current status of prescribing pharmacists in florida
TRANSCRIPT

REGULAR ARTICLES
Journal ofPharmaceutical
Marketing & Management Current Statusof Prescribing Pharmacists in Florida:
Implications from the 1989Florida Prescriber Pharmacists
Practice Survey (FPPPS)
Volume 7Number 21992
CONTENTS Shelley I. White-MeansAlbert A. OkunadeEDITOR'S NOTE 1
REGULAR ARTICLES
Current Status of Prescribing Pharmacists in Florida:Implications from the 1989 Florida Prescriber PharmacistsPractice Survey (FPPPS)
Shelley 1. White-MeansAlbert A. Okunade
ABSTRACT. Providers of primary health care services. are see~n~expansion of their post-World War IT spheres of vrofesslOnal activi-ties. For example, on 1 October 1986, the Flonda State Board ofPharmacy extended prescribing authority to its pharmacists, effec~veMay 1987. This study presents the findings from a survey of Flondapharmacists conducted in the spring of 1989. Both the current status
3
Providers of primary health care services are seeking expansion of theirpost-World War II spheres of professional activities. For example, on 1October 1986, the Florida State Board of Pharmacy extended prescribingauthority to its pharmacists, effective May 1987. This study presents the
findings from a survey of Florida pharmacists conducted in the spring of1989. Both the current status of prescribing and motivations for choosinga prescribing role are investigated. Perceptions of community needs, thepharmacist's inherent abilities. and attitudes about how prescribingwould dictate a change in pharmacy practice are all crucial factors inthe pharmacist's decision.
Shelley I. White-Means, Ph.D., and Albert A. Okunade, Ph.D., are AssociateProfessors in the Department of Economics, Memphis State University, Memphis,TN 38152.
This research was supported by a grant from the Tennessee Board of Regentsand a supplemental faculty research grant. The results reported here do not neces-sarily represent the views of the grant sources.
The authors thank Cyril F. Chang, Richard D. Evans, Howard P. Tuckman, andthe JPMM editor and reviewers for insightful comments on earlier drafts. They alsothank Yeramilli Rao and Sandy Vora for proficient data entry.
Journal of Pharmaceutical Marketing & Management, Vol. 7(2) 1992© 1992 by The Haworth Press, Inc. All rights reserved 3
4 JOURNAL OF PHARMACEUTICAL MARKETING & MANAGEMENT Shelley I. White-Means and Albert A. Okunade 5
of prescribing and motivations for c~oosing a prescribing ~ol~~einvestigated. Perceptionsof commurutyneeds, ~e pharmacI.sts m-herent abilities and attitudesabout how prescnbmg woulddictate achange inph~acy practiceare all crucialfactors in thepharmacist'sdecision.
efficacy of the pharmacists' independent prescribing law under theFHCAA, and reflects on the lessons previously learned from imple-menting Florida's 1976 Drug Product Selection Law, (FDPSL) (6).
INTRODUCTIONMETHODS
Provid~rs of primary health care services are seeking expansion oftheir post-World War IIspheres of professional activities. Considerthe case of Florida pharmacists. On 1 October 1986, the Florida StateBoard of Pharmacy extended prescribing authority to its pharmacists,effective May 1987 (1). This new law (Florida Pharmacists Self-CareConsultant Law, SCCL) is unique in design and controversial in im-plications because it grants pharmacists independent authority to pre-scribe from a list of some 30 medications for mild, self-limiting medi-cal ailments (3).1 Thus, under the SCCL section of Florida's HealthCare Access Act (FHCAA), pharmacists can choose to order andprescribe these drugs autonomously, without physician supervision,and provide a door of access to mainstream medical care for themostly uninsured indigent population (4, 5). Although other stateshave granted pharmacists limited prescribing authority (California,Mississippi, and Washington), the new law in Florida is the first in thepost-World War IIera to grant pharmacists independent prescribingauthority.
The goals of this paper are to present the fmdings of the 1989Florida Prescriber Pharmacists Practice Survey (FPPPS) conductedby the authors to assess the current status of independent prescribingby Florida pharmacists two years after the law was enacted, to ex-amine correlates of the choice to prescribe, and to discuss policyimplications of the fmdings. The next section of this paper describesthe survey design, implementation, response rate, and sample. Sec-tion three presents a comparison of differences and similarities be-tween prescribing and nonprescribing pharmacists' practice settings,skills, and attitudes about prescribing. Section four focuses on bothpersonal and professional reasons why prescribing pharmacists electthat practice. The concluding section draws implications from thefindings, addresses potential policy initiatives designed to improve the
The 1989 FPPPS was fielded by the authors in the spring of 1989.Prior to administration, the instrument was scrutinized and certifiedby a select group of pharmacists in each of the practice settings, theExecutive Vice President of the Florida Pharmacy Association, mem-bers of the American College of Apothecaries, physicians of diversespecialties, and nationally r~nowned ?larketing resear~~ expert~. !heinstrument contained questions relatmg to the prescnbmg deCISIOnsof pharmacists, attitudes and perceptions about prescribing, practicesettings, and several sociodemographic attributes.
The census of active-status pharmacists who were licensed in flor-ida during 1989 showed 13,483 practitioners, about 64% of whomresided and practiced year-round in Florida. The list of pharmacistslicensed in Florida was obtained from the Department of ProfessionalRegulation in Tallahassee.
The FPPPS was administered through a mail questionnaire thatwas distributed to a stratified random sample of about 1,800 licensedpharmacists who resided in Florida. Stratification was gender-based,as male and female pharmacists are likely to differ in their decisionsto market prescribing services. This insight derives from the work ofChristensen and Bush, who found differences among male and femalephysicians' prescribing patterns (7).2 Given the population frame andassuming statistical sampling error, the approximate optimal samplesize is 300 (8). To attain the optimal size, 1,800 pharmacists weresurveyed (rather than the 1,200 required to achieve at least a 30% rateof return). Nonrespondents to the initial mailing were served remindernotices to assure an adequate response rate. Statistical hypothesis testsof differences in the mean values of responses of first versus secondmailings show that significant differences do not exist due to timingof the pharmacists' responses. The actual return rate of 32.3% (3.80individual respondents) exceeded that expected. However, some biasmay be present if the prescribing rate among nonrespondents differs
6 JOURNAL OF PHARMACElffICAL MARKETING & MANAGEMENT - Shelley I. White-Means and Albert A. Okunade 7
from that of respondents. This issue notwithstanding, our FPPPSresponse rate is similar to Eng's mail survey of 1,600 Florida consum-ers of pharmacy prescribing services; his response rate was 30% (3).
The majority of the responding pharmacists are employed in chaindrugstores (45%), provide computerized pharmacy services (91%),earn salaries ranging from $40,000 to $50,000 (48%), work full-time(89%), are not aware of other prescriber pharmacists (54%), and thinkprescriber pharmacists should receive higher fees than nonprescribers(67%). These pharmacists have practiced an average of21 years, with88% holding a B.S. in Pharmacy.
Figure 1
Practice Settings of Prescribers and Non-Prescribers
Prescribers
Supermarket1.0 %
(n-U
Other2.0 %(n-2)
RESULTS Institution7.0 %(n-7)
How different are pharmacists who choose to prescribe from thosewho do not? This question is answered by first partitioning the sampleaccording to whether or not the pharmacist prescribed medications atany time between the date of initial implementation of the law and thesurvey. Approximately 30% of the pharmacists who responded to thesurvey indicated this type of prescribing effort.
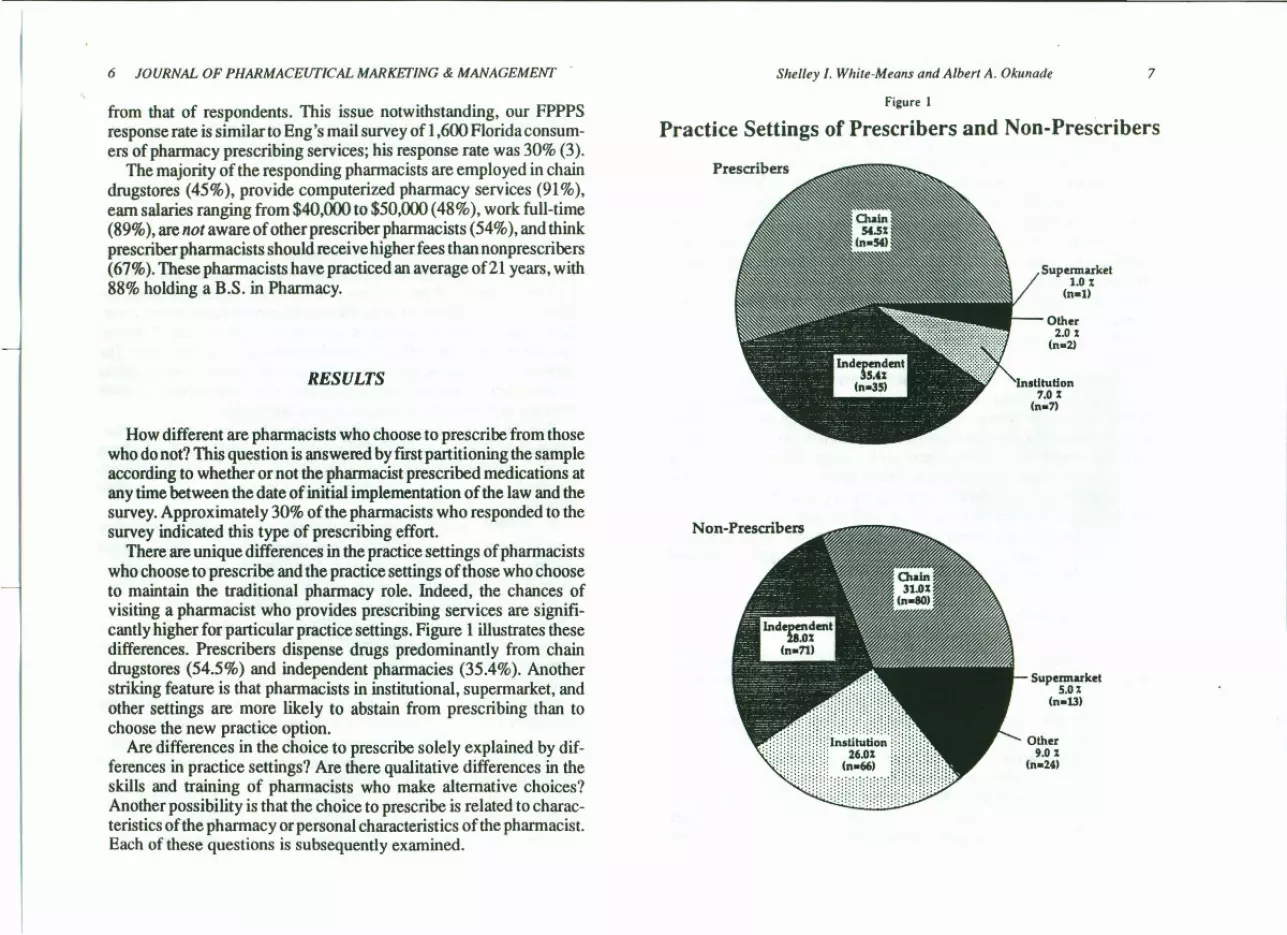
There are unique differences in the practice settings of pharmacistswho choose to prescribe and the practice settings of those who chooseto maintain the traditional pharmacy role. Indeed, the chances ofvisiting a pharmacist who provides prescribing services are signifi-cantly higher for particular practice settings. Figure 1 illustrates thesedifferences. Prescribers dispense drugs predominantly from chaindrugstores (54.5%) and independent pharmacies (35.4%). Anotherstriking feature is that pharmacists in institutional, supermarket, andother settings are more likely to abstain from prescribing than tochoose the new practice option.
Are differences in the choice to prescribe solely explained by dif-ferences in practice settings? Are there qualitative differences in theskills and training of pharmacists who make alternative choices?Another possibility is that the choice to prescribe is related to charac-teristics of the pharmacy or personal characteristics of the pharmacist.Each of these questions is subsequently examined.
Supermarket5.0%(n-13)
Other9.0 %(n-24)

8 JOURNAL OF PHARMACEUTICAL MARKETING & MANAGEMENT Shelley I. White-Means and Albert A. Okunade 5
Skills and Abilities efficacy of the pharmacists' independent prescribing law under theFHCAA, and reflects on the lessons previously learned from imple-menting Florida's 1976 Drug Product Selection Law, (FDPSL) (6).Table 1 contrasts the training and perceived skills of prescribers
and nonprescribers. Prescribers are slightly more likely to perceivethat they have enough training to prescribe (87.25% vs. 80.59%), lesslikelytothinkaPhann.D. is needed (10.68% vs.16.91 %), andsignifi-cantly more likely to view their inherent skills as comparable to thoseof physicians (90.82% vs. 80.59%). Additionally, note that the per-centage of nonprescribers who believe that they have enough trainingto prescribe is the same as the percentage of nonprescribers who viewtheir skills as equal to or better than those of physicians. Amongprescribing pharmacists, a larger percentage view their skills as com-parable to physicians than view their training as sufficient to pre-scribe.
These perceptions of competency contrast with the informationprovided on maximum education and experience. Prescribers havefewer years of education than nonprescribers. They are more likelythan nonprescribers to complete their education with the procurementof a B.S. degree. Moreover, prescribers have significantly fewer yearsof experience than nonprescribers. On the other hand, the data on yearof licensure and completion of education suggest that prescribers'added confidence in their prescribing abilities may result from differ-ences in the content of their education; prescribers completed theirtraining an average of three years subsequent to nonprescribers andreceived their licenses four years later.
METHODS
Weexamined the pharmacy and pharmacists' characteristics usingthree approaches. First, we explored whether unique differences inthe physical environment in which the pharmacist practices are re-lated to the prescribing decision; that is, we hypothesized that if ~epractice setting provides a more convenient atmosphere for pres.c~b~ing, then the pharmacist will be more likely to choose a prescnbmgpractice. Second, we hypothesized that there may be a relationshipbetween the personal sociodemographic characteristics of pharma-cists and the decision to prescribe. Finally, we examined whetherpharmacists perceive that prescribing would lead to changes in their
The 1989 FPPPS was fielded by the authors in the spring of 1989.Prior to administration, the instrument was scrutinized and certifiedby a select group of pharmacists in-each of the practice settings, theExecutive Vice President of the Florida Pharmacy Association, mem-bers of the American College of Apothecaries, physicians of diversespecialties, and nationally renowned marketing research experts. Theinstrument contained questions relating to the prescribing decisionsof pharmacists, attitudes and perceptions about prescribing, practicesettings, and several sociodemographic attributes.
The census of active-status pharmacists who were licensed in Flor-ida during 1989 showed 13,483 practitioners, about 64% of whomresided and practiced year-round in Florida. The list of pharmacistslicensed in Florida was obtained from the Department of,ProfessionalRegulation in Tallahassee.
The FPPPS was administered through a mail questionnaire thatwas distributed to a stratified random sample of about 1,800 licensedpharmacists who resided in Florida. Stratification was gender-based,as male and female pharmacists are likely to differ in their decisionsto market prescribing services. This insight derives from the work ofChristensen and Bush, who found differences among male and femalephysicians' prescribing patterns (7).2 Given the population frame andassuming statistical sampling error, the approximate optimal samplesize is 300 (8). To attain the optimal size, 1,800 pharmacists weresurveyed (rather than the 1,200 required to achieve at least a 30% rateof return). Nonrespondents to the initial mailing were served remindernotices to assure an adequate response rate. Statistical hypothesis testsof differences in the mean values of responses of first versus secondmailings show that significant differences do not exist due to timingof the pharmacists' responses. The actual return rate of 32.3% (380individual respondents) exceeded that expected. However, some biasmay be present if the prescribing rate among nonrespondents differs
Pharmacy and Pharmacists' Characteristics

8 JOURNAL OF PHARMACEUFICAL MARKETING & MANAGEMENT
Skills and Abilities
Table 1 contrasts the training and perceived skills of prescribersand nonprescribers. Prescribers are slightly more likely to perceivethat they have enough training to prescribe (87.25% vs. 80.59%), lesslikely to think a Pharm.D. is needed (10.68 % vs. 16.91%), and signifi-cantly more likely to view their inherent skills as comparable to thoseof physicians (90.82% vs. 80.59%). Additionally, note that the per-centage of nonprescribers who believe that they have enough trainingto prescribe is the same as the percentage of nonprescribers who viewtheir skills as equal to or better than those of physicians. Amongprescribing pharmacists, a larger percentage view their skills as com-parable to physicians than view their training as sufficient to pre-scribe.
These perceptions of competency contrast with the informationprovided on maximum education and experience. Prescribers havefewer years of education than nonprescribers. They are more likelythan nonprescribers to complete their education with the procurementof a B.S. degree. Moreover, prescribers have significantly fewer yearsof experience than nonprescribers. On the other hand, the data on yearof licensure and completion of education suggest that prescribers'added confidence in their prescribing abilities may result from differ-ences in the content of their education; prescribers completed theirtraining an average of three years subsequent to nonprescribers andreceived their licenses four years later.
Pharmacy and Pharmacists' Characteristics
We examined the pharmacy and pharmacists' characteristics usingthree approaches. First, we explored whether unique differences inthe physical environment in which the pharmacist practices are re-lated to the prescribing decision; that is, we hypothesized that if thepractice setting provides a more convenient atmosphere for prescrib-ing, then the pharmacist will be more likely to choose a prescribingpractice. Second, we hypothesized that there may be a relationshipbetween the personal sociodemographic characteristics of pharma-cists and the decision to prescribe. Finally, we examined whetherpharmacists perceive that prescribing would lead to changes in their
Shelley I. White-Means and Albert A. Okunade 9
Table 1: Pharmacists' Skills and Abilities
Skill/Ability NonprescribersPrescribers
'Perceive you haveenough training toprescribe"(% = yes)
"Perceive onlyclinicaJIy trainedpharmacists withPharmacy Doctorateshould prescribe"
(% = yes)
'Perceive differencesin the quality of yourprescribing relativeto physicians. i.e.,pharmacist prescribingis the same or betterquality" (% = yes)
Educational AttainmentB.S. PharmacyPharm. Doc.MastersPh.D./Other
(%)
Year completededucation
(mean)
Year of professionallicensure (mean)
Years Practiced as aPharmacist (mean)
87.25 80.59 2.28 (df = I. P = .(31)
10.68 16.91 2.25 (df= 1. p=.134)
90.82 80.59 5.15 (df= I, p=.076)
90.20 84.981.96 2.566.86 5.490.98 6.96
1975 1972
1969 1965
19.48 22.89
5.589 (de = 3, P = .232)
[-1.73] (p=.085)
[-2.51] (p =.013)
[2.33J (p=.021)
styles of delivering services and whether these perceptions are relatedto the prescribing decision.
The practice settings of prescribers and nonprescribers are signifi-cantly different in three important ways (Table 2). Prescribers aremore likely to have employer requirements that they prescribe (9.09%vs. 2.07%). Additionally, the pharmacy is more likely to maintainpatient profiles (95.96% vs. 90.08%), as well as have a private con-
10 JOURNAL OF PHARMACEUI'ICAL MARKElING & MANAGEMENT
Table 2: Pharmacy and Pharmacists' Characteristics of Prescribers and Nonprescnbers
Characteristic Prescribers
PharmacyOffers computerized
services (%) 91.92Maintains patient
profiles (%) 95.96Private consultation
area (%) 32.32Offers emergency
services (%) 36.36Requires Prescribing
services (%) 9.09
Hours of WorkFull-time (%) 87.50Part-time (%) 12.50
GenderMale (%) 94.12Female (%) 5.88
Marital StatusMarried (%) 88.24Non-married (%) 11.76
RaceWhite (%) 89.32Nonwhite (%) 10.68
Age18-29 5.8830-39 40.2040-49 23.53SO-59 18.6360-69 8.82
. 70+ 2.94
Income ($)< $40,000 (%) 16.85$40,000 - $50,000 (%) 53.93> $50,000 (%) 29.21
Children (mean) 1.35
Nonprescribers
88.43 0.91 (df= I, p= .341)
3.22 (df ••I. p-.073)
4.08 (df-I, p-.043)
0.21 (df"l, p-.649)
8.81 (df ••1, p =.003)
90.08
21.90
39.00
2.07
87.5512.45
0.00 (df=], p =.990)
88.8911.01
2.46 (df ••1. pa.292)
76.4723.53
6.34 (df ••1. p ••.012)
90.189.82
0.61 (df •• l, p=.804)
4.7824.6323.1624.6317.285.51
2.13 (df ••5. p= .033)
28.0551.5820.36
5.44 (df ••2. p=.066)
1.06 [-1.88] (p ••.062)
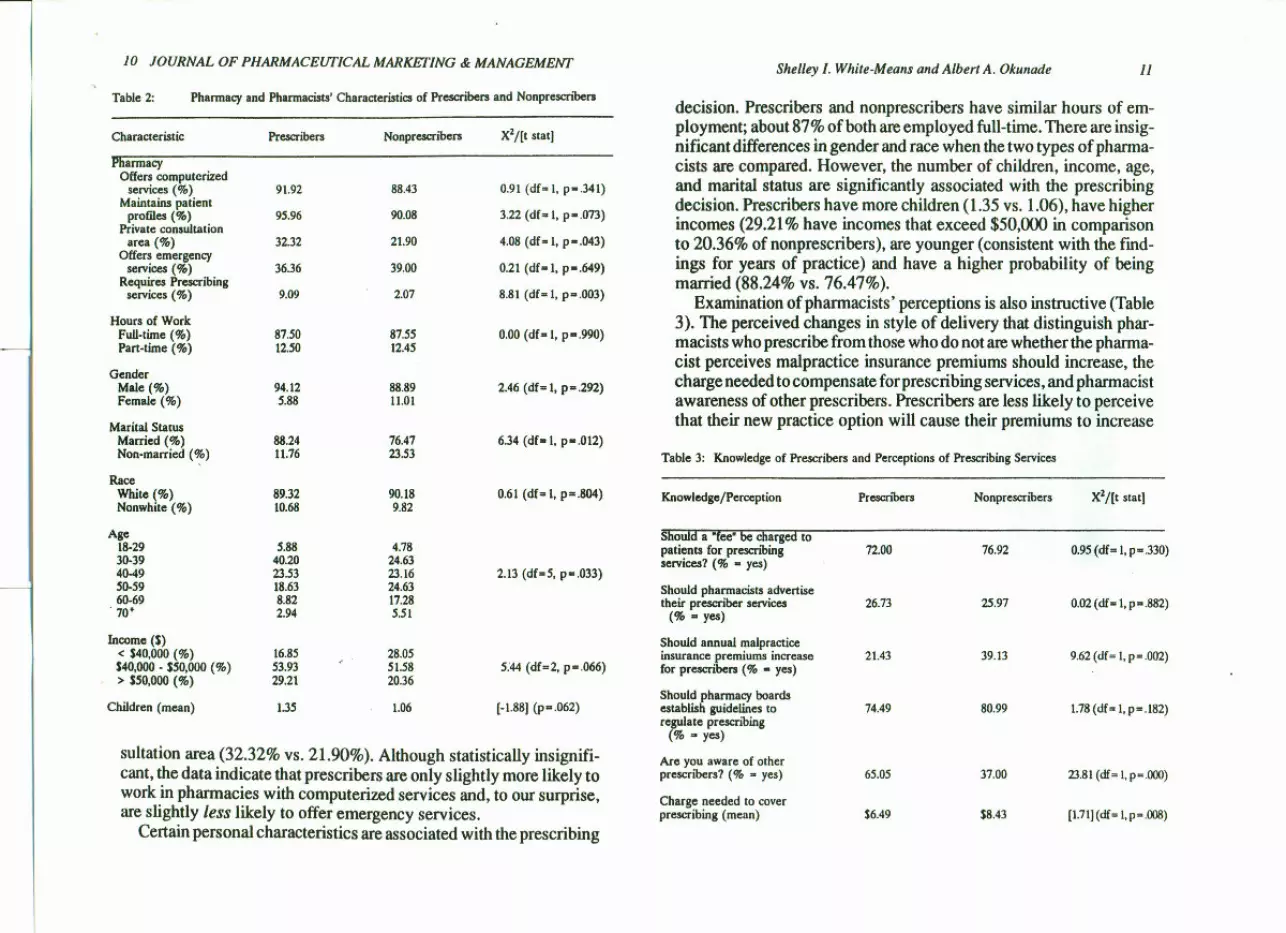
sultation area (32.32% vs. 21.90%). Although statistically insignifi-cant, the data indicate that prescribers are only slightly more likely towork in pharmacies with computerized services and, to our surprise,are slightly less likely to offer emergency services.
Certain personal characteristics are associated with the prescribing
Shelley I. White-Means and Albert A. Okunade 11
decision. Prescribers and nonprescribers have similar hours of em-ployment; about 87% of both are employed full-time. There are insig-nificant differences in gender and race when the two types of pharma-cists are compared. However, the number of children, income, age,and marital status are significantly associated with the prescribingdecision. Prescribers have more children (1.35 vs. 1.06), have higherincomes (29.21% have incomes that exceed $50,000 in comparisonto 20.36% of nonprescribers), are younger (consistent with the find-ings for years of practice) and have a higher probability of beingmarried (88.24% vs. 76.47%).
Examination of pharmacists' perceptions is also instructive (Table3). The perceived changes in style of delivery that distinguish phar-macists who prescribe from those who do not are whether the pharma-cist perceives malpractice insurance premiums should increase, thecharge needed to compensate for prescribing services, and pharmacistawareness of other prescribers. Prescribers are less likely to perceivethat their new practice option will cause their premiums to increase
Table 3: Knowledge of Prescribers and Perceptions of Prescribing Services
Knowledge/Perception Prescnbers Nonprescribers X2/[t stat]
72.00 76.92 0.95 (df= 1.p=.330)
26.73 25.97 0.02 (df "I, p" .882)
21.43 39.13 9.62(df = I, P= .002)
74.49 80.99 1.78(df: I. p=.182)
ShoUld a "fee" be charged topatients for prescnbingservices? (% - yes)
Should pharmacists advertisetheir prescriber services
(% •• yes)
Should annual malpracticeinsurance premiums increasefor prescribers (% - yes)
Should pharmacy boardsestablish guidelines toregulate prescribing
(% •• yes)
Are you aware of otherprescribers? (% •• yes) 65.05 37.00 23.81(df= I, p=.OOO)
Charge needed to coverprescribing (mean) $6.49 $8.43 [1.71](df•• l,p".OO8)
12 JOURNAL OF PHARMACEUTICAL MARKEfING & MANAGEMENJ Shelley I. White-Means and Albert A. Okunade J3
(21.43% vs. 39.13%). This response is consistent with their tendencyto perceive that their independent prescribing skills are comparable tothose of physicians; that is, if prescribing pharmacists have assessedtheir skills appropriately and have training that allows them to providequality prescribing services, the chances of lawsuits are low, and thelikelihood of increased malpractice premiums is also low.
Similarly, prescribers indicate that the charges they perceived suffi-cient to cover consultation time are lower than those suggested bynonprescribers ($6.49 vs. $8.43). It is unclear whether this differencein perception of the prescribing price is related to differences in per-ceived risks of prescribing (prescribers perceive a lower risk and thuscharge a lower price), to differences in experience (nonprescribershave more years of experience and may require a higher price for theirtime), or to differences in employer fmancing of malpractice insur-ance.
Prescribers are more likely to have peers who also prescribe. In-deed, prescribers are almost two times more likely to be aware of otherprescribers (65.05% vs. 37%). Is the decision to prescribe related toone's perception of how peers will view the decision?
Some statistically insignificant differences between prescribers'and nonprescribers' perceptions of the role of prescribing in pharma-cy practice also deserve mention. Nonprescribers are slightly morelikely to think that a fee should be charged for prescribing (76.92% vs.72%) and that pharmacy boards should establish guidelines for pre-scribers (80.99% vs. 74.49%). There are almost no differences in theperceptions that prescribers should advertise; both prescribers andnonprescribers think advertising should be limited. In an open-endedquestion, pharmacists were asked to elaborate on the reasons for theirviews on prescriber advertising. The general perception among phar-macists who opposed advertising was that it was unprofessional andwould encourage competition among prescribers and/or with physi-cians.
cause you engage in prescribing?" 98.2% of the prescribers claimedthey had not experienced increased earnings from their prescribingpractice. This observed distribution of responses may be due to pre-scribing activities accounting for a small percentage of total receipts(92.6% of prescribers replied "No" to the question, "Have you expe-rienced an increase in your overall prescription sales volume becauseyou now prescribe?").
Although most prescribing pharmacists expected to but do not earnadditional income from an elective prescribing practice, nonmonetaryreturns to their prescribing efforts appear to be more important. Es-sentially, over 33.8% of the responding prescribers claimed that itenhanced their personal satisfaction, about 35.1% agreed it improvedpatient (customer) relations, and roughly 31.5% thought prescribinghad augmented their professional status (personal prestige) as a pri-mary health care provider.
To gain a deeper understanding of why prescriber pharmacists mayhave elected to prescribe, prescribers were asked to respond, in theirown words, to an open-ended survey question: "When you prescribe,are you providing a needed health care service in the community? Ifyes, please explain." Their responses polarize to three groups, withthe largest (60%) claiming health care cost containment (that is, low-cost, more affordable service to the consumers) as the overridingfactor. Roughly 37% of the prescribers thought services they provideare convenient alternatives to physicians' treatments for minor, self-limiting ailments (as the self-care law mandated). This group alsoclaimed that a pharmacist's diagnosis and prescribing for non-life-threatening adverse health conditions are more timely and promotecontinuity of care (relative to a physician's).
DISCUSSION
Pharmacists' Motives for Prescribing The rationale for enacting FHCAA was to make traditional healthcare more accessible to indigent populations as health care costs con-tinue to escalate. The Florida self-care law attempts to achieve thisobjective by granting pharmacists complete autonomy in diagnosingcommon ailments and prescribing medications from a closed formu-lary, without direct physician intervention. This study surveyed Flori-
The survey asked prescribers about their prescribing practice toexplore further the prescribing pharmacists' perceptions. Whenasked, "Have you experienced an increase in your base salary be-
14 JOURNAL OF PHARMACEUTICAL MARKETING & MANAGEMENT Shelley I. White-Means and Albert A. Okunade 15
da pharmacists in 1989 to assess the current status of their prescribingpractice.
While exploratory, this paper has provided some initial clues aboutpharmacists' choices to prescribe when given legal authorization.Perceptions of community needs, the pharmacist's inherent abilities,and attitudes about how prescribing would dictate a change in phar-macy practice are all crucial factors in the pharmacist's decision.Specifically, the results indicate that about 30% of Florida pharma-cists currently engage in independent prescribing activities 2 yearsafter the law was enacted; pharmacists do not augment their incomesby prescribing, as independent prescribing, to date, does not appearto be generating enough revenues to cover associated costs; pharma-cists who prescribe are more aware of peers who prescribe; prescrib-ers are more likely to be married, recently licensed, younger (less than40 years old), practice in settings that are more conducive to a pre-scribing practice (e.g., keeping patient profiles, using computerizedpharmacy services, or working in noninstitutionalized pharmacieswhere physicians are absent), and believe that pharmacy boardsshould regulate pharmacists' prescribing activities.
Since prescribing and nonprescribing pharmacists felt equallywell-trained, employers may encourage higher rates of participationamong current nonprescribers by making prescribing a requirementfor employment, changing the facility layout and/or patient record-keeping mechanisms, offering prescri bers supplemental income, and/or providing assistance in covering the prescriber's malpractice insur-ance.
Does the percentage of Florida pharmacists engaged in prescribing(30% ) compare favorably with other states where some form of pre-scribing is granted pharmacists'P The great disparity in both the de-signs and the implementations of pharmacist prescribing in Floridaand other states provided no logical basis for comparing prescribingrates. This is because Washington, Mississippi, and California allowlimited prescribing by pharmacists, while Florida allows independentlimited prescribing without physician guidance.
Only one-third of the pharmacists in Florida elected to prescribe.Is this level of prescribing practice sufficient to enhance the serviceoptions of indigent patients in Florida? Do patients who obtain pre-scriptions from pharmacists perceive that they are provided with a
low-cost, alternative health care system? These questions are unan-swered by the present study. Future research that examines both thedemand and the supply side of prescribing would provide usefulinformation on the design of this service option to meet the needs ofpharmacists and their clientele.
Finally, it is uncertain whether a longer time period must elapse forFlorida pharmacists, physicians, and health care consumers to adaptto the intent and provisions of the law. From a historical perspective,it is interesting to note that there was very little change in the productselection and brand interchange behaviors of Florida pharmacists oneyear and four years after Florida's Drug Product Selection Law of1976 was implemented (6). The drug product selection law and inde-pendent prescribing laws are both discretionary for consumers andpharmacists. Essentially, the current adoption rate of pharmacists'prescribing may not increase appreciably with the passage of time ifleft to operate unaided. Unlike the drug product selection law, howev-er, the factors identified in this study as influencing the probability ofpharmacist prescribing could be used to launch timely policy initia-tives that are designed to increase pharmacists' participation rate (be-yond the current 30%), primarily if such efforts would increase com-munity access to quality prescribing services.
NOTES
1. The categories (specific drugs) of medications most often prescribed byoutpatient pharmacists under the Florida Pharmacists Self-Care Consultant Law,according to Cohen's survey, are scabicides/pediculocides (Kwell<ID,lindane), ear-drops' (Domeboro®, Auralgan ®), antifungals (Lotrimin ®, generics), and nonster-oidal anti-inflammatories (ibuprofen) (2).
2. While other bases for stratification (such as geographical location of practicesetting-type (or size) of practice establishment, year licensed, etc.) may be pre-ferred, they were not available ex ante for sample selection from the data files atthe Florida Department of Professional Regulation. The only information availableon the population of some 13,483 active-status pharmacists were their names,license numbers, and residential (not employment) mailing addresses. Thus, gen-der appears to be the only natural variate for stratification ex ante sample selection.Consequently, a table of random numbers was used to select sample elementsrandomly and independently (without replacement) from each gender subpopula-tion, based on the Neyman allocation scheme for implementing stratified randomsampling (8).
3. Response to this question requires an examination of the purpose, design, and

/6 JOURNAL OF PHARMACEUTICAL MARKETING & MANAGEMENT
implementation of pharmacist prescribing in other states compared to Florida.Florida pharmacists, clinically trained or otherwise, have complete autonomy toprescribe drugs from a restricted formulary for low-level, self-limiting ailments.Prescribing practice is elective. In 1980, Washington became the first state toimplement limited prescribing authority for pharmacists, with physician guidance.In 1983, Mississippi granted limited prescribing authority to institutional pharma-cists only. Finally, California's Assembly Bill 717 allowed two pilot projects inwhich pharmacists were certified (having passed a physical assessment course anda certifying examination) to prescribe and administer drugs under general supervi-sion of a physician, limited implementation to two inpatient sites (one of which wasthe University of Southern California) and seven outpatient settings, trained pre-scriber pharmacists from among those already in clinical areas, allowed a verybroad project formulary (excepting narcotic and Schedule Il and ill drugs) for avariety of disease states, provided a standardized triplicate prescription form forprescribing pharmacists (to evaluate their prescribing competency), and included30 certified pharmacists whose prescribing tasks were restricted to nine sites (9).
REFERENCES
1. State of Florida. Prescription of certain medicinal drugs. In: Rules of theprofessional regulation (Sec. 465.186). Tallahassee, FL: Board of Pharmacy, 1985.
2. Cohen H. Most Florida pharmacists not prescribing. Drug Store News1987;9(Feb 16):IP9-IPI6.
3. Eng HJ. Developments in pharmacy practice. The pharmacist as prescriber.I Clin Pharm Ther 1987; 12:237-42.
4. Butler PA. Too poor to be sick: access to medical care for the uninsured.Washington, DC: American Public Health Association, 1988.
5. Jones KR. The Florida Health Care Access Act: a blended regulatory/compet-itive approach to the indigent health care problem. I Health Polit Policy Law1989; 14:261-85.
6. Clouse EH, McCormick WC, Angom RA, Kimberlin CL, Bradham DO.Drug product selection: the Florida experience revisited. Am I Public Health1985;75:283-4.
7. Christensen DB, Bush PI. Drug prescribing: patterns, problems, and propos-als. Soc Sci Med 1981;15A:343-55.
8. Cochran WG. Sampling techniques. New York: John Wiley, 1977.9. Stimmel GL, McGhan WE The pharmacist as prescriber of drug therapy: the
USC pilot project. Drug Intell Clin Pharm 1981;15:665-72.
EDITOR
MICKEY C. SMITH, School of Pharmacy, UniverslJy of Mississippi
MANAGING EDITOR
nnrs A. FISHER. Univemty of Mississippi
POSTER PAPER EDITOR
W. MICHAEL DICKSON. Univemty of South Carolina
BDITORIAL BOARD
AT URGE
ROBERT SlATER (Marion Merrell Dow, Inc.)WilliAM W. BRADLEY (Nonprescription Drug Manufacturen Auociation)ALBERT WERTHEIMER (Philadelpbia College of Pharmacy and Science)HARRY SMITH (Univeraity of Kentucky)RICHARD JACKSON (Mercer University)STEVEN CHAPPElL (lMS America, Ltd.)D. C. HUFFMAN (National Auociation of Retail Druggista)JACK ROBBINS (ScbeM.-Plougb)RICHARD lEVY (National Pharmaceutical Council)HERMAN lAZARUS (Univeraity of Alabama at Birmingham)DEV PATHAK (Ohio State Univeraity)DAVID KNAPP (Univeraity of Maryland)LEE STRANDBERG (Oregon Slate Univeraity)WIWAM McCORMICK (Univeraity of HOUlton)ROBERT ZELNIO (Paragon Reaearch '" Conaulting)PATRICIA BUSH (Georgetown Univeraity)BENJAMIN F. BANAHAN, III (Univeraity of Miuinippi)U:ONARD J. DeMINO (National Auociation of Chain Drug Stores)JOSEPH B. WIEDERHOLT (Univeraity ofWllconain at Madison)O. JOSEPH NORWOOD (Univeraity of North Carolina)
REGIONAL
IAN JONES (Univenity of Bradford)S. I. BENRIMOI (Univeraity of Sydney)NO CHU TECK (lMS Pacific, Ltd.)HAROLD SEGAL (Univeraity of Toronto)SUnT DAS (Univeraa1Drug Houae)
EuropeAuatraliaFar ButCanadaAsia
EX OFFICIO
CHARLOTTE SIBLEY (Briltol-Myera Squibb)-IntemationalPharmaceutica1 Marlc.etingResearch OroupHOlLY MASON (Purdue Univeraity)-Pharmacy Administration Teachera Section, AACPPATRICK L. McKERCHER (Upjohn)-Economic, Marlc.etingand Management Science Section, AAPSFRANCIS B. PALUMBO (Univeraity of Maryland)-Economic, Social and Adminiatrativo Sciences
Section, Academy of Pharmaceutical Research and ScienceSAM OSIRIM (McNeil Pharmaceutical)-PharmaceuticaIMarlc.eting Research Group
Ex officio memberaofthe editorial board are appointed to represent the pertinentviewpoinll of their respectiveorlanizatiorll. Their inclusion does not represent an endonement of lPMM, nor of any specjfic articlespublished therein.