secondary microvascular tongue reconstruction: functional results
TRANSCRIPT
SECONDARY MICROVASCULAR TONGUE RECONSTRUCTION: FUNCTIONAL RESULTS
Arthur H. Salibian, MD, Glenn R. Allison, MD, Victor V. Streltow, MD, Mark E. Krugman, MD, Irving Rappaport, DMD, MD, Betty L. McMicken, PhD, and Terry L. Etchepare, MS
Between 1978 and 1991, 56 microvascular composite flaps were used for oromandibular reconstructions: 15 for primary to- tal and subtotal tongue reconstruction and five for secondary major tongue reconstruction. The delayed reconstructions were performed to improve the oral and pharyngeal phases of swal- lowing. Using a floor of the mouth composite bone grafting tech- nique to reposition the tongue and obliterate the oral dead space intraoral food transport was improved (three of five pa- tients), but aspiration persisted (three of four patients). When compared with 10 patients evaluated for primary total and sub- total tongue reconstruction the primary reconstruction group showed superior swallowing (eight dynamic oral transport, no aspiration) and speech results. The poor results of secondary reconstruction are attributed to scarring and irreversible damage to remaining functional muscles involved in protecting the laryn- geal aditus.
0 1993 John Wiley 8, Sons, Inc. HEAD & NECK 1993;15:389-397
Patients with major tongue resection, including total glossectomy, have a wide variety of deficits ranging from loss of dynamic intraoral food transport to severe aspiration of normal salivary secretions. 1,2 While some of these functional problems can be treated with aggressive physical
From the Center for Disorclers of the Head and Neck Western Medical Center Santa Ana. Califorriia
Address reprint requests lo Dr Salibian, 1201 West La Veta Avenue, Suite 603 Orange CA 92668
Accepted for publication Cecernber 23 1992
0 1993 John Wiley & Sons, Inc CCC 01 48-6403193105038El- 09
therapy others require additional operations to prevent aspiration and improve swallowing. These ancillary procedures such as epiglotopexy, laryngoplasty, glottic coverage, cricopharyngeus myotomy, laryngeal suspension, and laryngec- t ~ m y ~ - ~ are designed to prevent aspiration rather than improve oropharyngeal function. Methods to enhance tongue function and facili- tate oral food movement have mostly depended on prosthetic tongue or palatal devices rather than Very little has been written about corrective tongue surgery in patients who have established tongue deformities with im- paired swallowing.
This article describes a method of secondary tongue reconstruction using a composite mi- crovascular flap to improve the oral and pharyn- geal phases of swallowing in patients who are unable to actively transport food from the mouth to the esophagus. Five patients reconstructed with this method for established swallowing and speech deficits following major glossectomy form the basis of this study. The postoperative func- tional results of these five patients are described and compared with 10 patients who were evalu- ated after immediate total or subtotal tongue re- construction; the results of eight primary recon- structions have been described previously. lo
PATIENTS AND METHODS
Between 1978 and 1991, 56 microvascular com- posite flaps were used to reconstruct oromandib-
Microvascular Tongue Reconstruction HEAD & NECK Septernber/October 1993 389
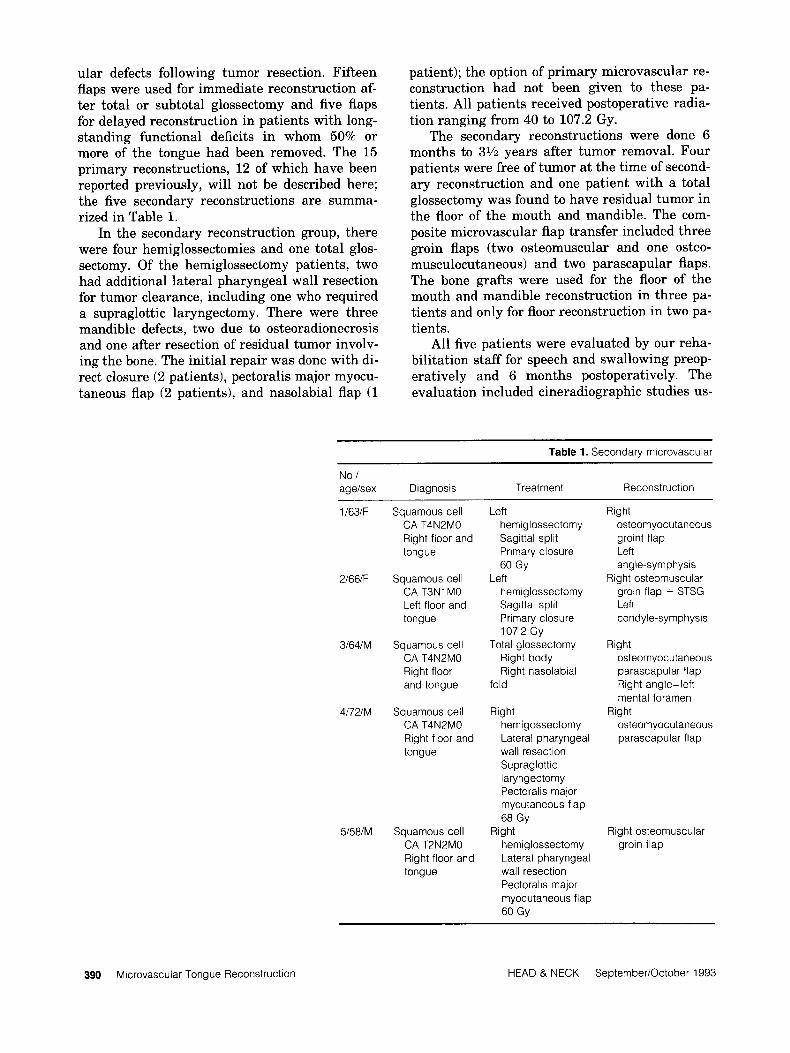
ular defects following tumor resection. Fifteen flaps were used for immediate reconstruction af- ter total or subtotal glossectomy and five flaps for delayed reconstruction in patients with long- standing functional deficits in whom 50% or more of the tongue had been removed. The 15 primary reconstructions, 12 of which have been reported previously, will not be described here; the five secondary reconstructions are summa- rized in Table 1.
In the secondary reconstruction group, there were four hemiglossectomies and one total glos- sectomy. Of the hemiglossectomy patients, two had additional lateral pharyngeal wall resection for tumor clearance, including one who required a supraglottic laryngectomy. There were three mandible defects, two due to osteoradionecrosis and one after resection of residual tumor involv- ing the bone. The initial repair was done with di- rect closure (2 patients), pectoralis major myocu- taneous flap (2 patients), and nasolabial flap (1
patient); the option of primary microvascular re- construction had not been given to these pa- tients. All patients received postoperative radia- tion ranging from 40 to 107.2 Gy.
The secondary reconstructions were done 6 months to 3% years after tumor removal. Four patients were free of tumor at the time of second- ary reconstruction and one patient with a total glossectomy was found to have residual tumor in the floor of the mouth and mandible. The com- posite microvascular flap transfer included three groin flaps (two osteomuscular and one osteo- musculocutaneous) and two parascapular flaps. The bone grafts were used for the floor of the mouth and mandible reconstruction in three pa- tients and only for floor reconstruction in two pa- tients.
All five patients were evaluated by our reha- bilitation staff for speech and swallowing preop- eratively and 6 months postoperatively. The evaluation included cineradiographic studies us-
Table 1. Secondary microvascular
No./ agelsex Diagnosis Treatment Reconstruction
1163lF
2166lF
3164lM
4172lM
5158lM
Squamous cell CA T4N2MO Right floor and tongue
Squamous cell CA T3N1 MO Left floor and tongue
Squamous cell CA T4N2MO Right floor and tongue
Squamous cell CA T4N2MO Right floor and tongue
Squamous cell CA T2N2MO Right floor and tongue
Left herniglossectomy Sagittal split Primary closure 60 Gy
herniglossectomy Sagittal split Primary closure 107.2 Gy
Total glossectomy Right body Right nasolabial
Left
fold
Right hernigossectomy Lateral pharyngeal wall resection Suprag lottic laryngectomy Pectoralis major mycutaneous flap 68 Gy
hemiglossectomy Lateral pharyngeal wall resection Pectoralis major myocutaneous flap 60 Gy
Right
Right osteomyocutaneous groint flap Left angle-symphysis
Right osteomuscular groin flap + STSG Left condyle-symphysis
Right osteomyocutaneous parascapular flap Right angle- left mental foramen
osteomyocutaneous parascapular flap
Right
Right osteomuscular groin flap
390 Microvascular Tongue Reconstruction HEAD & NECK SeptemberlOctober 1993
ing thin and thick barium as well as soft/pureed food mixed with barium paste. Speech was eval- uated using high-quality audio recordings for spectographic ana1,ysis of format levels and tran- sitions to identify vowel and consonant intelligi- bility. Perceptual analysis was performed by ex- pert listeners and intelligibility was rated on a scale of 1 to 7.1'3'2
SURGICAL TECHNIQUE
The technique of secondary microvascular recon- struction is derived from our method of primary microvascular reconstruction and consists of (1) a radical tongue release; (2) bone graft place- ment in the floor of the mouth; and (3) soft tissue tongue augmentation. The residual tongue, ap- proached through a median labiomandibulot- omy, is first released from the hyoid bone and the mandible on t.he resected side, raising it to reach the palate and moving it as far back as the posterior pharyngeal wall. The extent to which
the tongue can be repositioned superiorly and posteriorly depends on the amount of scarring in the tongue, its blood supply, and innervation.
Although the lingual artery, nerve, and hypo- glossal nerve limit tongue mobilization, it is im- perative that these structures be preserved re- gardless of the adequacy of the release. If severe scarring does not allow a hemitongue to be re- leased superiorly, it may be freed up on its neu- rovascular bundle for 90-degree rotation into the pharynx to line what will be the new tongue base. This provides a better sensory surface at the base of the tongue and eliminates a potential dead space in the oral cavity where food may ac- cumulate.
The microvascular composite flap harvesting is planned such that following the transfer the soft tissues lay on top of the graft and the vascu- lar pedicle is on the same side of the floor defect. The bone graft, usually a triangular piece 5 cm long with a 3-cm base, is fashioned to fit the de-
tongue reconstruction.
Other Preoperative Postoperative operations swallow swallow Follow-up
Con!ouring of neck B!endenzed diet Blendenzed diet 4 years- died and chin
None Gastrostorny tube Gastrostomy tube 3 years-died Aspiration Aspiration
Revision of lower lip Gastrostomy tube Dynamic oral 1 year-died x 2 Aspiration transport
Gastrostomy tube Aspiration
Revision of lower lip Gastrostomy tube Dynamic oral 1 year-died Contouring of neck Aspiration transport and cheek Gastrostomy tube
Aspiration
Cricopharyngeal Gastrostomy tube Dynamic oral 1.5 years myotomy transport
SofVpureed
Microvascular Tongue Reconstruction HEAD & NECK September/October 1993 391
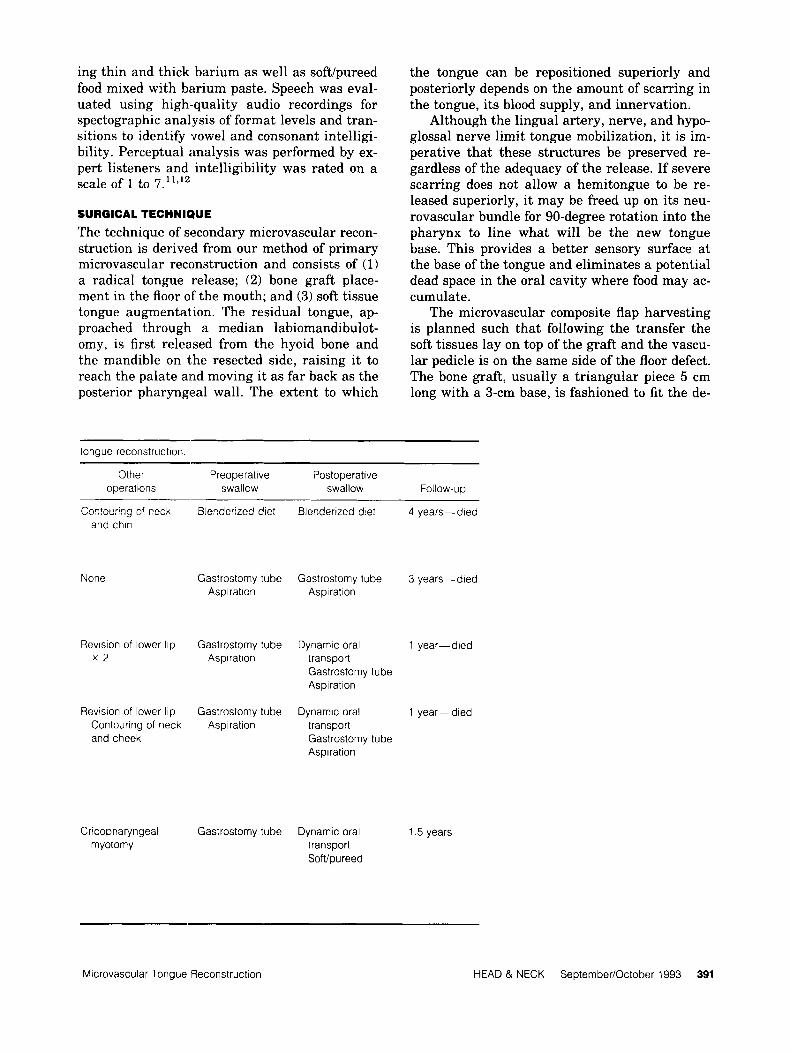
fect in the floor of the mouth. The graft, with its apex anteriorly and its base 3 to 4 cm from the posterior pharyngeal wall, is placed horizontally in the floor of the mouth to maintain the height of the reconstructed tongue and prevent the tongue base from being displaced anteriorly (Fig- ure 1).
The bone graft is then held in place with #24 wires passed through drill holes in the graft and the adjacent anterior mandible bodies. The wires are kept loose and tightened after the soft tissue reconstruction is completed. If a mandible defect is to be reconstructed at the same time, a single graft is used incorporating the shape of the floor graft with that of the mandible graft. Here fixa- tion is done with miniplates and screws.
Finally, a soft tissue mound is created over the floor graft using myocutaneous tissue or a muscle flap with split thickness skin graft. The cylindrical-shaped flap should touch the soft and hard palate when the jaws are approximated. Su- turing of the posterior half of the flap is done first, followed by the microvascular anastomosis. The midline mandibulotomy is then fixed with plate and screws, the graft wires tightened, and the previously placed anterior soft tissue sutures knotted.
RESULTS
Swallow. Preoperatively, only one patient was able to take in blenderized food, whereas the re- maining four patients relied entirely on gas-
FIGURE 1. Horizontal bone graft in the floor of the mouth sup- ports overlying soft tissue and prevents displacement of the tongue base anteriorly.
trostomy tube feedings. Cineradiographic studies in all five patients showed a large dead space in the oral cavity, restricted tongue mobility, and no palatoglossal closure or tongue base to poste- rior pharyngeal wall contact. The liquid barium ran freely from the mouth into the pharynx and passed into the esophagus without holdup at the cricopharyngeus. Four patients showed aspira- tion in spite of supraglottic swallows (breath- holding while swallowing), and only one patient was able to swallow without aspirating. Various amounts of barium were retained in the vallecu- lae and the pyriform sinuses but these did not contribute to the aspiration. In all patients, la- ryngeal and hyoid elevation was present, though reduced.
Postoperatively ingested liquid barium could not be held in the mouth and immediately spilled into the pharynx without accumulating at the cricopharyngeus. Small amounts of bar- ium retained in the valleculae and pyriform si- nuses did not cause aspiration, and laryngeal el- evation was basically similar to the preoperative findings. The reduction in the oral and pharyn- geal dead space with its effect on food transport is discussed separately.
Patients 7 and 2. There was no contact between the oral mound and the palate with no active food movement into the pharynx. The bolus of food remained stationary in the mouth and had to be washed down while the head was held back. One patient performed a successful supra- glottic swallow, whereas the second patient aspi- rated.
Patient 3. A small gap was demonstrated be- tween the flap and the hard palate, but there was good contact with the soft palate; compress- ing the flap against the palate moved the food into the pharynx. There was no flap-to-posterior pharyngeal wall contact leaving the pharynx with a large dead space through which the bolus moved by gravity. Repeated swallows were needed to pass the bolus into the esophagus. Sig- nificant aspiration was demonstrated with liquid barium.
Patient 4. There was good flap-to-palate contact and oropharyngeal closure allowing dynamic oral transport of the bolus without difficulty. The hemitongue, which had been transposed into the pharynx, made contact with the posterior pha- ryngeal wall (Figure 2) and expelled the food
392 Microvascular Tongue Reconstruction HEAD & NECK SeptemberiOctober 1993
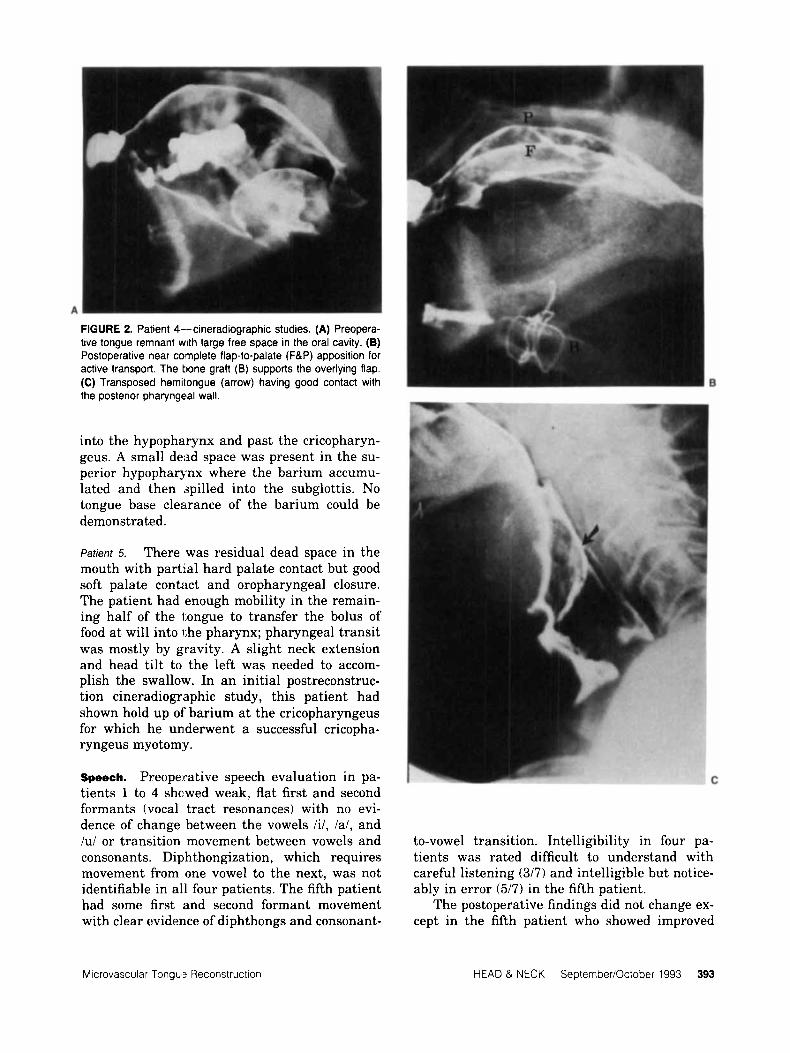
FIGURE 2. Patient 4--cineradiographic studies. (A) Preopera- tive tongue remnant with large free space in the oral cavity. (B) Postoperative near coqplete flap-to-palate (F&P) apposition for active transport. The tone graft (B) supports the overlying flap. (C) Transposed hemitongue (arrow) having good contact with the posterior pharyngeal wall.
into the hypopharynx and past the cricopharyn- geus. A small dead space was present in the su- perior hypopharynx where the barium accumu- lated and then (spilled into the subglottis. No tongue base clearance of the barium could be demonstrated.
Patrent 5. There was residual dead space in the mouth with partial hard palate contact but good soft palate contact and oropharyngeal closure. The patient had enough mobility in the remain- ing half of the tongue to transfer the bolus of food a t will into the pharynx; pharyngeal transit was mostly by gravity. A slight neck extension and head tilt to the left was needed to accom- plish the swallow. In an initial postreconstruc- tion cineradiographic study, this patient had shown hold up of' barium at the cricopharyngeus for which he underwent a successful cricopha- ryngeus myotom;y.
Speech. Preoperative speech evaluation in pa- tients l to 4 shcwed weak, flat first and second formants (vocal tract resonances) with no evi- dence of change between the vowels Iil, la/, and /u/ or transition movement between vowels and to-vowel transition. Intelligibility in four pa- consonants. Diphthongization, which requires tients was rated difficult to understand with movement from one vowel to the next, was not careful listening (317) and intelligible but notice- identifiable in all four patients. The fifth patient ably in error (517) in the fifth patient. had some first and second formant movement The postoperative findings did not change ex- with clear evidence of diphthongs and consonant- cept in the fifth patient who showed improved
Microvascular Tongue Reconstruction HEAD & NECK SeptemberiOctober 1993 393
first and second formant movement and transi- tion with definite diphthongs. His speech was rated intelligible with occasional errors (617).
DISCUSSION
Major glossectomy removes a larger portion of the tongue, floor of the mouth, suprahyoid mus- cles, and a segment of the mandible if the tumor involves the bone. The effect of removing these structures on intraoral transport, pharyngeal contraction, mandible excursion, and laryngeal movement are well do~umented.l~-’~ Loss of tongue volume and floor support impairs dy- namic oral transport and curtails food intake. Reduced tongue size and floor elevation prevents palatoglossal closure and directly influences pha- ryngeal transport by altering the normal pres- sure gradients needed for propulsive pharyngeal emptying. Resection of the suprahyoid muscles and the anterior mandible arch decreases laryn- geal elevation and exposes the laryngeal inlet to the ingested food, thereby increasing the risk of aspiration.
In addition to the above-mentioned factors, scarring plays an important role in swallowing dysfunction, particularly in long-standing oro- mandibular deformities. In the absence of appro- priate reconstruction, McGregor considering scarring to be the “more potent source of func- tional deficits than other (factors) combined.”18 Scarring adversely effects tongue function by (1) displacing the residual tongue; (2) restricting movement by its tethering effect; (3) defunction- alizing otherwise normal contractile muscle (is- chemic conditions or healing by secondary inten- tion); and (4) causing disuse atrophy of mal- positioned muscles. Extenuating circumstances such as repeated infections, orocutaneous fistu- lae, and osteoradionecrosis with mandible loss accentuate the adverse effects of scarring and further impair tongue function.
Positional changes in the tongue due to scar- ring are fortunately predictable and in part pre- ventable if adequately reconstructed. Contractile scar forces pull the tongue remnant toward the adjacent bone structures, namely the mandible anteriorly or laterally and the hyoid bone inferi- orly. In major anterior resections, the base of the tongue is typically pulled forward and down- ward, diametrically opposite the normal upward and backward tongue base elevation, precluding a successful palatoglossal closure and propulsive pharyngeal swallow. In hemiglossectomy pa- tients, on the other hand, the shift is lateral and
inferior allowing for better oropharyngeal clo- sure on the nonresected side. Nevertheless, in both situations, if the tongue defect is closed pri- marily rather than with a skin flap the combina- tion of scarring to the hyoid, tongue displace- ment and volume loss converts the remaining tongue into an ineffective organ that cannot reach the palate and pharynx for dynamic oral and pharyngeal food transport.
The untoward results of direct closure of ma- jor tongue defects has been improved by skin flap transfer^.^^,^^ A skin flap replaces lost tongue substance by virtue of its bulk at the same time acting as a “spacer” to prevent tongue displace- ment. Thinner flaps such as the microvascular radial forearm flap not only act as a “spacer” but allow the remaining tongue a certain degree of movement.21 Bulky flaps are suited for subtotal or total glossectomy defects but are known to re- strict tongue movement in lesser resections. Myocutaneous pedicled flaps such as the pectora- lis major and latissimus dorsi have made tongue reconstruction easier and yet the ver- tically oriented muscle pedicle can drastically compromise tongue elevation by its downward traction.
In spite of these advances, skin flap surgery of the tongue, whether pedicled or microvascu- lar, cannot counteract the harmful effects of gravity and vertical scarring to the hyoid with its resultant loss in tongue height. This makes tongue height recovery in established deformi- ties one of the most difficult aspects of recon- structive surgery. It is not surprising, therefore, that corrective methods have resorted to pros- thetic appliances to either augment the residual tongue or lower the roof of the palate for better lingual-palatal contact. Although deglutition and speech may be improved with prosthetic pal- atal augmentation, our patients with major glos- sectomies preferred not to wear a prosthesis for being deprived of an important sensory surface, ie, palate, which is essential for oral transport.
We have corrected long-standing major tongue deformities by relocating the tongue in a more functional position, using a bone graft for support, and replacing lost tongue substance with a skin flap. A radical release frees up the tongue from the hyoid bone and mandible for palatal and pharyngeal contact. The released tongue is buttressed with a bone graft placed horizontally in the floor of the mouth; if needed, the same graft can be used to reconstruct a man- dible defect. The dead space adjacent to the repo-
394 Microvascular Tongue Reconstruction HEAD & NECK Septernber/October 1993
sitioned tongue is then fully obliterated with a skin flap laid over the bone graft.
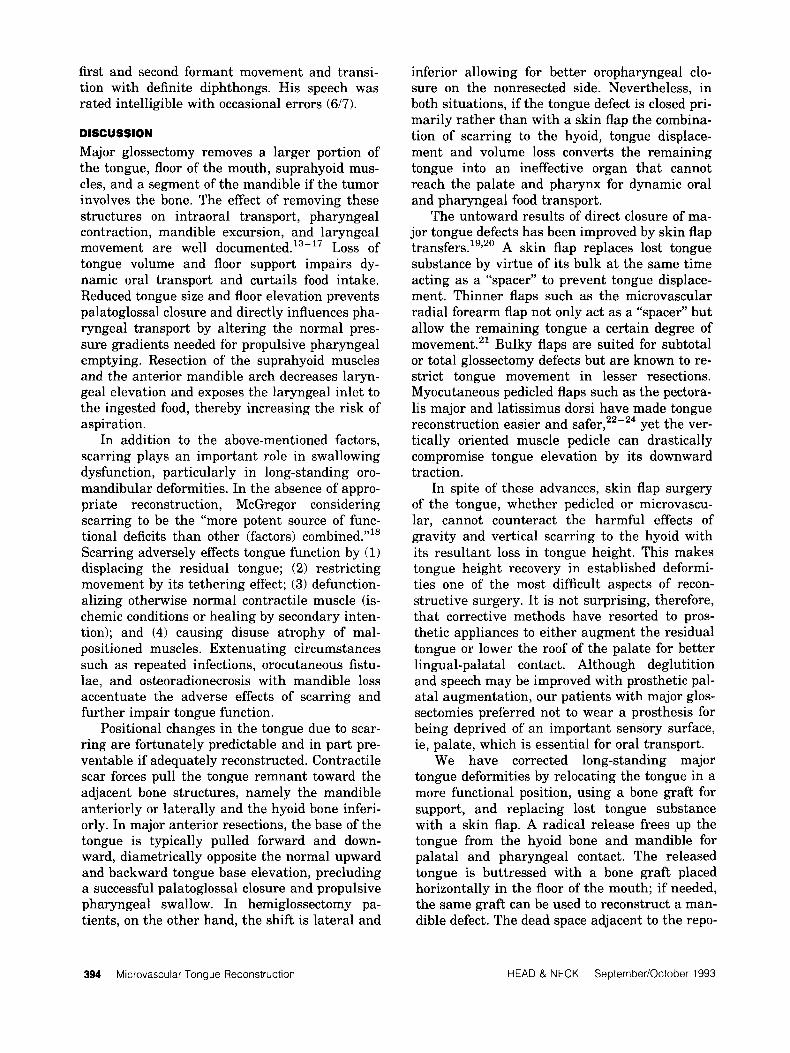
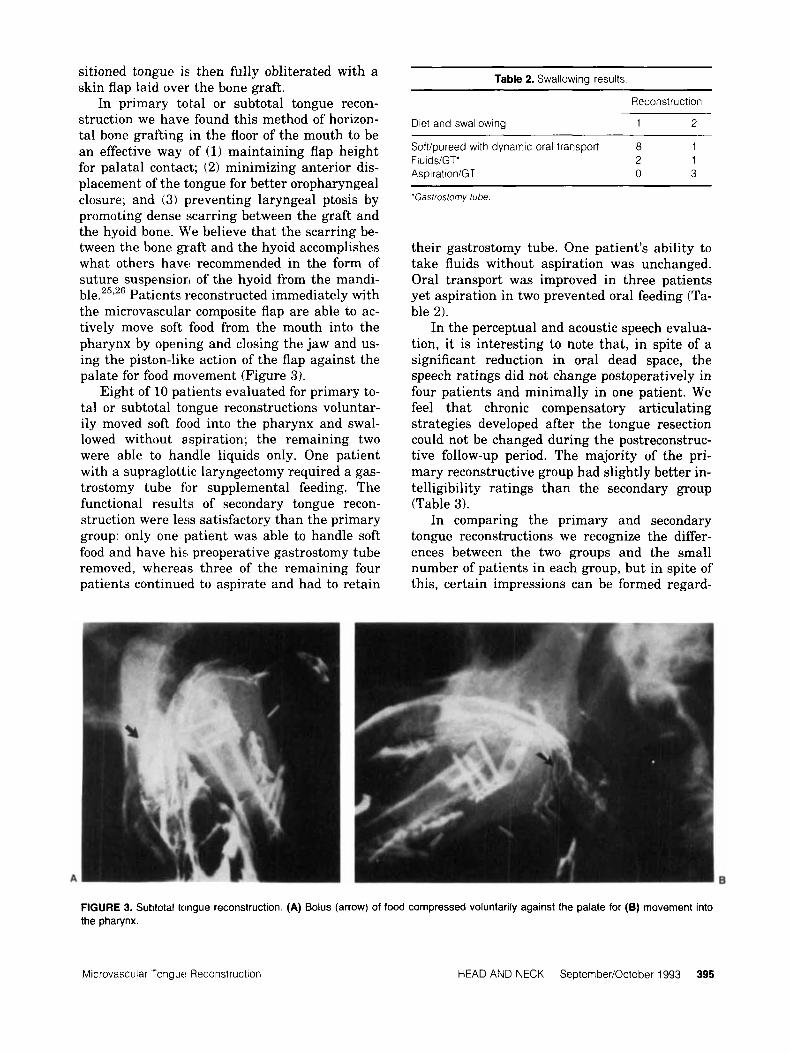
In primary total or subtotal tongue recon- struction we have found this method of horizon- tal bone grafting in the floor of the mouth to be an effective way of (1) maintaining flap height for palatal contact; (2) minimizing anterior dis- placement of the tongue for better oropharyngeal closure; and (3) preventing laryngeal ptosis by promoting dense scarring between the graft and the hyoid bone. We believe that the scarring be- tween the bone graft and the hyoid accomplishes what others have recommended in the form of suture suspension of the hyoid from the mandi- ble.2"26 Patients reconstructed immediately with the microvascular composite flap are able to ac- tively move soft food from the mouth into the pharynx by opening and closing the jaw and us- ing the piston-like action of the flap against the palate for food movement (Figure 3).
Eight of 10 patients evaluated for primary to- tal or subtotal tongue reconstructions voluntar- ily moved soft food into the pharynx and swal- lowed without aspiration; the remaining two were able to handle liquids only. One patient with a supraglottic laryngectomy required a gas- trostomy tube for supplemental feeding. The functional results of secondary tongue recon- struction were less satisfactory than the primary group: only one patient was able to handle soft food and have his preoperative gastrostomy tube removed, whereas three of the remaining four patients continued to aspirate and had to retain
Table 2. Swallowing results
Reconstruction
Diet and swallowing 1 2
Sofl/pureed with dynamic oral transport 8 1 FluidsiGT" 2 1 AspirationiGT 0 3
'Gastroslomv tube
their gastrostomy tube. One patient's ability to take fluids without aspiration was unchanged. Oral transport was improved in three patients yet aspiration in two prevented oral feeding (Ta- ble 2).
In the perceptual and acoustic speech evalua- tion, it is interesting to note that, in spite of a significant reduction in oral dead space, the speech ratings did not change postoperatively in four patients and minimally in one patient. We feel that chronic compensatory articulating strategies developed after the tongue resection could not be changed during the postreconstruc- tive follow-up period. The majority of the pri- mary reconstructive group had slightly better in- telligibility ratings than the secondary group (Table 3).
In comparing the primary and secondary tongue reconstructions we recognize the differ- ences between the two groups and the small number of patients in each group, but in spite of this, certain impressions can be formed regard-
FIGURE 3. Suhtotal tongue reconstruction. (A) Bolus (arrow) of food compressed voluntarily against the palate for (6) movement into the pharynx.
Microvascular .Tongue Reconstruction HEAD AND NECK September/October 1993 395

the mandible, floor of the mouth, and tongue, should be done immediately at the time of tumor
Table 3. Speech rating.
Intelligibility
Reconstruction extirpation to obtain the best functional result and avoid the irreparable sequelae of scarring. 1
317 Difficult to understand 1 4 - 417 Intelligible with careful 7
517 Intelligible but noticeably 2
617 Occasional errors -
listening
in error -
1
ing the findings: (1) Dynamic intraoral transport can be readily achieved in primary total or sub- total microvascular tongue reconstructions, but is more difficult to accomplish in secondary tongue reconstruction because neurovascular constraints do not allow full mobilization of the scarred tongue for palatal and pharyngeal con- tact. (2) A contoured intraoral skin flap having good palatal contact is functionally more desir- able than a contracted immobile tongue. In pa- tients with severe scarring, consideration should be given to transpose the tongue from the oral cavity into the pharynx for better obliteration of the free space in the mouth. (3) In primary re- constructions, patients are able to swallow with- out aspiration; in the secondary group, preopera- tive aspiration could not be corrected (except in 1 patient) by improving glossopharyngeal contact and/or palate-flap closure. It is postulated that (a) primary transfer of well-vascularized tissue protects preserved functional units about the tongue from the adverse effects of infection, poor healing, and ionizing radiation; and (b) scarring compromises tongue base clearance of food and irreversibly damages the remaining suprahyoid muscles and supraglottic intralaryngeal muscles involved in protecting the laryngeal introitus. This reaffirms Edgerton’s statement that imme- diate reconstruction “makes possible the mainte- nance of certain features and functions that can- not be practically obtained by any method of late recon~truction.”~~
The goal of major tongue reconstruction is to maximize oral articulatory movements and pro- vide an active intraoral and pharyngeal mecha- nism for food transport without aspiration. This can be accomplished only if a method for recon- structing the floor of the mouth is developed in conjunction with the overall scheme of tongue and mandible reconstruction. However, such a “multisystem” reconstruction, which includes
EDITORIAL COMMENT
The tongue is rivaled only by the heart as an an- atomically and physiologically complex muscular organ. Preservation or restoration of the tongue’s intricate function following a total glossectomy remains an elusive goal for the head and neck surgeon. The authors have previously published their approach to tongue reconstruction using immediate microvascular flaps and reported sat- isfactory results for both speech and swallowing. In the current article, they demonstrate that these same techniques were unable to reproduce similar function when utilized in a delayed fash- ion. This underscores a concept which has been well established in the past decade, namely the advantage of definitive immediate reconstruction following ablation of an extensive or complex head and neck neoplasm whenever possible.
It is interesting to note that the authors, like numerous others, believe that one of the keys to simulating tongue function following glossec- tomy is to “obliterate oral dead space.” In this case they have used a bone graft in the floor of the mouth to “buttress” the level of the recon- struction flap. Using cineradiographic studies a significant decrease in this space is documented postoperatively in the secondary reconstruction group. Despite this, no improvement in speech and swallowing was achieved. It seems unlikely then that bulk alone is the answer. At Emory University Hospital, we had the opportunity to obtain manofluorographic studies on six patients who had undergone a total glossectomy, includ- ing three in whom the larynx was preserved. The latter group were reconstructed immediately with flaps (pectoralis, radial forearm, scapular) which were used to pull forward and suspend the laryngoepiglottic complex from the mandible. Manofluorography confirmed that the patients were able to elevate the complex voluntarily dur- ing speech and swallowing by their residual in- tact musculature (Am J Surg 1989;158:297- 302). Salibian et a1 have observed the same phenomenon by cineradiography. It is possible that it is the maintenance or restoration of this ability which maximizes speech and swallowing following a total glossectomy. Further, it is pos- sible that the optimal method to achieve this is, as we have done, through the use of of a rela-
396 Microvascular Tongue Reconstruction HEAD & NECK SepternberiOctober 1993

tively thin flap which can pull the complex for- ward. This subject deserves additional study. An- other factor not commented upon by the authors which is central to the success of reconstruction following a glossectomy is the preservation of the superior laryngeal nerves, “the watchdogs of the larynx .”
The authors are to be commended for their critical assessment of the functional results of delayed reconstruction in this difficult group of patients. We should not assume that the task is impossible but rather, like them, continue to search for more effective methods to restore oral function secondarily. Until those advances are realized a strong argument can be made for pro- ceeding with definitive immediate reconstruction whenever possible.
Mark R. Sultan, MD Department of Plastic & Reconstructive Surgery Columbia Presbyterian Medical Center New York. NY
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
Razack MS, Sako K, Bakamjian VY, Shedd DP. Total glossectomy. A m .I Surg 1983;146:509-511. Conley JJ . Swallowing dysfunctions associated with rad- ical surgery of the head and neck. Arch Surg 1960;80602-612 Krespi YP, Sissori GA. Reconstruction after total or sub- total glossectomy A m J Surg 1983;146:488-492. Biller HF, Lawson WM, Baek SM. Total glossectomy: a technique of reconstruction eliminating laryngectomy. Arch Otolaryngol 1983;109:69- 73. Habal ME;, Murray JE. Surgical treatment of life- endangering chronic aspiration pneumonia. Plast Recon- str Surg 1972;49:305-311. Mladick RA, Horton CE, Adamson JE. Immediate cricopharyngeal myotomy: an adjunctive technique for major oropharyrigeal resection. Plast Reconstr Surg
DesPrez JD, Kiehn CL. Methods of reconstruction follow- ing resection of anterior oral cavity and mandible for ma- lignancy. Plast Reconstr Surg 1959;24:238. DeSousa LJ, Martins OJ. Swallowing and speech after radical total glossectomy with tongue prosthesis. Oral Surg 1975339356;-360. Robbins KT, Bowman JB, Jacob RF. Postglossectomy deglutitory and ;articulatory rehabilitation with palatal augmentation prosthesis. Arch Otolaryngol Head Neck Surg 1987;113:1214- 1218.
1971;47:6- 11.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
10. Salibian AH, Allison GR, Rappaport I, Krugman ME, McMicken B, Etchepare TL. Total and subtotal glossec- tomy: Function after microvascular reconstruction. Plast Reconstr Surg 1990;85:513-524.
11. McConnel FMS, Adler RK, Teichgraeber JF. Speech and swallowing function following surgery of the oral cavity. In: Myers EN, Barofsky I, Yates JW, eds. Rehabilitation and treatment of head and neck cancer (publication no. 86-2762). Bethesda, MD: National Institutes of Health,
12. Allison GR, Rappaport I, Salibian AH, et al. Adaptive mechanisms of speech and swallowing after combined jaw and tongue reconstruction in long term survivors. A m J Surg 1987;154:419.
1986:135- 151.
Shedd DP, Scatliff JA, Kirchner JA. A cineradiographic study of postresectional alterations in oropharyngeal physiology. Surg Gynecol Obstet 1960:69-89. Logemann JA, Bytell DE. Swallowing disorders in three types of head and neck surgical patients. Cancer
Effron MZ, Johnson JT, Myers EN, Curtin H, Berry Q, Sigler B. Advanced carcinoma of the tongue: manage- ment by total glossectomy without laryngectomy. Arch Orolaryngol 1981;107:694-697. Edgerton MT, McKee DM. Reconstruction with loss of the hyomandibular complex in excision of large cancers. Arch Surg 1959;78:425-436. Myers EN. The role of total glossectomy in management
1979;44:1095-1105.
of cancer of the oral cavity. Otolaryngol C l i n N A m 1972:5:343. McGregor IA, McGregor FM. Cancer of the face and mouth. London: Churchill Livingstone, 1986:492. McGregor IA. The temporal flap in intraoral cancer: its use in repairing the postexcisional defect. Br J Plast Surg 1963;16:318. Bakamjian VY, Long M, Rigg B. Experience with medi- ally based deltopectoral flap in reconstructive surgery of the head and neck. Br J Plast Surg 1971;24:174. McGregor IA. Fasciocutaneous flaps in intraoral recon- struction. Clin Plast Surg 1985;12:453-461. Keyserlingk JR, deFrancesco J , Breach N, Rhys-Evans P, Stafford N, Mott A. Recent experience with recon- structive surgery following major glossectomy. Arch Oto- laryngol Head Neck Surg 1989;115:331-338. Ariyan S. The pectoralis major myocutaneous flap: A ver- satile flap for reconstruction in the head and neck. Plast Reconstr Surg 1979;63:73-81. Baek SM, Biller HF, Krespi YP, Lawson WM. The pecto- ralis major myocutaneous island flap for reconstruction of the head and neck. Head Neck Surg 1979;1:293-300. Weber RS, Ohlms L, Bowman J , Jacob R, Goepfert H. Functional results after total or near total glossectomy with laryngeal preservation. Arch Otolaryngol Head Neck Surg 1991;117:512-515. Goode RL. Laryngeal suspension in head and neck sur- gery. Latyngoscope 1976;86:349- 355. Edgerton MT. Criteria for immediate reconstruction in treatment of head and neck cancer. In: Symposium on cancer of the head and neck, vol. 2. St. Louis: CV Mosby, 1969:69.
Microvascular Tonguls Reconstruction HEAD 8, NECK SeptemberIOctober 1993 397