solving a routing problem
TRANSCRIPT

Psychological Bulletin1990, Vol. 108, No. 1,77-92
Copyright 1990 by the American Psychological Association, Inc.0033-2909/90/$00.75
Is Eye Movement Dysfunction a Biological Marker for Schizophrenia?A Methodological Review
Brett A. Clementz and John A. SweeneyLaboratory of Clinical Psychophysiology, New York Hospital-Cornell Medical Center
There is a high prevalence of eye movement dysfunction (EMD) in persons with schizophrenia andtheir first-degree relatives. Studies addressing the prevalence, stability, familial transmission, andpsychological correlates of EMD in persons from both psychiatric and general populations offersuggestive evidence that this abnormality may serve as a biological marker for schizophrenia. Al-though these findings are promising, their significance for elucidating the diagnostic bandwidth,pathophysiology, and genetics of this disorder remains to be determined. More precise characteriza-tion of ocular motility, perhaps when used in conjunction with global measures of pursuit adequacy,may be essential for clarifying the pathophysiological and genetic significance of EMD for schizo-phrenia. Recent research efforts are beginning to identify particular abnormalities that could serveas more specific biological markers for schizophrenia.
Eye movement dysfunction (EMD) has been reported to beone of the most promising biological markers for schizophrenia(Holzman, 1975, 1985, 1987; lacono, 1983, 1985, 1988; Lip-ton, Levy, Holzman, & Levin, 1983). Diefendorf and Dodge(1908) conducted the seminal investigation of ocular motilityin psychiatric patients. Although their "immediate interest cen-tred in patients suffering from maniacal-depressive insanity"(p. 458), they reported that "the most marked variations arefound in the pendulum pursuit-movements in dementia prae-cox, where a marked hesitation to fall into the swing of the pen-dulum was found even in the mildest cases" (p. 468). They fur-ther stated, "while this peculiarity is apparently not restrictedto dementia praecox, it was found in other patients only wherethe disease process has produced marked deterioration"(p. 468).
Couch and Fox (1934) attempted to replicate the Diefendorfand Dodge (1908) results with limited success:
Steplike interruptions of pendular pursuit appears in the recordsof 27 patients, including 14 of 43 with dementia praecox. "Step-ping" was thought by Diefendorf and Dodge to be typical of thisdisease. This has not proved true in our series . . . many otherpatients revealed the same defect, (p. 565)
Some of the patients in the Couch and Fox study were receiving
Funds from the Scottish Rite Schizophrenia Research Program andU.S. Public Health Service Grant MH42969 supported work on thisproject.
Thanks go to Lisa Dixon, Allen Frances, Irving I. Gottesman,Gretchen Haas, Michael Hirt, Phillip Holzman, Elizabeth Chernoff,and three anonymous reviewers for critiquing earlier versions of thisarticle. Their suggestions and comments improved the quality of thefinal product. Darryl Blanck assisted with the literature review.
Correspondence concerning this article should be addressed to BrettA. Clementz, who is now at 481 Elliott Hall, Department of Psychology,University of Minnesota, 75 East River Road, Minneapolis, Minnesota55455.
sodium amytal, a drug that disrupts some aspects of ocular mo-tility. It appears that some patients from all diagnostic groupshad received this medication, making it difficult to attribute thisreplication failure to differential medication effects alone.White (1938) conducted another attempted replication of Die-fendorf and Dodge's report, but he was also unimpressed withthe differences between the ocular motility of "mentally dis-eased" and normal individuals.
Although Kraepelin (1919/1971, p. 6) had mentioned the po-tential significance of Diefendorf and Dodge's (1908) finding,not until a study by Holzman, Proctor, and Hughes (1973) wasthis interesting area of investigation further pursued. The Holz-man et al. study, along with numerous other reports (Bartfai,Levander, & Sedvall, 1983; Blackwood, St. Clair, & Muir, 1988;Cegalis & Sweeney, 1979, 1981; Holzman, Levy, & Proctor,1976; Holzman et al., 1974; lacono, Peloquin, Lumry, Valen-tine, & Tuason, 1982; lacono, Tuason, & Johnson, 1981;Kuechenmeister, Linton, Mueller, & White, 1977; Kufferle,Grunberger, Linzmayer, & Saletu, 1988; May, 1979; Mialet &Pichot, 1981; Pass, Salzman, Klorman, Kaskey, & Klein, 1978;Rea, Sweeney, Solomon, Walsh, & Frances, 1989; Scarone,Gambini, Hafele, Bellodi, & Smeraldi, 1987; Shagass, Amadeo,& Overton, 1974; Shagass, Roemer, & Amadeo, 1976; Spohn,Coyne, & Spray, 1988), demonstrated that persons with schizo-phrenia have less accurate smooth pursuit eye movements thannormal persons and nonpsychotic (personality-disordered andunipolar-depressive-disordered) patients. Some studies, how-ever, have failed to find a significant difference between accu-racy of smooth pursuit in persons with schizophrenia and inother groups, especially patients with bipolar affective disorder(Holzman, Solomon, Levin, & Waternaux, 1984; lacono &Koenig, 1983; lacono et al., 1982; Klein, Salzman, Jones, &Ritzier, 1976; Levin, Lipton, & Holzman, 1981; Lipton, Levin,& Holzman, 1980; Pivik, 1979a, 1979b; Salzman, Klein, &Strauss, 1978; Solomon, Holzman, Levin, & Gale, 1987).
Since Diefendorf and Dodge's (1908) and Holzman's (Holz-man et al., 1973) initial publications on EMD in schizophrenia,
77

78 BRETT A. CLEMENTZ AND JOHN A. SWEENEY
both psychopathology (Acker & Toone, 1978; Brezinova & Ken-dell, 1977; Couch & Fox, 1934; Klein etal., 1976;Pivik, 1979a,1979b; Salzman et al., 1978; White, 1938) and oculomotor(Abel, 1986; Abel &Hertle, 1988; Abel &Ziegler, 1988;Troost,Daroff, & Dell'Osso, 1974; Weinreb, 1983; Yee et al., 1987)researchers have questioned the validity of the EMD-schizo-phrenia association. Two of the most potentially obfuscatingfactors in this literature relate to the use of global as opposed tospecific measures of ocular motility (Abel, 1986; Abel & Hertle,1988; Abel & Ziegler, 1988; Troost et al., 1974; Whicker, Abel,& Dell'Osso, 1985) and variable methods of subject selectionin studies of HMD in schizophrenia. This article addresses theseconcerns by asking two questions: (a) What methodological fac-tors might enhance the study of EMD in psychiatric patients?and (b) given the existing data, does EMD qualify as a biologicalmarker for schizophrenia?
The second question cannot be adequately answered untilmethodology is given fair consideration. The potential biologi-cal marker status of EMD is addressed after we explore some ofthe most important methodological issues, including (a) assess-ment of eye movement protocols, (b) eye movement recording,and (c) stimulus characteristics. Understanding eye movementrecording and measurement requires first acquiring a basicknowledge of the oculomotor system.
Oculomotor System
The neural pathways for control of eye movements traversethe higher cortical centers (frontal eye fields and parietal lobes),through the basal ganglia and superior colliculus, to the vestibu-lar system, medial longitudinal fasciculus, cerebellum, andparamedian pontine reticular formation. Because of the lownerve-to-muscle ratio (approximately 1:1), the oculomotor sys-tem is extremely sensitive to toxic, neuroanatomic, and neuro-chemical insult. This system has relatively clearly delineatedneuroanatomic pathways, and insult to particular brain areasleads to unique eye movement patterns. As a result, a detailedneuro-ophthalmological assessment is helpful for the differen-tial diagnosis and localization of many encephalopathies (e.g.,cerebellar ataxia, Parkinson's disease, progressive supranuclearpalsy, Huntington's disease, Wilson's disease, and multiple scle-rosis; see Kuskowski, 1988, for a review).
There are six functional eye movement classes: vestibular, op-tokinetic, smooth pursuit, nystagmus quick phase, saccadic,and vergence (see Leigh & Zee, 1983, and Wirtschafter &Weingarden, 1988, for more complete coverage of this topic).These different oculomotor systems work in concert to allowredirection of the fovea to points of interest and are thereforeessential for accurate perception of the visual world. They canalso be functionally separated under experimental conditionsfor independent evaluation. The smooth pursuit and saccadicsystems have received the most specific attention from psycho-pathology researchers investigating EMD.
To ensure that smooth pursuit and saccadic functioning arebeing independently assessed, however, certain methodologicalprecautions should be taken. For instance, the vergence and ves-tibulo-optokinetic systems both interact with the smooth pur-suit and saccadic systems. To minimize interactions with thevergence system, targets could be maintained at a constant dis-
tance from subjects. To minimize vestibulo-optokinetic influ-ences, a subject's head could be firmly stabilized in head andchin restraint. These issues are rarely attended to in methodol-ogy sections of papers on EMD in schizophrenia. Because Ce-galis, Leen, and Solomon (1977) reported that persons withschizophrenia are more likely than normal persons to rely onhead movement in scanning the visual field, failure to use ahead restraint may be an especially serious confound in re-search on psychiatric patients.
Assessment of Eye Movement Protocols
Global Accuracy Measures
Benitez (1970) devised a scale for the qualitative scoring ofsmooth pursuit eye movement protocols. Cycles of pursuit ob-tained from subjects are compared with the four Benitezmodels and identified as either a or b (good) or cord (impaired)tracking. Shagass et al. (1974) devised a similar qualitative in-strument that extended the number of models to five.
Lindsey, Holzman, Haberman, and Yasillo (1978) and laconoand Lykken (1979b, 1979c) introduced "quantitative" proce-dures to complement the "qualitative" Benitez (1970) and Sha-gass et al. (1974) ratings. Lindsey et al. (1978) developed a mea-sure based on determining the amount of "noise" present in asubject's eye movement protocol and comparing this value withactual signal frequency [In (S/N)]. For instance, for targets trav-eling at 0.4 Hz, signal would be defined by this frequency,whereas noise (pursuit eye movements meaningfully differingfrom target frequency) would adopt some predetermined range,typically 1.2-12 Hz. lacono and Lykken (1979b, 1979c) devel-oped a mathematically related (Lykken, lacono, & Lykken,1981) measure based on calculation of root mean square(RMS) deviation between mean pursuit performance and thetarget wave form.
The Benitez-Shagass-type measures and the In (S/JV)-RMS-type measures are often referred to as qualitative and quantita-tive, respectively (Holzman, 1985, 1987; Lipton et al., 1983).The generic term global accuracy measures, however, seemsmore appropriate for two reasons. First, it has been reported(Lindsey et al., 1978; Siever, Coursey, Alterman, Buchsbaum,& Murphy, 1984) that these qualitative and quantitative mea-sures are highly correlated (rs = 0.82-0.86), suggesting signifi-cant redundancy. Subjects are reliably and similarly designatedas good or impaired trackers, using either scoring method(Levin, Lipton, & Holzman, 1981). On the basis of such find-ings, determination of the unique information brought to bearby these techniques is difficult. Specific measures of oculomotorfunctioning (e.g., pursuit gain, saccadic intrusions), on theother hand, correlate to substantially differing degrees withboth each other and RMS error deviation, suggesting that thereis something meaningfully different about the separate specificand global measures (see Clementz, in press, Appendix L, ms.pp. 217-220). Second, Abel and colleagues (Abel, 1986; Abel& Hertle, 1988; Abel & Ziegler, 1988; Kaufman & Abel, 1986;Whicker et al., 1985) have argued that a quantitative evaluationrequires differentiating among various possible eye movementabnormalities. Global accuracy measures are unable to meetthis requirement:

EMD IN SCHIZOPHRENIA 79
Of particular importance is the paucity of information that is re-ceived from the ln(S/N) ratio [and other like measures].. . . Thiswidely used measure, although free from dependence on the sub-jective perceptions of a panel of raters and quantitative in the sensethat it yields a numerical score for a given input, provides no infor-mation about what defects may be responsible for the generationof the score.. . . Although the global measures of pursuit qualityprovide an indication that a defect exists. . . it is only through theindividual analysis of whatever anomalies are present that we willcome to understand the relationship between psychiatric diseaseand ocular motility. (Abel & Ziegler, 1988, pp. 758-759)
The qualitative and quantitative measures were initial at-tempts to characterize and document oculomotor dysfunctionin the psychiatric literature. These global measures of pursuitadequacy have provided a wealth of information and somepromising leads that can be illuminated by subsequent re-search. Although useful for suggesting that an oculomotor ab-normality may exist in some persons with schizophrenia, thesemeasures will be unable to specifically describe the nature ofEMD in this subject population. This limitation may be par-tially responsible for some past failures to detect differences be-tween patients with schizophrenia and those with other psychi-atric disorders. The use of some system-specific, neuro-ophthal-mologically informed measures could be of utility in this regard(see Table 1). Future studies using both specific and global EMDmeasures with different subject populations will be able to ad-dress this hypothesis.
Specific Oculomotor Measures
Smooth pursuit system. The smooth pursuit system allowsfor the maintenance of slowly moving targets of interest on thefovea. Calculation of pursuit gain is the most useful laboratorymeasure of the pursuit system (Leigh & Zee, 1983; Wirtschafter& Weingarden, 1988). Pursuit gain is a measure of how accu-rately the eye is able to match target velocity during smoothpursuit, and is calculated as a ratio (eye velocity/target veloc-ity). Using a triangular wave (constant velocity) target allowsstraightforward calculation of this variable. When using a sinu-soidal waveform, defining gain for peak cycle velocities (peakeye velocity/peak target velocity) or using Fourier analysis is areasonable alternative (Yee et al., 1987). Medications, diseaseof the cerebellum, and dementia are among the common causesof low gain pursuit (Abel & Hertle, 1988; Kuskowski, 1988;Leigh & Zee, 1983; Wirtschafter & Weingarden, 1988).
Saccadic system. Saccades are the fastest eye movements,enabling rapid shift of gaze and foveation of interesting targets.They are ballistically preprogrammed and have approximatelya 200-msec initiation delay. There is an invariant exponentialrelation between peak velocity and amplitude (termed the"main sequence;" Bahill, Clark, & Stark, 1975) that can beused as one approach for assessing the integrity of the saccadesystem.
Disorders of saccades can be subdivided into those of velocity,accuracy, initiation, and inappropriate (intrusive) movements(Leigh & Zee, 1983). Saccadic movements that lie off the "mainsequence" characteristically indicate a mismatch between thenormally invariant peak velocity-amplitude relation. Saccadesmay also be dysmetric or demonstrate increased initiation la-tency. Inappropriate or intrusive saccadic movements occur ei-
Table 1Specific Measures of the Oculomotor System
Eye movement systemand measure Calculation
Smooth pursuitPursuit gain
Saccadic"Main sequence"
Accuracy
Reaction time
Intrusive events
(Eye velocity/target velocity) (Leigh &Zee, 1983)
Peak velocity-amplitude and peakvelocity-duration functions (Bahill etal., 1975)
Saccade amplitude/amplitude of stimulusmovement (Leigh & Zee, 1983)
Latency of response to saccade generation(Leigh & Zee, 1983)
Frequency of occurrence of square wavejerks, ocular flutter, macrosaccadicoscillations, macrosquare wave jerks,and anticipatory saccades (Abel &Ziegler, 1988;Dell'Ossoetal., 1977;Leigh & Zee, 1983)
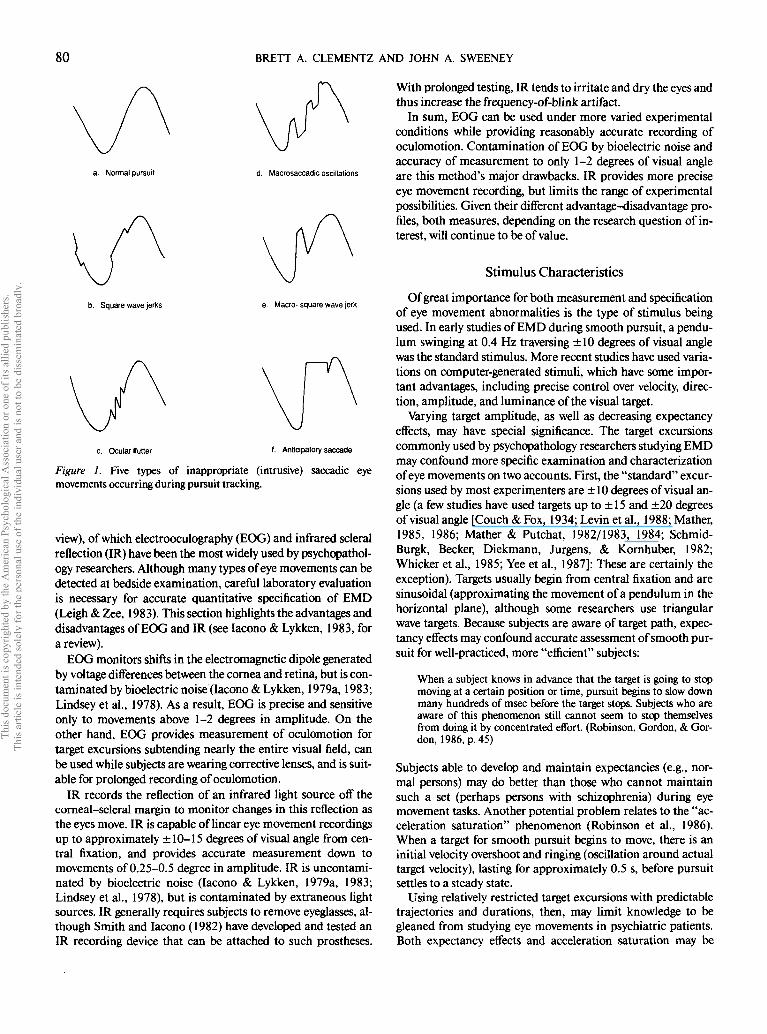
ther during fixation or smooth pursuit, and are of five maintypes (see Figure 1). Square wave jerks (SWJ), or saccadic intru-sions (Levin, Jones, Stark, Merrin, & Holzman, 1982a), arepairs of saccades of from 0.5 to usually 3 (although sometimesup to 5) degrees in amplitude, with an intersaccadic intervalof approximately 200-500 msec. Pursuit generally continuesparafoveally between the saccadic movements. SWJ are perhapsthe most nonspecific oculomotor sign of neurologic abnormal-ity (Leigh & Zee, 1983; Weinreb, 1983). Ocular flutter consistsof back-to-back saccades of approximately 5-10 degrees in am-plitude without an intersaccadic interval, and is usually attrib-uted to cerebellar or brain stem dysfunction (Kuskowski, 1988;Leigh & Zee, 1983). Macrosaccadic oscillations are greater than10-degree saccades made about target position separated byseveral hundred milliseconds, and reflect an inability to gener-ate saccades small enough to bring the target onto the fovea(Dell'Osso, Abel, & Daroff, 1977; Leigh & Zee, 1983). Macro-SWJ are large (10- to 40-degree) pairs of saccades with a rela-tively short (100- to 125-msec) intersaccadic interval hypothe-sized to result from pontine neuronal bursts (Dell'Osso et al.,1977) that have been observed in cerebellar ataxias and multi-ple sclerosis (Kuskowski, 1988). Anticipatory saccades (AS) arethe most recently described intrusive saccadic movement(Whicker et al., 1985). AS begin as large amplitude movementsin the direction of target motion during smooth pursuit. Pursuitceases after the original movement, and the eyes either await thetarget before resuming pursuit or another saccade is generatedthat accurately refoveates the target (Abel & Ziegler, 1988;Kaufman & Abel, 1986; Whicker et al., 1985). The intersac-cadic interval is from 0.5-1.5 s for 5-degree-per-second targets,a feature that may most accurately differentiate AS from ma-cro-SWJ (L. A. Abel, personal communication, September 23,1988).
Recording Eye Movements
There are a variety of techniques for detecting eye move-ments in the laboratory (see \bung & Sheena, 1975, for a re-
80 BRETT A. CLEMENTZ AND JOHN A. SWEENEY
a. Normal pursuit d. Macrosaccadic oscillations
b. Square wave jerks e. Macro- square wave jerk
f. Anticipatory saccade
Figure 1. Five types of inappropriate (intrusive) saccadic eyemovements occurring during pursuit tracking.
view), of which electrooculography (EOG) and infrared scleralreflection (IR) have been the most widely used by psychopathol-ogy researchers. Although many types of eye movements can bedetected at bedside examination, careful laboratory evaluationis necessary for accurate quantitative specification of EMD(Leigh & Zee, 1983). This section highlights the advantages anddisadvantages of EOG and IR (see lacono & Lykken, 1983, fora review).
EOG monitors shifts in the electromagnetic dipole generatedby voltage differences between the cornea and retina, but is con-taminated by bioelectric noise (lacono & Lykken, 1979a, 1983;Lindsey et al., 1978). As a result, EOG is precise and sensitiveonly to movements above 1-2 degrees in amplitude. On theother hand, EOG provides measurement of oculomotion fortarget excursions subtending nearly the entire visual field, canbe used while subjects are wearing corrective lenses, and is suit-able for prolonged recording of oculomotion.
IR records the reflection of an infrared light source off thecorneal-scleral margin to monitor changes in this reflection asthe eyes move. IR is capable of linear eye movement recordingsup to approximately ±10-15 degrees of visual angle from cen-tral fixation, and provides accurate measurement down tomovements of 0.25-0.5 degree in amplitude. IR is uncontami-nated by bioelectric noise (lacono & Lykken, 1979a, 1983;Lindsey et al., 1978), but is contaminated by extraneous lightsources. IR generally requires subjects to remove eyeglasses, al-though Smith and lacono (1982) have developed and tested anIR recording device that can be attached to such prostheses.
With prolonged testing, IR tends to irritate and dry the eyes andthus increase the frequency-of-blink artifact.
In sum, EOG can be used under more varied experimentalconditions while providing reasonably accurate recording ofoculomotion. Contamination of EOG by bioelectric noise andaccuracy of measurement to only 1-2 degrees of visual angleare this method's major drawbacks. IR provides more preciseeye movement recording, but limits the range of experimentalpossibilities. Given their different advantage-disadvantage pro-files, both measures, depending on the research question of in-terest, will continue to be of value.
Stimulus Characteristics
Of great importance for both measurement and specificationof eye movement abnormalities is the type of stimulus beingused. In early studies of EMD during smooth pursuit, a pendu-lum swinging at 0.4 Hz traversing ±10 degrees of visual anglewas the standard stimulus. More recent studies have used varia-tions on computer-generated stimuli, which have some impor-tant advantages, including precise control over velocity, direc-tion, amplitude, and luminance of the visual target.
Varying target amplitude, as well as decreasing expectancyeffects, may have special significance. The target excursionscommonly used by psychopathology researchers studying EMDmay confound more specific examination and characterizationof eye movements on two accounts. First, the "standard" excur-sions used by most experimenters are ±10 degrees of visual an-gle (a few studies have used targets up to ± 15 and ±20 degreesof visual angle [Couch & Fox, 1934; Levin et al., 1988; Mather,1985, 1986; Mather & Putchat, 1982/1983, 1984; Schmid-Burgk, Becker, Diekmann, Jurgens, & Kornhuber, 1982;Whicker et al., 1985; Yee et al., 1987]: These are certainly theexception). Targets usually begin from central fixation and aresinusoidal (approximating the movement of a pendulum in thehorizontal plane), although some researchers use triangularwave targets. Because subjects are aware of target path, expec-tancy effects may confound accurate assessment of smooth pur-suit for well-practiced, more "efficient" subjects:
When a subject knows in advance that the target is going to stopmoving at a certain position or time, pursuit begins to slow downmany hundreds of msec before the target stops. Subjects who areaware of this phenomenon still cannot seem to stop themselvesfrom doing it by concentrated effort. (Robinson, Gordon, & Gor-don, 1986, p. 45)
Subjects able to develop and maintain expectancies (e.g., nor-mal persons) may do better than those who cannot maintainsuch a set (perhaps persons with schizophrenia) during eyemovement tasks. Another potential problem relates to the "ac-celeration saturation" phenomenon (Robinson et al., 1986).When a target for smooth pursuit begins to move, there is aninitial velocity overshoot and ringing (oscillation around actualtarget velocity), lasting for approximately 0.5 s, before pursuitsettles to a steady state.
Using relatively restricted target excursions with predictabletrajectories and durations, then, may limit knowledge to begleaned from studying eye movements in psychiatric patients.Both expectancy effects and acceleration saturation may be
HMD IN SCHIZOPHRENIA 81
confounds during each cycle of predictable, restricted range si-nusoidal pursuit (the subject always knows the direction of tar-get motion and, because velocity goes to zero at the extremes oftarget oscillation, ringing may occur for approximately 1 s ofeach cycle). Global accuracy and specific oculomotor measurescores obtained during such target conditions may differ mean-ingfully and substantially from values obtained during unpre-dictable stimulus conditions. Perhaps more problematic, thesephenomena may differentially affect oculomotor functioningacross populations (see Ross, Ochs, Goldberg, Pandurangi, &Kendler, 1989, for a discussion of how acceleration saturationeffects may differ for patients with schizophrenia and normalpersons, and Levin et al., 1988, for how target predictabilitymay differentially affect pursuit gain for these two groups).
EMD as a Biological Marker for Schizophrenia
Method of oculomotor assessment, eye movement recording,and stimulus presentation are important factors to considerwhen evaluating the research on EMD in schizophrenia. Al-though the literature on EMD has been reviewed previously(Holzman, 1975,1985,1987;Iacono, 1983,1988;Liptonetal.,1983), only Erlenmeyer-Kimling (1987) and lacono (1983,1985) have systematically and specifically addressed the biologi-cal marker status of EMD. Furthermore, even though most ofthese reviews mentioned important methodological issues,none has focused on more specific, neuro-ophthalmologicallyinformed measures. Evaluating the literature from this perspec-tive could be critical for developing a more complete etiological,genetic, and pathophysiological understanding of EMD inschizophrenia.
The results of many family, twin, adoption, and quantitativegenetic studies demonstrate that schizophrenia is at least par-tially genetically determined (Faraone & Tsuang, 1985; Gottes-man, McGuffin, & Farmer, 1987; Gottesman, Shields, & Han-son, 1982). The answers to more specific questions about theinheritance of this disorder (appropriate definition of the phe-notype, mode of transmission, the relation between pathophysi-ology and genetics) remain unclear. One obstacle to further elu-cidating the genetics of schizophrenia has been the reliance onclinically derived symptom ascertainments both to define thedisorder and as indicators of liability for the disorder (Holzman,1983). The inherent confound in such a strategy makes the taskof separating subsyndromal manifestations of schizophreniafrom liability extremely difficult.
One approach for bypassing this confound is to identify bio-logical markers that are associated with schizophrenia yet notpart of its clinical expression. Biological markers may help toclarify important diagnostic, genetic, and pathophysiological is-sues. Variables considered to be potential biological markers forpsychiatric disorders need to have the following characteristics(lacono, 1982b, 1983,' 1985; Nuechterlein, 1987; Shields &Gottesman, 1973). In the general population, the marker shouldhave a low base rate, demonstrate temporal stability, be geneti-cally transmitted, and identify individuals at risk for syndromaland subsyndromal manifestations of the disorder in question.Studies of psychiatric patients must demonstrate that the pres-ence of the marker is relatively specific to a diagnostic category,is present during symptom remission, occurs among first-de-
gree relatives of the index case at a higher rate than in the gen-eral population, and segregates with illness in affected relatives.Although several psychophysiological variables have yielded en-couraging results (Erlenmeyer-Kimling, 1987; Freedman et al.,1987; Holzman, 1987; lacono, 1985), undoubtedly one of themost promising biological markers for schizophrenia is EMD(Erlenmeyer-Kimling, 1987; Holzman, 1987; lacono, 1983,1988).
EMD in the General Population
Population base rate of EMD: The pursuit system. Holzmanet al. (1984) studied 48 subjects (18-30 years of age) who hadnegative personal and family histories of psychiatric illness andwho were free of neurological disease. Eye movements were re-corded with EOG while subjects followed a monitor-presentedstimulus traveling at 0.4 Hz. Eye movement protocols wererated by using both a Benitez-Shagass-type qualitative rankingscale and In (S/N). High scores on both measures indicatedmore accurate pursuit. Subjects were required to have averagescores greater than 3.5 and 2.5 for the qualitative and In (S/N) measures, respectively, to be classified as "good" trackers.Subjects with scores below both of these values were considered"deviant" (it is unclear how subjects who fell above one cutoffand below the other would have been classified; such cases werenot reported). Eight percent (4 of 48) of the subjects were con-sidered to have deviant tracking.
This is the commonly cited figure in the psychiatric literaturefor the base rate of "abnormal" pursuit in the general popula-tion (Holzman, 1987; Holzman et al., 1974, 1988; lacono,1988;Liptonetal., 1983; Matthysse, Holzman, &Lange, 1986).Whether 8% most adequately captures the prevalence of EMDin the general population, however, must be carefully evaluated.
Holzman et al. (1984) thoroughly screened their normal pop-ulation. Of the remaining studies from which information per-taining to the base rate of EMD in the general population canbe obtained, most, but not all, used at least a minimal screeningprocedure. Because eye movements can be affected by neuro-logical disease and drug use, screening for these potential con-founds is important.
Abnormal smooth pursuit can be defined in different ways.Holzman et al. (1984) used two highly correlated global accu-racy measures. Their criteria for determining whether pursuitwas normal or deviant were "established psychometrically fromprior work in the testing of hundreds of both normal subjectsand psychiatric patients" (p. 137). lacono and Lykken (1979c)originally pointed out that there were potential problems withmaking base-rate comparisons across studies unless deviantperformance could be more precisely defined. The validity ofHolzman et al.'s (1984) cutoff-point choices and prevalence es-
1 lacono (1983, p. 372) actually used the term genetic marker. As hepointed out, "my definition of a genetic marker. . . stands at variancewith the strict usage of this term by human geneticists" (p. 372). Gottes-man et al. (1987) suggested that the term genetic marker is "best re-stricted to cover traits that have a simple, known mendelian mode ofinheritance and that are demonstrably polymorphic" (p. 39). Followingtheir advice, the term biological marker has been chosen to define thepsychophysiological variable of interest in this article.
82 BRETT A. CLEMENTZ AND JOHN A. SWEENEY
timates in the general population, however, can be in part as-sessed by comparison with the findings from other studies.
Using the Benitez (1970) system, mean accuracy scores haveranged from 1.17 (Lipton, Levin, & Holzman, 1980) to 1.41(Upton, Frost, & Holzman, 1980) for normal subjects. Usingthe similar Shagass scale, mean accuracy values have rangedfrom 1.13 (Levin, Lipton, & Holzman, 1981) to 2.7 (Kuechen-meisteretal., 1977). Other investigators (Acker &Toone, 1978;Shagass et al, 1974,1976) have reported mean accuracy scoresfor qualitative ratings that vary between these values. Usingdiffering cutoff points, the reported prevalence of deviant pur-suit in normal control subjects has varied between 0% (Levin,Lipton, & Holzman, 1981) and 16%(Scaroneetal., 1987), withothers (Holzman et al., 1973, 1974) reporting prevalences thatvaried between these values. lacono and Lykken (1979c) foundthat the base rate of abnormal pursuit could vary widely (3%-28% for the examples they provide), depending on the cutoffscore choice (see lacono & Lykken, 1979c, Table 3, p. 1368).Brezinova and Kendell (1977) found, using the Shagass scale,that 41.6% (10 of 24) of their control subjects had scores of 3 orworse, and 12.5% (3 of 24) had scores of 4 or worse.
Overall, these studies have suggested that the optimal cutoffscore on Benitez- or Shagass-type scales for determining deviantpursuit is uncertain because of considerable across-studies vari-ability. What factors might have been responsible for the widelydivergent findings in studies using qualitative ratings of pursuitaccuracy? First, these ratings may be difficult to operationalize-across laboratories, possibly resulting in different scores re-flecting similar performance. Second, studies in which recruit-ment and screening of potential subjects seem to have beenmore carefully conducted generally have found more accuratepursuit. Third, eye movement accuracy decreases with increas-ing age (Hainline, 1988). Clementz (in press) examined ageeffects on RMS error deviation in a mixed group of 117 nonpsy-chiatric control subjects, probands with schizophrenia, and thelatter's first-degree family members. There was a significant cor-relation between age and RMS error deviation for the total sam-ple (r = 0.37, p < .001, for a standard 0.4 Hz sinusoidal pursuittask), indicating that global pursuit performance significantlyworsens with increasing age. Using Fisher's z, the separategroups did not differ in the magnitude of their correlations be-tween age and RMS. Studies using populations of differing agesare bound to reflect this age-performance relation in theirEMD base-rate figures. It may be that laboratory, study, andsubject-specific (e.g., age) factors are important mediating vari-ables that preclude determination of a generalizable EMD base-rate figure, at least when using global measures of oculomotorfunctioning.
Although Holzman et al. (1984) took a conservative ap-proach to defining deviant pursuit by requiring subjects to ful-fill a "double-globally deviant" criterion, "global accuracy"may not be the best means of defining EMD for certainpurposes (Abel & Ziegler, 1988). Determining the prevalenceof particular types of EMD may help to clarify the base rateof abnormal smooth pursuit in the general population. Unlikeglobal accuracy measures, pursuit gain calculations providespecific information about the smooth pursuit system's intact-ness (Leigh & Zee, 1983).
Pursuit gain is normally close to 1 for targets traveling less
than 20 degrees per second (Leigh & Zee, 1983; Wirtschafter& Weingarden, 1988). Gain decreases to approximately 0.90(SD = 0.04) for targets traveling closer to 45 degrees per second(0.4 Hz in Yee et al., 1987), and decreases rapidly for stimulusfrequencies above 1 Hz (Leigh & Zee, 1983). Pursuit gain out-side the 0.85-1 (0.2 Hz-targets) and the 0.83-0.95 (0.4 Hz tar-gets) ranges is generally considered deviant (Yee et al., 1987).As target characteristics (Carl & Gellman, 1987), medications,visual distractions, and age may influence measures of pursuitadequacy (Abel & Hertle, 1988; Kaufman & Abel, 1986;Sharpe & Sylvester, 1978; Spooner, Sakala, & Balogh, 1980),controlling for these variables is necessary.
Population base rate of EMD: The saccade system. Somedynamic saccade characteristics (reaction time, accuracy, etc.)are sensitive to many variables, including luminance, size of thestimulus, target predictability, target information, age, motiva-tion, and attention (Bronstein & Kennard, 1985; Cegalis,Hafez, & Wong, 1983; Cegalis & Sweeney, 1981; Cegalis,Sweeney, & Dellis, 1982; Leigh & Zee, 1983; Mather, 1986). Asa result, "normal values for the specific testing conditions usedin one's own laboratory must be established" (Leigh & Zee,1983, p. 42). Such a necessity probably makes detailed estab-lishment of population base-rate figures for many saccade-re-lated phenomena unrealistic. There are, however, a few well-defined and easily quantifiable events for which laboratory-spe-cific base rates could be determined. These include measures ofreaction time, "main sequence" functions, and prevalence ofintrusive saccadic events (e.g., SWJ, AS) during different testingconditions.
SWJ have been discovered in as many as 20% of normal sub-jects (Elidan, Gay, & Lev, 1984; Herishanu & Sharpe, 1981;Sharpe & Sylvester, 1978). They become more frequent withincreasing age (Kaufman & Abel, 1986; Sharpe & Sylvester,1978), and are more frequent at targets traveling at 5 degreesper second than at 20 degrees per second (Kaufman & Abel,1986). Fatigue does not seem to influence the frequency of SWJ(Herishanu & Sharpe, 1981; Kaufman & Abel, 1986), but thereis some suggestive evidence that distraction may increase theirfrequency (Kaufman & Abel, 1986). Ocular flutter, macrosac-cadic oscillations, and macro-SWJ seem to be rare movementsin normal subjects, but base rates have yet to be determinedfor these variables. AS also appear to be uncommon in normalsubjects, although their frequency may increase during visualdistractions, and they may become more common with increas-ing age (Kaufman & Abel, 1986).
Temporal stability. Replicability of eye movement resultsmay be influenced by many factors, including drug ingestion,changes in target and measurement characteristics, and level ofattention. Studies have investigated the stability of global pur-suit tracking performance, saccadic reaction time, and saccadefrequency for normal subjects over periods ranging from 1 weekto 2 years. lacono and Lykken (1979b, 1979c) reported 1-weekretest reliabilities for a pursuit tracking task in normal monozy-gotic twins. Subjects followed a stimulus presented on a cath-ode-ray tube screen traveling at target frequencies between 0.2-1.2 Hz in 0.2-Hz steps. They found correlations for their RMSmeasure ranging from 0.79 for 0.2- and 0.4-Hz targets to 0.92for 1.0-Hz targets, and a mean reliability for all conditions of0.86. They also reported a retest reliability of 0.72 for large
HMD IN SCHIZOPHRENIA 83
(greater than 5 degrees) saccades over this same interval. Sha-gass et al. (1974) found similar correlations by using the 1 - to 5-point qualitative ratings for 11 normal subjects after a 6-monthretest. lacono and Lykken (1981) reevaluated their twin sampleafter 2 years and reported retest reliabilities similar to thosethey had reported after 1 week. lacono and Lykken (1979b) alsoreported a saccadic reaction time retest reliability of 0.72. Reaet al. (1989) discovered a 1-month retest reliability of 0.80 fortotal saccade frequency during a pursuit tracking task, 0.91 for3- to 5-degree saccades, but only 0.24 for saccades of 5 degreesor larger. These studies demonstrate that, at least in globalterms, retest reliability for pursuit tracking performance ap-pears to be high for as long as 2 years. Saccadic reaction timeand frequency of relatively small corrective saccades duringpursuit tracking also seem to be stable. There is presently lackof clarity, however, about the retest reliability of large saccades.
Fluctuating attention both during and between testing ses-sions may influence the stability of eye movement recordingsover time. As a result, it is important to consider the role thatattention enhancement and distraction play in oculomotor per-formance. Similar to studies using psychiatric patients, severalstudies using normal subjects have suggested that global accu-racy of pursuit improves, within-subjects variability in globalaccuracy is reduced, and the frequency of intrusive saccadesdecreases with attention enhancement (Shagass et al., 1976;Holzman et al., 1976; lacono & Koenig, 1983; lacono & Lyk-ken, 1979b, 1979c; lacono et al., 1981, 1982; Levin, Lipton,& Holzman, 1981). Furthermore, some studies have discoveredthat complex cognitive distractors (e.g., subtracting 13 from200 and writing each number in the series) may deleteriouslyaffect qualitative pursuit accuracy ratings (Acker & Toone,1978; Brezinova & Kendell, 1977; Tomer, Mintz, Levy, & Mys-lobodsky, 1981). Kaufman and Abel (1986) used auditory, cog-nitive, and visual distractors, and found that only during thelatter condition (pictures of forests, mountains, or cities servingas background for smooth pursuit) was performance alteredamong their young and elderly normal subjects. More specifi-cally, Kaufman and Abel reported decreased pursuit gain andmore time spent off-target following AS during visual distrac-tion.
These attention manipulation findings, although apparentlyreplicable, are somewhat ambiguous for at least two reasons.First, attention enhancement may improve performance, but itmay also invoke the use of different brain systems for processinga more complex stimulus. If this is the case, then the pathophys-iology related to an abnormality occurring during standardstimulus presentation may only be masked by attention en-hancement. Second, drawing a subject's attention from a taskdoes not address the potential pathophysiology behind an ab-normality that occurs while the subject is not distracted.
Although HMD may eventually prove to be the result of anattentional dysfunction (Holzman, Levy, & Proctor, 1978), pre-viously conducted attention manipulation studies (e.g., Brezi-nova & Kendell, 1977) do not necessarily have bearing on suchan issue. Lipton, Frost, and Holzman (1980) demonstrated thatunsophisticated raters could easily differentiate betweensmooth pursuit protocols of persons with schizophrenia andthose of distracted normal persons. This finding suggestsdifferences in both the specific types of oculomotor abnormali-
ties that occur and the mechanisms underlying HMD observedin these different populations.
Genetic determination of oculomotor control. lacono (1982a)and lacono and Lykken (1979b, 1979c) have investigated theinfluence of genetic factors on oculomotor control. lacono(1982a) reported on a sample of 34 monozygotic and 24 dizy-gotic twin pairs. Subjects engaged in smooth pursuit and sac-cadic tracking tasks. Measures of error deviation from perfectsmooth pursuit, phase lag, and saccadic reaction time were ob-tained. The intraclass correlation for global tracking accuracyfor monozygotic twins was nearly twice that for dizygotic twinsat all target velocities (0.61-0.68 vs. 0.29-0.40). Phase lag andsaccadic reaction time did not appear to be strongly geneticallyinfluenced. Additionally, lacono and Lykken (1979b, 1979c) re-ported similarly high intraclass correlations for a subset of thesemonozygotic twins using the RMS measure. Raters were alsoable to match twins' eye movement protocols by inspection.Correlations for phase lag and saccadic reaction time, again,were not statistically significant. These results suggest thatglobal accuracy of smooth pursuit is heavily genetically deter-mined (if subjects are not taking central-nervous-system-affecting drugs and have not experienced neurological insult).
EMD and psychopathology. A few studies have investigatedthe relation between EMD in nonpsychiatric populations anddifferent measures of psychopathology. lacono and Lykken(1979c) reported significant positive correlations between theRMS pursuit accuracy measure and psychoticism as measuredby the Differential Personality Questionnaire (Tellegen & At-kinson, 1974) at higher (1.0- and 1.2-Hz) target frequencies (r =0.31), and between psychoticism and saccadic reaction time(r = 0.31). They also found a significant negative correlationbetween the same global accuracy measure and a trait variablerelated to seeking and enjoyment of imaginative experiences(Tellegen & Atkinson, 1974) at lower (0.2-, 0.4-, and 0.6-Hz)target frequencies (rs = -0.32 to -0.41). Siever, Coursey, Alter-man, Buchsbaum, and Murphy (1982) and Siever, Haier, et al.,(1982) found that low global accuracy trackers had more devi-ant Minnesota Multiphasic Personality Inventory profiles,more movement responses on the Rorschach Inkblot Test, fewerheterosexual contacts, lower self-esteem, and less intact percep-tual boundaries than high global accuracy trackers. These per-sons, however, were preselected on the basis of the monoamineoxidase and Continuous Performance Test variables, leaving therelation between randomly sampled persons with EMD andpsychopathology in the general population somewhat obscure.
To further investigate the relation between EMD and psycho-pathology, Siever et al. (1984) screened a large number of malecollege students and selected the best and the worst accuracytrackers for further study. They found a significant relation be-tween schizophrenia-related symptomatology and low accuracytracking. Low global accuracy trackers were more likely thanhigh global accuracy trackers to have been previously hospital-ized for schizophrenia, to be diagnosed as having schizotypalpersonality disorder, to manifest schizotypal features, and tohave fewer social interactions per week. Simons and Katkin(1985) also studied a college population and discovered that lowglobal accuracy trackers had more variable scores on the Chap-man's Anhedonia and Perceptual Aberration scales (Chapman& Chapman, 1985), and that the poorest trackers also had the

84 BRETT A. CLEMENTZ AND JOHN A. SWEENEY
most pathological scores on both of these measures. These re-sults strongly suggest that schizophrenia-related psychopathol-ogy is related to poorer global smooth pursuit accuracy.
EMD in Psychiatric Patients
Discriminant validity: The pursuit system. A few studies havespecifically addressed the intactness of the smooth pursuit sys-tem in persons with schizophrenia. Mather and Putchat (1982/1983, 1984) reported pursuit gains in persons with schizophre-nia that were similar to those for normal control subjects. Fiveother investigations, however, have offered evidence that a sub-set of persons with schizophrenia may have low gain pursuit.Schmid-Burgk et al. (1982) found pursuit gains of 0.84 for inpa-tients, 0.88 for outpatients, and 0.92 for normal control subjectswhile subjects were pursuing a sinusoid with maximum velocityof 47.1 degrees per second. There was large overlap between thepatients and control subjects, and only the persons with schizo-phrenia who were inpatients significantly differed from normalsubjects. Yee et al. (1987) also found that persons with schizo-phrenia had lower pursuit gains than normal control subjectsat both 22.6 degree-per-second (0.92 vs. 0.98) and 45.2 degree-per-second (0.83 vs. 0.90) maximum target velocities. There wasagain a large overlap between persons with schizophrenia andnormal subjects, especially at the lower target velocity, but 9persons with schizophrenia (43%) were clearly outside the nor-mal range when following the higher velocity target. Yee et al.(1987) found significantly low pursuit gains for a mixed groupof psychiatric patients, but as 5 of those subjects were receivinglithium and 1 was receiving a benzodiazepine this finding issomewhat suspect. Ross et al. (1988) also reported lower pursuitgains for persons with schizophrenia (0.91) than for normalcontrol subjects (0.95). Although the patient's value is withinthe normal range, there was again considerable variabilityamong the patients. The five lowest gain calculations, with fourof those being clearly outside the normal range, belonged to per-sons with schizophrenia. Because some patients in this studywere receiving benzodiazepines, this finding should be consid-ered tentative. Abel and Ziegler (1988) reported pursuit gainsof persons with schizophrenia ranging from 0.66 to 1.07, andfor persons with unipolar affective disorders ranging from 0.91to 1.03. Levin et al. (1988) also reported significantly lower pur-suit gain for a group of five patients with chronic schizophrenia.Levin et al. (1988) found this deficit to be most pronouncedwhen subjects pursued unpredictable targets traveling at highervelocities.
There is some suggestive evidence, therefore, that some per-sons with schizophrenia may have low gain pursuit. Whetherthis finding is related to schizophrenia's pathophysiology re-mains to be determined. The potential discovery of such a spe-cific abnormality with the pursuit system may be a promisingstep toward clarifying the nature of EMD in at least some per-sons with schizophrenia.
Discriminant validity: The saccadic system. Although moststudies have found saccades of normal velocity in persons withschizophrenia (Levin, Jones, Stark, Merrin, & Holzman, 1982a,1982b; Mather & Putchat, 1982/1983; Yee et al., 1987), therehave been some notable exceptions. Cegalis et al. (1982) re-ported that persons with schizophrenia had higher peak veloci-
ties but significantly smaller saccades on a refixation task thandid normal control subjects. Levin, Holzman, Rothenberg, andLipton (1981) found that persons with schizophrenia tended tohave lower maximum velocity and longer duration of saccadesrelative to normal subjects at increased target amplitudes in theright visual field. This effect was not statistically significant (p <.08); however, the inclusion of small (1 -degree) with large (10- to20-degree) amplitude movements in the calculations may havemitigated an important abnormality of saccade dynamics inpersons with schizophrenia.
Most studies addressing the accuracy of saccadic movementsin persons with schizophrenia have not reported abnormalities(Levin, Holzman et al., 1981, 1982a, 1982b; Rosset al., 1988;Yee et al., 1987), but there are a few exceptions. Schmid-Burgket al. (1982) reported more dysmetric saccades, and Mather andPutchat (1982/1983) found less accurate, and more double-jump, saccades among persons with schizophrenia. Addition-ally, although most studies have reported normal-range initia-tion latencies for saccadic movements (Done & Frith, 1984;Fukushima et al., 1988; lacono et al., 1981, 1982; Levin,Holzman, et al., 1981,1982a, 1982b; Mather & Putchat, 1982/1983), a few (Schmid-Burgk et al., 1982; Yee et al., 1987) havefound longer reaction times among persons with schizophrenia.
These results leave some ambiguity about the dynamics ofsaccade characteristics among persons with schizophrenia. Themajority of the most methodologically sophisticated studiessuggest normal saccade dynamics, but the exceptions leaveroom for doubt and highlight the necessity of further investiga-tion in this area.
Although the intactness of saccadic eye movement dynamicsin persons with schizophrenia is somewhat uncertain, the highfrequency occurrence of inappropriate saccadic movementsduring both fixation and smooth pursuit is a relatively robustfinding. The majority of studies have found a significantlygreater frequency of saccades among persons with schizophre-nia as compared with normal control subjects and other psychi-atric patients (Cegalis & Sweeney, 1979, 1981; Cegalis et al.,1983; Kufferle et al, 1988; Mather & Putchat, 1982/1983;Matsueetal, 1986;Mialet&Pichot, 1981), with only two pub-lished failures to find such an effect (Ross et al, 1988; Schmid-Burgk et al, 1982). Three studies have also reported an in-creased frequency of SWJ among persons with schizophreniawhen compared with normal control subjects (Kufferle et al,1988; Levin et al, 1982a, 1982b), and one (Levin et al, 1988)failed to find an increased frequency of SWJ in patients withschizophrenia.
There is some evidence that the high frequency of saccadesmay be related to either low gain pursuit (Cegalis & Sweeney,1981; Ross et al, 1988), suggesting that some of these saccadesare corrective rather than intrusive, or frontal lobe-related fail-ures of attention (Levin, 1984). Fukushima et al. (1988) studied12 patients with schizophrenia and 10 normal control subjectson an antisaccade task. During this procedure, subjects areasked to generate a saccade in the direction opposite to a stimu-lus presented either to the left or right of central fixation. Thesuppression of reflexive (inappropriate) saccades is thought tobe controlled by frontal lobe eye movement systems. Only 1normal subject made a single reflexive saccade (in the directionof stimulus presentation) during the antisaccade task. On the
HMD IN SCHIZOPHRENIA 85
other hand, 5 patients had error rates of 25%-60%, and 4 ofthese 5 patients showed definite cortical atrophy on computedaxial tomography scans. One patient, who had 15% errors onthe antisaccade task, also showed mild cortical atrophy. Otherauthors have also reported positive relations between neurologi-cal (Siever et al., 1986; Sweeney, Solomon, Rea, Mann, & Fran-ces, 1987; Weinberger & Wyatt, 1982) and neuropsychological(Sweeney et al., 1987) abnormalities and globally measuredHMD in persons with schizophrenia. Taken together, these re-sults suggest that at least voluntary control of saccades, and per-haps other indices of HMD, may be related to brain abnormali-ties, particularly in the frontal lobe (Levin, 1984).
There is ample evidence that patients with schizophreniahave more frequent saccades during both tracking and fixationthan do normal control subjects and some other psychiatric pa-tients. This abnormality may be related to mechanisms of eyemovement control located in the frontal eye fields (Area 8), su-perior colliculus, and dorsomedial frontal cortex. There havebeen only six published studies, however, attempting to docu-ment the specific inappropriate saccade types occurring in per-sons with schizophrenia. These include a single report of abnor-malities during the antisaccade task (Fukushima et al., 1988),another reporting the occurrence of ocular flutter in a chronicpopulation (Cegalis & Sweeney, 1979), and four contradictorystudies addressing the frequency of SWJ (Kufferle et al., 1988;Levin etal., 1982a, 1982b, 1988).
Temporal stability. Given that both medications and state-related factors may affect ocular motility, temporal stabilitystudies of HMD in psychiatric patients are especially impor-tant. Shagass et al. (1976) reported that affixing numerals to apendulum improved the global accuracy of pursuit ratings.Other investigators have replicated this phenomenon (Holzmanet al., 1976; lacono & Koenig, 1983; lacono & Lykken, 1979b,1979c; lacono et al., 1981, 1982; Levin, Lipton, & Holzman,1981). Cegalis and Sweeney (1979) failed to replicate this effectfor RMS, although they did observe a reduction in saccade fre-quency during tracking with increased target information (asdid lacono & Lykken, 1979c). Likewise, Pivik (1979b) did notfind an improvement in performance for frequency of saccadesduring his signal-detection task.
Although persons with schizophrenia have more globally ac-curate pursuit during attention enhancement, they also con-tinue to have more inaccurate pursuit than normal persons un-der such conditions (Holzman et al., 1976; lacono & Koenig,1983; lacono et al., 1981, 1982), although attention enhance-ment may effectively reduce the frequency of large (greater than4 degrees) saccades (Spohn et al., 1988) among these subjects.Similarly, test-retest studies suggest that global accuracy of pur-suit remains relatively stable for 2-8 weeks (Rea et al., 1989;Siever et al., 1986; Spohn et al., 1988). Van den Bosch, Rosen-daal, and Mol (1987), however, found that accuracy of pursuitas measured by an error deviation score significantly decreasesafter 1 month in persons with schizophrenia, but that the corre-lation between a patient's performance at 1- and 2-month re-tests with measurements taken at initial hospitalization washigh (0.69-0.78). Similarly, Rea et al. (1989) found that a re-duction in large saccades was highly correlated with neurolepticdose and clinical stabilization, as measured by the Brief Psychi-atric Rating Scale (BPRS), during the acute phase of illness.
lacono and colleagues (lacono & Koenig, 1983; lacono et al.,1981, 1982) nevertheless reported that stabilized outpatientswith schizophrenia (BPRS mean = 22.8, Global AssessmentScale mean = 69.3) still have significantly poorer globalpursuit accuracy than unipolar-depressed and normal controlsubjects.
In all, it appears that, when defined by global ratings, pursuitaccuracy remains hierarchically stable over time in personswith schizophrenia, although the global accuracy score seemsto be significantly reduced with the addition of neurolepticmedication and during clinical stabilization (see Levy, Lipton,Holzman, & Davis, 1983, for a contradictory view). The fre-quency of large saccades may decrease when neuroleptic dosageis increased. Although large saccade frequency may decrease,the frequency of small saccades seems to increase with time andneuroleptic treatment, resulting in an overall small increase insaccade frequency for patients with schizophrenia (Rea et al.,1989). Spohn et al. (1988), however, reported that a small groupof patients (6 of 8) who were removed from medication demon-strated an increase in the frequency of large saccades in the ab-sence of a detectable increase in facial-oral tardive dyskinesia.This pattern of contradictory results suggests that the poten-tially confounding effects of medication and clinical status onboth global and more specific oculomotor measures need to befurther evaluated.
EMD in family members of psychiatric patients. One of themost interesting and potentially important findings in this liter-ature has been the observation of EMD in first-degree relativesof probands with schizophrenia (Holzman, 1975; Holzman etal., 1974, 1984; Kuechenmeister et al., 1977; Levy, Yasillo, etal., 1983; Mather, 1985; Siegel, Waldo, Miznor, Adler, & Freed-man, 1984). The percentages of globally inaccurate pursuit infirst-degree family members of probands with schizophreniarange from 34% to 58%. The prevalence of globally deviant pur-suit in the first-degree relatives of persons with other psychiatricdisorders has been reported to lie between 5%-13%. As withnormal subjects, studies of psychotic probands and their co-twins suggest that global accuracy ratings of pursuit seem to beat least partially genetically determined (Holzman, Kringlen,Levy, & Haberman, 1980; Holzman et al., 1977).
Using more specific eye movement scoring techniques,Whicker et al. (1985) studied eight parents of patients diag-nosed with schizophrenia (according to the Diagnostic and Sta-tistical Manual of Mental Disorders, third edition [DSM-HI]).They reported that six of these persons demonstrated a highfrequency of AS and spent considerable time off-target. Theseabnormal intrusive saccadic movements had not been pre-viously described in the neuro-ophthalmology literature. Cle-mentz (in press) also studied pursuit gain, the frequency of in-trusive saccadic events, and global error deviation (RMS) in agroup of 61 first-degree relatives (12 spectrum—3 with schizo-phrenia and 9 with schizophrenia-related personality disor-ders—and 49 nonspectrum) of 26 probands with Research Di-agnostic Criteria (RDC) schizophrenia. Both family membergroups had significantly lower pursuit gain (0.83 for spectrumsubjects and 0.93 for nonspectrum subjects) than a group of38 nonpsychiatric controls (0.97). Frequency of AS per cycledifferentiated the three groups, with nonpsychiatric controlsubjects having significantly fewer AS than nonspectrum sub-

86 BRETT A. CLEMENTZ AND JOHN A. SWEENEY
jects, and the latter group having significantly fewer AS than thespectrum subjects. RMS error deviation differentiated nonpsy-chiatric control subjects from the two family member groups,who did not differ on this variable. There was no difference inthe frequency of SWJ per cycle between groups.
lacono, Bassett, and Jones (1988) have studied the eye move-ments of Bassett, McGillivary, Jones, and Pantzer's (1988) re-cently described pedigree that suggested a link between a partialtrisomy of Chromosome 5 and schizophrenia.2 lacono et al.(1988) discovered that the two affected, partially trisomic fam-ily members had globally inaccurate smooth pursuit, and thethree unaffected, nontrisomic family members had globally ac-curate eye movements. This is the first study to suggest an asso-ciation between HMD and a genetic abnormality that may berelated to schizophrenia, and seems to further support the po-tential utility of HMD for helping to clarify the inheritance ofschizophrenia (see Holzman, Matthysse & Levy, 1989, and la-cono, Bassett, & Jones, 1989, for further discussion of how la-cono et al.'s [ 1988] finding relates to liability for schizophrenia).
These findings offer promising support for HMD's being abiological marker for schizophrenia. There are some findings,however, that obscure straightforward interpretation, and atfirst glance are problematic for inferring biological marker sta-tus for this variable (Holzman, 1987). First, a number of pro-bands with schizophrenia who have globally accurate pursuithave parents with globally inaccurate pursuit. Second, in thetwin studies (Holzman et al., 1977, 1980), there were five setsof dizygotic twins in which the twin with schizophrenia hadglobally accurate pursuit and the unaffected co-twin demon-strated globally inaccurate pursuit. In an effort to explain thesecomplications, while preserving HMD's marker status, Mat-thysse et al. (1986) and Matthysse and Holzman (1987) hypoth-esized the presence of a latent trait transmitted in quasi-Men-delian fashion.
The model proposed that the central nervous system diseaseprocess that is the outcome of the latent trait produces schizo-phrenia, bad tracking, or both (pleiotropy). The smooth pursuitsystem is assumed to be invaded with higher probability thanthe (hypothetical) system that is involved in schizophrenia.First-degree relatives are also assumed to be at high risk for hav-ing the same disease process. The disease process (the latenttrait) is not observed, but is only inferred from the presence ofHMD or schizophrenia. The results of Matthysse et al.'s (1986)mathematical modeling supported the latent trait model forschizophrenia, but suggested that HMD observed in bipolar-dis-ordered patients was an epiphenomenon probably of eithermedication or clinical status. Holzman et al. (1988) replicatedthese results on a separate sample composed of the offspring ofKringlen's (1967) twin population.
This is an intriguing and potentially valuable contribution tounderstanding the genetics of schizophrenia. Despite the seem-ing success of this quantitative genetic model for explaining thetransmission of both HMD and schizophrenia, however, theremay be some problems with Holzman and colleagues' postu-lates. First, Matthysse et al. (1986) and Holzman et al. (1988)assumed a base rate for EMD of 8%. The review of EMD in thegeneral population, however, suggests that more data are neededto verify this figure. Second, Gottesman and McGue (in press)and McGue and Gottesman (1989) have pointed out that the
latent trait model significantly underpredicts both the monozy-gotic twin concordance rate from Kringlen's (1967) data andthe expected risk for the offspring of two parents with schizo-phrenia, which, for Gottesman and McGue, casts doubt on themodel's predictive utility. Matthysse and Holzman (1989), how-ever, have replied that their model does not address schizophre-nia qua schizophrenia, but rather the transmission of a latenttrait with pleiotropic effects, and that it might be a useful heu-ristic for pursuing linkage studies.
Finally, Holzman et al. (1988) used two different diagnosticcriteria to define two separate patient populations. The Chi-cago-Boston sample was diagnosed by means of a combinedRDC-St. Louis definition, where patients were required to ful-fill both sets for study inclusion. Kringlen's (1967) "narrow"Norwegian diagnosis was used to define the subject populationfor his twin series. Holzman et al. assumed that their combinedRDC-St. Louis diagnosis defines schizophrenia in a morebroad-band fashion than Kringlen's definition. As a result,Holzman et al. multiplied the obtained probabilities that thosewith and without the latent trait manifest schizophrenia for theRDC-St. Louis-defined group by a correction factor to com-pensate for diagnostic bandwidth differences (which loweredthe number of persons with schizophrenia in this sample from19.0% to 11.4%). With this modification, their results replicateMatthysse etal.( 1986).
It appears, however, that when patients are required to meetboth RDC and St. Louis criteria for study inclusion, the defini-tion may be as strict as DSM-HI-R's schizophrenia definition.A joint RDC-St. Louis definition identifies approximately10%-20% fewer patients than DSM-IH for a schizophrenia di-agnosis (Stephens, Astrup, Carpenter, Shaffer, & Goldberg,1982). DSM-III-R excludes approximately 10%-20% of thepatients formerly diagnosed with schizophrenia by DSM-IH(Fenton, McGlashen, & Heinssen, 1988), making DSM-III-Rapproximately as narrow as traditional Scandinavian diagnoses(see Gottesman et al., 1987, p. 27, Table 1). Given these diag-nostic relations, Holzman et al.'s (1988) correction factor maynot have been fully necessary, and their replication may nothave been as promising as it initially appeared.
Risk for psychopathology in family members with EMD. Therelation between syndromal and subsyndromal manifestationsof schizophrenia and EMD is an important but little studiedarea within this literature. lacono et al.'s (1988) study of Bassetet al.'s (1988) Chromosome 5 pedigree offered preliminary sup-port for HMD's being associated with schizophrenia-relatedpsychopathology in family members of probands with schizo-phrenia. Besides the proband, who had globally defined inaccu-rate eye movements, four other family members were studied.The only other person in this pedigree with globally definedEMD was an uncle who had schizophrenia. Clementz (in press)also found a relation between the presence of schizophrenia-related psychopathology, pursuit gain, and frequency of AS infirst-degree relatives of probands with RDC schizophrenia.
2 Sherrington et al. (1988) have replicated and Kennedy et al. (1988),St. Clairet al. (1989), and Detera-Wadleigh et al. (1989) have reportedfailures to replicate Bassett et al.'s (1988) finding. These results supportthe notion of potential genetic heterogeneity for schizophrenia. Also seeByerley (1989) for a discussion of these conflicting results.

HMD IN SCHIZOPHRENIA 87
Conclusions and Comments
Methodological Considerations
Eye movement analysis. There are a variety of issues thatcould potentially improve the already valuable research thathas been conducted on HMD in psychiatric patients. First, psy-chiatric investigators have already begun to use measures (e.g.,pursuit gain, main sequence functions, types of saccadic intru-sions) that allow more precise characterization of ocular motil-ity. More extensive neuro-ophthalmological reports of oculo-motor functioning in persons with schizophrenia may help todetermine what, if any, specific HMDs are endemic to this sub-ject population. When used in conjunction with extensive neu-roanatomical, neurophysiological, and neuropsychologicalmeasurement, such studies may help to clarify the etiologicaland pathophysiological relations between HMD and schizo-phrenia. Second, investigators could also be cognizant of poten-tial interactions between the different eye movement systems,and attempt to minimize these interactions when possible.Third, researchers may want to carefully consider whetherEOG, IR, or some other recording device is best for their re-search question, and use the preferred technique. Finally, at-tending to the potential effects of target characteristics (distancefrom the subject, predictability, duration, amplitude, velocity)could be an entire and extremely important research area initself.
Subject selection. The final consideration for evaluating andconducting research on EMD in psychiatric patients relates toidentification and screening of potential subjects. Given the va-rieties of EMD that can arise as a result of neurological disease(Kuskowski, 1988) and drug ingestion (Abel & Hertle, 1988),all subjects should be screened for these potential confounds.Furthermore, until the issue of potential state-related influ-ences on performance is more clearly resolved (Kaufman &Abel, 1986; Rea et al., 1989; van den Bosch & Rozendaal,1987), investigators may want to obtain some measure of cur-rent clinical status from all participants (state-related influ-ences on performance under differing experimental conditionswhen using either global or more specific measures of ocularmotility is, of course, an additional potentially fruitful area ofinvestigation).
There are additional points of interest for selecting patientgroups and normal control subjects and for evaluating familymembers. First, Spohn and Patterson (1979) noted that caseascertainment is important for understanding the relation be-tween EMD and schizophrenia. Studies of EMD in schizophre-nia have used a variety of diagnostic rules, some specified andothers unspecified, for determining patient selection. This leadsto a major problem for comparing findings across laboratories,as subject similarity is often either widely variable or uncertain.Psychiatric classification systems differentially identify patientsfor a schizophrenia diagnosis (Stephens et al., 1982). It has beenestablished that diagnostic bandwidth significantly colors con-clusions about the inheritance of behavioral characteristics likeschizophrenia (Gottesman et al., 1987;Gottesmanetal., 1982).It follows that the potential usefulness of an ostensible biologi-cal or genetic marker will also be contingent on diagnostic deci-sions. Using an explicit polydiagnostic approach (Farmer, Mc-
Guffin, & Gottesman, 1988) may be a useful strategy until theboundaries of the schizophrenia spectrum are more clearly de-fined.
Second, although it appears that neuroleptics may not affectoculomotor functioning (Abel & Hertle, 1988; Levy etal., 1984,1985; Spohn et al., 1988), there is suggestive evidence to thecontrary (Rea et al., 1989). Furthermore, other medicationsused in treating psychiatric patients, including benzodiazepines(Abel & Hertle, 1988), sedatives (Abel & Hertle, 1988; Levy etal., 1984), and lithium (Abel & Hertle, 1988; lacono et al.,1982; Levy et al., 1985) clearly affect eye movements. Medica-tion status, therefore, should be clearly documented. Third,there is suggestive evidence that tardive dyskinesia (TD) is asso-ciated with some EMD (Spohn, Coyne, Lacoursiere, Mazur, &Hayes, 1985; Spohn etal., 1988; Thaker, Nguyen, &Tamminga,1989a, 1989b). Spohn et al. (1985) reported that facial-oralTD, extremity TD, and sex accounted for approximately 20%of global EMD variance in a multiple regression analysis.Spohn et al. (1988) found a significant tendency for patientswith TD to substitute large, nontracking saccades for smoothpursuit when compared with non-TD patients. Although thistendency clearly does not represent all patients with TD, Spohnet al. (1988) suggested excluding severely dyskinetic patientsfrom future discriminant validity studies. Investigators mayalso want to exclude such patients from family studies wherethere is an interest in identifying genetic correlations (e.g., be-tween proband oculomotor functioning and family memberschizotypy).
Fourth, as many relatives as possible (16-65 years old or so,given developmental considerations; Hainline, 1988) should beincluded in family studies. These persons in most circum-stances should be thoroughly evaluated for schizophrenia-re-lated signs and symptoms. Fifth, because qualitative andquantitative aspects of oculomotor functioning are age-relatedphenomena (Hainline, 1988), control subjects should be age-matched to both patients and family members. They shouldalso be evaluated for schizophrenia-related signs and symp-toms, and screened for psychiatric illness in their first-degreefamily members. This would constitute what Tsuang, Fleming,Kendler, and Gruenberg (1988) have called a "highly screened"control group, a selection procedure that has greatest utilitywhen a researcher's goal is identification of variables document-ing differential liability between cases and noncases.
Biological Marker Status of EMD
The claim that EMD may serve as a biological marker forschizophrenia must be evaluated with reference to the researchbearing on the biological marker criteria (lacono, 1982b, 1983;Shields & Gottesman, 1973). First, EMD should be specific toschizophrenia. Discriminant validity studies clearly documenta higher prevalence of EMD among persons with schizophreniathan among normal persons and psychiatric patients with non-psychotic disorders. Patients with schizophrenia have been fre-quently reported to have less globally accurate smooth pursuit,lower pursuit gain, and more frequent saccades than normalcontrol subjects. Discrimination from other patient groups, es-pecially patients with bipolar affective and other psychotic dis-orders, has not been as consistent, although studies attempting

BRETT A. CLEMENTZ AND JOHN A. SWEENEY
to differentiate these groups by means of specific oculomotormeasures have not been published. Given that there are poten-tial state-related influences on oculomotor functioning, morestudies are needed to clarify the ability of HMD to discriminatebetween persons with schizophrenia and other, equally psychot-ically disturbed psychiatric patients. Likewise, studies of sac-cade dynamics and frequency of intrusive saccadic events inpatients with schizophrenia are equivocal. There is a need formore studies addressing the similarities and differences betweenpersons with schizophrenia and those with other psychoses,using both specific and global measures of oculomotor func-tioning.
Second, EMD should have temporal stability for persons withschizophrenia and for normal control subjects. Using global ac-curacy measures, oculomotor functioning appears to be rela-tively stable over time for normal subjects, but psychiatric pa-tients may show improvements on this measure contemporane-ous with clinical stabilization. The frequency of saccades seemsto remain relatively stable, although large saccade frequencymay decrease with repeated testing and neuroleptic treatment.There are also potential medication and TD effects on ocularmotility that require further investigation.
Attention enhancement and distraction may change oculo-motor functioning, but the mechanisms underlying their effecton EMD are probably complex. Attention enhancements mayelicit the "best" level of performance from subjects, and distrac-tions may elicit EMD, but whether such methodological twistswill aid the understanding of EMD in schizophrenia remainsuncertain. It is also unclear whether attention manipulationsdifferentially affect patients and normal subjects, which raises aquestion about EMD in schizophrenia's being solely a volitionalattention dysfunction. Of importance, only one study (Kauf-man & Abel, 1986) has reported results during either attentionenhancement or distraction based on specific eye movementscoring techniques. Until more studies are conducted, unravel-ing the significance of attention manipulation and distractionfor understanding EMD in normal and psychiatric populationsmay be difficult.
Third, EMD should have a higher prevalence in the familymembers of probands with schizophrenia than in both normalsubjects and family members of probands with other psychiat-ric disorders. This seems to be the case when both global accu-racy and specific oculomotor measures are used as the depen-dent variable. Clementz (in press) found, however, that both ASper cycle and pursuit gain were able to discriminate spectrumfrom nonspectrum relatives. Other forms of saccadic intru-sions, as well as RMS error deviation, were unable to accom-plish this task. Further research is needed to clarify the potentialimportance of this finding.
Fourth, EMD should be related to the presence of syndromaland subsyndromal manifestations of schizophrenia among fam-ily members of probands with this disorder (Cloninger, 1987;Goldin & Gershon, 1983). Clementz (in press) found relationsbetween both pursuit gain and AS per cycle and schizophrenia-related psychopathology. lacono et al. (1988) found that bothmembers of Bassett et al.'s (1988) pedigree with a partial tri-somy of Chromosome 5 and schizophrenia had globally definedEMD, whereas the three unaffected, nontrisomic members ofthat pedigree who were tested had globally intact oculomotor
functioning. These results might indicate that particular typesof oculomotor disturbance are related to schizophrenia's patho-physiology. Further research could usefully attempt to clarifythis possibility.
Fifth, EMD should have a relatively low base rate in the gen-eral population. The frequency of EMD in the general popula-tion is often considered to be roughly 8%. Using global accuracymeasures, the base rate of EMD seems to be highly variableacross laboratories. Studies carefully documenting base-ratefigures for more specific measures of oculomotor functions aresparse. More research addressing this issue is sorely needed.
Sixth, the specific EMD associated with schizophrenia shouldbe genetically determined. Studies using global accuracy mea-sures with normal twins, offspring of twins, twins in which atleast one member of the pair was affected with a psychosis, andfamily members of persons with schizophrenia strongly suggestthat ocular motility is at least partially genetically determined.Studies have not reported whether more specific types of oculo-motor abnormalities are also genetically determined (i.e., doSWJ occur with similar frequency in monozygotic twins? Ispursuit gain more similar in monozygotic vs. dizygotic twins?)
Finally, EMD should also be associated with schizophrenia-related psychopathology in the general population. There is sug-gestive evidence that this is the case. Because the correlations instudies addressing this topic are only between global accuracyof pursuit measures and psychopathology, however, whetherspecific EMDs (pursuit gain and AS frequency, for instance)are related to schizophrenia-related symptoms in the generalpopulation (as they seem to be in family members) is not yetknown.
This review of the literature on EMD in schizophrenia sug-gests that there is great promise for this variable's serving as abiological marker for this disorder. A solid foundation has beenlaid, on which a more complete understanding of EMD inschizophrenia can be constructed. Studies of ocular motilitythat use both global and specific measures may be most helpfulfor coming to understand the pathophysiology, genetics, and di-agnostic bandwidth of this complex disorder. Although globalmeasures have provided helpful clues, and may continue to doso, more specific oculomotor assessment techniques may benecessary to tease apart the intricacies of the relation betweenocular motility and schizophrenia.
References
Abel, L. A. (1986). Measuring smooth pursuit eye movement in psychi-atric populations. A merican Journal of Psychiatry, 143, 111.
Abel, L. A., & Hertle, R. W. (1988). Effects of psychoactive drugs onocular motor behavior. In C. W. Johnston & F. J. Pirozzolo (Eds.),Neuropsychology of eye movements (pp. 81-114). Hillsdale, NJ: Erl-baum.
Abel, L. A., & Ziegler, A. S. (1988). Smooth pursuit eye movements inschizophrenics—What constitutes quantitative assessment? Biologi-cal Psychiatry, 24, 747-762.
Acker, W., & Toone, B. (1978). Attention, eye tracking and schizophre-nia. British Journal of Social and Clinical Psychology, 17, 173-181.
Bahill, A. X, Clark, M. R., & Stark, L. (1975). The main sequence: Atool for studying human eye movements. Mathematical Biosciences,24, 191-204.
Bartfai, A., Levander, S. E., & Sedvall, G. (1983). Smooth pursuit eye

EMD IN SCHIZOPHRENIA 89
movements, clinical symptoms, CSF metabolites, and skin conduc-tance habituation in schizophrenia patients. Biological Psychiatry,75,971-987.
Bassett, A. S., McGillivray, B. C, Jones, B. D., & Pantzer, J. T. (1988).Partial trisomy of chromosome 5 cosegregating with schizophrenia.Lancet, i (8589), 799-801.
Benitez, J. T. (1970). Eye tracking and optokinetic tests: Diagnostic sig-nificance in peripheral and central vestibular disorders. Laryngo-scope, 80, 834-848.
Blackwood, D. H. R., St. Clair, D. M., & Muir, W. J. (1988). AuditoryP300 and smooth pursuit eye tracking abnormalities in schizo-phrenic subjects and their relatives. Schizophrenia Research, 1, 177-178.
Brezinova, V., & Kendell, R. E. (1977). Smooth pursuit eye movementsof schizophrenics and normal people under stress. Brinish Journal ofPsychiatry, 130, 59-63.
Bronstein, A. M., & Kennard, C. (1985). Predictive ocular motor con-trol in Parkinson's disease. Brain, 109, 159-180.
Byerley, W. F. (1989). Schizophrenia: Genetic linkage revisited. Nature,540,340-341.
Carl, J. R., & Gellman, R. S. (1987). Human smooth pursuit: Stimulus-dependent responses. Journal of Neurophysiology, 57, 1446-1463.
Cegalis, J. A., Hafez, H., & Wong, P. S. (1983). What is deviant aboutsmooth pursuit eye movements in schizophrenia? Psychiatry Re-search, 10, 47-58.
Cegalis, J. A., Leen, D., & Solomon, E. J. (1977). Attention in schizo-phrenia: An analysis of selectivity in the functional visual field. Jour-nal of Abnormal Psychology, 86, 470-482.
Cegalis, J. A., & Sweeney, J. A. (1979). Eye movements in schizophre-nia: A quantitative analysis. Biological Psychiatry, 14, 13-26.
Cegalis, J. A., & Sweeney, J. A. (1981). The effect of attention on smoothpursuit eye movements of schizophrenics. Journal of Psychiatric Re-search, 16, 145-161.
Cegalis, J. A., Sweeney, J. A., & Dellis, E. M. (1982). Refixation sac-cades and attention in schizophrenia. Psychiatry Research, 7, 189-198.
Chapman, L. J., & Chapman, J. P. (1985). Psychosis proneness. In M.Alpert (Ed.), Controversies in schizophrenia: Proceedings of the 74thannual meeting of the American Psychopathological Association (pp.157-174). New York: Guilford Press.
Clementz, B. A. (in press). Pursuit eye movement dysfunction as a bio-logical marker for schizophrenia (Doctoral dissertation, Kent StateUniversity, 1989). Dissertation Abstracts International.
Cloninger, C. R. (1987). Genetic principles and methods in high-riskstudies of schizophrenia. Schizophrenia Bulletin, 13, 515-524.
Couch, F. H., & Fox, J. C. (1934). Photographic study of ocular move-ments in mental disease. Archives of Neurology and Psychiatry, 34,556-578.
Dell'Osso, L. F., Abel, L. A., & Daroff, R. B. (1977). "Inverse latent"macro square wave jerks and macrosaccadic oscillations. Annals ofNeurology, 2,57.
Detera-Wadleigh, S. D., Goldin, L. R., Sherrington, R., Encio, I., deMiguel, C., Berrettini, W., Gurling, H., & Gershon, E. S. (1989). Ex-clusion of linkage to 5q 11 -13 in families with schizophrenia and otherpsychiatric disorders. Nature, 340, 391-393.
Diefendorf, A. R., & Dodge, R. (1908). An experimental study of theocular reactions of the insane from photographic records. Brain, 31,451-489.
Done, D. J., & Frith, C. D. (1984). Automatic and strategic control ofeye movements in schizophrenia. In A. G. Gale & F. Johnson (Eds.),Theoretical and applied aspects of eye movement research (pp. 481-487). Amsterdam: North-Holland.
Elidan, J., Gay, I., & Lev, S. (1984). Square wave jerks: Incidence, char-acteristic, and significance. Journal of Otolaryngology, 13, 375-381.
Erlenmeyer-Kimling, L. (1987). Biological markers for the liability toschizophrenia. In H. Helmchen & F. A. Henn (Eds.), Biological per-spectives of schizophrenia (pp. 33-56). New York: Wiley.
Faraone, S. V., & Tsuang, M. T. (1985). Quantitative models of the ge-netic transmission of schizophrenia. Psychological Bulletin, 98, 41-66.
Farmer, A. E., McGuffin, P., & Gottesman, I. I. (1988). In reply to"Twin studies and genetic models of schizophrenia" by D. F. Levin-son. Archives of General Psychiatry, 45, 877-878.
Fenton, W. S., McGlashen, T. H., & Heinssen, R. K. (1988). DSM-HI-R schizophrenia is too narrow. Paper presented at the annual meetingof the American Psychiatric Association, Montreal, Quebec, Canada,May 1988.
Freedman, R., Adler, L. E., Gerhardt, G. A., Waldo, M., Baker, N.,Rose, G. M., Drebing, C., Nagamoto, H., Bickford-Wimer, P., &Franks, R. (1987). Neurobiological studies of sensory gating inschizophrenia. Schizophrenia Bulletin, 13, 669-678.
Fukushima, J., Fukushima, K., Chiba, T, Tanaka, S., Yamashita, I., &Kato, M. (1988). Disturbances of voluntary control of saccadic eyemovements in schizophrenic patients. Biological Psychiatry, 23, 670-677.
Goldin, L. R., & Gershon, E. S. (1983). Association and linkage studiesof genetic marker loci in major psychiatric disorders. Psychiatric De-velopments, 4. 387-418.
Gottesman, 1.1., & McGue, M. (in press). Mixed and mixed-up modelsfor the transmission of schizophrenia. In D. Cichetti & W. Grove(Eds.), Thinking clearly about psychology: Essays in honor of Paul E.Meehl. Minneapolis: University of Minnesota Press.
Gottesman, 1.1., McGuffin, P., & Farmer, A. E. (1987). Clinical geneticsas clues to the "real" genetics of schizophrenia (A decade of modestgains while playing for time). Schizophrenia Bulletin, 13, 23-47.
Gottesman, 1.1., Shields, J., & Hanson, D. (1982). Schizophrenia: Theepigenetic puzzle. New York: Cambridge University Press.
Hainline, L. (1988). Normal lifespan developmental changes in saccadicand pursuit eye movements. In C. W. Johnston & F. J. Pirozzolo(Eds.), Neuropsychology of 'eye movements (pp. 31-64). Hillsdale. NJ:Erlbaum.
Herishanu, Y. Q, & Sharpe, J. A. (1981). Normal square wave jerks.Investigative Ophthalmology and Visual Science, 20, 268.
Holzman, P. S. (1975). Smooth-pursuit eye movements in schizophre-nia: Recent findings. In D. X. Freedman (Ed.), Biology of the majorpsychoses (pp. 217-231). New York: Raven Press.
Holzman, P. S. (1983). Methodological consensus in smooth pursuit eyemovements: Workshop contributions. Schizophrenia Bulletin, 9, 33-36.
Holzman, P. S. (1985). Eye movement dysfunctions and psychosis. In-ternational Review of Neurobiology, 27, 179-205.
Holzman, P. S. (1987). Recent studies of psychophysiology in schizo-phrenia. Schizophrenia Bulletin, 13,49-75.
Holzman, P. S., Kringlen, E., Levy, D. L., & Haberman, S. J. (1980).Deviant eye tracking in twins discordant for psychosis: A replication.Archives of General Psychiatry, 37, 627-631.
Holzman, P. S., Kringlen, E., Levy, D. L., Proctor, L. R., Haberman,S. J., & Yasillo, N. J. (1977). Abnormal-pursuit eye movements inschizophrenia: Evidence for a genetic indicator. Archives of GeneralPsychiatry, 34, 802-805.
Holzman, P. S., Kringlen, E., Matthysse, S., Flanagan, S. D., Lipton,R. B., Cramer, G., Levin, S., Lange, K., & Levy, D. L. (1988). A singledominant gene can account for eye tracking dysfunctions and schizo-phrenia in offspring of discordant twins. Archives of General Psychia-try, 45, 641-647.
Holzman, P. S., Levy, D. L., & Proctor, L. R. (1976). Smooth pursuiteye movements, attention, and schizophrenia. Archives of GeneralPsychiatry, 33, 1415-1420.

90 BRETT A. CLEMENTZ AND JOHN A. SWEENEY
Holzman, P. S., Levy, D. L., & Proctor, L. R. (1978). The several quali-ties of attention in schizophrenia. Journal of Psychiatric Research,14,99-110.
Holzman, P. S., Matthysse, S., & Levy, D. L. (1989). Eye tracking dys-function is associated with partial trisomy of chromosome 5 andschizophrenia: A response. Archives of General Psychiatry, 46, 756-757.
Holzman, P. S., Proctor, L. R., & Hughes, D. W. (1973). Eye trackingpatterns in schizophrenia. Science, 181, 179-181.
Holzman, P. S., Proctor, L. R., Levy, D. L., Yasillo, N. J., Meltzer, H. Y,& Hurt, S. W. (1974). Eye-tracking dysfunctions in schizophrenic pa-tients and their relatives. Archives of General Psychiatry, 31,143-151.
Holzman, P. S., Solomon, C. M., Levin, S., & Waternaux, C. S. (1984).Pursuit eye movement dysfunctions in schizophrenia: Family evi-dence for specificity. Archives of General Psychiatry, 41, 136-139.
lacono, W. G. (1982a). Eye tracking in normal twins. Behavior Genet-ics, 72,517-526.
lacono, W. G. (1982b). The genetics of psychopathology as a tool forunderstanding the brain: The search for a genetic marker of schizo-phrenia. In I. Lieblich (Ed.), Genetics and the brain (pp. 115-146).Amsterdam: Elsevier/North-Holland.
lacono, W. G. (1983). Psychophysiology and genetics: A key to psycho-pathology research. Psychophysiology, 20, 371-383.
lacono, W. G. (1985). Psychophysiologic markers of psychopathology:A review. Canadian Psychology, 26, 96-112.
lacono, W. G. (1988). Eye movement abnormalities in schizophrenicand affective disorders. In C. W. Johnston & F. J. Pirozzolo (Eds.),Neuropsychology of eye movements (pp. 115-145). Hillsdale, NJ: Erl-baum.
lacono, W. G., Bassett, A. S., & Jones, B. D. (1988). Eye tracking dys-function is associated with partial trisomy of chromosome 5 andschizophrenia. Archives of General Psychiatry, 45,1140-1141.
lacono, W. G., Bassett, A. S., & Jones, B. D. (1989). In reply. Archivesof General Psychiatry, 46, 757-758.
lacono, W. G., & Koenig, W. G. R. (1983). Features that distinguish thesmooth-pursuit eye-tracking performance of schizophrenic, affective-disorder, and normal individuals. Journal of Abnormal Psychology,92,29-41.
lacono, W. G., & Lykken, D. T. (1979a). Comments on "Smooth-pur-suit eye movements: A comparison of two measurement techniques"by Lindsey, Holzman, Haberman, and Yasillo. Journal of AbnormalPsychology, 88, 678-680.
lacono, W. G., & Lykken, D. T. (1979b). Electro-oculographic record-ing and scoring of smooth pursuit and saccadic eye tracking: A para-metric study using monozygotic twins. Psychophysiology, 16, 94-107.
lacono, W. G., & Lykken, D. T. (1979c). Eye tracking and psycho-pa-thology: New procedures applied to a sample of normal monozygotictwins. Archives of General Psychiatry, 36, 1361-1369.
lacono, W. G., & Lykken, D. T. (1981). Two-year retest stability of eyetracking performance and a comparison of electrc-oculographic andinfrared recording techniques: Evidence of EEG in the electro-oculo-gram. Psychophysiology, 18, 49-55.
lacono, W. G., & Lykken, D. T. (1983). The assessment of smooth track-ing dysfunction. Schizophrenia Bulletin, 9, 44-50.
lacono, W. G., Peloquin, L. J., Lumry, A. E., Valentine, R. H., & Tua-son, V. B. (1982). Eye tracking in patients with unipolar and bipolaraffective disorders in remission. Journal of Abnormal Psychology, 91,35-44.
lacono, W. G., Tuason, V. B., & Johnson, R. A. (1981). Dissociation ofsmooth-pursuit and saccadic eye tracking in remitted schizophrenics.Archives of General Psychiatry. 38, 991-996.
Kaufman, S. R., & Abel, L. A. (1986). Effects of distraction on smoothpursuit in normal subjects. Acta OtolaryngolfStockh.), 102, 57-64.
Kennedy, J. L., Giuffra, L. A., Moises, H. W., Cavalli-Sforza, L. L.,Pakstis, A. J., Kidd, J. R., Castiglione, C. M., Sjogren, B., Wetterberg,L., & Kidd, K. K. (1988). Evidence against linkage of schizophreniato markers on chromosome 5 in a northern Swedish pedigree. Nature,336, 167-170.
Klein, R. H., Salzman, L. F., Jones, F, & Ritzier, B. (1976). Eye-track-ing in psychiatric patients and their offspring. Psychophysiology, 13,186.
Kraepelin, E. (1971). Dementia praecox andparaphrenia(R. M. Bark-lay, Trans.). Huntington, NY: Krieger. (Original work published1919)
Kringlen, E. (1967). Heredity and environment in the functional psycho-ses. London: Heinemann.
Kuechenmeister, C. A., Linton, P. H., Mueller, T. V., & White, H. B.(1977). Eye tracking in relation to age, sex, and illness. Archives ofGeneral Psychiatry, 34, 578-579.
Kufferle, B., Grunberger, J., Linzmayer, L., & Saletu, B. (1988). Distinc-tion between positive and negative schizophrenia in the light of psy-chophysiological measurements. Schizophrenia Research, 1, 179-180.
Kuskowski, M. A. (1988). Eye movements in progressive cerebral neu-rological disease. In C. W. Johnston & F. J. Pirozzolo (Eds.), Neuro-psychology of eye movements (pp. 147-176). Hilldale, NJ: Erlbaum.
Leigh, R. J., & Zee, D. S. (1983). The neurology of eye movements.Philadelphia: F. A. Davis.
Levin, S. (1984). Frontal lobe dysfunction in schizophrenia—I. Eyemovement impairments. Psychiatry Research, 18, 27-55.
Levin, S., Holzman, P. S., Rothenberg, S. J., & Lipton, R. B. (1981).Saccadic eye movements in psychotic patients. Psychiatry Research,5, 47-58.
Levin, S., Jones, A. J., Stark, L., Merrin, E. L., & Holzman, P. S.(1982a). Identification of abnormal patterns in eye movements ofschizophrenic patients. Archives of General Psychiatry, 39, 1125-1130.
Levin, S., Jones, A., Stark, L., Merrin, E. L., & Holzman, P. S. (1982b).Saccadic eye movements of schizophrenic patients measured by re-flected light technique. Biological Psychiatry, 17, 1277-1287.
Levin, S., Lipton, R. B., & Holzman, P. S. (1981). Pursuit eye move-ments in psychopathology: Effects of target characteristics. BiologicalPsychiatry, 16, 255-267.
Levin, S., Luebke, A., Zee, D. S., Hain, T. C., Robinson, D. A., & Holz-man, P. S. (1988). Smooth pursuit eye movements in schizophrenics:Quantitative measurements with the search-coil technique. Journalof Psychiatric Research, 22, 195-206.
Levy, D. L., Dorus, E., Shaughnessy, R., Yasillo, N. J., Pandey, G. N.,Janicak, P. G., Gibbons, R. D., Gaviria, M., & Davis, J. M. (1985).Pharmacologic evidence for specificity of pursuit dysfunction toschizophrenia: Lithium carbonate associated with abnormal pursuit.Archives of General Psychiatry, 42, 335-341.
Levy, D. L., Lipton, R. B., Holzman, P. S., & Davis, J. M. (1983). Eyetracking dysfunction unrelated to clinical state and treatment withhalapetidol. Biological Psychiatry, 18, 813-819.
Levy, D. L., Lipton, R. B., Yasillo, N. J., Peterson, J., Pandey, G., &Davis, J. M. (1984). Psychotropic drug effects on smooth pursuit eyemovements: A summary of recent findings. In A. G. Gale & F. John-son (Eds.), Theoretical and applied aspects of eye movement research(pp. 497-505). Amsterdam: Elsevier.
Levy, D. L., Yasillo, N. J., Dorus, E., Shaughnessy, R., Gibbons, R. D.,Peterson, J., Janicak, P. G., Gaviria, M., & Davis, J. M. (1983). Rela-tives of unipolar and bipolar patients have normal pursuit. PsychiatryResearch, 10, 285-293.
Lindsey, D. T, Holzman, P. S., Haberman, S., & Yasillo, N. J. (1978).Smooth-pursuit eye movements: A comparison of two measurement
EMD IN SCHIZOPHRENIA 91
techniques for studying schizophrenia. Journal of Abnormal Psychol-ogy, 87,491-496.
Lipton, R. B., Frost, L. A., & Holzman, P. S. (1980). Smooth pursuiteye movements, schizophrenia, and distraction. Perceptual and Mo-tor Skills, 50, 159-167.
Lipton, R. B., Levin, S., & Holzman, P. S. (1980). Horizontal and verti-cal pursuit eye movements, the oculocephalic reflex, and the func-tional psychoses. Psychiatry Research, 3, 193-203.
Lipton, R. B., Levy, D. L., Holzman, P. S., & Levin, S. (1983). Eyemovement dysfunctions in psychiatric patients: A review. Schizo-phrenia Bulletin, 9, 13-32.
Lykken, D. T., lacono, W. G., & Lykken, J. D. (1981). Measuring devi-ant eye tracking. Schizophrenia Bulletin, 7, 204-205.
Mather, J. A. (1985). Eye movements of teenage children of schizo-phrenics: A possible inherited marker of susceptibility to the disease.Journal of Psychiatric Research, 19, 523-532.
Mather, J. A. (1986). Saccadic eye movements to seen and unseen tar-gets: Oculomotor errors in normal subjects resembling those ofschizophrenics. Journal of Psychiatric Research, 20, 1-8.
Mather, J. A., & Putchat, C. (1982-1983). Motor control of schizo-phrenics—I. Oculomotor control of schizophrenics: A deficit in sen-sory processing, not strictly in motor control. Journal of PsychiatricResearch, 77,343-360.
Mather, J. A., & Putchat, C. (1984). Motor control of schizophrenics—II. Manual control and tracking: Sensory and motor deficits. Journalof Psychiatric Research, 18, 287-298.
Matsue, Y., Okuma, T., Saito, H., Aneha, S., Ueno, T., Chiba, H., &Matsuoka, H. (1986). Saccadic eye movements in tracking, fixation,and rest in schizophrenic and normal subjects. Biological Psychiatry,21, 382-389.
Matthysse, S., & Holzman, P. S. (1987). Genetic latent structuremodels: Implication for research on schizophrenia. PsychologicalMedicine, 77,271-274.
Matthysse, S., & Holzman, P. S. (1989). In reply to McGue and Gottes-man. Archives of General Psychiatry, 46, 479-480.
Matthysse, S., Holzman, P. S., & Lange, K. (1986). The genetic trans-mission of schizophrenia: Application of Mendelian latent structureanalysis to eye tracking dysfunctions in schizophrenia and affectivedisorder. Journal of Psychiatric Research, 20, 57-76.
May, H. J. (1979). Oculomotor pursuit in schizophrenia. Archives ofGeneral Psychiatry, 36, 827.
McGue, M., & Gottesman, I. I. (1989). A single dominant gene stillcannot account for the transmission of schizophrenia. Archives ofGeneral Psychiatry, 46, 478-479.
Mialet, J. P., & Pichot, P. (1981). Eye-tracking patterns in schizophre-nia: An analysis based on the incidence of saccades. Archives of Gen-eral Psychiatry, 38, 183-186.
Nuechterlein, K. H. (1987). Vulnerability models for schizophrenia:State of the art. In H. Hafner, W. F. Gattaz, & W. Janzarik (Eds.),Search for the causes of schizophrenia (pp. 297-316). Berlin, W. Ger-many: Springer-Verlag.
Pass, H. L., Salzman, L. F., Klorman, R., Kaskey, G. B., & Klein, R. H.(1978). The effect of distraction on acute schizophrenics' visual track-ing. Biological Psychiatry, 13, 587-593.
Pivik, R. T. (1979a). Smooth pursuit eye movements and attention inpsychiatric patients. Biological Psychiatry, 14, 859-879.
Pivik, R. T. (1979b). Target velocity and smooth pursuit eye movementsin psychiatric patients. Psychiatry Research, 1, 313-323.
Rea, M. M., Sweeney, J. A., Solomon, C. M., Walsh, V., & Frances, A.(1989). Changes in eye tracking during clinical stabilization in schizo-phrenia. Psychiatry Research, 28, 31-39.
Robinson, D. A., Gordon, J. L., & Gordon, S. E. (1986). A model of thesmooth pursuit eye movement system. Biological Cybernetics, 55,43-57.
Ross, D. E., Ochs, A. L., Goldberg, S. C., Pandurangi, A. K., & Kendler,K. S. (1989). Abnormal oscillations in the slow pursuit eye move-ments of schizophrenic patients [abstract]. Schizophrenia Research,2,91.
Ross, D. E., Ochs, A. L., Hill, M. R., Goldberg, S. C., Pandurangi,A. K., & Winfrey, C. J. (1988). Erratic eye tracking in schizophrenicpatients as revealed by high-resolution techniques. Biological Psychi-atry, 24, 675-688.
St. Clair, D., Blackwood, D., Muir, W., Baillie, D., Hubbard, A., Wright,A., & Evans, H. J. (1989). No linkage of chromosome 5ql 1-13 mark-ers to schizophrenia in Scottish families. Nature, 339, 305-309.
Salzman, L. F, Klein, R. H., & Strauss, J. S. (1978). Pendulum eye-tracking in remitted psychiatric patients. Journal of Psychiatric Re-search, 14, 121-126.
Scarone, S., Gambini, Q, Hafele, E., Bellodi, L., & Smeraldi, E. (1987).Neurofunctional assessment of schizophrenia: A preliminary investi-gation of the presence of eye-tracking (SPEMs) and quality extinctiontest (QET) abnormalities in a sample of schizophrenic patients. Bio-logical Psychology, 24, 253-259.
Schmid-Burgk, W., Becker, W., Diekmann, V., Jurgens, R., & Korn-huber, H. H. (1982). Disturbed smooth pursuit and saccadic eyemovements in schizophrenia. Archiv fur Psychiatric und Nerven-krankheiten,232,m-W9.
Shagass, C., Amadeo, M., & Overton, D. A. (1974). Eye-tracking perfor-mance in psychiatric patients. Biological Psychiatry, 9, 245-260.
Shagass, C., Roemer, R. A., & Amadeo, M. (1976). Eye-tracking perfor-mance and engagement of attention. Archives of General Psychiatry,33, 121-125.
Sharpe, J. A., & Sylvester, T. O. (1978). Effects of aging on horizontalsmooth pursuit. Investigative Ophthalmology and Visual Science, 17,465-468.
Sherrington, R., Brynjolfsson, J., Petursson, H., Potter, M., Dudleston,K., Barraclough, B., Wasmuth, J., Dobbs, M., & Curling, H. (1988).Localization of a susceptibility locus for schizophrenia on chromo-some 5 [letter]. Nature, 336, 164-166.
Shields, J., & Gottesman, 1.1. (1973). Genetic studies of schizophreniaas signposts to biochemistry. In L. I. Iverson & S. P. R. Rose (Eds.),Biochemistry of Mental Illness (pp. 165-174). London: BiochemicalSociety.
Siegel, C., Waldo, M., Miznor, G., Adler, L. E., & Freedman, R. (1984).Deficits in sensory gating in schizophrenic patients and their relatives.Archives of General Psychiatry, 41, 607-612.
Siever, L. J., Coursey, R. D., Alterman, I. S., Buchsbaum, M. S., & Mur-phy, D. L. (1982). Psychological and physiological correlates of varia-tions in smooth pursuit eye movements. In E. Usdin & I. Hanin(Eds.), Biological markers in psychiatry and neurology (pp. 359-370).Elmsford, NY: Pergamon Press.
Siever, L. J., Coursey, R. D., Alterman, I. S., Buchsbaum, M. S., & Mur-phy, D. L. (1984). Impaired smooth pursuit eye movement: Vulnera-bility marker for schizotypal personality disorder in a normal volun-teer population. American Journal of Psychiatry, 141, 1560-1566.
Siever, L. J., Haier, R. J., Coursey, R. D., Sostek, A. J., Murphy, D. L.,Holzman, P. S., & Buchsbaum, M. S. (1982). Smooth pursuit eyetracking impairment: Relation to other "markers" of schizophreniaand psychobiologic correlates. Archives of General Psychiatry, 39,1001-1005.
Siever, L. J., van Kammen, D. P., Linnoila, M., Alterman, I., Hare, T,& Murphy, D. L. (1986). Smooth pursuit eye movement disorder andits psychobiologic correlates in unmedicated schizophrenics. Biologi-cal Psychiatry, 21, 1167-1174.
Simons, R. F, & Katkin, W. (1985). Smooth pursuit eye movementsin subjects reporting physical anhedonia and perceptual aberrations.Psychiatry Research, 14, 275-289.
Smith, G. N., & lacono, W. G. (1982). Evaluation of a sensitive and

92 BRETT A. CLEMENTZ AND JOHN A. SWEENEY
versatile method for measuring eye movements. Psychophysiology,19, 565.
Solomon, C. M., Holzman, P. S., Levin, S., & Gale, H. J. (1987). Theassociation between eye-tracking dysfunctions and thought disorderin psychosis. Archives of General Psychiatry, 44, 31-35.
Spohn, H. E., Coyne, L., Lacoursiere, R., Mazur, D., & Hayes, K.(1985). Relation of neuroleptic dose and tardive dyskinesia to atten-tion, information-processing, and psychophysiology in medicatedschizophrenics. Archives of General Psychiatry, 42, 849-859.
Spohn, H. E., Coyne, L., & Spray, J. (1988). The effect of neurolepticsand tardive dyskinesia on smooth-pursuit eye movement in chronicschizophrenics. Archives of General Psychiatry, 45, 833-840.
Spohn, H. E., & Patterson, T. (1979). Recent studies of psychophysiol-ogy in schizophrenia. Schizophrenia Bulletin, 5, 581 -611.
Spooner, J. W., Sakala, S. M., & Balogh, R. W. (1980). Effect of agingon eye tracking. Archives of Neurology, 37, 575.
Stephens, J. H., Astrup, C., Carpenter, W. X, Shaffer, J. W., & Goldberg,J. (1982). A comparison of nine systems to diagnose schizophrenia.Psychiatry Research, 6, 127-143.
Sweeney, J. A., Solomon, C. M., Rea, M., Mann, J. J., & Frances, A.(1987). Eye tracking abnormalities in schizophrenia. Paper presentedat the 95th annual meeting of the American Psychological Associa-tion, New York, September 1987.
Tellegan, A., & Atkinson, G. (1974). Openness to absorbing and self-altering experiences ("absorption"), a trait related to hypnotic sus-ceptibility. Journal of Abnormal Psychology, 83, 268-277.
Thaker, G. K., Nguyen, J. A., & Tamminga, C. A. (1989a). Increasedsaccadic distractibility in tardive dyskinesia: Functional evidence forsubcortical GABA dysfunction. Biological Psychiatry, 25, 49-59.
Thaker, G. K., Nguyen, J. A., & Tamminga, C. A. (1989b). Saccadicdistractibility in schizophrenic patients with tardive dyskinesia. Ar-chives of General Psychiatry, 46, 755-756.
Tomer, R., Mintz, M., Levy, A., & Myslobodsky, M. (1981). Smoothpursuit pattern in schizophrenic patients during cognitive task. Bio-logical Psychiatry, 16, 131-144.
Troost, B. X, Daroff, R. B., & Dell'Osso, L. F. (1974). Eye trackingpatterns in schizophrenia. Science, 184, 1202-1203.
Tsuang, M. X, Fleming, J. A., Kendler, K. S., & Gruenberg, A. S. (1988).Selection of controls for family studies. Archives of General Psychia-try, 45, 1006-1008.
van den Bosch, R. J., & Rozendaal, N. (1988). Subjective cognitive dys-function, eye tracking, and slow brain potentials in schizophrenic andschizoaffective patients. Biological Psychiatry, 24, 741-746.
van den Bosch, R. J., Rozendaal, N., & Mol, J. M. F. A. (1987). Symp-tom correlates of eye tracking dysfunction. Biological Psychiatry, 22,919-921.
Weinberger, D. R., & Wyatt, R. J. (1982). Cerebral ventricular size: Abiological marker for subtyping chronic schizophrenia. In E. Usdin& I. Hanin (Eds.), Biological markers in psychiatry and neurology(pp. 505-512). Elmsford, New York: Pergamon Press.
Weinreb, H. J. (1983). Saccadic intrusions in schizophrenia: Identitywith square- wave jerks? Archives of General Psychiatry, 40, 1343.
Whicker, L., Abel, L. A., & Dell'Osso, L. F. (1985). Smooth pursuit eyemovements in the parents of schizophrenics. Neuro-ophthalmology,5, 1-8.
White, H. R. (1938). Ocular pursuit in normal and psychopathologicalsubjects. Journal of Experimental Psychology, 22, 17-31.
Wirtschafter, J. D., & Weingarden, A. S. (1988). Neurophysiology andcentral pathways in oculomotor control: Physiology and anatomy ofsaccadic and pursuit eye movements. In C. W. Johnston & F. J. Piroz-zolo (Eds.), Neuropsychology of eye movements (pp. 5-30). Hillsdale,NJ: Erlbaum.
Yee, R. D., Balogh, R. W., Marder, S. R., Levy, D. L., Sakala, S. M., &Honrubia, V. (1987). Eye movements in schizophrenia. InvestigativeOphthalmology and Visual Science, 28, 366-374.
Young, L. R., & Sheena, D. (1975). Survey of eye movement recordingmethods. Behavior Research Methods & Instrumentation, 7, 397-429.
Received March 15,1989Revision received October 10,1989
Accepted November 2,1989