invitro evaluation of side-branch creation in metal stents by balloon dilatation
TRANSCRIPT
Vol. 3, No. 4, Fall 2003 • The Journal of Applied Research380
Results: Of the self-expandable stents, theWallstent demonstrated the greatest dila-tion and maintenance of enlarged meshopening after dilatation. Side-branchdilatation of the Memotherm, Symphony,and Smart stents had little effect on themesh opening. Of the balloon expandablestents, Palmaz stent did not respond todilatation, resulting in balloon rupture andentrapment. The Omnilink and Expressstents exhibited good malleability and pro-gressive spherical enlargement in responseto dilatation.
Conclusion: The Wallstent was the mostsuitable self-expandable stent for creationof a side branch. The Memotherm,Symphony, and Smart stents are notamenable to side-branch formation due totheir elastic nature. The Palmaz stentshould not be used in situations where acreation of side branch is anticipatedbecause of its rigid nature and fixed strutjoint, which can lead to balloon entrap-ment. Both the Omnilink and Expressstents can be used when creation of a sidebranch is planned.
In Vitro Evaluation of Side-BranchCreation in Metal Stents by BalloonDilatationDavid Kirsch, MDJorge Lopera, MDZhong Qian, MDAwarat Janchai, MDArturo Gonzales, MDAugusto Brazzini, MDWilfrido Castaneda, MD
Louisiana State University Health Sciences CenterDepartment of RadiologyNew Orleans, Louisiana
K E Y WO R D S : side-branch dilatation,stent struts, deform a t i o n
ABSTRACTPurpose: To determine the effects of strutmesh dilatation in seven commonly usedstents used in interventional radiology.
Methods: Dilatation through the strutmesh opening on each stent was made byusing balloons to artificially create a sidebranch in translucent plastic tubing. Thestents used in the study included both bal-loon expandable stents (Palmaz stents,Omnilink, and Express) and self-expand-able stents (Symphony, SMART,Memotherm, and Wallstents). Stent diame-ters tested in this study were 8 mm and 14mm, except for the Omnilink and Express,which were 8 mm and 12 mm (commercial-ly available up to 10 mm, but were overdi-lated to 12 mm). Side-branch dilation wasmade with 4-mm and 6- mm balloons forthe 8-mm stents and 6-mm, 8-mm and 12-mm balloons for the 12/14-mm stents.
KirschJARFall03 12/29/03 2:09 PM Page 380
INTRODUCTIONThe use of metallic stents in the treatmentof peripheral arterial and venous stenosis iswell established. Indications include thetreatment of arterial and venous stenosisnot adequately treated by percutaneoustransluminal angioplasty (PTA), 1 chronicarterial occlusion,2 flow-limiting PTA-induced arterial dissections,3 as well aspost-PTA arterial or venous recoil.
There is a potential risk of side-branchstenosis and compromised flow whenmetallic stents are placed over the ostium ofsecondary branches. To solve this problemwith coronary stents, balloon dilatation ofthe side-branch ostium through the stentstrut mesh opening has been reported.There has been extensive research, both inanimal experiments4 and in vivo,5,6 on stentstrut deformity of various coronary stents.These studies have documented the effects
of sidewall balloon dilatation to maintainthe patency of side-branch vessels after pri-mary stent deployment. Deformity andmild narrowing of some stent designs werereported.4-6 However, in our literaturesearch, we did not find any documentationon the effects of sidewall dilatation withlarger peripheral vascular stents. In thisarticle, we report the results of an in vitroexperiment of serial balloon dilatationsthrough the stent strut mesh opening ofvariable stent designs commonly used in thetreatment of peripheral vascular disease.
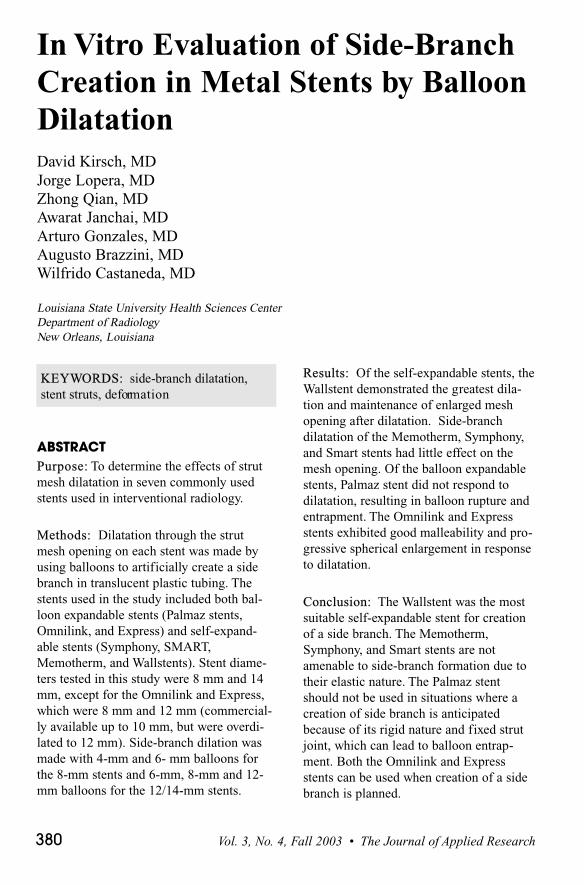
MATERIALS AND METHODSAn experimental vascular model was creat-ed from 14-mm and 12-mm inner-diametertranslucent plastic tubes for larger stents(depending on the stent diameter), and 8-mm inner-diameter tubes for medium-sizedstents. A side hole was then created withinthe tubes to mimic a side branch. Withinthe models, the stents were deployed insuch a way as to cover the side hole (Figure1A). A Bentson 0.035" guide wire (Cook,Bloomington, Ind.) was inserted throughthe stent strut covering the ostium of sidebranch (Figure 1B). Using an over-the-wiretechnique, a balloon catheter was thenadvanced inside the stent strut covering theostium of the side branch and was inflatedto 10 ATM by a pressure-control inflationdevice (Figure 1C). Shape observationsand photographs were performed before,during, and after balloon inflations.Measurements were also taken of the stentstrut mesh opening in longitudinal andtransverse dimensions with a calibratedcaliper; note in stents with intercalatedstruts, the greatest dimension was recorded.The experiment was performed twice withidentical technique.
Eight stent designs were involved inour experiment. The large-diameter stentsconsisted of three balloon-expandablestents: 308 Palmaz stent (Johnson &Johnson, Warren, NJ) dilated to 14 mm, 10-mm Omnilink (Guidant, Menlo Park,Calif.) dilated to 12 mm, and a 10-mm
Figure 1A-C. Stent deployment within theplastic tube covering the side hole (A).Insertion of a guidewire through the stent strutmesh opening that covers the ostium of theside branch (B). Balloon catheter advancedin between the stent struts in the region ofthe ostium of side branch and inflated to 10ATM by an inflation device (C).
The Journal of Applied Research • Vol. 3, No. 4, Fall 2003 381
KirschJARFall03 12/29/03 2:09 PM Page 381
Express (Boston Scientific, Natick, Mass.)dilated to 12 mm. These stents weredeployed inside the plastic tubes using bal-loons of the desired final diameter. Therationale for overdilatation of the Omnilinkand Express stents was to provide a moreuniform stent population for the large-diameter stents. Four self-expandablestents, a 14-mm Wallstent (BostonScientific, Natick, Mass.), a 14-mmSMART stent (Cordis, Warren, NJ), a 14-mm Symphony stent (Boston Scientific,Natick, Mass.), and a 12-mm Memothermstent (Bard, Murray Hill, NJ) were alsoused. Six-mm, 8-mm, and 12-mm diameterdilatation balloon catheters (Ultrathin,Boston Scientific, Natick, Mass.) were usedto sequentially dilate through the large-diameter stent strut mesh opening.
This study used three medium-diameterballoon expandable stents (294 Palmazstent dilated to 8 mm, Omnilink dilated to 8mm, and Express dilated to 8 mm) and 4self-expandable stents (8-mm Wallstent, 8-mm SMART stent, 8-mm Symphony stent,and 8-mm Memotherm stent). The strutmesh opening of these stents was sequen-tially dilated with 4-mm and 6-mm diame-ter balloons catheters.
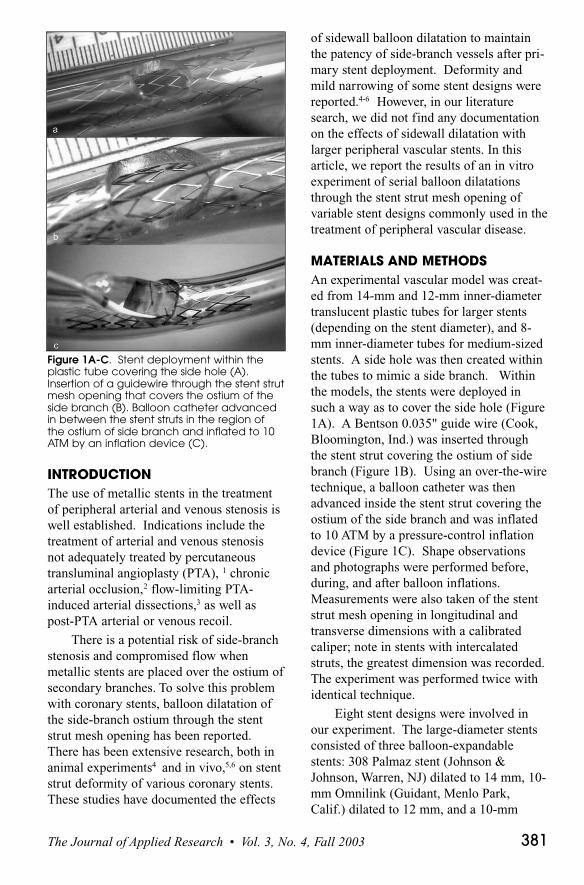
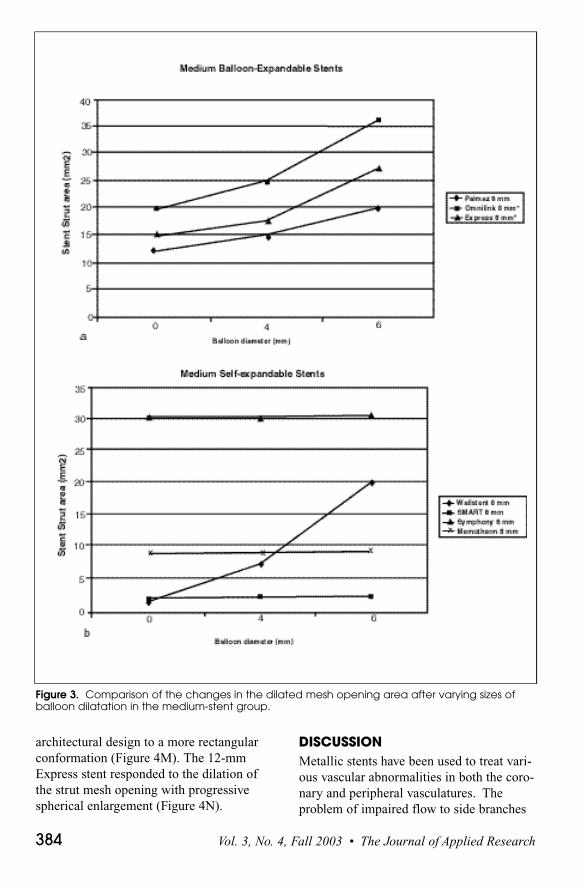
RESULTSThe results for the study were averaged andare shown in Figure 2 and 3.For the large Palmaz stent (Figure 4a) thesize of stent strut mesh opening was mini-mally increased after dilations with a 6-mmballoon without significant increase inoverall area, but the shape of the strut meshopening changed from hexagonal to circular(Figure 4b). After dilation of the largePalmaz stent with either the 8-mm or the12-mm balloon catheter, balloon ruptureand balloon entrapment within the stentstrut mesh opening was observed (Figure5). With the medium Palmaz stent, therewas progressive shape distortion fromhexagonal to circular with the 4-mm and 6-mm balloons; however, there was balloonentrapment within the stent strut mesh
opening but without balloon rupture. For both the medium and large Wallstents(Figure 4C), the size of stent strut meshopening was progressively increased fol-lowing the size of dilated balloons (Figure4D). With the largest balloon in bothWallstent groups, there was minimal distor-tion of the stent, causing 1-mm bowing ofthe dilated struts into the lumen of the stent(Figure 4D).
For the medium-sized SMART stent(Figure 4E), no change in the size or shapeof the strut mesh opening was observedafter applying any of the balloons. For thelarge SMART stent, mild irregular shapedistortion was observed after applying the12-mm balloon (Figure 4f), whereas nochange was observed after applying smallerballoons.
In both sizes of Memotherm stents(Figure 4G), 8 mm- and 12-mm diameters,separation of one stent strut joint wasobserved after applying the largest balloonsof each groups (Figure 4H).
For the 8-mm and 14-mm diameterSymphony stents (Figure 4I), minimal dis-tortion of stent strut mesh opening wasobserved after applying the largest balloonand no change after applying the small andmid-size balloons. Also, with the 8-mmand 12-mm side-strut balloon dilatation,there was joint separation in the 14-mmSymphony stent (Figure 4J).
In the 8-mm and 12-mm diameterOmnilink stent (Figure 4K), there was asignificant progressive enlargement of thestent strut mesh opening, with a change ofshape from triangular to circular. The 12-mm stent was created from a 10-mmOmnilink by overdilatation with a 12-mmballoon inside a 12-mm tube at 10 ATM.With overdilatation, there was a change ofthe stent strut design, from a more interca-lated design to more rectangular design,allowing easier entry into the strut meshopening with the guidewire and catheter(Figure 6). In the 6-mm and 8-mm bal-loons, the strut mesh opening responded
Vol. 3, No. 4, Fall 2003 • The Journal of Applied Research382
KirschJARFall03 12/29/03 2:09 PM Page 382
with progressive spherical enlargement(Figure 4L).
There was progressive sphericalenlargement with the 8-mm Express stent.
The 10-mm Express stent dilated to 12 mmwith a 12-mm balloon at 10 ATM within a12-mm tube. As with the Omnilink, overdi-latation produced flattening of the tandem
Figure 2. Comparison of the changes in the dilated mesh opening area after varying sizes ofballoon dilation in the large-stent group.
The Journal of Applied Research • Vol. 3, No. 4, Fall 2003 383
KirschJARFall03 12/29/03 2:09 PM Page 383
architectural design to a more rectangularconformation (Figure 4M). The 12-mmExpress stent responded to the dilation ofthe strut mesh opening with progressivespherical enlargement (Figure 4N).
DISCUSSIONMetallic stents have been used to treat vari-ous vascular abnormalities in both the coro-nary and peripheral vasculatures. Theproblem of impaired flow to side branches
Figure 3. Comparison of the changes in the dilated mesh opening area after varying sizes ofballoon dilatation in the medium-stent group.
Vol. 3, No. 4, Fall 2003 • The Journal of Applied Research384
KirschJARFall03 12/29/03 2:09 PM Page 384
covered by the primary stent has beendemonstrated in coronary circulation.Investigators have employed balloon dila-tion through the stent strut covering theostium of side branch as a method of treat-ing such compromised side-branch ves-sels.4-7 Problems after balloon dilationthrough stent strut opening covering theside-branch ostium of coronary stent havebeen reported in the literature. These prob-lems include balloon entrapment between
the stent strut,8 as well as stent deformitywith and without some degree of stenosiswithin the stent.4-6 Baldus et al havedesigned a new balloon-expandable side-branch stent with larger cells in the centerof the stent for the facilitation of angioplas-ty and stenting of side-branch stenosis incoronary lesions.9 Balloon dilation andstenting through the stent strut mesh open-ing covering side-branch ostium has onlybeen reported and approved for compro-mised side branches of coronary lesions. Inour general practice, we also encounter thesame situation in the peripheral vasculature.Potential problems with side-branch cover-ing include covering of the hypogastricartery during iliac stenting, covering of themajor venous confluences during SVCstenting, covering of the hepatic veins dur-ing IVC stenting, accidental covering of thecontralateral iliac during iliac stenting, andin the biliary system with hilar stricture ofthe biliary system with stent covering of thecontralateral hepatic duct. Although in mostcases covering these side branches has nosignificant immediate sequela, the sidebranches may develop compromised flowand thrombosis. The stents for peripheraland central vasculatures have differentproperties than coronary stents, includingthe diameter of stent, size of stent strutmesh openings, configuration of the mesh,and mechanical response of the stent to bal-loon dilatation. We investigated the effectsof dilatation through the strut mesh openingin 6 stent designs that we currently use forperipheral and central vascular lesions.
The Wallstent is composed of Elgiloy, ametal alloy woven into a criss-cross patternto form a tubular braid configuration. Thisbraided design provides high complianceand radial strength. In both the small- andlarge-diameter Wallstents, there was signifi-cant expansion of the mesh opening of thestent and minimal shape distortion afterserial balloon dilatation. Balloon angio-plasty through the stent strut mesh openingresulted in displacement of the struts. Thisoverlap of the struts near the area of dilata-
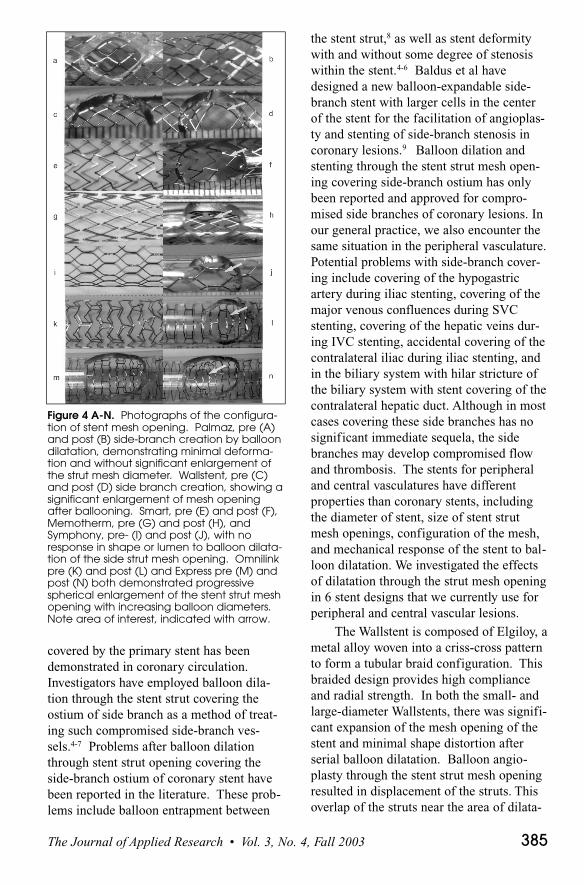
Figure 4 A-N. Photographs of the configura-tion of stent mesh opening. Palmaz, pre (A)and post (B) side-branch creation by balloondilatation, demonstrating minimal deforma-tion and without significant enlargement ofthe strut mesh diameter. Wallstent, pre (C)and post (D) side branch creation, showing asignificant enlargement of mesh openingafter ballooning. Smart, pre (E) and post (F),Memotherm, pre (G) and post (H), andSymphony, pre- (I) and post (J), with noresponse in shape or lumen to balloon dilata-tion of the side strut mesh opening. Omnilinkpre (K) and post (L) and Express pre (M) andpost (N) both demonstrated progressivespherical enlargement of the stent strut meshopening with increasing balloon diameters.Note area of interest, indicated with arrow.
The Journal of Applied Research • Vol. 3, No. 4, Fall 2003 385
KirschJARFall03 12/29/03 2:09 PM Page 385

tion maintained the dilated lumen and con-formed to the spherical shape/size of theballoon.
The Palmaz stent is made of biocom-patible 316L stainless steel, laser cut withclosed-cell geometric design, forming arepeating diamond configuration. Due tothe hexagonal cell construction of thePalmaz10 stent strut opening, balloon rup-ture and entrapment occurred when expand-ing the 8-mm and 12-mm balloon throughthe stent strut of the 14-mm diameterPalmaz stent. In the 8-mm diameterPalmaz stent, there was progressive shapedistortion from hexagonal to circular withthe 4-mm and 6-mm balloons but withoutsignificant increase in overall diameter;there was also balloon entrapment withinthe stent strut with larger balloon diameter.These results corroborate the potential riskof balloon rupture and entrapment whendilating through the strut mesh opening ofthe Palmaz stent.8
The Express is a laser cut, stainlesssteel, balloon expandable stent incorporat-ing Tandem Architecture™ system, whichintegrates wide Macro™ elements for radialstrength and Micro™ elements for increasedconformability. The Express can be overdi-lated by 1 mm to 2 mm with minimal sacri-fice in radial strength. With overdilatationof the stent the struts open to a more rec-tangular configuration, making it moreamenable to side-strut access for dilatation.
In both sizes, the Express demonstratedmalleability, conforming to the shape of theballoon with progressive dilatation of theside-strut mesh opening.
The Omnilink, is a laser-cut, 316Lstainless steel balloon expandable stent.The stent has a dense scaffolding patternproviding little unsupported surface area.The stent can be overdilated to providegreater diameter to the strut mesh openingand the 10-mm Omnilink dilated to 12 mmallowed easy access through the stent strut.The 8-mm Omnilink responded well todilatation with progressive sphericalenlargement. The stainless steel core of thestent was also malleable, with balloonexpansion through the strut mesh opening,providing progressive increasing dilatationof the stent through the strut.TheSymphony stent is a self-expanding hexag-onal designed nickel-titanium alloy stent.The Symphony expands to the uncon-strained diameter when exposed to bodytemperature. The large strut mesh openingof the Symphony stent demonstrated nodeformity with side-branch dilatation inboth the 8-mm and 14-mm stents.
The SMART stent is laser cut from aNitinol alloy of nickel and titanium. Thestruts are hexagonal and connected througharticulations, which provide shape memoryand spring-like recoverability. In the 14-mm SMART stent, there was no alterationin size or shape distortion of the stent strut
Figure 5. Balloon rupture and entrapmentwithin the stent strut mesh opening of thePalmaz stent after dilatation.
Figure 6. Flattening of the intercalateddesign to more rectangular design after 2-mm overdilatation of the Omnilink.
Vol. 3, No. 4, Fall 2003 • The Journal of Applied Research386
KirschJARFall03 12/29/03 2:09 PM Page 386
mesh opening with the 6-mm and 8-mmballoon. After applying the largest (12-mm) balloon, one of the SMART stentjoints disarticulated but with minimal over-all shape deformity. No changes were alsoobserved in the 9-mm SMART stent.
The Memotherm stent has similarproperties to the SMART stent. TheMemotherm stent is self-expandable andcomposed of a biocompatible Nitinol mem-ory metal laser cut into a diamond shape.We observed no change in size or shape ofthe stent strut mesh opening of the 12-mmMemotherm stents until separation of 1joint occurred after dilatation using thelargest balloon. The basic design of themesh of the SMART and Memotherm stentis very similar. The triangular configura-tions of the struts with articulationsbetween the rows of the struts resulted inminimal change in the shape or size of thestrut mesh opening after balloon dilatation,suggesting they may not respond to side-branch dilatation.
CONCLUSIONSIn our study of the self-expandable stents,the Wallstent demonstrated the most signif-icant increase in side-branch size and wasthe most appropriate self-expandable stentdesigns for balloon dilatation through thestent strut mesh opening covering the side-branch ostium. The Wallstent was the mostconforming of the stents and demonstratedappropriate distortion to theoretically main-tain side-branch patency after angioplastythrough the stent strut mesh opening. Dueto the minimal size increment in the meshopening of SMART and Memotherm stents,they appear not to respond to side-branchdilatation required for side-branch protec-tion. Of the balloon expandable stents, theOmnilink and the Express stents demon-strated malleability, making it possible toperform to adequate side-branch dilatation.Also, overdilatation of the Omnilink andExpress appears to facilitate access to theside branch. With the Palmaz stent, balloonrupture and entrapment are real potential
complications and side-branch dilationshould be avoided. Further trials will beneeded to corroborate the relevance of theseresults in vivo.
ACKNOWLEDGMENTThe following companies donated teststents: Johnson & Johnson, Guidant,Boston Scientific, Cordis, and Bard.
REFERENCES1. Johnston KW, Rae M, Hogg-Johnston SA, et al.
Five year results of a prospective study of percu-taneous transluminal angioplasty. Ann Surg.1987;206:403-413.
2. Vorwerk D, Geunther RW, Schurmann K, et al.Primary stent placement for chronic iliac arteryocclusions: Follow-up results in 103 patients.Radiology. 1995;194:745-749.
3. Becker GJ, Palmaz JC, Rces CR, et al.Angioplasty-induced dissections in human iliacarteries; management with balloon-expandableintraluminal stents. Radiology. 1990;176:31-38.
4. Pomirantz RM, Ling FS. Distortion of Palmaz-Schatz stent geometry following side-branch bal-loon dilatation through the stent in a rabbitmodel. Catheter Cardiovasc Diagn.1997;40:422-426.
5. Ormiston JA, Webster MW, et al. Stent deformityfollowing simulated side-branch dilatation: acomparison of five stent designs. CatheterCardiovasc Intervent. 1999;47:258-264.
6. Kinoshita T, Kobayashi Y, et al. Basic investiga-tions; difference in security of stent jail betweenPalmaz-Schatz, NIR, and multi-link stents; theeffect of balloon inflation through stent struts.Catheter Cardiovasc Intervent. 1999;48:230-234.
7. Prasad N, Ali H, et al. Short- and long-term out-come of balloon angioplasty for compromisedside branches after intracoronary stent deploy-ment. Catheter Cardiovasc Intervent.1999;46:421-424.
8. Chan AW, Lohavanichleutr K, et al. Balloonentrapment during side-branch angioplastythrough a stent. Catheter Cardiovasc Intervent.1999;46:202-204.
9. Baldus S, Hamm CW, et al. Protection of side-branches in coronary lesion with a new stentdesign. Catheter Cardiovasc Diagn.1998;45:456-459.
10. Allum CA, Lacina T, Watkinson AF. Metallicstent-individual designs and characteristics.Semin Intervent Radiol. 2001;18:191-204.
The Journal of Applied Research • Vol. 3, No. 4, Fall 2003 387
KirschJARFall03 12/29/03 2:09 PM Page 387