malaria and primary education: a cross-country analysis on
TRANSCRIPT

MALARIA AND PRIMARY EDUCATION: A CROSS-COUNTRY ANALYSIS ONREPETITION AND COMPLETION RATES
Josselin Thuilliez
De Boeck Supérieur | « Revue d'économie du développement »
2009/5 Vol. 17 | pages 127 à 157 ISSN 1245-4060ISBN 9782804162443DOI 10.3917/edd.235.0127
Article disponible en ligne à l'adresse :--------------------------------------------------------------------------------------------------------------------https://www.cairn.info/revue-d-economie-du-developpement-2009-5-page-127.htm--------------------------------------------------------------------------------------------------------------------
Distribution électronique Cairn.info pour De Boeck Supérieur.© De Boeck Supérieur. Tous droits réservés pour tous pays. La reproduction ou représentation de cet article, notamment par photocopie, n'est autorisée que dans leslimites des conditions générales d'utilisation du site ou, le cas échéant, des conditions générales de lalicence souscrite par votre établissement. Toute autre reproduction ou représentation, en tout ou partie,sous quelque forme et de quelque manière que ce soit, est interdite sauf accord préalable et écrit del'éditeur, en dehors des cas prévus par la législation en vigueur en France. Il est précisé que son stockagedans une base de données est également interdit.
Powered by TCPDF (www.tcpdf.org)
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

127
Malaria and Primary Education:A Cross-country Analysis on
Repetition and Completion Rates
Josselin Thuilliez *
This paper explores the link between P. falciparum malaria – the causative agent of most malaria-related morbidity and mortality – and primary education in terms of school performances at mac-roeconomic level. Cross-country regression analysis shows that the relationship between schoolresults (measured by repetition and completion rates) and the P. falciparum malaria index isstrong. The results imply that the achievement of the educational Millennium DevelopmentGoals will require more than just focusing on expenditure in primary education. This does notmean that resources allied to education are unnecessary, but simply that increasing resources ineducation and improving education resources management alone are unlikely to be sufficient.This paper suggests that health conditions, especially diseases such as malaria that could alterchildren’s cognitive capacities, should be taken into account much more seriously. We also see theneed to place emphasis on research that will improve the quality of interventions to preventmalaria. Specific education expenditure combined with health policies should be investigated fur-ther as a means of tackling malaria.
Key words:malaria incidence, human capital, development.
JEL Classification: O15, I10, I20.
1 INTRODUCTION
Malaria ranks among the foremost public health and development issues fac-ing tropical countries. The numbers are staggering: an estimated 41% of theworld population lives in malarial areas, and 300 to 500 million clinical cases
* Post-Doc. École des Hautes Études en Santé Publique – Département SHS-CS, CAPPS– avenue du Professeur-Léon-Bernard – CS 74312 – 35043 Rennes [email protected]
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

128 Josselin Thuilliez
are recorded every year. Malaria kills between 700,000 and 2.7 million peopleper year, 75% of whom are African children. Around 30% of external medicalchecks and 20-40% of hospitalisations in Africa are due to malaria.
Why are malarious countries poorer? Why do they develop slower thannon-malarious countries? A series of papers have explored the link betweeneconomic development and malaria.1 Contrary to other tropical diseases, sincethe failure of eradication efforts in the 1980s, malaria is widely described asan unavoidable effect of tropical location and natural forces (heavy rains,flooding). Recent empirical studies have used malaria as an exogenous vari-able in regression analyses of economic growth and income level on malariaendemicity. Nevertheless, even today, little is known on the transmissionchannels.
Sachs and Gallup (2001), using a malaria exposure index defined as thepopulation fraction at risk of contracting falciparum malaria in a country,show that poverty is not a leading cause of malaria ceteris paribus. The inten-sity and distribution of the disease are determined by the ecological condi-tions enabling the reproduction and development of malarial vectors.Working within a cross-country regression framework, the authors found thatcountries with intensive malaria are poorer and grew 1.3% less per person peryear. These results point to a causal link from malaria to poverty ⎯ not viceversa. In contrast, Acemoglu (2002) asserts that malaria “is unlikely to be thereason why many countries in Africa and Asia are very poor today.”2 What-ever conclusions are drawn, malaria plays a now well-acknowledged role as a“killer”, a “weakener”, and an element in this “vicious circle which makes thepoor malarious and the malarious poor” (Watts, 1999).
Using WHO estimates of malaria morbidity, McCarthy et al. (2000) sug-gest that economic development could influence malaria control. Althoughconfirming the dominant role of climate in determining malaria intensity andthe negative correlation between malaria and growth, they also found thataccess to rural health care and income equality influence malaria morbidityafter controlling for climate. This raises the problem of the endogeneity ofmalaria in respect to growth and the robustness of results in this field ofresearch.
1 See for instance McDonald (1950), Barlow (1967), Newman (1968), Gomes (1993) andAudibert et al. (1999).
2 Note that the relationship between malaria and growth is not the primary focus of thisstudy.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 129
A natural way to study growth is to identify and quantify all the possibletransmission channels (Rodrik and Rodriguez, 2000). As human capital for-mation and accumulation have been shown to be key variables in nation-levelgrowth and development, this paper explores the impact of malaria on humancapital development in children. As basic education and health are ends inthemselves, this paper contributes to understand the suffering of individualsand communities in affected areas. We investigate this issue using a datasetfrom Samer Al-Samarrai (2006) to build a cross-country regression frame-work for assessing the impact of a 1994 index of malaria endemicity on repe-tition and completion rates in 1996. We control for other variables alreadyused in the literature on the determinants of primary education quality. Weadd indicators of general health conditions, governance and climate to themodel, and check the robustness of our results via a series of tests. Our resultssuggest that high levels of malaria endemicity increase repetition rates anddecrease completion rates, ceteris paribus. These findings fill part of the gapbetween microeconomic assessments of the impact of malaria and macroeco-nomic assessments identifying one of the macroeconomic channels throughwhich the disease impacts development.
The next section gives the conceptual framework of the study and a sum-mary of previous literature on the link between malaria and school perfor-mances. Section 3 describes the variables and methodology used in the study.Section 4 presents the results of our cross-country regressions, while section 5goes on to provide robustness checks. Finally, section 6 discusses the results,and draws our conclusions.
2 BACKGROUND AND PREVIOUS LITERATURE
The link between malaria and school performances: medical and empirical evidence
Malaria is a parasitic disease transmitted by anopheles mosquitoes, and whichresults from biological developments of protozoal parasites. The present studyfocuses exclusively on P. falciparum malaria, which is far more severe thanthe other types of malaria. The incidence and severity of P. falciparummalaria depends on various entomological, environmental and human factors.There are numerous potential combinations between factors. The clinical pre-sentation of malaria varies, among other factors such as personal behavior orgenetic characteristics, according to immune status. Populations exposed to
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

130 Josselin Thuilliez
frequent infections acquire partially labile protective immunity. Level ofimmunity affects not only the mortality and severity of malaria but also non-complicated malarial attacks. Therefore, paradoxically, it is more difficult toassess the real burden of the pathology in highly endemic areas where peopleare more exposed to infected-mosquito bites, since parasitization is notdirectly and proportionally associated with apparent clinical symptoms. Con-versely, diagnosis is supposed to be easier in low-endemic areas where, in theabsence of immunity, symptoms are caused directly by infection. In children,acquired immunity does not play an efficient protective role until age 5-6years, even in highly endemic areas. This is part of the reason why malaria isa major threat to child survival. In 2000-2003, malaria accounted for 8% of the10.6 million deaths recorded in children under 5 (WHO-CHERG), making itthe third leading cause of mortality in under-5s. 94% of global child deathsattributable to the malaria occur in Africa (Bryce et al., 2005). In holo-endemic areas of Africa (where transmission is said to be stable), the diseaserepresents 20 to 25% of all-causes mortality in the 0-5-years age band and25% of paediatric hospitalizations, and lethality is around 15%. The depres-sion of acquired immunity during pregnancy means that malaria also causesacute prenatal disease, with severe health consequences for both mother andchild.3
A number of studies have emphasized the consequences of malaria onchildren’s behavioral and cognitive development, learning performances, andschool attendance. Nevertheless, the relationship is only beginning to beexplored. Figure 1 schematically illustrates the direct links between malariaand school performances. Other socioeconomic externalities may contributeto amplify the impact of malaria on school outcomes.
In 1917, the Texas State Health Department, the University of TexasExtension Department and the International Health Board made a firstattempt to measure the effects of malaria on physical and mental develop-ment (Kelley, 1917). One interesting conclusion was that being cured frommalaria leads to an immediate increase in physical and mental development,but the article does not give any explanation on the causal relationship. More-over, the method and data used in this study remain crude at best. McDonald(1950) also underlines the consequences of malaria on child education throughabsenteeism and chronic infections. From there until the 1980s, research in
3 For a historical perspective of childhood malaria mortality in Africa, see Snow et al.(2001). For a review of the economic effects of malaria in pregnancy, see Worrall et al.(2007).
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 131
this field did not progress further, and the indirect as well as direct conse-quences of malaria on child development remained neglected.
In a recent unpublished paper taking a historical perspective, Bleakley(2006) looks at the malaria eradication campaigns led in the USA (1920) andin Brazil, Colombia and Mexico (1950) to assess the impact of childhood expo-sure to malaria on labor productivity. Using a cohort-level dataset based onmicroeconomic data, Bleakley found that cohorts born after the eradicationcampaign had higher literacy at adulthood than the previous generation.Childhood malaria exposure had similar effects on adults across the fourcountries studied.
Holding and Snow (2001) reviewed the evidence on the impacts ofP. falciparum malaria on performance and learning through neurologicalimpairment after cerebral malaria, brain insults during malaria, complicationsof clinical cases, malaria induced-anaemia, nutritional effects, foetal exposureto malaria, low birth-weight, and prematurity. For instance, on a total of 1,854Kenyan children with cerebral malaria, they found that 302 died (16.3%) and248 (16% of survivors) were reported as presenting neurological sequelae atdischarge. These figures do not mean that the sequelae will be accompaniedby widespread impairment of cognitive functions or learning capacities, butthe association seems to exist. Our study attempts to quantify this impact ofmalaria on school performance at macroeconomic level. Another review of evi-dence (Kihara et al., 2006) found similar conclusions and gave further detailson the cognitive impacts of malaria. Malaria infection is known to lead to def-icits in attention, memory, visuo-spatial skills, language, and executive func-tions. These deficits are not only caused by cerebral falciparum malaria, butalso appear to occur in less severe infections. Finally, Holding and Kitsao-Wekulo (2004) outlined priorities for future research in this field. The fullrange of potential pathways to impaired development needs to be investigatedthrough different adapted methods. Understanding the source of the variabilityin outcome (differences in socioeconomic status, presence of other infections,age, environment) could also help identify malaria-specific impact, childrenmost at risk, and modalities for intervention.
Two case studies realized in Sri Lanka (Fernando et al., 2003) revealedthat initial and repeated malaria infections have an adverse impact on schoolperformances (measured by test scores in mathematics and language aftercontrolling for socioeconomic variables such as the education level of parents,household income, habitation types and nutritional status.) For instance, in571 schoolchildren aged 6-14 years, a child who had experienced more thanfive attacks of malaria would score roughly 15% less than a child who had
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

132 Josselin Thuilliez
experienced less than three attacks of malaria. The cognitive performance atschool entry of 325 grade-1 schoolchildren aged 5-6 years in two endemic dis-tricts decreases as the number of malaria infections increases. These studiessuggest that malaria in malaria-endemic areas adversely impacts cognitivecapacities not only at school entry but also during primary schooling.
Malaria can have non-cognitive consequences through school absentee-ism, general health conditions, or other socioeconomic conditions and behav-iors associated with the disease. For instance, in a case study led in Kenya,Brooker et al. (2000) attributed 13-50% of medically-related school absencesto malaria. Leighton and Foster (1993) also provide evidence on the numberof school days lost due to malaria in Kenya and Nigeria. In Kenya, primaryschool students were considered to miss 11% of the school year (20 schooldays missed per child per year) due to malaria, while in Nigeria the figure var-ied between 2% and 6% of the school year (3 to 12 days per year per student).Kimbi et al. (2005) estimated that in the Muea area in Cameroon, 53 out of144 (36.8%) malaria-infected children lose 0.5 to 14 days of school (averaging1.53 schooldays). The social and economic costs of the disease can amplifyabsences: parents can retain children at home to take care of younger siblingswho are sick or perform other household or productive tasks. This may beespecially true in agricultural economies due to coping mechanisms and thefact that farming activities are a family concern (Chima et al., 2003). Never-theless, these conclusions remain speculative, since we still know very littleabout the impact of malaria on school attendance. Absenteeism in developingcountries stems from numerous factors, many unrelated to malaria.
Malaria is associated with a number of neglected tropical diseases, includ-ing hookworm, schistosomiasis, onchocerciasis, filariasis, dengue fever andtrypanosomiasis. Brooker et al. (2006) suggest that controls on malaria andparasitic helminths in school children could be viewed as essential co-contrib-utors to promoting health among schoolchildren. The incidence of malaria canbe increased by co-infection with the other tropical diseases.
Taken together, these studies tend to emerge a complex relationshipbetween malaria infection, human capital formation, and a large number of riskfactors which themselves may be associated with performance at school. Ourpurpose here is not to exhaustively review the literature on the micro-impactsof malaria on the cognitive and learning capacities of children. We simplyunderline that the few case studies exploring the question conclude that thelink is strong. Microeconomic literature on health also recognizes that physicaland mental health problems can impede children’s human capital accumulation(see, for instance, Currie and Stabile, 2006). Hence, it would be surprising not
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 133
to encounter the impact of malaria at the macroeconomic stage, especiallysince the disease creates other negative external effects that can amplify thephenomenon.
Figure 1: Direct impacts of malaria on school performance (Source: Author)
Conceptual framework of the studyCross-country and panel literature on the determinants of schooling qualitytends to focus on education resources. Increasing investments in basic educa-tion has been seen as a key strategy for achieving the Education For All (EFA)goals (World Education Forum, 2000). Nevertheless, cross-country compari-sons consistently show the link between resources and educational outputs isweak (Al-Samarrai, 2006). Increases in expenditure in primary educationalone are unlikely to be sufficient to achieve the education millennium devel-opment goals. Other variables such as the effectiveness of the public expendi-ture management systems, household spending, and the composition of publiceducation spending may explain this weak link. This study explores anotherpotentially important factor that influences schooling quality in developingcountries and that may contribute to rendering expenditure on primary edu-cation ineffective. We use different datasets in a cross-country and panel
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

134 Josselin Thuilliez
regression framework to estimate the impact of an index of malaria endemic-ity on repetition and completion rates. A novel feature of our work is that weintroduce a proxy for general child health conditions, climate variables andgovernance indicators into the model.
The relationship between school outputs and inputs is generally analyzedwith an education production function, particularly at macroeconomic level.However, health conditions and diseases like malaria that alter cognitive andlearning abilities are not taken into account in macroeconomic studies of thedeterminants of education quality. Following Barro and Lee (2001), we definea highly simplified education production function taking health into account:
Q = Q (F, R, H) + ε (1)
Where Q denotes schooling quality, F, family factors (principally familyincomes), R, public resources used for primary education, H, child health con-ditions, and ε, unmeasured factors influencing schooling quality.
3 DATA AND METHODOLOGY
Dependant variable: primary school repetition and completion rates
Conceptually, education has two main qualitative goals. The first is to developthe cognitive capacities of students. The degree to which systems actuallyachieve this goal is one indicator of their quality. The second element is “edu-cation’s role in encouraging learners’ creative and emotional development, insupporting objectives of peace, citizenship and security, in promoting equality,and in passing global and local cultural values down to future generations”(EFA, Global Monitoring Report, 2005). It is difficult to measure educationquality for a broad number of countries, especially if the second objective isfactored in (Barro and Lee, 2000). A handful number of papers have tackledthis problem. Barro and Lee (2001) provide a panel dataset that includes out-put and input measures of schooling quality from 1965 to 1990. Hanushekand Kimko (2000) also develop cross-country measures of labor force qualitybased on information on international differences in mathematics and scienceknowledge for 1991. Altinok and Murseli (2007) followed a different method-ology to obtain qualitative indicators of human capital (QIHC). First, theycompiled recent surveys led between 1995 and 2003 in a cross-country data-base level covering 105 countries. Second, they updated the Barro and Lee
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 135
(2001) dataset. Third, they gathered all the international surveys on chil-dren’s achievement into a panel dataset spanning the period 1964 to 2005.However, the dataset published by Altinok and Murseli (2007) has not yetbeen intensively used, making it difficult to claim it as a benchmark for com-paring different cross-country studies. Moreover, the panel dataset poolingscores on international tests is highly unbalanced, and the cross-sectionalindicator compiled different years, again making interpretation difficult. Al-Samarrai (2006) proposed to use the simple measures of education qualityavailable through the UNESCO Institute for Statistics website (primary repeti-tion rates, primary completion rates, primary survival rates) which are widelyused to compare school outcomes across countries in international monitoringreports. Since one of our objectives is to compare our results to other studies,we have opted for these measures.
As we are particularly interested in measuring the specific impact ofmalaria on children’s cognitive and learning abilities, we elected to start withprimary school repetition rates which reflect this particular aspect of educationquality. Indeed, despite the fact that repetition rates are sometimes affected byschool and educational policies (such as national regulations), they are moredirectly determined by school results. The choice of this variable combined withour large database will allow us to work with a reasonably-sized sample withgood coverage of developing countries (particularly in Africa) for our regres-sions (from 80 to 84 observations in table 1). Other alternative indicators aretest scores. However, although some cross-country studies have been under-taken using students’ scores on internationally comparable tests of achieve-ment in knowledge, the samples are often downsized due to limited availabilityof internationally comparable data. Recent efforts to define a standardized indi-cator, through MLA (Monitoring Learning Achievement – UNESCO/UNICEF),SACMEQ (Consortium for Monitoring Educational Quality) and PASEC (“Pro-gramme d’Analyse des Systèmes Éducatifs de la CONFEMEN”), still include asmall sample of countries. Primary repetition rates are defined as the propor-tion of pupils enrolled in a given grade at a given school-year at primary leveland who study in the same grade in the following school-year (UNESCO).
In order to take into account other effects of malaria on school results, wealso use primary completion rates as an alternative dependent variable. 4 Thechoice of this variable gives us a smaller size sample due to the lack of data forboth the explained and explanatory variables in the models, but still with
4 See Samer Al-Samarrai (2006) for a discussion on conceptual problems associated withthe use of completion rates.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

136 Josselin Thuilliez
good coverage of developing countries (plus Africa) (from 54 to 55 observa-tions in table 2). Primary completion rates are defined as the total number ofstudents (of any age) in the last grade of primary school, minus the number ofrepeaters in that grade, divided by the total number of children of officialgraduation age (World Bank).
Repetition and completion rates have been widely used to compare schooloutcomes across countries in international monitoring reports.
The P. falciparum malaria indexA major problem when assessing the economic cost of malaria ⎯ at the mac-roeconomic level (Sachs and Gallup, 2001) as well as at the microeconomicone (Audibert et al., 2003) ⎯ is how to measure exposure to malaria risk andseverity of the disease. This is clearly due to the lack of malaria incidence sta-tistics. As stated in the general introduction, there are different methodologi-cal and technical barriers hampering accurate measurement of the number ofmalaria cases.
As a proxy for child malaria morbidity, we first used the index describedin Sachs and Gallup (2001), defined as the fraction of population at risk ofcontracting falciparum malaria in a country. This index uses historical mapsof the geographic extent of malaria prevalence combined with detailed data onworld population distribution and the fraction of cases of malaria that are fal-ciparum malaria (for 1990). We computed this indicator for four differentyears (1946, 1966, 1982, 1994). This assumes that the relative proportion ofP. falciparum cases did not change substantially over the period 1946 to 1994.As there are so many problems relative to the measurement of the number ofmalaria cases (even more so for historical data), we consider these indexes asthe best measures of falciparum malaria risk for these particular years.
Second, we extend these indicators with more recent data available fromthe Malaria Atlas Project. The main objective of this project is to develop adetailed model of the spatial limits of P. falciparum and P. vivax malaria at aglobal scale, and its endemicity within this range (Guerra et al., 2008). TheMAP identified 87 countries at risk of P. falciparum transmission between2002 and 2006. Figures for raw estimated population at risk are projectionsfor 2007 made from the Global Rural Mapping Project (GRUMP) alpha popu-lation surface (adjusted to United Nations national country estimates for2000) and national medium variant population growth rate by country fromthe United Nation Population Database (UNPD). To create the percentage ofpopulation at risk for 2007 by country, we used the UNPD estimates for 2000
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 137
as a baseline and the national population growth rate by country. This indexhas two main advantages. First, it enables us to update and improve the Sachsand Gallup (2001) database on falciparum malaria risk and to make cross-sec-tional regressions with recent years. Indeed, the MAP estimates are calcu-lated differently to the Sachs and Gallup (2001) Malaria index, and thereforethis new index is not strictly comparable to the first one. Nevertheless, it doesprovide a differently-constructed index that can be used for robustness analy-sis. Our assumption is that the quality of the Malaria Index is improved andupgraded. Second, the MAP database also provides projections of populationsat risk within areas of unstable and stable P. falciparum transmission. There-fore, among people at risk, it is possible to have the proportion of those wholive in stable or unstable areas and to dissociate the effects of malaria in bothcases.
Costs in terms of education are expected to differ with level of endemicityand percentage of areas in stable/unstable areas. Malaria is said to be stable ifit is transmitted throughout the year by long-lived, anthropophilic vectoranopheles mosquitoes (Kiszewski et al., 2004). MAP defines stability as anannual P. falciparum parasite prevalence ≥ 0.1 per 1,000 people per year. Wecan distinguish three main situations that will have different costs in terms ofhuman capital and basic education at macroeconomic level in our study. Inhighly endemic regions (where the fraction of the population at risk of con-tracting falciparum malaria is high), mortality and morbidity mainly occursamong children aged 4 months to 5 years and in pregnant women. Conse-quently, malaria would be expected to have a bigger impact on primary schoolquality and school performances in these areas through the channels detailedin the general introduction (figure 1), and due to the other external effectsassociated with the disease. By contrast, in regions where malaria transmis-sion is less stable and where herd immunity is lower, malaria and severemalaria can affect people of all ages, but less frequently (mainly during epi-demics or seasonal variations). Consequently, the educational impacts areexpected to be smaller. In malaria-free area, there will obviously be no impact.
In this study, we consider that a country is highly endemic when theP. falciparum malaria index is greater than 0.5 for both index measures. Wealso attempt to assess the impact in stable and unstable areas.
Other independent variablesThree resource variables that the literature has previously identified as poten-tial determinants of education outcomes are used to take into account the
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

138 Josselin Thuilliez
impact of public spending on repetition rates: primary current expenditureper pupil (PPP), public current expenditure in primary education as a per-centage of GNP, and primary-school pupil-teacher ratio.
Income per capita is also included in the regressions, for two main rea-sons. On the one hand, many studies have shown that countries with higherincome have better primary education quality. Indeed, income per capita maybe interpreted as a proxy for parents’ income (Barro and Lee, 2000). On theother hand, malaria and income levels are intimately connected, and our fal-ciparum malaria index could just serve as a proxy for poverty.
Level of urbanization, another explanatory variable that is a potentiallyinfluential factor in primary repetition and completion rates, is also includedin the model. Indeed, school results are expected to be higher in urban areassince the travel costs tied to school attendance may be lower than in ruralareas, and children can get better access to educational services or better gen-eral conditions to work in (electricity for instance) especially in developingcountries.
As stressed in the literature, the effectiveness of the public expendituremanagement system could explain the weak link between resources and edu-cation quality (see for instance Reinikka and Svensson, 2004). In order to con-trol for this factor, we include in the regressions a measure of governancequality developed by Kaufmann et al. (2006): “government effectiveness 1996”.The Worldwide Governance Indicators are a compilation of information andperceptions from diverse groups of respondents but have to be seen as proxiesof the complex phenomenon of governance. We do not pretend here to answerthe specific question of the impact of management system quality on educa-tion outcomes, but rather to capture the influential effects of these factors onour dependant variables, ceteris paribus.
Malaria could also be a proxy for a range of other variables, principallygeneral health conditions, notably child health conditions, plus climate andgeographical location. Therefore, the regressions given in tables 1 and 2include the under-5 mortality rate (as a proxy for child health conditions), andthe percent of land area in subtropics and tropics (Sachs and Gallup, 2001),which allow us to control for climate, ecological conditions and diseases asso-ciated with tropical and subtropical location that could drive our coefficientestimates on the falciparum malaria index. Alternative measures of geo-graphical location (regional dummies) have also been used in the robustnessanalysis.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 139
Descriptive statisticsDescriptive statistics, sources and definitions of the variables used in themain cross-sectional analysis (1996) presented in this paper can be found intable A1. Simple correlations between variables are given in table A2. Paneldata were drawn from the Barro and Lee (2001) dataset completed with WorldDevelopment Indicators (World Bank 2006). Data for robustness analysiswere also borrowed from the World Development Indicators (World Bank,several years) plus the UNESCO database.
As an example, take the 125 observations available for both the primaryrepetition rate for 1996 and the falciparum malaria index for 1994. 36 of the125 countries (29%) are host to intensive malaria (29 are African countries).Ranking the 125 countries by primary repetition rate, 25 of the 36 countrieswith severe malaria (69%) are in the bottom half of the ranking. A first look atthe data would however suggest that malaria could only be a proxy for geo-graphic location or other variables. In the next subsection, we detail the meth-odology used in the study to explore the link between malaria and schoolresults, and address possible sources of errors. We underline that we onlypresent our identification strategy for the cross-sectional regression analysis(1996), which is comparable to other studies.
MethodologyOur modelling approach is based on previous research (Barro and Lee, 2000;Al-Samarrai, 2006), and the relevance of including malaria in the model hasbeen tested using a stepwise selection procedure and the usual tests.
We begin by estimating the regressions using Ordinary Least Squares(OLS). Standard errors are adjusted for heteroscedasticity in all cases. In thisfirst step, the full set of available observations is considered. Outlying obser-vations are not automatically mistakes in data entry and can provide importanteconomic information by increasing variation in the explanatory variables. Inaddition to these regressions, we also analyze how robust the OLS resultsgiven in tables 1 and 2 are to different estimation techniques.
Firstly, this study assesses whether the coefficient estimate on themalaria index suffers from endogeneity bias (principally due to measurementerrors or two-way causation, but also to omitted variables). The falciparummalaria index is clearly exposed to measurement errors. It is also possible thatlow education levels have a negative impact on malaria eradication, eitherdirectly or through other variables such as income level or general health
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

140 Josselin Thuilliez
conditions. It is possible that countries with bad educational outcomes facegreater difficulties in controlling malaria, but this argument remains specula-tive as it is not clear whether or not the general level of formal education in acountry will improve malaria control. For instance, it can be argued that someMENA (Middle East and North Africa) countries have recently succeeded incontrolling malaria but still have relatively high rates of illiteracy. Indeed, theMalaria Report 2008 lists Algeria, Egypt, Iraq and Saudi Arabia among10 countries worldwide that have successfully reached the elimination phasefor malaria. The United Arab Emirates was malaria-free in January 2007.Much of this success in combating malaria may be attributed to improve-ments in anti-malaria interventions. The educational achievement of MENAcountries remains below other countries at similar levels of economic develop-ment. The 2007 TIMSS test on 8th-grade Math and Science capabilitiesresulted in none of the 12 participating MENA countries reaching the averagescale. 5 However, in this part of the world, malaria epidemiology differs widelyfrom Sub-Saharan Africa, with a higher proportion of P. vivax malaria casesand different predominant anopheles vectors. Moreover, despite low-leveleducation performance, MENA countries have almost reached full primaryeducation enrolment and have halved illiteracy rates within the space of thepast 20 years. Mother’s education is a key determinant of access to health ser-vices and use of ITNs in Africa. Hence, a bidirectional relationship cannot becompletely excluded.
To correct for potential endogeneity bias, we use the spatial index of thestability of malaria transmission based on the interaction of climate with thedominant biological properties of the anopheles vector of malaria (bitingactivity, proportion of blood meal taken from human hosts, daily survival ofthe vector, duration of the transmission season and of extrinsic incubation).This interaction determines vectorial capacity and explains a large part of thestrength, stability and regional variation of malaria transmission (Kiszewskiet al., 2004). This index is measured on a highly disaggregated level and thenaveraged for the entire country, weighted by population. The total number ofcountries in which malaria is endemic or potentially endemic has been dividedinto 260 different regions based on their particular characteristics (to repre-sent habitat diversity) and 34 anopheles vectors were considered as dominant.Because it is built on climatological and vector characteristics, “Malaria Ecol-ogy” is said to be exogenous to public health interventions and economic con-ditions. There is no reason to think that the ecology-based distribution ofmalarial mosquito vectors and the variation in their biological properties are
5 http://nces.ed.gov/timss/results07_math07.asp (accessed: November 2009)
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 141
causes of bad educational outcomes apart from the direct influence of malariaor through observable variables such as tropical location already included inour models. This variable is therefore a good candidate instrument for the fal-ciparum malaria index. As we said, Sachs and Gallup (2001) had already useda similar instrument. The first stage regression of the falciparum malariaindex on the instrument (“Malaria Ecology”) has an R2 of 0.56.
Secondly, the sample size dictates that we can only introduce a limitednumber of control variables to isolate the causal effect of the falciparummalaria index. The specification models presented in tables 1 and 2 alreadyinclude a relatively high number of independent variables. Introducing morevariables may lead to a “small sample size problem” and multicollinearity canincrease the variance of our unbiased estimators. We therefore performed dif-ferent specifications of the regression model with a restricted number of inde-pendent variables and a higher-size sample (from 85 to 117 observations forregressions with repetition rates and from 56 to 73 observations for regres-sions with completion rates). We separately control for different factors bysuccessively including in each regression a set of variables for geographicaland climate characteristics, variables for health conditions, governance indi-cators, and education resources (data available on request). Using these specifi-cation models does not alter the main conclusions of this paper. The regionaldummy variable that appears to play a significant role on the Two-Stage LeastSquares (2SLS) regressions with repetition rates is Latin America and theCaribbean. These countries, on average, have higher primary repetition ratesthan average, after controlling for the model-integrated variables. No dummyvariable appears to play significant role on the 2SLS regressions with repeti-tion rates. Malaria could also be a proxy for a range of tropical diseases thatare not adequately controlled for by under-5 child mortality (1995) and tropi-cal and/or subtropical location. To assess whether other diseases were respon-sible for the correlation of malaria with primary repetition and completionrates, we jointly include two relevant indicators for the time period understudy here: an average of the proportion of the population living in areas withdengue fever from 1975 to 1995, and an estimated fraction of the populationat risk of contracting yellow fever for 1996 (Sachs and Gallup, 2001). Descrip-tions and sources of these variables are given in table A1. Unfortunately, wedo not have macroeconomic-level indicators for other tropical diseases or forAIDS for 1996. Since AIDS has spread so quickly, the regressions did notinclude recent data on the AIDS burden. However, we do not think our con-clusions would change with the inclusion of an AIDS indicator since AIDSaffects education by different channels to malaria (for instance through itsimpact on teachers). The estimated impact of malaria remains relatively stable
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

142 Josselin Thuilliez
and statistically significant at the 5% level for regression (2) and the 1% levelfor regression (6). The two tropical diseases have no significant correlationwith repetition and completion rates.
Thirdly, OLS regressions assume that the residuals are independent. It iseminently possible that primary repetition rates within each subcontinentmay not be independent, and this could lead to residuals that are not indepen-dent within subcontinents. We thus allow regression observations to be clus-tered into subcontinents to take into account the probable spatial correlationof observations within subcontinents (not presented here but available onrequest). The 2SLS results are almost identical to those presented in tables 1and 2. Therefore, we cannot reject the assumption that the residuals are inde-pendent.
Fourthly, we explore whether or not our OLS and 2SLS results are drivenby influential observations. OLS is vulnerable to outlying observations sinceit minimizes the sum of squared residuals. Individual countries with largeresiduals and high leverage are identified and dropped for each regression. 6
From 8 to 11 countries were identified as outliers in the regressions and con-sequently dropped (data available upon request). The size and significance ofthe coefficient estimates on the falciparum malaria index show only slightchange.
4 RESULTS
The results from the OLS and 2SLS regression analysis with the Samer Al-Samarrai dataset for primary repetition and completion rates are presented intable 1 and table 2. Different models are reported so as to take into accountdifferent options chosen from the literature. There appears to be a very strongrelationship between the falciparum malaria index and primary repetitionand completion rates. The positive coefficient on the malaria index (0.096;se = 0.039) in regression (1) of table 1 indicates that countries with intensivemalaria have 9%-higher repetition rates in primary education than countrieswithout malaria. A one standard deviation increase in the falciparum malariaindex is associated with a 0.43 standard deviation increase in primary repeti-tion rates. The negative coefficient on the malaria index (-0.295; se = 0.087) in
6 Studentized residuals and leverages were examined as an initial approach for identifyingoutliers and observations that have a potentially strong influence on regression coeffi-cient estimates. Next, DFIT statistics were used as an overall measure of influence.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 143
regression (1) of table 2 indicates that countries with intensive malaria have29%-lower primary completion rates than countries without malaria. A onestandard deviation increase in the falciparum malaria index is associated witha 0.47 standard deviation decrease in primary completion rates.
The coefficient estimates on the malaria index are significantly differentfrom 0 (at the 5% level) in regressions (1) and (2) of table 1. In regression (3)of table 1, the p value of the coefficient estimate is 0.13, and the value itself islower than in the previous regressions. This may be due to the high correla-tion between the falciparum malaria index and the pupil-teacher ratio withinthe sample (r = 0.73). However, the corresponding Instrumental Variableestimation, given in regression (6) of table 1, shows that the impact of malariais still significant, positive, and high. In all the OLS regressions of table 2, thecoefficient estimates on the malaria index are significantly different fromzero, negative, and relatively stable.
Section 3 suggested that the falciparum malaria index may be endoge-nous, and went on to explain that the instrumental variable estimation can beused to account for this problem. 2SLS regressions are given in columns (4)to (6) of tables 1 and 2. We use the previously-described “Malaria Ecology”instrument for the falciparum malaria index. If there were a reverse causa-tion between the malaria index and primary repetition and completion rates,the coefficient estimates on the malaria index reported in columns (1) to (3)would be positively biased in table 1 and negatively biased in table 2.
After correcting for the possible endogeneity of the falciparum malariaindex, the absolute value of the estimated effect of malaria on repetition andcompletion rates is higher than our previous results, and still statistically sig-nificant in all regressions. This generally occurs when the endogenous vari-able suffers from measurement errors, and the falciparum malaria indexremains relatively crude. Therefore, the 2SLS regression analysis confirms thatthe link between falciparum malaria and primary repetition and completionrates is strong. The positive coefficient on the malaria index (0.180; se = 0.060)in regression (4) of table 1 indicates that countries with intensive malariahave 18%-higher repetition rates in primary education than countries withoutmalaria. The negative coefficient on the malaria index (-0.543; se = 0.184) inregression (4) of table 2 indicates that countries with intensive malaria have54%-lower primary completion rates than countries without malaria. As 2SLSand OLS estimates on the falciparum malaria index differ significantly (dueto measurement errors on the malaria index), the 2SLS estimator is more effi-cient than the OLS estimator. Therefore, we will now focus on regressions (4)to (6) of table 1 and 2 for the continuing analysis.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)
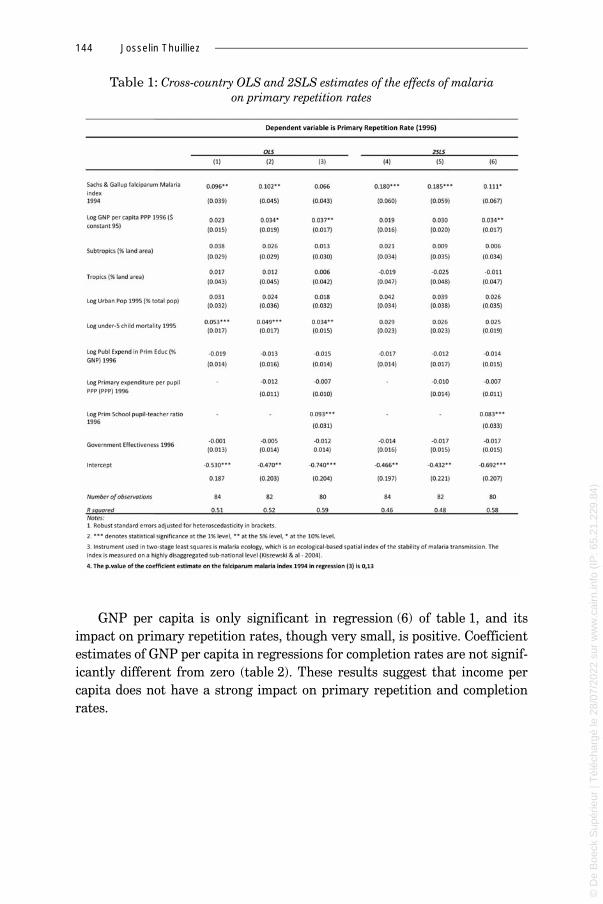
144 Josselin Thuilliez
Table 1: Cross-country OLS and 2SLS estimates of the effects of malaria on primary repetition rates
GNP per capita is only significant in regression (6) of table 1, and itsimpact on primary repetition rates, though very small, is positive. Coefficientestimates of GNP per capita in regressions for completion rates are not signif-icantly different from zero (table 2). These results suggest that income percapita does not have a strong impact on primary repetition and completionrates.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 145
Table 2: Cross-country OLS and 2SLS estimates of the effects of malaria on primary completion rates
Tropical and subtropical location does not appear to have a significantimpact on primary repetition and completion rates. It could be argued thatthe impact of malaria on educational outcomes reflects the influence of agiven region and not the isolated effect of malaria. For example, Sub-SaharanAfrica has, on average, high levels of malaria, high repetition rates and rela-tively low completion rates. Hence, the malaria index could just be a proxy forSub-Saharan Africa. However, results are globally unchanged when regionaldummies are included (South Asia, East Asia, Sub-Saharan Africa, MiddleEast and North Africa, and Latin America and the Caribbean).
Although under-5 mortality rate was positively and significantly associ-ated with repetition rates in the OLS regressions, it does not appear to have asignificant impact on repetition or completion rates in 2SLS regressions. In
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

146 Josselin Thuilliez
all the 2SLS regressions of table 1 and 2, the coefficient estimates on under-5mortality are not significantly different from zero.
Level of urbanization and the governance indicator have no significantimpact on the educational outcomes under study here.
The coefficient estimates on current public primary expenditure (% of GNP)is negative in all the regressions of table 1. It is positive in regressions (4) and(6) and negative in regression (5) of table 2, but never significantly differentfrom 0. This insignificant effect of total educational spending on repetition/completion rates suggests that an increase in total school resources may notitself lead to an increase in student achievement. This conclusion is in accor-dance with Hanushek (1995) and Samer Al-Samarrai (2006). There is no sys-tematic relationship between school performance and general measures ofschool resources.
Where regressions include two school variables (primary expenditure perpupil and current public primary expenditure as a proportion of GNP), theresults are not dramatically different. They suggest that primary expenditureper pupil is also an insignificant determinant of repetition and completionrates, ceteris paribus.
Nevertheless, when the regressions include the three school variables, thepupil-teacher ratio is positively and significantly (at 1% level) associated withrepetition rates in regression (6) of table 1. This result is coherent with theconclusions of Barro and Lee (2001) on the link between repetition rates andpupil-teacher ratio. It is estimated that a lower pupil-teacher ratio improvesrepetition rates and test scores. Components of school expenditure allocatedto lower pupil-teacher ratio will reduce primary repetition rates, whereas theother-resource variables still have no significant impact. Nevertheless, the lit-erature remains ambiguous on this point (Samer Al-Samarrai, 2006). More-over, pupil-teacher ratio is not significant in the primary completion rateregression (regression (6) of table 2). Therefore, as in the literature, thereseems to be an ambiguous relationship between educational outcomes andcommonly-measured school resources. Nevertheless, as this question is notthe primary focus of our study, we will refocus our efforts on testing therobustness of the coefficient estimates on the malaria index.
5 OTHER ROBUSTNESS TESTS
Panel dataset: Sachs and Gallup indices (2001)The panel data models used to estimate the effect of malaria on primary repe-tition rates are random effects models (table 3). This is justified by the fact
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 147
that 1) our time dimension is reduced, 2) our between-group variation ishigher than our within-group variation.
Table 3: Panel data estimates of the effects of malaria on primary repetition rates (1960-1995)
Since Sachs and Gallup (2001) gives malaria measures for 1946, 1966,1982, 1994 and the output measures for 5-year intervals from 1960 to 1995,we matched the input measures with outputs in the nearest year for whichthe malaria measure is available. Completion rates are not available for thisperiod. The results show similar patterns, but the coefficients appear lowerthan in our cross-country analysis. This may be due to the fact that we haveno time-variant instrument for malaria for this period of analysis, meaningthe coefficients are almost certainly biased downward.
Cross-country robustness analysis: using an updated malaria index from MAP (Malaria Atlas Project)
Table 4 below presents the results with the updated malaria index from MAP(2007). Since the dataset is more recent, some of the variables are still incom-plete and count very few observations, and have consequently been dropped
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

148 Josselin Thuilliez
from the analysis. This was the case for current primary expenditure perpupil (PPP) and current public expenditure in primary education as a per-centage of GNP. As these variables had no significant effect in the previousanalysis, we suppose that they are controlled through the well-documentedprimary school pupil-teacher ratio. All other variables have been kept in themodels. The malaria index used here and the Malaria Atlas Project have beendescribed earlier. The malaria index is the percentage of the population atrisk of falciparum malaria in 2007 (figure 1). This index is then broken downinto two sub-indexes:
% Tot Pop at risk of falciparum malaria in 2007 = % Tot Pop at risk of fal-ciparum malaria in 2007 living in stable transmission areas + % Tot Pop atrisk of falciparum malaria in 2007 living in unstable transmission areas
Table 4: OLS and 2SLS regressions of primary repetition and completion rates on the malaria⎯MAP index
According to Guerra et al. (2008), in 2007, 1 billion people were living underunstable or extremely low malaria risk while 1.37 billion were living under sta-ble and high malaria risk. Hence, we first use the global index of malaria sep-arately and next test the robustness of this index by introducing into the
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 149
regression the % Tot Population at risk of falciparum malaria in 2007 livingin stable transmission areas. This allows us to test the relative contribution ofstability of the malaria burden.
We find similar patterns in these results to our previous testing on the fal-ciparum malaria global index for both OLS and 2SLS analysis. However, itseems that the % of population at risk of falciparum malaria living in stabletransmission areas in 2007 is a driver of our estimates of the coefficient asso-ciated with the global falciparum malaria index. Indeed, the partial effect ofthe falciparum malaria index is no longer statistically significant once associ-ated with the “falciparum malaria index – stable area” (regressions (2), (4),(6) and (8)), whereas the partial effect of this stable-area falciparum malariaindex remains statistically significant. When holding other model-integratedfactors fixed, particularly the percent of population at risk of falciparummalaria in a country, the countries with a high proportion of population livingin stable transmission areas have 13%-higher primary repetition rates thancountries without stable transmission areas. This means that countries withrelatively higher proportions of population living in stable transmission areas(versus unstable areas) are more affected by the effects of malaria on humancapital accumulation.
6 DISCUSSION AND CONCLUSIONS
Our cross-country panel regression analysis has shown that the link betweenthe level of falciparum malaria endemicity and primary repetition rates isstrong and positive, while the link between the level of falciparum malariaendemicity and primary completion rates is strong and negative. Theseresults suggest that malaria contributes to impede children’s human capitalaccumulation at macroeconomic level.
Nevertheless, the results presented in the previous section should beinterpreted with caution. Why is there such a strong link? Malaria specificallyaffects children’s cognitive and learning abilities, and consequently theirschool results. Our conjecture was that high repetition rates and low comple-tion rates reflect particularly bad school results. Therefore, the strong linkbetween malaria and primary repetition and completion rates reflects theimpact of malaria on school results, and does not imply that there will system-atically be a similar relation between malaria and other educational out-comes. We did not explore the relationship between falciparum malaria andother educational indicators.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

150 Josselin Thuilliez
Moreover, malaria is a complex economic and social phenomenon. It isvery difficult to dissociate the direct medical impact of the disease from itsnumerous effects on society and human organization. In addition to its medi-cal effects, the behavioral and social aspects linked with malaria may explainpart of the estimated impact of malaria on repetition and completion ratesreported in this paper.
A major problem hampering assessments of the impact of malaria on edu-cation is the lack of good data. Our conclusions are valid within the limits ofdata precision and availability. Some variables that may be expected to influ-ence education outcomes or bias the coefficient values of the malaria indexwere not included due to the lack of cross-country data. We attempted toaccount for this problem by using different specifications of the regressionmodel and different estimation techniques, but there may still be variablescorrelated with the malaria index that are missing. Furthermore, the conclu-sions drawn are only valid at the macroeconomic stage, and are not a substitutefor detailed per-country analysis or case studies. Microeconomic evaluations ofthe impact of malaria on school performances may differ from macroeconomicprojections.
Some variables included in the regression models have ambiguous effects.Note that GNP per capita has a positive effect on primary repetition rates insome regressions. However, this effect is not robust to different model specifi-cations nor to the use of re-updated data. In regressions where GNP per cap-ita is not associated with under-5 mortality rate or pupil-teacher ratio, itseffect is insignificant or negative (see regression (4) of table 3 for instance).This may be due to the high correlation between GNP per capita, the malariaindex, under-5 mortality rate and pupil-teacher ratio. However, the results donot change when these variables are removed from the model (data availableon request). Recent empirical literature on this topic suggests unstable effectsof GNP or GDP per capita on education quality at the macroeconomic level.Al-Samarrai (2006), for instance, reported that this variable has a negativebut non-significant effect on primary completion rates. In Barro and Lee(2001), the GDP variable proves insignificantly associated with mathematicsand science test scores but significantly associated with reading scores (posi-tively) and repetition rates (negatively). Therefore, our analysis casts seriousdoubts on the relevance of using macroeconomic data to study such importantdevelopment issues due to the levels of data heterogeneity and quality involved.The same scepticism and criticism addressed at Sachs and Gallup (2001) or Ace-moglu et al. (2002) with respect to data quality hold true for our study.
However, our results on the link between falciparum malaria and primaryrepetition rates suggest that the achievement of the UN millennium develop-
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 151
ment goals for education (particularly the aspects concerning education qual-ity) will require more than just focusing on expenditure in primary education.These results have been shown to be robust to a series of tests (different spec-ification models, controls for influential observations, different estimationtechniques, different datasets, and different years). They appear to provide agood idea of the malaria burden at macroeconomic stage. Regressions withcompletion rates also suggest that there are other externalities linked withthe disease, as the impact is even higher. Hence, our macroeconomic resultsremain useful for a first-look analysis of the relationship. Nevertheless, thequestionable level of macroeconomic data quality discussed previously meansthese results are obviously insufficient to conclude that a causal relationshipexists between these variables. It is possible that we are asking questions thatare too subtle for the available data to answer with any meaningful precision.
Acknowledgements
The author is grateful for comments from M. Audibert, J.-C. Berthélémy,S. Poncet, C. Bros, A. Tatem, all the participants of the Séminaire d’économieCES (Paris), and particularly S. Al-Samarrai and J. Sachs who accepted toprovide part of the database for this study. The author remains solely respon-sible for any errors.
REFERENCES
ACEMOGLU D., JOHNSON S., ROBINSON J. (2002), “Institutional causes, macroeco-nomic symptoms, volatility, crises and growth”, NBER Working paper 9124.
AL-SAMARRAI S. (2006), “Achieving education for all: How much does money mat-ter?”, Journal of International Development, 18, 179-206.
AL SEROURI A. W., GRANTHAM-MCGREGOR S. M., GREENWOOD B. M., COSTELLO A.(2000), “Impact of asymptomatic malaria parasitaemia on cognitive functionand school achievement of schoolchildren in the Yemen Republic”, Parasitol-ogy, 121, 337-345.
AMOROSA L. F., CORBELLINI G., COLUZZI M. (2005), “Lessons learned from malaria:Italy’s past and sub-Sahara’s future”, Health and Place, 11, 67-73.
AUDIBERT M. (1986), “Agricultural non-wage production and health status: Acase study in a tropical environment”, Journal of Development Economics, 24,275-291.
AUDIBERT M., MATHONNAT J., NZEYIMANA I., HENRY M.-C. (1999), “Rôle du palu-disme dans l’efficience technique des producteurs de coton dans le nord de laCôte d’Ivoire”, Revue d’Économie du Développement, volume spécial “Santé etDéveloppement”, 4, 121-148.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

152 Josselin Thuilliez
AUDIBERT M., MATHONNAT J., HENRY M.-C. (2003), “Social and health determi-nants of the technical efficiency of cotton farmers in Northern Côte d’Ivoire”,Social Science and Medicine, 56, 1705-1717.
AUDIBERT M., MATHONNAT J., HENRY M.-C. (2003), “Malaria and property accu-mulation in rice production systems in the savannah zone of Côte d’Ivoire”,Tropical Medicine and International Health, 8(5), 471- 483.
BARLOW R. (1967), “The economic effects of malaria eradication”, American Eco-nomic Review, 57(2), 130-148.
BARRO R. J., LEE J. W. (2001), “Schooling quality in a cross-section of countries”,Economica, 68, 465- 488, 2001.
BLEAKLEY H. (2007), “Malaria in the Americas: A retrospective analysis of child-hood exposure”, BREAD Working Paper, 142.
BOWLES S. (1970), “Toward an educational production function”, In: W. L. Hanson(Eds), Education, Income and Human capital, 11-61, New York: Columbia Uni-versity Press.
BROOKER S., GUYATT H., OMUMBO J., SHRETTA R., DRAKE L., OUMA J. (2000), “Sit-uation analysis of malaria in school-aged children in Kenya – What can bedone?”, Parasitology Today, 16(5), 183-186.
BROOKER S., CLEMENTS A.C.A., HOTEZ P. J., HAY S. I., TATEM A. J., BUNDY D.A.P.,SNOW W. R. (2006), “The co-distribution of Plasmodium falciparum and hook-worm among African schoolchildren”, Malaria Journal, 5(99).
BROWN B. W., SAKS D. H. (1986), “Measuring the effects of instructional time onstudent learning: Evidence from the beginning teacher evaluation study”,American Journal of Education, 94(4), 480-500.
BRYCE J., BOSCHI-PINTO C., SHIBUYA K., BLACK R. E., WHO Child Health Epidemi-ology Reference Group (2005), “WHO estimates of the causes of death in chil-dren”, Lancet, 365, 1147-1152.
CARTER J. A., MURIRA G. M., ROSS A. J., MUNG’ALA-ODERA V., NEWTON C.R.J.C.(2003), “Speech and language sequelae of severe malaria in Kenyan children”,Brain Injury, 17(3), 217-224.
CARTER J. A., LEES J. A., GONA J. K., MURIRA G., RIMBA K., NEVILLE B.G.R., NEW-TON C.R.J.C. (2006), “Severe falciparum malaria and acquired childhood lan-guage disorder”, Developmental Medicine and Child Neurology, 48(1), 51-57.
CARTER J. A., NEWTON C.R.J.C. (2006), “The effects of Plasmodium falciparum oncognition: A systematic review”, Tropical Medicine and International Health,11(4), 386-397.
CARTER J. A., ROSS A. J., NEVILLE B.G.R., OBIERO E., KATANA K., MUNG’ALA-ODERA V., LEES J. A., NEWTON C.R.J.C. (2005), “Developmental impairmentfollowing severe falciparum malaria in children”, Tropical Medicine and Inter-national Health, 10(1), 3-10.
CHIMA R. I., GOODMAN C. A., MILLS A. (2003), “The economic impact of malaria inAfrica: A critical review of evidence”, Health Policy, 63, 17-36, 2003.
CONLY G. N. (1975), “The impact of malaria on economic development”, Pan Amer-ican Health Organization Scientific Publication 297, Washington.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 153
CURRIE J., STABILE J. (2006), “Child mental health and human capital accumula-tion: The case of ADHD”, Journal of Health Economics, 25, 1094-1118.
MAZER A., SANKALE M. (1988), Guide de médecine tropicale en Afrique et Océanindien, EDICEF/UNESCO, Vanves.
ETTLING M., MCFARLAND D. A., SCHULTZ L. J., CHITSULO L. (1994), “Economicimpact of malaria in Malawian households”, Tropical Medicine and Parasitol-ogy, 45(1), 74-79.
FERNANDO D., DE SILVA D., CARTER R., MENDIS K. N., WICKREMASINGHE R. (2006),“A randomized, double-blind, placebo-controlled, clinical trial of the impact ofmalaria prevention on the educational attainment of school children”, Ameri-can Journal of Tropical Medicine and Hygiene, 74(3), 386–393.
FERNANDO D., GUNAWARDENA D. M., BANDARA M.R.S.S., DE SILVA D., CARTER R.,MENDIS K. N., WICKREMASINGHE A. R. (2003), “The impact of repeated malariaattacks on the school performance of children”, American Journal of TropicalMedicine and Hygiene, 69(6), 582-588.
FERNANDO D., DE SILVA D., WICKREMASINGHE R. (2003), “Short-term impact of anacute attack of malaria on the cognitive performance of schoolchildren living ina malaria endemic area of Sri Lanka”, Transactions of the Royal Society of Trop-ical Medicine and Hygiene, 97, 633–639.
FERNANDO D., WICKREMASINGHE R., MENDIS K. N., WICKREMASINGHE A. R. (2003),“Cognitive performance at school entry of children living in malaria-endemicareas of Sri Lanka”, Transactions of the Royal Society of Tropical Medicine andHygiene, 97, 161-163.
GOMES M. (1993), “Economic and demographic research on malaria: A review ofthe evidence”, Social Science and Medicine, 37(9), 1093-1108.
GUERRA C., GIKANDI P., TATEM A., NOOR A., SMITH D., HAY S., SNOW R. (2008),“The limits and intensity of Plasmodium falciparum transmission: Implica-tions for malaria control and elimination worldwide”, PLoS Med, 5(2), e38.
HANUSHEK E. A. (1979), “Conceptual and empirical issues in the estimation of edu-cation production functions”, Journal of Human Resources, 14(3), 351-388.
HANUSHEK E. A. (1995), “Interpreting recent research on schooling in developingcountries”, The World Bank Research Observer, 10(2), 227-246.
HOLDING P. A., SNOW R. W. (2001), “Impact of P. falciparum malaria on perfor-mance and learning: Review of evidence”, American Journal of Tropical Medi-cine and Hygiene, 64(1,2)S, 68-75.
HOLDING P. A., KITSAO-WEKULO P. K. (2004), “Describing the burden of malariaon child development: What should we be measuring and how should we bemeasuring it?”, American Journal of Tropical Medicine and Hygiene, 71(2)S,71-79.
HUNG L. Q., DE VRIES P. J., GIAO P. T., NAM N. V., BINH T. Q., CHONG M. T., QUOC
N.T.T.A., THANH T. N., HUNG L. N., KAGER P. A. (2002), “Control of malaria:A successful experience from Vietnam”, Bulletin of the World Health Organiza-tion, 80(8), 660-666.
IMBERT P. (2003), “Criteria of severity in childhood falciparum malaria”, Archivesde Pédiatrie, 10(5)S, 532-538.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

154 Josselin Thuilliez
KATZMAN M. T. (1971), “The political economy of urban schools”, Cambridge, MA:Harvard University Press.
KELLEY T. L. (1917), “The effect of malaria and hookworm upon physical and mentaldevelopment of school children”, The Elementary School Journal, 18(1), 43-51.
KERE N. K., KENI J. F., BOBOGARE A., WEBER R. H. (1993), “The economic impactof Plasmodium falciparum malaria on education investment: A Pacific Islandcase study”, Southeast Asian J. Trop Med. Public Health, 24, 659-663.
KIHARA M., CARTER J. A., NEWTON C.R.J.C. (2006), “The effect of Plasmodium fal-ciparum on cognition: A systematic review”, Tropical Medicine and Interna-tional Health, 11(4), 386-397.
KISWESKI A., MELLINGER A., SPIELMAN A., MALANEY P., SACHS J., SACHS S. E.(2004), “A global index of the stability of malaria transmission”, AmericanJournal of Tropical Medicine and Hygiene, 71 (2)S, 141-146.
KROEGER A., MEYER R., MANCHENO M., GONZALEZ M. (1996), “Health education forcommunity-based malaria control: An intervention study in Ecuador, Colombiaand Nicaragua”, Tropical Medicine and International Health, 1(6), 836-846.
LEIGHTON C., FOSTER R. (1993), “Economic impacts of malaria in Kenya and Nige-ria”, Bethesda, Maryland: Abt Associates, Health Financing and SustainabilityProject.
MABIALA-BABELA J. R., SAMBA-LOUAKA C., MOUKO A., SENGA P. (2003), “Morbiditédans un service de pédiatrie du CHU de Brazaville: 12 ans après (1989-2001)”,Archives de Pédiatrie, 10.
MCDONALD G. (1950), “The economic importance of malaria in Africa”, WHO/MAL/60, AFR/MAL/Conf./16.
MAGNUSSEN P., NDAWI B., SEHSHE A. K., BYSKOV J., MBWANA K. (2001), “Malariadiagnosis and treatment administered by teachers in primary schools in Tanza-nia”, Tropical Medicine and International Health, 6, 273-279.
MAP, Malaria Atlas Project. http://www.map.ox.ac.uk/JUKES M.C.H., PINDER M., GRIGORENKO E. L., SMITH H. B., WALRAVEN G.,
BARIAU E. M., STERNBERG R. J., DRAKE L. J., MILLIGAN P., CHEUNG Y. B.,GREENWOOD B. M., BUNDY D.A.P. (2006), “Long-term impact of malaria chemo-prophylaxis on cognitive abilities and educational attainment: Follow-up of acontrolled trial”, PLOS Clinical Trial, 1(4): e19.
MENSAH O. A., KUMARANAYAKE L. (2004), “Malaria incidence in rural Benin: Doeseconomics matter in endemic area?”, Health Policy, 68:1, 93-102.
NEWMAN P. (1968), “Malaria eradication and population growth: With special ref-erence to Ceylon and British Guiana”, Research Series no.10, Bureau of PublicHealth Economics, School of Public Health, University of Michigan.
OKABAYASHI H., THONGTHIEN P., SINGHASVANON P., WAIKAGU J., LOOAREESUWAN
S., JIMBA M., KANO S., KOJIMA S., TAKEUCHI T., KOBAYASHI T. (2006), “Key tosuccess for a school-based malaria control program in primary school in Thai-land”, Parasitology International, 55(2), 121-126.
REINIKKA R, SVENSSON J (2004), “Local Capture: Evidence from a central govern-ment transfer program in Uganda”, The Quarterly Journal of Economics, MITPress, 119(2), 678-704.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 155
RHEE M., SISSOKO M., PERRY S., MCFARLAND W., PARSONNET J., DOUMBO O.(2005), “Use of insecticide-treated nets (ITNs) following a malaria educationintervention in Piron, Mali: A control trial with systematic allocation of house-holds”, Malaria Journal, 4(35).
RODRIK D., RODRIGUEZ F. (2001), “Trade policy and economic growth: A sceptic’sguide to the cross-national evidence”, NBER working paper, 7081, 2001.
SACHS J., MALANEY P. (2002), “The economic and social burden of malaria”,Nature, 415 (6872), 680-685.
SACHS J., GALLUP J. L. (2001), “The economic burden of malaria”, American Jour-nal of Tropical Medicine and Hygiene (Suppl.) 64(1.2)S, 85-96.
SHARMA A. K., AGGARWAL O. P., CHATURVEDI S., BHASIN S. K. (2003), “Is educationa determinant of knowledge about malaria among Indian tribal populations?”,Journal of Communicable Diseases, 35(2), 109-117.
SNOW R. W., TRAPE J. F., MARSH K. (2001), “The past, present and future of child-hood malaria mortality in Africa”, Trends in Parasitology, 17(12).
SNOWDEN N F. M. (2006), The conquest of Malaria: Italy 1900-1962. London: YaleUniversity Press New Haven.
UNESCO, EFA Global Monitoring Report, (2005), Education for All: The QualityImperative, Paris: UNESCO.
UNESCO, EFA (2005), Education for All: Paving the Way for Action, Regionaloffice in Dakar: UNESCO.
WATTS S. (1999), “British development policies and malaria in India 1897-1929”,Past and Present, 165, 141-181.
WHO, RBM, UNICEF (2005), World Malaria Report 2005, Geneva: World HealthOrganization and UNICEF.
WHO (2008), World Malaria Report 2008, Geneva: World Health Organization.WORRALL E., MOREL C., YEUNG S., BORGHI J., WEBSTER J., HILL J., WISEMAN V.,
MILLS A. (2007), “The economics of malaria in pregnancy – A review of the evi-dence and research priorities”, Lancet Infectious Diseases, 7, 156-168.
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

156 Josselin Thuilliez
APPENDIX
Table A1: Definitions, sources and descriptive statistics for main cross-country analysis (1996)
Variables
Obs Mean Std Dev Min Max
Malaria ecology 173 3.65 6.41 0.00 31.54
Subtropics (% land area) 150 0.28 0.32 0,00 0.98
Tropics (% land area) 150 0.16 0.25 0,00 1,00
Yellow fever 163 0.12 0.22 0,00 0.65
Dengue Fever 163 0.18 0.25 0,00 0.61
Control of Corruption 96 151 0.00 1.00 -2.19 2.50
Governance effectiveness 96 163 0.00 1.00 -1.98 2.23
Extent to which public power is exercised for private gain, including both petty and grand forms of corruption, as well as "capture" of the state by
elites and private interests
Aggregate Governance Indicators fromKaufmann D, Kray A & Mastruzzi M
(2006)
The quality of public services, the quality of civil services and the degree of its independence from political pressures, the quality of policy
formulation and implementation, and the credibility of the government's commitment to such policies
Aggregate Governance Indicators fromKaufmann D, Kray A & Mastruzzi M
(2006)
% of 1995 pop in area with yellow fever, 1996Sachs J & Gallup J.L (1999) CID
geography dataset
% of 1995 pop in area with dengue, 1975-1995
Subtropical land area (%) Sachs J & Gallup J.L (1999) CID geography dataset
Tropical land area (%) Sachs J & Gallup J.L (1999) CID
3.21 0.47 1.66 4.68Log Prim School pupil-teacher ratio 90 Log Primary School pupil-teacher ratio 90 Al Samarrai S (2006) from UNESCO 2001, WER 2000 171
6.21 1.39 1.09 8.94Log Primary expenditure per pupil PPP 1996 Log Public current expenditure in primary education per pupil, PPP, 1996 Al Samarrai S (2006) from UNESCO EFA
2000, WER 2000 and WDI 2000 146
-4.11 0.6 -5.8 -2.31Log Publ Expend in Prim Educ (% GNP) 1996
Log Public current expenditure in primary education as a percentage of GNP, 1996
Al Samarrai S (2006) from UNESCO EFA 2000, WER 2000 136
3.72 1.13 1.54 5.68Log Under 5 Child mortality 1995 Log Mortality Rate, under five years (total per 1000 live births), 1995 WDI 2005 WB 182
3.85 0.55 1.75 4.6Log Urban Pop 1996 (% total pop) Log Urban Population (% total pop), 1997 Al Samarrai S (2006) from WDI 1998 WB 191
10.87 4.88 1.00 18Subcontinents
1 = East asia, 2= Other East Asia, 3= South East Asia, 4 = South West Asia, 5= South Asia, 6 = Oceania, 7 = Eastern Africa, 8 = Middle Africa, 9
= Southern Africa, 10 = Western Africa, 11 = Caribbean, 12 = Middle America, 13 = Temperate South America, 14 = Tropical South America 15
= Arab States, 16 Western Europe, 17 = Eastern Europe, 18 = North America
Author & WB 193
0.18 0.39 0.00 1.00Latin America and the Caribbean Latin America and the Caribbean Dummy Author & WB 201
0.04 0.20 0.00 1.00South Asia South Asia Dummy Author & WB 201
0.10 0.30 0.00 1.00East Asia East Asia Dummy Author & WB 201
0.11 0.32 0.00 1.00MENA States Middle East and North Africa Dummy Author & OCDE 201
10.79
SSA Sub-Saharan Africa Dummy Author & WB 201 0.23 0.42 0.00 1.00
1.00
Ecological-based spatial index of the stability of malaria transmission. The index is measured on a highly disagregated sub-national level (Kiszewski
& al - 2004).
(Kiszewski & al - 2004). Dataset avalaible on the website of The Earth
Institute at Columbia University.
Log GNP per capita PPP ($ constant 95) Log GNP per capita PPP ($ constant), 1995 Al Samarrai S (2006) from WDI 2000 WB 176 7.55 1.59 4.69
167 0.30 0.41 0.00
0.35
Primary completion rate 1996Total number of students (of any age) in the last grade of primary school,
minus the number of repeaters in that grade, divided by the total number ofchildren of official graduation age, 1996
WDI 2005 WB 79 0.74 0.26 0.13 1.02
147 0.06 0.08 0.00
Definition Source Descriptive Statistics
Falciparum Malaria index 1994 % of 1995 population at risk of contracting falciparum malaria in a country, 1994
Sachs J & Gallup J.L (2001). Dataset avalaible on the website of The Earth
Institute at Columbia University.
% of repeaters in primary education, 1996 (some values are for 1995 or 1997)
Al Samarrai S (2006) from UNESCO 2001 & UNESCO EFA 2000Primary repetition rate 1996
© D
e B
oeck
Sup
érie
ur |
Tél
écha
rgé
le 2
8/07
/202
2 su
r w
ww
.cai
rn.in
fo (
IP: 6
5.21
.229
.84)
© D
e Boeck S
upérieur | Téléchargé le 28/07/2022 sur w
ww
.cairn.info (IP: 65.21.229.84)

Malaria and Primary Education 157
Table A2: Pairwise correlations
Table A3: Other collinearity diagnostics
VIF Tolerance
Sachs & Gallup falciparum Malaria index 1994 3.40 0.294
Log GNP per capita PPP 1996 ($ constant 95) 13.75 0.072
Subtropics (% land area) 1.59 0.628
Tropics (% land area) 1.59 0.628
Log Urban Pop 1995 (% total pop) 3.01 0.332
Log Under-5 Child mortality 1995 8.07 0.124Log Publ Expend in Prim Educ (% GNP) 1996 1.39 0.718
Log Primary expenditure per pupil PPP (PPP) 1996 6.67 0.150
Log Prim School pupil-teacher ratio 1996 3.10 0.322Government effectiveness 1996 3.82 0.261
Mean 4.64©
De
Boe
ck S
upér
ieur
| T
éléc
harg
é le
28/
07/2
022
sur
ww
w.c
airn
.info
(IP
: 65.
21.2
29.8
4)©
De B
oeck Supérieur | T
éléchargé le 28/07/2022 sur ww
w.cairn.info (IP
: 65.21.229.84)