should duration of dual antiplatelet therapy depend on the type and/or potency of implanted stent? a...
TRANSCRIPT

CLINICAL RESEARCH
Should duration of dual antiplatelet therapydepend on the type andor potency of implantedstent A pre-specified analysis from thePROlonging Dual antiplatelet treatment afterGrading stent-induced Intimal hyperplasia studY(PRODIGY)Marco Valgimigli12 Marco Borghesi1 Matteo Tebaldi1 Pascal Vranckx3Giovanni Parrinello4 and Roberto Ferrari12 for the PROlonging Dual antiplatelettreatment after Grading stent-induced Intimal hyperplasia studY (PRODIGY)Investigators1Cardiology Department Cardiovascular Institute University of Ferrara Arcispedale S Anna Hospital Crso Giovecca 203 44100 Ferrara Italy 2Cardiovascular Research CentreSalvatore Maugeri Foundation IRCCS Lumezzane (BS) Italy 3Virga Jesse Ziekenhuis Hasselt Belgium and 4Medical Statistics Unit University of Brescia Italy
Received 29 August 2012 revised 14 November 2012 accepted 6 December 2012
Aims The purpose of this pre-specified analysis of the PROlonging Dual antiplatelet treatment after Grading stent-inducedIntimal hyperplasia studY (PRODIGY) was to assess device-specific outcomes relative to different duration of dualantiplatelet therapy (DAPT) after Everolimus- (EES) Paclitaxel (PES) Zotarolimus- (ZES-S) eluting or bare metalstents (BMS)
Methodsand results
We randomized 2013 patients to BMS ZES-S PES or EES implantation At 30 days each stent group underwent upto 6 or 24 months clopidogrel therapy The primary endpoint which was a composite of death myocardial infarctionor cerebrovascular accident did not differ in patients receiving BMS [HR 089 (95CI 054ndash145)] PES [HR 074(95CI 043ndash125)] or EES [HR 063 (95CI 033ndash121)] implantation across DAPT groups whereas it was sig-nificantly higher in ZES-S patients undergoing long when compared with short-term DAPT therapy (HR 285P frac14 00018) with positive interaction testing (P-value frac14 0004) At the 6-month landmark analysis heterogeneityacross stent types persisted for the primary study endpoint and other secondary clinical outcomes whereas patientsreceiving PES showed a significantly higher rate of definite probable and definite probable possible stent thrombosisin the short DAPT regimen No association in absolute or relative terms was noted between stent potency in inhibit-ing intimal hyperplasia and greater vulnerability to shorter DAPT therapy
Conclusion Our study suggests that optimal duration of DAPT may be stent-specific and it does not support a clear associationbetween stent potency and vulnerability to shorter DAPT therapyTrial Registration clinicaltrialsgov Identifier NCT00611286 httpclinicaltrialsgovct2showNCT00611286term=prodigyamprank=2
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Dual antiplatelet therapy dagger Clopidogrel dagger Stent dagger Percutaneous coronary intervention
Corresponding author Tel +39 0532 236874 Fax +39 0532 236593 Email vlgmrcunifeit
Published on behalf of the European Society of Cardiology All rights reserved amp The Author 2013 For permissions please email journalspermissionsoupcom
European Heart Journaldoi101093eurheartjehs460
European Heart Journal Advance Access published January 12 2013 at U
niversitAtilde degli Studi di B
rescia on January 16 2013httpeurheartjoxfordjournalsorg
Dow
nloaded from
IntroductionBased on the concerns that delayed vessel healing may be respon-sible for late or very late stent thrombosis drug-eluting stent im-plantation (DES) irrespective of which type should prompt atleast 121 or at least 6ndash12-month2 dual antiplatelet therapy(DAPT) duration Recent data suggest that at least some newergeneration DES lead to a more favourable healing profile3 andthey are associated to a lower incidence of early late and verylate stent thrombosis compared with first generation DES45
Therefore the need for prolonged DAPT may differ based onthe type of implanted stent
Retrospective analyses of randomized controlled trials and regis-try data have shown that 6-month or even shorter DAPT durationwas not associated with increased likelihood of thrombotic eventsat long-term follow-up after everolimus- or zotarolimus (Endeavorsprint)-eluting stent implantation67
These observations have recently led to a CE Mark in Europefor 3-month only DAPT duration after Xience Prime or theXience V everolimus-eluting coronary stent systems Yetwhether the need for prolonged DAPT should differ based onthe type of implanted stent remains a controversial issue due tothe paucity of prospective randomized data
The purpose of this pre-specified analysis of the PROlongingDual antiplatelet treatment after Grading stent-Induced Intimalhyperplasia studY (PRODIGY)89 was to assess device-specific out-comes relative to DAPT duration in an all-comer patient popula-tion randomly allocated to paclitaxel (PES) Zotarolimus- (ZES-S)or everolimus- (EES) eluting or bare metal stents (BMS) at thetime of intervention
Methods
Study design and populationPRODIGY is a 4-by-2 randomized multicentre open-label clinical trialdesigned to evaluate the efficacy and safety of prolonging the durationof clopidogrel therapy for up to 24 months in all comer patients re-ceiving a balanced mixture of stents with various anti-intimal hyperpla-sia potency and belonging to both first and second generationdrug-eluting stents8 Patients undergoing elective urgent or emergentcoronary angioplasty with intended stent implantation at three referralItalian sites were randomly assigned in a 1111 fashion to one of fourstent types including everolimus-eluting stent (EES) paclitaxel-elutingstent (PES) zotarolimus-eluting Endeavor Sprintwstent (ZES-S) orthin-strut bare metal stent
As stent chronic recoil is negligible late lumen loss (LLL ie the dif-ference in minimal lumen diameter at quantitative coronary angiog-raphy undertaken after stent implantation and at 6ndash9 monthfollow-up) of a given stent quantifies the amount of neontimal hyper-plasia which has grown towards the lumen thereby determiningin-stent restenosis Typical average late loss figures for the stentswhich were used in the present study are 100 mm for BMS (ie noactive inhibition of stent-induced intimal hyperplasia) 065 mm forZES-S 04 mm for PES and 020 mm for EES At 30 days patients ineach stent group were randomized in a balanced fashion to either 6or 24 months of dual antiplatelet treatment In the 6-month DAPTgroup clopidogrel discontinuation at any time after 30 days wasallowed in patients who were randomized to bare metal stent if
coronary intervention was indicated by the presence of stable coron-ary artery disease
Individuals eligible for enrolment were patients 18 years of age orolder with chronic stable coronary artery disease or acute coronarysyndromes including non-ST-elevation and ST-elevation myocardialinfarction They were eligible if they had at least one lesion with adiameter stenosis of 50 or more that was suitable for coronarystent implantation in a vessel with a reference vessel diameter of atleast 225 mm Selection criteria were broad reflecting routine clinicalpractice We set no limit for the number of treated lesions vessels orlesion length and excluded no patients on the basis of comorbid dis-orders or age apart from the following pre-specified criteria knownallergy to acetyl salicylic acid or clopidogrel planned surgery within24 months of percutaneous coronary intervention unless the DAPTcould be maintained throughout the perisurgical period history ofbleeding diathesis major surgery within 15 days active bleeding orprevious stroke in the last 6 months concomitant or foreseeableneed for oral anticoagulation therapy pregnancy life expectancy24 months participation in another trial and inability to provideinformed consent
The Ethics Committees of the three participating centres independ-ently approved the protocol and all participants gave written informedconsent
Treatment protocol and follow-upproceduresAll patients received aspirin (160ndash325 mg orally or 500 mg iv as aloading dose and then 80ndash160 mg orally indefinitely) and clopidogrel(300 or 600 mg orally as a loading dose) and then 75 mgday forthe treatment duration according to the randomization scheme asfollows for either 6 months in the 6-month dual antiplateletgroupmdashin patients randomized to bare metal stent and presentingstable coronary artery disease a shorter (but not 30 day) durationof dual antiplatelet treatment was allowed to comply with available evi-dencemdashor 24 months in the 24-month dual antiplatelet arm irrespect-ive of the previously implanted stent type or indication to the coronaryprocedure
Anticoagulation during coronary intervention was accomplishedthrough administration of either unfractionated heparin or bivalirudinAll interventions were performed according to current standard guide-lines2 and the final interventional strategy including administration ofglycoprotein IIbIIIa antagonists pre- or post-dilatation or use of intra-vascular imaging techniques was left entirely to the discretion of theoperator except for the stent utilization Angiographic success wasdefined as residual stenosis 30 by visual analysis in the presenceof TIMI 3 grade flow
Follow-upAll randomized patients who were not lost-to-follow-up irrespectiveof their compliance to the assigned treatment schedule returned forstudy visits at 30 days and then every 6 months up to 2 yearsDuring follow-up visits patients were examined assessed foradverse events and 12-lead ECG recordings At all follow-up time-points patients were questioned on their compliance with the studymedication Any interruptions or termination as well as the reasonsfor this were documented To ensure a high adherence rate to theassigned study treatment a dedicated study nurse per site was tele-phonically contacting each patient on a monthly basis
M Valgimigli et alPage 2 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Study endpointsThe primary endpoint of this analysis was to evaluate the interactionwith stent type on the effect of short- vs long-term DAPT and out-comes with respect to the incidence of death from any cause non-fatalmyocardial infarction or cerebrovascular accident
As the therapy did not differ between the two groups in the firstmonth after stenting the time frame of major interest for theprimary endpoint was from 30 days to 24 months
Secondary endpoints included each component of the primary end-point cardiovascular death the incidence of stent thrombosis definedbased on the Academic Research Consortium (ARC) criteria10 for theentire duration of follow-up or from 6 months onwards
All study endpoints were confirmed on the basis of documentationcollected at each hospital and were centrally adjudicated by the clinicalevents committee whose members were unaware of patientsrsquotreatment-group assignments
Statistical analysisCategorical variables were expressed as frequency (percentage)whereas continuous variables were expressed as mean+ SD Baselinecontinuous variables were compared between randomized groupsusing the Wilcoxonrsquos rank sums test or the ANOVA test whereasfor baseline binary variables the likelihood-ratio chi-square test orFisherrsquos exact test was used
Estimation of the cumulative major adverse cardiovascular eventrate was done with the KaplanndashMeier method and events were com-pared by the log rank test Hazard ratios (HRs) with 95 confidenceintervals (CIs) were calculated as long-term clopidogrel vs short-termclopidogrel (ie values 1 indicating increased hazard in the long-termgroup) using a proportional hazards model The proportionalityassumptions were met as they were checked by visual estimationafter plotting the log Cumulative Hazard vs (log) time at follow-upafter index procedure and by applying a test for non-proportionalhazards using the Schoenfeld residuals as previously described11
which failed to reject the null hypothesis that event rate was affectedby time We performed a univariate Cox-regression analysis with inter-action testing to determine whether the effect of duration of DAPT onthe efficacy and safety endpoints at 2 year was consistent across stenttypes Interaction tests were done with likelihood-ratio tests of the nullhypothesis that the interaction coefficient is zero
In our analyses we define landmark time and study outcomes interms of their elapsed time from a patientrsquos index procedure Onelandmark was used in this study at 6-months alive patients completing6-month follow-up were analysed with respect to events occurringafter this timepoint and up to 24 months as per randomizationscheme (ie by stent type and DAPT duration) according to the inten-tion to treat principle Finally an explorative per protocol analysis fo-cusing on patients who permanently discontinued clopidogrel after 6months in the 6-month DAPT group vs those who never interruptedclopidogrel therapy either permanently or temporarily during thecourse of follow-up in the 24-month DAPT arm was also performed
A two-sided P-value 005 was considered significant All analysescarried out based on the intention to treat principle were performedusing STATA version 111 (Stata Corp College Station TX USA)
ResultsFrom December 2006 to December 2008 a total of 2789 patientsunderwent screening and 2013 were finally recruited into thestudy and randomized to receive one of the four stent typesThirty-three (16) patients died within 30 days and 10 patients
withdrew consent therefore 1970 patients were randomly allo-cated at 1 month to undergo 24-month vs 6-month duration ofclopidogrel therapy
The four-stent groups further stratified based on the differentDAPT duration arms were well balanced with regards to baselineand angiographic characteristics (Tables 1 and 2) with the only ex-ception of circumflex artery being more frequently treated in thepaclitaxel- and everolimus-eluting stent groups undergoing6-month DAPT compared with other treatment groups
Adherence to aspirin therapy during the course of the study washigh and it did not differ across stent groups whereas the vast ma-jority of BMS- and DES-treated patients in short-term DAPT armdiscontinued clopidogrel before or at 6-month follow-up respect-ively (Table 3)
Follow-up and clinical outcomesClinical follow-up at 2 years was complete for 997 of patients inthe long-term clopidogrel group and for 996 of those in theshort-term clopidogrel group
Table 4 shows cumulative 24-month event rates for each stentgroup There was a clear signal of heterogeneity for the primaryendpoint of death for any cause non-fatal myocardial infarctionand cerebrovascular accident across stent groups with respect tothe duration of DAPT (P-value for interaction frac14 0004) Theprimary outcomes did not formally differ in patients receivingBMS [HR 089 (95CI 054ndash145) P frac14 064] PES [HR 074(95CI 043ndash125) P frac14 026] or EES [HR 063 (95CI 033ndash121) P frac14 017] implantation across DAPT groups whereas itwas significantly lower in ZES-S patients undergoing short- whencompared with long-term DAPT therapy [HR 285 (95CI149ndash545) P frac14 00018] (Figure 1) Consistent findings wereobserved with respect to the composite of death for any causeor MI and for cardiovascular death or MI (Figure 1) The analysisof stent thrombosis endpoints did not formally disclose heterogen-eity across stent groups The analysis of definite and definite orprobable ST showed no event in the short-term DAPT group ofpatients receiving ZES-S and an excess of thrombotic events inpatients treated with PES receiving a short when compared witha long course of DAPT therapy which did not reach statistical sig-nificance (HR 020 95CI 002ndash169 P frac14 014 and HR 04495CI 014ndash143 P frac14 015 respectively Figure 2)
Landmark and per protocol analysisThere were 1924 patients reaching the 6-month follow-up ofwhom 963 were allocated to the 24-month DAPT group and961 to the short-term clopidogrel duration arm
The incidence of the primary composite endpoint from 6 to 24months consistently showed heterogeneity with respect to theprimary composite endpoint (P-value for interaction frac14 005) aswell as for any death or MI (P-value for interaction frac14 010) or car-diovascular death or MI (P-value for interaction frac14 003) withpatients receiving ZES-S showing lower event rates in the short-when compared with the long-term DAPT duration groups(Figure 3) Results were consistent when the primary study end-point from 30 days (P-value for interaction 00002) or from 6 to24 months (P-value for interaction 001) was assessed at perprotocol analysis
Dual antiplatelet therapy and stent-type Page 3 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
The composite of definite or probable [HR 012 (95CI 002ndash100) P frac14 0049] and definite probable or possible ST [HR 025(95CI 007ndash088) P frac14 0031] were both significantly lower inthe 24-month DAPT arm in patients receiving PES but not inthose treated for the other stent types (Figure 4) Yet no formalsignal for interaction was noted for stent thrombosis endpointsacross DAPT groups for each stent-type which suggests a lackof study power for this analysis (there were only three definiteprobable or possible ST events in the long when compared with12 in the short-term DAPT group in the PES arm) or the factthat results for stent thrombosis endpoints across stent groupsare consistent with the overall study findings
At per protocol analysis a consistent signal of heterogeneityacross stent types for the definite probable or possible ST wasalso observed (P-value frac14 007)
Stent potency and outcomes in relationto DAPT durationThe re-intervention rates in the target lesion(s) from 30 daysonwards was 159 in the BMS 114 in the ZES-S 60 in thePES and 49 in the EES groups (P00001 for the trend)which is consistent with the expected stent efficacy profiles
based on previously reported stent-specific late loss figuresSetting BMS as reference group ZES-S PES or EES implantationresulted in a relative risk reduction for TLR in the range of 29(95CI 129ndash555) 63 (95CI 384ndash873) or 69 (95CI460ndash936) respectively (Figure 5)
As shown in Figure 5 the relative risks of death non-fatal myo-cardial infarction or non-fatal stroke from 6 months onwards (iewhen DAPT largely differed in the two DAPT treatment groups) aswell as the 6-month landmark definite probable or possible stentthrombosis rates in the short when compared with the long-termDAPT group was not affected by the actual (ie based on theobserved TLR rates in the study) or expected (ie based on lateloss figures in previously reported studies) potency of each stenttype to inhibit intimal hyperplasia
DiscussionWe found that the composite of death myocardial infarction orcerebrovascular accident did not differ in patients receiving BMSPES or EES implantation across DAPT groups whereas it was sig-nificantly lower in ZES-S patients undergoing short when com-pared with long-term DAPT therapy with positive interaction
Table 1 Base-line characteristics of the patients
Characteristics 24-month clopidogrel 6-month clopidogrel P-value
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Age (year) 69+11 67+11 67+12 68+11 68+11 68+12 68+11 68+11 032
Male sex n () 181 (74) 195 (79) 191 (78) 197 (79) 174 (71) 190 (78) 187 (76) 196 (79) 026
Body mass index (kgm2) 29+5 27+4 27+4 28+4 27+4 28+4 28+5 27+4 067
Diabetes n () 62 (25) 60 (24) 68 (28) 54 (22) 48 (20) 58 (24) 69 (28) 58 (24) 036
Insulin-dependent n () 12 (5) 20 (8) 18 (7) 9 (4) 9 (4) 17 (7) 12 (5) 17 (7) 024
Hypertension n () 180 (73) 177 (71) 181 (74) 183 (74) 188 (76) 159 (65) 177 (72) 169 (68) 019
Hyperlipidaemia n () 124 (50) 138 (56) 137 (56) 154 (62) 124 (50) 122 (50) 140 (57) 139 (56) 009
Current smoking n () 61 (25) 58 (23) 49 (20) 54 (22) 63 (26) 67 (28) 60 (24) 57 (23) 056
Creatinine clearance (mLmin) 77+31 80+36 81+33 80+34 78+29 79+31 77+29 77+32 053
Prior MI n () 61 (25) 64 (26) 82 (33) 63 (25) 56 (23) 67 (27) 56 (23) 79 (32) 051
Prior CABG n () 24 (10) 23 (9) 31 (13) 32 (13) 19 (8) 34 (14) 23 (9) 29 (12) 029
Prior stroke or TIA n () 9 (4) 8 (3) 9 (4) 11 (4) 11 (4) 9 (4) 9 (4) 10 (4) 087
LVEF 50+11 52+10 50+10 51+10 51+10 50+11 51+11 50+10 016
Clinical presentation n ()
Stable angina pectoris 57 (23) 65 (26) 75 (31) 58 (23) 56 (23) 65 (27) 68 (28) 61 (25) 049
Acute Coronary syndrome 189 (77) 183 (74) 170 (69) 190 (77) 191 (78) 180 (73) 176 (72) 186 (76) 058
Non-ST-elevation ACS 107 (43) 95 (38) 101 (41) 108 (44) 102 (41) 96 (39) 102 (42) 106 (43) 066
Unstable angina 50 (19) 39 (16) 44 (18) 52 (21) 43 (17) 53 (22) 39 (16) 47 (19) 055
Non-ST-elevation MI 57 (23) 56 (23) 57 (23) 56 (23) 59 (24) 43 (18) 63 (26) 59 (24) 068
ST-segment-elevation MI 82 (33) 88 (35) 69 (28) 82 (33) 89 (36) 84 (34) 74 (30) 80 (32) 076
Angiographic features n ()
Single-vessel disease 87 (35) 78 (32) 69 (28) 68 (27) 83 (34) 61 (25) 79 (32) 76 (31) 018
Multi-vessel disease 159 (65) 170 (69) 176 (72) 180 (73) 163 (66) 184 (75) 166 (68) 171 (69)
ACS acute coronary syndrome LVEF left-ventricular ejection fraction
M Valgimigli et alPage 4 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Table 2 Procedural results
Characteristic 24-month clopidogrel 6-month clopidogrel P-value
BMS (n 5 246) ZES (n 5 248) PES (n 5 245) EES (n5 248) BMS (n5 246) ZES (n 5 245) PES (n 5 245) EES (n 5 247)
Number of treated lesions 147+08 153+09 151+09 151+08 148+08 160+10 164+10 156+09 035
ge2 treated lesions n () 85 (35) 97 (39) 83 (34) 100 (40) 83 (34) 92 (38) 104 (42) 92 (37) 038
ge3 treated lesions n () 23 (9) 28 (11) 29 (12) 28 (11) 23 (9) 31 (13) 33 (14) 28 (11) 082
ge4 treated lesions n () 8 (3) 13 (5) 12 (5) 5 (2) 7 (3) 14 (6) 11 (4) 12 (5) 034
LAD treated n () 150 (61) 146 (59) 136 (56) 141 (57) 137 (56) 149 (61) 142 (58) 146 (59) 043
CFX treated n () 66 (27) 69 (28) 84 (34) 102 (41) 81 (33) 78 (32) 76 (31) 83 (34) 003
RCA treated n () 87 (35) 92 (37) 88 (36) 79 (32) 98 (40) 86 (35) 84 (34) 95 (38) 070
SVG treated n () 5 (2) 6 (2) 6 (2) 6 (2) 4 (2) 5 (2) 3 (1) 5 (2) 073
At least one complex (type B2 or C)lesion n ()a
152 (62) 168 (68) 164 (67) 158 (64) 160 (65) 175 (71) 175 (71) 154 (62) 014
Total ACCAHA scoreab 37+21 37+22 38+23 39+22 37+22 39+23 39+23 40+24 028
Number of stents implanted 182+12 191+13 181+13 177+11 177+11 196+13 188+12 196+13 034
Length of stent (mm) 39+35 41+32 39+29 37+24 36+25 42+30 40+27 42+32 013
Quantitative coronary analysis
Lesion length (mm) 1307+845 1318+832 1409+951 1313+835 1351+825 1323+824 1375+898 1427+864 049
RVD before (mm) 264+054 264+051 269+053 263+056 267+053 261+063 260+053 268+053 031
MLD before (mm) 060+039 061+038 058+041 059+041 056+041 056+041 055+037 058+036 066
Stenosis before () 78+14 77+13 79+14 78+16 79+14 77+17 78+14 79+12 055
RVD after (mm) 276+050 274+042 286+047 276+050 279+046 279+054 279+051 279+048 047
MLD after (mm) 242+056 246+046 253+046 245+049 244+049 247+054 242+053 252+046 027
Stenosis after () 1057+825 968+874 1001+748 1104+867 1129+841 1025+799 1113+876 1145+933 032
aCalculated in 952 patients in the 24-month clopidogrel arm and in 943 patients in the 6-month clopidogrel arm who presented at least one de-novo lesion ACCAHA score was missing in three patientsLAD left anterior descending artery CFX circumflex artery RCA right coronary artery LMCA left main coronary artery SVG saphenous vein graftbAs previously described18 type A stenoses were coded 1 point typeB1 stenoses 2 points type B2 stenoses 3 points and type C stenoses 4 points
Dualantiplatelet
therapyand
stent-typeP
age5
of
11
at UniversitAtilde degli Studi di Brescia on January 16 2013 httpeurheartjoxfordjournalsorg Downloaded from
testing At the 6-month landmark analysis heterogeneity acrossstent types persisted whereas patients receiving PES showed a sig-nificantly higher rate of stent thrombosis in the short DAPTregimen No association was noted between expected or actualstent potency in inhibiting intimal hyperplasia and greater vulner-ability to shorter DAPT therapy
The main findings of our analysis challenge current recommen-dations endorsing a clear-cut dichotomy of BMS vs DES for theneed of prolonged DAPT after stenting Furthermore our datasuggest minimal duration of clopidogrel therapy may differamong DES irrespective of stent potency in inhibiting intimalhyperplasia
As previously reported9 no interaction was noted between BMSand the three different DES type clustered together with respectto duration of DAPT therapy On the other hand in the currentanalysis focusing on each DES type individually a clear andformal signal of heterogeneity with respect to overall death myo-cardial infarction or cerebrovascular accidents was noted for theneed of prolonged therapy with clopidogrel after interventionThis was driven by ZES-S treated patients showing an improvedprimary study and other secondary clinical outcomes with short-term DAPT when compared with 24-month duration of therapyand by an excess of stent thrombosis events particularly definiteor probable and definite probable or possible ST in patients
Table 3 Use of anti-platelet medications during the trial
24-month clopidogrel 6-month clopidogrel P-value
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Anti-platelet therapy at 30 days n ()
Numberevaluated
246 248 245 248 246 245 245 247
Aspirin 246 (100) 248 (100) 245 (100) 248 (100) 246 (100) 245 (100) 245 (100) 247 (100) 099
Clopidogrel 245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Aspirin andclopidogrel
245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Anti-platelet therapy at 6 months n ()
Numberevaluated total
241 241 238 246 240 244 239 240
Aspirin 240 (996) 240 (996) 234 (983) 246 (100) 236 (983) 241 (988) 238 (996) 238 (996) 024
Clopidogrel 239 (992) 239 (992) 237 (976) 245 (996) 94 (392) 241 (988) 234 (979) 236 (983) 0001
Aspirin andclopidogrel
238 (988) 238 (988) 233 (979) 245 (996) 97 (392) 238 (976) 233 (975) 235 (979) 0001
Anti-platelet therapy at 12 months n ()
Numberevaluated total
236 238 231 243 232 240 233 237
Aspirin 233 (987) 237 (996) 226 (978) 243 (100) 223 (961) 236 (983) 231 (991) 235 (992) 012
Clopidogrel 233 (987) 232 (975) 228 (987) 239 (983) 8 (35) 12 (5) 7 (3) 6 (25) 0001
Aspirin andClopidogrel
230 (975) 231 (971) 223 (965) 239 (984) 8 (35) 12 (5) 6 (26) 6 (25) 0001
Anti-platelet therapy at 18 months n ()
Numberevaluated total
234 234 227 238 231 239 228 234 034
Aspirin 232 (992) 232 (992) 223 (982) 234 (983) 221 (957) 232 (971) 226 (992) 233 (996) 012
Clopidogrel 231 (987) 222 (989) 220 (969) 231 (971) 2 (09) 2 (09) 3 (13) 1 (04) 0001
Aspirin andclopidogrel
229 (979) 221 (944) 216 (952) 229 (962) 2 (09) 1 (04) 2 (09) 1 (04) 0001
Anti-platelet therapy at 24 months n ()
Numberevaluated total
230 228 224 238 227 237 226 230
Aspirin 228 (991) 224 (983) 219 (978) 234 (983) 216 (952) 230 (971) 221 (978) 229 (996) 019
Clopidogrel 226 (983) 212 (93) 214 (955) 228 (958) 0 2 (08) 3 (13) 0 0001
Aspirin andclopidogrel
224 (974) 210 (921) 211 (942) 226 (947) 0 1 (04) 2 (09) 0 0001
M Valgimigli et alPage 6 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
undergoing 6-month clopidogrel therapy after PES implantationcompared with a longer duration of therapy
In our study adherence to aspirin and clopidogrel was similarlyhigh in the first 6 months after DES implantation in the two DAPTgroups Therefore events occurring during this time period in thethree DES groups may potentially confound the outcomes of thetwo different DAPT regimens tested in the study Based on thisnotion a landmark analysis focusing on events occurring after a6 month-follow-up has been pre-specified and previously reportedfor the whole patient population or for all DES treated patientsclustered together When the three tested DES types were ana-lysed separately at the 6-month landmark analysis the resultswere largely consistent with the findings observed for the entirefollow-up duration (i) patients treated with ZES-S showed abetter ischaemic outcomes in the 6-month when compared withthe 24-month DAPT groups (ii) event rates for the primary or sec-ondary ischaemic clinical endpoints were similar between DAPTgroups after BMS or EES implantation (iii) the primary clinicalcomposite endpoint trended higher and the ST rates were signifi-cantly increased in PES treated patients receiving PES and
undergoing 6-month when compared with 24-month duration ofclopidogrel
Kandzari et al6 recently analysed outcomes in 2032 patientsundergoing coronary revascularization with ZES-S in five trialswho for various reasons discontinued DAPT at 6 months andfound that outcomes did not differ compared with patients whoreceived longer clopidogrel therapy (up to 12 or 24 months)
In the Real Safety and Efficacy of 3-Month Dual AntiplateletTherapy Following Zotarolimus-Eluting Stent Implantation(RESET) trial of 2148 patients randomized to the ZES-S stentand three months of DAPT and 1058 patients treated with stand-ard 12-month DAPT and other DES the combined endpoint ofany death MI stent thrombosis occurred in 13 in the standardtherapy arm vs 08 in the 3-month group (P frac14 048)12 Interest-ingly prospective studies undertaken to evaluate the degree ofZES-S stent coverage have consistently showed a very low rateof uncoveredmalapposed struts at 6- or even 3-month optical co-herence tomography evaluation which favourably compared withboth first generation DES or even BMS13 ndash15 Based on thisfinding the Zotarolimus-eluting stent in uncertain DES candidates
Table 4 Outcome rates at 24 months according to treatment group
Outcome 24-month clopidogrel 6-month clopidogrel
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Death for any cause myocardialinfarction or cerebrovascularaccident
29 (118) 33 (133) 23 (94) 15 (61) 32 (13) 12 (49) 31 (127) 23 (91)
Death for cardiovascular causemyocardial infarction orcerebrovascular accident
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (56)
Death for any cause ormyocardial infarction
25 (102) 27 (109) 22 (89) 14 (57) 30 (122) 12 (49) 31 (127) 21 (85)
Death for cardiovascular causemyocardial infarction
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (53)
Death for any cause 16 (65) 20 (81) 19 (78) 10 (4) 20 (81) 8 (33) 20 (82) 17 (69)
Death for cardiovascular cause 9 (37) 13 (52) 10 (41) 4 (16) 12 (49) 7 (29) 12 (49) 6 (24)
Myocardial infarction 14 (57) 12 (48) 9 (37) 4 (16) 15 (61) 4 (16) 14 (57) 8 (32)
Cerebrovascular accident 7 (28) 7 (28) 5 (2) 1 (04) 5 (2) 1 (04) 4 (16) 2 (08)
Definite stent thrombosis
Late 3 (12) 2 (08) 1 (04) 0 (0) 1 (04) 0 (0) 2 (08) 1 (04)
Very late 0 (0) 1 (04) 0 (0) 1 (04) 0 (0) 0 (0) 3 (13) 0 (0)
Cumulative 3 (12) 3 (12) 1 (04) 1 (04) 1 (04) 0 (0) 5 (2) 1 (04)
Definite or probable stent thrombosis
Late 5 (2) 2 (08) 3 (12) 0 (0) 5 (2) 0 (0) 3 (12) 1 (04)
Very late 0 (0) 1 (04) 1 (04) 1 (04) 0 (0) 0 (0) 6 (26) 0 (0)
Cumulative 5 (2) 3 (12) 4 (16) 1 (04) 5 (2) 0 (0) 9 (37) 1 (04)
Definite probable or possible stent thrombosis
Late 7 (28) 8 (32) 8 (32) 3 (12) 10 (41) 4 (16) 10 (41) 4 (16)
Very late 2 (08) 5 (21) 3 (13) 2 (08) 5 (21) 3 (13) 8 (34) 2 (08)
Cumulative 9 (37) 13 (52) 11 (45) 5 (2) 15 (61) 7 (29) 18 (74) 6 (24)
Dual antiplatelet therapy and stent-type Page 7 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 1 Stent analyses of the primary study endpoint and other secondary clinical outcomes Stent-specific analyses are shown with hazardratios and 95 confidence intervals for the primary end point of death for any cause myocardial infarction (MI) or cerebrovascular accident(CVA) death or MI and cardiovascular (CV) death or MI among patients randomly assigned to either the six or the 24-month clopidogreltherapy The P-value for interaction represents the likelihood of interaction between the variable and the relative treatment effect
Figure 2 Stent analyses of the stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95 confidence inter-vals for the definite definite probable and definite probable possible stent thrombosis (ST) among patients randomly assigned to either the 6or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction between the variable and the relativetreatment effect
M Valgimigli et alPage 8 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 3 Stent analyses of the 6-month landmark primary study endpoint and other secondary clinical outcomes Stent-specific analyses areshown with hazard ratios and 95 confidence intervals for the 6-month landmark analyses of the primary endpoint of death for any causemyocardial infarction (MI) or cerebrovascular accident (CVA) death or MI and cardiovascular (CV) death or MI among patients randomlyassigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction betweenthe variable and the relative treatment effect
Figure 4 Stent analyses of the 6-month landmark stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95confidence intervals for the 6-month landmark analyses of definite definite probable and definite probable possible stent thrombosis (ST)among patients randomly assigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihoodof interaction between the variable and the relative treatment effect
Dual antiplatelet therapy and stent-type Page 9 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
(ZEUS) study is comparing ZES-S vs BMS in patients at highthrombotic bleeding or low restenosis risk allowing 1-monthDAPT duration in both stent arms in patients who cannot toleratelonger duration of therapy (NCT01385319)
Reassuring data on the safety of early DAPT discontinuationafter EES have also been reported by a retrospective analysis ofregistry data7 Moreover the pooled analysis of SPIRIT II III IVand COMPARE Trials of 6789 patients showed a persistentlylow ST rate in patients treated with EES but not PES who discon-tinued DAPT after 6 months which is consistent with our currentfindings16 Indeed while our analysis on primary study endpointand other secondary clinical outcomes numerically favoured long-term DAPT after EES implantation the stent thrombosis endpointsand 6-month clinical landmark analyses revealed no excess ofevents in the 6-month DAPT group compared with longer-termclopidogrel therapy which is at variance with the results observedafter PES implantation
The need for prolonged DAPT has been suggested to be in-versely related to stent late loss17 Potent inhibition of intimal
hyperplasia might more frequently lead to incomplete stent cover-age andor late stent mal-apposition requiring a more prolongedcourse of intensified anti-platelet therapy to maintain stentsafety17
Our study by randomizing patients to a balanced mixture ofstents with various anti-intimal hyperplasia and each stent groupto 6- vs 24-month DAPT duration offers no evidence supportingthe association between stent-related late-loss and need for pro-longed DAPT On the contrary the results of our explorativeyet pre-specified analysis suggest that the minimal DAPT durationmay be stent-specific and not clearly related to stent potencytowards inhibition of intimal hyperplasia
Several limitations of our study should be considered Our studywas not powered to assess outcomes with respect to the differentDAPT regimens tested in our study for each stent type Similarlyour study was overall underpowered to assess the effect ofDAPT duration on stent thrombosis endpoints Therefore ourfindings should be considered exploratory and hypothesisgenerating
Our observation that primary study endpoint and other second-ary clinical ischaemic endpoints may be significantly lower after6-month compared with 24-month DAPT duration in ZES-Streated patients is intriguing but it should be interpreted withcaution In light of the limitations outlined above this findingshould be reassuring on the safety of early DAPT discontinuationin patients treated with ZES-S Yet a new paradigm has beenrecently proposed by the results of the WOEST study (clinicaltrialsgov NCT00769938) according to which lessening intensity of anti-platelet inhibition via dropping aspirin has resulted in a dramaticreduction of not only bleeding but also ischaemic endpoints includ-ing overall and cardiac mortality This paradigm has also been shownto apply to periprocedural anti-thrombotic therapy and it will befurther investigated in the ongoing comparative effectiveness of1 month of ticagrelor plus aspirin followed by ticagrelor monother-apy vs a current-day intensive DAPT in all-comer patients undergo-ing percutaneous coronary intervention with unrestricted BiolimusA9-eluting stent (GLOBAL LEADERS) study
In conclusion our study offers preliminary evidence that optimalduration of DAPT may be stent-specific with no clear associationbetween late loss potency and vulnerability to shorter DAPT dur-ation DES-specific studies aiming at unraveling the optimal DAPTduration after stent implantation are eagerly required and some ofthem are currently ongoing
Conflict of interest MV has received honoraria for lecturesad-visory board and research grants from Merck Iroko Eli Lilly andMedtronic honoraria for advisory board and lectures from TheMedicines Company and Eli Lilly Co Daiichi Sankyo Inc St Judeand Abbott Vascular lectures from Cordis CID and Terumo
FundingThe study is an investigator-driven clinical trial The conduct of thisstudy did not receive any direct or indirect external funding but wasentirely supported by the University of Ferrara which employed dedi-cated personnel for data monitoring data management events adjudi-cation and independent statistical analysis
Figure 5 Stent potency in inhibiting repeated intervention andrelative risks of adverse outcomes after 6-month dual anti-platelet therapy Relative risk reductions and corresponding95 confidence intervals (vertical bars) for target lesion revascu-larization from 30 days onwards for each drug-eluting stentemployed in the study when compared with bare metal stentgroup (reference group) is shown to the left In the middle rela-tive risk reductions and corresponding 95 confidence intervals(vertical bars) for 6-month landmark analysis of death myocardialinfarction or stroke in the 6-month when compared with24-month dual antiplatelet group is shown for each stent Inthe right portion of the figure relative risk reductions and corre-sponding 95 confidence intervals (vertical bars) for 6-monthlandmark analysis of definite probable or possible stent throm-bosis (ST) in the 6-month when compared with 24-month dualantiplatelet group is shown for each stent Note that a negativerelative risk reduction such as that observed for PES or BMSgroups implies the possibility of a relative risk increase in thestudy arm when compared with reference group EP endpointTLR target lesion revascularization from 30 days onwards Ddeath MI myocardial infarction CV cerebrovascular accidentDAPT dual antiplatelet therapy ST stent thrombosis Ref refer-ence arm BMS bare metal stent ZES-S zotarolimus-eluting stentEndeavor Sprint PES paclitaxel-eluting stent EES everolimus-eluting stent
M Valgimigli et alPage 10 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from

IntroductionBased on the concerns that delayed vessel healing may be respon-sible for late or very late stent thrombosis drug-eluting stent im-plantation (DES) irrespective of which type should prompt atleast 121 or at least 6ndash12-month2 dual antiplatelet therapy(DAPT) duration Recent data suggest that at least some newergeneration DES lead to a more favourable healing profile3 andthey are associated to a lower incidence of early late and verylate stent thrombosis compared with first generation DES45
Therefore the need for prolonged DAPT may differ based onthe type of implanted stent
Retrospective analyses of randomized controlled trials and regis-try data have shown that 6-month or even shorter DAPT durationwas not associated with increased likelihood of thrombotic eventsat long-term follow-up after everolimus- or zotarolimus (Endeavorsprint)-eluting stent implantation67
These observations have recently led to a CE Mark in Europefor 3-month only DAPT duration after Xience Prime or theXience V everolimus-eluting coronary stent systems Yetwhether the need for prolonged DAPT should differ based onthe type of implanted stent remains a controversial issue due tothe paucity of prospective randomized data
The purpose of this pre-specified analysis of the PROlongingDual antiplatelet treatment after Grading stent-Induced Intimalhyperplasia studY (PRODIGY)89 was to assess device-specific out-comes relative to DAPT duration in an all-comer patient popula-tion randomly allocated to paclitaxel (PES) Zotarolimus- (ZES-S)or everolimus- (EES) eluting or bare metal stents (BMS) at thetime of intervention
Methods
Study design and populationPRODIGY is a 4-by-2 randomized multicentre open-label clinical trialdesigned to evaluate the efficacy and safety of prolonging the durationof clopidogrel therapy for up to 24 months in all comer patients re-ceiving a balanced mixture of stents with various anti-intimal hyperpla-sia potency and belonging to both first and second generationdrug-eluting stents8 Patients undergoing elective urgent or emergentcoronary angioplasty with intended stent implantation at three referralItalian sites were randomly assigned in a 1111 fashion to one of fourstent types including everolimus-eluting stent (EES) paclitaxel-elutingstent (PES) zotarolimus-eluting Endeavor Sprintwstent (ZES-S) orthin-strut bare metal stent
As stent chronic recoil is negligible late lumen loss (LLL ie the dif-ference in minimal lumen diameter at quantitative coronary angiog-raphy undertaken after stent implantation and at 6ndash9 monthfollow-up) of a given stent quantifies the amount of neontimal hyper-plasia which has grown towards the lumen thereby determiningin-stent restenosis Typical average late loss figures for the stentswhich were used in the present study are 100 mm for BMS (ie noactive inhibition of stent-induced intimal hyperplasia) 065 mm forZES-S 04 mm for PES and 020 mm for EES At 30 days patients ineach stent group were randomized in a balanced fashion to either 6or 24 months of dual antiplatelet treatment In the 6-month DAPTgroup clopidogrel discontinuation at any time after 30 days wasallowed in patients who were randomized to bare metal stent if
coronary intervention was indicated by the presence of stable coron-ary artery disease
Individuals eligible for enrolment were patients 18 years of age orolder with chronic stable coronary artery disease or acute coronarysyndromes including non-ST-elevation and ST-elevation myocardialinfarction They were eligible if they had at least one lesion with adiameter stenosis of 50 or more that was suitable for coronarystent implantation in a vessel with a reference vessel diameter of atleast 225 mm Selection criteria were broad reflecting routine clinicalpractice We set no limit for the number of treated lesions vessels orlesion length and excluded no patients on the basis of comorbid dis-orders or age apart from the following pre-specified criteria knownallergy to acetyl salicylic acid or clopidogrel planned surgery within24 months of percutaneous coronary intervention unless the DAPTcould be maintained throughout the perisurgical period history ofbleeding diathesis major surgery within 15 days active bleeding orprevious stroke in the last 6 months concomitant or foreseeableneed for oral anticoagulation therapy pregnancy life expectancy24 months participation in another trial and inability to provideinformed consent
The Ethics Committees of the three participating centres independ-ently approved the protocol and all participants gave written informedconsent
Treatment protocol and follow-upproceduresAll patients received aspirin (160ndash325 mg orally or 500 mg iv as aloading dose and then 80ndash160 mg orally indefinitely) and clopidogrel(300 or 600 mg orally as a loading dose) and then 75 mgday forthe treatment duration according to the randomization scheme asfollows for either 6 months in the 6-month dual antiplateletgroupmdashin patients randomized to bare metal stent and presentingstable coronary artery disease a shorter (but not 30 day) durationof dual antiplatelet treatment was allowed to comply with available evi-dencemdashor 24 months in the 24-month dual antiplatelet arm irrespect-ive of the previously implanted stent type or indication to the coronaryprocedure
Anticoagulation during coronary intervention was accomplishedthrough administration of either unfractionated heparin or bivalirudinAll interventions were performed according to current standard guide-lines2 and the final interventional strategy including administration ofglycoprotein IIbIIIa antagonists pre- or post-dilatation or use of intra-vascular imaging techniques was left entirely to the discretion of theoperator except for the stent utilization Angiographic success wasdefined as residual stenosis 30 by visual analysis in the presenceof TIMI 3 grade flow
Follow-upAll randomized patients who were not lost-to-follow-up irrespectiveof their compliance to the assigned treatment schedule returned forstudy visits at 30 days and then every 6 months up to 2 yearsDuring follow-up visits patients were examined assessed foradverse events and 12-lead ECG recordings At all follow-up time-points patients were questioned on their compliance with the studymedication Any interruptions or termination as well as the reasonsfor this were documented To ensure a high adherence rate to theassigned study treatment a dedicated study nurse per site was tele-phonically contacting each patient on a monthly basis
M Valgimigli et alPage 2 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Study endpointsThe primary endpoint of this analysis was to evaluate the interactionwith stent type on the effect of short- vs long-term DAPT and out-comes with respect to the incidence of death from any cause non-fatalmyocardial infarction or cerebrovascular accident
As the therapy did not differ between the two groups in the firstmonth after stenting the time frame of major interest for theprimary endpoint was from 30 days to 24 months
Secondary endpoints included each component of the primary end-point cardiovascular death the incidence of stent thrombosis definedbased on the Academic Research Consortium (ARC) criteria10 for theentire duration of follow-up or from 6 months onwards
All study endpoints were confirmed on the basis of documentationcollected at each hospital and were centrally adjudicated by the clinicalevents committee whose members were unaware of patientsrsquotreatment-group assignments
Statistical analysisCategorical variables were expressed as frequency (percentage)whereas continuous variables were expressed as mean+ SD Baselinecontinuous variables were compared between randomized groupsusing the Wilcoxonrsquos rank sums test or the ANOVA test whereasfor baseline binary variables the likelihood-ratio chi-square test orFisherrsquos exact test was used
Estimation of the cumulative major adverse cardiovascular eventrate was done with the KaplanndashMeier method and events were com-pared by the log rank test Hazard ratios (HRs) with 95 confidenceintervals (CIs) were calculated as long-term clopidogrel vs short-termclopidogrel (ie values 1 indicating increased hazard in the long-termgroup) using a proportional hazards model The proportionalityassumptions were met as they were checked by visual estimationafter plotting the log Cumulative Hazard vs (log) time at follow-upafter index procedure and by applying a test for non-proportionalhazards using the Schoenfeld residuals as previously described11
which failed to reject the null hypothesis that event rate was affectedby time We performed a univariate Cox-regression analysis with inter-action testing to determine whether the effect of duration of DAPT onthe efficacy and safety endpoints at 2 year was consistent across stenttypes Interaction tests were done with likelihood-ratio tests of the nullhypothesis that the interaction coefficient is zero
In our analyses we define landmark time and study outcomes interms of their elapsed time from a patientrsquos index procedure Onelandmark was used in this study at 6-months alive patients completing6-month follow-up were analysed with respect to events occurringafter this timepoint and up to 24 months as per randomizationscheme (ie by stent type and DAPT duration) according to the inten-tion to treat principle Finally an explorative per protocol analysis fo-cusing on patients who permanently discontinued clopidogrel after 6months in the 6-month DAPT group vs those who never interruptedclopidogrel therapy either permanently or temporarily during thecourse of follow-up in the 24-month DAPT arm was also performed
A two-sided P-value 005 was considered significant All analysescarried out based on the intention to treat principle were performedusing STATA version 111 (Stata Corp College Station TX USA)
ResultsFrom December 2006 to December 2008 a total of 2789 patientsunderwent screening and 2013 were finally recruited into thestudy and randomized to receive one of the four stent typesThirty-three (16) patients died within 30 days and 10 patients
withdrew consent therefore 1970 patients were randomly allo-cated at 1 month to undergo 24-month vs 6-month duration ofclopidogrel therapy
The four-stent groups further stratified based on the differentDAPT duration arms were well balanced with regards to baselineand angiographic characteristics (Tables 1 and 2) with the only ex-ception of circumflex artery being more frequently treated in thepaclitaxel- and everolimus-eluting stent groups undergoing6-month DAPT compared with other treatment groups
Adherence to aspirin therapy during the course of the study washigh and it did not differ across stent groups whereas the vast ma-jority of BMS- and DES-treated patients in short-term DAPT armdiscontinued clopidogrel before or at 6-month follow-up respect-ively (Table 3)
Follow-up and clinical outcomesClinical follow-up at 2 years was complete for 997 of patients inthe long-term clopidogrel group and for 996 of those in theshort-term clopidogrel group
Table 4 shows cumulative 24-month event rates for each stentgroup There was a clear signal of heterogeneity for the primaryendpoint of death for any cause non-fatal myocardial infarctionand cerebrovascular accident across stent groups with respect tothe duration of DAPT (P-value for interaction frac14 0004) Theprimary outcomes did not formally differ in patients receivingBMS [HR 089 (95CI 054ndash145) P frac14 064] PES [HR 074(95CI 043ndash125) P frac14 026] or EES [HR 063 (95CI 033ndash121) P frac14 017] implantation across DAPT groups whereas itwas significantly lower in ZES-S patients undergoing short- whencompared with long-term DAPT therapy [HR 285 (95CI149ndash545) P frac14 00018] (Figure 1) Consistent findings wereobserved with respect to the composite of death for any causeor MI and for cardiovascular death or MI (Figure 1) The analysisof stent thrombosis endpoints did not formally disclose heterogen-eity across stent groups The analysis of definite and definite orprobable ST showed no event in the short-term DAPT group ofpatients receiving ZES-S and an excess of thrombotic events inpatients treated with PES receiving a short when compared witha long course of DAPT therapy which did not reach statistical sig-nificance (HR 020 95CI 002ndash169 P frac14 014 and HR 04495CI 014ndash143 P frac14 015 respectively Figure 2)
Landmark and per protocol analysisThere were 1924 patients reaching the 6-month follow-up ofwhom 963 were allocated to the 24-month DAPT group and961 to the short-term clopidogrel duration arm
The incidence of the primary composite endpoint from 6 to 24months consistently showed heterogeneity with respect to theprimary composite endpoint (P-value for interaction frac14 005) aswell as for any death or MI (P-value for interaction frac14 010) or car-diovascular death or MI (P-value for interaction frac14 003) withpatients receiving ZES-S showing lower event rates in the short-when compared with the long-term DAPT duration groups(Figure 3) Results were consistent when the primary study end-point from 30 days (P-value for interaction 00002) or from 6 to24 months (P-value for interaction 001) was assessed at perprotocol analysis
Dual antiplatelet therapy and stent-type Page 3 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
The composite of definite or probable [HR 012 (95CI 002ndash100) P frac14 0049] and definite probable or possible ST [HR 025(95CI 007ndash088) P frac14 0031] were both significantly lower inthe 24-month DAPT arm in patients receiving PES but not inthose treated for the other stent types (Figure 4) Yet no formalsignal for interaction was noted for stent thrombosis endpointsacross DAPT groups for each stent-type which suggests a lackof study power for this analysis (there were only three definiteprobable or possible ST events in the long when compared with12 in the short-term DAPT group in the PES arm) or the factthat results for stent thrombosis endpoints across stent groupsare consistent with the overall study findings
At per protocol analysis a consistent signal of heterogeneityacross stent types for the definite probable or possible ST wasalso observed (P-value frac14 007)
Stent potency and outcomes in relationto DAPT durationThe re-intervention rates in the target lesion(s) from 30 daysonwards was 159 in the BMS 114 in the ZES-S 60 in thePES and 49 in the EES groups (P00001 for the trend)which is consistent with the expected stent efficacy profiles
based on previously reported stent-specific late loss figuresSetting BMS as reference group ZES-S PES or EES implantationresulted in a relative risk reduction for TLR in the range of 29(95CI 129ndash555) 63 (95CI 384ndash873) or 69 (95CI460ndash936) respectively (Figure 5)
As shown in Figure 5 the relative risks of death non-fatal myo-cardial infarction or non-fatal stroke from 6 months onwards (iewhen DAPT largely differed in the two DAPT treatment groups) aswell as the 6-month landmark definite probable or possible stentthrombosis rates in the short when compared with the long-termDAPT group was not affected by the actual (ie based on theobserved TLR rates in the study) or expected (ie based on lateloss figures in previously reported studies) potency of each stenttype to inhibit intimal hyperplasia
DiscussionWe found that the composite of death myocardial infarction orcerebrovascular accident did not differ in patients receiving BMSPES or EES implantation across DAPT groups whereas it was sig-nificantly lower in ZES-S patients undergoing short when com-pared with long-term DAPT therapy with positive interaction
Table 1 Base-line characteristics of the patients
Characteristics 24-month clopidogrel 6-month clopidogrel P-value
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Age (year) 69+11 67+11 67+12 68+11 68+11 68+12 68+11 68+11 032
Male sex n () 181 (74) 195 (79) 191 (78) 197 (79) 174 (71) 190 (78) 187 (76) 196 (79) 026
Body mass index (kgm2) 29+5 27+4 27+4 28+4 27+4 28+4 28+5 27+4 067
Diabetes n () 62 (25) 60 (24) 68 (28) 54 (22) 48 (20) 58 (24) 69 (28) 58 (24) 036
Insulin-dependent n () 12 (5) 20 (8) 18 (7) 9 (4) 9 (4) 17 (7) 12 (5) 17 (7) 024
Hypertension n () 180 (73) 177 (71) 181 (74) 183 (74) 188 (76) 159 (65) 177 (72) 169 (68) 019
Hyperlipidaemia n () 124 (50) 138 (56) 137 (56) 154 (62) 124 (50) 122 (50) 140 (57) 139 (56) 009
Current smoking n () 61 (25) 58 (23) 49 (20) 54 (22) 63 (26) 67 (28) 60 (24) 57 (23) 056
Creatinine clearance (mLmin) 77+31 80+36 81+33 80+34 78+29 79+31 77+29 77+32 053
Prior MI n () 61 (25) 64 (26) 82 (33) 63 (25) 56 (23) 67 (27) 56 (23) 79 (32) 051
Prior CABG n () 24 (10) 23 (9) 31 (13) 32 (13) 19 (8) 34 (14) 23 (9) 29 (12) 029
Prior stroke or TIA n () 9 (4) 8 (3) 9 (4) 11 (4) 11 (4) 9 (4) 9 (4) 10 (4) 087
LVEF 50+11 52+10 50+10 51+10 51+10 50+11 51+11 50+10 016
Clinical presentation n ()
Stable angina pectoris 57 (23) 65 (26) 75 (31) 58 (23) 56 (23) 65 (27) 68 (28) 61 (25) 049
Acute Coronary syndrome 189 (77) 183 (74) 170 (69) 190 (77) 191 (78) 180 (73) 176 (72) 186 (76) 058
Non-ST-elevation ACS 107 (43) 95 (38) 101 (41) 108 (44) 102 (41) 96 (39) 102 (42) 106 (43) 066
Unstable angina 50 (19) 39 (16) 44 (18) 52 (21) 43 (17) 53 (22) 39 (16) 47 (19) 055
Non-ST-elevation MI 57 (23) 56 (23) 57 (23) 56 (23) 59 (24) 43 (18) 63 (26) 59 (24) 068
ST-segment-elevation MI 82 (33) 88 (35) 69 (28) 82 (33) 89 (36) 84 (34) 74 (30) 80 (32) 076
Angiographic features n ()
Single-vessel disease 87 (35) 78 (32) 69 (28) 68 (27) 83 (34) 61 (25) 79 (32) 76 (31) 018
Multi-vessel disease 159 (65) 170 (69) 176 (72) 180 (73) 163 (66) 184 (75) 166 (68) 171 (69)
ACS acute coronary syndrome LVEF left-ventricular ejection fraction
M Valgimigli et alPage 4 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Table 2 Procedural results
Characteristic 24-month clopidogrel 6-month clopidogrel P-value
BMS (n 5 246) ZES (n 5 248) PES (n 5 245) EES (n5 248) BMS (n5 246) ZES (n 5 245) PES (n 5 245) EES (n 5 247)
Number of treated lesions 147+08 153+09 151+09 151+08 148+08 160+10 164+10 156+09 035
ge2 treated lesions n () 85 (35) 97 (39) 83 (34) 100 (40) 83 (34) 92 (38) 104 (42) 92 (37) 038
ge3 treated lesions n () 23 (9) 28 (11) 29 (12) 28 (11) 23 (9) 31 (13) 33 (14) 28 (11) 082
ge4 treated lesions n () 8 (3) 13 (5) 12 (5) 5 (2) 7 (3) 14 (6) 11 (4) 12 (5) 034
LAD treated n () 150 (61) 146 (59) 136 (56) 141 (57) 137 (56) 149 (61) 142 (58) 146 (59) 043
CFX treated n () 66 (27) 69 (28) 84 (34) 102 (41) 81 (33) 78 (32) 76 (31) 83 (34) 003
RCA treated n () 87 (35) 92 (37) 88 (36) 79 (32) 98 (40) 86 (35) 84 (34) 95 (38) 070
SVG treated n () 5 (2) 6 (2) 6 (2) 6 (2) 4 (2) 5 (2) 3 (1) 5 (2) 073
At least one complex (type B2 or C)lesion n ()a
152 (62) 168 (68) 164 (67) 158 (64) 160 (65) 175 (71) 175 (71) 154 (62) 014
Total ACCAHA scoreab 37+21 37+22 38+23 39+22 37+22 39+23 39+23 40+24 028
Number of stents implanted 182+12 191+13 181+13 177+11 177+11 196+13 188+12 196+13 034
Length of stent (mm) 39+35 41+32 39+29 37+24 36+25 42+30 40+27 42+32 013
Quantitative coronary analysis
Lesion length (mm) 1307+845 1318+832 1409+951 1313+835 1351+825 1323+824 1375+898 1427+864 049
RVD before (mm) 264+054 264+051 269+053 263+056 267+053 261+063 260+053 268+053 031
MLD before (mm) 060+039 061+038 058+041 059+041 056+041 056+041 055+037 058+036 066
Stenosis before () 78+14 77+13 79+14 78+16 79+14 77+17 78+14 79+12 055
RVD after (mm) 276+050 274+042 286+047 276+050 279+046 279+054 279+051 279+048 047
MLD after (mm) 242+056 246+046 253+046 245+049 244+049 247+054 242+053 252+046 027
Stenosis after () 1057+825 968+874 1001+748 1104+867 1129+841 1025+799 1113+876 1145+933 032
aCalculated in 952 patients in the 24-month clopidogrel arm and in 943 patients in the 6-month clopidogrel arm who presented at least one de-novo lesion ACCAHA score was missing in three patientsLAD left anterior descending artery CFX circumflex artery RCA right coronary artery LMCA left main coronary artery SVG saphenous vein graftbAs previously described18 type A stenoses were coded 1 point typeB1 stenoses 2 points type B2 stenoses 3 points and type C stenoses 4 points
Dualantiplatelet
therapyand
stent-typeP
age5
of
11
at UniversitAtilde degli Studi di Brescia on January 16 2013 httpeurheartjoxfordjournalsorg Downloaded from
testing At the 6-month landmark analysis heterogeneity acrossstent types persisted whereas patients receiving PES showed a sig-nificantly higher rate of stent thrombosis in the short DAPTregimen No association was noted between expected or actualstent potency in inhibiting intimal hyperplasia and greater vulner-ability to shorter DAPT therapy
The main findings of our analysis challenge current recommen-dations endorsing a clear-cut dichotomy of BMS vs DES for theneed of prolonged DAPT after stenting Furthermore our datasuggest minimal duration of clopidogrel therapy may differamong DES irrespective of stent potency in inhibiting intimalhyperplasia
As previously reported9 no interaction was noted between BMSand the three different DES type clustered together with respectto duration of DAPT therapy On the other hand in the currentanalysis focusing on each DES type individually a clear andformal signal of heterogeneity with respect to overall death myo-cardial infarction or cerebrovascular accidents was noted for theneed of prolonged therapy with clopidogrel after interventionThis was driven by ZES-S treated patients showing an improvedprimary study and other secondary clinical outcomes with short-term DAPT when compared with 24-month duration of therapyand by an excess of stent thrombosis events particularly definiteor probable and definite probable or possible ST in patients
Table 3 Use of anti-platelet medications during the trial
24-month clopidogrel 6-month clopidogrel P-value
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Anti-platelet therapy at 30 days n ()
Numberevaluated
246 248 245 248 246 245 245 247
Aspirin 246 (100) 248 (100) 245 (100) 248 (100) 246 (100) 245 (100) 245 (100) 247 (100) 099
Clopidogrel 245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Aspirin andclopidogrel
245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Anti-platelet therapy at 6 months n ()
Numberevaluated total
241 241 238 246 240 244 239 240
Aspirin 240 (996) 240 (996) 234 (983) 246 (100) 236 (983) 241 (988) 238 (996) 238 (996) 024
Clopidogrel 239 (992) 239 (992) 237 (976) 245 (996) 94 (392) 241 (988) 234 (979) 236 (983) 0001
Aspirin andclopidogrel
238 (988) 238 (988) 233 (979) 245 (996) 97 (392) 238 (976) 233 (975) 235 (979) 0001
Anti-platelet therapy at 12 months n ()
Numberevaluated total
236 238 231 243 232 240 233 237
Aspirin 233 (987) 237 (996) 226 (978) 243 (100) 223 (961) 236 (983) 231 (991) 235 (992) 012
Clopidogrel 233 (987) 232 (975) 228 (987) 239 (983) 8 (35) 12 (5) 7 (3) 6 (25) 0001
Aspirin andClopidogrel
230 (975) 231 (971) 223 (965) 239 (984) 8 (35) 12 (5) 6 (26) 6 (25) 0001
Anti-platelet therapy at 18 months n ()
Numberevaluated total
234 234 227 238 231 239 228 234 034
Aspirin 232 (992) 232 (992) 223 (982) 234 (983) 221 (957) 232 (971) 226 (992) 233 (996) 012
Clopidogrel 231 (987) 222 (989) 220 (969) 231 (971) 2 (09) 2 (09) 3 (13) 1 (04) 0001
Aspirin andclopidogrel
229 (979) 221 (944) 216 (952) 229 (962) 2 (09) 1 (04) 2 (09) 1 (04) 0001
Anti-platelet therapy at 24 months n ()
Numberevaluated total
230 228 224 238 227 237 226 230
Aspirin 228 (991) 224 (983) 219 (978) 234 (983) 216 (952) 230 (971) 221 (978) 229 (996) 019
Clopidogrel 226 (983) 212 (93) 214 (955) 228 (958) 0 2 (08) 3 (13) 0 0001
Aspirin andclopidogrel
224 (974) 210 (921) 211 (942) 226 (947) 0 1 (04) 2 (09) 0 0001
M Valgimigli et alPage 6 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
undergoing 6-month clopidogrel therapy after PES implantationcompared with a longer duration of therapy
In our study adherence to aspirin and clopidogrel was similarlyhigh in the first 6 months after DES implantation in the two DAPTgroups Therefore events occurring during this time period in thethree DES groups may potentially confound the outcomes of thetwo different DAPT regimens tested in the study Based on thisnotion a landmark analysis focusing on events occurring after a6 month-follow-up has been pre-specified and previously reportedfor the whole patient population or for all DES treated patientsclustered together When the three tested DES types were ana-lysed separately at the 6-month landmark analysis the resultswere largely consistent with the findings observed for the entirefollow-up duration (i) patients treated with ZES-S showed abetter ischaemic outcomes in the 6-month when compared withthe 24-month DAPT groups (ii) event rates for the primary or sec-ondary ischaemic clinical endpoints were similar between DAPTgroups after BMS or EES implantation (iii) the primary clinicalcomposite endpoint trended higher and the ST rates were signifi-cantly increased in PES treated patients receiving PES and
undergoing 6-month when compared with 24-month duration ofclopidogrel
Kandzari et al6 recently analysed outcomes in 2032 patientsundergoing coronary revascularization with ZES-S in five trialswho for various reasons discontinued DAPT at 6 months andfound that outcomes did not differ compared with patients whoreceived longer clopidogrel therapy (up to 12 or 24 months)
In the Real Safety and Efficacy of 3-Month Dual AntiplateletTherapy Following Zotarolimus-Eluting Stent Implantation(RESET) trial of 2148 patients randomized to the ZES-S stentand three months of DAPT and 1058 patients treated with stand-ard 12-month DAPT and other DES the combined endpoint ofany death MI stent thrombosis occurred in 13 in the standardtherapy arm vs 08 in the 3-month group (P frac14 048)12 Interest-ingly prospective studies undertaken to evaluate the degree ofZES-S stent coverage have consistently showed a very low rateof uncoveredmalapposed struts at 6- or even 3-month optical co-herence tomography evaluation which favourably compared withboth first generation DES or even BMS13 ndash15 Based on thisfinding the Zotarolimus-eluting stent in uncertain DES candidates
Table 4 Outcome rates at 24 months according to treatment group
Outcome 24-month clopidogrel 6-month clopidogrel
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Death for any cause myocardialinfarction or cerebrovascularaccident
29 (118) 33 (133) 23 (94) 15 (61) 32 (13) 12 (49) 31 (127) 23 (91)
Death for cardiovascular causemyocardial infarction orcerebrovascular accident
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (56)
Death for any cause ormyocardial infarction
25 (102) 27 (109) 22 (89) 14 (57) 30 (122) 12 (49) 31 (127) 21 (85)
Death for cardiovascular causemyocardial infarction
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (53)
Death for any cause 16 (65) 20 (81) 19 (78) 10 (4) 20 (81) 8 (33) 20 (82) 17 (69)
Death for cardiovascular cause 9 (37) 13 (52) 10 (41) 4 (16) 12 (49) 7 (29) 12 (49) 6 (24)
Myocardial infarction 14 (57) 12 (48) 9 (37) 4 (16) 15 (61) 4 (16) 14 (57) 8 (32)
Cerebrovascular accident 7 (28) 7 (28) 5 (2) 1 (04) 5 (2) 1 (04) 4 (16) 2 (08)
Definite stent thrombosis
Late 3 (12) 2 (08) 1 (04) 0 (0) 1 (04) 0 (0) 2 (08) 1 (04)
Very late 0 (0) 1 (04) 0 (0) 1 (04) 0 (0) 0 (0) 3 (13) 0 (0)
Cumulative 3 (12) 3 (12) 1 (04) 1 (04) 1 (04) 0 (0) 5 (2) 1 (04)
Definite or probable stent thrombosis
Late 5 (2) 2 (08) 3 (12) 0 (0) 5 (2) 0 (0) 3 (12) 1 (04)
Very late 0 (0) 1 (04) 1 (04) 1 (04) 0 (0) 0 (0) 6 (26) 0 (0)
Cumulative 5 (2) 3 (12) 4 (16) 1 (04) 5 (2) 0 (0) 9 (37) 1 (04)
Definite probable or possible stent thrombosis
Late 7 (28) 8 (32) 8 (32) 3 (12) 10 (41) 4 (16) 10 (41) 4 (16)
Very late 2 (08) 5 (21) 3 (13) 2 (08) 5 (21) 3 (13) 8 (34) 2 (08)
Cumulative 9 (37) 13 (52) 11 (45) 5 (2) 15 (61) 7 (29) 18 (74) 6 (24)
Dual antiplatelet therapy and stent-type Page 7 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 1 Stent analyses of the primary study endpoint and other secondary clinical outcomes Stent-specific analyses are shown with hazardratios and 95 confidence intervals for the primary end point of death for any cause myocardial infarction (MI) or cerebrovascular accident(CVA) death or MI and cardiovascular (CV) death or MI among patients randomly assigned to either the six or the 24-month clopidogreltherapy The P-value for interaction represents the likelihood of interaction between the variable and the relative treatment effect
Figure 2 Stent analyses of the stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95 confidence inter-vals for the definite definite probable and definite probable possible stent thrombosis (ST) among patients randomly assigned to either the 6or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction between the variable and the relativetreatment effect
M Valgimigli et alPage 8 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 3 Stent analyses of the 6-month landmark primary study endpoint and other secondary clinical outcomes Stent-specific analyses areshown with hazard ratios and 95 confidence intervals for the 6-month landmark analyses of the primary endpoint of death for any causemyocardial infarction (MI) or cerebrovascular accident (CVA) death or MI and cardiovascular (CV) death or MI among patients randomlyassigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction betweenthe variable and the relative treatment effect
Figure 4 Stent analyses of the 6-month landmark stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95confidence intervals for the 6-month landmark analyses of definite definite probable and definite probable possible stent thrombosis (ST)among patients randomly assigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihoodof interaction between the variable and the relative treatment effect
Dual antiplatelet therapy and stent-type Page 9 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
(ZEUS) study is comparing ZES-S vs BMS in patients at highthrombotic bleeding or low restenosis risk allowing 1-monthDAPT duration in both stent arms in patients who cannot toleratelonger duration of therapy (NCT01385319)
Reassuring data on the safety of early DAPT discontinuationafter EES have also been reported by a retrospective analysis ofregistry data7 Moreover the pooled analysis of SPIRIT II III IVand COMPARE Trials of 6789 patients showed a persistentlylow ST rate in patients treated with EES but not PES who discon-tinued DAPT after 6 months which is consistent with our currentfindings16 Indeed while our analysis on primary study endpointand other secondary clinical outcomes numerically favoured long-term DAPT after EES implantation the stent thrombosis endpointsand 6-month clinical landmark analyses revealed no excess ofevents in the 6-month DAPT group compared with longer-termclopidogrel therapy which is at variance with the results observedafter PES implantation
The need for prolonged DAPT has been suggested to be in-versely related to stent late loss17 Potent inhibition of intimal
hyperplasia might more frequently lead to incomplete stent cover-age andor late stent mal-apposition requiring a more prolongedcourse of intensified anti-platelet therapy to maintain stentsafety17
Our study by randomizing patients to a balanced mixture ofstents with various anti-intimal hyperplasia and each stent groupto 6- vs 24-month DAPT duration offers no evidence supportingthe association between stent-related late-loss and need for pro-longed DAPT On the contrary the results of our explorativeyet pre-specified analysis suggest that the minimal DAPT durationmay be stent-specific and not clearly related to stent potencytowards inhibition of intimal hyperplasia
Several limitations of our study should be considered Our studywas not powered to assess outcomes with respect to the differentDAPT regimens tested in our study for each stent type Similarlyour study was overall underpowered to assess the effect ofDAPT duration on stent thrombosis endpoints Therefore ourfindings should be considered exploratory and hypothesisgenerating
Our observation that primary study endpoint and other second-ary clinical ischaemic endpoints may be significantly lower after6-month compared with 24-month DAPT duration in ZES-Streated patients is intriguing but it should be interpreted withcaution In light of the limitations outlined above this findingshould be reassuring on the safety of early DAPT discontinuationin patients treated with ZES-S Yet a new paradigm has beenrecently proposed by the results of the WOEST study (clinicaltrialsgov NCT00769938) according to which lessening intensity of anti-platelet inhibition via dropping aspirin has resulted in a dramaticreduction of not only bleeding but also ischaemic endpoints includ-ing overall and cardiac mortality This paradigm has also been shownto apply to periprocedural anti-thrombotic therapy and it will befurther investigated in the ongoing comparative effectiveness of1 month of ticagrelor plus aspirin followed by ticagrelor monother-apy vs a current-day intensive DAPT in all-comer patients undergo-ing percutaneous coronary intervention with unrestricted BiolimusA9-eluting stent (GLOBAL LEADERS) study
In conclusion our study offers preliminary evidence that optimalduration of DAPT may be stent-specific with no clear associationbetween late loss potency and vulnerability to shorter DAPT dur-ation DES-specific studies aiming at unraveling the optimal DAPTduration after stent implantation are eagerly required and some ofthem are currently ongoing
Conflict of interest MV has received honoraria for lecturesad-visory board and research grants from Merck Iroko Eli Lilly andMedtronic honoraria for advisory board and lectures from TheMedicines Company and Eli Lilly Co Daiichi Sankyo Inc St Judeand Abbott Vascular lectures from Cordis CID and Terumo
FundingThe study is an investigator-driven clinical trial The conduct of thisstudy did not receive any direct or indirect external funding but wasentirely supported by the University of Ferrara which employed dedi-cated personnel for data monitoring data management events adjudi-cation and independent statistical analysis
Figure 5 Stent potency in inhibiting repeated intervention andrelative risks of adverse outcomes after 6-month dual anti-platelet therapy Relative risk reductions and corresponding95 confidence intervals (vertical bars) for target lesion revascu-larization from 30 days onwards for each drug-eluting stentemployed in the study when compared with bare metal stentgroup (reference group) is shown to the left In the middle rela-tive risk reductions and corresponding 95 confidence intervals(vertical bars) for 6-month landmark analysis of death myocardialinfarction or stroke in the 6-month when compared with24-month dual antiplatelet group is shown for each stent Inthe right portion of the figure relative risk reductions and corre-sponding 95 confidence intervals (vertical bars) for 6-monthlandmark analysis of definite probable or possible stent throm-bosis (ST) in the 6-month when compared with 24-month dualantiplatelet group is shown for each stent Note that a negativerelative risk reduction such as that observed for PES or BMSgroups implies the possibility of a relative risk increase in thestudy arm when compared with reference group EP endpointTLR target lesion revascularization from 30 days onwards Ddeath MI myocardial infarction CV cerebrovascular accidentDAPT dual antiplatelet therapy ST stent thrombosis Ref refer-ence arm BMS bare metal stent ZES-S zotarolimus-eluting stentEndeavor Sprint PES paclitaxel-eluting stent EES everolimus-eluting stent
M Valgimigli et alPage 10 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from

Study endpointsThe primary endpoint of this analysis was to evaluate the interactionwith stent type on the effect of short- vs long-term DAPT and out-comes with respect to the incidence of death from any cause non-fatalmyocardial infarction or cerebrovascular accident
As the therapy did not differ between the two groups in the firstmonth after stenting the time frame of major interest for theprimary endpoint was from 30 days to 24 months
Secondary endpoints included each component of the primary end-point cardiovascular death the incidence of stent thrombosis definedbased on the Academic Research Consortium (ARC) criteria10 for theentire duration of follow-up or from 6 months onwards
All study endpoints were confirmed on the basis of documentationcollected at each hospital and were centrally adjudicated by the clinicalevents committee whose members were unaware of patientsrsquotreatment-group assignments
Statistical analysisCategorical variables were expressed as frequency (percentage)whereas continuous variables were expressed as mean+ SD Baselinecontinuous variables were compared between randomized groupsusing the Wilcoxonrsquos rank sums test or the ANOVA test whereasfor baseline binary variables the likelihood-ratio chi-square test orFisherrsquos exact test was used
Estimation of the cumulative major adverse cardiovascular eventrate was done with the KaplanndashMeier method and events were com-pared by the log rank test Hazard ratios (HRs) with 95 confidenceintervals (CIs) were calculated as long-term clopidogrel vs short-termclopidogrel (ie values 1 indicating increased hazard in the long-termgroup) using a proportional hazards model The proportionalityassumptions were met as they were checked by visual estimationafter plotting the log Cumulative Hazard vs (log) time at follow-upafter index procedure and by applying a test for non-proportionalhazards using the Schoenfeld residuals as previously described11
which failed to reject the null hypothesis that event rate was affectedby time We performed a univariate Cox-regression analysis with inter-action testing to determine whether the effect of duration of DAPT onthe efficacy and safety endpoints at 2 year was consistent across stenttypes Interaction tests were done with likelihood-ratio tests of the nullhypothesis that the interaction coefficient is zero
In our analyses we define landmark time and study outcomes interms of their elapsed time from a patientrsquos index procedure Onelandmark was used in this study at 6-months alive patients completing6-month follow-up were analysed with respect to events occurringafter this timepoint and up to 24 months as per randomizationscheme (ie by stent type and DAPT duration) according to the inten-tion to treat principle Finally an explorative per protocol analysis fo-cusing on patients who permanently discontinued clopidogrel after 6months in the 6-month DAPT group vs those who never interruptedclopidogrel therapy either permanently or temporarily during thecourse of follow-up in the 24-month DAPT arm was also performed
A two-sided P-value 005 was considered significant All analysescarried out based on the intention to treat principle were performedusing STATA version 111 (Stata Corp College Station TX USA)
ResultsFrom December 2006 to December 2008 a total of 2789 patientsunderwent screening and 2013 were finally recruited into thestudy and randomized to receive one of the four stent typesThirty-three (16) patients died within 30 days and 10 patients
withdrew consent therefore 1970 patients were randomly allo-cated at 1 month to undergo 24-month vs 6-month duration ofclopidogrel therapy
The four-stent groups further stratified based on the differentDAPT duration arms were well balanced with regards to baselineand angiographic characteristics (Tables 1 and 2) with the only ex-ception of circumflex artery being more frequently treated in thepaclitaxel- and everolimus-eluting stent groups undergoing6-month DAPT compared with other treatment groups
Adherence to aspirin therapy during the course of the study washigh and it did not differ across stent groups whereas the vast ma-jority of BMS- and DES-treated patients in short-term DAPT armdiscontinued clopidogrel before or at 6-month follow-up respect-ively (Table 3)
Follow-up and clinical outcomesClinical follow-up at 2 years was complete for 997 of patients inthe long-term clopidogrel group and for 996 of those in theshort-term clopidogrel group
Table 4 shows cumulative 24-month event rates for each stentgroup There was a clear signal of heterogeneity for the primaryendpoint of death for any cause non-fatal myocardial infarctionand cerebrovascular accident across stent groups with respect tothe duration of DAPT (P-value for interaction frac14 0004) Theprimary outcomes did not formally differ in patients receivingBMS [HR 089 (95CI 054ndash145) P frac14 064] PES [HR 074(95CI 043ndash125) P frac14 026] or EES [HR 063 (95CI 033ndash121) P frac14 017] implantation across DAPT groups whereas itwas significantly lower in ZES-S patients undergoing short- whencompared with long-term DAPT therapy [HR 285 (95CI149ndash545) P frac14 00018] (Figure 1) Consistent findings wereobserved with respect to the composite of death for any causeor MI and for cardiovascular death or MI (Figure 1) The analysisof stent thrombosis endpoints did not formally disclose heterogen-eity across stent groups The analysis of definite and definite orprobable ST showed no event in the short-term DAPT group ofpatients receiving ZES-S and an excess of thrombotic events inpatients treated with PES receiving a short when compared witha long course of DAPT therapy which did not reach statistical sig-nificance (HR 020 95CI 002ndash169 P frac14 014 and HR 04495CI 014ndash143 P frac14 015 respectively Figure 2)
Landmark and per protocol analysisThere were 1924 patients reaching the 6-month follow-up ofwhom 963 were allocated to the 24-month DAPT group and961 to the short-term clopidogrel duration arm
The incidence of the primary composite endpoint from 6 to 24months consistently showed heterogeneity with respect to theprimary composite endpoint (P-value for interaction frac14 005) aswell as for any death or MI (P-value for interaction frac14 010) or car-diovascular death or MI (P-value for interaction frac14 003) withpatients receiving ZES-S showing lower event rates in the short-when compared with the long-term DAPT duration groups(Figure 3) Results were consistent when the primary study end-point from 30 days (P-value for interaction 00002) or from 6 to24 months (P-value for interaction 001) was assessed at perprotocol analysis
Dual antiplatelet therapy and stent-type Page 3 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
The composite of definite or probable [HR 012 (95CI 002ndash100) P frac14 0049] and definite probable or possible ST [HR 025(95CI 007ndash088) P frac14 0031] were both significantly lower inthe 24-month DAPT arm in patients receiving PES but not inthose treated for the other stent types (Figure 4) Yet no formalsignal for interaction was noted for stent thrombosis endpointsacross DAPT groups for each stent-type which suggests a lackof study power for this analysis (there were only three definiteprobable or possible ST events in the long when compared with12 in the short-term DAPT group in the PES arm) or the factthat results for stent thrombosis endpoints across stent groupsare consistent with the overall study findings
At per protocol analysis a consistent signal of heterogeneityacross stent types for the definite probable or possible ST wasalso observed (P-value frac14 007)
Stent potency and outcomes in relationto DAPT durationThe re-intervention rates in the target lesion(s) from 30 daysonwards was 159 in the BMS 114 in the ZES-S 60 in thePES and 49 in the EES groups (P00001 for the trend)which is consistent with the expected stent efficacy profiles
based on previously reported stent-specific late loss figuresSetting BMS as reference group ZES-S PES or EES implantationresulted in a relative risk reduction for TLR in the range of 29(95CI 129ndash555) 63 (95CI 384ndash873) or 69 (95CI460ndash936) respectively (Figure 5)
As shown in Figure 5 the relative risks of death non-fatal myo-cardial infarction or non-fatal stroke from 6 months onwards (iewhen DAPT largely differed in the two DAPT treatment groups) aswell as the 6-month landmark definite probable or possible stentthrombosis rates in the short when compared with the long-termDAPT group was not affected by the actual (ie based on theobserved TLR rates in the study) or expected (ie based on lateloss figures in previously reported studies) potency of each stenttype to inhibit intimal hyperplasia
DiscussionWe found that the composite of death myocardial infarction orcerebrovascular accident did not differ in patients receiving BMSPES or EES implantation across DAPT groups whereas it was sig-nificantly lower in ZES-S patients undergoing short when com-pared with long-term DAPT therapy with positive interaction
Table 1 Base-line characteristics of the patients
Characteristics 24-month clopidogrel 6-month clopidogrel P-value
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Age (year) 69+11 67+11 67+12 68+11 68+11 68+12 68+11 68+11 032
Male sex n () 181 (74) 195 (79) 191 (78) 197 (79) 174 (71) 190 (78) 187 (76) 196 (79) 026
Body mass index (kgm2) 29+5 27+4 27+4 28+4 27+4 28+4 28+5 27+4 067
Diabetes n () 62 (25) 60 (24) 68 (28) 54 (22) 48 (20) 58 (24) 69 (28) 58 (24) 036
Insulin-dependent n () 12 (5) 20 (8) 18 (7) 9 (4) 9 (4) 17 (7) 12 (5) 17 (7) 024
Hypertension n () 180 (73) 177 (71) 181 (74) 183 (74) 188 (76) 159 (65) 177 (72) 169 (68) 019
Hyperlipidaemia n () 124 (50) 138 (56) 137 (56) 154 (62) 124 (50) 122 (50) 140 (57) 139 (56) 009
Current smoking n () 61 (25) 58 (23) 49 (20) 54 (22) 63 (26) 67 (28) 60 (24) 57 (23) 056
Creatinine clearance (mLmin) 77+31 80+36 81+33 80+34 78+29 79+31 77+29 77+32 053
Prior MI n () 61 (25) 64 (26) 82 (33) 63 (25) 56 (23) 67 (27) 56 (23) 79 (32) 051
Prior CABG n () 24 (10) 23 (9) 31 (13) 32 (13) 19 (8) 34 (14) 23 (9) 29 (12) 029
Prior stroke or TIA n () 9 (4) 8 (3) 9 (4) 11 (4) 11 (4) 9 (4) 9 (4) 10 (4) 087
LVEF 50+11 52+10 50+10 51+10 51+10 50+11 51+11 50+10 016
Clinical presentation n ()
Stable angina pectoris 57 (23) 65 (26) 75 (31) 58 (23) 56 (23) 65 (27) 68 (28) 61 (25) 049
Acute Coronary syndrome 189 (77) 183 (74) 170 (69) 190 (77) 191 (78) 180 (73) 176 (72) 186 (76) 058
Non-ST-elevation ACS 107 (43) 95 (38) 101 (41) 108 (44) 102 (41) 96 (39) 102 (42) 106 (43) 066
Unstable angina 50 (19) 39 (16) 44 (18) 52 (21) 43 (17) 53 (22) 39 (16) 47 (19) 055
Non-ST-elevation MI 57 (23) 56 (23) 57 (23) 56 (23) 59 (24) 43 (18) 63 (26) 59 (24) 068
ST-segment-elevation MI 82 (33) 88 (35) 69 (28) 82 (33) 89 (36) 84 (34) 74 (30) 80 (32) 076
Angiographic features n ()
Single-vessel disease 87 (35) 78 (32) 69 (28) 68 (27) 83 (34) 61 (25) 79 (32) 76 (31) 018
Multi-vessel disease 159 (65) 170 (69) 176 (72) 180 (73) 163 (66) 184 (75) 166 (68) 171 (69)
ACS acute coronary syndrome LVEF left-ventricular ejection fraction
M Valgimigli et alPage 4 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Table 2 Procedural results
Characteristic 24-month clopidogrel 6-month clopidogrel P-value
BMS (n 5 246) ZES (n 5 248) PES (n 5 245) EES (n5 248) BMS (n5 246) ZES (n 5 245) PES (n 5 245) EES (n 5 247)
Number of treated lesions 147+08 153+09 151+09 151+08 148+08 160+10 164+10 156+09 035
ge2 treated lesions n () 85 (35) 97 (39) 83 (34) 100 (40) 83 (34) 92 (38) 104 (42) 92 (37) 038
ge3 treated lesions n () 23 (9) 28 (11) 29 (12) 28 (11) 23 (9) 31 (13) 33 (14) 28 (11) 082
ge4 treated lesions n () 8 (3) 13 (5) 12 (5) 5 (2) 7 (3) 14 (6) 11 (4) 12 (5) 034
LAD treated n () 150 (61) 146 (59) 136 (56) 141 (57) 137 (56) 149 (61) 142 (58) 146 (59) 043
CFX treated n () 66 (27) 69 (28) 84 (34) 102 (41) 81 (33) 78 (32) 76 (31) 83 (34) 003
RCA treated n () 87 (35) 92 (37) 88 (36) 79 (32) 98 (40) 86 (35) 84 (34) 95 (38) 070
SVG treated n () 5 (2) 6 (2) 6 (2) 6 (2) 4 (2) 5 (2) 3 (1) 5 (2) 073
At least one complex (type B2 or C)lesion n ()a
152 (62) 168 (68) 164 (67) 158 (64) 160 (65) 175 (71) 175 (71) 154 (62) 014
Total ACCAHA scoreab 37+21 37+22 38+23 39+22 37+22 39+23 39+23 40+24 028
Number of stents implanted 182+12 191+13 181+13 177+11 177+11 196+13 188+12 196+13 034
Length of stent (mm) 39+35 41+32 39+29 37+24 36+25 42+30 40+27 42+32 013
Quantitative coronary analysis
Lesion length (mm) 1307+845 1318+832 1409+951 1313+835 1351+825 1323+824 1375+898 1427+864 049
RVD before (mm) 264+054 264+051 269+053 263+056 267+053 261+063 260+053 268+053 031
MLD before (mm) 060+039 061+038 058+041 059+041 056+041 056+041 055+037 058+036 066
Stenosis before () 78+14 77+13 79+14 78+16 79+14 77+17 78+14 79+12 055
RVD after (mm) 276+050 274+042 286+047 276+050 279+046 279+054 279+051 279+048 047
MLD after (mm) 242+056 246+046 253+046 245+049 244+049 247+054 242+053 252+046 027
Stenosis after () 1057+825 968+874 1001+748 1104+867 1129+841 1025+799 1113+876 1145+933 032
aCalculated in 952 patients in the 24-month clopidogrel arm and in 943 patients in the 6-month clopidogrel arm who presented at least one de-novo lesion ACCAHA score was missing in three patientsLAD left anterior descending artery CFX circumflex artery RCA right coronary artery LMCA left main coronary artery SVG saphenous vein graftbAs previously described18 type A stenoses were coded 1 point typeB1 stenoses 2 points type B2 stenoses 3 points and type C stenoses 4 points
Dualantiplatelet
therapyand
stent-typeP
age5
of
11
at UniversitAtilde degli Studi di Brescia on January 16 2013 httpeurheartjoxfordjournalsorg Downloaded from
testing At the 6-month landmark analysis heterogeneity acrossstent types persisted whereas patients receiving PES showed a sig-nificantly higher rate of stent thrombosis in the short DAPTregimen No association was noted between expected or actualstent potency in inhibiting intimal hyperplasia and greater vulner-ability to shorter DAPT therapy
The main findings of our analysis challenge current recommen-dations endorsing a clear-cut dichotomy of BMS vs DES for theneed of prolonged DAPT after stenting Furthermore our datasuggest minimal duration of clopidogrel therapy may differamong DES irrespective of stent potency in inhibiting intimalhyperplasia
As previously reported9 no interaction was noted between BMSand the three different DES type clustered together with respectto duration of DAPT therapy On the other hand in the currentanalysis focusing on each DES type individually a clear andformal signal of heterogeneity with respect to overall death myo-cardial infarction or cerebrovascular accidents was noted for theneed of prolonged therapy with clopidogrel after interventionThis was driven by ZES-S treated patients showing an improvedprimary study and other secondary clinical outcomes with short-term DAPT when compared with 24-month duration of therapyand by an excess of stent thrombosis events particularly definiteor probable and definite probable or possible ST in patients
Table 3 Use of anti-platelet medications during the trial
24-month clopidogrel 6-month clopidogrel P-value
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Anti-platelet therapy at 30 days n ()
Numberevaluated
246 248 245 248 246 245 245 247
Aspirin 246 (100) 248 (100) 245 (100) 248 (100) 246 (100) 245 (100) 245 (100) 247 (100) 099
Clopidogrel 245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Aspirin andclopidogrel
245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Anti-platelet therapy at 6 months n ()
Numberevaluated total
241 241 238 246 240 244 239 240
Aspirin 240 (996) 240 (996) 234 (983) 246 (100) 236 (983) 241 (988) 238 (996) 238 (996) 024
Clopidogrel 239 (992) 239 (992) 237 (976) 245 (996) 94 (392) 241 (988) 234 (979) 236 (983) 0001
Aspirin andclopidogrel
238 (988) 238 (988) 233 (979) 245 (996) 97 (392) 238 (976) 233 (975) 235 (979) 0001
Anti-platelet therapy at 12 months n ()
Numberevaluated total
236 238 231 243 232 240 233 237
Aspirin 233 (987) 237 (996) 226 (978) 243 (100) 223 (961) 236 (983) 231 (991) 235 (992) 012
Clopidogrel 233 (987) 232 (975) 228 (987) 239 (983) 8 (35) 12 (5) 7 (3) 6 (25) 0001
Aspirin andClopidogrel
230 (975) 231 (971) 223 (965) 239 (984) 8 (35) 12 (5) 6 (26) 6 (25) 0001
Anti-platelet therapy at 18 months n ()
Numberevaluated total
234 234 227 238 231 239 228 234 034
Aspirin 232 (992) 232 (992) 223 (982) 234 (983) 221 (957) 232 (971) 226 (992) 233 (996) 012
Clopidogrel 231 (987) 222 (989) 220 (969) 231 (971) 2 (09) 2 (09) 3 (13) 1 (04) 0001
Aspirin andclopidogrel
229 (979) 221 (944) 216 (952) 229 (962) 2 (09) 1 (04) 2 (09) 1 (04) 0001
Anti-platelet therapy at 24 months n ()
Numberevaluated total
230 228 224 238 227 237 226 230
Aspirin 228 (991) 224 (983) 219 (978) 234 (983) 216 (952) 230 (971) 221 (978) 229 (996) 019
Clopidogrel 226 (983) 212 (93) 214 (955) 228 (958) 0 2 (08) 3 (13) 0 0001
Aspirin andclopidogrel
224 (974) 210 (921) 211 (942) 226 (947) 0 1 (04) 2 (09) 0 0001
M Valgimigli et alPage 6 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
undergoing 6-month clopidogrel therapy after PES implantationcompared with a longer duration of therapy
In our study adherence to aspirin and clopidogrel was similarlyhigh in the first 6 months after DES implantation in the two DAPTgroups Therefore events occurring during this time period in thethree DES groups may potentially confound the outcomes of thetwo different DAPT regimens tested in the study Based on thisnotion a landmark analysis focusing on events occurring after a6 month-follow-up has been pre-specified and previously reportedfor the whole patient population or for all DES treated patientsclustered together When the three tested DES types were ana-lysed separately at the 6-month landmark analysis the resultswere largely consistent with the findings observed for the entirefollow-up duration (i) patients treated with ZES-S showed abetter ischaemic outcomes in the 6-month when compared withthe 24-month DAPT groups (ii) event rates for the primary or sec-ondary ischaemic clinical endpoints were similar between DAPTgroups after BMS or EES implantation (iii) the primary clinicalcomposite endpoint trended higher and the ST rates were signifi-cantly increased in PES treated patients receiving PES and
undergoing 6-month when compared with 24-month duration ofclopidogrel
Kandzari et al6 recently analysed outcomes in 2032 patientsundergoing coronary revascularization with ZES-S in five trialswho for various reasons discontinued DAPT at 6 months andfound that outcomes did not differ compared with patients whoreceived longer clopidogrel therapy (up to 12 or 24 months)
In the Real Safety and Efficacy of 3-Month Dual AntiplateletTherapy Following Zotarolimus-Eluting Stent Implantation(RESET) trial of 2148 patients randomized to the ZES-S stentand three months of DAPT and 1058 patients treated with stand-ard 12-month DAPT and other DES the combined endpoint ofany death MI stent thrombosis occurred in 13 in the standardtherapy arm vs 08 in the 3-month group (P frac14 048)12 Interest-ingly prospective studies undertaken to evaluate the degree ofZES-S stent coverage have consistently showed a very low rateof uncoveredmalapposed struts at 6- or even 3-month optical co-herence tomography evaluation which favourably compared withboth first generation DES or even BMS13 ndash15 Based on thisfinding the Zotarolimus-eluting stent in uncertain DES candidates
Table 4 Outcome rates at 24 months according to treatment group
Outcome 24-month clopidogrel 6-month clopidogrel
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Death for any cause myocardialinfarction or cerebrovascularaccident
29 (118) 33 (133) 23 (94) 15 (61) 32 (13) 12 (49) 31 (127) 23 (91)
Death for cardiovascular causemyocardial infarction orcerebrovascular accident
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (56)
Death for any cause ormyocardial infarction
25 (102) 27 (109) 22 (89) 14 (57) 30 (122) 12 (49) 31 (127) 21 (85)
Death for cardiovascular causemyocardial infarction
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (53)
Death for any cause 16 (65) 20 (81) 19 (78) 10 (4) 20 (81) 8 (33) 20 (82) 17 (69)
Death for cardiovascular cause 9 (37) 13 (52) 10 (41) 4 (16) 12 (49) 7 (29) 12 (49) 6 (24)
Myocardial infarction 14 (57) 12 (48) 9 (37) 4 (16) 15 (61) 4 (16) 14 (57) 8 (32)
Cerebrovascular accident 7 (28) 7 (28) 5 (2) 1 (04) 5 (2) 1 (04) 4 (16) 2 (08)
Definite stent thrombosis
Late 3 (12) 2 (08) 1 (04) 0 (0) 1 (04) 0 (0) 2 (08) 1 (04)
Very late 0 (0) 1 (04) 0 (0) 1 (04) 0 (0) 0 (0) 3 (13) 0 (0)
Cumulative 3 (12) 3 (12) 1 (04) 1 (04) 1 (04) 0 (0) 5 (2) 1 (04)
Definite or probable stent thrombosis
Late 5 (2) 2 (08) 3 (12) 0 (0) 5 (2) 0 (0) 3 (12) 1 (04)
Very late 0 (0) 1 (04) 1 (04) 1 (04) 0 (0) 0 (0) 6 (26) 0 (0)
Cumulative 5 (2) 3 (12) 4 (16) 1 (04) 5 (2) 0 (0) 9 (37) 1 (04)
Definite probable or possible stent thrombosis
Late 7 (28) 8 (32) 8 (32) 3 (12) 10 (41) 4 (16) 10 (41) 4 (16)
Very late 2 (08) 5 (21) 3 (13) 2 (08) 5 (21) 3 (13) 8 (34) 2 (08)
Cumulative 9 (37) 13 (52) 11 (45) 5 (2) 15 (61) 7 (29) 18 (74) 6 (24)
Dual antiplatelet therapy and stent-type Page 7 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 1 Stent analyses of the primary study endpoint and other secondary clinical outcomes Stent-specific analyses are shown with hazardratios and 95 confidence intervals for the primary end point of death for any cause myocardial infarction (MI) or cerebrovascular accident(CVA) death or MI and cardiovascular (CV) death or MI among patients randomly assigned to either the six or the 24-month clopidogreltherapy The P-value for interaction represents the likelihood of interaction between the variable and the relative treatment effect
Figure 2 Stent analyses of the stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95 confidence inter-vals for the definite definite probable and definite probable possible stent thrombosis (ST) among patients randomly assigned to either the 6or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction between the variable and the relativetreatment effect
M Valgimigli et alPage 8 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 3 Stent analyses of the 6-month landmark primary study endpoint and other secondary clinical outcomes Stent-specific analyses areshown with hazard ratios and 95 confidence intervals for the 6-month landmark analyses of the primary endpoint of death for any causemyocardial infarction (MI) or cerebrovascular accident (CVA) death or MI and cardiovascular (CV) death or MI among patients randomlyassigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction betweenthe variable and the relative treatment effect
Figure 4 Stent analyses of the 6-month landmark stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95confidence intervals for the 6-month landmark analyses of definite definite probable and definite probable possible stent thrombosis (ST)among patients randomly assigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihoodof interaction between the variable and the relative treatment effect
Dual antiplatelet therapy and stent-type Page 9 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
(ZEUS) study is comparing ZES-S vs BMS in patients at highthrombotic bleeding or low restenosis risk allowing 1-monthDAPT duration in both stent arms in patients who cannot toleratelonger duration of therapy (NCT01385319)
Reassuring data on the safety of early DAPT discontinuationafter EES have also been reported by a retrospective analysis ofregistry data7 Moreover the pooled analysis of SPIRIT II III IVand COMPARE Trials of 6789 patients showed a persistentlylow ST rate in patients treated with EES but not PES who discon-tinued DAPT after 6 months which is consistent with our currentfindings16 Indeed while our analysis on primary study endpointand other secondary clinical outcomes numerically favoured long-term DAPT after EES implantation the stent thrombosis endpointsand 6-month clinical landmark analyses revealed no excess ofevents in the 6-month DAPT group compared with longer-termclopidogrel therapy which is at variance with the results observedafter PES implantation
The need for prolonged DAPT has been suggested to be in-versely related to stent late loss17 Potent inhibition of intimal
hyperplasia might more frequently lead to incomplete stent cover-age andor late stent mal-apposition requiring a more prolongedcourse of intensified anti-platelet therapy to maintain stentsafety17
Our study by randomizing patients to a balanced mixture ofstents with various anti-intimal hyperplasia and each stent groupto 6- vs 24-month DAPT duration offers no evidence supportingthe association between stent-related late-loss and need for pro-longed DAPT On the contrary the results of our explorativeyet pre-specified analysis suggest that the minimal DAPT durationmay be stent-specific and not clearly related to stent potencytowards inhibition of intimal hyperplasia
Several limitations of our study should be considered Our studywas not powered to assess outcomes with respect to the differentDAPT regimens tested in our study for each stent type Similarlyour study was overall underpowered to assess the effect ofDAPT duration on stent thrombosis endpoints Therefore ourfindings should be considered exploratory and hypothesisgenerating
Our observation that primary study endpoint and other second-ary clinical ischaemic endpoints may be significantly lower after6-month compared with 24-month DAPT duration in ZES-Streated patients is intriguing but it should be interpreted withcaution In light of the limitations outlined above this findingshould be reassuring on the safety of early DAPT discontinuationin patients treated with ZES-S Yet a new paradigm has beenrecently proposed by the results of the WOEST study (clinicaltrialsgov NCT00769938) according to which lessening intensity of anti-platelet inhibition via dropping aspirin has resulted in a dramaticreduction of not only bleeding but also ischaemic endpoints includ-ing overall and cardiac mortality This paradigm has also been shownto apply to periprocedural anti-thrombotic therapy and it will befurther investigated in the ongoing comparative effectiveness of1 month of ticagrelor plus aspirin followed by ticagrelor monother-apy vs a current-day intensive DAPT in all-comer patients undergo-ing percutaneous coronary intervention with unrestricted BiolimusA9-eluting stent (GLOBAL LEADERS) study
In conclusion our study offers preliminary evidence that optimalduration of DAPT may be stent-specific with no clear associationbetween late loss potency and vulnerability to shorter DAPT dur-ation DES-specific studies aiming at unraveling the optimal DAPTduration after stent implantation are eagerly required and some ofthem are currently ongoing
Conflict of interest MV has received honoraria for lecturesad-visory board and research grants from Merck Iroko Eli Lilly andMedtronic honoraria for advisory board and lectures from TheMedicines Company and Eli Lilly Co Daiichi Sankyo Inc St Judeand Abbott Vascular lectures from Cordis CID and Terumo
FundingThe study is an investigator-driven clinical trial The conduct of thisstudy did not receive any direct or indirect external funding but wasentirely supported by the University of Ferrara which employed dedi-cated personnel for data monitoring data management events adjudi-cation and independent statistical analysis
Figure 5 Stent potency in inhibiting repeated intervention andrelative risks of adverse outcomes after 6-month dual anti-platelet therapy Relative risk reductions and corresponding95 confidence intervals (vertical bars) for target lesion revascu-larization from 30 days onwards for each drug-eluting stentemployed in the study when compared with bare metal stentgroup (reference group) is shown to the left In the middle rela-tive risk reductions and corresponding 95 confidence intervals(vertical bars) for 6-month landmark analysis of death myocardialinfarction or stroke in the 6-month when compared with24-month dual antiplatelet group is shown for each stent Inthe right portion of the figure relative risk reductions and corre-sponding 95 confidence intervals (vertical bars) for 6-monthlandmark analysis of definite probable or possible stent throm-bosis (ST) in the 6-month when compared with 24-month dualantiplatelet group is shown for each stent Note that a negativerelative risk reduction such as that observed for PES or BMSgroups implies the possibility of a relative risk increase in thestudy arm when compared with reference group EP endpointTLR target lesion revascularization from 30 days onwards Ddeath MI myocardial infarction CV cerebrovascular accidentDAPT dual antiplatelet therapy ST stent thrombosis Ref refer-ence arm BMS bare metal stent ZES-S zotarolimus-eluting stentEndeavor Sprint PES paclitaxel-eluting stent EES everolimus-eluting stent
M Valgimigli et alPage 10 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from

The composite of definite or probable [HR 012 (95CI 002ndash100) P frac14 0049] and definite probable or possible ST [HR 025(95CI 007ndash088) P frac14 0031] were both significantly lower inthe 24-month DAPT arm in patients receiving PES but not inthose treated for the other stent types (Figure 4) Yet no formalsignal for interaction was noted for stent thrombosis endpointsacross DAPT groups for each stent-type which suggests a lackof study power for this analysis (there were only three definiteprobable or possible ST events in the long when compared with12 in the short-term DAPT group in the PES arm) or the factthat results for stent thrombosis endpoints across stent groupsare consistent with the overall study findings
At per protocol analysis a consistent signal of heterogeneityacross stent types for the definite probable or possible ST wasalso observed (P-value frac14 007)
Stent potency and outcomes in relationto DAPT durationThe re-intervention rates in the target lesion(s) from 30 daysonwards was 159 in the BMS 114 in the ZES-S 60 in thePES and 49 in the EES groups (P00001 for the trend)which is consistent with the expected stent efficacy profiles
based on previously reported stent-specific late loss figuresSetting BMS as reference group ZES-S PES or EES implantationresulted in a relative risk reduction for TLR in the range of 29(95CI 129ndash555) 63 (95CI 384ndash873) or 69 (95CI460ndash936) respectively (Figure 5)
As shown in Figure 5 the relative risks of death non-fatal myo-cardial infarction or non-fatal stroke from 6 months onwards (iewhen DAPT largely differed in the two DAPT treatment groups) aswell as the 6-month landmark definite probable or possible stentthrombosis rates in the short when compared with the long-termDAPT group was not affected by the actual (ie based on theobserved TLR rates in the study) or expected (ie based on lateloss figures in previously reported studies) potency of each stenttype to inhibit intimal hyperplasia
DiscussionWe found that the composite of death myocardial infarction orcerebrovascular accident did not differ in patients receiving BMSPES or EES implantation across DAPT groups whereas it was sig-nificantly lower in ZES-S patients undergoing short when com-pared with long-term DAPT therapy with positive interaction
Table 1 Base-line characteristics of the patients
Characteristics 24-month clopidogrel 6-month clopidogrel P-value
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Age (year) 69+11 67+11 67+12 68+11 68+11 68+12 68+11 68+11 032
Male sex n () 181 (74) 195 (79) 191 (78) 197 (79) 174 (71) 190 (78) 187 (76) 196 (79) 026
Body mass index (kgm2) 29+5 27+4 27+4 28+4 27+4 28+4 28+5 27+4 067
Diabetes n () 62 (25) 60 (24) 68 (28) 54 (22) 48 (20) 58 (24) 69 (28) 58 (24) 036
Insulin-dependent n () 12 (5) 20 (8) 18 (7) 9 (4) 9 (4) 17 (7) 12 (5) 17 (7) 024
Hypertension n () 180 (73) 177 (71) 181 (74) 183 (74) 188 (76) 159 (65) 177 (72) 169 (68) 019
Hyperlipidaemia n () 124 (50) 138 (56) 137 (56) 154 (62) 124 (50) 122 (50) 140 (57) 139 (56) 009
Current smoking n () 61 (25) 58 (23) 49 (20) 54 (22) 63 (26) 67 (28) 60 (24) 57 (23) 056
Creatinine clearance (mLmin) 77+31 80+36 81+33 80+34 78+29 79+31 77+29 77+32 053
Prior MI n () 61 (25) 64 (26) 82 (33) 63 (25) 56 (23) 67 (27) 56 (23) 79 (32) 051
Prior CABG n () 24 (10) 23 (9) 31 (13) 32 (13) 19 (8) 34 (14) 23 (9) 29 (12) 029
Prior stroke or TIA n () 9 (4) 8 (3) 9 (4) 11 (4) 11 (4) 9 (4) 9 (4) 10 (4) 087
LVEF 50+11 52+10 50+10 51+10 51+10 50+11 51+11 50+10 016
Clinical presentation n ()
Stable angina pectoris 57 (23) 65 (26) 75 (31) 58 (23) 56 (23) 65 (27) 68 (28) 61 (25) 049
Acute Coronary syndrome 189 (77) 183 (74) 170 (69) 190 (77) 191 (78) 180 (73) 176 (72) 186 (76) 058
Non-ST-elevation ACS 107 (43) 95 (38) 101 (41) 108 (44) 102 (41) 96 (39) 102 (42) 106 (43) 066
Unstable angina 50 (19) 39 (16) 44 (18) 52 (21) 43 (17) 53 (22) 39 (16) 47 (19) 055
Non-ST-elevation MI 57 (23) 56 (23) 57 (23) 56 (23) 59 (24) 43 (18) 63 (26) 59 (24) 068
ST-segment-elevation MI 82 (33) 88 (35) 69 (28) 82 (33) 89 (36) 84 (34) 74 (30) 80 (32) 076
Angiographic features n ()
Single-vessel disease 87 (35) 78 (32) 69 (28) 68 (27) 83 (34) 61 (25) 79 (32) 76 (31) 018
Multi-vessel disease 159 (65) 170 (69) 176 (72) 180 (73) 163 (66) 184 (75) 166 (68) 171 (69)
ACS acute coronary syndrome LVEF left-ventricular ejection fraction
M Valgimigli et alPage 4 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Table 2 Procedural results
Characteristic 24-month clopidogrel 6-month clopidogrel P-value
BMS (n 5 246) ZES (n 5 248) PES (n 5 245) EES (n5 248) BMS (n5 246) ZES (n 5 245) PES (n 5 245) EES (n 5 247)
Number of treated lesions 147+08 153+09 151+09 151+08 148+08 160+10 164+10 156+09 035
ge2 treated lesions n () 85 (35) 97 (39) 83 (34) 100 (40) 83 (34) 92 (38) 104 (42) 92 (37) 038
ge3 treated lesions n () 23 (9) 28 (11) 29 (12) 28 (11) 23 (9) 31 (13) 33 (14) 28 (11) 082
ge4 treated lesions n () 8 (3) 13 (5) 12 (5) 5 (2) 7 (3) 14 (6) 11 (4) 12 (5) 034
LAD treated n () 150 (61) 146 (59) 136 (56) 141 (57) 137 (56) 149 (61) 142 (58) 146 (59) 043
CFX treated n () 66 (27) 69 (28) 84 (34) 102 (41) 81 (33) 78 (32) 76 (31) 83 (34) 003
RCA treated n () 87 (35) 92 (37) 88 (36) 79 (32) 98 (40) 86 (35) 84 (34) 95 (38) 070
SVG treated n () 5 (2) 6 (2) 6 (2) 6 (2) 4 (2) 5 (2) 3 (1) 5 (2) 073
At least one complex (type B2 or C)lesion n ()a
152 (62) 168 (68) 164 (67) 158 (64) 160 (65) 175 (71) 175 (71) 154 (62) 014
Total ACCAHA scoreab 37+21 37+22 38+23 39+22 37+22 39+23 39+23 40+24 028
Number of stents implanted 182+12 191+13 181+13 177+11 177+11 196+13 188+12 196+13 034
Length of stent (mm) 39+35 41+32 39+29 37+24 36+25 42+30 40+27 42+32 013
Quantitative coronary analysis
Lesion length (mm) 1307+845 1318+832 1409+951 1313+835 1351+825 1323+824 1375+898 1427+864 049
RVD before (mm) 264+054 264+051 269+053 263+056 267+053 261+063 260+053 268+053 031
MLD before (mm) 060+039 061+038 058+041 059+041 056+041 056+041 055+037 058+036 066
Stenosis before () 78+14 77+13 79+14 78+16 79+14 77+17 78+14 79+12 055
RVD after (mm) 276+050 274+042 286+047 276+050 279+046 279+054 279+051 279+048 047
MLD after (mm) 242+056 246+046 253+046 245+049 244+049 247+054 242+053 252+046 027
Stenosis after () 1057+825 968+874 1001+748 1104+867 1129+841 1025+799 1113+876 1145+933 032
aCalculated in 952 patients in the 24-month clopidogrel arm and in 943 patients in the 6-month clopidogrel arm who presented at least one de-novo lesion ACCAHA score was missing in three patientsLAD left anterior descending artery CFX circumflex artery RCA right coronary artery LMCA left main coronary artery SVG saphenous vein graftbAs previously described18 type A stenoses were coded 1 point typeB1 stenoses 2 points type B2 stenoses 3 points and type C stenoses 4 points
Dualantiplatelet
therapyand
stent-typeP
age5
of
11
at UniversitAtilde degli Studi di Brescia on January 16 2013 httpeurheartjoxfordjournalsorg Downloaded from
testing At the 6-month landmark analysis heterogeneity acrossstent types persisted whereas patients receiving PES showed a sig-nificantly higher rate of stent thrombosis in the short DAPTregimen No association was noted between expected or actualstent potency in inhibiting intimal hyperplasia and greater vulner-ability to shorter DAPT therapy
The main findings of our analysis challenge current recommen-dations endorsing a clear-cut dichotomy of BMS vs DES for theneed of prolonged DAPT after stenting Furthermore our datasuggest minimal duration of clopidogrel therapy may differamong DES irrespective of stent potency in inhibiting intimalhyperplasia
As previously reported9 no interaction was noted between BMSand the three different DES type clustered together with respectto duration of DAPT therapy On the other hand in the currentanalysis focusing on each DES type individually a clear andformal signal of heterogeneity with respect to overall death myo-cardial infarction or cerebrovascular accidents was noted for theneed of prolonged therapy with clopidogrel after interventionThis was driven by ZES-S treated patients showing an improvedprimary study and other secondary clinical outcomes with short-term DAPT when compared with 24-month duration of therapyand by an excess of stent thrombosis events particularly definiteor probable and definite probable or possible ST in patients
Table 3 Use of anti-platelet medications during the trial
24-month clopidogrel 6-month clopidogrel P-value
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Anti-platelet therapy at 30 days n ()
Numberevaluated
246 248 245 248 246 245 245 247
Aspirin 246 (100) 248 (100) 245 (100) 248 (100) 246 (100) 245 (100) 245 (100) 247 (100) 099
Clopidogrel 245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Aspirin andclopidogrel
245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Anti-platelet therapy at 6 months n ()
Numberevaluated total
241 241 238 246 240 244 239 240
Aspirin 240 (996) 240 (996) 234 (983) 246 (100) 236 (983) 241 (988) 238 (996) 238 (996) 024
Clopidogrel 239 (992) 239 (992) 237 (976) 245 (996) 94 (392) 241 (988) 234 (979) 236 (983) 0001
Aspirin andclopidogrel
238 (988) 238 (988) 233 (979) 245 (996) 97 (392) 238 (976) 233 (975) 235 (979) 0001
Anti-platelet therapy at 12 months n ()
Numberevaluated total
236 238 231 243 232 240 233 237
Aspirin 233 (987) 237 (996) 226 (978) 243 (100) 223 (961) 236 (983) 231 (991) 235 (992) 012
Clopidogrel 233 (987) 232 (975) 228 (987) 239 (983) 8 (35) 12 (5) 7 (3) 6 (25) 0001
Aspirin andClopidogrel
230 (975) 231 (971) 223 (965) 239 (984) 8 (35) 12 (5) 6 (26) 6 (25) 0001
Anti-platelet therapy at 18 months n ()
Numberevaluated total
234 234 227 238 231 239 228 234 034
Aspirin 232 (992) 232 (992) 223 (982) 234 (983) 221 (957) 232 (971) 226 (992) 233 (996) 012
Clopidogrel 231 (987) 222 (989) 220 (969) 231 (971) 2 (09) 2 (09) 3 (13) 1 (04) 0001
Aspirin andclopidogrel
229 (979) 221 (944) 216 (952) 229 (962) 2 (09) 1 (04) 2 (09) 1 (04) 0001
Anti-platelet therapy at 24 months n ()
Numberevaluated total
230 228 224 238 227 237 226 230
Aspirin 228 (991) 224 (983) 219 (978) 234 (983) 216 (952) 230 (971) 221 (978) 229 (996) 019
Clopidogrel 226 (983) 212 (93) 214 (955) 228 (958) 0 2 (08) 3 (13) 0 0001
Aspirin andclopidogrel
224 (974) 210 (921) 211 (942) 226 (947) 0 1 (04) 2 (09) 0 0001
M Valgimigli et alPage 6 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
undergoing 6-month clopidogrel therapy after PES implantationcompared with a longer duration of therapy
In our study adherence to aspirin and clopidogrel was similarlyhigh in the first 6 months after DES implantation in the two DAPTgroups Therefore events occurring during this time period in thethree DES groups may potentially confound the outcomes of thetwo different DAPT regimens tested in the study Based on thisnotion a landmark analysis focusing on events occurring after a6 month-follow-up has been pre-specified and previously reportedfor the whole patient population or for all DES treated patientsclustered together When the three tested DES types were ana-lysed separately at the 6-month landmark analysis the resultswere largely consistent with the findings observed for the entirefollow-up duration (i) patients treated with ZES-S showed abetter ischaemic outcomes in the 6-month when compared withthe 24-month DAPT groups (ii) event rates for the primary or sec-ondary ischaemic clinical endpoints were similar between DAPTgroups after BMS or EES implantation (iii) the primary clinicalcomposite endpoint trended higher and the ST rates were signifi-cantly increased in PES treated patients receiving PES and
undergoing 6-month when compared with 24-month duration ofclopidogrel
Kandzari et al6 recently analysed outcomes in 2032 patientsundergoing coronary revascularization with ZES-S in five trialswho for various reasons discontinued DAPT at 6 months andfound that outcomes did not differ compared with patients whoreceived longer clopidogrel therapy (up to 12 or 24 months)
In the Real Safety and Efficacy of 3-Month Dual AntiplateletTherapy Following Zotarolimus-Eluting Stent Implantation(RESET) trial of 2148 patients randomized to the ZES-S stentand three months of DAPT and 1058 patients treated with stand-ard 12-month DAPT and other DES the combined endpoint ofany death MI stent thrombosis occurred in 13 in the standardtherapy arm vs 08 in the 3-month group (P frac14 048)12 Interest-ingly prospective studies undertaken to evaluate the degree ofZES-S stent coverage have consistently showed a very low rateof uncoveredmalapposed struts at 6- or even 3-month optical co-herence tomography evaluation which favourably compared withboth first generation DES or even BMS13 ndash15 Based on thisfinding the Zotarolimus-eluting stent in uncertain DES candidates
Table 4 Outcome rates at 24 months according to treatment group
Outcome 24-month clopidogrel 6-month clopidogrel
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Death for any cause myocardialinfarction or cerebrovascularaccident
29 (118) 33 (133) 23 (94) 15 (61) 32 (13) 12 (49) 31 (127) 23 (91)
Death for cardiovascular causemyocardial infarction orcerebrovascular accident
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (56)
Death for any cause ormyocardial infarction
25 (102) 27 (109) 22 (89) 14 (57) 30 (122) 12 (49) 31 (127) 21 (85)
Death for cardiovascular causemyocardial infarction
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (53)
Death for any cause 16 (65) 20 (81) 19 (78) 10 (4) 20 (81) 8 (33) 20 (82) 17 (69)
Death for cardiovascular cause 9 (37) 13 (52) 10 (41) 4 (16) 12 (49) 7 (29) 12 (49) 6 (24)
Myocardial infarction 14 (57) 12 (48) 9 (37) 4 (16) 15 (61) 4 (16) 14 (57) 8 (32)
Cerebrovascular accident 7 (28) 7 (28) 5 (2) 1 (04) 5 (2) 1 (04) 4 (16) 2 (08)
Definite stent thrombosis
Late 3 (12) 2 (08) 1 (04) 0 (0) 1 (04) 0 (0) 2 (08) 1 (04)
Very late 0 (0) 1 (04) 0 (0) 1 (04) 0 (0) 0 (0) 3 (13) 0 (0)
Cumulative 3 (12) 3 (12) 1 (04) 1 (04) 1 (04) 0 (0) 5 (2) 1 (04)
Definite or probable stent thrombosis
Late 5 (2) 2 (08) 3 (12) 0 (0) 5 (2) 0 (0) 3 (12) 1 (04)
Very late 0 (0) 1 (04) 1 (04) 1 (04) 0 (0) 0 (0) 6 (26) 0 (0)
Cumulative 5 (2) 3 (12) 4 (16) 1 (04) 5 (2) 0 (0) 9 (37) 1 (04)
Definite probable or possible stent thrombosis
Late 7 (28) 8 (32) 8 (32) 3 (12) 10 (41) 4 (16) 10 (41) 4 (16)
Very late 2 (08) 5 (21) 3 (13) 2 (08) 5 (21) 3 (13) 8 (34) 2 (08)
Cumulative 9 (37) 13 (52) 11 (45) 5 (2) 15 (61) 7 (29) 18 (74) 6 (24)
Dual antiplatelet therapy and stent-type Page 7 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 1 Stent analyses of the primary study endpoint and other secondary clinical outcomes Stent-specific analyses are shown with hazardratios and 95 confidence intervals for the primary end point of death for any cause myocardial infarction (MI) or cerebrovascular accident(CVA) death or MI and cardiovascular (CV) death or MI among patients randomly assigned to either the six or the 24-month clopidogreltherapy The P-value for interaction represents the likelihood of interaction between the variable and the relative treatment effect
Figure 2 Stent analyses of the stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95 confidence inter-vals for the definite definite probable and definite probable possible stent thrombosis (ST) among patients randomly assigned to either the 6or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction between the variable and the relativetreatment effect
M Valgimigli et alPage 8 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 3 Stent analyses of the 6-month landmark primary study endpoint and other secondary clinical outcomes Stent-specific analyses areshown with hazard ratios and 95 confidence intervals for the 6-month landmark analyses of the primary endpoint of death for any causemyocardial infarction (MI) or cerebrovascular accident (CVA) death or MI and cardiovascular (CV) death or MI among patients randomlyassigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction betweenthe variable and the relative treatment effect
Figure 4 Stent analyses of the 6-month landmark stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95confidence intervals for the 6-month landmark analyses of definite definite probable and definite probable possible stent thrombosis (ST)among patients randomly assigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihoodof interaction between the variable and the relative treatment effect
Dual antiplatelet therapy and stent-type Page 9 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
(ZEUS) study is comparing ZES-S vs BMS in patients at highthrombotic bleeding or low restenosis risk allowing 1-monthDAPT duration in both stent arms in patients who cannot toleratelonger duration of therapy (NCT01385319)
Reassuring data on the safety of early DAPT discontinuationafter EES have also been reported by a retrospective analysis ofregistry data7 Moreover the pooled analysis of SPIRIT II III IVand COMPARE Trials of 6789 patients showed a persistentlylow ST rate in patients treated with EES but not PES who discon-tinued DAPT after 6 months which is consistent with our currentfindings16 Indeed while our analysis on primary study endpointand other secondary clinical outcomes numerically favoured long-term DAPT after EES implantation the stent thrombosis endpointsand 6-month clinical landmark analyses revealed no excess ofevents in the 6-month DAPT group compared with longer-termclopidogrel therapy which is at variance with the results observedafter PES implantation
The need for prolonged DAPT has been suggested to be in-versely related to stent late loss17 Potent inhibition of intimal
hyperplasia might more frequently lead to incomplete stent cover-age andor late stent mal-apposition requiring a more prolongedcourse of intensified anti-platelet therapy to maintain stentsafety17
Our study by randomizing patients to a balanced mixture ofstents with various anti-intimal hyperplasia and each stent groupto 6- vs 24-month DAPT duration offers no evidence supportingthe association between stent-related late-loss and need for pro-longed DAPT On the contrary the results of our explorativeyet pre-specified analysis suggest that the minimal DAPT durationmay be stent-specific and not clearly related to stent potencytowards inhibition of intimal hyperplasia
Several limitations of our study should be considered Our studywas not powered to assess outcomes with respect to the differentDAPT regimens tested in our study for each stent type Similarlyour study was overall underpowered to assess the effect ofDAPT duration on stent thrombosis endpoints Therefore ourfindings should be considered exploratory and hypothesisgenerating
Our observation that primary study endpoint and other second-ary clinical ischaemic endpoints may be significantly lower after6-month compared with 24-month DAPT duration in ZES-Streated patients is intriguing but it should be interpreted withcaution In light of the limitations outlined above this findingshould be reassuring on the safety of early DAPT discontinuationin patients treated with ZES-S Yet a new paradigm has beenrecently proposed by the results of the WOEST study (clinicaltrialsgov NCT00769938) according to which lessening intensity of anti-platelet inhibition via dropping aspirin has resulted in a dramaticreduction of not only bleeding but also ischaemic endpoints includ-ing overall and cardiac mortality This paradigm has also been shownto apply to periprocedural anti-thrombotic therapy and it will befurther investigated in the ongoing comparative effectiveness of1 month of ticagrelor plus aspirin followed by ticagrelor monother-apy vs a current-day intensive DAPT in all-comer patients undergo-ing percutaneous coronary intervention with unrestricted BiolimusA9-eluting stent (GLOBAL LEADERS) study
In conclusion our study offers preliminary evidence that optimalduration of DAPT may be stent-specific with no clear associationbetween late loss potency and vulnerability to shorter DAPT dur-ation DES-specific studies aiming at unraveling the optimal DAPTduration after stent implantation are eagerly required and some ofthem are currently ongoing
Conflict of interest MV has received honoraria for lecturesad-visory board and research grants from Merck Iroko Eli Lilly andMedtronic honoraria for advisory board and lectures from TheMedicines Company and Eli Lilly Co Daiichi Sankyo Inc St Judeand Abbott Vascular lectures from Cordis CID and Terumo
FundingThe study is an investigator-driven clinical trial The conduct of thisstudy did not receive any direct or indirect external funding but wasentirely supported by the University of Ferrara which employed dedi-cated personnel for data monitoring data management events adjudi-cation and independent statistical analysis
Figure 5 Stent potency in inhibiting repeated intervention andrelative risks of adverse outcomes after 6-month dual anti-platelet therapy Relative risk reductions and corresponding95 confidence intervals (vertical bars) for target lesion revascu-larization from 30 days onwards for each drug-eluting stentemployed in the study when compared with bare metal stentgroup (reference group) is shown to the left In the middle rela-tive risk reductions and corresponding 95 confidence intervals(vertical bars) for 6-month landmark analysis of death myocardialinfarction or stroke in the 6-month when compared with24-month dual antiplatelet group is shown for each stent Inthe right portion of the figure relative risk reductions and corre-sponding 95 confidence intervals (vertical bars) for 6-monthlandmark analysis of definite probable or possible stent throm-bosis (ST) in the 6-month when compared with 24-month dualantiplatelet group is shown for each stent Note that a negativerelative risk reduction such as that observed for PES or BMSgroups implies the possibility of a relative risk increase in thestudy arm when compared with reference group EP endpointTLR target lesion revascularization from 30 days onwards Ddeath MI myocardial infarction CV cerebrovascular accidentDAPT dual antiplatelet therapy ST stent thrombosis Ref refer-ence arm BMS bare metal stent ZES-S zotarolimus-eluting stentEndeavor Sprint PES paclitaxel-eluting stent EES everolimus-eluting stent
M Valgimigli et alPage 10 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from

Table 2 Procedural results
Characteristic 24-month clopidogrel 6-month clopidogrel P-value
BMS (n 5 246) ZES (n 5 248) PES (n 5 245) EES (n5 248) BMS (n5 246) ZES (n 5 245) PES (n 5 245) EES (n 5 247)
Number of treated lesions 147+08 153+09 151+09 151+08 148+08 160+10 164+10 156+09 035
ge2 treated lesions n () 85 (35) 97 (39) 83 (34) 100 (40) 83 (34) 92 (38) 104 (42) 92 (37) 038
ge3 treated lesions n () 23 (9) 28 (11) 29 (12) 28 (11) 23 (9) 31 (13) 33 (14) 28 (11) 082
ge4 treated lesions n () 8 (3) 13 (5) 12 (5) 5 (2) 7 (3) 14 (6) 11 (4) 12 (5) 034
LAD treated n () 150 (61) 146 (59) 136 (56) 141 (57) 137 (56) 149 (61) 142 (58) 146 (59) 043
CFX treated n () 66 (27) 69 (28) 84 (34) 102 (41) 81 (33) 78 (32) 76 (31) 83 (34) 003
RCA treated n () 87 (35) 92 (37) 88 (36) 79 (32) 98 (40) 86 (35) 84 (34) 95 (38) 070
SVG treated n () 5 (2) 6 (2) 6 (2) 6 (2) 4 (2) 5 (2) 3 (1) 5 (2) 073
At least one complex (type B2 or C)lesion n ()a
152 (62) 168 (68) 164 (67) 158 (64) 160 (65) 175 (71) 175 (71) 154 (62) 014
Total ACCAHA scoreab 37+21 37+22 38+23 39+22 37+22 39+23 39+23 40+24 028
Number of stents implanted 182+12 191+13 181+13 177+11 177+11 196+13 188+12 196+13 034
Length of stent (mm) 39+35 41+32 39+29 37+24 36+25 42+30 40+27 42+32 013
Quantitative coronary analysis
Lesion length (mm) 1307+845 1318+832 1409+951 1313+835 1351+825 1323+824 1375+898 1427+864 049
RVD before (mm) 264+054 264+051 269+053 263+056 267+053 261+063 260+053 268+053 031
MLD before (mm) 060+039 061+038 058+041 059+041 056+041 056+041 055+037 058+036 066
Stenosis before () 78+14 77+13 79+14 78+16 79+14 77+17 78+14 79+12 055
RVD after (mm) 276+050 274+042 286+047 276+050 279+046 279+054 279+051 279+048 047
MLD after (mm) 242+056 246+046 253+046 245+049 244+049 247+054 242+053 252+046 027
Stenosis after () 1057+825 968+874 1001+748 1104+867 1129+841 1025+799 1113+876 1145+933 032
aCalculated in 952 patients in the 24-month clopidogrel arm and in 943 patients in the 6-month clopidogrel arm who presented at least one de-novo lesion ACCAHA score was missing in three patientsLAD left anterior descending artery CFX circumflex artery RCA right coronary artery LMCA left main coronary artery SVG saphenous vein graftbAs previously described18 type A stenoses were coded 1 point typeB1 stenoses 2 points type B2 stenoses 3 points and type C stenoses 4 points
Dualantiplatelet
therapyand
stent-typeP
age5
of
11
at UniversitAtilde degli Studi di Brescia on January 16 2013 httpeurheartjoxfordjournalsorg Downloaded from
testing At the 6-month landmark analysis heterogeneity acrossstent types persisted whereas patients receiving PES showed a sig-nificantly higher rate of stent thrombosis in the short DAPTregimen No association was noted between expected or actualstent potency in inhibiting intimal hyperplasia and greater vulner-ability to shorter DAPT therapy
The main findings of our analysis challenge current recommen-dations endorsing a clear-cut dichotomy of BMS vs DES for theneed of prolonged DAPT after stenting Furthermore our datasuggest minimal duration of clopidogrel therapy may differamong DES irrespective of stent potency in inhibiting intimalhyperplasia
As previously reported9 no interaction was noted between BMSand the three different DES type clustered together with respectto duration of DAPT therapy On the other hand in the currentanalysis focusing on each DES type individually a clear andformal signal of heterogeneity with respect to overall death myo-cardial infarction or cerebrovascular accidents was noted for theneed of prolonged therapy with clopidogrel after interventionThis was driven by ZES-S treated patients showing an improvedprimary study and other secondary clinical outcomes with short-term DAPT when compared with 24-month duration of therapyand by an excess of stent thrombosis events particularly definiteor probable and definite probable or possible ST in patients
Table 3 Use of anti-platelet medications during the trial
24-month clopidogrel 6-month clopidogrel P-value
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Anti-platelet therapy at 30 days n ()
Numberevaluated
246 248 245 248 246 245 245 247
Aspirin 246 (100) 248 (100) 245 (100) 248 (100) 246 (100) 245 (100) 245 (100) 247 (100) 099
Clopidogrel 245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Aspirin andclopidogrel
245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Anti-platelet therapy at 6 months n ()
Numberevaluated total
241 241 238 246 240 244 239 240
Aspirin 240 (996) 240 (996) 234 (983) 246 (100) 236 (983) 241 (988) 238 (996) 238 (996) 024
Clopidogrel 239 (992) 239 (992) 237 (976) 245 (996) 94 (392) 241 (988) 234 (979) 236 (983) 0001
Aspirin andclopidogrel
238 (988) 238 (988) 233 (979) 245 (996) 97 (392) 238 (976) 233 (975) 235 (979) 0001
Anti-platelet therapy at 12 months n ()
Numberevaluated total
236 238 231 243 232 240 233 237
Aspirin 233 (987) 237 (996) 226 (978) 243 (100) 223 (961) 236 (983) 231 (991) 235 (992) 012
Clopidogrel 233 (987) 232 (975) 228 (987) 239 (983) 8 (35) 12 (5) 7 (3) 6 (25) 0001
Aspirin andClopidogrel
230 (975) 231 (971) 223 (965) 239 (984) 8 (35) 12 (5) 6 (26) 6 (25) 0001
Anti-platelet therapy at 18 months n ()
Numberevaluated total
234 234 227 238 231 239 228 234 034
Aspirin 232 (992) 232 (992) 223 (982) 234 (983) 221 (957) 232 (971) 226 (992) 233 (996) 012
Clopidogrel 231 (987) 222 (989) 220 (969) 231 (971) 2 (09) 2 (09) 3 (13) 1 (04) 0001
Aspirin andclopidogrel
229 (979) 221 (944) 216 (952) 229 (962) 2 (09) 1 (04) 2 (09) 1 (04) 0001
Anti-platelet therapy at 24 months n ()
Numberevaluated total
230 228 224 238 227 237 226 230
Aspirin 228 (991) 224 (983) 219 (978) 234 (983) 216 (952) 230 (971) 221 (978) 229 (996) 019
Clopidogrel 226 (983) 212 (93) 214 (955) 228 (958) 0 2 (08) 3 (13) 0 0001
Aspirin andclopidogrel
224 (974) 210 (921) 211 (942) 226 (947) 0 1 (04) 2 (09) 0 0001
M Valgimigli et alPage 6 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
undergoing 6-month clopidogrel therapy after PES implantationcompared with a longer duration of therapy
In our study adherence to aspirin and clopidogrel was similarlyhigh in the first 6 months after DES implantation in the two DAPTgroups Therefore events occurring during this time period in thethree DES groups may potentially confound the outcomes of thetwo different DAPT regimens tested in the study Based on thisnotion a landmark analysis focusing on events occurring after a6 month-follow-up has been pre-specified and previously reportedfor the whole patient population or for all DES treated patientsclustered together When the three tested DES types were ana-lysed separately at the 6-month landmark analysis the resultswere largely consistent with the findings observed for the entirefollow-up duration (i) patients treated with ZES-S showed abetter ischaemic outcomes in the 6-month when compared withthe 24-month DAPT groups (ii) event rates for the primary or sec-ondary ischaemic clinical endpoints were similar between DAPTgroups after BMS or EES implantation (iii) the primary clinicalcomposite endpoint trended higher and the ST rates were signifi-cantly increased in PES treated patients receiving PES and
undergoing 6-month when compared with 24-month duration ofclopidogrel
Kandzari et al6 recently analysed outcomes in 2032 patientsundergoing coronary revascularization with ZES-S in five trialswho for various reasons discontinued DAPT at 6 months andfound that outcomes did not differ compared with patients whoreceived longer clopidogrel therapy (up to 12 or 24 months)
In the Real Safety and Efficacy of 3-Month Dual AntiplateletTherapy Following Zotarolimus-Eluting Stent Implantation(RESET) trial of 2148 patients randomized to the ZES-S stentand three months of DAPT and 1058 patients treated with stand-ard 12-month DAPT and other DES the combined endpoint ofany death MI stent thrombosis occurred in 13 in the standardtherapy arm vs 08 in the 3-month group (P frac14 048)12 Interest-ingly prospective studies undertaken to evaluate the degree ofZES-S stent coverage have consistently showed a very low rateof uncoveredmalapposed struts at 6- or even 3-month optical co-herence tomography evaluation which favourably compared withboth first generation DES or even BMS13 ndash15 Based on thisfinding the Zotarolimus-eluting stent in uncertain DES candidates
Table 4 Outcome rates at 24 months according to treatment group
Outcome 24-month clopidogrel 6-month clopidogrel
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Death for any cause myocardialinfarction or cerebrovascularaccident
29 (118) 33 (133) 23 (94) 15 (61) 32 (13) 12 (49) 31 (127) 23 (91)
Death for cardiovascular causemyocardial infarction orcerebrovascular accident
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (56)
Death for any cause ormyocardial infarction
25 (102) 27 (109) 22 (89) 14 (57) 30 (122) 12 (49) 31 (127) 21 (85)
Death for cardiovascular causemyocardial infarction
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (53)
Death for any cause 16 (65) 20 (81) 19 (78) 10 (4) 20 (81) 8 (33) 20 (82) 17 (69)
Death for cardiovascular cause 9 (37) 13 (52) 10 (41) 4 (16) 12 (49) 7 (29) 12 (49) 6 (24)
Myocardial infarction 14 (57) 12 (48) 9 (37) 4 (16) 15 (61) 4 (16) 14 (57) 8 (32)
Cerebrovascular accident 7 (28) 7 (28) 5 (2) 1 (04) 5 (2) 1 (04) 4 (16) 2 (08)
Definite stent thrombosis
Late 3 (12) 2 (08) 1 (04) 0 (0) 1 (04) 0 (0) 2 (08) 1 (04)
Very late 0 (0) 1 (04) 0 (0) 1 (04) 0 (0) 0 (0) 3 (13) 0 (0)
Cumulative 3 (12) 3 (12) 1 (04) 1 (04) 1 (04) 0 (0) 5 (2) 1 (04)
Definite or probable stent thrombosis
Late 5 (2) 2 (08) 3 (12) 0 (0) 5 (2) 0 (0) 3 (12) 1 (04)
Very late 0 (0) 1 (04) 1 (04) 1 (04) 0 (0) 0 (0) 6 (26) 0 (0)
Cumulative 5 (2) 3 (12) 4 (16) 1 (04) 5 (2) 0 (0) 9 (37) 1 (04)
Definite probable or possible stent thrombosis
Late 7 (28) 8 (32) 8 (32) 3 (12) 10 (41) 4 (16) 10 (41) 4 (16)
Very late 2 (08) 5 (21) 3 (13) 2 (08) 5 (21) 3 (13) 8 (34) 2 (08)
Cumulative 9 (37) 13 (52) 11 (45) 5 (2) 15 (61) 7 (29) 18 (74) 6 (24)
Dual antiplatelet therapy and stent-type Page 7 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 1 Stent analyses of the primary study endpoint and other secondary clinical outcomes Stent-specific analyses are shown with hazardratios and 95 confidence intervals for the primary end point of death for any cause myocardial infarction (MI) or cerebrovascular accident(CVA) death or MI and cardiovascular (CV) death or MI among patients randomly assigned to either the six or the 24-month clopidogreltherapy The P-value for interaction represents the likelihood of interaction between the variable and the relative treatment effect
Figure 2 Stent analyses of the stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95 confidence inter-vals for the definite definite probable and definite probable possible stent thrombosis (ST) among patients randomly assigned to either the 6or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction between the variable and the relativetreatment effect
M Valgimigli et alPage 8 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 3 Stent analyses of the 6-month landmark primary study endpoint and other secondary clinical outcomes Stent-specific analyses areshown with hazard ratios and 95 confidence intervals for the 6-month landmark analyses of the primary endpoint of death for any causemyocardial infarction (MI) or cerebrovascular accident (CVA) death or MI and cardiovascular (CV) death or MI among patients randomlyassigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction betweenthe variable and the relative treatment effect
Figure 4 Stent analyses of the 6-month landmark stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95confidence intervals for the 6-month landmark analyses of definite definite probable and definite probable possible stent thrombosis (ST)among patients randomly assigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihoodof interaction between the variable and the relative treatment effect
Dual antiplatelet therapy and stent-type Page 9 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
(ZEUS) study is comparing ZES-S vs BMS in patients at highthrombotic bleeding or low restenosis risk allowing 1-monthDAPT duration in both stent arms in patients who cannot toleratelonger duration of therapy (NCT01385319)
Reassuring data on the safety of early DAPT discontinuationafter EES have also been reported by a retrospective analysis ofregistry data7 Moreover the pooled analysis of SPIRIT II III IVand COMPARE Trials of 6789 patients showed a persistentlylow ST rate in patients treated with EES but not PES who discon-tinued DAPT after 6 months which is consistent with our currentfindings16 Indeed while our analysis on primary study endpointand other secondary clinical outcomes numerically favoured long-term DAPT after EES implantation the stent thrombosis endpointsand 6-month clinical landmark analyses revealed no excess ofevents in the 6-month DAPT group compared with longer-termclopidogrel therapy which is at variance with the results observedafter PES implantation
The need for prolonged DAPT has been suggested to be in-versely related to stent late loss17 Potent inhibition of intimal
hyperplasia might more frequently lead to incomplete stent cover-age andor late stent mal-apposition requiring a more prolongedcourse of intensified anti-platelet therapy to maintain stentsafety17
Our study by randomizing patients to a balanced mixture ofstents with various anti-intimal hyperplasia and each stent groupto 6- vs 24-month DAPT duration offers no evidence supportingthe association between stent-related late-loss and need for pro-longed DAPT On the contrary the results of our explorativeyet pre-specified analysis suggest that the minimal DAPT durationmay be stent-specific and not clearly related to stent potencytowards inhibition of intimal hyperplasia
Several limitations of our study should be considered Our studywas not powered to assess outcomes with respect to the differentDAPT regimens tested in our study for each stent type Similarlyour study was overall underpowered to assess the effect ofDAPT duration on stent thrombosis endpoints Therefore ourfindings should be considered exploratory and hypothesisgenerating
Our observation that primary study endpoint and other second-ary clinical ischaemic endpoints may be significantly lower after6-month compared with 24-month DAPT duration in ZES-Streated patients is intriguing but it should be interpreted withcaution In light of the limitations outlined above this findingshould be reassuring on the safety of early DAPT discontinuationin patients treated with ZES-S Yet a new paradigm has beenrecently proposed by the results of the WOEST study (clinicaltrialsgov NCT00769938) according to which lessening intensity of anti-platelet inhibition via dropping aspirin has resulted in a dramaticreduction of not only bleeding but also ischaemic endpoints includ-ing overall and cardiac mortality This paradigm has also been shownto apply to periprocedural anti-thrombotic therapy and it will befurther investigated in the ongoing comparative effectiveness of1 month of ticagrelor plus aspirin followed by ticagrelor monother-apy vs a current-day intensive DAPT in all-comer patients undergo-ing percutaneous coronary intervention with unrestricted BiolimusA9-eluting stent (GLOBAL LEADERS) study
In conclusion our study offers preliminary evidence that optimalduration of DAPT may be stent-specific with no clear associationbetween late loss potency and vulnerability to shorter DAPT dur-ation DES-specific studies aiming at unraveling the optimal DAPTduration after stent implantation are eagerly required and some ofthem are currently ongoing
Conflict of interest MV has received honoraria for lecturesad-visory board and research grants from Merck Iroko Eli Lilly andMedtronic honoraria for advisory board and lectures from TheMedicines Company and Eli Lilly Co Daiichi Sankyo Inc St Judeand Abbott Vascular lectures from Cordis CID and Terumo
FundingThe study is an investigator-driven clinical trial The conduct of thisstudy did not receive any direct or indirect external funding but wasentirely supported by the University of Ferrara which employed dedi-cated personnel for data monitoring data management events adjudi-cation and independent statistical analysis
Figure 5 Stent potency in inhibiting repeated intervention andrelative risks of adverse outcomes after 6-month dual anti-platelet therapy Relative risk reductions and corresponding95 confidence intervals (vertical bars) for target lesion revascu-larization from 30 days onwards for each drug-eluting stentemployed in the study when compared with bare metal stentgroup (reference group) is shown to the left In the middle rela-tive risk reductions and corresponding 95 confidence intervals(vertical bars) for 6-month landmark analysis of death myocardialinfarction or stroke in the 6-month when compared with24-month dual antiplatelet group is shown for each stent Inthe right portion of the figure relative risk reductions and corre-sponding 95 confidence intervals (vertical bars) for 6-monthlandmark analysis of definite probable or possible stent throm-bosis (ST) in the 6-month when compared with 24-month dualantiplatelet group is shown for each stent Note that a negativerelative risk reduction such as that observed for PES or BMSgroups implies the possibility of a relative risk increase in thestudy arm when compared with reference group EP endpointTLR target lesion revascularization from 30 days onwards Ddeath MI myocardial infarction CV cerebrovascular accidentDAPT dual antiplatelet therapy ST stent thrombosis Ref refer-ence arm BMS bare metal stent ZES-S zotarolimus-eluting stentEndeavor Sprint PES paclitaxel-eluting stent EES everolimus-eluting stent
M Valgimigli et alPage 10 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from

testing At the 6-month landmark analysis heterogeneity acrossstent types persisted whereas patients receiving PES showed a sig-nificantly higher rate of stent thrombosis in the short DAPTregimen No association was noted between expected or actualstent potency in inhibiting intimal hyperplasia and greater vulner-ability to shorter DAPT therapy
The main findings of our analysis challenge current recommen-dations endorsing a clear-cut dichotomy of BMS vs DES for theneed of prolonged DAPT after stenting Furthermore our datasuggest minimal duration of clopidogrel therapy may differamong DES irrespective of stent potency in inhibiting intimalhyperplasia
As previously reported9 no interaction was noted between BMSand the three different DES type clustered together with respectto duration of DAPT therapy On the other hand in the currentanalysis focusing on each DES type individually a clear andformal signal of heterogeneity with respect to overall death myo-cardial infarction or cerebrovascular accidents was noted for theneed of prolonged therapy with clopidogrel after interventionThis was driven by ZES-S treated patients showing an improvedprimary study and other secondary clinical outcomes with short-term DAPT when compared with 24-month duration of therapyand by an excess of stent thrombosis events particularly definiteor probable and definite probable or possible ST in patients
Table 3 Use of anti-platelet medications during the trial
24-month clopidogrel 6-month clopidogrel P-value
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Anti-platelet therapy at 30 days n ()
Numberevaluated
246 248 245 248 246 245 245 247
Aspirin 246 (100) 248 (100) 245 (100) 248 (100) 246 (100) 245 (100) 245 (100) 247 (100) 099
Clopidogrel 245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Aspirin andclopidogrel
245 (996) 247 (996) 245 (100) 248 (100) 246 (100) 244 (996) 245 (100) 247 (100) 055
Anti-platelet therapy at 6 months n ()
Numberevaluated total
241 241 238 246 240 244 239 240
Aspirin 240 (996) 240 (996) 234 (983) 246 (100) 236 (983) 241 (988) 238 (996) 238 (996) 024
Clopidogrel 239 (992) 239 (992) 237 (976) 245 (996) 94 (392) 241 (988) 234 (979) 236 (983) 0001
Aspirin andclopidogrel
238 (988) 238 (988) 233 (979) 245 (996) 97 (392) 238 (976) 233 (975) 235 (979) 0001
Anti-platelet therapy at 12 months n ()
Numberevaluated total
236 238 231 243 232 240 233 237
Aspirin 233 (987) 237 (996) 226 (978) 243 (100) 223 (961) 236 (983) 231 (991) 235 (992) 012
Clopidogrel 233 (987) 232 (975) 228 (987) 239 (983) 8 (35) 12 (5) 7 (3) 6 (25) 0001
Aspirin andClopidogrel
230 (975) 231 (971) 223 (965) 239 (984) 8 (35) 12 (5) 6 (26) 6 (25) 0001
Anti-platelet therapy at 18 months n ()
Numberevaluated total
234 234 227 238 231 239 228 234 034
Aspirin 232 (992) 232 (992) 223 (982) 234 (983) 221 (957) 232 (971) 226 (992) 233 (996) 012
Clopidogrel 231 (987) 222 (989) 220 (969) 231 (971) 2 (09) 2 (09) 3 (13) 1 (04) 0001
Aspirin andclopidogrel
229 (979) 221 (944) 216 (952) 229 (962) 2 (09) 1 (04) 2 (09) 1 (04) 0001
Anti-platelet therapy at 24 months n ()
Numberevaluated total
230 228 224 238 227 237 226 230
Aspirin 228 (991) 224 (983) 219 (978) 234 (983) 216 (952) 230 (971) 221 (978) 229 (996) 019
Clopidogrel 226 (983) 212 (93) 214 (955) 228 (958) 0 2 (08) 3 (13) 0 0001
Aspirin andclopidogrel
224 (974) 210 (921) 211 (942) 226 (947) 0 1 (04) 2 (09) 0 0001
M Valgimigli et alPage 6 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
undergoing 6-month clopidogrel therapy after PES implantationcompared with a longer duration of therapy
In our study adherence to aspirin and clopidogrel was similarlyhigh in the first 6 months after DES implantation in the two DAPTgroups Therefore events occurring during this time period in thethree DES groups may potentially confound the outcomes of thetwo different DAPT regimens tested in the study Based on thisnotion a landmark analysis focusing on events occurring after a6 month-follow-up has been pre-specified and previously reportedfor the whole patient population or for all DES treated patientsclustered together When the three tested DES types were ana-lysed separately at the 6-month landmark analysis the resultswere largely consistent with the findings observed for the entirefollow-up duration (i) patients treated with ZES-S showed abetter ischaemic outcomes in the 6-month when compared withthe 24-month DAPT groups (ii) event rates for the primary or sec-ondary ischaemic clinical endpoints were similar between DAPTgroups after BMS or EES implantation (iii) the primary clinicalcomposite endpoint trended higher and the ST rates were signifi-cantly increased in PES treated patients receiving PES and
undergoing 6-month when compared with 24-month duration ofclopidogrel
Kandzari et al6 recently analysed outcomes in 2032 patientsundergoing coronary revascularization with ZES-S in five trialswho for various reasons discontinued DAPT at 6 months andfound that outcomes did not differ compared with patients whoreceived longer clopidogrel therapy (up to 12 or 24 months)
In the Real Safety and Efficacy of 3-Month Dual AntiplateletTherapy Following Zotarolimus-Eluting Stent Implantation(RESET) trial of 2148 patients randomized to the ZES-S stentand three months of DAPT and 1058 patients treated with stand-ard 12-month DAPT and other DES the combined endpoint ofany death MI stent thrombosis occurred in 13 in the standardtherapy arm vs 08 in the 3-month group (P frac14 048)12 Interest-ingly prospective studies undertaken to evaluate the degree ofZES-S stent coverage have consistently showed a very low rateof uncoveredmalapposed struts at 6- or even 3-month optical co-herence tomography evaluation which favourably compared withboth first generation DES or even BMS13 ndash15 Based on thisfinding the Zotarolimus-eluting stent in uncertain DES candidates
Table 4 Outcome rates at 24 months according to treatment group
Outcome 24-month clopidogrel 6-month clopidogrel
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Death for any cause myocardialinfarction or cerebrovascularaccident
29 (118) 33 (133) 23 (94) 15 (61) 32 (13) 12 (49) 31 (127) 23 (91)
Death for cardiovascular causemyocardial infarction orcerebrovascular accident
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (56)
Death for any cause ormyocardial infarction
25 (102) 27 (109) 22 (89) 14 (57) 30 (122) 12 (49) 31 (127) 21 (85)
Death for cardiovascular causemyocardial infarction
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (53)
Death for any cause 16 (65) 20 (81) 19 (78) 10 (4) 20 (81) 8 (33) 20 (82) 17 (69)
Death for cardiovascular cause 9 (37) 13 (52) 10 (41) 4 (16) 12 (49) 7 (29) 12 (49) 6 (24)
Myocardial infarction 14 (57) 12 (48) 9 (37) 4 (16) 15 (61) 4 (16) 14 (57) 8 (32)
Cerebrovascular accident 7 (28) 7 (28) 5 (2) 1 (04) 5 (2) 1 (04) 4 (16) 2 (08)
Definite stent thrombosis
Late 3 (12) 2 (08) 1 (04) 0 (0) 1 (04) 0 (0) 2 (08) 1 (04)
Very late 0 (0) 1 (04) 0 (0) 1 (04) 0 (0) 0 (0) 3 (13) 0 (0)
Cumulative 3 (12) 3 (12) 1 (04) 1 (04) 1 (04) 0 (0) 5 (2) 1 (04)
Definite or probable stent thrombosis
Late 5 (2) 2 (08) 3 (12) 0 (0) 5 (2) 0 (0) 3 (12) 1 (04)
Very late 0 (0) 1 (04) 1 (04) 1 (04) 0 (0) 0 (0) 6 (26) 0 (0)
Cumulative 5 (2) 3 (12) 4 (16) 1 (04) 5 (2) 0 (0) 9 (37) 1 (04)
Definite probable or possible stent thrombosis
Late 7 (28) 8 (32) 8 (32) 3 (12) 10 (41) 4 (16) 10 (41) 4 (16)
Very late 2 (08) 5 (21) 3 (13) 2 (08) 5 (21) 3 (13) 8 (34) 2 (08)
Cumulative 9 (37) 13 (52) 11 (45) 5 (2) 15 (61) 7 (29) 18 (74) 6 (24)
Dual antiplatelet therapy and stent-type Page 7 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 1 Stent analyses of the primary study endpoint and other secondary clinical outcomes Stent-specific analyses are shown with hazardratios and 95 confidence intervals for the primary end point of death for any cause myocardial infarction (MI) or cerebrovascular accident(CVA) death or MI and cardiovascular (CV) death or MI among patients randomly assigned to either the six or the 24-month clopidogreltherapy The P-value for interaction represents the likelihood of interaction between the variable and the relative treatment effect
Figure 2 Stent analyses of the stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95 confidence inter-vals for the definite definite probable and definite probable possible stent thrombosis (ST) among patients randomly assigned to either the 6or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction between the variable and the relativetreatment effect
M Valgimigli et alPage 8 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 3 Stent analyses of the 6-month landmark primary study endpoint and other secondary clinical outcomes Stent-specific analyses areshown with hazard ratios and 95 confidence intervals for the 6-month landmark analyses of the primary endpoint of death for any causemyocardial infarction (MI) or cerebrovascular accident (CVA) death or MI and cardiovascular (CV) death or MI among patients randomlyassigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction betweenthe variable and the relative treatment effect
Figure 4 Stent analyses of the 6-month landmark stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95confidence intervals for the 6-month landmark analyses of definite definite probable and definite probable possible stent thrombosis (ST)among patients randomly assigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihoodof interaction between the variable and the relative treatment effect
Dual antiplatelet therapy and stent-type Page 9 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
(ZEUS) study is comparing ZES-S vs BMS in patients at highthrombotic bleeding or low restenosis risk allowing 1-monthDAPT duration in both stent arms in patients who cannot toleratelonger duration of therapy (NCT01385319)
Reassuring data on the safety of early DAPT discontinuationafter EES have also been reported by a retrospective analysis ofregistry data7 Moreover the pooled analysis of SPIRIT II III IVand COMPARE Trials of 6789 patients showed a persistentlylow ST rate in patients treated with EES but not PES who discon-tinued DAPT after 6 months which is consistent with our currentfindings16 Indeed while our analysis on primary study endpointand other secondary clinical outcomes numerically favoured long-term DAPT after EES implantation the stent thrombosis endpointsand 6-month clinical landmark analyses revealed no excess ofevents in the 6-month DAPT group compared with longer-termclopidogrel therapy which is at variance with the results observedafter PES implantation
The need for prolonged DAPT has been suggested to be in-versely related to stent late loss17 Potent inhibition of intimal
hyperplasia might more frequently lead to incomplete stent cover-age andor late stent mal-apposition requiring a more prolongedcourse of intensified anti-platelet therapy to maintain stentsafety17
Our study by randomizing patients to a balanced mixture ofstents with various anti-intimal hyperplasia and each stent groupto 6- vs 24-month DAPT duration offers no evidence supportingthe association between stent-related late-loss and need for pro-longed DAPT On the contrary the results of our explorativeyet pre-specified analysis suggest that the minimal DAPT durationmay be stent-specific and not clearly related to stent potencytowards inhibition of intimal hyperplasia
Several limitations of our study should be considered Our studywas not powered to assess outcomes with respect to the differentDAPT regimens tested in our study for each stent type Similarlyour study was overall underpowered to assess the effect ofDAPT duration on stent thrombosis endpoints Therefore ourfindings should be considered exploratory and hypothesisgenerating
Our observation that primary study endpoint and other second-ary clinical ischaemic endpoints may be significantly lower after6-month compared with 24-month DAPT duration in ZES-Streated patients is intriguing but it should be interpreted withcaution In light of the limitations outlined above this findingshould be reassuring on the safety of early DAPT discontinuationin patients treated with ZES-S Yet a new paradigm has beenrecently proposed by the results of the WOEST study (clinicaltrialsgov NCT00769938) according to which lessening intensity of anti-platelet inhibition via dropping aspirin has resulted in a dramaticreduction of not only bleeding but also ischaemic endpoints includ-ing overall and cardiac mortality This paradigm has also been shownto apply to periprocedural anti-thrombotic therapy and it will befurther investigated in the ongoing comparative effectiveness of1 month of ticagrelor plus aspirin followed by ticagrelor monother-apy vs a current-day intensive DAPT in all-comer patients undergo-ing percutaneous coronary intervention with unrestricted BiolimusA9-eluting stent (GLOBAL LEADERS) study
In conclusion our study offers preliminary evidence that optimalduration of DAPT may be stent-specific with no clear associationbetween late loss potency and vulnerability to shorter DAPT dur-ation DES-specific studies aiming at unraveling the optimal DAPTduration after stent implantation are eagerly required and some ofthem are currently ongoing
Conflict of interest MV has received honoraria for lecturesad-visory board and research grants from Merck Iroko Eli Lilly andMedtronic honoraria for advisory board and lectures from TheMedicines Company and Eli Lilly Co Daiichi Sankyo Inc St Judeand Abbott Vascular lectures from Cordis CID and Terumo
FundingThe study is an investigator-driven clinical trial The conduct of thisstudy did not receive any direct or indirect external funding but wasentirely supported by the University of Ferrara which employed dedi-cated personnel for data monitoring data management events adjudi-cation and independent statistical analysis
Figure 5 Stent potency in inhibiting repeated intervention andrelative risks of adverse outcomes after 6-month dual anti-platelet therapy Relative risk reductions and corresponding95 confidence intervals (vertical bars) for target lesion revascu-larization from 30 days onwards for each drug-eluting stentemployed in the study when compared with bare metal stentgroup (reference group) is shown to the left In the middle rela-tive risk reductions and corresponding 95 confidence intervals(vertical bars) for 6-month landmark analysis of death myocardialinfarction or stroke in the 6-month when compared with24-month dual antiplatelet group is shown for each stent Inthe right portion of the figure relative risk reductions and corre-sponding 95 confidence intervals (vertical bars) for 6-monthlandmark analysis of definite probable or possible stent throm-bosis (ST) in the 6-month when compared with 24-month dualantiplatelet group is shown for each stent Note that a negativerelative risk reduction such as that observed for PES or BMSgroups implies the possibility of a relative risk increase in thestudy arm when compared with reference group EP endpointTLR target lesion revascularization from 30 days onwards Ddeath MI myocardial infarction CV cerebrovascular accidentDAPT dual antiplatelet therapy ST stent thrombosis Ref refer-ence arm BMS bare metal stent ZES-S zotarolimus-eluting stentEndeavor Sprint PES paclitaxel-eluting stent EES everolimus-eluting stent
M Valgimigli et alPage 10 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from

undergoing 6-month clopidogrel therapy after PES implantationcompared with a longer duration of therapy
In our study adherence to aspirin and clopidogrel was similarlyhigh in the first 6 months after DES implantation in the two DAPTgroups Therefore events occurring during this time period in thethree DES groups may potentially confound the outcomes of thetwo different DAPT regimens tested in the study Based on thisnotion a landmark analysis focusing on events occurring after a6 month-follow-up has been pre-specified and previously reportedfor the whole patient population or for all DES treated patientsclustered together When the three tested DES types were ana-lysed separately at the 6-month landmark analysis the resultswere largely consistent with the findings observed for the entirefollow-up duration (i) patients treated with ZES-S showed abetter ischaemic outcomes in the 6-month when compared withthe 24-month DAPT groups (ii) event rates for the primary or sec-ondary ischaemic clinical endpoints were similar between DAPTgroups after BMS or EES implantation (iii) the primary clinicalcomposite endpoint trended higher and the ST rates were signifi-cantly increased in PES treated patients receiving PES and
undergoing 6-month when compared with 24-month duration ofclopidogrel
Kandzari et al6 recently analysed outcomes in 2032 patientsundergoing coronary revascularization with ZES-S in five trialswho for various reasons discontinued DAPT at 6 months andfound that outcomes did not differ compared with patients whoreceived longer clopidogrel therapy (up to 12 or 24 months)
In the Real Safety and Efficacy of 3-Month Dual AntiplateletTherapy Following Zotarolimus-Eluting Stent Implantation(RESET) trial of 2148 patients randomized to the ZES-S stentand three months of DAPT and 1058 patients treated with stand-ard 12-month DAPT and other DES the combined endpoint ofany death MI stent thrombosis occurred in 13 in the standardtherapy arm vs 08 in the 3-month group (P frac14 048)12 Interest-ingly prospective studies undertaken to evaluate the degree ofZES-S stent coverage have consistently showed a very low rateof uncoveredmalapposed struts at 6- or even 3-month optical co-herence tomography evaluation which favourably compared withboth first generation DES or even BMS13 ndash15 Based on thisfinding the Zotarolimus-eluting stent in uncertain DES candidates
Table 4 Outcome rates at 24 months according to treatment group
Outcome 24-month clopidogrel 6-month clopidogrel
BMS(n 5 246)
ZES(n 5 248)
PES(n 5 245)
EES(n 5 248)
BMS(n 5 246)
ZES(n 5 245)
PES(n 5 245)
EES(n 5 247)
Death for any cause myocardialinfarction or cerebrovascularaccident
29 (118) 33 (133) 23 (94) 15 (61) 32 (13) 12 (49) 31 (127) 23 (91)
Death for cardiovascular causemyocardial infarction orcerebrovascular accident
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (56)
Death for any cause ormyocardial infarction
25 (102) 27 (109) 22 (89) 14 (57) 30 (122) 12 (49) 31 (127) 21 (85)
Death for cardiovascular causemyocardial infarction
19 (77) 21 (85) 15 (61) 8 (32) 22 (89) 11 (45) 23 (94) 13 (53)
Death for any cause 16 (65) 20 (81) 19 (78) 10 (4) 20 (81) 8 (33) 20 (82) 17 (69)
Death for cardiovascular cause 9 (37) 13 (52) 10 (41) 4 (16) 12 (49) 7 (29) 12 (49) 6 (24)
Myocardial infarction 14 (57) 12 (48) 9 (37) 4 (16) 15 (61) 4 (16) 14 (57) 8 (32)
Cerebrovascular accident 7 (28) 7 (28) 5 (2) 1 (04) 5 (2) 1 (04) 4 (16) 2 (08)
Definite stent thrombosis
Late 3 (12) 2 (08) 1 (04) 0 (0) 1 (04) 0 (0) 2 (08) 1 (04)
Very late 0 (0) 1 (04) 0 (0) 1 (04) 0 (0) 0 (0) 3 (13) 0 (0)
Cumulative 3 (12) 3 (12) 1 (04) 1 (04) 1 (04) 0 (0) 5 (2) 1 (04)
Definite or probable stent thrombosis
Late 5 (2) 2 (08) 3 (12) 0 (0) 5 (2) 0 (0) 3 (12) 1 (04)
Very late 0 (0) 1 (04) 1 (04) 1 (04) 0 (0) 0 (0) 6 (26) 0 (0)
Cumulative 5 (2) 3 (12) 4 (16) 1 (04) 5 (2) 0 (0) 9 (37) 1 (04)
Definite probable or possible stent thrombosis
Late 7 (28) 8 (32) 8 (32) 3 (12) 10 (41) 4 (16) 10 (41) 4 (16)
Very late 2 (08) 5 (21) 3 (13) 2 (08) 5 (21) 3 (13) 8 (34) 2 (08)
Cumulative 9 (37) 13 (52) 11 (45) 5 (2) 15 (61) 7 (29) 18 (74) 6 (24)
Dual antiplatelet therapy and stent-type Page 7 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 1 Stent analyses of the primary study endpoint and other secondary clinical outcomes Stent-specific analyses are shown with hazardratios and 95 confidence intervals for the primary end point of death for any cause myocardial infarction (MI) or cerebrovascular accident(CVA) death or MI and cardiovascular (CV) death or MI among patients randomly assigned to either the six or the 24-month clopidogreltherapy The P-value for interaction represents the likelihood of interaction between the variable and the relative treatment effect
Figure 2 Stent analyses of the stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95 confidence inter-vals for the definite definite probable and definite probable possible stent thrombosis (ST) among patients randomly assigned to either the 6or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction between the variable and the relativetreatment effect
M Valgimigli et alPage 8 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 3 Stent analyses of the 6-month landmark primary study endpoint and other secondary clinical outcomes Stent-specific analyses areshown with hazard ratios and 95 confidence intervals for the 6-month landmark analyses of the primary endpoint of death for any causemyocardial infarction (MI) or cerebrovascular accident (CVA) death or MI and cardiovascular (CV) death or MI among patients randomlyassigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction betweenthe variable and the relative treatment effect
Figure 4 Stent analyses of the 6-month landmark stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95confidence intervals for the 6-month landmark analyses of definite definite probable and definite probable possible stent thrombosis (ST)among patients randomly assigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihoodof interaction between the variable and the relative treatment effect
Dual antiplatelet therapy and stent-type Page 9 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
(ZEUS) study is comparing ZES-S vs BMS in patients at highthrombotic bleeding or low restenosis risk allowing 1-monthDAPT duration in both stent arms in patients who cannot toleratelonger duration of therapy (NCT01385319)
Reassuring data on the safety of early DAPT discontinuationafter EES have also been reported by a retrospective analysis ofregistry data7 Moreover the pooled analysis of SPIRIT II III IVand COMPARE Trials of 6789 patients showed a persistentlylow ST rate in patients treated with EES but not PES who discon-tinued DAPT after 6 months which is consistent with our currentfindings16 Indeed while our analysis on primary study endpointand other secondary clinical outcomes numerically favoured long-term DAPT after EES implantation the stent thrombosis endpointsand 6-month clinical landmark analyses revealed no excess ofevents in the 6-month DAPT group compared with longer-termclopidogrel therapy which is at variance with the results observedafter PES implantation
The need for prolonged DAPT has been suggested to be in-versely related to stent late loss17 Potent inhibition of intimal
hyperplasia might more frequently lead to incomplete stent cover-age andor late stent mal-apposition requiring a more prolongedcourse of intensified anti-platelet therapy to maintain stentsafety17
Our study by randomizing patients to a balanced mixture ofstents with various anti-intimal hyperplasia and each stent groupto 6- vs 24-month DAPT duration offers no evidence supportingthe association between stent-related late-loss and need for pro-longed DAPT On the contrary the results of our explorativeyet pre-specified analysis suggest that the minimal DAPT durationmay be stent-specific and not clearly related to stent potencytowards inhibition of intimal hyperplasia
Several limitations of our study should be considered Our studywas not powered to assess outcomes with respect to the differentDAPT regimens tested in our study for each stent type Similarlyour study was overall underpowered to assess the effect ofDAPT duration on stent thrombosis endpoints Therefore ourfindings should be considered exploratory and hypothesisgenerating
Our observation that primary study endpoint and other second-ary clinical ischaemic endpoints may be significantly lower after6-month compared with 24-month DAPT duration in ZES-Streated patients is intriguing but it should be interpreted withcaution In light of the limitations outlined above this findingshould be reassuring on the safety of early DAPT discontinuationin patients treated with ZES-S Yet a new paradigm has beenrecently proposed by the results of the WOEST study (clinicaltrialsgov NCT00769938) according to which lessening intensity of anti-platelet inhibition via dropping aspirin has resulted in a dramaticreduction of not only bleeding but also ischaemic endpoints includ-ing overall and cardiac mortality This paradigm has also been shownto apply to periprocedural anti-thrombotic therapy and it will befurther investigated in the ongoing comparative effectiveness of1 month of ticagrelor plus aspirin followed by ticagrelor monother-apy vs a current-day intensive DAPT in all-comer patients undergo-ing percutaneous coronary intervention with unrestricted BiolimusA9-eluting stent (GLOBAL LEADERS) study
In conclusion our study offers preliminary evidence that optimalduration of DAPT may be stent-specific with no clear associationbetween late loss potency and vulnerability to shorter DAPT dur-ation DES-specific studies aiming at unraveling the optimal DAPTduration after stent implantation are eagerly required and some ofthem are currently ongoing
Conflict of interest MV has received honoraria for lecturesad-visory board and research grants from Merck Iroko Eli Lilly andMedtronic honoraria for advisory board and lectures from TheMedicines Company and Eli Lilly Co Daiichi Sankyo Inc St Judeand Abbott Vascular lectures from Cordis CID and Terumo
FundingThe study is an investigator-driven clinical trial The conduct of thisstudy did not receive any direct or indirect external funding but wasentirely supported by the University of Ferrara which employed dedi-cated personnel for data monitoring data management events adjudi-cation and independent statistical analysis
Figure 5 Stent potency in inhibiting repeated intervention andrelative risks of adverse outcomes after 6-month dual anti-platelet therapy Relative risk reductions and corresponding95 confidence intervals (vertical bars) for target lesion revascu-larization from 30 days onwards for each drug-eluting stentemployed in the study when compared with bare metal stentgroup (reference group) is shown to the left In the middle rela-tive risk reductions and corresponding 95 confidence intervals(vertical bars) for 6-month landmark analysis of death myocardialinfarction or stroke in the 6-month when compared with24-month dual antiplatelet group is shown for each stent Inthe right portion of the figure relative risk reductions and corre-sponding 95 confidence intervals (vertical bars) for 6-monthlandmark analysis of definite probable or possible stent throm-bosis (ST) in the 6-month when compared with 24-month dualantiplatelet group is shown for each stent Note that a negativerelative risk reduction such as that observed for PES or BMSgroups implies the possibility of a relative risk increase in thestudy arm when compared with reference group EP endpointTLR target lesion revascularization from 30 days onwards Ddeath MI myocardial infarction CV cerebrovascular accidentDAPT dual antiplatelet therapy ST stent thrombosis Ref refer-ence arm BMS bare metal stent ZES-S zotarolimus-eluting stentEndeavor Sprint PES paclitaxel-eluting stent EES everolimus-eluting stent
M Valgimigli et alPage 10 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
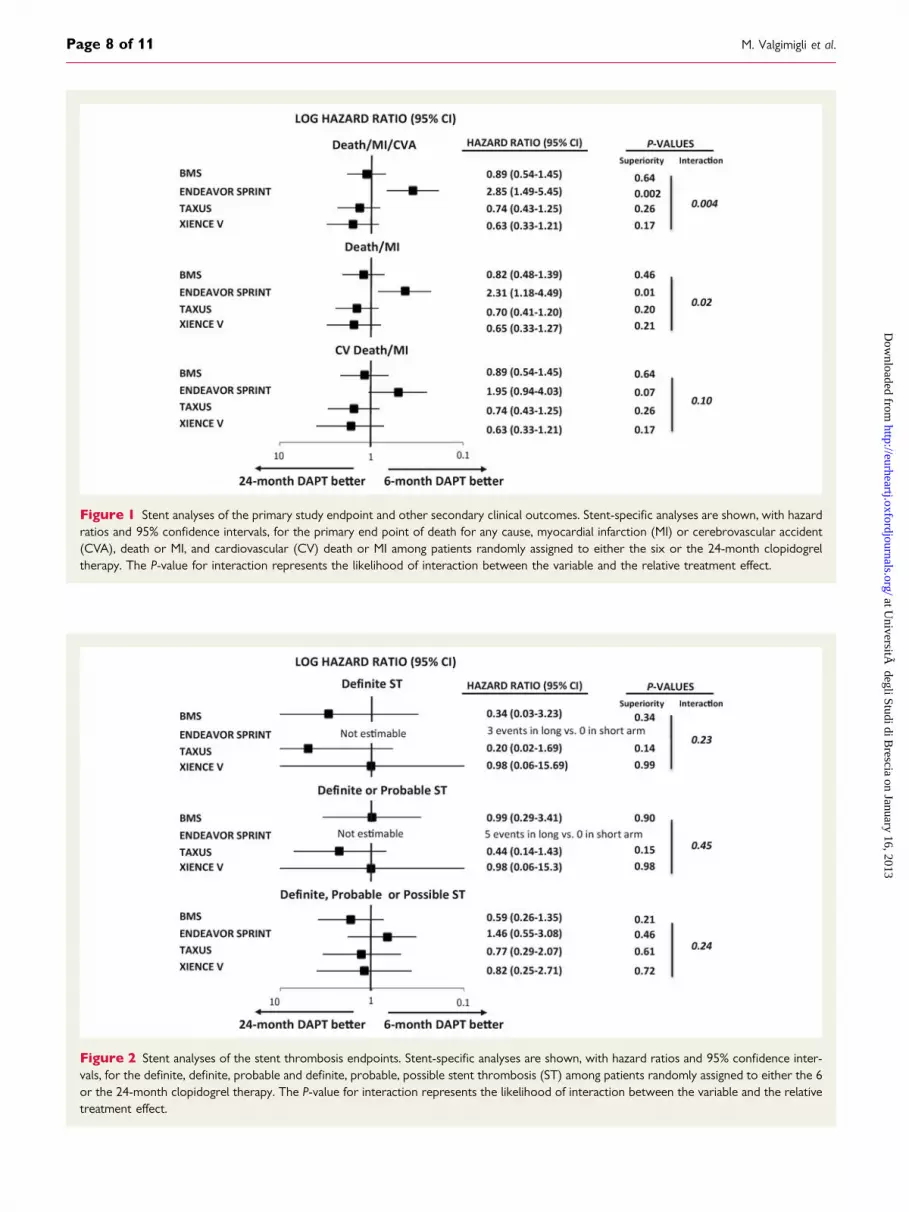
Figure 1 Stent analyses of the primary study endpoint and other secondary clinical outcomes Stent-specific analyses are shown with hazardratios and 95 confidence intervals for the primary end point of death for any cause myocardial infarction (MI) or cerebrovascular accident(CVA) death or MI and cardiovascular (CV) death or MI among patients randomly assigned to either the six or the 24-month clopidogreltherapy The P-value for interaction represents the likelihood of interaction between the variable and the relative treatment effect
Figure 2 Stent analyses of the stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95 confidence inter-vals for the definite definite probable and definite probable possible stent thrombosis (ST) among patients randomly assigned to either the 6or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction between the variable and the relativetreatment effect
M Valgimigli et alPage 8 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Figure 3 Stent analyses of the 6-month landmark primary study endpoint and other secondary clinical outcomes Stent-specific analyses areshown with hazard ratios and 95 confidence intervals for the 6-month landmark analyses of the primary endpoint of death for any causemyocardial infarction (MI) or cerebrovascular accident (CVA) death or MI and cardiovascular (CV) death or MI among patients randomlyassigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction betweenthe variable and the relative treatment effect
Figure 4 Stent analyses of the 6-month landmark stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95confidence intervals for the 6-month landmark analyses of definite definite probable and definite probable possible stent thrombosis (ST)among patients randomly assigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihoodof interaction between the variable and the relative treatment effect
Dual antiplatelet therapy and stent-type Page 9 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
(ZEUS) study is comparing ZES-S vs BMS in patients at highthrombotic bleeding or low restenosis risk allowing 1-monthDAPT duration in both stent arms in patients who cannot toleratelonger duration of therapy (NCT01385319)
Reassuring data on the safety of early DAPT discontinuationafter EES have also been reported by a retrospective analysis ofregistry data7 Moreover the pooled analysis of SPIRIT II III IVand COMPARE Trials of 6789 patients showed a persistentlylow ST rate in patients treated with EES but not PES who discon-tinued DAPT after 6 months which is consistent with our currentfindings16 Indeed while our analysis on primary study endpointand other secondary clinical outcomes numerically favoured long-term DAPT after EES implantation the stent thrombosis endpointsand 6-month clinical landmark analyses revealed no excess ofevents in the 6-month DAPT group compared with longer-termclopidogrel therapy which is at variance with the results observedafter PES implantation
The need for prolonged DAPT has been suggested to be in-versely related to stent late loss17 Potent inhibition of intimal
hyperplasia might more frequently lead to incomplete stent cover-age andor late stent mal-apposition requiring a more prolongedcourse of intensified anti-platelet therapy to maintain stentsafety17
Our study by randomizing patients to a balanced mixture ofstents with various anti-intimal hyperplasia and each stent groupto 6- vs 24-month DAPT duration offers no evidence supportingthe association between stent-related late-loss and need for pro-longed DAPT On the contrary the results of our explorativeyet pre-specified analysis suggest that the minimal DAPT durationmay be stent-specific and not clearly related to stent potencytowards inhibition of intimal hyperplasia
Several limitations of our study should be considered Our studywas not powered to assess outcomes with respect to the differentDAPT regimens tested in our study for each stent type Similarlyour study was overall underpowered to assess the effect ofDAPT duration on stent thrombosis endpoints Therefore ourfindings should be considered exploratory and hypothesisgenerating
Our observation that primary study endpoint and other second-ary clinical ischaemic endpoints may be significantly lower after6-month compared with 24-month DAPT duration in ZES-Streated patients is intriguing but it should be interpreted withcaution In light of the limitations outlined above this findingshould be reassuring on the safety of early DAPT discontinuationin patients treated with ZES-S Yet a new paradigm has beenrecently proposed by the results of the WOEST study (clinicaltrialsgov NCT00769938) according to which lessening intensity of anti-platelet inhibition via dropping aspirin has resulted in a dramaticreduction of not only bleeding but also ischaemic endpoints includ-ing overall and cardiac mortality This paradigm has also been shownto apply to periprocedural anti-thrombotic therapy and it will befurther investigated in the ongoing comparative effectiveness of1 month of ticagrelor plus aspirin followed by ticagrelor monother-apy vs a current-day intensive DAPT in all-comer patients undergo-ing percutaneous coronary intervention with unrestricted BiolimusA9-eluting stent (GLOBAL LEADERS) study
In conclusion our study offers preliminary evidence that optimalduration of DAPT may be stent-specific with no clear associationbetween late loss potency and vulnerability to shorter DAPT dur-ation DES-specific studies aiming at unraveling the optimal DAPTduration after stent implantation are eagerly required and some ofthem are currently ongoing
Conflict of interest MV has received honoraria for lecturesad-visory board and research grants from Merck Iroko Eli Lilly andMedtronic honoraria for advisory board and lectures from TheMedicines Company and Eli Lilly Co Daiichi Sankyo Inc St Judeand Abbott Vascular lectures from Cordis CID and Terumo
FundingThe study is an investigator-driven clinical trial The conduct of thisstudy did not receive any direct or indirect external funding but wasentirely supported by the University of Ferrara which employed dedi-cated personnel for data monitoring data management events adjudi-cation and independent statistical analysis
Figure 5 Stent potency in inhibiting repeated intervention andrelative risks of adverse outcomes after 6-month dual anti-platelet therapy Relative risk reductions and corresponding95 confidence intervals (vertical bars) for target lesion revascu-larization from 30 days onwards for each drug-eluting stentemployed in the study when compared with bare metal stentgroup (reference group) is shown to the left In the middle rela-tive risk reductions and corresponding 95 confidence intervals(vertical bars) for 6-month landmark analysis of death myocardialinfarction or stroke in the 6-month when compared with24-month dual antiplatelet group is shown for each stent Inthe right portion of the figure relative risk reductions and corre-sponding 95 confidence intervals (vertical bars) for 6-monthlandmark analysis of definite probable or possible stent throm-bosis (ST) in the 6-month when compared with 24-month dualantiplatelet group is shown for each stent Note that a negativerelative risk reduction such as that observed for PES or BMSgroups implies the possibility of a relative risk increase in thestudy arm when compared with reference group EP endpointTLR target lesion revascularization from 30 days onwards Ddeath MI myocardial infarction CV cerebrovascular accidentDAPT dual antiplatelet therapy ST stent thrombosis Ref refer-ence arm BMS bare metal stent ZES-S zotarolimus-eluting stentEndeavor Sprint PES paclitaxel-eluting stent EES everolimus-eluting stent
M Valgimigli et alPage 10 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from

Figure 3 Stent analyses of the 6-month landmark primary study endpoint and other secondary clinical outcomes Stent-specific analyses areshown with hazard ratios and 95 confidence intervals for the 6-month landmark analyses of the primary endpoint of death for any causemyocardial infarction (MI) or cerebrovascular accident (CVA) death or MI and cardiovascular (CV) death or MI among patients randomlyassigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihood of interaction betweenthe variable and the relative treatment effect
Figure 4 Stent analyses of the 6-month landmark stent thrombosis endpoints Stent-specific analyses are shown with hazard ratios and 95confidence intervals for the 6-month landmark analyses of definite definite probable and definite probable possible stent thrombosis (ST)among patients randomly assigned to either the 6 or the 24-month clopidogrel therapy The P-value for interaction represents the likelihoodof interaction between the variable and the relative treatment effect
Dual antiplatelet therapy and stent-type Page 9 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
(ZEUS) study is comparing ZES-S vs BMS in patients at highthrombotic bleeding or low restenosis risk allowing 1-monthDAPT duration in both stent arms in patients who cannot toleratelonger duration of therapy (NCT01385319)
Reassuring data on the safety of early DAPT discontinuationafter EES have also been reported by a retrospective analysis ofregistry data7 Moreover the pooled analysis of SPIRIT II III IVand COMPARE Trials of 6789 patients showed a persistentlylow ST rate in patients treated with EES but not PES who discon-tinued DAPT after 6 months which is consistent with our currentfindings16 Indeed while our analysis on primary study endpointand other secondary clinical outcomes numerically favoured long-term DAPT after EES implantation the stent thrombosis endpointsand 6-month clinical landmark analyses revealed no excess ofevents in the 6-month DAPT group compared with longer-termclopidogrel therapy which is at variance with the results observedafter PES implantation
The need for prolonged DAPT has been suggested to be in-versely related to stent late loss17 Potent inhibition of intimal
hyperplasia might more frequently lead to incomplete stent cover-age andor late stent mal-apposition requiring a more prolongedcourse of intensified anti-platelet therapy to maintain stentsafety17
Our study by randomizing patients to a balanced mixture ofstents with various anti-intimal hyperplasia and each stent groupto 6- vs 24-month DAPT duration offers no evidence supportingthe association between stent-related late-loss and need for pro-longed DAPT On the contrary the results of our explorativeyet pre-specified analysis suggest that the minimal DAPT durationmay be stent-specific and not clearly related to stent potencytowards inhibition of intimal hyperplasia
Several limitations of our study should be considered Our studywas not powered to assess outcomes with respect to the differentDAPT regimens tested in our study for each stent type Similarlyour study was overall underpowered to assess the effect ofDAPT duration on stent thrombosis endpoints Therefore ourfindings should be considered exploratory and hypothesisgenerating
Our observation that primary study endpoint and other second-ary clinical ischaemic endpoints may be significantly lower after6-month compared with 24-month DAPT duration in ZES-Streated patients is intriguing but it should be interpreted withcaution In light of the limitations outlined above this findingshould be reassuring on the safety of early DAPT discontinuationin patients treated with ZES-S Yet a new paradigm has beenrecently proposed by the results of the WOEST study (clinicaltrialsgov NCT00769938) according to which lessening intensity of anti-platelet inhibition via dropping aspirin has resulted in a dramaticreduction of not only bleeding but also ischaemic endpoints includ-ing overall and cardiac mortality This paradigm has also been shownto apply to periprocedural anti-thrombotic therapy and it will befurther investigated in the ongoing comparative effectiveness of1 month of ticagrelor plus aspirin followed by ticagrelor monother-apy vs a current-day intensive DAPT in all-comer patients undergo-ing percutaneous coronary intervention with unrestricted BiolimusA9-eluting stent (GLOBAL LEADERS) study
In conclusion our study offers preliminary evidence that optimalduration of DAPT may be stent-specific with no clear associationbetween late loss potency and vulnerability to shorter DAPT dur-ation DES-specific studies aiming at unraveling the optimal DAPTduration after stent implantation are eagerly required and some ofthem are currently ongoing
Conflict of interest MV has received honoraria for lecturesad-visory board and research grants from Merck Iroko Eli Lilly andMedtronic honoraria for advisory board and lectures from TheMedicines Company and Eli Lilly Co Daiichi Sankyo Inc St Judeand Abbott Vascular lectures from Cordis CID and Terumo
FundingThe study is an investigator-driven clinical trial The conduct of thisstudy did not receive any direct or indirect external funding but wasentirely supported by the University of Ferrara which employed dedi-cated personnel for data monitoring data management events adjudi-cation and independent statistical analysis
Figure 5 Stent potency in inhibiting repeated intervention andrelative risks of adverse outcomes after 6-month dual anti-platelet therapy Relative risk reductions and corresponding95 confidence intervals (vertical bars) for target lesion revascu-larization from 30 days onwards for each drug-eluting stentemployed in the study when compared with bare metal stentgroup (reference group) is shown to the left In the middle rela-tive risk reductions and corresponding 95 confidence intervals(vertical bars) for 6-month landmark analysis of death myocardialinfarction or stroke in the 6-month when compared with24-month dual antiplatelet group is shown for each stent Inthe right portion of the figure relative risk reductions and corre-sponding 95 confidence intervals (vertical bars) for 6-monthlandmark analysis of definite probable or possible stent throm-bosis (ST) in the 6-month when compared with 24-month dualantiplatelet group is shown for each stent Note that a negativerelative risk reduction such as that observed for PES or BMSgroups implies the possibility of a relative risk increase in thestudy arm when compared with reference group EP endpointTLR target lesion revascularization from 30 days onwards Ddeath MI myocardial infarction CV cerebrovascular accidentDAPT dual antiplatelet therapy ST stent thrombosis Ref refer-ence arm BMS bare metal stent ZES-S zotarolimus-eluting stentEndeavor Sprint PES paclitaxel-eluting stent EES everolimus-eluting stent
M Valgimigli et alPage 10 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from

(ZEUS) study is comparing ZES-S vs BMS in patients at highthrombotic bleeding or low restenosis risk allowing 1-monthDAPT duration in both stent arms in patients who cannot toleratelonger duration of therapy (NCT01385319)
Reassuring data on the safety of early DAPT discontinuationafter EES have also been reported by a retrospective analysis ofregistry data7 Moreover the pooled analysis of SPIRIT II III IVand COMPARE Trials of 6789 patients showed a persistentlylow ST rate in patients treated with EES but not PES who discon-tinued DAPT after 6 months which is consistent with our currentfindings16 Indeed while our analysis on primary study endpointand other secondary clinical outcomes numerically favoured long-term DAPT after EES implantation the stent thrombosis endpointsand 6-month clinical landmark analyses revealed no excess ofevents in the 6-month DAPT group compared with longer-termclopidogrel therapy which is at variance with the results observedafter PES implantation
The need for prolonged DAPT has been suggested to be in-versely related to stent late loss17 Potent inhibition of intimal
hyperplasia might more frequently lead to incomplete stent cover-age andor late stent mal-apposition requiring a more prolongedcourse of intensified anti-platelet therapy to maintain stentsafety17
Our study by randomizing patients to a balanced mixture ofstents with various anti-intimal hyperplasia and each stent groupto 6- vs 24-month DAPT duration offers no evidence supportingthe association between stent-related late-loss and need for pro-longed DAPT On the contrary the results of our explorativeyet pre-specified analysis suggest that the minimal DAPT durationmay be stent-specific and not clearly related to stent potencytowards inhibition of intimal hyperplasia
Several limitations of our study should be considered Our studywas not powered to assess outcomes with respect to the differentDAPT regimens tested in our study for each stent type Similarlyour study was overall underpowered to assess the effect ofDAPT duration on stent thrombosis endpoints Therefore ourfindings should be considered exploratory and hypothesisgenerating
Our observation that primary study endpoint and other second-ary clinical ischaemic endpoints may be significantly lower after6-month compared with 24-month DAPT duration in ZES-Streated patients is intriguing but it should be interpreted withcaution In light of the limitations outlined above this findingshould be reassuring on the safety of early DAPT discontinuationin patients treated with ZES-S Yet a new paradigm has beenrecently proposed by the results of the WOEST study (clinicaltrialsgov NCT00769938) according to which lessening intensity of anti-platelet inhibition via dropping aspirin has resulted in a dramaticreduction of not only bleeding but also ischaemic endpoints includ-ing overall and cardiac mortality This paradigm has also been shownto apply to periprocedural anti-thrombotic therapy and it will befurther investigated in the ongoing comparative effectiveness of1 month of ticagrelor plus aspirin followed by ticagrelor monother-apy vs a current-day intensive DAPT in all-comer patients undergo-ing percutaneous coronary intervention with unrestricted BiolimusA9-eluting stent (GLOBAL LEADERS) study
In conclusion our study offers preliminary evidence that optimalduration of DAPT may be stent-specific with no clear associationbetween late loss potency and vulnerability to shorter DAPT dur-ation DES-specific studies aiming at unraveling the optimal DAPTduration after stent implantation are eagerly required and some ofthem are currently ongoing
Conflict of interest MV has received honoraria for lecturesad-visory board and research grants from Merck Iroko Eli Lilly andMedtronic honoraria for advisory board and lectures from TheMedicines Company and Eli Lilly Co Daiichi Sankyo Inc St Judeand Abbott Vascular lectures from Cordis CID and Terumo
FundingThe study is an investigator-driven clinical trial The conduct of thisstudy did not receive any direct or indirect external funding but wasentirely supported by the University of Ferrara which employed dedi-cated personnel for data monitoring data management events adjudi-cation and independent statistical analysis
Figure 5 Stent potency in inhibiting repeated intervention andrelative risks of adverse outcomes after 6-month dual anti-platelet therapy Relative risk reductions and corresponding95 confidence intervals (vertical bars) for target lesion revascu-larization from 30 days onwards for each drug-eluting stentemployed in the study when compared with bare metal stentgroup (reference group) is shown to the left In the middle rela-tive risk reductions and corresponding 95 confidence intervals(vertical bars) for 6-month landmark analysis of death myocardialinfarction or stroke in the 6-month when compared with24-month dual antiplatelet group is shown for each stent Inthe right portion of the figure relative risk reductions and corre-sponding 95 confidence intervals (vertical bars) for 6-monthlandmark analysis of definite probable or possible stent throm-bosis (ST) in the 6-month when compared with 24-month dualantiplatelet group is shown for each stent Note that a negativerelative risk reduction such as that observed for PES or BMSgroups implies the possibility of a relative risk increase in thestudy arm when compared with reference group EP endpointTLR target lesion revascularization from 30 days onwards Ddeath MI myocardial infarction CV cerebrovascular accidentDAPT dual antiplatelet therapy ST stent thrombosis Ref refer-ence arm BMS bare metal stent ZES-S zotarolimus-eluting stentEndeavor Sprint PES paclitaxel-eluting stent EES everolimus-eluting stent
M Valgimigli et alPage 10 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from
Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from

Clinical sitesAzienda Ospedaliero Universitaria di Ferrara ItalymdashM ValgimigliG Campo M Tebaldi C Tumscitz C Cavazza E CangianoM Minarelli C Arcozzi A Scalone M Borghesi J Marchesini MMonti Valle Oppio Hospitalmdash GF Percoco M KubbajehA Frangione Villa Maria Cecilia Hospitalmdash A CremonesiF Castriota F Colombo K Oshoala C Garattoni P SbarzagliaCento HospitalmdashG Fucarsquo
AppendixThe following investigators participated in the studyExecutive CommitteemdashM Valgimigli (principal investigator)G Campo G Percoco R Ferrari Data and Safety MonitoringBoardmdashN Avigni R Mazzucco Clinical Events CommitteemdashPVranckx (chair) Belgium S Curello Italy G Guardigli Italy DataManagement and MonitoringmdashMedial trial Analysis Switzerlandand Eustrategy Research Coordination Italymdash M MontiS Gambetti and L Bristot Statistical CommitteemdashGParrinello(chair) University of Brescia
References1 King SB III Smith SC Jr Hirshfeld JW Jr Jacobs AK Morrison DA Williams DO
Feldman TE Kern MJ OrsquoNeill WW Schaff HV Whitlow PL Adams CDAnderson JL Buller CE Creager MA Ettinger SM Halperin JL Hunt SAKrumholz HM Kushner FG Lytle BW Nishimura R Page RL Riegel BTarkington LG Yancy CW 2007 focused update of the ACCAHASCAI 2005guideline update for percutaneous coronary intervention a report of the Ameri-can College of CardiologyAmerican Heart Association Task Force on Practiceguidelines J Am Coll Cardiol 200851172ndash209
2 Wijns W Kolh P Danchin N Di Mario C Falk V Folliguet T Garg S Huber KJames S Knuuti J Lopez-Sendon J Marco J Menicanti L Ostojic M Piepoli MFPirlet C Pomar JL Reifart N Ribichini FL Schalij MJ Sergeant P Serruys PWSilber S Sousa Uva M Taggart D Vahanian A Auricchio A Bax J Ceconi CDean V Filippatos G Funck-Brentano C Hobbs R Kearney P McDonagh TPopescu BA Reiner Z Sechtem U Sirnes PA Tendera M Vardas PEWidimsky P Alfieri O Dunning J Elia S Kappetein P Lockowandt U Sarris GVouhe P von Segesser L Agewall S Aladashvili A Alexopoulos D Antunes MJAtalar E Brutel de la Riviere A Doganov A Eha J Fajadet J Ferreira RGarot J Halcox J Hasin Y Janssens S Kervinen K Laufer G Legrand VNashef SA Neumann FJ Niemela K Nihoyannopoulos P Noc M Piek JJ Pirk JRozenman Y Sabate M Starc R Thielmann M Wheatley DJ Windecker SZembala M Guidelines on myocardial revascularization The Task Force on Myo-cardial Revascularization of the European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2010312501ndash2555
3 Joner M Nakazawa G Finn AV Quee SC Coleman L Acampado E Wilson PSSkorija K Cheng Q Xu X Gold HK Kolodgie FD Virmani R Endothelial cell re-covery between comparator polymer-based drug-eluting stents J Am Coll Cardiol200852333ndash342
4 Leon MB Nikolsky E Cutlip DE Mauri L Liberman H Wilson H Patterson JMoses J Kandzari DE Improved late clinical safety with zotarolimus-elutingstents compared with paclitaxel-eluting stents in patients with de novo coronarylesions 3-year follow-up from the ENDEAVOR IV (Randomized Comparison ofZotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary ArteryDisease) trial JACC Cardiovasc Interven 201031043ndash1050
5 Stone GW Rizvi A Newman W Mastali K Wang JC Caputo R Doostzadeh JCao S Simonton CA Sudhir K Lansky AJ Cutlip DE Kereiakes DJEverolimus-eluting versus paclitaxel-eluting stents in coronary artery disease NEngl J Med 20103621663ndash1674
6 Kandzari DE Barker CS Leon MB Mauri L Wijns W Fajadet J Mehran R Dualantiplatelet therapy duration and clinical outcomes following treatment withzotarolimus-eluting stents JACC Cardiovasc Interven 201141119ndash1128
7 Naidu SS Krucoff MW Rutledge DR Mao VW Zhao W Zheng Q Wilburn OSudhir K Simonton C Hermiller JB Contemporary Incidence and Predictors ofStent Thrombosis and Other Major Adverse Cardiac Events in the Year AfterXIENCE V Implantation Results From the 8061-Patient XIENCE V UnitedStates Study JACC Cardiovasc Interven 20125626ndash635
8 Valgimigli M Campo G Percoco G Monti M Ferrari F Tumscitz C Zuffi AColombo F Kubbajeh M Cavazza C Cangiano E Tebaldi M Minarelli MArcozzi C Scalone A Frangione A Borghesi M Marchesini J Parrinello GFerrari R Randomized comparison of 6- vs 24-month clopidogrel therapy afterbalancing anti-intimal hyperplasia stent potency in all-comer patients undergoingpercutaneous coronary intervention Design and rationale for the PROlongingDual-antiplatelet treatment after Grading stent-induced Intimal hyperplasiastudy (PRODIGY) Am Heart J 2010160804ndash811
9 Valgimigli M Campo G Monti M Vranckx P Percoco G Tumscitz C Castriota FColombo F Tebaldi M Fuca G Kubbajeh M Cangiano E Minarelli M Scalone ACavazza C Frangione A Borghesi M Marchesini J Parrinello G Ferrari R Short-vs long-term duration of dual-antiplatelet therapy after coronary stenting a ran-domized multicenter trial Circulation 20121252015ndash2026
10 Cutlip DE Windecker S Mehran R Boam A Cohen DJ van Es GA Steg PGMorel MA Mauri L Vranckx P McFadden E Lansky A Hamon MKrucoff MW Serruys PW Clinical end points in coronary stent trials a casefor standardized definitions Circulation 20071152344ndash51
11 Therneau TM Grambsch PM Modeling Survival Data Extending the Cox ModelNew York NY Springer-Verlag 2000
12 Hong MK A New Strategy for Discontinuation of Dual Antiplatelet Therapy RealSafety and Efficacy of 3-Month Dual Antiplatelet Therapy FollowingZotarolimus-Eluting Stent Implantation RESET Trial ACC 2012Chicago(24March)oral presentation
13 Guagliumi G Ikejima H Sirbu V Bezerra H Musumeci G Lortkipanidze NFiocca L Tahara S Vassileva A Matiashvili A Valsecchi O Costa M Impact ofdrug release kinetics on vascular response to different zotarolimus-elutingstents implanted in patients with long coronary stenoses the LongOCT study(Optical Coherence Tomography in Long Lesions) JACC Cardiovasc Interven20114778ndash785
14 Guagliumi G Musumeci G Sirbu V Bezerra HG Suzuki N Fiocca L Matiashvili ALortkipanidze N Trivisonno A Valsecchi O Biondi-Zoccai G Costa MA Opticalcoherence tomography assessment of in vivo vascular response after implantationof overlapping bare-metal and drug-eluting stents JACC Cardiovasc Interven 20103531ndash539
15 Kim JS Jang IK Fan C Kim TH Park SM Choi EY Lee SH Ko YG Choi DHong MK Jang Y Evaluation in 3 months duration of neointimal coverage afterzotarolimus-eluting stent implantation by optical coherence tomography the EN-DEAVOR OCT trial JACC Cardiovasc Interven 200921240ndash1247
16 Kedhi E Stone GW Kereiakes DJ Serruys PW Parise H Fahy M Simonton CAKrishnankutty S Soodll P Smits PS Stent thrombosis insights on outcomes pre-dictors and impact of dual antiplatelet therapy interruption from the SPIRIT IISPIRIT III SPIRIT IV and COMPARE Trials Eurointervention 20128599ndash606
17 Camenzind E Steg PG Wijns W Stent thrombosis late after implantation of first-generation drug-eluting stents a cause for concern Circulation 20071151440ndash55 discussion 1455
18 Ellis SG Vandormael MG Cowley MJ DiSciascio G Deligonul U Topol EJBulle TM Coronary morphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronary disease Implications forpatient selection Multivessel Angioplasty Prognosis Study Group Circulation1990821193ndash1202
Dual antiplatelet therapy and stent-type Page 11 of 11
at UniversitAtilde
degli Studi di Brescia on January 16 2013
httpeurheartjoxfordjournalsorgD
ownloaded from