radiographic findings associated with aging - ohsu
TRANSCRIPT
Radiographic Findings Associated with Aging: Normal or Abnormal?
Dave Pettersson, MDAssistant Professor of NeuroradiologyOregon Health & Science University
5th Annual Musculoskeletal Updatefor Primary CareSeptember 6, 2018
Sag MRISag MRI Sag MRI
Disc herniation:Protrusion
Disc herniation:Extrusion
Disc herniation:Schmorl node
Disclosures:
Nothing to disclose
Spine Imaging and Aging:
Outline:
Spine degenerative changes on imaging:• Prevalence• Appearance on MRI, CT, radiographs
Low back pain• When to image• “Red flag” conditions
Age related changes on brain MRI
Spine Imaging and Aging: Question
What percentage of asymptomatic 20 year olds havedegenerative disc findings on lumbar spine MRI?
A. 5 %B. 15 %C. 25 %D. 35 %E. 45%
Spine Imaging and Aging: Question
What percentage of asymptomatic 80 year olds have degenerativedisc findings on lumbar spine MRI?
A. 35 %B. 55 %C. 75 %D. 95%
Spine Imaging and Aging: Answers
Disc protrusion Prevalence of degenerative findings on Lumbar MRI:• 148 volunteers• All asymptomatic at time of MRI• 46% reported never having back pain
Age under 40 years: Age under 40 60 years: Age over 60 years:
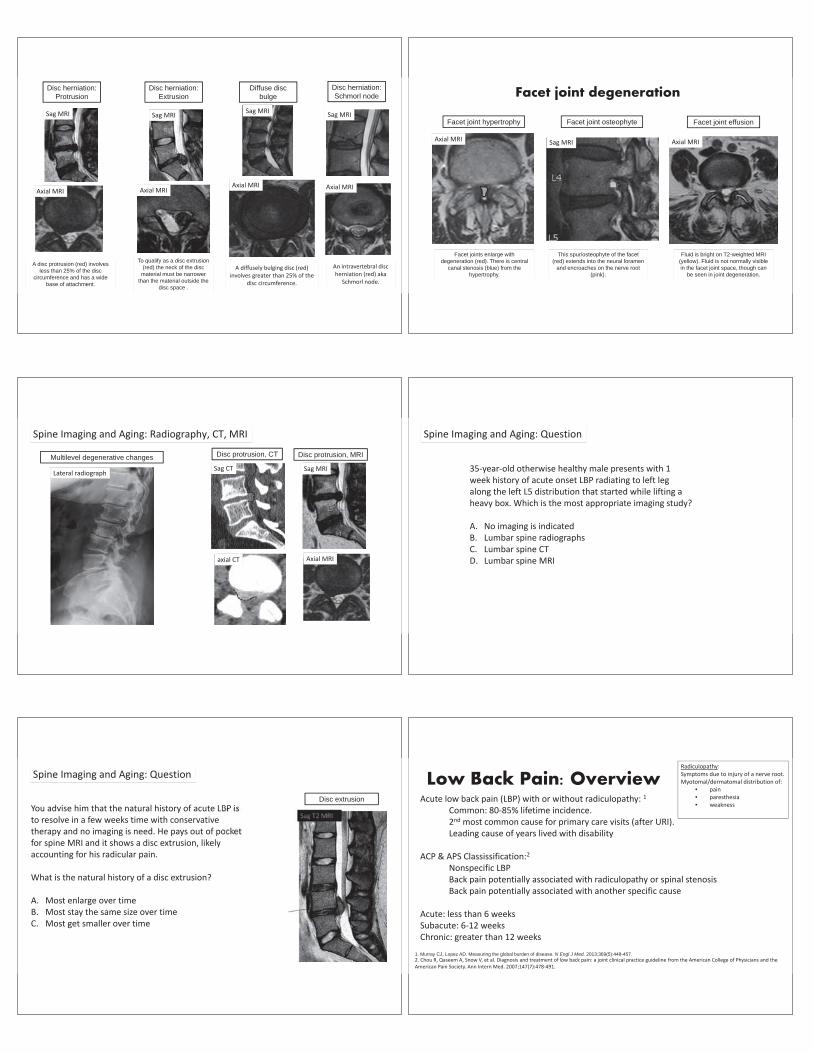
A disc protrusion (red) involves less than 25% of the disc
circumference and has a wide base of attachment.
Sag MRI
A diffusely bulging disc (red)involves greater than 25% of the
disc circumference.
Sag MRISag MRI
Axial MRIAxial MRIAxial MRI
To qualify as a disc extrusion (red) the neck of the disc
material must be narrower than the material outside the
disc space .
An intravertebral discherniation (red) aka
Schmorl node.
Sag MRI
Axial MRI
Disc herniation:Protrusion
Disc herniation:Extrusion
Disc herniation:Schmorl node
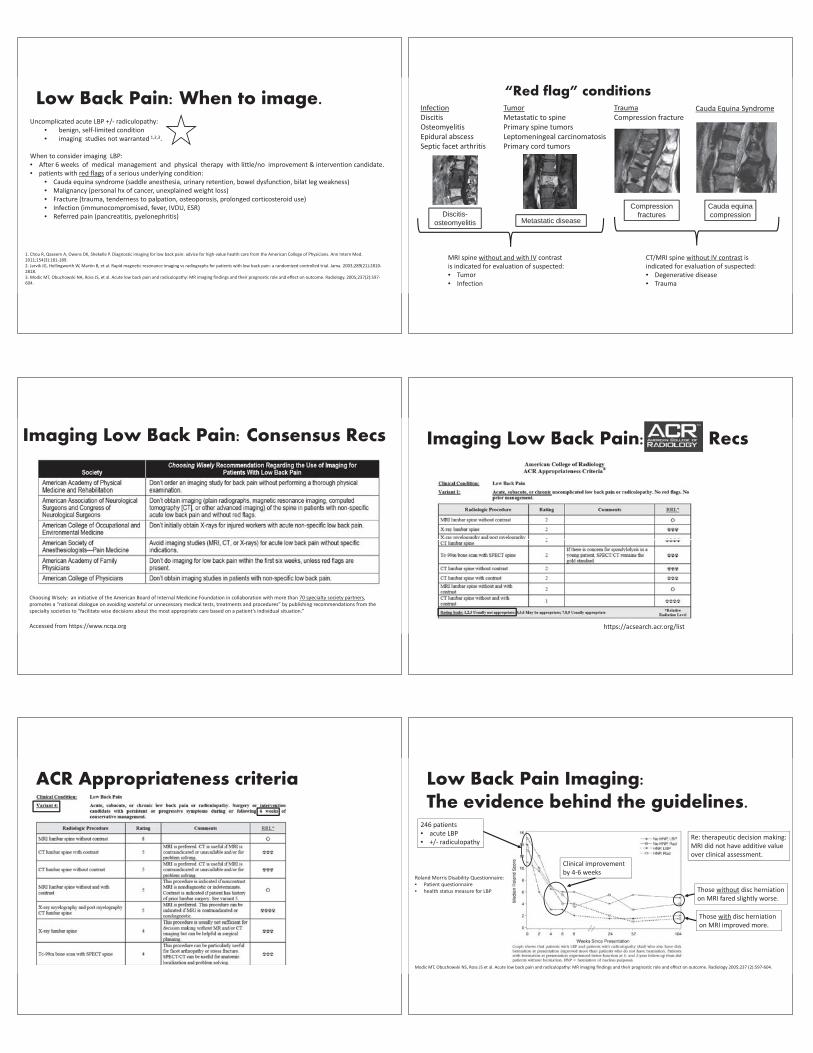
Diffuse disc bulge Facet joint degeneration
Facet joints enlarge with degeneration (red). There is central
canal stenosis (blue) from the hypertrophy.
Axial MRIAxial MRI Sag MRI
This spur/osteophyte of the facet (red) extends into the neural foramen
and encroaches on the nerve root (pink).
Fluid is bright on T2-weighted MRI (yellow). Fluid is not normally visible in the facet joint space, though can
be seen in joint degeneration.
Facet joint hypertrophy Facet joint osteophyte Facet joint effusion
Spine Imaging and Aging: Radiography, CT, MRI
Sag CT
axial CT
Sag MRI
Axial MRI
Lateral radiograph
Multilevel degenerative changes Disc protrusion, CT Disc protrusion, MRI
Spine Imaging and Aging: Question
35 year old otherwise healthy male presents with 1week history of acute onset LBP radiating to left legalong the left L5 distribution that started while lifting aheavy box. Which is the most appropriate imaging study?
A. No imaging is indicatedB. Lumbar spine radiographsC. Lumbar spine CTD. Lumbar spine MRI
Spine Imaging and Aging: Question
You advise him that the natural history of acute LBP isto resolve in a few weeks time with conservativetherapy and no imaging is need. He pays out of pocketfor spine MRI and it shows a disc extrusion, likelyaccounting for his radicular pain.
What is the natural history of a disc extrusion?
A. Most enlarge over timeB. Most stay the same size over timeC. Most get smaller over time
Disc extrusion
Low Back Pain: OverviewAcute low back pain (LBP) with or without radiculopathy: 1
Common: 80 85% lifetime incidence.2nd most common cause for primary care visits (after URI).Leading cause of years lived with disability
ACP & APS Classissification:2
Nonspecific LBPBack pain potentially associated with radiculopathy or spinal stenosisBack pain potentially associated with another specific cause
Acute: less than 6 weeksSubacute: 6 12 weeksChronic: greater than 12 weeks
1. Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369(5):448-457.2. Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and theAmerican Pain Society. Ann Intern Med. 2007;147(7):478 491.
Radiculopathy:Symptoms due to injury of a nerve root.Myotomal/dermatomal distribution of:
• pain• paresthesia• weakness
Uncomplicated acute LBP +/ radiculopathy:• benign, self limited condition• imaging studies not warranted 1,2,3.
When to consider imaging LBP:• After 6 weeks of medical management and physical therapy with little/no improvement & intervention candidate.• patients with red flags of a serious underlying condition:
• Cauda equina syndrome (saddle anesthesia, urinary retention, bowel dysfunction, bilat leg weakness)• Malignancy (personal hx of cancer, unexplained weight loss)• Fracture (trauma, tenderness to palpation, osteoporosis, prolonged corticosteroid use)• Infection (immunocompromised, fever, IVDU, ESR)• Referred pain (pancreatitis, pyelonephritis)
Low Back Pain: When to image.
1. Chou R, Qaseem A, Owens DK, Shekelle P. Diagnostic imaging for low back pain: advice for high value health care from the American College of Physicians. Ann Intern Med.2011;154(3):181 189.2. Jarvik JG, Hollingworth W, Martin B, et al. Rapid magnetic resonance imaging vs radiographs for patients with low back pain: a randomized controlled trial. Jama. 2003;289(21):28102818.3. Modic MT, Obuchowski NA, Ross JS, et al. Acute low back pain and radiculopathy: MR imaging findings and their prognostic role and effect on outcome. Radiology. 2005;237(2):597604.
“Red flag” conditions InfectionDiscitisOsteomyelitisEpidural abscessSeptic facet arthritis
TumorMetastatic to spinePrimary spine tumorsLeptomeningeal carcinomatosisPrimary cord tumors
TraumaCompression fracture
Cauda Equina Syndrome
MRI spine without and with IV contrastis indicated for evaluation of suspected:• Tumor• Infection
CT/MRI spine without IV contrast isindicated for evaluation of suspected:• Degenerative disease• Trauma
Discitis-osteomyelitis Metastatic disease
Compression fractures
Cauda equina compression
Accessed from https://www.ncqa.org
Choosing Wisely: an initiative of the American Board of Internal Medicine Foundation in collaboration with more than 70 specialty society partners,promotes a “national dialogue on avoiding wasteful or unnecessary medical tests, treatments and procedures” by publishing recommendations from thespecialty societies to “facilitate wise decisions about the most appropriate care based on a patient’s individual situation.”
Imaging Low Back Pain: Consensus Recs Imaging Low Back Pain: Recs
https://acsearch.acr.org/list
ACR Appropriateness criteria
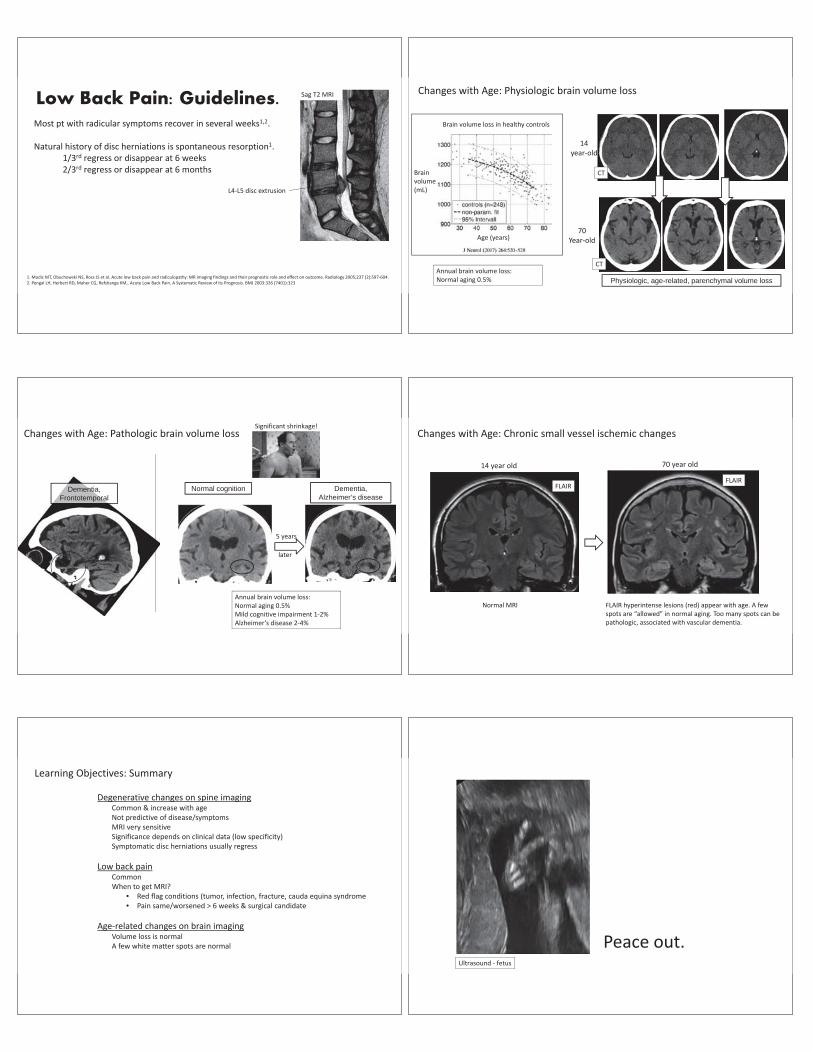
Modic MT, Obuchowski NS, Ross JS et al. Acute low back pain and radiculopathy: MR imaging findings and their prognostic role and effect on outcome. Radiology 2005;237 (2):597 604.
Roland Morris Disability Questionnaire:• Patient questionnaire• health status measure for LBP
246 patients• acute LBP• +/ radiculopathy
Low Back Pain Imaging:The evidence behind the guidelines.
Clinical improvementby 4 6 weeks
Those with disc herniationon MRI improved more.
Those without disc herniationon MRI fared slightly worse.
Re: therapeutic decision making:MRI did not have additive valueover clinical assessment.
Low Back Pain: Guidelines. Most pt with radicular symptoms recover in several weeks1,2.
Natural history of disc herniations is spontaneous resorption1.1/3rd regress or disappear at 6 weeks2/3rd regress or disappear at 6 months
1. Modic MT, Obuchowski NS, Ross JS et al. Acute low back pain and radiculopathy: MR imaging findings and their prognostic role and effect on outcome. Radiology 2005;237 (2):597 604.2. Pengal LH, Herbert RD, Maher CG, Refshange KM,. Acute Low Back Pain. A Systematic Review of its Prognosis. BMJ 2003:326 (7401):323
L4 L5 disc extrusion
Sag T2 MRI
Annual brain volume loss:Normal aging 0.5%
Brainvolume(mL)
Age (years)
Brain volume loss in healthy controls
Changes with Age: Physiologic brain volume loss
14year old
70Year old
CT
CT
Physiologic, age-related, parenchymal volume loss
Dementia,Frontotemporal
Changes with Age: Pathologic brain volume loss
Annual brain volume loss:Normal aging 0.5%Mild cognitive impairment 1 2%Alzheimer’s disease 2 4%
Significant shrinkage!
5 years
later
Dementia,Alzheimer’s disease
Normal cognition
Changes with Age: Chronic small vessel ischemic changes
FLAIRFLAIR
14 year old 70 year old
Normal MRI FLAIR hyperintense lesions (red) appear with age. A fewspots are “allowed” in normal aging. Too many spots can bepathologic, associated with vascular dementia.
Degenerative changes on spine imagingCommon & increase with ageNot predictive of disease/symptomsMRI very sensitiveSignificance depends on clinical data (low specificity)Symptomatic disc herniations usually regress
Low back painCommonWhen to get MRI?
• Red flag conditions (tumor, infection, fracture, cauda equina syndrome• Pain same/worsened > 6 weeks & surgical candidate
Age related changes on brain imagingVolume loss is normalA few white matter spots are normal
Learning Objectives: Summary
Peace out.Ultrasound fetus
Radiographic Findings Associatedwith Aging: Normal or Abnormal?
Barry G. Hansford, MDOregon Health & Science University
Assistant Professor RadiologyMusculoskeletal Radiology Fellowship Director
Osteoporosis: Terminology
Osteopenia: Paucity of bone, increased radiolucency, descriptive term w/out causality
Osteoporosis: Bone loss/decreased density, normal quality, decreased quantity
Osteomalacia: Malformed bone
Why Is Osteopenia Preferred?• Cannot tell cause of osteoporosis radiographically• Cannot discern osteoporosis from osteomalacia• Generic term encompassing both osteoporosis and osteomalacia
Primary Osteoporosis: Most common in post menopausal females, osteoporosis of aging
Secondary Osteoporosis: Implies underlying disorder, broad DDX, only 5% of cases
Osteoporosis: Definition
World Health Organization: Bone mineral density 2.5 or more standard deviations less than thatof a young healthy adult
T Score: 2.5 SD or less as measured with dual energy x ray absorptiometry (DEXA scan) for postmenopausal women and men over 50
Z Score: Abnormal if 2 SD away from mean for age and sex matched norm, relative quantity
Clinical Utility: T score more useful for predicting fracture risk, absolute quantity
Women: Estrogen deficiency after menopause, accelerated cancellous bone loss
Men: More linear pattern of bone loss
Equivalent loss by 80 years of age
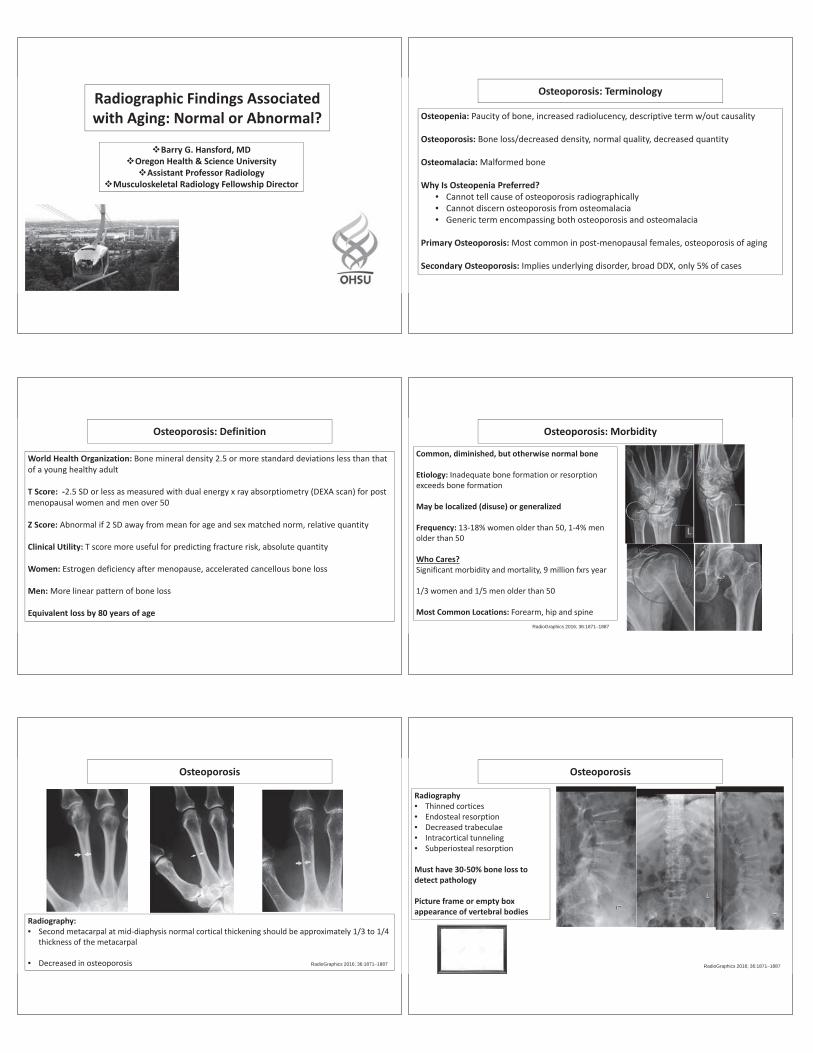
Osteoporosis: Morbidity
Common, diminished, but otherwise normal bone
Etiology: Inadequate bone formation or resorptionexceeds bone formation
May be localized (disuse) or generalized
Frequency: 13 18% women older than 50, 1 4% menolder than 50
Who Cares?Significant morbidity and mortality, 9 million fxrs year
1/3 women and 1/5 men older than 50
Most Common Locations: Forearm, hip and spineRadioGraphics 2016; 36:1871–1887
Osteoporosis
Radiography:• Second metacarpal at mid diaphysis normal cortical thickening should be approximately 1/3 to 1/4
thickness of the metacarpal
• Decreased in osteoporosis RadioGraphics 2016; 36:1871–1887
Osteoporosis
Radiography• Thinned cortices• Endosteal resorption• Decreased trabeculae• Intracortical tunneling• Subperiosteal resorption
Must have 30 50% bone loss todetect pathology
Picture frame or empty boxappearance of vertebral bodies
RadioGraphics 2016; 36:1871–1887
Osteoporosis: Morbidity
Vertebral Bodies: Weight bearing bones with little cortical bone• Vertical trabeculae thicker• Horizontal trabeculae thinner, preferentially lost earlier in disease
History of osteoporotic vertebral body fracture• Increases risk of future vertebral body fracture X5, 50% asymptomatic• Increases risk of future hip fracture X2 RadioGraphics 2016; 36:1871–1887
Insufficiency Fractures
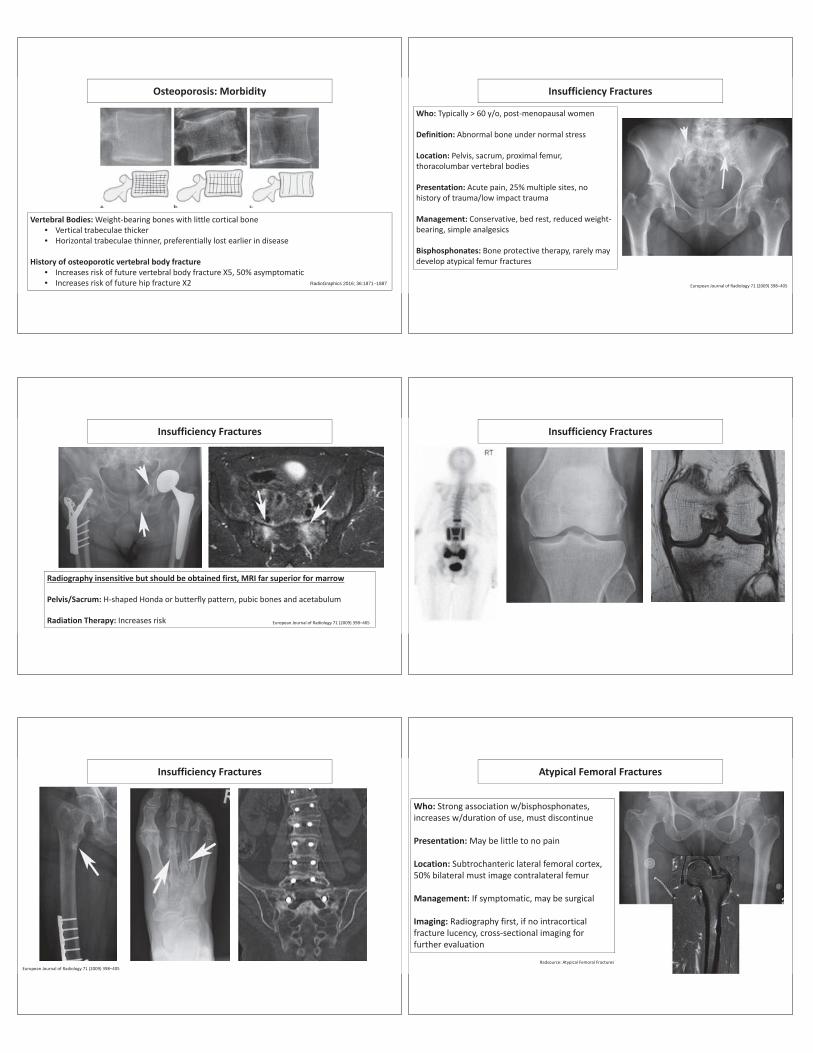
Who: Typically > 60 y/o, post menopausal women
Definition: Abnormal bone under normal stress
Location: Pelvis, sacrum, proximal femur,thoracolumbar vertebral bodies
Presentation: Acute pain, 25% multiple sites, nohistory of trauma/low impact trauma
Management: Conservative, bed rest, reduced weightbearing, simple analgesics
Bisphosphonates: Bone protective therapy, rarely maydevelop atypical femur fractures
European Journal of Radiology 71 (2009) 398–405
Insufficiency Fractures
Radiography insensitive but should be obtained first, MRI far superior for marrow
Pelvis/Sacrum: H shaped Honda or butterfly pattern, pubic bones and acetabulum
Radiation Therapy: Increases risk European Journal of Radiology 71 (2009) 398–405
Insufficiency Fractures
Insufficiency Fractures
European Journal of Radiology 71 (2009) 398–405
Atypical Femoral Fractures
Who: Strong association w/bisphosphonates,increases w/duration of use, must discontinue
Presentation: May be little to no pain
Location: Subtrochanteric lateral femoral cortex,50% bilateral must image contralateral femur
Management: If symptomatic, may be surgical
Imaging: Radiography first, if no intracorticalfracture lucency, cross sectional imaging forfurther evaluation
Radsource: Atypical Femoral Fractures
Osteoarthritis
Most common joint disorder
Etiology: Primary/idiopathic, post traumatic,metabolic bone disease, endocrine disorders
Frequency: > 50% over 65 y/o and > 80% over 75y/o have radiographic evidence
Symptoms matter! Not radiographic findings inisolation
Imaging Work up: Always start with radiographs,little to no role for MRI
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Osteoarthritis
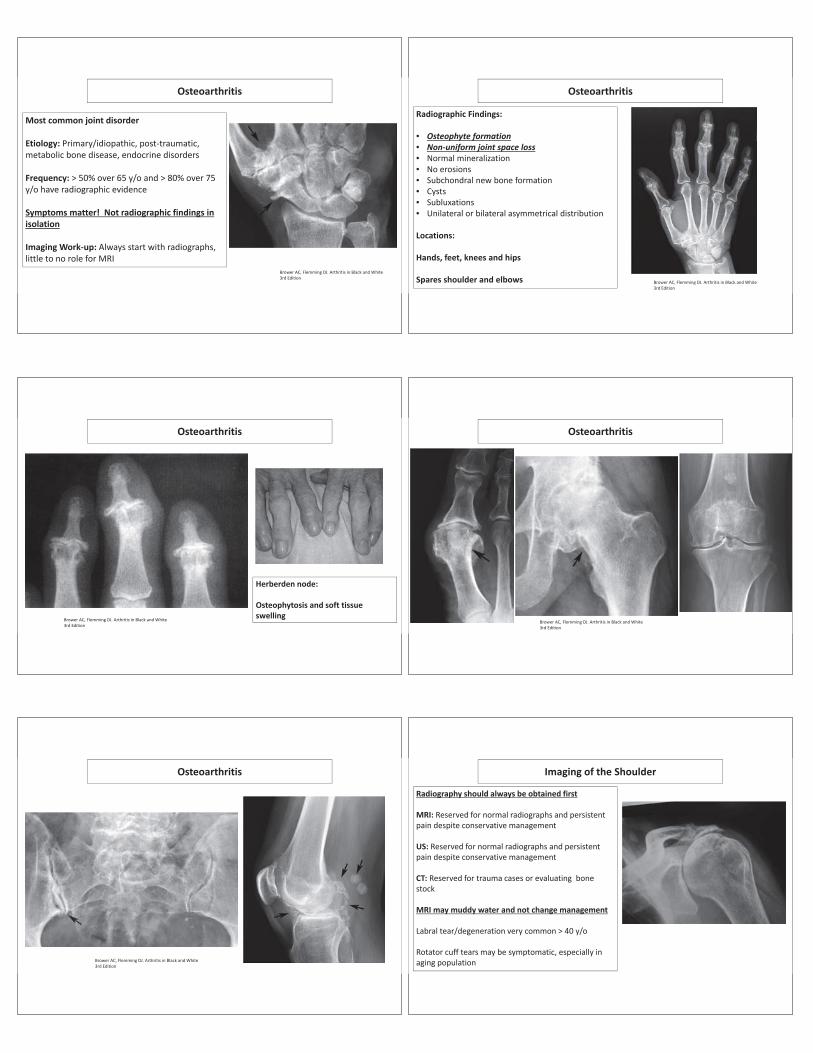
Radiographic Findings:
• Osteophyte formation• Non uniform joint space loss• Normal mineralization• No erosions• Subchondral new bone formation• Cysts• Subluxations• Unilateral or bilateral asymmetrical distribution
Locations:
Hands, feet, knees and hips
Spares shoulder and elbows Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Osteoarthritis
Herberden node:
Osteophytosis and soft tissueswellingBrower AC, Flemming DJ. Arthritis in Black and White
3rd Edition
Osteoarthritis
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Osteoarthritis
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Imaging of the Shoulder
Radiography should always be obtained first
MRI: Reserved for normal radiographs and persistentpain despite conservative management
US: Reserved for normal radiographs and persistentpain despite conservative management
CT: Reserved for trauma cases or evaluating bonestock
MRI may muddy water and not change management
Labral tear/degeneration very common > 40 y/o
Rotator cuff tears may be symptomatic, especially inaging population
Imaging of the Shoulder Imaging of the Shoulder
Imaging of the Knee
Radiography should always be obtained first
MRI: Reserved for normal radiographs andpersistent pain despite conservative management
CT: Reserved for trauma cases or evaluating bonestock
MRI may muddy water and not changemanagement
Meniscal tears may be asymptomatic and surgicaltreatment may precipitate osteoarthritis
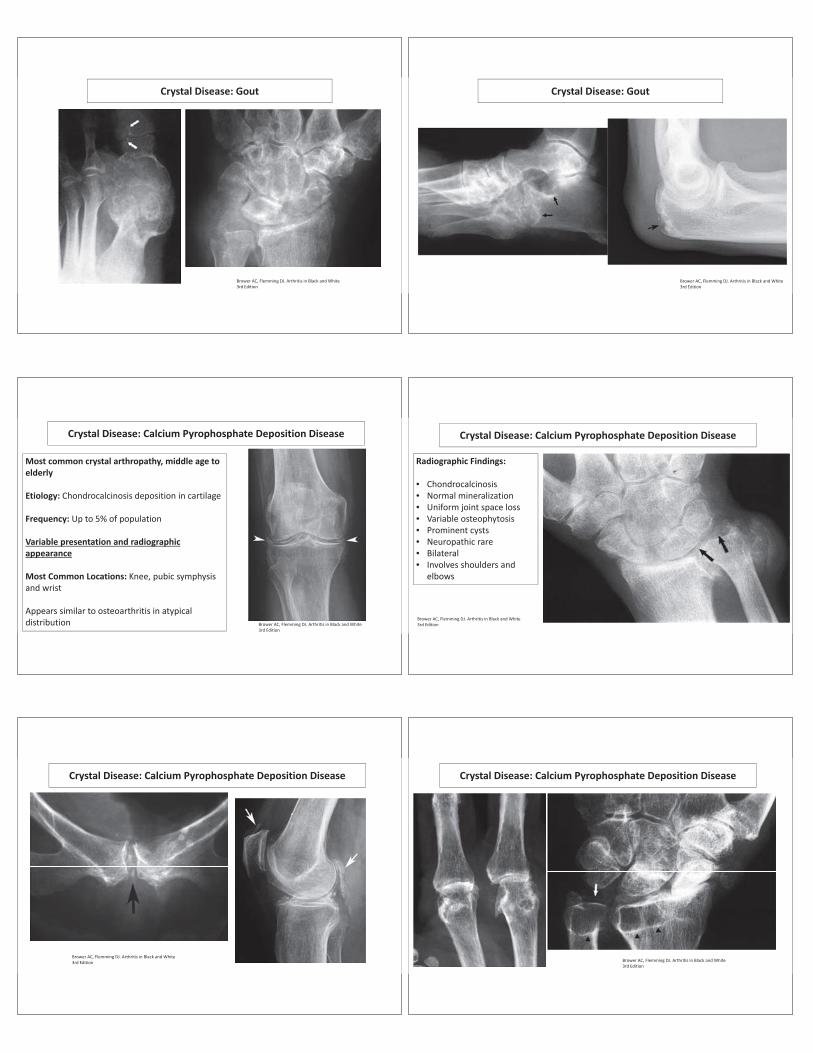
Crystal Disease: Gout
Increasing frequency with aging, 20x M>F
Etiology: Monosodium urate deposition, primary andsecondary
Presentation: Hot, painful, swollen joint, can mimicinfection
Radiographic findings depend on location of crystals
Only 45% of patients have radiographic findings, takes6 8 years
Cartilage: Osteoarthritis
Soft Tissues: Tophaceous goutBrower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Crystal Disease: Gout
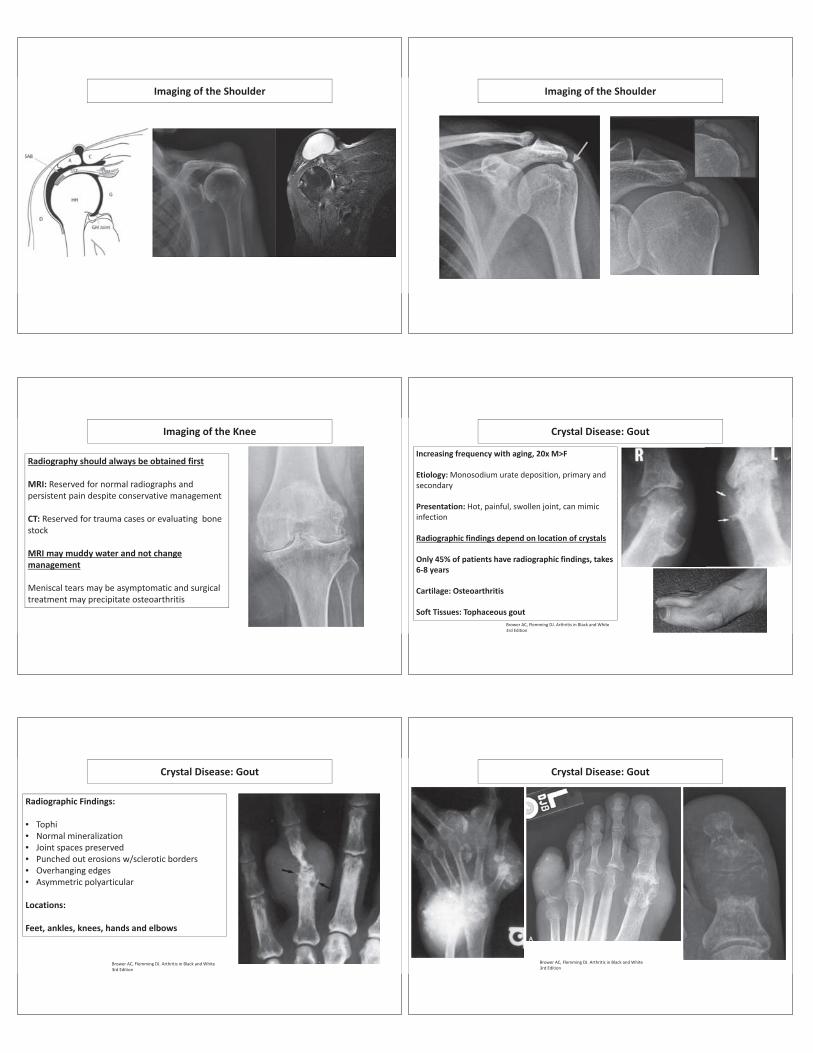
Radiographic Findings:
• Tophi• Normal mineralization• Joint spaces preserved• Punched out erosions w/sclerotic borders• Overhanging edges• Asymmetric polyarticular
Locations:
Feet, ankles, knees, hands and elbows
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Crystal Disease: Gout
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Crystal Disease: Gout
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Crystal Disease: Gout
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
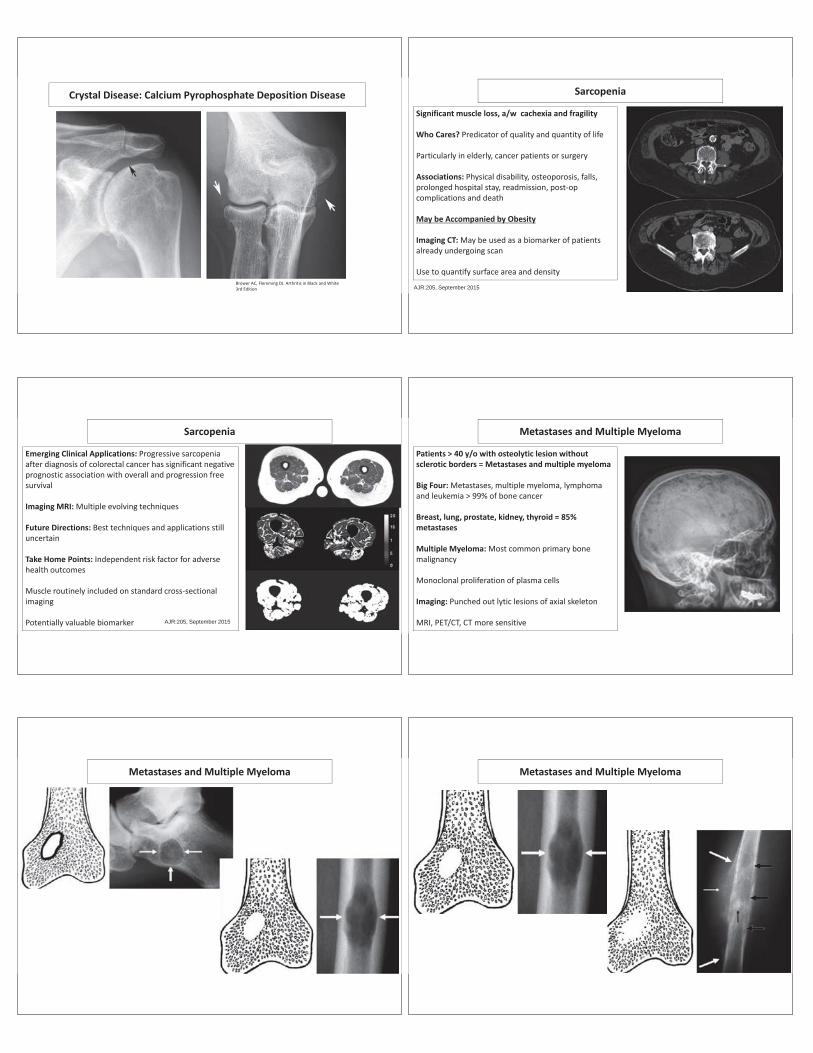
Crystal Disease: Calcium Pyrophosphate Deposition Disease
Most common crystal arthropathy, middle age toelderly
Etiology: Chondrocalcinosis deposition in cartilage
Frequency: Up to 5% of population
Variable presentation and radiographicappearance
Most Common Locations: Knee, pubic symphysisand wrist
Appears similar to osteoarthritis in atypicaldistribution Brower AC, Flemming DJ. Arthritis in Black and White
3rd Edition
Radiographic Findings:
• Chondrocalcinosis• Normal mineralization• Uniform joint space loss• Variable osteophytosis• Prominent cysts• Neuropathic rare• Bilateral• Involves shoulders and
elbows
Crystal Disease: Calcium Pyrophosphate Deposition Disease
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Crystal Disease: Calcium Pyrophosphate Deposition Disease
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Crystal Disease: Calcium Pyrophosphate Deposition Disease
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Crystal Disease: Calcium Pyrophosphate Deposition Disease
Brower AC, Flemming DJ. Arthritis in Black and White3rd Edition
Sarcopenia
Significant muscle loss, a/w cachexia and fragility
Who Cares? Predicator of quality and quantity of life
Particularly in elderly, cancer patients or surgery
Associations: Physical disability, osteoporosis, falls,prolonged hospital stay, readmission, post opcomplications and death
May be Accompanied by Obesity
Imaging CT: May be used as a biomarker of patientsalready undergoing scan
Use to quantify surface area and density
AJR:205, September 2015
Sarcopenia
Emerging Clinical Applications: Progressive sarcopeniaafter diagnosis of colorectal cancer has significant negativeprognostic association with overall and progression freesurvival
Imaging MRI: Multiple evolving techniques
Future Directions: Best techniques and applications stilluncertain
Take Home Points: Independent risk factor for adversehealth outcomes
Muscle routinely included on standard cross sectionalimaging
Potentially valuable biomarker AJR:205, September 2015
Metastases and Multiple Myeloma
Patients > 40 y/o with osteolytic lesion withoutsclerotic borders = Metastases and multiple myeloma
Big Four: Metastases, multiple myeloma, lymphomaand leukemia > 99% of bone cancer
Breast, lung, prostate, kidney, thyroid = 85%metastases
Multiple Myeloma: Most common primary bonemalignancy
Monoclonal proliferation of plasma cells
Imaging: Punched out lytic lesions of axial skeleton
MRI, PET/CT, CT more sensitive
Metastases and Multiple Myeloma Metastases and Multiple Myeloma
Questions
SUPPLEMENTS AND THE SUPPLEMENT INDUSTRY
Kerry Kuehl, M.D., Dr.P.H., M.S.Professor of MedicineChief Health Promotion and Sports MedicineDirector Human Performance LaboratoryOregon Health & Science University
Health Promotion & Sports Medicine
RESEARCH
REHABILITATION
WILDERNESSMEDICINETEAM PHYSICIAN
WEIGHT LOSS
Human Performance LaboratoryHealth Risk AssessmentPhysician conducted H&P examBlood tests for cholesterol and diabetesBody composition analysis Cardiopulmonary exercise stress testBasal Metabolic Rate measurementDietary analysis and prescription Weight loss counselingElite athlete testing and trainingSports nutrition and supplements
Nutritional Supplement Types
VitaminsMineralsHerbs or BotanicalsSports SupplementsThermogenic or Weight Loss ProductsMeal Replacements“Healthy” Water
SPORTS SUPPLEMENTS
Sports Drinks (Gatorade, Red Bull, etc.)Bars and Gels (Powerbar, Supergel)Amino Acids (Arginine, BCAA, Creatine)Protein Powders (Whey, Casein)Minerals (Chromium, Iron, Sodium, etc)Stimulants (Ephedrine, Caffeine, etc)Anabolic Precursors (DHEA, Andro, etc)Vitamins (Vit B, C, folate, etc)
GROWTH OF AN INDUSTRY
2016
$50 billion
Consumer Use of Supplements
Dissatisfaction with limitations of conventional medicinePerception of Western model of medicine –“Drugs” only and not “natural”Medical practices of other cultures“Lifestyle” causes of diseasePrevention issues and desire to reduce medsConvenience shopping and think less costly
Dietary Supplement Health and Education Act of 1994
Congress passed into law this act which allows a supplement to be excluded from regulation as a food additive or drug.Can bring the product to market without any reports or studies or safety or efficacy of the product.
Supplement Claims
The act allows manufacturers to make nutritional benefit claims that are not disease-related claims
OK to make health claim as long as product or ingredients cannot prevent, treat, or cure a specific disease.
Cure For The Common Cold
Zinc: Inconsistent evidence 2008- $24 million fraud NEJM 2011: No effect
New Dietary Ingredients and Labeling
The act allows ingredients in supplements only if they have been present in the food supply in a natural form that is not chemically altered, or have a history of use or other evidence of safety.Ingredients and dosages must be stated on the label.
Supplement Studies on Product Purity
50% of dietary supplements tested had mislabeled ingredients (FTC, 2000)25% of sports supplements tested were contaminated with “banned” substances (USADA, Jan 2010) FTC trying to enforce supplement labels and content with USP (US Pharmacopoeia) which means product passed tests for purity.
Statements of Nutritional Safety
The act exempts, from the definition of labeling, information in the form of an article, report, safety study, book chapter, or official abstract of a peer-reviewed scientific publication used in connection with the sale of supplements.
Formula-One: The Ultimate Supplement
“all natural supplement that will make you feel better and have more energy”“control of hunger, reduced sugar cravings, burn more fat and lose weight”Contains boron, chromium, Vitamins B3, C and E, multiple herbs including Ma-huang (ephedrine), Kola Nut (caffeine), White Willow Bark (salicylate), Gingko Biloba (aspirin + Vit E), Bladderwrack (iodine).
FDA Pulls Formula One
Affiliated Consultants International has been instructed to stop marketing this product due to numerous adverse events and fatalities associated with this product.
How can this be prevented?
SAFETY BURDEN ON US
The act considers a supplement to be adulterated if it presents a significant or unreasonable risk of illness or injury under conditions of use stated on label or understood under ordinary use.
Healthcare providers have become the watchdogs of the industry.
FTC Releases Report on Dietary Supplement Advertising
Report shows 55% false claims and another 40 % misleading or deceptive ads.Two major trends in past 10 years: 1) For weight loss, shift away from exerciseto taking the diet pill only to lose weight.2) New ads much more likely to make misleading and deceptive promises.
Examples of Weight Loss Ads False Claims
Claim: Lose weight while you sleep or with a patch.
Fact: Products and programs that promise quick easy weight loss are bogus. To lose weight, you have to lower your intake of calories and increase your physical activity.
False Claim
Lose 12 pounds in 2 days, or lose 30 ponds in 30 days
Fact: The faster you lose weight, the more likely you’ll gain it back. Experts recommend a goal of 1 pound/week
Healthier Water? Healthy or Unhealthy?
On January 14, 2009, the Center for Science in the Public Interest filed a class-action lawsuit against Energy Brands alleging that the marketing of the drink as a "healthful alternative" to water is deceptive and in violation of FTCCSPI states that the 33 grams of sugar in each bottle of Vitaminwater do more to promote obesity, diabetes and other health problems than the vitamins in the drinks do to perform the advertised benefits listed on the bottles". Coca-Cola dismissed the suit as "ridiculous," on the grounds that "no consumer could reasonably be misled into thinking Vitaminwater was a healthy beverage" and was only an attempt by the group to increase its readership
Interactions of Supplements and Medications ?
“Check with your health care provider or pharmacist if there is the potential for an interaction.”
We know about drug/nutrient interactions and drug/drug interactions. Now there is thesupplement/drug interactions.
Specific Supplement Interactions
Ginkgo Biloba:Mechanism of action: antioxidant like Vitamin E and antiplatelet effect like aspirin. Interaction: with anti-coagulant medications such as Aspirin, Coumadin (Warfarin), Heparin.Adverse Event: Multiple cases of spontaneous hemorrhage (GI, Brain)
DIETARY SUPPLEMENTS TARGETING KIDS
Source Nutraceuticals “Focus Child” has over 400 items including “Rhino Pops” (Echinacea) for “colds”.Fresh Samantha “Oh Happy Day” Vitamin line contains St. John’s Wort.MLO Products, Inc. provides free creatine monohydrate supplement to Mater Dei H.S. and claims credit for “building champions”.
VIT D – Super Hormone? Strong biological and mechanistic bases indicate that vitamin D plays a role in the prevention of colon, prostate, and breast cancers.
Emerging epidemiologic data suggest that vitamin D has a protective effect against colon cancer, but the data are not as strong for a protective effect against prostate and breast cancer, and are variable for cancers at other sites.
Studies do not consistently show a protective effect or no effect, however.
Dietary Supplement Fact Sheet: Vitamin D
NIH Office of Dietary Supplements: Vitamin D is a fat-soluble vitamin naturally present in very few
foods (cod liver oil) and produced endogenously when ultraviolet rays from sunlight strike the skin and trigger vitamin D synthesis
Vitamin D (+ Calcium) helps protect adults from osteoporosis.
Serum concentration of 25(OH)D best indicator of vitamin D status.
ANTIOXIDANTS and CANCER
Mechanism of action: inhibit oxidant formation, interfere with the oxidant activity once already formed, and repair injury caused by oxidants.Findings are from molecular and cellular experiments done on animals. Human trials ongoing (50,000 sites mentioning subject).Epidemiologic data show association of antioxidants ONLY FROM FOOD (not from supplements) in prevention of cancer.
Antioxidants and CHD
Antioxidant Supplements have not been proven to prevent heart disease by current clinical and epidemiological evidence.Recommendation: obtain antioxidants from food (mainly fruits, vegetables).US Surgeon General: Healthy People 2020
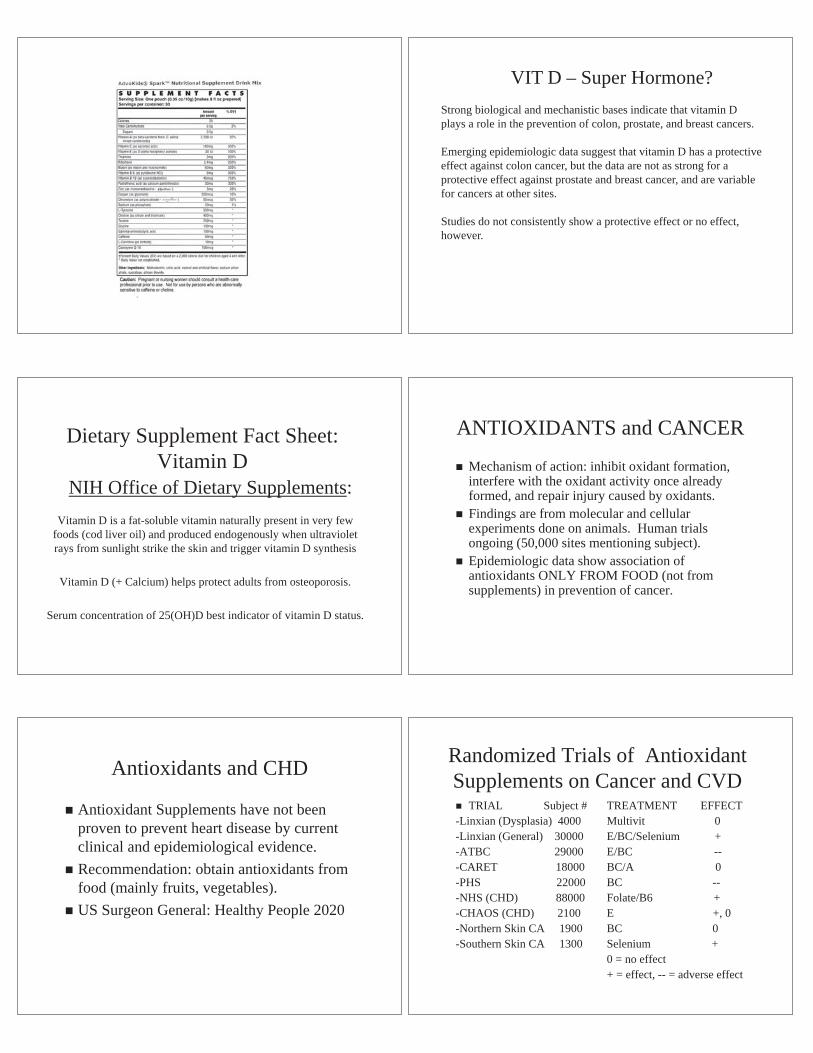
Randomized Trials of Antioxidant Supplements on Cancer and CVD
TRIAL Subject #-Linxian (Dysplasia) 4000 -Linxian (General) 30000-ATBC 29000-CARET 18000-PHS 22000-NHS (CHD) 88000-CHAOS (CHD) 2100-Northern Skin CA 1900-Southern Skin CA 1300
TREATMENT EFFECTMultivit 0E/BC/Selenium +E/BC --BC/A 0BC --Folate/B6 +E +, 0BC 0Selenium +0 = no effect+ = effect, -- = adverse effect
Fruits and vegetables derive antioxidant properties from the chemical that causes their various colors
Red - tomato, red plum, watermelon, pink grapefruit. Lycopene inhibit cancer cell growth.
Red/Purple - grapes, cherries, strawberries, raspberries, blueberries, prunes, red apples. Proanthocyanins inhibit cancer cell growth.
Green - broccoli, Brussel sprouts, cabbage, bok choy. Isothio-cyanates increase liver proteins against carcinogens.
Green/Yellow - spinach, corn, kale, avocado, mustard greens. Lutein protects vision, the heart, and inhibits cancer cell growth.
Orange - carrots, cantaloupe, pumpkin, apricots. Beta carotene (vision/immune fxn).
Orange/Yellow - oranges, lemons, papaya, peaches, nectarines, pineapple. Flavonoids inhibit tumor growth and repair DNA. Limonoids in the skin of oranges and lemon inhibit tumor growth.
Green/White - Garlic, onion, celery, chives, pears, leeks. Allyl sulfides inhibit tumor cell.
Kuehl Research on Tart Cherries
Fibromyalgia Study
Hood To Coast Runner Study
Inflammatory Osteoarthritis Study
Tart Cherries and Muscle Damage
45
Tart cherries have both antioxidant and anti-inflammatory properties. They contain flavonoids (anti-inflammatory), which inhibit cyclo-oxygenase 1 and 2, and anthocyanins with high antioxidant activities.
Why Study Tart Cherries?
46
1
48
**
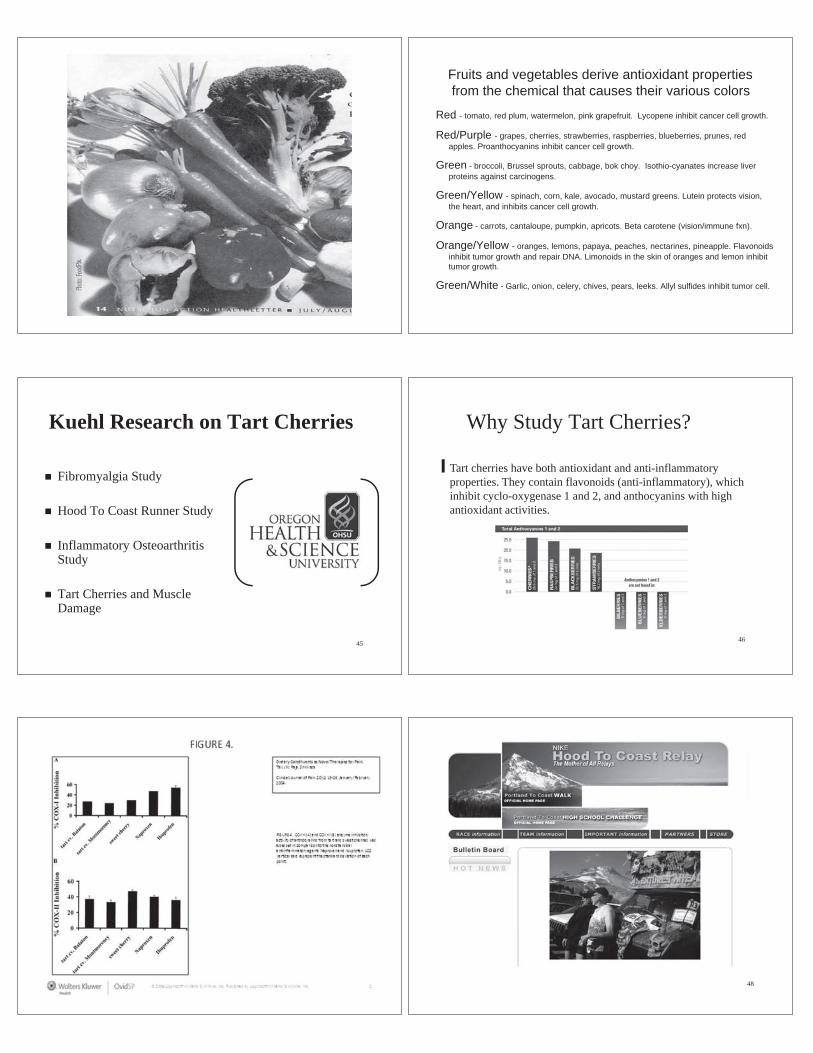
**p<.01 The Tart Cherry Group had a 25 mm lower pain score
37 mm
12mm
Post-Race Pain Assessment
49
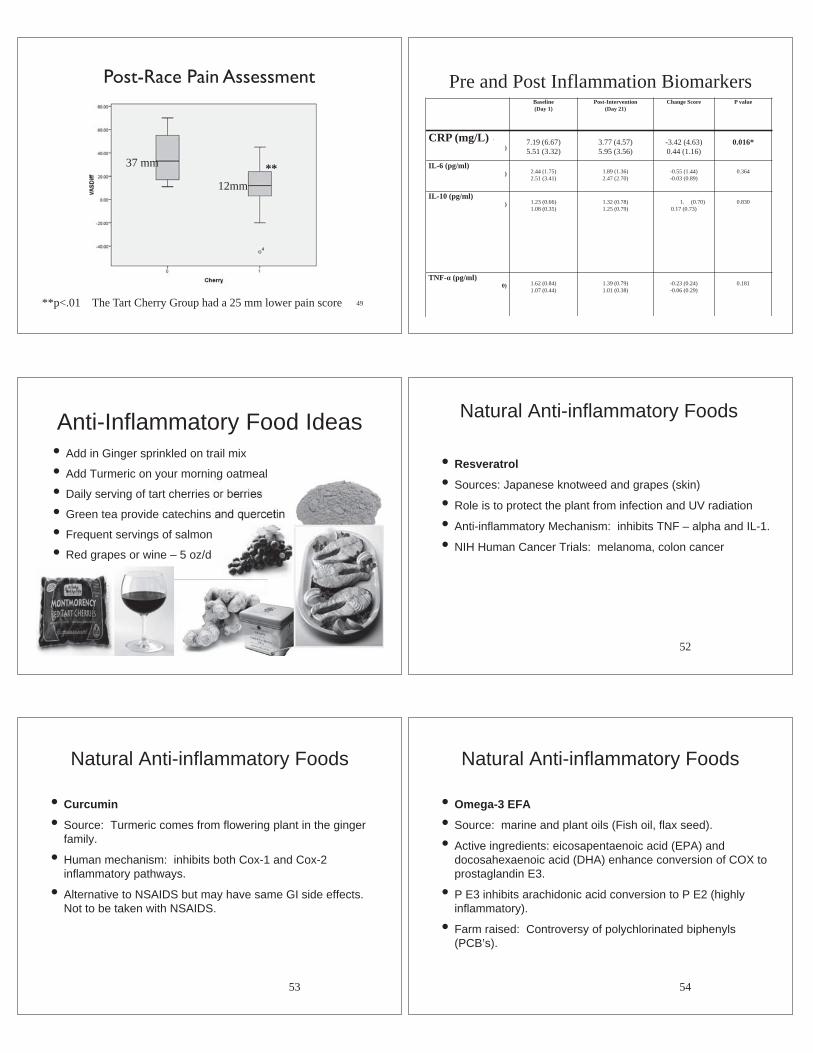
Pre and Post Inflammation BiomarkersBaseline(Day 1)
Post-Intervention(Day 21)
Change Score P value
CRP (mg/L))
7.19 (6.67)5.51 (3.32)
3.77 (4.57) 5.95 (3.56)
-3.42 (4.63)0.44 (1.16)
0.016*
IL-6 (pg/ml)) 2.44 (1.75)
2.51 (3.41)1.89 (1.36)2.47 (2.70)
-0.55 (1.44)-0.03 (0.89)
0.364
IL-10 (pg/ml)) 1.23 (0.66)
1.08 (0.35)1.32 (0.78)1.25 (0.79)
1. (0.70)0.17 (0.73)
0.830
TNF- (pg/ml)0) 1.62 (0.84)
1.07 (0.44)1.39 (0.79)1.01 (0.38)
-0.23 (0.24)-0.06 (0.29)
0.181
.
Anti-Inflammatory Food Ideas• Add in Ginger sprinkled on trail mix
• Add Turmeric on your morning oatmeal
• Daily serving of tart cherries or berries
• Green tea provide catechins and quercetin
• Frequent servings of salmon
• Red grapes or wine – 5 oz/d
Natural Anti-inflammatory Foods
• Resveratrol
• Sources: Japanese knotweed and grapes (skin)
• Role is to protect the plant from infection and UV radiation
• Anti-inflammatory Mechanism: inhibits TNF – alpha and IL-1.
• NIH Human Cancer Trials: melanoma, colon cancer
52
Natural Anti-inflammatory Foods
• Curcumin
• Source: Turmeric comes from flowering plant in the ginger family.
• Human mechanism: inhibits both Cox-1 and Cox-2 inflammatory pathways.
• Alternative to NSAIDS but may have same GI side effects. Not to be taken with NSAIDS.
53
Natural Anti-inflammatory Foods
• Omega-3 EFA
• Source: marine and plant oils (Fish oil, flax seed).
• Active ingredients: eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) enhance conversion of COX to prostaglandin E3.
• P E3 inhibits arachidonic acid conversion to P E2 (highly inflammatory).
• Farm raised: Controversy of polychlorinated biphenyls (PCB’s).
54

Supplements Needed in the Pacific Northwest?
• Vitamin D – Should get Vit D level checked.
• Iron– Athletes should get serum ferritin checked for anemia.
• Calcium – Menopausal women, adolescents females, lactose intolerance patients should be assessed.
• Vitamin B12 - Vegetarians should get level checked and individuals on Proton Pump Inhibitors.
• Seasonal Affective Disorder Syndrome – Vitamin D Deficiency associated with SADS. St John’s Wort does not work. Try to supplement with a light therapy box.
CONCLUSION
Since DSHEA, explosion in nutritional supplement industry.FDA takes action on Supplement Safety in 2003.Use must be guided by scientific study of efficacy, minimum and maximum safety doses, interactions, adverse effects, and costs.
Resources
Ask the pharmacistConsumerLab.comSupplementwatch.comNutrition Action LetterFDA Supplement websiteNIH Office of Dietary SupplementsNCCAM

+
Nels Carlson, M.D.Assistant Dean
Continuing Professional Development
School of Medicine
Associate Professor
Department of Orthopaedics and Rehabilitation
Oregon Health and Sciences University
+
Physical Medicine and RehabilitationFocus on restoring functionExercise is the mainstay of treatment for most
musculoskeletal conditions
-Musculoskeletal Medicine
-- Non-operative treatment:
-- Muscles and nerves
-- Joints and bones
-- Osteoarthritis
-- Spine
- Sports
+Overview1. Benefits of Exercise
2. “Quality of Life” Insurance
3. “Quantity of Life” Insurance
4. What Does the Research Show?
5. Maintaining an ExerciseProgram
6. Recommendations and Prescription for Physical Activity
7. What’s New in Exercise Science?
+ Why Exercise?Top Ten List of Reasons to Exercise – Mayo Clinic
Exercise will reduce fatigue levels.
Aerobic exercise reduces the risk of diabetes, heart disease, cancer.
Aerobic exercise can help prevent heart attacks, and subsequent heart attacks.
Exercise activates the immune system, making you less susceptible to viral illness, such as colds and the flu.
Exercise and diet will help you lose weight and maintain weight loss.
Exercise can reduce tension, promote relaxation and decrease depression.
With long-term exercise, your heart is stronger, pumps blood more efficiently.
Aerobic exercise can favorably effect your cholesterol levels.
Aerobic exercise can help older people maintain muscle strength, maintain mobility, decrease falls, and decrease age-related cognitive decline.
People who participate in regular aerobic exercise appear to live longer than those who don’t exercise regularly.
+ Gait Speed - The Next Vital Sign?
• Predicted survival based on:• age, sex and gait speed
• was as accurate as predicted survival based on:• age, sex, chronic conditions, smoking
history, blood pressure, body mass index and hospitalization.
• “Why does walking speed predict survival? Walking requires energy, movement control, and support and places demands on multiple organ systems, including the heart, lungs, circulatory, nervous and musculoskeletal systems.”
• Studenski S, et al. Gait Speed and Survival in Older Adults. JAMA. 2011;305(1):50-58.
+
Do you have “Quality of Life” Insurance?Exercise not only helps to prevent or manage disease, exercise may be the “Fountain of Youth” that maintains independence and quality of life as we age.
+Exercise – your “Quality of Life” Insurance
People are less physically active as they age.
Nearly 40% of people age 55 or greater report no leisure-time physical activity.
Inactive people lose muscle at a rate of 3-5% every decade after age 30.
15% of muscle is lost by age 60.
Loss of strength results in:Decreased balanceIncreased fall riskDecreased ability to perform activities of daily living
Decreased exercise tolerance results in a diminished “threshold of physical ability”
A minor illness or injury may result in complete dependence for daily care
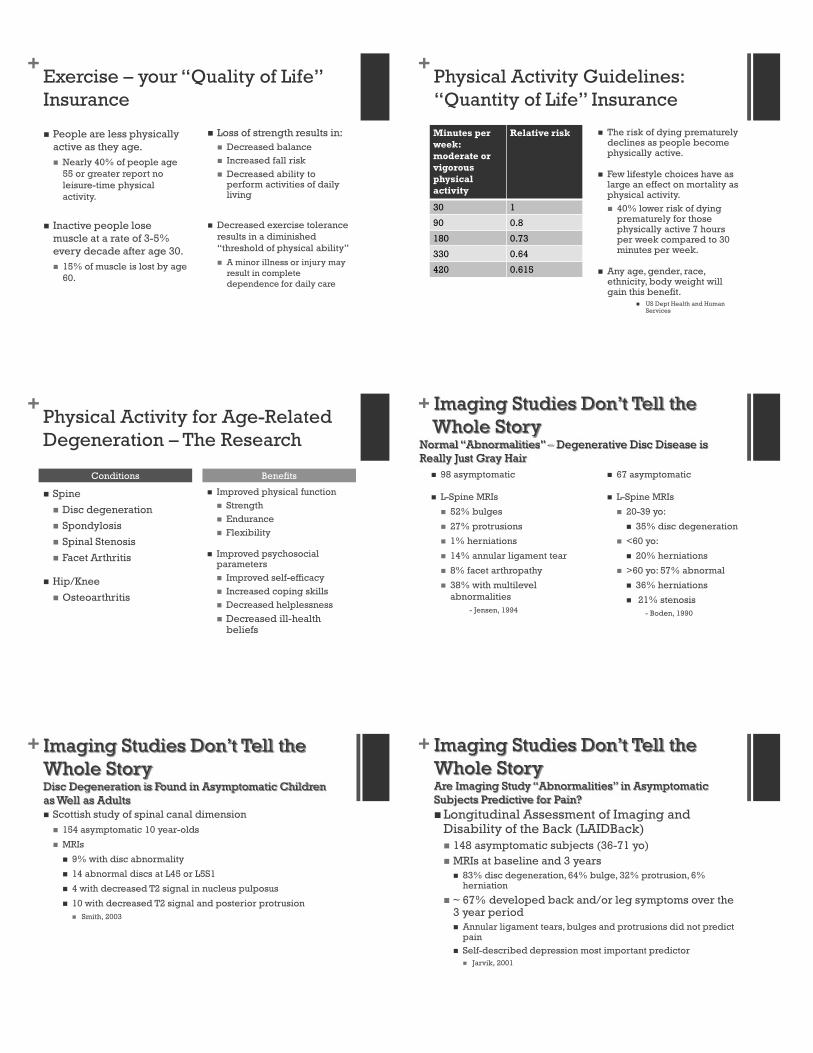
+Physical Activity Guidelines:“Quantity of Life” Insurance
Minutes per week:moderate or vigorous physical activity
Relative risk
30 1
90 0.8
180 0.73
330 0.64
420 0.615
The risk of dying prematurely declines as people become physically active.
Few lifestyle choices have as large an effect on mortality as physical activity.
40% lower risk of dying prematurely for those physically active 7 hours per week compared to 30 minutes per week.
Any age, gender, race, ethnicity, body weight will gain this benefit.
US Dept Health and Human Services
+Physical Activity for Age-Related Degeneration – The Research
Spine
Disc degeneration
Spondylosis
Spinal Stenosis
Facet Arthritis
Hip/Knee
Osteoarthritis
Improved physical functionStrengthEndurance Flexibility
Improved psychosocial parameters
Improved self-efficacyIncreased coping skillsDecreased helplessness
Decreased ill-health beliefs
Conditions Benefits
++ Imaging Studies Don’t Tell the ++ Imaging StudiWhole Storyy
Normal “Abnormalities” y
” –– Degenerative Disc Disease is NNormal AbnormalitieReally Just Gray Hair
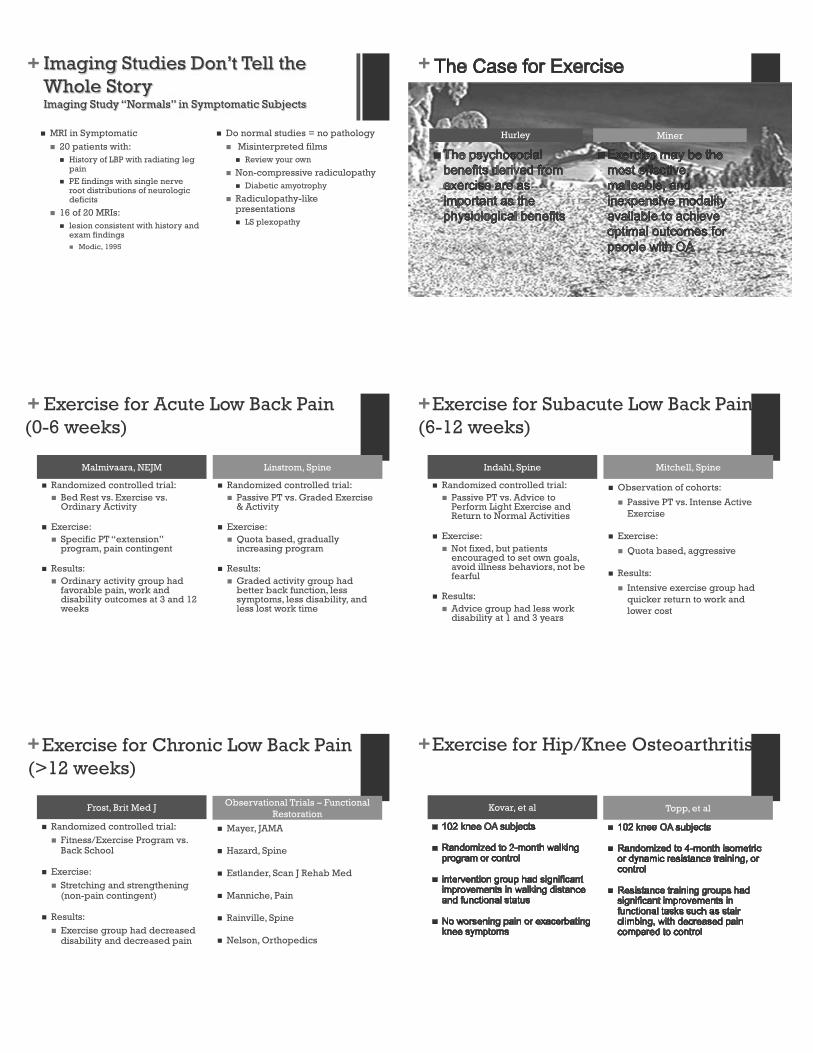
98 asymptomatic
L-Spine MRIs
52% bulges
27% protrusions
1% herniations
14% annular ligament tear
8% facet arthropathy
38% with multilevel abnormalities
- Jensen, 1994
67 asymptomatic
L-Spine MRIs
20-39 yo:
35% disc degeneration
<60 yo:
20% herniations
>60 yo: 57% abnormal
36% herniations
21% stenosis - Boden, 1990
++ Imaging Studies Don’t Tell the Imaging StudiWhole StoryyDisc Degeneration is Found in Asymptomatic Children gDisc Degenerationas Well as Adults
Scottish study of spinal canal dimension154 asymptomatic 10 year-olds
MRIs
9% with disc abnormality
14 abnormal discs at L45 or L5S1
4 with decreased T2 signal in nucleus pulposus
10 with decreased T2 signal and posterior protrusionSmith, 2003
++ Imaging Studies Don’t Tell the Imaging StudiWhole StoryyAre Imaging Study “Abnormalities” in Asymptomatic Are Imaging Study AbnormalAre Imaging Study AbnSubjects Predictive for Pain?
Longitudinal Assessment of Imaging and Disability of the Back (LAIDBack)
148 asymptomatic subjects (36-71 yo)MRIs at baseline and 3 years
83% disc degeneration, 64% bulge, 32% protrusion, 6% herniation
~ 67% developed back and/or leg symptoms over the 3 year period
Annular ligament tears, bulges and protrusions did not predict painSelf-described depression most important predictor
Jarvik, 2001
++ Imaging g Studies Don’t Tell the + ImagingWhole
tudiStngg e e Story
Imaging Study “y
“Normalssl ” in Symptomatic Subjects
MRI in Symptomatic20 patients with:
History of LBP with radiating leg pain
PE findings with single nerve root distributions of neurologic deficits
16 of 20 MRIs:lesion consistent with history and exam findings
Modic, 1995
Do normal studies = no pathologyMisinterpreted films
Review your own
Non-compressive radiculopathyDiabetic amyotrophy
Radiculopathy-like presentations
LS plexopathy
+
Hurley Miner
+ Exercise for Acute Low Back Pain (0-6 weeks)
Malmivaara, NEJM
Randomized controlled trial:Bed Rest vs. Exercise vs. Ordinary Activity
Exercise:Specific PT “extension” program, pain contingent
Results:Ordinary activity group had favorable pain, work and disability outcomes at 3 and 12 weeks
Linstrom, Spine
Randomized controlled trial:Passive PT vs. Graded Exercise & Activity
Exercise:Quota based, gradually increasing program
Results:Graded activity group had better back function, less symptoms, less disability, and less lost work time
+Exercise for Subacute Low Back Pain (6-12 weeks)
Indahl, Spine
Randomized controlled trial:Passive PT vs. Advice to Perform Light Exercise and Return to Normal Activities
Exercise:Not fixed, but patients encouraged to set own goals, avoid illness behaviors, not be fearful
Results:Advice group had less work disability at 1 and 3 years
Mitchell, Spine
Observation of cohorts:
Passive PT vs. Intense Active Exercise
Exercise:
Quota based, aggressive
Results:
Intensive exercise group had quicker return to work and lower cost
+Exercise for Chronic Low Back Pain (>12 weeks)
Frost, Brit Med J
Randomized controlled trial:Fitness/Exercise Program vs. Back School
Exercise:Stretching and strengthening (non-pain contingent)
Results:Exercise group had decreased disability and decreased pain
Observational Trials – Functional Restoration
Mayer, JAMA
Hazard, Spine
Estlander, Scan J Rehab Med
Manniche, Pain
Rainville, Spine
Nelson, Orthopedics
+Exercise for Hip/Knee Osteoarthritis
Kovar, et al Topp, et al
+Exercise for Hip/Knee Osteoarthritis
Ettinger, et al Hopman-Rock, et al
+Exercise for Hip/Knee Osteoarthritis
Van Baar, et al Van Baar, et al
+
Exercise AdherenceNow that you are exercising, how do you stick with a program?
+Exercise Adherence
Complex, multifactorialperceptions of personal capabilities
positive attitudes toward exercise
sense of control over exercise
level of confusion regarding exercise
attrition rates of 50% within the first 6 months
+Exercise Adherence
Jette et al102 sedentary older subjects
Home-based resistance training program
Identified adherence factors
Physical factors:
Indicators of overall exercise participation
Psychological factors:
Indicators of program adherence
+Exercise Adherence
McAuley et al114 middle-aged subjectsRandomly assigned to 5 month exercise - education vs. control groupEducation group included educational intervention focusing on increasing confidence regarding ability to exerciseEducation group had increased adherence, decreased attrition over time
+Exercise Adherence
Keeping it simple:
Get out of the house!
Peer support
Work out with someone or in a group
Do exercises that you like
Any activity is better than no activity
+
Physical Activity GuidelinesU.S. Department of Health & Human Services-Research Findings
-Types of Physical Activity
-Which Physical Activity is Best
-Recommendations for Youth, Adults, Older Adults
+Physical Activity Guidelines:Research on Health Benefits
Decreased risk of adverse health events.
Increased amount of physical activity is associated with increased benefits.
Both aerobic and resistance activities are beneficial.
Decreased risk of premature death (heart disease, some cancers).
Children
Adolescents
Adults
Older adults
Every racial and ethnic group
Disabilities
Chronic disease
What are the Benefits? Who Benefits?
+Physical Activity Guidelines:Type of exercise
Aerobic (endurance, cardio)Brisk walking
Running
Jumping rope
Cycling
Swimming
Components
Intensity
Frequency
Duration
+Physical Activity Guidelines:Type of exercise
Muscle-strengthening (resistance)
MachinesFree weightsElastic bands (theraband)Body weight (push-ups)
Components
Intensity
Frequency
Repetitions
+Physical Activity Guidelines:Type of exercise
Bone-strengtheningWeight-bearing exercisesPromotes bone growth and strength“Impact” activities
Brisk walk, weight lifting
Flexibility
Stretching
Yoga
Pilates

+Physical Activity Guidelines:Adults
AerobicAt least 3 days per weekAt least
150 minutes per week of moderateor 75 minutes of vigorous activity
For additional health benefits:300 minutes of moderateor 150 minutes of vigorous
Muscle-strengthening2 or more days per weekInvolve all major muscle groups
+Physical Activity Guidelines:Older Adults
Same as for adults, plus:If unable to do 150 minutes per week, be as active as chronic condition allows.
If at risk of falling, do exercises that maintain/improve balance.
Determine level of physical activity relative to fitness level.
Determine how chronic condition will affect ability to do regular activity.
+ A Function-Based Approach to Age-Related Degeneration and Pain
Build:
Strength
Endurance
Flexibility
Pain follows function
When function improves, pain improves
This is a process that takes months (especially as we get older), not days or weeks
Improve Function Decreae Pain
+
James Rainville, MDDept of PM&RHarvard Medical SchoolThe Spine CenterNew England Baptist HospitalBoston, MA
Rethinking Back Pain Based on
Epidemiology and Basic Science
Discoveries
+Conservative Treatment
Physical Activity
Why Self-Induced Pain Feels Less Painful than Externally Generated Pain: Distinct Brain Activation Patterns in Self- and Externally Generated Pain
Wang Y, et al.
PLoS ONE, 2011; 6(8):e23536
Prospective Cohort Study
25 subjects, asked to hold “ring” with points or spheres
Trial 1–squeeze with other handTrial 2–examiner squeezes hand
ResultsActive movement inhibited pain response in somatosensory cortexPain-inhibiting effect of voluntary activity may explain beneficial impact of exercise on pain
+NeuroscienceEffects of Exercise on PainAerobic exercise for 5 weeks
Results of exercise
Reversed mechanical sensitivity of limb
Normalized injury induced changes in dorsal ganglia and spinal cord
peripheral nerve growth factors (NGF)
brain-derived neurotrophic factor (BDNF)
phosphorylation status of PLCI-1
astrocyte and microglia hyperactivity
Almeida C, et al. Exercise therapy normalizes BDNF upregulation and glial hyperactivity in a mouse model of neuropathic pain.Pain 2015;156(3):504-13.
+NeuroscienceEffects of Exercise on PainLow intensity exercise
Results of exercise
Reduced pain behaviorsBrainstem
Increased serotonin (5-HT) production
Decreased 5-HT transport
Increased 5-HT receptors
Reduced inflammatory cytokines, tumor necrosis factor-alpha, and interleukin-1 beta
(These factors are known to modulate pain)
Bobinski F, et al. Role of brainstem serotonin in analgesia produced by low-intensity exercise on neuropathic pain after sciatic nerveinjury in mice. Pain 2015;156(12):2595-606.
+NeuroscienceEffects of Exercise on Pain
High intensity exercise
Results of exercise
Reduced withdrawal reflex
Mu-opioid receptors
Altered expression of mu-opioid receptors in brain stem and spinal cord shifting balance of pain modulation to inhibition.
This effect is blocked by opioid receptor antagonist naloxone.
Kim YJ, Byun JH, Choi IS. Effect of Exercise on Âμ-Opioid Receptor Expression in the Rostral Ventromedial Medulla in Neuropathic Pain Rat Model. Ann Rehabil Med 2015;39(3):331-9.Stagg NJ, et al. Regular exercise reverses sensory hypersensitivity in a rat neuropathic pain model: role of endogenous
opioids. Anesthesiology 2011;114(4):940-8.
+NeuroscienceEffects of Exercise on PainGraded exercise
Results of exercise
Reduced hyperalgesia in the skinNeurological changes
Prevented nerve fiber sprouting in the skin
Lowers neurotrophic factors in the sciatic nerve
Reduced NGF and BDNF in sensory neurons and spinal cord
Normalized pain disregulated ion transport in dorsal ganglia and spinal cord
Reduce microglia cell proliferation in spinal cord
Lopez-Alvarez VM, et al. Early increasing-intensity treadmill exercise reduces neuropathic pain by preventing nociceptorcollateralsprouting and disruption of chloride cotransporters homeostasis after peripheral nerve injury. Pain 2015;156(9):1812-25.
Chen YW, et al. Exercise training attenuates neuropathic pain and cytokine expression after chronic constriction injury of rat sciatic nerve. Anesth Analg 2012;114(6):1330-7.
+Neuroscience
The stimulus from exercise reverses pain sensitizing changes in the brainstem, spinal cord, dorsal ganglia and peripheral nerves.
Ossipov MH, et al. Descending pain modulation and chronification of pain. Curr Opin Support Palliat Care 2014;8:143-51.
+Human studies of exercise
Exercise
+Clinical Trials – Exercise
Spinal stabilizationGeneral exercise
Improvements in pain and disability similar in both groups.
Woo SD, Kim TH. The effects of lumbar stabilization exercise with thoracic extensionexercise on lumbosacral alignment and the low back pain disability index in patients with chronic low back pain. J Phys Ther Sci (2016 Jan) 28(2):680-4
+Clinical Trials – Exercise
Pilates exerciseGeneral exercise
Improvements in pain and disability similar in both groups.
Mostagi FQ, et al. Pilates versus general exercise effectiveness on pain and functionality in non-specific chronic low back pain subjects. J Bodyw Mov Ther (2015 Oct) 19(4):636-45
+Clinical Trials – Exercise
Motor control impairmentGeneral exercise
Improvements in pain and disability similar in both groups.
Saner J, et al. A tailored exercise program versus general exercise for a subgroup of patients with low back pain andmovement control impairment: Short-term results of a randomised controlled trial. J Bodyw Mov Ther (2016 Jan) 20(1):189-202
+Clinical Trials – Exercise
High load liftingLow load motor control
Improvements in pain and disability similar in both groups.
Michaelson P, et al. High load lifting exercise and low load motor control exercises as interventions for patients with mechanical low back pain: A randomized controlled trial with 24-month follow-up. J Rehabil Med (2016 Apr 28) 48(5):456-63
+Clinical Trials – Exercise
Supervised walkingFitness training
Improvements in pain and disability similar in both groups.
Hurley DA, et al. Supervised walking in comparison with fitness training for chronic back pain in physiotherapy: results of the SWIFT single-blinded randomized controlled trial Pain 2015;156:131-7.
+ The neurological effects of exercise are rather non-specific!
Specific exercise techniques may be less important than reaching a certain threshold of exercise needed to induce neurological changes that reduce pain stimulus threshold
“We are not responsible for what patients believes before they come to our practice.”
“We are responsible for what they believe when they leave.”
Aage Indahl, Spine 1995
+Goals: STAY FIT FOR QUALITY AND QUANTITY LIFE
The best exercise?
Meet the physical activity guidelines
Aerobic
Muscle-strengthening
Flexibility
Develop exercise buddiesPeer support
Maintain an exercise program over time
+Any activity is better than no activity!
MUSCULOSKELETAL UPDATE FOR PRIMARY CAREHans Carlson, MDAssociate Professor Physical Medicine & RehabilitationOHSU
INTERESTING CASES / PANELMaking the diagnosis with musculoskeletal pain
IF YOU’VE NEVER HEARD OF THE DIAGNOSIS…
…you can’t make the diagnosis.
IF YOU’VE NEVER HEARD OF THE DIAGNOSIS…
…you can’t make the diagnosis.Hans Carlson MS1, 1988
The prepared mind…
Where does it hurt?
What’s there that can hurt?
Musculoskeletal Injuries
TendonsMusclesLigamentsJointsBursaNervesReferred Pain
Know the patterns!
MusculoskeletalPain
• 44 y.o. female • 9 month history of progressive right hand/thumb numbness
• Complaints of grip weakness• Occasional radiation to the elbow and shoulder
• Symptoms increased at night or with driving
• No neck pain
A. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPain
• No history of prior surgery• No prescription medications• Occasional left knee pain with jogging
• Works as teacher
A. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
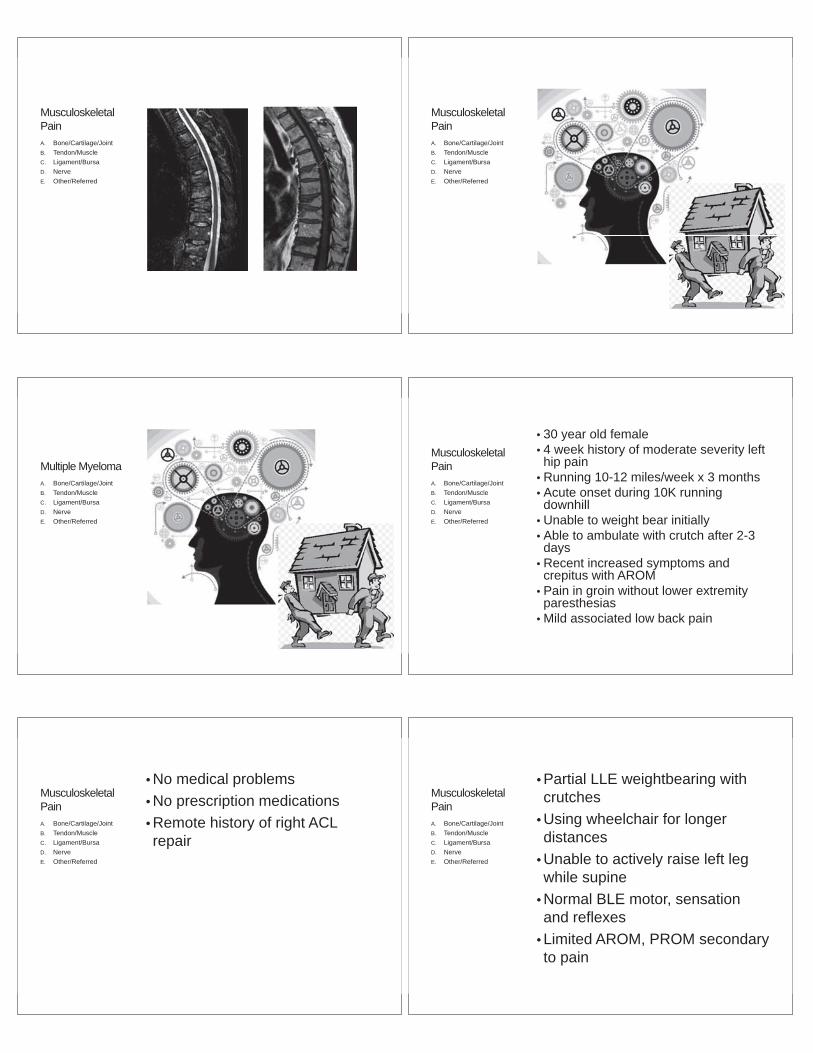
MusculoskeletalPain
• Mild left APB weakness• No intrinsic atrophy • Normal interosseii and finger flexor strength
• Normal sensation• Equivocal Tinel’s at wrist and Phalen’s maneuvers
A. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
Carpal Tunnel SyndromeA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPain
• 59 year old male• 4 month history of moderate to severe right thoracic spine pain
• Started with housework, no trauma• Continued symptoms despite rest with progression to low back pain
• No lower extremity numbness, weakness
• Increased symptoms with forward flexion, sitting, getting out of bed
• Decreased symptoms with NSAID, sitting with arm rest
• No red flags
A. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPain
• BPH• Hyperlipidemia• Allergic rhinitis• Meralgia paresthetica• Achilles tendon repair• No prior imaging
A. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
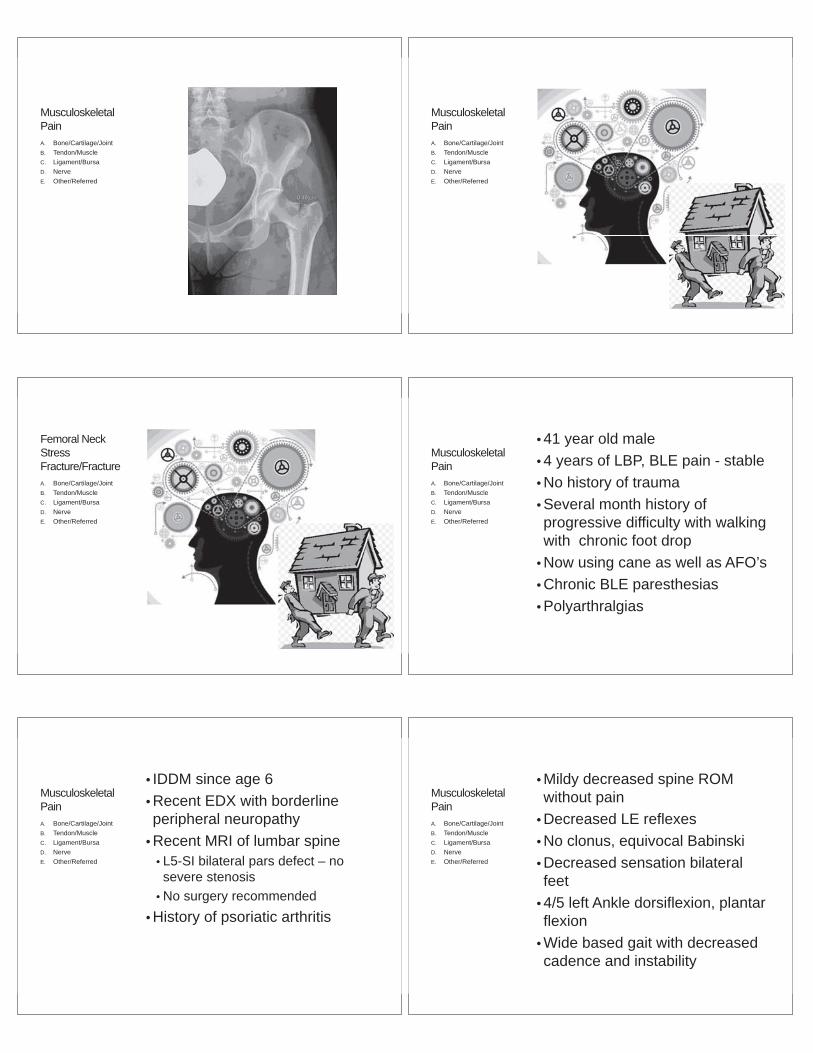
MusculoskeletalPain
• Decreased, painful thoracic and lumbar spine ROM
• Normal LE motor, sensory, reflexes
• Unremarkable gait, skin• Cervical spine ROM normal• Moderate to severe thoracolumbar paraspinal muscle and spinous process tenderness
• Normal, pain-free bilateral hip ROM
A. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
Multiple MyelomaA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• 30 year old female• 4 week history of moderate severity left hip pain
• Running 10-12 miles/week x 3 months• Acute onset during 10K running downhill
• Unable to weight bear initially• Able to ambulate with crutch after 2-3 days
• Recent increased symptoms and crepitus with AROM
• Pain in groin without lower extremity paresthesias
• Mild associated low back pain
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• No medical problems• No prescription medications• Remote history of right ACL repair
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Partial LLE weightbearing with crutches
• Using wheelchair for longer distances
• Unable to actively raise left leg while supine
• Normal BLE motor, sensation and reflexes
• Limited AROM, PROM secondary to pain
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
Femoral Neck StressFracture/FractureA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• 41 year old male• 4 years of LBP, BLE pain - stable• No history of trauma• Several month history of progressive difficulty with walking with chronic foot drop
• Now using cane as well as AFO’s• Chronic BLE paresthesias• Polyarthralgias
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• IDDM since age 6 • Recent EDX with borderline peripheral neuropathy
• Recent MRI of lumbar spine• L5-SI bilateral pars defect – no severe stenosis
• No surgery recommended• History of psoriatic arthritis
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Mildy decreased spine ROM without pain
• Decreased LE reflexes• No clonus, equivocal Babinski• Decreased sensation bilateral feet
• 4/5 left Ankle dorsiflexion, plantar flexion
• Wide based gait with decreased cadence and instability
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
Thoracic SyrinxA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
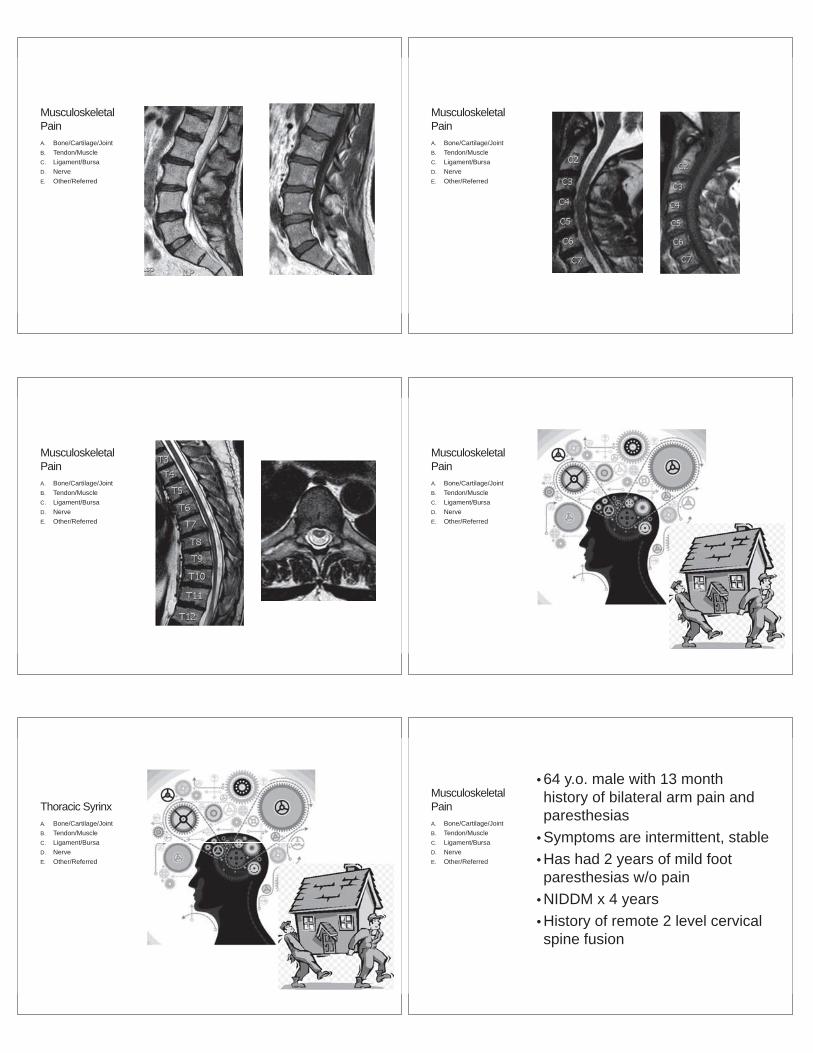
• 64 y.o. male with 13 month history of bilateral arm pain and paresthesias
• Symptoms are intermittent, stable• Has had 2 years of mild foot paresthesias w/o pain
• NIDDM x 4 years• History of remote 2 level cervical spine fusion
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Onset of symptoms shortly after ATV accident• Associated rib fractures
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Normal BUE motor strength• Normal BUE sensation to light touch
• Normal gait, balance and BLE sensation
• Negative CTS provocative maneuvers
• Negative Spurling s maneuver
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Symptoms only occur while he is urinating! Musculoskeletal
PainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Remote imaging of the thoracic spine and ribs following injury
• No other work-up or treatment
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
Severe Cervical Stenosis with InstabilityA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
Quick Radic:Efficient and Effective Assessment for
Radiating Upper Extremity Pain
OHSU Musculoskeletal Update for Primary Care
Erik Ensrud, MDAssociate Professor, Orthopaedics and Rehabilitation, OHSU
Board Certified in PM&R/EMG/Neurology/Neuromuscular Disease
What percentage of your patients arecomplaining of radiating arm or leg pain?A. < 5%
B. 5 10%
C. 10 15%
D. 15 20%
E. > 20%
Ms.K, a 38 yo new pt, c/o 2 months right arm painthat radiates down the arm to just past the elbow.You decide to…A. Order a cervical MRI
B. Order an EMG
C. Examine 8 muscles for strength
D. Examine 6 muscles, one neck test, and 3 shoulder tests
E. Examine 4 muscles, 2 MSK tests, and 3 sensory points…and do this in< 60 sec
PAIN THAT TRAVELS ALONG A LIMB
Radiating (vs radicular) pain is a very common clinical complaint
Often assumed to be radicularradicular pain pain “radiated along a dermatome of a nerve dueto inflammation or irriation of a nerve root”
But radiating pain is often not due to nerve irritation muddles theworkup
So sometimes radiating pain can be MSK
But many DO have radicular pain from pinching ofnerve roots…how to effectively find that ?
Let’s start with what we are looking at…
Let’s back up…what Do Normal Peripheral Nerves Do?3 Functions
1. Carry a signal to muscle to contract
2. Carry normal sensation, such as light touch for skin orposition of joints
3. Carry pain signals from non nerve tissues (skin, bone,joints, soft tissue). *This message does not mean thatthe nerve is injured or abnormal.
Such as, a fire alarm going off may mean the fire alarm is injured/malfunctioning(injured nerve), or…
that the fire alarm is working as designed to carry a message that there is a fire inthis case the fire alarm/NERVE is functioning normally.
Ordering an MRI as First Step
• BENEFITS• Time saver few clicks…“Smart” Set• Likely to be abnormal
confirmation bias• Pts are always worried about their
spine, want to know• Very sensitive test• Picture for the Instagram Age
• Drawbacks• High likelihood of normal
abnormalities• Often requires pre auth, denials• Much explanation needed in f/u
about disc bulges, foraminalstenosis on wrong side
• Often low specificity test
Exam?? We’re going somewhere,but it’s foggy and old fashioned….
Amish community outside of Champaign-Urbana, IL
Is the exam relevant today?
Sun setting on that way back when windmill thing…
MOTOR EXAMINATION
• Advantages• FEE Fast, Easy, Effective in clinic• QUICK much faster than even rapid CT• Can provide valuable info regarding the longest tracks
throughout the central and peripheral nervous system• Pattern recognition allows for rapid diagnosis
• Disadvantages• Relies on pt effort/level of alertness/cooperation• Relies on examiner’s interpretation of muscle force• Difficult to learn this on the web or in a book
it’s a learned motor skill, like riding a bike
Basic Principles of Muscle Force Testing 1
• Each muscle crosses a joint and causeschanges in that joint ROM with contraction
• Try to STABILIZE the joint the muscle crosseswhenever possible, to help isolate the muscleaction
Basic Principles of Muscle Force Testing 2
• Use your similar sized muscles only in hand muscles
• You will use your perception of the force you deliver and yourexperience of what is “normal” this is a learned motor skilland takes time to learn try to do a focused exam on pts withknown diagnoses so that you know what to expect
• In motor testing, the EXAMINER has the subjective sensationbeing judged c/w sensory where the PATIENT has thesubjective sensation
• In non hand muscles, use your additional muscles/bodyweight as needed this is not a force competition (i.e., I amstronger and therefore the pt is “weak” or vice versa)
Basic Principles of Muscle Force Testing 3
• Muscle Strength testing =• = Force (M x A)
• Measured in Pounds/Kilograms/Newtons• Not time dependent
• Work =• = Force x Distance• Units are joules
• Power =• = Work/time• Units are units of energy divided by time,• i.e watt = one joule/second
TORQUE !
• The tendency of a force to rotate an object about anaxis (aka joint in MST)
• Physics = Torque• Mechanical Engineering = Moment
Maximize d !!
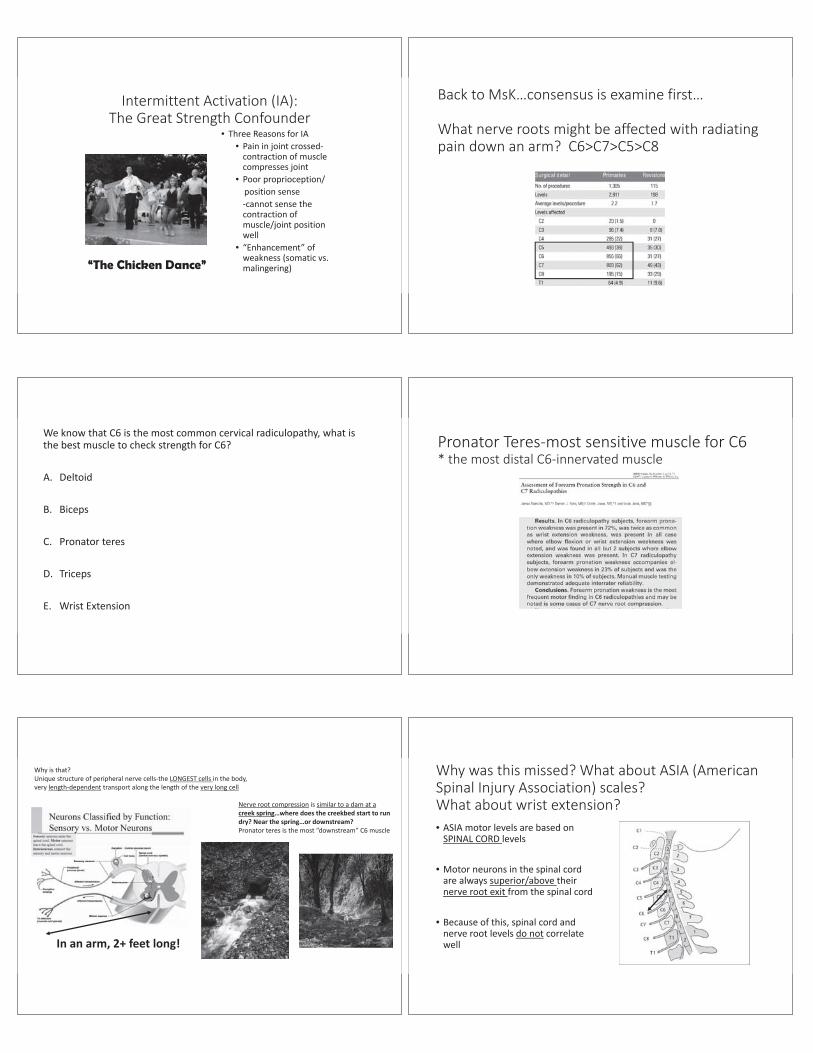
Basic Principles of Muscle Force Testing 4
• The score assigned to the muscle is the maximumforce generated at any point in time during thetesting of that muscle
• Rapid decreases in force do not represent weakness;rather, almost without exception they representvariability in lower motor neuron drive (exceptionsevere myasthenia)
• * Do not report the average when intermittentactivation occurs report the PEAK force
Score Peak force
0
10
20
30
40
50
60
70
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5
Forc
e in
lbs
Time in seconds
Score this
Another look at peak strength testing
Intermittent Activation (IA):The Great Strength Confounder
• Three Reasons for IA• Pain in joint crossed
contraction of musclecompresses joint
• Poor proprioception/position sensecannot sense the
contraction ofmuscle/joint positionwell
• “Enhancement” ofweakness (somatic vs.malingering)“The Chicken Dance”
Back to MsK…consensus is examine first…
What nerve roots might be affected with radiatingpain down an arm? C6>C7>C5>C8
We know that C6 is the most common cervical radiculopathy, what isthe best muscle to check strength for C6?
A. Deltoid
B. Biceps
C. Pronator teres
D. Triceps
E. Wrist Extension
Pronator Teres most sensitive muscle for C6* the most distal C6 innervated muscle
Why is that?Unique structure of peripheral nerve cells the LONGEST cells in the body,very length dependent transport along the length of the very long cell
Nerve root compression is similar to a dam at acreek spring…where does the creekbed start to rundry? Near the spring…or downstream?Pronator teres is the most “downstream” C6 muscle
In an arm, 2+ feet long!
Why was this missed? What about ASIA (AmericanSpinal Injury Association) scales?What about wrist extension?• ASIA motor levels are based on
SPINAL CORD levels
• Motor neurons in the spinal cordare always superior/above theirnerve root exit from the spinal cord
• Because of this, spinal cord andnerve root levels do not correlatewell
4 Muscle, Side to Side Comparison, C5 8 Screen
• Infraspinatus C5
• Pronator teres C6
• Extensor Digitorum Communis (EDC) C7
• Extensor Indicis Proprius (EIP) C8
IInfraspinatus force testing C5side to side immediate comparison (also upper motor neuron advantages)
Extends and laterally rotates the humerus
Pronator Teres most sensitive muscle for C6* the most distal C6 innervated muscle
PPronator teres C6
• Shake pts hand, ask themto keep the thumbDOWN
• Pts elbow must be fullyextended (if flexed testpronator quadratus)
• Weak in ~2/3 of C6 radics• check side to side• Bend your trunk sideways
prn for additional force
EEDC (Extensor digitorum communis)highly C7
• Have pt grasp knees with all fingers,then lift up the 2 middle fingers
• Minimal force muscle, like all fingerextensors
• Don’t push too hard too fastmarshmallow analogy
• Check force side to side
EExtensor indicis propius (EIP)radial nerve, highly C8
• Have pt grasp knees withall fingers, then lift up the2 index fingers
• Slight force muscle, likeall finger extensors(finger flexors muchstronger cause oftrigger fingers)
• Check force side to side• Great advantage of not
being involved in ulnarneuropathy or CTS
SENSORY EXAM
• “CAN YOU FEEL IT” IS A…
• A. Good question to ask during the usual sensory exam
• B. 1980 epic hit single/video by The Jacksons
• C. Poor question to ask a pt with an acute spinal cordinjury
• D. Album by the innovative 1980’s Australian band,Hunters and Collectors (best known for their single,“Throw Your Arms Around Me”)
CAN YOU FEEL IT
Which circle is darker gray? PAUSE
Which of those 2 previous ovals was darkerthe 1st or 2nd?
A. FirstB. Second
DST double simultaneous testing DST double simultaneous testing
• Use to test• Distal to proximal gradients for length dependent
neuropathy.Light touch is best subserved by both systems
• Side to side distal dermatomes for radiculopathy
• Different peripheral nerve distributions for focalneuropathies
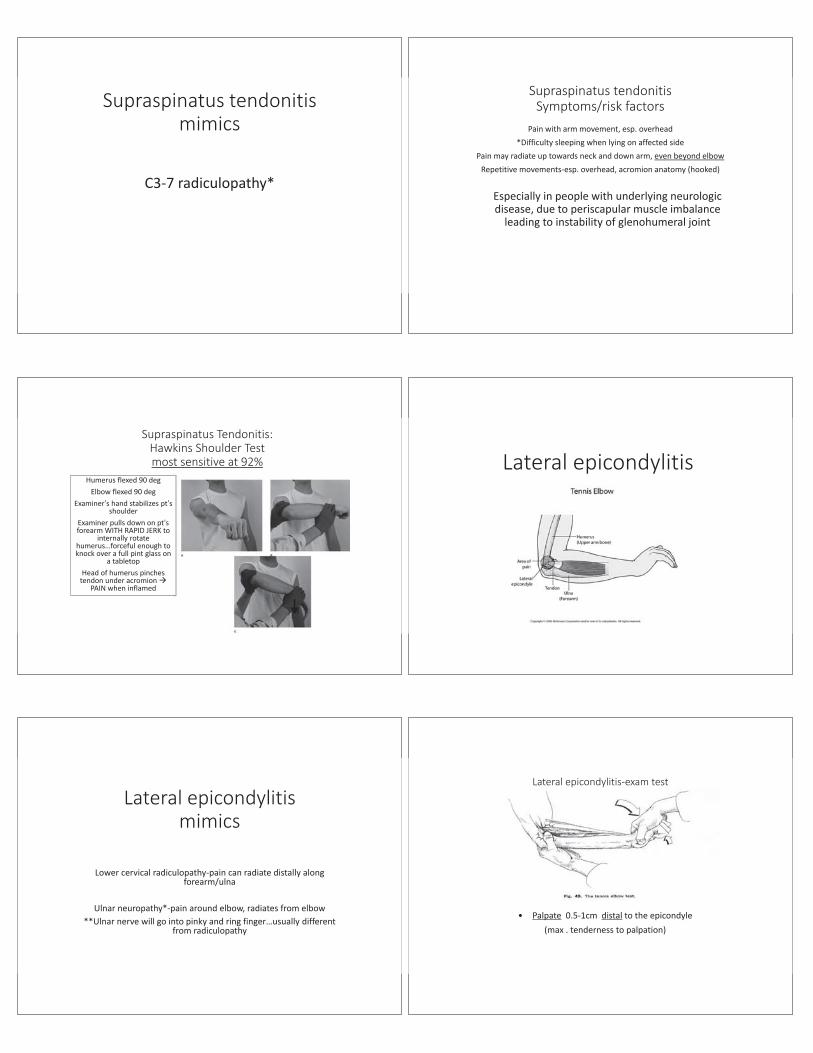
Side to side distal aspect of dermatomes forradiculopathy
Simultaneously touchBack of Left and Right hand
Thumb C6
Middle Finger C7
Pinky C8
10 sec
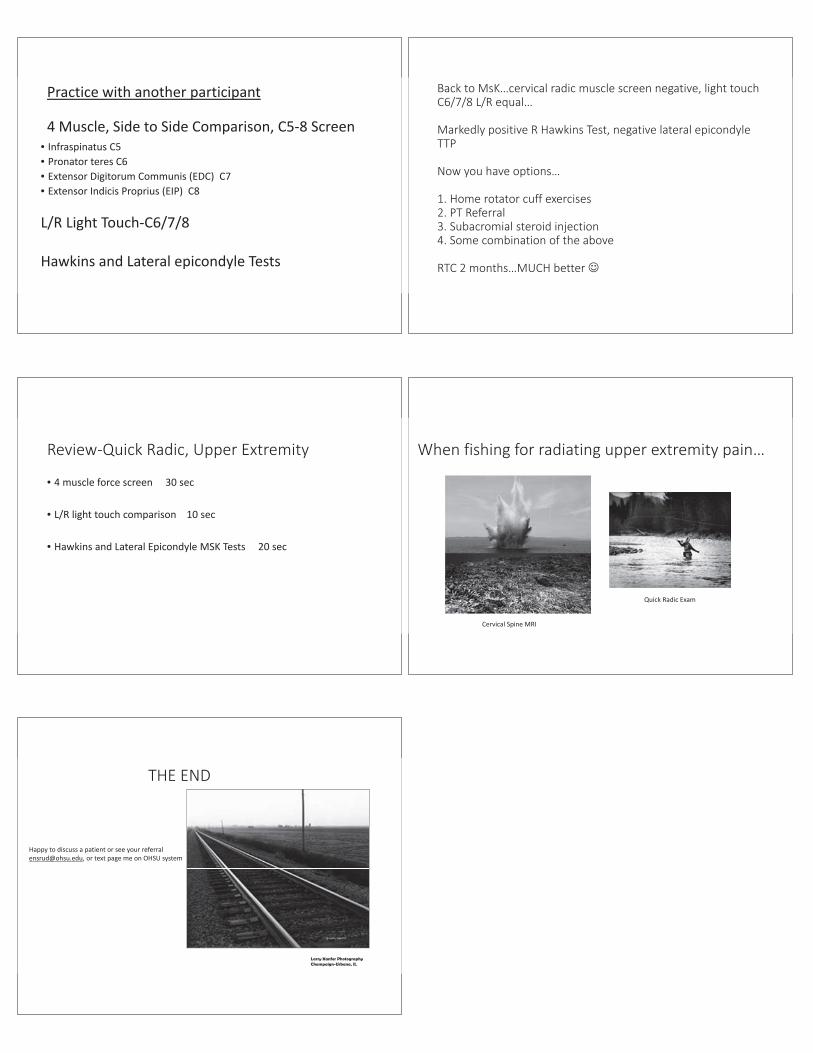
Different peripheral nerve distributions for focalneuropathies
Ulnar
Median
vs
Back to MsK…cervical radic muscle screennegative…
What else might be affected with radiating paindown an arm?
MSK Mimic definition
A musculoskeletal condition that presents with pain ordiscomfort suggestive of a nerve injury/neuropathic etiology

Reasons to care about MSK Mimics
Common causes of limb pain
Frequent reason for clinic referral
Pts may have radiculopathy AND mimics
Your extremity skeleton and spinal nerve roots don’t coordinate their painlike your 2 kids crying at the same time about 2 different things
”Pain in limb ? radiculopathy, ? CTS”
Treatable conditions
Musculoskeletal Exam Tests:Advantages
FAST/EASY/EFFECTIVEAbility to diagnose quickly at bedside or exam room with
appropriate physical exam
Timesavers for the Provider…keep up your clinic flow
Fewer unnecessary MRIs ordered with time consuming followup
Musculoskeletal Exam Tests:Pearls
Check bilateral limbs for side to side comparison: non involvedside first when possible
Ask, “Is that the same pain you have been experiencing?”
* Patients can have more than one condition i.e. radiculopathyand rotator cuff tendinitis
Musculoskeletal Exam Tests Pearls:Wince sign
Look for the “Wince” sign forpositive test
•Eye blink/face grimace•Not just mild discomfort
When doing an MSK test,Watch their eyes
2 High Yield MSK Mimic Tests forRadiating/? Radic Exam
• Hawkins Sign
• Lateral epicondyle tenderness
Supraspinatus/Rotator Cuff Tendonitis
Supraspinatus tendonitismimics
C3 7 radiculopathy*
Supraspinatus tendonitisSymptoms/risk factors
Pain with arm movement, esp. overhead*Difficulty sleeping when lying on affected side
Pain may radiate up towards neck and down arm, even beyond elbowRepetitive movements esp. overhead, acromion anatomy (hooked)
Especially in people with underlying neurologicdisease, due to periscapular muscle imbalance
leading to instability of glenohumeral joint
Supraspinatus Tendonitis:Hawkins Shoulder Testmost sensitive at 92%
Humerus flexed 90 degElbow flexed 90 deg
Examiner’s hand stabilizes pt’sshoulder
Examiner pulls down on pt’sforearm WITH RAPID JERK to
internally rotatehumerus…forceful enough toknock over a full pint glass on
a tabletopHead of humerus pinches
tendon under acromionPAIN when inflamed
Lateral epicondylitis
Lateral epicondylitismimics
Lower cervical radiculopathy pain can radiate distally alongforearm/ulna
Ulnar neuropathy* pain around elbow, radiates from elbow**Ulnar nerve will go into pinky and ring finger…usually different
from radiculopathy
Lateral epicondylitis exam test
• Palpate 0.5 1cm distal to the epicondyle(max . tenderness to palpation)
Practice with another participant
4 Muscle, Side to Side Comparison, C5 8 Screen• Infraspinatus C5• Pronator teres C6• Extensor Digitorum Communis (EDC) C7• Extensor Indicis Proprius (EIP) C8
L/R Light Touch C6/7/8
Hawkins and Lateral epicondyle Tests
Back to MsK…cervical radic muscle screen negative, light touchC6/7/8 L/R equal…
Markedly positive R Hawkins Test, negative lateral epicondyleTTP
Now you have options…
1. Home rotator cuff exercises2. PT Referral3. Subacromial steroid injection4. Some combination of the above
RTC 2 months…MUCH better
Review Quick Radic, Upper Extremity
• 4 muscle force screen 30 sec
• L/R light touch comparison 10 sec
• Hawkins and Lateral Epicondyle MSK Tests 20 sec
When fishing for radiating upper extremity pain…
Cervical Spine MRI
Quick Radic Exam
THE END
Larry Kanfer PhotographyChampaign-Urbana, IL
Happy to discuss a patient or see your [email protected], or text page me on OHSU system
Osteoporosis in Spinal Surgery
Clifford Lin, MDAssistant Professor
Department of Orthopaedics and RehabilitationOregon Health & Science University
OutlineDefinitions
Bone metabolism
Epidemiology
Classification
Presentation
Diagnosis
Management
Techniques in Spinal Fixation
Osteoporosis
Age-related decrease in bone mass secondary to unbalanced bonemetabolism characterized by:
Microarchitectural deterioration of bone tissue
Skeletal fragility
Increased risk of fracture
Bone Metabolism
Osteoblasts
Mononucleated cells
Osteoblasts
Mononucleated cells
Synthesize unmineralized bone matrix Type 1 Collagen
Proteoglycans
Osteoblasts
Mononucleated cells
Synthesize unmineralized bone matrixType 1 Collagen
Proteoglycans
Synthesize bone mineralHydroxyapatite
Deposited into Type 1 collagen
Osteoblasts
Mononucleated cells
Synthesize unmineralized bone matrix Type 1 Collagen
Proteoglycans
Synthesize bone mineralHydroxyapatite
Deposited into Type 1 collagen
Osteoblasts embedded in the matrix become osteocytes
Maintain the bone matrix
Osteoblasts
Mononucleated cells
Synthesize unmineralized bone matrixType 1 Collagen
Proteoglycans
Synthesize bone mineralHydroxyapatite
Deposited into Type 1 collagen
Osteoblasts embedded in the matrix become osteocytes
Maintain the bone matrix
Blastic phase takes 80 days
Bone Metabolism
Osteoclasts
Multinucleated cells
Bind to bone integrins to form resorption cavity (Howship lacuna)
Creates acidic microenvironment that dissolves hydroxyapatite mineral
Clastic phase takes 20 days
Regulation of Bone Metabolism
PTHSecreted in response to ionized calcium
Increases reabsorption of calcium in kidneys Activates Vitamin DStimulates bone resorption by osteoclasts
Vitamin DIncreases absorption of calcium from GI
CalcitoninInhibits osteoclast activity and favors storage of calcium in bone
Gonadal hormonesStimulate osteoblast proliferation and synthesis of bone
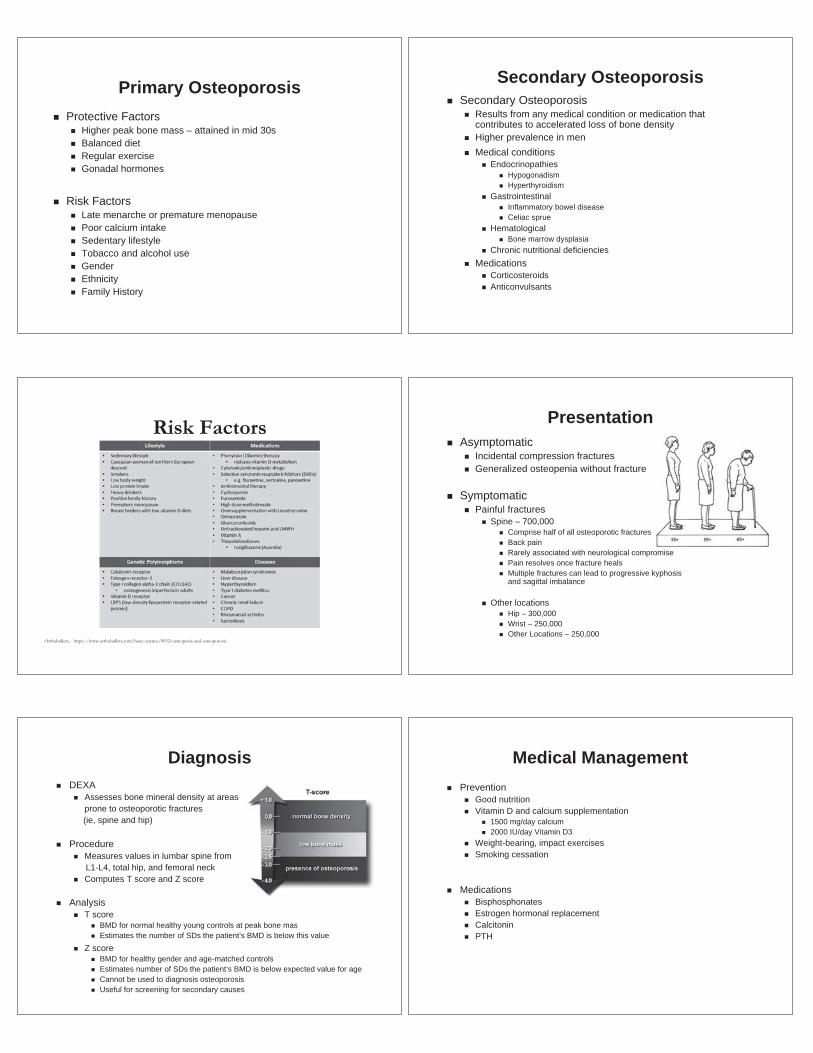
EpidemiologyThe Recent Prevalence of Osteoporosis and Low Bone Mass in the United States Based on Bone
Mineral Density at the Femoral Neck or Lumbar Spine
Journal of Bone and Mineral ResearchVolume 29, Issue 11, pages 2520-2526, 20 OCT 2014 DOI: 10.1002/jbmr.2269http://onlinelibrary.wiley.com/doi/10.1002/jbmr.2269/full#jbmr2269-fig-0001
Perc
enta
ge o
f ad
ults
ove
r age
50
EpidemiologyThe Prevalence of Osteoporosis and Low Bone Mass in the United States Based on Bone Mineral
Density among Men and Women
Bone Health and Osteoporosis: A Report of the Surgeon General.Office of the Surgeon General (US).Rockville (MD): Office of the Surgeon General (US); 2004.
EpidemiologyMean Bone Mineral Density among Men and Women by Age and Ethnicity
Bone Health and Osteoporosis: A Report of the Surgeon General.Office of the Surgeon General (US).Rockville (MD): Office of the Surgeon General (US); 2004.
Economic Impact
Bone Health and Osteoporosis: A Report of the Surgeon General.Office of the Surgeon General (US).Rockville (MD): Office of the Surgeon General (US); 2004.
2002 Annual Direct Care Expenditures (Hospital and Nursing Home Care)
$17 billion dollars $47 million dollars daily7% of all healthcare costs among women 45 and older
2030 Estimates$60 billion dollars$154 million dollars daily
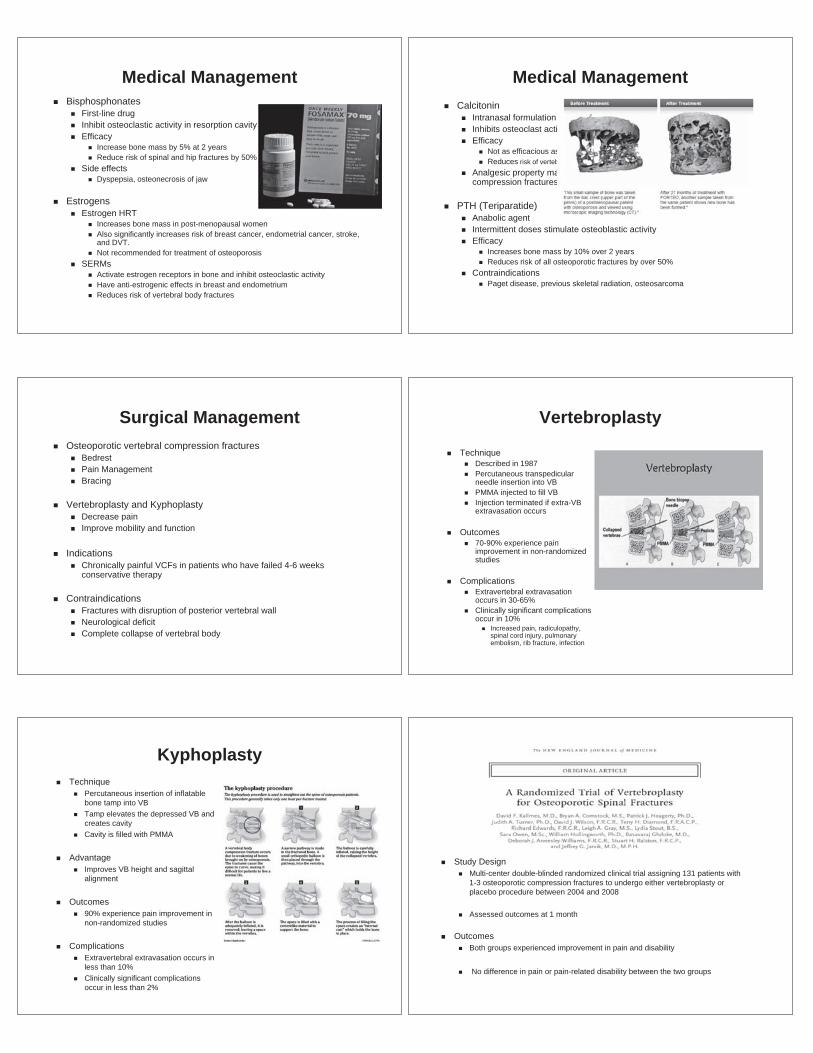
Economic Impact ClassificationPrimary Osteoporosis
Occurs as a result of aging
Slow phaseOccurs in both men and womenDue to impaired Vitamin D metabolism by kidneysBone mass decreases at rate of 0.3% -0.5% per year
Accelerated phaseOccurs only in post-menopausal womenDue to loss of estrogen and increased bone resorptionBone mass decreases at rate of 2% -3% per yearLasts ~5 years
Primary OsteoporosisProtective Factors
Higher peak bone mass – attained in mid 30sBalanced dietRegular exerciseGonadal hormones
Risk FactorsLate menarche or premature menopausePoor calcium intakeSedentary lifestyleTobacco and alcohol useGenderEthnicityFamily History
Secondary OsteoporosisSecondary Osteoporosis
Results from any medical condition or medication that contributes to accelerated loss of bone densityHigher prevalence in menMedical conditions
EndocrinopathiesHypogonadismHyperthyroidism
GastrointestinalInflammatory bowel diseaseCeliac sprue
HematologicalBone marrow dysplasia
Chronic nutritional deficienciesMedications
CorticosteroidsAnticonvulsants
Risk Factors
Orthobullets, - https://www.orthobullets.com/basic-science/9032/osteopenia-and-osteoporosis
PresentationAsymptomatic
Incidental compression fracturesGeneralized osteopenia without fracture
SymptomaticPainful fractures
Spine – 700,000Comprise half of all osteoporotic fracturesBack painRarely associated with neurological compromisePain resolves once fracture healsMultiple fractures can lead to progressive kyphosis and sagittal imbalance
Other locationsHip – 300,000Wrist – 250,000Other Locations – 250,000
DiagnosisDEXA
Assesses bone mineral density at areasprone to osteoporotic fractures (ie, spine and hip)
ProcedureMeasures values in lumbar spine fromL1-L4, total hip, and femoral neckComputes T score and Z score
AnalysisT score
BMD for normal healthy young controls at peak bone masEstimates the number of SDs the patient’s BMD is below this value
Z scoreBMD for healthy gender and age-matched controlsEstimates number of SDs the patient’s BMD is below expected value for ageCannot be used to diagnosis osteoporosisUseful for screening for secondary causes
Medical ManagementPrevention
Good nutritionVitamin D and calcium supplementation
1500 mg/day calcium2000 IU/day Vitamin D3
Weight-bearing, impact exercisesSmoking cessation
MedicationsBisphosphonatesEstrogen hormonal replacementCalcitoninPTH
Medical ManagementBisphosphonates
First-line drugInhibit osteoclastic activity in resorption cavityEfficacy
Increase bone mass by 5% at 2 yearsReduce risk of spinal and hip fractures by 50%
Side effectsDyspepsia, osteonecrosis of jaw
EstrogensEstrogen HRT
Increases bone mass in post-menopausal womenAlso significantly increases risk of breast cancer, endometrial cancer, stroke, and DVT.Not recommended for treatment of osteoporosis
SERMsActivate estrogen receptors in bone and inhibit osteoclastic activityHave anti-estrogenic effects in breast and endometriumReduces risk of vertebral body fractures
Medical ManagementCalcitonin
Intranasal formulationInhibits osteoclast activityEfficacy
Not as efficacious as other agents in increasing BMDReduces risk of vertebral body fractures
Analgesic property makes it useful in treating painful vertebral compression fractures
PTH (Teriparatide)Anabolic agent Intermittent doses stimulate osteoblastic activityEfficacy
Increases bone mass by 10% over 2 yearsReduces risk of all osteoporotic fractures by over 50%
ContraindicationsPaget disease, previous skeletal radiation, osteosarcoma
Surgical ManagementOsteoporotic vertebral compression fractures
BedrestPain ManagementBracing
Vertebroplasty and KyphoplastyDecrease painImprove mobility and function
IndicationsChronically painful VCFs in patients who have failed 4-6 weeks conservative therapy
ContraindicationsFractures with disruption of posterior vertebral wallNeurological deficitComplete collapse of vertebral body
Vertebroplasty
TechniqueDescribed in 1987Percutaneous transpedicular needle insertion into VBPMMA injected to fill VBInjection terminated if extra-VB extravasation occurs
Outcomes70-90% experience pain improvement in non-randomized studies
ComplicationsExtravertebral extravasation occurs in 30-65%Clinically significant complications occur in 10%
Increased pain, radiculopathy, spinal cord injury, pulmonary embolism, rib fracture, infection
KyphoplastyTechnique
Percutaneous insertion of inflatable bone tamp into VBTamp elevates the depressed VB and creates cavityCavity is filled with PMMA
AdvantageImproves VB height and sagittal alignment
Outcomes90% experience pain improvement in non-randomized studies
ComplicationsExtravertebral extravasation occurs in less than 10%Clinically significant complications occur in less than 2%
Study DesignMulti-center double-blinded randomized clinical trial assigning 131 patients with 1-3 osteoporotic compression fractures to undergo either vertebroplasty or placebo procedure between 2004 and 2008
Assessed outcomes at 1 month
OutcomesBoth groups experienced improvement in pain and disability
No difference in pain or pain-related disability between the two groups
Study DesignMulti-center double-blinded randomized clinical trial assigning 78 patients with 1-2 osteoporotic fractures to undergo either vertebroplasty or placebo procedure between 2004 and 2008
Assessed outcomes at 1 week, 1 month, 3 months, and 6 months
OutcomesBoth groups experienced improvement in pain, physical function, quality of life
No benefit of vertebroplasty over placebo
Osteoporosis and Spinal Fusion
MethodsIdentified 2293 patients with adult spinal deformity undergoing thoracolumbar fusion > 8 levels
Multivariate analysis of risk factors for revision surgery at 1 and 5 years
Results44% of patients had osteoporosis
10.5% revision rate at 1 year and 18.5% revision rate at 5 years
Osteoporosis significantly associated with revision surgery in univariate analysis at 1, 2, 3, 4, and 5 years
Osteoporosis was significantly associated with revision surgery in multivariate analysis at 5 years
Osteoporosis and Spinal FixationStrategies
Screw Placement
Screw Augmentation with Hooks
Screw Augmentation with Cement
Multiple Points of Fixation
Expandable Screws
Screw PlacementIncrease Screw Length
Greater pullout strength
Increase Screw DiameterGreater pullout strength
Bicortical screws30% greater pullout strength
CementPMMA bone cement
Can be injected into the pedicle around the screw
Increases screw pullout strength by three-fold
Risks Extraosseous extravasation
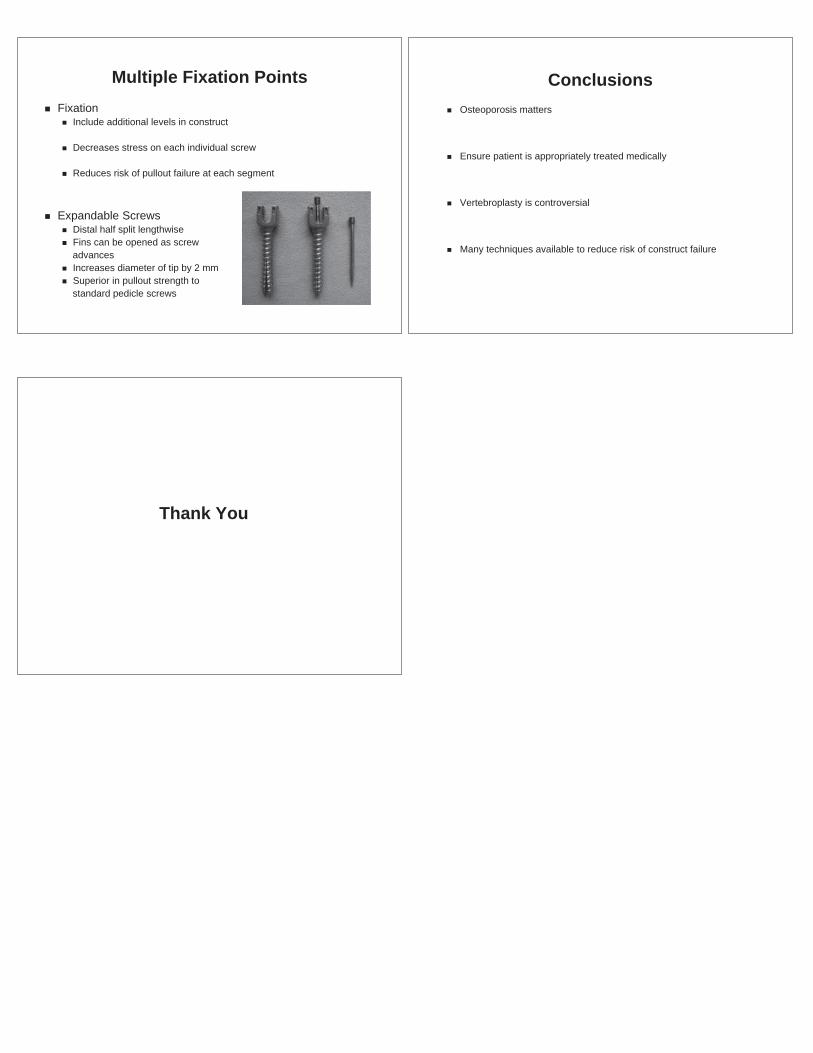
Multiple Fixation PointsFixation
Include additional levels in construct
Decreases stress on each individual screw
Reduces risk of pullout failure at each segment
Expandable ScrewsDistal half split lengthwiseFins can be opened as screwadvancesIncreases diameter of tip by 2 mmSuperior in pullout strength tostandard pedicle screws
ConclusionsOsteoporosis matters
Ensure patient is appropriately treated medically
Vertebroplasty is controversial
Many techniques available to reduce risk of construct failure
Thank You
OHSU Musculoskeletal Update
Scoliosis
Matthew F. Halsey, M.D.Doernbecher Children’s Hospital
OHSU
6 Sep 2019 OHSU Musculoskeletal Update
Scoliosis
Definition:An abnormal curvature
of the spine in all three planes resulting in deformity, pain and functional impairment
6 Sep 2019
OHSU Musculoskeletal Update
Definition
• Coronal plane– Evaluated on P/A
radiographs– Measured by Cobb
angle– Must measure >10°
6 Sep 2019
verywellhealth.com
OHSU Musculoskeletal Update
Definition
• Sagittal plane– Evaluated on lateral
radiograph– Usually characterized by
flattening of thoracickyphosis andaccentuation of lumbarlordosis
6 Sep 2019
jcvjs.com
OHSU Musculoskeletal Update
Definition
• Transverse plane– Evaluated on physical exam– Adam’s forward bending
test– Characterized by rib and/or
lumbar prominences• Measured with a scoliometer
– Posterior prominence islocated on the convex side ofthe curve
6 Sep 2019 OHSU Musculoskeletal Update
Incidence
• Idiopathic– 4.5%– Gender ratio is 1.25:1::female:male– For curves >20° ratio is 5.4:1– Treatment required 2.75/1000– 1/20 progress to possible bracing– 1/25 progress to possible surgery
– Rogala EJ, et al. JBJS 60A:173, 1978
6 Sep 2019
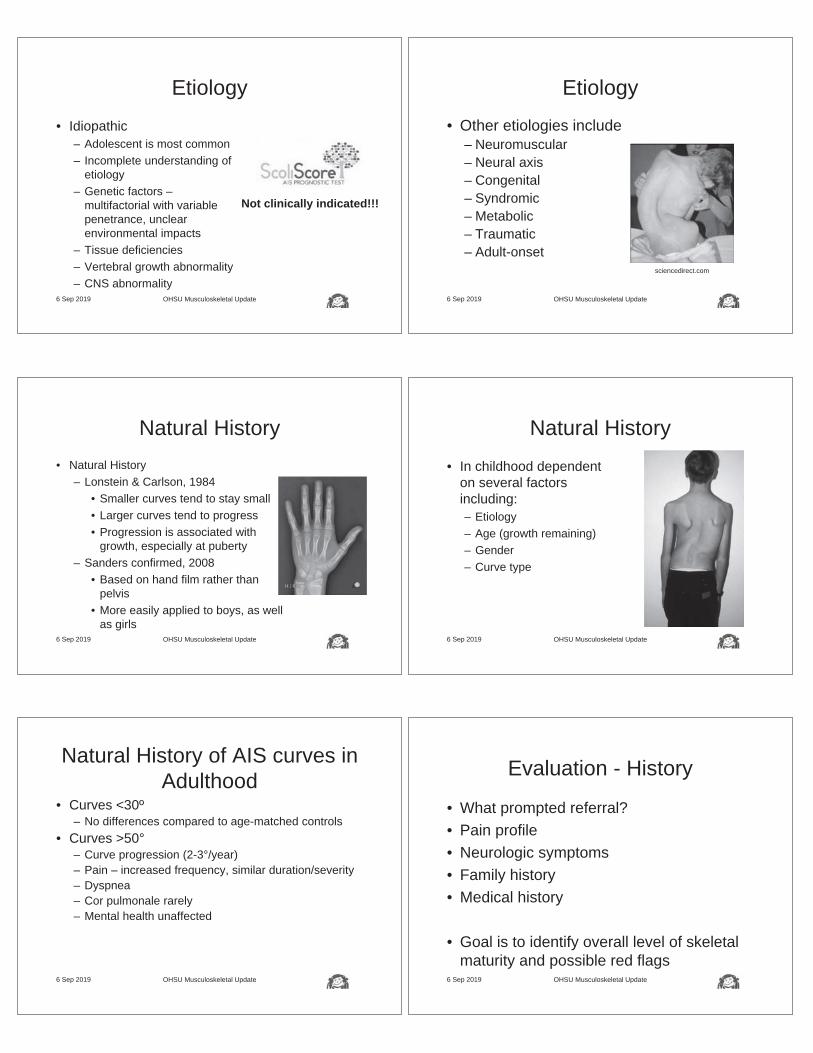
Etiology
• Idiopathic– Adolescent is most common– Incomplete understanding of
etiology– Genetic factors –
multifactorial with variable penetrance, unclear environmental impacts
– Tissue deficiencies– Vertebral growth abnormality– CNS abnormality
6 Sep 2019 OHSU Musculoskeletal Update
Not clinically indicated!!!
OHSU Musculoskeletal Update
Etiology
• Other etiologies include– Neuromuscular– Neural axis– Congenital– Syndromic– Metabolic– Traumatic– Adult-onset
6 Sep 2019
sciencedirect.com
Natural History• Natural History
– Lonstein & Carlson, 1984• Smaller curves tend to stay small• Larger curves tend to progress• Progression is associated with
growth, especially at puberty– Sanders confirmed, 2008
• Based on hand film rather than pelvis
• More easily applied to boys, as well as girls
OHSU Musculoskeletal Update6 Sep 2019 OHSU Musculoskeletal Update
Natural History
• In childhood dependent on several factors including:– Etiology– Age (growth remaining)– Gender– Curve type
6 Sep 2019
Natural History of AIS curves in Adulthood
• Curves <30º– No differences compared to age-matched controls
• Curves >50°– Curve progression (2-3°/year)– Pain – increased frequency, similar duration/severity– Dyspnea– Cor pulmonale rarely – Mental health unaffected
6 Sep 2019 OHSU Musculoskeletal Update OHSU Musculoskeletal Update
Evaluation - History
• What prompted referral?• Pain profile• Neurologic symptoms• Family history• Medical history
• Goal is to identify overall level of skeletal maturity and possible red flags
6 Sep 2019
Red Flags in the History
• Night pain, especially if easily relieved by NSAIDs– Osteoid osteoma, osteoblastoma, aneurysmal
bone cyst, giant cell tumor• Neurologic deficit
– Spinal cord tumor, tethered cord• Either of these findings should prompt
MRI evaluation
6 Sep 2019 OHSU Musculoskeletal Update OHSU Musculoskeletal Update
Physical Examination
• Height, Weight, Proportions• Skin exam• Normal neuromuscular exam
– Strength– Sensation– Deep tendon reflexes– Clonus– Babinski– Abdominal reflex
6 Sep 2019
youtube.com
OHSU Musculoskeletal Update
Physical Examination
• Back– Shoulders– Flanks– Pelvis - limb length
discrepancy– Sagittal– Forward bend test– Flexibility – posture
• Use a robe and paper shorts for this exam
6 Sep 2019 OHSU Musculoskeletal Update
Physical Examination
• Standing position
• Forward bending position
• Scoliometer
6 Sep 2019
Red Flags in Physical Examination
• Neurologic deficits or asymmetries – Suggests neural axis disorder (MRI)
• Café au lait spots– Suggests neurofibromatosis (MRI)
• Leg length discrepancy– Perhaps not a structural (true) scoliosis (leg
length x-ray)
6 Sep 2019 OHSU Musculoskeletal Update OHSU Musculoskeletal Update
Radiologic Examination
• Scoliosis Screen– Standing PA entire spine
– Standing lateral entire spine
– Cobb method
– Risser sign
– Left-hand film
6 Sep 2019
Radiologic Examination
• EOS imaging– Lower radiation dose– May allow concurrent
hand imaging
6 Sep 2019 OHSU Musculoskeletal Update OHSU Musculoskeletal Update
Radiologic Examination
• MRI– Suspicion of neural axis abnormality
• Left thoracic curve• Babinski/clonus• Asymmetric abdominal reflex
6 Sep 2019
Goals of Treatment• Potential Goals
– Maintain straight spine and normal figure– Avoid pain– Avoid activity limitations– Avoid surgery– Avoid pulmonary limitations– Have a normal life; not be disabled– Not waste time or treasure
OHSU Musculoskeletal Update6 Sep 2019
Goals of Treatment
• Whose goals do we address?– Patients– Families– Primary care providers– Therapists– Surgeons– Hospital administrators– Insurance payors– Government policy makers
OHSU Musculoskeletal Update6 Sep 2019
Choices
• Typical treatments– Surgery– Observation– Bracing– Physiotherapeutic
scoliosis specific exercises (PSSE), e.g. the Schroth method
• Atypical treatments– Typical physical
therapy– Muscle stimulation– Chiropractic– Acupuncture
OHSU Musculoskeletal Update6 Sep 2019
Surgery• Option of last resort• Powerful tool with significant risks• Main goals
– Prevent progression of curve– Correction of deformity– Secondary prevention of problems associated with
worsening of curve (pain, restrictive lung disease)• Typical indication: Cobb > 50º
OHSU Musculoskeletal Update6 Sep 2019
Surgery
6 Sep 2019 OHSU Musculoskeletal Update
srs.org
Surgery
• Challenges– Surgical risks including:
• Neurologic injury• Infection• Mal-positioned hardware
– Long-term problems• Curve progression• Pain• Degenerative disk disease
– 10% reoperation rate for all reasons
OHSU Musculoskeletal Update6 Sep 2019
Observation
• Benefits of observation– Low cost in terms of time and treasure– No risks associated with treatment– Less anxiety (usually)
• Challenges– Predicting natural history is imperfect– Curve size and maturity level (age) are inadequate to
predict outcome– Identify other curve parameters (EOS 3D analysis)
OHSU Musculoskeletal Update6 Sep 2019
Bracing
• Alternative to casting• Well-established “industry”
– Orthotists in most communities– Standardized techniques and
approaches
OHSU Musculoskeletal Update6 Sep 2019
Bracing
• Demonstrated efficacy in high-level prospective multi-center study (BrAIST)– Weinstein & Dolan, 2013, New England
Journal of Medicine– Bracing works!!!– So many more questions are raised though!
OHSU Musculoskeletal Update6 Sep 2019
Bracing
• Challenges– Patient compliance – monitoring?– How many hours each day?– Plethora of choices
• Day v night; soft v hard; Boston v Rigo-Cheneau
– Quality control – correction in brace• Stiff curve v inadequate brace mold; does it matter?
– When to start?– When to stop?– How to reduce number needed to treat (NNT=3)
OHSU Musculoskeletal Update6 Sep 2019
Physiotherapeutic Scoliosis Specific Exercises
• Initial development in 1920s
• Alternative to casting and fusion surgeries
• Promoted in European centers for decades
• Over the last decade has gained a foothold in North America
OHSU Musculoskeletal Update6 Sep 2019
Physiotherapeutic Scoliosis Specific Exercises
• Potential benefits– Prevent progression– Improve deformity (curve
correction)!?– Maintain figure and overall
appearance
OHSU Musculoskeletal Update6 Sep 2019
Physiotherapeutic Scoliosis Specific Exercises
• Challenges– Data are more limited
• Are results generalizable?• Are results persistent and/or sustainable?
– Infrastructure• Limited number of trained therapists• What patient and therapist commitment is
required?– Insurance does not always cover this therapy
OHSU Musculoskeletal Update6 Sep 2019
Standard Physical Therapy
• Potential– Common method
• Well-promulgated• Easily taught and communicated• Easy maintenance
– Very helpful to limit pain that may be associated with AIS (Zapata et al, 2015)
OHSU Musculoskeletal Update6 Sep 2019
Standard Physical Therapy
• Challenges– Little impact on natural history– Pain not always completely relieved
OHSU Musculoskeletal Update6 Sep 2019
Lateral Electrical Surface Stimulation
• Developed by Axelgaard in 1976– Nighttime application of
electrodes on lateral convexity of spine
– Potential replacement of bracing
– Supportive articles through the 1980s
OHSU Musculoskeletal Update6 Sep 2019
Lateral Electrical Surface Stimulation
• Challenges– A subsequent study found results equal to
natural history (Nachemson, 1995). SRS-funded, prospective study
• Bracing success 74% (95% CI=52-84%)• LESS success 33% (12-60%)• Natural history success 34% (16-49%)
• Abandoned treatment modalityOHSU Musculoskeletal Update6 Sep 2019
Chiropractic Manipulation• Potential
– Limit progression of scoliosis without surgery
– Decrease pain associated with scoliosis
• Challenges– Lack of data (Romano & Negrini,
2008)– Emphasis on early diagnosis and
treatment (? NNT elevated)– Lack of anatomic basis of treatment
OHSU Musculoskeletal Update6 Sep 2019
Acupuncture
• Few studies available to analyze– Weiss et al, 2008
• Brief exploratory study• No follow-up data to this point
OHSU Musculoskeletal Update6 Sep 2019
Synopsis
• Scientific understanding of scoliosis remains elusive
• Natural history is not without consequence and remains difficult to predict
• Treatments are imperfect and flawed• Goals for patients/parents, providers, and
payors are frequently disparate and incongruent
OHSU Musculoskeletal Update6 Sep 2019
Challenges
• Identify the etiology
• Improve our prediction models
• Evaluate rigorously our treatment methods
• Increase value
OHSU Musculoskeletal Update6 Sep 2019 OHSU Musculoskeletal Update
Thanks!
6 Sep 2019
NAME THAT GROAN! NAME THAT GROAN!Hans Carlson, MDAssociate Professor Physical Medicine & RehabilitationOHSU
NAME THAT GROAN!Using our clinical skills to
make the diagnosis
The prepared mind…
Where does it hurt?
What’s there that can hurt?
Musculoskeletal Injuries
TendonsMusclesLigamentsJointsBursaNervesReferred Pain
Know the patterns!
History - “Red Flags”
TraumaFeverWeight LossNight/Rest PainHistory of CancerRecurrent Pain or Failure to ImproveBowel or Bladder DysfunctionSensory or Motor DeficitsLeg > Back Pain
NAME THAT GROAN!
Name that Groan!
• Rules• Cases will be presented…
• Slowly• Contestants may write their diagnosis at any time.• Hold card up when done
• Briefly explain your thought process• One attempt per contestant/case• Correct answer will be given at the end
• The contestants with the earliest correct answer wins
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• 50 year old male• Chronic LBP of 25 years duration• Remote left sciatica/foot drop• Increased pain with walking/standing
• No prior surgery/hospitalization• No bowel or bladder dysfunction
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• No recent spine imaging for 9 years• History of degenerative changes
• Otherwise healthy
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Decreased spine ROM with mild low back pain, no leg pain
• Normal, symmetric LE reflexes• No clonus or Babinski• Decreased sensation left foot• Normal motor bilateral legs• Normal gait with decreased cadence
• Negative straight leg raise• Decreased ROM
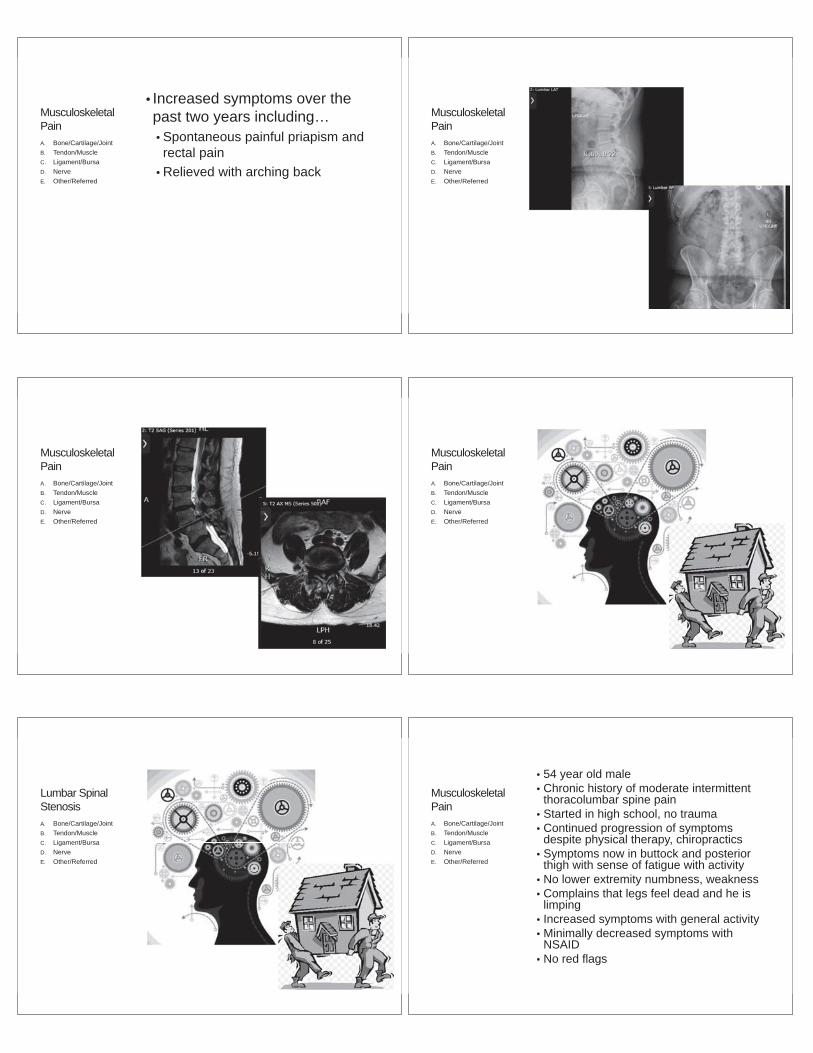
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Increased symptoms over the past two years including…• Spontaneous painful priapism and rectal pain
• Relieved with arching back
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
Lumbar Spinal StenosisA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPain
• 54 year old male• Chronic history of moderate intermittent
thoracolumbar spine pain• Started in high school, no trauma• Continued progression of symptoms
despite physical therapy, chiropractics• Symptoms now in buttock and posterior
thigh with sense of fatigue with activity• No lower extremity numbness, weakness• Complains that legs feel dead and he is
limping• Increased symptoms with general activity• Minimally decreased symptoms with
NSAID• No red flags
A. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
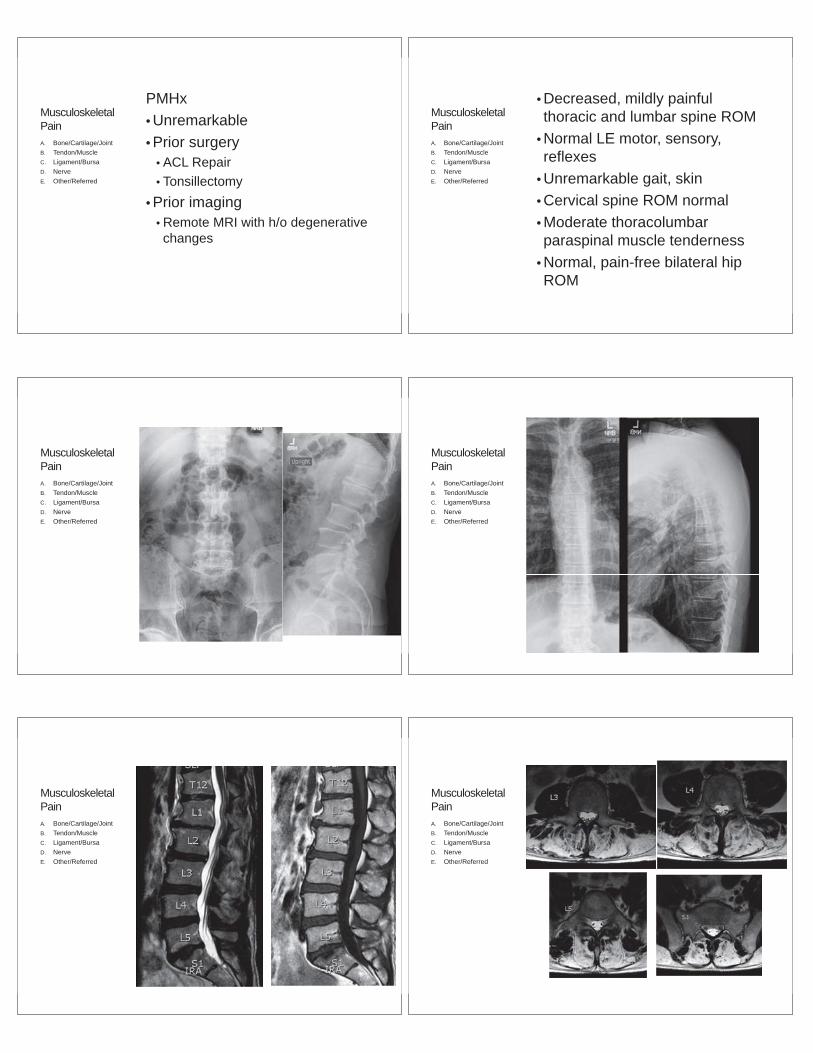
MusculoskeletalPain
PMHx• Unremarkable• Prior surgery
• ACL Repair• Tonsillectomy
• Prior imaging• Remote MRI with h/o degenerative changes
A. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPain
• Decreased, mildly painful thoracic and lumbar spine ROM
• Normal LE motor, sensory, reflexes
• Unremarkable gait, skin• Cervical spine ROM normal• Moderate thoracolumbar paraspinal muscle tenderness
• Normal, pain-free bilateral hip ROM
A. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
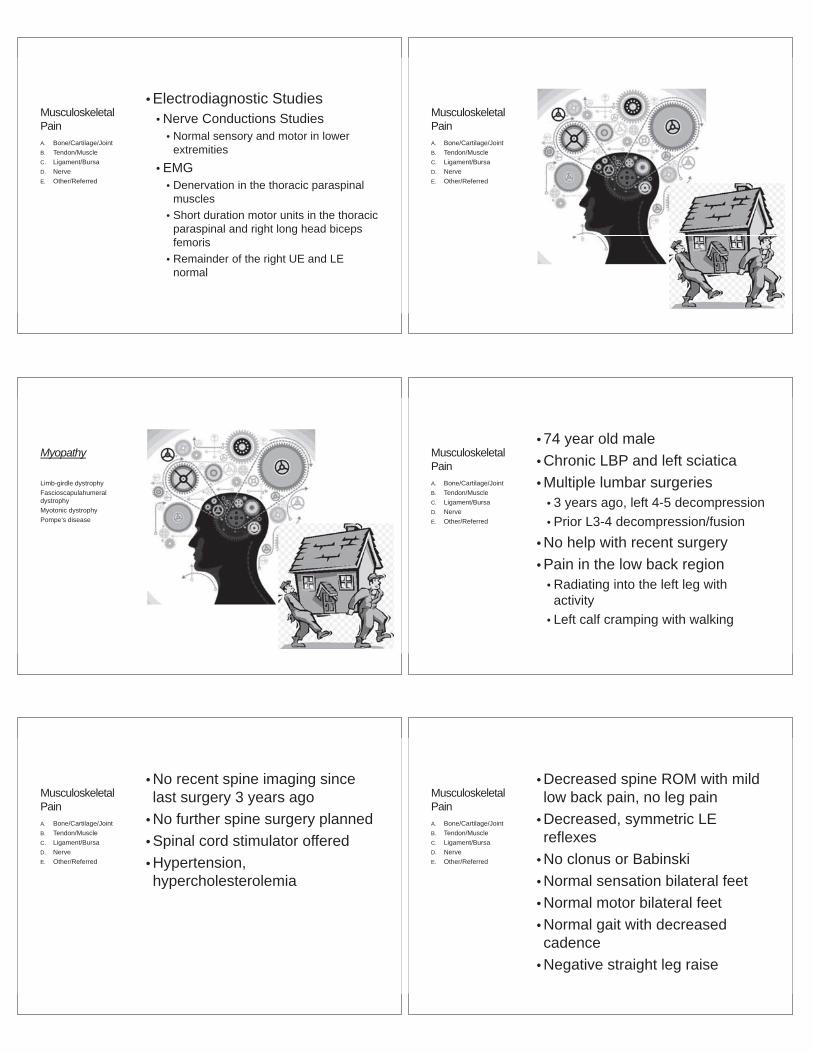
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Electrodiagnostic Studies• Nerve Conductions Studies
• Normal sensory and motor in lower extremities
• EMG• Denervation in the thoracic paraspinal
muscles• Short duration motor units in the thoracic
paraspinal and right long head biceps femoris
• Remainder of the right UE and LE normal
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
Myopathy
Limb-girdle dystrophyFascioscapulahumeraldystrophyMyotonic dystrophyPompe’s disease
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• 74 year old male• Chronic LBP and left sciatica• Multiple lumbar surgeries
• 3 years ago, left 4-5 decompression• Prior L3-4 decompression/fusion
• No help with recent surgery• Pain in the low back region
• Radiating into the left leg with activity
• Left calf cramping with walking
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• No recent spine imaging since last surgery 3 years ago
• No further spine surgery planned• Spinal cord stimulator offered• Hypertension,hypercholesterolemia
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Decreased spine ROM with mild low back pain, no leg pain
• Decreased, symmetric LE reflexes
• No clonus or Babinski• Normal sensation bilateral feet• Normal motor bilateral feet• Normal gait with decreased cadence
• Negative straight leg raise
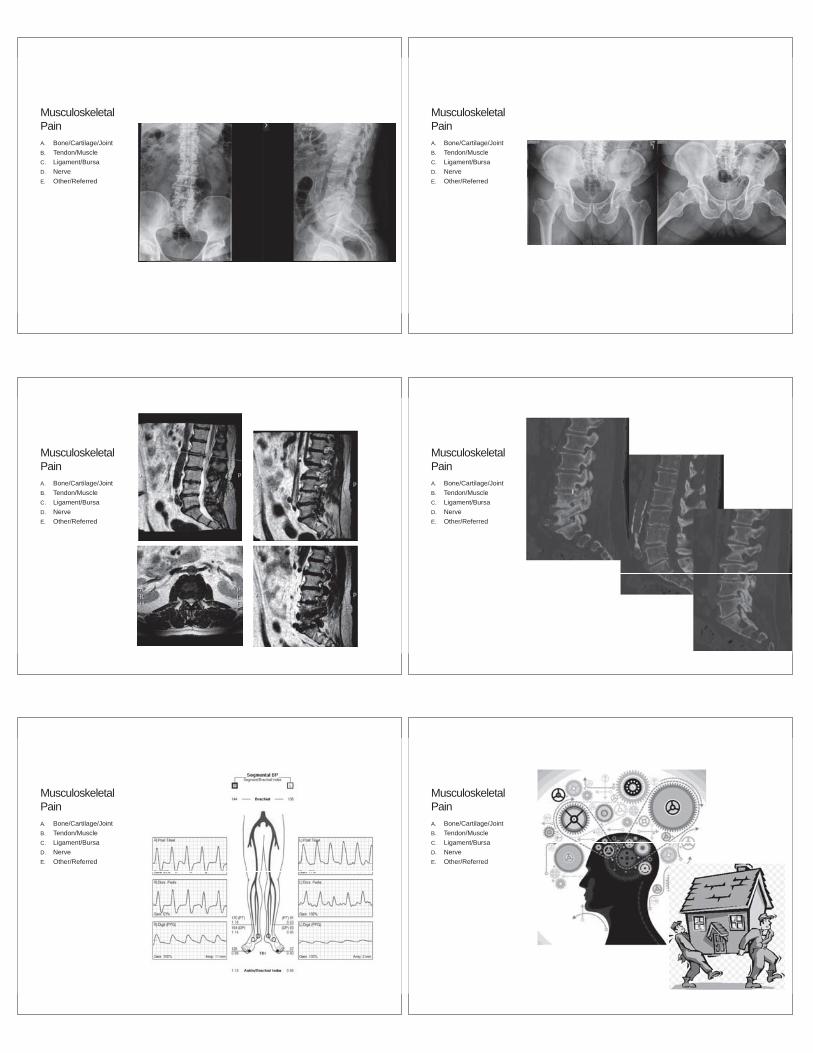
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred

IntermittentClaudicationA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• 65 year old female• Right THA 5 years ago with good relief of right hip pain
• Left THA 4 years ago with good relief of left hip pain but …
• Immediately felt leg length discrepancy (L>R) with walking leading to …
• New right anterior-lateral hip pain • Increased with weight-bearing, walking• Radiation to knee• No LE paresthesia
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Re-evaluation with Orthopedist• Unremarkable exam and imaging
• Treatment with PT, chiropractor, shoe lift, NSAIDs without help.
• History of mild scoliosis, no back pain
• Hypertension, fibromyalgia, hypercholesterolemia
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Normal spine ROM with mild low back pain, no leg pain
• Decreased, symmetric LE reflexes• Normal bilateral hip ROM
• No pain• Normal sensation bilateral feet• Normal motor bilateral legs• Antalgic gait with decreased cadence• Pain with RLE weight bearing
• Negative straight leg raise, reverse straight leg raise
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
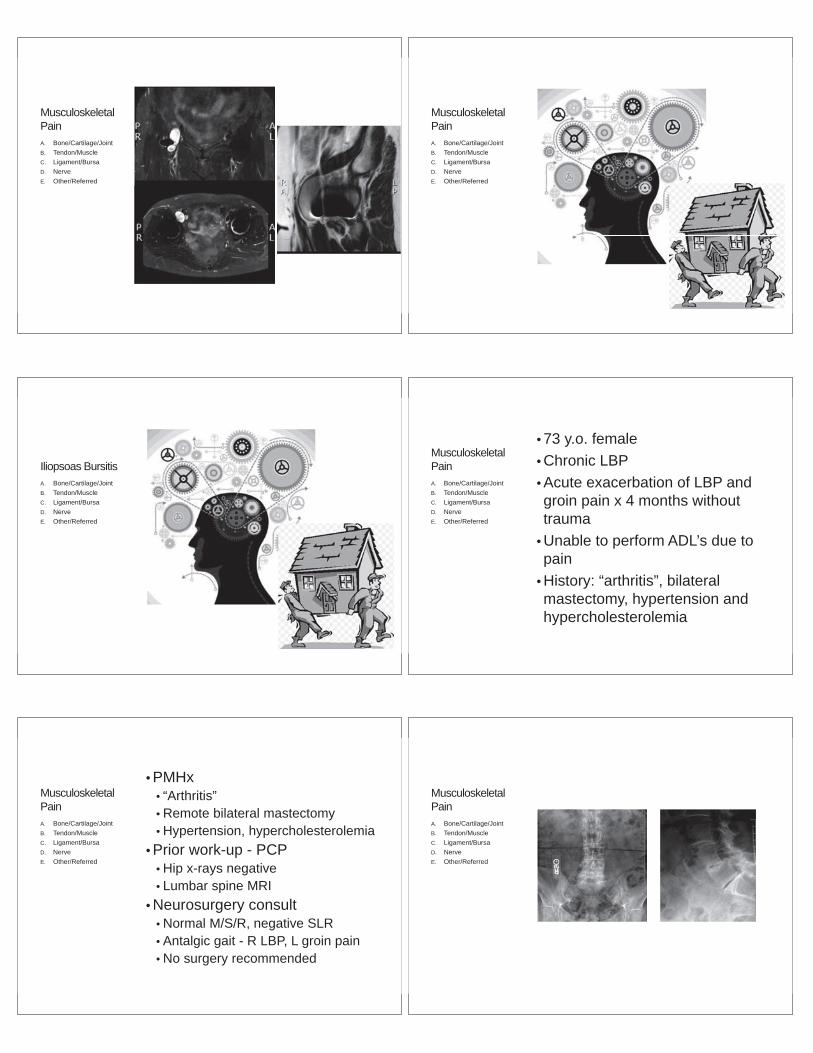
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
Iliopsoas BursitisA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• 73 y.o. female• Chronic LBP• Acute exacerbation of LBP and groin pain x 4 months without trauma
• Unable to perform ADL’s due to pain
• History: “arthritis”, bilateral mastectomy, hypertension and hypercholesterolemia
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• PMHx• “Arthritis”• Remote bilateral mastectomy• Hypertension, hypercholesterolemia
• Prior work-up - PCP• Hip x-rays negative• Lumbar spine MRI
• Neurosurgery consult • Normal M/S/R, negative SLR• Antalgic gait - R LBP, L groin pain• No surgery recommended
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
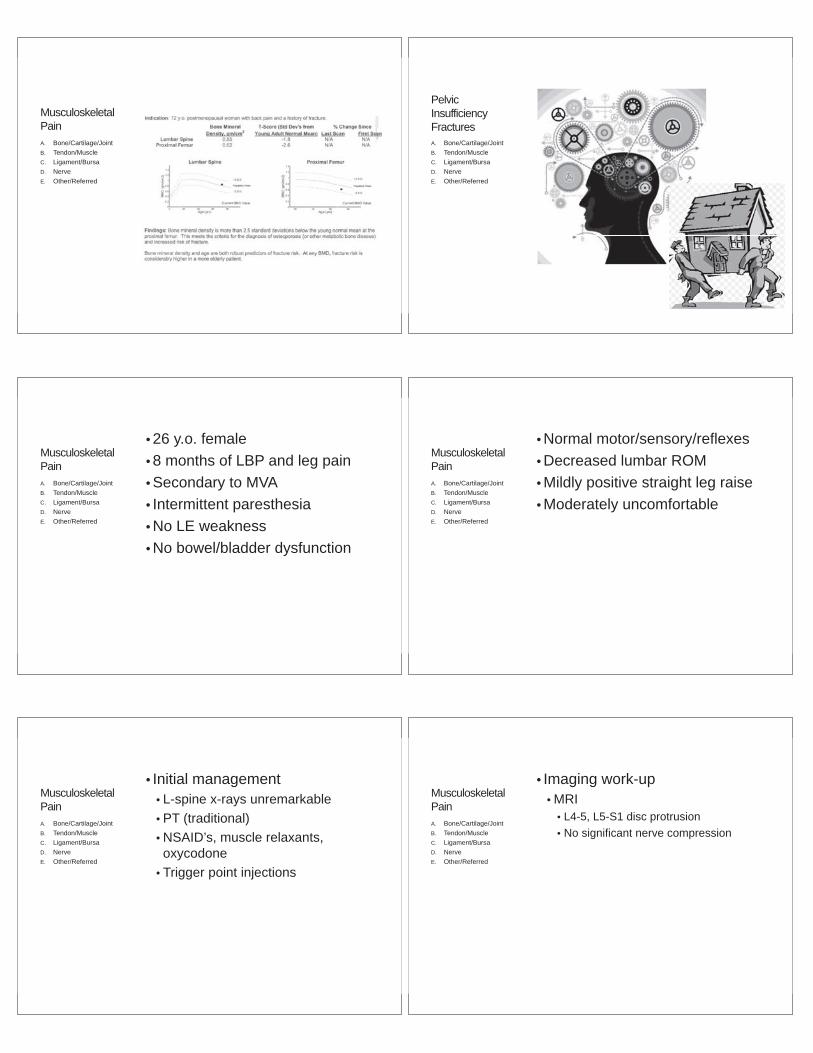
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
PelvicInsufficiency FracturesA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• 26 y.o. female• 8 months of LBP and leg pain • Secondary to MVA• Intermittent paresthesia• No LE weakness• No bowel/bladder dysfunction
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Normal motor/sensory/reflexes• Decreased lumbar ROM• Mildly positive straight leg raise• Moderately uncomfortable
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Initial management• L-spine x-rays unremarkable• PT (traditional)• NSAID’s, muscle relaxants, oxycodone
• Trigger point injections
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Imaging work-up• MRI
• L4-5, L5-S1 disc protrusion• No significant nerve compression
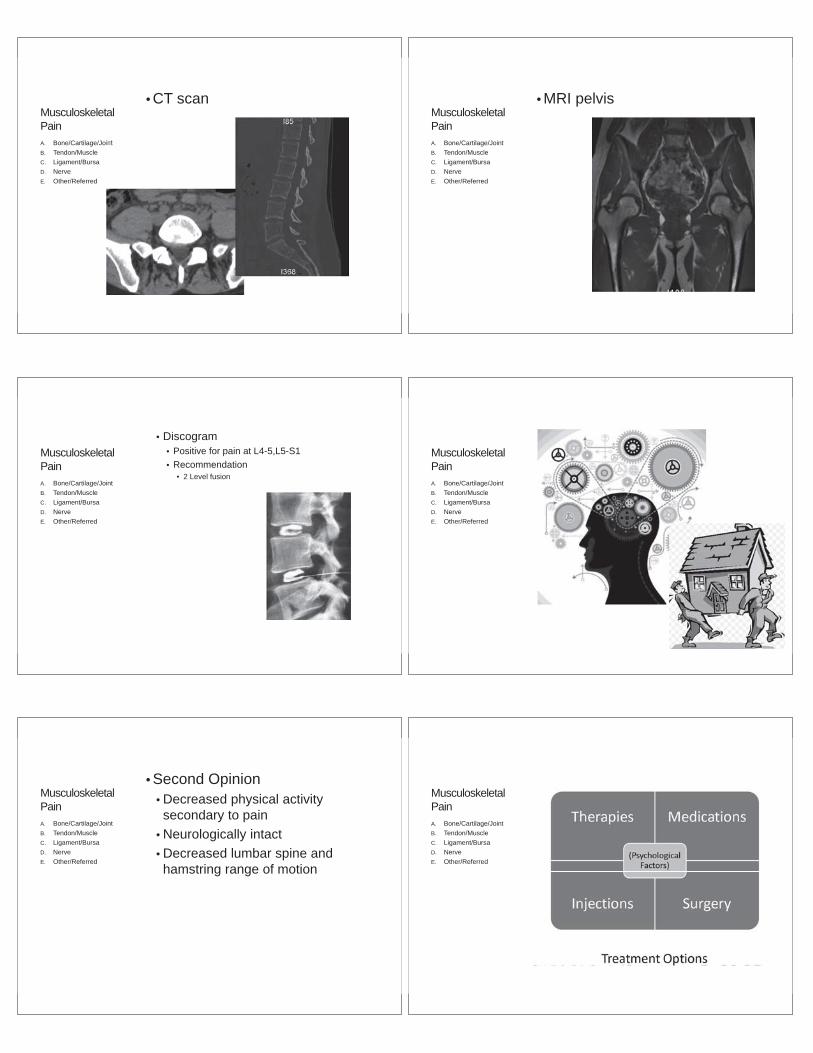
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• CT scanMusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• MRI pelvis
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Discogram• Positive for pain at L4-5,L5-S1• Recommendation
• 2 Level fusion
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
• Second Opinion• Decreased physical activity secondary to pain
• Neurologically intact• Decreased lumbar spine and hamstring range of motion
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
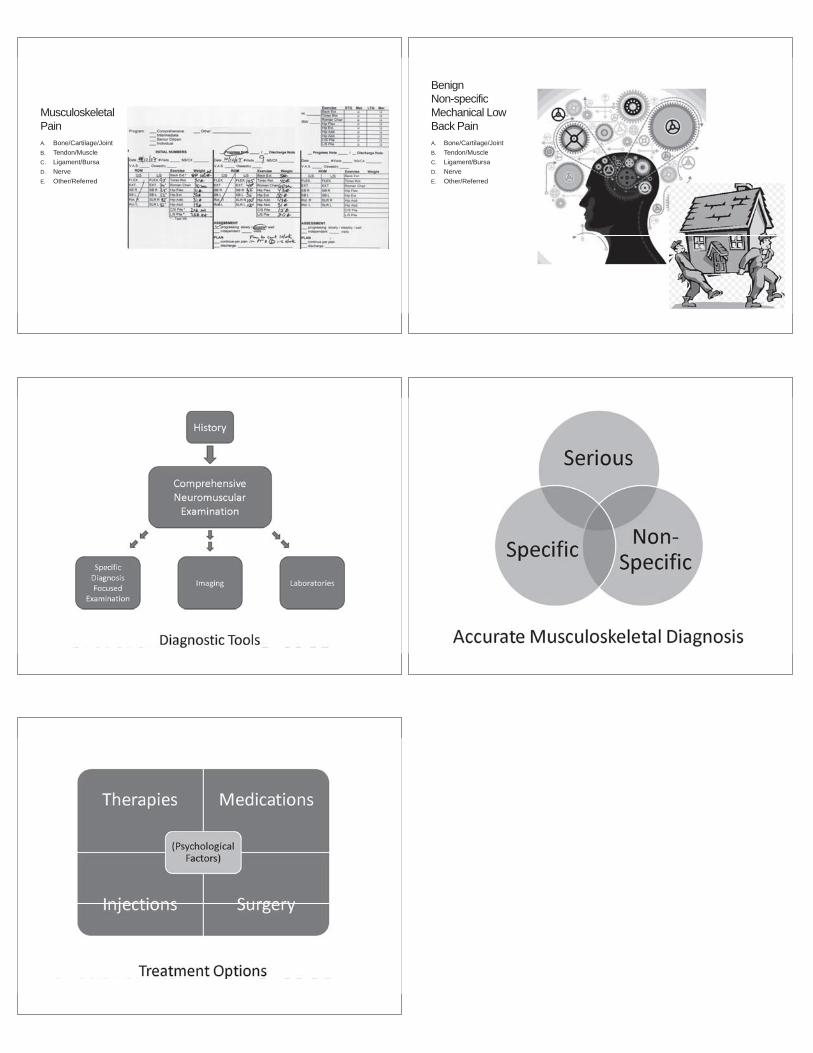
MusculoskeletalPainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred
BenignNon-specificMechanical Low Back PainA. Bone/Cartilage/JointB. Tendon/MuscleC. Ligament/BursaD. NerveE. Other/Referred