obesity and psoriasis: from the medical board of the national psoriasis foundation
TRANSCRIPT

ARTICLE IN PRESS
REVIEW
Obesity and psoriasis: From the Medical Board of theNational Psoriasis Foundation
Samuel Bremmer, BS,a Abby S. Van Voorhees, MD,c Sylvia Hsu, MD,d Neil J. Korman, MD, PhD,e
Mark G. Lebwohl, MD,f Melodie Young, ARNP,g Bruce F. Bebo, Jr, PhD,h and Andrew Blauvelt, MDa,b,i
for the National Psoriasis Foundation
Portland, Oregon; Philadelphia, Pennsylvania; Houston and Dallas, Texas; Cleveland, Ohio;
New York, New York; and Portland, Oregon
From
ol
Po
va
le
th
Re
m
Yo
as
A
Fund
Discl
Vo
A
ne
ha
be
an
an
fo
An association between obesity and psoriasis has been reported. For a variety of reasons, obese personswith psoriasis are often more difficult to treat. We sought to review the literature on obesity and psoriasisand to discuss efficacy and safety data that could be utilized by clinicians who are making treatmentdecisions for obese persons with psoriasis. We performed a literature review using the terms ‘‘obesity andpsoriasis’’ and ‘‘metabolic syndrome and psoriasis.’’ Evidence from relevant literature was evaluated andcategorized according to the criteria of Shekelle et al (published 1999). Numerous reports cite anassociation between obesity and psoriasis. When compared with non-obese patients with psoriasis, obesepatients with psoriasis are more likely to experience certain adverse effects to medications and are lesslikely to respond favorably to systemic therapies. The amount of category I evidence for objectivelydetermining the best treatment choices for obese patients with psoriasis was scarce and thus did not allowfor the development of a treatment algorithm that could be generally applied for all psoriasis patients whoare obese. Efficacy and safety concerns affected by obesity are important considerations for clinicians whoare making decisions on proper treatment of psoriasis. ( J Am Acad Dermatol 10.1016/j.jaad.2009.09.053.)
INTRODUCTION
Abbreviations used:BMI: body mass indexHDL: high-density lipoproteinIFN-g: interferon gammaIL: interleukinOR: odds ratioPASI: Psoriasis Area and Severity IndexTNF-a: tumor necrosis factor alpha
The association between obesity and psoriasis hasbeen the focus of several recent reviews.1-4 Obesity isdefined as a body mass index (BMI) of 30 or greater,whereas morbid obesity is defined as a BMI of 35 orgreater. Lindegard5 first described an associationbetween obesity and psoriasis in a study of 159,200registered Swedish citizens over a 10-year period.
the Departments of Dermatologya and Molecular Microbi-
ogy & Immunology,b Oregon Health & Science University,
rtland; Department of Dermatology, University of Pennsyl-
nia, Philadelphiac; Department of Dermatology, Baylor Col-
ge of Medicine, Houstond; Department of Dermatology and
e Murdough Family Center for Psoriasis, Case Western
serve University/University Hospital of Clevelande; Depart-
ent of Dermatology, Mount Sinai School of Medicine, New
rk Universityf; Modern Dermatology, Dallasg; National Psori-
is Foundation, Portlandh; and Dermatology Service, Veterans
ffairs Medical Center, Portland.i
ed by the National Psoriasis Foundation, Portland, OR.
osures: Dr Bremmer has no disclosures to report. Dr Van
orhees has been a consultant, investigator, or speaker for
bbott, Amgen, Astellas, Centocor, Genentech, Incyte, Con-
tics, Warner Chilcott, Photomedix, Roche, and Synta; she also
s a significant conflict of interest with Merck. Dr Hsu has
en a consultant for Abbott, Amgen, Biogen Idec, Centocor,
d Genentech; she has been a clinical investigator for Amgen
d Centocor. Dr Korman has been an investigator or speaker
r Abbott, Amgen, Astellas, Centocor, and Genentech. Dr
Lebwohl has been a consultant for Abbott, Amgen, Astellas,
Centocor, Genentech, UCB Pharma, Stiefel, Triax, Pharmaderm,
Medicis, Novartis, and Warner Chilcott; he has been a speaker
for Abbott, Amgen, Astellas, Centocor, and Genentech. Ms
Young has been a consultant or speaker for Abbott, Amgen,
Astellas, Biogen Idec, Centocor, and Genentech. Dr Bebo is
employed by the National Psoriasis Foundation. The Founda-
tion receives unrestricted financial support from Abbott,
Centocor, Amgen, Wyeth, Genentech, Astellas, Stiefel, Gal-
derma, Warner Chilcott, and Photomedix. Dr Blauvelt has
been a consultant, investigator, or speaker for Abbott, Amgen,
Centocor, Genentech, Anacor, Coria, Vascular Biogenics, PM
Toleikis & Associates, MacroGenics, Eli Lilly, CombinatoRx,
Cerimon, Barrier Therapeutics, Pfizer, and Novo Nordisk.
Reprint requests: Andrew Blauvelt, MD, 3710 SW US Veterans
Hospital Rd., Mail Code R&D 55, Portland, OR 97239. E-mail:
Published online August 06, 2010.
0190-9622/$36.00
ª 2010 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2009.09.053
1

J AM ACAD DERMATOL2 Bremmer et al
ARTICLE IN PRESS
This association has been confirmed in many morerecent publications.6-13 In an Italian case-controlstudy with 560 psoriatic patients, the odds of havingpsoriasis with a BMI between 26 and 29 or above 30were 1.6 and 1.9, respectively, compared to non-obese control subjects.7 A study from the UnitedKingdom of 127,706 patients with mild psoriasis
CAPSULE SUMMARY
d Numerous reports cite an associationbetween obesity and psoriasis.
d When compared with non-obesepatients with psoriasis, obese patientswith psoriasis are more likely toexperience certain adverse effects tomedications and are less likely torespond favorably to systemic therapies.
d The amount of category I evidence forobjectively determining the besttreatment choices for obese patientswith psoriasis is scarce and thus does notallow for the development of atreatment algorithm.
(defined as those who werenot treated with systemictherapies or phototherapies)and 3,854 patients with se-vere psoriasis (defined asthose who were treatedwith systemic therapies orphototherapies) demon-strated higher adjusted oddsof obesity in patients withsevere psoriasis (odds ratio[OR] = 1.8) than in patientswith mild psoriasis (OR =1.3) compared with patientswithout psoriasis.8 In a re-port encompassing 16,851individuals with psoriasis,patients younger than 35years old were more likelyto demonstrate obesity (OR =
2.2) than patients older than 65 years of age (OR =1.6) compared with normal controls.9 In anotherstudy, morbidly obese patients self-reported thepresence of inverse psoriasis in 13% of cases com-pared to 11% of obese and 5% of non-obese pa-tients.10 In combination, these studies suggest apositive correlation between body weight and bothprevalence and severity of psoriasis.According to National Health and NutritionExamination Survey data, 30% of all adult U.S.citizens were obese in the 4-year period of 1999-2002.14 Given that approximately 2% of the generalpopulation has psoriasis,15 and given that psoriasis isassociated with obesity, it will become increasinglyimportant for clinicians to become familiar withappropriate treatment regimens for patients withboth of these conditions. Furthermore, ongoinggenetic and pathophysiologic studies offer the prom-ise of understanding how these two common con-ditions are related.
METHODSMEDLINE and PubMed were both searched for a
combination of the following terms: ‘‘obesity andpsoriasis’’ and ‘‘metabolic syndrome and psoriasis.’’Literature relevant to psoriasis and obesity or themetabolic syndrome was reviewed. Literature wasadditionally acquired through citations from reviews
in our initial search and by searching ‘‘psoriasis’’concurrentlywith thenameof amedicationor class ofmedications. Reports in the literature were evaluatedaccording to the criteria of Shekelle et al.16 CategoryIA evidence consists of data from meta-analysis frommultiple randomized controlled trials; category IBevidence includes data from at least one randomized
controlled trial. Category IIAevidence includes evidencefrom at least one controlledstudy without randomiza-tion, whereas category IIBevidence involves evidencefrom at least one other typeof quasi-experimental study.Category III evidence con-sists of data from non-exper-imental descriptive studies,including comparative, cor-relation, and case-controlstudies. Finally, category IVevidence consists of evi-dence fromexpert committeereports or opinions and clin-ical experiences of respectedauthorities.
Evidence
1. The evidence for using topical therapies, includ-ing corticosteroids, calcipotriol, the two-com-pound formulation of calcipotriol andbetamethasone dipropionate, and tazarotene, inobese patients with psoriasis is primarily anec-dotal (Table I). The evidence for use of excimerlaser is also anecdotal in these patients.
2. With psoralen plus long-wave ultraviolet radia-tion A (UVA) photochemotherapy, the dose ofmethoxsalen is dosed by weight, and thereforeefficacy is unaffected by patient weight (TableII). Efficacy of narrow-band UVB phototherapy ispredicted to be unaffected by the weight of thepatient; however, there is no published evidenceto support this assertion.
3. Weight-based dosing for infliximab offers thepossibility of similar outcomes in obese and non-obese patients (Table III).17-20
4. Adalimumab and ustekinumab efficacy is dimin-ished somewhat in obese patients, but to a lesserextent than efficacy of etanercept and alefacept(Tables IV-VII).21-25
5. Since obesity may be associated with elevatedlipids, acitretin should be used judiciously in
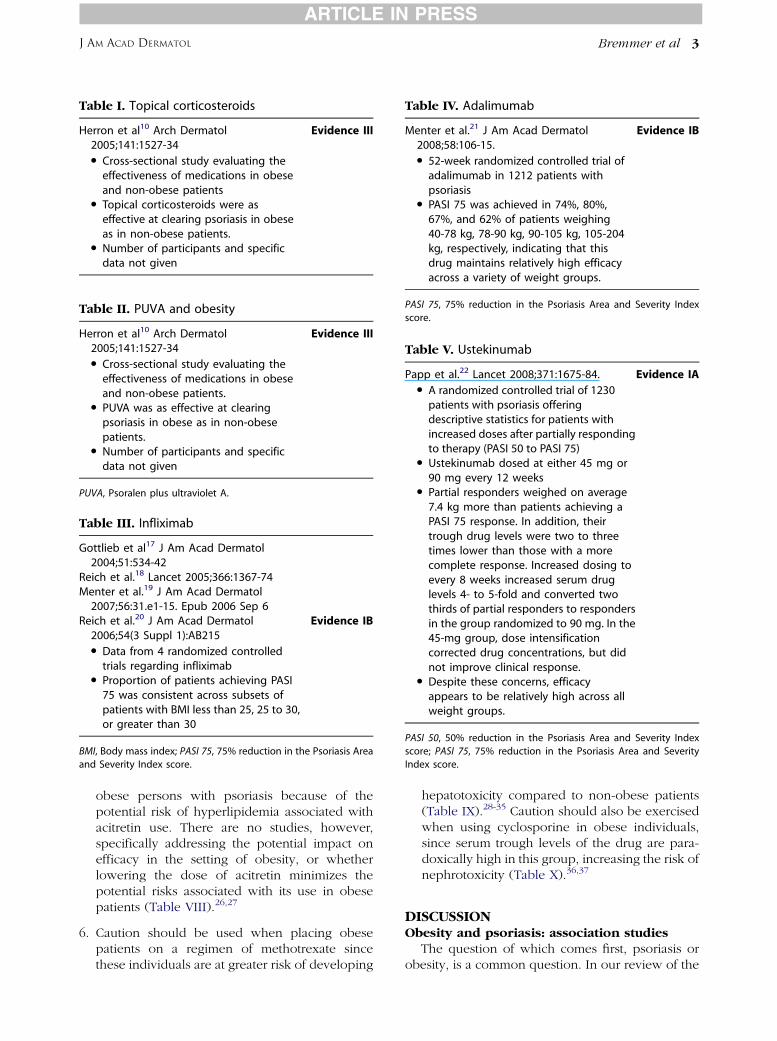
Table I. Topical corticosteroids
Herron et al10 Arch Dermatol2005;141:1527-34
Evidence III
d Cross-sectional study evaluating theeffectiveness of medications in obeseand non-obese patients
d Topical corticosteroids were aseffective at clearing psoriasis in obeseas in non-obese patients.
d Number of participants and specificdata not given
Table II. PUVA and obesity
Herron et al10 Arch Dermatol2005;141:1527-34
Evidence III
d Cross-sectional study evaluating theeffectiveness of medications in obeseand non-obese patients.
d PUVA was as effective at clearingpsoriasis in obese as in non-obesepatients.
d Number of participants and specificdata not given
PUVA, Psoralen plus ultraviolet A.
Table III. Infliximab
Gottlieb et al17 J Am Acad Dermatol2004;51:534-42
Reich et al.18 Lancet 2005;366:1367-74Menter et al.19 J Am Acad Dermatol
2007;56:31.e1-15. Epub 2006 Sep 6Reich et al.20 J Am Acad Dermatol
2006;54(3 Suppl 1):AB215Evidence IB
d Data from 4 randomized controlledtrials regarding infliximab
d Proportion of patients achieving PASI75 was consistent across subsets ofpatients with BMI less than 25, 25 to 30,or greater than 30
BMI, Body mass index; PASI 75, 75% reduction in the Psoriasis Area
and Severity Index score.
Table IV. Adalimumab
Menter et al.21 J Am Acad Dermatol2008;58:106-15.
Evidence IB
d 52-week randomized controlled trial ofadalimumab in 1212 patients withpsoriasis
d PASI 75 was achieved in 74%, 80%,67%, and 62% of patients weighing40-78 kg, 78-90 kg, 90-105 kg, 105-204kg, respectively, indicating that thisdrug maintains relatively high efficacyacross a variety of weight groups.
PASI 75, 75% reduction in the Psoriasis Area and Severity Index
score.
Table V. Ustekinumab
Papp et al.22 Lancet 2008;371:1675-84. Evidence IAd A randomized controlled trial of 1230
patients with psoriasis offeringdescriptive statistics for patients withincreased doses after partially respondingto therapy (PASI 50 to PASI 75)
d Ustekinumab dosed at either 45 mg or90 mg every 12 weeks
d Partial responders weighed on average7.4 kg more than patients achieving aPASI 75 response. In addition, theirtrough drug levels were two to threetimes lower than those with a morecomplete response. Increased dosing toevery 8 weeks increased serum druglevels 4- to 5-fold and converted twothirds of partial responders to respondersin the group randomized to 90 mg. In the45-mg group, dose intensificationcorrected drug concentrations, but didnot improve clinical response.
d Despite these concerns, efficacyappears to be relatively high across allweight groups.
PASI 50, 50% reduction in the Psoriasis Area and Severity Index
score; PASI 75, 75% reduction in the Psoriasis Area and Severity
Index score.
ARTICLE IN PRESS
J AM ACAD DERMATOL Bremmer et al 3
obese persons with psoriasis because of thepotential risk of hyperlipidemia associated withacitretin use. There are no studies, however,specifically addressing the potential impact onefficacy in the setting of obesity, or whetherlowering the dose of acitretin minimizes thepotential risks associated with its use in obesepatients (Table VIII).26,27
6. Caution should be used when placing obesepatients on a regimen of methotrexate sincethese individuals are at greater risk of developing
hepatotoxicity compared to non-obese patients(Table IX).28-35 Caution should also be exercisedwhen using cyclosporine in obese individuals,since serum trough levels of the drug are para-doxically high in this group, increasing the risk ofnephrotoxicity (Table X).36,37
DISCUSSIONObesity and psoriasis: association studies
The question of which comes first, psoriasis orobesity, is a common question. In our review of the
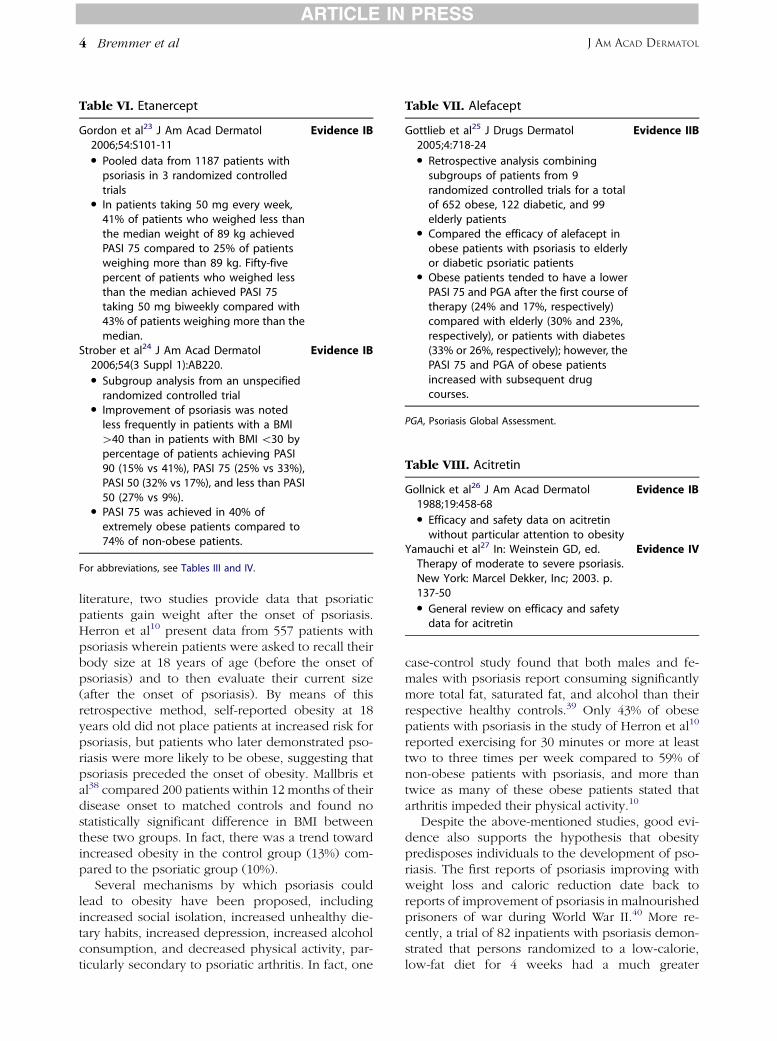
Table VI. Etanercept
Gordon et al23 J Am Acad Dermatol2006;54:S101-11
Evidence IB
d Pooled data from 1187 patients withpsoriasis in 3 randomized controlledtrials
d In patients taking 50 mg every week,41% of patients who weighed less thanthe median weight of 89 kg achievedPASI 75 compared to 25% of patientsweighing more than 89 kg. Fifty-fivepercent of patients who weighed lessthan the median achieved PASI 75taking 50 mg biweekly compared with43% of patients weighing more than themedian.
Strober et al24 J Am Acad Dermatol2006;54(3 Suppl 1):AB220.
Evidence IB
d Subgroup analysis from an unspecifiedrandomized controlled trial
d Improvement of psoriasis was notedless frequently in patients with a BMI[40 than in patients with BMI \30 bypercentage of patients achieving PASI90 (15% vs 41%), PASI 75 (25% vs 33%),PASI 50 (32% vs 17%), and less than PASI50 (27% vs 9%).
d PASI 75 was achieved in 40% ofextremely obese patients compared to74% of non-obese patients.
For abbreviations, see Tables III and IV.
Table VII. Alefacept
Gottlieb et al25 J Drugs Dermatol2005;4:718-24
Evidence IIB
d Retrospective analysis combiningsubgroups of patients from 9randomized controlled trials for a totalof 652 obese, 122 diabetic, and 99elderly patients
d Compared the efficacy of alefacept inobese patients with psoriasis to elderlyor diabetic psoriatic patients
d Obese patients tended to have a lowerPASI 75 and PGA after the first course oftherapy (24% and 17%, respectively)compared with elderly (30% and 23%,respectively), or patients with diabetes(33% or 26%, respectively); however, thePASI 75 and PGA of obese patientsincreased with subsequent drugcourses.
PGA, Psoriasis Global Assessment.
Table VIII. Acitretin
Gollnick et al26 J Am Acad Dermatol1988;19:458-68
Evidence IB
d Efficacy and safety data on acitretinwithout particular attention to obesity
Yamauchi et al27 In: Weinstein GD, ed.Therapy of moderate to severe psoriasis.New York: Marcel Dekker, Inc; 2003. p.137-50
Evidence IV
d General review on efficacy and safetydata for acitretin
ARTICLE IN PRESS
J AM ACAD DERMATOL4 Bremmer et al
literature, two studies provide data that psoriaticpatients gain weight after the onset of psoriasis.Herron et al10 present data from 557 patients withpsoriasis wherein patients were asked to recall theirbody size at 18 years of age (before the onset ofpsoriasis) and to then evaluate their current size(after the onset of psoriasis). By means of thisretrospective method, self-reported obesity at 18years old did not place patients at increased risk forpsoriasis, but patients who later demonstrated pso-riasis were more likely to be obese, suggesting thatpsoriasis preceded the onset of obesity. Mallbris etal38 compared 200 patients within 12 months of theirdisease onset to matched controls and found nostatistically significant difference in BMI betweenthese two groups. In fact, there was a trend towardincreased obesity in the control group (13%) com-pared to the psoriatic group (10%).
Several mechanisms by which psoriasis couldlead to obesity have been proposed, includingincreased social isolation, increased unhealthy die-tary habits, increased depression, increased alcoholconsumption, and decreased physical activity, par-ticularly secondary to psoriatic arthritis. In fact, one
case-control study found that both males and fe-males with psoriasis report consuming significantlymore total fat, saturated fat, and alcohol than theirrespective healthy controls.39 Only 43% of obesepatients with psoriasis in the study of Herron et al10
reported exercising for 30 minutes or more at leasttwo to three times per week compared to 59% ofnon-obese patients with psoriasis, and more thantwice as many of these obese patients stated thatarthritis impeded their physical activity.10
Despite the above-mentioned studies, good evi-dence also supports the hypothesis that obesitypredisposes individuals to the development of pso-riasis. The first reports of psoriasis improving withweight loss and caloric reduction date back toreports of improvement of psoriasis in malnourishedprisoners of war during World War II.40 More re-cently, a trial of 82 inpatients with psoriasis demon-strated that persons randomized to a low-calorie,low-fat diet for 4 weeks had a much greater
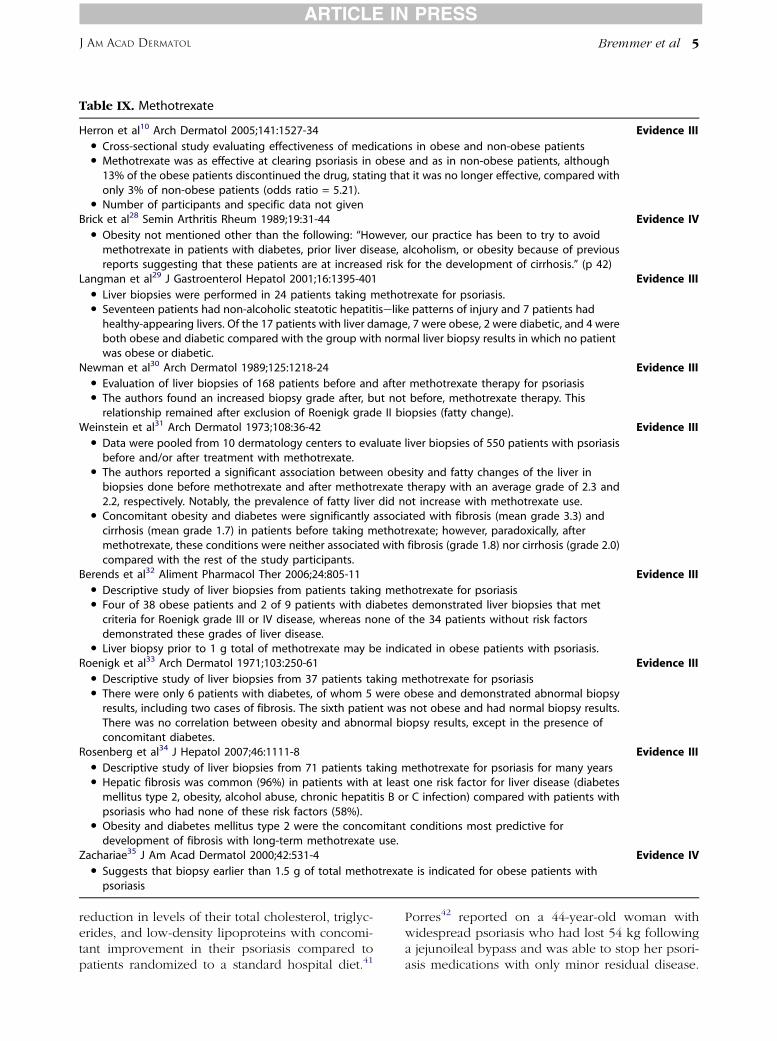
Table IX. Methotrexate
Herron et al10 Arch Dermatol 2005;141:1527-34 Evidence IIId Cross-sectional study evaluating effectiveness of medications in obese and non-obese patientsd Methotrexate was as effective at clearing psoriasis in obese and as in non-obese patients, although
13% of the obese patients discontinued the drug, stating that it was no longer effective, compared withonly 3% of non-obese patients (odds ratio = 5.21).
d Number of participants and specific data not givenBrick et al28 Semin Arthritis Rheum 1989;19:31-44 Evidence IV
d Obesity not mentioned other than the following: ‘‘However, our practice has been to try to avoidmethotrexate in patients with diabetes, prior liver disease, alcoholism, or obesity because of previousreports suggesting that these patients are at increased risk for the development of cirrhosis.’’ (p 42)
Langman et al29 J Gastroenterol Hepatol 2001;16:1395-401 Evidence IIId Liver biopsies were performed in 24 patients taking methotrexate for psoriasis.d Seventeen patients had non-alcoholic steatotic hepatitiselike patterns of injury and 7 patients had
healthy-appearing livers. Of the 17 patients with liver damage, 7 were obese, 2 were diabetic, and 4 wereboth obese and diabetic compared with the group with normal liver biopsy results in which no patientwas obese or diabetic.
Newman et al30 Arch Dermatol 1989;125:1218-24 Evidence IIId Evaluation of liver biopsies of 168 patients before and after methotrexate therapy for psoriasisd The authors found an increased biopsy grade after, but not before, methotrexate therapy. This
relationship remained after exclusion of Roenigk grade II biopsies (fatty change).Weinstein et al31 Arch Dermatol 1973;108:36-42 Evidence III
d Data were pooled from 10 dermatology centers to evaluate liver biopsies of 550 patients with psoriasisbefore and/or after treatment with methotrexate.
d The authors reported a significant association between obesity and fatty changes of the liver inbiopsies done before methotrexate and after methotrexate therapy with an average grade of 2.3 and2.2, respectively. Notably, the prevalence of fatty liver did not increase with methotrexate use.
d Concomitant obesity and diabetes were significantly associated with fibrosis (mean grade 3.3) andcirrhosis (mean grade 1.7) in patients before taking methotrexate; however, paradoxically, aftermethotrexate, these conditions were neither associated with fibrosis (grade 1.8) nor cirrhosis (grade 2.0)compared with the rest of the study participants.
Berends et al32 Aliment Pharmacol Ther 2006;24:805-11 Evidence IIId Descriptive study of liver biopsies from patients taking methotrexate for psoriasisd Four of 38 obese patients and 2 of 9 patients with diabetes demonstrated liver biopsies that met
criteria for Roenigk grade III or IV disease, whereas none of the 34 patients without risk factorsdemonstrated these grades of liver disease.
d Liver biopsy prior to 1 g total of methotrexate may be indicated in obese patients with psoriasis.Roenigk et al33 Arch Dermatol 1971;103:250-61 Evidence III
d Descriptive study of liver biopsies from 37 patients taking methotrexate for psoriasisd There were only 6 patients with diabetes, of whom 5 were obese and demonstrated abnormal biopsy
results, including two cases of fibrosis. The sixth patient was not obese and had normal biopsy results.There was no correlation between obesity and abnormal biopsy results, except in the presence ofconcomitant diabetes.
Rosenberg et al34 J Hepatol 2007;46:1111-8 Evidence IIId Descriptive study of liver biopsies from 71 patients taking methotrexate for psoriasis for many yearsd Hepatic fibrosis was common (96%) in patients with at least one risk factor for liver disease (diabetes
mellitus type 2, obesity, alcohol abuse, chronic hepatitis B or C infection) compared with patients withpsoriasis who had none of these risk factors (58%).
d Obesity and diabetes mellitus type 2 were the concomitant conditions most predictive fordevelopment of fibrosis with long-term methotrexate use.
Zachariae35 J Am Acad Dermatol 2000;42:531-4 Evidence IVd Suggests that biopsy earlier than 1.5 g of total methotrexate is indicated for obese patients with
psoriasis
ARTICLE IN PRESS
J AM ACAD DERMATOL Bremmer et al 5
reduction in levels of their total cholesterol, triglyc-erides, and low-density lipoproteins with concomi-tant improvement in their psoriasis compared topatients randomized to a standard hospital diet.41
Porres42 reported on a 44-year-old woman withwidespread psoriasis who had lost 54 kg followinga jejunoileal bypass and was able to stop her psori-asis medications with only minor residual disease.

Table X. Cyclosporine
Shibata et al36 Am J Health Syst Pharm1998;55:1598-602
Evidence III
d Trough concentrations of cyclosporineevaluated in 16 patients with psoriasisaccording to an obesity index
d Serum trough concentrations weresignificantly correlated with the obesityindex (r2 = 0.509; P \.0001). Afteradjustment to the same milligram perkilogram dosage, obesity still correlatedwith increased serum cyclosporine levels.
d The patient with the highest obesityindex and highest trough concentration ofcyclosporine experienced nephrotoxicity,despite having the lowest milligram perkilogram dosing regimen.
Gisondi et al37 Am J Clin Nutr2008;88:1242-7
Evidence IB
d 24-week randomized, controlled,investigator-blinded study comparingcyclosporine, 2.5 mg/kg/d, versuscyclosporine, 2.5 mg/kg/d plus dietaryrestriction
d PASI 75 achieved in 20 of 30 patients(67%) in the cyclosporine plus diet groupand in 9 of 31 patients (29%) in thecyclosporine-only group
ARTICLE IN PRESS
J AM ACAD DERMATOL6 Bremmer et al
Two case reports have since described the complete,medication-free resolution of severe, widespread,chronic psoriasis refractory to medical managementwithin a year of roux-en-Y gastric bypass sur-gery.43,44 Perhaps most convincingly, prospectivedata on 78,626 women (892 with self-reported pso-riasis) in a nurses’ health study found that weightgain placed individuals at an increased risk for thesubsequent development of psoriasis. Additionally,the incidence of psoriasis was found to be linearlyassociated with the BMI with the greatest relative riskof 2.69 for patients with a BMI of 35 or morecompared to patients with a BMI of 21 to 23. Therisk of psoriasis at 18 years of age was also linearlyassociated with BMI.45 These results are in contrast tothose of Herron et al10 and Mallbris et al.38 Given theprospective study design and larger sample size ofthe nurses’ health study, it is likely that obesitypredisposes to development of psoriasis.
Links between pathogenesis of obesity andpsoriasis
The recent understanding of obesity as a proin-flammatory state and adipose tissue as an immuneand endocrine organ help explain how obese pa-tients may be predisposed to the development ofpsoriasis. Tumor necrosis factor alpha (TNF-a)
mRNA expression is elevated in adipocytes of ge-netically obese rodents.46 Biopsy specimens of hu-man adipose tissue have also demonstratedincreased levels of TNF-a mRNA in patients with ahigh percentage of body fat (r = 0.46).47 TNF-amRNA and protein expression is 2 and 2.5 timeshigher, respectively, in adipocytes of obese individ-uals compared with controls.48 TNF-a expression inadipocytes of obese patients has been shown todecrease with weight loss.47,48
Some data also support the function of TNF-a as asystemic hormone. A study of 38 obese women and30 normal-weight control subjects demonstrated asignificantly lower mean serum TNF-a concentrationof 0.82 pg/mL in lean women compared to 3.45pg/mL in their obese counterparts, which dropped to2.63 pg/mL following weight loss.49 Additionally,obesity has been shown to be associated with highlevels of circulating TNF-a receptors in humans.50
TNF-a administration causes an increase in serumtriglycerides and very-low-density lipoproteins inrats and humans.46 It should be noted, however,that most studies have failed to demonstrate sub-stantial quantities of TNF-a in human serum; thusmost experts believe that the pro-adipogenic effectsof TNF-a are caused by autocrine or paracrine effectsdirectly within adipose tissue.48,50
Additionally, TNF-a contributes to insulin resis-tance by inducing serine phosphorylation of insulinreceptor substrate 1, which reduces tyrosine kinaseactivity of the insulin receptor.51,52 Treatment ofobese rats with soluble TNF-a receptors normalizesTNF-a expression and increases insulin sensitivity.46
The administration of exogenous TNF-a into healthyanimals has also been shown to decrease insulinsensitivity.53 These findings suggest a ‘‘lipostat’’function of TNF-a or that insulin resistance couldbe induced in order to limit obesity, as suggestedpreviously by Eckel.54 Unfortunately, a human studywith 20 obese patients with insulin-resistant diabetesdemonstrated that the TNF-a blocking agent etaner-cept does not significantly increase insulin sensitivitydespite reducing serum levels of the inflammatorycytokines interleukin 6 (IL-6) and C-reactiveprotein.55
Other inflammatory cytokines, which are elevatedin the serum of obese patients with psoriasis, includeIL-6, IL-1b, CCL2, CXCL8, CXCL9, and C-reactiveprotein.56-58 Of these, CXCL8 has been shown to bedecreased following UVB therapy.56 Most studieshave also shown increased levels of apolipoproteinA-1 in the serum of patients with psoriasis.38,59,60 Ithas been demonstrated that apolipoprotein A-1 oxi-dizes high-density lipoprotein (HDL), making it pro-atherogenic.61

ARTICLE IN PRESS
J AM ACAD DERMATOL Bremmer et al 7
The metabolic syndrome is a constellation of riskfactors known to increase a patient’s risk of coronaryheart disease and is defined by the NationalCholesterol Education Program Adult TreatmentPanel III as the presence of 3 of the following 5 riskfactors: fasting glucose $ 110 mg/dL, blood pressure$ 130/85 mm Hg, triglycerides $ 150 mg/dL, HDL-C\40 mg/dL in men or \50 mg/dL in women, andwaist circumference [102 cm in men or [88 cm inwomen.62 Given the increased inflammation seen inpatients with psoriasis, it is not surprising that thesepatients are at an increased risk for meeting criteria ofthe metabolic syndrome (OR = 1.7-5.3).9,11,63
Numerous groups have published reports of psoriasisbeing associated with increased serum insulinlevels,62 diabetes (OR = 1.5-2.5),5,6,8,9,11,64-68 hyper-tension (OR = 1.1-3.3),5,6,8,9,11,12,65,66,69 hypertriglyc-eridemia,9,58-60,63,65 abdominal obesity,63 ordecreased HDL-C.9,58,59,70 Additionally, hypercholes-terolemia,58,59,65 increased serum LDL-C,58,59 andgeneralized hyperlipidemia (OR = 1.3-3.1)8,11,69
have been reported to be more common in patientswith psoriasis. Although the best and greatest amountof evidence supports these associations, it should benoted that a few studies have failed to demonstrate anassociation between psoriasis and increasedinsulin,70 glucose,63,70 triglycerides,70 total choles-terol,60,70 LDL-C,70 hypertension,63 or low HDL-C.60,63
Understanding hormonal and cytokine biologycan also explain the association between psoriasisand the metabolic syndrome. In mice, leptin hasbeen shown to bind directly to T cells and tostimulate IL-2 and interferon gamma (IFN-g) pro-duction. Withholding food from mice for 48 hoursdecreases leptin levels and causes a 69% decrease indelayed-type hypersensitivity responses, an effectthat was completely reversed by leptin injection.71 Inaddition, TNF-a induces the rapid release of leptinfrom adipocytes in culture, causes circulating leptinlevels to increase in vivo,72 and acts independently todecrease food intake.73 In a report of children withleptin deficiency, IFN-g levels were low and trans-forming growth factor beta levels were high, sup-porting a predominantly anti-inflammatory cytokinemilieu in leptin-deficient individuals.74 Althoughleptin levels were first reported as normal in psoriaticpatients compared to BMI-matched controls,56 arecent study showed high levels of leptin in personswith psoriasis.11 The clinical implication of thisfinding is that leptin contributes to the proinflamma-tory environment observed in both obesity andpsoriasis.
Resistin, produced by macrophages in the stromalcompartment of abdominal and omental adipose
tissue, induces insulin resistance.75 Serum levels ofresistin have been shown to be elevated in patientswith psoriasis compared to BMI-matched controls.Furthermore, two independent studies have shownthat serum resistin levels correlate with psoriasisdisease severity.56,64
Adiponectin is an anti-inflammatory hormone thatimproves insulin sensitivity; suppresses the effects ofTNF-a, IL-6, and IFN-g,9,57; and reduces TNF-aemediated monocyte attachment to human aorticendothelial cells.76 Patients with a mean reduction of21% of their BMI following gastric bypass alsoexperienced a 46% increase in serum levels ofadiponectin.77 In a study with 22 psoriatic patients,adiponectin levels were twice as high in patients ofnormal weight with psoriasis compared with healthycontrols, possibly owing to a compensatory effectagainst the inflammatory cytokines in psoriasis.However, adiponectin levels in obese patients withpsoriasis trended toward being even lower than inhealthy controls.57
Treatment considerations for obese personswith psoriasis: Efficacy
The efficacy of medications for psoriasis can beaffected by a patient’s weight.78 As discussed in areview by Clark and Lebwohl,79 weight-based dos-ing is used only for infliximab (5 mg/kg), whereasthe dosing for alefacept, etanercept, and adalimu-mab is fixed. In a review of data from 3 randomizedcontrolled trials regarding infliximab, Reich et al20
state that the proportion of patients achievingPsoriasis Area and Severity Index (PASI) 75 wasconsistent across subsets of patients with BMI lessthan 25, 25 to 30, or greater than 30.
In a 52-week study using adalimumab in 1212psoriatic patients, PASI 75 was achieved in 74%, 80%,67%, and 62% of patients weighing 40-78 kg, 78-90kg, 90-105 kg, 105-204 kg, respectively, indicatingthat this drug retains relatively high levels of efficacyin various weight groups.21 Ustekinumab is a bio-logic agent that blocks the shared p40 protein sub-unit of human IL-23 and IL-12, which blocksproliferation of both T helper 17 and T helper1 cells.80 A study using ustekinumab dosed at either45 mg or 90 mg every 12 weeks in 1230 psoriasispatients found that partial responders (defined ashaving PASI 50-PASI 75) weighed on average 7.4 kgmore than patients achieving a PASI 75 response.22
Increasing the dosing frequency to every 8 weeksincreased serum drug levels 4- to 5-fold and con-verted two thirds of partial responders in the grouprandomized to 90 mg of drug to full responders.However, in the 45-mg group, increasing the dosingfrequency corrected drug concentrations, but did not

ARTICLE IN PRESS
J AM ACAD DERMATOL8 Bremmer et al
improve clinical responses.22 It is unknown whetherdosing of ustekinumab will be fixed or weight based,but these data suggest that weight appears to impactustekinumab efficacy at fixed doses, although overallefficacy still appears to remain relatively high inobese patients.
In a study of 1187 patients with psoriasis, etaner-cept was given at 50 mg every week or twice weekly,and the number of patients achieving PASI 75 atweek 12 was evaluated. In patients taking 50 mgevery week, 41% of patients who weighed less thanthe median weight of 89 kg achieved PASI 75compared to 25% of patients weighing more than89 kg. Fifty-five percent of patients who weighed lessthan the median achieved PASI 75 taking 50 mg twiceweekly compared to 43% of patients weighing morethan the median.23 These results not only suggestthat heavier patients are less responsive to a fixeddose of etanercept, but that there was a 16% differ-ence between lighter and heavier patients respond-ing to a weekly dose and only a 12% difference forthe twice-weekly dose suggest that more drug wouldlead to greater efficacy in obese persons with pso-riasis. A separate trial evaluated the efficacy ofetanercept given at 50 mg twice weekly accordingto differences in BMI. Improvement of psoriasis wasnoted less frequently in patients with a BMI greaterthan 40 than in patients with BMI less than 30 bypercentage of patients achieving PASI 90 (15% vs41%), PASI 75 (25% vs 33%), PASI 50 (32% vs 17%),and less than PASI 50 (27% vs 9%).24 Of note, for all ofthe ‘‘fixed dose biologics’’ mentioned herein, doseescalation is likely to improve efficacy in obesepatients with psoriasis, and thus should be consid-ered if possible.
In addition to clinical efficacy in psoriasis, it ispossible that systemic anti-inflammatory treatment ofobese patients with psoriasis protects against cardi-ovascular disease, which is associated with severepsoriasis and is likely worsened by obesity.69,81-83 Tothis point, Prodanovich and colleagues83 found thatincidence of cardiovascular events was lower inpatients with psoriasis that had used methotrexatecompared to those who had not, supporting the viewthat there could be important systemic health ben-efits to individuals with psoriasis when treated withsystemic medications. An open and important issueis whether use of TNF-a blockers will reduce theincidence of cardiovascular events in patients withpsoriasis.
Treatment considerations for obese psoriatics:Adverse events
The lack of studies on the use of acitretin in thesetting of obesity limits the conclusions that can be
drawn about its role in this particular group ofpatients. Since obesity may be associated with ele-vated lipids, acitretin should be used judiciously inobese psoriatics. It remains unknown whether adose alteration is recommended in this setting inorder to try to reduce this potential risk.
In the study by Herron et al,10 methotrexate wasas effective in clearing psoriasis in obese patients asit was in non-obese patients, although 13% of obesepatients discontinued the drug, stating that it was nolonger effective compared to only 3% of non-obesepatients (OR = 5.21). However, the possible risk ofliver cirrhosis in obese patients taking methotrexatehas raised significant concerns. Although liver bi-opsy is recommended after a cumulative metho-trexate dose of 1.5 g, many authors have suggestedthat biopsy should be performed after a lowercumulative dosage in obese patients.31,33,34,84
Among patients taking methotrexate for psoriasis,4 of 38 obese patients and 2 of 9 patients withdiabetes demonstrated liver biopsy results that metcriteria for Roenigk grade III or IV, whereas none ofthe 34 patients without risk factors demonstratedthese grades of liver disease.32 Another study of liverbiopsies from 24 patients taking methotrexate forpsoriasis demonstrated 17 patients with a non-alco-holic steatotic hepatitis-like pattern of injury and 7patients with a healthy-appearing liver. Of the 17patients with liver damage, 7 were obese, 2 werediabetic, and 4 were both obese and diabetic com-pared with the group with normal liver biopsies inwhich no patient was obese or diabetic.29 Newmanet al30 evaluated the liver biopsies of 168 patientsbefore and after methotrexate therapy for psoriasisand found an increased biopsy grade after, but notbefore, methotrexate therapy. This relationshipremained after excluding Roenigk grade II biopsies(fatty change); this exclusion analysis was per-formed because obesity correlates with fatty liverchanges in the general population.30 In a report byRoenigk et al33 of a group of 37 psoriatic patientswho had taken methotrexate for psoriasis, therewere 5 patients with diabetes and concomitantobesity, all of whom demonstrated abnormal biopsyresults, including two cases of fibrosis. One diabeticpatient who was not obese had normal liver biopsyresults. Recently, Rosenberg et al34 also reported ahigh degree of liver fibrosis in psoriasis patients onlong-term methotrexate therapy who were eitherobese or diabetic. Thus, in these studies, there was aclear correlation between obesity and abnormalliver biopsy results in psoriatics being treated withmethotrexate.
Weinstein et al31 pooled data from 10 dermatologycenters to evaluate the liver biopsies of 550 patients

ARTICLE IN PRESS
J AM ACAD DERMATOL Bremmer et al 9
with psoriasis before and/or after treatment withmethotrexate. They reported a significant associationbetween obesity and fatty changes in the liver inbiopsies done before and after methotrexate ther-apy, with an average grade of 2.3 and 2.2, respec-tively. Notably, the prevalence of fatty liver did notincrease with methotrexate use. Concomitant obe-sity and diabetes were significantly associated withfibrosis (mean grade 3.3) and cirrhosis (mean grade1.7) in patients before taking methotrexate, butparadoxically, after methotrexate therapy, theseconditions were neither associated with fibrosis(1.8) nor cirrhosis (2.0) compared with the rest ofthe study participants. In total, these studies supportthe judicious use of methotrexate in obese patientswith psoriasis, and relatively early monitoring withliver biopsy when methotrexate is chosen as atherapeutic option.
The risk of nephrotoxicity in patients taking theweight-based immunosuppressant cyclosporine alsoseems to be increased in obese patients. Shibataet al36 conducted a study of 16 patients with psoriasiswho were treated with cyclosporine in which theserum trough concentrations were significantly cor-related with the obesity index (r2 = 0.509, P\.0001).After adjustment to the same milligram per kilogramdosage, obesity still paradoxically correlated withincreased serum cyclosporine levels despite cyclo-sporine’s lipophilic properties. This finding is ofparticular concern considering the risks of nephro-toxicity associated with this medication and thepredilection for nephrotoxicity associated with othercomorbid conditions, such as hypertension anddiabetes, in obese patients with psoriasis.Cyclosporine is associated with renal toxicity that isrelated to the dose and duration of treatment85 and isalso associated with other side effects, includinghypertriglyceridemia and hypercholesterolemia.3
During treatment of obese psoriatic patients withcyclosporine, careful monitoring for high serumdrug levels, hypertension, nephrotoxicity, diabetes,and hyperlipidemia should be employed. In addi-tion, dietary restrictions are also recommended,since they have been shown to improve therapeuticresponses to cyclosporine in obese patients withpsoriasis.37
In a disease that places patients at increased riskof each component of the metabolic syndrome, therisk of weight gain as a side effect of anti-psoriaticmedications should not be taken lightly.Unfortunately, use of TNF-a inhibitors may causeweight gain.86,87 In a 6-month study of 141 patientswith psoriasis, methotrexate, 15 mg weekly, wasused as a first-line agent, but patients with severe orrecalcitrant psoriasis were randomized to receive
either etanercept, 25 mg twice weekly, or inflix-imab, 5 mg/kg at weeks 0, 2, and 6 followed byevery 8 weeks. Patients taking infliximab andetanercept gained 2.5 kg (standard deviation [SD]63.3 kg; P \ .004) and 1.5 kg (SD 6 2.7 kg; P \.0002), respectively, compared to patients whocontinued to take methotrexate; these latter patientslost 0.6 kg on average (SD 6 1.4 kg, P \.40).86 Thisstudy was limited by the lack of a control group andselection bias in the study design. Saraceno et al87
observed significant increases in body weight andBMI in 50 psoriatics treated with etanercept com-pared to 100 control patients, with significant dif-ferences observed as early as 12 weeks followingonset of treatment. It has been postulated thatblocking TNF-a, which normally induces the pro-duction73 and release72 of the satiety hormoneleptin, may lead to an increase in hunger andexplain a subsequent weight gain. Despite anapparent increased risk of weight gain from TNF-ablockade, these drugs are highly effective in psori-asis and should probably not be withheld out ofconcern for this side effect.
Data derived from rheumatoid arthritis patientssuggest that TNF-a inhibitor therapy (ie, infliximab)causes a transient decrease in serum HDL levelsimmediately following infusions, with increasedHDL levels occurring just prior to subsequent infu-sions.88,89 Total cholesterol levels were also shownto significantly increase in a transient manner in thefirst 2 weeks after an infusion and then to decreaseslightly before subsequent infusions.89 The implica-tions of these findings in psoriatics are unclear at thistime.
In conclusion, an association between obesityand psoriasis is well established, with evidence tosupport that preexisting obesity can increase the riskof developing psoriasis and that preexisting psoriasiscan increase the risk of becoming obese. Genetic,metabolic, and environmental factors are all likely tocontribute to the association between obesity andpsoriasis. For a variety of reasons, obese psoriaticsare often more difficult to treat. Diminished efficacyand increased risk of certain side effects with certainagents contribute to this complex and challengingclinical situation. Because both obesity itself andconditions associated with obesity can vary widely inany given individual, and because there is scarcecategory I evidence on treating obese psoriatics,broad treatment guidelines or algorithms should notbe utilized for these patients. Nevertheless, efficacyand safety concerns affected by obesity, as reviewedherein, are important considerations for clinicianswho are making decisions on proper treatment ofpsoriasis.

ARTICLE IN PRESS
J AM ACAD DERMATOL10 Bremmer et al
REFERENCES
1. Mallbris L, Ritchlin CT, Stahle M. Metabolic disorders in
patients with psoriasis and psoriatic arthritis. Curr Rheumatol
Res 2006;8:355-63.
2. Sterry W, Strober BE, Menter A. Obesity in psoriasis: The
metabolic, clinical and therapeutic implications. report of an
interdisciplinary conference and review. Br J Dermatol 2007;
157:649-55.
3. Wakkee M, Thio HB, Prens EP, Sijbrands EJ, Neumann HA.
Unfavorable cardiovascular risk profiles in untreated and
treated psoriasis patients. Atherosclerosis 2007;190:1-9.
4. Yosipovitch G, DeVore A, Dawn A. Obesity and the skin: skin
physiology and skin manifestations of obesity. J Am Acad
Dermatol 2007;56:901-16.
5. Lindegard B. Diseases associated with psoriasis in a general
population of 159,200 middle-aged, urban, native Swedes.
Dermatologica 1986;172:298-304.
6. Henseler T, Christophers E. Disease concomitance in psoriasis.
J Am Acad Dermatol 1995;32:982-6.
7. Naldi L, Chatenoud L, Linder D, Belloni Fortina A, Peserico A,
Virgili AR, et al. Cigarette smoking, body mass index, and
stressful life events as risk factors for psoriasis: results from an
Italian case-control study. J Invest Dermatol 2005;125:61-7.
8. Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB, Gelfand
JM. Prevalence of cardiovascular risk factors in patients with
psoriasis. J Am Acad Dermatol 2006;55:829-35.
9. Cohen AD, Sherf M, Vidavsky L, Vardy DA, Shapiro J,
Meyerovitch J. Association between psoriasis and the meta-
bolic syndrome. A cross-sectional study. Dermatology 2008;
216:152-5.
10. Herron MD, Hinckley M, Hoffman MS, Papenfuss J, Hansen CB,
Callis KP, et al. Impact of obesity and smoking on psoriasis
presentation and management. Arch Dermatol 2005;141:1527-
34.
11. Sommer DM, Jenisch S, Suchan M, Christophers E, Weichen-
thal M. Increased prevalence of the metabolic syndrome in
patients with moderate to severe psoriasis. Arch Dermatol Res
2006;298:321-8.
12. Chen YJ, Wu CY, Shen JL, Chu SY, Chen CK, Chang YT, Chen
CM. Psoriasis independently associated with hyperleptinemia
contributing to metabolic syndrome. Arch Dermatol 2008;144:
1571-5.
13. Murray ML, Bergstresser PR, Adams-Huet B, Cohen JB. Rela-
tionship of psoriasis to obesity using same-gender siblings as
controls for obesity. Clin Exp Dermatol 2008;34:140-4.
14. Prevalence of overweight and obesity among adults:
United States, 1999-2002 Hyattsville (MD): National Center
for Health Statistics 01/11/2007. Available from:
http://www.cdc.gov/nchs/products/pubs/pubd/hestats/obese/
obse99.htm. Accessed August 5, 2009.
15. Raychaudhuri SP, Farber EM. The prevalence of psoriasis in the
world. J Eur Acad Dermatol Venereol 2001;15:16-7.
16. Shekelle PG, Woolf SH, Eccles M, Grimshaw J. Clinical guide-
lines: developing guidelines. BMJ 1999;318:593-6.
17. Gottlieb AB, Evans R, Li S, Dooley LT, Guzzo CA, Baker D, et al.
Infliximab induction therapy for patients with severe plaque-
type psoriasis: a randomized, double-blind, placebo-controlled
trial. J Am Acad Dermatol 2004;51:534-42.
18. Reich K, Nestle FO, Papp K, Ortonne JP, Evans R, Guzzo C, et al.
Infliximab induction and maintenance therapy for moderate-
to-severe psoriasis: a phase III, multicentre, double-blind trial.
Lancet 2005;366:1367-74.
19. Menter A, Feldman SR, Weinstein GD, Papp K, Evans R, Guzzo
C, et al. A randomized comparison of continuous vs. intermit-
tent infliximab maintenance regimens over 1 year in the
treatment of moderate-to-severe plaque psoriasis. J Am Acad
Dermatol 2007;56(13):31.e1-15. Epub 2006 Sep 6.
20. Reich K, Gottlieb AB, Kimball A, Li S. Consistency of infliximab
response across subgroups of patients with psoriasis: inte-
grated results from randomized clinical trials. J Am Acad
Dermatol 2006;54(Suppl 1):AB215.
21. Menter A, Tyring SK, Gordon K, Kimball AB, Leonardi CL,
Langley RG, et al. Adalimumab therapy for moderate to severe
psoriasis: a randomized, controlled phase III trial. J Am Acad
Dermatol 2008;58:106-15.
22. Papp KA, Langley RG, Lebwohl M, Krueger GG, Szapary P,
Yeilding N, et al. Efficacy and safety of ustekinumab, a human
interleukin-12/23 monoclonal antibody, in patients with pso-
riasis: 52-week results from a randomised, double-blind, pla-
cebo-controlled trial (PHOENIX 2). Lancet 2008;371:1675-84.
23. Gordon K, Korman N, Frankel E, Wang H, Jahreis A, Zitnik R,
et al. Efficacy of etanercept in an integrated multistudy
database of patients with psoriasis. J Am Acad Dermatol
2006;54:S101-11.
24. Strober B, Gottlieb A, Leonardi C, Papp K. Levels of response of
psoriasis patients with different baseline characteristics trea-
ted with etanercept. J Am Acad Dermatol 2006;54(3, Suppl. 1):
AB220.
25. Gottlieb AB, Boehncke WH, Darif M. Safety and efficacy of
alefacept in elderly patients and other special populations. J
Drugs Dermatol 2005;4:718-24.
26. Gollnick H, Bauer R, Brindley C, Orfanos CE, Plewig G, Wokalek
H, Hoting E. Acitretin versus etretinate in psoriasis: clinical and
pharmacokinetic results of a German multicenter study. J Am
Acad Dermatol 1988;19:458-68.
27. Yamauchi PS, Rizk D, Kormeili T, Patnaik R, Lowe NJ. In:
Weinstein GD, editor. Therapy of moderate to severe psoriasis.
New York: Marcel Dekker; 2003. pp. 137-50.
28. Brick JE, Moreland LW, Al-Kawas F, Chang WW, Layne RD, Di
Bartolomeo AG. Prospective analysis of liver biopsies before
and after methotrexate therapy in rheumatoid patients. Semin
Arthritis Rheum 1989;19:31-44.
29. Langman G, Hall PM, Todd G. Role of non-alcoholic steatohe-
patitis in methotrexate-induced liver injury. J Gastroenterol
Hepatol 2001;16:1395-401.
30. Newman M, Auerbach R, Feiner H, Holzman RS, Shupack J,
Migdal P, et al. The role of liver biopsies in psoriatic patients
receiving long-term methotrexate treatment. Improvement in
liver abnormalities after cessation of treatment. Arch Dermatol
1989;125:1218-24.
31. Weinstein G, Roenigk H, Maibach H, Cosmides J, Halprin K,
Millard M. Psoriasis-liver-methotrexate interactions. Arch Der-
matol 1973;108:36-42.
32. Berends MA, Snoek J, de Jong EM, van de Kerkhof PC, van
Oijen MG, van Krieken JH, et al. Liver injury in long-term
methotrexate treatment in psoriasis is relatively infrequent.
Aliment Pharmacol Ther 2006;24:805-11.
33. Roenigk HH Jr, Bergfeld WF, St Jacques R, Owens FJ, Hawk WA.
Hepatotoxicity of methotrexate in the treatment of psoriasis.
Arch Dermatol 1971;103:250-61.
34. Rosenberg P, Urwitz H, Johannesson A, Ros AM, Lindholm J,
Kinnman N, et al. Psoriasis patients with diabetes type 2 are at
high risk of developing liver fibrosis during methotrexate
treatment. J Hepatol 2007;46:1111-8.
35. Zachariae H. Liver biopsies and methotrexate: a time for
reconsideration? J Am Acad Dermatol 2000;42:531-4.
36. Shibata N, Hayakawa T, Hoshino N, Minouchi T, Yamaji A,
Uehara M. Effect of obesity on cyclosporine trough concen-
trations in psoriasis patients. Am J Health Syst Pharm 1998;55:
1598-602.
ARTICLE IN PRESS
J AM ACAD DERMATOL Bremmer et al 11
37. Gisondi P, Del Gigio M, Di Francesco V, Zamboni M, Girolomoni
G. Weight loss improves the response of obese patients with
moderate-to-severe chronic plaque psoriasis to low-dose cy-
closporine therapy: a randomized, controlled, investigator-
blinded clinical trial. Am J Clin Nutr 2008;88:1242-7.
38. Mallbris L, Granath F, Hamsten A, Stahle M. Psoriasis is
associated with lipid abnormalities at the onset of skin
disease. J Am Acad Dermatol 2006;54:614-21.
39. Zamboni S, Zanetti G, Grosso G, Ambrosio GB, Gozzetti S,
Peserico A. Dietary behaviour in psoriatic patients. Acta Derm
Venereol Suppl (Stockh) 1989;146:182-3.
40. Simons RD. Additional studies on psoriasis in the tropics and
in starvation camps. J Invest Dermatol 1949;12:285-94.
41. Rucevic I, Perl A, Barisic-Drusko V, Adam-Perl M. The role of the
low energy diet in psoriasis vulgaris treatment. Coll Antropol
2003;27(Suppl. 1):41-8.
42. Porres JM. Jejunoileal bypass and psoriasis. Arch Dermatol
1977;113:983.
43. de Menezes Ettinger JE, Azaro E, de Souza CA, dos Santos
Filho PV, Mello CA, Neves M Jr, et al. Remission of psoriasis
after open gastric bypass. Obes Surg 2006;16:94-7.
44. Higa-Sansone G, Szomstein S, Soto F, Brasecsco O, Cohen C,
Rosenthal RJ. Psoriasis remission after laparoscopic roux-
en-Y gastric bypass for morbid obesity. Obes Surg 2004;14:
1132-4.
45. Setty AR, Curhan G, Choi HK. Obesity, waist circumference,
weight change, and the risk of psoriasis in women: Nurses
Health Study II. Arch Intern Med 2007;167:1670-5.
46. Hotamisligil GS, Shargill NS, Spiegelman BM. Adipose expres-
sion of tumor necrosis factor-alpha: direct role in obesity-
linked insulin resistance. Science 1993;259:87-91.
47. Kern PA, Saghizadeh M, Ong JM, Bosch RJ, Deem R, Simsolo
RB. The expression of tumor necrosis factor in human adipose
tissue. regulation by obesity, weight loss, and relationship to
lipoprotein lipase. J Clin Invest 1995;95:2111-9.
48. Hotamisligil GS, Arner P, Caro JF, Atkinson RL, Spiegelman BM.
Increased adipose tissue expression of tumor necrosis factor-
alpha in human obesity and insulin resistance. J Clin Invest
1995;95:2409-15.
49. Dandona P, Weinstock R, Thusu K, Abdel-Rahman E, Aljada A,
Wadden T. Tumor necrosis factor-alpha in sera of obese
patients: fall with weight loss. J Clin Endocrinol Metab 1998;
83:2907-10.
50. Hauner H, Bender M, Haastert B, Hube F. Plasma concentra-
tions of soluble TNF-alpha receptors in obese subjects. Int J
Obes Relat Metab Disord 1998;22:1239-43.
51. Hotamisligil GS, Peraldi P, Budavari A, Ellis R, White MF,
Spiegelman BM. IRS-1-mediated inhibition of insulin receptor
tyrosine kinase activity in TNF-alpha- and obesity-induced
insulin resistance. Science 1996;271:665-8.
52. Hotamisligil GS, Spiegelman BM. Tumor necrosis factor alpha:
a key component of the obesity-diabetes link. Diabetes 1994;
43:1271-8.
53. Lang CH, Dobrescu C, Bagby GJ. Tumor necrosis factor impairs
insulin action on peripheral glucose disposal and hepatic
glucose output. Endocrinology 1992;130:43-52.
54. Eckel RH. Insulin resistance: an adaptation for weight mainte-
nance. Lancet 1992;340:1452-3.
55. Dominguez H, Storgaard H, Rask-Madsen C, Steffen Hermann
T, Ihlemann N, Baunbjerg Nielsen D, et al. Metabolic and
vascular effects of tumor necrosis factor-alpha blockade with
etanercept in obese patients with type 2 diabetes. J Vasc Res
2005;42:517-25.
56. Johnston A, Arnadottir S, Gudjonsson JE, Aphale A, Sigmars-
dottir AA, Gunnarsson SI, et al. Obesity in psoriasis: leptin and
resistin as mediators of cutaneous inflammation. Br J Dermatol
2008;159:342-50.
57. Kaur S, Zilmer K, Kairane C, Kals M, Zilmer M. Clear differences
in adiponectin level and glutathione redox status revealed in
obese and normal-weight patients with psoriasis. Br J Derma-
tol 2008;159:1364-7. Epub 2008 Jul 22.
58. Vanizor Kural B, Orem A, Cimsit G, Yandi YE, Calapoglu M.
Evaluation of the atherogenic tendency of lipids and lipopro-
tein content and their relationships with oxidant-antioxidant
system in patients with psoriasis. Clin Chim Acta 2003;328:71-
82.
59. Rocha-Pereira P, Santos-Silva A, Rebelo I, Figueiredo A,
Quintanilha A, Teixeira F. Dislipidemia and oxidative stress in
mild and in severe psoriasis as a risk for cardiovascular disease.
Clin Chim Acta 2001;303:33-9.
60. Seishima M, Seishima M, Mori S, Noma A. Serum lipid and
apolipoprotein levels in patients with psoriasis. Br J Dermatol
1994;130:738-42.
61. Zheng L, Nukuna B, Brennan ML, Sun M, Goormastic M, Settle M,
et al. Apolipoprotein A-I is a selective target for myeloperoxi-
dase-catalyzed oxidation and functional impairment in subjects
with cardiovascular disease. J Clin Invest 2004;114:529-41.
62. National Cholesterol Education Program (NCEP) Expert Panel
on Detection, Evaluation, and Treatment of High Blood
Cholesterol in Adults (Adult Treatment Panel III). National
Cholesterol Education Program (NCEP) Expert Panel on De-
tection, Evaluation, and Treatment of High Blood Cholesterol
in Adults (Adult Treatment Panel III) final report. Circulation
2002;106:3143e3421.
63. Gisondi P, Tessari G, Conti A, Piaserico S, Schianchi S, Peserico
A, et al. Prevalence of metabolic syndrome in patients with
psoriasis: a hospital-based case-control study. Br J Dermatol
2007;157:68-73.
64. Boehncke S, Thaci D, Beschmann H, Ludwig RJ, Ackermann H,
Badenhoop K, et al. Psoriasis patients show signs of insulin
resistance. Br J Dermatol 2007;157:1249-51.
65. Ena P, Madeddu P, Glorioso N, Cerimele D, Rappelli A. High
prevalence of cardiovascular diseases and enhanced activity of
the renin-angiotensin system in psoriatic patients. Acta
Cardiol 1985;40:199-205.
66. Qureshi AA, Choi HK, Setty AR, Curhan GC. Psoriasis and the
risk of diabetes and hypertension. Arch Dermatol 2009;145:
379-82.
67. Shapiro J, Cohen AD, David M, Hodak E, Chodik G, Viner A,
et al. The association between psoriasis, diabetes mellitus, and
atherosclerosis in Israel: a case-control study. J Am Acad
Dermatol 2007;56:629-34.
68. Binazzi M, Calandra P, Lisi P. Statistical association between
psoriasis and diabetes: further results. Arch Dermatol Res
1975;254:43-8.
69. Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel
AB. Risk of myocardial infarction in patients with psoriasis.
JAMA 2006;296:1735-41.
70. Reynoso-von Drateln C, Martinez-Abundis E, Balcazar-Munoz
BR, Bustos-Saldana R, Gonzalez-Ortiz M. Lipid profile, insulin
secretion, and insulin sensitivity in psoriasis. J Am Acad
Dermatol 2003;48:882-5.
71. Lord GM, Matarese G, Howard JK, Baker RJ, Bloom SR, Lechler
RI. Leptin modulates the T-cell immune response and reverses
starvation-induced immunosuppression. Nature 1998;394:897-
901.
72. Kirchgessner TG, Uysal KT, Wiesbrock SM, Marino MW,
Hotamisligil GS. Tumor necrosis factor-alpha contributes to
obesity-related hyperleptinemia by regulating leptin release
from adipocytes. J Clin Invest 1997;100:2777-82.

ARTICLE IN PRESS
J AM ACAD DERMATOL12 Bremmer et al
73. Grunfeld C, Zhao C, Fuller J, Pollack A, Moser A, Friedman J,
et al. Endotoxin and cytokines induce expression of leptin,
the ob gene product, in hamsters. J Clin Invest 1996;97:
2152-7.
74. Farooqi IS, Matarese G, Lord GM, Keogh JM, Lawrence E, Agwu C,
et al. Beneficial effects of leptin on obesity, T cell hyporesponsive-
ness, and neuroendocrine/metabolic dysfunction of human
congenital leptin deficiency. J Clin Invest 2002;110:1093-103.
75. McTernan CL, McTernan PG, Harte AL, Levick PL, Barnett AH,
Kumar S. Resistin, central obesity, and type 2 diabetes. Lancet
2002;359:46-7.
76. Ouchi N, Kihara S, Arita Y, Maeda K, Kuriyama H, Okamoto Y,
et al. Novel modulator for endothelial adhesion molecules:
adipocyte-derived plasma protein adiponectin. Circulation
1999;100:2473-6.
77. Yang WS, Lee WJ, Funahashi T, Tanaka S, Matsuzawa Y, Chao
CL, et al. Weight reduction increases plasma levels of an
adipose-derived anti-inflammatory protein, adiponectin. J Clin
Endocrinol Metab 2001;86:3815-9.
78. Naldi L, Addis A, Chimenti S, Giannetti A, Picardo M, Tomino C,
et al. Impact of body mass index and obesity on clinical
response to systemic treatment for psoriasis. Dermatology
2008;217:365-73.
79. Clark L, Lebwohl M. The effect of weight on the efficacy of
biologic therapy in patients with psoriasis. J Am Acad
Dermatol 2008;58:443-6.
80. Fitch E, Harper E, Skorcheva I, Kurtz SE, Blauvelt A. Patho-
physiology of psoriasis: recent advances on IL-23 and Th17
cytokines. Curr Rheumatol Rep 2007;9:461-7.
81. Friedewald VE, Cather JC, Gelfand JM, Gordon KB, Gibbons
GH, Grundy SM, et al. AJC editor’s consensus: psoriasis
and coronary artery disease. Am J Cardiol 2008;102:1631-
43.
82. Gelfand JM, Dommasch ED, Shin DB, Azfar RS, Kurd SK, Wang
X, Troxel AB. The risk of stroke in patients with psoriasis. J
Invest Dermatol 2009;129:2327.
83. Prodanovich S, Ma F, Taylor JR, Pezon C, Fasihi T, Kirsner RS.
Methotrexate reduces incidence of vascular diseases in vet-
erans with psoriasis or rheumatoid arthritis. J Am Acad
Dermatol 2005;52:262-7.
84. Roenigk HH Jr, Auerbach R, Maibach HI, Weinstein GD.
Methotrexate guidelines—revised. J Am Acad Dermatol
1982;6:145-55.
85. Griffiths CE, Dubertret L, Ellis CN, Finlay AY, Finzi AF, Ho VC,
et al. Ciclosporin in psoriasis clinical practice: an interna-
tional consensus statement. Br J Dermatol 2004;150(Suppl
67):11-23.
86. Gisondi P, Cotena C, Tessari G, Girolomoni G. Anti-tumour
necrosis factor-alpha therapy increases body weight in pa-
tients with chronic plaque psoriasis: a retrospective cohort
study. J Eur Acad Dermatol Venereol 2008;22:341-4.
87. Saraceno R, Schipani C, Mazzotta A, Esposito M, Di Renzo L, De
Lorenzo A, Chimenti S. Effect of anti-tumor necrosis factor-
alpha therapies on body mass index in patients with psoriasis.
Pharmacol Res 2008;57:290-5.
88. Irace C, Mancuso G, Fiaschi E, Madia A, Sesti G, Gnasso A. Effect
of anti TNF-alpha therapy on arterial diameter and wall shear
stress and HDL cholesterol. Atherosclerosis 2004;177:113-8.
89. Vis M, Nurmohamed MT, Wolbink G, Voskuyl AE, de Koning
MHMT, van de Stadt RJ, et al. Short term effects of infliximab
on the lipid profile in patients with rheumatoid arthritis. J
Rheumatol 2005;32:252-5.