feasibility of bremsstrahlung dosimetry for direct dose estimation in patients undergoing treatment...
TRANSCRIPT
ORIGINAL ARTICLE
Feasibility of bremsstrahlung dosimetry for direct doseestimation in patients undergoing treatmentwith 90Y-ibritumomab tiuxetan
C. Arrichiello & L. Aloj & M. Mormile & L. D’Ambrosio &
F. Frigeri & C. Caracò & M. Arcamone & F. De Martinis &
A. Pinto & S. Lastoria
Received: 13 July 2011 /Accepted: 13 December 2011# Springer-Verlag 2012
AbstractPurpose Radioimmunotherapy with 90Y-ibritumomab tiuxe-tan has been used successfully used in the treatment ofCD20-positive non-Hodgkin’s lymphoma (NHL). Pretherapyimaging with 111In-ibritumomab tiuxetan has been used inprovisional dosimetry studies. Posttherapy imaging of 90Y-ibritumomab tiuxetan for clinical use is appealing as it wouldsimplify the data acquisition process and allow measurementsof actual doses absorbed during treatment.Methods The study included 29 patients with non-Hodgkin’slymphoma, of whom 16 (group I) received a pretherapy 111In-ibritumomab tiuxetan diagnostic study and 90Y-ibritumomabtiuxetan treatment 1 week later, and 13 (group II) receivedonly 90Y-ibritumomab tiuxetan treatment. Planar imaging andblood sampling were performed in all patients. The dosesabsorbed by organs at risk were calculated using a whole-
body average attenuation correction factor (relative dosimetryapproach) and, in the case of the 111In-ibritumomab tiuxetanimage sets, also using organ-specific attenuation correctionfactors (absolute dosimetry method). Red marrow absorbeddoses were based on gamma counting of blood samples.Results The estimated red marrow absorbed doses from111In and 90Y data were equivalent. In all cases, the dosesabsorbed by organs at risk were found to be within prescribedlimits. The relative dosimetry approach applied to both the90Y and 111In data significantly underestimated the dosesrelative to those obtained with the 111In absolute dosimetrymethod which is generally accepted as the reference method(MIRD 16). In the case of 111In, the relative dosimetryapproach values were highly correlated (R200.61) with thereference method values. Relative dosimetry estimates maybe adjusted multiplying by a correction factor of 2.8. The90Y-ibritumomab tiuxetan relative dosimetry data correlatedpoorly with the reference method values (R200.02).Conclusion Based on patient-specific dosimetry, the adminis-tered activity may be increased by an average factor of 2.4,indicating that most patients could be undertreated. The relativedosimetry approach based on planar imaging largelyunderestimates doses relative to reference values. Dosimetrybased on planar bremsstrahlung imaging is not a dependablealternative to 111In dosimetry.
Keywords Radioimmunotherapy . Ibritumomab tiuxetan .
Non-Hodgkin’s lymphoma . Dosimetry . Bremsstrahlungimaging
Introduction
Radioimmunotherapy (RIT) with 90Y-ibritumomab tiuxetan(Zevalin, Bayer Schering) combines the targeting properties
C. Arrichiello : L. Aloj :M. Mormile : L. D’Ambrosio :C. Caracò : F. De Martinis : S. LastoriaNuclear Medicine Department,Istituto Nazionale per lo Studio e la Cura dei Tumori,Fondazione “G. Pascale”,Napoli, Italy
C. Arrichielloe-mail: [email protected]
F. Frigeri :M. Arcamone :A. PintoHematology-Oncology and Stem Cells Transplantation Unit,Department of Hematology,Istituto Nazionale per lo Studio e la Cura dei Tumori,Fondazione “G. Pascale”,Napoli, Italy
S. Lastoria (*)IRCCS, Istituto Nazionale per lo Studio e la Cura dei Tumori,Fondazione “G. Pascale”,Via M. Semmola,80131 Napoli, Italye-mail: [email protected]
Eur J Nucl Med Mol ImagingDOI 10.1007/s00259-011-2040-5

of the ibritumomab monoclonal antibody against theCD20 antigen with the proven high radiosensitivity ofnon-Hodgkin's lymphoma (NHL) cells [1]. There isstrong preclinical evidence for the use of this approach[2]. RIT with 90Y-ibritumomab tiuxetan has been validated ina number of studies that have shown clinical efficacy [3–7].Aside from current indications for clinical use in follicular celllymphoma or transformed B-cell NHL (only in theUnited States) [8–11], this treatment is currently beingevaluated for other applications, including earlier use inthe treatment algorithm (i.e. upfront treatment in follic-ular lymphoma, as consolidation after chemotherapy orat the time of first relapse), in aggressive lymphomasubtypes (including diffuse large B-cell lymphoma ormantle-cell lymphoma), as part of the conditioning treatmentin myeloablative regimens prior to autologous stem cell trans-plantation, repeated cycles in the same patient for curativepurposes, and using higher administered activity (high-doseRIT) [12, 13].
This expanded scenario warrants the development ofaccurate and preferably straightforward methods to assessthe doses absorbed by organs at risk (OARs) including theheart, spleen, liver, lungs, kidneys and red marrow (RM).Dosimetry for OARs has been defined in preliminary studiesperformed during the process of clinical approval of the druginvolving the pretreatment 111In-ibritumomab tiuxetanimaging 1 week prior to RIT (pre-RIT dosimetry).These dosimetry studies were based on the assumptionthat the biodistribution kinetics of 111In-ibritumomabtiuxetan and 90Y-ibritumomab tiuxetan are superimposable.111In-ibritumomab tiuxetan imaging prior to 90Y-ibritumomabtiuxetan RIT, while mandatory in the US where it is used todetermine if there is adequate biodistribution and whetherpatients are eligible for treatment [14], is not required in mostcountries in Europe. The rationale behind not performing suchpretherapy imaging is that doses to OARs during therapy,based on historical data, never exceed accepted thresholdvalues (<2 Gy for RM and <20 Gy for all other organs) [15],and the current approved treatment schedule is considered safe[16].
Although pre-RIT dosimetry is currently considered thegold standard method for accurate dosimetry estimates for90Y-ibritumomab tiuxetan RIT, direct dosimetry estimatesbased on bremsstrahlung emission from 90Y-ibritumomabtiuxetan (post-RIT dosimetry) through nuclear imaging isappealing. The implementation of post-RIT dosimetrywould allow OAR absorbed dose data to be recorded inpatients undergoing treatment in countries where the pretreat-ment 111In-ibritumomab tiuxetan study is neither required norapproved. Furthermore, regardless of the regulatory environ-ment, it would appear reasonable to obtain adequate imaginginformation following 90Y-ibritumomab tiuxetan infusion as away to verify distribution and dosimetry. There are some
further arguments in favour of post-RIT dosimetry. Thechemical properties of 90Y and 111In are similar but notidentical [17]. The behaviours of free 90Y and free 111Inare different. Both free radionuclides may be releasedfrom radiolabelled ibritumomab tiuxetan preparationsafter injection. Free 111In has been shown to bind toother, circulating, proteins such as transferrin, and free90Y concentrates in the bone so that there may becomplications in accurately estimating RM dose. Indeed,there are reports of a lack of correlation between theRM doses estimated with 111In-ibritumomab tiuxetanand bone marrow toxicity [18], and differences in thepharmacokinetics of the two radiopharmaceuticals havebeen suggested [19]. Conversely, preclinical data inanimals shows very similar biodistribution properties of90Y- and 111In-ibritumomab tiuxetan as well as high invitro stability of both conjugates [2]. Another issue isthe different timing of the injection protocol for the twocompounds. The 90Y-ibritumomab tiuxetan RIT protocolcalls for two injections of rituximab (250 mg/m2), thefirst administered 7 days prior to treatment and thesecond immediately before the administration of thetherapeutic dose. 111In-Ibritumomab tiuxetan dosimetryis performed at the time of the first administration of rituximab.Since rituximab has known therapeutic effects at doses as lowas 250 mg/m2, there may be changes in the biodistributionbetween the two studies caused by such therapeutic effects,including possible variations in tumour size. This impliesthat pre-RIT dosimetry may not accurately assess dosesto OARs in the treatment phase under certain clinicalconditions.
Dose estimation can be performed with either planar orSPECT acquisitions. Dosimetry performed with SPECTshould be preferred since it is more accurate than planarimaging [19]. This holds particularly true for SPECT/CT,where more precise corrections for attenuation and scattercan be performed. The drawbacks of using SPECT, however,are that longer acquisition times are necessary and, forSPECT/CT, a hybrid system must be available. Whole0bodygamma camera imaging on the other hand is more rapid andcan be performed in any nuclear medicine department. A fewwhole-body images obtained in the days following adminis-tration of therapy can be sufficient to provide dosimetrymeasurements. In the present work we compared the imaging,biodistribution and dosimetry estimates obtained by planarimaging of 111In-ibritumomab tiuxetan and 90Y-ibritumomabtiuxetan. We analysed two groups of patients. In onegroup of patients both 111In and the 90Y imaging studieswere performed and in the other group only the post-RITdosimetric imaging study was performed. Our goal wasto assess the feasibility of obtaining suitable estimates oforgan absorbed doses through assessment of post-RITdosimetry.
Eur J Nucl Med Mol Imaging

Material and methods
Patient selection
Enrolled in the study were 29 patients with NHL. All hadhistologically proven CD20-positive G1/G2 follicular celllymphoma requiring therapy, were over 18 years of age andshowed adequate vital functions. Disease burden wasassessed in each patient by whole-body 18F-FDG PET/CTwith and without contrast enhancement. Particular emphasiswas placed on the evaluation of extranodal and splenicinvolvement. Ten patients received 90Y-ibritumomab tiuxetanas up-front therapy, while the remaining 19 underwentstandard "on-label" treatment according to current eligibilitycriteria in our country.
Eligibility
Patients needed to fulfil the following requirements beforereceiving RIT with 90Y-ibritumomab tiuxetan: bone marrowinfiltration by lymphoma cells <25%, platelet count>100,000 μl−1 and neutrophil count >1,500 μl−1, and no priorexternal beam radiation therapy involving >25% of the bonemarrow. Myelotoxicity has been found to be the dose-limiting factor and the standard administered dose is15 MBq/kg with a maximum administrable dose of1,184 MBq. The treatment schedule included intravenousinfusion of rituximab at a dose of 250 mg/m2 on days 1and 8. Rituximab pretreatment was administered using alower dosage than commonly adopted for therapeuticpurposes to reduce the binding of 90Y-ibritumomab tiuxetanto CD20-positive B cells present in the blood and the spleen[20], and to improve targeting of 90Y-ibritumomab tiuxetan totumour-containing areas by saturating antigen sites of normalorgans [1].
Radiolabelling
111In-Ibritumomab tiuxetan was labelled according to a pre-viously described procedure [21]. 90Y-Ibritumomab tiuxetanlabelling and quality control for both radiopharmaceuticalswas performed according to the manufacturer’s procedureon the package insert. Radiochemical purity higher than95% was required for administration.
Study design
In 16 patients (group I) image sets and blood samples wereobtained following 111In-ibritumomab tiuxetan administrationand following the 90Y-ibritumomab tiuxetan administration.Dosimetric calculations with the two datasets were evaluatedfor correlation between the pre- and post-RIT OAR dosimetryresults. The other 13 patients (group II) only received 90Y-
ibritumomab tiuxetan, and only the post-RIT dosimetriccalculations were performed. The two groups of patients(with and without 111In-ibritumomab tiuxetan administration)were compared to determine the feasibility of stand-alonepost-RIT dosimetry. The MIRD scheme was used to evaluatedoses to OARs after administration of either compound (111In-ibritumomab tiuxetan or 90Y-ibritumomab tiuxetan).
Pre-RIT dosimetry
Patients having pre-RIT dosimetry were injected withabout 185 MBq of 111In-ibritumomab tiuxetan immediatelyfollowing the first rituximab injection (day 1). After 111In-ibritumomab tiuxetan administration (pre-RIT dosimetry)blood samples were collected and whole-body images ac-quired at fixed time-points: 30 min, 3 h, 18 h, 90 h, 160 h.The pre-RIT dosimetric estimates were based on the distribu-tion kinetics of 111In-ibritumomab tiuxetan correcting the datafor differences between the half-lives of 90Y and 111In, using
the factor eðl111In�l90YÞt , where l represents the decay constant.RM doses were estimated from blood samples. A
known volume of blood was diluted to a fixed volume(5 ml) with normal saline, and an activity standard wasmeasured to obtain a gamma counter counts/activityconversion factor. Activity was measured with a Wizard1480 gamma counter (Wallac, Turku, Finland) using thefactory preset energy window for 111In. The residencetime in blood (tBL) was obtained by biexponential fitting
y ¼ A1e� x
t1 þ A2e� x
t2 þ y0; y0 ¼ 0� �
of the experimental data
using Origin 7.0 (OriginLab, Northampton, MA) and calcu-lated using the equation tBL ¼ A1 � t1 þ A2 � t2 . The RMresidence time (tRM), based on the Sgouros method [22], islinearly correlated with the residence time in blood (tBL),according to the formula: tRM ¼ RMECFF
1�HCT tBLVRMð Þ; whereRMECFF is the RM extracellular fluid (assumed to be0.19), VRM is the RM volume (assumed to be 1,120 mlfor men and 1,050 ml for women, and HCT is thehaematocrit. Doses were estimated using the MIRD
formula: DRM ¼ A90Yinj tRMSRM RM; using Snyder (S) factors
provided by OLINDA/EXM [23], respectively for male orfemale adult phantoms adjusted for patient weight. Only theself-absorption component was taken into account.
Reference measurements of the doses to the remainingnormal OARs (heart, liver, lungs, spleen and kidneys) wereobtained with the absolute dosimetry approach in whichattenuation-corrected 111In-ibritumomab tiuxetan biodistri-bution data were analysed. Each patient had a transmissionscan with a 57Co flood source performed prior to the 111In-ibritumomab tiuxetan injection. All had current CT dataavailable in order to define organ volumes and relativemasses. Serial whole-body scans were acquired on an E.cam dual head gamma camera system (Siemens, Erlangen,
Eur J Nucl Med Mol Imaging

Germany) with the following acquisition parameters: scanspeed 10 cm/min, energy window 173 and 247 keV±15%peak [24], medium energy collimators, and acquisitionmatrix size 256 × 1024. OAR doses were obtained byregion of interest (ROI) analysis as previously described[15] using the geometric mean (GM) of the anterior andposterior ROI counts. ROIs were drawn on imagesacquired 18 h after injection and subsequently trans-ferred to all the other images acquired. The softwareOSIRIX [25] was utilized for ROI definition and analysis.OAR residence times (t) were estimated directly from GMj(t)of counts in conjugated images (absolute dosimetry approach)according to the equation:
t Abs ¼RGMjðtÞ � ACFf � eðl
111In�tÞ � e�ðl90Y �tÞ � dtA
111Ininj
;
where attenuation correction factors (ACFs) were derivedfrom the 57Co transmission scans as illustrated in the MIRD20 pamphlet [26], μ57Co (0.1066 cm−1) was determined ex-perimentally from 57Co transmission scans of watercolumns of different thickness, while μ111In (0.1206 cm−1)and the system calibration factor (f06.69 cpm/kBq) wereestimated using a spherical 111In activity source placed atdifferent water depths. The activity in the whole body wasexpressed as the percentage relative to the first image ac-
quired, according to the equation: AwbðtÞAwbð0Þ ¼
GMwbðtÞGMwbð0Þ . A time-
percentage activity curve was constructed assuming monoex-
ponential decay y ¼ A1e� x
t1 þ y0; y0 ¼ 0� �
and estimated
using the equation t ¼ A1 � t1 , where A1 and t1 were obtainedusing Origin 7.0. All the OAR residence times were analysedwith OLINDA/EXM [27]. Organ dose estimates were cor-rected for patient weight and individual organ mass deter-mined by CT. Both self-absorption and external organ dosecontributions were taken into account.
Post-RIT dosimetry
The time-course of 90Y-ibritumomab tiuxetan biodistribu-tion was evaluated directly by measuring bremsstrahlungradiation for all OARs at each time-point. Image and blooddata were collected at 30 min, 3 h, 6 h, 18 h and 90 h afterinjection. RM dosimetry was performed using the samemethod described for pre-RIT with the exception of thegamma counter energy window that was set to 15–2,000 keV for 90Y. For OAR dosimetry, serial whole-bodyscans were acquired with the same parameters used foracquiring 111In images, with exception of the energy win-dow that was set to 50–300 keV. These settings have beenused previously [17] and were selected so as to maximizesystem sensitivity, although they include a contaminationpeak due to the k absorption edge at 88 keV in the lead of the
collimator. In studies in which a matching pre-RIT datasetwas available, the same ROIs were used to analyse the 90Ydata, as the higher quality of the 111In-ibritumomab tiuxetanimages allowed better contouring of the organs. Thecontribution of activity to each ROI by residual 111Infrom the pre-RIT study was measured by performing abaseline (pre 90Y-ibritumomab tiuxetan injection) scan using90Y energy settings. OAR residence times (t) were estimatedbased on the assumption that total counts from the whole-bodyimage acquired immediately after 90Y-ibritumomab tiuxetaninjection, prior to bladder voiding, GMwb(0), were representa-tive of all administered activity Awb(0) (relative dosimetryapproach). The activity in each organ (j) was expressed as apercentage relative to the first image acquired, according to the
equation: Aj tð ÞAwb 0ð Þ ¼ GMj tð Þ
GMwb 0ð Þ ; and individual doses were calcu-
lated as described above. For patients undergoing only post-RIT dosimetry, ROIs were drawn on images acquired 18 hfollowing 90Y-ibritumomab tiuxetan administration and copiedto all other images, and doses were determined as describedwith the relative dosimetry approach.
Statistical analysis
Statistical analysis was performed using Wilcoxon’s signed-ranks test to compare paired data and the Mann-Whitney testto compare unpaired samples. Differences were consideredstatistically significant when the p values were <0.05.
Results
Pre-RIT dosimetry
111In-ibritumomab tiuxetan biodistribution was assessed in16 patients with follicular cell lymphoma (group I) in orderto define the individual reference estimates for doses toOARs. The serial whole-body images showed the expecteddistribution mainly in the blood pool on initial images withlater visibility of NHL lesions and decreased vascularactivity. Lesions identified on 18F-FDG PET imageswere indeed recognizable only on images acquired atdelayed times following injection (90 h), as shown inFig. 1. Mean estimated doses to OARs by pre-RIT dosimetrywere (mean±SD, range; gray; Fig. 2): heart 5.6±1.9, 2.2–10.7; liver 8.5±4.0, 4.5–19.2; lungs 4.4±2.1, 2.0–9.3; spleen6.9±1.9, 4.1–10.2; kidneys 6.8±3.4, 3.0–15.9; RM 0.56±0.17, 0.31–0.97; and whole body 0.90±0.12, 0.73–1.1.OAR dose estimates were compared to the relative dose limitsfor each patient to obtain the maximum administrable activity,defined as the highest activity allowing the absorbeddose to remain within the threshold values. Four patientsshowed spleen involvement by disease that was documented
Eur J Nucl Med Mol Imaging

on 18F-FDG PET. In one of these patients the estimated doseto the spleenwas 38Gy (Fig. 1). Since in such cases the spleen
must be considered a target organ, the data from these fourpatients were excluded from the OAR analysis. Dose-limiting
Fig. 1 Images of a group I patient. The PET 18F-FDG image ismaximum intensity projection of an18F-FDG PET/CT study performedprior to therapy showing multiple areas of nodal involvement andelevated spleen uptake consistent with presence of disease. The 57Coimage is a transmission scan performed with a 57Co flood source usedfor attenuation correction of the 111In studies. The 111In-ibritumomab
tiuxetan images are serial whole-body anterior images obtained from0.5 to 90 h after injection of 185 MBq 111In-ibritumomab tiuxetanshowing progressively decreasing blood pool activity and concomitantprogressive accumulation of the radiopharmaceutical in knownlocations of disease (arrows)
Fig. 2 RM and OARs pre-RITabsolute dosimetry and whole-body relative dosimetryestimates (D) for patientsundergoing 111In-ibritumomabtiuxetan (group I). The resultsobtained in 16 patients areshown (mean±SD). Theabsorbed dose estimates for thespleen are relative to 12 of 16patients (see text). The RMdose was 0.56±0.17 Gy and thewhole-body dose was0.90±0.12 Gy in this group
Eur J Nucl Med Mol Imaging

organs were identified based on the pre-RIT estimates: spleen(6 patients), liver (6 patients), kidneys (4 patients). There wereno patients in whom the dose limit was reached for any of theOARs not involved by disease. Dose estimates are presentedin Table 1.
Post-RIT dosimetry
Post-RIT dosimetry was performed in patients of group Iand II. The post-RIT serial whole-body scans performed ingroup I (Fig. 3a) showed a poor imaging resolution whencompared to the pre-RIT images. In several patients uptakein tumour lesions was already visible on the first imageobtained (t030 min), as shown in Fig. 3b. This finding, insharp contrast with those in the pre-RIT studies, wasattributed to residual 111In activity in patients of group Iat the time of the 90Y-ibritumomab tiuxetan injection.Furthermore, tumour lesions were poorly visible on thefirst image (t030 min) in group II, and appeared only inlater scans. Aiming to correct for residual 111In activity,a whole-body scan was performed using the energysettings for 90Y immediately prior to 90Y-ibritumomabtiuxetan administration (Fig. 3b). The 111In contributionfor each organ was found to be significant (of the orderof 25% of the total counts measured immediately following90Y-ibritumomab tiuxetan injection), and was thus subtracted.This correction was performed on ROI data from all90Y serial images assuming monoexponential decay ofthe 111In contribution based on the effective decay observed inthe pre-RIT study.
Pre-RIT dosimetry vs. post-RIT dosimetry
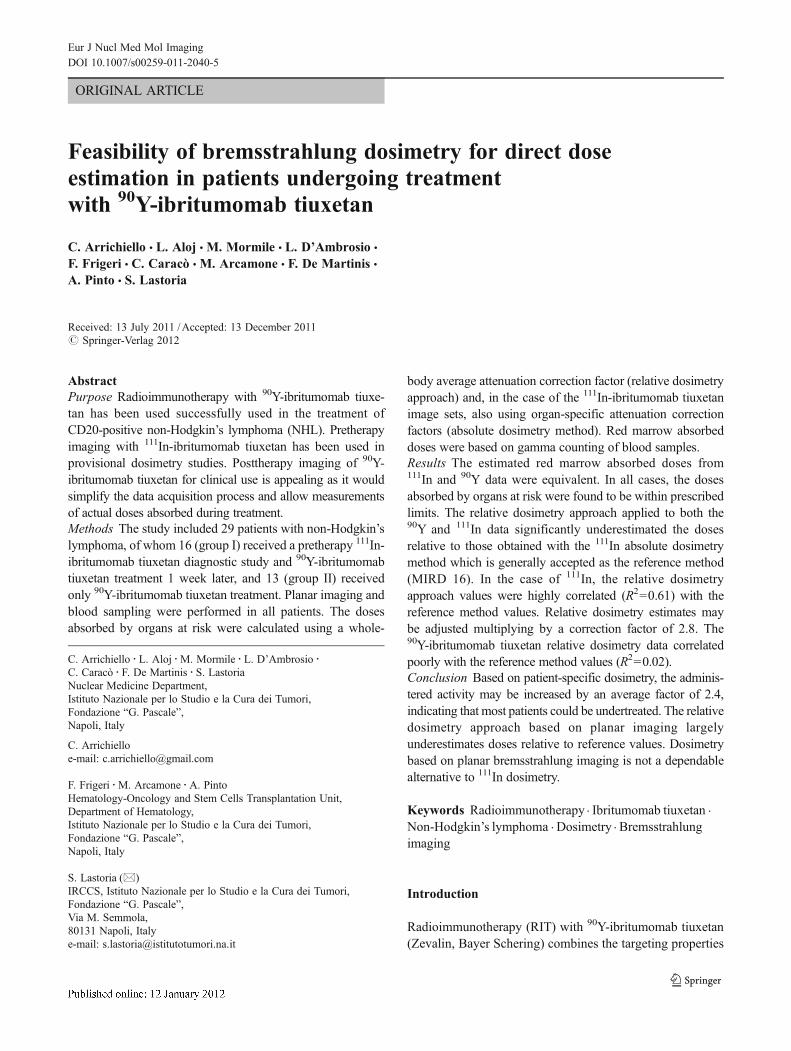
The generated clearance curves by pre- and post-RITdosimetry for the RM (Fig. 4) and whole-body weresuperimposable. For each of the remaining OARs, asystematic underestimation of the percentage of activityon the 90Y images was found, although the kineticsobserved were similar. The average doses to the OARsalong with the relative standard deviations estimated bythe two approaches were compared (Table 1) and, while
for the RM and whole-body, dose estimates were notsignificantly different (p>0.05), the post-RIT doses forthe remaining OARs were significantly underestimated(p<0.05, paired Wilcoxon signed-ranks test).
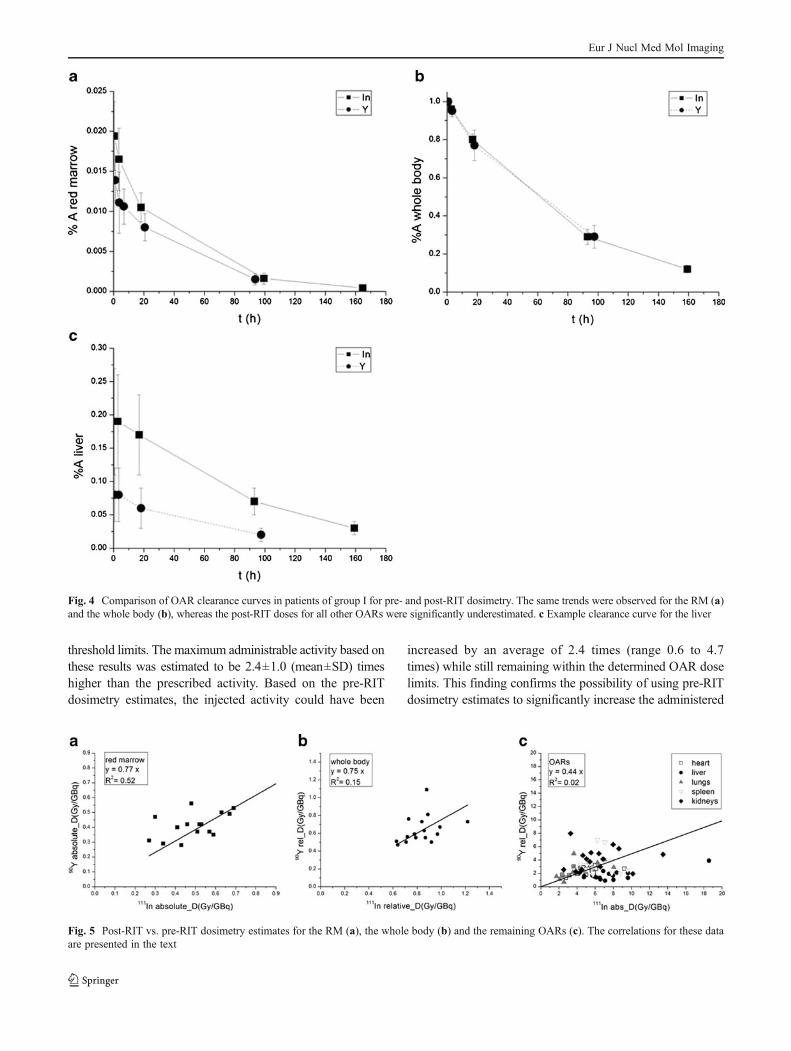
In order to correlate the results obtained in post-RITdosimetry with the pre-RIT gold standard results, OARdosimetry estimates for all individual organs (n092)analysed are presented in (x,y) diagrams (Fig. 5). Theline of best fit (y0A+Bx, assuming A00) for RM had aslope of 0.77±0.04 and a correlation coefficient R2 of0.52 (p00.0016; Fig. 5a), while the whole-body valueswere 0.75±0.05 and R200.15 (p00.167; Fig. 5b), andthe values for the remaining OARs were 0.44±0.03 and R200.02 (p<0.0001; Fig. 5c), the poor correlation coefficientreflecting the dispersion of the data observed.
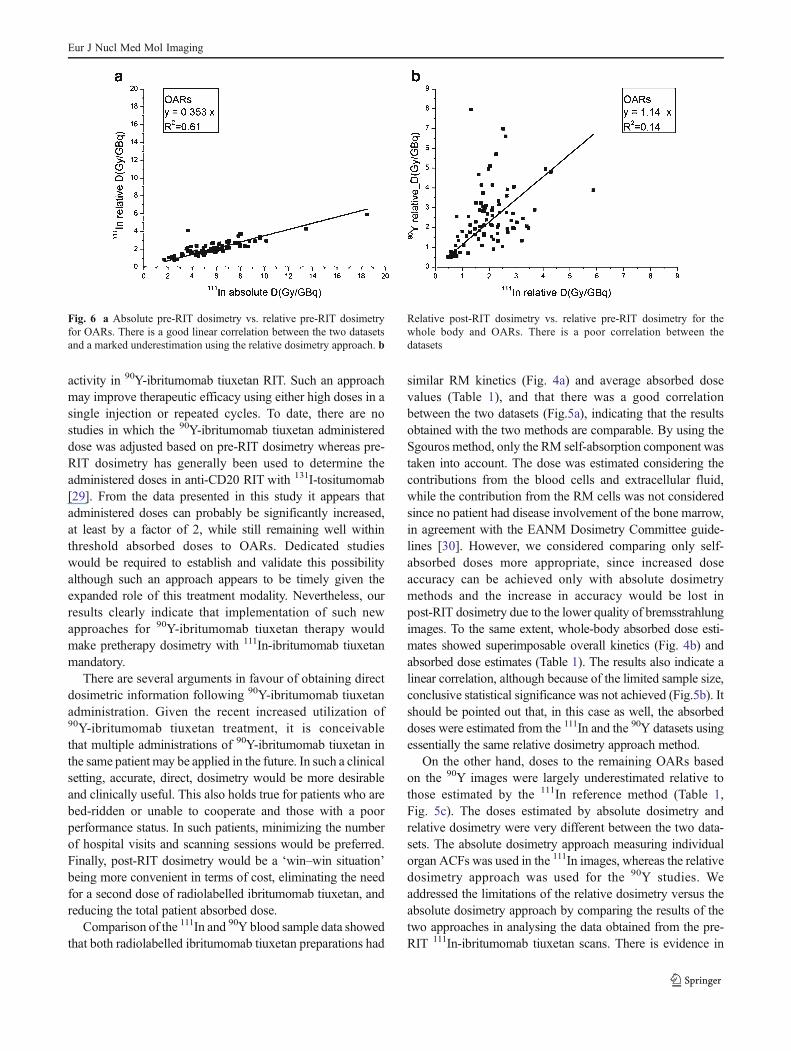
As the main technical limit of performing bremsstrahlungimaging dosimetry is the inability to obtain ACFs, wecompared the results of the pre-RIT 111In data analysedwith the reference absolute dosimetry method and thoseof the same data analysed with the relative dosimetryapproach, in which organ-specific attenuation correctionwas not taken into account. A linear correlation wasobserved between the estimates obtained with the twomethods (R200.61, p<0.0001, B00.353±0.009; Fig. 6a).The main observation in this comparison is that the relativedosimetry approach underestimated the doses relative to thereference data by a factor of 2.83. The 111In data analysed withthe relative dosimetry approach and the 90Y paired data werecompared in a similar manner to evaluate whether neglectingattenuation correction and absolute quantitation would yieldcomparable results between the two datasets. Again, there wasa poor linear correlation between the two datasets (R200.14,p<0.0001, B01.14±0.07, Fig. 6b).
In order to rule out errors in the post-RIT dosimetrymeasurements introduced by the corrections carried out forresidual 111In activity, we performed post-RIT dosimetry in13 patients undergoing 90Y-ibritumomab tiuxetan treatment.The results obtained in this population were compared to thesame data in group I patients. This comparison showed thataverage dose estimates to all OARs were not significantlydifferent between the two groups (Mann-Whitney test,
Table 1 Doses to OARsestimated with pre-RIT and post-RIT dosimetry in patients ofgroup I and II. The data arepresented as means±SD (range)
OAR Dose (Gy/GBq)
111In (group I) 90Y (group I) 90Y (group II)
Heart 5.1±1.7 (2.4–9.2) 2.3±0.6 (1.3–3.2) 2.6±0.5 (1.6–3.5)
Liver 7.6±2.7 (4.8–18.8) 1.8±0.9 (0.9–3.9) 2.4±0.9 (1.1–4.5)
Lungs 4.2±2.0 (1.7–8.0) 2.5±1.3 (0.7–4.9) 2.7±1.6 (1.2–6.2)
Spleen 6.6±1.8 (4.4–9.6) 3.1±1.9 (0.8–6.9) 5.2±2.4 (1.8–9.2)
Kidneys 6.4±3.3 (2.5–13.5) 4.2±1.9 (1.9–7.8) 5.1±2.0 (1.6–8.8)
Red marrow 0.54±0.22 (0.27–1.04) 0.43±0.12 (0.28–0.67) 0.38±0.18 (0.18–0.80)
Eur J Nucl Med Mol Imaging

p>0.2; Table 1), suggesting that the correction methodapplied for subtracting residual 111In activity did not intro-duce significant errors.
Discussion
Currently, pre-RIT dosimetry is generally accepted as thegold standard method for estimating doses to OARs inpatients undergoing 90Y-ibritumomab tiuxetan treatment.Doses estimated with pre-RIT dosimetry in group I patientsin this study were in agreement with results previouslyreported by other groups using whole-body planar imaging
[26, 28]. A significant, high interindividual variability inabsorbed dose estimates was found, as shown in Fig. 2. Itis worth mentioning that 10 out of 16 patients in group Iincluded in this study received 90Y-ibritumomab tiuxetan asup-front treatment in contrast to the patients in most90Y-ibritumomab tiuxetan clinical studies who have generallybeen heavily pretreated with chemo- and/or radiation therapy.The particular features of our patients is of importance as mostdosimetry studies in the literature were performed according tothe current indications for which 90Y-ibritumomab tiuxetanRIT is used in patients who have received a variety of previoustherapies, and thus are more heterogeneous. In all patients, thedoses to the OARs were estimated to be far below the dose
Fig. 3 a Serial whole-body anterior images obtained from 0.5 to 90 hafter injection of 999 MBq 90Y-ibritumomab tiuxetan. Images show pro-gressively decreasing blood pool activity as seen on the 111In images. b
Known areas of disease visible on the 18F-FDG PET/CT image arevisualized on late 111In-ibritumomab tiuxetan images and are visible onthe baseline and 0.5-h 90Y images due to residual 111In activity
Eur J Nucl Med Mol Imaging
threshold limits. The maximum administrable activity based onthese results was estimated to be 2.4±1.0 (mean±SD) timeshigher than the prescribed activity. Based on the pre-RITdosimetry estimates, the injected activity could have been
increased by an average of 2.4 times (range 0.6 to 4.7times) while still remaining within the determined OAR doselimits. This finding confirms the possibility of using pre-RITdosimetry estimates to significantly increase the administered
Fig. 4 Comparison of OAR clearance curves in patients of group I for pre- and post-RIT dosimetry. The same trends were observed for the RM (a)and the whole body (b), whereas the post-RIT doses for all other OARs were significantly underestimated. c Example clearance curve for the liver
Fig. 5 Post-RIT vs. pre-RIT dosimetry estimates for the RM (a), the whole body (b) and the remaining OARs (c). The correlations for these dataare presented in the text
Eur J Nucl Med Mol Imaging
activity in 90Y-ibritumomab tiuxetan RIT. Such an approachmay improve therapeutic efficacy using either high doses in asingle injection or repeated cycles. To date, there are nostudies in which the 90Y-ibritumomab tiuxetan administereddose was adjusted based on pre-RIT dosimetry whereas pre-RIT dosimetry has generally been used to determine theadministered doses in anti-CD20 RIT with 131I-tositumomab[29]. From the data presented in this study it appears thatadministered doses can probably be significantly increased,at least by a factor of 2, while still remaining well withinthreshold absorbed doses to OARs. Dedicated studieswould be required to establish and validate this possibilityalthough such an approach appears to be timely given theexpanded role of this treatment modality. Nevertheless, ourresults clearly indicate that implementation of such newapproaches for 90Y-ibritumomab tiuxetan therapy wouldmake pretherapy dosimetry with 111In-ibritumomab tiuxetanmandatory.
There are several arguments in favour of obtaining directdosimetric information following 90Y-ibritumomab tiuxetanadministration. Given the recent increased utilization of90Y-ibritumomab tiuxetan treatment, it is conceivablethat multiple administrations of 90Y-ibritumomab tiuxetan inthe same patient may be applied in the future. In such a clinicalsetting, accurate, direct, dosimetry would be more desirableand clinically useful. This also holds true for patients who arebed-ridden or unable to cooperate and those with a poorperformance status. In such patients, minimizing the numberof hospital visits and scanning sessions would be preferred.Finally, post-RIT dosimetry would be a ‘win–win situation’being more convenient in terms of cost, eliminating the needfor a second dose of radiolabelled ibritumomab tiuxetan, andreducing the total patient absorbed dose.
Comparison of the 111In and 90Y blood sample data showedthat both radiolabelled ibritumomab tiuxetan preparations had
similar RM kinetics (Fig. 4a) and average absorbed dosevalues (Table 1), and that there was a good correlationbetween the two datasets (Fig.5a), indicating that the resultsobtained with the two methods are comparable. By using theSgouros method, only the RM self-absorption component wastaken into account. The dose was estimated considering thecontributions from the blood cells and extracellular fluid,while the contribution from the RM cells was not consideredsince no patient had disease involvement of the bone marrow,in agreement with the EANM Dosimetry Committee guide-lines [30]. However, we considered comparing only self-absorbed doses more appropriate, since increased doseaccuracy can be achieved only with absolute dosimetrymethods and the increase in accuracy would be lost inpost-RIT dosimetry due to the lower quality of bremsstrahlungimages. To the same extent, whole-body absorbed dose esti-mates showed superimposable overall kinetics (Fig. 4b) andabsorbed dose estimates (Table 1). The results also indicate alinear correlation, although because of the limited sample size,conclusive statistical significance was not achieved (Fig.5b). Itshould be pointed out that, in this case as well, the absorbeddoses were estimated from the 111In and the 90Y datasets usingessentially the same relative dosimetry approach method.
On the other hand, doses to the remaining OARs basedon the 90Y images were largely underestimated relative tothose estimated by the 111In reference method (Table 1,Fig. 5c). The doses estimated by absolute dosimetry andrelative dosimetry were very different between the two data-sets. The absolute dosimetry approach measuring individualorgan ACFs was used in the 111In images, whereas the relativedosimetry approach was used for the 90Y studies. Weaddressed the limitations of the relative dosimetry versus theabsolute dosimetry approach by comparing the results of thetwo approaches in analysing the data obtained from the pre-RIT 111In-ibritumomab tiuxetan scans. There is evidence in
Fig. 6 a Absolute pre-RIT dosimetry vs. relative pre-RIT dosimetryfor OARs. There is a good linear correlation between the two datasetsand a marked underestimation using the relative dosimetry approach. b
Relative post-RIT dosimetry vs. relative pre-RIT dosimetry for thewhole body and OARs. There is a poor correlation between thedatasets
Eur J Nucl Med Mol Imaging

the literature that the results of relative dosimetry may bedifferent from those of absolute dosimetry [26]. Dose esti-mates obtained with the absolute dosimetry approach weresystematically higher and significantly different from theresults of relative dosimetry (Fig. 6a). In absolute dosimetryorgan-specific ACFs are used to convert counts into activity asdescribed above, but in relative dosimetry the activity in asource organ is determined directly by the GM count ratio.The assumption is that the total counts from the whole-bodyimage acquired immediately after ibritumomab tiuxetaninjection is representative of all the administered activity.Using this approach, the number of detected photons emittedfrom each patient corresponds to the administered activity thatis exposed to the specific whole-body attenuation effect in anaverage patient (ACFwb(0)). The main drawback of usingthis method is the assumption that each investigatedorgan has the same attenuation contribution as the wholebody. This parameter is implicitly estimated when acquiringthe first image (ACFwb(0)0ACFj). This approach, althoughvery practical in its application since there is no need todirectly measure organ-specific ACFs, appears to beoversimplified and not sufficiently accurate. Our resultsfrom absolute dosimetry showed that for all the OARsbeing analysed, the ACFj/ACFwb(0) ratio was in therange 2.3–3.6, i.e. the attenuation contribution of OARsis much higher than that of the measured whole-bodyvalues, and therefore the underlying hypothesis onwhich relative dosimetry is based is clearly inaccurate.
The change in 90Y-ibritumomab tiuxetan biodistributionover time is another possible source of inaccuracy with therelative dosimetry approach for the definition of injectedactivity. For example, in the first image, higher blood poolactivity is probably less attenuated in certain regions of thebody such as the limbs. In the subsequent images, however,activity concentrates in organs in the torso where higherattenuation contribution is probable. Therefore, since theinjected activity can only be determined in the first whole-body image where there may be a lower overall attenuationcontribution, it is likely that activity measured in the OARson later scans is underestimated.
We found a good linear correlation between the relativeand absolute dosimetry results for the 111In data (R200.61;Fig. 6a). In this paired comparison, the relative dosimetryapproach underestimated the doses relative to the absolutedosimetry approach by a factor of 2.8. Thus, the limitationsof the relative dosimetry approach can be resolved byapplying a correction factor (in this series and with ourmethods, multiplying the relative dosimetry values by2.8). Such a correction may yield fairly accurate esti-mates of absorbed doses when absolute dosimetry measure-ments cannot be performed. Overall, our findings support thenotion that measured ACFs are very important for accuratedose estimation and that the absolute dosimetry approach is
superior to the relative dosimetry method. A further improve-ment to this approach may be the application of scatter cor-rection through appropriate energy window acquisitions [24],although some reports suggest that there may be little gain inapplying such a correction [26].
The inability to acquire absolute measurements of radio-activity after 90Y-ibritumomab tiuxetan injection is the mainlimitation in obtaining adequate dose estimates using thepost-RIT dosimetry approach. The broad energy spectrumof bremsstrahlung X-rays does not allow adequate scatterand ACFs to be defined for this method to be applied. Thislimitation is particularly evident when using stand-alonegamma camera SPECT systems, as in our study. We there-fore did not attempt to apply absolute dosimetry to the 90Ydata. Nevertheless, some reports suggest that these limita-tions may be adequately addressed by using hybrid SPECT/CT systems so that CT-based attenuation correction can beapplied [31]. In order to test whether the limitations of therelative dosimetry approach in analysing the post-RIT datacould be overcome by application of a conversion factor asfor the pre-RIT data, we compared the dosimetry results fromthe analysis of the 111In and 90Y-ibritumomab tiuxetan datausing the relative dosimetry method. Our hypothesis was thatthe overall attenuation effect was comparable between the twodatasets. The correlation between the values obtained from thetwo datasets was linear with a slope of approximately 1,suggesting a certain degree of correspondence of the resultsobtained, but the degree of correlation was quite poor (R200.13; Fig. 6b). The application of a conversion factor to the 90Ydata would therefore not produce reliable results. This findingimplies that there are further limitations to planar post-RITdosimetry besides the inability to apply the absolute dosimetrymethod. These limitations are probably linked to differences inattenuation and scatter effects between 111In and 90Y. The lowerresolution bremsstrahlung images appear to be less representa-tive of the actual activity distribution the 111In images.
Conclusion
Pre-RIT 111In-ibritumomab tiuxetan studies provide usefulhigh-quality clinical images in patients undergoing 90Y-ibritumomab tiuxetan treatment. Analysis of these datausing the relative dosimetry approach underestimates thedoses relative to absolute dosimetry results by a factor of 2.8.Pre-RIT OAR absorbed dose estimates suggest that activityadministered to patients undergoing 90Y-ibritumomab tiuxetantreatment could be significantly increased while still maintain-ing absorbed doses within threshold values.
Direct monitoring of the distribution of 90Y-ibritumomabtiuxetan would ideally allow accurate estimation of effectivedoses to OARs during treatment. Post-RIT dosimetry allowsaccurate determination only of RM absorbed doses. Thepoor correlation between pre-RIT and post-RIT dosimetry
Eur J Nucl Med Mol Imaging

results observed for the remaining OARs indicates thatplanar bremsstrahlung dosimetry estimates are affected bythe lower overall accuracy of this imaging method. Thislimitation is likely to be solved only through the use ofmore sophisticated imaging and processing methods, suchas the use of hybrid SPECT/CT systems and pixel-basedattenuation correction and compensation for scatter andcollimator response. Keeping in mind all these limitations,bremsstrahlung imaging can provide useful clinical informa-tion, and imaging based dosimetry can still provide approxi-mate estimates of doses to OARs.
Conflicts of interest None.
References
1. Rao AV, Akabani G, Rizzieri DA. Radioimmunotherapy fornon-Hodgkin's lymphoma. Clin Med Res. 2005;3:157–65.
2. Chinn PC, Leonard JE, Rosenberg J, Hanna N, Anderson DR. Pre-clinical evaluation of 90Y-labeled anti-CD20 monoclonal antibody fortreatment of non-Hodgkin's lymphoma. Int J Oncol. 1999;15:1017–25.
3. Juweid ME. Radioimmunotherapy of B-cell non-Hodgkin'slymphoma: from clinical trials to clinical practice. J NuclMed. 2002;43:1507–29.
4. Knox SJ, Goris ML, Trisler K, Negrin R, Davis T, Liles TM, et al.Yttrium-90-labeled anti-CD20 monoclonal antibody therapy ofrecurrent B-cell lymphoma. Clin Cancer Res. 1996;2:457–70.
5. Morschhauser F, Radford J, Van Hoof A, Vitolo U, Soubeyran P,Tilly H, et al. Phase III trial of consolidation therapy with yttrium-90-ibritumomab tiuxetan compared with no additional therapyafter first remission in advanced follicular lymphoma. J ClinOncol. 2008;26:5156–64.
6. Witzig TE, Gordon LI, Cabanillas F, CzuczmanMS, EmmanouilidesC, Joyce R, et al. Randomized controlled trial of yttrium-90-labeledibritumomab tiuxetan radioimmunotherapy versus rituximabimmunotherapy for patients with relapsed or refractory low-grade, follicular, or transformed B-cell non-Hodgkin's lymphoma. JClin Oncol. 2002;20:2453–63.
7. Witzig TE, Molina A, Gordon LI, Emmanouilides C, Schilder RJ,Flinn IW, et al. Long-term responses in patients with recurring orrefractory B-cell non-Hodgkin lymphoma treated with yttrium 90ibritumomab tiuxetan. Cancer. 2007;109:1804–10.
8. Grillo-Lopez AJ. Zevalin: the first radioimmunotherapy approvedfor the treatment of lymphoma. Expert Rev Anticancer Ther.2002;2:485–93.
9. Illidge T, Morschhauser F. Radioimmunotherapy in follicularlymphoma. Best Pract Res Clin Haematol. 2011;24:279–93.
10. Morschhauser F, Dreyling M, Rohatiner A, Hagemeister F, BischofDelaloye A. Rationale for consolidation to improve progression-free survival in patients with non-Hodgkin's lymphoma: a reviewof the evidence. Oncologist. 2009;14 Suppl 2:17–29.
11. Witzig TE, White CA, Wiseman GA, Gordon LI, Emmanouilides C,Raubitschek A, et al. Phase I/II trial of IDEC-Y2B8 radioimmuno-therapy for treatment of relapsed or refractory CD20(+) B-cell non-Hodgkin's lymphoma. J Clin Oncol. 1999;17:3793–803.
12. Devizzi L, Guidetti A, Tarella C, Magni M, Matteucci P, Seregni E,et al. High-dose yttrium-90-ibritumomab tiuxetan with tandemstem-cell reinfusion: an outpatient preparative regimen forautologous hematopoietic cell transplantation. J Clin Oncol.2008;26:5175–82.
13. Jacobs SA. Yttrium ibritumomab tiuxetan in the treatment of non-Hodgkin's lymphoma: current status and future prospects. Biologics.2007;1:215–27.
14. Conti PS, White C, Pieslor P, Molina A, Aussie J, Foster P. Therole of imaging with (111)In-ibritumomab tiuxetan in theibritumomab tiuxetan (Zevalin) regimen: results from a ZevalinImaging Registry. J Nucl Med. 2005;46:1812–8.
15. WisemanGA,White CA, StabinM,DunnWL, ErwinW,DahlbomM,et al. Phase I/II 90Y-Zevalin (yttrium-90 ibritumomab tiuxetan, IDEC-Y2B8) radioimmunotherapy dosimetry results in relapsed or refractorynon-Hodgkin's lymphoma. Eur J Nucl Med. 2000;27:766–77.
16. Wiseman GA, Kornmehl E, Leigh B, Erwin WD, Podoloff DA,Spies S, et al. Radiation dosimetry results and safety correlationsfrom 90Y-ibritumomab tiuxetan radioimmunotherapy for relapsedor refractory non-Hodgkin's lymphoma: combined data from 4clinical trials. J Nucl Med. 2003;44:465–74.
17. Shen S, DeNardo GL, Yuan A, DeNardo DA, DeNardo SJ.Planar gamma camera imaging and quantitation of yttrium-90bremsstrahlung. J Nucl Med. 1994;35:1381–9.
18. Cremonesi M, Ferrari M, Grana CM, Vanazzi A, Stabin M,Bartolomei M, et al. High-dose radioimmunotherapy with90Y-ibritumomab tiuxetan: comparative dosimetric study fortailored treatment. J Nucl Med. 2007;48:1871–9.
19. Minarik D, Sjogreen-Gleisner K, Linden O, Wingardh K, TennvallJ, Strand SE, et al. 90Y Bremsstrahlung imaging for absorbed-doseassessment in high-dose radioimmunotherapy. J Nucl Med.2010;51:1974–8.
20. Wiseman GA, Gordon LI, Multani PS, Witzig TE, Spies S, BartlettNL, et al. Ibritumomab tiuxetan radioimmunotherapy for patientswith relapsed or refractory non-Hodgkin lymphoma and mild throm-bocytopenia: a phase II multicenter trial. Blood. 2002;99:4336–42.
21. Zimmer AM. Logistics of radioimmunotherapy with yttrium 90ibritumomab tiuxetan (Zevalin). Semin Nucl Med. 2004;34:14–9.
22. Sgouros G. Bone marrow dosimetry for radioimmunotherapy:theoretical considerations. J Nucl Med. 1993;34:689–94.
23. Stabin MG, Eckerman KF, Bolch WE, Bouchet LG, Patton PW.Evolution and status of bone and marrow dose models. CancerBiother Radiopharm. 2002;17:427–33.
24. Holstensson M, Hindorf C, Ljungberg M, Partridge M, Flux GD.Optimization of energy-window settings for scatter correction inquantitative (111)In imaging: comparison ofmeasurements andMonteCarlo simulations. Cancer Biother Radiopharm. 2007;22:136–42.
25. Rosset A, Spadola L, Ratib O. OsiriX: an open-source software fornavigating in multidimensional DICOM images. J Digit Imaging.2004;17:205–16.
26. Fisher DR, Shen S, Meredith RF. MIRD dose estimate report No.20: radiation absorbed-dose estimates for 111In- and 90Y-ibritumomab tiuxetan. J Nucl Med. 2009;50:644–52.
27. Stabin MG, Sparks RB, Crowe E. OLINDA/EXM: the second-generation personal computer software for internal dose assessmentin nuclear medicine. J Nucl Med. 2005;46:1023–7.
28. Chiesa C, Botta F, Di Betta E, Coliva A, Maccauro M, Aliberti G,et al. Dosimetry in myeloablative (90)Y-labeled ibritumomabtiuxetan therapy: possibility of increasing administered activityon the base of biological effective dose evaluation. Preliminaryresults. Cancer Biother Radiopharm. 2007;22:113–20.
29. Baechler S, Hobbs RF, Jacene HA, Bochud FO, Wahl RL, SgourosG. Predicting hematologic toxicity in patients undergoingradioimmunotherapy with 90Y-ibritumomab tiuxetan or 131I-tositumomab. J Nucl Med. 2010;51:1878–84.
30. Hindorf C, Glatting G, Chiesa C, Linden O, Flux G. EANMDosimetry Committee guidelines for bone marrow and whole-body dosimetry. Eur J Nucl Med Mol Imaging. 2010;37:1238–50.
31. Minarik D, Ljungberg M, Segars P, Gleisner KS. Evaluation ofquantitative planar 90Y bremsstrahlung whole-body imaging. PhysMed Biol. 2009;54:5873–83.
Eur J Nucl Med Mol Imaging