obesity and genomics in the netherlands
TRANSCRIPT

Chapter 10Obesity and Genomics in the Netherlands
Michiel Korthals
Introduction
In this chapter the Dutch debate on the main causes of obesity is described andreviewed as well as the current initiatives adopted by the Governament and privateinitiatives to tackle the problem. The first part gives an overview of the Dutch situa-tion. The second part of the chapter reports on expert opinions on the possibility toaddress the problem of obesity through different approaches. Several Dutch expertsand practitioners are invited to express their views on the problem of rising rate ofobesity in the Dutch context and their opinion on the possible ways to tackling itthrough cure, prevention, and regulation. The three constellations of responsibilitiesand causes, as described in the previous chapters in this book, have been used toprompt a debate with about the genomics approach to obesity by a group of Dutchexperts, addressing more specifically the possibilities and problems.
Overview of the Dutch Situation
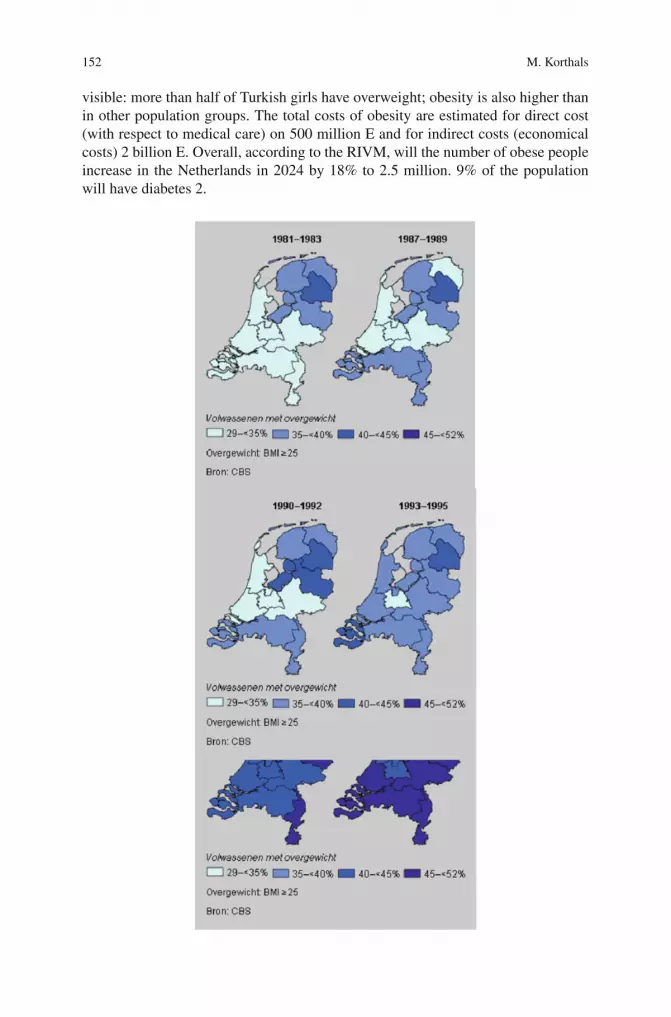
Just like other European countries, the Netherlands show rising numbers of over-weight and obese people. Approximately in 1990 one in three Dutch inhabitantsis overweight and one in ten is obese. For 2008 the numbers are: 40% of the menand 30% of the women are having overweight and 10% of the men and 12% of thewomen are obese (CBS 2008, p. 113). As everywhere, overweight and obese peo-ple are not equally spread over the population. In the developed world and contraryto the developing world, lower income groups are overrepresented, but also peo-ple that live only one or two generations in the Netherlands. In the Netherlands ofthe 2–21 year old children 13% of the boys and 14% of the girls have overweight(Fredriks et al., 2000; figures from www.cbs.nl)). In the big cities and in places withchildren from non-Dutch parents the overweight rate is even higher (De Wilde et al.,2003). In particular under girls from Turkish parents a strong trend to overweight is
M. Korthals (B)Department of Applied Philosophy, Wageningen University, Wageningen, The Netherlandse-mail: [email protected]
151M. Korthals (ed.), Genomics, Obesity and the Struggle over Responsibilities,The International Library of Environmental, Agricultural and Food Ethics 18,DOI 10.1007/978-94-007-0127-4_10, C© Springer Science+Business Media B.V. 2011
152 M. Korthals
visible: more than half of Turkish girls have overweight; obesity is also higher thanin other population groups. The total costs of obesity are estimated for direct cost(with respect to medical care) on 500 million E and for indirect costs (economicalcosts) 2 billion E. Overall, according to the RIVM, will the number of obese peopleincrease in the Netherlands in 2024 by 18% to 2.5 million. 9% of the populationwill have diabetes 2.
10 Obesity and Genomics in the Netherlands 153
However, it is not that in the Netherlands a non-obese life style is difficult tokeep up with compared with for example the United States, with an obesity rate ofone in third (32% male and 37% female (WHO)). With respect to consumption offood, fruit and vegetables are rather easy to get and they are not more expensivethan calorie rich food. Moreover, there is a long standing habit of going by bike towork or school (although that is changing) which means that people are encouragedto perform exercises daily (see for more information on the USA, Stearns, 2002).
These habits can be easily connected with the way food and health is seen byDutch consumers; it is illuminating to refer to several comparative studies on thisissue. The most fundamental idea of those studies is that food choices are part of afood- and lifestyle and express and explicate the identity of the person making thatchoice. The different food- and lifestyles comprise different conceptions of foodand health Payer, (1998); Grünert ,(1997). In general, we can distinguish differentways of relating to food, such as the dichotomy expressed in whether one eats tolive or lives to eat (Stearns, 2002). Food choices are generally based on attraction ordisgust of which Rozin and Fallon (1987) state: ‘Disgust is triggered not primarilyby the sensory properties of an object, but by ideational concerns about what it is,or where it has been. In fact, we conceptualize disgust as a distinct form of foodrejection, different from rejections based on bad taste or on fear of harm to thebody.’
In the Netherlands, just like other countries, one can discern a multiplicity offood- and lifestyles that represent multiple – sometimes unconventional – formsof mutual solidarity and socialization. Sociologists such as Giddens (1991), Beck(1990) and Schulze (1992) identify this as typically for Western people living in alate or postmodern society in which individualization is the main structural trend.Food- and lifestyles are in a state of flux, to a significant degree due to technolog-ical and scientific developments, such as food innovations, computer technology,modern means of communication, or new means of transport. It is quite surprisingthat these studies all agree upon a similar general frame of four or five foodstylesand they are also characteristic for the Netherlands, although the proportions aredifferent compared with for example France and Italy.
Rozin et al. (1999) have done extensive research on the different conceptions thatpeople in different cultures have with respect to food and health. They conclude that‘generally, the group associating food most with health and least with pleasure isthe Americans, and the group most food–pleasure-oriented and least food–health-oriented is the French.’ Rozin et al. (1999) emphasize that the pleasure orientationtowards food and the minor role of health considerations is probably an importantfactor in the explanation of the French paradox, i.e., the fact that overweight andobesity is less prevalent in France although fat intake is as large as in the US. ‘Oneaccount of the French–American contemporary differences has to do with differenttraditional eating patterns in the two countries, with a French emphasis on mod-eration and high quality, and an American emphasis on high quantity.’ The Dutchconsumers are to be placed somewhere in the middle; the Italians agree with theFrench.
On the basis of a structural theoretical background Douglas (1982) has analysedempirically four broad types of food styles or food cultures. She distinguishes a tra-ditional (hierarchical) food culture, where food is seen as unspoilt nature (regional,

154 M. Korthals
authentic cuisine); an exclusive food (individualist) culture, where food counts as anexclusive identity item (high culture); an information and fast food (egalitarian) cul-ture, where food is viewed as fuel; and an eclectic (individualist) food culture, wherefood is seen as part of an enlarged global conversation of a plurality of cuisines (slowfood). These cultures or styles are confirmed by the work of the Dutch marketing andresearch company Motivaction (www.cbs.nl, www.motivaction.com). Motivactiondeveloped a research instrument to disclose value orientation of Dutch consumersand concludes on the basis of longitudinal studies since 1997 that four styles in moreor less equal proportion are dominant: the traditional, egalitarian, self-realizationand responsible life style. Only for the egalitarian food style is health a dominantissue in choosing food items. This means also that strategies from the side of gov-ernment or industry to eat healthy will only be successful with these categories ofconsumers.
It is striking that all the elements of the three constellations, behaviour, environ-ment and body, are present in the Dutch governance of obesity, with emphasis onthe first two. Genomics applications are not used on a large scale, but see belowfor experts views on the relationship between genomics and obesity. The currentgenomics innovation strategy in the Netherlands favours only certain social institu-tions and values (concepts) vis-à-vis the ones that are available, as is shown in thetable. For other institutions and food- and life styles this strategy is not attractive(Table 10.1).
Table 10.1 The current Dutch nutrigenomics innovation strategy and its implications for existingconcepts of consumers, food styles, responsibilities and obesity discourses
Genomics concepts andapplications and theirattraction for existingconcepts and values
Framing of consumer(food style)(Chapters 8 and 10)
Framing ofresponsibility(Chapter 6)
Discourse(Chapter 3)
Concept of health Egalitarian Individualresponsibility;second one: industry
Behaviour;body
Concept of food Egalitarian Idem idemApplication: testing Active, gene driven Market; second one:
governmentidem
Application: biomarkers Idem idem idemApplication: products Passive Retail; second one:
governmentEnvironment
Role of Stakeholders
Government
The Dutch government took the decision not to regulate the problem itself but askeda self-regulatory body, consisting of the most important stakeholders, to organize themeasures against obesity. Interesting enough however, is that the Dutch consumer
10 Obesity and Genomics in the Netherlands 155
organizations refused to take part in this covenant. The covenant of 2006 stimu-lates voluntary actions that improve a ‘healthy life style’, including healthy foodand fitness. Younger and elderly people seem to be the target of those programs.However, the minister of health want to give the highest priority to prevention andtherefore he will propose a system of reimbursement of costs made for health andfitness programmes, so they will paid by public money. (Antwoorden op de vragenvan de vaste commissie voor Volksgezondheid, Welzijn en Sport, over de kabinet-snota Langer gezond leven; Ook een kwestie van gezond gedrag (Tweede Kamer,vergaderjaar 2003–2004, 22 894, nr. 20).
Health Policy: Insurance Companies
The structure of the health assurances system in the Netherlands is now so orga-nized, that assurance companies also give reduction of premiums, but not in thebasic part, which is common to all companies, but in the additional assurancesschemes. In these last schemes, companies are not obliged to accept everyoneand they can differentiate sharply between what they call healthy and unhealthypersons. Moreover, they want all to incorporate health prevention measures, like fit-ness and sport courses; according to the present minister of health this should alsohappen with the basic part of the health assurance system. The companies mostlyagree with the liberal Minister Hans Hogervorst (of the second cabinet Balkenende,2004–2007); he delivered a speech on 14-04-2005, in Rotterdam, saying: ‘I don’tthink that there exists something like a right on an unhealthy life. This don’tsound very liberal, but I believe that one can’t bring together living a life ofrisks and becoming ill and accordingly expect that one can use our health caresystem.’
Industry and Retail
Most large food companies are participating in the self-regulatory organization orCovenant, since 2006; to participate costs quite a lot, so small scale companies cannot afford to participate (Dagevos and Munnichs, 2007). The covenant stresses indi-vidual responsibility of consumers and stimulates consumers to exercise more, andto eat healthy by a self regulatory system of branding. The system uses phraseslike ‘I choose consciously’ and ‘the healthy choice’. It is striking that for examplecucumber, according to all scientific criteria a very healthy product, don’t get theapproval of this system. Packaged soup and other processed food get the approvaland many products with as yet not proven health claims, like Actimel, because intheir category they are less unhealthy; it would be more integer and transparentif the system used phrases like ‘the healthier choice’. The organization is there-fore seriously flawed and it remains to be seen in how far consumers trust thesystem.
156 M. Korthals
NGO’s
In the Netherlands there is not an effective organisation with the same kind of polit-ical strategy as the American National Association to Advance Fat Acceptance(NAAFA). In Chapter 4 we already mentioned the Dutch counterpart for theNAAFA, the ‘Formidable Movement’ (Beweging van Formaat), which is a muchsmaller organisation. It thus appears that a consistent campaign for fat acceptancecannot be pursued by organisations that strive to cater to the needs of the majorityof obese and overweight people.
NAAFA’s rejection of the disease label of obesity can be contrasted with themore ambivalent viewpoint of the Dutch Obesity Association (Nederlandse ObesitasVereniging), which endorses the status of obesity (and overweight) as a disease onrather pragmatic grounds: ‘Within the Dutch Obesity Association we prefer to referto overweight as a chronic condition, because somebody who has gained overweightwill only very rarely lose it again. Treatments have very low percentages of success.’(Dutch Obesity Association website: www.dikke-mensen.nl). Here the disease sta-tus of obesity (overweight) is supported not to argue for the urgency of treatmentbut to caution against unrealistic expectations of treatment! The Association appar-ently does not want to make a strategic choice for ‘fat acceptance’ only: ‘For theDutch Obesity Association it does not matter [. . .] whether you have accepted yourweight or whether you engage in a daily struggle with the scales. We are at yourservice’ (Dagevos and Munnichs, 2007). Nonetheless, some board members of theDutch Obesity Association share the main tenets of the counter discourse on obe-sity (see Jeurissen and van Spanje, 2001). The association wants to correct biases ofoverweight people, although is doesn’t want to idealize obese people and to neglectthe physical and psychological problems they have. There are not against medical-isation or geniticalization, mostly because it rehabilitates their own respectabilitywhen it is shown that being obese is not their personal fault.
Schools
In the Netherlands schools mostly do not organize meals for the approximately750,000 children that visit them daily, but they still have considerable influenceon eating patterns of children, for example by organizing what they call a kind ofin between at the middle of the morning, mostly around 11:00. This ‘n between’stimulates kids to bring with them chocolate bars, chips and energy dense drinks.Schools also organize school milk for the lunch, thanks to the strong lobby of themilk associations that have a lot to say in what type of milk and how much.
Parents have started school movements like ‘Time for eating’ to organize betterand more informative school menu times, by introducing cooking lessons duringlunchtime. Others are busy in getting kids more exercise, by paying attention toschool playfields and safe bicycle pathways to and from schools (Tijdvooreten.nl).However, these are initiatives from below and initiated or facilitated by low levelgovernmental agencies.

10 Obesity and Genomics in the Netherlands 157
Experts on Obesity and Genomics in the Netherlandsand the Three Discourses
We organized a round table discussion with several experts on obesity in theNetherlands in which we asked their opinion about the three discourses/ constel-lations and about future scenarios (June 2003). The science scientific experts werefrom biology and human genetics; community genetics and epidemiology; nutri-tional research on metabole syndrome and cell research; population genetics andgenetic diversity and finally genetics and pharmacogenetics. We also invited thepresident of the Dutch Obesitas Vereniging, a voluntary organisation of overweightand obese people.
The Three (Plus One) Discourses
We presented first the three discourses which ascribe a specific meaning to obesity,point out causes, remedies and responsible actors, lay down the rules for what canbe said and what cannot. Discourses are not simply factual descriptions of exist-ing states of affairs. They have a practical point in so far as their diagnoses locateresponsibilities and accountabilities, and indicate the direction for finding solutionsto this problem. All three agree that obesity constitutes a pressing problem, butthen continue by focusing on different causes of and solutions to this problem. Thefirst discourse centres around individual actions (behaviour), the second gives cen-tre stage to environmental influences, and the third discourse focuses on biologicalcauses in the body. As a result, discourse I individualizes and moralizes; discourseII moralizes but does not individualize; and discourse III finally individualizes butdoes not moralize.
Response of the Experts
The science experts agreed that the three discourses covered the Dutch landscaperather completely, but there were some doubts about aspects, like the lack of dif-ferentiation between genetics and genomics (see below), the shifting meaning ofresponsibilities and the role of new practices, like screening and the emergence ofnew patient and consumer groups, like fat people. They also liked the easy dis-cernability of the three; so one can speak with respect to the first discourse ofindividualisation, with respect to the second of politicization and with respect tothe third of biologicalization.
The community genetics expert argued that responsibility for public healthis very fragmented organized compared with the USA (by Centres for DiseaseControl and Prevention, CDC; www.cdc.gov), and United Kingdom has theDepartment of Health (DH; www.dh.gov.uk). In the Netherlands we havethe Gemeentelijke Gezondheids Dienst (GGD; Municipal Health Service), hetRijksinstituut voor Volksgezondheid en Milieu (RIVM) and the National Instituut

158 M. Korthals
voor Gezondheidszorg en Ziektepreventie (NIGZ; National Institute for Health andPrevention). It is very unclear which institutions in the Netherlands have respon-sibility for prevention. Some insurance companies like Achmea (Achmea HealthCenters) organize on a voluntary basis already preventive activities.
For many individuals it is often very easy to discriminate fat people, because youfeel morally superior in morally disapproving of fat people. This means that the firstdiscourse that stresses individual responsibility is strongly anchored in daily life ofpeople and will not easy be changed. Others stressed the differences between ethnicgroups in approving or disapproving thin or thick bodies.
Most of the experts underlined the future of genomics is more uncertain thanmany think. It is probably not the case that genomics in the end will produce foreveryone in particular a clear message how to life healthy. The research is extremelydifficult and costs a lot of money which most government and companies are notwilling to pay. There is now interesting research on monogenetic afflictions but mostdiseases are multifactorial.
The difference between genetics and genomics was also extensive discussed.Most did agree that genomics compared to genetics is a large scale researchenterprise, but also that genomics emphasises the interaction between genes andenvironment and also life style, which also means that interdisciplinarity andcomplexity is at the core of genomics.
The Future of Genomics and Obesity
First, the experts made it clear that in the Netherlands there is a rather strict regimewith respect to screening of the population, In fact, only under very restricted condi-tions is such an enterprise thing possible. But the experts also stressed that familiarresearch can do a lot. Indeed, prevention is rather neglected in the Netherlands, andhere again only preventive research is possible when there is some outlook on a ther-apy. Preventive research on nutrition is very costly and done only by a few in theworld. This implies that the hopes a fast application of genomics results in healthcare or in coping with obesity are utopian.
According to the patient group, the introduction of genomics can be a relieve forobese people because they eliminate the bases for blame or guilt.
More and more the body is seen as something to be managed (60% of the womenand 50% of the man is dieting according to one or another scheme). The relationshipbetween private and public health is seen by most an important item, where slowlythe emphasis is shifted towards the individual. In the future more privatised healthcare will be delivered, with its concomitant effect of more responsibility to privateindividuals.
However, the professions can also concentrate more on prevention and in par-ticular general practioners could be more alert to incorporate food and life stylerecommendations on the basis of genetic and genomics services in their dailypractice.

10 Obesity and Genomics in the Netherlands 159
More liberal ruling of screening is not seen as a realistic option in the near future,as is more strict government intervention to decrease the number of obese people.
Conclusion
In the Netherlands the attitude towards food as an health item is dominant in onelife- and food style (app. 25% of the population), and in the other styles, food ismore connected with being social, responsible, pragmatic or self-determined. Forstrategies to implement (nutri) genomics products, services and other innovatorydevices it is therefore questionable in how far an orientation exclusively towardhealth can influence adherents of these other life styles.
With respect to the expert discussion, the three discourses were seen by theexperts as useful tools in structuring the field of obesity, but they had their doubtsabout fast applications of genomics services and products in Dutch health caresystem. Individualisation, Politicalisation and Biologicalisation seem to be rele-vant catchwords of three different approaches. However, all experts stressed theemergence of new responsibilities, new practices, and new groups involved inthe emerging services and products. They also underlined the difficulties withundertaking research, in producing practical applications, and with regulatingnew responsibilities. Finally, the relationship between public health and privateresponsibilities was put on the agenda; we will tackle this issue in Chapter 13.
References
Beck, U. (1990), Risk Society. London: SageCBS, (2008), Statistisch Jaarboek, Den Haag: CBSDagevos, H. and G. Munnichs (2007), De Obesogene Samenleving, Den Haag: Cahiers
Biowetenschappen en Maatschappijde Wide, J.A., B.J.C. Middelkoop, S. van Buuren and P.H. Verkerk (2003), Overgewicht bij Haagse
schoolkinderen, Epidemiologisch Bulletin, 38, 4, 12–23Douglas, M. (1982), Food as a system of communication. In: Douglas M.(ed), The Active Voice.
London: Routledge, pp. 81–118Fredriks, A.M., S. Buuren van, J.M. Wit and S.P. Verloove-Vanhorick (2000), Body mass index
measurements in 1996–1997 compared with 1980, Archives of Disease in Childhood, 82,107–112
Giddens, A. (1991), Modernity and Self-identity. Stanford, CA: StanfordGrunert, K. (1997), Food related lifestyle: Results from three continents, Asian Pacific Advances
in Consumer Research, 2, 64–69Jeurissen, E. and M. van Spanje (2001), Rondom dik: Zin en onzin over zwaarlijvigheid.
Amsterdam: AmboPayer, L. (1998), Medicine and Culture. New York, NY, Henry HoltRozin, P. and A. Fallon. (1987), A perspective on disgust, Psychological Review, 2, 14Rozin, P., C. Fischler, S. Imada, A. Sarubin and A. Wrzesniewski (1999), Attitudes to food and the
role of food in life in the U.S.A., Japan, Flemish Belgium and France: Possible implications forthe diet–health debate, Appetite, 33, 2, 163–180, 64–65
Schulze, G. (1992), Die Erlebnisgesellschaft. Kultursoziologie der Gegenwart. Frankfurt: Campus,1992
Stearns, P. (2002), Fat History: Bodies and Beauty in the Modern West. New York, NY: New YorkUniversity