duration of dual antiplatelet therapy after drug-eluting stent implantation
TRANSCRIPT
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . - , N O . - , 2 0 1 5
ª 2 0 1 5 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N DA T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 5 . 0 1 . 0 3 9
Duration of Dual Antiplatelet TherapyAfter Drug-Eluting Stent ImplantationA Systematic Review and Meta-Analysis of RandomizedControlled Trials
Gennaro Giustino, MD,* Usman Baber, MD,* Samantha Sartori, PHD,* Roxana Mehran, MD,* Ioannis Mastoris, MD,*Annapoorna S. Kini, MD,* Samin K. Sharma, MD,* Stuart J. Pocock, PHD,y George D. Dangas, MD, PHD*
ABSTRACT
Fro
Yo
Dr
Inc
Ab
Me
on
Co
sci
Bo
lat
Ma
BACKGROUND The optimal duration of dual antiplatelet therapy (DAPT) after drug-eluting stent (DES) implantation is
unclear, and its risks and benefits may vary according to DES generation.
OBJECTIVES The goal of this study was to evaluate the efficacy and safety of DAPT after DES implantation.
METHODS We included randomized controlled trials that tested different durations of DAPT after DES implantation:
shorter dual antiplatelet therapy (S-DAPT) was defined as the per-protocol minimum duration of DAPT after the pro-
cedure, and longer dual antiplatelet therapy (L-DAPT) was defined as the per-protocol period of more prolonged DAPT.
The primary efficacy and safety outcomes were definite/probable stent thrombosis and clinically significant bleeding
(CSB), respectively.
RESULTS Ten randomized controlled trials (N ¼ 32,135) were included. Compared with L-DAPT, S-DAPT had an overall
higher rate of stent thrombosis (odds ratio [OR] 1.71 [95% confidence interval (CI) 1.26 to 2.32]; p ¼ 0.001). The effect of
S-DAPT on stent thrombosis was attenuated with the use of second-generation DES (OR 1.54 [95% CI 0.96 to 2.47])
compared with the use of first-generation DES (OR 3.94 [95% CI 2.20 to 7.05]; p for interaction ¼ 0.008). S-DAPT had
an overall significantly lower risk of CSB (OR 0.63 [95% CI 0.52 to 0.75]; p < 0.001). Finally, a numerically lower
all-cause mortality rate was observed with S-DAPT (OR 0.87 [95% CI 0.74 to 1.01]; p ¼ 0.073).
CONCLUSIONS S-DAPT had overall lower rates of bleeding yet higher rates of stent thrombosis compared with
L-DAPT; the latter effect was significantly attenuated with the use of second-generation DES, although the analysis may
have been limited by the varying DAPT durations among studies. All-cause mortality was numerically higher with L-DAPT
without reaching statistical significance. Prolonging DAPT requires careful assessment of the trade-off between ischemic
and bleeding complications. (J Am Coll Cardiol 2015;-:-–-) © 2015 by the American College of Cardiology Foundation.
A period of dual antiplatelet therapy (DAPT) isrequired to prevent thrombotic complica-tions after percutaneous coronary inter-
vention (PCI) with drug-eluting stents (DES) (1,2).
m the *The Zena and Michael A. Wiener Cardiovascular Institute, Icahn
rk; and the yDepartment of Medical Statistics, London School of Hygien
. Mehran is consultant for AstraZeneca, Bayer, CSL Behring, Janssen Pha
., Regado Biosciences Inc., The Medicines Company and Watermark Co
bott Laboratories, AstraZeneca, Boston Scientific Corporation, Covidien, J
dicines Company, and Sanofi. Dr. Dangas is consultant for GE HealthCare,
the scientific advisory board of AstraZeneca. Dr. Pocock has received res
mpany, Pfizer, Edwards Lifesciences, Biosensors, Amgen, Boston Scientific
entific advisory board of Cardiovascular Systems Inc and serves on the
ston Scientific, Lilly/Daiichi Sankyo, and The Medicines Company. All
ionships relevant to the contents of this paper to disclose. Sanjay Kaul, M
nuscript received December 18, 2014; revised manuscript received Janua
Interruption or disruption of DAPT during thisperiod is associated with a high risk for ischemicevents, including stent thrombosis, especially duringthe first weeks after DES implantation (3,4).
School of Medicine at Mount Sinai, New York, New
e and Tropical Medicine, London, United Kingdom.
rmaceuticals Inc., Merck & Co. Inc., Osprey Medical
nsulting, and is on the scientific advisory board of
anssen Pharmaceuticals Inc., Merck & Co. Inc., The
Janssen Pharmaceuticals Inc., and Medtronic; and is
earch grants from GlaxoSmithKline, The Medicines
, AstraZeneca, and Janssen; and Dr. Sharma is on the
Speakers Bureaus of Abbott Vascular, Angioscore,
other authors have reported that they have no re-
D, served as Guest Editor for this paper.
ry 16, 2015, accepted January 20, 2015.

ABBR EV I A T I ON S
AND ACRONYMS
CI = confidence interval
CSB = clinically
significant bleeding
DAPT = dual antiplatelet
therapy
DES = drug-eluting stent(s)
L-DAPT = longer dual
antiplatelet therapy
MI = myocardial infarction
OR = odds ratio
PCI = percutaneous
coronary intervention
RCT = randomized
controlled trial
S-DAPT = shorter dual
antiplatelet therapy
TIMI = Thrombolysis In
Myocardial Infarction
Giustino et al. J A C C V O L . - , N O . - , 2 0 1 5
DAPT After DES Implantation - , 2 0 1 5 :- –-
2
The pathobiological rationale of DAPT afterDES-PCI is based on the need to protect thestented vascular segment from the develop-ment of stent thrombosis while vascularhealing and progressive strut endotheliza-tion are ongoing (5). In addition, more pro-longed DAPT may confer protection fromatherothrombotic events occurring outsidethe stented segment throughout the coro-nary vasculature (6).
Prolonged DAPT after the recommendedperiod reduces stent-related and non–stent-related adverse ischemic events following PCI(7). Recently, the DAPT (Dual AntiplateletTherapy) trial demonstrated reduced rates ofstent thrombosis andmyocardial infarction (MI)with DAPT extended beyond 1 year after DESimplantation. However, this ischemic benefitwas paired with an increased risk in bleedingand possibly subsequent all-cause mortality.
Several randomized controlled trials (RCTs) haveattempted to address the question of what would bethe safest and shortest DAPT duration (ranging from3 to 6 months) after implantation of first- and second-generation DES. Due to the rarity of stent thrombosisevents, each trial had limited statistical power, andthe safest and shortest DAPT duration has not yetbeen reliably determined. Previously published meta-analyses of RCTs comparing short- versus long-termDAPT had limited statistical power and showed nosignificant differences in antithrombotic efficacybetween regimens, while longer dual antiplatelettherapy (L-DAPT) treatment was associated with anincreased risk for bleeding (8,9). With inclusion ofseveral recent large RCTs, the present meta-analysishas enhanced statistical power, and we thereforesought to assess the efficacy and safety of shorterdual antiplatelet therapy (S-DAPT) versus L-DAPTafter DES implantation, with particular focus on therisk of stent thrombosis with the use of current (sec-ond-generation) DES.
METHODS
Study groups were pre-specified as follows: S-DAPT,defined as the per-protocol minimum duration ofDAPT after DES implantation (after which, patients ofthis treatment arm were continued on aspirin alone);and L-DAPT, defined as the per-protocol period ofprolonged DAPT in each trial. In addition, RCTsevaluating durations of DAPT were classified asabbreviated-term DAPT studies (i.e., RCTs evaluatingS-DAPT duration of 3 or 6 months vs. longer duration)and extended-term DAPT studies (i.e., RCTs
evaluating DAPT discontinuation at 12 months vs.longer duration).
The pre-specified primary efficacy outcome wasthe incidence of definite or probable stent throm-bosis, as defined by using the criteria of the AcademicResearch Consortium (10). The main safety outcomewas clinically significant bleeding (CSB), defined asa bleeding event fulfilling the definition of: 1) minoror major Thrombolysis In Myocardial Infarction(TIMI) bleeding; 2) type 3 or 5 bleeding according tothe Bleeding Academic Research Consortium (BARC);3) Safety and Efficacy of Enoxaparin in PercutaneousCoronary Intervention Patients major bleeding; or 4)Global Use of Strategies to Open Occluded Arteriesmoderate or severe bleeding (11). Bleeding definitionsdetails are described in Online Table 1. Additionaloutcomes of interest were MI, stroke, cardiovasculardeath, and all-cause mortality. Outcomes were re-ported at the maximum time of follow-up available(Table 1). The study was performed according to theQuality of Reporting of Meta-Analysis statement (12).
MEDLINE, Scopus, the Cochrane Library, andInternet sources were searched for abstracts, manu-scripts, and conference reports; there were no lan-guage or date restrictions. All the RCTs comparingdifferent durations of DAPT after implantation of aDES were included in the meta-analysis. The finalsearch yielded 10 RCTs comparing various durationsof S-DAPT and L-DAPT after implantation of differenttypes of DES.
DATA EXTRACTION. Two investigators indepen-dently reviewed the studies and reported theresults in a structured dataset. Disparities betweeninvestigators regarding the inclusion of each trialwere resolved by consensus by a third independentinvestigator. Pre-specified data elements were ex-tracted from each trial; these elements includedS-DAPT and L-DAPT duration, maximum length offollow-up, sample size, baseline characteristics,outcome measures, and endpoints of interest. Eventsfrom each trial were recorded according to theintention-to-treat principle. Endpoint definitionsused in each trial are outlined in Online Table 2.
STATISTICAL ANALYSIS. The odds ratios (ORs)associated with S-DAPT versus L-DAPT from theabstracted data were estimated. Analyses werestratified according to DAPT trial type (abbreviated-term and extended-term DAPT studies). The averageeffects for the outcomes and 95% confidence intervals(CIs) were calculated by means of random effectsmodels according to the method of DerSimonianand Laird (13). The test for small-study effects wasconducted by using Harbord’s modified test.
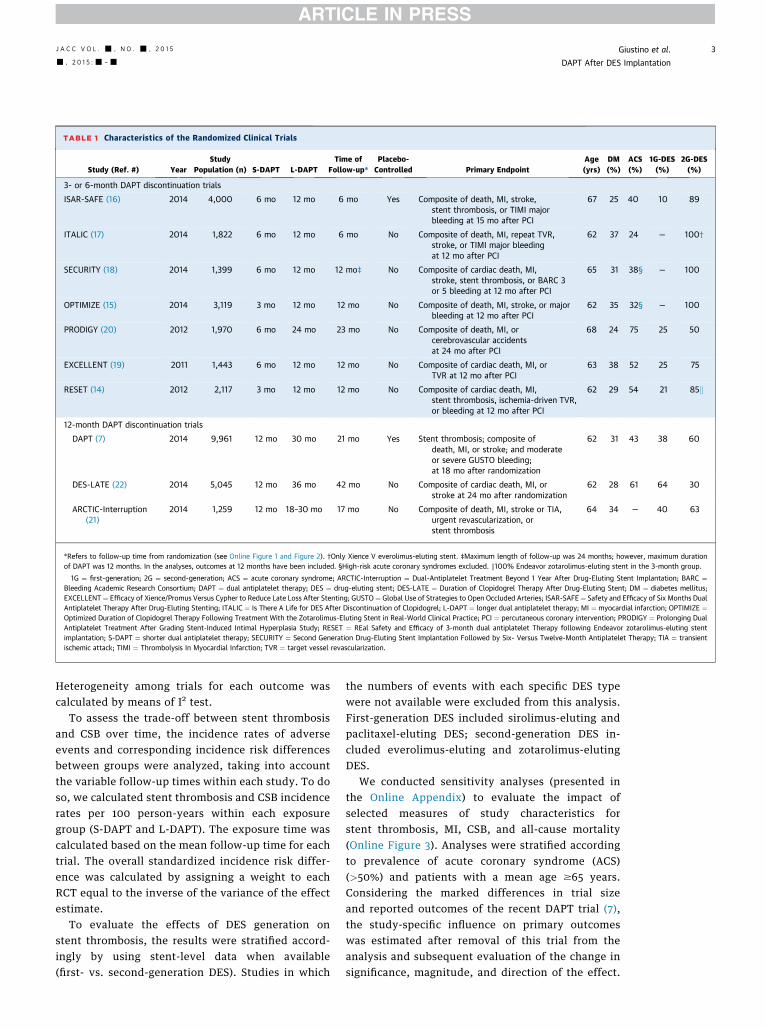
TABLE 1 Characteristics of the Randomized Clinical Trials
Study (Ref. #) YearStudy
Population (n) S-DAPT L-DAPTTime of
Follow-up*Placebo-Controlled Primary Endpoint
Age(yrs)
DM(%)
ACS(%)
1G-DES(%)
2G-DES(%)
3- or 6-month DAPT discontinuation trials
ISAR-SAFE (16) 2014 4,000 6 mo 12 mo 6 mo Yes Composite of death, MI, stroke,stent thrombosis, or TIMI majorbleeding at 15 mo after PCI
67 25 40 10 89
ITALIC (17) 2014 1,822 6 mo 12 mo 6 mo No Composite of death, MI, repeat TVR,stroke, or TIMI major bleedingat 12 mo after PCI
62 37 24 — 100†
SECURITY (18) 2014 1,399 6 mo 12 mo 12 mo‡ No Composite of cardiac death, MI,stroke, stent thrombosis, or BARC 3or 5 bleeding at 12 mo after PCI
65 31 38§ — 100
OPTIMIZE (15) 2014 3,119 3 mo 12 mo 12 mo No Composite of death, MI, stroke, or majorbleeding at 12 mo after PCI
62 35 32§ — 100
PRODIGY (20) 2012 1,970 6 mo 24 mo 23 mo No Composite of death, MI, orcerebrovascular accidentsat 24 mo after PCI
68 24 75 25 50
EXCELLENT (19) 2011 1,443 6 mo 12 mo 12 mo No Composite of cardiac death, MI, orTVR at 12 mo after PCI
63 38 52 25 75
RESET (14) 2012 2,117 3 mo 12 mo 12 mo No Composite of cardiac death, MI,stent thrombosis, ischemia-driven TVR,or bleeding at 12 mo after PCI
62 29 54 21 85k
12-month DAPT discontinuation trials
DAPT (7) 2014 9,961 12 mo 30 mo 21 mo Yes Stent thrombosis; composite ofdeath, MI, or stroke; and moderateor severe GUSTO bleeding;at 18 mo after randomization
62 31 43 38 60
DES-LATE (22) 2014 5,045 12 mo 36 mo 42 mo No Composite of cardiac death, MI, orstroke at 24 mo after randomization
62 28 61 64 30
ARCTIC-Interruption(21)
2014 1,259 12 mo 18–30 mo 17 mo No Composite of death, MI, stroke or TIA,urgent revascularization, orstent thrombosis
64 34 — 40 63
*Refers to follow-up time from randomization (see Online Figure 1 and Figure 2). †Only Xience V everolimus-eluting stent. ‡Maximum length of follow-up was 24 months; however, maximum durationof DAPT was 12 months. In the analyses, outcomes at 12 months have been included. §High-risk acute coronary syndromes excluded. k100% Endeavor zotarolimus-eluting stent in the 3-month group.
1G ¼ first-generation; 2G ¼ second-generation; ACS ¼ acute coronary syndrome; ARCTIC-Interruption ¼ Dual-Antiplatelet Treatment Beyond 1 Year After Drug-Eluting Stent Implantation; BARC ¼Bleeding Academic Research Consortium; DAPT ¼ dual antiplatelet therapy; DES ¼ drug-eluting stent; DES-LATE ¼ Duration of Clopidogrel Therapy After Drug-Eluting Stent; DM ¼ diabetes mellitus;EXCELLENT ¼ Efficacy of Xience/Promus Versus Cypher to Reduce Late Loss After Stenting; GUSTO¼ Global Use of Strategies to Open Occluded Arteries; ISAR-SAFE¼ Safety and Efficacy of Six Months DualAntiplatelet Therapy After Drug-Eluting Stenting; ITALIC ¼ Is There A Life for DES After Discontinuation of Clopidogrel; L-DAPT ¼ longer dual antiplatelet therapy; MI ¼ myocardial infarction; OPTIMIZE ¼Optimized Duration of Clopidogrel Therapy Following Treatment With the Zotarolimus-Eluting Stent in Real-World Clinical Practice; PCI ¼ percutaneous coronary intervention; PRODIGY ¼ Prolonging DualAntiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia Study; RESET ¼ REal Safety and Efficacy of 3-month dual antiplatelet Therapy following Endeavor zotarolimus-eluting stentimplantation; S-DAPT ¼ shorter dual antiplatelet therapy; SECURITY ¼ Second Generation Drug-Eluting Stent Implantation Followed by Six- Versus Twelve-Month Antiplatelet Therapy; TIA ¼ transientischemic attack; TIMI ¼ Thrombolysis In Myocardial Infarction; TVR ¼ target vessel revascularization.
J A C C V O L . - , N O . - , 2 0 1 5 Giustino et al.- , 2 0 1 5 :- –- DAPT After DES Implantation
3
Heterogeneity among trials for each outcome wascalculated by means of I2 test.
To assess the trade-off between stent thrombosisand CSB over time, the incidence rates of adverseevents and corresponding incidence risk differencesbetween groups were analyzed, taking into accountthe variable follow-up times within each study. To doso, we calculated stent thrombosis and CSB incidencerates per 100 person-years within each exposuregroup (S-DAPT and L-DAPT). The exposure time wascalculated based on the mean follow-up time for eachtrial. The overall standardized incidence risk differ-ence was calculated by assigning a weight to eachRCT equal to the inverse of the variance of the effectestimate.
To evaluate the effects of DES generation onstent thrombosis, the results were stratified accord-ingly by using stent-level data when available(first- vs. second-generation DES). Studies in which
the numbers of events with each specific DES typewere not available were excluded from this analysis.First-generation DES included sirolimus-eluting andpaclitaxel-eluting DES; second-generation DES in-cluded everolimus-eluting and zotarolimus-elutingDES.
We conducted sensitivity analyses (presented inthe Online Appendix) to evaluate the impact ofselected measures of study characteristics forstent thrombosis, MI, CSB, and all-cause mortality(Online Figure 3). Analyses were stratified accordingto prevalence of acute coronary syndrome (ACS)(>50%) and patients with a mean age $65 years.Considering the marked differences in trial sizeand reported outcomes of the recent DAPT trial (7),the study-specific influence on primary outcomeswas estimated after removal of this trial from theanalysis and subsequent evaluation of the change insignificance, magnitude, and direction of the effect.
FIGURE 1 Meta-An
7885 Citations IdeLiterature S
10 Randomized CInclud
After exclusion, 10 ra
Giustino et al. J A C C V O L . - , N O . - , 2 0 1 5
DAPT After DES Implantation - , 2 0 1 5 :- –-
4
All sensitivity analyses were conducted with both arandom effects model (primary analysis method) anda fixed effects model. Analyses were conducted byusing Stata version 12.0 (Stata Corp., College Station,Texas).
RESULTS
Of the 7,885 citations found, 10 RCTs (n ¼ 32,135)were identified (Figure 1); characteristics of these 10studies are summarized in Table 1. Additional detailsare available in Online Table 2 and Online Figure 1and Figure 2.
Two RCTs (RESET [REal Safety and Efficacy of3-month dual antiplatelet Therapy following Endeavorzotarolimus-eluting stent implantation] and OPTI-MIZE [Optimized Duration of Clopidogrel TherapyFollowing Treatment With the Zotarolimus-ElutingStent in Real-World Clinical Practice]) evaluated 3months versus 12 months of DAPT (14,15). In theOPTIMIZE trial, second-generation DES were used in100% of patients in both randomization arms. In theRESET trial, second-generation DESwere used in 100%of patients in the 3-month arm and in 70% in the 12-month arm. In these 2 trials, the average age was 62years, the prevalence of diabetes mellitus was 32%,and 43% had ACS.
Five RCTs evaluated a 6-month versus either a12-month DAPT regimen (ISAR-SAFE [Safety andEfficacy of Six Months Dual Antiplatelet Therapy Af-ter Drug-Eluting Stenting], ITALIC [Is There A Life forDES After Discontinuation of Clopidogrel], SECURITY[Second Generation Drug-Eluting Stent Implantation
alysis Flow Diagram
1 Randomized Clinical TrialIdentified from Internet
sources
7876 Citations Excludedafter screening of
study design
ntified fromearch
linical Trialsed
ndomized controlled (n ¼ 32,135) were included in the meta-analysis.
Followed by Six- Versus Twelve-Month AntiplateletTherapy], and EXCELLENT [Efficacy of Xience/Promus Versus Cypher to Reduce Late Loss AfterStenting]) or a 24-month DAPT regimen (PRODIGY[Prolonging Dual Antiplatelet Treatment AfterGrading Stent-Induced Intimal Hyperplasia Study])(16–20). In the recent ITALIC and SECURITY trials,second-generation DES were used in 100% of patientsin both randomization arms. In the EXCELLENT andISAR-SAFE trials, second-generation DES were usedin >70% of patients. Finally, in the PRODIGY trial,second-generation DES were implanted in 50% ofpatients, while the remainder received bare-metalstents or first-generation DES. Across these 5 trials,the average patient age was 65 years, the prevalenceof diabetes mellitus was 31%, and 46% had ACS.
Three RCTs (DAPT, DES-LATE [Duration ofClopidogrel Therapy After Drug-Eluting Stent], andARCTIC-Interruption [Dual-Antiplatelet TreatmentBeyond 1 Year After Drug-Eluting Stent Implanta-tion]) explored the efficacy and safety of prolongedDAPT beyond 12 months after the original DES im-plantation (7,21,22). Second-generation DES wereused in 30% of patients in the DES-LATE trial and inz60% of the population in the DAPT and ARCTIC-Interruption trials. Therefore, the mean second-generation DES use across the studies was 51%. Themean patient age among these 3 RCTs was 63 years,the prevalence of diabetes mellitus was 31%, and 52%had ACS. The mean weighted follow-up time amongall 10 RCTs was 19.6 months; the mean weightedexposure time to antiplatelet therapy within theS-DAPT and L-DAPT groups was 8.5 and 23.2 months,respectively. All the endpoints of interest in each ofthe trials were independently adjudicated by aClinical Event Committee (Online Table 3).STENT THROMBOSIS. Rates of stent thrombosis werereported in all trials. The overall frequency of stentthrombosis in the S-DAPT group was 0.9% (143 of15,997) compared with 0.5% (80 of 16,138) in theL-DAPT group. The combined OR for stent thrombosiswith an S-DAPT regimen versus an L-DAPT regimenwas 1.71 (95% CI 1.26 to 2.32; p ¼ 0.001) (Figure 2).The magnitude of the effect was attenuated inabbreviated-term DAPT studies (OR 1.20 [95% CI 0.77to 1.88]) compared with extended-term DAPT studies(OR 2.22 [95% CI 1.55 to 3.17]; p for interaction ¼0.044). There was no evidence of statistical hetero-geneity among studies (p heterogeneity ¼ 0.387).The test for small-studies effect was not significant(p ¼ 0.905).
Rates of stent thrombosis with second-generationDES were reported in 6 RCTs (7,15,17–19,23); stentthrombosis rates with first-generation DES were
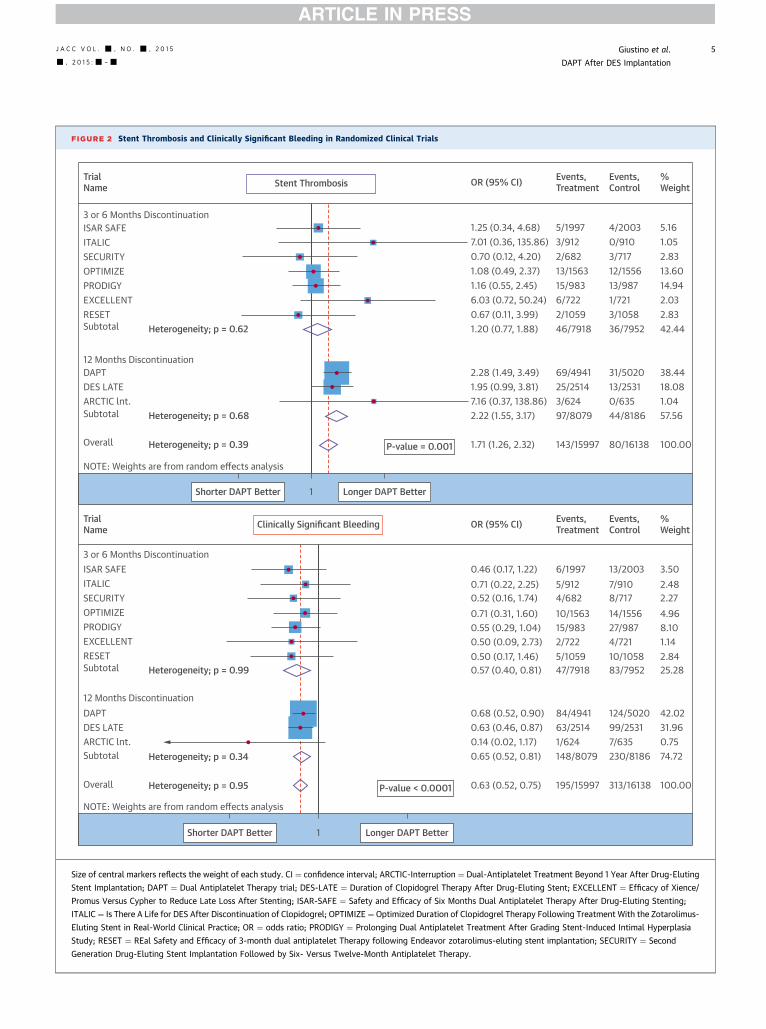
FIGURE 2 Stent Thrombosis and Clinically Significant Bleeding in Randomized Clinical Trials
1.25 (0.34, 4.68)
Stent Thrombosis
5/1997 4/2003 5.161.052.8313.6014.942.032.8342.44
38.4418.081.0457.56
100.00
0/9103/71712/155613/9871/7213/105836/7952
31/502013/25310/63544/8186
80/16138
3/9122/68213/156315/9836/7222/105946/7918
69/494125/25143/62497/8079
143/15997
6/1997 13/2003 3.502.482.274.968.101.142.8425.28
42.0231.960.7574.72
100.00
7/9108/71714/155627/9874/72110/105883/7952
124/502099/25317/635230/8186
313/16138
5/9124/68210/156315/9832/7225/105947/7918
84/494163/25141/624148/8079
195/15997
7.01 (0.36, 135.86)0.70 (0.12, 4.20)1.08 (0.49, 2.37)1.16 (0.55, 2.45)6.03 (0.72, 50.24)0.67 (0.11, 3.99)1.20 (0.77, 1.88)
2.28 (1.49, 3.49)1.95 (0.99, 3.81)7.16 (0.37, 138.86)2.22 (1.55, 3.17)
1.71 (1.26, 2.32)
0.46 (0.17, 1.22)
Clinically Significant Bleeding
0.71 (0.22, 2.25)0.52 (0.16, 1.74)0.71 (0.31, 1.60)0.55 (0.29, 1.04)0.50 (0.09, 2.73)0.50 (0.17, 1.46)0.57 (0.40, 0.81)
0.68 (0.52, 0.90)0.63 (0.46, 0.87)0.14 (0.02, 1.17)0.65 (0.52, 0.81)
0.63 (0.52, 0.75)
P-value = 0.001
P-value < 0.0001
12 Months DiscontinuationDAPTDES LATEARCTIC lnt.
ARCTIC lnt.
Subtotal Heterogeneity; p = 0.68
Heterogeneity; p = 0.39Overall
NOTE: Weights are from random effects analysis
TrialName
TrialName
3 or 6 Months Discontinuation
ITALICSECURITYOPTIMIZEPRODIGYEXCELLENTRESETSubtotal Heterogeneity; p = 0.99
12 Months DiscontinuationDAPT
3 or 6 Months DiscontinuationISAR SAFE
ISAR SAFE
ITALICSECURITYOPTIMIZEPRODIGYEXCELLENTRESETSubtotal Heterogeneity; p = 0.62
DES LATE
Subtotal Heterogeneity; p = 0.34
Overall Heterogeneity; p = 0.95
NOTE: Weights are from random effects analysis
OR (95% CI) Events, Treatment
Events, Control
%Weight
OR (95% CI) Events, Treatment
Events, Control
%Weight
Shorter DAPT Better Longer DAPT Better1
Shorter DAPT Better Longer DAPT Better1
Size of central markers reflects the weight of each study. CI ¼ confidence interval; ARCTIC-Interruption ¼ Dual-Antiplatelet Treatment Beyond 1 Year After Drug-Eluting
Stent Implantation; DAPT ¼ Dual Antiplatelet Therapy trial; DES-LATE ¼ Duration of Clopidogrel Therapy After Drug-Eluting Stent; EXCELLENT ¼ Efficacy of Xience/
Promus Versus Cypher to Reduce Late Loss After Stenting; ISAR-SAFE ¼ Safety and Efficacy of Six Months Dual Antiplatelet Therapy After Drug-Eluting Stenting;
ITALIC ¼ Is There A Life for DES After Discontinuation of Clopidogrel; OPTIMIZE ¼ Optimized Duration of Clopidogrel Therapy Following Treatment With the Zotarolimus-
Eluting Stent in Real-World Clinical Practice; OR ¼ odds ratio; PRODIGY ¼ Prolonging Dual Antiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia
Study; RESET ¼ REal Safety and Efficacy of 3-month dual antiplatelet Therapy following Endeavor zotarolimus-eluting stent implantation; SECURITY ¼ Second
Generation Drug-Eluting Stent Implantation Followed by Six- Versus Twelve-Month Antiplatelet Therapy.
J A C C V O L . - , N O . - , 2 0 1 5 Giustino et al.- , 2 0 1 5 :- –- DAPT After DES Implantation
5
Giustino et al. J A C C V O L . - , N O . - , 2 0 1 5
DAPT After DES Implantation - , 2 0 1 5 :- –-
6
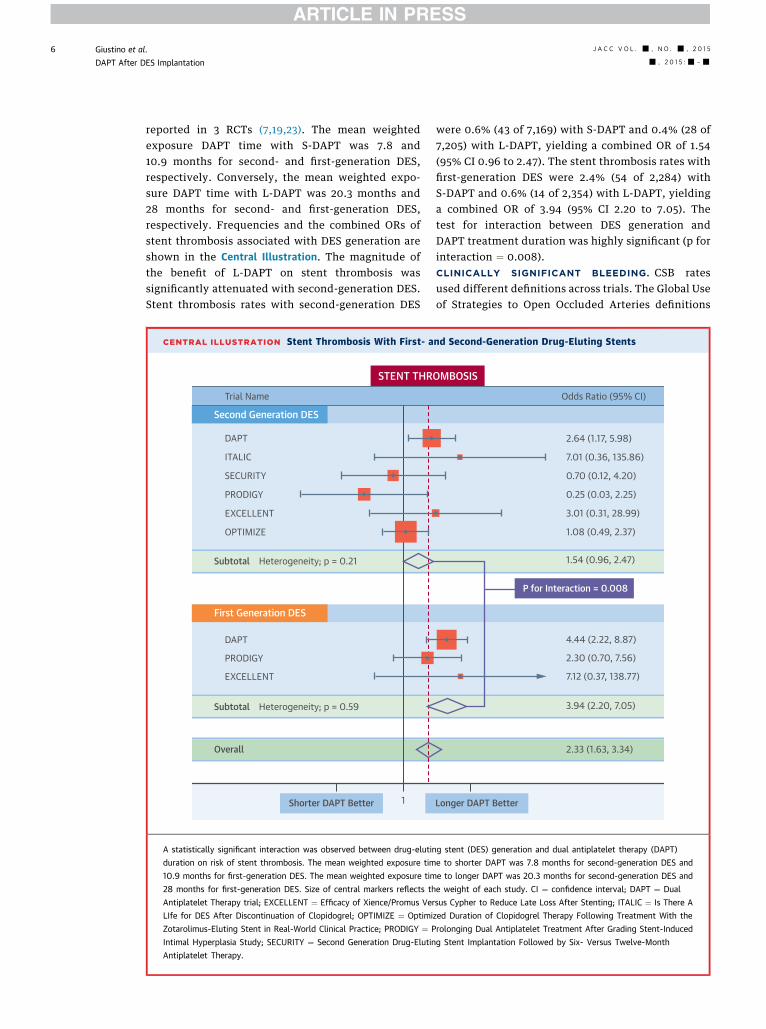
reported in 3 RCTs (7,19,23). The mean weightedexposure DAPT time with S-DAPT was 7.8 and10.9 months for second- and first-generation DES,respectively. Conversely, the mean weighted expo-sure DAPT time with L-DAPT was 20.3 months and28 months for second- and first-generation DES,respectively. Frequencies and the combined ORs ofstent thrombosis associated with DES generation areshown in the Central Illustration. The magnitude ofthe benefit of L-DAPT on stent thrombosis wassignificantly attenuated with second-generation DES.Stent thrombosis rates with second-generation DES
CENTRAL ILLUSTRATION Stent Thrombosis With First- a
DAPT
Shorter DAPT Better 1
STENT THR
SECURITY
PRODIGY
DAPT
Subtotal Heterogeneity; p = 0.59
Overall
Second Generation DES
First Generation DES
ITALIC
Trial Name
Subtotal Heterogeneity; p = 0.21
EXCELLENT
OPTIMIZE
PRODIGY
EXCELLENT
A statistically significant interaction was observed between drug-elutin
duration on risk of stent thrombosis. The mean weighted exposure tim
10.9 months for first-generation DES. The mean weighted exposure tim
28 months for first-generation DES. Size of central markers reflects th
Antiplatelet Therapy trial; EXCELLENT ¼ Efficacy of Xience/Promus Ver
LIfe for DES After Discontinuation of Clopidogrel; OPTIMIZE ¼ Optimi
Zotarolimus-Eluting Stent in Real-World Clinical Practice; PRODIGY ¼ P
Intimal Hyperplasia Study; SECURITY ¼ Second Generation Drug-Elutin
Antiplatelet Therapy.
were 0.6% (43 of 7,169) with S-DAPT and 0.4% (28 of7,205) with L-DAPT, yielding a combined OR of 1.54(95% CI 0.96 to 2.47). The stent thrombosis rates withfirst-generation DES were 2.4% (54 of 2,284) withS-DAPT and 0.6% (14 of 2,354) with L-DAPT, yieldinga combined OR of 3.94 (95% CI 2.20 to 7.05). Thetest for interaction between DES generation andDAPT treatment duration was highly significant (p forinteraction ¼ 0.008).CLINICALLY SIGNIFICANT BLEEDING. CSB ratesused different definitions across trials. The Global Useof Strategies to Open Occluded Arteries definitions
nd Second-Generation Drug-Eluting Stents
Longer DAPT Better
OMBOSIS
Odds Ratio (95% CI)
P for Interaction = 0.008
2.64 (1.17, 5.98)
7.01 (0.36, 135.86)
0.70 (0.12, 4.20)
0.25 (0.03, 2.25)
3.01 (0.31, 28.99)
1.08 (0.49, 2.37)
1.54 (0.96, 2.47)
4.44 (2.22, 8.87)
2.30 (0.70, 7.56)
7.12 (0.37, 138.77)
3.94 (2.20, 7.05)
2.33 (1.63, 3.34)
g stent (DES) generation and dual antiplatelet therapy (DAPT)
e to shorter DAPT was 7.8 months for second-generation DES and
e to longer DAPT was 20.3 months for second-generation DES and
e weight of each study. CI ¼ confidence interval; DAPT ¼ Dual
sus Cypher to Reduce Late Loss After Stenting; ITALIC ¼ Is There A
zed Duration of Clopidogrel Therapy Following Treatment With the
rolonging Dual Antiplatelet Treatment After Grading Stent-Induced
g Stent Implantation Followed by Six- Versus Twelve-Month
J A C C V O L . - , N O . - , 2 0 1 5 Giustino et al.- , 2 0 1 5 :- –- DAPT After DES Implantation
7
were used in the DAPT trial; a BARC 3 or 5 bleedingdefinition was used to extract CSB rates from theSECURITY trial; and a TIMI major or minor bleedingdefinition was used in the ISAR-SAFE, PRODIGY,RESET, and ITALIC trials. In the DES-LATE andEXCELLENT trials, the only available bleeding ratewas major TIMI type. The incidence of CSB acrossall RCTs was 1.2% in the S-DAPT group (195 of15,997) and 1.9% in the L-DAPT group (313 of 16,138),yielding a combined OR (Figure 2) with S-DAPTversus L-DAPT of 0.63 (95% CI: 0.52 to 0.75;p < 0.001). Results were consistent across abbrevi-ated- and extended-term DAPT studies. There was noevidence of statistical heterogeneity among studies(p heterogeneity ¼ 0.953).
TRADE-OFF BETWEEN STENT THROMBOSIS AND
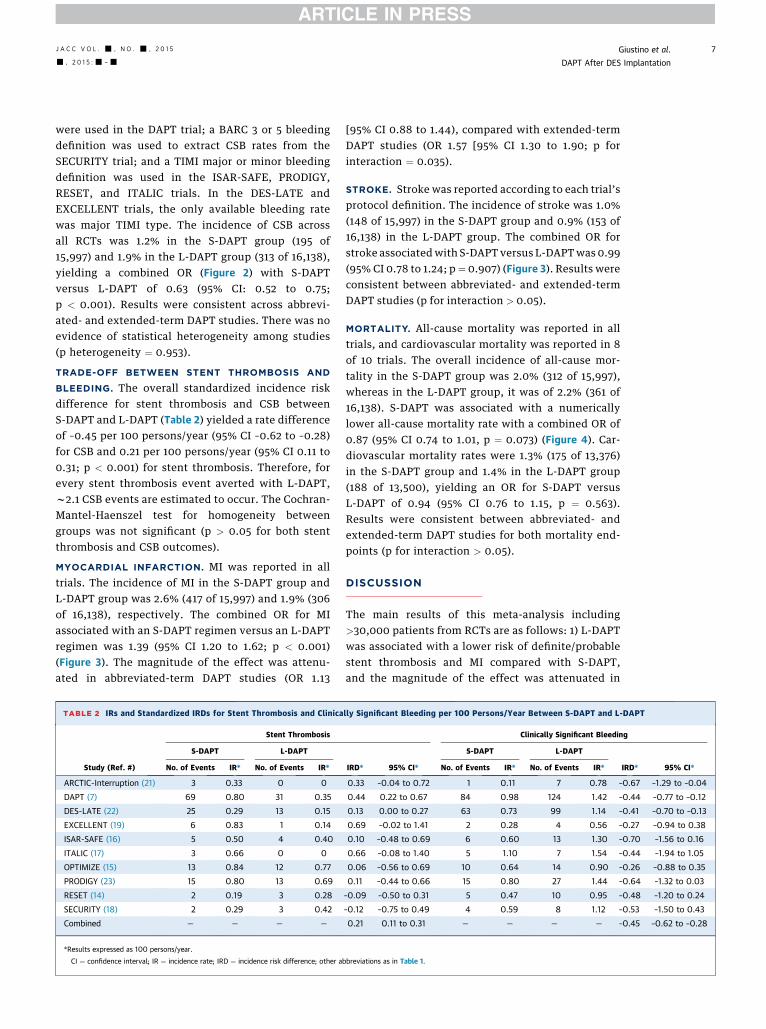
BLEEDING. The overall standardized incidence riskdifference for stent thrombosis and CSB betweenS-DAPT and L-DAPT (Table 2) yielded a rate differenceof –0.45 per 100 persons/year (95% CI –0.62 to –0.28)for CSB and 0.21 per 100 persons/year (95% CI 0.11 to0.31; p < 0.001) for stent thrombosis. Therefore, forevery stent thrombosis event averted with L-DAPT,w2.1 CSB events are estimated to occur. The Cochran-Mantel-Haenszel test for homogeneity betweengroups was not significant (p > 0.05 for both stentthrombosis and CSB outcomes).
MYOCARDIAL INFARCTION. MI was reported in alltrials. The incidence of MI in the S-DAPT group andL-DAPT group was 2.6% (417 of 15,997) and 1.9% (306of 16,138), respectively. The combined OR for MIassociated with an S-DAPT regimen versus an L-DAPTregimen was 1.39 (95% CI 1.20 to 1.62; p < 0.001)(Figure 3). The magnitude of the effect was attenu-ated in abbreviated-term DAPT studies (OR 1.13
TABLE 2 IRs and Standardized IRDs for Stent Thrombosis and Clinica
Study (Ref. #)
Stent Thrombosis
S-DAPT L-DAPT
No. of Events IR* No. of Events IR*
ARCTIC-Interruption (21) 3 0.33 0 0
DAPT (7) 69 0.80 31 0.35
DES-LATE (22) 25 0.29 13 0.15
EXCELLENT (19) 6 0.83 1 0.14
ISAR-SAFE (16) 5 0.50 4 0.40
ITALIC (17) 3 0.66 0 0
OPTIMIZE (15) 13 0.84 12 0.77
PRODIGY (23) 15 0.80 13 0.69
RESET (14) 2 0.19 3 0.28
SECURITY (18) 2 0.29 3 0.42
Combined — — — —
*Results expressed as 100 persons/year.
CI ¼ confidence interval; IR ¼ incidence rate; IRD ¼ incidence risk difference; other a
[95% CI 0.88 to 1.44), compared with extended-termDAPT studies (OR 1.57 [95% CI 1.30 to 1.90; p forinteraction ¼ 0.035).
STROKE. Stroke was reported according to each trial’sprotocol definition. The incidence of stroke was 1.0%(148 of 15,997) in the S-DAPT group and 0.9% (153 of16,138) in the L-DAPT group. The combined OR forstroke associatedwith S-DAPT versus L-DAPTwas 0.99(95% CI 0.78 to 1.24; p ¼ 0.907) (Figure 3). Results wereconsistent between abbreviated- and extended-termDAPT studies (p for interaction > 0.05).
MORTALITY. All-cause mortality was reported in alltrials, and cardiovascular mortality was reported in 8of 10 trials. The overall incidence of all-cause mor-tality in the S-DAPT group was 2.0% (312 of 15,997),whereas in the L-DAPT group, it was of 2.2% (361 of16,138). S-DAPT was associated with a numericallylower all-cause mortality rate with a combined OR of0.87 (95% CI 0.74 to 1.01, p ¼ 0.073) (Figure 4). Car-diovascular mortality rates were 1.3% (175 of 13,376)in the S-DAPT group and 1.4% in the L-DAPT group(188 of 13,500), yielding an OR for S-DAPT versusL-DAPT of 0.94 (95% CI 0.76 to 1.15, p ¼ 0.563).Results were consistent between abbreviated- andextended-term DAPT studies for both mortality end-points (p for interaction > 0.05).
DISCUSSION
The main results of this meta-analysis including>30,000 patients from RCTs are as follows: 1) L-DAPTwas associated with a lower risk of definite/probablestent thrombosis and MI compared with S-DAPT,and the magnitude of the effect was attenuated in
lly Significant Bleeding per 100 Persons/Year Between S-DAPT and L-DAPT
Clinically Significant Bleeding
IRD* 95% CI*
S-DAPT L-DAPT
IRD* 95% CI*No. of Events IR* No. of Events IR*
0.33 –0.04 to 0.72 1 0.11 7 0.78 –0.67 –1.29 to –0.04
0.44 0.22 to 0.67 84 0.98 124 1.42 –0.44 –0.77 to –0.12
0.13 0.00 to 0.27 63 0.73 99 1.14 –0.41 –0.70 to –0.13
0.69 –0.02 to 1.41 2 0.28 4 0.56 –0.27 –0.94 to 0.38
0.10 –0.48 to 0.69 6 0.60 13 1.30 –0.70 –1.56 to 0.16
0.66 –0.08 to 1.40 5 1.10 7 1.54 –0.44 –1.94 to 1.05
0.06 –0.56 to 0.69 10 0.64 14 0.90 –0.26 –0.88 to 0.35
0.11 –0.44 to 0.66 15 0.80 27 1.44 –0.64 –1.32 to 0.03
–0.09 –0.50 to 0.31 5 0.47 10 0.95 –0.48 –1.20 to 0.24
–0.12 –0.75 to 0.49 4 0.59 8 1.12 –0.53 –1.50 to 0.43
0.21 0.11 to 0.31 — — — — –0.45 –0.62 to –0.28
bbreviations as in Table 1.
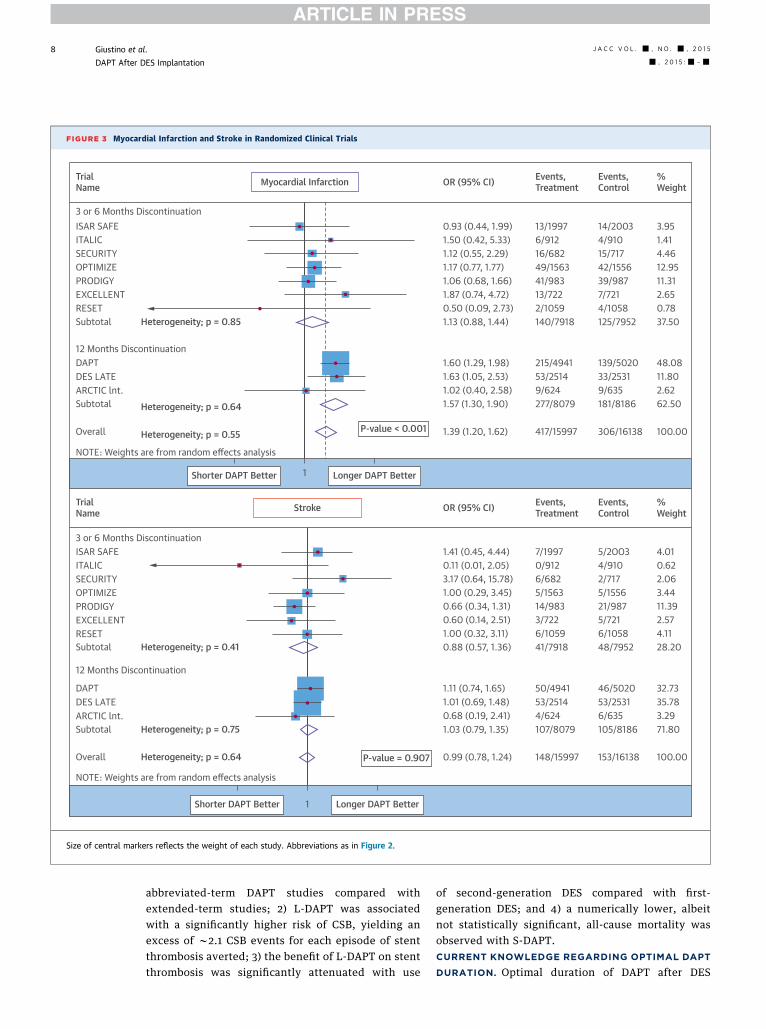
FIGURE 3 Myocardial Infarction and Stroke in Randomized Clinical Trials
0.93 (0.44, 1.99)1.50 (0.42, 5.33)1.12 (0.55, 2.29)1.17 (0.77, 1.77)1.06 (0.68, 1.66)1.87 (0.74, 4.72)0.50 (0.09, 2.73)1.13 (0.88, 1.44)
1.60 (1.29, 1.98)1.63 (1.05, 2.53)1.02 (0.40, 2.58)1.57 (1.30, 1.90)
1.39 (1.20, 1.62) 417/15997
277/80799/62453/2514215/4941
140/79182/105913/72241/98349/1563
13/19976/91216/682
14/20034/91015/71742/155639/9877/7214/1058125/7952
139/502033/25319/635181/8186
306/16138
3.951.414.4612.9511.312.650.7837.50
48.0811.802.6262.50
100.00
1.41 (0.45, 4.44) 7/19970.11 (0.01, 2.05)3.17 (0.64, 15.78)1.00 (0.29, 3.45)0.66 (0.34, 1.31)0.60 (0.14, 2.51)1.00 (0.32, 3.11)0.88 (0.57, 1.36)
1.11 (0.74, 1.65)1.01 (0.69, 1.48)0.68 (0.19, 2.41)1.03 (0.79, 1.35)
0.99 (0.78, 1.24)
0/9126/6825/156314/9833/7226/105941/7918
50/494153/25144/624107/8079
148/15997
5/2OO34/910
4.01
2.063.4411.392.574.1128.20
32.7335.783.2971.80
100.00
2/7175/155621/9875/7216/105848/7952
46/502053/25316/635105/8186
153/16138
0.62
Myocardial Infarction
Stroke
P-value < 0.001
P-value = 0.907
12 Months DiscontinuationDAPTDES LATEARCTIC lnt.
ARCTIC lnt.
Subtotal Heterogeneity; p = 0.64
Heterogeneity; p = 0.55Overall
NOTE: Weights are from random effects analysis
TrialName
TrialName
3 or 6 Months Discontinuation
ITALICSECURITYOPTIMIZEPRODIGYEXCELLENTRESETSubtotal Heterogeneity; p = 0.41
12 Months Discontinuation
DAPT
3 or 6 Months DiscontinuationISAR SAFE
ISAR SAFE
ITALICSECURITYOPTIMIZEPRODIGYEXCELLENTRESETSubtotal Heterogeneity; p = 0.85
DES LATE
Subtotal Heterogeneity; p = 0.75
Overall Heterogeneity; p = 0.64
NOTE: Weights are from random effects analysis
Shorter DAPT Better Longer DAPT Better
Shorter DAPT Better Longer DAPT Better
1
1
OR (95% CI) Events, Treatment
Events, Control
%Weight
OR (95% CI) Events, Treatment
Events, Control
%Weight
Size of central markers reflects the weight of each study. Abbreviations as in Figure 2.
Giustino et al. J A C C V O L . - , N O . - , 2 0 1 5
DAPT After DES Implantation - , 2 0 1 5 :- –-
8
abbreviated-term DAPT studies compared withextended-term studies; 2) L-DAPT was associatedwith a significantly higher risk of CSB, yielding anexcess of w2.1 CSB events for each episode of stentthrombosis averted; 3) the benefit of L-DAPT on stentthrombosis was significantly attenuated with use
of second-generation DES compared with first-generation DES; and 4) a numerically lower, albeitnot statistically significant, all-cause mortality wasobserved with S-DAPT.CURRENT KNOWLEDGE REGARDING OPTIMAL DAPT
DURATION. Optimal duration of DAPT after DES
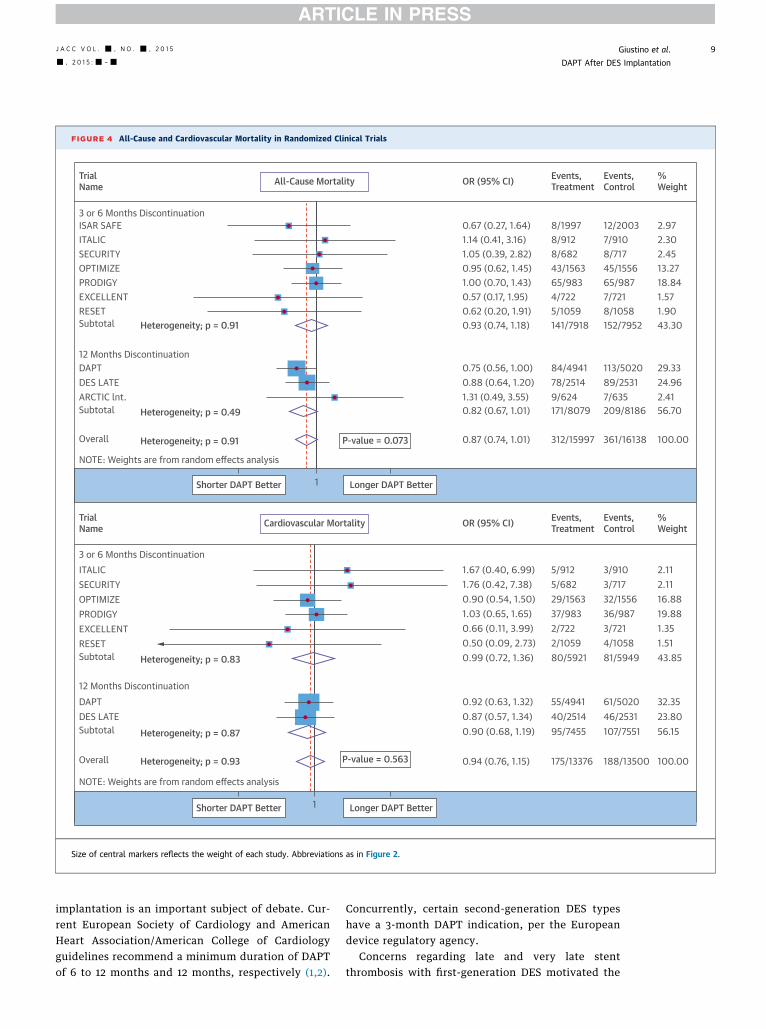
FIGURE 4 All-Cause and Cardiovascular Mortality in Randomized Clinical Trials
12 Months DiscontinuationDAPTDES LATEARCTIC lnt.Subtotal Heterogeneity; p = 0.49
Overall Heterogeneity; p = 0.91
NOTE: Weights are from random effects analysis
TrialName
TrialName
3 or 6 Months DiscontinuationITALICSECURITYOPTIMIZEPRODIGYEXCELLENTRESETSubtotal Heterogeneity; p = 0.83
12 Months DiscontinuationDAPT
3 or 6 Months DiscontinuationISAR SAFEITALICSECURITYOPTIMIZEPRODIGYEXCELLENTRESETSubtotal Heterogeneity; p = 0.91
DES LATESubtotal Heterogeneity; p = 0.87
Overall Heterogeneity; p = 0.93
NOTE: Weights are from random effects analysis
Shorter DAPT Better Longer DAPT Better
Shorter DAPT Better Longer DAPT Better
1
1
0.67 (0.27, 1.64)1.14 (0.41, 3.16)1.05 (0.39, 2.82)0.95 (0.62, 1.45)1.00 (0.70, 1.43)0.57 (0.17, 1.95)0.62 (0.20, 1.91)0.93 (0.74, 1.18)
0.75 (0.56, 1.00)0.88 (0.64, 1.20)1.31 (0.49, 3.55)0.82 (0.67, 1.01)
0.87 (0.74, 1.01)
2.972.302.4513.2718.841.571.9043.30
29.3324.962.4156.70
100.00
1.67 (0.40, 6.99)1.76 (0.42, 7.38)0.90 (0.54, 1.50)1.03 (0.65, 1.65)0.66 (0.11, 3.99)0.50 (0.09, 2.73)0.99 (0.72, 1.36)
0.92 (0.63, 1.32)0.87 (0.57, 1.34)0.90 (0.68, 1.19)
0.94 (0.76, 1.15)
2.112.1116.8819.881.351.5143.85
32.3523.8056.15
100.00P-value = 0.563
Cardiovascular Mortality OR (95% CI) Events, Treatment
Events, Control
%Weight
OR (95% CI) Events, Treatment
Events, Control
%Weight
P-value = 0.073
All-Cause Mortality
8/9128/1997
8/68243/156365/9834/7225/1059141/7918
84/494178/25149/624171/8079
312/15997
7/91012/2003
8/71745/155665/9877/7218/1058152/7952
113/502089/25317/635209/8186
361/16138
3/9103/71732/155636/9873/7214/105881/5949
5/9125/68229/156337/9832/7222/105980/5921
55/494140/251495/7455
61/502046/2531107/7551
175/13376 188/13500
Size of central markers reflects the weight of each study. Abbreviations as in Figure 2.
J A C C V O L . - , N O . - , 2 0 1 5 Giustino et al.- , 2 0 1 5 :- –- DAPT After DES Implantation
9
implantation is an important subject of debate. Cur-rent European Society of Cardiology and AmericanHeart Association/American College of Cardiologyguidelines recommend a minimum duration of DAPTof 6 to 12 months and 12 months, respectively (1,2).
Concurrently, certain second-generation DES typeshave a 3-month DAPT indication, per the Europeandevice regulatory agency.
Concerns regarding late and very late stentthrombosis with first-generation DES motivated the
Giustino et al. J A C C V O L . - , N O . - , 2 0 1 5
DAPT After DES Implantation - , 2 0 1 5 :- –-
10
scientific community to investigate the potentiallybeneficial role of long-term DAPT. Several observa-tional studies and registries found a strong andindependent association between DAPT cessation andstent thrombosis (24,25), particularly when cessationoccurs early after DES implantation (3). Importantly,the concerns regarding stent thrombosis after stop-ping DAPT led to the development of newer genera-tion DES, with improved vascular healing andre-endothelialization properties (26–28). Permanentpolymer DES and bioresorbable polymer DES haveshown improved safety compared with initial first-generation DES (29,30).
The improved safety of current-generation DESconstituted the basis to evaluate abbreviated regi-mens of DAPT duration after PCI. Before the presentmeta-analysis, 7 trials evaluated the safety and effi-cacy of interrupted DAPT at 3 or 6 months comparedwith prolonged DAPT at 12 or 24 months (14–20).Interestingly, a significant increased hazard forischemic events with reduced DAPT duration didnot occur in any of these trials. Conversely, an in-creased risk for bleeding events was observed in thePRODIGY trial that compared 6 versus 24 months ofDAPT after the implantation of various stent types(20). Therefore, in all of these RCTs, S-DAPT seemedto be noninferior to a regimen of L-DAPT. However,several issues must be considered when interpretingthese results. First, most of these trials were under-powered to detect differences in hard endpointsbecause of study design issues, slow enrollment, andlower-than-expected event rates. Second, except forthe ISAR-SAFE trial, all of these studies were open-label (not placebo controlled). Third, primaryendpoint definitions were heterogeneous, makingcomparisons between trials limited and somewhatinappropriate when ischemic and bleeding eventswere included in the composite primary endpointdefinition. Fourth, in some of these studies, non-inferiority was demonstrated for margins fixed asabsolute risk difference but not relative risk differ-ence (EXCELLENT and OPTIMIZE); because theobserved active control rate was lower than ex-pected, fixing the margin in terms of absolute riskdifference may have biased the results favoringnoninferiority.
The recently published DAPT trial randomized9,961 event-free patients after the first year followingDES-PCI to either continue with DAPT for another 18months or to stop the thienopyridine (7). This trialchanged the perspective on L-DAPT by demonstratinga significant long-term benefit in stent-related andnon–stent-related thrombotic events with the pro-longed DAPT regimen. Nevertheless, the ischemic
benefit with L-DAPT was paired with an increased riskin major bleeding and a significantly higher non-cardiovascular mortality. However, a recent meta-analysis of RCTs evaluating extended DAPT indifferent clinical scenarios (including PCI, atrialfibrillation, stroke, and vascular surgery) did notsupport an association between all-cause, non-cardiovascular, or cardiovascular mortality and alonger DAPT regimen (31).
CLINICAL IMPLICATIONS. The results of the presentmeta-analysis, which included all of the most recenttrials evaluating optimal DAPT duration after PCIwith DES, offer useful insights regarding the impactof extended DAPT on clinical outcomes and on theunfavorable role of first-generation DES as animportant ischemic risk modifier. According to ourresults, L-DAPT is associated with a significantreduction in late stent thrombosis and MI risk inpatients undergoing PCI with DES implantation.Importantly, after exclusion of the DAPT trial fromthe analysis (the sensitivity analysis is presented inthe Online Appendix), the association betweenS-DAPT and stent thrombosis was of only borderlinesignificance (numerically higher, without reachingstatistical significance) according to the morerigorous random effects model approach. Thisfinding suggests that a thrombotic benefit withDAPT might become evident with longer exposureto treatment. However, L-DAPT is a therapeuticstrategy not exempt from risk, particularly in rela-tion to bleeding. In fact, the thrombotic benefit ofL-DAPT was counterbalanced by an increase inbleeding risk that was consistent across the exam-ined trials. Interestingly, the risk reduction in stentthrombosis and MI with L-DAPT did not translateinto an all-cause or cardiovascular mortality benefit.Conversely, L-DAPT was associated with a numeri-cally higher all-cause mortality (without statis-tical significance) compared with S-DAPT. Thevalidity and consistency of this finding remaincontroversial.
The clinical message of the present meta-analysisis that the trade-off between ischemic and bleedingevents with L-DAPT is a matter of concern and shouldbe carefully evaluated when the decision to continueDAPT after a recommended period is considered. Wefound that for each stent thrombosis event averted byprolonging DAPT, an excess of 2.1 CSB events wouldbe expected. Moreover, the risk of late and very latestent thrombosis with S-DAPT is notably increasedin patients receiving a first-generation DES, which areused rarely (if at all) at the present time. Assuming acomparable bleeding risk across stent generations
J A C C V O L . - , N O . - , 2 0 1 5 Giustino et al.- , 2 0 1 5 :- –- DAPT After DES Implantation
11
with provision of prolonged DAPT, our findings sug-gest that the risk/benefit ratio for extending DAPT hasan important variation according to type of DES used.In the current cardiology practice, only the results ofsecond-generation DES are clinically applicable.Accordingly, the prevention of a single episode oflate stent thrombosis will require exposing a largernumber of patients with a second-generation DESto potentially serious bleeding harm (CentralIllustration). This difference is clinically relevantwhen the decision to prolong DAPT after the initialrecommended period is being considered. The inter-action between DAPT duration and DES generationwas previously described by Camenzind et al. (32); inthe absence of DAPT prolonged beyond 1 year, stentthrombosis at 3 years was significantly lower with asecond-generation DES, whereas no differencesbetween first- and second-generation DES wereobserved with extended-term DAPT treatment.
The counterbalancing influences of preventingthrombosis while simultaneously increasing bleedingrisk may account for the lack of mortality benefit (andpossibly the suggestion of increased all-cause mor-tality) observed with extended DAPT duration.Beyond risk of stent thrombosis, it would still beacceptable to use an extended DAPT regimen; thegoal would be to offer a broader coronary athero-thrombotic benefit in terms of MI protection (oftenunrelated to a stent thrombosis event) in patientswho are tolerating the initially recommended DAPTduration well and have been judged to be at moderateor high ischemic risk along with having a low bleedinghazard. Therefore, the optimal duration of DAPT withcurrent-generation DES outside ACS remains unde-fined, and the timing of interruption of the thieno-pyridine can be as short as 3 or 6 months after stentimplantation. Finally, considering the continuousdevice and pharmacology evolution, further trials areneeded to evaluate optimal duration with use of thecurrent- and forthcoming-generation DES and thehigh-potency antiplatelet drugs.
STUDY LIMITATIONS. The main limitation of thepresent study is the lack of patient-level data, whichdoes not allow us to evaluate ischemic and net com-posite endpoints or perform time-to-event analysesand covariate-adjusted analyses among differenttypes of DAPT discontinuation and durations.Patient-level data would allow identifying indepen-dent predictors of ischemic and bleeding events usingdifferent durations of DAPT as a risk modifier. Inaddition, the different studies did not explicitlyreport results of all the clinical endpoints according tostent type.
Second, the lower rate of stent thrombosisobserved with second-generation DES could berelated to the fact that the duration of the RCTs withmore frequent second-generation DES use were thosewith shorter term follow-up; therefore, the lowerexposure and follow-up time might have accountedfor the lower event rates. However, lower incidenceof late and very late stent thrombosis with second-generation DES compared with older generation DESis strongly supported by earlier clinical evidence(28,29).
Third, we did not perform a risk/benefit trade-offanalysis between MI and bleeding because clinicalevent severity was not available in the studies, andthus the external validity of such results would bepoor. Fourth, another limitation of the meta-analysisis the substantial diversity in protocol designs of theincluded abbreviated- and extended-term DAPTRCTs; caution is therefore required in interpretingany overall effect estimate for S-DAPT versus L-DAPT.Finally, we found heterogeneity at the sensitivityanalysis regarding the effect of S-DAPT on stentthrombosis following exclusion of the DAPT trial. Thisfinding suggests that the thrombotic benefits associ-ated with DAPT become evident over time and thatthe overall effect of S-DAPT on stent thrombosismight have been attenuated by the abbreviated-termDAPT trials. Therefore, to clarify the effect ofextended DAPT on ischemic and bleeding outcomes,and eventually survival, additional randomized dataevaluating longer DAPT duration in contemporaryclinical practice are needed.
CONCLUSIONS
S-DAPT was associated with significantly higher def-inite or probable stent thrombosis rates comparedwith L-DAPT. The magnitude of the effect of S-DAPTon stent thrombosis was significantly attenuated withthe use of second-generation DES. However, thethrombotic benefit of L-DAPT was paired with ahigher risk of bleeding and numerically higher all-cause mortality. The results of the present meta-analysis indicate that the risk/benefit ratio betweenstopping or continuing DAPT after an initially rec-ommended period should be carefully individualizedconsidering the trade-off between ischemic andbleeding future risk.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.George D. Dangas, Division of Cardiology, MountSinai Hospital, One Gustave L. Levy Place, Box 1030,New York, New York 10029. E-mail: [email protected].

PERSPECTIVES
COMPETENCIES IN MEDICAL KNOWLEDGE: DAPT
is associated with protection against ischemic events but
increases the risk of bleeding in patients with DES. The
benefit of extended DAPT is strongly significant in
patients treated with first-generation DES and attenuated
with the use of current second-generation DES.
COMPETENCY IN PATIENT CARE: Physicians should
carefully evaluate patients’ ischemic and bleeding risks
and consider the type of stent implanted, in addition to
how well therapy has been tolerated, in determining how
long to extend DAPT (beyond an initial period) after DES
implantation.
TRANSLATIONAL OUTLOOK: Additional randomized
trials are needed to evaluate the optimum duration of
DAPT in patients with the latest generation DES devices
and high-potency antiplatelet drugs.
Giustino et al. J A C C V O L . - , N O . - , 2 0 1 5
DAPT After DES Implantation - , 2 0 1 5 :- –-
12
RE F E RENCE S
1. Levine GN, Bates ER, Blankenship JC, et al. 2011ACCF/AHA/SCAI guideline for percutaneouscoronary intervention. A report of the AmericanCollege of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelinesand the Society for Cardiovascular Angiographyand Interventions. J Am Coll Cardiol 2011;58:e44–122.
2. Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS guidelines on myocardial revascularization:the Task Force on Myocardial Revascularization ofthe European Society of Cardiology (ESC) and theEuropean Association for Cardio-Thoracic Surgery(EACTS) Developed with the special contributionof the European Association of PercutaneousCardiovascular Interventions (EAPCI). Eur Heart J2014;35:2541–619.
3. Mehran R, Baber U, Steg PG, et al. Cessation ofdual antiplatelet treatment and cardiac eventsafter percutaneous coronary intervention (PARIS):2 year results from a prospective observationalstudy. Lancet 2013;382:1714–22.
4. van Werkum JW, Heestermans AA, Zomer AC,et al. Predictors of coronary stent thrombosis:the Dutch Stent Thrombosis Registry. J Am CollCardiol 2009;53:1399–409.
5. Holmes DR Jr., Kereiakes DJ, Garg S, et al.Stent thrombosis. J Am Coll Cardiol 2010;56:1357–65.
6. Stone GW, Maehara A, Lansky AJ, et al.A prospective natural-history study of coronaryatherosclerosis. N Engl J Med 2011;364:226–35.
7. Mauri L, Kereiakes DJ, Yeh RW, et al. Twelveor 30 months of dual antiplatelet therapy afterdrug-eluting stents. N Engl J Med 2014;371:2155–66.
8. Stefanini GG, Siontis GC, Cao D, Heg D, Juni P,Windecker S. Short versus long duration of DAPTafter DES implantation: a meta-analysis. J Am CollCardiol 2014;64:953–4.
9. Cassese S, Byrne RA, Tada T, King LA,Kastrati A. Clinical impact of extended dual anti-platelet therapy after percutaneous coronaryinterventions in the drug-eluting stent era: ameta-analysis of randomized trials. Eur Heart J2012;33:3078–87.
10. Cutlip DE, Windecker S, Mehran R, et al. Clin-ical end points in coronary stent trials: a case forstandardized definitions. Circulation 2007;115:2344–51.
11. Mehran R, Rao SV, Bhatt DL, et al. Standard-ized bleeding definitions for cardiovascular clinicaltrials: a consensus report from the Bleeding Aca-demic Research Consortium. Circulation 2011;123:2736–47.
12. Moher D, Cook DJ, Eastwood S, Olkin I,Rennie D, Stroup DF. Improving the quality ofreports of meta-analyses of randomised con-trolled trials: the QUOROM statement. Quality ofReporting of Meta-analyses. Lancet 1999;354:1896–900.
13. DerSimonian R, Laird N. Meta-analysis in clin-ical trials. Control Clin Trials 1986;7:177–88.
14. Kim BK, Hong MK, Shin DH, et al. A newstrategy for discontinuation of dual antiplatelettherapy: the RESET Trial (REal Safety and Efficacyof 3-month dual antiplatelet Therapy followingEndeavor zotarolimus-eluting stent implantation).J Am Coll Cardiol 2012;60:1340–8.
15. Feres F, Costa RA, Abizaid A, et al. Three vstwelve months of dual antiplatelet therapy afterzotarolimus-eluting stents: the OPTIMIZE ran-domized trial. JAMA 2013;310:2510–22.
16. Schulz-Schupke S, Byrne RA, Ten Berg JM,et al. ISAR-SAFE: a randomized, double-blind,placebo-controlled trial of 6 versus 12 monthsof clopidogrel therapy after drug-eluting stent-ing. Eur Heart J 2015 Jan 23 [E-pub aheadof print].
17. Gilard M, Barragan P, Noryani AA, et al.Six-month versus 24-month dual antiplatelettherapy after implantation of drug eluting stentsin patients non-resistant to aspirin: ITALIC, arandomized multicenter trial. J Am Coll Cardiol2015;65:777–86.
18. Colombo A, Chieffo A, Frasheri A, et al.Second-generation drug-eluting stent implanta-tion followed by 6- versus 12-month dual anti-platelet therapy: the SECURITY randomizedclinical trial. J Am Coll Cardiol 2014;64:2086–97.
19. Gwon HC, Hahn JY, Park KW, et al. Six-monthversus 12-month dual antiplatelet therapy after
implantation of drug-eluting stents: the Efficacyof Xience/Promus Versus Cypher to Reduce LateLoss After Stenting (EXCELLENT) randomized,multicenter study. Circulation 2012;125:505–13.
20. Valgimigli M, Campo G, Monti M, et al.Short- versus long-term duration of dual-antiplatelet therapy after coronary stenting: arandomized multicenter trial. Circulation 2012;125:2015–26.
21. Collet JP, Silvain J, Barthelemy O, et al. Dual-antiplatelet treatment beyond 1 year after drug-eluting stent implantation (ARCTIC-Interruption):a randomised trial. Lancet 2014;384:1577–85.
22. Lee CW, Ahn JM, Park DW, et al. Optimalduration of dual antiplatelet therapy after drug-eluting stent implantation: a randomized,controlled trial. Circulation 2014;129:304–12.
23. Valgimigli M, Borghesi M, Tebaldi M,Vranckx P, Parrinello G, Ferrari R. Should durationof dual antiplatelet therapy depend on the typeand/or potency of implanted stent? A pre-specified analysis from the PROlonging Dual anti-platelet treatment after Grading stent-inducedIntimal hyperplasia studY (PRODIGY). Eur Heart J2013;34:909–19.
24. Airoldi F, Colombo A, Morici N, et al. Incidenceand predictors of drug-eluting stent thrombosisduring and after discontinuation of thienopyridinetreatment. Circulation 2007;116:745–54.
25. Iakovou I, Schmidt T, Bonizzoni E, et al. Inci-dence, predictors, and outcome of thrombosisafter successful implantation of drug-elutingstents. JAMA 2005;293:2126–30.
26. Dangas GD, Serruys PW, Kereiakes DJ, et al.Meta-analysis of everolimus-eluting versuspaclitaxel-eluting stents in coronary artery dis-ease: final 3-year results of the SPIRIT clinicaltrials program (Clinical Evaluation of the Xience VEverolimus Eluting Coronary Stent System in theTreatment of Patients With De Novo Native Cor-onary Artery Lesions). J Am Coll Cardiol Intv 2013;6:914–22.
27. Camenzind E. Final five-year results from therandomized drug-eluting stent trial PROTECT:the Patient-Related Outcomes With Endeavorvs Cypher Stenting Trial. European Society of

J A C C V O L . - , N O . - , 2 0 1 5 Giustino et al.- , 2 0 1 5 :- –- DAPT After DES Implantation
13
Cardiology Congress; September 2, 2014; Barce-lona, Spain 2014.
28. Finn AV, Joner M, Nakazawa G, et al. Patho-logical correlates of late drug-eluting stentthrombosis: strut coverage as a marker of endo-thelialization. Circulation 2007;115:2435–41.
29. Baber U, Mehran R, Sharma SK, et al. Impact ofthe everolimus-eluting stent on stent thrombosis:a meta-analysis of 13 randomized trials. J Am CollCardiol 2011;58:1569–77.
30. Stefanini GG, Byrne RA, Serruys PW, et al.Biodegradable polymer drug-eluting stents reduce
the risk of stent thrombosis at 4 years in patientsundergoing percutaneous coronary intervention: apooled analysis of individual patient data from theISAR-TEST 3, ISAR-TEST 4, and LEADERS ran-domized trials. Eur Heart J 2012;33:1214–22.
31. Elmariah S, Mauri L, Doros G, et al. Extendedduration dual antiplatelet therapy and mortality: asystematic review and meta-analysis. Lancet 2014Nov 16 [E-pub ahead of print].
32. Camenzind E, Boersma E, Wijns W, et al.Modifying effect of dual antiplatelet therapy onincidence of stent thrombosis according to
implanted drug-eluting stent type. Eur Heart J2014;35:1932–48.
KEY WORDS bleeding, myocardialinfarction, percutaneous coronaryintervention, stent thrombosis
APPENDIX For supplemental tables andfigures, please see the online version ofthis article.