pleural effusions and sera from patients with benign or malignant diseases
TRANSCRIPT
BIOLOGICALTRACE ELEMENTRESEARCH
EDITOR-IN-CHIEF
GERHARD N. SCHRAUZER
EDITORS
CHARLES H. HILL
PETER SCHRAMEL
YASUSHI KODAMA
Volume 78 • Nos. 1-3Winter 2000
ISSN: 0163–4984 HUMANA PRESShumanapress.com
Pleural Effusions and Serafrom Patients with Benign
or Malignant DiseasesCopper, Zinc, and Laboratory Parameters
WOLFGANG DOMEJ,*,1 MICHAEL KRACHLER,3
WALTER GOESSLER,3 ALFRED MAIER,2 AND KURT J. IRGOLIC3,†
1Department of Internal Medicine and 2Department of Surgery,and 3Institute for Analytical Chemistry, Karl-Franzens-University,
Graz, Austria
Received February 25, 2000; Accepted April 30, 2000
ABSTRACT
In pleural effusions and sera from 66 patients copper and zincwere quantified by inductively coupled argon plasma–mass spec-trometry after mineralizations in a closed-pressurized microwave unitwith a mixture of concentrated nitric acid and 30% hydrogen peroxide.Total protein, pH, leukocyte count, lactate dehydrogenase, glucose,C-reactive protein, ceruloplasmin, and α1-antitrypsin were determinedin many of the effusions. All but four effusions had concentrations ofcopper (range 58–1720 µg/kg) and zinc (range 27–1001 µg/kg) thatwere lower than the concentrations in the corresponding sera. Veryhigh concentrations of zinc (1930–6470 µg/kg) were characteristic forthoracic empyemata. In the scatterplots of serum copper versus effu-sion copper, serum zinc versus effusion zinc, and serum copper/effusioncopper versus serum zinc/effusion zinc no clearly delineated regionswere noticeably useful for identifying malignant effusions. Similar plotsof the concentrations of copper or zinc versus the eight clinical lab-oratory parameters or plots of clinical parameter versus clinicalparameter failed to be of diagnostic value. Statistically highly signifi-cant correlations (p ≤ 0.05, n > 45, r2 > 0.25) were observed for 9 of 28pairs of the clinical parameters, for total protein and copper in theeffusions and zinc in the effusions and for ceruloplasmin and copper
© Copyright 2000 by Humana Press Inc.All rights of any nature, whatsoever, reserved.0163–4984/00/7801–3–0013 $15.25
Biological Trace Element Research 13 Vol. 78, 2000
*Author to whom all correspondence and reprint requests should be addressed.†Deceased.
in the effusions. Among the patients suffering from benign or malig-nant effusions, 52% had zinc concentrations in the sera below the lowlimit of the normal range (600 µg/kg). Supplementation of suchpatients with zinc should be considered.
Index Entries: Pleural effusion; serum; copper; zinc; clinicallaboratory parameters; malignancies.
INTRODUCTION
Physiologically, a small volume (approx 10 mL) of fluid is presentbetween the visceral and parietal membranes of the pleural space (1).Several pathological conditions may lead to the accumulation of excessliquid between these membranes, causing symptoms such as dyspnea,nonproductive cough, and thoracic tightness. Increased capillary perme-ability, elevated hydrostatic pressure, insufficient lymphatic drainage offluids, and low colloid osmotic pressure may be contributing to the accu-mulation of fluids (1). These liquids and the substances dissolved inthem, including trace elements, are derived from the circulating blood.When these effusions are withdrawn upon thoracentesis, the body isdeprived of the trace elements present in the effusions. Thoracentesis andespecially repeated thoracenteses may lead to imbalances of trace ele-ments, to depletion of depots of trace elements in the body, to deficiency-related diseases, and to functional disturbances.
The medical literature is almost devoid of data about trace elementsin pleural effusions (2–11) and has no data on concentrations of trace ele-ments in the normal gliding fluid between the pleural membranes. Thedetermination of 14 trace elements in pleural effusions withdrawn from17 patients revealed that 1 kg of an effusion may contain trace elementsin amounts equal to 30% of the total amounts of these trace elements incirculation (9). Concentrations of trace elements in pleural effusionscould be of diagnostic value and could perhaps assist in differentiatingeffusions associated with benign or malignant diseases. Such diagnosticassistance would be especially welcome in those cases (approx 20% of alleffusions) that remain without a definite diagnosis (6). Inspection of theconcentrations of trace elements in effusions and sera from 23 patientswith benign and malignant diseases indicated that the concentrations ofCs, Cu, Mn, Mg, Mo, Pb, Rb, Sr, and Zn tended to be higher and the con-centrations of Ca, Cd, and Co lower in the effusions of patients withbenign diseases than in the effusions of patients with malignancies (10).Whether concentrations of trace elements in the effusions alone or incombination with concentrations in sera could be diagnostically helpfulis an unsettled issue. The concentrations of Cu (3,7,8), Zn (5,8), Se (8), andMg (8) were claimed to have no diagnostic value and the ratios of theconcentrations of zinc in sera and effusions to be unlikely of diagnosticvalue (6) for pleural diseases. Insufficient information about the analytical
14 Domej et al.
Biological Trace Element Research Vol. 78, 2000
procedures (3–8), incorrect units for the concentrations (5), suspiciouslyhigh concentrations for Cu (7,8), absence of individual concentrations(only ranges, medians, or averages reported) in the articles (5–8), and thefailure to analyze appropriate standard reference materials concomitantlywith the sera and effusions prevent an evaluation of the quality of thereported data and of the conclusiveness of the conclusions.
To explore the potential diagnostic value of trace elements in pleuraleffusions and in sera in more detail, the concentrations of the essentialelements copper and zinc were quantified in the sera and effusions col-lected from 66 patients with benign or malignant diseases. The sera andeffusions were mineralized in closed vessels and copper and zinc deter-mined in the digests by inductively coupled argon plasma–mass spec-trometry (ICP-MS). Correlations between the concentrations of copperand zinc, between the concentrations of these two trace elements andclinical laboratory parameters, and the benign or malignant nature of thediseases were sought.
METHODS
Patients were recruited from the outpatient pulmonary and medicalclinics of the KF-University Hospital in Graz, Austria. Effusions wereobtained by thoracentesis with troikard needles or a pleura catheter sys-tem (Pleuracath®) in conjunction with medically necessary therapeutic anddiagnostic interventions. Approximately 20 mL of fluid were collectedwith a plastic syringe and transferred into a polyethylene tube (BectonDickinson, France). Venous blood (5 mL) taken immediately after thora-centesis with a vacutainer system and silicone-coated, evacuated bloodcollection tubes without any anticoagulant were centrifuged for 10 min(10g at 4˚C). Sera and effusions were stored in a refrigerator. An aliquot ofeach pleural fluid was collected in a heparinized glass capillary for theimmediate determination of pH with a blood gas analyzer (AVL 995 Hb).
Mineralization
Aliquots (approx 1.5 mL) of the effusions (density 1004–1035 g/L)(12) and of the sera (density 1000 g/L) weighed to 0.1 mg were mixedwith 1.50 mL of concentrated HNO3 purified by subboiling distillation inan all-quartz distillation unit and 0.50 mL high-purity hydrogen perox-ide (30%, Suprapur®, Merck) in Teflon digestion vessels and mineralizedin a closed-pressurized microwave digestion unit (MLS 1200 MEGA,MLS GmbH, Leutkirch, Germany) equipped with a rotor for 10 Teflonvessels that are designed for pressures up to 30 bar. The mixtures wereexposed to microwave energy at 250 W for 2 min, 0 W for 30 s, 300 Wfor 5 min, 0 W for 30 s, 400 W for 10 min, 0 W for 30 s, 500 W for 5 min,and 600 W for 2 min (9). The completely clear, pale yellow, homogeneous
Copper and Zinc in Pleural Effusions and Sera 15
Biological Trace Element Research Vol. 78, 2000
digests were transferred with 10-mL volumetric flasks. The flasks werefilled to the mark with NANOpure water.
Determination of Cu and Zn in Effusionsand Sera
Copper and zinc were quantified in the diluted digests with anICP-MS (VG Plasma Quad PQ 2 Turbo Plus, VG Elemental Ltd., Winford,UK) equipped with a Meinhard concentric glass nebulizer, a double-pass,Scott-type spray chamber (water cooled, 0˚C), and a Gilson Miniplus-3peristaltic pump. The operating conditions for the ICP-MS are summa-rized in Table 1. The count rate of the instrument was optimized with asolution of indium nitrate (115In). All solutions were spiked to 50 µg In/L.Indium served as an internal standard to compensate instrumental drift.External calibration curves for Cu and Zn were obtained in the requiredconcentration ranges with standard dilutions for atomic absorption spec-trometry. Because the densities of the effusions and sera are at most 0.4%higher than the density of distilled water, the concentrations expressedper kilogram are numerically equal to the concentrations expressed perliter within the experimental error.
Clinical Laboratory Parameters
Total protein in the effusions were quantified spectrophotometrically(13) at 546 nm (Hitachi 747 Analyzer) after reaction with an alkaline cop-per sulfate solution (Biuret reagent). C-reactive protein was determinedwith an immunoassay (anti-human-CRP-goat serum) turbidimetrically at700/340 nm (14) and ceruloplasmin and α1-antitrypsin nephelometrically
16 Domej et al.
Biological Trace Element Research Vol. 78, 2000
Table 1Operating Conditions for the VG PlasmaQuad 2
Turbo Plus ICP-MS
with an N-antiserum (15,16). Lactate dehydrogenase was quantified ac-cording to the optimized standard method of the German Society forClinical Chemistry (17).
Quality Control and Statistical Methods
The accuracy of the procedure (microwave digestion and ICP-MS)was ascertained for the first set of samples with Seronom™ “Trace Ele-ments in Serum” (Nycomed, Oslo, Norway) and for the second set with aserum standard provided by Dr. Rita Cornelis, Laboratory for AnalyticalChemistry, University of Gent, Belgium. Reference materials were ana-lyzed with every batch of the effusions and sera. The data were analyzedwith the statistical software package Stat View 4.5® (Abacus Concepts, Inc.,Berkely, CA, 1994) using linear least squares correlations and regressions.
RESULTS AND DISCUSSION
In an earlier publication (9), we reported the concentrations of traceelements in pleural effusions and in sera from 17 patients and found thatfor most of the elements investigated and for most patients, the concen-trations of 14 trace elements in the effusions were lower than in the sera.In the meantime, effusions and sera from additional patients had becomeavailable, in which trace elements were quantified by ICP-MS after min-eralization of aliquots of these body fluids in a microwave digestion unit.With results from 66 pairs of effusions and sera including the original 17pairs (9), the data were screened for correlations that might exist betweenthe concentrations of copper and zinc in effusions and sera from patientswith benign and malignant diseases and the eight clinical laboratoryparameters total protein, leukocyte count, lactate dehydrogenase, glu-cose, pH, C-reactive protein, ceruloplasmin, and α1-antitrypsin. Diagnos-tic data for the 66 patients (40 female, 26 male), 34 with malignancies and32 with benign diseases, are summarized in Table 2.
Copper and Zinc in Effusions and Sera
The concentrations of copper and zinc in the effusions and in thesera are, with exception of three effusions, at least 10 times higher thanthe method detection limits (MDL) (Table 2). Under these conditions, theanalytical uncertainties associated with the concentrations are low (relativestandard deviations <10%) and are unlikely to obscure any correlationsbetween the concentrations of copper and zinc and the clinical laboratoryparameters. The concentrations of copper and zinc in the reference mate-rials determined concomitantly with the effusions and sera were inacceptable agreement with the recommended values: Nycomed serumCu 1150 ± 30 µg/kg (n = 12), recommended range 1200–1380 µg/kg (18) /Zn 1480 ± 70 (n = 12), recommended range 1600–1800 µg/kg (18); Gentserum Cu 980 ± 30 µg/kg (n = 10), certified 1009 ± 36; Zn 850 ± 30 µg/kg
Copper and Zinc in Pleural Effusions and Sera 17
Biological Trace Element Research Vol. 78, 2000
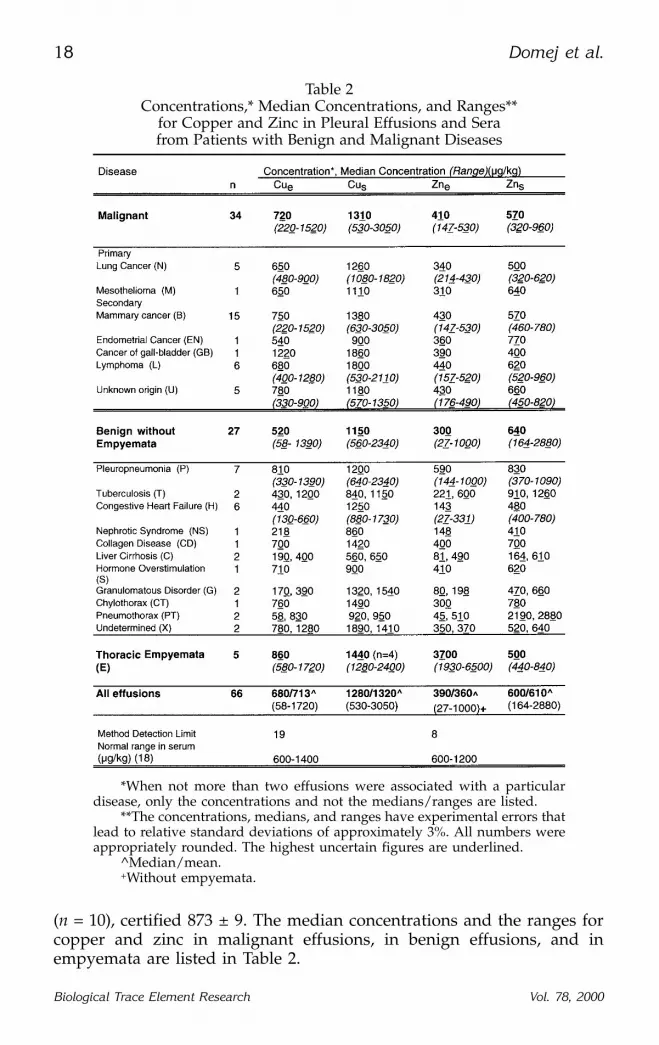
(n = 10), certified 873 ± 9. The median concentrations and the ranges forcopper and zinc in malignant effusions, in benign effusions, and inempyemata are listed in Table 2.
18 Domej et al.
Biological Trace Element Research Vol. 78, 2000
Table 2Concentrations,* Median Concentrations, and Ranges**
for Copper and Zinc in Pleural Effusions and Serafrom Patients with Benign and Malignant Diseases
*When not more than two effusions were associated with a particulardisease, only the concentrations and not the medians/ranges are listed.
**The concentrations, medians, and ranges have experimental errors thatlead to relative standard deviations of approximately 3%. All numbers wereappropriately rounded. The highest uncertain figures are underlined.
^Median/mean.+Without empyemata.
Copper
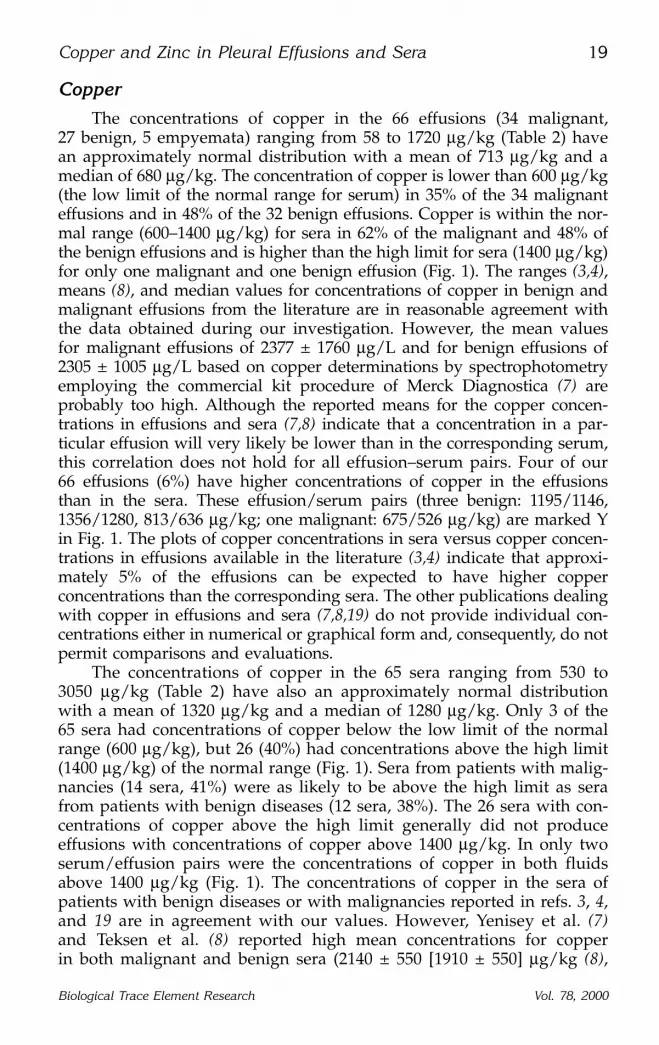
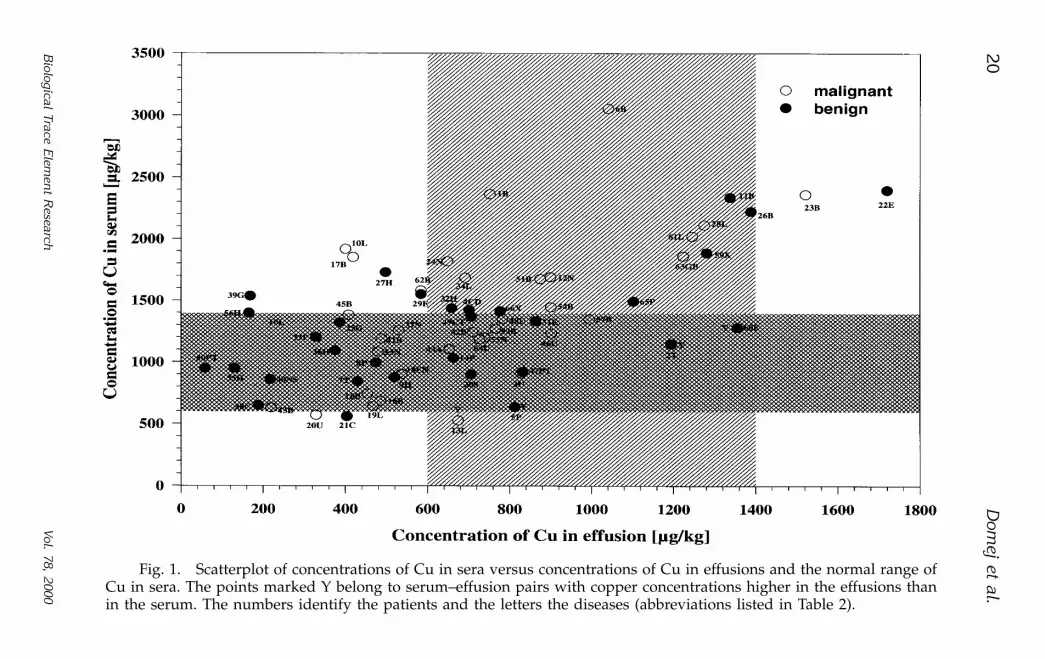
The concentrations of copper in the 66 effusions (34 malignant,27 benign, 5 empyemata) ranging from 58 to 1720 µg/kg (Table 2) havean approximately normal distribution with a mean of 713 µg/kg and amedian of 680 µg/kg. The concentration of copper is lower than 600 µg/kg(the low limit of the normal range for serum) in 35% of the 34 malignanteffusions and in 48% of the 32 benign effusions. Copper is within the nor-mal range (600–1400 µg/kg) for sera in 62% of the malignant and 48% ofthe benign effusions and is higher than the high limit for sera (1400 µg/kg)for only one malignant and one benign effusion (Fig. 1). The ranges (3,4),means (8), and median values for concentrations of copper in benign andmalignant effusions from the literature are in reasonable agreement withthe data obtained during our investigation. However, the mean valuesfor malignant effusions of 2377 ± 1760 µg/L and for benign effusions of2305 ± 1005 µg/L based on copper determinations by spectrophotometryemploying the commercial kit procedure of Merck Diagnostica (7) areprobably too high. Although the reported means for the copper concen-trations in effusions and sera (7,8) indicate that a concentration in a par-ticular effusion will very likely be lower than in the corresponding serum,this correlation does not hold for all effusion–serum pairs. Four of our66 effusions (6%) have higher concentrations of copper in the effusionsthan in the sera. These effusion/serum pairs (three benign: 1195/1146,1356/1280, 813/636 µg/kg; one malignant: 675/526 µg/kg) are marked Yin Fig. 1. The plots of copper concentrations in sera versus copper concen-trations in effusions available in the literature (3,4) indicate that approxi-mately 5% of the effusions can be expected to have higher copperconcentrations than the corresponding sera. The other publications dealingwith copper in effusions and sera (7,8,19) do not provide individual con-centrations either in numerical or graphical form and, consequently, do notpermit comparisons and evaluations.
The concentrations of copper in the 65 sera ranging from 530 to3050 µg/kg (Table 2) have also an approximately normal distributionwith a mean of 1320 µg/kg and a median of 1280 µg/kg. Only 3 of the65 sera had concentrations of copper below the low limit of the normalrange (600 µg/kg), but 26 (40%) had concentrations above the high limit(1400 µg/kg) of the normal range (Fig. 1). Sera from patients with malig-nancies (14 sera, 41%) were as likely to be above the high limit as serafrom patients with benign diseases (12 sera, 38%). The 26 sera with con-centrations of copper above the high limit generally did not produceeffusions with concentrations of copper above 1400 µg/kg. In only twoserum/effusion pairs were the concentrations of copper in both fluidsabove 1400 µg/kg (Fig. 1). The concentrations of copper in the sera ofpatients with benign diseases or with malignancies reported in refs. 3, 4,and 19 are in agreement with our values. However, Yenisey et al. (7)and Teksen et al. (8) reported high mean concentrations for copperin both malignant and benign sera (2140 ± 550 [1910 ± 550] µg/kg (8),
Copper and Zinc in Pleural Effusions and Sera 19
Biological Trace Element Research Vol. 78, 2000
20D
omej et al.
Biological Trace E
lemen
t Research
Vol. 78, 2000
Fig. 1. Scatterplot of concentrations of Cu in sera versus concentrations of Cu in effusions and the normal range ofCu in sera. The points marked Y belong to serum–effusion pairs with copper concentrations higher in the effusions thanin the serum. The numbers identify the patients and the letters the diseases (abbreviations listed in Table 2).
3760 ± 1170 [2630 ± 1410] (7), respectively). Copper in the sera had beenquantified either by flame atomic absorption spectrometry (8) or by spec-trophotometry (7) (Merck Diagnostica procedure). Systematic errors—notunknown for these methods—could have produced the high results. Allresults indicate, however, that the mean and median concentrations ofcopper in sera decrease in the sequence malignant > benign > healthy.The ranges for these concentrations overlap to such an extent that malig-nancies cannot be distinguished from benign diseases on the basis of cop-per concentrations in sera.
The plot of the concentrations of copper in the sera versus theconcentrations of copper in the effusions (Fig. 1) reveals that all pointsare within a broad band extending on both sides of the straight lineCus = 0.88Cue + 716 with a least squares slope of 0.88 (r2 = 0.36). The leastsquares straight line calculated for the 34 malignant effusions has a slopeof 1.20 and an intercept of 500 (r2 = 0.37). The values for the 31 benigneffusions are 0.70 and 809 (r2 = 0.41). That the malignant effusions pro-duce higher slopes than the benign effusions were previously observed(3,4). The slopes created by sets of malignant effusions are very likelydependent on the mix of types of malignancies. Whereas lymphomasgenerated slopes of 1.42 (n = 14) (3), 1.15 (n = 21) (4), and 1.03 (n = 6)(our results), mammary cancers (n = 15) produced a straight line with aslope of only 0.32 (intercept 224, r2 = 0.42) (our results).
In Fig. 1, no region is evident that could be called characteristic foreffusions associated either with malignant or with benign diseases. Theranges for the concentrations of copper in the sera and in the effusionsassociated with either benign or malignant diseases are so similar thatmalignant effusions cannot be differentiated unambiguously from benigneffusions. Previous investigators (3,4,7,8) reached the same conclusion.The mean concentrations of copper in the sera of patients with malignanteffusion were higher than in the sera of patients with benign effusions.This difference between the means for malignant and benign effusionswas statistically significant for sera but not for effusions (7). However,even statistically significant differences between means are not diagnos-tically helpful for individual serum–effusion pairs, nor are differences inslopes and medians, unless the concentration ranges do not overlapappreciably. Even the concentrations of copper in the sera and effusionsfrom patients with mammary cancer (n = 15), malignant lymphoma (n = 6),or primary lung cancer (n = 5) are evenly distributed over the entire con-centration ranges. In empyemata (n = 5) and in the corresponding sera,the copper concentrations tend to be in the upper half of the concentra-tion ranges for patients with benign diseases.
Zinc
The concentrations of zinc in the 61 effusions (34 malignant, 27 be-nign) ranging from 27 to 1000 µg/kg (Table 2) possess an approximatelynormal distribution with a mean of 360 µg/kg (n = 61) and a median of
Copper and Zinc in Pleural Effusions and Sera 21
Biological Trace Element Research Vol. 78, 2000
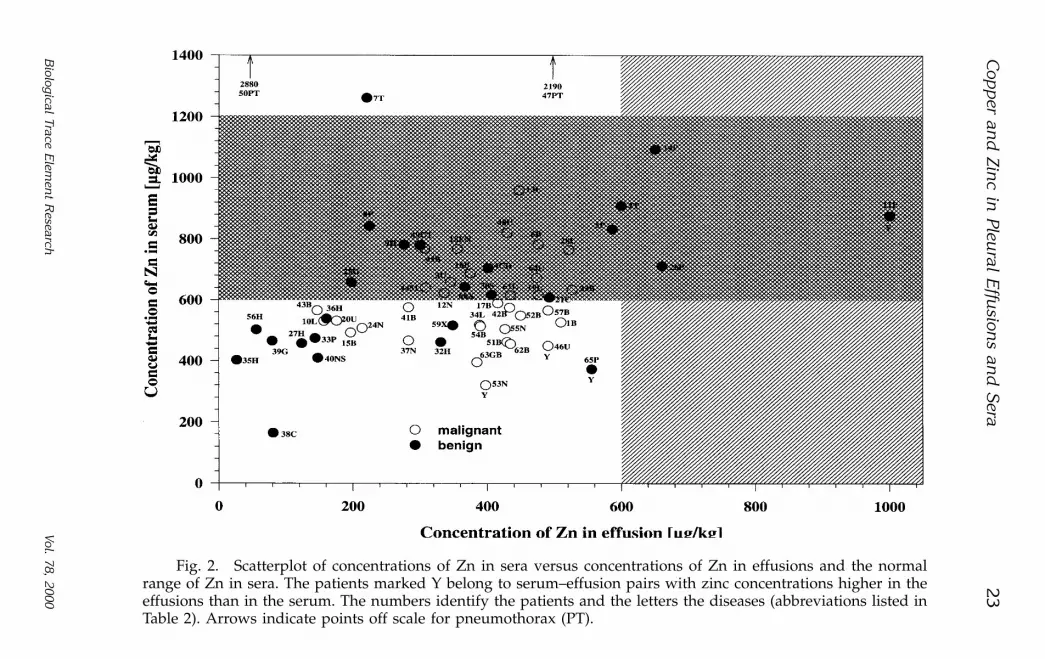
390 µg/kg. The five empyemata were excluded, because their zinc concen-trations are considerably higher (1930–6500 µg/kg) than the concentrationin any other effusion. The concentration of zinc is lower than 600 µg/kg(the low limit of the normal range in serum) in 100% of the 34 malignantand in 85% of the 27 benign effusions (without empyemata). None ofthe effusions have zinc concentrations higher than the high limit for sera(1200 µg/kg). The highest concentration of zinc in the malignant effusionswas 530 µg/kg, and in the benign effusions (exclusive of empyemata), itwas 1000 µg/kg (Table 2). The ranges (3–5), means (8), and median values(3,4) for concentrations of zinc reported for benign and malignant effu-sions are in reasonable agreement with the data obtained during our in-vestigation. With the exception of four effusion/serum pairs (two benign:560/370, 1000/880; two malignant: 400/320, 490/450) marked Y in Fig. 2,all effusions have lower concentrations of zinc than the correspondingsera. The concentrations of zinc in benign and malignant effusions from theliterature (3–4,8) are in the same range as our results. A detailed compari-son is not possible, because only medians, means, or ranges are reported.
The concentrations of zinc in the sera (inclusive of empyemata; theirzinc concentrations are within the range for the other sera) from 164 to2880 µg/kg (Table 2) are normally distributed with a mean of 610 µg/kg(n = 63) and a median of 600 µg/kg. The sera from patients #47 and#50 (diagnosis pneumothorax) with zinc concentrations of 2190 and2880 µg/kg were excluded as outliers. Among the 65 sera, 34 (52%) hadzinc concentrations below the low limit of the normal range (600 µg/kg)and only three sera (one tuberculosis, two pneumothoraces) had concen-trations above the high limit of the normal range (1200 µg/kg). Sera frompatients with malignancies (20 from 34, 59%) are more likely to have zincconcentrations below 600 µg/kg than sera from patients with benign dis-eases (14 from 31, 45%) (Fig. 2). Low concentrations for zinc in sera werereported for patients with lung cancer (19,20).
The plot of the concentrations of zinc in the sera versus the concen-trations of zinc in the effusions with the five empyemata excluded (Fig. 2)shows that clearly delineated regions for effusions associated with malig-nant or benign diseases are not recognizable. However, low concentrationsof zinc in effusion–serum pairs and high concentrations either in effusionsor in sera appear to indicate benign conditions. The two patients withpneumothorax (PT) have high zinc concentrations in the sera (2190 and2880 µg/kg) but unremarkable concentrations in the pleural fluid (510and 45 µg/kg). The six patients with congestive heart failure (H) tendedto possess low concentrations of zinc in their sera and their effusions,whereas five of the seven patients with pleuropneumonia (P) had highconcentrations of zinc in the effusions. The zinc concentrations for the 15patients with mammary carcinomas (marked B in Fig. 2) did not define aregion suitable for diagnosing breast cancer on the basis of zinc concen-trations in the sera and/or the effusions (Fig. 2). Consequently, the limitednumber of zinc concentrations in effusions and the corresponding sera
22 Domej et al.
Biological Trace Element Research Vol. 78, 2000
Cop
per an
d Zin
c in Pleu
ral Effu
sions an
d S
era23
Biological Trace E
lemen
t Research
Vol. 78, 2000
Fig. 2. Scatterplot of concentrations of Zn in sera versus concentrations of Zn in effusions and the normalrange of Zn in sera. The patients marked Y belong to serum–effusion pairs with zinc concentrations higher in theeffusions than in the serum. The numbers identify the patients and the letters the diseases (abbreviations listed inTable 2). Arrows indicate points off scale for pneumothorax (PT).
(approximately 110 from all sources) do not permit a final statement aboutthe diagnostic usefulness of zinc concentrations, although earlier investi-gators expressed pessimistic opinions (4–6,8).
When the two pneumothorax patients (#47, #50) and the tuberculo-sis patient (#7) are excluded because of high zinc concentrations in thesera, the plots Zn in serum versus Zn in effusion produced linear leastsquares lines with the following characteristics (slope, intercept, r2):benign 0.56, 426, 0.41 (n = 27); all malignant 0.25, 497, 0.04 (n = 34); mam-mary cancer 0.047, 564, 0.003 (n = 15); benign and malignant 0.48, 428,0.25 (n = 61). Only the benign set produces a correlation coefficient in-dicative of a highly significant linear dependence (p ~0.05).
Zinc/Copper Correlations
The concentrations of zinc and copper in the sera and the effusionswere plotted against each other (Zns/Cus, Zns/Cue, Zne/Cue, Zne/Cus).Linear least squares lines and correlation coefficients were calculated forthe four plots. Empyemata and the sera from patients with pneumothorax(#47, #50) or tuberculosis (#11) were excluded because of the high concen-trations of zinc. The concentrations of zinc in the sera are not correlatedwith the concentrations of copper in the sera (r2 ≤ 0.002) for the entireset, for the set of benign, and for the set of malignant effusion–serum pairs, whereas a good correlation exists for the concentrations in theeffusions (Zne = kCue + d; k, d, r2 for the entire set 0.35, 110, 0.56,n = 59; for the benign set 0.43, 50.4, 0.61, n = 26; for the malignant set 0.24,198, 0.42, n = 34). The zinc concentrations in the effusions are weakly cor-related with the copper concentrations in the sera (r2 for the entire set 0.056,for the benign set 0.008, for the malignant set 0.12). The corresponding r2
values for Zn serum/copper effusion are 0.12 (entire set), 0.25 (benign), and0.014 (malignant). Clearly discernable regions characteristic for either be-nign or malignant effusions/sera are not present in the scattergrams.
Diez and co-workers (19) reported that the ratios of the concen-trations of copper to zinc in the sera have a greater discriminating valuethan the concentrations of copper and zinc alone. The Cu/Zn ratioswere significantly higher for patients with lung cancer (mean 2.34 ± 0.78,n = 64) than for patients with not identified benign pulmonary condi-tions (1.62 ± 0.23, n = 20) or for healthy patients (1.43 ± 0.29, n = 100).In our studies, the five sera associated with primary lung cancer hadhigh Cu/Zn ratios of 2.18, 2.38, 2.69, 3.39, and 3.59, whereas the five seraassociated with benign lung diseases had low ratios (tuberculosis 0.67,1.26; pneumothorax 0.33, 0.42; chylothorax 1.91). These two sets of ratiossupport the results of Diez et al. (19). However, the sera from patientswith pleuropneumonia (marked P in Figs. 1 and 2) produce ratios of0.76, 0.94, 1.18, 2.53, 2.67, 3.13, and 4.01. A discrimination between lungcancer and pneumothorax is not possible on the basis of Cu/Zn ratiosin sera.
24 Domej et al.
Biological Trace Element Research Vol. 78, 2000
An inspection of the concentration ratios of copper in effusion/zincin effusion did not reveal a pattern that would allow diagnosing primarylung cancer, mammary cancer, or lymphomas on the basis of copper andzinc concentrations in the effusions. Effusions associated with benignpulmonary diseases (two pneumothorax, two tuberculosis, seven pleuro-pneumonia) had Cu/Zn ratios in the same range as effusions associatedwith malignancies. Empyemata, because of their elevated concentrationsof zinc, have low Cu/Zn ratios that are well separated from the ratios formalignant effusions and the ratios for other benign effusions.
The scattergrams of Zns/Zne versus Cus/Cue and Cue/Zne versusCus/Zns did not contain any regions characteristic for either benign ormalignant effusions. Consequently, benign effusions cannot be differenti-ated from malignant effusions on the basis of Cu/Zn concentrationsratios (serum–effusion).
Clinical Laboratory Parameters
The median values and ranges for the clinical laboratory parametersobtained from the effusions are summarized in Table 3. The volumes ofeffusions withdrawn by thoracentesis ranged from 30 to 2500 mL. Themedian volume (1200 mL) for patients with malignant diseases waslarger than for patients with benign disease (800 mL), although the rangewas wider for the benign than for the malignant cases (Table 3). The vol-umes of effusions from the 15 patients with metastatic cancer of thebreast were in the range from 300 to 1500 mL with a median of 900 mL.These volumes withdrawn from patients are not necessarily equal to thetotal volumes of fluid that had accumulated between the parietal and vis-ceral pleural membranes. When the accumulated volume is large, all thefluid must not be withdrawn at once, because complete removal maycause circulatory collapse. When thoracentesis yields only small vol-umes, the effusion may be divided into noncommunicating compart-ments by pleural adhesions.
The protein concentrations for the 65 effusions ranged from 0.3 to8.2 g/dL with a median of 3.8 g/dL and a mean of 3.8 ± 1.5 g/dL) (nor-mal range in serum 6.6–8.7 g/dL) in agreement with literature values(21,22). Of the 65 effusions, in which total protein was quantified, 22 (11each from benign and malignant effusions) must be classified as transu-dates (total protein ≤ 3.0 g/dL) and 43 (20 from benign and 23 frommalignant effusions) as exudates (total protein >3 g/dL) (21,22). The pro-tein concentrations in pleural effusions vary widely (12) and are unsuit-able for differentiating between benign and malignant conditions.
The pH values measured in 48 effusions (range 6.96–7.53, median7.38, mean 7.36 ± 0.11) exceed the physiological range in arterial blood(7.35–7.45) in the acidic as well as in the alkaline direction. The differencebetween the highest and lowest pH is 0.57 for benign and 0.40 for malig-nant effusions (Table 3). Values characteristic of acidosis were found for
Copper and Zinc in Pleural Effusions and Sera 25
Biological Trace Element Research Vol. 78, 2000
19% of the 19 benign and for 30% of the 29 malignant effusions. Effusionswith pH <7.30 were observed to have been associated with several benignand malignant diseases (23,24).
The leukocyte count in the 50 effusions (range in effusions withoutempyemata 0.2–23.5 G/L, median 1.0 G/L, mean 3.1 G/L; normal rangein whole blood 4 to 10 G/L) was ≤4.00 G/L for 84% of the malignant and63% of the benign effusions. Three of the 31 malignant and 5 of the 19benign effusions had counts between 14.6 and 29.6 G/L. These highcounts were associated with four thoracic empyemata, two lymphomas,one lung cancer, and one pleuropneumonia. The leukocyte count is diag-nostically not useful for differentiating between effusions associated witheither benign or malignant conditions (12,25).
Lactate dehydrogenase (LDH), an enzyme that catalyzes the con-version of pyruvate to lactate, is known to be elevated in sera frompatients with severe inflammation, infarction, or neoplasms. The LDHconcentrations in sera and pleural effusions had been used to distin-guish exudates from transudates (21,26). Effusions of malignant originhad been observed to have higher LDH activity than the correspond-ing sera (27–31). Effusions from patients with Laennec’s cirrhosis, con-gestive heart failure, myocardial infarction, tuberculosis, pneumonia, orpleuritis had LDH below 128 U/L, whereas 85% of the 27 effusions frompatients with malignancies had LDH higher than 128 U/L (range128–823 U/L). Therefore, LDH activity in the effusions without referenceto LDH in sera was suggested to be of diagnostic value in the detectionof malignancy (32).
26 Domej et al.
Biological Trace Element Research Vol. 78, 2000
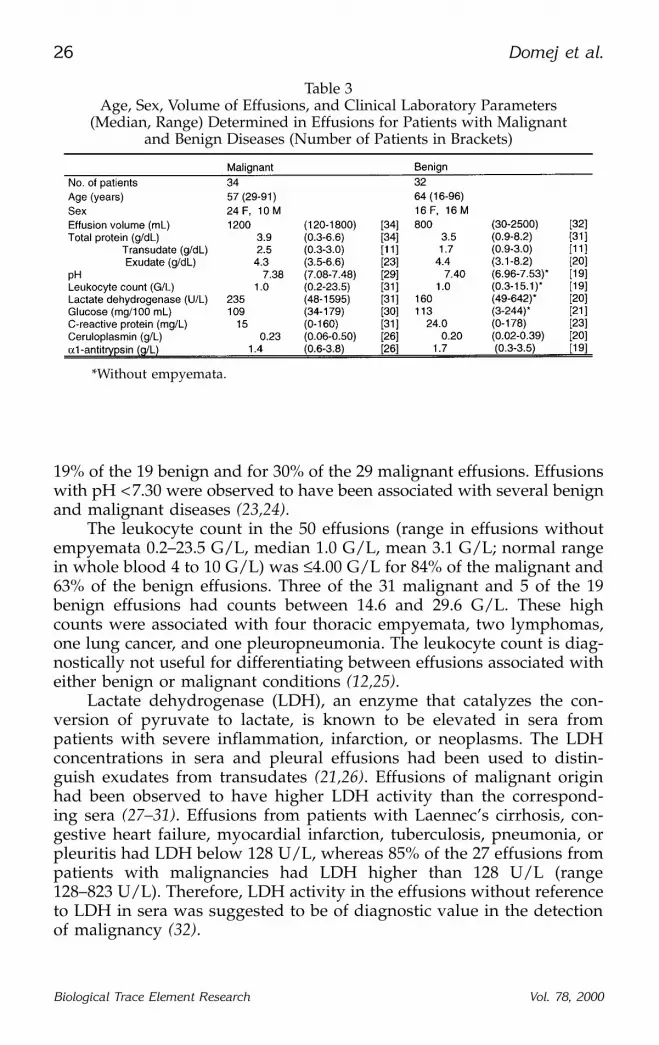
Table 3Age, Sex, Volume of Effusions, and Clinical Laboratory Parameters
(Median, Range) Determined in Effusions for Patients with Malignantand Benign Diseases (Number of Patients in Brackets)
*Without empyemata.
Among the 51 effusions (empyemata excluded), in which we quanti-fied LDH, 31 were associated with malignancies. The range for LDH inthe malignant effusions (48–1595 U/L) overlapped with the range for thebenign effusions (49–642 U/L) (Table 3). Because of this extensive overlapa secure decision, whether or not an effusion is associated with a malig-nancy, appears not to be possible on the basis of LDH determinations ineffusions. When only the 14 effusions associated with mammary carcino-mas (range 78–1473 U/L) are considered, a differentiation between malig-nant and benign effusions is still not possible. Whereas the five effusionsassociated with congestive heart failure had LDH values below 128 U/L(range 49–90 U/L) in general agreement with the literature (21,32), ouronly cirrhotic effusion (182 U/L) was considerably higher than 128 U/L.The median LDH value for the 31 malignant effusions was 235 U/L, forthe 14 effusions associated with mammary carcinomas 253 U/L, and for the20 benign effusions 160 U/L. The median values are not useful for declar-ing an individual effusion to be benign or malignant. Among malignantas well as benign effusions were fluids with very low LDH (48 U/L) andvery high LDH (642 U/L, 1595 U/L). The graphical display of LDH in 150effusions associated with malignancies, tuberculosis, pneumonia, andseveral other benign diseases (21) strengthens the suspicion that LDHalone is not suitable to assign the label malignant or benign to effusions.
The glucose concentrations in the 21 benign and 30 malignant effusions(empyemata excluded) have almost the same median (109/113 mg/dL).The ranges for these concentrations (Table 3) stretch from values charac-teristic in sera for hypoglycaemia (< 50 mg/dL) to values characteristicfor hyperglycaemia (>120 mg/dL). Characteristic differences betweenconcentrations of glucose in benign and malignant effusions are notapparent in the set of 51 effusions, although low glucose concentrationsin malignant effusions were reported to be associated with a high pleuraltumor burden (33,34). Generally, the glucose concentrations in the effu-sions and sera are similar (33) and effusions with low glucose have alsoa low pH (24,35).
The concentration of C-reactive protein, a sensitive but not specificindicator for inflammatory processes and tissue damage, is in all but twoeffusions (inclusive empyemata) higher than the concentration of 0.8 mg/Lin the serum of healthy adults (Table 3). Such high concentrations (up to178 mg/L) are not unexpected, because bacterial, noninfectious inflam-matory, and necrotizing processes may increase the normal concentrationof C-reactive protein in sera by three orders of magnitude within hours.In the collection of 23 benign effusions 12 were below 20 mg/L and 17below 50 mg/L, whereas among 31 malignant effusions, 16 were below20 mg/L and 26 below 50 mg/L of C-reactive protein. Based on theavailable concentrations of C-reactive protein, benign effusions cannot bedistinguished from malignant effusion. Data about C-reactive protein ineffusions were not found in the literature.
Copper and Zinc in Pleural Effusions and Sera 27
Biological Trace Element Research Vol. 78, 2000
Ceruloplasmin, the copper-transport protein with a normal concen-tration in serum between 0.22 and 0.61 g/L, was present in all 20 benign(inclusive empyemata) and all 26 malignant effusions. Approximatelyhalf of the effusions in each group had ceruloplasmin below the low limitin serum and several below 0.1 g/L. In none of the effusions was ceru-loplasmin above the high limit of 0.61 g/L (Table 3). Similar concentra-tions were found for ceruloplasmin in malignant (0.30 ± 0.11 g/L) andbenign (0.30 ± 0.16 g/L) effusions (7). In these patients, the ceruloplasminconcentration in malignant sera (n = 14) was 0.54 ± 0.16 g/L, andin benign sera (n = 34) it was 0.50 ± 0.17 g/L. Benign and malignanteffusions cannot be distinguished on the basis of the concentrations ofceruloplasmin.
α1-Antitrypsin is present in benign and malignant effusions in therange from 0.3 to 3.8 g/L (Table 3). The normal range in serum isreported to be 1.22–2.24 g/L. Of the 26 malignant effusions, 42% hadconcentrations below 1.22 g/L, and of the 19 benign effusions, only 26%did. Only four effusions from each group exceeded 2.3 g/L. Benign effu-sions cannot be distinguished from malignant effusions on the basis ofthe concentrations of α1-antitrypsin. Literature data about this inhibitorin effusions were not found.
Correlations Between Clinical Parameters
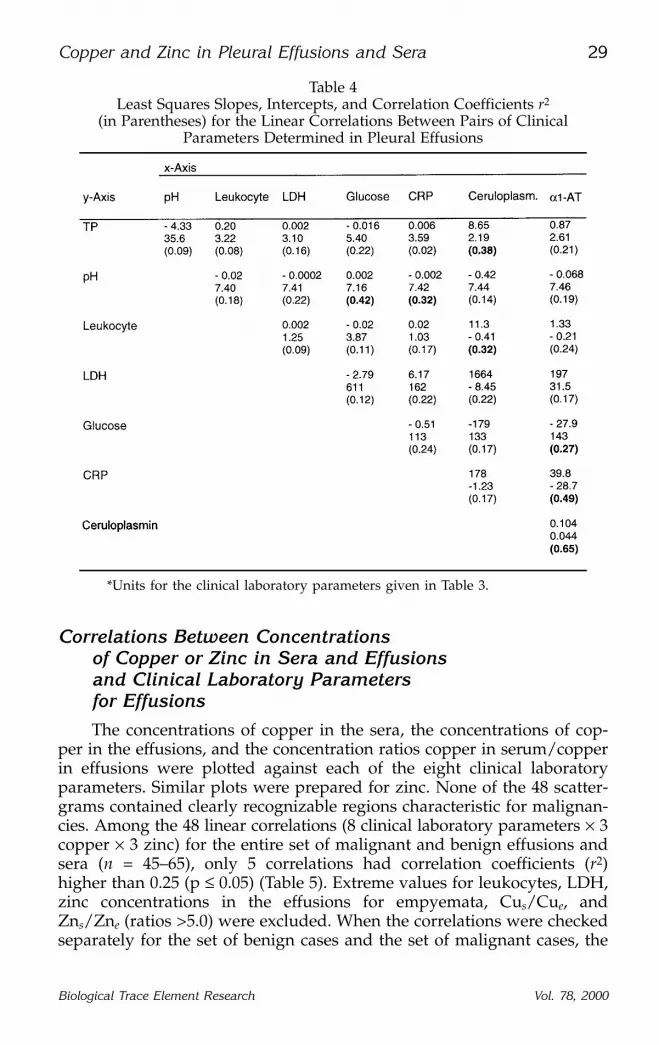
Linear correlations between each pair of the eight clinical laboratoryparameters (total protein, pH, LDH, leukocytes, ceruloplasmin, glucose,C-reactive protein, α1-antitrypsin) determined in benign and malignanteffusions were explored. Slopes, intercepts, and correlation coefficientswere strongly influenced by the high values for leukocytes associatedwith empyema, pleuropneumonia, and lymphoma and for LDH associ-ated with empyema and lymphoma. These high values were excluded.In spite of such exclusions, 41–55 pairs of values were available for thecorrelations and the graphical representations. Clearly delineatedregions characteristic for benign or malignant effusions were not appar-ent in any of the 28 scattergrams. The slopes for the linear least squareslines, the intercepts, and the correlations coefficients (r2) are summarizedin Table 4.
Correlations with p ≤ 0.05 for n > 40 exist between ceruloplas-min and α1-antitrypsin (r2 = 0.65), α1-antitrypsin and C-reactive protein(r2 = 0.49), α1-antitrypsin and glucose (r2 = 0.27), pH and glucose (r2 = 0.42),pH and C-reactive protein (r2 = 0.32), and total protein and ceruloplas-min (r2 = 0.38). The direct proportionality between pH and glucoseappears to be generally valid for effusions (24,35). However, none of thehighly significant correlations or scattergrams for any pair of the eightclinical parameters appears to be diagnostically useful for the differenti-ation between malignant and benign effusions.
28 Domej et al.
Biological Trace Element Research Vol. 78, 2000
Correlations Between Concentrationsof Copper or Zinc in Sera and Effusionsand Clinical Laboratory Parametersfor Effusions
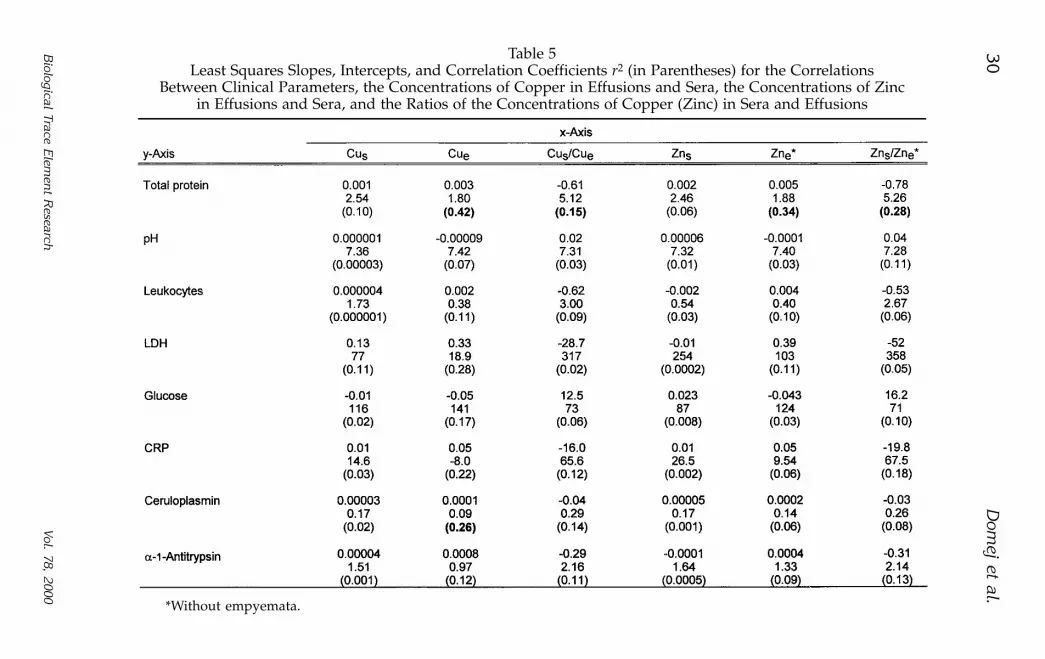
The concentrations of copper in the sera, the concentrations of cop-per in the effusions, and the concentration ratios copper in serum/copperin effusions were plotted against each of the eight clinical laboratoryparameters. Similar plots were prepared for zinc. None of the 48 scatter-grams contained clearly recognizable regions characteristic for malignan-cies. Among the 48 linear correlations (8 clinical laboratory parameters × 3copper × 3 zinc) for the entire set of malignant and benign effusions andsera (n = 45–65), only 5 correlations had correlation coefficients (r2)higher than 0.25 (p ≤ 0.05) (Table 5). Extreme values for leukocytes, LDH,zinc concentrations in the effusions for empyemata, Cus/Cue, andZns/Zne (ratios >5.0) were excluded. When the correlations were checkedseparately for the set of benign cases and the set of malignant cases, the
Copper and Zinc in Pleural Effusions and Sera 29
Biological Trace Element Research Vol. 78, 2000
*Units for the clinical laboratory parameters given in Table 3.
Table 4Least Squares Slopes, Intercepts, and Correlation Coefficients r2
(in Parentheses) for the Linear Correlations Between Pairs of ClinicalParameters Determined in Pleural Effusions
30D
omej et al.
Biological Trace E
lemen
t Research
Vol. 78, 2000
Table 5Least Squares Slopes, Intercepts, and Correlation Coefficients r2 (in Parentheses) for the Correlations
Between Clinical Parameters, the Concentrations of Copper in Effusions and Sera, the Concentrations of Zincin Effusions and Sera, and the Ratios of the Concentrations of Copper (Zinc) in Sera and Effusions
*Without empyemata.
correlation coefficients did not change appreciably. Correlations with highstatistical significance for the entire set remained highly significant for thebenign and the malignant sets and weak correlations remained weak.
Total protein in the effusions was strongly correlated with the con-centrations of copper in the effusions (r2 = 0.42) and the concentrationsof zinc in the effusions (r2 = 0.34) but not with the concentrations of theseelements in the sera (Table 5). Copper and zinc in body fluids are largelyprotein bound, and protein-rich effusions are expected and were foundto possess high concentrations of these elements. The concentration of cop-per in the effusions is also highly correlated with the concentration ofceruloplasmin in the effusions (r2 = 0.26). This correlation is also notunexpected, because ceruloplasmin functions as the copper-carrying pro-tein in blood. Total protein is also highly correlated with the concentra-tion ratios for Cus/Cue and Zns/Zne.
CLINICAL CONCLUSIONS
Our study indicates that the concentrations of zinc and copper deter-mined in sera and in the effusions, the serum/effusion ratios for copperand zinc, and the eight clinical laboratory parameters (total protein, pH,leukocyte count, lactate dehydrogenase, glucose, C-reactive protein, cerulo-plasmin, α1-antitrypsin) determined in the effusions cannot discriminatebetween benign and malignant conditions. Although statistically signifi-cant correlations exist between several pairs of these parameters, thescattergrams do not reveal regions characteristic for either benign ormalignant diseases. A single parameter or a pair of parameters is un-likely to separate reliably benign effusions from malignant effusions (21).Multidimensional correlations might provide better discrimination. Dis-crimination on the basis of a single parameter would be clinically desir-able and would certainly be less costly than discrimination requiringseveral parameters. Although means and median values for benign andmalignant effusions are rarely coincident, the means and medians forcopper, zinc, and the eight clinical laboratory parameters are unsuitablediagnostically for the identification of a malignant effusion from a singlepatient. When groups of selected benign and malignant diseases are con-sidered that are associated with effusions, a differentiation with consid-erable certainty is possible [for instance, between cirrhosis or congestiveheart failure on the basis of lactate dehydrogenase (32) and betweenbenign diseases and lung cancer on the basis of Cu/Zn ratios in the sera(19)]. Success and failure will, however, depend on the mix of diseases.The diagnostic problem raised by a single patient with an unidentifieddisease will not be solvable with confidence on the basis of the concen-trations of copper or zinc or the eight clinical parameters.
Of potential clinical significance is the observation that in 52% of the65 sera from patients suffering from benign and malignant effusions, the zinc
Copper and Zinc in Pleural Effusions and Sera 31
Biological Trace Element Research Vol. 78, 2000
concentration is below the low limit of the normal range (600 µg/kg).Withdrawal of the effusions, particularly of the zinc-rich empyemic fluids,may deprive the body of zinc. If a patient, because of inadequate intakeor uptake of zinc or because of depleted body depots of zinc is driftingtoward a zinc deficiency, removal of zinc with the effusions may exacer-bate deficiency and may cause manifestations of deficiency diseases. Zincis known to be necessary for wound healing and to be a cofactor for sev-eral hundred enzymes. Consequently, supplementation of such patientswith appropriate zinc compounds should be considered. Suggestions tostudy the therapeutic role of zinc in cancer patients can be found in theliterature (20).
ACKNOWLEDGMENT
This research was funded by a grant from the Austrian National Bank(Jubiläumsfondprojekt #6786/98).
REFERENCES
1. L. F. Black, The pleural space and pleural fluid, Mayo Clin. Proc. 47, 493–506 (1972).2. A. O. Vladutin, Pleural Effusion. Future Publishing, Mount Kisco, NY, 1986.3. D. E. Dines, L. R. Elveback, and J. T. McCall, Zinc, copper, and iron content of pleural
fluid in benign and neoplastic disease, Thorax 27, 368–371 (1972).4. D. E. Dines, L. R. Elveback, and J. T. McCall, Zinc, copper, and iron contents of
pleural fluid in benign and neoplastic disease, Mayo Clin. Proc. 49, 102–106 (1974).5. K. E. Shepherd, Diagnostic value of zinc levels in pleural effusions, Am. J. Med. 83,
1003–1004 (1987).6. K. E. Shepherd, Diagnostic value of serum to pleural fluid zinc ratios in pleural effu-
sions, Chest 95, 707 (1989).7. C. Yenisey, M. Fadiloglu, B. Onvural, and F. O. Erer, Clinical evaluation of copper and
ceruloplasmin levels in effusions of malignant and benign origin, Biochem. Soc. Trans.23, 606S (1995).
8. F. Teksen, D. Mungan, A. Sayal, Z. Misirligil, A. Aydin, L. Gürbütz, et al., Serum andpleural fluid selenium, copper, zinc, and magnesium levels in malignant and non-malignant pleural diseases, Respiration 63, 25–27 (1997).
9. W. Domej, M. Krachler, C. Schlagenhaufen, M. Trinker, G. J. Krejs, and K. J. Irgolic,Trace elements in pleural effusions, J. Trace Elements Med. Biol. 11, 232–238 (1997).
10. M. Krachler, W. Domej, and K. J. Irgolic, Trace elements in pleural effusions caused bybenign and neoplastic conditions, in Metal Ions in Biology and Medicine, P. H. Collery,P. Brätter, V. Negretti de Brätter, L. Khassanova, and J. C. Etienne, eds., John LibbeyEurotext, Paris, Vol. 5, pp. 603–607 (1998).
11. M. Franciolli and A. Rosenmund, Eisen und eisenbindende Proteine in der Differen-tialdiagnose von Pleuraergüssen, Schweiz. Med. Wochenschr. 119, 785–790 (1989).
12. F. K. Paddock, The diagnostic significance of serious fluids in disease, N. Engl. J. Med.223, 1010–1015 (1940).
13. Boehringer Mannheim, TP Gesamt Eiweiß (August 1993).14. Boehringer Mannheim, CRP Tina-quant (June 1996).15. Behring Diagnostics GmbH, N-Antisera gegen Human-Transferrin, -Haptoglobin,
-Coeruloplasmin und Hämopexin (November 1997).16. Behring Diagnostics GmbH, N-Antisera to Human alpha-1-Antitrypsin and alpha-2-
Macroglobulin (March 1997).
32 Domej et al.
Biological Trace Element Research Vol. 78, 2000
17. Boehringer Mannheim, LDH optimiert (July 1996).18. S. Caroli, A. Alimonti, E. Coni, F. Petrucci, O. Senofonte, and N. Violante, The assess-
ment of reference values for elements in human biological tissues and fluids: a sys-tematic review, Crit. Rev. Anal. Chem. 24, 363–398 (1994).
19. M. Diez, F. J. Cerdan, M. Arroys, and J. L. Balibrea, Use of the copper/zinc ratio inthe diagnosis of lung cancer, Cancer 63, 726–730 (1989).
20. B. F. Issell, B. V. Mac Fadyen, E. T. Gum, M. Valdivieso, S. J. Dudrick, and G. P. Bodey,Serum zinc levels in lung cancer patients, Cancer 47, 1845–1848 (1981).
21. R. W. Light, M. I. Mac Gregor, and P. C. Luchsinger, Pleural effusion: the diagnosticseparation of transudates and exudates, Ann. Intern. Med. 77, 507–513 (1972).
22. R. W. Light, M. I. Mac Gregor, Jr., W. C. Ball, and P. C. Luchsinger, Diagnostic sig-nificance of pleural fluid pH and PCO2, Chest 64, 591–596 (1973).
23. R. W. Light, Pleural Diseases, 3rd ed., Williams & Wilkins, Baltimore, MD, pp. 45–46(1995).
24. F. Rodriguez-Panadero and J. Lopez Mejias, Low glucose and pH levels in malignantpleural effusions, Am. Rev. Respir. Dis. 139, 663–667 (1989).
25. R. W. Light, Y. S. Erozan, and W. C. Ball, Cells in pleural fluid: their value in differ-ential diagnosis, Arch. Intern. Med. 132, 854–860 (1973).
26. R. W. Light and W. C. Ball, Lactate dehydrogenase isoenzymes in pleural effusions,Am. Rev. Respir. Dis. 108, 660–664 (1973).
27. F. Wroblewski and R. Wroblewski, Clinical significance of lactic dehydrogenase activ-ity of serous effusions, Ann. Intern. Med. 48, 813–822 (1958).
28. F. Wroblewski, Clinical significance of alterations in lactic dehydrogenase acitivity ofbody fluids, Ann. J. Med. Sci. 234, 301–312 (1957).
29. F. Wroblewski, Mechanisms of alterations in lactic dehydrogenase activity of bodyfluids, Ann. NY Acad. Sci. 75, 322–338 (1958).
30. F. Wroblewski, Significance of alterations in lactic dehydrogenase activity of body flu-ids in diagnosis of malignant tumors, Cancer 12, 27–39 (1959).
31. M. V. de Torregrosa, Results of lactic dehydrogenase determinations in benign andmalignant effusions, Am. J. Med. Sci. 238, 552–556 (1959).
32. R. J. Erickson, Lactic dehydrogenase activity of effusion fluids as an aid to differen-tial diagnosis, JAMA 176, 794–796 (1961).
33. R. W. Light, W. M. Girard, S. G. Jenkinson, and R. B. George, Parapneumonic effu-sions, Am. J. Med. 69, 507–511 (1980).
34. H. W. Berger and G. Maher, Decreased glucose concentration in malignant pleuraleffusion, Am. Rev. Respir. Dis. 103, 427–429 (1971).
35. D. E. Potts, M. Wilcox, and J. T. Good, The acidosis of low-glucose pleural effusions,Am. Rev. Respir. Dis. 117, 665–671 (1978).
Copper and Zinc in Pleural Effusions and Sera 33
Biological Trace Element Research Vol. 78, 2000
