antioxidant and antiplatelet effects of atorvastatin by nox2 inhibition
TRANSCRIPT
Available online at www.sciencedirect.com
www.elsevier.com/locate/tcm
T R E N D S I N C A R D I O V A S C U L A R M E D I C I N E 2 4 ( 2 0 1 4 ) 1 4 2 – 1 4 8
1050-1738/$ - see frohttp://dx.doi.org/10.
nCorresponding auE-mail address:
Review article
Antioxidant and antiplatelet effects of atorvastatinby Nox2 inhibition
Francesco Violin, Roberto Carnevale, Daniele Pastori, and Pasquale Pignatelli
I Clinica Medica, Sapienza University of Rome, Viale del Policlinico 155, Rome 00161, Italy
a r t i c l e i n f o
Article history:
Received 1 August 2013
Received in revised form
17 September 2013
Accepted 18 September 2013
Available online 2 October 2013
nt matter & 2014 Elsevie1016/j.tcm.2013.09.006
thor. Tel.: þ39-064-46-193francesco.violi@uniroma
a b s t r a c t
In recent years, it became evident that reactive oxygen species (ROS) are implicated in the
thrombotic process. Statins are lipid-lowering agents able to lower serum cholesterol levels
and retard atherosclerotic complications and their clinical sequelae. There is evidence that,
among statins, atorvastatin may exert antiplatelet effects by interfering with redox
signaling. Recent studies demonstrated that atorvastatin possesses antiplatelet activity
via inhibition of platelet formation of NADPH oxidase-derived ROS. This effect results in
down-regulation of isoprostanes, which are pro-aggregating molecules, and up-regulation
of nitric oxide, which is a platelet inhibitor; such changes occurred immediately after
atorvastatin administration and were independent from lipid-lowering property. Exper-
imental and clinical studies documented that statins possess antithrombotic effects, which
may account for the reduction of thrombotic-related vascular outcomes. This has been
evidenced in different cardiovascular clinical settings such as percutaneous coronary
intervention (PCI), myocardial infarction (MI), and venous thrombosis. Future studies
should be addressed to analyze if the antiplatelet effect of atorvastatin may preferentially
occur at high dosage. Interestingly, the antiplatelet effects of statins could be useful in
clinical settings where the clinical efficacy of aspirin and other antiplatelet drugs is still
uncertain.
& 2014 Elsevier Inc. All rights reserved.
Introduction
Reactive oxygen species (ROS) are chemically unstable mol-ecules, which rapidly react with other molecules givingformation of oxidized products such as oxidized low-density lipoprotein (LDL), peroxy-nitrite, or protein adducts(Sugamura and Keaney, 2011). At physiologic concentration,ROS serve as second messengers, behaving as intracellularsignals for cell activation (Sugamura and Keaney, 2011). Thisprocess is particularly evident in platelets, where ROS aredirectly implicated in cell activation. Upon activation bycommon agonists, platelets produce several types of ROS like
r Inc. All rights reserved.
3; fax: þ39-064-997-0103.1.it (F. Violi).
superoxide anion or hydrogen peroxide, which contribute topropagation of platelet aggregation (Violi and Pignatelli,2012). The knowledge of mechanisms underlying up-regulation of ROS could be useful to work out an effectivetherapeutic approach to modulate oxidative stress in thesetting of athero-thrombosis. Basic, experimental and clinicalstudies provided definite evidence on the key role played byplatelets in the process of athero-thrombosis. Therefore,interventional trials with aspirin (a platelet COX-1 inhibitor)(Vane, 1971), thienopyridines such as ticlopidine or clopidog-rel (a platelet P2Y12 receptor inhibitor) (Cattaneo, 2004), orthe combination of the two drugs, i.e., aspirin plus

T R E N D S I N C A R D I O V A S C U L A R M E D I C I N E 2 4 ( 2 0 1 4 ) 1 4 2 – 1 4 8 143
clopidogrel, reduced clinical outcomes in patients with acutecoronary syndromes (ACS) (Yusuf et al., 2001). Meta-analysisof trials with antiplatelet drugs in patients with stableatherosclerosis, such as those with stable angina, peripheralarterial disease, or cerebro-vascular diseases, confirmed theclinical efficacy of this drugs' category (AntithromboticTrialists, 2002).Despite the encouraging results obtained from interven-
tional trials, the real world of athero-thrombosis is stillburdened by a high rate of morbidity and mortality. Thereare several issues that may potentially account for the lack ofeffect of some antithrombotic treatments and cardiovascularrelapses. For example, poor adherence to prescribed therapymay play a relevant role in this context, as shown by thehigher rate of adverse events and hospital readmission inpatients who do not completely adhere to aspirin treatment(Cotter et al., 2004). Concomitant multiple anti-athero-sclerotic treatments are an important cause of poor aspirincompliance and should be taken into account in monitoringpatients' adherence to antiplatelet treatment (Pignatelli et al.,2008). Insufficient antiplatelet effect of the drugs currentlyavailable for clinical use may be another relevant explanationfor vascular relapses (Violi and Pignatelli, 2006). Recently,prasugrel, a new P2Y12 receptor antagonist, reduced vascularcomplications in patients with ACS (Montalescot et al., 2009)when compared to clopidogrel.Another explanation for this “apparent” partial protective
action may be found in the inability of most drugs inmodulating platelet ROS formation. In fact, experimentaland clinical studies demonstrated that aspirin minimallyaffects platelet production of ROS (Basili et al., 2011; Leoet al., 1997; Pignatelli et al., 1998), and it is still unclear ifthienopyridines have some influence on the platelet produc-tion of ROS (Evangelista et al., 2005). A crucial issue is,however, to establish if inhibition of ROS formation hasimplications for platelet activation and for clinical progres-sion of atherosclerotic diseases. Recent studies on this topicsuggest that modulating the generation or blunting ROSactivity is translated to inhibition of platelet aggregation(Pignatelli et al., 2011). In this context, recent data showed arole for statins in impairing platelet ROS formation; this effectcontributes to the inhibition of platelet cellular intra-signaling that ultimately leads to platelet activation(Pignatelli et al., 2012a, 2012b). This effect of statins may beof clinical relevance as it can explain some of the beneficialproperties that cannot be solely related to the statins' lipid-lowering efficacy. This review deals with the relationshipbetween statins and platelet activation, focusing in particularon the antioxidant effect of statins through the impairing ofplatelet ROS formation. Furthermore, we will analyze thepotential clinical implications of this statin property in thesetting of athero-thrombosis.
Patho-physiology of platelets in thrombosis andbleeding
Upon endothelium disruption, sub-endothelial componentsand, above all, collagen trigger the accumulation and activa-tion of platelets, and tissue factor (TF) initiates the generation
of thrombin, which also activates platelets (Ignarro, 2002;Marcus et al., 2002). Recently, two distinct pathways acting inparallel or separately in activating platelets have been iden-tified (Dubois et al., 2006; Mangin et al., 2006). In the firstpathway, the exposure of sub-endothelial collagen initiatesplatelet activation; in the second one, thrombin generated byTF is the initial trigger. Both these pathways result in theinitiation of the thrombotic event (Dubois et al., 2006; Manginet al., 2006).Thrombus formation is a dynamic process in which some
platelets adhere to damaged wall and others separate fromthe developing thrombus (Dubois et al., 2007). This phenom-enon is mediated by a conformational transition in glyco-protein IIb/IIIa (gp IIb/IIIa) that increases its affinity forfibrinogen and von Willebrand factor (Du et al., 1993). Thefollowing propagation of platelet activation depends upon theformation and release of several molecules. Among them arethe powerful thrombin, adenosine diphosphate (ADP), andeicosanoids (Davi and Patrono, 2007).Amid the eicosanoids, thromboxane A2 (TxA2) and isopros-
tanes are of particular interest as these two platelet agonistsshare a similar receptor on platelet surface but possessdifferent properties (Pratico et al., 1996).TXA2 is synthesized from arachidonic acid (AA) through a
phospholipase A2 (PLA2) and cyclooxygenase (COX)-depend-ent pathway. TXA2 activates phospholipase C and finallyinduces the increase of cytosolic levels of Ca2þ.Isoprostanes are produced from AA by a free radical-
mediated mechanism likely dependent upon NADPH oxidaseactivation (Violi et al., 2006); they modulate the adhesion andactivation of platelets induced by low levels of other agonistsand are involved in platelet recruitment and thrombusenlargement (Pignatelli et al., 2011).Platelet recruitment represents the final phase of thrombus
formation; it depends upon the release of several pro-aggregating substances able to induce the activation of newplatelets approaching the site of thrombus growth (Krotzet al., 2002). In this phase, the role of ROS-generatingenzymes, such as NADPH oxidase, is of particular relevance.A reduced platelet recruitment in subjects lacking the func-tional catalytic core of NADPH oxidase, with a mechanismdependent on isoprostanes, was recently demonstrated(Pignatelli et al., 2011). Evidence in support of this mechanismis given by the observation that the addition of isoprostanesto samples from these patients restored platelet recruitment(Pignatelli et al., 2011). During platelet recruitment, latesignaling events enhance platelet–platelet affinity. Molecules,such as CD40 ligand (CD40L), participate in the platelet–platelet synapse to create a protected environment in theinterstices of the clot that stabilizes the thrombus (Brasset al., 2005). Also, soluble CD40L (sCD40L) is released fromplatelets by a NADPH oxidase-dependent mechanism(Pignatelli et al., 2004).
Role of ROS on platelet function
ROS play a specific role in platelet activation; the first studydemonstrating that platelets were able to generate ROS waspublished in 1977 (Marcus et al., 1977). Nowadays, we know

T R E N D S I N C A R D I O V A S C U L A R M E D I C I N E 2 4 ( 2 0 1 4 ) 1 4 2 – 1 4 8144
that in platelets, ROS are mainly produced by NADPH oxidaseand are implicated in the propagation of platelet activation(Pignatelli et al., 2011). Platelets possess all the subunits of theNADPH oxidase, including gp91phox (NOX2), which is itscatalytic subunit (Pignatelli et al., 2011, 2004; Seno et al.,2001). Activation of NADPH oxidase is crucial for O2� produc-tion as shown by its complete suppression in case of NADPHoxidase hereditary deficiency. We recently demonstrated thatplatelets from patients with chronic granulomatous disease(X-CGD) have an almost complete suppression of platelet O2�
as a consequence of the hereditary deficiency of NOX2(Pignatelli et al., 2004). Moreover, in X-CGD patients we foundincreased level of another ROS, namely Nitric Oxide (NO)(Pignatelli et al., 2011). NO is produced by endothelial cellsand by activated platelets and acts by inhibiting plateletfunction (Loscalzo, 2013; Walford and Loscalzo, 2003). Thereaction of O2� derived from NADPH oxidase with NO resultsin the formation of the highly reactive species peroxy-nitrite,so negatively affecting the antithrombotic properties of NO(Gresele et al., 2011).The role of ROS in platelet activation was originally studied
by Del Principe et al. (1991) who observed a role for catalase ininhibiting platelet function by interfering with H2O2.A more prominent role in platelet recruitment seems to be
played by isoprostanes (8-iso-PGF2α), as shown by a recentwork from our group (Pignatelli et al., 2011). The experimentswere conducted using a specific inhibitor peptide, namelygp91ds-tat. This peptide is able to block the binding of thecytosolic NADPH oxidase subunit p47phox to the membranesubunit gp91phox (Williams and Griendling, 2007). The studyshowed that gp91ds-tat prevented p47phox binding to plateletgp91phox and significantly inhibited both platelet recruitmentand platelet 8-iso-PGF2α productions. From the resultsobtained, we can define (1) a key role for NADPH oxidase inthe formation of platelet 8-iso-PGF2α and (2) a potential rolefor 8-iso-PGF2α in the process of platelet recruitment(Pignatelli et al., 2011). This hypothesis was strengthened byexperiments performed in platelets from healthy subjects(HS) or patients with X-CGD. In platelets from HS, a signi-ficant increase of platelet recruitment was observedwhen platelets were incubated with scalar concentration of8-iso-PGF2α. Platelets lacking NADPH oxidase had reduced 8-iso-PGF2α production, coinciding with impaired plateletrecruitment. Incubation of platelets from X-CGD patientswith 8-iso-PGF2α resulted in a partial restoration of plateletrecruitment (Pignatelli et al., 2011).In order to investigate the mechanism through which 8-iso-
PGF2α enhanced platelet recruitment, the attention waspointed to the gp IIb/IIIa. At physiological concentration, 8-iso-PGF2α produced by platelets stimulated with AAenhanced the activation of gp IIb/IIIa. This effect seemed tobe attributable to the mobilization of Ca2þ (Phillips et al.,1987), that was increased by 8-iso-PGF2α both in normalplatelets and in platelets from X-CGD patients (Pignatelliet al., 2011).The role of ROS in the process of platelet activation may be
relevant in clinical settings characterized by a process ofanoxia-reoxygenation (AR), which is usually associated with aburst of ROS (Basili et al., 2011). In vitro experiments of plateletsfrom AR models, such as PCI, showed up-regulation of
platelet ROS, which were elicited by NOX2 with ensuingPLA2 activation. These changes were associated withenhanced formation of both platelet eicosanoids (8-iso-PGF2αand TxA2) and platelet activation (Basili et al., 2011). Anin vivo study performed in patients undergoing PCI (Basiliet al., 2011) confirmed that oxidative stress and plateletactivation were amplified immediately after the procedure.This phenomenon was mitigated by the intravenous infusionof ascorbic acid, a known antioxidant (Basili et al., 2011).The role of ROS in platelet activation has also been
indirectly documented by experiments using animal knock-outs for antioxidant enzymes (Dayal et al., 2013; Jin et al.,2011; Liu et al., 2013) or pharmacologic tools to inhibit NADPHoxidase-dependent ROS formation and by clinical studieswith antioxidants such as statins (for references see sectionsbelow).In a genetic mouse model characterized by Glutathione
peroxidase-3 (GPx-3) deficiency, attenuated bleeding time,enhanced platelet response to agonists, and increased circu-lating levels of P-selectin were detected compared to wild-type animals (Jin et al., 2011). In a no-flow ischemia–reperfu-sion stroke model, GPx-3-deficient mice had significantlylarger cerebral infarctions compared with wild-type miceand platelet-dependent strokes (Jin et al., 2011). Togetherthese findings suggest that in case of impaired or absenthydrogen peroxide degradation, platelet aggregation isenhanced and may facilitate thrombosis.Another study by Dayal et al. tested the hypothesis that
aged mice overexpressing the antioxidant enzyme gluta-thione peroxidase-1 (Gpx1) were protected from experimentalthrombosis (Dayal et al., 2013). Transgenic mice overexpress-ing Gpx1 (Gpx1-Tg) did not exhibit shortened times toocclusion of the carotid artery at 12 or 18 months of ageand were protected from age-related enhanced susceptibilityto venous thrombosis compared to wild-type mice.Of note, platelet activation was age-related and was asso-
ciated with increased hydrogen peroxide formation andactivation of fibrinogen receptor αIIbβ3, suggesting thathydrogen peroxide contributes to age-related platelet over-activation; all these changes were attenuated in Gpx1-Tgmice (Dayal et al., 2013). Aged mice displayed increasedintraplatelet expression of p47phox and superoxide dismu-tase-1, suggesting a mechanistic pathway for increasedhydrogen peroxide generation. Platelet inhibition by apocy-nin, a molecule that inhibits NADPH oxidase by impairingp47phox translocation to platelet membrane, resulted in pre-venting age-related platelet activation (Dayal et al., 2013).Together these findings indicate that platelet aggregation byhydrogen peroxide is regulated by NADPH oxidase activity.This finding was corroborated by another experimental
study performed in mice deficient for both the low-densitylipoprotein receptor (LDL-R) and Apobec-1. Animals werestudied at 30 weeks of age and again after 10 weeks with orwithout apocynin treatment (10 or 50 mg/kg/day orally) (Liuet al., 2013). Molecular imaging in control mice demonstrateda significant increase in P-selectin expression, VCAM-1expression, and platelet adhesion between 30 and 40 weeksof age. Apocynin reduced all of these endothelial events in adose-dependent fashion. On histology, apocynin reducedtotal monocyte accumulation in a dose-dependent manner
T R E N D S I N C A R D I O V A S C U L A R M E D I C I N E 2 4 ( 2 0 1 4 ) 1 4 2 – 1 4 8 145
as well as platelet adhesion, indicating a crucial role forNADPH oxidase in the inflammatory and thrombotic eventsthat complicate the course of athero-thrombosis (Liu et al.,2013).
Antioxidant effects of statins and plateletaggregation inhibition
Statins are lipid-lowering drugs that inhibit cholesterol bio-synthesis via down-regulation of 3-hydroxy-3-methyl-glu-taryl-CoA (HMG-CoA) reductase. These drugs are largelyused in patients with or at risk of cardiovascular disease(Istvan, 2002), and multiple randomized trials consistentlyreported that statins are able to lower the rate of myocardialinfarction, ischemic stroke, and cardiovascular death(Ludman et al., 2009). The favorable effect on cardiovascularevents depends mostly on the cholesterol-lowering functionand eventually to plaque stabilization (Pucci et al., 2007).However, experimental data demonstrated that statins mayalso act through a direct, and lipid-independent, antithrom-botic effect as demonstrated in models of arterial and venousthrombosis (Bea et al., 2003; Gertz et al., 2003). The role ofstatins on platelet function was largely investigated inpatients at risk of cardiovascular disease such as those withhypercholesterolemia, diabetes mellitus, metabolic syn-drome, or in patients with established atherosclerosis suchas those with peripheral artery disease or coronary heartdisease (Alber et al., 2006; Blann et al., 2001; Pignatelli et al.,2007; Serebruany et al., 2006; Sommeijer et al., 2005; Tannouset al., 1999). Long-term studies lasting at least 30 daysdemonstrated that statins inhibit platelet function asassessed by ex vivo tests of platelet aggregation (Pignatelliet al., 2010). Moreover, clinical studies demonstrated thatstatins, and in particular atorvastatin, were able to modulatethe circulating levels of molecules released by platelets upon
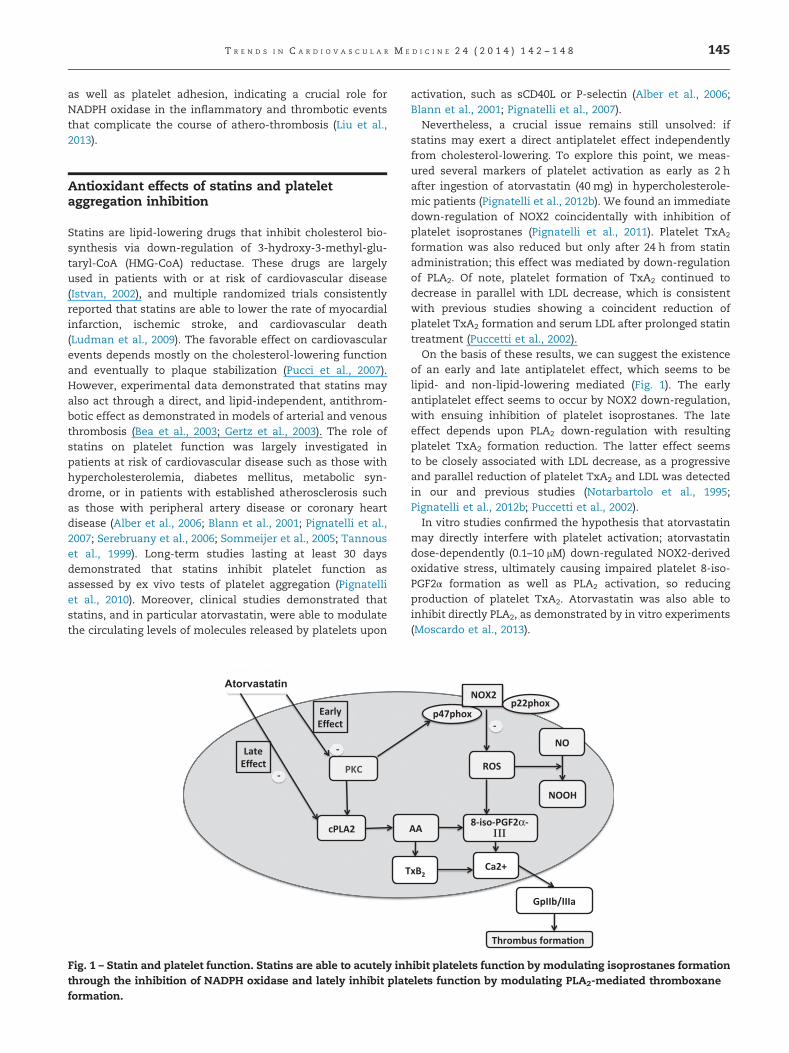
Fig. 1 – Statin and platelet function. Statins are able to acutely inhthrough the inhibition of NADPH oxidase and lately inhibit platformation.
activation, such as sCD40L or P-selectin (Alber et al., 2006;Blann et al., 2001; Pignatelli et al., 2007).Nevertheless, a crucial issue remains still unsolved: if
statins may exert a direct antiplatelet effect independentlyfrom cholesterol-lowering. To explore this point, we meas-ured several markers of platelet activation as early as 2 hafter ingestion of atorvastatin (40 mg) in hypercholesterole-mic patients (Pignatelli et al., 2012b). We found an immediatedown-regulation of NOX2 coincidentally with inhibition ofplatelet isoprostanes (Pignatelli et al., 2011). Platelet TxA2
formation was also reduced but only after 24 h from statinadministration; this effect was mediated by down-regulationof PLA2. Of note, platelet formation of TxA2 continued todecrease in parallel with LDL decrease, which is consistentwith previous studies showing a coincident reduction ofplatelet TxA2 formation and serum LDL after prolonged statintreatment (Puccetti et al., 2002).On the basis of these results, we can suggest the existence
of an early and late antiplatelet effect, which seems to belipid- and non-lipid-lowering mediated (Fig. 1). The earlyantiplatelet effect seems to occur by NOX2 down-regulation,with ensuing inhibition of platelet isoprostanes. The lateeffect depends upon PLA2 down-regulation with resultingplatelet TxA2 formation reduction. The latter effect seemsto be closely associated with LDL decrease, as a progressiveand parallel reduction of platelet TxA2 and LDL was detectedin our and previous studies (Notarbartolo et al., 1995;Pignatelli et al., 2012b; Puccetti et al., 2002).In vitro studies confirmed the hypothesis that atorvastatin
may directly interfere with platelet activation; atorvastatindose-dependently (0.1–10 mM) down-regulated NOX2-derivedoxidative stress, ultimately causing impaired platelet 8-iso-PGF2α formation as well as PLA2 activation, so reducingproduction of platelet TxA2. Atorvastatin was also able toinhibit directly PLA2, as demonstrated by in vitro experiments(Moscardo et al., 2013).
ibit platelets function by modulating isoprostanes formationelets function by modulating PLA2-mediated thromboxane

T R E N D S I N C A R D I O V A S C U L A R M E D I C I N E 2 4 ( 2 0 1 4 ) 1 4 2 – 1 4 8146
This antiplatelet effect is not peculiar of atorvastatin;similar results have been obtained with rosuvastatin, anotherpowerful lipid-lowering molecule (Carter, 2010). Hypercholes-terolemic patients acutely treated with rosuvastatin (20 mg),a significant inhibition of sNOX2dp release, a direct marker ofNADPH oxidase activation (Carnevale et al., 2012), wasobserved, associated to inhibited 8-iso-PGF2α formation andreduced platelet activation as early as 2 h after the first drugingestion (Pignatelli et al., 2012a).Over-generation of platelet NO is another mechanism
accounting for the antioxidant and antiplatelet effect bystatins. Also, in this case, the effect of statins on platelet redoxsignaling is likely to play a crucial role. It is well established, infact, that ROS negatively influence NO biosynthesis and activ-ity (Cangemi et al., 2012). Therefore, the impaired production ofNOX2-derived oxidative stress by statins is likely to up-regulateNO generation as demonstrated in rosuvastatin-treatedpatients where NOX2 inhibition is associated to increased NO(Pignatelli et al., 2012a). However, other studies demonstratedthat statins directly enhance platelet cGMP, indicating thatthey up-regulate platelet eNOS activity (Chou et al., 2008;Tannous et al., 1999; Yokoyama et al., 2005).
Clinical perspectives and conclusions
The data reported in this review suggest that statins mayexert an antiplatelet effect by reducing platelet ROS forma-tion with a mechanism involving NADPH oxidase down-regulation. In this context, the peculiarity of statins is intheir ability to inhibit not only platelet TxA2 but also platelet8-iso-PGF2α formation via inhibition of NOX2 activation. Thisproperty is unrelated, at least partly, to its primary mecha-nism of action, i.e., the lipid-lowering activity, as the anti-platelet and antioxidant effect occurs as early as 2 h fromstatin's administration and may contribute to the short-termreduction of thrombotic-related events observed after earlyand high dosage administration of statins in some clinicalconditions where patients are at high risk of arterial orvenous thrombosis. In the setting of arterial thrombosis ithas been suggested that statins reduce the rate of peri-procedural myocardial infarction occurring early from PCI(Patti et al., 2011). Furthermore, high doses of statins havebeen associated with a significant reduction of cardiovascularevents in patients with ACS (Patti et al., 2011). The antipla-telet and antioxidant effect of statins may turn useful in avariety of diseases complicated by athero-thrombosis. Forexample, diabetes mellitus is characterized by acceleratedatherosclerosis with serious complication in the coronary andcerebral tree. Despite aspirin administration being useful toreduce cardiovascular events in patients with acute andchronic coronary heart disease (Antithrombotic Trialists,2002), it is consistently shown that aspirin is less efficaciousin diabetic patients with a lower reduction of cardiovascularevents than that observed in those with other atheroscleroticsettings. We have recently showed that in these patients onaspirin treatment, platelet NOX2 is up-regulated and isresponsible for 8-iso-PGF2α over-production and plateletactivation (Cangemi et al., 2012). In a pilot study, we rec-ently demonstrated that combining atorvastatin with aspirin
down-regulates platelet NOX2 and reduces platelet isopros-tanes formation (Carnevale et al., 2013).In the setting of venous thrombosis, trials performed in
apparently healthy subjects showed that statins significantlyreduce the rate of venous thrombosis (Winchester et al.,2010). Moreover, study with different statins dosages inatherosclerotic patients supported a role for high dose ofstatins in preventing venous thrombosis (Khemasuwan et al.,2011). This effect may be exploited in patients with venousthrombosis recurrence in whom the use of anticoagulant iscontraindicated.Statin dosage may represent an important challenge for its
future use as antiplatelet drugs as the clinical efficacy wasoften achieved comparing high doses of statins such as 40–80 mg/day simvastatin or atorvastatin or 20–40 mg/day rosu-vastatin versus lower statin dosage. Therefore, the existenceof a dose-related anti-thrombotic effect by statins could beargued, but this hypothesis needs to be evaluated.In conclusion, experimental and clinical studies suggest
that atorvastatin and other statins, such as rosuvastatin,exert an antioxidant and antiplatelet effect via down-regulation of NOX2. This provides new perspectives forclinical use of statins in human models characterized byenhanced oxidative stress and pro-thrombotic state in orderto further reduce vascular ischemic complications.
r e f e r e n c e s
Alber HF, Frick M, Suessenbacher A, et al. Effect of atorvastatinon circulating proinflammatory T-lymphocyte subsets andsoluble CD40 ligand in patients with stable coronary arterydisease—A randomized, placebo-controlled study. AmericanHeart Journal 2006;151:139.
Antithrombotic Trialists C. Collaborative meta-analysis of rand-omised trials of antiplatelet therapy for prevention of death,myocardial infarction, and stroke in high risk patients. BritishMedical Journal 2002;324:71–86.
Basili S, Pignatelli P, Tanzilli G, et al. Anoxia-reoxygenationenhances platelet thromboxane A2 production via reactiveoxygen species-generated NOX2: effect in patients undergoingelective percutaneous coronary intervention. Arteriosclerosis,Thrombosis, and Vascular Biology 2011;31:1766–71.
Bea F, Blessing E, Shelley MI, Shultz JM, Rosenfeld ME. Simvastatininhibits expression of tissue factor in advanced atheroscleroticlesions of apolipoprotein E deficient mice independently of lipidlowering: potential role of simvastatin-mediated inhibitionof Egr-1 expression and activation. Atherosclerosis 2003;167:187–94.
Blann AD, Gurney D, Hughes E, Buggins P, Silverman SH, Lip GY.Influence of pravastatin on lipoproteins, and on endothelial,platelet, and inflammatory markers in subjects with periph-eral artery disease. The American Journal of Cardiology2001;88(A7–8):89–92.
Brass LF, Zhu L, Stalker TJ. Minding the gaps to promotethrombus growth and stability. The Journal of Clinical Inves-tigation 2005;115:3385–92.
Cangemi R, Pignatelli P, Carnevale R, et al. Platelet isoprostaneoverproduction in diabetic patients treated with aspirin.Diabetes 2012;61:1626–32.
Carnevale R, Iuliano L, Nocella C, et al. Relationship betweenplatelet and urinary 8-Iso-PGF2alpha levels in subjects withdifferent degrees of NOX2 regulation. Journal of the AmericanHeart Association 2013;2:e000198.

T R E N D S I N C A R D I O V A S C U L A R M E D I C I N E 2 4 ( 2 0 1 4 ) 1 4 2 – 1 4 8 147
Carnevale R, Loffredo L, Pignatelli P, et al. Dark chocolate inhibitsplatelet isoprostanes via NOX2 down-regulation in smokers.Journal of Thrombosis And Haemostasis 2012;10:125–32.
Carter NJ. Rosuvastatin: a review of its use in the prevention ofcardiovascular disease in apparently healthy women or menwith normal LDL-C levels and elevated hsCRP levels. Ameri-can Journal of Cardiovascular Drugs: Drugs, Devices, andOther Interventions 2010;10:383–400.
Cattaneo M. Aspirin and clopidogrel: efficacy, safety, and theissue of drug resistance. Arteriosclerosis, Thrombosis, andVascular Biology 2004;24:1980–7.
Chou TC, Lin YF, Wu WC, Chu KM. Enhanced nitric oxide andcyclic GMP formation plays a role in the anti-platelet activity ofsimvastatin. British Journal of Pharmacology 2008;153:1281–7.
Cotter G, Shemesh E, Zehavi M, et al. Lack of aspirin effect: aspirinresistance or resistance to taking aspirin? American HeartJournal 2004;147:293–300.
Davi G, Patrono C. Platelet activation and atherothrombosis. TheNew England Journal of Medicine 2007;357:2482–94.
Dayal S, Wilson KM, Motto DG, Miller Jr., Chauhan AK, Lentz SR.Hydrogen peroxide promotes aging-related platelet hyperac-tivation and thrombosis. Circulation 2013;127:1308–16.
Del Principe D, Menichelli A, De Matteis W, et al. Hydrogenperoxide is an intermediate in the platelet activation cascadetriggered by collagen, but not by thrombin. ThrombosisResearch 1991;62:365–75.
Du X, Gu M, Weisel JW, et al. Long range propagation ofconformational changes in integrin alpha IIb beta 3. TheJournal of Biological Chemistry 1993;268:23087–92.
Dubois C, Panicot-Dubois L, Gainor JF, Furie BC, Furie B.Thrombin-initiated platelet activation in vivo is vWF inde-pendent during thrombus formation in a laser injury model.The Journal of Clinical Investigation 2007;117:953–60.
Dubois C, Panicot-Dubois L, Merrill-Skoloff G, Furie B, Furie BC.Glycoprotein VI-dependent and -independent pathways ofthrombus formation in vivo. Blood 2006;107:3902–6.
Evangelista V, Manarini S, Dell'Elba G, et al. Clopidogrel inhibitsplatelet-leukocyte adhesion and platelet-dependent leukocyteactivation. Thrombosis and Haemostasis 2005;94:568–77.
Gertz K, Laufs U, Lindauer U, et al. Withdrawal of statin treatmentabrogates stroke protection in mice. Stroke 2003;34:551–7.
Gresele P, Cerletti C, Guglielmini G, Pignatelli P, de Gaetano G,Violi F. Effects of resveratrol and other wine polyphenols onvascular function: an update. The Journal of NutritionalBiochemistry 2011;22:201–11.
Ignarro LJ. Nitric oxide as a unique signaling molecule in thevascular system: a historical overview. Journal of Physiologyand Pharmacology 2002;53:503–14.
Istvan ES. Structural mechanism for statin inhibition of3-hydroxy-3-methylglutaryl coenzyme A reductase. AmericanHeart Journal 2002;144:S27–32.
Jin RC, Mahoney CE, Coleman Anderson L, et al. Glutathioneperoxidase-3 deficiency promotes platelet-dependent throm-bosis in vivo. Circulation 2011;123:1963–73.
Khemasuwan D, Chae YK, Gupta S, et al. Dose-related effect ofstatins in venous thrombosis risk reduction. The AmericanJournal of Medicine 2011;124:852–9.
Krotz F, Sohn HY, Gloe T, et al. NAD(P)H oxidase-dependentplatelet superoxide anion release increases platelet recruit-ment. Blood 2002;100:917–24.
Leo R, Pratico D, Iuliano L, et al. Platelet activation by superoxideanion and hydroxyl radicals intrinsically generated by plate-lets that had undergone anoxia and then reoxygenated.Circulation 1997;95:885–91.
Liu Y, Davidson BP, Yue Q, et al. Molecular imaging of inflamma-tion and platelet adhesion in advanced atherosclerosis effectsof antioxidant therapy with NADPH oxidase inhibition. Circu-lation. Cardiovascular Imaging 2013;6:74–82.
Loscalzo J. The identification of nitric oxide as endothelium-derived relaxing factor. Circulation Research 2013;113:100–3.
Ludman A, Venugopal V, Yellon DM, Hausenloy DJ. Statins andcardioprotection—more than just lipid lowering? Pharmacol-ogy & Therapeutics 2009;122:30–43.
Mangin P, Yap CL, Nonne C, et al. Thrombin overcomes thethrombosis defect associated with platelet GPVI/FcRgammadeficiency. Blood 2006;107:4346–53.
Marcus AJ, Broekman MJ, Pinsky DJ. COX inhibitors and throm-boregulation. The New England Journal of Medicine 2002;347:1025–6.
Marcus AJ, Silk ST, Safier LB, Ullman HL. Superoxide productionand reducing activity in human platelets. The Journal ofClinical Investigation 1977;59:149–58.
Montalescot G, Wiviott SD, Braunwald E, et al. Prasugrel com-pared with clopidogrel in patients undergoing percutaneouscoronary intervention for ST-elevation myocardial infarction(TRITON-TIMI 38): double-blind, randomised controlled trial.Lancet 2009;373:723–31.
Moscardo A, Valles J, Latorre A, Madrid I, Santos MT. Reduction ofplatelet cytosolic phospholipase A2 activity by atorvastatinand simvastatin: biochemical regulatory mechanisms.Thrombosis Research 2013;131:e154–9.
Notarbartolo A, Davi G, Averna M, et al. Inhibition of thrombox-ane biosynthesis and platelet function by simvastatin in typeIIa hypercholesterolemia. Arteriosclerosis, Thrombosis, andVascular Biology 1995;15:247–51.
Patti G, Cannon CP, Murphy SA, et al. Clinical benefit of statinpretreatment in patients undergoing percutaneous coronaryintervention: a collaborative patient-level meta-analysis of 13randomized studies. Circulation 2011;123:1622–32.
Phillips DR, Fitzgerald LA, Charo IF, Parise LV. The plateletmembrane glycoprotein IIb/IIIa complex. Structure, function,and relationship to adhesive protein receptors in nucleatedcells. Annals of the New York Academy of Sciences1987;509:177–87.
Pignatelli P, Carnevale R, Cangemi R, et al. Atorvastatin inhibitsgp91phox circulating levels in patients with hypercholester-olemia. Arteriosclerosis, Thrombosis, and Vascular Biology2010;30:360–7.
Pignatelli P, Carnevale R, Di Santo S, et al. Rosuvastatin reducesplatelet recruitment by inhibiting NADPH oxidase activation.Biochemical Pharmacology 2012a;84:1635–42.
Pignatelli P, Carnevale R, Di Santo S, et al. Inherited humangp91phox deficiency is associated with impaired isoprostaneformation and platelet dysfunction. Arteriosclerosis, Throm-bosis, and Vascular Biology 2011;31:423–34.
Pignatelli P, Carnevale R, Pastori D, et al. Immediate antioxidantand antiplatelet effect of atorvastatin via inhibition of Nox2.Circulation 2012b;126:92–103.
Pignatelli P, Di Santo S, Barilla F, Gaudio C, Violi F. Multiple anti-atherosclerotic treatments impair aspirin compliance: effectson aspirin resistance. Journal of Thrombosis and Haemostasis2008;6:1832–4.
Pignatelli P, Pulcinelli FM, Lenti L, Gazzaniga PP, Violi F. Hydrogenperoxide is involved in collagen-induced platelet activation.Blood 1998;91:484–90.
Pignatelli P, Sanguigni V, Lenti L, et al. gp91phox-dependentexpression of platelet CD40 ligand. Circulation 2004;110:1326–9.
Pignatelli P, Sanguigni V, Lenti L, et al. Oxidative stress-mediatedplatelet CD40 ligand upregulation in patients with hyper-cholesterolemia: effect of atorvastatin. Journal of Thrombosisand Haemostasis 2007;5:1170–8.
Pratico D, Smyth EM, Violi F, FitzGerald GA. Local amplification ofplatelet function by 8-Epi prostaglandin F2alpha is not medi-ated by thromboxane receptor isoforms. The Journal of Bio-logical Chemistry 1996;271:14916–24.

T R E N D S I N C A R D I O V A S C U L A R M E D I C I N E 2 4 ( 2 0 1 4 ) 1 4 2 – 1 4 8148
Puccetti L, Pasqui AL, Pastorelli M, et al. Time-dependent effect ofstatins on platelet function in hypercholesterolaemia. Euro-pean Journal of Clinical Investigation 2002;32:901–8.
Pucci A, Sheiban I, Formato L, et al. In vivo coronary plaquehistology in patients with stable and acute coronary syn-dromes: relationships with hyperlipidemic status and statintreatment. Atherosclerosis 2007;194:189–95.
Seno T, Inoue N, Gao D, et al. Involvement of NADH/NADPHoxidase in human platelet ROS production. ThrombosisResearch 2001;103:399–409.
Serebruany VL, Miller M, Pokov AN, et al. Effect of statins onplatelet PAR-1 thrombin receptor in patients with the meta-bolic syndrome (from the PAR-1 inhibition by statins [PARIS]study). The American Journal of Cardiology 2006;97:1332–6.
Sommeijer DW, Joop K, Leyte A, Reitsma PH, ten Cate H.Pravastatin reduces fibrinogen receptor gpIIIa on platelet-derived microparticles in patients with type 2 diabetes. Jour-nal of Thrombosis and Haemostasis 2005;3:1168–71.
Sugamura K, Keaney Jr. Reactive oxygen species in cardiovasculardisease. Free Radical Biology & Medicine 2011;51:978–92.
Tannous M, Cheung R, Vignini A, Mutus B. Atorvastatin increasesecNOS levels in human platelets of hyperlipidemic subjects.Thrombosis and Haemostasis 1999;82:1390–4.
Vane JR. Inhibition of prostaglandin synthesis as a mechanism ofaction for aspirin-like drugs. Nature: New Biology 1971;231:232–5.
Violi F, Pignatelli P. Aspirin resistance: is this term meaningful?Current Opinion in Hematology 2006;13:331–6.
Violi F, Pignatelli P. Platelet oxidative stress and thrombosis.Thrombosis Research 2012;129:378–81.
Violi F, Sanguigni V, Loffredo L, et al. Nox2 is determinant forischemia-induced oxidative stress and arterial vasodilatation: apilot study in patients with hereditary Nox2 deficiency. Arterio-sclerosis, Thrombosis, and Vascular Biology 2006;26:e131–2.
Walford G, Loscalzo J. Nitric oxide in vascular biology. Journal ofThrombosis and Haemostasis 2003;1:2112–8.
Williams HC, Griendling KK. NADPH oxidase inhibitors: newantihypertensive agents? Journal of Cardiovascular Pharma-cology 2007;50:9–16.
Winchester DE, Wen X, Xie L, Bavry AA. Evidence of pre-procedural statin therapy a meta-analysis of randomizedtrials. Journal of the American College of Cardiology 2010;56:1099–109.
Yokoyama S, Ikeda H, Haramaki N, Yasukawa H, Katoh A,Imaizumi T. HMG-CoA reductase inhibitor protects againstin vivo arterial thrombosis by augmenting platelet-derivednitric oxide release in rats. Journal of Cardiovascular Pharma-cology 2005;45:375–81.
Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in additionto aspirin in patients with acute coronary syndromes withoutST-segment elevation. The New England Journal of Medicine2001;345:494–502.