section 3: exploring the pharmacists' world - the
TRANSCRIPT
SECTION 4: STRATEGIC OPTIONS FOR PHARMACY
Assessment of current cognitive services offeredIntroduction of Pharmacy Viability Matrix (PVM)Analysis of PVM from mail survey resultsPresentation of 24 pharmacy case studiesInnovation in Community Pharmacy
SECTION 1: INTRODUCTION
Research ObjectivesActual vs Desired Outcomes
SECTION 2: FUTURE CERTAINTIES IN HEALTHExamination of social trends to identify future opportunities for the provision of cognitive services through community pharmaciesIntroduction of Characterising Opportunities Filter
SECTION 5: CLOSING THE GAPIntegrates research results from all sources to show how gap can be closed between current service delivery and desired future service deliveryIntroduction of Pharmind Wheel: implementing change in context of the health and pharmacy industryIntroduction of Pharmacy Change Readiness Wheel: a practical tool for pharmacists to use to check whether their pharmacy is ready to introduce a change in service provisionIntroduction of Pharmacy Implementation Wheel: a tool to help pharmacists design and implement change for their pharmacyPractical application of the five introduced tools
SECTION 3: EXPLORING THE PHARMACISTS’ WORLD
Targeted literature review of change management in community pharmacyResearch methodology: mail survey, focus groups, case studies, consumer forums, stakeholder interviews
Section 3 – Exploring the Pharmacists’ World
1. Targeted International Pharmacy Literature Review
2. Research Methodology a. National Mail Survey of Community
Pharmacies b. Focus Groups c. Stakeholder Interviews d. Community Pharmacy Case Studies e. Consumer Forums
Section 3: Exploring the Pharmacists’ World
Section 3: Chapter 1
1 Targeted Pharmacy Literature Review: Community Pharmacy, Service Provision and Change
1.1 Introduction We now proceed to review international research literature relevant to understanding key issues relating to increasing service provision by pharmacy and the change issues associated with making such a move. Pharmacy in Australia is not alone in moving toward more service provision and, before we discuss what our research here discloses about these issues, we summarise what our literature search has revealed about Australian and overseas developments. Internationally, perceptions of pharmacy and the role of the pharmacist vary. According to the World Bank Group, pharmacy services are “the provision or sale of pharmaceutical products by drug retailers” (The World Bank Group 2004 p.1). Pharmacists themselves are defined as “individuals who have had formal training in dispensing pharmaceutical products” (The World Bank Group 2004 p.1). Pharmacy associations across the globe have begun the challenging task of changing these views of pharmacy and pharmacists by highlighting the value that pharmacy services can add to the health of their communities. The unit of analysis and the primary subject of change in this project is the community pharmacy. This has been defined previously as being the “…walk-in pharmacies in non-institutionalised settings and includes chain drugstores, independent pharmacies, and apothecaries” (Cipolle et al. 1998, p. 269). In this project the term community pharmacy is meant to incorporate the network of 5,000 community pharmacies across Australia. In this study, it has also been noted that a community pharmacy is made up of a variety of different businesses competing with each other (Munroe and Rosenthal 1994). This includes the division between the pharmacy dispensary and the front-of-shop. This literature review draws from selected articles in the pharmacy related literature on change and the implementation of services. These two areas were targeted as specifically related to this research project. As proposed in the project tender both national and international examples were be identified and examined. This activity included reviewing literature held by the Guild and other selected sources. As the Guild has previously funded research projects with extensive literature search on pharmacy related issues, we have concentrated on relevant papers compiled through Internet searches, international pharmacy association web searches and database searches. Here the literature is reported in the following parts: pharmacist level, pharmacy level, government/industry level and consumer/stakeholder level. These four levels highlight previous international research that feeds into the remainder of the report.
© Change Management and Community Pharmacy Project 73
Section 3: Exploring the Pharmacists’ World
1.2 Methodology This literature review was completed by locating, reading and critically analysing relevant books and articles. The following databases were used to locate articles relating to pharmacy and change management:
(a) ProQuest (online information service providing access to a number of databases). (b) Sage Publications (c) ABI Inform (d) EBSCO Online (e) Business Source Premier (f) Medline (g) Cochrane Database of Systematic Reviews
International pharmacy associations and general Internet search engines were also used to locate relevant articles. This report attempted to use business databases to a greater extent than previous reports of its kind but found little literature addressing the focus areas. Papers that were included covered topics including community pharmacy, service provision and change. The search terms used included:
Pharmacy Change management Pharmacist Cognitive services Pharmaceutical care Health Industry Management Implementation
1.3 Types of services in community pharmacy Some research has been done in the areas of pharmaceutical care, cognitive services and practice change in the pharmacy. While it is important to highlight this previous research as an invaluable source of information, it is also imperative to acknowledge a difference between previous research studies and the current research. Most of the research based in the United States focuses on the development and implementation of pharmaceutical care. This research project, however, has been specifically asked to address the implementation of cognitive pharmacy services (CPS) not Pharmaceutical Care. As Cipolle et al (1998) have argued, cognitive services and Pharmaceutical Care are not synonymous, although often used interchangeably.
1.3.1 Pharmaceutical Care Pharmaceutical Care, on the other hand, highlights more specifically the extended role of the pharmacist when involved in designing, implementing and monitoring a therapeutic plan to provide specific therapeutic outcomes for the patient (Hepler and Strand 1990). It
© Change Management and Community Pharmacy Project 74
Section 3: Exploring the Pharmacists’ World
is an “umbrella” term that is used predominantly in the United States to describe the concept of enhanced consultations in community pharmacy.
1.3.2 Cognitive Services The provision of services includes an intangible element which is difficult to measure (Holdford and Kennedy 1999). The value of any service is considered differently by the recipient of the service and the provider, but the ultimate assessment of value is made by the recipient (Cipolle et al. 1998). The services, however, are defined by the input of the provider. That is, CPS are defined as “…those services provided by a pharmacist to or for a patient or health care professional that are either judgemental or educational in nature” (Christensen and Hansen 1999 p.268). They are interventions by the pharmacist often related to drug therapy, and can also be termed as “professional services, value-added services, clinical pharmacy services, consulting services, and patient oriented (or patient focused) services” (Cipolle et al. 1998 p. 268). Various categories and groupings have been suggested for services provided by pharmacy that can be applied to CPS. Services can be categorised according to the benefit they provide:
Services that benefit society Services that benefit an organisation (other health care professionals) Services that benefit an individual
(Cipolle et al. 1998 p. 271)
Or they can be classified by the groups of patients and specific areas they can service: Specific patient groups Specific diseases Product-related services e.g. home health care, alternative medicine Other services
(Chen et al. 1999 p.141) A recent national pharmacy survey was conducted within Australia to measure pharmacy’s activities and the results outline the services that were being provided in pharmacy (Berbatis et al. 2003). This survey analysed the “enhanced services” that were being provided within community pharmacy. That is “those [services] offered in community pharmacies requiring additional or special skills, knowledge and/or facilities and are provided to sub-groups with special needs” (Berbatis et al. 2003, p. 33). The term “enhanced services” and the listing of services given in the National Pharmacy Database Survey has also been used and further developed in this research (see 2.2 in this section for details on the survey conducted). This literature review is being used to contextualise the pharmacy profession and to highlight the key themes relating to service delivery and change that have emerged from previous international literature. It is not intended to be a thorough examination of all pharmacy literature available but rather as background to the pharmacy profession. Following is an analysis of key pharmacy articles that have informed this project. The analysis has been divided into four sections:
Pharmacist level: this examines literature applicable to the pharmacist as an individual and the various themes that arise from studies in this area
© Change Management and Community Pharmacy Project 75
Section 3: Exploring the Pharmacists’ World
Pharmacy level: this analyses literature on the pharmacy profession, both in Australia and overseas, to assess the influencing factors in this area
Government/Industry level: this looks at government related issues and their influence on pharmacy. This also includes an analysis of the health systems and the funding structures in the PharmIntercom countries1
Consumer/Stakeholder level: here research that has been conducted with consumer groups and key stakeholders is reported for comparative purposes.
1.4 Pharmacist Level The introduction of cognitive pharmacy services and pharmaceutical care launches the industry into a new and evolving area of health care by taking pharmacists out of their “comfort level” (Gruda 1996 p.544). These initiatives potentially change the core offering of pharmacy. Pharmacy has traditionally been a product-based profession and by changing the value of pharmacy beyond the mere provision of medicines changes the paradigm in which pharmacists operate (Wertheimer 1998). This paradigm shift requires change at a number of levels. Herein lies the major challenge as “the difficulty in changing pharmacists’ practice patterns is evident in the limited success of past attempts to influence pharmacists’ consultation activities” (Odedina et al.1996 p.75). An apt model for providing extended pharmacy services to the community in the American context is pharmaceutical care (Bell et al.1998) although there is little evidence to suggest that it is the appropriate model for the Australian environment.
1.4.1 Pharmacists’ perceptions of change/new services There are a number of factors that influence the implementation of new services and change within community pharmacy. An analysis of the factors relating to pharmaceutical care includes the following:
Private counselling area Professional relationships General public’s perception of pharmacy Pharmacists’ perception of their developing role Remuneration Time
(Hepler and Strand 1990) These factors can also influence the pharmacists’ perception of their ability to change and provide services. It has been said that “the provider of services would probably place a value on the services that was higher than the price the recipient of those services would prefer to pay” (Wertheimer 1998 p.2). This discrepancy between the pharmacists’ and the consumers’ perception of the value of new services and of change in pharmacy offerings leads to a number of challenges for community pharmacy. For example, consumers have indicated that they would be willing to pay for selected services but pharmacists believe that this is not the case (Bell et al. 2000). 1 The PharmIntercom countries, Australia, Canada, Ireland, New Zealand, South Africa, the United Kingdom and the United States of America, are a consortium of pharmacy associations from English-speaking countries that aims to “promote improvement in the quality and effectiveness of healthcare” (National Community Pharmacists Association 2002)
© Change Management and Community Pharmacy Project 76
Section 3: Exploring the Pharmacists’ World
Previous research has found that one of the most significant barriers to the provision of services and change is the structure of remuneration (Christensen and Hansen 1999). Remuneration is currently tied to products and prescription dispensing and this can influence the way in which services are offered, the way they are perceived and their potential remuneration structure. This research result has been verified in previous studies which also identified additional situational variables affecting the process of service provision (Christensen and Hansen 1999). The perception of the change required by individual pharmacists in order to implement new services is multi-layered.
1.4.2 Pharmacists’ Skills It has been said that some pharmacists lack the fundamental practice skills needed to implement new services and successful manage the change involved. Research suggests that in particular they may lack a number of more advanced practice skills such as “therapeutics, clinical problem solving, communication skills, documentation and drug information” (Rovers et al 1998b p.198). Despite consumer belief that pharmacists have extensive knowledge of medicines (Bell et al 2000)and the pharmacists’ acceptance of the benefits of potential changes, pharmacists themselves lack confidence in their clinical knowledge (Kassam et al. 1999) and in their grasp of the business strategies needed to implement CPS successfully (Farris and Schopflocher 1999). From a change management perspective, it has been noted that pharmacists have underdeveloped management skills (Desselle and Tipton 2001), with the majority of their educational training focusing on the clinical nature of pharmacy and overlooking the potential small business ownership side of running a community pharmacy.
1.4.3 Interpersonal Communication and Confidentiality Pharmacists are considered by consumers to be one of the most trusted professionals (Roy Morgan Research 2004). Their working environment, however, can lead to communication problems and consumers can be discouraged by these problems from using the pharmacy’s services for personal medical issues. A past survey in the United States showed that over 60% of consumers were reluctant to discuss health issues within the pharmacy setting (Bell et al. 2000).
1.4.4 Inter-professional issues The area of cognitive services, by definition, may require the interaction between pharmacists and other health care professionals (Christensen et al. 2000). Developing and maintaining these types of relationships has been problematic for the profession (Rovers et al 1998a) and pharmacists have felt somewhat disassociated from the primary health care team (Bell et al. 1998). An Australian study showed that when given the chance to meet face-to-face with general practitioners, as opposed to the typical telephone communication (Chen et al. 2001), a higher level of inter-professional interaction was achieved. The model, however, was not without its difficulties and challenges (Chen et al. 1999). It has been suggested that “in
© Change Management and Community Pharmacy Project 77
Section 3: Exploring the Pharmacists’ World
order for community pharmacists to adopt a more professional role in relation to other health care professionals… alternative communication arrangements need to be identified (for inter-professional communication), so that discussion about complex clinical issues can occur” (Chen et al. 2001 p.89). Communication lies at the core of inter-professional interactions and must be addressed.
1.4.5 Mentors A lack of mentors in the pharmacy industry has been identified as an educational and academic obstacle in the implementation of Pharmaceutical Care (Rovers et al 1998a). The role of an experienced mentor is a functional way to approach professional clinical development (March et al. 1999) and change management (Doucette and Koch 2000). Previous research showed that proprietors of “change pharmacies” were found more likely to take on industry leadership positions and therefore an exemplary position for other pharmacists (Doucette and Koch 2000). In the Australian context mentors and advisors specific to cognitive pharmacy services have been introduced. MMR facilitators have been put in place in 122 geographic areas, covering the whole of Australia, to provide support, advice, eduction and information to pharmacists and general practitioners on Medication Management Reviews (MMR) (The Pharmacy Guild of Australia 2004a). This program has helped to overcome territorial issues between pharmacists and general practitioners; this tension is discussed in more detail in section 1.5.2 of this chapter.
1.4.6 Workflow Cognitive services have implications for the workflow of the pharmacy and the implementation of services will generally require workflow redesign. Services that require high involvement by the pharmacist decrease the efficiency of the prescription dispensing process (Holdford and Kennedy 1999), and therefore alternative arrangements must be made to maintain dispensing output. This could include the use of dispensary technicians and pharmacy assistants or other innovative practices (Whitehead et al. 1999). Generally, pharmacists’ priority when dispensing repeat prescriptions is efficient and expedient service (Bell et al. 2000) and CPS could impede the capacity for this to occur unless there is a reorganisation of workflow.
1.4.7 Behaviour Professional services require the pharmacist to change and take on new behaviours (Berger and Grimley 1997). When implementing cognitive services “pharmacists must make the psychological commitment and the effort required to improve patients’ outcomes” (Odedina et al. 1996, p. 75). This psychological commitment that influences “pharmacists’ behaviour is directly determined by past behaviour recency, behavioural intention and perceived behavioural control” (Odedina et al. 1996, p. 76). There have been extensive studies on behaviour and its effects on service implementation that have found inconsistencies between the behavioural intention of pharmacists and their actual behaviour. This was discovered to be “due to differences in social norms, perceived behavioural control, self efficacy and affect” (Farris and Schopflocher 1999). Three individual factors were proposed to influence patient-focused care: “self-efficacy, ego strength and locus of control” (Latif 2000). The five stages of voluntary change have been applied to the pharmacy profession (Farris and Schopflocher 1999) and were an effective
© Change Management and Community Pharmacy Project 78

Section 3: Exploring the Pharmacists’ World
model for understanding behavioural change. The change went through the stages of pre-contemplation, contemplation, preparation, action and maintenance (Levesque et al. 1999). It was only by going through this process that change was accepted and became the norm. Interventions within a profession should be individualised, through the five stage process, which will result in accelerated rates of change and a sense of ownership during the change process (Levesque et al. 1999). A study using this model was undertaken in the United States and a high proportion of pharmacists were not found to be ready for the implementation of Pharmaceutical Care (Berger and Grimley 1997). The same model was used successfully in Australia and behavioural change was achieved in relation to over the counter medicines (de Almeida Neto, Kelly and Benrimoj 2001).
1.4.8 Attitude The attitude of the pharmacist towards CPS can influence the adoption rate of these services. A positive attitude is essential (Odedina et al. 1996). The difficulties caused by a pharmacist’s conventional attitude can arise from “inadequate comprehension of what [the service] is and what it entails, misconceptions and false assumptions, fears related to changing roles; and [a] lack of personal motivation” (Rovers et al 1998a). There must be a clear understanding and assessment of what motivates the “average” pharmacist (Tully et al. 2000). The use of CPS by the pharmacist is also positively influenced by an employer’s belief in the provision of patient care and is not entirely dependent on an employee pharmacist’s attitude (Christensen and Hansen 1999). Behavioural control and subjective norms were found to influence the tendency to provide services. Adapting change methods to address these issues would result in more effective implementation of CPS (Odedina et al. 1997)
1.4.9 Perceived roles
“The community pharmacist’s contribution to the primary health care team is, arguably, something of an enigma… the team role of the pharmacist is far from clear”
(Harris et al. 1997) Their retail setting makes the pharmacist accessible and available to the public and enhances their role as a front line contributor to primary health care (Whitehead et al. 1999). The role of pharmacists can vary greatly in different situations and involve a vast range of activities (Roberts et al. 2003). Pharmacists view themselves as technical advisors, drug experts, leaders and counsellors of therapeutic needs. Their role, however, is evolving and in the future, the role of pharmacists appears likely to extend into a number of additional areas such as authority on disease states, IT expert and provider of individualised information (Norgaard et al. 2001).
1.4.10 Core role - what pharmacists “should” be doing Interpretations of what constitutes the core role of pharmacy vary. The education of pharmacists has traditionally emphasised the scientific nature of their training. Pharmacy, therefore, is still primarily orientated towards dispensing of medicines. Often the broader health issues of customers are overlooked (Harris et al. 1997). It has been suggested that
© Change Management and Community Pharmacy Project 79
Section 3: Exploring the Pharmacists’ World
pressure from high volumes of dispensing and poor delegation limits the role of pharmacists in the workplace, particularly in offering services (Roberts et al. 2003). This core focus on dispensing is currently being reassessed. It has been suggested by community pharmacists that the role of a pharmacist should involve “greater contact time with patients/customers, [the] extension of their role to provide new services and decreasing the time spent dispensing” (Rutter et al. 2000, p. 205).
1.4.11 Steps for professional change Previously, the following steps have been recommended to assist pharmacists in the process of change:
Develop awareness of new purpose and responsibilities examine personal competence to accomplish purpose identify resources available develop working relationships to achieve new purpose create outcome, experience reward return to step one with renewed motivation and commitment
(Hepler 1990, p. 26) The general model for change identified by Farris & Schopflocher (1999)goes through the stages of preparation, acceptance and commitment. It is through the preparation stage that contact and awareness of the proposed change are achieved. By understanding and perceiving the change in a positive way, pharmacists accept the process of change. When the change is adopted, institutionalised and internalised by the pharmacists they exhibit signs of commitment to the change (Rovers et al 1998a).
1.5 Pharmacy Level It was predicted in 1990 that the next/ following 10 to 20 years would bring forced changes to the pharmacy industry in the US and in order to make a mark in the medical marketplace, pharmacists would need to should how they could be an integral part of the health care team (Hepler 1990). Pharmacies can be divided into a number of categories. In the US the profession has been divided into the following four groups (Munroe and Rosenthal 1994):
The ‘conventional’ chain: pharmacies equivalent to the Traditional Pharmacy in the Pharmacy Viability Matrix. This group focuses on a specific geographical catchment area and their point of differentiation is their convenience to the local community.
The mass-merchandiser store: Pharmacies in this group focus on price competition and use this to create customer loyalty and maintain their image. This is equivalent to the Expanded Pharmacy in the Pharmacy Viability Matrix.
The food-drug combination store: Pharmacies in this group are considered one-stop shops for health and beauty needs. This is most closely related to the Multi Specialty in the matrix.
Non-traditional pharmacy providers: The point of differentiation for pharmacies in this group is their method of distribution, e.g. mail order or dispensing doctors. None of the proposed Pharmacy Viability Matrix models correspond closely to this
© Change Management and Community Pharmacy Project 80
Section 3: Exploring the Pharmacists’ World
category but as all of the strategic models allow for differentiation in the mode of product or service distribution, these non-traditional distribution methods could be used in any of the strategic options.
The Pharmacy Viability Matrix will be outlined in detail in section 4 chapter 2.
1.5.1 Rural vs urban The pressures on pharmacy are often intensified in the rural setting as pharmacy is an important source of health care in areas suffering from a lack of other health care professionals. For rural constituencies, pharmacies are “available and accessible to the public usually at no cost for long hours and almost every day” (Venkataraman et al. 1997, p. 209). Research also suggests that community pharmacists in rural areas are actively taking up pharmaceutical care services (Venkataraman et al. 1997) and other cognitive services, but the lack of skilled employees in these areas can make effective service provision difficult.
1.5.2 International models The push to encourage service provision in pharmacy is a worldwide development (see section 2). There have been a number of models for Pharmaceutical Care developed in Canada to support the move towards improved patient care and to integrate the role of pharmacy (Ramaswamy-Krishnarajan and Grainger-Rousseau 2000). These models have not been replicated in Australia but the outcomes and key learnings from overseas experience are important to acknowledge and build on in Australian research. In the European context, similar barriers to enhanced services have been found, including lack of time, limited funding and limited knowledge. American research has indicated that the culture of the pharmacy must be supportive of this change. Without this internal support structure professional services can not be effectively provided to consumers (Latif 1998).
1.5.2.1 International Financial Models of Pharmacy International financial models of pharmacy were also sought out and it was clear that the level of financial analysis used in research is very restricted and narrow in focus. With the exception of one study (Carroll 1997), which provided evidence of modelling product and service options but again in a narrow definitional context, little evidence was found of research into pharmacy business models. The extant literature provides little direction for developing an approach to modelling and financial comparison. The Medici Capital financial analyses present an approach to financial modelling in Pharmacy.
1.5.3 Barriers and Facilitators to Change Australia-based research has resulted in comparable findings to the European models. In the National Pharmacy Database Survey conducted in 2002 (Berbatis et al. 2003) “time shortage” was the top ranked barrier to implementing enhanced services. This was followed by “pharmacist shortage” which is also a major problem in Australia. Australian research has also tried to identify the facilitators of change (Berbatis et al. 2003; Roberts et al. 2003; Roberts et al. 2004). The National Pharmacy Database Survey (Berbatis et al. 2003) found that the top ranked facilitator of change was access to patient
© Change Management and Community Pharmacy Project 81
Section 3: Exploring the Pharmacists’ World
notes. A collaborative program, MediConnect, is currently being piloted in Ballarat and Launceston to enable shared access to patient records by a number of health care professionals (The Pharmacy Guild of Australia 2004d). The other facilitators were internal pharmacy issues, such as closed counselling areas and appointment systems, which need to be addressed by individual pharmacies. The business and professional facilitators for change were analysed in greater detail in a qualitative study with Australian pharmacy professionals (Roberts et al. 2003). This was further developed in a quantitative analysis of facilitators of practice change (Roberts et al. 2004). These facilitators are listed below:
Relationship with doctors Remuneration Patient expectation Pharmacy layout Manpower/staff Communication/teamwork (incorporating leadership) External support/assistance
(Roberts et al. 2004, p. 72) Change programs in Australia, therefore, need to take into account these facilitators of service implementation.
1.5.4 Strategy Pharmacies that are making the move to CPS need to use strategic planning to align their business with the new services being incorporated into their pharmacy. Strategic planning can be seen as “the continuous process of adapting to change” (Harrison and Ortmeier 1996, p. 583). There is limited discussion of strategic planning in relation to community pharmacy but it is now becoming a much more prominent issue (see Odedina et al. 1995; Harrison and Ortmeier 1996; Doucette and Koch 2000; Tully et al. 2000). Those pharmacies that are strategically focused on profit, rather than patient care, were found to be non-providers of professional services (Odedina et al. 1995). The strategic features that divided pharmacies into those that implemented change and those that did not, were “futurity of decisions and addressing constraints” (Doucette and Koch 2000, p. 388). For the majority of pharmacies, strategic decisions are made on an ad-hoc basis and there is little formalised strategic planning (Tully et al. 2000).
1.5.5 Services The momentum to introduce cognitive services into the pharmacy has been driven by the evidence of substantial savings to health budgets that can achieved when the pharmacy provides primary care to consumers (Donato et al. 2001). The success of these services relies on collaborative relationships with other health care professionals as well as the “innovative restructuring of pharmacy practices and responsibilities of pharmacists” (Ramaswamy-Krishnarajan et al. 2000). Research has suggested that there is a low performance rate on professional services provided by pharmacy and the pharmacy profession’s move into this area has yet to become a reality across the board (Christensen and Hansen 1999). There is evidence of some resistance within the profession (Roberts et al. 2003). Despite this resistance, increased pharmacist involvement with the consumer
© Change Management and Community Pharmacy Project 82
Section 3: Exploring the Pharmacists’ World
is considered a desirable move in Australia (Roberts et al. 2003). In Australia there are a number of services that are remunerated by the Federal Government, these are outlined in the next section.
1.5.5.1 Services in Australia Government remuneration for cognitive pharmacy services in Australia comes through the Third Community Pharmacy Agreement between the Pharmacy Guild of Australia and the Australian Government. It is a five year agreement and it came into effect on 1 July 2000. One of its goals is to expand the professional role of community pharmacists as health care providers. The Third Agreement was the second of the Agreements to obtain specific remuneration for payment of professional pharmacist services, including:
Consumer Medicine Information (CMI) Home Medicine Reviews (HMR) Residential Medication Management Reviews (RMMR) Aboriginal Health Services (AHS)
Since the negotiation of the Third Agreement, many pharmacists have decided to offer more professional services than are provided for to date. In negotiating the Fourth Guild Government Agreement, the Guild intends to try to further expand on the pharmacists’ role in providing professional services. There are a number of other services which are possible candidates for the Fourth Agreement negotiations. There has been significant investment in research and development to investigate these potential services. Four possible services will be discussed below. They are:
Disease state management for diabetes Disease state management for asthma Harm reduction, and Provision of dose administration aids.
These services are outlined in more detail below.
1.5.5.1.1 Consumer Medicine Information (CMI) Consumer Medicine Information (CMI) is one of the funded initiatives under the Medicines Information to Consumers (MIC) Program introduced in August 2001. CMI is a written piece of information about a specific drug product which conforms to special provisions as set out by Therapeutic Goods Regulations (The Pharmacy Guild of Australia 2002). CMIs are prepared by pharmaceutical companies, and come in a variety of forms, including leaflets or package inserts. Pharmacists are not specifically required to supply CMIs under any specific legislation or regulation; however they do have a professional and legal obligation to ensure patients have the required information to enable them to make informed decisions about their medicines, and CMIs are one method to meet these obligations. Under the Third Community Pharmacy Agreement, pharmacies enrolled in the MIC program received an initial ‘Readiness’ payment of $3,000 for the first phase of the program, a Registration Incentive of $1,000 and an ongoing Participation Allowance of 10 cents per claimable PBS/RPBS prescription. Payment is based on prescription volume, and the Program is administered by the HIC.
© Change Management and Community Pharmacy Project 83
Section 3: Exploring the Pharmacists’ World
1.5.5.1.2 Home Medicine Reviews (HMR) Home Medicine Reviews (HMR) (The Pharmacy Guild of Australia 2004b) were introduced in October 2001, and have been implemented both as an initiative under the Third Agreement as well as through the introduction of a Medicare item for GP involvement. HMRs consist of a review of a patient’s medical regimes in the patient’s home. An HMR is conducted by an accredited pharmacist upon referral by the medical practitioner, a medication management report is prepared and the outcome discussed by the pharmacist and GP. The goal of the review is to maximise an individual’s benefit from his/her medication program and to improve their quality of life and health outcomes. Pharmacists are currently remunerated $140 for each review prepared.
1.5.5.1.3 Residential Medication Management Reviews (RMMR) Residential Medication Management Reviews (RMMR) were one of the earliest professional services to be negotiated as part of the Second Agreement. These reviews are similar to HMRs; however they are conducted in aged care facilities or other similar institutions. The current remuneration per RMMR is $100.
1.5.5.1.4 Aboriginal Health Services (AHS) Aboriginal Health Services (AHS) is an allowance for providing remote area support services as part of one of the specific incentives to improve access to pharmacy services in rural and remote Australia. Under Section 100 of the National Health Act 1953 clients of a remote area Aboriginal Health Service are able to receive PBS medications directly without a formal prescription form and without charge, at the time of consultation. The initiative was introduced in 1999 (Department of Health and Ageing 2001), and there are currently approvals for approximately 40 out of the 50 Commonwealth-funded remote area Aboriginal Medical Services to provide PBS medicines in this way.
1.5.5.1.5 Disease State Management (DSM) Disease State Management (DSM) has been defined as a continuous coordinated evolutionary process that seeks to manage and improve the health status of a carefully defined patient population over the entire course of the disease. A successful DSM program achieves this goal by identifying and delivering the most effective and efficient combination of available interventions and resources. DSM distinguishes itself in that it shifts the focus way from treating patients for discrete episodes of care towards a high quality and continuous service covering all stages of the disease.
Diabetes: A major element of diabetes care is self-management and this can involve blood glucose monitoring, diet modification, weight control and regular physical activity. Community pharmacy is well placed to support such a self-management approach as well as provide advice on and monitoring of prescribed medicines. A National Diabetes Services Scheme subsidises the supply of syringes, needles, test strips, etc to registered people with diabetes. The program is funded by the Federal Government and administered through Diabetes Australia which coordinates the supply of products in all states. Government expenditure for this scheme in 2002-03 was $81.4M.
© Change Management and Community Pharmacy Project 84
Section 3: Exploring the Pharmacists’ World
Asthma: Despite the success of many interventions designed to improve asthma management, there is a significant proportion of people with asthma who do not have effective asthma management. Pharmacists see many people with asthma on a regular basis and may be the one health professional group with whom many people with asthma have regular contact.
1.5.5.1.6 Harm reduction Providing harm reduction services through pharmacies is seen as an effective public health measure. This service involves dispensing methadone/buprenorphine for managing opioid dependence. It also includes selling and supplying clean needles, syringes and other items used by injecting drug users. The program assists individuals to achieve quality of life by improving health and social functioning, and works to reduce or eliminate illicit opioid drug use.
1.5.5.1.7 Dose Administration Aids (DAA) Dose Administration Aids (DAA) for administering medicines are widely recognised by patients, pharmacists, carers, doctors and nursing staff as highly effective for people who require assistance with oral medications. DAA are frequently used in environments of long term aged care, people with intellectual disabilities living in the community, and community settings of managed palliative care and people receiving assistance to reside in their own home. They come in a variety of forms, ranging from manually packed compartmentalised boxes and blister packs to automatically packed bar-coded sachet systems. Examples of DAA include: Dosette, Medidos, Mediplanner, Daily Pillminder, Webster-Pak, Perso Pak and Nomad Monitored Dosage System.
1.5.6 Change
“Like other programs intended to change core work activities, attitudes, and behaviours of health care providers, implementing pharmaceutical care is a difficult task as it requires fundamental changes in practice”
(Odedina et al. 1995). It has been said that pharmacy practice change has two primary components that influence the success of the intended change. These components are the resourcing within the pharmacy and the activities of the pharmacist and pharmacy staff (Doucette and Koch 2000). Resourcing issues include: “physical layout of pharmacy, qualified personnel, practice orientation, patient expectation, physician cooperation, computer support, patient medical information and competency” (Odedina et al. 1995, p. 170). The three most significant areas for improvement in the pharmacy are: highly skilled pharmacy staff, additional support for the pharmacist and an “enhanced working environment" (Rutter et al. 2000). The implementation of CPS requires a transformation from a retail-centred to a patient-centred approach and increased training for pharmacy technicians (Odedina et al. 1995). This constitutes significant change for the pharmacy that must be carefully managed. The specific activities of the pharmacy staff generally depend on the organisation of workflow (as discussed above).
© Change Management and Community Pharmacy Project 85
Section 3: Exploring the Pharmacists’ World
The Holland-Nimmo Practice Change Model has also been theoretically developed to better understand the motivation of pharmacists. The model indicates that the following are the three basic components of motivation and pharmacists must lead their pharmacy effectively when addressing these components in order to create a positive environment for practice change. The components are:
practice environment learning resources motivational strategies
(Holland and Nimmo 1999)
1.5.7 Tools Many models and tools have been developed to aid the implementation of pharmaceutical services. There have been attempts to create a structured plan for the implementation of CPS and to indicate how the barriers and facilitators to change can be addressed (Munroe and Rosenthal 1994; Holdford and Kennedy 1999; Donato et al. 2001). Research in the Australian context has outlined the facilitators of change in the pharmacy (Roberts et al. 2003) but there has yet to be a systematic analysis of tools to implement change and encourage the implementation of services. This process has been initiated, however, with the “V2O PHARM” model (Roberts et al. 2003, p. 103) that we have built on in this report.
1.6 Government/Industry Level
1.6.1 Public Health
“Concerns about rising levels of demand for primary health care services in general, and the mismatch between supply and demand, suggests there is a need to understand the place of community pharmacy in primary care and its role in helping to manage demand”
(Hassell et al. 1999, p. 51) A major public health issue in Australia is medication-related problems and hospital admissions due to the misuse of medicines. The implementation of extended services in pharmacy is designed to help overcome this issue (March et al. 1999) and to increase the quality use of medicines. The ageing population is becoming increasingly dependent on Australia’s health system and the system needs to make best use of government expenditure to meet the needs of the population. Government acceptance of the extended role of pharmacy in the health care system is evident through the current remuneration for CPS in the Third Community Pharmacy Agreement. Internationally there has been an attempt to gain government support through changes in legislation for this extended role. In Iceland Pharmaceutical Care was not legislated and it was concluded that the move to implement and encourage service provision must come from within the profession (Rossing et al. 2001). In Australia, the pharmacy profession, through the Community Pharmacy Agreement, is encouraging the extended role of pharmacy in providing services.
© Change Management and Community Pharmacy Project 86
Section 3: Exploring the Pharmacists’ World
1.6.2 Remuneration In the mid-1990s there had been little change in the remuneration scheme for pharmacy despite the introduction of professional services (Gruda 1996). The remuneration systems have begun to evolve in various countries (see section 3.1.5.4) but the central source of funding is still linked to prescription dispensing (Wertheimer 1998). The level of clinical intervention and the professional commitment of the pharmacist are not incorporated into the current structure of remuneration. This is one of the barriers to implementing change (Roberts et al. 2003) as financial incentives were found to support the adoption of CPS (Christensen et al. 2000). Third party remuneration for pharmacy services could also increase consumer demand and promote regard for these professional services (Ganther 2002). It has also been suggested that consumers could pay for value added services but consumer perception associates pharmacy fees with medicinal products rather than services and government remuneration systems largely reinforce this (Reutzel 1994). A shift in consumer and governmental thinking would, therefore, also be required.
1.6.3 Professional Status
“The lay understanding of a pharmacist’s expertise probably extends little further than a dictionary definition such as ‘a person qualified to prepare and dispense drugs’”
(Harris et al. 1997 p.196). The profession of pharmacy is valued differently by different stakeholders. This disjunction between the value given to pharmacy by stakeholders and consumers and the value given by pharmacists themselves (Indritz and Artz 1999) results in the under-utilisation of pharmacy expertise in the community (Munroe and Rosenthal 1994). In the face of a radical transformation into a predominantly patient focused model, the potential role for pharmacy has not been entirely understood by consumers and stakeholders alike (Desselle and Tipton 2001).
1.6.4 Services The uptake of services relies on the development of relationships between pharmacists and consumers and stakeholders who will be affected by the provision of new service(s) (Donato et al. 2001). The low rate of adoption internationally has been attributed to the lack of information shared with other stakeholders. “[T]he lack of communication between the designers and implementers [of the service] and the inadequate planning of the implementation programs” (Holdford and Kennedy 1999 p.546) have resulted in tension between stakeholder groups and the pharmacy profession.
1.6.5 PharmIntercom Country Analysis An overview of the health systems in Canada, the United Kingdom and the United States has been outlined in section 2. This highlights the relevance of overseas models to the Australian pharmacy profession and the implications of international trends in service provision. In this section, the PharmIntercom country reports have been analysed (PharmIntercom 2003) to further explore the information available on international models. The PharmIntercom countries, Australia, Canada, Ireland, New Zealand, South
© Change Management and Community Pharmacy Project 87
Section 3: Exploring the Pharmacists’ World
Africa, the United Kingdom and the United States of America, are a consortium of pharmacy associations from English-speaking countries that aims to “promote improvement in the quality and effectiveness of health care” (National Community Pharmacists Association 2002). These countries share common issues that stem from the provision of professional services in community pharmacy. As articulated by the Irish Pharmaceutical Union (IPU) “there is considerable scope to deliver the current level of professional services delivered by community pharmacies into a more comprehensive, structured and organised service to the community” (Irish Pharmaceutical Union 2004). This report goes some way to providing this structure to Australian community pharmacy. The following summarises the common elements of the associations’ efforts to promote practice change in their respective countries. This analysis draws on “sections” outlined by the PharmIntercom co-operative and reported on by each country. The “sections” that are discussed below are as follows: funding, personnel, value proposition, change management, supply chain, profile and alliances, quality and ownership2. These “sections” also have implications for service provision and these are addressed below.
1.6.5.1 Funding Many of the PharmIntercom countries have changed or are changing the remuneration structure for pharmacy. Internationally, pharmacy associations are seeking to ensure more equitable levels of funding for pharmacy. Countries such as New Zealand are facing limited government funding, and in Ireland, pharmacists are faced with reduced margins on prescription drugs. Pharmacists are beginning to charge consumers for cognitive pharmacy services such as asthma and diabetes management. Countries such as Canada, the UK and South Africa have started to introduce fee-for-service models to varying degrees. In the UK there has been government conducted research to ensure that cost structures are flexible and able to adapt to changes in service structures. The current South African fee-for-service model as used in the private sector is no longer considered sustainable. The market is predicted to move quickly through managing fee for service, managed care and capitation stages. Developing a “pharmacist professional fee” based on an hourly rate has been made a priority for the recently established Pharmaceutical Services Negotiating Committee in South Africa. Only a few countries, such as the United States, have third party payers that have added pharmacy services to their schedule of claimable items. Changes to pharmacy across the globe are commonplace. Ireland has recently restructured their remuneration system making it one of the most deregulated markets in Europe. Many countries are currently negotiating new policies and funding structures to support cognitive pharmacy services. A notable exception is New Zealand where the balance between new services and the core dispensing role of pharmacists is still being clarified by the pharmacy association.
1.6.5.2 Personnel A number of countries such as Ireland, South Africa, UK and the United States that are troubled by a shortage of skilled pharmacists and support staff. There are also countries, such as New Zealand, with a surplus of pharmacists. For the countries lacking enough
2 These have been adapted from the 2003 PharmIntercom report
© Change Management and Community Pharmacy Project 88
Section 3: Exploring the Pharmacists’ World
qualified pharmacists there have been efforts to alleviate this problem by either opening new schools of pharmacy and/or concentrating support at the pharmacy student level. Most countries, whether suffering from a deficit or surplus of pharmacists, are developing comprehensive training programs for pharmacy technicians and pharmacy assistants. Better trained staff will support the implementation of cognitive pharmacy services. In Canada, a joint research project has been developed between the pharmacists’ association and the medical and nurses’ associations to address staffing issues in rural and remote areas.
1.6.5.3 Value Proposition Many countries have funded research projects in their respective countries to determine the value of pharmacy to the community. In Ireland, it has been estimated that the health care budget is saved at least 155million annually through pharmacy interventions. The value of pharmacy to the community is being promoted to ensure that the skills and experience of pharmacists are being fully utilised and pharmacy is being endorsed as a primary health care service provider. In Australia the Guild commissioned a paper that assessed community pharmacy in terms of the value that professional services provided to the community (Roughead et al. 2003).
1.6.5.4 Change Management Internationally, the pharmacy profession is focusing its energies on promoting services and highlighting the contribution that pharmacists can make to the primary health care team. This requires a comprehensive and structured change management strategy to support sustainable implementation programs. It has been proposed in Canada that pharmacists be given limited prescribing rights. South African pharmacy associations have focused on changing remuneration structures for pharmacy services and reframing the mind-set of pharmacists to encourage change in pharmacy management and operations. In the UK, the government has encouraged the differentiation of services in pharmacy and has prioritised the reduction of health inequalities through health care providers including pharmacy. In Australia, the Second and Third Community Pharmacy Agreements have included remuneration for CPS.
1.6.5.5 Supply Chain The scope of pharmacy within the health care supply chain is being developed in many countries. In North America, mail order prescriptions are an issue for the profession. The Canadian association opposes the issuing of scripts when the patient does not have a relationship with the pharmacist and the prescriber. Pharmacy Benefit Managers in the US have responded to the growing trend of cross-border prescription services by introducing their own mail order operations that their members are strongly encouraged to use. Pharmacy functions in other countries are changing and there has been a move to introduce a prescribing role for pharmacy. The use of collaborative groups with other health care professionals is also directed at promoting the integration of primary health care services and ensuring their pharmacy is included. This is also the case in Australia where the Guild is attempting to strengthen the role of pharmacies in the Health System.
© Change Management and Community Pharmacy Project 89
Section 3: Exploring the Pharmacists’ World
1.6.5.6 Profile & Alliances The need to promote the role of pharmacists to consumers and other health care professionals is apparent internationally. Research on consumer behaviour in New Zealand has highlighted that pharmacy services need to save the consumer time but not compromise quality. The changing role of pharmacists has been promoted through large scale advertising campaigns in the UK and the United States. In Australia, pharmacists are one of the most highly valued professionals and an attempt is being made to maintain this reputation. International pharmacy associations have also attempted to create stronger ties with other health care bodies. They have done this through partnerships with other health care professionals, conducting research into interorganisational collaboration and joint working committees. The attempt to strengthen these relationships promotes information sharing and the use of multi-disciplinary teams to look at a range of health issues.
1.6.5.7 Quality The emphasis on quality and standard practice requirements has been strongly emphasised. Standard operating procedures and training courses have been established internationally to provide guides and governance structures to pharmacists. Canada has set up a national association to regulate competency-based pharmacy practices. Ireland has enforced protocols through training programs. The United States and UK have developed quality assurance measures to standardise practices. New Zealand has concentrated on educating both consumers and pharmacists on the required level of service. The South African Pharmacy Council has compiled protocols to guide best practice. The Guild in Australia has implemented the formalised program, the Quality Care Pharmacy Program (QCPP), intended to improve the level of health care services and advice available in pharmacies and address issues of quality and standard practice in Australia pharmacies.
1.6.5.8 Ownership
While Australia has maintained its requirement of pharmacist-only ownership of pharmacies, Ireland, South Africa and the United States have loosened this regulation. Irish pharmacies require only a supervising pharmacist to be on the premises. The Irish Pharmaceutical Union (IPU), however, is attempting to change this regulation to pharmacist-only ownership. Rulings have also relaxed in the UK, Canada and South Africa to allow corporate ownership of pharmacies. This has resulted in reduced numbers of independent pharmacies and a growth in chains and franchises. For example, in the UK, 40 % of pharmacies are owned by seven companies. New Zealand retained its closely regulated ownership laws but a pharmacy has recently been opened within a supermarket. Changes in ownership could potentially have an effect on services. Pharmacy representative bodies often claim that non-pharmacist owners are more likely to be motivated by profit and that this may decrease the quality of patient care and the focus on services. For example, Ireland currently allows non-pharmacist ownership of pharmacies but the IPU is putting forward a recommendation to change the Pharmacy Bill in support of pharmacist only ownership of pharmacies. As the Union notes, “many of the pharmacist activities depend on the good will of individual pharmacists” (Irish Pharmaceutical Union 2004). They argue that this good will could be lost if there is an increase in non-
© Change Management and Community Pharmacy Project 90
Section 3: Exploring the Pharmacists’ World
pharmacist owners. This is a crucial issue in most countries and there is need for cross-empirical research to examine whether deregulation of this kind does affect trust in pharmacists and the effective provision of services.
1.6.5.9 Implications Each of the topics outlined above has significant implications for service provision in pharmacy. Adequate funding is a key factor in the adoption rate of services and varying forms and models of remuneration are being tested internationally. No country has developed an equitable model for pharmacy remuneration that suits all stakeholders. Without sufficient pharmacy personnel, enhanced services cannot be provided to consumers to required standards without threatening the core functions of pharmacy. The training of pharmacy staff is an important factor in allowing the pharmacist to focus more on the provision of services and maintain a consistent quality of service. The savings that pharmacy services can provide to reduce health care expenditure have been analysed in a number of countries. There is evidence that pharmacy services offer value to the government and provide a better health care system to the population. The professional services proposed by pharmacy also appeal to consumers who are seeking better health care at the community level. The accessibility of pharmacists and their high level of knowledge can potentially provide consumers with immediate access to more health care services than are currently available. In order to provide more cognitive services, the profession must address the need to change the pharmacists’ and consumers’ traditional understanding of the role of pharmacy. Our research indicates that this change is already underway in Australia. Detailed change management strategies are beginning to be developed by pharmacy associations across the globe to ensure that this attitudinal change intensifies. The image of pharmacy needs to be raised with both consumers and stakeholder groups. Overseas experience reinforces the need, when implementing new services that cross the boundaries of traditional pharmacy, to involve stakeholders affected by the change. In many cases, standard operating procedures and quality control measures are currently lacking for the provision of services. Hence there is a perceived lack of consistency in service quality. Most countries are moving towards enforcing standard practices so that consumers can expect a benchmarked level of quality from pharmacy services. The aim of these defining and reinforcing standards is to increase the credibility of professional pharmacy services by ensuring the delivery of high quality services.
1.7 Consumer/Stakeholder Level
1.7.1 Consumers Hassell et al (1999) argue that the basis for consumer decisions to utilise pharmacy services can be found in the health belief and socio-behavioural models. The first model highlights individual consumer characteristics that impact on the decision to utilise services. The latter model suggests that “people’s use of health services is a function of their
© Change Management and Community Pharmacy Project 91

Section 3: Exploring the Pharmacists’ World
predisposition to use services, factors which enable or impede use, and their need for care” (Hassell et al. 1999p. 41). Their study concludes that process factors (e.g. previous use of services), organisational and supply factors in the pharmacy and the accessibility of community pharmacy contribute to the utilisation of pharmacy services by consumers (Hassell et al. 1999). Pharmacy consumers are predominantly women, who account for between 60 and 80% of customers (Hassell et al. 1999). Women tend to prefer advice given by pharmacists rather than self-treatment options, which are more popular with men (Hassell et al. 1999; Bell et al. 2000). Research has shown that consumers under the age of 60 are also more likely to seek self-care options when faced with minor ailments, so they are more likely to seek guidance from a pharmacist than a GP (Bell et al. 2000). This could be an area of potential growth and development for community pharmacy but this market is traditionally difficult to access. Consumer satisfaction is an important measure for pharmacy (Whitehead et al. 1999). Its intangible nature makes it a challenging measure to capture but it indicates loyalty to a specific pharmacy. Once loyal, research has suggested that a consumer will only seek an alternative pharmacy after approximately three negative experiences. The initial decision to use one pharmacy over another is generally accepted as being convenience “followed by “like the pharmacist,” “price” and a lot of “pharmaceutical service”” (Whitehead et al. 1999 p.72). By monitoring customer satisfaction, pharmacy performance can be improved and developed over time.
1.7.2 GP interactions Much of the negativity surrounding extended service offering in pharmacy has come from the medical profession. Research found that medical practitioners believed pharmacists could help improve patient care by:
[Helping to refine] dose regimen Identifying and resolving side effects Improving knowledge and understanding of medication Practical assistance with compliance and the provision of medication profiles to
consumers (March et al. 1999 p.227)
The threat of “turf-wars”, however, needs to be carefully managed by all health care professionals (March et al. 1999). The need to maintain good relationships with GPs in Australia spurred a pilot program encouraging formalised interaction between pharmacists and GPs (Chen et al. 1999). Insufficient communication between the two groups was fuelled by the pharmacists’ lack of confidence when communicating with practitioners and the lack of trust practitioners have in the clinical knowledge of pharmacists (Ranelli and Biss 2000). The Australian model enabled the collaboration of these two groups through a structured and government-funded support system and showed that effective communication could help promote CPS (Chen et al. 1999).
© Change Management and Community Pharmacy Project 92

Section 3: Exploring the Pharmacists’ World
1.8 Conclusion The above targeted pharmacy literature review has provided a broad overview of literature relevant to change in the profession and the various forces that affect service offerings in community pharmacy internationally. It can be seen from this review of the literature that to date there has not been a national change management program that assists pharmacists with the implementation of new services and that there has been only limited emphasis on strategic planning and business strategies for pharmacies. This area, however, is beginning to be developed in Australia through groups such as the Pharmacy Practice Foundation (The Pharmacy Practice Foundation 2004). This report aims to fill this gap by providing a change implementation plan for community pharmacy in Australia at the levels of the industry context, the individual pharmacy or pharmacy network and the pharmacist. The following chapter lays the foundation for this by examining how the research methods we have used to fill this gap in the literature and to provide evidence needed to define the necessary steps in a comprehensive change management program for community pharmacy.
© Change Management and Community Pharmacy Project 93
Section 3: Exploring the Pharmacists’ World
Section 3: Chapter 2
2 Research Methodology
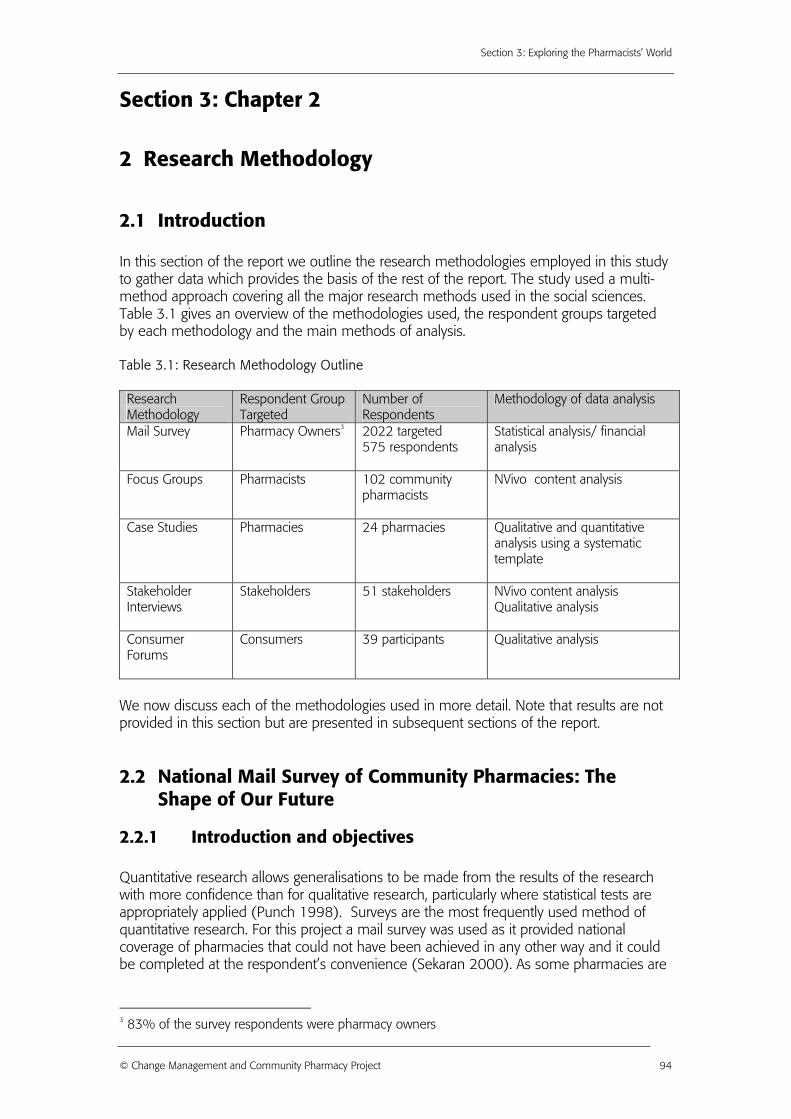
2.1 Introduction In this section of the report we outline the research methodologies employed in this study to gather data which provides the basis of the rest of the report. The study used a multi-method approach covering all the major research methods used in the social sciences. Table 3.1 gives an overview of the methodologies used, the respondent groups targeted by each methodology and the main methods of analysis. Table 3.1: Research Methodology Outline Research Methodology
Respondent Group Targeted
Number of Respondents
Methodology of data analysis
Mail Survey Pharmacy Owners3 2022 targeted 575 respondents
Statistical analysis/ financial analysis
Focus Groups Pharmacists 102 community pharmacists
NVivo content analysis
Case Studies Pharmacies 24 pharmacies Qualitative and quantitative analysis using a systematic template
Stakeholder Interviews
Stakeholders 51 stakeholders NVivo content analysis Qualitative analysis
Consumer Forums
Consumers 39 participants Qualitative analysis
We now discuss each of the methodologies used in more detail. Note that results are not provided in this section but are presented in subsequent sections of the report.
2.2 National Mail Survey of Community Pharmacies: The Shape of Our Future
2.2.1 Introduction and objectives Quantitative research allows generalisations to be made from the results of the research with more confidence than for qualitative research, particularly where statistical tests are appropriately applied (Punch 1998). Surveys are the most frequently used method of quantitative research. For this project a mail survey was used as it provided national coverage of pharmacies that could not have been achieved in any other way and it could be completed at the respondent’s convenience (Sekaran 2000). As some pharmacies are
3 83% of the survey respondents were pharmacy owners
© Change Management and Community Pharmacy Project 94
Section 3: Exploring the Pharmacists’ World
not on-line, mail surveys (rather than online surveys) have to date been the main survey research approach used to study community pharmacy. The specific objectives of the mail survey were to:
Provide an assessment of the current services offered by community pharmacies; Identify current business strategies adopted by community pharmacies and obtain
an initial categorisation into the Pharmacy Viability Matrix; Identify the sources of information found useful when looking to implement new
pharmacy services and the importance of certain factors in this decision; Explore the role and influence of networks and banner groups; Investigate some of the attitudes to change and the role of the Guild in the
change process; Obtain relevant financial data to enable economic and business modelling for
comparing the case studies to the mail survey; and Determine views of the future for community pharmacy.
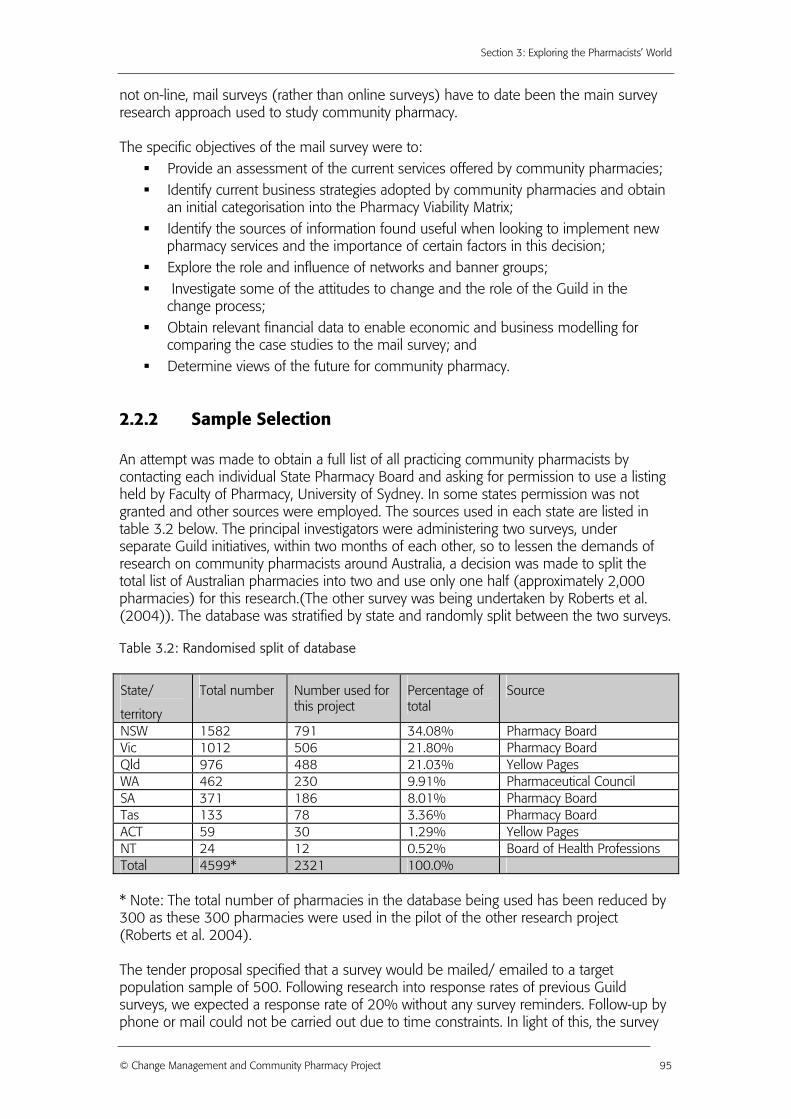
2.2.2 Sample Selection An attempt was made to obtain a full list of all practicing community pharmacists by contacting each individual State Pharmacy Board and asking for permission to use a listing held by Faculty of Pharmacy, University of Sydney. In some states permission was not granted and other sources were employed. The sources used in each state are listed in table 3.2 below. The principal investigators were administering two surveys, under separate Guild initiatives, within two months of each other, so to lessen the demands of research on community pharmacists around Australia, a decision was made to split the total list of Australian pharmacies into two and use only one half (approximately 2,000 pharmacies) for this research.(The other survey was being undertaken by Roberts et al. (2004)). The database was stratified by state and randomly split between the two surveys. Table 3.2: Randomised split of database
State/
territory
Total number Number used for this project
Percentage of total
Source
NSW 1582 791 34.08% Pharmacy Board Vic 1012 506 21.80% Pharmacy Board Qld 976 488 21.03% Yellow Pages WA 462 230 9.91% Pharmaceutical Council SA 371 186 8.01% Pharmacy Board Tas 133 78 3.36% Pharmacy Board ACT 59 30 1.29% Yellow Pages NT 24 12 0.52% Board of Health Professions Total 4599* 2321 100.0% * Note: The total number of pharmacies in the database being used has been reduced by 300 as these 300 pharmacies were used in the pilot of the other research project (Roberts et al. 2004). The tender proposal specified that a survey would be mailed/ emailed to a target population sample of 500. Following research into response rates of previous Guild surveys, we expected a response rate of 20% without any survey reminders. Follow-up by phone or mail could not be carried out due to time constraints. In light of this, the survey
© Change Management and Community Pharmacy Project 95
Section 3: Exploring the Pharmacists’ World
was sent to the maximum possible pharmacy respondents available, i.e. the 2001 pharmacies on the database. The number of usable responses from the pilot and final survey was 575, representing a response rate of 28.4%.
2.2.3 Survey Design The survey was structured in order to gain the most genuine responses from respondents. It is argued that respondents who feel comfortable with what the survey is asking them will answer the questions with a true indication of their attitudes and opinions (Malhorta et al. 2000). A copy of the questionnaire is shown in appendix 3. The survey used a variety of question styles with a Likert Scale of 5 points, 3 open-ended questions and the remainder dichotomous variable questions. The survey was separated into five sections and the topics covered in each section are outlined here:
Section 1 o About you and your pharmacy: These questions gathered data on the
demographic characteristics of the respondent and their pharmacy. The survey findings were compared to other Australian survey findings so that a financial analysis could be completed
o Business strategies: This was a self-categorisation tool that placed respondents in one of the four business strategy types proposed by Miles and Snow (1978): prospector, analyser, defender or reactor. Respondents also selected statements to allow them to be placed in one of the four Pharmacy Viability Matrix models (outlined in section 4 chapter 2)
o Pharmacy networks: Here respondents were asked to outline their involvement with formal or informal pharmacy networks and the influence these networks have on their business
Section 2: o Change in the pharmacy: This examined the various sources of
information that were most useful to pharmacists, the factors that influence pharmacists’ decisions to implement a service and various aspects relating to change in pharmacy.
Section 3: o Service adoption: This section asked pharmacists:
What enhanced services they offered (where “enhanced services” includes those services requiring additional or special skills, knowledge and/or facilities in community pharmacies. This was consistent with the wording of Berbatis et al. (2003))
If they did not currently offer the specific service, were they planning to adopt it over the next 12 months?
Was the customer charged for the service? Was there a specially trained pharmacist or other trained personnel
to provide the service? How satisfied they were with the program/service they offered (on
a scale of 1 to 5, where 1=very dissatisfied and 5=very satisfied)? What was their perception of the profitability of the particular
service (on a scale of 1 to 5, where 1=low profitability and 5=high profitability)?
What was their perception of the take-up rate by customers (on a scale of 1 to 5, where 1=low take-up and 5=high take-up rate)?
© Change Management and Community Pharmacy Project 96
Section 3: Exploring the Pharmacists’ World
Section 4: o Financial Information 2003-2004: This covered various financial
questions for the last financial year. These statistics were used in the financial modelling of the mail survey results. All financial questions were devised by Medici Capital.
Section 5: o The future of pharmacy: Respondents were asked to indicate their level
of agreement or disagreement with a variety of changes relating to the future of the pharmacy profession.
o Open questions: There were also three open ended questions asking: In order of priority, list three critical issues you will need to manage
in your pharmacy in the next 3-5 years In order of priority, list three reasons why you would implement a
new service One key piece of advice to give to a pharmacist looking to
implement a new service.
2.2.4 Survey Pretesting The survey was pre-tested with 15 pharmacy professionals who were well-known to members of the project team to assess the appropriateness of the survey’s language and the time taken to complete the questionnaire. Feedback from the pre-test was discussed and changes were made to the format and order of the questions for the survey pilot.
2.2.5 Pilot Survey In September 2004, a pilot questionnaire was sent to a sample of 299 community pharmacies. An online random number generator was used to select this sample from the original study sample of 2321 community pharmacies. After analysing the pilot data, minor changes were made to question order and language. A full copy of the mail survey can be found in appendix 3.
2.2.6 Main Survey - Data Collection In October 2004, a randomly selected sample of 2022 pharmacies across Australia was sent the questionnaire addressed to the Pharmacist-in-charge. Although Pharmacy Owners were the target group for this survey, the letters were addressed to the Pharmacist-in-charge and a note was placed inside to clarify that the survey was best completed by the Pharmacy Owner but in their absence it could be completed by the Pharmacist-in-charge. No formal reminders were sent due to time constraints but an article about this research project was published in Community Pharmacy (a newsletter published by the Guild) with a reminder note two weeks after the survey had been mailed. A request was also placed on website http://www.auspharmlist.net.au at the time of the Community Pharmacy publication reminding survey recipients to complete the questionnaire. In addition, a website was developed for the project with an electronic version of the questionnaire available for pharmacists in the sample to participate in the survey online. 403 surveys were received from the first mailout, and included in the draft final report. The survey was resent to non-respondents in early November, with an additional 172 completed surveys received.
© Change Management and Community Pharmacy Project 97
Section 3: Exploring the Pharmacists’ World
2.2.7 Main Survey - Data Analysis In total, 575 useable survey responses were received after two mailouts. Once the completed questionnaires were received, the data was entered into Excel and then transferred to SPSS Version 11. The initial analysis was completed by an external consultant and verified by the project team. The final analysis was completed by the project team. The second analysis was consistent in findings with the initial analysis. The detailed findings of the final analysis can be found in full in appendix 3 and are also repeated where relevant in other parts of the Report. The offering of the enhanced services and other consistent variables were compared against those measured in Berbatis et al. (2003). The financial data were processed and analysed by Medici Capital.
2.2.8 Survey Limitations Similar to previous surveys investigating cognitive or enhanced services, there is variation in how to interpret “services” and what is actually being provided when pharmacists indicate they are providing the service. One of the limitations in the survey methodology was the difficulty in knowing how pharmacists interpreted the delivery of services. For example, whilst smoking cessation services may provide the opportunity to offer a service to consumers, some respondents may interpret this “service” offering as selling products related to smoking cessation while others may interpret it as offering substantial information and advice and an individually tailored self-management program for the consumer. One of the limitations of using a survey approach is that we are entirely dependent on respondents’ personal views, in this case as to what constitutes a ‘service’. Due to the large number of services listed, the description of the service on the survey form was limited to the title of the service, and did not provide a detailed behavioural definition of what offering the service involves. Consequently, the interpretation of what the service entailed was determined subjectively by the respondent. These issues arise from the limitations of survey methodology as a research tool. There is always a choice to be made between obtaining a broad coverage of issues versus achieving depth and specificity. If we had chosen to explore a single service, such as asthma management, we could have more closely specified various levels of service offering. However we chose to look at the provision of a range of services to acquire a broad coverage and to use a variety of other research methodologies (e.g. case studies and interviews) to explore in more depth what service provision means in practice.
2.2.9 Conclusion The results from the survey conducted have been integrated in throughout the report. The following sections contain some discussion of the mail survey as analysed by either the Change Management and Community Pharmacy research team or Medici Capital:
Section 4: Analysis of Current and Future Service Offerings Section 4: Analysis of the Pharmacy Viability Matrix from the Mail Survey Section 5: Change Readiness Wheel Appendix 3: Mail Survey Results
© Change Management and Community Pharmacy Project 98

Section 3: Exploring the Pharmacists’ World
2.3 Focus Group Methodology
2.3.1 Introduction A series of ten focus groups was held with Australian community pharmacists as the initial research stage of the project. Focus groups are an invaluable method for obtaining in-depth information in a short time. Consequently these discussions with groups of pharmacists were positioned as a discovery, or an exploratory process by which the remainder of the research project was shaped. The overall aim of this stage of the research was to use the focus groups as a way to sensitise the researchers and determine pharmacists’ perceptions of the state of professional services offered within community pharmacy and the future of the industry. In using this as a way of exploring the pharmacy industry, the research team has allowed the views of the pharmacists “on the ground” to influence the direction of the research and to help formulate valid and relevant research questions. The views of the pharmacists who participated and the overall findings of the focus groups were also compared to previous research projects funded by the Pharmacy Guild to ensure continuity of research design (Berbatis et al. 2003; Roberts et al. 2004).
2.3.2 Focus Group Objectives The stated objectives of the focus groups were:
To determine some of the perceived facilitators and barriers in implementing services;
To determine what pharmacists consider to be successful versus unsuccessful implementation of services;
To determine the perceived future of the pharmacy industry and Cognitive Pharmacy Services ;
To highlight innovative concepts within the current context of pharmacy; To identify the potential problems that emerge in the process of implementing
services; To uncover the community pharmacists’ perceptions of the pharmacy associations
and their place within the pharmacy industry; To learn the “language” that pharmacists use when discussing the provision of
services and the generally accepted rhetoric within the industry; and To obtain key themes to help design the subsequent survey.
The focus groups were used to acquaint the researchers with the issues that face community pharmacists in Australia today and to ensure that the subsequent research addressed pharmacists’ concerns.
© Change Management and Community Pharmacy Project 99
Section 3: Exploring the Pharmacists’ World
2.3.3 Methodology Focus groups are a frequently used form of qualitative research for a variety of disciplines (Stewart and Shamdasani 1990). A focus group is defined as a group that “generally involves 8 to 12 individuals who discuss a particular topic under the direction of a moderator who promotes interaction and assures that the discussion remains the topic of interest” (Stewart and Shamdasani 1990, p. 10).
2.3.4 Format of the session Two independent facilitators contracted by the University of Technology, Sydney moderated the focus groups. Ms Catherine Smithson from “being human” and Dr Angela Todd from the Sydney Health Projects Group are both experienced focus group facilitators aware of the challenging issues involved in focus groups. At nine of the ten sessions a research team member was also present as an observer. This method was used to maintain the quality and consistency of the focus groups across locations and between facilitators. The facilitators began each session by stating the objectives of the session and outlining the research project for which it was being conducted. In order to achieve these objectives a question guide for facilitators was developed covering the following topics:
the services that had been implemented, implemented and discontinued, or never considered in community pharmacy;
the motivators for change and reasons why services were implemented; the enablers and barriers to change; and the way pharmacists think about new initiatives and how they perceive the future
of pharmacy. The complete script as used by the facilitators is shown in appendix 4. The independent facilitators who ran the focus groups encouraged a diversity of opinions and a sharing of experiences during group sessions. This approach developed general information on the pharmacy industry across a variety of locations in Australia. The rich qualitative data gathered in the focus groups was supplemented by a brief questionnaire that all participants were asked to complete. This questionnaire, as shown in appendix 4, gathered basic demographic information on participants and more detailed information on the services that may or may not have been implemented in community pharmacies. This analysis of the services being implemented in community pharmacy was similar to a previously conducted national survey (Berbatis et al. 2003). This questionnaire was used to gain a more systematic understanding of the services the focus group participants were involved in and as a stimulus for discussion. The proposed outcomes for the focus groups were:
Listing of what services are offered at the pharmacies represented in the focus groups;
An understanding of why they have been implemented or why they have not been implemented – motivational drivers versus barriers;
© Change Management and Community Pharmacy Project 100
Section 3: Exploring the Pharmacists’ World
An understanding of how the services have been implemented – so that some initial assessment could be made of the pharmacists’ capabilities for change management and what has hindered/helped the implementation process;
Listing of potential future services which might be offered.
2.3.5 Recruitment of Participants Participants in the focus groups were community pharmacists at different stages of their careers. All were still currently involved in pharmacy in some way, although a small number of participants no longer worked as community pharmacists. Focus group meetings were held in capital cities and regional centres. Locations were decided after talking to professional associations in each state and were selected on the basis of offering a relatively central location for most participants, availability and cost. Names of potential participants were gathered from the Guild/Government Third Agreement Co-ordinators (TACs) in each state and the Guild MMR facilitators where appropriate. These names were supplemented by additional pharmacists listed in the Yellow Pages. This was done so as not to skew the pool of participants. Community pharmacists were contacted initially by telephone to assess their suitability for participation and willingness to be involved in the project. Approximately 400 calls to pharmacists were required to generate the final attendance of 102. Potential participants were given these reasons to attend:
opportunity to network with other pharmacists opportunity for information sharing with fellow pharmacists opportunity to learn how colleagues deal with implementing new services; what
hinders, what helps opportunity to think about change within their own pharmacy and to gain a
resulting competitive advantage. Finally, focus group participants were reimbursed $300 for their time.
2.3.6 Focus Group Locations The focus groups were conducted in locations across Australia (see figure 3.1). Due to time constraints, the majority of the focus groups were conducted on the east coast. Apart from Sydney, only one focus group was conducted in each location in order to increase the geographical coverage. In regional areas the majority of participants were local but an attempt was made to encourage pharmacists from one-pharmacy towns to participate. Pharmacists were offered accommodation and reimbursement of travel expenses. As a result, all regional focus groups included representative pharmacists from nearby smaller towns.
© Change Management and Community Pharmacy Project 101
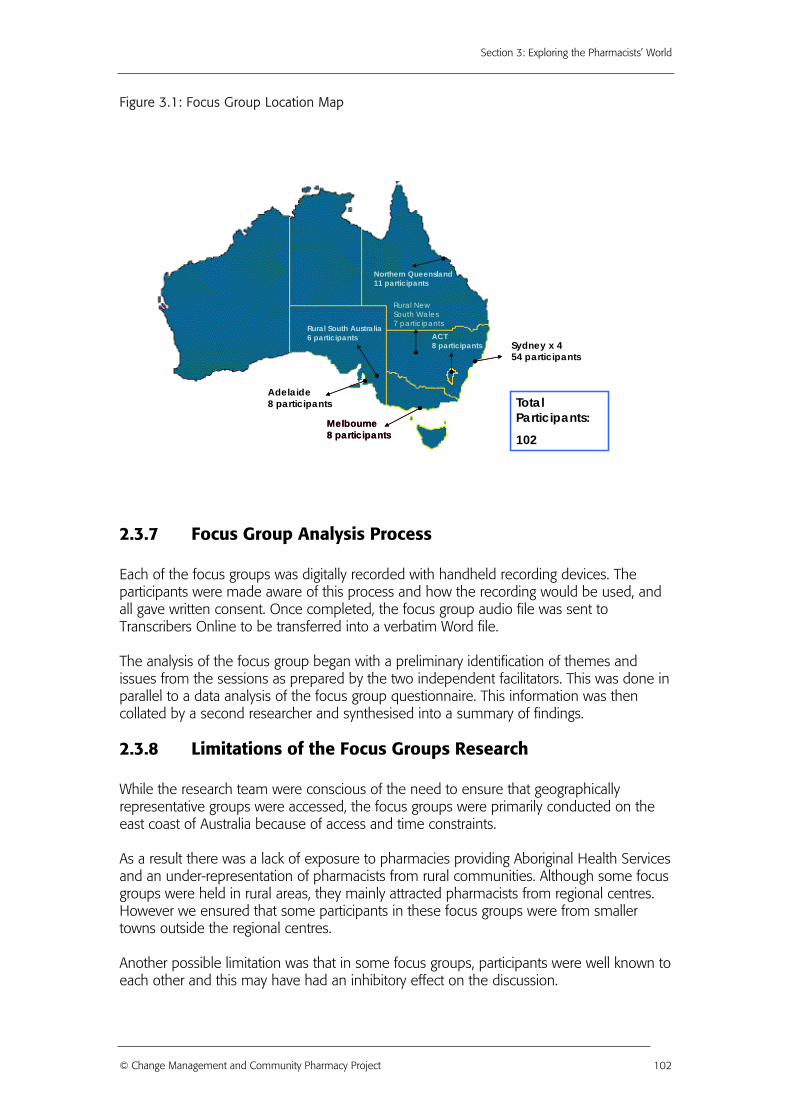
Section 3: Exploring the Pharmacists’ World
Figure 3.1: Focus Group Location Map
Northern Queensland11 participants
ACT8 participants
Rural New South Wales7 participantsRural South Australia
6 participants
Melbourne8 participants
Total Participants:
102Melbourne8 participants
Adelaide8 participants
Sydney x 454 participants
2.3.7 Focus Group Analysis Process Each of the focus groups was digitally recorded with handheld recording devices. The participants were made aware of this process and how the recording would be used, and all gave written consent. Once completed, the focus group audio file was sent to Transcribers Online to be transferred into a verbatim Word file. The analysis of the focus group began with a preliminary identification of themes and issues from the sessions as prepared by the two independent facilitators. This was done in parallel to a data analysis of the focus group questionnaire. This information was then collated by a second researcher and synthesised into a summary of findings.
2.3.8 Limitations of the Focus Groups Research While the research team were conscious of the need to ensure that geographically representative groups were accessed, the focus groups were primarily conducted on the east coast of Australia because of access and time constraints. As a result there was a lack of exposure to pharmacies providing Aboriginal Health Services and an under-representation of pharmacists from rural communities. Although some focus groups were held in rural areas, they mainly attracted pharmacists from regional centres. However we ensured that some participants in these focus groups were from smaller towns outside the regional centres. Another possible limitation was that in some focus groups, participants were well known to each other and this may have had an inhibitory effect on the discussion.
© Change Management and Community Pharmacy Project 102
Section 3: Exploring the Pharmacists’ World
It also became apparent during analysis that the participants were pharmacists who were more highly involved in service provision. Pharmacists with more experience in the implementation of services and with an interest in changes in community pharmacy were more likely to attend. However these participants were able to offer the researchers a better understanding of the various elements of service implementation. Those who had no experience in this area could provide little additional knowledge to build on recent research. In selecting case studies we endeavoured to offset these problems by choosing pharmacies in other areas and ensuring coverage of rural and urban and banner and independent pharmacies.
2.3.9 Conclusion The results from the focus groups that were conducted across Australia have been integrated in throughout the report. The following sections contain discussion of the focus groups as analysed by the Change Management and Community Pharmacy research team or Medici Capital:
Section 5: Change Readiness Wheel Section 5: Change Implementation Wheel Section 5: PharmInd Wheel Appendix 5: Focus Group Report
© Change Management and Community Pharmacy Project 103
Section 3: Exploring the Pharmacists’ World
2.4 Community Pharmacy Case Studies
2.4.1 Introduction The case study is a method of learning about a complex instance through extensive description and contextual analysis. Yin (1994) has recommended the use of a particular case-study protocol as part of a carefully designed research project that includes the following sections:
Overview of the project (project objectives and case study issues) Field procedures (credentials and access to sites) Questions (specific questions that the investigator must keep in mind during data
collection) Guide for the report (outline, format for the narrative)
(Yin 1994, p. 64) For this project twenty-four case studies were carried out across Australia. These case studies were descriptive, illustrating the situation in real Australian community pharmacies. Researchers were interested in the “how” and “why” in a real life context. The objective of this stage of the research project was to collect data about the business practices and financial viability of each business model that formed part of the Pharmacy Viability Matrix: Traditional Pharmacy, Expanded Pharmacy, Focused Speciality and Multi Speciality pharmacies (see section 4 chapter 2). The goal was also to identify the key components of each business model in the category of ownership, banner or independent, and by location, rural/regional or urban. Positive examples were preferred for selection as we were interested in studying best practice if possible. In addition, the selection of cases also offered the opportunity for a holistic understanding of the situation in general in community pharmacy in Australia. The case studies were conducted using a short questionnaire and an in-depth semi-structured interview. The goal of the interview was to create an opportunity for dialogue about the business practices in the case study pharmacy. The decision to implement or to discontinue services was also assessed. The principal interviewer was interested in procedures and policies developed by the pharmacy.
2.4.2 Methodology While case study research does not attempt to be statistically representative, as asserted by the major researchers in the field including Yin (1994), this does not mean that sampling is unguided. Cases must be selected to maximise what can be learned in the period of time available for the study. Sixteen sites were chosen because they fitted into the business models of the Pharmacy Viability Matrix. This purposive sampling aimed “to select information-rich cases for in-depth study to examine meanings, interpretations, processes and theory” (Ezzy and Liamputtong Rice 1999, p. 43). Pharmacies with a positive reputation were preferred as this was an opportunity to discuss best practice.
© Change Management and Community Pharmacy Project 104

Section 3: Exploring the Pharmacists’ World
A further eight case studies were identified as innovative business models (see section 4 chapter 5) and these were not restricted to any one business model in the Matrix. These cases were selected as an extreme sample, that is, as having “unusual or distinctive characteristics that illustrate the processes being examined” (Ezzy and Liamputtong Rice 1999, p. 43). The aim of this sample was to obtain a new perspective on more typical cases, particularly to identify potential new options for pharmacy in the future. The first stage of selection was based on advice from leading pharmacy professionals and pharmacy industry material, e.g., articles in Australian pharmacy journals. While it was not possible to represent all types of community pharmacies in the case studies, a range of rural and regional/urban and independent/banner pharmacies were selected as required by the project tender. The second stage of selection was based on a preliminary allocation of case studies to the Pharmacy Viability Matrix categories. Once potential case studies had been identified, the subjects were approached by telephone and invited to participate. Information about the project and the commitment required was sent out to the pharmacy owners. A questionnaire, including financial information, was also sent out to be completed by the pharmacy owners. A case study protocol was developed by the research team. The case study interviews were semi-structured interviews based on a question guide (see appendix 6). The participant was, however, given the opportunity to express their views on matters that extended beyond the set interview questions. This allowed the pharmacists to talk about their own experiences with implementing services, their solutions to problems and to provide insights into current pharmacy practices. The data considered in the development of the case study interview guide included (adapted from the Burke-Litwin Causal Model (Burke 2002)):
External Environment: The elements that are outside the pharmacy and influence the performance of the pharmacy.
Mission and Strategy: The focus and objectives of the pharmacy, and the way these aims will be achieved
Structure: How the pharmacy is arranged in relation to its particular functions and personnel placed in those areas
Management Practices: The way in which the manager of the pharmacy uses the physical and human resources available to achieve the goals of the business. This also incorporates the manager’s behaviour, eg. encouraging employees to take on new roles and to be innovative
Systems: The policies and procedures that assist with the efficiency of the working environment – covers areas such as Human Resource Management, information technology and reward systems within the pharmacy
Motivation: How one’s behaviour moves toward the goals and objectives of the pharmacy
Individual Needs and Values: The personal and psychological dimensions that validate a person’s actions or desires.
While these themes were used for gathering data they were reported under the heading that are outlining below. This was because in reporting the data the above headings were too specific and more generalised topic areas were identified for the final case study reporting process.
© Change Management and Community Pharmacy Project 105
Section 3: Exploring the Pharmacists’ World
2.4.3 Process After the preliminary contact, the case study site was visited by the principal interviewer. The case study site visits typically involved an in-depth interview with the pharmacy owner or manager and an observation of pharmacy operations. When the interview was not located at the pharmacy, the principal interviewer visited the location at another time. There was one instance where the case study pharmacy was not visited but photographs were provided by the pharmacy owner. In some cases short interviews were also conducted with senior pharmacy staff. Six of the initial case study interviews were conducted with two or more members of the research team. This was to ensure that the methodology being used was appropriate to meet the objectives of the project. Before commencing the interview, the full project objectives were outlined to the participant, permission was sought to record the interview and the participant completed a consent form approved by the Ethics Committee of UTS (see appendix 6). The audio recording of the interview was then transcribed and the case study was written up under the following headings:
Background Information: background details of the pharmacy, descriptions of customer groups, local competitors and an overview of the pharmacy’s product and service offering.
Customer Demographics: Australian Bureau of Statistics (ABS) demographics data for the area of the pharmacy’s location were analysed to determine population trends potentially influencing the pharmacy. The most recent figures that could be standardised for all areas from were from the 2001 Census.
Pharmacy Strategy: outlines the pharmacy’s strategic direction and the pharmacy’s higher “purpose”
Pharmacy Processes and Systems: outlines process and systems used, such as key roles in the pharmacy, reporting in the pharmacy, human resources management etc
Pharmacy Product and Service Offering: outlines the products and services currently available in the pharmacy
New Products and Services and the Implementation of Change: outlines the recent changes and future plans for service implementation in the pharmacy
Potential Limitations for Change Management: the issues that the pharmacy will need to address when considering change in the future
Key Learnings: the key issues that other pharmacists can learn from the case study
Financial Information: an analysis of the financial viability of 20 out of the 24 case studies. Four financial categories were used for this analysis: financial performance, cost structure, risk and indicative value. The following terms are used in the financial analysis for the case studies and are explained in brief here
o The Sample Index: The financial analysis and comparisons for each case study is based on a Sample score of 100 for all of the pharmacies used in the modelling. By using the Sample score as 100 and indexing the other measures to this we are able to compare all cases on a relative basis.
o The Australian Average: Each case study’s data is compared to the Australian average which is indexed to the Sample. This is based on the Guild Digest published by the Pharmacy Guild of Australia and Medici Capital data bases and is considered to provide an unbiased comparison or “benchmark”.
© Change Management and Community Pharmacy Project 106
Section 3: Exploring the Pharmacists’ World
o Financial Performance Score: The financial performance score is based on a model that uses turnover and prescription volumes as key variables.
o Cost Structure Score: The cost structure index is a composite of Cost of Goods Sold, Salaries and Rent as a percentage of turnover.
o Risk Score: Risk comprises Business and Operating Risk. Business risk takes account of Prescription Numbers, Prescription Percent (of turnover), Sales Growth and Sales Variability (an inverse relationship); operating risk take account of Prescription Numbers, Size of premises, Staff Hours and Trading hours.
o Indicative Value: The expected business value assuming normal operating cost ratio, given the measured contribution margin expressed as a percentage of Turnover.
2.4.4 Analysis The coding was undertaken using the computerised software package NVivo, specifically designed to assist with the content analysis of such qualitative data. By using a computer aided process of analysis the coding was simplified in that cross coding and referencing was more easily facilitated and monitored. The information from the case studies was coded by the themes of the Change Wheels (see section 5). An additional analysis was made of the case studies to determine the “ideal” characteristics of each model in the Matrix. These findings are discussed in section 4. The financial analysis was completed by Medici Capital and their role in this broad context was to: Part 1:
Assist in determining financial and other information to be obtained for all case studies and survey
Design and use of financial/economic models in order to assess profitability for different product-service delivery mixes including sales forecast, risk assessment, cost, financial performance and valuation
Conduct financial and economic analysis, including profitability analysis to develop and fully cost business models for first 2 case studies – the method for assessing the viability of these two cases to be applicable to other case studies carried out in Part 2 below
Provide model output with listing of assumptions Part 2:
Review and refine model to format applied to remaining 22 case studies Assist (where feasible) with data collection for up to additional 22 cases, or use
information provided to further develop and fully cost business models for up to additional 22 case studies
Test models, highlighting: o Profitability o Impact on pharmacy financial and operational risk model viability; o Impact on pharmacy valuation; o Cost/benefit analysis;
Provide a summary of the analysis.
© Change Management and Community Pharmacy Project 107
Section 3: Exploring the Pharmacists’ World
Outcomes of the modelling and analysis included: Interpretation of different product/service mixes Identification of profitability and the costs and benefits of a move towards a
product/service model; and Translation of these benefits into financial outcomes and catalysts for business
change (change triggers).
2.4.5 Limitations A possible research limitation was the purposive sample of case studies. The research results show that these cases are not representative of the full diversity of the population of Australian pharmacies. They were not intended to be, but rather to represent the business strategies in the Pharmacy Viability Matrix and to provide examples of innovative pharmacies. We also sought to find best practice examples. Although case studies are a valid form of qualitative data analysis for descriptive purposes, the majority of these case studies were based on a single interview with a pharmacy owner or manager. As the owner or the manager, the participant expressed a particular interpretation of the pharmacy’s business practices and change strategies. Different issues and interpretations may have been obtained from other pharmacy staff members but this was not also possible due to time limitations. The availability of participants was another limitation. Although all participants were willing to take part in the research, time constraints at times prevented more in-depth examination of the pharmacy which may have added to the value of the illustrative case study.
2.4.6 Conclusion The results from the case studies have each been reported in four page documents that profile the participating pharmacy. The findings from these have been analysed by either the Change Management and Community Pharmacy research team or Medici Capital. The findings are integrated within the report in various sections:
Section 4: Case Study Reports (the individual case studies can be found in this section of the report)
Section 4: Innovation in Pharmacy Section 5: Change Readiness Wheel Section 5: Change Implementation Wheel Section 5: PharmInd Wheel
© Change Management and Community Pharmacy Project 108
Section 3: Exploring the Pharmacists’ World
2.5 Stakeholder Interview Methodology
2.5.1 Introduction and objectives As a requirement of the project proposal, 51 formal interviews were conducted with representatives of stakeholder groups across Australia. The objective of this stage of the research was to identify the internal and external factors that impact on the ability of community pharmacy to effectively deliver various services. The stakeholder interviews were conducted to provide insights into the views and objectives of major players in the pharmacy profession as well as external groups with an interest in the changes in community pharmacy. By going beyond the information contained in available documents and previous research in the area, these in-depth interviews explored the views of stakeholders on the strengths and weaknesses of community pharmacy, sought opinions on alternative methods of achieving objectives and canvassed potential future opportunities.
2.5.2 Methodology
“Interviewing is rather like marriage: everybody knows what it is, an awful lot of people do it, and yet behind each closed front door there is a world of secrets”
(Oakley 1981, p. 31) Traditionally an interview is seen as ‘a specialised pattern of verbal interaction – initiated for a specific purpose, and focussed on some specific content areas, with consequent elimination of extraneous material’ (Kahn & Cannell 1957 as referenced in Oakley 1981, p. 33). It can also be considered a form of conversation between a seeker of knowledge and an interpreter of reality (Kvale 1996). This stage of the project involved seeking the views and opinions of a range of community pharmacy’s key stakeholders and partners through a series of focussed interviews. This method encourages openness to the research process as this form of interview is “neither an open conversation nor a highly structured questionnaire” (Kvale 1996, p. 27). During the interview process, however, it is important to be wary of the content of interviewee responses. The respondent is aware of being observed and analysed by what they are saying and may, therefore, alter the representation of themselves and the images through which they identify in the data collection method. Gillman (2000, p. 94) highlights the ambiguity of the congruence between a person’s beliefs and their actual behaviour. He states that “[w]hat people say in an interview is not the whole picture; adequate research and, in particular, adequate theorizing, needs to take account of that”. This is addressed as a potential limitation of the research methodology.
2.5.3 Process From the beginning of the project, key partners and stakeholders were recorded from a listing of the Guild’s strategic alliance partners (PharmIntercom 2003). This was further developed with information provided from key Guild members or other pharmacy profession or industry contacts.
© Change Management and Community Pharmacy Project 109
Section 3: Exploring the Pharmacists’ World
The stakeholders came from a range of backgrounds with a strong interest or involvement in various aspects of community pharmacy in Australia. This list of 120 potential interviewees was then assessed by the project’s Steering Committee. These key stakeholder groupings were pharmacy organisations, consumers and consumer groups, pharmacy schools, patient support organisations, regulatory and other industry bodies, other health care providers, rural associations and pharmacists, retail competitors and wholesalers. Each stakeholder was approached initially by telephone or email and information about the research project was sent. Interviewees signed a consent form before each interview (see appendix 7). The interviewees were also asked for permission to record the interviews and de-identification of any comments was assured. The interviews were semi-structured which allowed the questions to be tailored to the experience and circumstances of individual stakeholders. The focus of the interviews varied depending upon the interest and expertise of the interviewee. A copy of the general stakeholder interview schedule is given in appendix 7. The majority of the interviews were conducted face to face and generally lasted an hour to an hour and a half. Four of the interviews were conducted by telephone where it was not possible to arrange a face to face meeting. By the end of the research fieldwork period, it had been possible to arrange fifty-one interviews (with fifty-nine interviewees) out of the original list of eighty-three key partners and stakeholders identified by the researchers. Many more were contacted and either declined to be interviewed or were unavailable. There were additional informal discussions conducted opportunistically by the principal investigators during this period. However, those who were interviewed represented a good cross-section of the various categories of stakeholders and demonstrated a range of different interests and perspectives. It also became apparent that there were a number of key themes emerging from the interviews and it was uncertain whether conducting many more interviews would have added substantially to the final research findings. Interviews were recorded and transcribed into Word documents. As a quality assurance process, each audio file was re-checked by the researchers. The key stakeholder interviews were de-identified, coded and analysed using the computerised software package NVivo, specifically designed to assist with the content analysis of such qualitative data. By using a computer aided process of analysis the process of coding was simplified in that cross coding and referencing was more easily facilitated and monitored (Coffey and Atkinson 1996). The information from the stakeholder interviews informed the PharmInd and Pharmacy Change Readiness and Implementation Wheels (see section 5) and was coded by themes.
2.5.4 Limitations These interviews with key partners and stakeholders took a great deal of time and energy during the research period. Initial contact and setting up of appointments was a time consuming process. Due to time constraints, some potential interviewees were unable to participate.
© Change Management and Community Pharmacy Project 110

Section 3: Exploring the Pharmacists’ World
2.5.5 Conclusion The results from the stakeholder interviews have been integrated predominantly in section 5 of this report. More specifically discussions from the interview findings can be found in:
Section 5: Change Readiness Wheel Section 5: Change Implementation Wheel Section 5: PharmInd Wheel (see Health and Allied Stakeholders section for a more
detailed discussion)
© Change Management and Community Pharmacy Project 111
Section 3: Exploring the Pharmacists’ World
2.6 Consumer Forum Methodology As discussed under Focus Groups – Pharmacists (2.4 of this section) a focus group is a frequently used form of qualitative research that provides a rich and detailed set of data about the perceptions, thoughts, feelings, and impressions of people in their own words (Stewart and Shamdasani 1990). A series of seven such focus groups were held with consumers or associated representative groups to discuss issues relating to their expectations of community pharmacy and any shortfalls around these expectations that they have experienced. Levels of satisfaction with pharmacy services were also canvassed. These groups were referred to as consumer forums to limit the confusion between these and the focus groups with pharmacists conducted earlier in the research project. Six consumer forums were conducted in Melbourne and Sydney with an additional teleconference linkup with health consumer representatives in rural and remote locations across Australia conducted from Canberra. The overall aims of the consumer forums were to determine the degree of consumer awareness and acceptance of professional services offered in community pharmacy and to obtain consumers’ views on the future of the industry. We were also interested in exploring consumers’ perceptions of the care provided within the pharmacy industry. The specific objectives were:
To understand some of the wider consumer related factors impacting upon practice change in pharmacies
To better understand the relationships amongst community groups and community pharmacies
To gain an understanding of the knowledge/awareness of cognitive pharmacy services within the community
To determine the needs – both present and future – of consumers/consumer groups that could be satisfied through pharmacy-provided services
To uncover consumers’ perceptions of the role of community pharmacists in the provision of enhanced health care services
Consumers participated as patients, carers and support group members. We were interested in exploring the views of both consumers’ and their associated representative group. For this reason, four of the consumer forums included people who are typically high pharmacy users, and three were conducted with community representative groups.
2.6.1 Recruitment of Participants When planning the forums, the research team identified consumer agencies that could assist with arranging the logistics including arranging the premises for the forums etc. Participants for the groups were recruited with the assistance of COTA (NSW), the Chronic Illness Alliance (Vic), Health Consumers of Rural & Remote Australia and the Mental Health Foundation (Vic). People with chronic conditions and their carers were invited to participate through these organisations. Consumer advocates or representatives were also recruited to voice the perspectives and concerns of a broader population of consumers. In some cases though,
© Change Management and Community Pharmacy Project 112
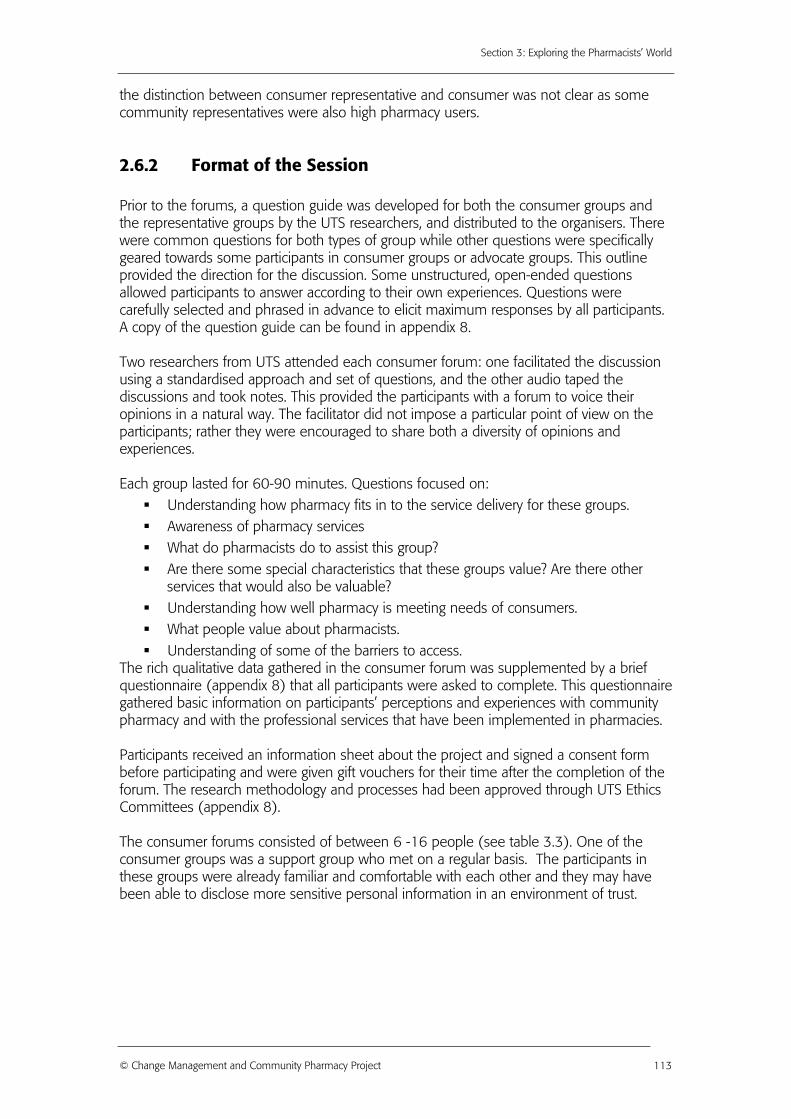
Section 3: Exploring the Pharmacists’ World
the distinction between consumer representative and consumer was not clear as some community representatives were also high pharmacy users.
2.6.2 Format of the Session Prior to the forums, a question guide was developed for both the consumer groups and the representative groups by the UTS researchers, and distributed to the organisers. There were common questions for both types of group while other questions were specifically geared towards some participants in consumer groups or advocate groups. This outline provided the direction for the discussion. Some unstructured, open-ended questions allowed participants to answer according to their own experiences. Questions were carefully selected and phrased in advance to elicit maximum responses by all participants. A copy of the question guide can be found in appendix 8. Two researchers from UTS attended each consumer forum: one facilitated the discussion using a standardised approach and set of questions, and the other audio taped the discussions and took notes. This provided the participants with a forum to voice their opinions in a natural way. The facilitator did not impose a particular point of view on the participants; rather they were encouraged to share both a diversity of opinions and experiences. Each group lasted for 60-90 minutes. Questions focused on:
Understanding how pharmacy fits in to the service delivery for these groups. Awareness of pharmacy services What do pharmacists do to assist this group? Are there some special characteristics that these groups value? Are there other
services that would also be valuable? Understanding how well pharmacy is meeting needs of consumers. What people value about pharmacists. Understanding of some of the barriers to access.
The rich qualitative data gathered in the consumer forum was supplemented by a brief questionnaire (appendix 8) that all participants were asked to complete. This questionnaire gathered basic information on participants’ perceptions and experiences with community pharmacy and with the professional services that have been implemented in pharmacies. Participants received an information sheet about the project and signed a consent form before participating and were given gift vouchers for their time after the completion of the forum. The research methodology and processes had been approved through UTS Ethics Committees (appendix 8). The consumer forums consisted of between 6 -16 people (see table 3.3). One of the consumer groups was a support group who met on a regular basis. The participants in these groups were already familiar and comfortable with each other and they may have been able to disclose more sensitive personal information in an environment of trust.
© Change Management and Community Pharmacy Project 113
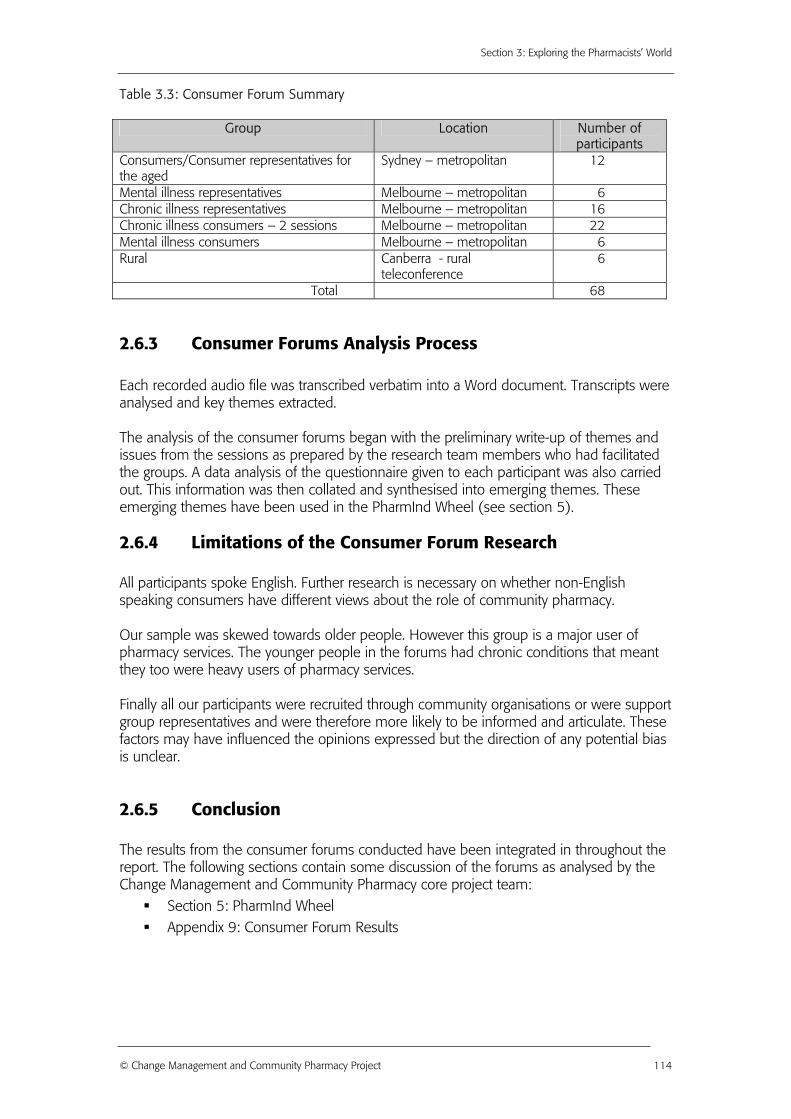
Section 3: Exploring the Pharmacists’ World
Table 3.3: Consumer Forum Summary
Group Location Number of participants
Consumers/Consumer representatives for the aged
Sydney – metropolitan 12
Mental illness representatives Melbourne – metropolitan 6 Chronic illness representatives Melbourne – metropolitan 16 Chronic illness consumers – 2 sessions Melbourne – metropolitan 22 Mental illness consumers Melbourne – metropolitan 6 Rural Canberra - rural
teleconference 6
Total 68
2.6.3 Consumer Forums Analysis Process Each recorded audio file was transcribed verbatim into a Word document. Transcripts were analysed and key themes extracted. The analysis of the consumer forums began with the preliminary write-up of themes and issues from the sessions as prepared by the research team members who had facilitated the groups. A data analysis of the questionnaire given to each participant was also carried out. This information was then collated and synthesised into emerging themes. These emerging themes have been used in the PharmInd Wheel (see section 5).
2.6.4 Limitations of the Consumer Forum Research All participants spoke English. Further research is necessary on whether non-English speaking consumers have different views about the role of community pharmacy. Our sample was skewed towards older people. However this group is a major user of pharmacy services. The younger people in the forums had chronic conditions that meant they too were heavy users of pharmacy services. Finally all our participants were recruited through community organisations or were support group representatives and were therefore more likely to be informed and articulate. These factors may have influenced the opinions expressed but the direction of any potential bias is unclear.
2.6.5 Conclusion The results from the consumer forums conducted have been integrated in throughout the report. The following sections contain some discussion of the forums as analysed by the Change Management and Community Pharmacy core project team:
Section 5: PharmInd Wheel Appendix 9: Consumer Forum Results
© Change Management and Community Pharmacy Project 114
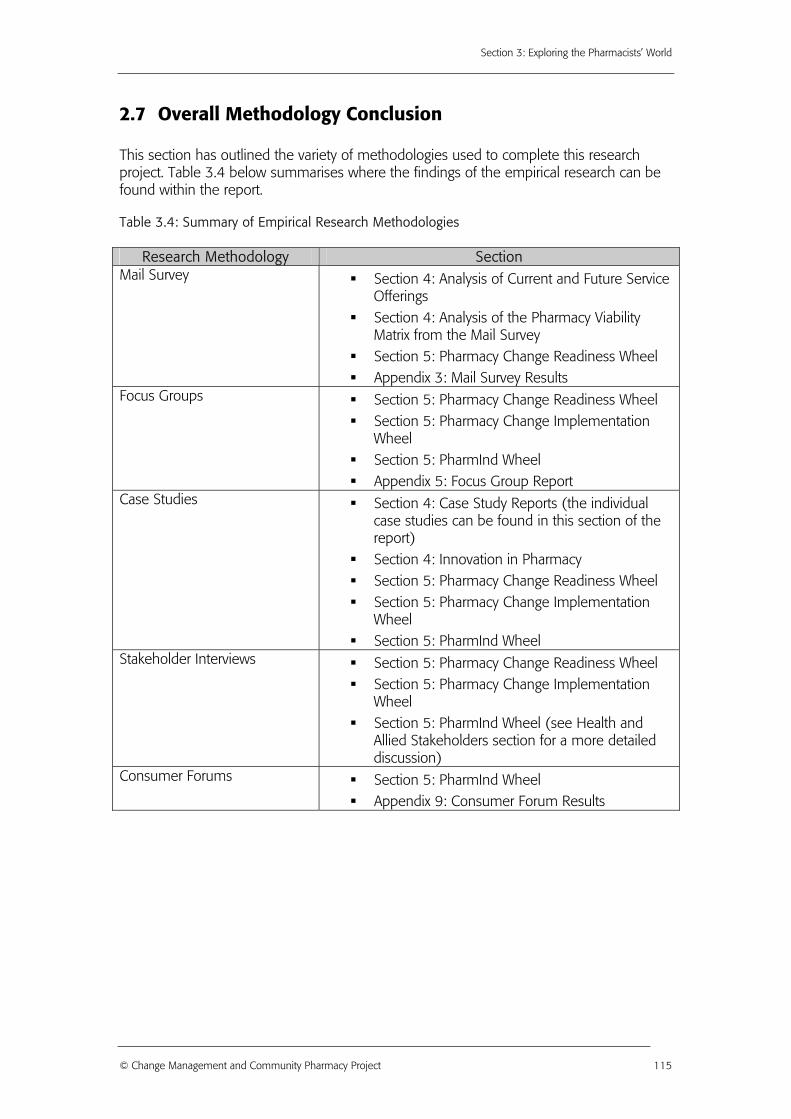
Section 3: Exploring the Pharmacists’ World
2.7 Overall Methodology Conclusion This section has outlined the variety of methodologies used to complete this research project. Table 3.4 below summarises where the findings of the empirical research can be found within the report. Table 3.4: Summary of Empirical Research Methodologies
Research Methodology Section Mail Survey Section 4: Analysis of Current and Future Service
Offerings Section 4: Analysis of the Pharmacy Viability
Matrix from the Mail Survey Section 5: Pharmacy Change Readiness Wheel Appendix 3: Mail Survey Results
Focus Groups Section 5: Pharmacy Change Readiness Wheel Section 5: Pharmacy Change Implementation
Wheel Section 5: PharmInd Wheel Appendix 5: Focus Group Report
Case Studies Section 4: Case Study Reports (the individual case studies can be found in this section of the report)
Section 4: Innovation in Pharmacy Section 5: Pharmacy Change Readiness Wheel Section 5: Pharmacy Change Implementation
Wheel Section 5: PharmInd Wheel
Stakeholder Interviews Section 5: Pharmacy Change Readiness Wheel Section 5: Pharmacy Change Implementation
Wheel Section 5: PharmInd Wheel (see Health and
Allied Stakeholders section for a more detailed discussion)
Consumer Forums Section 5: PharmInd Wheel Appendix 9: Consumer Forum Results
© Change Management and Community Pharmacy Project 115

© Change Management and Community Pharmacy Project 116