immunogenicity of anti-tnfα therapy in psoriasis: a clinical issue?
TRANSCRIPT

1. Introduction
2. Immunologic responses
elicited by anti-TNFa agents
3. Immunogenicity of anti-TNFaagents may reduce the efficacy
of treatment
4. Lack of efficacy of anti-TNFaagents in dermatologic
diseases: is immunogenicity a
problem?
5. Conclusion
6. Expert opinion
Review
Immunogenicity of anti-TNFatherapy in psoriasis: a clinicalissue?Clara De Simone†, Paolo Amerio, Giuseppe Amoruso, Federico Bardazzi,Anna Campanati, Andrea Conti, Paolo Gisondi, Giulio Gualdi,Claudio Guarneri, Luca Leoni, Francesco Loconsole, Annamaria Mazzotta,Maria Letizia Musumeci, Stefano Piaserico, Concetta Potenza &Francesca Prestinari†Catholic University of the Sacred Heart, Department of Dermatology, Rome, Italy
Introduction: Immunogenicity of antitumor necrosis factor-alpha (TNFa)agents has been proven to play a significant role in the variability of clinical
responses among patients with chronic inflammatory diseases. However, its
clinical impact on the outcome of patients with psoriasis and psoriatic arthritis
receiving anti-TNFa treatment is not yet fully clear. Despite the high rates of
efficacy of anti-TNFa agents in psoriasis, a substantial proportion of patients
remain who experience a primary or secondary failure or significant side
effects, which are potentially ascribable to immunogenicity.
Areas covered: Topics include immunologic response elicited by anti-TNFaagents, the impact of immunogenicity on treatment response to anti-TNFa and
the role played by immunogenicity in the lack of efficacy of anti-TNFa agents
(infliximab, adalimumab and etanercept) in psoriasis.
Expert opinion: Based on data available in the literature and the clinical expe-
rience of the authors, this article suggests the optimal approach to drug mon-
itoring and antidrug antibody assay and the most effective use of biologic
immunotherapies in this setting. Immunogenicity should be taken into
account in the adoption of therapeutic choices in psoriatic patients, such as
anti-TNFa agent intensification, or switching to another anti-TNFa agent or
a drug with a different mechanism of action.
Keywords: anti-TNFa agent, immunogenicity, psoriasis
Expert Opin. Biol. Ther. [Early Online]
1. Introduction
The prognosis of several autoimmune diseases, including psoriasis and psoriaticarthritis (PsA), has improved considerably in the past decade with the introductionof antitumor necrosis factor-alpha (TNFa) agents (i.e., infliximab, adalimumab,etanercept and golimumab), which are thought to be more efficacious and tolerablethan conventional therapies such as cyclosporine and methotrexate (MTX), owingto their activity on the specific therapeutic target [1]. However, infusion reactionsand lack or loss of response are significant clinical issues still associated with currentbiologic therapies, and immunogenicity of anti-TNFa recombinant proteinspotentially plays a role in these issues [2].
Immunogenicity appears to be related to the specific molecular structure of theanti-TNFa agent, with the constitution of each acting as a different immunologicstimulus. The clinical consequences of antidrug antibody (ADA) development arealso heterogeneous, including severe allergic and anaphylactic reactions and a reduc-tion or loss of therapeutic efficacy. The incidence and clinical relevance of these con-sequences have been extensively investigated in patients with rheumatoid arthritis
10.1517/14712598.2013.848194 © 2013 Informa UK, Ltd. ISSN 1471-2598, e-ISSN 1744-7682 1All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
109.
129.
219.
196
on 1
0/13
/13
For
pers
onal
use
onl
y.

(RA) and Crohn’s disease (CD) [3]. On the whole,immunogenicity-associated issues may have a significantimpact on the efficacy and safety of treatment, the complianceto therapy and the individualization of patient management.Fewer data are available for patients with psoriatic diseases
than for those with rheumatologic and intestinal diseases;however, data from clinical studies seem to indicate that theimmunogenicity of anti-TNFa drugs may be a relevant prob-lem in the management of psoriatic diseases. Based on dataavailable in the literature and the clinical experience of theauthors, this article attempts to evaluate the impact of immu-nogenicity with anti-TNFa therapy on patients with psoriasisand PsA, and to define the optimal approach to monitoringdrug and ADA levels and the most effective use of biologicimmunotherapies in this setting.
2. Immunologic responses elicited byanti-TNFa agents
All biotechnology-derived therapeutic proteins, whetherentirely of human origin, chimeric or ‘humanized’ can elicitimmune responses, because they contain unique sequences
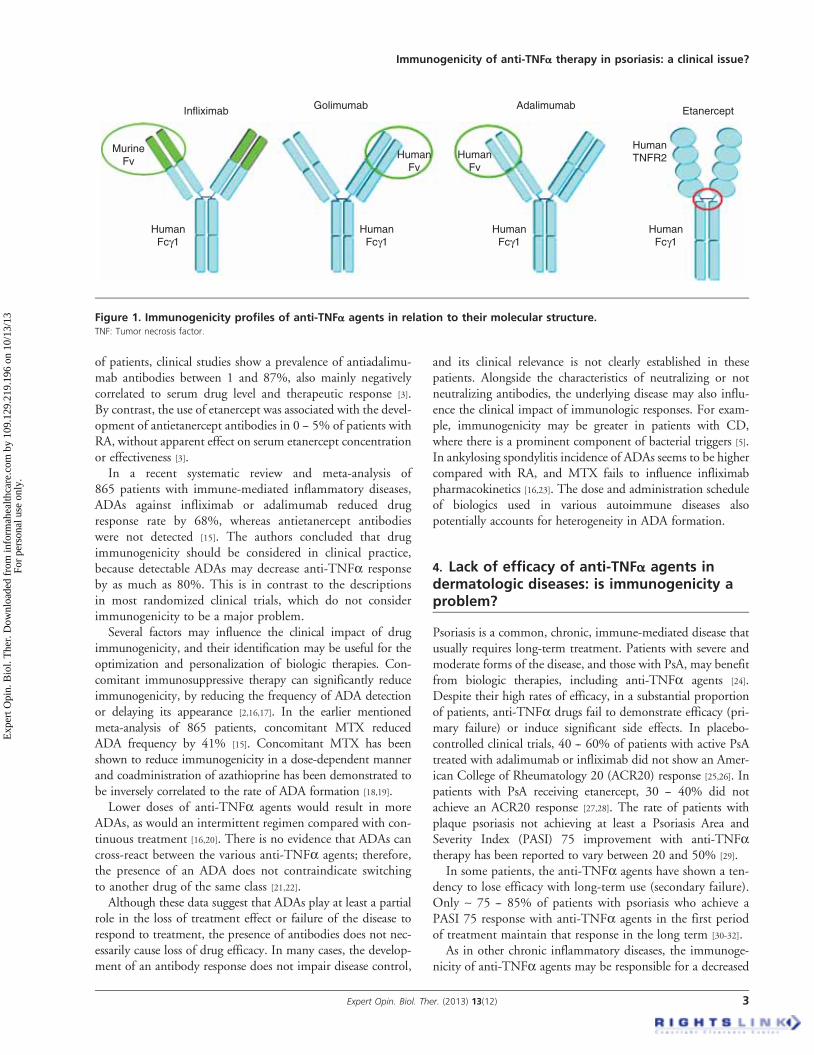
that generate antibodies against themselves [4]. These immuneresponses are complex and can contribute to the appearanceof adverse events, as well as to treatment failure. However,the different molecular structures of the various anti-TNFaagents translate to different immunogenicity profiles, with dis-tinctive clinical implications. Chimeric drugs such as infliximab(chimeric mouse/human anti-TNFa monoclonal antibody)may induce the production of antibodies against the murinecomponent of Fab fragments [5], whereas fully humananti-TNFa monoclonal antibodies (e.g., adalimumab andgolimumab) elicit anti-idiotypic antibodies [6]. In the case ofetanercept (a TNF-receptor-IgG fusion protein), only the junc-tion region between the TNF receptor and the Fc fragment ofhuman IgG1 incorporates immunogenic epitopes [3,7].
The lack or loss of clinical response in patients with ADAsmay be explained by immune--complex formation betweenanti-TNFa agents and ADAs, leading to their increased clear-ance, or to the impossibility of drug fixation to TNFa, andthereby to inhibition of its biologic activity. The latter is par-ticularly true for ADAs directed against anti-TNFa agents(infliximab, adalimumab, golimumab), which are inducedby the hypervariable region of the Fab fragment, essentialfor the link to TNFa [8-11]. Conversely, antietanercept anti-bodies are not usually neutralizing, as they target the centralpart of the molecule and do not block the site of interactionwith TNFa (Figure 1) [12,13].
In addition to treatment failure, the presence of ADAs maybe associated with adverse events, such as acute or delayedinfusion reactions, including headache, pruritus, hypotension,nausea, fever, skin rash and arthralgias. Such reactions aremore frequent in patients treated with infliximab (15 -- 20%of patients) and the risk is doubled in those with anti-infliximab antibodies [8,9]. By contrast, the development ofADAs directed against adalimumab and etanercept does notappear to be associated with an increased risk of adverseeffects [10-13].
3. Immunogenicity of anti-TNFa agents mayreduce the efficacy of treatment
Several pieces of evidence reveal a significant impact of immu-nogenicity on treatment response to anti-TNFa drugs,although it must be stressed that the quantification of ADAsis challenging and may be undertaken by different assays,and quantitative data are difficult to compare across clinicalstudies [9,14]. The wide variations in ADA prevalence depend-ing on the type of assay used, together with the false-negativeresults and nonspecific binding that may occur with some ofthese, make it difficult to precisely assess the clinical impactof immunogenicity.
This phenomenon has been studied mainly in patients withRA and CD treated with infliximab. In these patients, theprevalence of anti-infliximab antibodies varies from 6 to60% [3] and appears to be inversely associated with seruminfliximab level and clinical response. In the same subgroup
Article highlights.
. Prognosis of psoriasis and PsA improved considerablywith the introduction of anti-TNFa agents. However,immunogenicity of anti-TNFa recombinant proteins canplay a role in infusion reactions and lack or loss ofresponse of these therapies.
. The reported extent of ADA development in psoriaticpatients treated with infliximab ranges from 15 to 50%,with an inverse correlation with serum drug levels andclinical response. Fewer data are available foradalimumab (ADA prevalence ranging from 6 to 45%),whereas etanercept appears to be less immunogenicthan anti-TNFa antibodies and ADAs to etanercept arenot associated with clinical response or adverse events.
. A better knowledge of the implications of biologicimmunogenicity in psoriasis and PsA would allow amore rational approach to the management of patientswith primary or secondary failure, with the adoption oftherapeutic choices such as anti-TNFa agentintensification, switching to another anti-TNFa agent orto a drug with a different mechanism of action. As lowserum levels of drug have been associated with a morelikely appearance of ADAs, the issue of immunogenicityshould also be considered in patients with a goodclinical response, in which reducing drug dosage orfrequency of infusions, although apparently a rationalapproach with significant short-term economic benefits,may favor the development of immunogenicity.
. The appraisal of immunogenicity of anti-TNFa agentscan translate into a better understanding of patients’clinical heterogeneity and in a practical tool for theoptimization and personalization of therapeuticapproach in psoriasis and PsA.
This box summarizes key points contained in the article.
C. De Simone et al.
2 Expert Opin. Biol. Ther. (2013) 13(12)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
109.
129.
219.
196
on 1
0/13
/13
For
pers
onal
use
onl
y.
of patients, clinical studies show a prevalence of antiadalimu-mab antibodies between 1 and 87%, also mainly negativelycorrelated to serum drug level and therapeutic response [3].By contrast, the use of etanercept was associated with the devel-opment of antietanercept antibodies in 0 -- 5% of patients withRA, without apparent effect on serum etanercept concentrationor effectiveness [3].
In a recent systematic review and meta-analysis of865 patients with immune-mediated inflammatory diseases,ADAs against infliximab or adalimumab reduced drugresponse rate by 68%, whereas antietanercept antibodieswere not detected [15]. The authors concluded that drugimmunogenicity should be considered in clinical practice,because detectable ADAs may decrease anti-TNFa responseby as much as 80%. This is in contrast to the descriptionsin most randomized clinical trials, which do not considerimmunogenicity to be a major problem.
Several factors may influence the clinical impact of drugimmunogenicity, and their identification may be useful for theoptimization and personalization of biologic therapies. Con-comitant immunosuppressive therapy can significantly reduceimmunogenicity, by reducing the frequency of ADA detectionor delaying its appearance [2,16,17]. In the earlier mentionedmeta-analysis of 865 patients, concomitant MTX reducedADA frequency by 41% [15]. Concomitant MTX has beenshown to reduce immunogenicity in a dose-dependent mannerand coadministration of azathioprine has been demonstrated tobe inversely correlated to the rate of ADA formation [18,19].
Lower doses of anti-TNFa agents would result in moreADAs, as would an intermittent regimen compared with con-tinuous treatment [16,20]. There is no evidence that ADAs cancross-react between the various anti-TNFa agents; therefore,the presence of an ADA does not contraindicate switchingto another drug of the same class [21,22].
Although these data suggest that ADAs play at least a partialrole in the loss of treatment effect or failure of the disease torespond to treatment, the presence of antibodies does not nec-essarily cause loss of drug efficacy. In many cases, the develop-ment of an antibody response does not impair disease control,
and its clinical relevance is not clearly established in thesepatients. Alongside the characteristics of neutralizing or notneutralizing antibodies, the underlying disease may also influ-ence the clinical impact of immunologic responses. For exam-ple, immunogenicity may be greater in patients with CD,where there is a prominent component of bacterial triggers [5].In ankylosing spondylitis incidence of ADAs seems to be highercompared with RA, and MTX fails to influence infliximabpharmacokinetics [16,23]. The dose and administration scheduleof biologics used in various autoimmune diseases alsopotentially accounts for heterogeneity in ADA formation.
4. Lack of efficacy of anti-TNFa agents indermatologic diseases: is immunogenicity aproblem?
Psoriasis is a common, chronic, immune-mediated disease thatusually requires long-term treatment. Patients with severe andmoderate forms of the disease, and those with PsA, may benefitfrom biologic therapies, including anti-TNFa agents [24].Despite their high rates of efficacy, in a substantial proportionof patients, anti-TNFa drugs fail to demonstrate efficacy (pri-mary failure) or induce significant side effects. In placebo-controlled clinical trials, 40 -- 60% of patients with active PsAtreated with adalimumab or infliximab did not show an Amer-ican College of Rheumatology 20 (ACR20) response [25,26]. Inpatients with PsA receiving etanercept, 30 -- 40% did notachieve an ACR20 response [27,28]. The rate of patients withplaque psoriasis not achieving at least a Psoriasis Area andSeverity Index (PASI) 75 improvement with anti-TNFatherapy has been reported to vary between 20 and 50% [29].
In some patients, the anti-TNFa agents have shown a ten-dency to lose efficacy with long-term use (secondary failure).Only ~ 75 -- 85% of patients with psoriasis who achieve aPASI 75 response with anti-TNFa agents in the first periodof treatment maintain that response in the long term [30-32].
As in other chronic inflammatory diseases, the immunoge-nicity of anti-TNFa agents may be responsible for a decreased
MurineFv
HumanFv
HumanFv
HumanTNFR2
Infliximab Golimumab Adalimumab Etanercept
HumanFcγ1
HumanFcγ1
HumanFcγ1
HumanFcγ1
Figure 1. Immunogenicity profiles of anti-TNFa agents in relation to their molecular structure.TNF: Tumor necrosis factor.
Immunogenicity of anti-TNFa therapy in psoriasis: a clinical issue?
Expert Opin. Biol. Ther. (2013) 13(12) 3
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
109.
129.
219.
196
on 1
0/13
/13
For
pers
onal
use
onl
y.

or absent response to these drugs, at least in a proportion ofpatients with psoriasis. However, it is difficult to quantify theextent of ADA formation in psoriatic patients and their impacton the therapeutic efficacy of different anti-TNFa drugs.
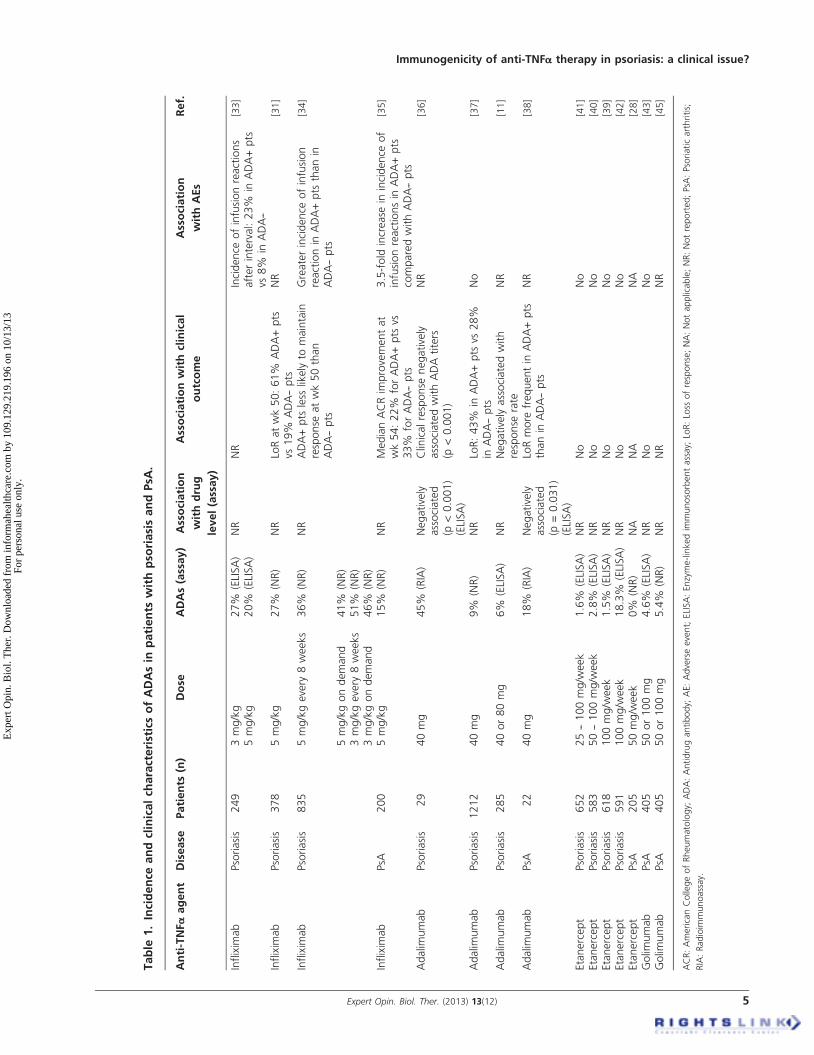
4.1 InfliximabIn a large series of 249 patients with severe plaque psoriasis,ADAs were detected by enzyme-linked immunosorbent assay(ELISA) in 27.6% of patients receiving 3 mg/kg of infliximaband in 19.5% of those receiving the higher dose (5 mg/kg).The presence of antibodies to infliximab was associated withinfusion reactions only in patients retreated after a 20-weekinterval (23% of infusion reactions in ADA-positive patientsvs 8% in ADA-negative ones) [33]. A similar incidence ofADAs (27%) was observed by Reich et al. in patients with mod-erate-to-severe plaque psoriasis receiving infliximab 5 mg/kg [31].In a trial of 835 patients with moderate-to-severe psoriasis,
randomized to induction therapy with infliximab 3 or 5 mg/kg(or placebo) then to scheduled or intermittent maintenanceregimens at their induction dose, higher rates of ADAs wererecorded. Antibodies to infliximab were detected in35.8 and 41.5% of patients in the 5 mg/kg every 8 weeksand as-needed groups, respectively, and in 51.5 and 46.2%of patients in the 3 mg/kg every 8 weeks and as-neededgroups, respectively. Antibody-positive patients were lesslikely to maintain response at week 50 than antibody-negativepatients, although positive-antibody status did not precludeclinical responsiveness. Moreover, ADA-positive patients hada greater risk of experiencing an infusion reaction thanADA-negative patients [34].In patients with active PsA treated with infliximab 5 mg/kg
(IMPACT 2 trial), ADA development was observed in15.4%. Antibodies to infliximab were more frequent inpatients not receiving MTX at baseline (26.1 vs 3.6%in patients receiving MTX) and showed an inverse correlationwith clinical response: the median percentage ACR improve-ment at week 54 for patients who were ADA-positive was lowerthan for those who were ADA-negative (21.7 vs 33.3%, respec-tively). Among antibody-positive patients, an ~ 3.5-foldincrease in the incidence of mild-to-moderate infusion reac-tions occurred compared with antibody-negative patients [35].
4.2 AdalimumabData are more limited for the anti-TNFa agent adalimumab.An ADA incidence as high as 45% was reported in a smallseries of adalimumab-treated patients with psoriasis, with asignificant inverse correlation with serum drug level and clin-ical response. All patients with high titers of antibodies to ada-limumab at weeks 12 or 24 were nonresponders, andsignificant differences in response rates were recorded amongpatients with low, high and no titers of ADAs [36]. However,antiadalimumab antibodies were detected in only 6 and 9%of patients with psoriasis receiving 40 or 80 mg of adalimu-mab in two large trials enrolling 285 and 1212 patients,respectively; both trials suggested a negative impact of ADAs
on clinical outcomes [11,37]. The use of a different method ofADA detection might partially explain these differences.
In a small study of 22 patients with PsA specifically assessingthe incidence of antiadalimumab antibodies and the relation-ship with serum drug concentration and clinical response,ADAs were detected in 18% of patients. Those with antiadali-mumab antibodies had lower median adalimumab concentra-tions than those without (1.7 vs 9.8 mg/l at 12 months), andserum levels of adalimumab were undetectable in patientswith high concentrations of antibodies. In addition, patientswith antibodies appeared to lose their initial good response [38].
No evidence of an association between antiadalimumabantibodies and adverse events was reported in these trials.
4.3 EtanerceptAs earlier mentioned, etanercept is thought to be less immu-nogenic than anti-TNFa antibodies. In patients with psoria-sis, the frequency of detection of antietanercept antibodieshas ranged from 1.5 to 2.8% [39-41], although an open-labelextension of one large Phase III trial in 591 patients reporteda rate of 18.3% ADA-positive patients [42]. In one study ofpatients with PsA treated with 25 mg etanercept twice weekly,no evidence of ADA development was found among the 205patients enrolled [28].
Where detectable, in each case antietanercept antibodieswere nonneutralizing. To date, no association has beenreported between ADAs to etanercept and serum drug levels,clinical response or adverse events.
4.4 Other agentsAmong other anti-TNFa agents, the fully human anti-TNFaantibody golimumab is indicated, alone or in association withMTX, for the treatment of patients with PsA not respondingto other disease-modifying antirheumatic drug. In this categoryof patients, subcutaneous golimumab has been shown to signif-icantly improve arthritic manifestations of PsA and associatedskin disease, and reduce radiographic progression [43,44]. Theconstant regions of golimumab are identical to the correspond-ing human constant regions of infliximab, but the variableregions of golimumab, at variance from infliximab, have fullyhuman sequences. The reported frequency of antigolimumabADAs ranges from 0 to 7%, without apparent association withclinical response and adverse events [3]. In PsA patients receivinggolimumab therapy, ADAs have been detected in 4 -- 5% ofcases, without correlation with clinical response [43-45].
The incidence and clinical characteristics of ADAs inpatients with psoriasis and PsA are summarized in Table 1.
5. Conclusion
Immunogenicity of recombinant proteins has been shown to sig-nificantly impact on the clinical outcome of patients withchronic inflammatory diseases receiving anti-TNFa therapy.The evidence available in the literature confirms immunogenicityto anti-TNFa agents may be present in a variable but significant
C. De Simone et al.
4 Expert Opin. Biol. Ther. (2013) 13(12)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
109.
129.
219.
196
on 1
0/13
/13
For
pers
onal
use
onl
y.
Table
1.Incidence
andclinicalch
aracteristicsofADAsin
patients
withpso
riasisandPsA
.
Anti-TNFa
agent
Disease
Patients
(n)
Dose
ADAs(assay)
Association
withdrug
level(assay)
Associationwithclinical
outcome
Association
withAEs
Ref.
Inflixim
ab
Psoriasis
249
3mg/kg
5mg/kg
27%
(ELISA)
20%
(ELISA)
NR
NR
Incidence
ofinfusionreactions
afterinterval:23%
inADA+pts
vs8%
inADA--
[33]
Inflixim
ab
Psoriasis
378
5mg/kg
27%
(NR)
NR
LoRatwk50:61%
ADA+pts
vs19%
ADA--pts
NR
[31]
Inflixim
ab
Psoriasis
835
5mg/kgevery
8weeks
36%
(NR)
NR
ADA+pts
less
likely
tomaintain
response
atwk50than
ADA--pts
Greaterincidence
ofinfusion
reactionin
ADA+pts
thanin
ADA--pts
[34]
5mg/kgondemand
41%
(NR)
3mg/kgevery
8weeks
51%
(NR)
3mg/kgondemand
46%
(NR)
Inflixim
ab
PsA
200
5mg/kg
15%
(NR)
NR
MedianACRim
provementat
wk54:22%
forADA+pts
vs33%
forADA--pts
3.5-fold
increase
inincidence
of
infusionreactionsin
ADA+pts
comparedwithADA--pts
[35]
Adalim
umab
Psoriasis
29
40mg
45%
(RIA)
Negatively
associated
(p<0.001)
(ELISA)
Clinicalresponse
negatively
associatedwithADAtiters
(p<0.001)
NR
[36]
Adalim
umab
Psoriasis
1212
40mg
9%
(NR)
NR
LoR:43%
inADA+pts
vs28%
inADA--pts
No
[37]
Adalim
umab
Psoriasis
285
40or80mg
6%
(ELISA)
NR
Negatively
associatedwith
response
rate
NR
[11]
Adalim
umab
PsA
22
40mg
18%
(RIA)
Negatively
associated
(p=0.031)
(ELISA)
LoRmore
frequentin
ADA+pts
thanin
ADA--pts
NR
[38]
Etanercept
Psoriasis
652
25--100mg/w
eek
1.6%
(ELISA)
NR
No
No
[41]
Etanercept
Psoriasis
583
50--100mg/w
eek
2.8%
(ELISA)
NR
No
No
[40]
Etanercept
Psoriasis
618
100mg/w
eek
1.5%
(ELISA)
NR
No
No
[39]
Etanercept
Psoriasis
591
100mg/w
eek
18.3%
(ELISA)
NR
No
No
[42]
Etanercept
PsA
205
50mg/w
eek
0%
(NR)
NA
NA
NA
[28]
Golim
umab
PsA
405
50or100mg
4.6%
(ELISA)
NR
No
No
[43]
Golim
umab
PsA
405
50or100mg
5.4%
(NR)
NR
NR
NR
[45]
ACR:AmericanCollegeofRheumatology;
ADA:Antidrugantibody;
AE:Adverseevent;ELISA:Enzyme-linkedim
munosorbentassay;
LoR:Loss
ofresponse;NA:Notapplicable;NR:Notreported;PsA
:Psoriaticarthritis;
RIA:Radioim
munoassay.
Immunogenicity of anti-TNFa therapy in psoriasis: a clinical issue?
Expert Opin. Biol. Ther. (2013) 13(12) 5
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
109.
129.
219.
196
on 1
0/13
/13
For
pers
onal
use
onl
y.

percentage of patients with psoriasis or PsA and be variably asso-ciated with therapeutic response and adverse events.The implications for the clinical practice of biologic immu-
nogenicity in dermatologic patients are still poorly character-ized, although a better knowledge of this issue would allow amore rational approach to the management of patients with pri-mary or secondary treatment failure. Because low serum levels ofdrug have been associated with a greater likelihood for develop-ment of ADAs, the issue of immunogenicity should also be con-sidered in patients with a good clinical response. In thesepatients, reducing drug dosage or frequency of infusions mayappear to be a rational approach, with significant economic ben-efits; however, this should be weighed against the risk ofpromoting ADA development and then secondary failure.A reliable definition of the predictive power of therapeutic
drug level and ADA detection in the adoption of therapeuticchoices such as anti-TNFa agent intensification, or switchingto another anti-TNFa agent or a drug with a different mech-anism of action, could drastically change the management ofpatients in the future. Given the economic costs of these drugsand the costs associated with therapeutic failure (in terms oflack of improvement or worsening of damage), the potentialusefulness of therapeutic drug monitoring and ADA assess-ment could be quantified and justified from an economicpoint of view. As illustrated further, the evaluation of theseparameters could efficaciously support therapeutic choices inclinical practice. In patients with inadequate disease control,this might drive the strategy to improve therapeutic response.In responding patients, the demonstration that higher drugdoses may actually decrease immunogenicity might result inan improved cost/effectiveness ratio in the long term, despitethe high costs of anti-TNFa drugs.On the whole, the appraisal of immunogenicity of anti-
TNFa agents may eventually lead to a better understandingof patients’ clinical heterogeneity and to a practical tool forthe optimization and personalization of therapeutic approachin treating psoriasis and PsA.
6. Expert opinion
Available data clearly point to a significant incidence of ADAsin patients with psoriasis or PsA treated with anti-TNFaagents. Approximately 15 -- 50% of patients treated with inflix-imab and 10 -- 40% of those receiving adalimumab are at riskof developing ADAs [3]. However, the real impact of immuno-genicity on clinical outcome is more difficult to ascertain, as isthe proportion of primary or secondary failures that might beascribed to ADA development. A clinically significant reduc-tion in therapeutic efficacy may be seen in patients developinganti-infliximab or antiadalimumab antibodies, but how thistranslates to rate of response is not yet established. Moreover,in many nonresponders no evidence of immunogenicity isseen, and some patients show a good treatment responsedespite the presence of ADAs [36,46,47]. A significant proportionof these uncertainties may be related to the limits that most
commonly used assays for drug monitoring and ADA detectionpresent when used in a clinical setting.
At present, the decision to modify the dose or frequency ofadministration as well as to switch to another drug is based onclinical response and safety profile. A rational approach tothese therapeutic changes, considering potential clinicalimplications of drug immunogenicity, might benefit fromdrug monitoring and ADA detection, although treatmentdecisions cannot rely solely on laboratory parameters, mainlydue to the lack of standardization of these methods.
6.1 The need for serum drug monitoringThe efficacy of anti-TNFa agents is dose-dependent. Higherserum trough levels of infliximab, adalimumab or etanercepthave been shown to correlate with increased clinical responserates in RA [47-49]. In patients with psoriasis, plasma troughlevels of adalimumab and infliximab were reported to bepositively associated with clinical response [36,50].
Even for equal drug dosages, interindividual variability inthe pharmacokinetics of anti-TNFa agents is relevant andmay be ascribed to patient characteristics, genetic back-ground, underlying disease and concomitant drugs [48]. Inaddition, ADA presence may reduce the half-life and serumlevel of infliximab and adalimumab by increasing their clear-ance. Therefore, in patients with absent or suboptimal diseaseresponse to anti-TNFa therapy, determining serum drug con-centration may be clinically useful in informing therapeuticstrategy. If steady-state trough serum levels are low or unde-tectable, increasing drug dosage or frequency of injectionsmay be a rational approach; conversely, if serum levels arewithin the target range, switching to another anti-TNFaagent or class of drugs may be recommended, as dose increaseis unlikely to add to disease control. Anti-TNFa intensifica-tion in patients with low drug level and evidence of immuno-genicity is more controversial: some authors reported aless-frequent clinical improvement in response to doseescalation or shortened infusion intervals in patients withanti-infliximab antibodies [51,52]. However, higher exposureto infliximab may reduce ADA levels in a significant propor-tion of patients [52]. The influence of serum drug concentra-tion on therapeutic efficacy thus may justify drug-levelmonitoring, even in terms of cost-effectiveness.
6.2 The need for ADA assayThe presence and titers of ADAs might also influence thera-peutic decisions in patients with inadequate disease controlor adverse events. If ADA development is detected in a patientwith primary or secondary failure, and the drug serum level iswithin the target range, switching to another TNFa antago-nist should be considered. ADAs do not show cross-reactivity,and experience in RA has demonstrated that patients with aprevious clinical failure associated with ADA presence usuallyshow a good response after switching to another TNFa antag-onist [22,53]. However, in patients who experience a failure notascribable to immunization, switching to another anti-TNFa
C. De Simone et al.
6 Expert Opin. Biol. Ther. (2013) 13(12)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
109.
129.
219.
196
on 1
0/13
/13
For
pers
onal
use
onl
y.
agent is often ineffective, probably because different or multi-ple pathogenetic mechanisms are involved, and a drug withanother mechanism of action should be considered. There-fore, ADA detection can be helpful in deciding which patientswould benefit from switching, and may be part of a personal-ized treatment regimen.
Addition of an immunosuppressant drug, such as MTX,might be another choice in patients with evidence of immuni-zation, because its association with anti-TNFa agents reducesADA formation [16,18,54].
In patients with clinical adverse drug reactions to inflixi-mab, ADAs can be evaluated to assess if the adverse event isrelated to immunization [55]. If ADAs are detected, readminis-tration of the same drug may be dangerous. However, even inthe absence of detectable ADAs, the decision to continue withthe same antagonist must be taken with caution, and the pos-sibility of a false-negative induced by interference by thecirculating anti-TNFa agent ruled out [14].
6.3 When and how to switch?Based on the above considerations, switching to another anti-TNFa agent may be considered for patients with absent or
inadequate response or with clinical-relevant adverse events.Patients who stopped their first anti-TNFa treatment becauseof toxicity are more likely to respond after switching toanother anti-TNFa than those who experienced a failure [56]
and in this setting, no rational for the use of a specificanti-TNFa agent in terms of clinical outcome is available.
Patients with inadequate disease control, and without evi-dence of low serum drug levels that can suggest a doseincrease, may benefit from switching to a second anti-TNFaagent if ADAs are present, as ADA-negative patients aremore likely to respond to drugs with a different mechanismof action. However, it has been reported that patients whodeveloped immunogenicity against a first anti-TNFa agentwere more likely to produce ADAs against a second. In astudy in patients with RA, switchers with anti-infliximab anti-bodies were reported to form antibodies against adalimumabmore often than anti-TNFa-naıve patients [53]. However,switching to etanercept from infliximab or adalimumab hasbeen shown to induce a better clinical outcome in patientswith ADAs compared with those without evidence of immu-nogenicity. These data need to be confirmed in the psoriasissetting, and suggest a potential influence of immunogenicity
Anti-TNFα therapy
Infusion reaction
ADA assay
-+
Resume thedrug?
Switch to anotheranti-TNFα
Disease control
NoYes
Drug level assayContinue treatment
LowHigh
ADA assayADA assay
-+
IntensificationIntensification orswitch to another
anti-TNFα
-+
Switch to a differentclass of drug
Switch toanother
anti-TNFα
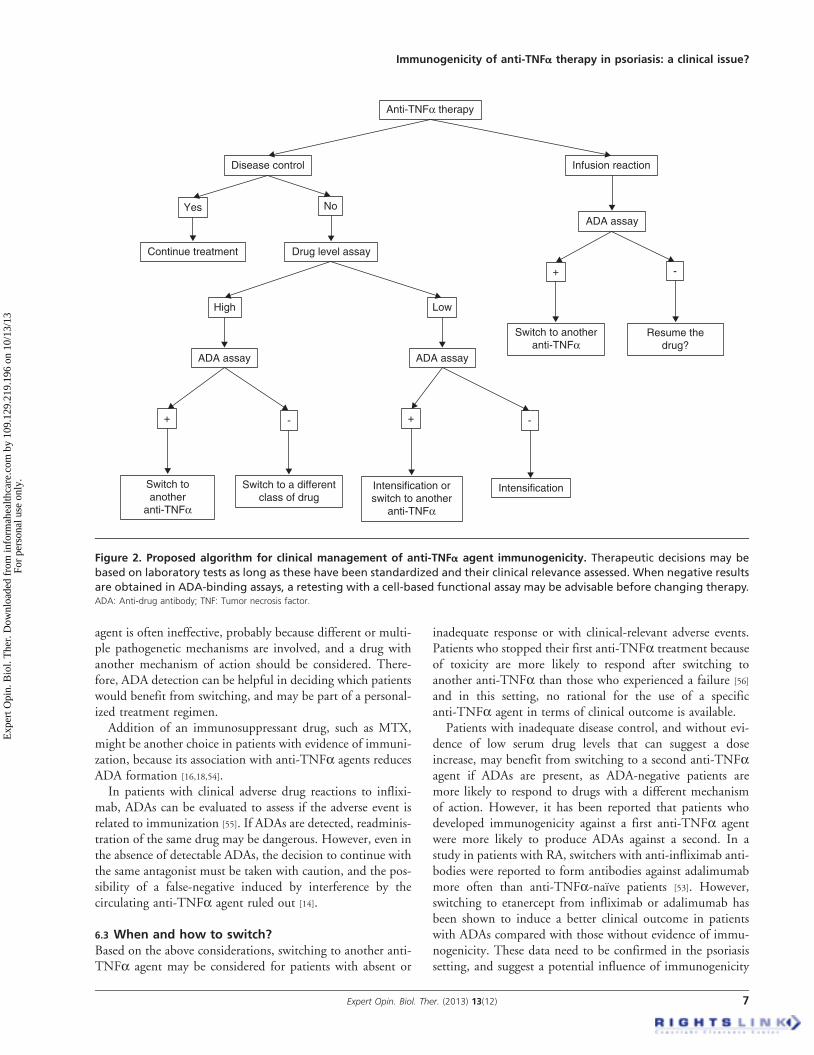
Figure 2. Proposed algorithm for clinical management of anti-TNFa agent immunogenicity. Therapeutic decisions may be
based on laboratory tests as long as these have been standardized and their clinical relevance assessed. When negative results
are obtained in ADA-binding assays, a retesting with a cell-based functional assay may be advisable before changing therapy.ADA: Anti-drug antibody; TNF: Tumor necrosis factor.
Immunogenicity of anti-TNFa therapy in psoriasis: a clinical issue?
Expert Opin. Biol. Ther. (2013) 13(12) 7
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
109.
129.
219.
196
on 1
0/13
/13
For
pers
onal
use
onl
y.

status not only in the decision to switch to another agent butalso in the choice of which anti-TNFa drug to use.
6.4 Unmet needsMost reported evidence on the clinical consequences ofimmunogenicity in patients receiving anti-TNFa therapyhas been obtained in rheumatologic and intestinal diseases.How applicable these data are to patients with psoriasis andPsA and the impact of immunogenicity on therapeuticchoices in these setting still need to be established throughwell-designed clinical studies. In relation to these issues, dif-ferences among the various chronic inflammatory diseasesalso need to be defined, as well as among the various anti-TNFa agents, including the imminently available biosimilars.In addition, international consensus is needed on the ther-
apeutic range of serum drug concentrations, and detectionand characterization of ADAs. At present, a number of meth-ods are generally used to detect the presence of ADAs(standard ELISA, two-site or bridging ELISA and radioim-munoassay antigen-binding test), and the prevalence ofADAs may vary widely depending on which assay is used.All these tests are error-prone when used in a clinical setting,as for example many of them are ‘drug-sensitive’ and cannotdetect ADA in the presence of the drug in the sample, which
may results in false-negative data. Moreover, the frequentlyused two-site ELISA fails to detect IgG4 antibodies, commonin long-term treated patients. Mostly importantly, all bindingassays do not assess functionality of measured drug and ADA,a factor that may affect the in vivo relevance of data generatedwith these tests [57]. Standardization of these methods and thedevelopment of assays able to measure the functionality ofboth drugs and ADAs are warranted to assure the clinicalutility of therapeutic drug monitoring.
Even considering these limitations, an algorithm for theclinical management of anti-TNFa agent immunogenicityand for the application of drug level and ADA measurementmay be proposed (Figure 2), whose clinical applicability neces-sarily rely on the availability of reliable assays for drug andADA determination.
Declaration of interest
This work, including travel and meeting expenses, was funded byan unrestricted grant by Pfizer. The sponsor had no role inreviewing the literature, defining recommendations, drafting orreviewing the article, or in the decision to submit the manuscriptfor publication. All views expressed are solely those of the authors.The authors have no other competing interests to declare.
BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. Ash Z, Gaujoux-Viala C, Gossec L, et al.
A systematic literature review of drug
therapies for the treatment of psoriatic
arthritis: current evidence and
meta-analysis informing the EULAR
recommendations for the management of
psoriatic arthritis. Ann Rheum Dis 2012;
71:319-26
2. Emi Aikawa N, de Carvalho JF,
Artur Almeida Silva C, Bonfa E.
Immunogenicity of Anti-TNF-alpha
agents in autoimmune diseases. Clin Rev
Allergy Immunol 2010;38:82-9
.. The role of immunogenicity in
treatment failure, infusion reactions
and relapses in patients treated with
anti-TNFa agents.
3. Vincent FB, Morand EF, Murphy K,
et al. Antidrug antibodies (ADAb) to
tumour necrosis factor (TNF)-specific
neutralising agents in chronic
inflammatory diseases: a real issue, a
clinical perspective. Ann Rheum Dis
2013;72:165-78
4. Harding FA, Stickler MM, Razo J,
DuBridge RB. The immunogenicity of
humanized and fully human antibodies:
residual immunogenicity resides in the
CDR regions. MAbs 2010;2:256-65
5. Anderson PJ. Tumor necrosis factor
inhibitors: clinical implications of their
different immunogenicity profiles.
Semin Arthritis Rheum 2005;34:19-22
6. van Schouwenburg PA, van de Stadt LA,
de Jong RN, et al. Adalimumab elicits a
restricted anti-idiotypic antibody response
in autoimmune patients resulting in
functional neutralisation. Ann Rheum
Dis 2013;72:104-9
7. Christen U, Thuerkauf R, Stevens R,
Lesslauer W. Immune response to a
recombinant human TNFR55-IgG1
fusion protein: auto-antibodies in
rheumatoid arthritis (RA) and multiple
sclerosis (MS) patients have neither
neutralizing nor agonist activities.
Hum Immunol 1999;60:774-90
8. Ducourau E, Mulleman D, Paintaud G,
et al. Antibodies toward infliximab are
associated with low infliximab
concentration at treatment initiation and
poor infliximab maintenance in rheumatic
diseases. Arthritis Res Ther 2011;13:R105
9. Bendtzen K, Geborek P, Svenson M, et al.
Individualized monitoring of drug
bioavailability and immunogenicity in
rheumatoid arthritis patients treated with the
tumor necrosis factor alpha inhibitor
infliximab. Arthritis Rheum 2006;54:3782-9
10. Bartelds GM, Krieckaert CL,
Nurmohamed MT, et al. Development of
antidrug antibodies against adalimumab
and association with disease activity and
treatment failure during long-term
follow-up. JAMA 2011;305:1460-8
11. Papp K, Crowley J, Ortonne JP, et al.
Adalimumab for moderate to severe
chronic plaque psoriasis: efficacy and
safety of retreatment and disease
recurrence following withdrawal from
therapy. Br J Dermatol 2011;164:434-41
12. Klareskog L, Gaubitz M, Rodriguez-
Valverde V, et al. Assessment of
long-term safety and efficacy of
etanercept in a 5-year extension study in
patients with rheumatoid arthritis.
Clin Exp Rheumatol 2011;29:238-47
13. Dore RK, Mathews S, Schechtman J, et al.
The immunogenicity, safety, and efficacy of
etanercept liquid administered once weekly
in patients with rheumatoid arthritis.
Clin Exp Rheumatol 2007;25:40-6
14. Hart MH, de Vrieze H, Wouters D,
et al. Differential effect of drug
interference in immunogenicity assays.
J Immunol Methods 2011;372:
196-203
C. De Simone et al.
8 Expert Opin. Biol. Ther. (2013) 13(12)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
109.
129.
219.
196
on 1
0/13
/13
For
pers
onal
use
onl
y.
15. Garces S, Demengeot J, Benito-Garcia E.
The immunogenicity of anti-TNF
therapy in immune-mediated
inflammatory diseases: a systematic
review of the literature with a
meta-analysis. Ann Rheum Dis
2012; [Epub ahead of print]
.. Clinical relevance of immunogenicity.
16. Maini RN, Breedveld FC, Kalden JR,
et al. Therapeutic efficacy of multiple
intravenous infusions of anti-tumor
necrosis factor alpha monoclonal
antibody combined with low-dose weekly
methotrexate in rheumatoid arthritis.
Arthritis Rheum 1998;41:1552-63
17. Farrell RJ, Alsahli M, Jeen YT, et al.
Intravenous hydrocortisone
premedication reduces antibodies to
infliximab in Crohn’s disease:
a randomized controlled trial.
Gastroenterology 2003;124:917-24
18. Krieckaert CL, Nurmohamed MT,
Wolbink GJ. Methotrexate reduces
immunogenicity in adalimumab treated
rheumatoid arthritis patients in a dose
dependent manner. Ann Rheum Dis
2012;71:1914-15
. Addition of methotrexate to
anti-TNFa agents can reduce the
formation of ADAs.
19. Colombel JF, Sandborn WJ, Reinisch W,
et al. Infliximab, azathioprine, or
combination therapy for Crohn’s disease.
N Engl J Med 2010;362:1383-95
20. Breban M, Ravaud P, Claudepierre P,
et al. Maintenance of infliximab treatment
in ankylosing spondylitis: results of a
one-year randomized controlled trial
comparing systematic versus on-demand
treatment. Arthritis Rheum 2008;58:
88-97
21. van der Bijl AE, Breedveld FC,
Antoni CE, et al. An open-label pilot
study of the effectiveness of adalimumab
in patients with rheumatoid arthritis and
previous infliximab treatment:
relationship to reasons for failure and
anti-infliximab antibody status.
Clin Rheumatol 2008;27:1021-8
22. Jamnitski A, Bartelds GM,
Nurmohamed MT, et al. The presence
or absence of antibodies to infliximab or
adalimumab determines the outcome of
switching to etanercept. Ann Rheum Dis
2011;70:284-8
. The presence of ADAs does not
contraindicate the switch with another
drug of the same class.
23. Mulleman D, Lauferon F, Wendling D,
et al. Infliximab in ankylosing
spondylitis: alone or in combination with
methotrexate? A pharmacokinetic
comparative study. Arthritis Res Ther
2011;13:R82
24. Weigle N, McBane S. Psoriasis.
Am Fam Physician 2013;87:626-33
25. Poddubnyy DA, Rudwaleit M.
Adalimumab for the treatment of
psoriatic arthritis. Expert Rev
Clin Immunol 2009;5:671-81
26. Bachmann F, Nast A, Sterry W,
Philipp S. Safety and efficacy of the
tumor necrosis factor antagonists.
Semin Cutan Med Surg 2010;29:35-47
27. Mease PJ, Goffe BS, Metz J, et al.
Etanercept in the treatment of psoriatic
arthritis and psoriasis: a randomised trial.
Lancet 2000;356:385-90
28. Mease PJ, Kivitz AJ, Burch FX, et al.
Etanercept treatment of psoriatic
arthritis: safety, efficacy, and effect on
disease progression. Arthritis Rheum
2004;50:2264-72
29. Leman J, Burden AD. Sequential use
of biologics in the treatment of
moderate-to-severe plaque psoriasis.
Br J Dermatol 2012;167(Suppl 3):12-20
30. Pink AE, Fonia A, Allen MH, et al.
Antinuclear antibodies associate with loss
of response to antitumour necrosis
factor-alpha therapy in psoriasis:
a retrospective, observational study.
Br J Dermatol 2010;162:780-5
31. Reich K, Nestle FO, Papp K, et al.
Infliximab induction and maintenance
therapy for moderate-to-severe psoriasis:
a phase III, multicentre, double-blind
trial. Lancet 2005;366:1367-74
32. Gordon KB, Langley RG, Leonardi C,
et al. Clinical response to adalimumab
treatment in patients with moderate to
severe psoriasis: double-blind, randomized
controlled trial and open-label extension
study. J Am Acad Dermatol 2006;55:
598-606
33. Gottlieb AB, Evans R, Li S, et al.
Infliximab induction therapy for patients
with severe plaque-type psoriasis:
a randomized, double-blind,
placebo-controlled trial. J Am
Acad Dermatol 2004;51:534-42
34. Menter A, Feldman SR, Weinstein GD,
et al. A randomized comparison of
continuous vs intermittent infliximab
maintenance regimens over 1 year in the
treatment of moderate-to-severe plaque
psoriasis. J Am Acad Dermatol 2007;
56:31; e1-15
35. Kavanaugh A, Krueger GG, Beutler A,
et al. Infliximab maintains a high degree
of clinical response in patients with active
psoriatic arthritis through 1 year of
treatment: results from the IMPACT
2 trial. Ann Rheum Dis 2007;66:498-505
36. Lecluse LL, Driessen RJ, Spuls PI, et al.
Extent and clinical consequences of
antibody formation against adalimumab
in patients with plaque psoriasis.
Arch Dermatol 2010;146:127-32
37. Menter A, Tyring SK, Gordon K, et al.
Adalimumab therapy for moderate to
severe psoriasis: a randomized, controlled
phase III trial. J Am Acad Dermatol
2008;58:106-15
38. van Kuijk AW, de Groot M, Stapel SO,
et al. Relationship between the clinical
response to adalimumab treatment and
serum levels of adalimumab and
anti-adalimumab antibodies in patients
with psoriatic arthritis. Ann Rheum Dis
2010;69:624-5
39. Tyring S, Gottlieb A, Papp K, et al.
Etanercept and clinical outcomes, fatigue,
and depression in psoriasis: double-blind
placebo-controlled randomised phase III
trial. Lancet 2006;367:29-35
40. Papp KA, Tyring S, Lahfa M, et al.
A global phase III randomized controlled
trial of etanercept in psoriasis: safety,
efficacy, and effect of dose reduction.
Br J Dermatol 2005;152:1304-12
41. Leonardi CL, Powers JL, Matheson RT,
et al. Etanercept as monotherapy in
patients with psoriasis. N Engl J Med
2003;349:2014-22
42. Tyring S, Gordon KB, Poulin Y, et al.
Long-term safety and efficacy of 50 mg
of etanercept twice weekly in patients
with psoriasis. Arch Dermatol
2007;143:719-26
43. Kavanaugh A, McInnes I, Mease P, et al.
Golimumab, a new human tumor
necrosis factor alpha antibody,
administered every four weeks as a
subcutaneous injection in psoriatic
arthritis: twenty-four-week efficacy and
safety results of a randomized,
placebo-controlled study.
Arthritis Rheum 2009;60:976-86
44. Kavanaugh A, van der Heijde D,
McInnes IB, et al. Golimumab in
psoriatic arthritis: one-year clinical
Immunogenicity of anti-TNFa therapy in psoriasis: a clinical issue?
Expert Opin. Biol. Ther. (2013) 13(12) 9
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
109.
129.
219.
196
on 1
0/13
/13
For
pers
onal
use
onl
y.

efficacy, radiographic, and safety results
from a phase III, randomized, placebo-
controlled trial. Arthritis Rheum
2012;64:2504-17
45. Kavanaugh A, McInnes IB, Mease PJ, et al.
Clinical efficacy, radiographic and safety
findings through 2 years of golimumab
treatment in patients with active psoriatic
arthritis: results from a long-term extension
of the randomised, placebo-controlled GO-
REVEAL study. Ann Rheum Dis
2012; [Epub ahead of print]
46. Wolbink GJ, Vis M, Lems W, et al.
Development of antiinfliximab antibodies
and relationship to clinical response in
patients with rheumatoid arthritis.
Arthritis Rheum 2006;54:711-15
47. Bartelds GM, Wijbrandts CA,
Nurmohamed MT, et al. Clinical response
to adalimumab: relationship to
anti-adalimumab antibodies and serum
adalimumab concentrations in rheumatoid
arthritis. Ann Rheum Dis 2007;66:921-6
48. St Clair EW, Wagner CL, Fasanmade AA,
et al. The relationship of serum infliximab
concentrations to clinical improvement in
rheumatoid arthritis: results from
ATTRACT, a multicenter, randomized,
double-blind, placebo-controlled trial.
Arthritis Rheum 2002;46:1451-9
49. Jamnitski A, Krieckaert CL,
Nurmohamed MT, et al. Patients
non-responding to etanercept obtain
lower etanercept concentrations
compared with responding patients.
Ann Rheum Dis 2012;71:88-91
50. Takahashi H, Tsuji H,
Ishida-Yamamoto A, Iizuka H. Plasma
trough levels of adalimumab and
infliximab in terms of clinical efficacy
during the treatment of psoriasis.
J Dermatol 2013;40:39-42
51. Plasencia C, Pascual-Salcedo D, Nuno L,
et al. Influence of immunogenicity on
the efficacy of longterm treatment of
spondyloarthritis with infliximab.
Ann Rheum Dis 2012;71:1955-60
52. Pascual-Salcedo D, Plasencia C, Ramiro S,
et al. Influence of immunogenicity on the
efficacy of long-term treatment with
infliximab in rheumatoid arthritis.
Rheumatology (Oxford) 2011;50:1445-52
53. Bartelds GM, Wijbrandts CA,
Nurmohamed MT, et al. Anti-infliximab
and anti-adalimumab antibodies in
relation to response to adalimumab in
infliximab switchers and anti-tumour
necrosis factor naive patients: a cohort
study. Ann Rheum Dis 2010;69:817-21
54. Weinblatt ME, Keystone EC, Furst DE,
et al. Adalimumab, a fully human
anti-tumor necrosis factor alpha
monoclonal antibody, for the treatment
of rheumatoid arthritis in patients taking
concomitant methotrexate: the
ARMADA trial. Arthritis Rheum
2003;48:35-45
55. Kerbleski JF, Gottlieb AB.
Dermatological complications and safety
of anti-TNF treatments. Gut 2009;58:
1033-9
56. Gomez-Reino JJ, Carmona L, Group B.
Switching TNF antagonists in patients
with chronic arthritis: an observational
study of 488 patients over a four-year
period. Arthritis Res Ther 2006;8:R29
57. Bendtzen K. Personalized medicine:
theranostics (therapeutic diagnostics)
essential for rational use of tumor
necrosis factor-alpha antagonists.
Discov Med 2013;15:201-11
AffiliationClara De Simone†1, Paolo Amerio2,
Giuseppe Amoruso3, Federico Bardazzi4,
Anna Campanati5, Andrea Conti6,
Paolo Gisondi7, Giulio Gualdi8,
Claudio Guarneri9, Luca Leoni10,
Francesco Loconsole11, Annamaria Mazzotta12,
Maria Letizia Musumeci13, Stefano Piaserico14,
Concetta Potenza15 & Francesca Prestinari16
†Author for correspondence1Catholic University of the Sacred Heart,
Department of Dermatology, L.go A.Gemelli 8;
00168 Rome, Italy
Tel: +390630154227;
Fax: +39063016293;
E-mail: [email protected]
2University G. D’Annunzio,
Dermatologic Clinic,
Department of Oncology and Neuroscience,
Chieti, Italy3University of Catanzaro (Italy) C/O Fondazione
per la Ricerca e la Cura dei Tumori ‘Tommaso
Campanella’ COE, Dermatology Unit, Viale
Europa, 88100 Germaneto di Catanzaro (CZ),
Italy4University of Bologna, S.Orsola-Malpighi
Hospital, Department of Specialistic,
Diagnostic and Experimental Medicine,
Dermatology Unit, Via Albertoni 15,
40138 Bologna, Italy5Marche Polytechinic University, Department of
Medicine and Applied Biotechnology, Section of
dermatology, Via Brecce Bianche, 1,
60131 Ancona, Italy6University of Modena and Reggio Emilia,
Department of Dermatology, Via Del Pozzo 71 -
41100, Modena, Italy7University of Verona, Department of Medicine,
Section of Dermatology and Venereology,
Verona, Italy8University of Brescia, Department of
Dermatology, Piazzale Spedali Civili 1,
25123 Brescia, Italy9University of Messina (Italy) c/o A.O.U,
Department of Clinical and Experimental
Medicine, Section of Dermatology, ‘G. Martino’,
Consolare Valeria, 1, 98125 Messina, Italy10IDI-IRCCS, Via Monti Creta, 104,
00167 Rome, Italy11University of Bari, Dermatology Clinic, Piazza
Giulio Cesare 11, 70124 Bari, Italy12University of Rome ‘Tor Vergata’,
Department of Dermatology,
Viale Oxford 81, 00133 Rome, Italy13AOU Policlinico-Vittorio Emanuele,
Department of Dermatology, PO G. Rodolico,
Via S. Sofia 78 -- 95123 Catania, Italy14University of Padova, Department of Medicine,
Dermatology Unit, via Cesare Battisti 206,
35128 Padova, Italy15Sapienza University, Polo Pontino, A. Fiorni
Terracina Hospital, UOC of Dermatology
‘Daniele Innocenzi’, Rome, Italy16S.Anna Hospital, Department of Dermatology,
Como, Italy
C. De Simone et al.
10 Expert Opin. Biol. Ther. (2013) 13(12)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
109.
129.
219.
196
on 1
0/13
/13
For
pers
onal
use
onl
y.