neuropathic pain section
TRANSCRIPT

NEUROPATHIC PAIN SECTION
Original Research ArticlePlacebo Response Changes Depending on theNeuropathic Pain Syndrome: Results of aSystematic Review and Meta-Analysispme_1340 575..595
M. Soledad Cepeda, MD, PhD,*Jesse A. Berlin, ScD,* C. Yuying Gao, MD, PhD,†Frank Wiegand, MD, PhD,‡ and D. Russell Wada,PhD†
*Janssen Research and Development, L.L.C.,Titusville, New Jersey;
†Quantitative Solutions, Inc., Menlo Park, California;
‡Janssen Global Services L.L.C., Raritan, New Jersey,USA
Reprint requests to: M. Soledad Cepeda, MD, PhD,Janssen Research and Development, L.L.C., 1125Trenton Harbourton Road, Office: E30001, Titusville,NJ 08560, USA. Tel: 609-730-2413; Fax:609-730-7927; E-mail: [email protected].
Financial disclosure: M. Soledad Cepeda and JesseBerlin are employees of Janssen PharmaceuticalResearch & Development, LLC. JanssenPharmaceutical Research & Development, LLC is anaffiliate of Ortho-McNeil-Janssen Pharmaceuticals,Inc, which markets several analgesic drug productsincluding opioids and over-the-counter analgesics.Frank Wiegand is an employee and shareholder ofJanssen Global Services LLC. During the conduct ofthe work described herein; C. Yuying Gao and D.Russell Wada were paid consultants to JanssenPharmaceutical Research & Development.
Abstract
Objective. To compare placebo responses inneuropathic pain syndromes.
Design. Systematic literature review and meta-analysis.
Setting and Patients. Randomized placebo-controlled trials assessing pain intensity or painrelief in any neuropathic pain syndrome publishedsince 1995 with �5 days follow-up.
Interventions. Placebo response.
Outcome Measures. Pain intensity and responderrates (proportion reporting �50% pain relief). Meta-regression models were built.
Results. Ninety-four studies (N = 5,317) wereincluded in the pain intensity analysis; 47 studies(N = 3,087) were included in the responder analysis.After controlling for potential confounders (e.g.,subject characteristics, study design characteris-tics), the placebo response was found to be largeand varied with the pain syndrome. Compared withdiabetic neuropathic/polyneuropathic pain (DPN),the placebo response for a decline in pain intensityand responder rate was smaller in trials thatassessed central pain and postherpetic neuralgia(PHN) and larger in trials that assessed HIV pain.The model-predicted mean decrease (95% confi-dence interval [CI]) from baseline in pain intensity(0–10 scale) was as follows: DPN, 1.45 (1.35 to 1.55);PHN, 1.16 (1.03 to 1.29); central pain, 0.44 (-0.41 to1.30); HIV pain, 1.82 (1.51 to 2.12). The predictedresponder rates (95% CI) were as follows: DPN, 20%(14.6 to 25.8); PHN, 11.5% (8.4 to 14.5); central pain,7.2% (2.1 to 12.3); HIV pain, 42.8% (34.9 to 50.7). Thetype of treatment in the active arm also influencedthe placebo response.
Conclusions. Placebo response is influenced bythe pain syndrome evaluated. These differencesshould be considered when evaluating novelcompounds for the treatment of neuropathic painconditions.
Key Words. Placebos; Anticonvulsants; Antide-pressants; NMDA Antagonists; Opioids; Post-Herpetic Neuralgia; Reflex Sympathetic Dystrophy;Risk Factors; Neuropathy
Introduction
A high placebo response has been identified as one of thestrongest factors that lead to failed clinical trials, evenwhen the active treatment has been previously shown tobe effective [1]. A better understanding of the factors thatinfluence placebo response in clinical trials could permitresearchers to design trials that may be more able to
bs_bs_banner
Pain Medicine 2012; 13: 575–595Wiley Periodicals, Inc.
575
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022

detect the benefit of efficacious treatments compared withplacebo.
Evaluations of the placebo response rates in painstudies have revealed that both subject and study char-acteristics may influence the observed response. In termsof subject characteristics, subject expectations are asso-ciated with a placebo response (i.e., the higher a subject’sexpectations, the higher the placebo response) and sub-jects who are highly adherent to the study medicationhave a higher placebo response than non-adherent sub-jects [2,3]. Although subjects with larger fluctuations inpain are more likely to have higher placebo responsesthan subjects with less variability in pain over time [4], theeffect of baseline pain intensity on the placebo response isnot yet clear. Some findings suggest that subjects withhigher baseline pain intensity have a significantly greaterreduction in pain intensity than subjects with lower base-line scores [5] while other findings suggest that the base-line pain intensity has no effect on the placebo response[6]. Gender does not seem to affect the placebo response[7]. In terms of study characteristics, a greater placeboresponse is generally observed in trials with longerfollow-up [8] and larger sample sizes [5], and parallel-group studies seem to have a higher placebo responsethan crossover studies [5].
Recent research suggests that the pain syndromes underevaluation may also affect the placebo response [5,9].Studies evaluating painful diabetic neuropathy have beenfound to have a higher placebo response than studiesevaluating postherpetic neuralgia [8,9]. These findingswere primarily based on an analysis of pain intensityreduction in the placebo arms of 58 studies [9]. The trialsincluded in that analysis assessed diabetic neuropathyand postherpetic neuralgia. Because only two pain syn-dromes and only pain intensity (not the responder rate)were evaluated, a more comprehensive comparison ofthe placebo response in studies evaluating neuropathicpain was conducted for the current analysis, using a sys-tematic review of the literature and meta-analysis of trialsthat assessed pain intensity or responder rates in anyneuropathic pain syndrome.
Methods
Data Sources and Study Selection
A systematic review of English-language articles was per-formed using MEDLINE and the ClinicalTrials.gov registryon November 16, 2010. Search terms included the fol-lowing: randomized controlled trial, diabetic neuropathy,postherpetic neuralgia, neuropath*, or neuralg*, carpaltunnel syndrome, phantom, postamputation, central pain,complex regional pain, trigeminal, reflex sympatheticdystrophy, polyneuropathy, postmastectomy, and post-thoracotomy. The search strategy used is described inAppendix 1.
Included studies were randomized, placebo-controlled,parallel-group or crossover studies published in 1995 or
later with at least 5 days of treatment exposure or follow-upthat reported pain intensity (on a 0–10 or a 0–100 scale) orresponder rate. Open-label studies were excluded.
The following information was extracted from each study:mean age; percentage of participants who were male;sample size; whether the study was parallel or crossover;number of arms; year of completion of the study; studydesign, conduct, and reporting information (was thestudy described as double-blind?, was the randomiza-tion scheme described?, was the allocation sequenceconcealed?, and was there a description of dropoutsand withdrawals?); treatment information (treatment drugclass) and route of administration; duration of follow-up;type of pain syndrome; mean pain intensity at baseline, atthe end of treatment, and mean change from baseline;and responder rate data, all in the placebo group only, andthe corresponding measures of variability.
Data Synthesis
Scales from 0 to 100 were converted to 0 to10.For crossover studies, only data from the first periodwere used, treating this first period as a parallel-groupcomparison.
To compare the placebo response in the variousneuropathic pain syndromes and to explain hetero-geneity of results among studies, random-effects meta-regression models were built, one for pain intensity andanother for responder rate (proportion of subjects whoreported at least 50% pain relief vs baseline pain intensity).Random-effects meta-regression is recommended overfixed-effects meta-regression because fixed-effects meta-regression leads to excessive false positives results in thepresence of heterogeneity [10].
Pain intensity was analyzed using a linear regressionmodel in two ways: mean final pain intensity and meanchange from baseline. Eighty percent of the studies thatreported mean change from baseline and 50% of the trialsthat reported mean final pain intensity did not report ameasure of dispersion. The standard deviations wereimputed using the average of the standard deviations ofthe trials that reported it [11]. The results of both analyseswere almost identical; the difference consisted in a slightlywider confidence interval in the change from baselineanalysis. Because the change from baseline is easier tointerpret, the results of that analysis are presented.
The various pain syndromes were grouped into the follow-ing categories: cancer-related neuropathic pain, centralneuropathic pain (induced by multiple sclerosis, spinalcord injury, stroke), diabetic neuropathic/polyneuropathicpain, human immunodeficiency virus (HIV)-associatedneuropathic pain, postherpetic neuralgia, phantom pain,posttraumatic/postsurgical/complex regional pain syn-drome (CRPS) pain, and neuropathic pain (when a mixtureof neuropathic pain syndromes was included in the trialand results were not reported separately).
576
Cepeda et al.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022

Because individuals’ expectations of treatment efficacycould affect the placebo response, the type of treatmentclass evaluated in the trial and the route of administrationwere included in the analysis. The treatments weregrouped into the following categories: opioids (e.g., mor-phine), antidepressants (e.g., amitriptyline), anticonvul-sants (e.g., gabapentin), sodium channel blockers (e.g.,lidocaine), N-methyl d-aspartate (NMDA) antagonists(e.g., ketamine), cannabinoids (e.g., sativex), combination(when the trial evaluated more than one of the aboveclasses), and nontraditional (to include miscellaneousmedications such as clodronate and levodopa). The routeof administration was grouped into intravenous and non-intravenous. Because subject characteristics and studydesign characteristics can affect the placebo response,the models also included the pain syndrome, mean base-line pain intensity, year of completion of the study, meanage of subjects in the trial, percentage of males in the trial,treatment duration of the trial, number of arms in the trial,treatment class in the active control group, whether infor-mation regarding dropouts was reported, and whether theplacebo was an “active placebo” (i.e., a placebo thatmimics the adverse effects of the experimental drug).
For the responder rate, the percentage of subjects whoreported at least 50% pain relief was analyzed because 47trials assessed this outcome compared with 34 trials thatevaluated the percentage of subjects who reported atleast 30% pain relief. Responder rate was treated as acontinuous outcome. To allow analyses of studies withzero events (i.e., in which none of the subjects reported�50% pain relief) and calculate approximate standarderrors, we added a constant—1/number of subjects in theplacebo arm to such studies. This is similar, in principle, toadding a continuity correction to studies with no events inone arm to calculate odds ratios or relative risk in meta-analysis. We used the reciprocal of the number of subjectsin the placebo group because this continuity correction isthe one that has been shown to exhibit less bias in meta-analysis of rare events [12], although that finding strictlyapplies to situations in which two treatment groups arebeing compared.
Because the number of studies that reported responderrate was fewer than the studies that reported pain inten-sity, the meta-regression model for responder rateincluded fewer covariates—active treatment assessed inthe active arm, age, baseline pain intensity and year ofpublication of the study.
Diabetic neuropathic/polyneuropathic pain and anticon-vulsants were used as the “reference” groups in theregression models because they were the most frequentlyoccurring groups.
After the random-effects meta-regression models werebuilt, we predicted the decrease in pain intensity and theresponder rate adjusted for all the variables in the regres-sion models, using the fitted values from the models. Wethen produced forest plots with the adjusted results usingthe fixed- and random-effects models to combine the
results by pain syndrome. The fixed-effects model givesmore weight to studies with large sample sizes and smallvariances and the random-effects models, by incorporat-ing into the weights the among-study heterogeneity, givesrelatively more weight to smaller studies. The results areidentical in the absence of heterogeneity, and the resultswill generally differ in the presence of heterogeneity. Wecalculated I2 statistics to quantify the heterogeneity. I2 isthe percentage of variation attributable to heterogeneity. I2
values higher than 50% suggest substantial heterogeneity.
The analyses were conducted with STATA version 10.1(StataCorp, College Station, TX, USA) using the“metareg,” “predict,” and “metan” commands.
Results
The searches provided 624 results; 251 full manuscriptswere reviewed and 141 trials met the inclusion criteria witha total of 6,239 subjects. The number of studies screened,assessed for eligibility, and included in the review withreasons for exclusion at each stage, is listed in Figure 1.
The characteristics of included studies are described inTable 1. The mean (standard deviation [SD]) age of sub-jects included in the trials was 57.1 (8.3) years. The meanproportion of males in the studies was 53%. The mean(SD) duration of follow-up of the studies was 7.8(7.0) weeks. The majority of the trials (93%) reported meanbaseline pain intensity, and 33% of the trials reportedresponder rates (Table 2).
The neuropathic pain syndrome most frequently evaluatedwas diabetic neuropathic/polyneuropathic pain (39.6% ofthe trials), and the least frequently evaluated was cancerrelated neuropathic pain (4.0% of the trials; Table 3). Anti-convulsants were the medications most commonlystudied (49.5% of the trials). The type of treatments evalu-ated varied with the pain syndrome evaluated. Forexample, the studies that assessed cancer neuropathicpain more often evaluated anticonvulsants. The studiesthat assessed phantom pain more commonly evaluatedNMDA receptors antagonists (Table 3).
In terms of study design and reporting features, 99.9% ofthe trials were double-blind, reported the scheme of ran-domization, and had the allocation concealed. Thirtypercent of the trials did not describe dropouts or withdraw-als. Therefore, only the description of dropouts and with-drawals variable was included in the regression models.
Pain Intensity
Ninety-four studies were included in the pain intensityanalysis, with a total of 5,317 subjects [13–106]. Themean (SD) baseline pain intensity was 6.3 (1.0). The unad-justed mean (SD) decrease in pain intensity from baselinewas 1.2 (1.0) units. The unadjusted mean decrease in painintensity from baseline for each of the pain syndromes,along with the corresponding number of trials and number
577
Type of Pain Influences Placebo Response
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022

of subjects included for each of the pain syndromes, canbe seen in Table 4.
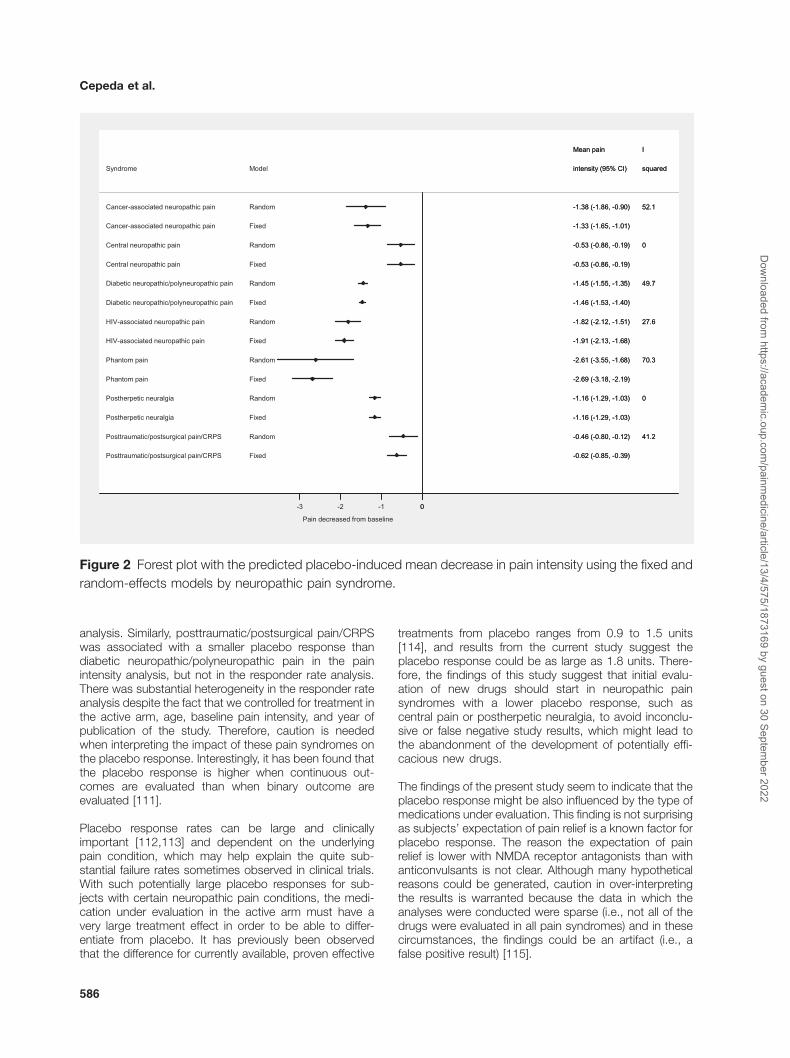
After adjusting for potential risk factors, the placeboresponse was statistically significantly smaller in trials thatevaluated central pain, posttraumatic/postsurgical pain/CRPS and postherpetic neuralgia than in the trials thatevaluated diabetic neuropathic/polyneuropathic pain. Onthe other hand, the placebo response was larger in trialsthat assessed HIV-associated neuropathic pain andphantom pain (Table 5).
These findings translate into a predicted placebo-inducedmean decline in pain intensity on a 0 to 10 scale in sub-jects with diabetic neuropathy of 1.45 units (95% confi-dence interval [CI], 1.35 to 1.55), 1.16 units (95% CI, 1.03to1.29) in subjects with postherpetic neuralgia, 0.53 (95%CI, 0.19 to 0.86) in subjects with central neuropathic painand 1.82 units (95% CI, 1.51 to 2.12) in subjects withHIV-associated neuropathic pain using a random effectmodel. The predicted placebo-induced mean decline inpain intensity was similar when the fixed-effects modelwas used to combine the results despite the
heterogeneity, although as expected, the CIs were nar-rower (Figure 2).
In terms of the effect of the type of drug on the placeboresponse, the trials that assessed NMDA blockers had asmaller placebo response (0.87 units smaller [95% CI,0.04 to 1.71]) than the trials that assessed anticonvulsants(Table 5).
Mean baseline pain intensity, mean age, gender, type ofplacebo used, description of dropouts and withdrawals,year of completion of the study and route of administrationdid not affect the placebo response.
Responder Rate
Forty-seven studies were included in the responderrate analysis, with a total of 3,087 subjects [13,15,16,18–22,27,30,31,34,35,38,41–43,48,49,52,53,55–61,64,66–68,70,79,81,84,92,93,95,96,99,100,106–110]. Theproportion of subjects who achieved at least 50% painrelief was on average 17%, but it ranged from 0% to 43%.
Figure 1 Flow of information through the different phases of the systematic review.
578
Cepeda et al.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022

Tab
le1
Cha
ract
eris
tics
ofin
clud
edst
udie
s
Stu
dyD
esig
nR
oute
ofA
dmin
istr
atio
nC
ondi
tion
Trea
tmen
t1
(Sub
ject
sR
ando
miz
ed)
Trea
tmen
t2
(Sub
ject
sR
ando
miz
ed)
Trea
tmen
t3
(Sub
ject
sR
ando
miz
ed)
Trea
tmen
t4
(Sub
ject
sR
ando
miz
ed)
Dou
ble
Blin
dR
ando
miz
atio
nA
ppro
pria
teA
lloca
tion
Con
ceal
edD
escr
iptio
nof
Dro
pout
s
Agr
awal
etal
.[3
7]C
ross
over
Ora
lD
PN
Pla
cebo
(24)
Gly
cery
ltrin
itrat
e(2
4)y
yy
nA
graw
alet
al.
[25]
Par
alle
lO
ral
DP
NP
lace
bo(2
1)G
lyce
rylt
rinitr
ate
(20)
Val
proa
te(2
0)G
lyce
rylt
rinitr
ate
+va
lpro
ate
(22)
yy
yn
Am
inan
dS
turr
ock
[109
]C
ross
over
Intr
aven
ous
DP
NP
lace
bo(2
0)A
man
tadi
ne(2
0)y
yy
nA
rbai
zaan
dV
idal
[40]
Par
alle
lIn
trav
enou
sC
ance
rne
urop
athi
cpa
in
Pla
cebo
(18)
Tram
adol
(18)
yy
yn
Are
zzo
etal
.[2
7]P
aral
lel
Ora
lD
PN
Pla
cebo
(85)
Pre
gaba
lin(8
2)y
yy
nA
tlian
dD
ogra
[55]
Par
alle
lO
ral
DP
NP
lace
bo(1
2)Z
onis
amid
e(1
3)y
yy
nB
acko
nja
etal
.[8
6]P
aral
lel
Ora
lD
PN
Pla
cebo
(81)
Gab
apen
tin(8
4)y
yy
yB
acko
nja
[83]
Par
alle
lO
ral
DP
NP
lace
bo(1
16)
Gab
apen
tin(1
13)
yy
yy
Ben
Abr
aham
etal
.[9
9]C
ross
over
Ora
lP
hant
omlim
bpa
inP
lace
bo(1
0)D
extr
omet
horp
han
(10)
Dex
trom
etho
rpha
n(1
0)y
yy
n
Bey
doun
etal
.[4
7]P
aral
lel
Ora
lD
PN
Pla
cebo
(89)
Oxc
arba
zepi
ne(8
3)O
xcar
baze
pine
(87)
Oxc
arba
zepi
ne(8
8)y
yy
n
Bon
eet
al.
[119
]C
ross
over
Ora
lP
hant
omlim
bpa
inP
lace
bo(1
9)G
abap
entin
(19)
yy
yn
Bou
reau
etal
.[9
4]P
aral
lel
Ora
lP
HN
Pla
cebo
(63)
Tram
adol
(64)
yy
yn
Bre
uer
etal
.[1
20]
Cro
ssov
erO
ral
Cen
tral
neur
opat
hic
pain
Pla
cebo
(12)
Lam
otrig
ine
(12)
yy
yn
Car
acen
ieta
l.[6
9]P
aral
lel
Ora
lC
ance
rne
urop
athi
cpa
in
Pla
cebo
(41)
Gab
apen
tin(8
0)y
yy
y
Che
net
al.
[18]
Par
alle
lIn
trav
enou
sP
HN
Pla
cebo
(20)
Asc
orba
te(2
1)y
yy
yC
hevi
lleet
al.
[26]
Cro
ssov
erTo
pica
lP
osttr
aum
atic
/po
stsu
rgic
alne
urop
athi
cpa
in
Pla
cebo
(14)
Lido
cain
e(1
4)y
yy
y
Chi
ou-T
anet
al.
[121
]C
ross
over
Ora
lC
entr
alne
urop
athi
cpa
in
Pla
cebo
(15)
Mex
iletin
e(1
5)y
yy
n
De
Gra
ndis
and
Min
ardi
[78]
Par
alle
lO
ral
DP
NP
lace
bo(1
66)
Leva
ceca
rnin
e(1
67)
yy
yy
Dog
raet
al.
[52]
Par
alle
lO
ral
DP
NP
lace
bo(7
7)O
xcar
baze
pine
(69)
yy
yy
Dow
det
al.
[98]
Par
alle
lTo
pica
lP
HN
Pla
cebo
(9)
Vin
cris
tine
(11)
yy
yy
Dw
orki
net
al.
[95]
Par
alle
lO
ral
PH
NP
lace
bo(8
4)P
rega
balin
(89)
yy
yy
Eis
enbe
rget
al.
[81]
Par
alle
lO
ral
DP
NP
lace
bo(2
6)La
mot
rigin
e(2
7)y
yy
yE
isen
berg
etal
.[4
4]P
aral
lel
Ora
lP
osttr
aum
atic
/po
stsu
rgic
alne
urop
athi
cpa
in
Pla
cebo
(10)
Am
anta
dine
(12)
yy
yn
Ert
aset
al.
[88]
Par
alle
lO
ral
DP
NP
lace
bo(1
1)Le
vodo
pa+
bens
eraz
ide
(14)
yy
yn
Fin
neru
pet
al.
[122
]C
ross
over
Ora
lC
entr
alne
urop
athi
cpa
in
Pla
cebo
(30)
Lam
otrig
ine
(30)
yy
yy
579
Type of Pain Influences Placebo Response
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
Tab
le1
Con
tinue
d
Stu
dyD
esig
nR
oute
ofA
dmin
istr
atio
nC
ondi
tion
Trea
tmen
t1
(Sub
ject
sR
ando
miz
ed)
Trea
tmen
t2
(Sub
ject
sR
ando
miz
ed)
Trea
tmen
t3
(Sub
ject
sR
ando
miz
ed)
Trea
tmen
t4
(Sub
ject
sR
ando
miz
ed)
Dou
ble
Blin
dR
ando
miz
atio
nA
ppro
pria
teA
lloca
tion
Con
ceal
edD
escr
iptio
nof
Dro
pout
s
Fin
neru
pet
al.
[20]
Cro
ssov
erO
ral
Cen
tral
neur
opat
hic
pain
Pla
cebo
(36)
Leve
tirac
etam
(36)
yy
yy
Fre
eman
etal
.[3
8]P
aral
lel
Ora
lD
PN
Pla
cebo
(153
)Tr
amad
ol(1
60)
yy
yy
Fre
ynha
gen
etal
.[5
7]P
aral
lel
Ora
lN
euro
path
icpa
inP
lace
bo(6
5)P
rega
balin
(141
)P
rega
balin
(132
)y
yy
yG
aler
etal
.[1
23]
Cro
ssov
erO
ral
PH
NP
lace
bo(2
9)R
iluzo
le(2
9)y
yy
yG
aler
etal
.[1
23]
Cro
ssov
erO
ral
PH
NP
lace
bo(2
6)R
iluzo
le(2
6)y
yy
yG
ilron
etal
.[1
24]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Act
ive
plac
ebo
(44)
Gab
apen
tin(4
8)M
orph
ine
(49)
Gab
apen
tin+
mor
phin
e(4
9)y
yy
y
Gim
bele
tal.
[76]
Par
alle
lO
ral
DP
NP
lace
bo(7
7)O
xyco
done
(82)
yy
yy
Gol
dste
inet
al.
[56]
Par
alle
lO
ral
DP
NP
lace
bo(1
15)
Dul
oxet
ine
(115
)D
ulox
etin
e(1
14)
Dul
oxet
ine
(113
)y
yy
yG
ordh
etal
.[3
0]C
ross
over
Ora
lP
osttr
aum
atic
/po
stsu
rgic
alne
urop
athi
cpa
in
Pla
cebo
(59)
Gab
apen
tin(6
1)y
yy
y
Gor
son
etal
.[1
25]
Par
alle
lO
ral
DP
NP
lace
bo(2
1)G
abap
entin
(19)
yy
yn
Gra
ff-R
adfo
rdet
al.
[97]
Par
alle
lO
ral
PH
NA
ctiv
epl
aceb
o(1
3)
Am
itrip
tylin
e(1
1)A
mitr
ipty
line
+flu
phen
azin
e(1
2)F
luph
enaz
ine
(13)
yy
yy
Gro
ssko
pfet
al.
[46]
Par
alle
lO
ral
DP
NP
lace
bo(7
0)O
xcar
baze
pine
(71)
yy
yy
Hah
net
al.
[62]
Par
alle
lO
ral
HIV
-ass
ocia
ted
neur
opat
hic
pain
Pla
cebo
(11)
Gab
apen
tin(1
5)y
yy
y
Ham
mac
ket
al.
[80]
Cro
ssov
erO
ral
PH
NP
lace
bo(2
5)N
ortr
ipty
line
(26)
yy
yy
Han
naet
al.
[29]
Par
alle
lO
ral
DP
NP
lace
bo(1
69)
Oxy
codo
ne(1
69)
yy
yy
Hau
ptet
al.
[126
]P
aral
lel
Ora
lD
PN
Pla
cebo
(20)
Ben
fotia
min
e(2
0)y
yy
nH
oet
al.
[127
]C
ross
over
Topi
cal
Neu
ropa
thic
pain
Pla
cebo
(35)
Lido
cain
e(3
5)A
mitr
ipty
line
(35)
yy
yn
Ho
etal
.[1
07]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Act
ive
plac
ebo
(18)
Gab
apen
tin(1
8)Tr
amad
ol(1
8)y
yy
y
Hof
fman
etal
.[1
3]P
aral
lel
Ora
lD
PN
Pla
cebo
(135
)P
rega
balin
(271
)y
yy
yH
use
etal
.[1
10]
Cro
ssov
erO
ral
Pha
ntom
limb
pain
Pla
cebo
(12)
Mst
(12)
yy
yn
Irvi
nget
al.
[92]
Par
alle
lO
ral
PH
NP
lace
bo(5
1)G
abap
entin
ER
(52)
Gab
apen
tinE
R(5
5)y
yy
nK
also
etal
.[1
28]
Cro
ssov
erO
ral
Can
cer
neur
opat
hic
pain
Pla
cebo
(20)
Am
itrip
tylin
e(2
0)y
yy
y
Kar
stet
al.
[74]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Pla
cebo
(11)
Ct-
3(1
0)y
yy
yK
autio
etal
.[1
29]
Par
alle
lO
ral
Can
cer
neur
opat
hic
pain
Pla
cebo
(22)
Am
itrip
tylin
e(2
2)y
yy
y
Kem
per
etal
.[1
30]
Cro
ssov
erO
ral
HIV
-ass
ocia
ted
neur
opat
hic
pain
Pla
cebo
(10)
Mex
iletin
e(9
)y
yy
y
Kho
rom
ieta
l.[1
31]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Act
ive
plac
ebo
(40)
Mor
phin
e(4
1)N
ortr
ipty
line
(34)
Mor
phin
e+
nort
ripty
line
(39)
yy
yy
580
Cepeda et al.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022

Kho
rom
ieta
l.[1
32]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Act
ive
plac
ebo
(42)
Topi
ram
ate
(42)
Na
(42)
yy
yy
Koc
har
etal
.[7
1]P
aral
lel
Ora
lD
PN
Pla
cebo
(21)
Val
proa
te(2
2)y
yy
yK
ocha
ret
al.
[60]
Par
alle
lO
ral
PH
NP
lace
bo(2
2)D
ival
proe
x(2
3)y
yy
yLe
sser
etal
.[6
1]P
aral
lel
Ora
lD
PN
Pla
cebo
(97)
Pre
gaba
lin(7
7)P
rega
balin
(82)
Pre
gaba
lin(8
2)y
yy
yLe
vend
oglu
etal
.[1
33]
Cro
ssov
erO
ral
Cen
tral
neur
opat
hic
pain
Pla
cebo
(20)
Gab
apen
tin(2
0)y
yy
n
Lync
het
al.
[53]
Par
alle
lTo
pica
lN
euro
path
icpa
inP
lace
bo(2
5)K
etam
ine
(22)
Am
itrip
tylin
e(2
2)A
mitr
ipty
line
+ke
tam
ine
(23)
yy
yy
Mai
eret
al.
[100
]P
aral
lel
Ora
lP
hant
omlim
bpa
inP
lace
bo(1
8)M
eman
tine
(18)
yy
yn
Man
icou
rtet
al.
[101
]P
aral
lel
Ora
lP
osttr
aum
atic
/po
stsu
rgic
alne
urop
athi
cpa
in
Pla
cebo
(20)
Ale
ndro
nate
(20)
yy
yn
Mar
iette
etal
.[1
34]
Par
alle
lIn
trav
enou
sD
PN
Pla
cebo
(12)
Alp
ha-in
terf
eron
(12)
yy
yy
McC
lean
e[8
4]P
aral
lel
Ora
lN
euro
path
icpa
inP
lace
bo(4
6)La
mot
rigin
e(4
6)y
yy
yM
cCle
ane
[82]
Par
alle
lTo
pica
lN
euro
path
icpa
inP
lace
bo(4
1)D
oxep
in(4
1)C
apsa
icin
(33)
Dox
epin
+ca
psai
cin
(36)
yy
yn
McC
lean
e[1
35]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Pla
cebo
(44)
L-36
5260
(44)
L-36
5260
(44)
yy
yn
Mei
eret
al.
[73]
Par
alle
lTo
pica
lN
euro
path
icpa
inP
lace
bo(3
0)Li
doca
ine
(28)
yy
yy
Mer
cada
nte
etal
.[1
36]
Cro
ssov
erO
ral
Can
cer
neur
opat
hic
pain
Pla
cebo
(16)
Am
itrip
tylin
e(1
6)y
yy
n
Mor
ley
etal
.[1
37]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Pla
cebo
(19)
Met
hado
ne(1
9)y
yy
yM
orle
yet
al.
[137
]C
ross
over
Ora
lN
euro
path
icpa
inP
lace
bo(1
7)M
etha
done
(17)
yy
yy
Nik
olaj
sen
etal
.[1
38]
Cro
ssov
erO
ral
Pha
ntom
limb
pain
Pla
cebo
(19)
Mem
antin
e(1
9)y
yy
n
Nik
olaj
sen
etal
.[1
02]
Par
alle
lO
ral
Pha
ntom
limb
pain
Pla
cebo
(23)
Gab
apen
tin(2
3)y
yy
y
Nor
rbrin
kan
dLu
ndeb
erg
[24]
Par
alle
lO
ral
Cen
tral
neur
opat
hic
pain
Pla
cebo
(12)
Tram
adol
(23)
yy
yy
Nur
mik
koet
al.
[31]
Par
alle
lO
ro-m
ucos
alN
euro
path
icpa
inP
lace
bo(6
2)S
ativ
ex(6
3)y
yy
yO
nofr
jeta
l.[9
1]P
aral
lel
Intr
amus
cula
rN
euro
path
icpa
inP
lace
bo(3
1)S
t200
(31)
St2
00(3
2)y
yy
nO
skar
sson
etal
.[8
9]P
aral
lel
Ora
lD
PN
Pla
cebo
(31)
Mex
iletin
e(3
1)M
exile
tine
(33)
Mex
iletin
e(3
1)y
yy
yO
ttoet
al.
[139
]C
ross
over
Ora
lD
PN
Pla
cebo
(37)
Val
proi
cac
id(3
7)y
yy
yO
ttoet
al.
[140
]C
ross
over
Ora
lD
PN
Pla
cebo
(47)
Esc
italo
pram
(47)
yy
yy
Raj
a[1
41]
Cro
ssov
erO
ral
PH
NP
lace
bo(7
6)M
orph
ine
(76)
Nor
trip
tylin
e(7
6)y
yy
yR
aoet
al.
[32]
Cro
ssov
erO
ral
Can
cer
neur
opat
hic
pain
Pla
cebo
(58)
Gab
apen
tin(5
7)y
yy
y
Rao
etal
.[2
8]P
aral
lel
Ora
lC
ance
rne
urop
athi
cpa
in
Pla
cebo
(62)
Lam
otrig
ine
(63)
yy
yy
Ras
kin
etal
.[6
4]P
aral
lel
Ora
lD
PN
Pla
cebo
(109
)To
pira
mat
e(2
14)
yy
yy
Ras
kin
etal
.[4
9]P
aral
lel
Ora
lD
PN
Pla
cebo
(116
)D
ulox
etin
e(1
16)
Dul
oxet
ine
(116
)y
yy
yR
auck
etal
.[3
9]P
aral
lel
Ora
lD
PN
Pla
cebo
(59)
Laco
sam
ide
(60)
yy
yy
Ric
ean
dM
aton
[96]
Par
alle
lO
ral
PH
NP
lace
bo(1
11)
Gab
apen
tin(1
15)
Gab
apen
tin(1
08)
yy
yy
Ric
hter
etal
.[5
9]P
aral
lel
Ora
lD
PN
Pla
cebo
(85)
Pre
gaba
lin(7
9)P
rega
balin
(82)
yy
yy
Rin
tala
etal
.[1
42]
Cro
ssov
erO
ral
Cen
tral
neur
opat
hic
pain
Act
ive
plac
ebo
(38)
Gab
apen
tin(3
8)A
mitr
ipty
line
(38)
yy
yy
Ros
enst
ock
etal
.[6
7]P
aral
lel
Ora
lD
PN
Pla
cebo
(70)
Pre
gaba
lin(7
6)y
yy
y
581
Type of Pain Influences Placebo Response
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
Tab
le1
Con
tinue
d
Stu
dyD
esig
nR
oute
ofA
dmin
istr
atio
nC
ondi
tion
Trea
tmen
t1
(Sub
ject
sR
ando
miz
ed)
Trea
tmen
t2
(Sub
ject
sR
ando
miz
ed)
Trea
tmen
t3
(Sub
ject
sR
ando
miz
ed)
Trea
tmen
t4
(Sub
ject
sR
ando
miz
ed)
Dou
ble
Blin
dR
ando
miz
atio
nA
ppro
pria
teA
lloca
tion
Con
ceal
edD
escr
iptio
nof
Dro
pout
s
Ros
siet
al.
[23]
Par
alle
lO
ral
Cen
tral
neur
opat
hic
pain
Pla
cebo
(8)
Leve
tirac
etam
(12)
yy
yy
Row
both
amet
al.
[85]
Par
alle
lO
ral
PH
NP
lace
bo(1
16)
Gab
apen
tin(1
13)
yy
yy
Row
both
amet
al.
[66]
Par
alle
lO
ral
DP
NP
lace
bo(8
1)V
enla
faxi
ne(8
1)V
enla
faxi
ne(8
2)y
yy
yR
owbo
tham
etal
.[1
9]P
aral
lel
oral
DP
NP
lace
bo(6
2)Te
bani
clin
e(6
4)Te
bani
clin
e(6
7)Te
bani
clin
e(6
6)y
yy
yS
abat
owsk
ieta
l.[7
0]P
aral
lel
Ora
lP
HN
Pla
cebo
(81)
Pre
gaba
lin(8
1)P
rega
balin
(76)
yy
yy
Sal
imet
al.
[58]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Pla
cebo
(11)
Ver
um(1
0)y
yy
yS
chifi
ttoet
al.
[45]
Par
alle
lO
ral
HIV
-ass
ocia
ted
neur
opat
hic
pain
Pla
cebo
(21)
Mem
antin
e(2
4)un
know
nun
know
nun
know
nn
Sch
ley
etal
.[1
03]
Par
alle
lO
ral
Pha
ntom
limb
pain
Pla
cebo
(9)
Mem
antin
e(1
0)y
yy
n
Sch
war
tzm
anet
al.
[104
]P
aral
lel
Ora
lP
osttr
aum
atic
/po
stsu
rgic
alne
urop
athi
cpa
in
Pla
cebo
(10)
Ket
amin
e(9
)y
yy
n
Sel
vara
jah
etal
.[1
7]P
aral
lel
Oro
-muc
osal
DP
NP
lace
bo(1
5)S
ativ
ex(1
5)y
yy
yS
emen
chuk
etal
.[1
43]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Pla
cebo
(41)
Bup
ropi
onsr
(41)
yy
yy
Ser
pell
[79]
Par
alle
lO
ral
Neu
ropa
thic
pain
Pla
cebo
(152
)G
abap
entin
(153
)y
yy
yS
hack
elfo
rdet
al.
[22]
Par
alle
lO
ral
PH
NP
lace
bo(6
6)G
w40
6381
(72)
Gw
4063
81(7
1)y
yy
yS
haib
anie
tal.
[21]
Par
alle
lO
ral
DP
NP
lace
bo(6
5)La
cosa
mid
e(1
41)
Laco
sam
ide
(125
)La
cosa
mid
e(1
37)
yy
yy
Sid
dall
etal
.[4
2]P
aral
lel
Ora
lC
entr
alne
urop
athi
cpa
in
Pla
cebo
(67)
Pre
gaba
lin(7
0)y
yy
y
Silv
eret
al.
[34]
Par
alle
lO
ral
Neu
ropa
thic
pain
Pla
cebo
(109
)La
mot
rigin
e(1
11)
yy
yy
Sim
pson
etal
.[7
5]P
aral
lel
Ora
lH
IV-a
ssoc
iate
dne
urop
athi
cpa
in
Pla
cebo
(47)
Lam
otrig
ine
(88)
yy
yy
Sim
pson
etal
.[1
5]P
aral
lel
Ora
lH
IV-a
ssoc
iate
dne
urop
athi
cpa
in
Pla
cebo
(151
)P
rega
balin
(151
)y
yy
y
Sin
drup
etal
.[5
1]P
aral
lel
Ora
lD
PN
Pla
cebo
(42)
Tka
731
(44)
yy
yn
Sm
ithet
al.
[144
]C
ross
over
Ora
lP
hant
omlim
bpa
inP
lace
bo(2
4)G
abap
entin
(24)
yy
yn
Sta
cey
etal
.[9
3]P
aral
lel
Ora
lP
HN
Pla
cebo
(90)
Pre
gaba
lin(8
8)P
rega
balin
(91)
yy
yy
Sve
ndse
net
al.
[68]
Cro
ssov
erO
ral
Cen
tral
neur
opat
hic
pain
Pla
cebo
(12)
Dro
nabi
nol(
12)
yy
yn
Taie
tal.
[145
]C
ross
over
Ora
lC
entr
alne
urop
athi
cpa
in
Pla
cebo
(14)
Gab
apen
tin(1
4)y
yy
n
Tasm
uth
etal
.[1
46]
Cro
ssov
erO
ral
Can
cer
neur
opat
hic
pain
Pla
cebo
(15)
Ven
lafa
xine
(15)
Ven
lafa
xine
(15)
yy
yy
Thi
enel
etal
.[6
5]P
aral
lel
Ora
lD
PN
Pla
cebo
(136
)To
pira
mat
e(1
28)
Topi
ram
ate
(130
)To
pira
mat
e(1
30)
yy
yy
Thi
enel
etal
.[6
5]P
aral
lel
Ora
lD
PN
Pla
cebo
(119
)To
pira
mat
e(1
16)
Topi
ram
ate
(129
)y
yy
yT
hien
elet
al.
[65]
Par
alle
lO
ral
DP
NP
lace
bo(1
26)
Topi
ram
ate
(122
)To
pira
mat
e(1
23)
yy
yy
582
Cepeda et al.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
Tolle
etal
.[3
5]P
aral
lel
Ora
lD
PN
Pla
cebo
(96)
Pre
gaba
lin(9
9)P
rega
balin
(99)
Pre
gaba
lin(1
01)
yy
yy
van
deV
usse
etal
.[6
3]C
ross
over
Ora
lP
osttr
aum
atic
/po
stsu
rgic
alne
urop
athi
cpa
in
Pla
cebo
(29)
Gab
apen
tin(2
9)y
yy
y
van
Sev
ente
ret
al.
[48]
Par
alle
lO
ral
PH
NP
lace
bo(9
4)P
rega
balin
(87)
Pre
gaba
lin(9
8)P
rega
balin
(91)
yy
yy
van
Sev
ente
ret
al.
[14]
Par
alle
lO
ral
Pos
ttrau
mat
ic/
post
surg
ical
neur
opat
hic
pain
Pla
cebo
(127
)P
rega
balin
(127
)y
yy
y
Var
enna
etal
.[1
05]
Par
alle
lO
ral
Pos
ttrau
mat
ic/
post
surg
ical
neur
opat
hic
pain
Pla
cebo
(17)
Clo
dron
ate
(15)
yy
yy
Ves
terg
aard
etal
.[1
47]
Cro
ssov
erO
ral
Cen
tral
neur
opat
hic
pain
Pla
cebo
(30)
Am
itrip
tylin
e(3
0)y
yy
y
Vilh
olm
etal
.[1
08]
Cro
ssov
erO
ral
Pos
ttrau
mat
ic/
post
surg
ical
neur
opat
hic
pain
Pla
cebo
(27)
Leve
tirac
etam
(27)
yy
yy
Vin
iket
al.
[41]
Par
alle
lO
ral
DP
NP
lace
bo(9
0)La
mot
rigin
e(9
0)La
mot
rigin
e(9
0)La
mot
rigin
e(9
0)y
yy
yV
rank
enet
al.
[50]
Par
alle
lO
ral
Cen
tral
neur
opat
hic
pain
Pla
cebo
(11)
S(+
)-ke
tam
ine
(11)
S(+
)-ke
tam
ine
(11)
yy
yn
Vra
nken
etal
.[3
3]P
aral
lel
Ora
lC
entr
alne
urop
athi
cpa
in
Pla
cebo
(20)
Pre
gaba
lin(2
0)y
yy
y
Vre
them
etal
.[1
48]
Cro
ssov
erO
ral
DP
NP
lace
bo(1
9)A
mitr
ipty
line
(19)
Map
rotil
ine
(19)
yy
yy
Vre
them
etal
.[1
48]
Cro
ssov
erO
ral
DP
NP
lace
bo(1
8)A
mitr
ipty
line
(18)
Map
rotil
ine
(18)
yy
yy
Wal
lace
etal
.[1
49]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Pla
cebo
(20)
Mex
iletin
e(2
0)y
yy
nW
alla
ceet
al.
[77]
Par
alle
lO
ral
Neu
ropa
thic
pain
Pla
cebo
(31)
Gv1
9677
1(3
2)y
yy
yW
alla
ceet
al.
[72]
Cro
ssov
erO
ral
Neu
ropa
thic
pain
Pla
cebo
(41)
4030
w92
(41)
yy
yy
Wat
son
and
Bab
ul[1
50]
Cro
ssov
erO
ral
PH
NP
lace
bo(5
0)O
xyco
done
(50)
yy
yn
Wat
son
etal
.[1
51]
Cro
ssov
erO
ral
DP
NA
ctiv
epl
aceb
o(4
5)
Oxy
codo
ne(4
5)y
yy
y
Wer
nick
eet
al.
[43]
Par
alle
lO
ral
DP
NP
lace
bo(1
08)
Dul
oxet
ine
(114
)D
ulox
etin
e(1
12)
yy
yy
Wild
er-S
mith
etal
.[1
52]
Par
alle
lO
ral
Pha
ntom
limb
pain
Pla
cebo
(31)
Tram
adol
(33)
Am
itrip
tylin
e(3
0)y
yy
n
Win
deba
nket
al.
[153
]P
aral
lel
Ora
lN
euro
path
icpa
inP
lace
bo(2
0)Ig
f-1
(20)
yy
yn
Wrig
htet
al.
[90]
Par
alle
lO
ral
DP
NP
lace
bo(1
6)M
exile
tine
(15)
yy
yy
Wu
etal
.[1
06]
Cro
ssov
erO
ral
Pha
ntom
limb
pain
Pla
cebo
(60)
Mor
phin
e(6
0)M
exile
tine
(60)
yy
yn
Wym
eret
al.
[154
]P
aral
lel
Ora
lD
PN
Pla
cebo
(93)
Laco
sam
ide
(93)
Laco
sam
ide
(91)
Laco
sam
ide
(93)
yy
yy
Yella
ndet
al.
[155
]C
ross
over
Ora
lN
euro
path
icpa
inP
lace
bo(5
5)G
abap
entin
(55)
yy
yy
Youl
ean
dO
sio
[36]
Par
alle
lO
ral
HIV
-ass
ocia
ted
neur
opat
hic
pain
Pla
cebo
(47)
L-ca
rniti
ne(4
3)y
yy
y
Yuc
elet
al.
[54]
Par
alle
lO
ral
Neu
ropa
thic
pain
Pla
cebo
(19)
Ven
lafa
xine
(19)
Ven
lafa
xine
(17)
yy
yn
Yue
net
al.
[156
]C
ross
over
Topi
cal
DP
NP
lace
bo(2
2)Is
osor
bide
dini
trat
e(2
2)y
yy
n
Zie
gler
etal
.[1
57]
Par
alle
lO
ral
DP
NP
lace
bo(2
86)
Act
oveg
in(2
81)
yy
yn
Zie
gler
etal
.[1
6]P
aral
lel
Ora
lD
PN
Pla
cebo
(74)
Laco
sam
ide
(150
)La
cosa
mid
e(1
33)
yy
yY
583
Type of Pain Influences Placebo Response
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022

The unadjusted responder rate in each neuropathic painsyndrome, along with the number of trials and number ofsubjects in each of the pain syndromes, can be found inTable 4.
After adjusting for potential confounders, trials thatassessed central pain and postherpetic neuralgia hadlower placebo responses than trials evaluating diabeticneuropathic/polyneuropathic pain. Similar to the painintensity analysis, a higher placebo response wasobserved for the trials that assessed HIV-related neuro-pathic pain compared with the trials evaluating diabeticneuropathic/polyneuropathic pain (Table 6).
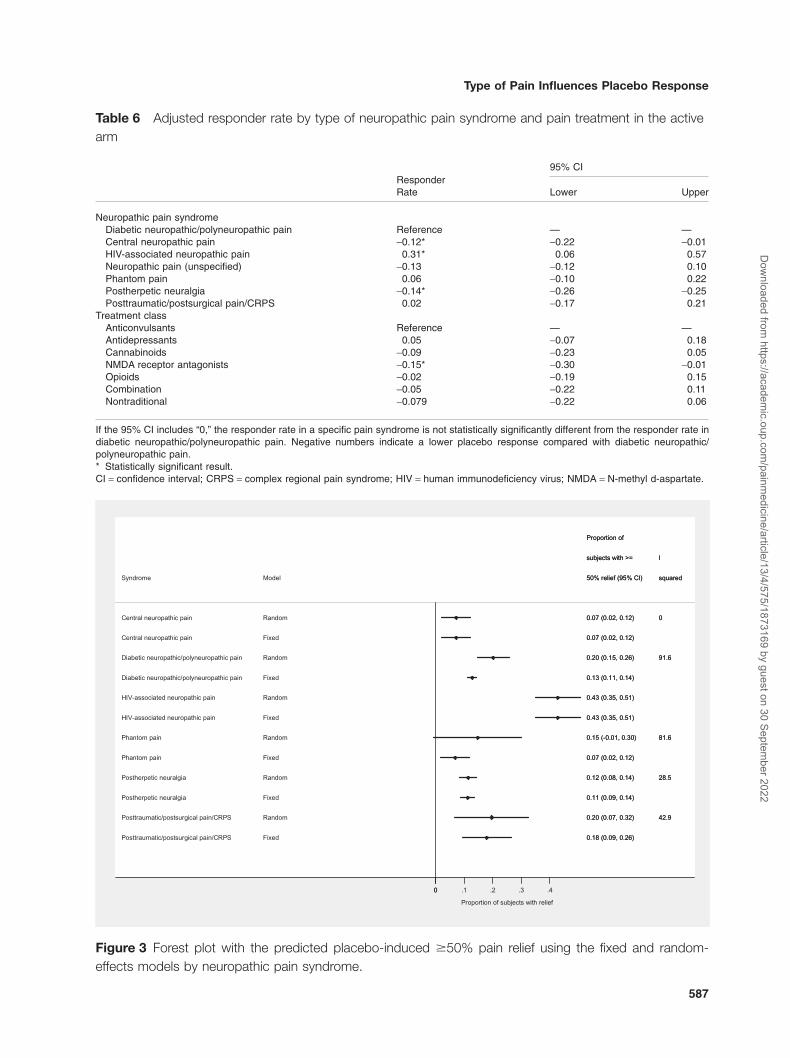
These findings translate into a predicted placebo-inducedresponder rate using a random-effects model in subjectswith diabetic neuropathic/polyneuropathic pain of 20.2%(95% CI, 14.6 to 25.8), 7.2% (95% CI, 2.1 to 12.3) insubjects with central pain, 11.5% (95% CI, 8.4 to 14.5) insubjects with postherpetic neuralgia, and 42.8% (95% CI,34.9 to 50.7) in subjects with HIV-associated neuropathicpain (Figure 3). When the fixed-effects model was used,the predicted placebo-induced responder rate differedfrom the random-effects model predictions for diabeticneuropathic/polyneuropathic pain and phantom pain (itwas roughly half) due to the high levels of heterogeneity.
In terms of the effect of drug class on the placeboresponse, the trials that assessed NMDA blockers had asmaller placebo response than in trials in which anticon-vulsants were used 15.7% lower (1.0% to 30.4) (Table 6).
Age was positively associated with the placebo response(the higher the age, the greater the placebo response).With each increasing year in age, the placebo responseincreased 0.81% (95% CI, 0.01% to 1.6%). Note that thisfinding is adjusted for neuropathic pain syndrome and asa result, is not simply an artifact of an association betweenpain syndrome and mean age.
Mean baseline pain intensity and year of completion of thestudy did not affect the placebo responder rate response.
Table 2 Outcomes assessed in the included trials
Outcome
Numberof Trials(N = 141)
Numberof Subjects(N = 6,239)
Baseline pain intensity 131 6,205Posttreatment pain intensity 130 6,226Mean change from baseline in
pain intensity132 6,239
�30% reduction in pain intensityfrom baseline values
34 2,420
�50% reduction in pain intensityfrom baseline values
47 3,087
�70% reduction in pain intensityfrom baseline values
7 633
Tab
le3
Type
oftr
eatm
ents
asse
ssed
inth
eac
tive
arm
ofth
etr
ials
incl
uded
inth
ean
alys
isof
pain
inte
nsity
and/
orpa
inre
lief
byne
urop
athi
cpa
insy
ndro
me
Neu
ropa
thic
Pai
nS
yndr
ome,
N(%
)A
ntic
onvu
lsan
tsA
ntid
epre
ssan
tsC
anna
bino
ids
NM
DA
Rec
epto
rA
ntag
onis
tsO
pioi
ds
Sod
ium
Cha
nnel
Blo
cker
sC
ombi
natio
nN
ontr
aditi
onal
Tota
l
Can
cer
neur
opat
hic
pain
3(7
5)—
——
1(2
5)—
——
4(4
.0)
Cen
tral
neur
opat
hic
pain
4(5
7.1)
—1
(14.
3)1
(14.
3)1
(14.
3)—
——
7(6
.9)
Dia
betic
neur
opat
hic/
poly
neur
opat
hic
pain
23(5
7.5)
4(1
0.0)
1(2
.5)
1(2
.5)
3(7
.5)
2(5
.0)
1(2
.5)
5(1
2.5)
40(3
9.6)
HIV
-ass
ocia
ted
neur
opat
hic
pain
3(5
0)—
—1
(16.
7)—
1(1
6.7)
—1
(16.
7)6
(5.9
)
Neu
ropa
thic
pain
(uns
peci
fied)
4(2
6.7)
1(6
.7)
3(2
0.0)
1(6
.7)
—2
(13.
3)3
(20.
0)1
(6.7
)15
(14.
7)
Pha
ntom
pain
1(1
6.7)
——
3(5
0.0)
1(1
6.7)
—1
(16.
7)—
6(5
.8)
Pos
ther
petic
neur
algi
a8
(57.
1)1
(7.1
4)—
—1
(7.1
4)—
1(7
.14)
3(2
1.4)
14(1
3.9)
Pos
ttrau
mat
ic/p
osts
urgi
cal
pain
/CR
PS
4(4
4.4)
2(2
2.2)
1(1
1.1)
2(2
2.2)
9(8
.9)
Tota
l50
(49.
5)6
(5.9
4)5
(4.9
)9
(8.9
)7
(6.9
)6
(5.9
4)6
(5.9
4)12
(11.
9)10
1(1
00)
CR
PS
=co
mpl
exre
gion
alpa
insy
ndro
me;
HIV
=hu
man
imm
unod
efici
ency
viru
s;N
MD
A=
N-m
ethy
ld-a
spar
tate
.
584
Cepeda et al.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022

Discussion
This comprehensive, systematic search and meta-analysis showed substantial variation in placebo responsein the different types of pain syndromes evaluated. Themagnitude of the placebo-induced decline in pain intensityfrom baseline could be as large as 1.8 units with a 42.8%responder rate in subjects with HIV-associated neuro-pathic pain or as small as 0.5 units with a 7.2% responderrate in subjects with central neuropathic pain.
Postherpetic neuralgia and central pain were associatedwith smaller placebo responses, and HIV-associated painwas associated with a higher placebo response in bothpain intensity and responder rate analyses. This consis-tency across analyses provides confidence in our results.A previous study also supports the finding that posther-petic neuralgia has a smaller placebo response [9] thanpainful diabetic neuropathy, but the authors are not awareof studies that have evaluated the placebo response inother neuropathic pain syndromes.
Phantom pain was associated with a higher placeboresponse than diabetic neuropathic/polyneuropathic painin the pain intensity analysis, but not in the responder rateTa
ble
4U
nadj
uste
dpl
aceb
o-in
duce
dde
crea
sein
pain
inte
nsity
from
base
line
and
resp
onde
rra
teby
neur
opat
hic
pain
synd
rom
e
Neu
ropa
thic
Pai
nS
yndr
ome
Num
ber
ofTr
ials
inth
eP
ain
Inte
nsity
Ana
lysi
s
Num
ber
ofS
ubje
cts
inth
eP
ain
Inte
nsity
Ana
lysi
s
Mea
nB
asel
ine
Pai
nIn
tens
ity�
Sta
ndar
dD
evia
tion
Mea
nD
ecre
ase
inP
ain
Inte
nsity
from
Bas
elin
e(0
–10
Sca
le)
Num
ber
ofTr
ials
inth
eR
espo
nder
Ana
lysi
s
Num
ber
ofS
ubje
cts
inth
eR
espo
nder
Ana
lysi
s
Mea
nP
lace
boR
espo
nder
Rat
es(�
50%
Pai
nR
elie
f)
Can
cer
neur
opat
hic
pain
413
85.
5�
1.3
-1.5
1—
——
Cen
tral
neur
opat
hic
pain
612
86.
5�
1.4
-0.5
03
997.
1D
iabe
ticne
urop
athi
c/po
lyne
urop
athi
cpa
in39
2,96
96.
4�
1.5
-1.4
220
1,63
021
.1
HIV
-ass
ocia
ted
neur
opat
hic
pain
628
06.
0�
1.9
-1.6
01
150
43.0
Neu
ropa
thic
pain
(uns
peci
fied)
1363
76.
6�
1.6
-0.7
98
436
13.4
Pha
ntom
pain
457
6.0
�0.
9-2
.35
483
18.0
Pos
ther
petic
neur
algi
a14
839
6.3
�1.
5-1
.17
961
412
.2P
osttr
aum
atic
/pos
tsur
gica
lpa
in/C
RP
S8
269
5.6
�2.
0-0
.31
275
23.0
CR
PS
=co
mpl
exre
gion
alpa
insy
ndro
me;
HIV
=hu
man
imm
unod
efici
ency
viru
s.
Table 5 Adjusted placebo-induced meandecrease in pain intensity by type of neuropathicpain syndrome and pain treatment in the active arm
Mean Decreasein Pain Intensityfrom Baseline
95% CI
Lower Upper
Neuropathic pain syndromeDiabetic neuropathic/
polyneuropathic painReference — —
Cancer neuropathic pain 0.03 -0.87 0.92Central neuropathic pain 1.02* 0.18 1.86HIV-associated neuropathic pain -0.50* -0.77 -0.23Neuropathic pain (unspecified) 0.53 -0.06 1.13Phantom pain -1.80* -2.90 -0.69Postherpetic neuralgia 0.17* 0.008 0.33Posttraumatic/postsurgical
pain/CRPS0.66* 0.39 0.94
Treatment classAnticonvulsants Reference — —Antidepressants 0.002 -0.68 0.69Cannabinoids 0.36 -0.62 1.34NMDA receptor antagonists 0.87* 0.04 1.71Opioids -0.37 -1.07 0.33Sodium channel blockers 0.72 -0.30 1.73Combination 0.59 -0.33 1.51Nontraditional 0.33 -0.24 0.89
For example, the mean decrease in pain intensity from baseline in centralneuropathic pain was 1.02 units smaller than the trials that evaluated diabeticneuropathic/polyneuropathic pain. If the 95% CI includes “0,” the decline inpain intensity in a specific pain syndrome is not statistically significantlydifferent from the decline in diabetic neuropathic/polyneuropathic pain. Nega-tive numbers indicate a larger placebo response compared with diabeticneuropathic/polyneuropathic pain.* Statistically significant result.CI = confidence interval; CRPS = complex regional pain syndrome;HIV = human immunodeficiency virus; NMDA = N-methyl d-aspartate.
585
Type of Pain Influences Placebo Response
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
analysis. Similarly, posttraumatic/postsurgical pain/CRPSwas associated with a smaller placebo response thandiabetic neuropathic/polyneuropathic pain in the painintensity analysis, but not in the responder rate analysis.There was substantial heterogeneity in the responder rateanalysis despite the fact that we controlled for treatment inthe active arm, age, baseline pain intensity, and year ofpublication of the study. Therefore, caution is neededwhen interpreting the impact of these pain syndromes onthe placebo response. Interestingly, it has been found thatthe placebo response is higher when continuous out-comes are evaluated than when binary outcome areevaluated [111].
Placebo response rates can be large and clinicallyimportant [112,113] and dependent on the underlyingpain condition, which may help explain the quite sub-stantial failure rates sometimes observed in clinical trials.With such potentially large placebo responses for sub-jects with certain neuropathic pain conditions, the medi-cation under evaluation in the active arm must have avery large treatment effect in order to be able to differ-entiate from placebo. It has previously been observedthat the difference for currently available, proven effective
treatments from placebo ranges from 0.9 to 1.5 units[114], and results from the current study suggest theplacebo response could be as large as 1.8 units. There-fore, the findings of this study suggest that initial evalu-ation of new drugs should start in neuropathic painsyndromes with a lower placebo response, such ascentral pain or postherpetic neuralgia, to avoid inconclu-sive or false negative study results, which might lead tothe abandonment of the development of potentially effi-cacious new drugs.
The findings of the present study seem to indicate that theplacebo response might be also influenced by the type ofmedications under evaluation. This finding is not surprisingas subjects’ expectation of pain relief is a known factor forplacebo response. The reason the expectation of painrelief is lower with NMDA receptor antagonists than withanticonvulsants is not clear. Although many hypotheticalreasons could be generated, caution in over-interpretingthe results is warranted because the data in which theanalyses were conducted were sparse (i.e., not all of thedrugs were evaluated in all pain syndromes) and in thesecircumstances, the findings could be an artifact (i.e., afalse positive result) [115].
Cancer-associated neuropathic pain
Cancer-associated neuropathic pain
Central neuropathic pain
Central neuropathic pain
Diabetic neuropathic/polyneuropathic pain
Diabetic neuropathic/polyneuropathic pain
HIV-associated neuropathic pain
HIV-associated neuropathic pain
Phantom pain
Phantom pain
Postherpetic neuralgia
Postherpetic neuralgia
Posttraumatic/postsurgical pain/CRPS
Posttraumatic/postsurgical pain/CRPS
Syndrome
Random
Fixed
Random
Fixed
Random
Fixed
Random
Fixed
Random
Fixed
Random
Fixed
Random
Fixed
Model
-1.38 (-1.86, -0.90)
-1.33 (-1.65, -1.01)
-0.53 (-0.86, -0.19)
-0.53 (-0.86, -0.19)
-1.45 (-1.55, -1.35)
-1.46 (-1.53, -1.40)
-1.82 (-2.12, -1.51)
-1.91 (-2.13, -1.68)
-2.61 (-3.55, -1.68)
-2.69 (-3.18, -2.19)
-1.16 (-1.29, -1.03)
-1.16 (-1.29, -1.03)
-0.46 (-0.80, -0.12)
-0.62 (-0.85, -0.39)
intensity (95% CI)
Mean pain
52.1
0
49.7
27.6
70.3
0
41.2
squared
I
-1.38 (-1.86, -0.90)
-1.33 (-1.65, -1.01)
-0.53 (-0.86, -0.19)
-0.53 (-0.86, -0.19)
-1.45 (-1.55, -1.35)
-1.46 (-1.53, -1.40)
-1.82 (-2.12, -1.51)
-1.91 (-2.13, -1.68)
-2.61 (-3.55, -1.68)
-2.69 (-3.18, -2.19)
-1.16 (-1.29, -1.03)
-1.16 (-1.29, -1.03)
-0.46 (-0.80, -0.12)
-0.62 (-0.85, -0.39)
intensity (95% CI)
Mean pain
52.1
0
49.7
27.6
70.3
0
41.2
squared
I
enilesabmorfdesaercedniaP
0-3 -2 -1 0
Figure 2 Forest plot with the predicted placebo-induced mean decrease in pain intensity using the fixed andrandom-effects models by neuropathic pain syndrome.
586
Cepeda et al.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
Central neuropathic pain
Central neuropathic pain
Diabetic neuropathic/polyneuropathic pain
Diabetic neuropathic/polyneuropathic pain
HIV-associated neuropathic pain
HIV-associated neuropathic pain
Phantom pain
Phantom pain
Postherpetic neuralgia
Postherpetic neuralgia
Posttraumatic/postsurgical pain/CRPS
Posttraumatic/postsurgical pain/CRPS
Syndrome
Random
Fixed
Random
Fixed
Random
Fixed
Random
Fixed
Random
Fixed
Random
Fixed
Model
0.07 (0.02, 0.12)
0.07 (0.02, 0.12)
0.20 (0.15, 0.26)
0.13 (0.11, 0.14)
0.43 (0.35, 0.51)
0.43 (0.35, 0.51)
0.15 (-0.01, 0.30)
0.07 (0.02, 0.12)
0.12 (0.08, 0.14)
0.11 (0.09, 0.14)
0.20 (0.07, 0.32)
0.18 (0.09, 0.26)
50% relief (95% CI)
subjects with >=
Proportion of
0
91.6
81.6
28.5
42.9
squared
I
0.07 (0.02, 0.12)
0.07 (0.02, 0.12)
0.20 (0.15, 0.26)
0.13 (0.11, 0.14)
0.43 (0.35, 0.51)
0.43 (0.35, 0.51)
0.15 (-0.01, 0.30)
0.07 (0.02, 0.12)
0.12 (0.08, 0.14)
0.11 (0.09, 0.14)
0.20 (0.07, 0.32)
0.18 (0.09, 0.26)
50% relief (95% CI)
subjects with >=
Proportion of
0
91.6
81.6
28.5
42.9
squared
I
feilerhtiwstcejbusfonoitroporP
00 .1 .2 .3 .4
Figure 3 Forest plot with the predicted placebo-induced �50% pain relief using the fixed and random-effects models by neuropathic pain syndrome.
Table 6 Adjusted responder rate by type of neuropathic pain syndrome and pain treatment in the activearm
ResponderRate
95% CI
Lower Upper
Neuropathic pain syndromeDiabetic neuropathic/polyneuropathic pain Reference — —Central neuropathic pain -0.12* -0.22 -0.01HIV-associated neuropathic pain 0.31* 0.06 0.57Neuropathic pain (unspecified) -0.13 -0.12 0.10Phantom pain 0.06 -0.10 0.22Postherpetic neuralgia -0.14* -0.26 -0.25Posttraumatic/postsurgical pain/CRPS 0.02 -0.17 0.21
Treatment classAnticonvulsants Reference — —Antidepressants 0.05 -0.07 0.18Cannabinoids -0.09 -0.23 0.05NMDA receptor antagonists -0.15* -0.30 -0.01Opioids -0.02 -0.19 0.15Combination -0.05 -0.22 0.11Nontraditional -0.079 -0.22 0.06
If the 95% CI includes “0,” the responder rate in a specific pain syndrome is not statistically significantly different from the responder rate indiabetic neuropathic/polyneuropathic pain. Negative numbers indicate a lower placebo response compared with diabetic neuropathic/polyneuropathic pain.* Statistically significant result.CI = confidence interval; CRPS = complex regional pain syndrome; HIV = human immunodeficiency virus; NMDA = N-methyl d-aspartate.
587
Type of Pain Influences Placebo Response
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
Findings of this study also indicated that higher age wasassociated with higher responder rates, but was notassociated with a decline in pain intensity. The number oftrials that reported responder rates was much lower thanthe number of trials that reported pain intensity; as aresult, the findings could be the consequence of analyzingonly a subset of studies. In the literature, the association ofage with placebo response ranges from no effect[116,117] to increasing age being associated withdecreasing the placebo response (i.e., opposite to thefinding in this current study) [118].
Although the current analyses were controlled for theeffect of study design characteristics and subject charac-teristics that could be associated with placebo response,no adjustments were made for use of rescue medicationsin the trial. In order for this or other unmeasured variablesto invalidate the results, the effect of these variables on theplacebo response has to be differential in the pain syn-dromes, which seems unlikely.
In this study, the placebo response for achieving aresponder rate of at least 50% pain relief was assessed;however, an unanswered question is whether the placeboresponse changes depending on the selection of thecutoff value used to define a “responder” (e.g., at least30% pain relief, total pain relief). This question could beaddressed by selecting and analyzing trials that reportmultiple responder rates.
Placebo response is substantial in neuropathic pain.Understanding the placebo response could lead toimprovements in study design that will enhance the likeli-hood of detecting beneficial treatments and avoid theabandonment of medications due to erroneous percep-tions of lack of efficacy. When designing clinical trials toassess the efficacy of drugs, the pain syndrome should beconsidered.
Acknowledgment
This study was funded by Janssen Global Services, LLC.
References1 Khan A, Detke M, Khan SR, Mallinckrodt C. Placebo
response and antidepressant clinical trial outcome. JNerv Ment Dis 2003;191:211–8.
2 Turner JA, Deyo RA, Loeser JD, Von KM, FordyceWE. The importance of placebo effects in pain treat-ment and research. JAMA 1994;271:1609–14.
3 Linde K, Witt CM, Streng A, et al. The impact ofpatient expectations on outcomes in four randomizedcontrolled trials of acupuncture in patients withchronic pain. Pain 2007;128:264–71.
4 Harris RE, Williams DA, McLean SA, et al. Character-ization and consequences of pain variability in indi-viduals with fibromyalgia. Arthritis Rheum 2005;52:3670–4.
5 Katz J, Finnerup NB, Dworkin RH. Clinical trialoutcome in neuropathic pain: Relationship to studycharacteristics. Neurology 2008;70:263–72.
6 Averbuch M, Katzper M. Baseline pain and responseto analgesic medications in the postsurgery dentalpain model. J Clin Pharmacol 2000;40:133–7.
7 Irizarry MC, Webb DJ, Ali Z, et al. Predictors ofplacebo response in pooled lamotrigine neuropathicpain clinical trials. Clin J Pain 2009;25:469–76.
8 Quessy SN, Rowbotham MC. Placebo response inneuropathic pain trials. Pain 2008;138:479–83.
9 Dworkin RH, Turk DC, Peirce-Sandner S, et al.Placebo and treatment group responses in posther-petic neuralgia vs painful diabetic peripheral neuropa-thy clinical trials in the REPORT database. Pain2010;150:12–6.
10 Higgins JP, Thompson SG. Controlling the risk ofspurious findings from meta-regression. Stat Med2004;23:1663–82.
11 Follmann D, Elliott P, Suh I, Cutler J. Variance impu-tation for overviews of clinical trials with continuousresponse. J Clin Epidemiol 1992;45:769–73.
12 Sweeting MJ, Sutton AJ, Lambert PC. What to addto nothing? Use and avoidance of continuity correc-tions in meta-analysis of sparse data. Stat Med2004;23:1351–75.
13 Hoffman DL, Sadosky A, Dukes EM, Alvir J. How dochanges in pain severity levels correspond tochanges in health status and function in patientswith painful diabetic peripheral neuropathy? Pain2010;149:194–201.
14 van Seventer R, Bach FW, Toth CC, et al. Pregabalinin the treatment of post-traumatic peripheral neuro-pathic pain: A randomized double-blind trial. Eur JNeurol 2010;17:1082–9.
15 Simpson DM, Schifitto G, Clifford DB, et al. Pregaba-lin for painful HIV neuropathy: A randomized, double-blind, placebo-controlled trial. Neurology 2010;74:413–20.
16 Ziegler D, Hidvegi T, Gurieva I, et al. Efficacy andsafety of lacosamide in painful diabetic neuropathy.Diabetes Care 2010;33:839–41.
17 Selvarajah D, Gandhi R, Emery CJ, Tesfaye S. Ran-domized placebo-controlled double-blind clinical trialof cannabis-based medicinal product (Sativex) inpainful diabetic neuropathy: Depression is a majorconfounding factor. Diabetes Care 2010;33:128–30.
588
Cepeda et al.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
18 Chen JY, Chang CY, Feng PH, et al. Plasma vitaminC is lower in postherpetic neuralgia patients andadministration of vitamin C reduces spontaneouspain but not brush-evoked pain. Clin J Pain2009;25:562–9.
19 Rowbotham MC, Duan WR, Thomas J, Nothaft W,Backonja MM. A randomized, double-blind, placebo-controlled trial evaluating the efficacy and safety ofABT-594 in patients with diabetic peripheral neuro-pathic pain. Pain 2009;146:245–52.
20 Finnerup NB, Grydehoj J, Bing J, et al. Levetiracetamin spinal cord injury pain: A randomized controlledtrial. Spinal Cord 2009;47:861–7.
21 Shaibani A, Fares S, Selam JL, et al. Lacosamide inpainful diabetic neuropathy: An 18-week double-blind placebo-controlled trial. J Pain 2009;10:818–28.
22 Shackelford S, Rauck R, Quessy S, et al. A random-ized, double-blind, placebo-controlled trial of a selec-tive COX-2 inhibitor, GW406381, in patients withpostherpetic neuralgia. J Pain 2009;10:654–60.
23 Rossi S, Mataluni G, Codeca C, et al. Effects of leve-tiracetam on chronic pain in multiple sclerosis:Results of a pilot, randomized, placebo-controlledstudy. Eur J Neurol 2009;16:360–6.
24 Norrbrink C, Lundeberg T. Tramadol in neuropathicpain after spinal cord injury: A randomized, double-blind, placebo-controlled trial. Clin J Pain 2009;25:177–84.
25 Agrawal RP, Goswami J, Jain S, Kochar DK. Man-agement of diabetic neuropathy by sodium valproateand glyceryl trinitrate spray: A prospective double-blind randomized placebo-controlled study. DiabetesRes Clin Pract 2009;83:371–8.
26 Cheville AL, Sloan JA, Northfelt DW, et al. Use of alidocaine patch in the management of postsurgicalneuropathic pain in patients with cancer: A phase IIIdouble-blind crossover study (N01CB). Support CareCancer 2009;17:451–60.
27 Arezzo JC, Rosenstock J, Lamoreaux L, Pauer L.Efficacy and safety of pregabalin 600 mg/d for treat-ing painful diabetic peripheral neuropathy: A double-blind placebo-controlled trial. BMC Neurol 2008;8:33.
28 Rao RD, Flynn PJ, Sloan JA, et al. Efficacy of lamot-rigine in the management of chemotherapy-inducedperipheral neuropathy: A phase 3 randomized,double-blind, placebo-controlled trial, N01C3.Cancer 2008;112:2802–8.
29 Hanna M, O’Brien C, Wilson MC. Prolonged-releaseoxycodone enhances the effects of existing gabap-entin therapy in painful diabetic neuropathy patients.Eur J Pain 2008;12:804–13.
30 Gordh TE, Stubhaug A, Jensen TS, et al. Gabapentinin traumatic nerve injury pain: A randomized, double-blind, placebo-controlled, cross-over, multi-centerstudy. Pain 2008;138:255–66.
31 Nurmikko TJ, Serpell MG, Hoggart B, et al. Sativexsuccessfully treats neuropathic pain characterised byallodynia: A randomised, double-blind, placebo-controlled clinical trial. Pain 2007;133:210–20.
32 Rao RD, Michalak JC, Sloan JA, et al. Efficacy ofgabapentin in the management of chemotherapy-induced peripheral neuropathy: A phase 3 random-ized, double-blind, placebo-controlled, crossover trial(N00C3). Cancer 2007;110:2110–8.
33 Vranken JH, Dijkgraaf MG, Kruis MR, et al. Pregaba-lin in patients with central neuropathic pain: A ran-domized, double-blind, placebo-controlled trial of aflexible-dose regimen. Pain 2008;136:150–7.
34 Silver M, Blum D, Grainger J, Hammer AE, Quessy S.Double-blind, placebo-controlled trial of lamotriginein combination with other medications for neuro-pathic pain. J Pain Symptom Manage 2007;34:446–54.
35 Tolle T, Freynhagen R, Versavel M, Trostmann U,Young JP Jr. Pregabalin for relief of neuropathic painassociated with diabetic neuropathy: A randomized,double-blind study. Eur J Pain 2008;12:203–13.
36 Youle M, Osio M. A double-blind, parallel-group,placebo-controlled, multicentre study of acetylL-carnitine in the symptomatic treatment of antiretro-viral toxic neuropathy in patients with HIV-1 infection.HIV Med 2007;8:241–50.
37 Agrawal RP, Choudhary R, Sharma P, et al. Glyceryltrinitrate spray in the management of painful diabeticneuropathy: A randomized double blind placebocontrolled cross-over study. Diabetes Res Clin Pract2007;77:161–7.
38 Freeman R, Raskin P, Hewitt DJ, et al. Randomizedstudy of tramadol/acetaminophen vs placebo inpainful diabetic peripheral neuropathy. Curr Med ResOpin 2007;23:147–61.
39 Rauck RL, Shaibani A, Biton V, Simpson J, Koch B.Lacosamide in painful diabetic peripheral neuropa-thy: A phase 2 double-blind placebo-controlledstudy. Clin J Pain 2007;23:150–8.
40 Arbaiza D, Vidal O. Tramadol in the treatment ofneuropathic cancer pain: A double-blind, placebo-controlled study. Clin Drug Investig 2007;27:75–83.
589
Type of Pain Influences Placebo Response
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
41 Vinik AI, Tuchman M, Safirstein B, et al. Lamotriginefor treatment of pain associated with diabetic neur-opathy: Results of two randomized, double-blind,placebo-controlled studies. Pain 2007;128:169–79.
42 Siddall PJ, Cousins MJ, Otte A, et al. Pregabalin incentral neuropathic pain associated with spinal cordinjury: A placebo-controlled trial. Neurology2006;67:1792–800.
43 Wernicke JF, Pritchett YL, D’Souza DN, et al. A ran-domized controlled trial of duloxetine in diabeticperipheral neuropathic pain. Neurology 2006;67:1411–20.
44 Eisenberg E, Pud D, Koltun L, Loven D. Effect of earlyadministration of the N-methyl-d-aspartate receptorantagonist amantadine on the development of post-mastectomy pain syndrome: A prospective pilotstudy. J Pain 2007;8:223–9.
45 Schifitto G, Yiannoutsos CT, Simpson DM, et al. Aplacebo-controlled study of memantine for the treat-ment of human immunodeficiency virus-associatedsensory neuropathy. J Neurovirol 2006;12:328–31.
46 Grosskopf J, Mazzola J, Wan Y, Hopwood M. Arandomized, placebo-controlled study of oxcarba-zepine in painful diabetic neuropathy. Acta NeurolScand 2006;114:177–80.
47 Beydoun A, Shaibani A, Hopwood M, Wan Y. Oxcar-bazepine in painful diabetic neuropathy: Results of adose-ranging study. Acta Neurol Scand 2006;113:395–404.
48 van Seventer R, Feister HA, Young JP Jr, et al. Effi-cacy and tolerability of twice-daily pregabalin fortreating pain and related sleep interference in pos-therpetic neuralgia: A 13-week, randomized trial.Curr Med Res Opin 2006;22:375–84.
49 Raskin J, Pritchett YL, Wang F, et al. A double-blind,randomized multicenter trial comparing duloxetinewith placebo in the management of diabetic periph-eral neuropathic pain. Pain Med 2005;6:346–56.
50 Vranken JH, Dijkgraaf MG, Kruis MR, van DasselaarNT, van der Vegt MH. Iontophoretic administration ofS(+)-ketamine in patients with intractable centralpain: A placebo-controlled trial. Pain 2005;118:224–31.
51 Sindrup SH, Graf A, Sfikas N. The NK1-receptorantagonist TKA731 in painful diabetic neuropathy:A randomised, controlled trial. Eur J Pain 2006;10:567–71.
52 Dogra S, Beydoun S, Mazzola J, Hopwood M, WanY. Oxcarbazepine in painful diabetic neuropathy:A randomized, placebo-controlled study. Eur J Pain2005;9:543–54.
53 Lynch ME, Clark AJ, Sawynok J, Sullivan MJ. Topical2% amitriptyline and 1% ketamine in neuropathicpain syndromes: A randomized, double-blind,placebo-controlled trial. Anesthesiology 2005;103:140–6.
54 Yucel A, Ozyalcin S, Koknel Talu G, et al. The effect ofvenlafaxine on ongoing and experimentally inducedpain in neuropathic pain patients: A double blind,placebo controlled study. Eur J Pain 2005;9:407–16.
55 Atli A, Dogra S. Zonisamide in the treatment of painfuldiabetic neuropathy: A randomized, double-blind,placebo-controlled pilot study. Pain Med 2005;6:225–34.
56 Goldstein DJ, Lu Y, Detke MJ, Lee TC, Iyengar S.Duloxetine vs placebo in patients with painful diabeticneuropathy. Pain 2005;116:109–18.
57 Freynhagen R, Strojek K, Griesing T, Whalen E, Balk-enohl M. Efficacy of pregabalin in neuropathic painevaluated in a 12-week, randomised, double-blind,multicentre, placebo-controlled trial of flexible- andfixed-dose regimens. Pain 2005;115:254–63.
58 Salim K, Schneider U, Burstein S, Hoy L, Karst M.Pain measurements and side effect profile of thenovel cannabinoid ajulemic acid. Neuropharmacol-ogy 2005;48:1164–71.
59 Richter RW, Portenoy R, Sharma U, et al. Relief ofpainful diabetic peripheral neuropathy with pregaba-lin: A randomized, placebo-controlled trial. J Pain2005;6:253–60.
60 Kochar DK, Garg P, Bumb RA, et al. Divalproexsodium in the management of post-herpetic neural-gia: A randomized double-blind placebo-controlledstudy. QJM 2005;98:29–34.
61 Lesser H, Sharma U, Lamoreaux L, Poole RM. Pre-gabalin relieves symptoms of painful diabetic neur-opathy: A randomized controlled trial. Neurology2004;63:2104–10.
62 Hahn K, Arendt G, Braun JS, et al. A placebo-controlled trial of gabapentin for painful HIV-associated sensory neuropathies. J Neurol2004;251:1260–6.
63 van de Vusse AC, Stomp-van den Berg SG, KesselsAH, Weber WE. Randomised controlled trial of gaba-pentin in Complex Regional Pain Syndrome type 1[ISRCTN84121379]. BMC Neurol 2004;4:13.
64 Raskin P, Donofrio PD, Rosenthal NR, et al. Topira-mate vs placebo in painful diabetic neuropathy: Anal-gesic and metabolic effects. Neurology 2004;63:865–73.
590
Cepeda et al.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
65 Thienel U, Neto W, Schwabe SK, Vijapurkar U. Topi-ramate in painful diabetic polyneuropathy: Findingsfrom three double-blind placebo-controlled trials.Acta Neurol Scand 2004;110:221–31.
66 Rowbotham MC, Goli V, Kunz NR, Lei D. Venlafaxineextended release in the treatment of painful diabeticneuropathy: A double-blind, placebo-controlledstudy. Pain 2004;110:697–706.
67 Rosenstock J, Tuchman M, Lamoreaux L, Sharma U.Pregabalin for the treatment of painful diabeticperipheral neuropathy: A double-blind, placebo-controlled trial. Pain 2004;110:628–38.
68 Svendsen KB, Jensen TS, Bach FW. Does the can-nabinoid dronabinol reduce central pain in multiplesclerosis? Randomised double blind placebo con-trolled crossover trial. BMJ 2004;329:253.
69 Caraceni A, Zecca E, Bonezzi C, et al. Gabapentinfor neuropathic cancer pain: A randomized controlledtrial from the Gabapentin Cancer Pain Study Group.J Clin Oncol 2004;22:2909–17.
70 Sabatowski R, Galvez R, Cherry DA, et al. Pregabalinreduces pain and improves sleep and mood distur-bances in patients with post-herpetic neuralgia:Results of a randomised, placebo-controlled clinicaltrial. Pain 2004;109:26–35.
71 Kochar DK, Rawat N, Agrawal RP, et al. Sodiumvalproate for painful diabetic neuropathy: A random-ized double-blind placebo-controlled study. QJM2004;97:33–8.
72 Wallace MS, Rowbotham M, Bennett GJ, et al. Amulticenter, double-blind, randomized, placebo-controlled crossover evaluation of a short course of4030W92 in patients with chronic neuropathic pain. JPain 2002;3:227–33.
73 Meier T, Wasner G, Faust M, et al. Efficacy oflidocaine patch 5% in the treatment of focal periph-eral neuropathic pain syndromes: A randomized,double-blind, placebo-controlled study. Pain2003;106:151–8.
74 Karst M, Salim K, Burstein S, et al. Analgesic effect ofthe synthetic cannabinoid CT-3 on chronic neuro-pathic pain: A randomized controlled trial. JAMA2003;290:1757–62.
75 Simpson DM, McArthur JC, Olney R, et al. Lamot-rigine for HIV-associated painful sensory neuropa-thies: A placebo-controlled trial. Neurology 2003;60:1508–14.
76 Gimbel JS, Richards P, Portenoy RK. Controlled-release oxycodone for pain in diabetic neuropathy: Arandomized controlled trial. Neurology 2003;60:927–34.
77 Wallace MS, Rowbotham MC, Katz NP, et al. A ran-domized, double-blind, placebo-controlled trial of aglycine antagonist in neuropathic pain. Neurology2002;59:1694–700.
78 De Grandis D, Minardi C. Acetyl-L-carnitine (levace-carnine) in the treatment of diabetic neuropathy.A long-term, randomised, double-blind, placebo-controlled study. Drugs R D 2002;3:223–31.
79 Serpell MG. Gabapentin in neuropathic pain syn-dromes: A randomised, double-blind, placebo-controlled trial. Pain 2002;99:557–66.
80 Hammack JE, Michalak JC, Loprinzi CL, et al. PhaseIII evaluation of nortriptyline for alleviation of symp-toms of cis-platinum-induced peripheral neuropathy.Pain 2002;98:195–203.
81 Eisenberg E, Lurie Y, Braker C, Daoud D, Ishay A.Lamotrigine reduces painful diabetic neuropathy: Arandomized, controlled study. Neurology 2001;57:505–9.
82 McCleane G. Topical application of doxepin hydro-chloride, capsaicin and a combination of both pro-duces analgesia in chronic human neuropathic pain:A randomized, double-blind, placebo-controlledstudy. Br J Clin Pharmacol 2000;49:574–9.
83 Backonja MM. Gabapentin monotherapy for thesymptomatic treatment of painful neuropathy: A mul-ticenter, double-blind, placebo-controlled trial inpatients with diabetes mellitus. Epilepsia 1999;40(suppl 6):S57–9.
84 McCleane G. 200 mg daily of lamotrigine has noanalgesic effect in neuropathic pain: A randomised,double-blind, placebo controlled trial. Pain1999;83:105–7.
85 Rowbotham M, Harden N, Stacey B, Bernstein P,Magnus-Miller L. Gabapentin for the treatment ofpostherpetic neuralgia: A randomized controlled trial.JAMA 1998;280:1837–42.
86 Backonja M, Beydoun A, Edwards KR, et al. Gaba-pentin for the symptomatic treatment of painful neu-ropathy in patients with diabetes mellitus: Arandomized controlled trial. JAMA 1998;280:1831–6.
87 Kong MF, Stubbs TA, King P, et al. The effect ofsingle doses of pramlintide on gastric emptying oftwo meals in men with IDDM. Diabetologia1998;41:577–83.
88 Ertas M, Sagduyu A, Arac N, Uludag B, Ertekin C.Use of levodopa to relieve pain from painful sym-metrical diabetic polyneuropathy. Pain 1998;75:257–9.
591
Type of Pain Influences Placebo Response
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
89 Oskarsson P, Ljunggren JG, Lins PE. Efficacy andsafety of mexiletine in the treatment of painful diabeticneuropathy. The Mexiletine Study Group. DiabetesCare 1997;20:1594–7.
90 Wright JM, Oki JC, Graves L III. Mexiletine in thesymptomatic treatment of diabetic peripheral neur-opathy. Ann Pharmacother 1997;31:29–34.
91 Onofrj M, Fulgente T, Melchionda D, et al.L-acetylcarnitine as a new therapeutic approach forperipheral neuropathies with pain. Int J Clin Pharma-col Res 1995;15:9–15.
92 Irving G, Jensen M, Cramer M, et al. Efficacy andtolerability of gastric-retentive gabapentin for thetreatment of postherpetic neuralgia: Results of adouble-blind, randomized, placebo-controlled clinicaltrial. Clin J Pain 2009;25:185–92.
93 Stacey BR, Barrett JA, Whalen E, Phillips KF, Row-botham MC. Pregabalin for postherpetic neuralgia:Placebo-controlled trial of fixed and flexible dosingregimens on allodynia and time to onset of pain relief.J Pain 2008;9:1006–17.
94 Boureau F, Legallicier P, Kabir-Ahmadi M. Tramadolin post-herpetic neuralgia: A randomized, double-blind, placebo-controlled trial. Pain 2003;104:323–31.
95 Dworkin RH, Corbin AE, Young JP Jr, et al. Pregaba-lin for the treatment of postherpetic neuralgia: A ran-domized, placebo-controlled trial. Neurology2003;60:1274–83.
96 Rice AS, Maton S. Gabapentin in postherpeticneuralgia: A randomised, double blind, placebo con-trolled study. Pain 2001;94:215–24.
97 Graff-Radford SB, Shaw LR, Naliboff BN. Amitrip-tyline and fluphenazine in the treatment of posther-petic neuralgia. Clin J Pain 2000;16:188–92.
98 Dowd NP, Day F, Timon D, Cunningham AJ, BrownL. Iontophoretic vincristine in the treatment of pos-therpetic neuralgia: A double-blind, randomized,controlled trial. J Pain Symptom Manage 1999;17:175–80.
99 Ben Abraham R, Marouani N, Weinbroum AA. Dex-tromethorphan mitigates phantom pain in canceramputees. Ann Surg Oncol 2003;10:268–74.
100 Maier C, Dertwinkel R, Mansourian N, et al. Efficacyof the NMDA-receptor antagonist memantine inpatients with chronic phantom limb pain—Results ofa randomized double-blinded, placebo-controlledtrial. Pain 2003;103:277–83.
101 Manicourt DH, Brasseur JP, Boutsen Y, DepreseuxG, Devogelaer JP. Role of alendronate in therapy forposttraumatic complex regional pain syndrome typeI of the lower extremity. Arthritis Rheum 2004;50:3690–7.
102 Nikolajsen L, Finnerup NB, Kramp S, et al. A ran-domized study of the effects of gabapentin onpostamputation pain. Anesthesiology 2006;105:1008–15.
103 Schley M, Topfner S, Wiech K, et al. Continuousbrachial plexus blockade in combination with theNMDA receptor antagonist memantine preventsphantom pain in acute traumatic upper limb ampu-tees. Eur J Pain 2007;11:299–308.
104 Schwartzman RJ, Alexander GM, Grothusen JR,et al. Outpatient intravenous ketamine for thetreatment of complex regional pain syndrome:A double-blind placebo controlled study. Pain2009;147:107–15.
105 Varenna M, Zucchi F, Ghiringhelli D, et al. Intrave-nous clodronate in the treatment of reflex sympa-thetic dystrophy syndrome. A randomized, doubleblind, placebo controlled study. J Rheumatol2000;27:1477–83.
106 Wu CL, Agarwal S, Tella PK, et al. Morphine vsmexiletine for treatment of postamputation pain:A randomized, placebo-controlled, crossover trial.Anesthesiology 2008;109:289–96.
107 Ho TW, Backonja M, Ma J, et al. Efficient assess-ment of neuropathic pain drugs in patients with smallfiber sensory neuropathies. Pain 2009;141:19–24.
108 Vilholm OJ, Cold S, Rasmussen L, Sindrup SH.Effect of levetiracetam on the postmastectomy painsyndrome. Eur J Neurol 2008;15:851–7.
109 Amin P, Sturrock ND. A pilot study of the beneficialeffects of amantadine in the treatment of painful dia-betic peripheral neuropathy. Diabet Med 2003;20:114–8.
110 Huse E, Larbig W, Flor H, Birbaumer N. The effect ofopioids on phantom limb pain and cortical reorgani-zation. Pain 2001;90:47–55.
111 Ellison N, Loprinzi CL, Kugler J, et al. Phase IIIplacebo-controlled trial of capsaicin cream in themanagement of surgical neuropathic pain in cancerpatients. J Clin Oncol 1997;15:2974–80.
112 Cepeda MS, Africano JM, Polo R, Alcala R, Carr DB.What decline in pain intensity is meaningful topatients with acute pain? Pain 2003;105:151–7.
592
Cepeda et al.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
113 Cepeda MS, Carr DB. No debate on the minimaldecline in pain intensity that patients can discern. AmJ Emerg Med 2006;24:391–2.
114 Dworkin RH, Turk DC, McDermott MP, et al. Inter-preting the clinical importance of group differences inchronic pain clinical trials: IMMPACT recommenda-tions. Pain 2009;146:238–44.
115 Cepeda MS, Boston R, Farrar JT, Strom BL. Com-parison of logistic regression vs propensity scorewhen the number of events is low and there aremultiple confounders. Am J Epidemiol 2003;158:280–7.
116 Brunoni AR, Lopes M, Kaptchuk TJ, Fregni F.Placebo response of non-pharmacological and phar-macological trials in major depression: A systematicreview and meta-analysis. PLoS ONE 2009;4:e4824.
117 Lee S, Malhotra B, Creanga D, Carlsson M, Glue P.A meta-analysis of the placebo response in antimus-carinic drug trials for overactive bladder. BMC MedRes Methodol 2009;9:55.
118 Ho TW, Fan X, Rodgers A, et al. Age effects onplacebo response rates in clinical trials of acuteagents for migraine: Pooled analysis of rizatriptantrials in adults. Cephalalgia 2009;29:711–8.
119 Bone M, Critchley P, Buggy DJ. Gabapentin in pos-tamputation phantom limb pain: A randomized,double-blind, placebo-controlled, cross-over study.Reg Anesth Pain Med 2002;27:481–6.
120 Breuer B, Pappagallo M, Knotkova H, et al. A ran-domized, double-blind, placebo-controlled, two-period, crossover, pilot trial of lamotrigine in patientswith central pain due to multiple sclerosis. Clin Ther2007;29:2022–30.
121 Chiou-Tan FY, Tuel SM, Johnson JC, et al. Effect ofmexiletine on spinal cord injury dysesthetic pain. AmJ Phys Med Rehabil 1996;75:84–7.
122 Finnerup NB, Sindrup SH, Bach FW, Johannesen IL,Jensen TS. Lamotrigine in spinal cord injury pain: Arandomized controlled trial. Pain 2002;96:375–83.
123 Galer BS, Twilling LL, Harle J, et al. Lack of efficacy ofriluzole in the treatment of peripheral neuropathicpain conditions. Neurology 2000;55:971–5.
124 Gilron I, Bailey JM, Tu D, et al. Morphine, gabapentin,or their combination for neuropathic pain. N Engl JMed 2005;352:1324–34.
125 Gorson KC, Schott C, Herman R, Ropper AH, RandWM. Gabapentin in the treatment of painful diabetic
neuropathy: A placebo controlled, double blind,crossover trial. J Neurol Neurosurg Psychiatry1999;66:251–2.
126 Haupt E, Ledermann H, Kopcke W. Benfotiamine inthe treatment of diabetic polyneuropathy—A three-week randomized, controlled pilot study (BEDIPstudy). Int J Clin Pharmacol Ther 2005;43:71–7.
127 Ho KY, Huh BK, White WD, Yeh CC, Miller EJ.Topical amitriptyline vs lidocaine in the treatment ofneuropathic pain. Clin J Pain 2008;24:51–5.
128 Kalso E, Tasmuth T, Neuvonen PJ. Amitriptylineeffectively relieves neuropathic pain following treat-ment of breast cancer. Pain 1996;64:293–302.
129 Kautio AL, Haanpaa M, Saarto T, Kalso E. Amitrip-tyline in the treatment of chemotherapy-induced neu-ropathic symptoms. J Pain Symptom Manage2008;35:31–9.
130 Kemper CA, Kent G, Burton S, Deresinski SC. Mexi-letine for HIV-infected patients with painful peripheralneuropathy: A double-blind, placebo-controlled,crossover treatment trial. J Acquir Immune DeficSyndr Hum Retrovirol 1998;19:367–72.
131 Khoromi S, Cui L, Nackers L, Max MB. Morphine,nortriptyline and their combination vs placebo inpatients with chronic lumbar root pain. Pain2007;130:66–75.
132 Khoromi S, Patsalides A, Parada S, et al. Topiramatein chronic lumbar radicular pain. J Pain 2005;6:829–36.
133 Levendoglu F, Ogun CO, Ozerbil O, Ogun TC, UgurluH. Gabapentin is a first line drug for the treatment ofneuropathic pain in spinal cord injury. Spine (Phila Pa1976) 2004;29:743–51.
134 Mariette X, Brouet JC, Chevret S, et al. A ran-domised double blind trial vs placebo does notconfirm the benefit of alpha-interferon in polyneur-opathy associated with monoclonal IgM. J NeurolNeurosurg Psychiatry 2000;69:279–80.
135 McCleane GJ. A randomised, double blind, placebocontrolled crossover study of the cholecystokinin 2antagonist L-365,260 as an adjunct to strong opioidsin chronic human neuropathic pain. Neurosci Lett2003;338:151–4.
136 Mercadante S, Arcuri E, Tirelli W, Villari P, CasuccioA. Amitriptyline in neuropathic cancer pain in patientson morphine therapy: A randomized placebo-controlled, double-blind crossover study. Tumori2002;88:239–42.
593
Type of Pain Influences Placebo Response
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
137 Morley JS, Bridson J, Nash TP, et al. Low-dosemethadone has an analgesic effect in neuropathicpain: A double-blind randomized controlled cross-over trial. Palliat Med 2003;17:576–87.
138 Nikolajsen L, Gottrup H, Kristensen AG, Jensen TS.Memantine (a N-methyl-D-aspartate receptorantagonist) in the treatment of neuropathic pain afteramputation or surgery: A randomized, double-blinded, cross-over study. Anesth Analg 2000;91:960–6.
139 Otto M, Bach FW, Jensen TS, Sindrup SH. Valproicacid has no effect on pain in polyneuropathy: A ran-domized, controlled trial. Neurology 2004;62:285–8.
140 Otto M, Bach FW, Jensen TS, Brosen K, Sindrup SH.Escitalopram in painful polyneuropathy: A random-ized, placebo-controlled, cross-over trial. Pain2008;139:275–83.
141 Raja SN, Haythornthwaite JA, Pappagallo M, et al.Opioids vs antidepressants in postherpetic neuralgia:A randomized, placebo-controlled trial. Neurology2002;59:1015–21.
142 Rintala DH, Holmes SA, Courtade D, et al. Compari-son of the effectiveness of amitriptyline and gabap-entin on chronic neuropathic pain in persons withspinal cord injury. Arch Phys Med Rehabil2007;88:1547–60.
143 Semenchuk MR, Sherman S, Davis B. Double-blind,randomized trial of bupropion SR for the treatment ofneuropathic pain. Neurology 2001;57:1583–8.
144 Smith DG, Ehde DM, Hanley MA, et al. Efficacy ofgabapentin in treating chronic phantom limb andresidual limb pain. J Rehabil Res Dev 2005;42:645–54.
145 Tai Q, Kirshblum S, Chen B, et al. Gabapentin in thetreatment of neuropathic pain after spinal cord injury:A prospective, randomized, double-blind, crossovertrial. J Spinal Cord Med 2002;25:100–5.
146 Tasmuth T, Hartel B, Kalso E. Venlafaxine in neuro-pathic pain following treatment of breast cancer. EurJ Pain 2002;6:17–24.
147 Vestergaard K, Andersen G, Gottrup H, KristensenBT, Jensen TS. Lamotrigine for central poststrokepain: A randomized controlled trial. Neurology2001;56:184–90.
148 Vrethem M, Boivie J, Arnqvist H, et al. A comparisona amitriptyline and maprotiline in the treatment ofpainful polyneuropathy in diabetics and nondiabetics.Clin J Pain 1997;13:313–23.
149 Wallace MS, Magnuson S, Ridgeway B. Efficacy oforal mexiletine for neuropathic pain with allodynia: Adouble-blind, placebo-controlled, crossover study.Reg Anesth Pain Med 2000;25:459–67.
150 Watson CP, Babul N. Efficacy of oxycodone in neu-ropathic pain: A randomized trial in postherpetic neu-ralgia. Neurology 1998;50:1837–41.
151 Watson CP, Moulin D, Watt-Watson J, Gordon A,Eisenhoffer J. Controlled-release oxycodone relievesneuropathic pain: A randomized controlled trial inpainful diabetic neuropathy. Pain 2003;105:71–8.
152 Wilder-Smith CH, Hill LT, Laurent S. Postamputationpain and sensory changes in treatment-naivepatients: Characteristics and responses to treatmentwith tramadol, amitriptyline, and placebo. Anesthesi-ology 2005;103:619–28.
153 Windebank AJ, Sorenson EJ, Civil R, O’Brien PC.Role of insulin-like growth factor-I in the treatment ofpainful small fiber predominant neuropathy. JPeripher Nerv Syst 2004;9:183–9.
154 Wymer JP, Simpson J, Sen D, Bongardt S. Efficacyand safety of lacosamide in diabetic neuropathicpain: An 18-week double-blind placebo-controlledtrial of fixed-dose regimens. Clin J Pain2009;25:376–85.
155 Yelland MJ, Poulos CJ, Pillans PI, et al. N-of-1 ran-domized trials to assess the efficacy of gabapentinfor chronic neuropathic pain. Pain Med2009;10:754–61.
156 Yuen KC, Baker NR, Rayman G. Treatment ofchronic painful diabetic neuropathy with isosorbidedinitrate spray: A double-blind placebo-controlledcross-over study. Diabetes Care 2002;25:1699–703.
157 Ziegler D, Movsesyan L, Mankovsky B, et al. Treat-ment of symptomatic polyneuropathy with actoveginin type 2 diabetic patients. Diabetes Care2009;32:1479–84.
594
Cepeda et al.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022
Appendix 1
Search Criteria Search Hits
1 Title = carpal tunnel syndrome (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) AND carpal tunnelsyndrome[Title]
20Type = RCTAny Field = placeboLanguage = English
2 Title = phantom (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) AND phantom[Title]
11Type = RCTAny field = placeboLanguage = English
3 Title = postamputation (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) ANDpostamputation[Title]
5Type = RCTAny Field = placeboLanguage = English
4 Title = central pain (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) AND central pain[Title]
32Type = RCTAny field = placeboLanguage = English
5 Title = complex regional pain (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) AND complex regionalpain[Title]
23Type = RCTAny field = placeboLanguage = English
6 Title = trigeminal (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) AND trigeminal[Title]
15Type = RCTAny Field = placeboLanguage = English
9 Title = reflex sympathetic dystrophy (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) AND reflex sympatheticdystrophy[Title]
9Type = RCTAny Field = placeboLanguage = English
10 Title = polyneuropathy (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) ANDpolyneuropathy[Title]
44Type = RCTAny field = placeboLanguage = English
11 Title = postmastectomy (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) ANDpostmastectomy[Title]
7Type = RCTAny field = placeboLanguage = English
12 Title = postthoracotomy (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) ANDpostthoracotomy[Title]
6Type = RCTAny field = placeboLanguage = English
15 Any field = neuropath* (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) AND neuropath*[Title]
594Any field = placeboType = RCTLanguage = English
16 Any field = neuralg* (((English[Language]) AND randomized controlledtrial[Publication Type]) AND placebo) AND neuralg*[Title]
186Any field = placeboType = RCTLanguage = English
Total 782
Published in 1995 to Nov 2009and no duplicates
Total 624
595
Type of Pain Influences Placebo Response
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/13/4/575/1873169 by guest on 30 September 2022