risk factors for systolic dysfunction and ventricular dilatation in hypertrophic cardiomyopathy
TRANSCRIPT

International Journal of Cardiology 44 (1994) 225-233
Risk factors for systolic dysfunction and ventricular dilatation in hypertrophic cardiomyopathy
Roland Bingisser, Reto Candinas, Jakob Schneider, Otto M. Hess*
Deparfment of Internal Medicine. Cardiology, and Institute of Pafhhology, Universiry Hospital, Riimisrrasse lO0, Zurich, S~~i~=er~and
(Received 28 September 1993; accepted 23 December 1993)
Abstract
The history of an 18-year-old male with hypertrophic cardiomyopathy (HCM) and ventricular dilatation is presented and the literature on systolic dysfunction and ventricular dilatation in patients with HCM is StatisticaIly analyzed in search of risk factors. The patient was followed for ‘7 years when he developed recurrent ventricular fibrillation, left ventricular dilatation and low cardiac output. An automatic cardioverter-defibrillator was implanted but the patient
died of electro-mechanical dissociation. In order to define risk factors for systolic dysfunction and ventricular dilata- tion in HCM, the literature data of 17 patients with this complication were compared to a group of 139 consecutive patients with HCM from our hospital. The risk factors identi~ed were a more markedly increased septaI(20.i vs. 18.0 mm, P c 0.05) and posterior wall thickness (13.6 vs. 11.0 mm, P < 0.001) in the patients subsequently developing systolic dysfunction and ventricular dilatation, whereas age, sex and the ratio between septal and posterior wall thickness were not significantly different between the two groups. A severely increased ventricular mass appears to be a risk factor for the development of systolic dysfunction with ventricular dilatation in HCM. Prognosis is usually poor and the reported case showed fatal ventricular arrhythmia despite the implantation of an automatic cardioverter-
defibrillator.
Key words: Hypertrophic cardiomyopathy; Systolic dysfunction; Ventricular dilatation; Ventricular tachyarrhythmias; Myocardial histology
1. Introduction
Hy~~rophic cardiomyopathy (HCM) is char- acterized by asymmetric hypertrophy of the left ventricle with or without systolic outflow tract obstruction and diastolic compliance failure [ 1,2].
* Corresponding author.
Typically a small, hypercontractile left ventricle is found with increased ventricular filling pressures. Clinical follow-up is usually benign but cardiac symptoms such as dizziness, dypnoea, and syncope as well as diastolic heart failure and sudden car- disc death can occur. Annual mortality rates have been reported to be in the range of 2-6% [ 1,181, whereby most patients die suddenly and only a
0167-5273/94/%07.00 0 1994 Elsevier Science Ireland Ltd. All rights reserved. SSDI 0167-5273(94)01998-Q

226
minority develops heart failure with low-output
syndrome. Rarely, impaired systolic function with dilatation of the left ventricle can be observed but only a few cases have been reported until now [3-141. Traditionally, it was thought that ventricu- lar dilatation can not occur in HCM because myo-
cardial stiffness is increased due to the extensive scarring of the ventricular wall. Thus, systolic overstretch of the cardiac muscle and ventricular dilatation is prevented in most patients [ 1,2]. How- ever, an increase in heart size can often be observed due to the increase in left atria1 volume as a result of diastolic compliance failure.
Proposed risk factors for systolic dysfunction and left ventricular dilatation in HCM are midven- tricular obstruction [ 111, the extent of the myocar- dial hypertrophy [9] and genetic predisposition [17]. Since midventricular obstruction is a rare form of hypertrophic cardiomyopathy, left ven- tricular dilatation is described only in four cases
with this form of HCM, and it may be associated with apical myocardial infarction [ 11. There is only one report about a family with HCM which show- ed a tendency for systolic dysfunction and left ven-
tricular dilatation [ 171. Overall, true ventricular dilatation has been reported to occur in approx- imately l-5% of patients with HCM [9,11,15].
The purpose of the present study was: (a) to de-
scribe a patient with HCM who developed severe systolic dysfunction and died; and (b) to compare the literature data with the data of 139 patients with HCM from our hospital in order to define
risk factors for systolic dysfunction.
2. Case report
2.1. Clinical history and physical examination An 18-year-old man was admitted to a
peripheral hospital after he had been resuscitated for ventricular fibrillation. He was complaining of dizziness during moderate exercise for the last 7 years. He was seen by his family doctor because of this symptom, but physical examination and chest X-ray were always normal.
Three years before admission the patient was re- examined because of dyspnoea at exercise. The heart was slightly enlarged in the chest X-ray (Fig. 1, 1989) and the ECG showed a newly developed left bundle branch block.
Fig. I. Chest X-ray demonstrating progressive cardiac dilata- tion in a patient with hypertrophic cardiomyopathy from 1986
(top) to 1989 (middle) and 1992 (bottom), respectively.

R. Bingisser et al. / ht. J. Cardiol. 44 (1994) 225-233 227
Echocardiography revealed mild asymmetric hypertrophy of the interventricular septum (11 mm) with a mildly dilated left atrium (Table 1).
Bicycle ergometry elicited a normal physical work- ing capacity (175 W for 2 min) with a drop in systolic blood pressure at maximal work load. Only a few ventricular premature beats were
observed during the exercise test. On the day of admission the patient was at
school and suddenly fell from his chair. He was hospitalized after successful cardiopulmonary re-
suscitation. The following day he developed hypo- tension and oliguria. Ventricular fibrillation reoccurred on the 9th and 12th day after admis- sion. Amiodarone (15 g over 10 days) was given
and ventricular arrhythmias disappeared. For fur- ther evaluation the patient was admitted to our hospital on the 23rd day after resuscitation.
Table I Patient data
1989 1992 Normal
values
Chest X-ray:
CTR (‘+‘A) 50 62 <50
EGG
HR (bpm) 80 60 <IO0
PQ (s) 0.12 0.18 <0.21
QRS (s) 0.12 0.18 <0.12
QT ts) 0.4 0.52 < 0.40
Exercise test
PWC (Yu)
ST (mV)
RR (mmHg)
Rest
Max.ex.
100 > 80
0.05 <O.l
80/60
155160
Echocardiogramm
Septum (mm) 11 14 < 12 PW (mm) 9 10 <12 SIPW 1.2 1.4 < 1.4
FS (“/u) 41 17 29-46
Patient data. CTR, Cardio-thoracic ratio; ECG, Electrocar- diogram; HR, heart rate; PQ, PQ-interval; QRS, QRS-interval;
QT, QT-interval; PWC, physical working capacity; ST, ST-
segment depression; RR, cuff blood pressure; max ex., maximal
exercise; Septum, septal wall thickness; PW, posterior wall thickness; S/PW, septahposterior wall thickness ratio; FS, frac-
tional shortening.
Physical examination. The patient was able to
walk with slight ataxia on tandem gait. Orienta- tion in regard to place and time was poor. The blood pressure was 120180 mmHg and the pulse was regular at 60 bpm. There were no heart mur-
murs and peripheral pulses were normal. Rales over the basal pulmonary regions were the only signs of congestive heart failure.
2.2. Laboratory findings Chest X-ray. An enlarged cardiac silhouette
with pulmonary congestion and baso-apical redis- tribution was found. Compared to the X-ray of
1986 and 1989, the heart size had increased con- siderably with pronounced lung congestion (Fig. 1, 1992).
ECG. Sinus bradycardia and a left bundle
branch block (QRS duration 0.16 s.) were found in the routine electrocardiogram.
Echocardiography. Standard two-dimensional and M-Mode echocardiography were performed
using a Hewlett-Packard 77020 AC unit. A moder- ately thickened (14 mm) septal wall was found with a normal LV posterior wall (10 mm). Generalized hypokinesia of the left ventricle was
seen with a shortening fraction of 17% (normal 29-46%). Left ventricular ejection fraction was 35% (normal 2 55%). The left atrium was severely dilated (65 mm, normal range 15-40 mm) and
mild mitral regurgitation was found. Early diastolic (E-wave) and atria1 (A-wave) flow veloci- ty were normal and showed no restrictive filling pattern. There was mild tricuspid regurgitation
with a right ventricular systolic pressure of 25 mmHg above right atria1 pressure.
Left and right heart catheterization. Heart rate was 57 bpm. Cardiac index was 1.6 limin per m2
according to the Fick method. Left ventricular peak systolic pressure amounted to 95 mmHg, left ventricular end-diastolic pressure to 28 mmHg. Mean right atria1 pressure was 14 mmHg, right
ventricular systolic pressure 48 mmHg and right ventricular end-diastolic pressure 23 mmHg. Pul- monary capillary wedge pressure was 21 mmHg, aortic pressure was 95/75 mmHg with a mean of 80
mmHg. Mixed venous oxygen saturation was 37% and aortic oxygen saturation 97%. Systemic vascu- lar resistance was 1640 dyn s cmm5 (normal range

228 R. Bingisser et al. / Int. J. Cardiol. 44 (1994) 225--733
I 1350) and pulmonary vascular resistance was 174 dyn s cmm5 (normal range: I 120).
Left ventricular cineangiography showed mild
enlargement of the left ventricle (end-diastolic volume 106 ml/m2, normal range 50-90 ml/m’, 25) with generalized hypokinesia. Ejection fraction of a post-extrasystolic beat was 45% (normal range
2 57%). Coronary angiography revealed normal but
slightly enlarged coronary arteries. No milking
phenomenon was observed. Electrophysiologic examination. Serum amiodar-
one level was 10.4 mg/l (desethylamiodarone 1.1 mg/l) after intravenous administration of a total
dose of 15 g amiodarone at the time of elec- trophysiologic stimulation. Under these blood serum levels the sinus node recovery time was 1700 ms and the effective refractory period of the AV
node 420 ms. The atrioventricular-His bundle time was 105 ms and the His bundle-ventricular interval 60 ms. With programmed right ventricular stimu- lation (3 extra stimuli) no ventricular tachycardia
was induced.
2.3. Follow-up An automatic implantable cardioverter-defibril-
lator (AICD, Guardian ATP 4210, Teletronic pac- ing systems) was implanted on the 32nd day because of repeated ventricular fibrillation despite adequate antiarrhythmic therapy. Magnesium and
potassium serum levels were always normal (0.82 mmol/l and 5.0 mmol/l after implantation).
Repeated testing of the defibrillator system was carried out successfully during the implantation procedure. The following week the patient was in a stable condition and was discharged from the in- tensive care unit after a second control of the AICD. The same night the patient died of electro-
mechanical dissociation despite application of seven defibrillator shocks at maximal energy of 30 J.
2.4. Patho-anatomical findings At autopsy the left ventricle was macroscopical-
ly enlarged (Fig. 2) with the typical asymmetric septal hypertrophy. Septal thickening was most
prominent halfway between the base and the apex. Septal wall thickness was 20 mm and posterior
Fig. 2. Longitudinal section of the heart through the midpoint
of the mitral valve and the center of the aortic valve. Asym-
metric thickening of the interventricular septum (right) can
clearly be seen. Septal thickness is maximal (20 mm) in the mid-
portion of the septum 3-4 cm below the aortic valve. Subendo-
and subepicardial layers are strikingly pale and whitish. The
right ventricular wall is hypertrophied.
wall thickness 14 mm. The inner layer of the left ventricular wall was strikingly pale or whitish,
especially the tip of the posterior papillary muscle. The right ventricular wall thickness (5 mm) was in- creased. The pattern of hypertrophy corresponded to type II of Maron et al. [20].
Histologic examination revealed marked fiber disarray in the thickened ventricular septum (Fig. 3). The disorganized septal architecture involved
approximately 70-75X of the septal cut surface in a plane perpendicular to the long axis of the left ventricle. The mean muscle fiber diameter was 29.2 + 9.0 pm in the disorganized and hyper- trophied septum and 13.3 + 4.1 pm in the suben- docardial area of the normally arranged muscle
fibers (normal value 5 23 pm). Interstitial collagen was not only increased in the disorganized septal regions but also in the subendocardial regions with normal architecture. The posterior wall showed
extensive fibrosis not only of the inner but also of the outer layers but no muscle fiber disarray. In

R. Bingisser et al. / In:. J. Cardiol. 44 (1994) 225-233 229
Fig. 3. Histologic section (Hematoxylin-Eosin stain) of the
interventricular septum at high (top; x 300) and low magnific-
ation (bottom; x 150). The abnormally arranged muscle fibers
in the hypertophied septal wall can clearly be seen.
these regions there were also scattered infiltrates of lymphocytes and macrophages accompanied by
small scars. Most of these scars consisted of very loosely arranged thin collagen fibers.
3. Materials and methods
3.1. Comparison to literature data Data from seventeen patients with HCM and
systolic dysfunction with left ventricular dilatation have been published including clinical and echo-
cardiographic data [5,8-l 11. These patients have been compared to a group of 139 patients with HCM from our hospital [ 191. Because the 17 pati- ents from the literature were medically treated, the
79 surgically treated patients from the control group were excluded from the analysis of the risk factors.
3.2. Statistical analysis The 60 medically treated patients (control
group) have been compared to the 17 patients from the literature using a Student’s t-test for un-
paired groups. The groups were equal in regard to age and sex (P > 0.1) but the follow-up time was significantly longer in the control group (8.9 vs. 6.2 years, P < 0.05) than in the literature group.
4. Results
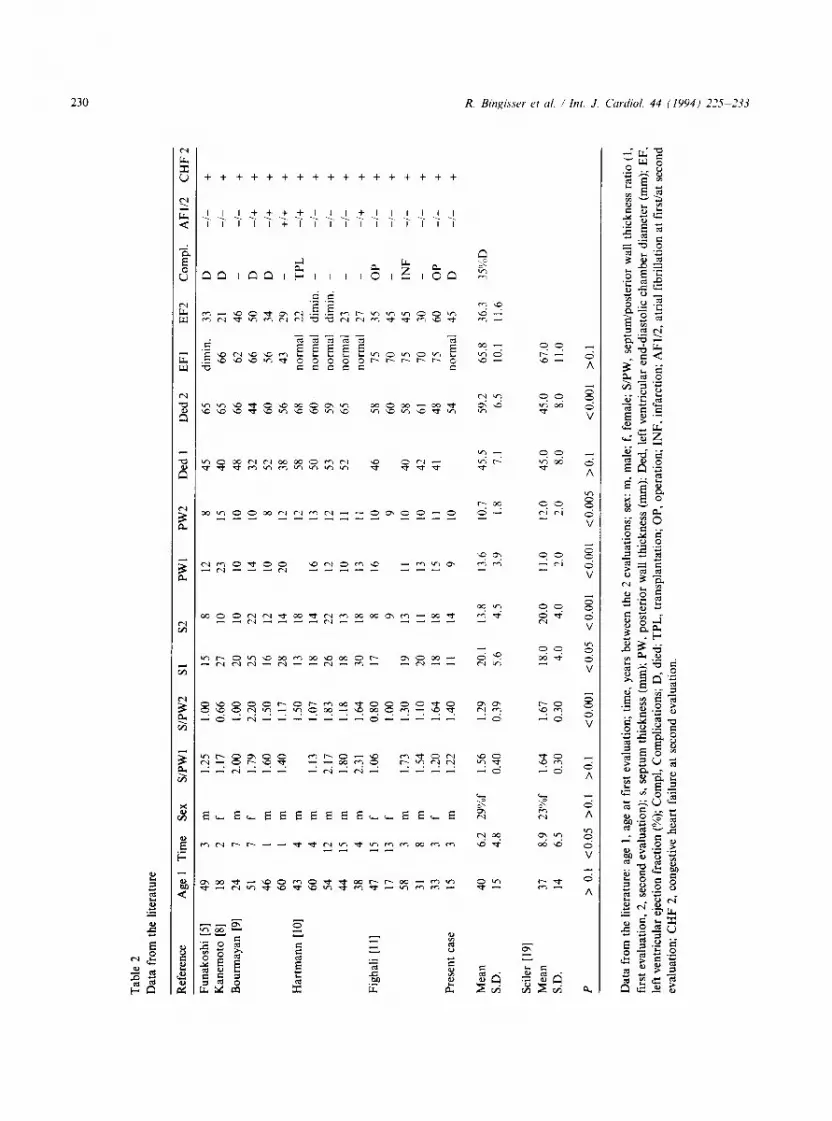
At the first examination the septal/posterior wall ratio, left ventricular end-diastolic diameter and
ejection fraction were not significantly different (P > 0.1) between our group and the group from the literature (Table 2). Differences between the two groups were observed in regard to septal wall
thickness (20.1 mm in the group from the litera- ture, 18.0 mm in our control group, P < 0.05) and posterior wall thickness (13.6 mm vs. 11 .O mm in the control group, P < 0.001).
At the second examination the mean septal/pos- terior wall ratio in the patients from the literature declined from 1.56 to 1.29 (P < 0.05). This was mainly due to septal wall thinning from 20.1 to
13.8 mm (P < O.OOS), whereas the posterior wall thinning (from 13.6 to 10.7 mm) was only mild (P < 0.01). In the control group septal/posterior wall ratio remained unchanged during the follow-up.
Left ventricular end-diastolic chamber diameter increased significantly from 46 to 59 mm (P < O.OOl), whereas ejection fraction decreased from 66 to 36% (P < 0.001) in the 17 patients (Table 2).
In the group developing systolic dysfunction and ventricular dilatation six of 17 patients died or underwent transplantation (35%), two had to be operated and one suffered from myocardial infarc- tion. In the control group from our hospital the mortality rate at 6 years follow-up was 22% in the medically and 8% in the surgically treated sub- groups.
Interestingly, only five of 17 patients from the literature (including our own patient) developed atria1 fibrillation while 14 of 17 showed wall- thinning. All patients with an ejection fraction below 50% developed left ventricular dilatation and congestive heart failure.
Tab
le
2
Dat
a fr
om
the
liter
atur
e
Ref
eren
ce
Age
1
Tim
e Se
x S/
PWI
SlPW
2 Sl
s2
PW
I PW
2 D
ed
1 D
ed
2 E
FI
EF2
C
ompl
. A
Fli2
C
HF2
Funa
kosh
i (5
1
Kan
emot
o [8
]
Bou
rmay
an
[9]
Har
tman
n [I
O]
Figh
ali
[ 1 l]
Pres
ent
case
Mea
n
S.D
.
Seile
r [ 1
91
Mea
n
SD.
P
49
3 m
1.
25
1.00
I5
8
18
2 f
1.17
0.
66
27
IO
24
7 m
2.
00
1.00
20
10
51
7 f
1.79
2.
20
25
22
46
I m
1.
60
1.50
16
I2
60
1 m
1.
40
1.17
28
14
43
4 m
1.
50
13
18
60
4 m
1.
13
I .07
18
14
54
12
m
2.17
1.
83
26
22
44
15
m
1.80
1.
18
18
13
38
4 m
2.
31
1.64
30
18
47
15
f 1.
06
0.80
17
8
17
I3
f 1.
00
9
58
3 m
1.
73
I .30
19
13
31
8 m
1.
54
1.10
20
II
33
3 f
1.20
1.
64
18
18
15
3 m
1.
22
1.40
II
14
40
15
37
14
6.2
29%
f 1.
56
1.29
4.8
0.40
0.
39
8.9
23%
f 1.
64
1.67
6.5
0.30
0.
30
20. I
13.8
5.6
4.5
18.0
20
.0
4.0
4.0
12
23
10
14
10
20
16
12
10
13
16
8 15
10
IO
8 12
12
13
12
11
11
10
9 10
IO
II
IO
45
65
40
65
48
66
32
44
52
60
38
56
58
68
50
60
53
59
52
65
II
13
15 9
46
40
42
41
58
60
58
61
48
54
dim
in.
33
D
-l-
+
66
21
D
-l-
+
62
46
- -I
- +
66
50
D
-i+
+
56
34
D
-I
+ +
43
29
-
+I+
+
norm
al
22
TPL
4-
b +
no
rmal
di
min
. -
-/-
+
norm
al
dim
in.
- -l
- +
no
rmal
23
_
-/-
+
norm
al
27
_ -l+
+
75
35
O
P -/
- +
70
45
-
-/-
+
75
45
INF
-/
- +
70
30
-
-/-
+
75
60
OP
-l-
+
norm
al
45
D
-l-
+
13.6
10
.7
45.5
59
.2
65.8
36
.3
3 5%
D
3.9
1.8
7.1
6.5
10.1
11
.6
11.0
12.0
45
.0
45.0
67
.0
2.0
2.0
8.0
8.0
11.0
> 0.
1 <0
.05
>O.l
>O.l
<O.O
Ol
<0.0
5 <O
.OO
l <O
.OO
l <0
.005
>O
.l <
O.O
Ol
>O.l
Dat
a fr
om
the
liter
atur
e:
age
1, a
ge
at
firs
t ev
alua
tion;
tim
e,
year
s be
twee
n th
e 2
eval
uatio
ns;
sex:
m,
mal
e:
f, fe
mal
e;
S/PW
. se
ptum
/pos
teri
or
wal
l th
ickn
ess
ratio
(1
, fi
rst
eval
uatio
n,
2, s
econ
d ev
alua
tion)
; s,
sep
tum
th
ickn
ess
(mm
);
PW,
post
erio
r w
all
thic
knes
s (m
m);
D
ed,
left
ve
ntri
cula
r en
d-di
asto
lic
cham
ber
diam
eter
(m
m);
E
F.
left
ven
tric
ular
ej
ectio
n fr
actio
n (%
); C
ompl
, C
ompl
icat
ions
; D
, di
ed;
TPL
, tr
ansp
lant
atio
n;
OP,
op
erat
ion;
IN
F.
infa
rctio
n;
AF1
/2,
atri
al
fibr
illat
ion
at
firs
t/at
seco
nd
eval
uatio
n;
CH
F 2,
con
gest
ive
hear
t fa
ilure
at
se
cond
ev
alua
tion.

R. Bingisser et al. / hr. J. Cardiol. 44 (1994) 225-233 231
5. Discussion
Approximately 17 patients with systolic dys- function and left ventricular dilatation have been described in the literature including our present case (Table 2); this underlines the relatively rare
occurrence of this complication in HCM. Progno- sis is usually poor in these patients (35% mortality rate in 6.2 years) compared to 22% after 6 years in the medically and 8% in the surgically treated
patients of our control group [ 191. The incidence of systolic dysfunction is higher
than the occurrence of left ventricular dilatation [13,14], because only about a quarter of the pati- ents with reduced left ventricular ejection fraction showed chamber dilatation [14]. This observation suggests that systolic dysfunction preceeds cham-
ber dilatation, or that the left ventricle can not dilate due to its severe structural alterations in three-quarters of the patients.
5.1. Previous observations of left ventricular dilata-
tion in HCM The first report describing the typical patho-
anatomical features of HCM were written by
Brock and Teare in the late fifties [26-281. In 1973 Roberts and coworkers presented an autopsy series of 32 patients with hypertrophic cardiomyopathy. Only one patient showed left ventricular dilatation
[29]. In 1977 Hess reported the case of a patient with hypertrophic cardiomyopathy who suffered from acute myocardial infarction despite normal coronary arteries. The patient died after rapid pro-
gression of congestive heart failure [ 181. Dilatation of all heart chambers was found with a septal thickness of 16 mm and posterior wall thickness of 12 mm (septal/posterior wall thickness ratio 1.3,
generalized fibrosis and muscle fiber hypertrophy with fiber diameters up to 90 pm). At that time it was not clear whether this case represented an in- termediate type between hypertrophic and dilated
cardiomyopathy or if this was the first case of hy- pertrophic cardiomyopathy with secondary dilata- tion of the left ventricle. In 1979 ten Cate and Roelandt 131 described two cases of hypertrophic obstructive cardiomyopathy who showed progres- sive left ventricular dilatation after septal myec- tomy. The same year Maron [ 151 reported the
occurrence of transmural myocardial infarction in patients with hypertrophic cardiomyopathy without significant atherosclerosis of the ex- tramural coronary arteries. In the reported series
transmural infarction was found in seven of 48 non-surgically treated patients who died of hyper- trophic cardiomyopathy. In two of these seven pa- tients there was a follow-up of 8 and 9 years,
respectively, which showed the evolution from a non-dilated to a dilated left ventricle coinciding with symptomatic deterioration (4% incidence of left ventricular dilatation). In the eighties several
cases with dilatation of the left ventricle as a rare complication of unoperated hypertrophic cardio- myopathy were published in Japan [5-81. Fighali
et al. [ 1 l] presented the clinical follow-up of 62 pa- tients with hypertrophic cardiomyopathy (mean observation time 8 years); three patients developed a dilated left ventricle with generalized
hypokinesia. None had coronary artery disease (5% incidence of left ventricular dilatation). The overall incidence of congestive heart failure in hy- pertrophic cardiomyopathy ranged from 4 to 8% [ll-141.
5.2. Pathophysiologic mechanisms Several mechanisms which could explain systo-
lic dysfunction and progressive dilatation have been discussed: transmural myocardial infarction with extensive scarring resulting from coronary muscle bridging, coronary vasospasms, coronary
embolization in patients with atria1 fibrillation, small vessel disease [ 161 and severe mismatch be- tween oxygen supply and demand in the presence of massive LV hypertrophy or disruption of LV
geometry after septal myotomy. The exact anatomic basis for the development of cardiac dilatation in hypertrophic cardiomyopathy re- mains, however, speculative.
Myocardial ischemia and ultimately, infarction may be an important mechanism in the develop- ment of myocardial scarring because of decreased vasodilator reserve [3 1,321 and reversible Thal- lium-201 myocardial perfusion defects [23,24] in patients with hypertrophic cardiomyopathy. Other factors which may be involved are an abnormal calcium homeostasis [30] and genetically mediated

232
differences in the expression of the hypertrophic process [5-8,17,19].
5.3. Risk factors for left ventricular dilatation in HCM
The incidence of coronary artery disease, coro- nary myocardial bridging, and left ventricular
outflow tract obstruction appears to be similar in patients who developed left ventricular dilatation and in those who did not [1 11. Previous septal myotomy-myectomy was not found to be a risk-
factor by Fighali [11], but in our hospital only 1.5% of the medically treated and 12.5% of the surgically treated patients showed progressive left ventricular dilatation (defined as a > 1% increase
in LV end-diastolic diameter/year and a > l”Al decrease in the shortening fraction/year) for an ob- servation period of 8.9 years [33].
Wall thinning appears to be a prerequisite for
systolic dysfunction and left ventricular dilatation: Spirit0 and Maron [ 131 found that none of 65 adult patients showed an increase in left ventricu- lar wall size of more than 5 mm over a follow-up
period of 3-6 years but nine patients demonst- rated significant wall-thinning of 5-9 mm with an increase in LV end-diastolic diameter during the same observation period. The absolute cavity size
remained, however, in seven of the nine patients within normal limits. Eight of the nine patients developed congestive heart failure during the follow-up and live died or underwent cardiac
transplantation. In another study Spirit0 et al. [ 141 followed 67 patients of whom 13 had a left ventric- ular ejection fraction below 50%. Eight of these 13 patients showed a decrease in left ventricular wall
thickness during follow-up, whereas ten had a left ventricular cavity size which remained within nor- mal limits. A significant proportion (9%) of pa- tients with HCM develop systolic dysfunction
during long-term follow-up but left ventricular dilatation occurs only in a minority of these pa- tients (l-5%).
6. Conclusions
In HCM with systolic dysfunction the size of the left ventricle rarely increases above the upper
limits of normal, although the end-diastolic di-
R. Bingisser et ul. / ht. J. Cardiol. 44 (1994) 225-233
mension of the left ventricle enlarges somewhat in these patients compared to previous values. This relatively mild degree of dilatation is associated
with a fall in ejection fraction, but because of the absence of real compensatory dilatation, the result is a drop in stroke volume. In the present case the end-diastolic volume index was only slightly
elevated with an ejection fraction of 45%. These data considerably differ from dilated cardiomyo- pathy, in which the patient often is asymptomatic until the ejection fraction has fallen below 40”/0
with an end-diastolic volume index of around 200 ml/m2 not being unusual.
The attempt to define risk factors for systolic dysfunction and ventricular dilatation using the
data from the literature showed that patients with left ventricular dilatation have a higher extent in mean septal and posterior wall thickness, and, thus, a more severe form of left ventricular hyper- trophy. Therefore, patients with severe myocardial hypertrophy may be candidates for systolic dysfunction and may have a poor prognosis with low-output syndrome and fatal arrhythmias.
7. References
Wigle ED. Sasson Z, Henderson MA, Ruddy TD, Fulop
J. Rakowski H, Williams WG. Hypertrophic cardiomyo- pathy. The importance of the site and the extent of hyper-
trophy. A review. Prog Cardiovasc Dis 1985; 28: l-83.
Frank S. Braunwald E. Idiopathic hypertrophic subaortic
stenosis: clinical analysis of 126 patients with emphasis on
the natural history. Circulation 1968; 35: 759-763.
ten Cate FJ, Roelandt J. Progression to left ventricular
dilatation in patients with hypertrophic obstructive car- diomyopathy. Am Heart J 1979; 97: 762-765.
Beder SD, Gutgesell HP. Mullins CE, McNamara DG.
Progression from hypertrophic obstructive cardiomyo-
pathy to congestive cardiomyopathy in a child. Am Heart
J 1982; 104: 155-156.
Funakoshi M, Imamura M, Sasaki J. Seventeen year
follow up of a patient with hypertophic cardiomyopathy which progressed to dilated cardiomyopathy. Jpn Heart J 1984; 25: 805-809.
Fujiwara H, Onodera T. Tanaka M. Progression from hy-
pertrophic obstructive cardiomyopathy to typical dilated cardiomyopathy-like features in the end stage. Jpn Circ 1984; 48: 1210-1214.
Yutani C, lmakita M, Ishibashi-Ueda H. Three autopsy cases of progression to left ventricular dilatation in pa-
tients with hypertrophic cardiomyopathy. Am Heart J 1985; 109: 545-553.

R. Bingisser et al. / ht. J. Cardiol. 44 (1994) 225-233
8
9
10
11
12
13
14
15
16
17
18
19
Kanemoto N. Kawana M. Imaoka C. Goto Y. A case
showing a rare evolution from hypertrophic obstructive cardiomyopathy to “dilated” cardiomyopathy demonstr-
ated by echocardiography. Jpn Heart J 1987; 28: 445-450.
Bourmayan C, Desnos M, Baragan J. Progression from
hypertrophic obstructive cardiomyopathy to dilated car-
diomyopathy in 4 patients (in French). Arch Mal Coeur
1990; 83: 537-542.
Hartmann A, Olbrich HG, Hopf R. Schneider M, L&se
B, Kaltenbach M. Left ventricular dilatation in the natu-
ral course of hypertrophic cardiomyopathy (in German).
Z Kardiol 1991; 80: 338-343.
Fighali S, Krajcer Z. Edelmann S. Leachman RD. Pro-
gression of hypertophic cardiomyopathy into a hypokine-
tic left ventricle: Higher incidence in patients with
midventricular obstruction. J Am Co11 Cardiol 1987; 9:
288-294.
Spirit0 P, Maron BJ. Bonow RO, Epstein SE. Severe functional limitation in patients with hypertrophic cardio-
myopathy and only mild localized left ventricular hyper-
trophy. J Am Co11 Cardiol 1986; 8: 537-544.
Spirit0 P, Maron BJ. Absence of progression of left ven-
tricular hypertrophy in adult patients with hypertophic
cardiomyopathy. J Am Co11 Cardiol 1987: 9: 1013-1017.
Spirit0 P, Maron BJ. Bonow RO. Epstein SE. Occurrence
and significance of progressive left ventricular wall thinn- ing and relative cavitiy dilatation in hypertrophic cardio-
myopathy. Am J Cardiol 1987: 9: 123-129.
Maron BJ. Epstein SE. Roberts WC. Hypertrophic car-
diomyopathy and transmural myocardial infarction
without significant atherosclerosts of the extramural coro-
nary arteries. Am J Cardiol 1979; 43: 1086-l 102.
Maron BJ. Wolfson JK, Epstein SE, Roberts WC. Intra-
mural (“small vessel”) coronary artery disease in hyper-
tophic cardiomyopathy. J Am Coll Cardiol 1986; 8:
545-557.
Chino M. Saito S, Yoshino H. Sakai T. Soma Y.
Nishikawa K. Familial hypertrophic cardiomyopathy
with left ventricular dilatation and conduction distur-
bances. Am J Cardiol 1988: 62: 484-486.
Hess OM. Schneider J. Gloor HO, Liltolf UM. Keiser G.
Congestive. hypertrophic cardiomyopathy ~ Intermed-
iary form of primary myocardial disease? (in German) Z Kardiol 1977; 66: 95-98.
Seiler C. Hess OM. Schonbeck M. Turina J. Jenni R. Turina M. Krayenbuehl HP. Long-term follow-up of
medical versus surgical therapy for hypertrophic cardio-
20
21
22
23
24
25
26
27
28
29
30
31
32
33
233
myopathy: A retrospective study. J Am Coll Cardiol 1991;
17: 634-642.
Maron BJ. Anan TJ, Roberts WC. Quantitative analysis
of the distribution of cardiac muscle cell disorganization
in the left ventricular wall of patients with hypertrophic
cardiomyopathy. Circulation 1981; 63: 882-894.
Tanaka M. Fujiwara H. Onodera T. Wu DJ. Hamashima
Y, Kawai C. Quantitative analysis of myocardial fibrosis
in normals, hypertensive hearts and hypertrophic cardio- myopathy. Br Heart J 1986; 55: 575-581.
St John Sutton MG. Lie JT, Anderson KR, O’Brien PC,
Frye RL. Histopathological specificity of hypertrophic
obstructive cardiomyopathy. Br Heart J 1980; 44: 433-43.
Cannon RO, Dilsizian V, O’Gara PT. Impact of surgical
relief of outflow obstruction on Thallium perfusion
abnormalities in hypertrophic cardiomypathy. Circula-
tion 1992; 85: 1039-1045.
Cannon RO, Dilsizian V. O’Gara PT. Myocardial meta-
bolic, hemodynamic, and electrocardiographic significance
of reversible Thallium-201 abnormalities in hypertrophic
cardiomyopathy. Circulation 1991: 83: 1660- 1667.
Kennedy JW. Baxley WA, Figley MM, Dodge HT.
Blackman JR. Quantitative angiography: The normal left
ventricle in man. Circulation 1966; 34: 2727-2778.
Brock RC. Functional obstruction of the left ventricle.
Guys Hosp Rep 1957; 106: 221-238.
Teare RD. Asymmetrical hypertrophy of the heart in young adults. Br Heart J 1958; 20: l-8.
Brock RC. Functional obstruction of the left ventricle.
Guys Hosp Rep 1959; 108: 126-133.
Roberts WC, Ferrans VJ. Morphologic observations in
cardiomyopathies. In: Noble 0. Fowler, editor. Myocar-
dial diseases. New York and London: Grune & Stratton. 1973.
Wagner JA. Sax FL, Weisman HF. Calcium antagonist receptors in the atria1 tissue of patients with hypertrophic
cardiomypathy. N Engl J Med 1989; 320: 755-761.
Frenneaux MP, Counihan PJ. Caforio ALP, Chikamori
T, McKenna WJ. Abnormal blood pressure response dur- ing exercise in hypertrophic cardiomyopathy. Circulation
1990; 82: 1995-2002.
Counihan PJ, Frenneaux MP, Webb DJ, McKenna WJ.
Abnormal vascular response to supine exercise in hyper-
trophic cardomyopathy. Circulation 1991; 84: 686-696.
Seiler Ch, Hess OM, Jenni R. Krayenbuehl HP. Left ven- tricular chamber dilatation in hypertrophic cardiomyo-
pathy: prevalence in medically and surgically treated
patients (abstract). Circulation 1993; 88 (suppl): I-212.