimum funds were available for rural health service development and most of the health ser- vices were concentrated in towns and at a few mission centres Therapeutic practice was divided between low cost treatment provided by healers for relatives and neighbours as opposed to high cost specialized practice for strangers and very distant relations.
In 1920,8 series of complaints about witch doctors were noted by the British colonial government and led to the introduction of the witchcraft ordinance in 1929 In the same year the medical practitioners and dentist ordinance was passed which carried a provision for the practice of tradi- tional medicine by traditional healers.
Between 1929 and 1937, one of the British Colonial Pro- vincial Commissioner stated that only black art (Uchawi) was criminal and it must be distinguished from 'uganga , the diagnosis and treatment of diseases. He was convinced that "black art" had evil intentions while "Uganga" could be described as a Science" practice by many charlatans and not always with benign intentions.
It is to be noted that during the first to third health development plans of the Ministry of Health (1945—1961), there was no mention, of the role of traditional healers in health services, like wise, in the first pot independence 5 year's development plan (1964—1969), the question of trad- itional medical practice was left untouched. Even after the 1967 Arusha Declaration when a lot of emphasis was put on the development of appropriate rural health facilities and rural health personnel the contributions of traditional heal- ers and traditional birth attendants were not considered.
Although the role of healers and traditional birth atten- dants was not tal'en into account in the Ministry of Health development plans, individual researchers such as Imperato (1961/62) made observations among the Luos of North Mara on witchcraft and traditional medicine, noting that even edu- cated persons could not disregard traditional medicine. Other investigators such as Bura4 wrote a paper on the Wairaq concepts of causation diagnosis and treatment of disease. Similarly Hautvast-Marters5 while working in a
8
Nyakyusa community identified diseases which the Nyakyusa called natural in origin, and listed diseases caused
by spirits and those of magico-religious in origin and solved only by a traditional healer.
Although the practice of traditional medicine in Tanzania is legalized, the collaboration of traditional healers and mod- ern medical practitioners has not been legalised. The relationship between the medical institutions including medicine is very different on the central and at the local level6. The government is well aware of the problems and benefits of traditional medicine. The policy all along has been one of encouraging concilliation and understanding between traditional doctors and modern medical practition- ers, not relations between them, particularly in the rural areas are either none-existant or tense. The reason for the conflict could be that:-
(a) Medical practice introduced by the colonists in the late 19th and 20th century was the only legitimate therapeu- tic course in Tanzania. The European Missionary doc- tors in particular were not used to competing with tradi- tional healers for clients they were treating. This attitude has not changed to date.
(b) Doctors regard the healers and their practice as unac- ceptable, because they have not had any formal training in the medical field and therefore, any Association with healers would a undermining their medical ethics.
(c) Tanzania doe not have a separate law govening the practice of tra itional medicine There is also no Party or Government Policy on the collaboration issue. As a result there is fear among allopathic doctors of being prosecuted should a patient whose medical care was undetaken in collaboration with traditional healers die lnspite of the above reasons, studies carried out by Sem-
ali7 on the opinion of allopathic health workers on traditional medicine and traditional healers on the degree of contact between the two, some of the modern health workers indi- cated their acceptance of traditional healers' involvement in delivery of primary health care. In another study which he carried out in 1983 involving interviews with 320 traditional healers in Kinondoni district, in Dares Salaam Region to find out whether traditional healers would accept collaboration with modern health workers and what should be the nature of such collaboration 28% said modern medicine was more advanced and therefore traditional healers would benefit and 29% saidthey were treating the same people and there- fore they would be willing to join forces 25% said that some of the diseases had no cure in modern medicine and there- fore they could be cured by traditional meldicine The rest of those interviewed, had their own reservations on the issue of collaboration. The healers felf thatthey could collaborate on the exchange of patients and have common clinics where both practitioners could practice.
Tanzania has an estimated number of between 3,000 - 60,000 traItional heaters.
DEVELOPMENTS AND ACHIEVEMENTS (1969-1985)
Although traditional healers in Tanzania continued to exist on their own outside government control since inde- pendence, their secrecy made the medical profession feel uneasy. In 1969 the government took new initiativs towards traditional medicine practice aimed at its planned intergra- tion. This was largely due to the following factors:- (a) There was an awareness of the value of traditiopal
medicine as noted in various regional meetings throughout African countries assisted by WHO.
(b) There was a realisation of the shortage of resources and manpower essential for the continued expansion of all types of curative and preventive services in all African states.
(c) The practice of traditional medicine was flourishing even in urban centres despite their otherwise rapid changes towards modernization. The Chief Medical Officer in the Ministry of Health in
1969 directed the Regional Medical Officers in Tanzania mainland to collect information from healers on traditional medicine practices including drugs which were being used. These would be subjected to clinical trials and chemical analysis. The directive was however, not implemented for various reasons.
The University of Dar es Salaam was subsequently asked to carry out research into traditional medicine The task was given to the Faculty 'of Medicine In July 1974 the Traditional Medicine Research Unit was established with the following objectives (a) To carry out collection of comprehensive information
about traditional medical practicies including methods of treatment and drugs employed.
(b) To identify the sources of drugs and subject them to chemical analysis or other tests for the purpose of sing- ling out the active ingredients and the analysis of which later might suggest ways in which the isolated materials could be used for the preparation of clinically useful drugs.
(c) To study the traditional practitioners practices and cus toms and the role they play in the Tanzania Society and work out ways of integrating the useful practices and customs with modern medicine.
(d) Finally to carry ou experimented cultivation of medici- nal plants which were proved to be effective and safe. Since the Unit's establishment in 1974 the following
work has been done in the implementation of the objectives, namely:- (a) Ethnobotanical Studies:
The Unit has carried out a comprehensive collection of information from over 1,000 traditional healers in 5 reg- ions of Tanzania mainland and on plants and diseases treated by the healers. 2,720 plants specimens have been collected and about 2,000 of those have been iden- tified botanically. Ethnobotanical literature survey has' been carried out on 110 popular medicinal plants of Tan- zania. A book will be published on this. Another pre-occupation of the Unit has been expemen- tal cultivation of exotic medicinal and aromatic plants under a Joint Project financed by the Tanzania Govern ment and UNIDO/UNDP. This aims at producing plant based drugs which could be used instead of drugs which are imported into the country. Trial production of such drugs will be carried out before the end of this year, 1986 Some of the medicinal and aromatic plants under experimental cultivation are:- Calendula officinaflis, Cynara scolymus, Tagetes fatula, Dracocerphalum mol- darica, Thymus vulgaris, Glacium flavum, Saponaria officianalis, and Digitals lanata.
(b) Phytochemical & Pharmacological Screening: Although theUrut was established in 1974 phytochemi cal screerting did not take place until 1979. The section has carried outiytochemicaI studies on a number of
traditionally used plants including some exotic plants which have been under experimental cultivation. The results of the phytochemical screening have been pub- lished in some international journals. In addition, the section has carried out determination of total alkaloids in Cinchona barks using kerosine, and alkaloids in Dat- ura strammonium. Analysis of oil content in essential oil bearing plants such as, Eucalyptus globulus, Cm-' namomum camphora and Elletaria cardamomum has been undertaken. Five hundred traditionally used plant samples have been
extracted and prepared for different bioassays. 240 plants have been screened for antimicrobial activity and results have been published in international journals. Further screening has been carried out on plants claimed by healers to have antifungal and anti-gonococcal activity, and the results are promising. Other investigations have been car- ried out on plants claimed by healers to be useful in the treat- ment of malaria, sickle cell anaemia, bilharzia and trypanosomiasis. This work is still in progress.
Pharmacological studies which started in 1982, were concentrated on isolated tissues and toxicity studies. Two. plants namely:- Harrisonia abyssinica and Zahna africana were studied in detail. Harrisonal abyssinica used tradition- ally for abdominal problems, skin conditions and asthma has. been established to possess spasmolytic and antifungal activity. The plant is non-toxic. The plant extracts have been recommended for clinical trials in cases of various spas- mogenic conditions, such as, abdominal colics and bronchial asth ma.
Zahna africana (Mdaula) used traditionally as an antifun- gal has' been found to be toxic due to the presence of sapo- nins or tannins. Indeed the plant extracts are unsafe for use externally or internally unless detoxicated before use.
Twenty five plants traditionally claimed to be useful for the treatment of mental illness have been screened phar- macologically for anticonvulsant activity against metrazo!
induced convulsion. All of them were found to have no sig- nificant activity. However, Hyptis sauvelonsis, a herb used traditionally for the control of convulsions was phar- macologically screened and found to have a significant pro- longation of barbiturate sleeping time in mice and further studies on isolated tissues have indicated the presenceof cholinergic principles. The plant has stimulant effects aè well as effects against oxytocin induced contractions on the uterine muscle. The plant has been found to be non toxic on experimental animals.
CONCLUSION:
Traditional medicine is indeed an invaluable resource that can be meaningfully and profitably harnessed in practi- cally all African countries. In Tanzania, we require a well defined policy and appropriate legislation on traditional medicine. Although the significance of traditional medicine is acknowledged there is need for continued systematic research into various aspects of the field, such as, sociologi- cal, anthropological, historical, ethnobotanical, phar- macological, toxicological, phytochemical and clinical research.
The Traditional Medicine Research Unit is already carry ing out some of this research particularly in the ethnobotan- ical, phytochemical and pharmacological fields. The Unit hopes to undertake anthropological and clinical research in the near future.
REFERENCES
1. Fejerman K. Alternantive medical services inrural Tan- zania: A physician's view Soc. Sc. Med. 1981: 15b; 399 - 404.
2. Feierman S. The Shambaa Kingdom: A History. Univer- sity of Wisconsin Press Medison, Wisconsin 1984.
3. Weck. Hehe Medicine. Tanzania Notes and Records No. 70, 1969.
4. Bura MWT. The Wairaq concepts of causation, diagnosis and treatment of disease. Dares Salaam Medical Journal 1974;6:55-61. -
5. Hautvart-Martens Analysis, of Bantu Medicinal System a - Nyakyusa Case Study (Tanzania). Tropical and Geog- raphical Medicine 1972; 24: 406- 14.
6. Felerman S. Therapy as a system in Action in Northern Eastern Tanzania. Soc. Sc. & Med. 1981; 1 5b: 353 - 60.
7. Semali IAJ. The opinion of Allopathic health workers on Traditional Medicine Healers and Degree of contact between the two. Thesis submitted to the University of Dar es Salaam for the partial fulfilment of the award of DPH 1982.
TRADITIONAL MEDICINE
INTRODUCTION
TO-MORRQW By Murray Last
While much debate has taken place on the role of tradi- tional medicine (indeed it represents a remarkable shift even to think of incorporating healers into a nation's health ser- vices), most of the discussion, however, has been about the. short-term-treating to-day's policies as a series of stop-gap mesures. I want instead to raise here such longer-term issues as:
What sort of future (if any) is envisaged for traditional medicine — beyoridthe year 2000? What effect, for example, are to-day's policies intended to have on the next generation of traditional healers?
Or is it seriously being assumed that, once the present generation dies dut and the entire population have passed' through modern schools, the demand for 'traditional - medicine' will have disappeared? Will there be nothing in its' place but 'scientific medicine' and if so, what is the evidence for such a prediction? What developments, for example, in psychiatric provision are foreseen?
It needs to be recognised that many sectors of society do wish to see traditional medicine disapper, and have their own logics to back their argument. Opposition to traditional, medicine is not confined to the hospital or any other elite.
Murray Last University College London
problematic. -
But, by way of introduction, a number of points need be nade. 1. That "traditional" does not mean "unchanging".
Although the history of traditional medical thought in any one community is extremely hard to re-construct (certain' institutions or practices are of course better documented e.g. the Lemba 'drum of affliction' chronicled by Janzen, the mere fact that traditional medicine changes is more easily demonstrated. For example, in the colonial period, the years 1918 - 1925, after the first world war, appear to have been a major watershed: the older generation of healers were dis- credited as they proved ineffective against the new epidemics, and a new generation experimented with and elaborated new therapeutic rituals and recipes. Another per- sistent theme in oral traditional is how, compared with their predecesso;s, "to-day's healers are charlatans; they know none of the old secrets". But each generation has to find new ways to cure new complaints, since it is not just treatment that changes, but ideas about the ecology of illness too. "Traditional", then, can be as 'modern' as so-called "modern medicine". In recognition of this, "alternative medicine" would be a more accurate (if sometimes less persuasive) label, were it not that such "alternative" imports as chirop- ractice, ostecspathy are already well established in parts of the continent alongside Christian faith healing. In short, one must be wary of taking the label "traditional" too literally, or of assuming that all cultures (or all people) revere "tradition" as the stereotype suggests!
2. Equally obvious is the point that in continent the size of Africa "traditional" includes a wide range of therapeutic practices, some of which conflict sharply in their logic with others. More important, however, is the fact that within any one society's medical culture there is diversity too. One 'school' may be dominant at a particular time, but the rationale for diversity is the same as in agriculture: mixed cropping gives better results than monoculture in the long run, as crises come and go; and even in monoculture, a range of seed types is a necessary reserve against new con- ditions in the future. In short, the diversity within traditional medicine is as crucial to traditional medicine as its ability to change.2
3. As part of the ability to change and diversify, many medical cultures are not highly systematised. Researchers may record a society's "common sense" and analyse it as a model. But such models are like "first aid"; they bear little relation to the complexity of a difficult case as it develops, or how it is treated over time. Far too many variables are deemed relevant for practice to be boiled down to a formula. Nor do individual healers necessarily know their medicine systematically; apparent inconsistencies of thought are problemaltic more for the academic analyst than for the suc- cessfull practitioner!3 -
Traditional medicine; then, is a living style of treatment, and caplable of development. Given this record of change, diversity and relative freedom from systematisation, it is very probable that traditional medicine will survive in som&
- In Tanzania,traditjonl medicine is part and parcel of our There are things wrong with traditional medicine (as there culture which should be preserved and developed for the are with any system), and its future lies in part in putting good of our people. ,some of them right. My purpose here is not to propose solu-,
I am grateful to all the national and international Organi- tions but to draw attention, for purposes àf starting the dis- zations, such as, World Health Organization for assisting in cussionoff,towhatisbeingdoneelsewhereinAfrjca,fjrston 'the development of traditional medicine in this country. two aspects of policy, and then on two areas that seem to be.
10
form. And I would suggest that it needs to survive, if only as
part of people's broader resources with which to face crises. The obvious question then is, what is the best form of tradi- tional medicine for patients? The more problematic ques- tion, however, is what is the best form, too, for the develop- ment of an effective range of alternative therapies for use in a specific community? Using the word "best" raises the problems of medical audits and tests for efficacy — all of which are hard to devise without excluding the very cultural context that helps to make any medical culture successful. Academically, proof may be impossible— in which case how shouldnon-academics decide? But there remains the ques-. tion of how to encourage (and finance?) the development of local alternative or traditional therapies; mere survival in some form or other may prove inadequate to prevent the improverishment of a traditional and its expertise. Without experiments, experience shrivels.
.1. Issues of policy
A. NATIONAL OR LOCAL?
The essential fluidity of traditional medicine makes its organisation by government particularly difficult even more difficult than, say, local administration in areas where cul- tural differences demand recognition Given the diversity of healing traditions within any particular state a national traditional medicine necessarily is a coalition of different and possibly conflicting traditions No state has yet attempted to homogenize those traditions into a single system (it would be very disruptive and probably counter-productive to do so) not leeast because the efficacy of a given treatment lies
partly in its specific cultural context So long as communities have their distinctive cultures, it is possible to use that con- text to enhance the placebo effect.
Two very different models of organising traditional medicine are being tried, one in Ghana, the other in Zim babwe. The Zimbabwean model is to emphasise intra-pro- fessional co-operation and local autonomy. Thus the Zim- babwe National Healers Association (ZINATHA), under its President Professor Chavunduka and with the backing of the Ministry of Health, has taken over the examining and certifi- cation of eventually all recognised healers. It is however still a voluotary body, financially supported only by its member-
ship dues and not an arm of government. The idea is to ena- ble healers develop their own systems of training and research and thus put them on a par with the hospital-based medical profession—undertheir own equivalent of the Gen- eral Medical Council.4 At present, however, ZINATHA is necessarily decentralised, with a small headquarters staff and much of its local control over healers execised by its branches at the local level. Given the importance of healers both historically and more recently during the war of inde- pendence, there was good reason politically to try and bring, for national unity's sake, all such locally influential leaders under a single umbrella. Not all the important spirit mediums have yet joined, apparently; the majority of the membership are primarily herbalists, as they had been in earlier healer's associations.
The Ghanaian alternative is new. A fortnight ago in Ghana, the Secretary for Health announced that a lw was shortly to be promulgated decentralising the Ministry of. Health. "District Health Committes would be expected to for-
mulate and implement health policies within their areas, with Accra only giving general guidelines."5 Furthermore, "under decentralisation, certain categories of staff could be recruited locally." This is, it seems, the culmination of a number of pilot schemes.6 Areas elected their own district health committees on which sit a wide range of people involved in health care, including healers. Decentralisation is seen not merely as an exercise in local democracry but also as one way of overcoming the problem of formulating a nation-wide policy on how healers might be incorporated. By leaving the selection and validation of local competent heal- ers to the various districts, the Ministry is relieved of examin- ing and certifying an enormous range of practitioners in some standardised way. It also means that healers may find it harder to get reegistered to practise in another district or at the capital. Clearly much will depend on personalities of the committee members, in particular whether the officials and doctors posted by the Ministry will try and dominate policy; but at least they, like other members, will be accountable to the community. Co-operation from local healers has not been a problem, apparently; pilot schemes, however, with all the extra inputs they attract, may not proveso easily generalisable across the country. Another problem may be overpoliticisation if health issues becomes just another weapon in a local struggle for power.
Whereas the Zimbabwean model seeks to unite the pro- fession across the urban-rural, herbalist-spirit medium divide, the new Ghanaian system will make the greatest use of local diversity, and of both communities' and individuals'
willingness to experiment. In consequence, in some areas healers are likely to be central to the health services, in other
areasmarginal. It is not clear whatthe government proposes for Accra itself: the policy was designed overtly to meet criti- cisms from the countryside, and demands for more local autonomy generally. If the Accra conurbation is to be treated differently, there is a danger that traditional medicine will be
ghetto-ized, equated simply with rural cultures.
B URBAN OR RURAL?
What is to be the role of traditional medicine in the cities is government for example to build traditional clinics and hospitals (e g for bone settlers as in northern Nigeria) are premises to be shared by healer and doctor side by side (as in a Bulawayo experiment) or hospital beds allocated to healers? Or are the towns adequately served with hospitals dispensaries — healers being only relevant where medical martpower is short, as in the rural areas? But first, which "traditional medicine" does the government have in mind?
Given the importance of context to successful traditional therapy, it ought not to be surprising that there has been, in recent years, two distinct "traditional medicines" one based in rural areas, the other found in the large cities. The existing literature on traditional medicine does not always make the distinction. But very crudely speaking, rural th'erapy calls upon rural religious beliefs and •as a conse quence has often been analysed not as medicine but as part of religion. 'Traditional medicine', then, in such analyses, is associated with herbalist traditions (and sometimes, rather quaintly, called 'leechcraft'); historically, however, the. her- balist tradition was an integral part of rural religion and therapy. In towns, this herb-oriented 'traditional medicine' is usually the dominant stand — its dominance much assisted by colonial legislation, which tended to legalise herbahists
11
while making diviners liable to prosecution whenever a diag- nosis of witchcraft was to be made.
Under colonial rule, herbalists (many of them immig- rants from other countries flourished in the towns, trading in market place and forming associations, whereas spirit mediums and cults, though to be found in towns, were consi- dered more efficacious if they were located in the coun- tryside. Many of the cults' healing functions in the towns have been taken over by independent Zionist churches spec- ialising in healing and prophecy; theirs, they say, is Christ- ian, not traditional medicine. It is in the towns, too, that a
range of "alternative" therapies have become available. Urban medicine, whether traditional or alternative, lacks
the legitimacy that rural healers acquirethrough long, visible service in a small community. Urban healers, if newcomers, rely on certificates, on claims to foreign origin and various forms of self-advertising unnecessary in the countryside. The result is not only extravagant claims but marketing through an appeal to the unconventional and exotic. "Char- latanry" is a problem, and helps to call into disrepute tradi- tional medicine as a whole. Thus the urban press, city gossip and the revelations of the law counts tend to focus on the bizarre goings-on of some practitioners, encouraging a popular stereotype not very different from that of the col- onialist 'witchdoctor'. By contrast, established urban heal- ers, well known in their own quarters, function more like their rural counterparts, with the minimum of publicity.
A long established, urban tradition of medicine is prac- tised by Muslims. The identity of Islam with traditional, pre- colonial values has meant that Muslim healers, unlike their Christian counterparts, come under the rubric of traditional medicine, at least in a country like Nigeria. But the attitude of Muslim institutions towa rds medicine has always been more secular than has traditional Christianity's (since according to tradition the Prophet Muhammad was less engaged in per- forming medical mirables than was Jesus Christ), and as a consequence the rural religious elements in traditional medicine were traditionalism's "unacceptable face". In
towns, such rural beliefs and practices were deemed inap- propriate, improper; they were associated more with harm- ing than with healing, with providing power and protection for the arnbitioiis.or vengeful. The new influx of migrants into the towns and the competition of contemporary urban life may have mide such practices (if not beliefs) more com- monplace, but for many urban-dwellers such therapies are not the respectable form of traditional medicine. Fears of. such practices are further accentuated by the very invisibility of life in towns, in contrast to the social transprency of the country life.
Urban traditional medicine, then, has two major prob- lems: 1. "charlatanry", and a lack of 'qualifications'; 2. misuse in the form of sorcery. Rural medicine's problems are different: the rejection, for example, of its religious premis- ses outside the immediate local context with people gradu- ally losing faith (or fear) in its sanctions; the acceptance, instead; of zionist churches or of reformist interpretations of Islam; finally, the relegation of rural medicine as the pre- serve of a few speqjalists to whom the urban healers can refer only the hardest of their cases — in short, the town- smen's notion of the deep countryside, thj "bush", as a kind of natural asylum. In this process, urban traditional medicine eventually replaces rural medicine even in the countryside. In which case, rural medicine's problems become the same as the town's: "charlatanry" and misuse.
12
II. Problematic areas
A. EDUCATION
"Charlatanry" is central to the issue of medical educa- tion. Traditionally in rural areas the would-be healer received
training either by apprenticeships under recognised healers
orthrough the guiding "spirit" who initially called the healer. In the latter case (as Dr Reynolds has shown) the trainee has been taught his (or her) herbal expertise as a child and will have participated (along with many others) at sessions of therapy; what is unique to him (his "gift") is his personal style which potentiates, for him and his patient, an otherwise standard format of medical treatment locally.7 The training and subsequent validation of the healer's skill comes through time, as the healer practises under the scrutiny of the community. For the community contains many who know enough to be healers, should they ever receive the "call". There may even be, as Dr. Ngubane has shown, a net- work of healers meeting regularly to discuss cases and "examine" new healers.7 Under such conditions "char- latanry" cannot last long.
None of this is new, though how long the system will continue may depend on the stability of rural communities. What is new is the attempt formally to teach trainee healers and have the training officially recognised. Again, this seems to be a consequence of the growth of urban traditional medicine, with its need for qualifications and its oppor- tunities for young people to embark on the sale of medicine. Schools have been started in Zimbabwe the one organised by ZINATHA has been temporarily closed — it was perhaps too ambitious intellectually and financially; the other has been founded by the Ford Foundation and is herbalist in orientation. The major obstacle in theory is how to sys- tematise the skills and expertise of traditional medicine to fit a school model. In the Zimbabwe case, where plants pre- scribed for specific ailments may depend not on the plant's pharmacology but on which clan the patient belongs, the
teaching appears to be deliberately "un-traditional" in the local context.
A further development is the exposure of hospital medi- cal students to courses on traditional medicine given by local healers. The results are, not surprisingly, reported as being good. What is not clear, however, is what exactly is taught and, more importantly, how far the teaching has been mod- ified to match medical students'. (and teachers') expecta- tions. A "package" of traditional medicine is being created and "sold" to medical schools, a package that had not existed before the demand created it, and as such, it is an indirect product of the medical school system.
Such foreign influence is not new, of course. There is, for example, inthe curriculum of old-established schools of her- bal medicine such as exist in South Africa considerabfle bor- rowing from traditions of herbalism developed abroad; and these schools have trained many traditional herbalists in southern Africa. Similarly, textbooks of Indian or British pharmacognosy are widely available in the continent, as are Muslim texts (in Arabic). Given that these texts are available, and nothing comparable has so far been produced from with in the African tradition, it is perhaps invevitable that they are in use. Lists of medicinal plants are being published state by state, but their classifications not just of plants but of dis- ease terms (in translation) as well tend to follow international. conventions. The dominance of academic medicine is further evident whenever new schools of traditional
medicine are being planned; offers of help are not easily refused, locally respected healers shy away and in the pro- cess 'traditional medicine' (as taught) is transformed.
The 'colonisation' (or 'modernisation', as some call it) of traditional medicine has its own logic: therapies are linked up to the legitmacy of internationalism herbalism, its funds and its research. The pattern iswidesprad: for years now, for example, the London covens of witches have exported mate- rial to Lagos, just as Rosicrucian and other mystical tradi- tions from Europe have their adherents at all levels of soci- ety. Nor is the trade confined to Europe. Indian and Chinese techniques and material medical find a ready market. The internationalisation of magic (good and bad) is ancient, and two-way: West African scholars were noted pre-colonially for their learning in the occult sciences and settled in Egypt and elsewhere. And it is through this internationalisation that many changes in traditional medicine have apparently come about.
Training, however, is perhaps less problematic than establishing an examination system with uniform standards. Again, the solution adopted has usually been to leave it to a committee Of other loc3l heaters who would be responsive to wider opinion in the community. In rural areas that would not pose problems, but in the towns an equiatent community opinion is more elusive. The churches solve the problem by creating their own community, institutionally within the church hierarchy, and congragationally through its mem- bers. Associations of healers have tried to fill this institu- tional role, as have cults which involve both healers nd healed (like the Lemba 'drum of affliction' described by Jan- zen).
If licensing solves the problem of protecting the con- sumer from "charlatans", it also creates the problem of examinations, and from examinations arise such problems as an agreed syllabus, which in turn requires formalising a particular tradition of medical expertise. No government, as far as I know, has tried to confront these problems; at best, they have been left to the profession itself to resolve.
B LEGAL RESPONSIBIUTY
Licensing requires legal powes to make it effective. An alternantive solution to "charlatanry" and misuse of medicine has been through criminal law. While the various witchcraft ordinances and their successor statutes are well known, much less known (and much more difficult to research) is the attitude of the police and local courts towards healers' malpractice. The most gross cases may go to court as manslaughter, but the majority of instances involving negligence, malpractice or simple errors of judgment (as in paediatric dosage) seldom result in litigation — at least, as yet. Consumers' rights and the responsibility of a healer in his capacity as a trader in particular services are, apparently, rarely tested in traditional medicine — sometimes, presuma- bly, out of fear of retaliation from the healer.
Once again, the use of the law to "clear up" traditional medie is above all an urban problem. In the countryside communities could act against a healer who was thought to have been negligent or had poisoned a patient. This requires a delegation of powers few nation-states easily permit; but few states too can prevent "self-help" by a community intent on ridding itself of a social outcast, whatever the claims of fo-mal justice. In the towns such actions constitute a riot. Yet unless some formal channels, of the kind the legal system
normally provides, are available, riots are simply seen as themselves a necessary kind of judicial process
If the courts are to be the way of obtaining redress against a healer's malpractice, then once again standards of reasonable practice have first to be established. As expert witnesses on matters of health healers evidence would have to be admissible in court, just as healers' signatures might have to be as valid as doctors' certificates, or adequate for medical insurance documents. The legal recognition of heal- ers' expertise would presumably require some form of licensing of healers generally and with it appropriate criteria for assessing that expertise. In the multiplicity of traditional practice, that my not be easy, but it is probably inevitable.
IN CONCLUSION
In this brief essay I have tried to focus attention on more general points of policy, and on problems which will require considerably more research to resolve. I have stressed the im potance of traditional medicine in the major cities of Africa as the arena in which I suspect the greatest difficulties will be encountered. My own experience of traditional medicine has been predominantly rural; this essay is therefore for me exploratory, yet presented to colleagues who have undoub- tedly considered these kinds of issuesbefore.I look forward to their comments!
REFERENCES
1. J. Janzen, Lemba, 1650- 1930, New York, 1982. 2. On local agricultural expertise, see P. Richards, Indigen
ous Agricultural Revolution London 1985 Coping with Hunger London, 1986.
3. M. Last, "The importance of knowing about not know- ing", Social Science & Medicine, 1981
4. G. L. Chavunduka, in M. Last, G. L. Chavunduka, The Pro- féssionalisation of African Medicine, Manchester, 1986, ch. 1.
5 WestAfrica 22 September 1986 p 1999 6. Cf. the work of D.M. Warren and colleagues in P. Yoder
(ed) African Healing Systems Los Angeles 1982 7 P Reynolds in M Last G L Chavunduka op cit ch 8 8. H. Ngubane (Sibisi), "Aspects of clinical practice & tradi-
tional organisation of indigenous healers in South Africa," Social Science & Medicine, 1981.
13

USE OF NON-FACTUAL QUESTIONS IN A SURVEY: RESPONDENT'S OR
INTERVIEWERS' OPINION? C. K. Makwa ye1, J. Z. J. KiIlewo2,l. A. J. Semali3, R. Msuya1,
E. N. Mshiu3, D. M. Do Amsi1, E. P. V. Muhondwa4.
ABSTRACT
It isquite common in survey practice to use non-factual sometimes also called opinion questions in seeking for some useful information. Unlike the case with factual questions, it is somewhat difficult to examine the reliability of responses fron non-factual questions.
Imprecision in question wording may lead the individual respondent or sometimes the interviewer to make personal interpretations. One typical non-factual question expressed in a rather unbalanced form of "do you think traditional medicine practice should be banned?" is being used to assess the interviewer's influence on the respondent's reply. This paper highlights some problems in a form of observer bias, with non-factual questions particularly when different interviewers are used in survey questioning.
INTRODUCTION
The type of questions widely used in survey practice may broadly be classified as being factual or non-factual. An important difference between them is that with factual ques- tions there are individual true values for the information sought which, in principle, can be determined from some external, independent source other than the respondents' report, whereas with non-factual question this does not apply.
Literature survey abounds with examples demonstrat- ing that survey responses apart from being sensitive to the precise wording format and placement of the questions asked may also be biased by the interviewer. While validity studies may be conducted to examine how successful factual questions are in obtaining respondents individual true value, with non-factual questions validation is much more difficult and less certain. One way of examining the reliability of responses from non-factual questions is to determine whether the relationships of the responses with other vari- able conform to those predicted by a tIffiory.
This paper assessesthe contribution of the interviewers' bias in relation to responses from particular non-factual question.
14
1 Department of Biostatistics Muhimbili Medical Centre P.O. Box 65001 DAR ES SALAAM.
2Department of Epidemiology Muhimbili Medical Centre P.O. Box 65001 DAR ES SALAAM.
3Traditional Medicine Research Unit Muhimbili Medical Centre P.O. Box 65001 DAR ES SALAAM.
4Department of Behavioural Sciens Muhim'bili Medical Centre DAR ES SALAAM.
METHODS
In this survey of "The Practice and Use of TraditionI Medicine" upon which this paper is based, three different questionnaires were used: One was directed to the tradi- tional healer the other was specific for the traditional birth attendant and a general questionnaire that was meant for heads of households as representatives of the general com- munity presumably the recipient of the traditional mejdicine practice. Eleven interviewers were trained together to par- ticipate in the survey by making home visits and actually ask-
ing the questions and recording the answers following a structured questionnaire. The study areas selected for the survey were Iringa, and Hanang, both rural districts. Prior to the actual field work a pilot study, clearly meant among other things, to check against any effect of the precise wording of the questions on the responses was conducted.
Responses to an important question seeking for an opin- ion about the future of traditional medicine practice have been used to assess the relibility of responses to a non-fac- tual question with reference to the interviewer. In particular the question was an open ended one reading Do you think the practice of traditional medicine should be banned?" and thereby leaving the interviewer to "judge" whether a given response amounted to saying either "Yes" should be ban- ned" or "no, should not be banned", or "don'tknow". More to the point is that as Kalton and Schuman put it, the question was expressed in an unbalanced form simply as "Do you favour X?", with the contrary opinion left entirely unmen- tioned.
A chi-square test for independence was used to test the null-hypothesis of non-dependence of the respondents' opinion on the interviewer.
RESULTS
There were in total 3988 members of different house- holds interviewed and their responses to the question at hand, recorded. Of these, about 90% expressed some opin- ion, with 81.5% of them saying that traditional medicine practice should not be banned.
We note from the table below that the type of opinion depends o. the interviewer, that is the distribution of the type of response is not stable across the interviewers. At one extreme interviewer 9 for instance, recorded 3.6% of th responses as suggesting banning of the traditional medicine practice while at the other extreme interviewer 1 indicated that as much as 25.0% of the study population would favour banning of the traditional medicine practice. A similar and indeed equivalent argument can be built by looking at the proportions in the other categories of opinion including the "Don't know". . -
A statistical signifance test on the null hypothesis that the proportion observed in the various categories of opinion are indepent of the interviewers give (20) — 240.03, p 0.001. Thus we can't reasonably.estimate the proportion of a kind of 'opinion regarding the banning of traditional medicine ser- vices as this would significantly depend on the interviewer.
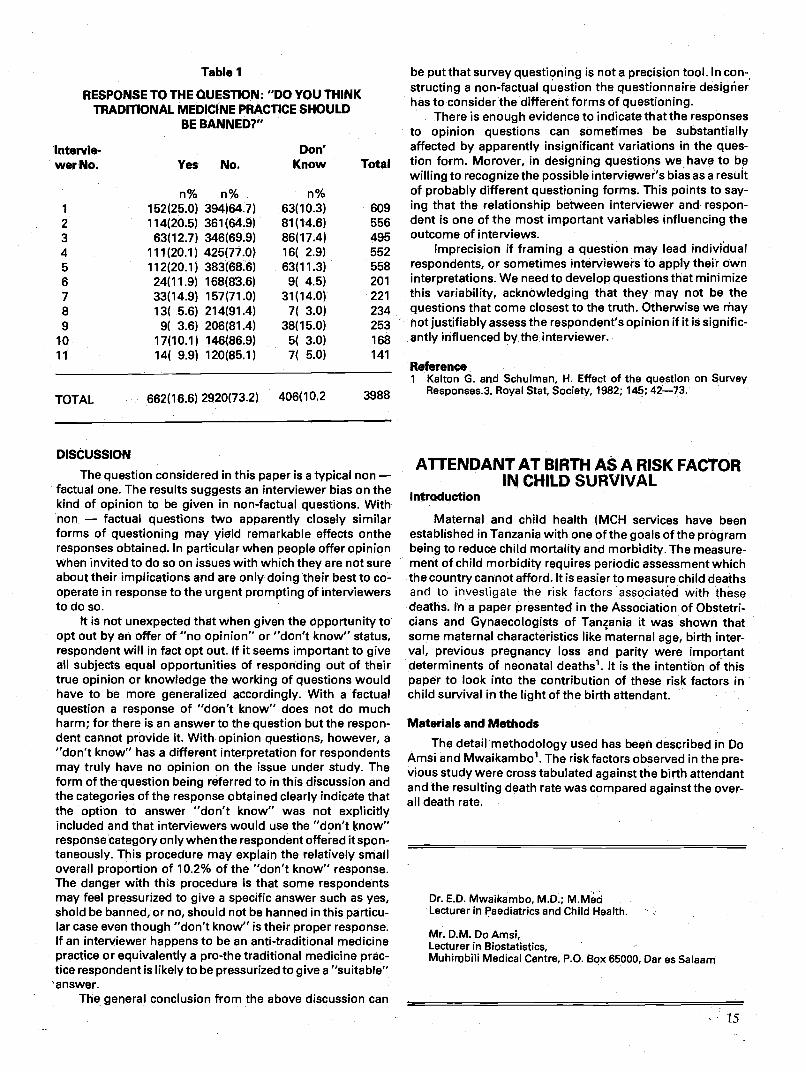
Table 1
RESPONSE TO THE QUESTION; "DO YOU THINK TRADITIONAL MEDICINE PRACTICE SHOULD
BE BANNED?"
intervie- Don' wer No. Yes No. Know
1
n% n% 152(25.0) 394)64.7)
n% 63(10.3)
2 114(20.5) 361(64.9) 81(14.6) 3 63(12.7) 346(69.9) 86(17.4) 4 111(20.1) 425(77.0) 16( 2.9) 5 112(20.1) 383(68.6) 63(11.3) 6 24(11.9) 168(83.6) 9( 4.5) 7 33(14.9) 157(71.0) 31(14.0) 8 13( 5.6) 214(91.4) 7( 3.0) 9 9( 3.6) 206(81.4) 38(15.0)
10 17(10.1) 146(86.9) 5( 3.0) 11 14( 9.9) 120(85.1) 7( 5.0)
TOTAL 662(16.6) 2920(73.2) 406(10.2 3988
DISCUSSION
The question considered in this paper is a typical non — factual one. The results suggests an interviewer bias on the kind of opinion to be given in non-factual questions. With non — factual questions two apparently closely similar forms of questioning may yield remarkable effects onthe responses obtained. In particular when people offer opinion when invited to do so on issues with which they are not sure about their implications and are only doing their best to co- operate in response to the urgent prompting of interviewers to do so.
It is not unexpected that when given the Opportunity to opt out by an offer of "no opinion" or "don't know" status, respondent will in fact opt out. If it seems important to give aB subjects equal opportunities of responding out of their true opinion or knowledge the working of questions would have to be more generalized accordingly. With a factual question a response of "don't know" does not do much harm; for there is an answerto the question but the respon- dent cannot provide it. With opinion questions, however, a "don't know" has a different interpretation for respondents may truly have no opinion on the issue under study. The form of the-question being referred to in this discussion and the categories of the response obtained clearly indicate that the option to answer "don't know" was not explicitly included and that interviewers would use the "don't know" responsecategory only when the respondent offered it spon- taneously. This procedure may explain the relatively small overall proportion of 10.2% of the "don't know" response. The danger with this procedure is that some respondents may feel pressurized to give a specific answer such as yes, shold be banned, or no, should not be hanned in this particu- lar case even though "don't know" is their proper response. If an interviewer happens to be an anti-traditional medicine practice or equivalently a pro-the traditional medicine prac- tice respondent is likely to be pressurized to give a "suitable" answer.
The general conclusion from the above discussion can
be put that survey questioning is not a precision tool. In con- structing a non-factual question the questionnaire designer has to consider the different forms of questioning.
There is enough evidence to indicate that the responses to opinion questions can sometimes be substantially affected by apparently insignificant variations in the ques-
Total tion form. Morover, in designing questions we have to bp willing to recognize the possible interviewer's bias as a result of probably different questioning forms. This points to say- ing that the relationship between interviewer and respon- dent is one of the most important variables influencing the outcome of interviews.
609 556 495 552 Imprecision if framing a question may lead individual 558 respondents, or sometimes interviewers to apply their own 201 interpretations. We need to develop questions that minimize 221 this variability, acknowledging that they may not be the 234 questions that come closest to the truth. Otherwise we may 253 hot justifiably assess the respondent's opinion if it is signific- 168 antly influenced by the interviewer. 141
Reference 1 Kalton G. and Schulman, H. Effect of the question on Survey
Responses.3. Royal Stat, Society, 1982; 145; 42—73.
ATTENDANT AT BIRTH ASA RISK FACTOR IN CHILD SURVIVAL
Introduction
Maternal and child health (MCH services have been established in Tanzania with one of the goals of the program being to reduce child mortality and morbidity. The measure- ment of child morbidity requires periodic assessment which the country cannot afford. It is easier to measure child deaths and to investigate the risk factors associated with these deaths. In a paper presented in the Association of Obstetri- cians and Gynaecologists of Tanania it was shown that some maternal characteristics like maternal age, birth inter- val, previous pregnancy loss and parity were important determinents of neonatal deaths1. It is the intention of this. paper to look into the contribution of these risk factors in child survival in the light of the birth attendant.
Materials and Methods The detail methodology used has been described in Do
Amsi and Mwaikambo'. The riskfactors observed in the pre- vious study were cross tabulated against the birth attendant and the resulting death rate was compared against the over- all death rate.
Dr. E.D. Mwaikambo, M.D.; M.Med Lecturer in Paediatrics and Child Health.
Mr. D.M. Do Amsi, Lecturer in Biostatistics,
*
Muhibili Medical Centre, P.O. Box 65000, Oar es Salaam
15
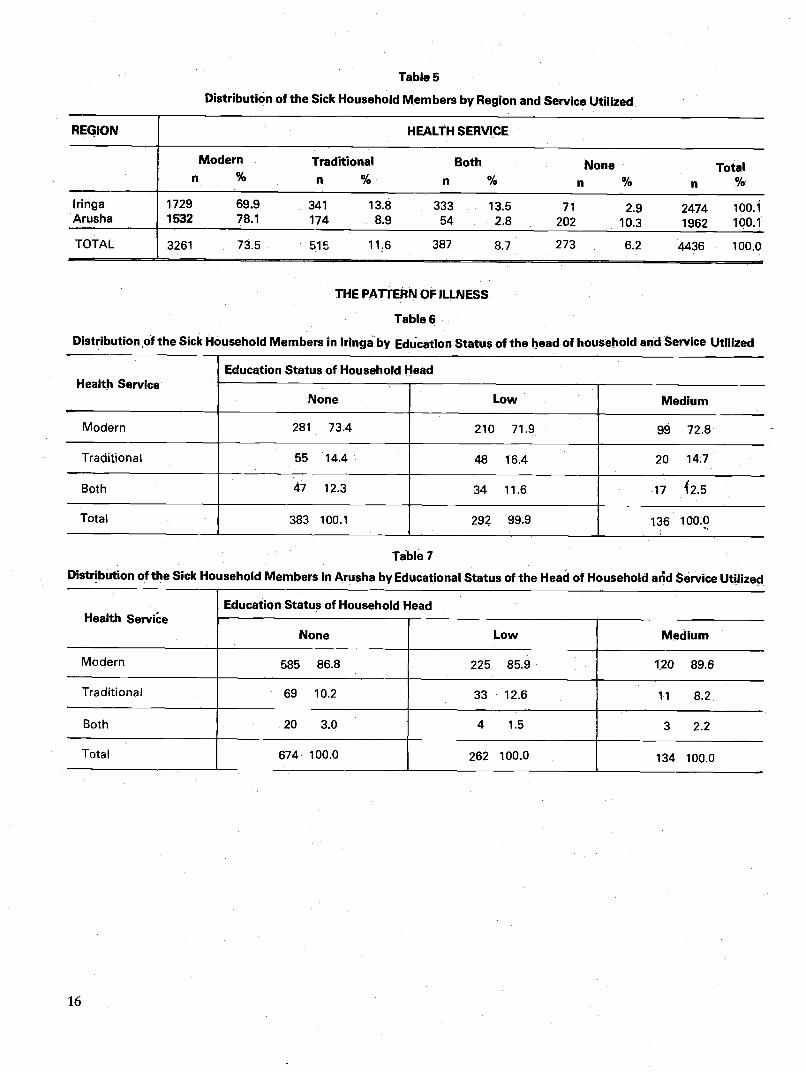
Table 5
Distribution of the Sick Household Members by Region and Service Utilized
REGION HEALTH SERVICE
Modern Traditional Both None Total n % % % % n %
Iringa Arusha
1729 69.9 341 13.8 333 13.5 71 2.9 2474 100.1 1532 78.1 174 8.9 54 2.8 202 10.3 1962 1QO.i
TOTAL 3261 735 515 116 387 87 273 62 4436 1000
THE PATrERN OF ILLNESS
Table6
Distribution of the Sick Household Members in tringaby Education Status of the head of household aOd Service Utilized
Health Service Education Status of Household Head
None Low Medium
Modern 281 73.4 210 71.9 99 72.8
Traditional 55 144 48 164 20 147
Both 47 12.3 34 11.6 17 2.5
Total 383 100.1 29 99.9 136 100.0
Tablèl Distribution of the Sick Household Members in Arusha by Educational Status of the Head of Household atid Service Utilized
Health Servie Education Status of Household Head
None Low Medium
Modern 585 86.8 225 85.9 120 89.6
Traditional 69 10.2 33 12.6 11 8.2
Both 20 3.0 4 1.5 3 2.2
Total 674 100.0 262 100.0 134 100.0
16
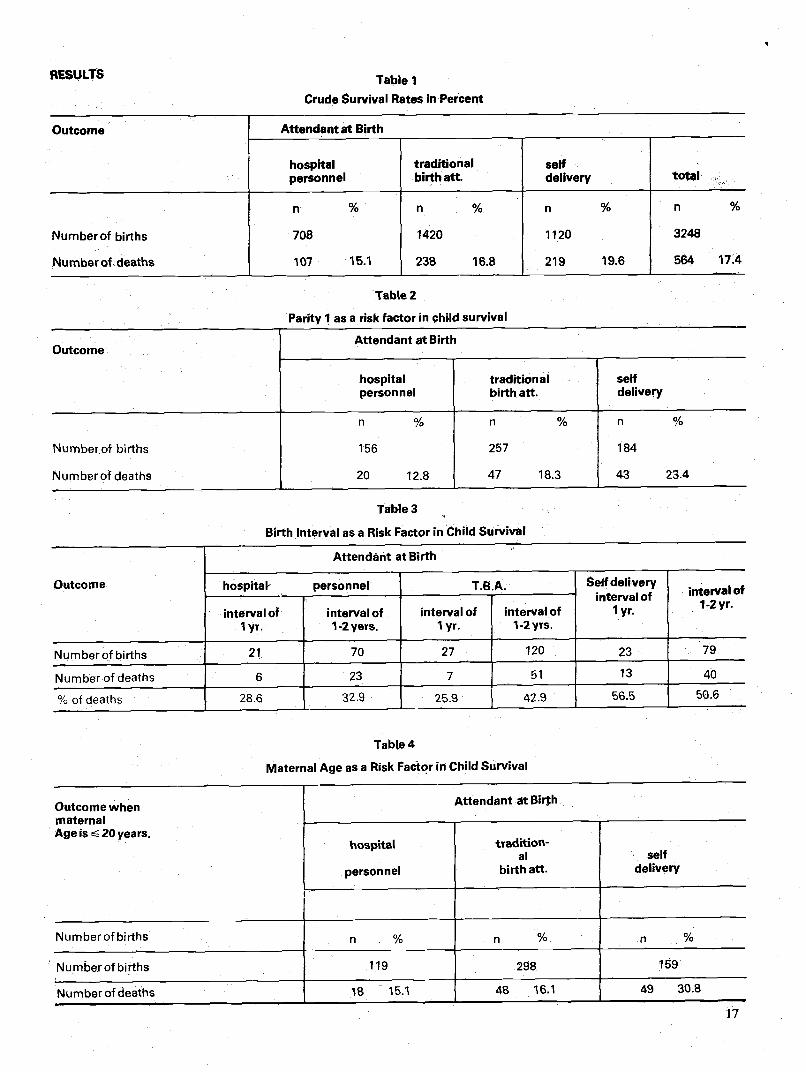
RESULTS Table I Crude Survival Rates in Percent
Outcome Attendant at Birth
hospital personnel
traditional birth att
self delivery
' total
Numberof births
Numberof deaths
n %
708
107 15 1
n % 1420
238 168
n %
1120
219 196
n %
3248
564 17 4
Table 2
Parity 1 as a risk factor in chld survival
Outcome Attendant at Birth
hospital personnel
traditional birth att.
self delivery
Number of births
Numberof deaths
n %
156
20 128
n %
257
47 18.3
Ii %
184
43 23.4
Tabie3
Birth Interval as a Risk Factor in Child Survival
Outcome
Attendant at Birth
hospital- personnel T.B.A. SeØ delivery interval of
1 yr.
• interVa 1-2 yr.
interval of lyr.
interval of 1-2yers.
interval of lyr.
interval of 1-2yrs.
Numberofbirths 21 70 — 27 120 23 79
Numbetof deaths 6 23 — 7 51 13 40
%of deaths 286 329 259 429 565 506
TabLe 4
Maternal Age as a Risk Factor in Child Survival
Outcome when maternal Age is 20 years.
Attendant t Birth
hospital
personnel
tTad%tOfl- al
birth aft. self
delivery
Numberof births % % %
Numberof births 119 298 159
Numberofdeaths l 151 48 161 49 308
17
Discussion
The proportion of births carried outside the health sys- tem has remained at more than 50 percent2' 3• In Tanzania, this setup will prevail for a long time to come. The risks of deaths associated with known risk factors are lowest for the deliveries carried out by the orthodox health workers, fol- lowed by the births carried out by the traditional birth atten- dants and lastly the worst outcome are from unattended deliveries. The risk factors of child survival identified are not peculiar to Tanzania. Training and encouragement of tradi- tional birth attendants should decrease child deaths, where- lse self deliveries when coupled with other known risk fac- tors increase risk of child survival. In the meantime the tradi- tional birth attendants and the women should be educateu on the risk factors of child survival so that the high risk groups are referred for the required care.
REFERENCES
1. Mwaikambo ED, Do Amsi DM. Maternal Relative and Attributable Risks of Neonatal mortality. Paper pre- sented in 11th Annual Scientific Meeting of Association of Obstetricians and Gynaecologists of Tanzania, 1986.
2. The United Republic of Tanzania Inventory of Health Facilities, Dares Salaam, 1979 p. 135.
3. National Demographic Survey of Tanzania, Dar es Salaam 1973; 1: 325.
TRADITIONALMEDICINE IN THARAKA, KENYA
INTRODUCTION
I wish to contribute to the discussion on Traditional Medicine issue by presenting a short report about the research project we are conducting among the Tharaka people of Meru District in Kenya.
I shall brleifly illustrate the basic theoretical principles of the Participatory Action Research approach used in the pro- ject; showing, afterwares, how such an approach can work in practice in a field research project on traditional medicine.
Finally, since this is a work in progress, instead of pre- senting final results I shall state some tentative findings only; I shall conclude by adding two recommendations.
Participatory Action Research (PAR) is a new methodol- ogy which has emerged from the work of social scientists in the Developing Countries of Asia, Latin America and Africa1 to effectively assist rural communities in such countries in their efforts to gain more control over their lives. This method involves a fundamental change from the conven- tional role played by development professionals to a role in which the people are no longer seen as "objects" of develop- ment but as "subjects".2
According to PAR methodology, professional resear- chers should attempt to help local communities to under-
Dr. Guido Giarelli, University of Bologna, Italy Department of Sociology.
stand their situation better and work out solutions together using local resources.and initiative. The aim isto stimulate grass-roots self-reliance, seeking to generate processes of the people's own consciousness and action according to their own priorities.
The role played by the researcher consists of catalyzing, supporting, co-ordinating and synthesizing tasks. As time goes on the dependence of the people on the initial catalysts is suppsed cease, through the generation and develop- ment of internal leadership and skills. The people should within a reasonable time be able to carry on with their collec- tive activities on their own3.
External resources and expertise are not considered to be primary in solving local communities problems, but are offered only as supplements when needed and available to the mobilization of the people's own resources and skills.
A development process can be really effective only if is self-reliant. Passive acceptance of inputs supplied by exter- nal professionals or agencies in a more or less paternalistic manner can only produce cultural parasitism and economi- cal dependence. The failure of thousands of non-participat- ory cooperation programmes in the Third World confirms this statement.
THE PROJECT
(a) Personnel and Institutions involved There is a pre-existing Rural Health Care (RHC) Co-oper-
ation Program being carried out in Tharaka by Nkubu Hospi- tal, where some voluntary doctors belonging to the Italian NGO; CUAMM; are woking. The Department of Sociology of the University of Bologna particularly the Social and Cultural Anthropology Section has started a PAR Project within the framework of such pre-existing RHC Co-operation Program. It is a Joint Research Project, with the membership of CUAMM (which is sponsoring the project through the Italian Ministry of Foreign Affairs) and of the University of Nairobi, particularly the Institute of African Studies and the Depart- ment of Community Health Moreover, there is in Italy a theoretical-methodological elaboration team, composed of many sociologists, anthropologists, medical doctors and public health spelcialists, which plays a role of supervision ofthe work and its reu Its.
Furthermore, for the specific purpose of a phytochemi- cal and pharmacological evaluation of Tharaka hebalistic practices, collaboration with the Kenya Medical Research Institute (KEMRI) as a member in the Joint Research Project has been established. In fact, the Institute has been charged by Kenya Government with the responsibility of evaluating traditional medicines and herbs. (b) Objectivesof the Research
The objective of the research in the Social and Cultural Dynamics of Health Development among Tharaka people. and in particular, the relations between internal (endogenus) dynamisms coming from cultural heritage and creative pre- sent inventiveness of the local community and external (exogenus) dynamisms — coming from multiple contacts of Tharaka culture with foreign cultures are considered.
The aims of this research are mainly two:- (i) to stimulate a self-development process in the health
field of Tharaka people through the methodology of anthropological PAR involving in particular actively the Tharaka traditional health practitioners,
(ii) to foster the integration of their precious traditional
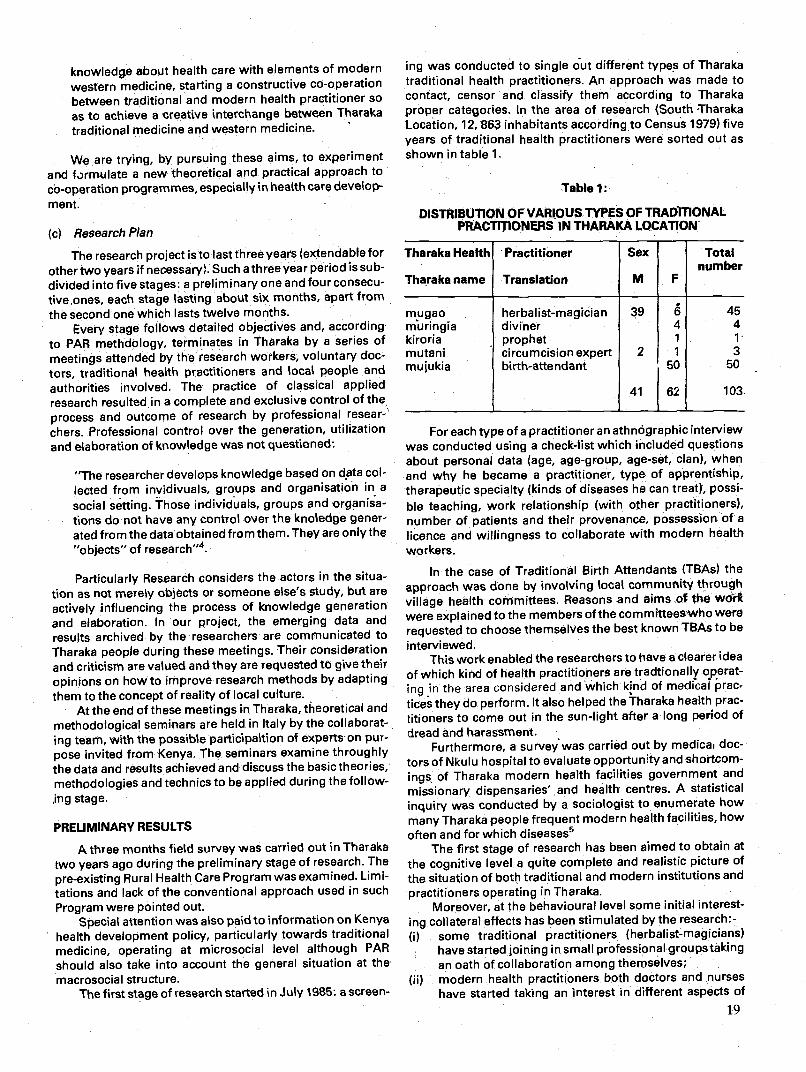
knowledg.e about health care with elements of modern western medicine starting a constructive Co operation between traditional and modern health practitioner so as to achieve a creative interchange between Tharaka traditional medicine and western medicine.
We are trying by pursuing these aims to experiment and Lrmulate a new theoretical and practical approach to co-operation programmes, especially inhea(th care develop- ment.
(c) Research Plan
The research project is to last three years (extendable for other two years if necessary). Such a threeyear period is sub- divided into five stages: a preliminary one andfour consecu- tive ones each stage lasting about six months apart from the second one which lasts twelve months
Every stage follows detailed objectives and according to PAR methdology terminates in Tharaka by a series of
meetings attended by the research workers, voluntary doc-
tors, traditional health practitioners and local people and
authorities involved. The practice of classical applied research resultedin a complete and exclusive control of the process and outcome of research by professional resear-
chers. Professional control over the generation, utilization and elaboration of knowledge was not questioned:
"The researcher develops knowledge based on data col-
lected from irivjdivuals, groups and organisatiofl in a
social setting. Those individuals, groups and organisa- • tions do not have any control over the knoledge gener-
ated from the data obtained from them. They are only the "objects" of research"4.
Particularly Research considers the actors in the situa- tion as not merely objects or someone else's study, but are actively influencing the process of knowledge generation and elaboration. In our project, the emerging data and results archived by the researchers are communicated to Tharaka people during these meetings. Their consideration and criticism are valued and they are requested to give their
opinions on how to improve research methods by adapting them to the concept of reality of local culture.
At the end of these meetings in Tharaka, theoretical and methodological seminars are held in Italy by the collaborat- ing team, with the possible participaltion of experts on pur- pose invited from Kenya. The seminars examine throughly the data and results achieved and discuss the basic theories, methodologies and technics to be applied during the follow-
irig stage.
PRELIMINARY RESULTS
A three months field survey was carried out in Tharaka two years ago during the preliminary stage of research. The
pre-existing Rural Health Care Program was examined. Limi- tations and lack of the conventional approach used in such Program were pointed out.
Special attention was also paid to information on Kenya health development policy, particularly towards traditional medicine, operating at microsocial level although PAR should also take into account the general situation at the macrosocial structure.
The first stage of research started in July 1985: a screen-
ing was conducted to single out different types of Tharaka traditional health practitioners. An approach was made to contact censor and classify them according to Tharaka proper categories. In the area of research (South Tharaka Location 12 863 inhabitants according to Census 1979) five years of traditional health practitioners were sorted out as shown in table 1
Table 1:
DISTRIBUTION OF VARIOUS TYPES OF TRADiTIONAL PRACTiTIONERS IN THARAKA L.OCATION
Tharaka Health
Tharaka name
Practitioner
Translation
Sex
M F
Total number
mugao muringia kiroria mutani mujukia
herbalist-magician diviner prophet circumcision expert birth-attendant
39
2
4 1
1
50
62
45 4 1
3 50
103
For each type of a practitioner an athnOgraphic interview was conducted using a check-list which included questions about personal data (age age group age set clan) when and why he became a practitioner type of apprentiship therapeutic specialty (kinds of diseases he can treat) possi ble teaching, work relationship (with other practitioners), number of patients and their provenance, possession ofa licence and willingness to collaborate with modern health workers.
In the case of Traditional Birth Attendants (TBAs) the
approach was done by involving local commuflity through village health committees. Reasons and aims of the wOk were explained to the members of the commltteeswho were
requested to choose themselves the best known TBAs to be interviewed.
This work enabled the researchers to have a clearer idea of which kind of health practitioners are tradtionally operat ing in the area considered and which kind of medical prac- tices they do perform. It also helped the Tharaka health prac- titioners to come out in the sun-light after a long period of dread and harassment.
Furthermore, a survey was carried out by medicai doc- tors of Nkulu hospital to evaluate opportunity and shortcom-
ings of Tharaka modern health facilities government and
missionary dispensaries and health centres A statistical
inquiry was conducted by a sociologist to enumerate how many Tharaka people frequent modern health facilities, how often and for which diseases5
The first stage of research has been aimed to obtain at the cognitive level a quite complete and realistic picture of the situation of both traditional and modern institutions and
practitioners operating in Tharaka. Moreover, at the behavioural level some initial interest-
ing collateral effects has been stimulated by the research:- (i) some traditional practitioners (herbalist magicians)
have started joining in small professional groupstaking an oath of collaboration among themselves;
(ii) modern health practitioners both doctors and nurses have started taking an interest in different aspects of
19
traditional medical practices and believes, previously ignored or opposed;
(iii) it has been possible to arrange some meetings at the local dispensaries between doctors and traditional health practitioners, so as they have started knowing one another, exchanging ideas and information.
The second stage of research, which is still going on, is aimed at a fuller understanding of the main concepts of health, disease, healing, death, and birth which belong to medical field of Tharaka culture. This is probably more important for an applied research project aiming at a fuller understendrng of the related behaviour of Tharaka people in the so-called "health-seeking process".
We are particularly interested to sort out changes and persistences in the cultural choices of Tharaka people regarding both traditional and modern medicine.
Methodologically we are using two types of approach: (a) Through participant observation and by collection of
certain number of "stories of patients" we are trying to understand the relevance of different choices and con- straints in the health-seeking behaviour of common people of Tharaka.
(b) With traditional health practitioners, using ethnog- raphic interview and participant observation during the healing rituals we are trying to understand the therapeu- tic value of such rituals. Medical practitioners of Nkubu hospital are, in the mean-
while, trying to carry out a scientific evaluation of healing treatments from the bio-medical point of view with the assistance of KEMRI researchers from Nairobi.
Afterwards, they will try to compare the two different redical approaches namely the western and Tharaka tradi- tional healing inquired through some particular clinical cases followed up during this stage so as to formulate, prac- tical proposals of integrating the two systems.
If the main outcome of the participatory approach is increased knowledge about the social setting that is availa- ble to both the researcher and actors in the situation6, then the second stage of research—is readly the greatest effort will be placed on sharing the acquired knowledge about Tharaka health situation with local póople particularly traditional health practitioners and birth-attendants. A series of grass- roots work-shops will probably be arranged with them dur- ing the third stage of research, so as to assist them to improve their knowledge in a changing situation as an effec- tive participatory process must increase the capacity of the actors involved to inquire into and change their situation.
RECOMMENDATIONS
I would like to conclude by adding two recommenda- tions with some relevance for health policies related to trad- itional medicine:- 1. It is important, before starting any kind of integration programme between traditional and modern medicines to undertake a field research to know exactly what traditional medicine means in that area. "Traditional Medicine" is a very general terminology for many different things; and "Traditional Health Practitioners" is just a cover term. Each local culture has got its own traditional medical practices and its own practitioners, classified according to different categories by indigenous terminology. It is important to carry out a long-term, face-to-face approach with the people in the field; and the research should continue even after the integration process has started, so as to survey which social
20
and cultural 'lynamics will spring from such process. 2. PAR approach seems to be the best one to be used to
involve local people particularly local traditional health practitioners since the beginning; stimulating their creativity, their local cultural resources and leaving them to decide which sort of integration to operate between traditional and modern medicine, which selected ele- ments to borrow from western medicine to incorporate into their traditional one. Theoretically, we distinguish in PAR approach between an "action level" and an "inter- vention level": where the former relates to self-reliant actions carried out by local community, stimulated by inputs coming from collateral effects provoked bythe lat- ter level, by the external agents of acculturation on the whole (doctors, researchers, central authorities, etc).
A correct PAR approach should give so much inputs by intervention level that action level of local community will be stimulated without beinf stifled, in a symetric process of common struggle where people and researchers become partners and each side has to learn qually from the other one.
REFERENCES
1. Callaway, H (ed). Participation in Research, Case Studies of Part,icipatory Research in Adult Education. Amersfoort, 1980; Fals Borda, 0.; "Investigating Reality in Order to Transform it", Dialectical Anthropology, 4,
(1), 1979: 33-56; Mustáfa K., "Participatory Research amongst Pastroralist Peasants in Tanzania", Interna- tional Labour Office, Geneva, 1981; TANDON, R. Par-
ticipatory Research in Asia, New Delhi, 1980. 2. Fals Borda, Q., "The Challnge of Action Research",
Development: Seeds of Change, 1, 1981: 55-61; Moser, H., "Action Research as a New Research Paradigm in the Social Sciences", Symposium on Action Research, Car- tagena, Colombia, April 1977; Moser, H., "Participatory Action Research: The Aspect of Research", internan- tional Seminar on Participatory Research, Lepolampi, Finland, September 1981; Oquist, P., "The Epistemology of Action Research," Symposium on Action Research, Cartagena, Colombia, April, 1977.
3. Rahman MA, "The Theory and Practice of Participatory Action Research", in Fals Borda (ed) The Challenge of Social Change, SAGE studies, 1985:116.
4. Tandon, R. Participatory Evaluation and Research: Main Conceptls and Issues", in Fernandes Tandon, R. Par- ticipatory Research and Evaluation, New Delhi, 1981.
5. Data elaboration is still in progress at the Computer labo- ratory of the Department of Sociology in Bologna.
6. Tandon, R., cit., p. 32.

KNOWLEDGE OF MALARIA AND SOME ASPECTS OF ITS CONTROL IN TANGA,
Introduction:
TANZANIA By M. Fivawo
Mataria is an acute or chronic infection, of red biuod cells caused by protozoa parasites of the genus Plasmodium. Among symptoms of malaria include attacks of fever, headaches, chills rigors, general malaise, joint and muscle pains, nauses, vomiting and diarrhoea.
The German Scientist, Robert Koch, reported fromWest- em Usambara in 1898 that the native people called the dis- ease which he was sent to study homa ya mbu (fever of mos- quitoes), which they said was contracted after being bitten by mosquitoes of the lowlands. This clear epidemiological knowledge of the natives has not been followed up to see how the people's knowledge can be integrated into other knowledges of malaria in the effort to effectively control the disease.
One aspect of the malaria problem which has not been adequately given attention to is the behavioral one which could show the interaction processes between community members and health providers to facilitate epidemiological control. The study of the behavioral aspects of malaria in rural Muheza was done to explore and determine factors which influence people's behaviour towards malaria control in order to suggest strategies which would facilitate the development of more effective approaches to generate health programs which will improve malaria control. Studies of people's own ways of dealing with a disease can be used to facilitate acceptable control measures.
Bonde and Sambaa people two major ethnic groups in Tanga have known malaria for as long as they have been in the area. They call the disease 'nyongo', 'homa ya mbu', as well as the latin term 'malaria' itself. Traditional healers diag- nose the disease from the type of fever which is not accom- paniéd by any cold symptomps, as well as from examining the vomitus of the patient or the colour of the patient's urine. Patients often use the traditional as well as biomedicines to treat malaria.
Malaria is today the commonest disease in Tanzania National statistics show that malaria is the most frequent cause of hospital out patient attendances accounting for 10 — 15% attendances. It also account for 6— 10% of hospital admissions. In hospitals, malaria death rate is estimated to be 4—5% and is therefore one of the top-ten killing diseases in Tanzania.
Muheza district of Tanga region is holoendemic for malaria, which means that malaria transmission goes on for more than six months in a year. The inpatient monthly records from the district hospital for 1983 for example, show peak admission of malaria patients during March, April, May, July, August, October and November. The remaining months show lower figures which does not mean improve- ment in the management of the disease but that parasitaemia is maintained at low levels showing no alarm-
ing malaria symptoms. Results of parasitaemia check of a
Dr. M. Fivawo PhD, Department of Traditional Medicine Muhimbili Medical Centre
sample of 136 healthy looking individuals from Tongwe vil- lagein March 1984 showedthat only 41 of them (30%) were negative for malaria parasites. Fifteen percent had high para- site levels between 201 and 1600 parasites for 200 white blood cells (see table 1). The problem of malaria is therefore still serious in spite of the numerous scientific knowledge which we have accumulated.
Medhods.
300 young women were interviewed about their knowl- edge of malaria and malaria control using a questionnaire The subjects for the study were of child bearing age who have participated in the malaria prophylaxis program them selves or for their small children Ten key persons including health personel healers brith attendants and elders in the community were also interviewed Individual cases of dis ease management were studied through follow ups
Results
Response to the questionnaire showed that respondents have very good knowledge of malaria its symptoms, cause, lethality as well as ways of protecting one self from frequent attacks, 84% of the respondents had used chioroquine prophylaxis during previous pregancy. The knowledge which the people have about malaria is a result of both experience with the disease and health education. It is there- fore not surprising that people use both the traditional and Western methods to manage the disease.
More respondents (67%) reported having experienced side effects from therapeutic use of chloroquine than those who reported side effects from prphylactic use of the drug. Attitude research shows that attitudes arise from individuals experiences. Positive experience give rise to positive attitudes about an object while negative experience indicate precaution. With regards to malaria management a high report of side effects is consistt with low level of therapeu- tic compliance to chloroquine. Because-of experienced side effects individuals do not complete the therapeutic dosages. A discriminant analysis of compliance behaviour showed that the individuals behaviour is strongly influenced by the therapeutic experience which she/he has with chloroquine use. Twelve other factors, including knowledge and use of herbal medicine for malaria, were also found to have-influ- ence on prophylaxis use.
Herbal medicine are used both for treatment of malaria and for self protection. (Table 2). Muarobaini, Mzugwa, Mvumbasi, Hozandoghoi and other medicinal plants are often used to treat malaria alongside hospital medicines. Some of the above named medicines are known to contain medicinal compounds which do work on malaria parasites and/or mosquito. Others are still being studied for their chemical contents and biological activity. Mvumbasi, Ocimurn suave for example, which is a shrub native to Tan- zania, is extensively used in Muheza to repel mosquito and has some antimicrobial activity as well. The other medicinal plants which are used by the people may also contain chem- icals which work on malaria.
Another important factor which is influencial in the man-
agement of malaria is the community's social structure. The individual is not always dependent on other People's advices for her/his medical behaviour, but is influenced by "impor- tant others" in her behaviour particularly with regard to the
21
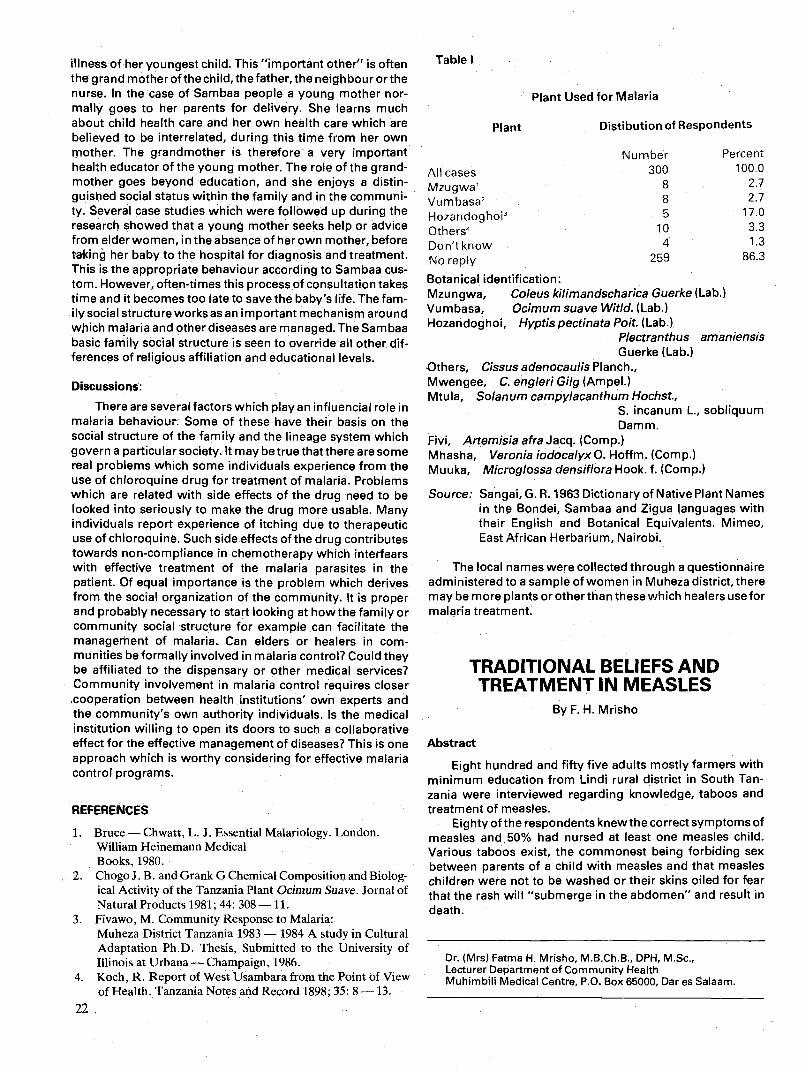
illness of her youngest child. This "important other" is often the grand mother ofthe child, the father, the neighbour orthe nurse. In the case of Sambaa people a young mother nor- mally goes to her parents for delivery. She learns much about child health care and her own health care which are believed to be interrelated, during this time from her own mother. The grandmother is therefore a very important health educator of the young mother. The role of the grand- mother goes beyond education, and she enjoys a distin- guished social status within the family and in the communi- ty. Several case studies which were followed up during the research showed that a young mother seeks help or advice from elder women, in the absence of her own mother, before taking her baby to the hospital for diagnosis and treatment This is the appropriate behaviour according to Sambaa cus- tom. However, often-times this process of consultation takes time and it becomes too late to save the baby's life. The fam- ily social structureworksas an important mechanism around which malaria and other diseases are managed. The Sambaa basic family social structure is seen to override all other dif- ferences of religious affiliation and educational levels.
Discussions:
There are several factors which play an influencial role in malaria behaviour Some of these have their basis on the social structure of the family and the lineage system which govern a particular society. It may be true that there are some real problems which some individuals experience from the use of chloroquine drug for treatment of malaria. Problems which are related with side effects of the drug need to be looked into seriously to make the drug more usable. Many individuals report experience of itching due to therapeutic use of chloroquine. Such side effects of the drug contributes towards non-compliance in chemotherapy which interfears with effective treatment of the malaria parasites in the patient. Of equal importance is the problem which derives from the social organization of the community. It is proper and probably necessary to start looking at how the family or community social structure for example can facilitate the management of malaria. Can elders or healers in com- munities be formally involved in malaria control? Could they be affiliated to the dispensary or other medical services? Community involvement in malaria control requires closer cooperation between health institutions' own experts and the community's own authority individuals. Is the medical institution willing to open its doors to such a collaborative effect for the effective management of diseases? This is one approach which is worthy considering for effective malaria control programs.
REFERENCES
1. Bruce — Chwatt, L. J. Essential Malariology. London. William Heinemaun Medical Books, 1980.
2. Chogo J. B. and Grank G Chemical Composition and Biolog- ical Activity of the Tanzania Plant Ocimum Suave. Jornal of Natural Products 1981; 44: 308—11.
3. Fivawo, M. Community Response to Malaria: Muheza District Tanzania 1983 — 1984 A study in Cultural Adaptation Ph.D. Thesis, Submitted to the University of Illinois at Urbana — Champaign, 1986.
4. Koch, R. Report of West Usámbara from the Point of View of Health. Tanzania Notes and Record 1898; 35: 8—13.
22
Plant Used for Malaria
Plant Distibution of Respondents
Percent
All cases 100.0
Mzugwa1 8 2.7
Vumbasa2 8 2.7
Hozandoghoi3 5 17.0
Others4 10 3.3
Don't know 4 1.3
No reply 259 86.3
Botanical identification: Mzungwa, Coleus kilimandscharica Guerke (Lab.) Vumbasa, Ocimum suave Witld. (Lab.) Hozandoghoi, Hyptis pectinata Poit. (Lab.)
Plectranthus amaniensis Guerke (Lab.)
Others, Cissus adenocaulis Planch., Mwengee, C. engleri GiIg (Ampel.) Mtula, Solanum camp ylacanthum Hochst.,
S. incanum L., sobliquum Damm.
Fivi, Artemisia afra Jacq. (Comp.) Mhasha, VeroniaiodocalyxO. Hoffm. (Comp.) Muuka, Microglossa densiflora Hook. f. (Comp.)
Source: Sangal, G. R. 1963 Dictionary of Native Plant Names in the Bondei, Sambaa and Zigua languages with their English and Botanical Equivalents. Mimeo, East African Herbarium, Nairobi.
The local names were collected through a questionnaire administered to a sample of women in Muheza district, there may be more plants or other than these which healers use for malaria treatment.
Abstract
TRADITIONAL BELIEFS AND TREATMENT IN MEASLES
By F. H. Mrisho
Eight hundred and fifty five adults mostly farmers with minimum education from Lindi rural district in South Tan- zania were interviewed regarding knowledge, taboos and treatment of measles.
Eighty of the respondents knew the correct symptoms of measles and 50% had nursed at least one measles child. Various taboos exist, the commonest being forbiding sex between parents of a child with measles and that measles children were not to be washed or their skins oiled for fear that the rash will "submerge in the abdomen" and result in death.
Table I
Number 300
Dr. (Mrs) Fatma H. Mrisho, M.B.Ch.B., DPH, M.Sc., Lecturer Department of Community Health Muhimbili Medical Centre, P.O. Box 65000, Dares Salaam.
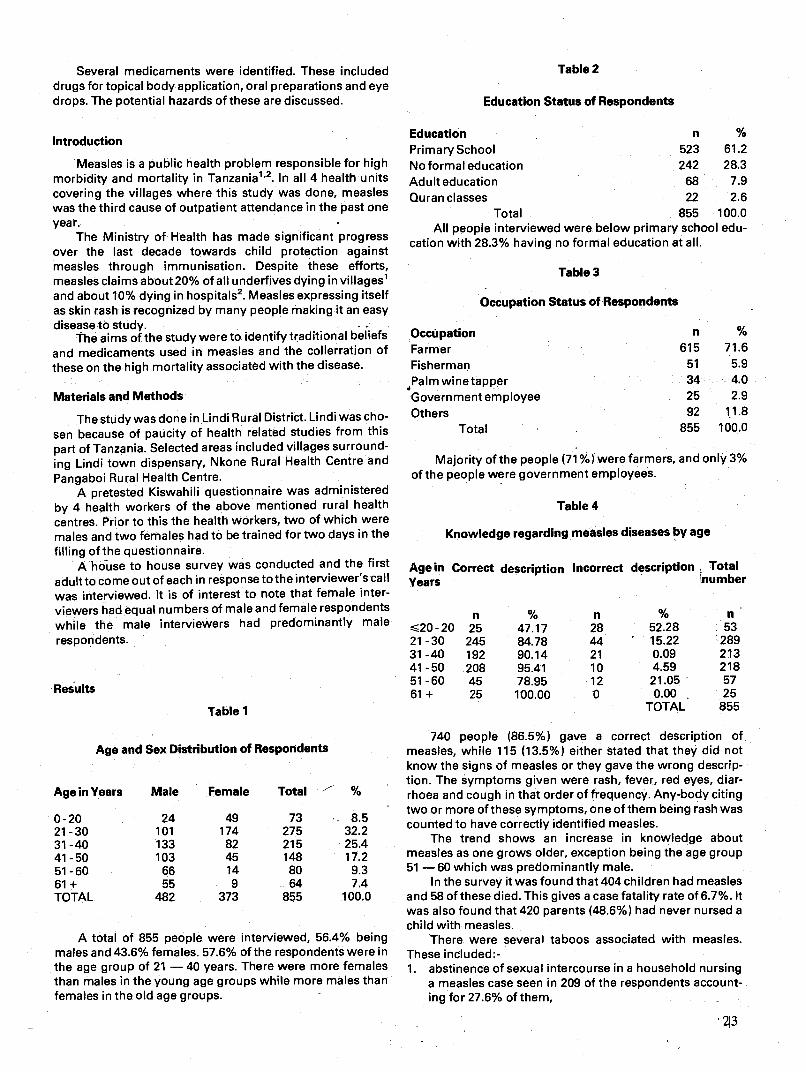
Table 2
Education Status of Respondents
Education n %
PrimarySchool 523 61.2 No formal education 242 28.3 Adult education 68 7.9 Quran classes 22 2.6
Total 855 100.0 All people interviewed were below primary school edu-
cation with 28.3% having no formal education at all.
Table 3
Occupation Status of Respondents
Several medicaments were identified. These included drugs for topical body application, oral preparations and eye drops. The potential hazards of these are discussed.
Introduction
Measles is a public health problem responsible for high morbidity and mortality in Tanzania"2. In all 4 health units covering the villages where this study was done, measles was the third cause of outpatient attendance in the past one year.
The Ministry of Health has made significant progress over the last decade towards child protection against measles through immunisation. Despite these efforts, measles claims about 20% of all underfives dying in villages1 and about 10% dying in hospitals2. Measles expressing itself as skin rash is recognized by many people making it an easy disease to study
The aims of the study were to identify traditional beliefs and medicaments used in measles and the collerration of these on the high mortality associated with the disease.
Materials and Methods
The study was done in Lindi Rural District. Lindi was cho- sen because of paucity of health related studies from this
part of Tanzania Selected areas included villages surround
ing Lindi town dispensary, Nkone Rural Health Centre and
Pangaboi Rural Health Centre. A pretested Kiswahili questionnaire was administered
by 4 health workers of the above mentioned rural health centres Prior to this the health workers two of which were males and two females had to be trained for two days in the
filling of the questionnaire. A hOuse to house survey was conducted and the first
adult to come out of each in response to the interviewer's call was interviewed It is of interest to note that female inter viewers had equal numbers of male and female respondents while the male interviewers had predominantly male
respondents.
Results
Table 1
Age and Sex Distribution of Respondents
Male Female Total
OccUpation Farmer Fisherman Palm wine tapper Government employee Others
Total
n % 615 71.6
51 5.9 34 4.0 25 2.9 92 11.8
855 100.0
Majority of the people (71%) were farmers and only 3% of the people were government employees.
Table 4
Knowledge regarding measles diseases by age
description Incorrect description Age in Correct Years
n 20-20 25 21-30 245 31-40 192 41-50 208 51-60 45 61+ 25
Total number
% 47.17 84.78 90.14 95.41 78,95 100.00
n % n 28 52.28 53 44 15.22 289 21 0.09 213 10 4.59 218 12 21.05 57
0.00. TOTAL
25 855
Age in Years
0-20 24 49 73 8.5 21-30 101 174 275 32.2 31-40 133 82 215 25.4 41-50 103 45 148 17.2 51-60 66 14 80 9.3 61+ 55 9 64 7.4 TOTAL 482 373 855 100.0
740 people (86.5%) gave a correct description of measles, while 115 (13.5%) either stated that they did not know the signs of measles or they gave the wrong descrip- tion. The éymptoms given were rash, fever, red eyes, diar- rhoea and cough in that order of frequency. Any-body citing two or more of these symptoms, one of them being rash was counted to have correctly identified measles.
The trend shows an increase in knowledge about measles as one grows older, exception being the age group 51 —60 which was predominantly male.
In the survey it was found that 404 children had measles and 58 of these died. This gives a case fatality rate of 6.7%. It was also found that 420 parents (48.6%) had never nursed a
A total of 855 people were interviewed, 56.4% being males and 43.6% females. 57,6% of the respondents were in the age group of 21 — 40 years. There were more females than males in the young age groups while more males than females in the old age groups.
child with measles. There were several taboos associated with measles.
These included:- 1. abstinence of sexual intercourse in a household nursing
a measles case seen in 209 of the respondents account- ing for 27.6% of them,
213
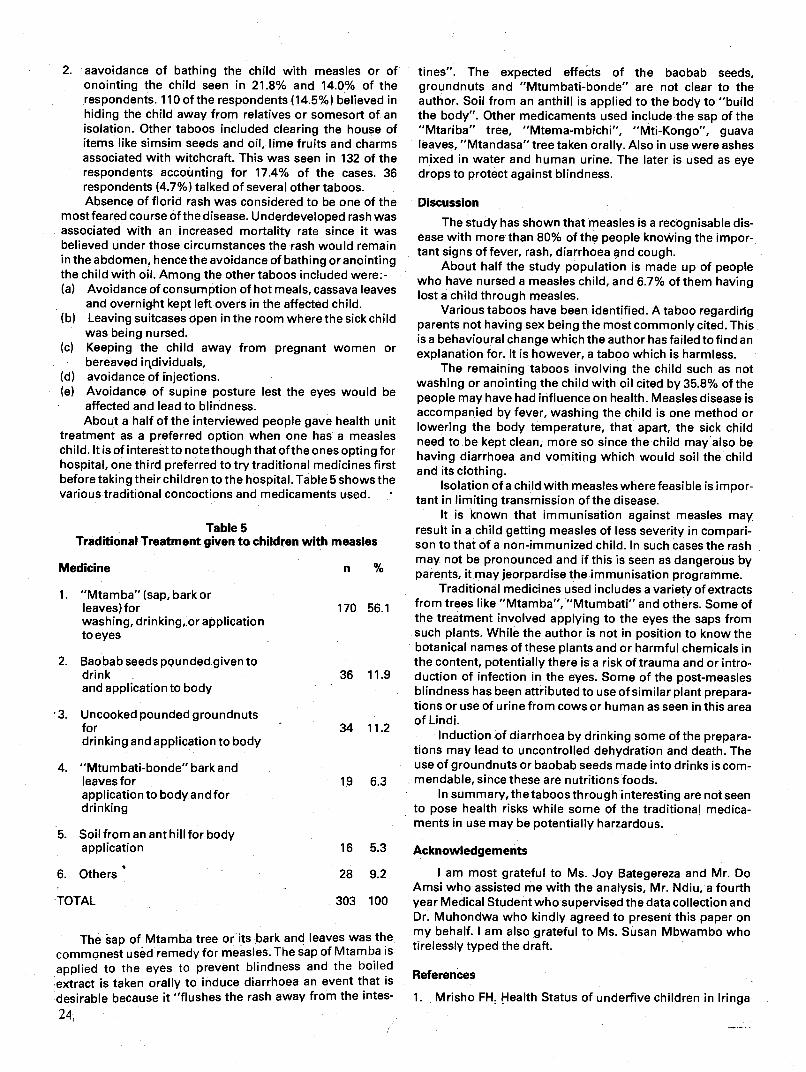
2. aavoidance of bathing the child with measles or of onointing the child seen in 21.8% and 14.0% of the respondents. 110 of the respondents (14.5%) believed in hiding the child away from relatives or somesort of an isolation. Other taboos included clearing the house of items like simsim seeds and oil, lime fruits and charms associated with witchcraft. This was seen in 132 of the respondents accounting for 17.4% of the cases. 36 respondents (4.7%) talked of several other taboos. Absence of florid rash was considered to be one of the
most feared course of the disease. Underdeveloped rash was associated with an increased mortality rate since it was believed under those circumstances the rash would remain in the abdomen, hence the avoidance of bathing or anointing the child with oil. Among the other taboos included were:- (a) Avoidance of consumption of hot meals, cassavä leaves
and overnight kept left overs in the affected child. (b) Leaving suitcases open in the room where the sick child
tines". The expected effects of the baobab seeds, groundnuts and "Mtumbati-bonde" are not clear to the author. Soil from an anthill is applied to the body to "build the body". Other medicaments used include the sap of the "Mtariba" tree, "Mtema-mbichi", "Mti-Kongo", guava leaves, "Mtandasa" tree taken orally. Also in use were ashes mixed in water and human urine. The later is used as eye drops to protect against blindness.
Discussion The study has shown that measles is a recognisable dis-
ease with more than 80% of the people knowing the impor- tant signs of fever, rash, diarrhoea nd cough.
About half the study population is made up of people who have nursed a measles child, and 6.7% of them having lost a child through measles.
Various taboos have been identified. A taboo regarding parents not having sex being the most commonly cited. This is a behavioural change which the author has failed to find an explanation for. It is however, a taboo which is harmless.
The remaining taboos involving the child such as not washing or anointing the child with oil cited by 35.8% of the people may have had influence on health. Measles disease is accompanied by fever, washing the child is one method or lowering the body temperature, that apart, the sick child need to be kept clean, more so since the child mayalso be having diarrhoea and vomiting which would soil the child and its clothing.
Isolation of a child with measles where feasible is impor- tant in limiting transmission of the disease.
It is known that immunisation against measles may. result in a child getting measles of less severity in compari- son to that of a non-immunized child. In such cases the rash may not be pronounced and if this is seen as dangerous by n to parents, it may jeorpardise the immunisation programme.
Traditional medicines used includes a variety of extracts 170 56 1
from trees like "Mtamba", "Mtumbati" and others. Some of the treatment involved applying to the eyes the saps from such plants. While the author is not in position to know the botanical names of these plants and or harmful chemicals in the content, potentially there is a risk of trauma and or intro-
36 11.9 duction of infection in the eyes. Some of the post-measles blindness has been attributed to use of similar plant prepara- tions or use of urine from cows or human as seen in this area
34 11 2 of Lindi.
Induction of diarrhoea by drinking some of the prepara- tions may lead to uncontrolled dehydration and death. The use of groundnuts or baobab seeds made into drinks is corn-
19 6.3 mendable, since these are nutritions foods. In summary, the taboos through interesting are not seen
to pose health risks while some of the traditional medica-
was being nursed. (C) Keeping the child away from pregnant women or
bereaved irtdividuals, (d) avoidance of injections. (e) Avoidance of supine posture lest the eyes would be
affected and lead to blindness. About a half of the interviewed people gave health unit
treatment as a preferred option when one has a measles child. It is of interest to note though that of the ones opting for hospital, one third preferred to try traditional medicines first before taking their children to the hospital. Table 5 shows the various traditional concoctions and medicaments used.
Table 5 Traditional Treatment given to children with measles
Medicine
1. "Mtamba" (sap, bark or leaves) for washing, drinking,or application to eyes
2. Baobab seeds pounded given to drink and application to body
3. Uncooked pounded groundnuts for drinking and application to body
4. "Mtumbati-bonde" bark and leaves for application to body and for drinking
5. Soil from an ant hill for body application
6. Others'
TOTAL 303 100
ments in use may be potentially harzardous.
Acknowledgements
I am most grateful to Ms. Joy Bategereza and Mr. Do Amsi who assisted me with the analysis, Mr. Ndiu, a fourth year Medical Student who supervised the data collection and Dr. Muhondwa who kindly agreed to present this paper on my behalf. I am also grateful to Ms. Susan Mbwarnbo who tirelessly typed the draft.
16 5.3
28 9.2
The èap of Mtamba tree or its bark and leaves was the commonest used remedy for measles. The sap of Mtamba is
applied to the eyes to prevent blindness and the boiled R
extract is taken orally to induce diarrhoea an event that is e erences
desirable because it "flushes the rash away from the intes- 1. Mrisho Fll! Health Status of underfive children in Iringa 24

Region. Report UNICEF/WHO Joint Support Nutrition Programme. 1984; 9.
2. Ministry of Health, United Republic of Tanzania Guidelines for the implementation of The Primary Health Care Programme in Tanzania.. 1983; 20.
THE PATTERN OF ILLNESS AND THE UTILIZATION OF AVAILABLE HEALTH
SERVICES IN TWO REGIONS OF TANZANIA
Dr. J.Z. Kilewo1, LA.J Semali2,LA.J.R. Msuya3, E. N.Mshiu2,D.M. Do Amsi3,CK. Makwaya3,
E.P.Y. Muhondwa4
Introduction
In order to officially recognize and effectively deploy the services of traditional healers, it is necessayto collect data on baseline utilization rates of the available health services. It is also imperative to have some knowledge of the pattern of diseases generally affecting the population as well as the therapeutic efficacy of the available services.
One of the problems affecting the recognition and effec- tive depolyrnent of traditional health practices by the mod- ern medical practitioners however, is the different concept ofdisease causation that is strongly held by these two sides. Furthermore, the diagnostic and treatment methods of dis- ease also differ greatly between the two groups. The only way of bringing the two systems together is by the people accepting and utilizing them without prejudicq. Traditional systems have always been with the people and the concept of disease causation in the general population bears much resemblance of that held by traditional healers because of their closeness and cultural integration in the community. Modern systems however, have not been so close to the people in many of the developing countries because of the expenses involved and the inadequacy of the facilities for the majority of the people. This should make traditional systems more popular than modern systems if no system supresses
the other as is the tendency with the modern system in many countries.
In Tanzania there is no policy regarding traditional med- ical practice except that the law does not prohibit or prevent the bona fide practice of systems of therapeutics according to native methods by persons recognized by the comm unity in which they belong1. Traditional healers are therefore acceptable as health providers by the people because mod— sm health facilities do not adequately cover the entire coun- try. It has been estimated that about 75% of the country population is living within a radius of 10 kilometers of a mod- ern. health facility. But the need and demand for health ser- iices has not been adequately assessed in this country because of lack of appropriate studies and inadequate dis- ase reporting mechanisms. This paper reports some of the indings of a study which attempted to determine the pattern f illness and people's utilization of available health services n order to shed light into extent to which people use the ser- iices provided by traditional healers.
Materials and Methods
Two regions in Tanzania were selected for the study, one to the North of the country, Arusha, and the other to the South, Iringa. The two regions were taken to repu!esent the socio-cultural aspects of the respective north and south extremes of the country. Arusha region Is placed to the north east with an area of about 44,000 sq. km. and a population of 926, 223 from the 1978 population census2. The inhabitants are engaged in both pastural and agricultural life. lringa reg- ions on the other hand is to the south with an area of about 40,000 sq. km. and a population of 925,044, the majority of whom are engaged in agriculture.
A list of villages was obtained from each ren and a random sample of 50 villages was taken from each. In each
village one ten-cell leader was randomly selected and all the households (usually 10 but could be more) under his jurisdic- tion were studied. The heads of these households were asked about members of their hOuseholds who developed illness during the month preceeding the interview. They were also asked to state the type of illness, where it was treated and the outcome of such treatment. In addition they were asked about diseases which they considered best treated by traditional healers.
Results
3Department of Epidemiology, Muhimbili Medical Centre, P.O. Box 65000, DARESSALAAM.
'Traditional Medicine Research Unit, Muhimbiji Medical Centre, P.O. Box 65000, DAB ES SALAAM.
2Peprtment of Biostatisticts, Muhimbili Medical Centre, P.O. Box 65000, OAR ES SALAAM.
4Department of Behavioural Sciences, Muhimbili Medical Centre, P.O. Box 65000, DAR ES SALAAM.
The actual diseases developed by household members and the hypothetical ones best treated by traditional healers were so many and varied that it became necessary to categorize them into 28 groups of related diseases. Since the diseases were mostly descriptions of signs and symptoms by those interviewed and rtot based on standardized proce- dures it was not possible to classify them according to the scientific method of disease classification. For example, all diseases producing fever as their main symptom, were placed in one group, those producing predominantly gas- trointestinal symptoms in another, and so on. Diseases like measles, leprosy and asthma which seemed well known to those interviewed were given the same names. Diseases producing ill defined symptoms were placed in one cate- gory.
A list of the top ten group of diseases according to the descriptions of the heads of households for Arusha and Iringa was then compiled and compared with that for Tan-
25
zania's most frequent cause of admissions to hospitals and out-patient attendances3. The ranking was found to compare rather well with only minor differences as shown, fevers, respiratory diseases and gastrointestinal disorders were found to rank high on the !Ists.
Table 2 shows that relatively, Iringa region had more gastrointestinal disorders, more obstetric and gynaecologi- cal disorders and more leprosy than Arusha which had a higher relative frequency of respiratory diseases and fevers.
Table 3 and 4 s(ow disease pattern as seen in fringa and Arusha respectively. The tables clearly show that the pattern in these two regions is similar. Some differences however do exist. For example respiratory diseases in Arusha have the lowest frequency in the age group 10-19 years where else in lringa it is lowest in the 20 - 29 year age group. In Aruha Obstetric and Gynaecologicai disorders show the highest frequency in the age group.20 - 29 while in lringa in the 30 - 39 year age group. Table 5 shows that 73.5% of all the sick consulted modern health services while 11.6% consulted traditional health services. Itcan also beseenthat6.2% of the sick did not consult ny health services.
In table 6 and 7 the educational status of the heads of households is categorised. The first category comprises of those who had never had any form of formal education, the
ond those who had either attained adult literacy educa- tion or primary IV education, and the third, those who had either attained primary VII or secondary school form IV edu- cation. The results show that the level of education of the head of household did not influence the utilization.
Figure 1 -3 show the differences in utilization by age and place. Modern health service-utilization was the highest in both regions but it was higher in Arusha than lringa. There was some tendency for utilization to decline with age in both regions but this could be a cohort effect.
Traditional health service utilization was slightly higher in the older age groups, Iringa having higher utilization rates than Arusha. Older age groups tended toutilize both services more than the younger ones and Iringa utilized both services more than Arusha.
Figure 4 shows that there is a significant difference in the health service utilization rates between Iringa and Arusha but virtually no difference between the sexes.
Figure 5 and 6 show utilization rates by disease category and place. Although utilization rates are higher for modern than for traditional health services the order of utilization by disease category is quite different. Diseases like paralysis, obstetrics and gynaecoiogical conditions and unknown dis- eases ranked high in traditional healer utilization while they ranked low in modern health service utilization.
Discussion
Although there are many ways in which the top ten causes for admission and out-patient attendance resemble the groups of diseases for Iringa and Arusha, there are some striking differencs like those seen for obstetrics and
gynaecological disorders. This forms the first cause for hos- pital admissions but one of the last conditions causing illhealth in the community. This can be explained by the fact that most deliveries taking place in hospitals are probably normal and not considered to be a cause for iflhealth by the community.
It can be seen from Table 1 that respiratory diseases rank
high in the group of diseases for Iringa and Arusha while they
26
do no rank So high in the out-patient attendances. If pneumonias, bronchitis and other diseases of the respiratory system are combined, this would rsnkrespiratóry diseases higher on the list. Similarly, on the list of causes for admim- mision to hospitals respiratorydtseaseswouldranksecond if tuberculosis, pneumonias and respiratory diseases other than pneumoniaswerecombined.
The differences ifl disease pattern between the bvo reg- ions reflect true 4ifferences in the magnitude-of these dis- ease groups. This is so because inspite of using proportional morbidity rates for comparison of the two ragions, their population structures were very similar and the interviewers used in both regions were the same.
The results have shown that 73.5% of the household members who developed illness during the one month period before the interview sought health care from modern medical services. This finding is in great contrast to that of other studies elsewhere where the majority of those inter- viewed would prefer to consult traditional healers rather than modern medical services for various health problems. Of those interviewed in Ethiopia, 45.6% consulted traditional healers, 32.8% consulted modern medical services and 21.6% consulted traditional health services4. The difference between our study and the Ethiopian study is that while we dealt with people who had developed disease during the pre- ceeding one month period, the Ethiopian study interviewed individuals who had developed in the proceeding one year period. The reasons for such health service utilization con- trast are not clear. In Botswana which is at about the same stage of development as Tanzania, trditional healing is reported to be a declining profession. (. -f the reasons for such a decline is the development of the scientific health care which tends to make the traditional healer lose his credibility and deprive him of his former prestige and patients5. How- ever, the experience of other workers show that traditional curing systems do not simply fade away when confronted with western and style medicine'°.
In a study involving high school students in Liberia majority of students aged 18-22 years did not prefer the ser- vices of traditional healers11. In another study in Nigeria it was shown that educated people tend to utilize the orthodox system while the illiterates prefer the traditional health sys- tem12. Our study did not enquire about the educational status of each of the individuals who had developed illness but only that of the head of the households in which the sick individuals lived. It is not known how much his educational status would influence utilization by other members of the household but it is known that the head of the household is normally a very powerful decision maker in the African cul- ture. The hrghst educational level achieved by heads of households was ordinary level secondary school, which was actually attained by very few household heads. Our results - show that for the educational levels studied increasing levels of education did not influence utilization pattern. It is how- ever, not known whether higher educational levels would- influence the utilization pattern.
In Tanzania the level of literacy is the highest among other developing countries in Africa. It is however not clear 'how much this achievement has contributed to our findings. Another limitation in our study was that the interviewers were not detailed enough to obtain the true pattern of illhealth and health service utilization. The pattern of illhealth - obtained seemed mostly to reflect physical types of illhealth and not the types of illhealth such as would be brought about
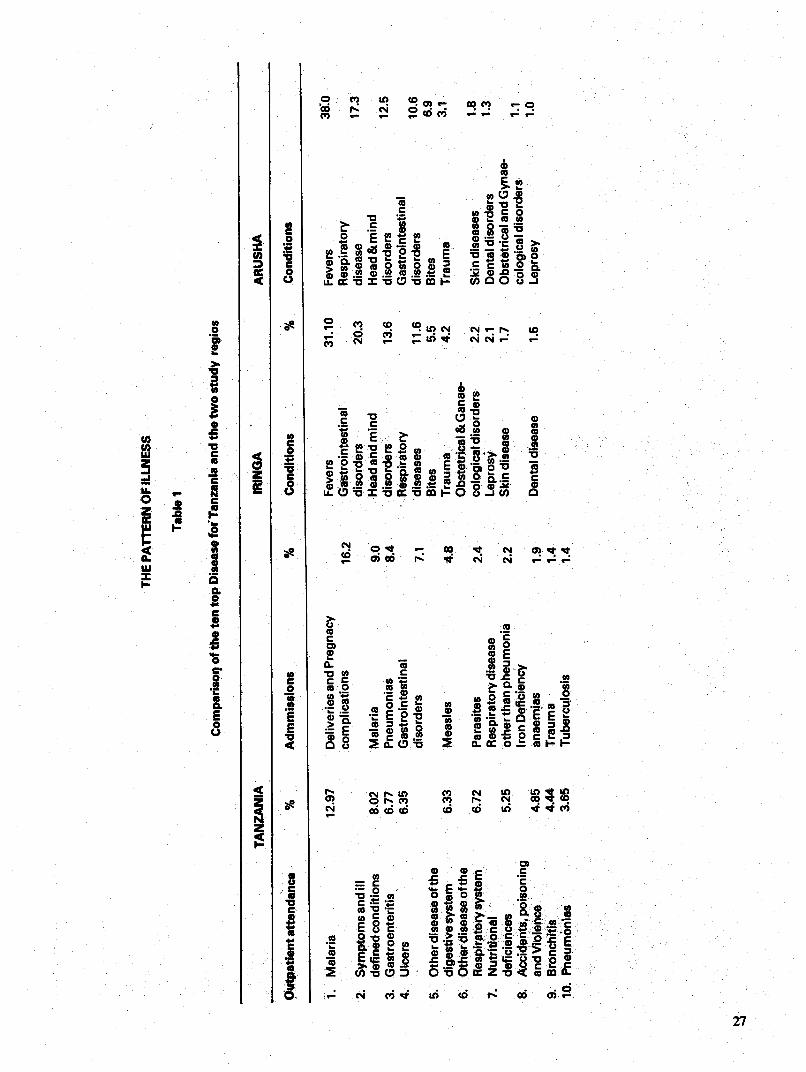
1.
Mal
aria
2.
Sym
ptor
nsan
diU
de
fined
cond
ition
s 3.
G
astr
oent
eriti
s 4.
U
lcer
s
5.
Oth
er d
isea
se o
f the
di
gest
ive
syst
em
6.33
6.
O
ther
dise
ase
of th
e R
espw
etor
y sy
stem
67
2 7
Nut
ritio
nal
defic
ienc
es
5 25
8
Acc
iden
ts, p
oiso
ning
an
d V
iole
nce
485
9 B
ronc
hitis
44
4 10
P
neum
onia
s 36
5
Mal
aria
P
rieum
onia
s G
astr
oint
estin
al
diso
rder
s
Mea
sles
Par
asite
s R
espi
rato
ry di
seas
e ot
her t
han
pheu
mon
ia
Iron
Def
icie
ncy
anae
rnia
s T
raum
a T
uber
culo
sis
TH
E P
AT
rER
N O
F IL
LNE
SS
380
17.3
12.5
10.6
6.
9 3.
1
1.8
1.3
1.1
1.0
Tab
le I
Com
paris
oq of
the
ten
tOp
Dis
ease
for T
anza
nia a
nd th
e tw
o st
udy
regi
os
TA
NZ
AN
IA
IRIN
GA
A
RU
SH
A
Out
patie
nt a
ttend
ance
%
A
dmm
ussi
ons
%
Con
ditio
ns
%
Con
ditio
ns
12.9
7 D
eliv
erie
s and
Pre
gnac
y co
mpl
icat
ions
8.02
6.
77
6.35
Fev
ers
16.2
G
astr
oint
estin
al
diso
rder
s 9.
0 H
ead a
nd m
ind
8.4
diso
rder
s R
espi
rato
ry
7.1
dise
ases
B
ites
4.8
Tra
uma
Obs
tetr
ical
& G
anae
24
co
logi
cal d
isor
ders
Le
pros
y 2
2 S
kin
dise
ase
1.9
Den
tal d
isea
se
1.4
1.4
31.10
Fevers
-
Res
pira
tory
20.3
dise
ase
Hea
d &
min
d 13
.6
diso
rder
s G
astr
oint
estin
al
11.6
diso
rder
s 5.
5 B
ites
4.2
Tra
uma
2.2
Ski
n di
seas
es
2.1
Den
tal d
isor
ders
1.
7 O
bste
tric
al an
d G
ynae
- co
logi
cal d
isor
ders
1.
5 Leprosy
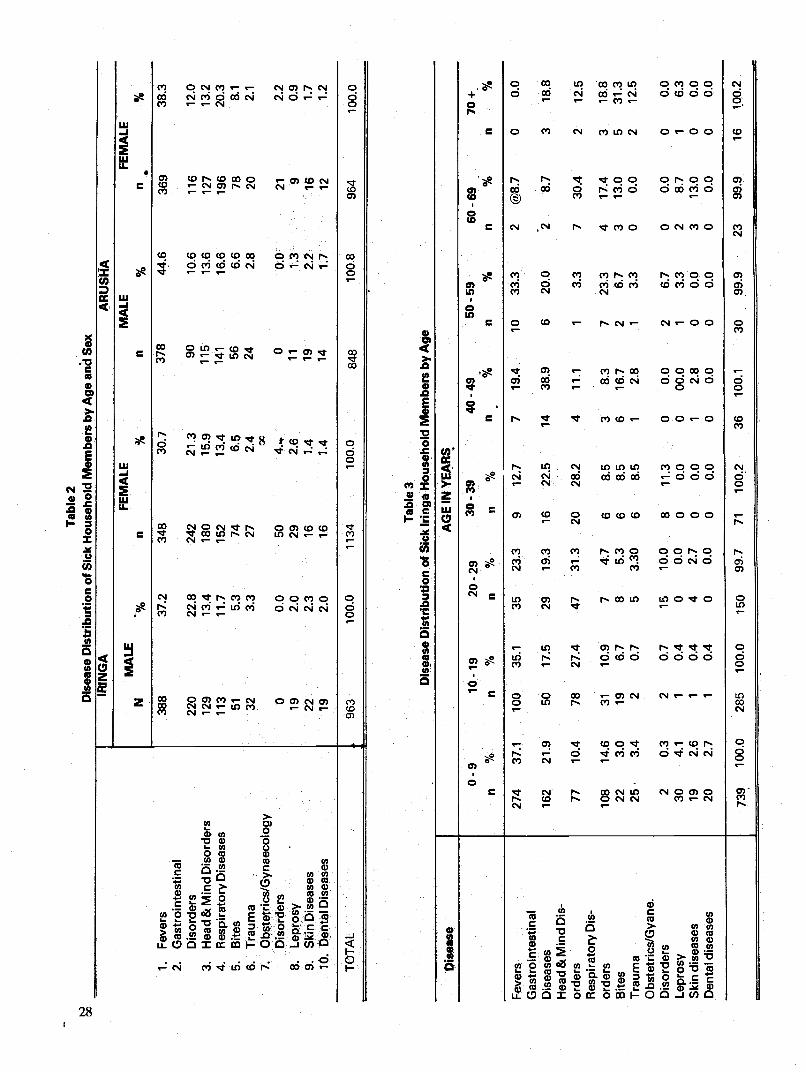
t.)
00
IRIN
GA
Tab
le 2
D
isea
se D
istr
ibut
ion
of S
iók
Hou
seho
ld M
embe
rs b
y A
ge a
nd S
ex
1.
Fev
ers
2.
Gas
troi
ntes
tinal
D
isor
ders
3.
H
ead &
Min
d D
isor
ders
4.
R
espi
rato
ry D
isea
ses
5.
Bite
s 6.
T
raum
a 7.
O
bste
tric
s/G
ynae
colo
gy
Dis
orde
rs
8 Le
pros
y 9
Ski
n D
isea
ses
10
Den
tal D
isea
ses
AR
US
HA
MA
LE
FE
MA
LE
MA
LE
FE
MA
LE
N
%
fl %
n
%
n %
388
37.2
34
8 30
.7
378
44.6
36
9 38
.3
220
22.8
24
2 21
.3
90
10.6
11
6 12
.0
129
13.4
18
0 15
.9
115
13.6
12
7 13
.2
113
11.7
15
2 13
.4
141
16.6
19
6 20
.3
51
5.3
74
6.5
56
6.6
78
8.1
32
3.3
27
2.4 00
24
2.
8 20
2.
1
0
0.0
50
4.-i
0 0.
0 21
2.
2 19
2.
0 29
2.
6 11
1.
3 9
0.9
22
2.3
16
1.4
19
2.2
16
1.7
19
2.0
16
1.4
14
1.7
12
1.2
TOTAL
963
1000
1134
1000
848
1008
964
1000
Table 3
Disease Distribution of Sick Irunga Household Members by Age
Disease
AGE IN YEARS
0 9
10 19
20 29
30 39
40 49
50 59
60 69
70+
%
%
%
%
fl %
n
%
n %
n
%
Fev
ers
Gas
troi
ntes
tinal
Diseases
Head & Mind Dis-
orders
Res
pira
tory
Dis
- or
ders
B
ites
Tra
uma
Obs
tetr
ics/
Gya
ne.
Dis
orde
rs
Lepr
osy
Ski
ndis
ease
s D
enta
l dis
ease
s
274
37 1
10
0 35
1
35
233
9 12
7
7 19
4 10
33
3 2
@87
0
0 0
162
219
50
175
29
193
16
225
14
389
6
200
2
87
3
188
77
10.4
78
27
.4
47
31.3
20
28
.2
4 11
.1
1 3.
3 7
30.4
2
12.5
108
14.6
31
10
.9
7 4.
7 6
8.5
3 8.
3 7
23.3
4
17.4
3
18.8
22
3.
0 19
6.
7 8
5.3
6 8.
5 6
16.7
2
6.7
3 13
.0
5 31
.3
25
3.4
2 0.
7 5
3.30
6
8.5
1 2.
8 1
3.3
0 0.
0 2
12.5
2 0.
3 2
0.7
15
10.0
8
11.3
0
0.0
2 6.
7 0
0.0
0 0.
0 30
4.
1 1
0.4
0 0.
0 0
0.0
0 00
.0
1 3.
3 2
8.7
1 6.
3 19
2.
6 1
0.4
4 2.
7 0
0.0
1 2.
8 0
0.0
3 13
.0
0 0.
0 20
2.
7 1
0.4
0 0.
0 0
0.0
0 0.
0 0
0.0
0 0.
0 0
0.0
739
100.0
285
100.0
150
99.7
71
100.2
36
100.1
30
99.9
23
99.9
16
100.2
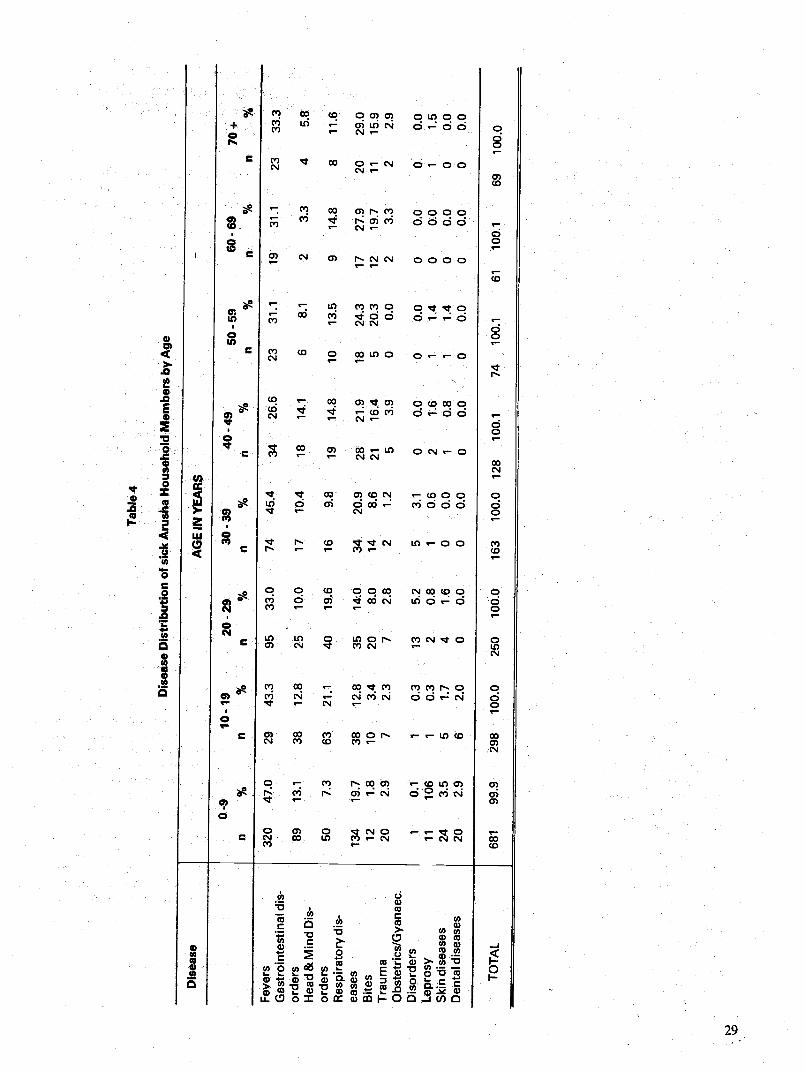
Tab
Ie4
Dis
ease
Dis
trib
utio
n of
sick
Aru
sha H
ouse
hold
Mem
bers
by A
ge
Dis
ease
A
GE
IN Y
EA
RS
0-9
10-1
9 20
-29
30-3
9 40
-49
50-5
9 60
-69
70+
%
n
%
n %
n
%
n %
n
Fev
ers
Gas
troi
ntes
tinal
dis-
or
ders
H
ead
& M
ind
Dis
- or
ders
R
espi
rato
ry di
s-
ease
s B
ites
Tra
uma
Obs
tetr
ics/
Gya
naec
. D
isor
ders
Le
pros
y S
kind
isea
ses
Den
tal d
isea
ses
320
47.0
29
43
.3
95
33.0
74
45
.4
34
26.6
23
31
.1
19
31.1
23
33
.3
89
13.1
38
12
.8
25
10.0
17
10
.4
18
14.1
6
8.1
2 3.
3 4
5.8
50
7.3
63
21.1
40
19
.6
16
9.8
19
14.8
10
13
.5
9 14
.8
8 11
.6
134
19.7
38
12
.8
35
14'0
34
20
.9
28
21.9
18
24
.3
17
27.9
20
29
.0
12
1.8
10
3.4
20
8.0
14
8.6
21
16.4
5
20.3
12
19
.7
11
15.9
20
2.
9 7
2.3
7 2.
8 2
1.2
5 3.
9 0
0.0
2 3.
3 2
2.9
1 0.
1 1
0.3
13
5.2
5 3.
1 0
00
0 0.
0 0
0.0
0 0.
0 11
10
6 1
0.3
2 0.
8 1
0.6
2 1.
6 1
1.4
0 0.
0 1
1.5
24
3.5
5 1.
7 4
1.6
0 0.
0 1
0.8
1 1.
4 0
0.0
0 0.
0 20
2.
9 6
2.0
0 0.
0 0
0.0
0 0.
0 0
0.0
0 0.
0 0
0.0
TO
TA
L 68
1 99
.9
298
100.
0 25
0 10
0.0
163
100.
0 12
8 .1
00.1
74
10
0.1
61
100.
1 69
10
0.0
by bad luck, devils, bewitchment and other forms of social discruption for which a traditional healer is normally con- sulted. This may be the reason for such low utilization for traditional healers in our study.
Modern health services are costly compared to tradi- itional health services mainly due to the sophistication of the facilities used Governments are therefore unable to afford this type of service for the majority of itjs people. For this reason traditional healers should be encouraged after care- ful assessment of their therapeutic procedures to see which are not likely to be harmful and therefore to be deployed. Traditional birth attendants for example, can be taught to treat or refer some gynaecological and obstetrical conditions in addition to attending deliveries.
In summary of the pattern of diseases in Iringa and Arusha regions resembles that of the causes for admission and out-patient attendances in Tanzania in general. The majority of the household members sought health caie from traditional health system, Iringa utilized them more than Arusha. The explanations given for such utilization pattern are found to be due to differences in disease pattern and to the types of illhealth for which people normally consulttrad- itional healers. l is therefore, suggested that further studies should be carried out to determine the pattern of diseases for which traditional healers are normally consulted. This would require detailed interviews of key informants in the commu- nity.
References:
1. Attorney General, Tanzania. Medical Practitioners and Dentists Ordinance Special Supplement No. 1 Cap. 409, section 37; Dares Salaam, 1968.
2. 1978 National Population Census. Volume II. Population by Age and Sex for villages/wards and Urban Areas Bureau of Statistics, Ministry of Planning and Economic Affairs,DaresSalaam,1981.
3. Planning Unit Tanzania Ministry of Health Tanzania Health Sector Strastegy. Ed. Albert E. Hen. Health Nutri- tion and Population Office, USAID/Tanzania, 1980.
4. Slikkerveer U. Rural Helith Development in Ethiopia: Problems of Utilization of Traditional Healers. Soc. 3d. Med. 1982; 16: 1859- 72.
5. Ulin PR. The Traditional Healer of Botswana in a Chang- ing Society. In: Traditional Healers: Use and Non-use in Health Care Delivery. Eds. Harrison IE, Dunlop DW. East
Lansing, Michigan: Michigan State.University, The Afri- can studies Centre, Rural Africana No. 26, 1974: 123-30.
6. Janzen JM. Pluralistic Legitimation of therapy system in contemporary Zaire. In: Traditional Healers: Use-and Non—use in Health Care Delivery. Eds.: Harrison IE, Dun- lop DW. East Lansing, Michigan: Michigan State Univer- sity, The African Studies Centre Rural Africana No. 26, 1974: 105-22.
7. Maclean CMU. Magical medicine. A nigerian Case Study. London. Allan Lane, 1961.
8. Press l.Urban Illness. Physicians, cures and Dual Use.
Bogota Journal of Health and Social Behaviour 1969; 10. 209-18.
9. Schwartz LR. The Hierarchy of Resort in Curative Prac- tices: The Admirality Islands, Melanesia Journal of Health and Social Behaviour, 1969; 10: 20 1-9.
10. Twamasi PA. Scientific Medicine: The Ghanaian Experi- ence. Internantional Journal of Nursing 1972; 9: 63-75.
30
THE IMPACT OF TRADITIONAL HEALTH BELIEFS AND PRACTICES ON
HEALTH CARE UTILIZATION PATIERNS
Abstract By J.K. Nguma
This paper argues that traditional health beliefs and practices greatly influence peoples' decisions to seek health care and the nature of health care sought. Long after the introduction of Western medicine in developing countries, traditional healers continue to have a key role in the provi- sion of health care among many communities. It is proposed that in the efforts to ensure "health for all by the year 2000", health planners in the developing countries should examine the role of traditional healers and explore possibilities of integrating them in the health care delivery system.
Introduction
The discovering of the "germ theory" in Europe in the 19th century laid a great foundation for what is now known as "Western Medicine". Armed with the "germ theory" Western medicine gained ground and the new medicinal profession that ensured started to claim monopoly in health care delivery over traditional homeopathic and herbal heal-' ers. These new developments set off some competitions for patients between physicians trained in the new scientific medicine and the traditional healers1. These competitions have been and still are part and parcel of health care deliveries in both developed and underveloped countries.
This paper argues that even with the introduction of new Western medicine in a developing countries, the health care provided by traditional healers is still widely used due to the influence of traditional health beliefs. It is proposed that in the efforts to ensure "health for all by the year 2000", developing countries should not lose sight of the key role played by traditional healers in the provision of health care and that possibilities of integrating these practitioners into the official health care system should be explored.
Traditional Beliefs About Disease Causation
Traditionally, health care responsibilities in most developing countries (Asia, Africa, South America and Latin America) are placed upon the patient's family and his kin. Usuallywhen an individual falls sick, the family members get together and embark on the search for causes of such sick- ness and its eventual treatment. This exercise is simple since the culture of each community has specific belief about dis- ease causation, and the family's role in the diagnosis process is to identify the kind of etiological pattern the symptoms appear to follow.
Various studies have addressed the subject of disease causation or disease etiology2'3'4' 5 Clements2 classified dis-, ease etiologies into three patterns according to peoples' beliefs. Foster5, on the other hand, classifies belief boui dis- ease causation into two categories. Both authors appear to
J.K. Ngurna, Lecture Department of Behavi oural Sciences, P.O. Box 65015 Dares SaIam.
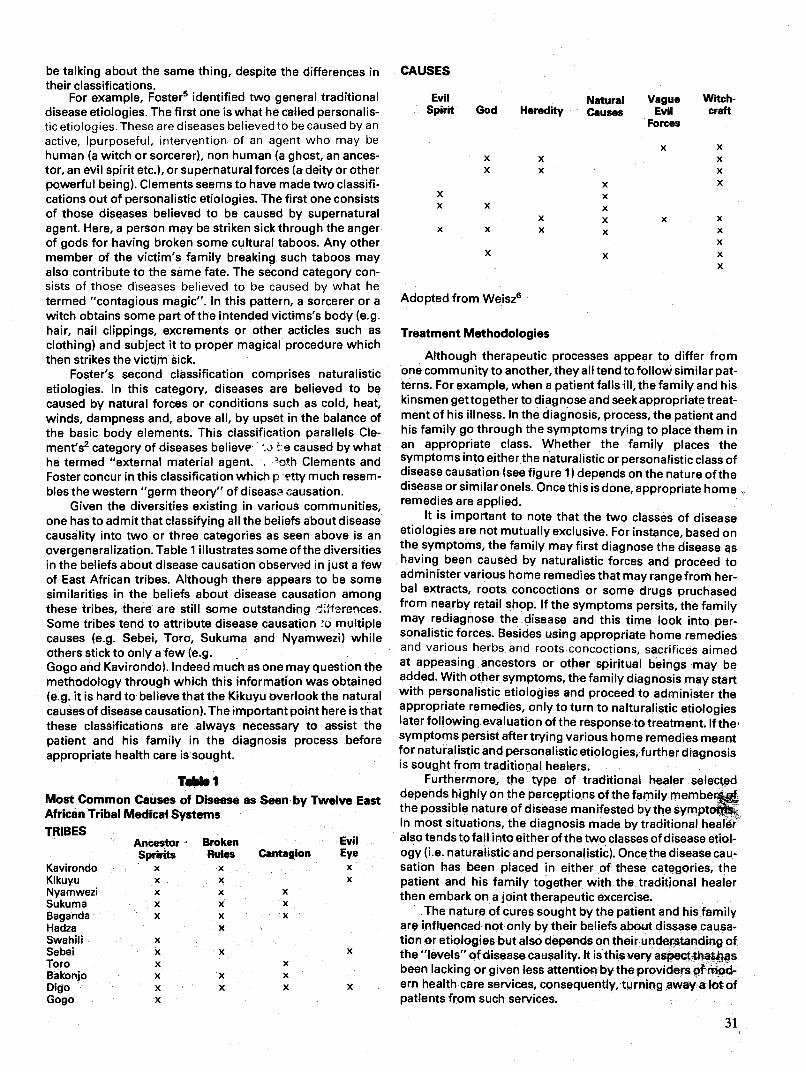
be talking about the same thing, despite the differences in CAUSES their classifications.
For example, Foster5 identified two general traditional Evil disease etiologies. The first one is what he called personalis- SPirit tic etiologies. These are diseases believed to be caused by an
active, purposeful, intervention of an agent who may be human (a witch or sorcerer), non human (a ghost, an ances- tor, an evil spirit etc.), or supernatural forces (a deity or other powerful being). Clements seems to have made two classifi- cations out of personalistic etiologies. The first one consists X
of those diseases believed to be caused by supernatural agent. Here, a person may be striken sick through the anger of gods for having broken some cultural taboos. Any other member of the victim's family breaking such taboos may also contribute to the same fate. The second category con- sists of those diseases believed to be caused by what he termed "contagious magic". In this pattern, a sorcerer or a witch obtains some part of the intended victims's body (e.g. hair, nail clippings, excrements or other acticles such as
clothing) and subject it to proper magical procedure which then strikes the victim sick.
Foster's second classification comprises naturalistic etiologies. In this category, diseases are believed to be caused by natural forces or conditions such as cold, heat, winds, dampness and, above all, by upset in the balance of the basic body elements. This classification parallels Cle- ment's2 category of diseases believe i !::e caused by what he termed "external material agent.. . 'oth Clements and Foster concur in this classification which p E'tty much resem- bles the western "germ theory" of diseast causation.
Given the diversities existing in various communities, one has to admit that classifying all the beliefs about disease causality into two or three categories as seen above is an overgeneralization. Table 1 illustrates some of the diversities in the beliefs about disease causation observed in just a few of East African tribes. Although there appears to be some similarities in the beliefs about disease causation among these tribes, there are still some outstanding ftf'are'ices. Some tribes tend to attribute disease causation o multiple causes (e.g. Sebei, Toro, Sukuma and Nyamwezi) while others stick to only a few (e.g. Gogo and Kavirondo). Indeed much as one may question the methodology through which this information was obtained (e.g. it is hard to believe that the Kikuyu overlook the natural causes of disease causation). The important point here is that these classifications are always necessary to assist the patient and his family in the diagnosis process before appropriate health care is sought.
Ta&s I Most Common Causes of Disease as Seen by Twelve East African Tribal Medical Systems TRIBES
Ancestor Broken Sprints Rules Cantagion
Kavirondo Kikuyu Nyamwezi Sukuma Baganda Hadza Swahili Sebel Toro Bakonjo Digo Gogo
Although therapeutic processes appear to differ from one community to another, they alitend to follow similar pat- terns. For example, when a patient falls ill, the family and his kinsmen gettogether to diagnose and seek appropriate treat- ment of his illness. In the diagnosis, process, the patient and his family go through the symptoms trying to place them in an appropriate class. Whether the family places the symptoms into either the naturalistic or personalistic class of disease causation (see figure 1) depends on the nature of the disease or similar onels. Once this is done, appropriate home remedies are applied.
It is important to note that the two classes of disease etiologies are not mutually exclusive. For instance, based on the symptoms, the family may first diagnose the disease as having been caused by naturalistic forces and proceed to administer various home remedies that may range from her- bal extracts, roots concoctions or some drugs pruchased from nearby retail shop. If the symptoms persits, the family may rediagnose the disease and this time look into per- sonalistic forces. Besides using appropriate home remedies and various herbs and roots concoctions, sacrifices aimed at appeasing ancestors or other spiritual beings may be added. With other symptoms, the family diagnosis may start with personalistic etiologies and proceed to administer the appropriate remedies, only to turn to nalturalistic etiologies laterfollowing evaluation of the response to treatment. If the symptoms persist after trying various home remedies meant for naturalistic and personalistic etiologies, further diagnosis is sought from traditional healers.
Furthermore, the type of traditional healer selected depends highly on the perceptions of the family member&o the possible nature of disease manifested by the symptofl'l. In most situations, the diagnosis made by traditional healer
Evil also tends to fall into either of the two classes of disease etiol- Eye ogy (i.e. naturalistic and personalistic). Once the disease cau- x sation has been placed in either of these categories, the x patient and his family together with the traditional healer
then embark on a joint therapeutic excercise. The nature of cures sought by the patient and his family
are influenced not only by their beliefs about dissase causa- tion or etiologies but also depends on their understanding of
X the "levels" of disease causality, It is this very aspect thathas been lacking or given less attention by the providers of mod- em health care services, consequently, turning away a lot of patients from such services.
31
Natural Vague Causes Evil
Forces
Witch- craft God Heredity
X x x x
x x x
x x x
Adopted from Weisz6
Treatment Methodologies
x x x x
x x x x x x x x x
x x x
x x
x x x x x
x x x x x x
x x x x x x x x x
x x
x x x x
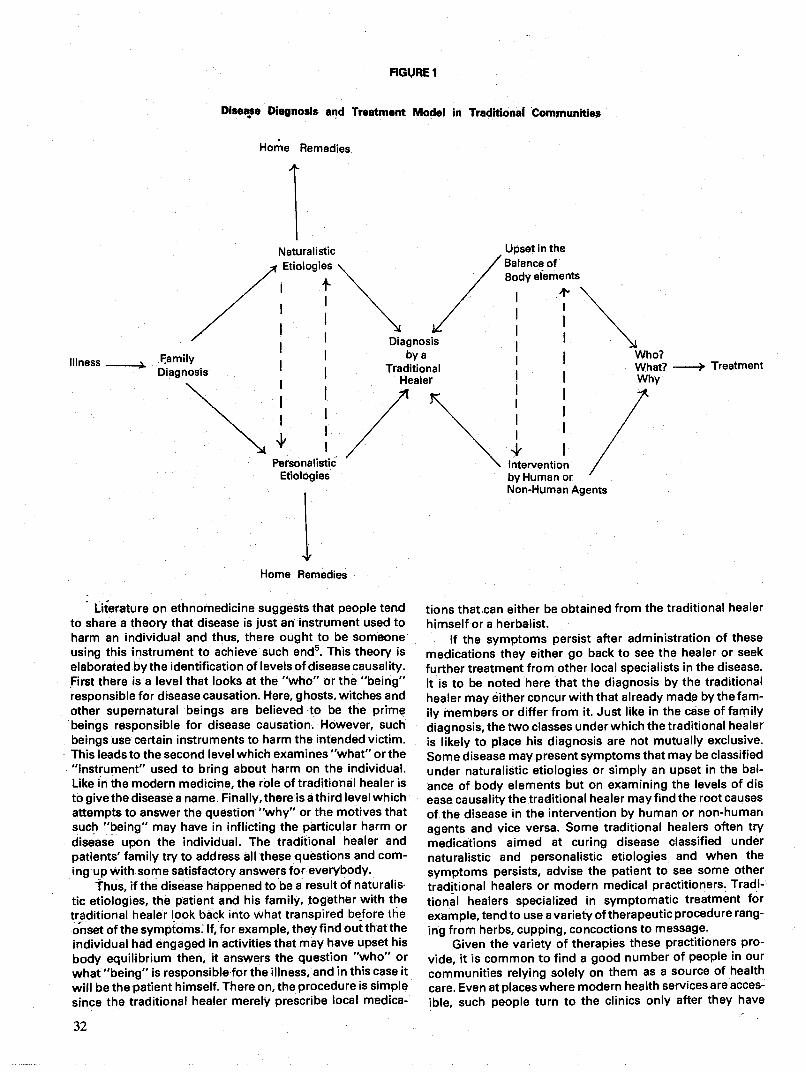
FIGURE 1
Disease Diagnosis and Treatment Model in Traditional Communities
Home Remedies
Home Remedies
Literature on ethnomedicine suggests that people tend to share a theory that disease is just an instrument used to harm an individual and thus, there ought to be someone using this instrument to achieve such end5. This theory is elaborated by the identification of levels of disease causality. First there is a level that looks at the "who" or the "being" responsible for disease causation. Here, ghosts. witches and other supernatural beings are believed to be the prime beings responsible for disease causation. However, such beings use certain instruments to harm the intended victim. This leads to the second level which examines "what" or the "instrument" used to bring about harm on the individual. Like in the modern medicine, the role of traditional healer is to give the disease a name. Finally, there is a third level which attempts to answer the question "why" or the motives that such "being may have in inflicting the particular harm or disease upon the individual. The traditional healer and patients' family try to address all these questions and com- ing up with some satisfactory answers for everybody
Thus, if the disease happened to be a result of naturalis tic etiologies, the patient and his family, together with the traditional healer look back into what transpired before the onset of the symptoms. If, for example, they find out that the individual had engaged in activities that may have upset his
body equilibrium then, it answers the question "who" or what "being" is responsiblefor the illness, and in this case it will be the patient himself. There on, the procedure is simple since the traditional healer merely prescribe local medica-
32
4' I Intervention by Human or Non-Human Agents
tions that can either be obtained from the traditional healer himself or a herbalist.
If the symptoms persist after administration of these medications they either go back to see the healer or seek further treatment from other local specialists in the disease. It is to be noted here that the diagnosis by the traditional healer may either concur with that already made by the fam- ily members or differ from it. Just like in the case of family diagnosis, the two classes under which the traditional healer is likely to place his diagnosis are not mutually exclusive. Some disease may present symptoms that may be classified under naturalistic etiologies or simply an upset in the bal- ance of body elements but on examining the levels of dis ease causality the traditional healer may find the root causes of the disease in the intervention by human or non-human agents and vice versa. Some traditional healers often try medications aimed at curing disease classified under naturalistic and personalistic etiologies and when the
symptoms persists, advise the patient to see some other traditional healers or modern medical practitioners. Tradi- tional healers specialized in symptomatic treatment for example, tend to use a variety of therapeutic procedure rang- ing from herbs, cupping, concoctions to message.
Given the variety of therapies these practitioners pro- vide, it is common to find a good number of people in our communities relying solely on them as a source of health care. Even at places where modern health services are acces-
ible, such people turn to the clinics only after they have
Illness _______
Naturalistic Upset in the
,//// \\ //eents I Diagnosis
_____ F.amily I bya Diagnosis I
I Traditional
Healer
Personalistic Etiologies
- Treatment
I

administered a variety of home remedies and at times use both services simultaneously.
Personalist etiologies with multiple levels of causation require more sophisticated therapies. Logically, such dis- ease require the shaman with supernatural and/or magical skills or other traditional healers who then address the main concerns of the patient and his family. In the majority of casesthe patient and his family are more concerned not with the "instrument" or the immediate cause of illness but rather with "who" and "why'. However, even here, one:finds some variations in what the individuals are more interested to know For example, Jansen7 had this to say about the Xhosa: "They are less interested to know: Howdid it happen? rather than Who is responsible". On the other hand lmperato8 had a different observation among the Bambara: "In general, they want to know whythey are ill and not howthey got ill".
Once the "who", the "what" and the "why" of disease causation are known, the individual is advised accordingly to seek appropriate treatment for the immediate problem. Treatment modalities as seen in figure 1 vary, but highly depend on the beliefs of disease causation.
For example, diseases believed to be caused by a sor- cerer or a witch may be treated by a traditional healer who first of all identifies the "being" involved and then treat the immediate problem. At times, he may go as far as providing the patient with protective medicines against similar harm in the future. Illness diagnosed as having been brought about by supernatural agency on the other hand may be cured through processes which usually require some sacrifices. The exercise involves manipulation of various symbols ger- mane to patient's culture during such sacrifices.
Doctor — Patient Relationship
The discussions in the'foregoing two sections paint a picture of what happens once an individual falls ill the diag nosis made and the nature of medical therapy sought once the disease is placed in its appropriate classification.
Indeed, what is striking is that even now in the 20th cen- tury when the western health services are accessible to many people still peoples beliefs about disease causation appear to be a prime factor in their decisions to seek health care and the nature of health care they seek. In the Tanzanian situation, the past experience indicates that accessibility to modern health care services has been the major reason for low or non utilization of such services Today there is at least one clinic in the nearby if not in every village Yet a good number of our people are still stuck up with traditional heal ers and only go to the clinic as a last resort after trying van ous traditional cures
Quite often the argument has been thatthese people are
lacking in health education and thus do not understand the effectiveness of the services provided by modern medicine Even more seriously it is alleged that they are too hung up in their traditional health beliefs and practices Much as one may not object to the role of health education in human attitude and behaviour change, one would hesitate to assume that such changes can be achieved overnight. Further, and understanding'and perhaps an appreciation of modern health services in itself is not enough to attract people to seek such services.
For example the organization of modern heaith services and the manner in which such services are provided leaves a lot to be desired. As mentioned earlier, the key interest of the
patient and his family in the therapeutic process is not
merely to cure the illness but to have abroad understanding of "who" is responsible for such illness and "why". Tradi- tional healers are very much aware of such expectations and do all their best to provide such information to their clients in a plain and understandable language. As for modern health care services, the existing imbalance in the doctor — patient ratio in most developing countries, make it difficult for doc- tors to spend as much time with each patient to address all the burningconcerns the patients may have. This shortcom- ing, when coupled with other inconviniences experienced by patients suchas longwalks from their home to the clinic, the long queues they have to go through before they finally see the physician, not to mention other extreme situations where they may not get any medication even after seeing the physi- cian, makes future decisions for clinic attendance unapalata- ble. Todate, in place where there is good accessibility to modern health services such as in towns and cities, there are still people who choose traditional healers over modern physicians.
The decision to seek modern health services becomes even more difficult when there are possibilities of the patient being hospitalized Hospitalization is an anxiety arising experience not only for the patient but also for the family members and relatives. To start with, the patient is isolated from his family and kinship members, and attended by unfamiliar faces, a situation which makes him feel betrayed by his kinsmen. Secondly, the family members are not involved in the diagnosis and treatment of the patient which makes them less helpful to the patient during the recovery process after discharge from hospital. Thirdly, the patient himself is not provided with adequate information (if any) about his diases and at times he is not informed about what is being done to him and why. It is common therefore, for a patient to find himself surrounded by a number of health pro- viders who only talk about him and not to him. This in no doubt makes the patient alienated, demoralized and anx- ious.9
The relaxed atmosphere and pe'rsonal interest tradi- tional healers take in the patient's total life-style, his relation- ships with others, his gender, as well as his moral and spiritual convictions, enhances patient's pride and feeling of self-worth.
Conclusion
The long history of traditional healers is too informative to be ignored. Although ineffective insome disease; the kind of care the tadition healers have been providing has earned them a lot of popularity. There is no doubt that modern health providers have a lot to learn from these practitioners
'and vice versa. While the traditional health beliefs and prac- tices cherIshed by their clients constitute the prime factor for the success of traditional healers, the emphasis these heal- ers place on the doctor — patient relationship and their awareness of the role of cultural and emotional aspects on physical disorders appears to have a great contribution towards their popularity.
The reality to be reckoned with here is that the traditional healers have been, and will still be working alongside the modern physician, treating more or less the same clients. It is critical therefore, for the health planners to examine the vari- ous activities of traditional healers so as to determine the kind of contributions they will have in the primary health care program. As it has been suggested by others1° health plan- ners should determine the numbers and location of these
33

practitioners, the diagnostic and therapeutic methods they employ, as well as their role in their respective communites. Based on this information, those practitioners who will be deemed as suitable for integration into the official health care system will further be assessed to determine the kind of orientation they have had, if any, and what type of training they may need to improve their services.
Given their already accepted role in their respective communities, the provision of basic orientation to these practitioners together with adequate supervision will greatly enhance the general health care provision in their com- munities. Further, with adequate orientation, traditional healers can be ubed to spearhead some of the basic health programs in our communities such as sanitation, immuniza- tion, nutrition and child survival and development.
References 1. Brown ER, Rockefeller Medicine Man. University of
California Press Berkeley, 1949. 2. Clements EF. Primitive Concepts of Disease. University
of California Press Berktey—.- California, 1973. 3. Weatherby JN. Sebei conceptions of health and dis-
ease. One day symposium on Attitudes to Health and Disease among some East African Tribes Makerere Institute of Social Research Study D, 1959.
4. Orley J. Epilepsy among the Baganda. Department of Psychiatry, Makerere University, mimeo 1968.
5. Foster MG. Disease Etiologies in Non-Western Medical System. Amer. Anthr. 1976; 78: 773-82.
6. Weizz JR. East African Medical Attitude. Soc. Sci. Med. 1972; 6.
7. Jansen G. The Doctor Patient Relationship in an Afri can Tribal Society. Assen. The Netherlands: Van Gor- cum. 1973.
8. Imperato PJ. Traditional Medical Practitioners among the Bambora of Mali and their role in the Modern Health Care Delivery System. In Traditional Healers: Use and Non-use of Health Care Delivery. Harrison IE, Dunlop DW, Eds. Rural African 1974; 26: 41-53.
9. Tag liacozzo LD; Mackch DH. The Patient's view of the Patient's Role. In: Jaco GE. Patients, Physicians and Ill- ness. The Free Press, New York 1 972.p. 162-75.
10. Bannerman HR et al. Traditional Medicine and Health Care Coverage WHO Geneva, 1983.
br. B. Sibanda and Dr. T.E.C. Harvey on CollaboratIon of Allopathic Orthodox Medical Practice with Traditional Heal- ing Methods in Zimbabwe.
Zimbabwe is one African country where specific moves have been made towards the intergration of modern and traditional medicine. One such move is the establishment in Bulawayo of the Zimbabwe Traditional and Medical Clinic.
The conference was attended by a delegation of two per- Sons Dr. Sibanda and Dr. Harvey from the Zimbabwe Tradi- tional and Medical Clinic who had the opportunity to brief the participants about the centre and its activities.
Dr. B. Sibanda and Dr. T.E.C. Harvey, Zimbabwe Traditional and Medical Clinic, Bulawayo.
34
Zimbabwe Traditional and Medical Clinic offers both traditional and modern medical care. A patient coming to the Centre has the option of chosing between the two forms of medical care which are available under one roof. Besides the initial choice which the patient can make the practitioners of one form of medical practice may refer the patient to prac- titioners of the other form of medical practice.
In her presentation Dr. Sibanda made the point that te clinic allows not only for treating illnesses with which people present but also for identifying and dealing with any social- psychological factors associated with such illnesses. Prac- titioners at the Centre strive to treat the whole person and not only that part of the body which is diseased. Their joint prac- tice and medicines in effect deal not only with the physical or biological diseases but also with the mental, spiritual and social aspects of the disease situation.
Dr. Harvey, himself a modern medical doctor, reported that he sends to traditional healers patients that he cannot cure. Many of these tend to have psychosomatic disorders. He claimed that the approach used by traditional healers in dealing with such disorders is much more dynamic, that tranquillisers are not used, and that an explanation astowhy a disorder is present is offered in terms which the sufferers understand. Furthemore traditional healers may prescribe ablation, prayers and rituals bpsides performing some form of hypnotherapy as well as giving herbal concoction to drink, including for-bidding the sufferers to do certain things. All this the patients understand and fits in with the background to their social and cultural life. He contrasts this to the approach of modern doctors who in their ignorance often claim that what the traditional healers practice is black magic, voodoo rites or witchcraft. Dr. Harvey admitted how- ever that not all traditional healers are of the same calibre as the one he has worked with and come to trust. He also indi- cated that psychosomatic disorders are not the only types of illnesses which he refers to traditional healers.
Address of Dr Stephen Moses Regional Representative for Eastern and Southern Africa, Health Sciences Division, IDRC. to the International Conference on Traditional Medicine, Arusha 6-8 October 1986
The involvement of the International Development Research Centre (IDRC), Canada, in supporting research in the field of traditional medicine began in the early 1970s in Zaire. Research was conducted by the "Department del "En- seignement superieur et de Ia Recherche scientifique" of the Republic of Zaire, and resulted in a publication entitled "Traditional Medicine in Zaire: President and Potential Con- tribution to the Health Services" (IDRC-137e). This work was followed by research projects on traditional medicine and traditional birth attendants in Egypt, Ecuador, Nepal, Thai- land and the Phillippines. Currently, research in this field is being sponsored by IDRC in the Philippines, Sudan, Tan- zania, Kenya and Zimbabwe. Thus IDRC has been part of the
Dr. S. Moses, - Regional Representative for Eastern and Southern Africa, Health Sciences Division IDRC.

process which has led traditional medicine as a legitimate, and indeed crucial, element in primary health care.
I am very pleased that IDRC has had the opportunity to be involved in this important conference on traditional medicine, and that I have been able to attend. I would like to congratulate Mr. Mshiu and his colleagues in the Traditional Medicine Research Unit of the University of Dar es Salaam for their superb organizational work and their initiative in putting the conference together.
I would also like to congratulate the investigators from the University of Dar es Salaam on the quality of their research, with respectto both the IDRC-supported project on traditional medicine and other studies conducted by scien- tists in the Department of Behavioural Science, Community Medicine, Epidemiology and Biostatistics, and other depart- ments. Participants from outside Tanzania have in addition made extremely important contributions regarding issues in traditional medicine globally, and in particular in Kenya, Uganda, Zimbabwe, Nigeria and Zaire.
The many papers presented atthe conference have been interesting, provocative and controversial. Extremely impor- tant concepts have been introduced and discussed. Perhaps more questions have been raised than answers provided but this is not, I feel, a cause for concern. Debate on traditional medicFne internationally, .and particularly in Africa, is still in its early stages, and if we subscribe to Murray Last's analysis, will continue for some time, perhaps well beyond the year 2,000. Much work remains to be done, but I think you will all agree that much has already been accomplished.
Although in a sense this conference marks the end of three years of research in Tanzania, I see it as signifying a beginning more than an ending. In the first instance, I expect that several publications will emerge from the Tanzanian research, in both local and international bra. In addition, the Proceedings of this Conference will likeW be published as a special issue of the Tanzania Medical Journal. It is clear, how- ever, that more research is needed, and the issuesidentified so clearly by Dr. Akerele in his paper must be addressed over the coming years. IDRC, the World Health Organization, and many other internantional agencies, governments, academic institutions, and non-governmental agencies will assist in this process.
In the final analysis, however, it is of course action which is required, and we know that the link between research and action can be problematic. The people in this room will be involved in making that link, and working with colleagues, with traditional practitioners, and with communities to this end. The real challenge in the years ahead, then, is to "make it happen," i.e., to ensure that traditional medicine occupies its rightful place in the delivery of health services and in the improvemnt of the health and well-being of people, which is the chief concern of us all. Thank you very much, Mr. Chair- man, for allowing me this opportunity to address the confer- ence.
35
ARCHIV Proceedirgs of the Intern 615.89618) I 5 1986
c.1 18729
1032 15
Typeset and Printed by Inter Press of Tanzania Ltd. P.O. Box 6130, DAR ES SALAAM.