epidemiological and therapeutic aspects of inflammatory
TRANSCRIPT
Epidemiological and therapeutic aspects of inflammatory bowel disease

To my family
Örebro Studies in Medicine 178
CARL ERIKSSON
Epidemiological and therapeutic aspects of inflammatory bowel disease

© Carl Eriksson, 2018
Title: Epidemiological and therapeutic aspects of inflammatory bowel disease
Publisher: Örebro University 2018 www.oru.se/publikationer-avhandlingar
Print: Örebro University, Repro 04/2018
ISSN 1652-4063 ISBN 978-91-7529-242-7
Abstract Carl Eriksson (2018): Epidemiological and therapeutic aspects of inflam-matory bowel disease. Örebro Studies in Medicine 178. Introduction: The two main forms of inflammatory bowel disease (IBD) are Crohn’s disease and ulcerative colitis. These are chronic inflammato-ry disorders, mainly affecting the gastrointestinal tract.
Aims: The overall aims of this thesis were to study the epidemiology of ulcerative colitis in Örebro, Sweden; to examine certain aspects of anaemia in IBD; and to determine the clinical effectiveness of medical treatments.
Material and methods: Cohort studies with the sampling frame de-fined by the geographic boundaries of the primary catchment area of Örebro University Hospital (Papers I‒III), or by the entire IBD popula-tion in Sweden registered in the Swedish national quality registry for IBD (SWIBREG; paper IV), were performed to determine the epidemiology of ulcerative colitis, the incidence and prevalence of anaemia in IBD, and the clinical effectiveness of thiopurine drugs and vedolizumab in routine care.
Results: A fivefold increase in the incidence and a tenfold increase in the prevalence of ulcerative colitis was observed in Örebro during the past 50 years. In parallel, the prognosis, in terms of risk for colectomy within 10 years from diagnosis, improved during the same time period. Earlier and more widespread use of thiopurine drugs may have contrib-uted to the decrease in colectomies. Anaemia is common in IBD, particu-larly in Crohn’s disease. Vedolizumab, a new drug targeting leucocyte migration to the gut, appears to be well tolerated and effective in Swe-dish real-world IBD care.
Conclusion: Ulcerative colitis is on the rise, and data from Örebro in-dicate that the number of IBD patients in Sweden already exceeds 70,000. Improved knowledge of long-term outcomes of medical therapy may have far-reaching implications for future IBD management.
Keywords: Inflammatory bowel disease; ulcerative colitis; Crohn’s disease; cohort study; population-based; colectomy; disease course; anaemia; aza-thioprine; 6-mercaptopurine; vedolizumab Carl Eriksson, School of Health and Medical Sciences, Örebro University, SE-701 82, Sweden, [email protected]

Table of contents
LIST OF PUBLICATIONS ....................................................................... 13
ABBREVIATIONS ................................................................................... 14
INTRODUCTION ................................................................................... 15 Historical remarks .................................................................................... 15 Definitions and diagnosis ......................................................................... 16
Classification of Crohn’s disease .......................................................... 17 Classification of ulcerative colitis ......................................................... 18 Histopathological aspects of IBD ......................................................... 19
Clinical features of IBD ............................................................................ 20 Monitoring of disease activity .................................................................. 23
Endoscopy ............................................................................................ 23 Disease activity indices ......................................................................... 23 Biomarkers ........................................................................................... 24
Epidemiology ........................................................................................... 25 Aetiology and pathogenesis ...................................................................... 27 Environmental risk factors ....................................................................... 28
Smoking ............................................................................................... 29 Appendectomy ..................................................................................... 29 Oral contraceptive agents ..................................................................... 30 Non-steroidal anti-inflammatory drugs ................................................ 30 The gut microbiota............................................................................... 30 Antibiotics ............................................................................................ 31 Diet ...................................................................................................... 32
Treatment of IBD ..................................................................................... 33 Aminosalicylates .................................................................................. 33 Glucocorticosteroids ............................................................................ 33 Immunomodulators.............................................................................. 33 Biological agents .................................................................................. 34 Surgery ................................................................................................. 35
AIMS ........................................................................................................ 37 Paper I .................................................................................................. 37 Paper II ................................................................................................ 37 Paper III ............................................................................................... 37 Paper IV ............................................................................................... 37
ETHICS .................................................................................................... 37
MATERIAL AND METHODS ................................................................ 38 Papers I‒III ............................................................................................... 38
Patients ................................................................................................. 38 Inclusion criteria................................................................................... 38 Data collection ..................................................................................... 39
Paper IV ................................................................................................... 40 Patients ................................................................................................. 40 Inclusion criteria................................................................................... 40 Data collection ..................................................................................... 40
Statistics ................................................................................................... 41 Incidence rate ....................................................................................... 41 Regression analysis ............................................................................... 42
RESULTS ................................................................................................. 44 Paper I ...................................................................................................... 44
Incidence rate ....................................................................................... 44 Prevalence ............................................................................................ 44 Long-term outcome of ulcerative colitis ............................................... 45 Progression in extent of disease ............................................................ 45 Colectomy ............................................................................................ 46 Temporal trends in medical therapy ..................................................... 47
Paper II ..................................................................................................... 47 Patients ................................................................................................. 47 Incidence rate ....................................................................................... 48 Period prevalence ................................................................................. 49 Risk factors for anaemia ...................................................................... 49 Treatment and outcome of anaemia ..................................................... 49
Paper III .................................................................................................... 50 Patients ................................................................................................. 50 Colectomy ............................................................................................ 50 Hospital admission ............................................................................... 50 Progression in extent of disease ............................................................ 53 Anti-TNF exposure .............................................................................. 54
Paper IV ................................................................................................... 55 Patients ................................................................................................. 55 Drug continuation rate ......................................................................... 55 Predictors of discontinuation ................................................................ 56 Clinical and biochemical effectiveness in Crohn’s disease..................... 56
Clinical and biochemical effectiveness in ulcerative colitis ................... 56
DISCUSSION ........................................................................................... 57 Methodological considerations................................................................. 59
Bias and random error ......................................................................... 60 Confounding ........................................................................................ 61 Validity ................................................................................................ 61 Limitations ........................................................................................... 61
GENERAL CONCLUSIONS ................................................................... 65
FUTURE PERSPECTIVES ........................................................................ 66
SAMMANFATTNING PÅ SVENSKA ..................................................... 68
ACKNOWLEDGMENTS ........................................................................ 70
REFERENCES ......................................................................................... 72

CARL ERIKSSON Inflammatory Bowel Disease 13
List of publications This thesis is based on the following studies, which are referred to in the text by their Roman numerals.
I. Eriksson C, Cao Y, Rundquist S, Zhulina Y, Henriksson I, Montgomery S, Halfvarson J. Changes in medical management and colectomy rates: a population-based cohort study on the epidemiology and natural history of ulcerative colitis in Ore-bro, Sweden, 1963-2010. Aliment. Pharmacol. Ther. 2017; 46:748-757.
II. Eriksson C, Henriksson I, Brus O, Zhulina Y, Nyhlin N, Tysk C, Montgomery S, Halfvarson J. Incidence, prevalence and clinical outcome of anaemia in inflammatory bowel disease: A population-based cohort study. Submitted.
III. Eriksson C, Rundquist S, Cao Y, Montgomery S, Halfvarson J. The impact of thiopurines on the natural history and surgical outcome of ulcerative colitis: A cohort study. Accepted for publication in Gut.
IV. Eriksson C, Marsal J, Bergemalm D, Vigren L, Bjork J, Eber-hardson M, Karling P, Söderman C, Myrelid P, Cao Y, Sjöberg D, Thörn M, Karlen P, Hertervig E, Strid H, Ludvigsson JF, Almer S, Halfvarson J. Long-term effectiveness of vedolizumab in inflammatory bowel disease: a national study based on the Swedish National Quality Registry for Inflammatory Bowel Disease (SWIBREG). Scand. J. Gastroenterol. 2017; 52: 722-729.
Published papers have been reprinted with permission from the publisher.
14 CARL ERIKSSON Inflammatory Bowel Disease
Abbreviations CI Confidence interval CDAI Crohn’s disease activity index CRP C-reactive proteinHBI Harvey-Bradshaw indexIBD Inflammatory bowel diseaseIBD-U Inflammatory bowel disease unclassifiedICD International Statistical Classification of Diseases and Relat-
ed Health ProblemsIQR Interquartile rangeLOD Lowest limit of detectionMCS Mayo Clinic scoreP-HBI Patient Harvey-Bradshaw indexP-SCCAI Patient Simple Clinical Colitis Activity indexRCT Randomized controlled trialSWIBREG Swedish national quality registry for IBD TNF Tumour necrosis factor

CARL ERIKSSON Inflammatory Bowel Disease 15
Introduction The two main forms of inflammatory bowel disease (IBD) are Crohn’s disease and ulcerative colitis. These are chronic, relapsing and remitting inflammatory disorders, mainly affecting the gastrointestinal tract.
Despite having some common features, the two forms can usually be distinguished by differences in clinical, endoscopic, and histopathological characteristics. Crohn’s disease affects any region of the intestine, often discontinuously,1 while ulcerative colitis always involves the rectum and to a varying extent the colon in a continuous fashion.2, 3 In Crohn’s disease, transmural inflammation is common, whereas in ulcerative colitis―with the exception of acute severe ulcerative colitis―the inflammation is re-stricted to the colonic mucosa.4 However, the term IBD unclassified (IBD-U) is used in a small proportion of cases in whom there is evidence of chronic colonic inflammation but no evidence to favour a definitive diag-nosis of either Crohn’s disease or ulcerative colitis,5 while the term inde-terminate colitis is reserved for cases where a reliable distinction is impos-sible after colectomy.4, 6
Historical remarks Ulcerative colitis was the first subtype of IBD to be characterized as a dis-tinct disease entity. The term is generally ascribed to Sir Samuel Wilks (1824‒1911) who, in a case report written in 1859, described a condition similar to what is understood as being ulcerative colitis today (even though it has later been argued that Wilks actually described a patient with Crohn’s disease).7,8 The first series of Crohn’s disease patients was published in 1913 by the Scottish surgeon Thomas Kennedy Dalziel (1961‒1924). His report included nine patients who had been treated surgically and in whom the pathologist observed giant cells, granulomas, but no signs of infectious agents. In the report, Dalziel described the bowel as having “the consistence and smoothness of an eel in a state of rigor mortis” and proposed a radical surgical approach: “one does not hesitate in resecting large proportions of the intestine”.9
Although Dalziel’s and several other reports preceded Burrill Crohn’s (1884‒1983), Leon Ginzburg’s (1898‒1988), and Gordon Oppenheimer’s (1900‒1974) contribution by nearly 20 years,9-11 it was their landmark article (published in 1932) that alerted the medical world to the existence of Crohn’s disease.12 Dr. Crohn himself strongly discouraged the use of the eponym Crohn’s disease, which was attributed to him through an odd set

16 CARL ERIKSSON Inflammatory Bowel Disease
of circumstances. Ginzburg and Oppenheimer were the ones who discov-ered the pattern of disease, collected the first 12 cases, and proposed the term “regional ileitis”.13 However, in order to increase the number of pa-tients in their report, they were put in contact with Crohn who contribut-ed with two additional patients and became a co-author of the report. In the 1930s, the journal’s policy was to arrange the authors alphabetically by surname. In Scotland Crohn’s disease is sometimes still termed Dalziel’s disease, as many Scots considered his description to be the first.14 In 1956, when President Eisenhower, who suffered from Crohn’s disease, required an emergent operation in the middle of the night due to bowel obstruc-tion, the disorder went from a being a medical curiosity to a relatively well-known disease.15
Definitions and diagnosis An accurate definition and classification of IBD is crucial, both from a clinician’s and a basic scientist’s point of view. However, at present no pathognomonic feature of either Crohn’s disease or ulcerative colitis has been identified. Instead, these diagnoses are established based on clinical presentation and confirmed by objective laboratory, histopathological, and endoscopic or radiological findings. The diagnostic criteria and classi-fication of IBD have improved over the past six decades along with ad-vancements in diagnostic methods,16-19 particularly with the introduction of fibre-optic endoscopy and the possibility of obtaining biopsies from the entire colon.20, 21 Today, in the absence of an international consensus, the Lennard-Jones criteria published in 1989 are often regarded to be the gold standard for diagnosis of Crohn’s disease and ulcerative colitis (Table 1).22
CARL ERIKSSON Inflammatory Bowel Disease 17
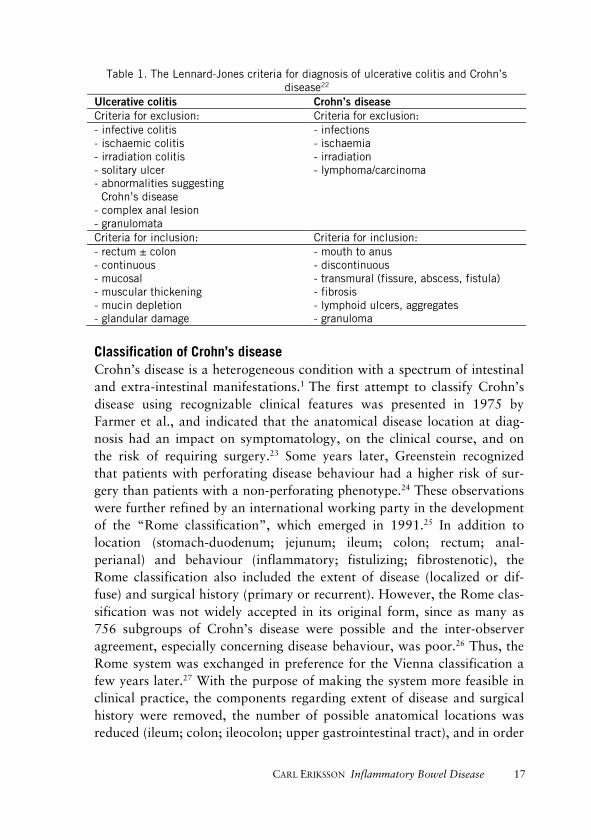
Table 1. The Lennard-Jones criteria for diagnosis of ulcerative colitis and Crohn’s disease22
Ulcerative colitis Crohn’s disease Criteria for exclusion: Criteria for exclusion: - infective colitis - ischaemic colitis - irradiation colitis - solitary ulcer - abnormalities suggesting Crohn’s disease - complex anal lesion - granulomata
- infections - ischaemia - irradiation - lymphoma/carcinoma
Criteria for inclusion: Criteria for inclusion: - rectum ± colon - continuous - mucosal - muscular thickening - mucin depletion - glandular damage
- mouth to anus - discontinuous - transmural (fissure, abscess, fistula) - fibrosis - lymphoid ulcers, aggregates - granuloma
Classification of Crohn’s disease Crohn’s disease is a heterogeneous condition with a spectrum of intestinal and extra-intestinal manifestations.1 The first attempt to classify Crohn’s disease using recognizable clinical features was presented in 1975 by Farmer et al., and indicated that the anatomical disease location at diag-nosis had an impact on symptomatology, on the clinical course, and on the risk of requiring surgery.23 Some years later, Greenstein recognized that patients with perforating disease behaviour had a higher risk of sur-gery than patients with a non-perforating phenotype.24 These observations were further refined by an international working party in the development of the “Rome classification”, which emerged in 1991.25 In addition to location (stomach-duodenum; jejunum; ileum; colon; rectum; anal-perianal) and behaviour (inflammatory; fistulizing; fibrostenotic), the Rome classification also included the extent of disease (localized or dif-fuse) and surgical history (primary or recurrent). However, the Rome clas-sification was not widely accepted in its original form, since as many as 756 subgroups of Crohn’s disease were possible and the inter-observer agreement, especially concerning disease behaviour, was poor.26 Thus, the Rome system was exchanged in preference for the Vienna classification a few years later.27 With the purpose of making the system more feasible in clinical practice, the components regarding extent of disease and surgical history were removed, the number of possible anatomical locations was reduced (ileum; colon; ileocolon; upper gastrointestinal tract), and in order

18 CARL ERIKSSON Inflammatory Bowel Disease
to avoid combinations, a hierarchy regarding disease behaviour was estab-lished (inflammatory; stricturing; penetrating). Furthermore, the variable “age at diagnosis” was implemented (less than 40 years; 40 years or old-er). The current classification system, which in contrast to previous ver-sions also provides recommendations for ulcerative colitis, was presented at the World Congress of Gastroenterology in Montreal, 2005 (Table 2A).28
Classification of ulcerative colitis It has been recognized for years that the disease extent of ulcerative colitis has implications for the long-term prognosis in terms of medication use,29 hospital admissions,30, 31 surgical resection rates, and the risk of colorectal cancer.32 However, it is important to note that these associations were established when the extent of disease was assessed by macroscopic find-ings from double-contrast barium enema or endoscopy, and that the sig-nificance of histological changes in an endoscopically normal mucosa re-mains uncertain. However, there are some data to suggest that the histo-logical extent of disease is associated with the risk of developing colorectal cancer.33 Furthermore, proximal disease progression of proctitis or left-sided colitis may occur in 12–70% of cases within 10 years of diagnosis.28 As a consequence of these obstacles, the Montreal classification working party proposes that the disease extent of ulcerative colitis should be de-fined as the maximal macroscopic extent of disease at endoscopy (Table 2B). In general, rectal involvement and continuous distribution of inflam-mation are essential characteristics of ulcerative colitis. However, “rectal sparring” has been described in children at the time of diagnosis and in adults who have received topical therapy.34, 35 Furthermore, involvement of the cecum or the orifice of the appendix may be observed in patients with left-sided colitis, and “backwash ileitis” occurs in about 20% of patients with extensive colits.36, 37
CARL ERIKSSON Inflammatory Bowel Disease 19
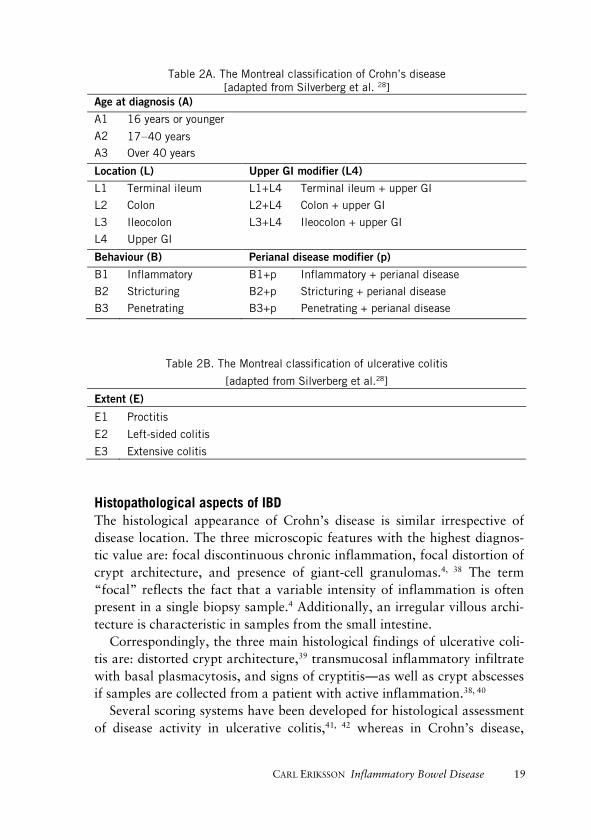
Table 2A. The Montreal classification of Crohn’s disease [adapted from Silverberg et al. 28]
Age at diagnosis (A)
A1 16 years or younger
A2 17‒40 years A3 Over 40 years
Location (L) Upper GI modifier (L4)
L1 Terminal ileum L1+L4 Terminal ileum + upper GI
L2 Colon L2+L4 Colon + upper GI
L3 Ileocolon L3+L4 Ileocolon + upper GI
L4 Upper GI
Behaviour (B) Perianal disease modifier (p)
B1 Inflammatory B1+p Inflammatory + perianal disease
B2 Stricturing B2+p Stricturing + perianal disease
B3 Penetrating B3+p Penetrating + perianal disease
Table 2B. The Montreal classification of ulcerative colitis
[adapted from Silverberg et al.28]
Extent (E)
E1 Proctitis
E2 Left-sided colitis
E3 Extensive colitis
Histopathological aspects of IBD The histological appearance of Crohn’s disease is similar irrespective of disease location. The three microscopic features with the highest diagnos-tic value are: focal discontinuous chronic inflammation, focal distortion of crypt architecture, and presence of giant-cell granulomas.4, 38 The term “focal” reflects the fact that a variable intensity of inflammation is often present in a single biopsy sample.4 Additionally, an irregular villous archi-tecture is characteristic in samples from the small intestine.
Correspondingly, the three main histological findings of ulcerative coli-tis are: distorted crypt architecture,39 transmucosal inflammatory infiltrate with basal plasmacytosis, and signs of cryptitis―as well as crypt abscesses if samples are collected from a patient with active inflammation.38, 40
Several scoring systems have been developed for histological assessment of disease activity in ulcerative colitis,41, 42 whereas in Crohn’s disease,
20 CARL ERIKSSON Inflammatory Bowel Disease
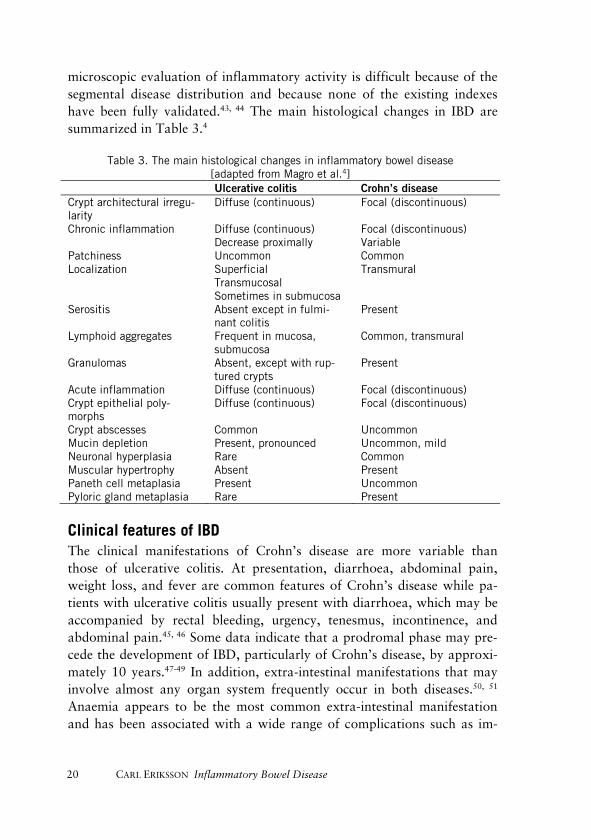
microscopic evaluation of inflammatory activity is difficult because of the segmental disease distribution and because none of the existing indexes have been fully validated.43, 44 The main histological changes in IBD are summarized in Table 3.4
Table 3. The main histological changes in inflammatory bowel disease [adapted from Magro et al.4] Ulcerative colitis Crohn’s disease
Crypt architectural irregu-larity
Diffuse (continuous) Focal (discontinuous)
Chronic inflammation Diffuse (continuous) Decrease proximally
Focal (discontinuous) Variable
Patchiness Uncommon Common Localization Superficial
Transmucosal Sometimes in submucosa
Transmural
Serositis Absent except in fulmi-nant colitis
Present
Lymphoid aggregates Frequent in mucosa, submucosa
Common, transmural
Granulomas Absent, except with rup-tured crypts
Present
Acute inflammation Diffuse (continuous) Focal (discontinuous) Crypt epithelial poly-morphs
Diffuse (continuous) Focal (discontinuous)
Crypt abscesses Common Uncommon Mucin depletion Present, pronounced Uncommon, mild Neuronal hyperplasia Rare Common Muscular hypertrophy Absent Present Paneth cell metaplasia Present Uncommon Pyloric gland metaplasia Rare Present
Clinical features of IBD The clinical manifestations of Crohn’s disease are more variable than those of ulcerative colitis. At presentation, diarrhoea, abdominal pain, weight loss, and fever are common features of Crohn’s disease while pa-tients with ulcerative colitis usually present with diarrhoea, which may be accompanied by rectal bleeding, urgency, tenesmus, incontinence, and abdominal pain.45, 46 Some data indicate that a prodromal phase may pre-cede the development of IBD, particularly of Crohn’s disease, by approxi-mately 10 years.47-49 In addition, extra-intestinal manifestations that may involve almost any organ system frequently occur in both diseases.50, 51 Anaemia appears to be the most common extra-intestinal manifestation and has been associated with a wide range of complications such as im-

CARL ERIKSSON Inflammatory Bowel Disease 21
paired quality of life, increased rate of hospital admissions, and even mor-tality.52, 53 The occurrence of anaemia in IBD is still uncertain, however, as most data come from tertiary referral centres or cohorts of newly diag-nosed patients.53-57
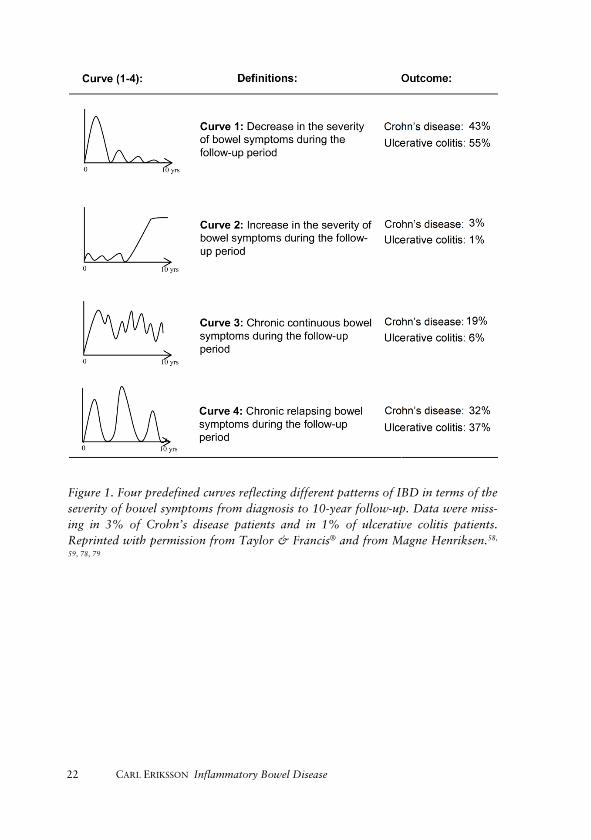
Traditionally, IBD has been renowned for an episodic behaviour with periods of relapses and remissions. However, recent studies have shown that the clinical course varies substantially between patients, ranging from an indolent disease with minimal symptoms to a severe disease that strongly interferes with the individual’s daily life and has a pronounced adverse effect on quality of life.58-61 At the 10-year follow-up of patients diagnosed with IBD in southeastern Norway during the period 1990‒1994, only 35% of them reported the classic episodic pattern of disease whereas a decrease in the severity of symptoms over time was the most common course in both Crohn’s disease and ulcerative colitis (Figure 1).58,
59 Even so, a sizeable proportion of the patients suffered from chronic relapsing―or even chronic continuous symptoms.58, 59 Ulcerative colitis patients with proctitis or left-sided colitis at diagnosis may have a progres-sion in extent of disease during follow-up.28 In Crohn’s disease, the disease location is usually rather stable,62 while the majority of patients will have a change in disease behaviour from purely inflammatory to stricturing and/or penetrating disease, suggesting that the latter phenotypes are mere-ly complications of chronic inflammation.62, 63 Furthermore, the all-cause mortality is slightly increased in both Crohn’s disease and ulcerative colitis compared to the general population,64-67 and both disorders have been associated with an increased risk of colorectal cancer, although the risk has been studied more extensively in ulcerative colitis.68, 69 Even though medical treatment is the mainstay of management in IBD, about 50% of Crohn’s disease patients and 15% of patients with ulcerative colitis will require surgery within 10 years of diagnosis.70 Nowadays, the most com-mon surgical procedure in Crohn’s disease is ileocaecal resection, whereas a total colectomy is the operation of choice in ulcerative colitis.71 There is emerging evidence that the resection rate in Crohn’s disease has decreased in recent decades, while with ulcerative colitis the literature is incon-sistent.70, 72-77 However, indications and timing of surgery have changed over time, and whether improvements in medical management in recent decades have been associated with reduced resection rates and a decreased risk of long-term complications remains largely unknown for both diseas-es.
22 CARL ERIKSSON Inflammatory Bowel Disease
Figure 1. Four predefined curves reflecting different patterns of IBD in terms of the severity of bowel symptoms from diagnosis to 10-year follow-up. Data were miss-ing in 3% of Crohn’s disease patients and in 1% of ulcerative colitis patients. Reprinted with permission from Taylor & Francis® and from Magne Henriksen.58,
59, 78, 79

CARL ERIKSSON Inflammatory Bowel Disease 23
Monitoring of disease activity Today, we have limited ability to predict the disease course in individual patients. Adequate disease monitoring is therefore essential to evaluate the response to medical interventions, in order to identify therapies that are ineffective and also avoid complications.1, 2 During the past decade, “treat to target” has emerged as a concept in the clinical management of IBD.80 The simplest way of monitoring IBD is to assess clinical symptoms. In both Crohn’s disease and ulcerative colitis, a strong association between clinical disease activity and quality of life has been observed.81, 82 In ulcera-tive colitis, the number of stools and the presence of blood in stool are associated with the endoscopic activity,83 while in Crohn’s disease there is a greater discrepancy between the presence of inflammatory lesions at endoscopy and clinical symptoms.84 For example, in a randomized con-trolled trial involving Crohn’s disease patients treated with anti-tumour necrosis factor (anti-TNF) agents and/or immunomodulators, 47% of patients in clinical remission still had lesions visible at colonoscopy, whereas 35% of patients with persistent clinical symptoms did not have any active inflammation visible at colonoscopy.85 Thus, the absence of clinical symptoms is no guarantee that the underlying inflammation is adequately controlled, indicating that a symptomatic response alone is insufficient to prevent future complications of IBD.
Endoscopy Endoscopic examination to determine the mucosal inflammation is the gold standard for assessment of disease activity in the colon and ileum. In both Crohn’s disease and ulcerative colitis, endoscopic improvements and mucosal healing (absence of visible signs of active inflammation) have been associated with better long-term outcomes, including reduced resec-tion rates.86, 87 There are several endoscopic scoring indices for evaluation of disease activity, and the best validated include the Mayo Clinic endo-scopic sub-score for ulcerative colitis, Crohn’s disease endoscopic index of severity, and the simple endoscopic scale for Crohn’s disease.88, 89 How-ever, frequent endoscopies are not always feasible because of poor accept-ability by patients, the risk of complications, high cost, and poor availabil-ity.
Disease activity indices The first disease activity index to be used in IBD, the Trulove and Witts severity index, dates back to 1955 when hydrocortisone was shown to be

24 CARL ERIKSSON Inflammatory Bowel Disease
effective in ulcerative colitis.90 Since then, numerous instruments have been developed, although none of these indices have been completely validated.91, 92 Nowadays, the Crohn’s disease activity index (CDAI) and the Mayo Clinic score (MCS) are the most common outcome measures used in clinical trials.93, 94 However, these indices have several limitations. The CDAI, which consists of 18 clinical items and ranges from 0 to 600, is generally far too complex to be used in clinical practice and correlates poorly with endoscopic and biochemical measures of inflammation.92, 95, 96
The Harvey-Bradshaw Index (HBI) has a high correlation with CDAI and was introduced in order to simplify the assessment.97, 98 Remission is defined as an HBI of < 5 and corresponds to a CDAI score of < 150, while a 3-point change in HBI correlates with a 100-point change in the CDAI.98 The MCS is a composite instrument, ranging from 0 to 12, including both clinical and endoscopic items.93 The main limitation of the MCS is that its sub-components are not easy to properly interweave. For this reason, both symptom-based and endoscopic criteria of response and remission are commonly used in clinical trials.99 The Patient Harvey-Bradshaw index (P-HBI) and the Patient Simple Clinical Colitis Activity index (P-SCCAI) are validated, patient-based, disease activity questionnaires developed to facili-tate assessment of disease severity in clinical practice.100, 101
Biomarkers Although numerous biomarkers that can be detected in blood, faeces, or urine have been evaluated in IBD, the most widely used in both clinical practice and in research include C-reactive protein (CRP) and calprotec-tin.102
CRP was originally discovered by Tillett et al. in 1930, and is an acute-phase protein synthesized by the liver in response to inflammatory cyto-kines.103 Early studies found increased levels of CRP in nearly 100% of patients with active Crohn’s disease and in approximately 50% of those with ulcerative colitis.104-106 However, according to recent data the sensitiv-ity of CRP to detect active disease, based on colonoscopy, is only about 50% in both conditions and it has been estimated that as many as 20% of healthy individuals do not generate CRP under inflammatory conditions.107, 108 Furthermore, levels of CRP can be confounded by age, sex, body mass index, and other inflammatory conditions.109 Faecal bi-omarkers have the potential to detect mucosal inflammation with higher sensitivity and specificity.

CARL ERIKSSON Inflammatory Bowel Disease 25
Calprotectin is a calcium- and zinc-binding protein secreted by activated neutrophil granulocytes; it was discovered in 1983.110 Soluble calprotectin is stable in faeces for up to seven days, and in a meta-analysis of diagnos-tic accuracy studies, the sensitivity and specificity for active IBD according to endoscopy was 88% and 73%, respectively.108
Epidemiology Epidemiology is the science of the frequency and distribution of disease in the general population.111 Although it is common to associate the disci-pline with the study of acute outbreaks of infections, epidemiology still remains important as variations in incidence across geographical regions and changes in the incidence over time may provide clues about the aetiol-ogy and pathogenesis of diseases of unknown cause. Fifty years after the publication of John Snow’s seminal work “On the Mode of Communica-tion of Cholera” in 1849, the first epidemiological study of IBD was pre-sented at a symposium at the Royal Society of Medicine in London. One hundred and seventy-seven patients with ulcerative colitis had been identi-fied at three London hospitals, and the report included observations on the common presentation (diarrhoea and haemorrhage) and on risk fac-tors for the disease (early adult and middle age).112 Since then, more than 1,000 publications have appeared.113
The occurrence of IBD varies considerably, both within and between geographic regions.113 Traditionally, there has been a north-south gradient in the occurrence of IBD, with the highest incidence in “westernized” na-tions including northern Europe,16, 72, 114-119 United Kingdom and North America,120-123 while IBD was rare in southern areas with the exceptions of Israel,124, 125 Australia and South Africa.126-128 Intriguingly, a change in the incidence pattern has occurred in recent decades, with increasing incidence in eastern Europe,129 Asia,130 and Latin America.131
It is believed that IBD is associated with the industrialization of nations, and the observed increase in southern areas is possibly a result of adapta-tion to a “westernized” way of living. In parallel with the increase in IBD in previous low-incidence areas, some reports have indicated a plateau or even a decline in traditional high-incidence regions,132, 133 although by far the highest age-standardized incidence rate of IBD, with no signs of level-ling off (74 per 100,000 inhabitants) has been reported from the Faroe Islands, which are located far north.134 One must also remember that there are several methodological challenges in the assessment of epidemiological data that may easily have influenced the incidence patterns observed in
26 CARL ERIKSSON Inflammatory Bowel Disease
recent decades.135 For example, advances in healthcare systems and the availability of diagnostic modalities necessary for recognition of IBD, such as endoscopy, may be associated with industrialization.136 In addition, most recent epidemiological studies lack the necessary observation time to allow analysis of temporal trends.113
Within one country, the incidence of IBD is higher in urban areas than in rural areas.137-139 Individuals living in cities are exposed to completely different environmental risk factors than people living outside these re-gions. In the late 1980s, Strachan proposed that improved childhood hy-giene and reduced contact with microorganisms in terms of decreased family size, increased use of antibiotics and vaccinations, clean drinking water, and a “westernized” diet, could explain the increase in incidence of autoimmune and allergic diseases associated with industrialization and urbanization.140 The “hygiene hypothesis”, however, may not apply per-fectly to IBD. For instance, in India, proxy markers of low hygiene were found to be associated with an increased risk of ulcerative colitis,141 and several other theories that might explain the increased incidence in urban societies have also emerged, including smoking, air-pollution, and occupa-tional exposure associated with urban employment.139, 142-144
Within countries, the incidence of IBD can also vary among different ethnic groups living in the same area. Early studies demonstrated that Ashkenazic Jews of western Europe, the United States, and South Africa were at increased risk of developing IBD compared to their non-Jewish neighbours.145, 146 The consistency of this finding over time, across differ-ent geographical areas, with studies demonstrating a higher prevalence of CARD15/NOD2 mutations in Ashkenazic Jews, indicates that this differ-ence may be explained by genetic factors.147 (CARD15/NOD2 was the first Crohn’s disease susceptibility gene to be identified).148, 149 In contrast, studies of migrants from low-incidence areas to the United Kingdom and Canada have demonstrated that immigrants―and particularly their off-spring―have incidence rates that are comparable with those of the native population.150, 151 The fact that age at the time of migration appears to be critical, with the highest risk of IBD in children who have grown up in the adoptive country, suggest that differences in incidence depending on eth-nicity might be more related to lifestyle and environmental factors, partic-ularly early in life, than to genetic factors. These results emphasize the importance of including both children and adults in epidemiological sur-veys of IBD.
CARL ERIKSSON Inflammatory Bowel Disease 27
Although IBD affects individuals of all ages, the disease is commonly diagnosed during late adolescence or early adulthood, with a median age of onset of approximately 20‒30 years.113 Some early studies demonstrat-ed a second incidence peak later in life,152, 153 while most current epidemio-logical studies have not shown such a bimodal age distribution.113 In a systematic review of 109 studies reporting the sex-stratified incidence of IBD, no gender-related difference in the incidence was observed in either Crohn’s disease or ulcerative colitis.113
Another reason for performing epidemiological surveys is that studies of incidence and prevalence may provide important information about the burden of disease in a population, which is valuable to politicians and planners of healthcare resources. As Crohn’s disease and ulcerative colitis are incurable conditions with low mortality, the global prevalence is ex-pected to grow exponentially over the next few decades through an epi-demiological phenomenon termed compounding prevalence.154
Aetiology and pathogenesis The cause of IBD is currently unknown, although particularly in Crohn’s disease it appears that affected individuals develop an inappropriate im-mune response to commensal gut bacteria.155-157 Several studies have indi-cated that the strongest independent risk factor for IBD is having a family history of the disease, and the concordance rates of Crohn’s disease in monozygotic twins range from 20% to 55% as compared to from 0% to 3.6% in dizygotic twins.158-162 In ulcerative colitis, the corresponding fig-ures are 6.3% to 18.8% and 0% to 6.3%, respectively, suggesting that genetic susceptibility is more important in the development of Crohn’s disease than in development of ulcerative colitis.158-162 To date, genome-wide association studies have identified 240 distinct loci that modulate the risk of IBD.163 Despite these great efforts, there does remain a substantial “missing heritability”, as the loci identified only explain about 20% of the heritability of IBD.164 However, subsequent studies of the identified loci have revealed several pathways that appear to be of importance in the pathogenesis of IBD, including intestinal barrier function, epithelial resto-ration, innate immune regulation, formation of reactive oxygen species, autophagy, and regulation of adaptive immunity.165
28 CARL ERIKSSON Inflammatory Bowel Disease
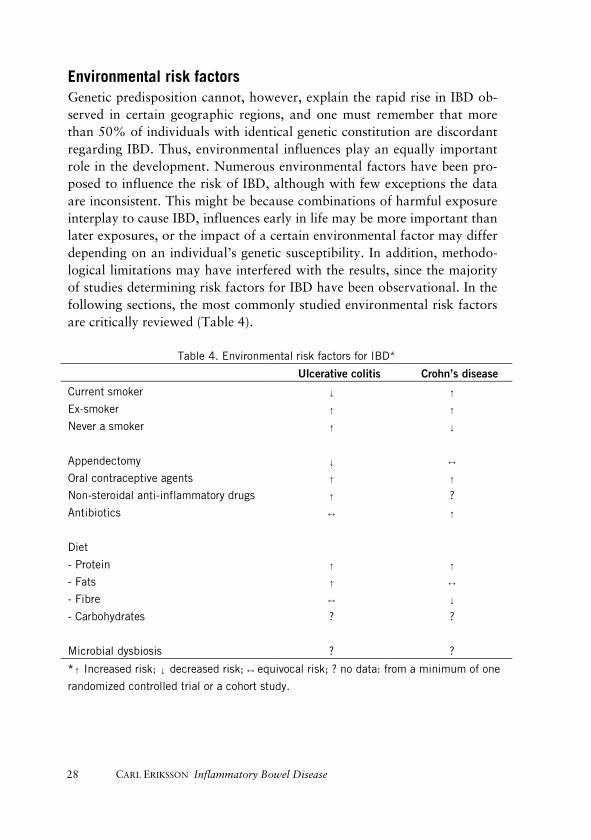
Environmental risk factors Genetic predisposition cannot, however, explain the rapid rise in IBD ob-served in certain geographic regions, and one must remember that more than 50% of individuals with identical genetic constitution are discordant regarding IBD. Thus, environmental influences play an equally important role in the development. Numerous environmental factors have been pro-posed to influence the risk of IBD, although with few exceptions the data are inconsistent. This might be because combinations of harmful exposure interplay to cause IBD, influences early in life may be more important than later exposures, or the impact of a certain environmental factor may differ depending on an individual’s genetic susceptibility. In addition, methodo-logical limitations may have interfered with the results, since the majority of studies determining risk factors for IBD have been observational. In the following sections, the most commonly studied environmental risk factors are critically reviewed (Table 4).
Table 4. Environmental risk factors for IBD*
Ulcerative colitis Crohn’s disease
Current smoker ↓ ↑
Ex-smoker ↑ ↑
Never a smoker ↑ ↓
Appendectomy ↓ ↔
Oral contraceptive agents ↑ ↑
Non-steroidal anti-inflammatory drugs ↑ ?
Antibiotics ↔ ↑
Diet
- Protein ↑ ↑
- Fats ↑ ↔
- Fibre ↔ ↓
- Carbohydrates ? ?
Microbial dysbiosis ? ?
*↑ Increased risk; ↓ decreased risk; ↔ equivocal risk; ? no data: from a minimum of one
randomized controlled trial or a cohort study.

CARL ERIKSSON Inflammatory Bowel Disease 29
Smoking The first environmental risk factor for IBD to be identified was cigarette smoking. In a thesis from 1976, Samuelsson reported that the occurrence of ulcerative colitis was considerably higher in former smokers and in non-smokers than in active smokers.166 However, the thesis was written in Swedish and the observation passed unnoticed until 1982 when the same finding was made from a mail questionnaire used in Cardiff, United King-dom.167 Since then, many studies have confirmed the inverse association between smoking and ulcerative colitis.168-171 Interestingly, cigarette smok-ing has also been associated with a reduced risk of colectomy and hospital admission due to ulcerative colitis, although the mechanism of action re-mains to be explained.172 However, the effect does not seem to be mediat-ed by nicotine alone, as three randomized controlled trials did not find any positive effect on the clinical remission rate of transdermal nicotine treat-ment.173-175 Correspondingly, the use of oral moist snuff does not appear to affect the risk of developing IBD.176, 177
In contrast to the beneficial effects observed in ulcerative colitis, ciga-rette smoking appears to be one of the most important risk factors for Crohn’s disease.170, 171, 178 Similarly, active smoking has been associated with complications such as increased risk of Crohn’s disease-related sur-gery and of recurrent disease after an operation.179, 180
Appendectomy Another influence that has been associated with the development of ulcer-ative colitis is appendectomy. The inverse association was first noticed in an multi-centre case-control study of newly diagnosed patients with IBD.181 A subsequent Swedish cohort study involving 425,000 individuals found that patients who had undergone appendectomy for an inflammato-ry condition such as appendicitis or lymphadenitis before the age of 20 had a reduced risk of developing ulcerative colitis, while in a large Danish cohort a 13% decrease in the relative risk of ulcerative colitis was ob-served, but the association was not statistically significant.182, 183
Studies on the risk of Crohn’s disease after appendectomy have been conflicting.183-185 In a meta-analysis, past appendectomy was associated with a future risk of Crohn’s disease, although no significant association remained five years after the operation.186 At presentation, Crohn’s disease may mimic appendicitis and according to a large Swedish-Danish popula-tion-based study, the association between appendectomy and Crohn’s disease may be explained by diagnostic bias.187 The mechanism by which
30 CARL ERIKSSON Inflammatory Bowel Disease
appendectomy may be protective against ulcerative colitis is not known, but several hypotheses have been proposed. The appendix may act as a reservoir for enteric bacteria, and the development of an appendicular dysbiosis may be a priming event in the development of ulcerative colitis.188
Oral contraceptive agents Several studies have investigated the effect of oral contraceptive agents on the occurrence of IBD. In a meta-analysis of 14 studies, a modest associa-tion with both Crohn’s disease and ulcerative colitis was observed.189 The risk of Crohn’s disease increased with prolonged exposure, while in ulcer-ative colitis no dose-response effect was evaluated because of an insuffi-cient sample size. Similarly, in a recent cohort study of more than 230,000 women, an increased risk of Crohn’s disease was observed in users of oral contraceptive agents whereas in ulcerative colitis, the association was re-stricted to women with a history of smoking.190 Oral contraceptive agents may influence the risk of IBD through the effects of oestrogen, which has immune-enhancing properties with regard to secretion of TNF and mac-rophage proliferation.189 Correspondingly, hormone therapy in post-menopausal women has also been associated with the risk of IBD.191, 192
Non-steroidal anti-inflammatory drugs Several studies have demonstrated that the use of non-steroidal anti-inflammatory drugs is associated with relapse in patients with quiescent IBD.193-195 A possible explanation for this finding may be the effect on the intestinal permeability of these drugs.196 Increased permeability of the intestinal epithelium has been demonstrated in both Crohn’s disease and ulcerative colitis, although whether the barrier impairment is a conse-quence of the inflammatory response or a primary defect is a matter of debate.197, 198 One large cohort study has assessed the effect of non-steroidal anti-inflammatory drugs on the development of IBD and found an association in terms of an increased risk of both Crohn’s disease and ulcerative colitis in heavy users (at least 15 days per month). However, the absolute increase in risk was small and the adjusted risk estimate in Crohn’s disease was not statistically significant.192, 199
The gut microbiota While most of the above-mentioned risk factors have been known for decades, one environmental factor that has gained increasing attention in

CARL ERIKSSON Inflammatory Bowel Disease 31
recent years is the community of bacteria that colonizes the human intes-tine, the microbiome.200 The highest concentration of microbiota is found in the colon, with a level of 1011‒1012 cells/g, thus out-numbering the cells of the entire human body.201 The microbiome has been found to carry out a range of useful functions for the host, including repression of harmful microorganisms, education of the mucosal immune system, and digestion of nutrients that are inaccessible to the host.202 One model to explain how the intestinal microbiota might contribute to chronic inflammation in IBD is the concept of dysbiosis. This model suggests that an imbalance between protective/aggressive commensal bacteria may drive host inflammatory responses in the gut.181 The most consistent observation regarding dysbio-sis in IBD includes a decrease of bacteria in the Firmicutes phylum, an increase in the Protiobacteria phylum, and a reduced diversity of the gut microbiota.203-206 Interestingly, the composition of the gut microbiota has been associated with the IBD phenotype and the risk of relapse of inactive Crohn’s disease.205, 207 Furthermore, several epidemiological risk factors for IBD including diet, age, drug treatment, and smoking appear to have an interplay with the microbial composition, and there is some evidence that faecal microbiota transplantation may induce remission of ulcerative coli-tis.208, 209 However, despite these promising results, it is still not clear whether the dysbiosis observed in IBD is just a consequence of chronic inflammation or a triggering event in the pathogenesis. Prospective longi-tudinal studies to address this question will be essential for further investi-gation.
Antibiotics The first data to support the idea that the use of antibiotics might contrib-ute to the development of Crohn’s disease were from two retrospective case-control studies.210, 211 Since then, several studies have confirmed this finding.212 In a prospective, nationwide Danish cohort study, childhood antibiotic use was found to be associated with Crohn’s disease. The asso-ciation appeared to be stronger within 3 months of initiation of treatment and in children with seven or more courses of antibiotics, whereas no in-crease in the risk of ulcerative colitis was observed.213 Two studies demon-strated that the association between antibiotics and Crohn’s disease was stronger in boys than in girls,214, 215 while the type of antibiotics used did not appear to affect disease development.214, 215
Interestingly, antibiotic use does not appear to influence the occurrence of ulcerative colitis.212 This finding supports the idea that different patho-genic mechanisms are involved in the development of Crohn’s disease and

32 CARL ERIKSSON Inflammatory Bowel Disease
ulcerative colitis. The most conceivable explanation of how antibiotics affect the risk of Crohn’s disease is by alteration of the intestinal microbiota.
Diet It has been proposed that the global variation in dietary habits is the most plausible explanation for the differences in incidence of IBD observed between different geographic regions.216 However, despite numerous stud-ies of dietary influences on the risk of IBD,217 no consensus has emerged. One possible explanation is that these studies are difficult to perform be-cause of poor recall of diet, the time-varying nature of dietary habits, and the possibility that dietary habits change due to symptoms of incipient disease. However, in recent years some large cohort studies have high-lighted some potentially important dietary factors.218-221 A large French prospective cohort study of more than 67,000 women aged 40‒65 years found that a high total protein intake, specifically animal protein, was associated with an increased risk of IBD.221 However, the study was un-der-powered for evaluation of the impact in Crohn’s disease and ulcerative colitis separately. Data from the Nurses’ Health Study, with a cohort of more than 170,000 women followed over 26 years with food frequency questionnaires collected every 2 years, indicated that a high fibre in-take―especially from fruits and to a lesser extent from vegetables and cruciferous vegetables―reduces the risk of Crohn’s disease but not of ulcerative colitis.218 Reverse causation is an unlikely explanation of this finding, as the association remained despite a lag of 4‒8 years between the assessment of fibre intake and diagnosis. In a subsequent study of the Nurses’ Health cohort, high intake of long-chain n-3 polyunsaturated fatty acids was found to be associated with a trend of lower risk of ulcerative colitis whereas high intake of trans-unsaturated fatty acids was associated with a trend of an increased incidence of ulcerative colitis.220 Neither total fat intake nor specific fatty acids modified the risk of Crohn’s disease. Similar results were achieved in a large European, nested case-control study.222 Although several case-control studies have suggested that a high intake of carbohydrates and refined sugars increases the risk of IBD, no such association has been established in more rigorous cohort studies.217 There are several biologically plausible mechanisms by which diet may affect gut inflammation, including antigen presentation, change in prosta-glandin balance, and modification of the microbiota. 223, 224 Interestingly, in newly diagnosed children with Crohn’s disease, nutritional therapy with exclusive enteral nutrition appears to be effective in inducing remission,225,
226 but no beneficial effect has been observed in adults.227
CARL ERIKSSON Inflammatory Bowel Disease 33
Treatment of IBD There is no cure for IBD, but once the diagnosis has been established, the goal of therapy is to induce and sustain remission with the use of medica-tion. It has been hypothesized that control of chronic inflammation may prevent long-term complications such as progression in disease extent, stenosis, or penetrating disease, but there is no proof. Both single-drug therapy and combination therapy are used.
Aminosalicylates In an attempt to treat the arthritis of his King, Gustav V of Sweden, Nan-na Svartz (1890–1986) combined the anti-inflammatory substance 5-aminosalicylic acid with the antibacterial substance sulfapyridine and cre-ated sulphasalazine. When the new drug was serendipitously found to improve ulcerative colitis in patients with both joint symptoms and IBD, sulphasalazine also came in to use in IBD.228 Because of adverse drug reac-tions caused by the sulphapyridine component, 5-aminosalicylate prepara-tions without sulphapyridine (mesalazin, balsalazid, and olsalazine) were developed and have successively replaced sulphasalazine. In ulcerative colitis, 5-aminosalicylates are effective and safe both in inducing remission of active disease and in preventing disease relapse,229, 230 whereas these drugs play a limited role in treatment of Crohn’s disease.231-234
Glucocorticosteroids In 1955, just a few years after the discovery of cortisol by Hench et al., 235 Truelove published the first randomized controlled trial on treatment of IBD in the British Medical Journal, demonstrating improvement and re-duced mortality in ulcerative colitis patients who received corticosteroid treatment.90 However, subsequent studies have revealed that corticoster-oids are a poor choice for maintenance therapy and carry an undesirable side-effect profile.236 Thus, systemic corticosteroids are mainly used for induction of remission in the setting of disease flares.237, 238
Immunomodulators 6-mercaptopurine and its pro-drug azathioprine are among the first de-signer drugs to be developed, and were initially intended for use as chemo-therapeutic agents. Being structural analogues of nucleic acids, they inter-fere with DNA synthesis and inhibit the growth of rapidly dividing cells such as cancer cells or inflammatory cells. In 1958, it was documented that 6-mercaptopurine inhibited the formation of antibodies to protein
34 CARL ERIKSSON Inflammatory Bowel Disease
antigens given to rabbits, and the first study of thiopurines in IBD was published in 1962.239, 240 Subsequent randomized controlled trials demon-strated that thiopurines are effective in maintaining remission in both Crohn’s disease and ulcerative colitis, and that thiopurines prevent recur-rence of Crohn’s disease after surgery.241-243 However, thiopurines have a slow onset of action and there is no clear evidence that these drugs are effective in inducing remission in either Crohn’s disease or ulcerative coli-tis.244, 245 Furthermore, there is no evidence that thiopurines reduce the risk of colectomy in ulcerative colitis. An unfortunate disadvantage of thiopu-rines is the risk of adverse drug reactions, which occur in about 15‒30% of patients and include skin rash, nausea, fever, pancreatitis, hepatotoxici-ty, and bone marrow toxicity.246-248 In 1980, it was found that patients with polymorphisms in the gene encoding the enzyme thiopurine methyl-transferase (TPMT) were at increased risk of bone marrow toxicity and gastrointestinal symptoms because of reduced drug inactivation.249 Thus, TPMT gene variation and also levels of the active metabolites, thioguanine nucleotides, are increasingly being measured in patients on thiopurine treatment.
Biological agents The first biological agents used in common diseases such as IBD were monoclonal antibodies directed at the pro-inflammatory cytokine tumour necrosis factor alpha (TNF). Early studies associated TNF-alfa with the pathogenesis of septic shock, and the first human trials of anti-TNF agents were conducted for sepsis during the late 1980s.250-252 Although anti-TNF agents were never approved for clinical use in sepsis, these studies led oth-er laboratories to investigate the role of TNF-alfa in other diseases such as rheumatoid arthritis and Crohn’s disease.253, 254 In 1995, van Dullemen et al. reported that eight out of 10 Crohn’s disease patients showed normali-zation of CDAI scores and improved endoscopic activity within 4 weeks after a single infusion of anti-TNF, and in 1998 infliximab was the first biological agent to be approved for IBD.255 Even though anti-TNF agents have markedly improved the management of both Crohn’s disease and ulcerative colitis that are refractory to conventional treatment,256-258 many patients do not respond, lose response over time, or become intolerant towards the treatment.259 For instance, patients may develop anti-drug antibodies, which can lead to a loss of response, and anti-TNF therapy has been associated with safety issues such as increased susceptibility to infec-tions and exacerbation of congestive heart failure.260, 261 Thus, drugs with

CARL ERIKSSON Inflammatory Bowel Disease 35
other mechanisms of action are being developed. Vedolizumab is a mono-clonal antibody targeting the alpha4beta7 integrin, blocking the adhesion and migration of leucocytes into the intestinal mucosa.262 Randomized controlled trials have demonstrated that vedolizumab is effective in both Crohn’s disease and ulcerative colitis, although future studies will be re-quired to define the long-term efficacy, the clinical effectiveness, and the safety of this drug.263, 264
Surgery Despite the increasing array of pharmacological treatments for IBD, surgi-cal management has remained a mainstay of therapy for patients who do not respond to medical treatment, suffer intolerable side effects of drug therapy, or develop complications such as dysplasia, adenocarcinoma, perforation, or bowel obstruction.
Operations for IBD during the early 1900s such as appendicostomy, in-testinal bypass, therapeutic pneumo-peritoneum, and vagotomy were spo-radic, were mainly experimental, and were later abandoned.265-268 Howev-er, surgical interventions gradually became more standardized. Beginning in 1913, ileostomy was performed to “rest” the inflamed colon.269 Alt-hough subsequent studies found that this procedure settles the inflamma-tion distal to the stoma, particularly in Crohn’s disease, 270-273 wide resec-tions to remove all histologically detectable disease with the hope of cur-ing the disease were advocated by Dr. Crohn and others.274-276
In ulcerative colitis, early colectomy for patients refractory to steroids was a major advancement, reducing the mortality in acute severe ulcera-tive colitis from approximately 30–40% down to less than 1%.90, 277-279 Proctocolectomy with permanent ileostomy was considered the gold standard of surgical management until the early 1980s, when the currently favoured operation, proctocolectomy with restorative ileal pouch-anal anastomosis, emerged.3, 280 In Crohn’s disease, however, it soon became clear that excision of the affected bowel segment did not cure the disease and that postoperative recurrence was common regardless of resection margins.281 It was also discovered that repeated surgery may produce the short-bowel syndrome.282, 283 Nowadays, surgery is deferred for as long as possible and bowel-preserving operations with minimal resections and techniques for strictureplasty that conserve the bowel length have been widely adopted in the surgical management of Crohn’s disease.284-286
With the exception of colectomy in the setting of acute severe ulcerative colitis that is refractory to corticosteroids, there is still not much evidence

36 CARL ERIKSSON Inflammatory Bowel Disease
from randomized controlled trails to support decisions regarding surgery in IBD. Joint care by multidisciplinary teams remains vitally important for safe management.
CARL ERIKSSON Inflammatory Bowel Disease 37
Aims The overall aim of the work described in this thesis was to study the epi-demiology of ulcerative colitis in Örebro, Sweden, to examine certain as-pects of anaemia in IBD, and to determine the clinical effectiveness of medical treatment.
Paper I To study time trends in the incidence and prevalence of ulcerative colitis and in the risk of progression in disease extent and of colectomy, in the primary catchment area of Örebro University Hospital during the period 1963‒2010.
Paper II To determine the incidence, prevalence, and clinical outcome of anaemia in a population-based IBD cohort and to identify risk factors for anaemia in IBD.
Paper III To study the impact of thiopurines in ulcerative colitis in terms of 10-year risk of colectomy, hospital admission, progression in disease extent, and need for anti-TNF therapy.
Paper IV To describe the vedolizumab-treated IBD population in Sweden, to assess the long-term clinical effectiveness in real-world, and to identify predictors of successful treatment.
Ethics The studies were approved by the Uppsala Regional Ethics Committee (studies I‒III; DNR: 2010/304 and 2010/304/1) or by the Linköping Re-gional Ethics Committee (study IV; DNR: 2014/375-31 and 2015/247-32).

38 CARL ERIKSSON Inflammatory Bowel Disease
Material and methods
Papers I‒III
Patients Papers I‒III were population-based cohort studies with the sampling frame defined by the geographic boundaries of Örebro University Hospital pri-mary catchment area, including the following five municipalities: Asker-sund, Hallsberg, Kumla, Lekeberg, and Örebro. The catchment area co-vers both urban and rural areas and is representative of the whole of Swe-den in terms of migration, demographic profile, and socio-economic fea-tures. During the period 1963‒2010, the population increased by 26% from 150,177 to 189,603 and the median age increased from 36 years (interquartile range [IQR] 18‒57) to 39 years (IQR 20‒59).287 Within the area, there are no private gastroenterologists and everyone with a suspect-ed or verified IBD is referred to Örebro University Hospital. Similarly, all colonoscopies, radiological examinations, and histopathological examina-tions are performed at the University Hospital and all medical rec-ords―including endoscopy, laboratory, radiological, and histopathologi-cal data on patients with inflammatory bowel disease―have been stored at the private archive of the Department of Gastroenterology since the opening in 1976. We identified patients with possible ulcerative colitis by evaluation of all the medical records in this archive. We also performed computerized searches in the County Council’s digital diagnostic database of in-patients and out-patients, which was established in 1988, in order to identify additional cases. The following International Statistical Classifica-tion of Diseases and Related Health Problems (ICD) codes were used in the searches: the ICD-10 codes K510-K519 (ulcerative colitis), K528-K529 (colitis UNS), K500-K509 (Crohn’s disease), M074-M076 (IBD-associated arthropathy), and M091-M092 (IBD-associated juvenile arthritis); and the ICD-9 codes 555 (regional enteritis), 556 (ulcerative colitis), and 558 (oth-er and unspecified non-infectious gastroenteritis and colitis).
Inclusion criteria Individuals who were resident in the catchment area of Örebro University Hospital were included in paper I if they were diagnosed with ulcerative colitis according to the Lennard-Jones criteria before 31 December 2010.22 Patients who were diagnosed during the period 1963‒2010 and who lived
CARL ERIKSSON Inflammatory Bowel Disease 39
within the catchment area at the time of diagnosis were considered to be incident cases. Patients were surveyed until death, until migration, or to the end of follow-up, i.e. 31 December 2015. All incident patients who had received treatment with thiopurine drugs at any time during their disease course until the end of follow-up were included in paper III, while a random subset of patients with IBD who were living in the catchment area on 31 December 2010 was included in paper II. The Crohn’s disease patients included in paper II were identified in previous epidemiological studies conducted in the area.77, 115, 288, 289
Data collection Age- and sex-stratified data on the study population were obtained from Statistics Sweden.287 Medical records of the included patients, from the Department of Gastroenterology, and, if relevant, from the Departments of Surgery, Paediatrics, Infectious Diseases, Clinical Chemistry, and Pa-thology, were evaluated using a standardized case report form including the following key information:
Descriptive epidemiology: - Date of diagnosis, death, and migration. - Demographic information including sex and date of birth.
Exposure: - Start and stop dates of medical treatments and reasons for discon-
tinuation. Outcomes: - Dates of surgical procedures. - Extent of disease at diagnosis and during follow-up, according to
the Montreal classification.28 - Dates of hospital admissions because of ulcerative colitis or infec-
tious diseases. - Haemoglobin levels recorded during the period 2011‒2013 (for pa-
tients included in study II).
40 CARL ERIKSSON Inflammatory Bowel Disease
Paper IV
Patients The Swedish National Quality Registry for Inflammatory Bowel Disease (SWIBREG) is a large, prospectively maintained national quality registry, established in 2005. The purpose of SWIBREG is to continuously improve treatment and follow-up of patients with IBD. Currently, the registry con-tains information on more than 40,000 patients from 45 hospitals, and the national coverage rate is about 60%.290 The list of variables has been up-dated on a regular basis, and includes clinical data such as date of diagno-sis, disease characteristics according to the Montreal classification, sur-gery, endoscopy, prescribed and administered drugs, reasons for drug discontinuation, clinical and biochemical disease activity, and measures of quality of life.290-293 Information is captured both at out-patient visits and at hospital admissions. According to a recent study, the data registered in SWIBREG have high validity with a positive predictive value of 99% for IBD diagnoses.291
Inclusion criteria In paper IV, we used SWIBREG to identify patients with IBD who started on vedolizumab therapy during the inclusion period, 1 June 2014 until 30 May 2015, and to survey the included patients until death, emigration, or the end of follow-up, i.e. June 2016.
Data collection The following information was extracted from SWIBREG:
Descriptive epidemiology: - Date of diagnosis.- Demographic information including sex and date of birth.- Disease characteristics at baseline according to the Montreal classi-
fication.28
Exposure: - Start and stop dates of medical treatments including vedolizumab,
and reasons for discontinuation according to the criteria used inSWIBREG: lack of or loss of response (termination because of pri-mary non-response or secondary loss of response); intolerance (dis-

CARL ERIKSSON Inflammatory Bowel Disease 41
continuation due to side effects including infusion reactions); or other reasons, including pregnancy.
Outcomes: - Clinical disease activity indices including P-HBI and P-SCCAI at
baseline and during follow-up.100, 101 - Results from biochemistry such as CRP and faecal calprotectin lev-
els at baseline and during follow-up.
Statistics Continuous variables that were not normally distributed―including age, disease duration, and biochemical measurements, and also data on an ordinal scale such as clinical disease activity―are presented as median (IQR). Non-parametric methods including the Mann-Whitney U-test were used to compare these variables between groups and Wilcoxon signed-rank test was used to investigate changes in one individual over time.294, 295 Bonferroni correction was used to adjust for multiple comparisons.296 Results from clinical laboratory measurements below the lowest limit of detection (LOD) were generally transformed to LOD/√2.297 Pearson’s chi-squared test (or Fisher’s exact test when appropriate) was performed to compare categorical data such as disease phenotype and previous medica-tion use between groups.298, 299 Life tables and survival plots were con-structed by Kaplan-Meier analysis and the log-rank test was used to com-pare survival data between groups.300, 301 One-sample z-tests were conduct-ed to determine whether observed proportions differed from hypothesized proportions.302 All tests were two-tailed and any p-value of < 0.05 or a 95% confidence interval of a relative risk estimate, not involving 1.0, was considered statistically significant.
Incidence rate In epidemiology, most rates such as incidence, prevalence, and mortality are strongly age-dependent. For example, IBD is commonly diagnosed early in life―during adolescence or early adulthood.113 Since the age struc-ture of a population may change over time and differ considerably be-tween geographic regions, comparisons of age-specific rates may be mis-leading. Thus, several methods for adjusting age-specific rates have been developed. In paper I, the crude age-specific incidence and prevalence were weighted using the characteristics of the Örebro population in 1999 (as the standard population). This method for age-adjustment is termed direct standardization and requires age-specific rates for each stratum of the

42 CARL ERIKSSON Inflammatory Bowel Disease
population. In contrast, indirect standardization can be performed when data are missing from some strata.303 We used the Örebro population of 1999 as the standard population to adjust for changes in population struc-ture over time, while for international comparisons other standard popula-tions―such as the world or European standard populations―might be more appropriate.303, 304
Regression analysis In papers I‒IV, multiple regression models were constructed in order to adjust the observed results for influences of confounding factors. In all regression analyses, covariates were selected on the basis of their potential biological association with the outcome and no statistical methods for variable selection such as forward selection, backward elimination, or stepwise method were applied.305
Binary logistic regression is a model developed by Cox during the 1950s.306 This method can be used to estimate the probability (odds ratio) of a dichotomous outcome, given the values of one or more explanatory variables. Dichotomous means that the outcome variable can take one of two values, “yes” or “no” (e.g. dead or alive), and dichotomous outcomes are common endpoints in medical research. Variables that are not natural-ly binary can often be transformed using a cut-off level. The explanatory variables however, can be ether categorical or continuous. Logistic models use “maximum likelihood estimation” to determine the effect of explana-tory variables on the results.307 This process begins with a tentative solu-tion, then revises it slightly and repeats the process until no more im-provements can be made. In some instances, however, no solution is pos-sible. For example, logistic regression requires that there is little or no multi-colinearity among the independent variables. This means that the explanatory variables should not be to highly correlated to each other. Furthermore, maximum likelihood estimation requires a large sample size. A widely used guideline states that at least 10 cases with the outcome per every explanatory variable are necessary to achieve consistent results.308
Cox proportional hazard regression is a method for investigating the ef-fect of explanatory variables on the time to a specified event, the “survival time”. In this type of analysis, it is uncommon that the event of interest is observed in all subjects, so individuals without events are censored at the end of follow-up. When censoring individual subjects, it is important to make sure that the continuation of follow-up does not depend on a partic-ipant’s medical condition. The distribution of survival time is often un-

CARL ERIKSSON Inflammatory Bowel Disease 43
known and may vary depending on the outcome of interest. To deal with this problem, Cox demonstrated in 1972 that if the effect of a predictor on the survival time is constant over time, i.e. the proportional hazard as-sumption holds, no assumptions regarding the distribution of survival times is necessary.309 The proportional hazard assumption can be tested visually from Kaplan-Meier curves and, additionally, there are several statistical methods that can be used to verify the assumption, including testing the significance of time-dependent covariates and plotting Schoen-feld residuals.310 The output of a Cox regression model is a hazard ratio for each explanatory variable and, as in logistic regression, the model is fitted by maximum likelihood estimation. Poisson regression was introduced by von Bortkiewicz in 1898, and is an appropriate method when data is a count of events, particularly rare events―for example, the number of new IBD patients during a period of time, in a specified geographical region. However the method is named after the French mathematician Poisson, who derived the mathematical form of the distribution. As with logistic regression and Cox regression, estimation of the influence of explanatory variables is done using maxi-mum likelihood and the output from a Poisson regression is an incidence rate ratio.311 All statistical analyses in this thesis were performed using SPSS version 22 (IBM Corporation, Armonk, NY, 2013) or STATA version 14 SE (Stata Corporation, College Station, TX, 2013)
44 CARL ERIKSSON Inflammatory Bowel Disease
Results
Paper I
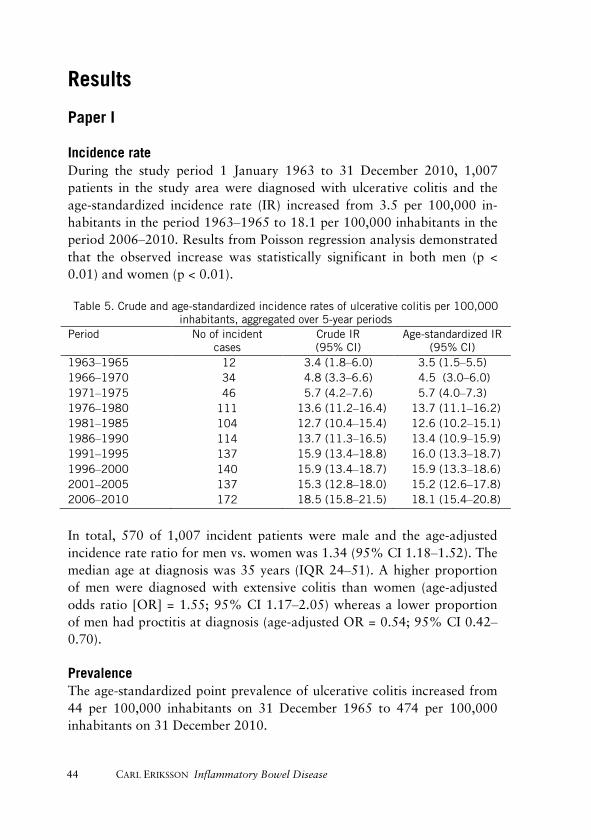
Incidence rate During the study period 1 January 1963 to 31 December 2010, 1,007 patients in the study area were diagnosed with ulcerative colitis and the age-standardized incidence rate (IR) increased from 3.5 per 100,000 in-habitants in the period 1963‒1965 to 18.1 per 100,000 inhabitants in the period 2006‒2010. Results from Poisson regression analysis demonstrated that the observed increase was statistically significant in both men (p < 0.01) and women (p < 0.01).
Table 5. Crude and age-standardized incidence rates of ulcerative colitis per 100,000 inhabitants, aggregated over 5-year periods
Period No of incident cases
Crude IR (95% CI)
Age-standardized IR (95% CI)
1963‒1965 12 3.4 (1.8‒6.0) 3.5 (1.5‒5.5) 1966‒1970 34 4.8 (3.3‒6.6) 4.5 (3.0‒6.0) 1971‒1975 46 5.7 (4.2‒7.6) 5.7 (4.0‒7.3) 1976‒1980 111 13.6 (11.2‒16.4) 13.7 (11.1‒16.2) 1981‒1985 104 12.7 (10.4‒15.4) 12.6 (10.2‒15.1) 1986‒1990 114 13.7 (11.3‒16.5) 13.4 (10.9‒15.9) 1991‒1995 137 15.9 (13.4‒18.8) 16.0 (13.3‒18.7) 1996‒2000 140 15.9 (13.4‒18.7) 15.9 (13.3‒18.6) 2001‒2005 137 15.3 (12.8‒18.0) 15.2 (12.6‒17.8) 2006‒2010 172 18.5 (15.8‒21.5) 18.1 (15.4‒20.8)
In total, 570 of 1,007 incident patients were male and the age-adjusted incidence rate ratio for men vs. women was 1.34 (95% CI 1.18‒1.52). The median age at diagnosis was 35 years (IQR 24‒51). A higher proportion of men were diagnosed with extensive colitis than women (age-adjusted odds ratio [OR] = 1.55; 95% CI 1.17‒2.05) whereas a lower proportion of men had proctitis at diagnosis (age-adjusted OR = 0.54; 95% CI 0.42‒0.70).
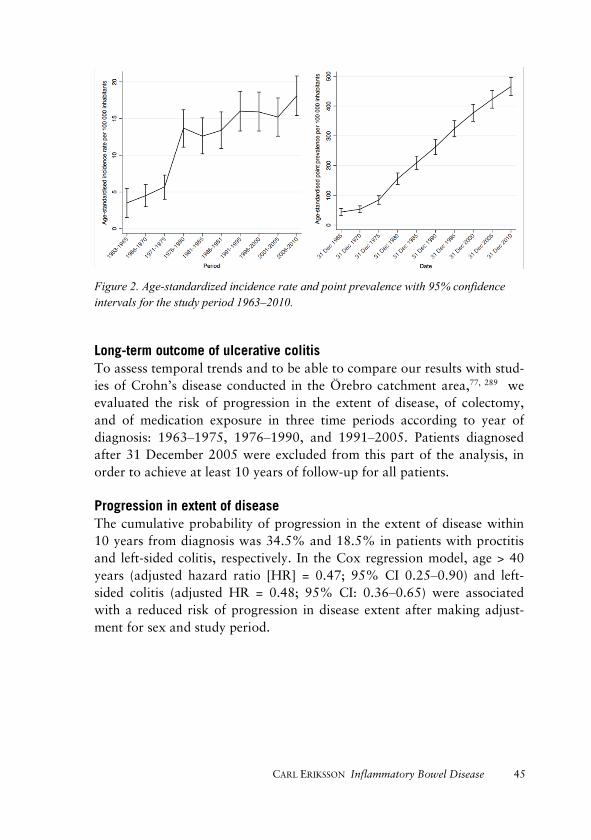
Prevalence The age-standardized point prevalence of ulcerative colitis increased from 44 per 100,000 inhabitants on 31 December 1965 to 474 per 100,000 inhabitants on 31 December 2010.
CARL ERIKSSON Inflammatory Bowel Disease 45
Figure 2. Age-standardized incidence rate and point prevalence with 95% confidence intervals for the study period 1963‒2010.
Long-term outcome of ulcerative colitis To assess temporal trends and to be able to compare our results with stud-ies of Crohn’s disease conducted in the Örebro catchment area,77, 289 we evaluated the risk of progression in the extent of disease, of colectomy, and of medication exposure in three time periods according to year of diagnosis: 1963‒1975, 1976‒1990, and 1991‒2005. Patients diagnosed after 31 December 2005 were excluded from this part of the analysis, in order to achieve at least 10 years of follow-up for all patients.
Progression in extent of disease The cumulative probability of progression in the extent of disease within 10 years from diagnosis was 34.5% and 18.5% in patients with proctitis and left-sided colitis, respectively. In the Cox regression model, age > 40 years (adjusted hazard ratio [HR] = 0.47; 95% CI 0.25‒0.90) and left-sided colitis (adjusted HR = 0.48; 95% CI: 0.36‒0.65) were associated with a reduced risk of progression in disease extent after making adjust-ment for sex and study period.
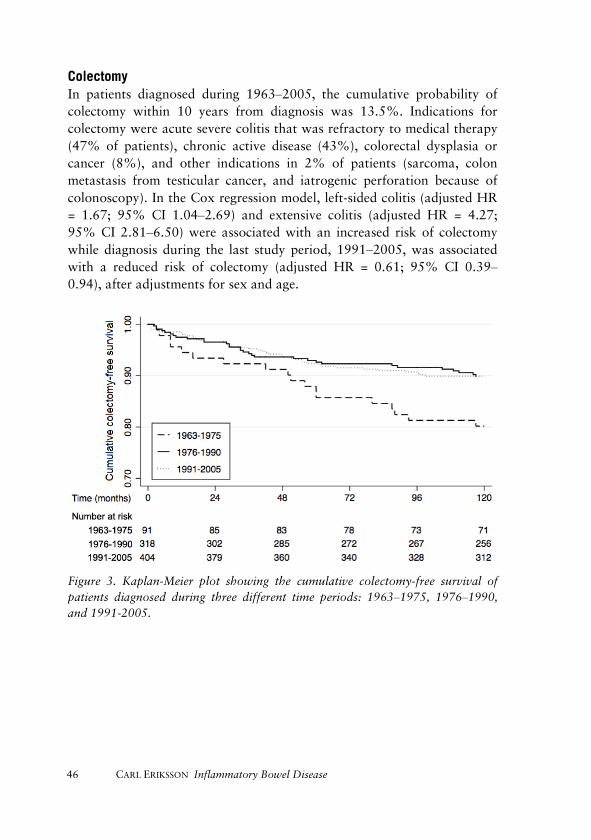
46 CARL ERIKSSON Inflammatory Bowel Disease
Colectomy In patients diagnosed during 1963‒2005, the cumulative probability of colectomy within 10 years from diagnosis was 13.5%. Indications for colectomy were acute severe colitis that was refractory to medical therapy (47% of patients), chronic active disease (43%), colorectal dysplasia or cancer (8%), and other indications in 2% of patients (sarcoma, colon metastasis from testicular cancer, and iatrogenic perforation because of colonoscopy). In the Cox regression model, left-sided colitis (adjusted HR = 1.67; 95% CI 1.04‒2.69) and extensive colitis (adjusted HR = 4.27; 95% CI 2.81‒6.50) were associated with an increased risk of colectomy while diagnosis during the last study period, 1991‒2005, was associated with a reduced risk of colectomy (adjusted HR = 0.61; 95% CI 0.39‒0.94), after adjustments for sex and age.
Figure 3. Kaplan-Meier plot showing the cumulative colectomy-free survival of patients diagnosed during three different time periods: 1963‒1975, 1976‒1990, and 1991-2005.
CARL ERIKSSON Inflammatory Bowel Disease 47
Temporal trends in medical therapy Between the two earliest study periods, 1963‒1975 and 1976‒1990, there was a significant increase in the cumulative probability of receiving oral 5-aminosalicylates (79% vs. 92%; p < 0.01) and corticosteroids (37% vs. 70%; p < 0.01) within 10 years of diagnosis. Thiopurines were introduced in selected cases during the 1980s and an increasing probability of receiv-ing thiopurines within 10 years was observed between the two most recent study periods (7% vs. 34%; p < 0.01). The first anti-TNF agent, inflixi-mab, was approved in 2005 and 9% of patients diagnosed during the last study period received anti-TNF within 10 years from diagnosis.
Paper II
Patients A random sample of 342 IBD patients, diagnosed with Crohn’s disease (n = 171) or ulcerative colitis (n = 171) in the period 1963‒2010 and resident in the Örebro University Hospital catchment area on 31 December 2010, was obtained from the IBD cohort of Örebro University Hospital.77, 289, 312 One hundred and seventy-seven (52%) of the patients were male, the me-dian age was 57 years (IQR 41‒66), and the corresponding disease dura-tion was 19 years (IQR 9‒31).
Table 6. Indications for colectomy, according to study period
Period 1 (1963‒1975)
No. (%)
Period 2 (1976‒1990)
No. (%)
Period 3 (1991‒2005)
No. (%) Acute severe colitis 9 (26) 31 (48) 35 (58)
Chronic active disease 23 (66) 26 (41) 20 (33)
Colorectal dysplasia or cancer 3 (8) 5 (8) 4 (7)
Other indications 0 (0) 2 (3) 1 (2)
Chi-squared test for trend, p = 0.04.
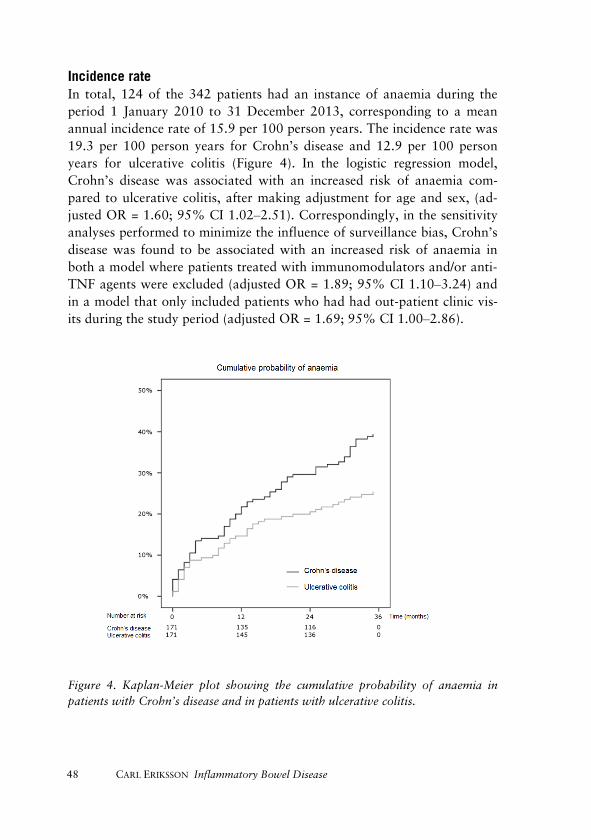
48 CARL ERIKSSON Inflammatory Bowel Disease
Incidence rate In total, 124 of the 342 patients had an instance of anaemia during the period 1 January 2010 to 31 December 2013, corresponding to a mean annual incidence rate of 15.9 per 100 person years. The incidence rate was 19.3 per 100 person years for Crohn’s disease and 12.9 per 100 person years for ulcerative colitis (Figure 4). In the logistic regression model, Crohn’s disease was associated with an increased risk of anaemia com-pared to ulcerative colitis, after making adjustment for age and sex, (ad-justed OR = 1.60; 95% CI 1.02‒2.51). Correspondingly, in the sensitivity analyses performed to minimize the influence of surveillance bias, Crohn’s disease was found to be associated with an increased risk of anaemia in both a model where patients treated with immunomodulators and/or anti-TNF agents were excluded (adjusted OR = 1.89; 95% CI 1.10‒3.24) and in a model that only included patients who had had out-patient clinic vis-its during the study period (adjusted OR = 1.69; 95% CI 1.00‒2.86).
Figure 4. Kaplan-Meier plot showing the cumulative probability of anaemia in patients with Crohn’s disease and in patients with ulcerative colitis.
CARL ERIKSSON Inflammatory Bowel Disease 49
Period prevalence Overall, 76 patients had an episode of anaemia during 2013, correspond-ing to a period prevalence of 22.6%. For Crohn’s disease, the prevalence was 28.7% as compared to 16.5% for ulcerative colitis. In the logistic regression model, Crohn’s disease was found to be associated with an increased risk of anaemia, after making adjustment for age and sex (ad-justed OR = 2.04; 95% CI 1.20‒3.46). The association between Crohn’s disease and increased risk of anaemia remained in both a model where patients treated with immunomodulators and/or anti-TNF agents were excluded (adjusted OR = 1.96; 95% CI 1.03‒3.37) and in a model that only included patients who had had out-patient clinic visits during the study period (adjusted OR = 2.25; 95% CI 1.22‒4.14).
Risk factors for anaemia Cox proportional hazard regression was used in the assessment of risk factors for anaemia. For Crohn’s disease, stricturing disease behaviour was found to be associated with an increased risk of anaemia (adjusted HR = 2.59; 95% CI 1.00‒6.79), after making adjustment for sex, disease dura-tion, disease location, and past bowel surgery. For ulcerative colitis, exten-sive disease was found to be associated with a higher risk of anaemia (ad-justed HR = 2.40; 95% CI 1.10‒5.36), after making adjustment for sex, disease duration, and past colectomy.
Treatment and outcome of anaemia In total, 51 (41%) of the 124 patients who were diagnosed with anaemia during the study period received supplementation therapy (oral iron, n = 18; iron intravenously, n = 22; oral folic acid, n = 3; or oral vitamin B12, n = 8) and eight patients received a blood transfusion within 3 months of diagnosis of anaemia. Similarly, 42 patients (34%) received intensified anti-inflammatory treatment (introduction or dose optimization of oral 5-aminosalicylates, n = 8; immunomodulators, n = 15; anti-TNF, n = 4; leukocyte apheresis, n = 1; or corticosteroids, n = 14). However, none of the patients were treated with erythropoietin, and 42 (36%) of the pa-tients diagnosed with anaemia received no treatment at all within 3 months.
Repeated measurement of haemoglobin was performed 12 months after the diagnosis of anaemia in 123 of the 124 patients, and at this point 80 (65%) had a restored haemoglobin level. Although, Crohn’s disease pa-tients received more specific therapy (supplementation or anti-
50 CARL ERIKSSON Inflammatory Bowel Disease
inflammatory therapy) than patients with ulcerative colitis (72% vs. 55%; p = 0.05), Crohn’s disease was associated with a worse prognosis than ulcerative colitis in terms of resolution of anaemia within 12 months (56% vs. 75%; p = 0.03). Correspondingly, females received more specific ther-apy than males (73% vs. 56%; p = 0.05) and were more likely to have resolution of the anaemia within 12 months (75% vs. 54%; p = 0.02)
Paper III
Patients Of the 1,007 patients who were diagnosed with ulcerative colitis in the period 1963‒2010 in the catchment area of Örebro University Hospital, 253 patients had received at least one dose of a thiopurine drug before the end of follow-up on 31 December 2015 and were included in this study.312 Within 12 months of commencement, 76 of the 253 (30%) stopped thera-py because of intolerance, whereas 177 patients continued treatment or stopped for other reasons. Fifty-eight percent of the patients included were male, the median age was 30 years (IQR 21‒42), and the median disease duration was 2 years (IQR 0‒6) at baseline, i.e. initiation of first thiopu-rine drug. There were no significant differences between the two groups in terms of age, sex, smoking habits, family history of IBD, disease duration, extent of disease, hospital admission at diagnosis, or previous medical or surgical treatment at baseline.
Colectomy The cumulative probability of colectomy within 10 years was 19.5% in patients who tolerated thiopurines, as compared to 29.0% in patients who stopped treatment because of intolerance. In the Cox regression analysis, thiopurine tolerance was found to be associated with a reduced risk of colectomy (adjusted HR = 0.39; 95% CI 0.21‒0.73) after making adjust-ment for sex, age, extent of disease, previous medical or surgical therapy, hospital admission at diagnosis, and year of thiopurine initiation in 5-year intervals.
Hospital admission The cumulative probability of hospital admission because of ulcerative colitis or ulcerative colitis-related conditions within 10 years of first thio-purine exposure was 34.0% in tolerant patients as compared to 56.2% in

CARL ERIKSSON Inflammatory Bowel Disease 51
patients who discontinued treatment due to adverse drug reactions. In the Cox regression model, thiopurine tolerance was found to be associated with a reduced risk of hospital admission (adjusted HR = 0.36; 95% CI 0.23‒0.56) after making adjustment for sex, age, extent of disease, previ-ous medical or surgical therapy, hospital admission at diagnosis, and year of thiopurine initiation in 5-year intervals.
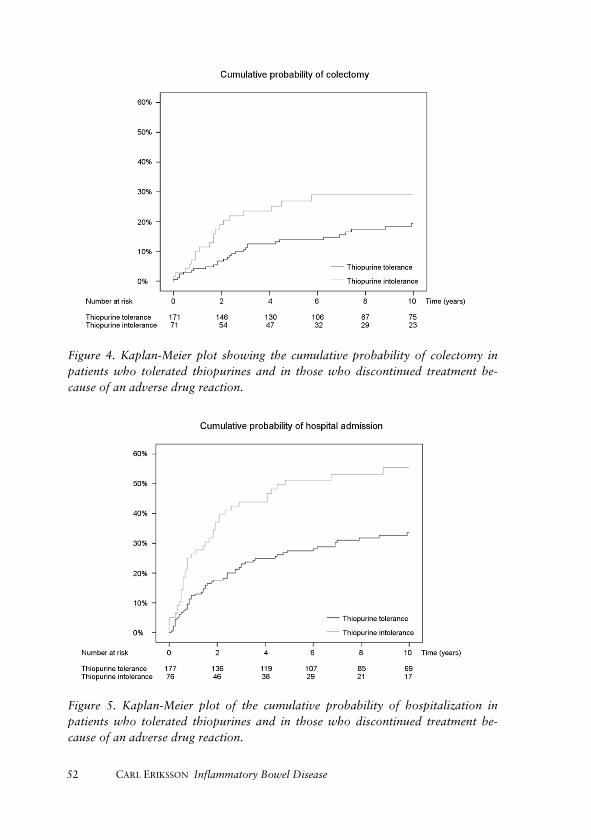
52 CARL ERIKSSON Inflammatory Bowel Disease
Figure 4. Kaplan-Meier plot showing the cumulative probability of colectomy in patients who tolerated thiopurines and in those who discontinued treatment be-cause of an adverse drug reaction.
Figure 5. Kaplan-Meier plot of the cumulative probability of hospitalization in patients who tolerated thiopurines and in those who discontinued treatment be-cause of an adverse drug reaction.

CARL ERIKSSON Inflammatory Bowel Disease 53
Progression in extent of disease The risk of progression in the extent of disease within 10 years in thiopu-rine-tolerant patients with proctitis or left-sided colitis was 20.4%, and the corresponding figure in intolerant patients was 48.8%. Cox regression analysis gave an adjusted HR of 0.45 (95% CI 0.21‒0.97) for disease progression in thiopurine-tolerant patients, after making adjustment for sex, age, extent of disease, previous medical or surgical therapy, hospital admission at diagnosis, and year of thiopurine initiation in 5-year inter-vals.
Figure 6. Kaplan-Meier plot showing the cumulative probability of progression in the extent of disease in patients with ulcerative proctitis or left-sided colitis who tolerated thiopurines and in those who discontinued treatment because of an ad-verse drug reaction.
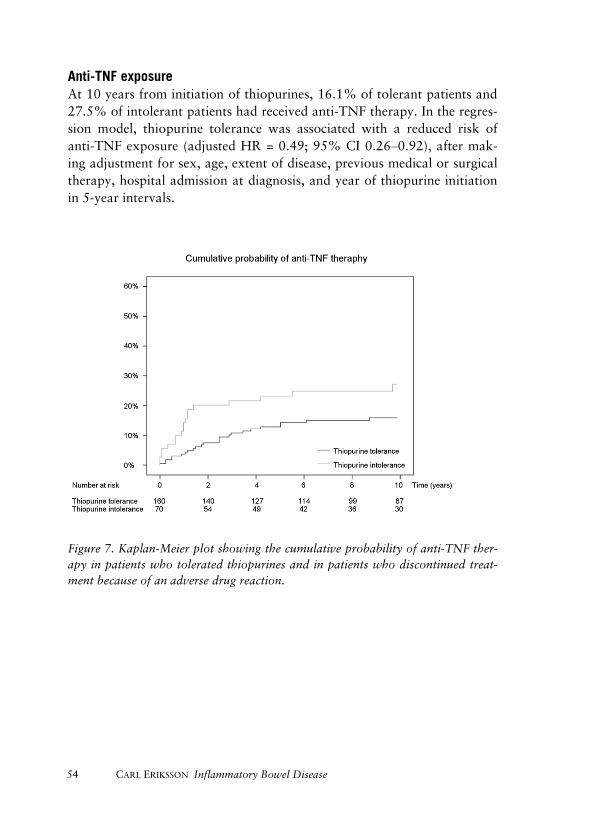
54 CARL ERIKSSON Inflammatory Bowel Disease
Anti-TNF exposure At 10 years from initiation of thiopurines, 16.1% of tolerant patients and 27.5% of intolerant patients had received anti-TNF therapy. In the regres-sion model, thiopurine tolerance was associated with a reduced risk of anti-TNF exposure (adjusted HR = 0.49; 95% CI 0.26‒0.92), after mak-ing adjustment for sex, age, extent of disease, previous medical or surgical therapy, hospital admission at diagnosis, and year of thiopurine initiation in 5-year intervals.
Figure 7. Kaplan-Meier plot showing the cumulative probability of anti-TNF ther-apy in patients who tolerated thiopurines and in patients who discontinued treat-ment because of an adverse drug reaction.
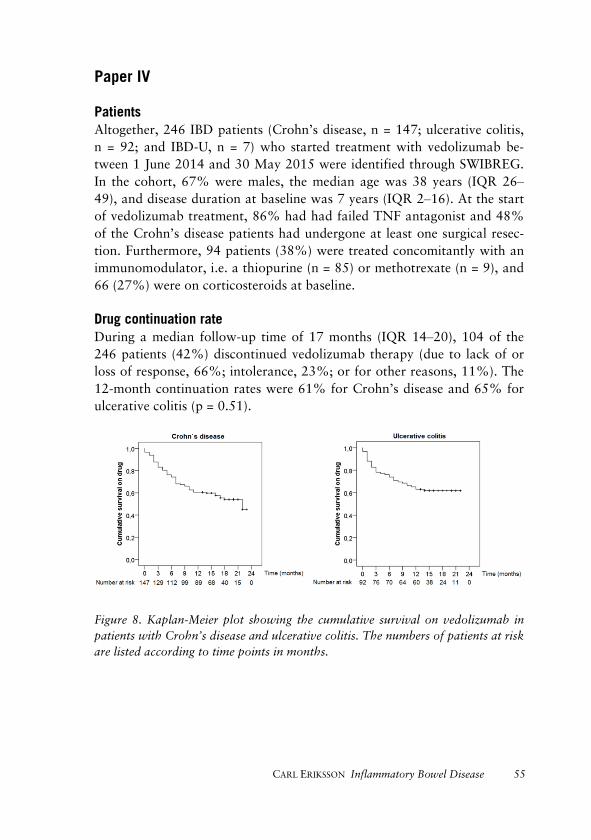
CARL ERIKSSON Inflammatory Bowel Disease 55
Paper IV
Patients Altogether, 246 IBD patients (Crohn’s disease, n = 147; ulcerative colitis, n = 92; and IBD-U, n = 7) who started treatment with vedolizumab be-tween 1 June 2014 and 30 May 2015 were identified through SWIBREG. In the cohort, 67% were males, the median age was 38 years (IQR 26‒49), and disease duration at baseline was 7 years (IQR 2‒16). At the start of vedolizumab treatment, 86% had had failed TNF antagonist and 48% of the Crohn’s disease patients had undergone at least one surgical resec-tion. Furthermore, 94 patients (38%) were treated concomitantly with an immunomodulator, i.e. a thiopurine (n = 85) or methotrexate (n = 9), and 66 (27%) were on corticosteroids at baseline.
Drug continuation rate During a median follow-up time of 17 months (IQR 14‒20), 104 of the 246 patients (42%) discontinued vedolizumab therapy (due to lack of or loss of response, 66%; intolerance, 23%; or for other reasons, 11%). The 12-month continuation rates were 61% for Crohn’s disease and 65% for ulcerative colitis (p = 0.51).
Figure 8. Kaplan-Meier plot showing the cumulative survival on vedolizumab in patients with Crohn’s disease and ulcerative colitis. The numbers of patients at risk are listed according to time points in months.
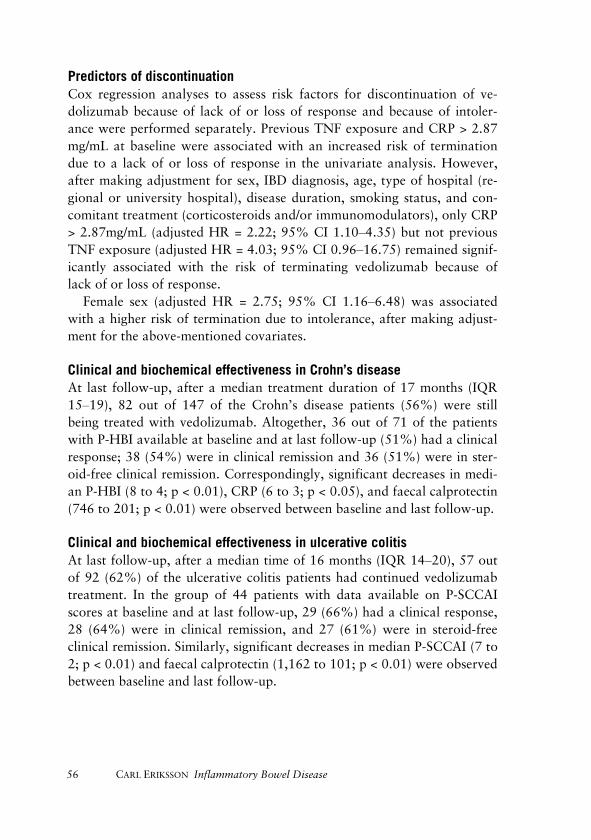
56 CARL ERIKSSON Inflammatory Bowel Disease
Predictors of discontinuation Cox regression analyses to assess risk factors for discontinuation of ve-dolizumab because of lack of or loss of response and because of intoler-ance were performed separately. Previous TNF exposure and CRP > 2.87 mg/mL at baseline were associated with an increased risk of termination due to a lack of or loss of response in the univariate analysis. However, after making adjustment for sex, IBD diagnosis, age, type of hospital (re-gional or university hospital), disease duration, smoking status, and con-comitant treatment (corticosteroids and/or immunomodulators), only CRP > 2.87mg/mL (adjusted HR = 2.22; 95% CI 1.10‒4.35) but not previousTNF exposure (adjusted HR = 4.03; 95% CI 0.96‒16.75) remained signif-icantly associated with the risk of terminating vedolizumab because oflack of or loss of response.
Female sex (adjusted HR = 2.75; 95% CI 1.16‒6.48) was associated with a higher risk of termination due to intolerance, after making adjust-ment for the above-mentioned covariates.
Clinical and biochemical effectiveness in Crohn’s disease At last follow-up, after a median treatment duration of 17 months (IQR 15‒19), 82 out of 147 of the Crohn’s disease patients (56%) were still being treated with vedolizumab. Altogether, 36 out of 71 of the patients with P-HBI available at baseline and at last follow-up (51%) had a clinical response; 38 (54%) were in clinical remission and 36 (51%) were in ster-oid-free clinical remission. Correspondingly, significant decreases in medi-an P-HBI (8 to 4; p < 0.01), CRP (6 to 3; p < 0.05), and faecal calprotectin (746 to 201; p < 0.01) were observed between baseline and last follow-up.
Clinical and biochemical effectiveness in ulcerative colitis At last follow-up, after a median time of 16 months (IQR 14‒20), 57 out of 92 (62%) of the ulcerative colitis patients had continued vedolizumab treatment. In the group of 44 patients with data available on P-SCCAI scores at baseline and at last follow-up, 29 (66%) had a clinical response, 28 (64%) were in clinical remission, and 27 (61%) were in steroid-free clinical remission. Similarly, significant decreases in median P-SCCAI (7 to 2; p < 0.01) and faecal calprotectin (1,162 to 101; p < 0.01) were observed between baseline and last follow-up.
CARL ERIKSSON Inflammatory Bowel Disease 57
Discussion Despite the great variation in occurrence of IBD geographically and in spite of reports indicating a plateau or even a decline in some parts of Europe,133, 313-315 data from the Örebro region―including the results of paper I―show a clear increase in both the incidence and the prevalence of IBD in the area over the past 50 years.115, 119, 288, 289 Our findings, which are supported by some recent Scandinavian studies including reports from the neighbouring county of Uppsala,118, 316-319 indicate that the total number of IBD patients in Sweden already exceeds 70,000 and that this number will continue to grow during the next few decades as IBD is diagnosed primari-ly in young individuals, since the mortality is low and there is no cure.
The growing number of IBD patients will pose a significant challenge to gastroenterologists and gastrointestinal surgeons in Sweden, which may necessitate innovations in healthcare delivery to meet the increasing de-mand. However, just in the last few years the pharmacological armamen-tarium of IBD has been augmented with several new biological agents, and many new therapies, targeting novel pathogenic pathways, are under de-velopment.320, 321 Short-term follow-up of participants in clinical trials supports the idea that anti-TNF therapy is associated with a reduced risk of surgery, a reduced risk of hospital admission, and better quality of life in IBD patients, compared to conventional treatment.99, 322 In the future, having a number of drugs with different mechanisms of action available may allow clinicians to customize therapy for the individual patient. This new paradigm of IBD management will possibly have far-reaching impli-cations―not only for patients and clinicians, but also for society as a whole.
On the other hand, numerous questions remain regarding the optimal use of the therapies that are already on the market. Traditionally, the ap-proach to managing active IBD has been based on progressive intensifica-tion of medical treatment as symptoms become worse.323, 324 In recent years, however, a top-down approach in medical therapy has been intro-duced for patients with risk factors for a severe outcome already at diag-nosis.325, 326 It also appears that treatment targeting the underlying inflam-mation in terms of biomarkers and endoscopic findings is more effective than traditional management, aimed at the control of symptoms only.327
More aggressive treatment algorithms, including combination of drug therapies, and more ambitious goals with the treatment may, however, be associated with increased toxicity. Unfortunately, clinical trials are rarely
58 CARL ERIKSSON Inflammatory Bowel Disease
designed to study long-term events such as uncommon but potentially life-threating side effects.328 For example, the risk of progressive multifocal leukoencephalopathy, which affects about four per cent of patients ex-posed to the integrin antagonist natalizumab, was not detected in the piv-otal trials.329-332 This severe viral disease of the central nervous system has a 6-month mortality rate of 25% and highlights the importance of large observational studies with long-term observation periods to assess the safety and clinical effectiveness of new pharmacological treatments.333
In paper IV we found that vedolizumab, another integrin antagonist that is gut-selective, appears to be well tolerated and effective in Swedish clinical practice. However, previous exposure to anti-TNF agents and elevated CRP at start of treatment were associated with a less favourable clinical response, and women were more likely to discontinue therapy because of intolerance.
Given that complications of IBD, such as disease progression or events necessitating a surgical resection, often arise after years of disease, another advantage of observational studies with a long duration of follow-up is the possibility to investigate outcome measures other than the endpoints commonly used in clinical trials.
In paper I, we observed that patients diagnosed with ulcerative colitis during the last study period, 1991‒2005, had a reduced risk of colectomy compared to patients diagnosed during the first study period, 1963‒1975. This finding is supported by recent Danish observational studies and also by a meta-analysis of population-based studies of patients diagnosed be-tween 1955 and 2006.70, 76, 334 Interestingly, we observed that the reduction in colectomies was temporally associated with increased use of thiopurines and anti-TNF agents, but this finding should be interpreted with caution, since associations were at the group level only.
The aim of paper III was to further investigate the long-term effect of thiopurine drugs on the disease course and risk of colectomy in ulcerative colitis. However, the fact that patients exposed to thiopurines represent a treatment-refractory group challenges the assessment of the long-term effectiveness of thiopurines in a real-world setting, since the thiopurine-exposed population has a different risk of colectomy and other long-term outcomes compared to the general ulcerative colitis population.335
In order to avoid differential bias due to confounding by indication, a novel study approach was adopted. We only included patients exposed to thiopurines, and compared patients who stopped treatment because of adverse drug reactions within 12 months from initiation of treatment with

CARL ERIKSSON Inflammatory Bowel Disease 59
patients who continued treatment or who discontinued the therapy for other reasons. Using this method, we observed that thiopurine therapy is associated with a reduced risk of colectomy and that these drugs have a profound beneficial effect on the natural history of the disease. Perhaps increased and earlier use of thiopurine drugs may explain the decrease in colectomies seen in the catchment area of Örebro University Hospital in 1991‒2005.
Although the occurrence of IBD has been studied in many parts of the world during the latter part of the twentieth century, there have only been a few continuous surveys with a total observation time of more than 50 years:113 ulcerative colitis in Uppsala, 1945‒2007; ulcerative colitis and Crohn’s disease in Olmsted county, 1940‒2000; and Crohn’s disease in Cardiff, 1931‒2005.118, 132, 336 The Örebro region has a long tradition of epidemiological studies of IBD, and the incidence and prevalence of ulcer-ative colitis have previously been studied over two time periods, 1939‒1958 and 1963‒1987.119, 288 In addition, the epidemiology of Crohn’s dis-ease has been reported for the period 1963‒2010 and that of microscopic colitis for the period 1984‒2008.289, 337 Having a well-characterized popu-lation-based cohort of patients covering the whole spectrum of IBD, fol-lowed up during many years, allows almost endless possibilities for per-forming further research.
In paper II, we studied the incidence and prevalence of anaemia in a randomized subset of patients with established IBD allocated from the entire IBD cohort. We found that anaemia is a common complication even beyond the first years after diagnosis of IBD. The risk of developing anaemia was higher in Crohn’s disease than in ulcerative colitis. Interest-ingly, the prognosis of anaemia in terms of resolution within 12 months was also worse in Crohn’s disease. Unfortunately, the study also indicated that despite current guidelines, many patients did not receive adequate therapy.338 The risk factors for anaemia, stricturing behaviour in Crohn’s disease, and extensive disease in ulcerative colitis should be recognized and current treatment guidelines should be better implemented in clinical practice.
Methodological considerations Randomized controlled trails (RCTs) are generally regarded to be the best source of medical data on the effects of clinical interventions.339 However, RCTs are unethical for testing the causes of disease, and cannot be used to quantify the occurrence of a disease in a population. Cohort studies are
60 CARL ERIKSSON Inflammatory Bowel Disease
the best available substitute when an RCT would be inappropriate or im-possible.340
A cohort is a group of individuals who share a defining characteristic, e.g. people who live in the same area or have a specific disease. At the startof a study, participants are divided into groups depending on exposure.The subjects are then followed up over a period of time to determine theproportion in each group who develop the outcome of interest.
Cohort studies are either prospective (where participants are followed up forward from the present) or retrospective (where participants are fol-lowed up from a date in the past). Prospective cohort studies are generally expensive and time consuming whereas retrospective studies are not.340 All the papers in the current thesis describe retrospective cohort studies, alt-hough the capture of data was prospective and based on medical records (papers I‒III) or registry data (paper IV).
Bias and random error There are two broad types of errors in medical research: random error and systematic error. Random error is a difference between the observed value and the true value that is due to chance or imprecise measurement. Ran-dom errors can be reduced by increasing the sample size or averaging of multiple measurements. A confidence interval can be computed from the observed data to estimate the interference of random variation, and statis-tical methods may be applied in hypothesis testing.341 Type-II error occurs when a hypothesis is rejected even though the hypothesis is true, and the power of the test expresses the probability of committing a type-II error. (The power is determined by the sample size, the precision with which the data are measured, and the magnitude of the effect or difference of inter-est). Type-I error occurs when the hypothesis is not rejected even though it was false, and the risk of committing a type-I error is determined by the significance level (p-value).342
Bias is a systematic error i.e. results have been obtained that consistent-ly deviate from the truth (by under- or over-estimation). Bias cannot be eliminated by increasing the sample size. Instead, it is minimized by proper study design and conduction of the study. There are virtually dozens of types of bias that might distort the estimation of a scientific measure,343 although two general types are important to remember: selection bias and information bias. Selection bias is error because of systematic differences between individuals who take part in a study and those who do not, while information bias arises from inaccurate measurement of exposures and
CARL ERIKSSON Inflammatory Bowel Disease 61
outcomes.344 Bias in a study does not necessarily mean that the conclusion of the study should be disregarded. However, the impact of systematic errors on the study results and the methods used to minimize the influence of bias should be openly presented.
Confounding A confounding factor is independently associated with both the exposure and the outcome of a test, and should always be considered as a possible explanation for an observed association. In non-randomized studies, the influence of confounding can be reduced by proper study design and by adjustments for potential confounders using methods such as regression analysis. However, only known and measured confounders can be adjust-ed for.344
Validity For a study to be regarded as valid, it must be shown that the conclusions of the study can be logically drawn from the results and that the results are based on an appropriate methodology. Internal validity reflects the extent to which a conclusion is correct for the participants of a study and may be threatened by bias, confounding, and random error. External va-lidity relates to the value of the conclusion to other populations (generali-zability).345
Limitations A main limitation of all the studies in this thesis was the retrospective study design, i.e. the studies were conducted after the events of interest had already occurred. In studies I‒III, data were extracted from medical records whereas in study IV information was obtained from the Swedish national quality registry for IBD (SWIBREG). Thus, data on relevant ex-posures and outcomes were collected from existing records and were not originally gathered to answer our specific research questions.
In paper I, patients with ulcerative colitis were identified by assessment of all medical records in the private archive of the Department of Gastro-enterology, Örebro University Hospital, amended by computerized search in digital records. Since there are no private gastroenterologists in the area, and as all colonoscopies and histopathological examinations are per-formed at the University Hospital, we believe that our ability to detect patients diagnosed with ulcerative colitis during the study period was good. However, we cannot exclude the possibility that patients with an
62 CARL ERIKSSON Inflammatory Bowel Disease
indolent disease and few episodes of inflammation were more often over-looked in the early part of the study period. Correspondingly, the retro-spective study design did not allow the assessment of disease activity and other potentially interesting covariates, such as smoking habits over time. On the other hand, one advantage of the retrospective ascertainment of data and the follow-up of all patients until 31 December 2015 was the possibility of correcting the diagnosis, based on information recorded later during the follow-up period. As a consequence of these limitations, we may have underestimated the incidence of ulcerative colitis during the first study period, 1963‒1975. Correspondingly, the reduced risk of colectomy observed between the periods 1963‒1975 and 1991‒2005 may to some extent be artificial, reflecting improved detection of patients with indolent disease in recent years. However, the proportion of patients who were colectomised because of acute severe ulcerative colitis that was refractory to steroids (Table 6) was stable over the study period, and there was no significant change in the proportion of patients with extensive colitis at diagnosis during the study period, suggesting that the method used for case ascertainment was valid. Unfortunately, data on hospital admission at the time of diagnosis, which could have been used as a surrogate marker of disease severity at presentation, were not recorded.
In paper II, we examined the incidence and prevalence of anaemia in a randomized subset of IBD patients, obtained from the entire Örebro IBD cohort and consisting of (1) patients with ulcerative colitis identified in paper I and (2) Crohn’s disease patients identified through corresponding studies of Crohn’s disease in Örebro, 1963‒2010.77, 115, 289 IBD patients with anaemia may often present with unspecific symptoms such as fatigue, pallor, and dyspnea on exertion, although patients with mild anaemia may be asymptomatic.346 During the study period 1 January 2011 to 31 De-cember 2013, haemoglobin levels were measured in 332 of 342 (97%) of the patients included, with a median of 6 (2‒13) samples per individual. Despite the large number of haemoglobin measurements, the incidence and prevalence estimates may have been influenced by bias―and since patients without haemoglobin measurements were considered non-anaemic, we may have underestimated the true occurrence. At the De-partment of Gastroenterology, Örebro University Hospital, patients with second-line IBD therapy (i.e. immunomodulators and anti-TNF agents) are followed with blood sampling―including haemoglobin measure-ment―every third month, while patients without these medications are followed less rigorously. To confirm that the occurrence of anaemia was
CARL ERIKSSON Inflammatory Bowel Disease 63
increased in Crohn’s disease compared to ulcerative colitis, we performed subgroup analysis with patients on second-line therapy excluded, and by only including patients with out-patient clinic visits during the study peri-od.
In order to include an adequate number of patients in this study, a power calculation was performed. However, the power analysis was used to calculate the minimum sample size required to detect a difference in the occurrence of anaemia between patients with Crohn’s disease and patients with ulcerative colitis in the overall study population. The study was pos-sibly under-powered for assessment of risk factors for anaemia and also for the subgroup analyses that were performed.
All patients diagnosed with ulcerative colitis within the catchment area of Örebro University Hospital in 1963‒2010 who were treated with thio-purine drugs at any time during their disease course were included in pa-per III. Patients who stopped therapy within 12 months because of an adverse drug reaction were compared with patients who continued the therapy or stopped for other reasons. Generally, it was not difficult to classify patients into these two groups based on information from medical records.
The main limitation of this study is probably that no patients diagnosed after 31 December 2010 were included. The first anti-TNF agent, inflixi-mab, was approved for maintenance therapy of ulcerative colitis in 2005; this was followed by adalimumab in 2012 and by golimumab in 2013.99,
347-350 Furthermore, the integrin antagonist vedolizumab became available during 2014.351 Biological therapies have markedly improved the medical management of ulcerative colitis in patients who do not respond to or do not tolerate conventional treatment. Since the availability of other treat-ment options in thiopurine-intolerant patients have varied over time, all main analyses in the study were adjusted for the year of thiopurine initia-tion in 5-year intervals. Despite this, most of the study period was during the pre-biologic era, and the study may have over-estimated the impact of thiopurines in the medical management of ulcerative colitis in 2018.
In paper IV, SWIBREG was used to identify patients who had received vedolizumab treatment in Swedish routine care at any time since the ap-proval (in June 2014) until 30 May 2015. The reason for not including patients who started on vedolizumab after this time was that these patients were included in a prospective study being run through the registry.
SWIBREG contains information from a broad sample of hospitals and has a national coverage rate of about 60%, although we believe that the
64 CARL ERIKSSON Inflammatory Bowel Disease
coverage is even better for some subgroups of patients―such as patients on biologic treatment. Data are prospectively recorded at acute referrals, at hospital admissions, and at scheduled appointments. Although the cov-erage of SWIBREG is not 100%, we believe that the study population in study IV was fairly representative of the vedolizumab-treated patient pop-ulation in Sweden. However, participation in this study was optional for the patients. Furthermore, patients who received just a single dose of ve-dolizumab and then stopped might have been more easily overlooked and unrecorded by the treating clinician than patients who received several doses of the drug.
Thus, it cannot be excluded that the observed drug continuation rate was slightly over-estimated. Another limitation of the study was that data on clinical and biochemical activity were missing for some patients during follow-up. In general, these data are gathered at out-patient clinic visits, and (theoretically) patients who do well might be more likely to miss scheduled appointments. Attrition analysis, i.e. the comparison of known characteristics between patients with and without data, can be used to evaluate whether data are missing at random or whether individuals with-out data differ from the overall population. Unfortunately, no such analy-sis was done in this study. Instead, paired statistical methods to assess changes in disease severity over time were applied, i.e. only patients with data available both at baseline and during follow-up were included. In theory, the observed results could be either an over-estimation or an un-der-estimation of the true clinical effectiveness, although the most con-servative and probably the best approach would have been to consider patients with missing data as being non-responders.
A third limitation was the absence of detailed data on intolerance. Al-most one of every 10 patients stopped vedolizumab treatment because of adverse drug reactions. However, we were unable to retrieve information on type of intolerance, since this information is not recorded in SWIB-REG.
CARL ERIKSSON Inflammatory Bowel Disease 65
General conclusions
I. Both the incidence and the prevalence of ulcerative colitis are increasing in the catchment area of Örebro University Hospital. Patients diagnosed in the period 1991‒2005 had a lower risk of colectomy than patients diagnosed in the period 1963‒1975. The decrease in colectomies was tem-porally associated with increased use of thiopurines and an-ti-TNF agents.
II. Anaemia is a common complication, even beyond the first
years after diagnosis of IBD. The risk of developing anae-mia is higher in Crohn’s disease than in ulcerative colitis. Stricturing behavior in Crohn´s disease and extensive dis-ease extent in ulcerative colitis is associated with an in-creased risk of anaemia. The prognosis of anaemia, in terms of resolution of anaemia within 12 months, is worse in Crohn’s disease.
III. Thiopurine drugs have a profound beneficial effect on the
natural history and long-term colectomy rates of ulcerative colitis.
IV. Despite the fact that vedolizumab-treated patients in Swe-
den are generally a treatment-refractory group, the majori-ty continued the therapy after a median follow-up period of almost 1.5 years. Previous exposure to anti-TNF and ele-vated CRP appear to be associated with a less favourable clinical response, and female sex was found to be associat-ed with an increased risk of intolerance.
66 CARL ERIKSSON Inflammatory Bowel Disease
Future perspectives
• To deal with the above-mentioned limitations in paper IV, includ-ing the absence of detailed data on adverse drug reactions andproblems with missing data, a prospective observational study ofvedolizumab-treated patients in Swedish clinical practice is cur-rently being undertaken.
• Clinical trials have demonstrated the efficacy of golimumab in ul-cerative colitis. However, randomized trials do not readily reflecteveryday clinical practice, and the efficacy of golimumab inCrohn´s disease has not been evaluated. Two observational stud-ies to address the clinical effectiveness of golimumab in Crohn’sdisease and ulcerative colitis are currently being performed.
• Active smoking has an impact on the risk of developing IBD andalso on the risk of having a complicated disease course (decreasedrisks in ulcerative colitis and increased risks in Crohn’s disease).On the other hand, there are no data on the effect of oral moistsnuff on the disease course of IBD, and a study to address this is-sue is currently under way.
• Concomitant infections with Clostridium difficile appear to be agrowing problem in IBD, and are associated with increased mor-bidity and mortality. A study to investigate the epidemiology andclinical outcome of Clostridium difficile infections based on datafrom our population-based IBD cohort is currently being planned.
• Sweden offers exceptional conditions for epidemiological researchin the field of IBD, since almost all healthcare is publicly financedand because the Swedish personal identity number allows large-scale linkage of data from different nationwide computerized reg-istries.352 Studies on the epidemiology of IBD at a national levelhave several advantages over single-centre studies.
• In recent years, several new drugs have been approved for use inIBD. In most cases however, the efficacy of these drugs has onlybeen shown to be superior to that of placebo. Studies that com-

CARL ERIKSSON Inflammatory Bowel Disease 67
pare the efficacy of new drugs to the efficacy of currently availa-ble therapies, such as anti-TNF agents, are very much needed. In the future, it might be possible to include a randomization module in SWIBREG and to perform this type of study through the regis-try. In this way, the advantages of a randomized trial could be combined with the strengths of a large, unselected clinical registry.
68 CARL ERIKSSON Inflammatory Bowel Disease
Sammanfattning på svenska De kroniska inflammatoriska tarmsjukdomarna (IBD) utgörs av Chrons sjukdom och ulcerös kolit. Dessa tillstånd kännetecknas av inflammation i gastrointestinal-kanalen, debuterar ofta tidigt i livet och har starkt negativ inverkan på den drabbades dagliga liv, livskvalité och arbetsförmåga. Be-handlingen är i första hand medicinsk men en betydande andel av de drabbade behöver någon gång opereras på grund av sjukdomskomplikat-ioner eller bristande svar på medicinering. Orsaken till inflammatorisk tarmsjukdom är fortfarande okänd men under 1900-talet rapporterades en kraftig ökning i insjuknande i många delar av västvärden. Under senare år har det kommit rapporter om utplanande eller till och med minskande insjuknande i länder som tidigare haft hög förekomst samtidigt som insjuknandet ökat i medel och låginkomstländer, där IBD tidigare varit ovanligt. Förändringarna i insjuknande har gått för fort för att kunna förklaras av genetiska faktorer och forskarvärlden har dragit slutsatsen att de betingas av okända miljöfaktorer. I delarbete I påvisar vi en femfaldig ökning av antalet insjuknande i ulcerös kolit i Öre-bro under perioden 1963-2010. Orsaken till denna ökning kan inte full-ständigt förklaras men minskning av cigarettrökning har sannolikt bidra-git. Studien påvisar också att andelen patienter som behöver opereras gått ner, möjligen till följd av förbättrad medicinsk behandling. En av de vanligaste komplikationerna vid IBD är anemi men förekomsten är otillräckligt studerad. I delarbete II påvisar vi att både insjuknande och förekomst av anemi är större vid Crohns sjukdom än vid ulcerös kolit. Våra resultat visar också att individer med Crohns sjukdom svarar sämre på behandling mot anemi än vad patienter med ulcerös kolit gör. En tänk-bar förklaring kan vara kraftigare systemisk inflammatorisk aktivitet vid Crohns sjukdom. Något som i tidigare studier visat sig hämma upptaget av järn i tunntarmen. Syftet med delarbete III var att undersöka långtidseffekter av behandling med så kallade thiopuriner vid ulcerös kolit. Thiopuriner är läkemedel som minskar mängden vita blodkroppar genom att hämma celldelning och användningen vid ulcerös kolit har gradvis ökat i Sverige sedan 80-talet. Omkring 30% av individer som får thiopurinbehandling slutar inom 1 år på grund av biverkningar och hittills har det varit okänt hur dessa läke-medel påverkar sjukdomsförloppet på lång sikt. I genomförandet av stu-dien utnyttjade vi det faktum att många patienter avbryter behandlingen på grund av biverkningar och jämförde effekten mellan de som slutat

CARL ERIKSSON Inflammatory Bowel Disease 69
inom ett år på grund av biverkningar med de som fortsatt i ett år eller slutat av andra orsaker. Med denna nya studiedesign kunde vi visa att thiopurinbehandling minskar risken för operation, ökad sjukdomsutbred-ningen, sjukhusinläggning samt för att behöva TNF-hämmande läkemedel. Under den senaste 10-årsperioden har flera nya läkemedel godkänts för behandling av IBD. Efter att läkemedel godkänts är det viktigt med upp-följande studier för att säkerställa att läkemedlet är säkert och fungerar även i rutinsjukvård. Vedolizumab hör till gruppen integrin-hämmare och fungerar genom att förhindra vandring av vita blodkroppar från blodet till den inflammerade tarmen. I delarbete IV visar vi att vedolizumab är effek-tivt och säkert att använda i Svensk rutinsjukvård. Dock visar vår studie att vedolizumab fungerar sämre hos patienter med förhöjt CRP vid be-handlingsstart, hos patienter som tidigare haft TNF-hämmande läkemedel samt att kvinnor jämfört med män oftare slutar på grund av biverkningar.
70 CARL ERIKSSON Inflammatory Bowel Disease
Acknowledgments I wish to express my sincere gratitude to everyone who has helped and supported me during the work for this thesis. Without your help, this work would never have been accomplished. In particular, I would like to thank:
Jonas Halfvarson, for being my main supervisor, mentor, and dear friend during the past 3 years, and for introducing me to science and the field of inflammatory bowel disease. Your constant support―not only academi-cally, but also personally―has been exceptional. Thank you!
Scott Montgomery, for being my co-supervisor, for stimulating epidemio-logical discussions, and for your linguistic excellence. I have learnt a lot from our collaboration.
Yang Cho, Ruzan Udumyan, Anders Magnusson, and Ole Brus, for inval-uable statistical support.
Curt Tysk, for being my tutor during residency in Internal Medicine, for invaluable support with my first scientific publication, and for generously helping me with recent work―including the “kappa” of this thesis. Your generosity and encouragement is amazing!
Jan Marsal, Lina Vigren, Jan Björk, Michael Eberhardson, Pontus Karling, Charlotte Söderman, Pär Myrelid, Daniel Sjöberg, Mari Thörn, Per Kar-lén, Erik Hertervig, Hans Strid, Jonas F Ludvigsson and Sven Almer, for inspiring collaboration.
Anna Wickbom, for being my mentor during residency in Gastroenterolo-gy and Hepatology, for all your kindness, and for always taking the time to answer my questions.
Johan Bohr, Nils Nyhlin, Michiel van Nieuwenhoven, Yeshi Yiman, Ebba Salén, Bengt Curman, and Robert Brummer, my senior clinical colleagues, for your immense knowledge, fruitful discussions, valuable guidance, and for creating such an inviting and stimulating atmosphere.
CARL ERIKSSON Inflammatory Bowel Disease 71
Ida Henriksson and Daniel Bergemalm―my dear friends, fellow residents, and co-authors. Thanks for the stimulating discussions and for the fun we have had together. I am hoping for long and fruitful collaboration.
Gunnar Järnerot, founder of IBD research in Örebro, for your interest and encouragement. Margareta Lundin, Lena Ericsson, Emma Stenlund, Åsa Ekblom, and Ma-lin Olsson, for all your help with data extraction. Without you, this thesis wouldn’t have been finished within half a decade.
Sara Rundquist, Erik Andersson, Isabella Visuri, Yaroslava Zhulina, Peter Wildeman, Johan Jendeberg, and Evelina Panzar, fellow PhD students, for scientific collaboration―but also for all the jokes and discussions during the mandatory courses.
Marianne Axman, Carina Emilsson, Susanne Enblom, Anna Calais, Hanna Falck, Stina Figaro, Amelie Härenstam, Hanna Johnsson, Haile Kocubo, Ann-Britt Löf, Karin Marjamaa, Birgitta Meijer, Karina Molina, Martina Ragnarsson, Eva Ståhl, Ida Svanerud, Anna Svensson, Ulla Vid-mark, Anette Wendt, and Ulla-Britt Widén, for all your support in the clinics. It is a privilege to work with you all!
All my dear friends, for enriching my life.
My parents Torbjörn and Eva and my brothers Olle and Hannes, for your love and encouragement.
My beloved wife Azadeh and daughters Natalie and Olivia, for putting up with me during these years and for reminding me that there are much more important things in life than work. Love you!
72 CARL ERIKSSON Inflammatory Bowel Disease
References 1. Gomollon F, Dignass A, Annese V, et al. 3rd European Evidence-
based Consensus on the Diagnosis and Management of Crohn'sDisease 2016: Part 1: Diagnosis and Medical Management. Journalof Crohn's & colitis 2017;11(1):3-25.
2. Harbord M, Eliakim R, Bettenworth D, et al. Third EuropeanEvidence-based Consensus on Diagnosis and Management ofUlcerative Colitis. Part 2: Current Management. Journal of Crohn's& colitis 2017;11(7):769-784.
3. Magro F, Gionchetti P, Eliakim R, et al. Third European Evidence-based Consensus on Diagnosis and Management of UlcerativeColitis. Part 1: Definitions, Diagnosis, Extra-intestinalManifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. Journal of Crohn's & colitis 2017;11(6):649-670.
4. Magro F, Langner C, Driessen A, et al. European consensus on thehistopathology of inflammatory bowel disease. Journal of Crohn's& colitis 2013;7(10):827-51.
5. Satsangi J, Silverberg MS, Vermeire S, Colombel JF. The Montrealclassification of inflammatory bowel disease: controversies,consensus, and implications. Gut 2006;55(6):749-53.
6. Kent TH, Ammon RK, DenBesten L. Differentiation of ulcerativecolitis and regional enteritis of colon. Arch. Pathol. 1970;89(1):20-9.
7. Wilks S. Morbid appearances in the intestine of Miss Bankes.London Medical Gazette 1859;2:264.
8. Fielding JF. "Inflammatory" bowel disease. Br. Med. J. (Clin. Res.Ed) 1985;290(6461):47-8.
9. Dalziel TK. Chronic interstitial enteritis. Br. Med. J. 1913;2:1068–70.
10. A. L. Pryczynek do chirurgii kiszek. . Medycyna 1903;31:460-4.11. Morgagni GB. De sedibus et causis morborum per anatomen
indagatis libri quinque Venice. typographia Remondiniana 1761.12. Crohn BB, Ginzburg L, Oppenheimer GD. Regional ileitis; a
pathologic and clinical entity. JAMA 1932;99(16):1323-1329.13. Ginzburg L. Regional enteritis: historical perspective (B. Crohn and
L. Ginzburg). Gastroenterology 1986;90(5 Pt 1):1310-1.14. Kyle J. RARER COMPLICATIONS OF CROHN'S (DALZIEL'S)
DISEASE*. Aust. N. Z. J. Surg. 1991;61(7):489-492.15. Heaton LD, Ravdin IS, Blades B, Whelan TJ. PRESIDENT
EISENHOWER'S OPERATION FOR REGIONAL ENTERITIS: AFOOTNOTE TO HISTORY. Ann. Surg. 1964;159:661-6.
CARL ERIKSSON Inflammatory Bowel Disease 73
16. Binder V, Both H, Hansen PK, Hendriksen C, Kreiner S, Torp-Pedersen K. Incidence and prevalence of ulcerative colitis and Crohn's disease in the County of Copenhagen, 1962 to 1978. Gastroenterology 1982;83(3):563-8.
17. Evans JG, Acheson ED. An epidemiological study of ulcerative colitis and regional enteritis in the Oxford area. Gut 1965;6(4):311-24.
18. Garland CF, Lilienfeld AM, Mendeloff AI, Markowitz JA, Terrell KB, Garland FC. Incidence rates of ulcerative colitis and Crohn's disease in fifteen areas of the United States. Gastroenterology 1981;81(6):1115-24.
19. Morson BS. Histopathology of Crohn's disease. Proc. R. Soc. Med. 1968;61(1):79-81.
20. Wolff WI, Shinya H. Colonofiberoscopy. JAMA 1971;217(11):1509-12.
21. Morson BC, Pang LS. Rectal biopsy as an aid to cancer control in ulcerative colitis. Gut 1967;8(5):423-34.
22. Lennard-Jones JE. Classification of inflammatory bowel disease. Scand. J. Gastroenterol. Suppl. 1989;170:2-6; discussion 16-9.
23. Farmer RG, Hawk WA, Turnbull RB, Jr. Clinical patterns in Crohn's disease: a statistical study of 615 cases. Gastroenterology 1975;68(4 Pt 1):627-35.
24. Greenstein AJ, Lachman P, Sachar DB, et al. Perforating and non-perforating indications for repeated operations in Crohn's disease: evidence for two clinical forms. Gut 1988;29(5):588-92.
25. Sachar DB, Andrews HA, Farmer RG, et al. Proposed classification of patients subgroups in Crohn's disease. Gastroenterology int 1992;5:141-54.
26. Steinhart AH, Girgrah N, McLeod RS. Reliability of a Crohn's disease clinical classification scheme based on disease behavior. Inflamm. Bowel Dis. 1998;4(3):228-34.
27. Gasche C, Scholmerich J, Brynskov J, et al. A simple classification of Crohn's disease: report of the Working Party for the World Congresses of Gastroenterology, Vienna 1998. Inflamm. Bowel Dis. 2000;6(1):8-15.
28. Silverberg MS, Satsangi J, Ahmad T, et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can. J. Gastroenterol. 2005;19 Suppl A:5a-36a.
74 CARL ERIKSSON Inflammatory Bowel Disease
29. Moum B, Ekbom A, Vatn MH, et al. Clinical course during the 1styear after diagnosis in ulcerative colitis and Crohn's disease. Resultsof a large, prospective population-based study in southeasternNorway, 1990-93. Scand. J. Gastroenterol. 1997;32(10):1005-12.
30. Lennard-Jones JE. The clinical outcome of ulcerative colitis dependson how much of the colonic mucosa is involved. Scand. J.Gastroenterol. Suppl. 1983;88:48-53.
31. Ritchie JK, Powell-Tuck J, Lennard-Jones JE. Clinical outcome ofthe first ten years of ulcerative colitis and proctitis. Lancet1978;1(8074):1140-3.
32. Devroede GJ, Taylor WF, Sauer WG, Jackman RJ, Stickler GB.Cancer risk and life expectancy of children with ulcerative colitis.N. Engl. J. Med. 1971;285(1):17-21.
33. Gupta RB, Harpaz N, Itzkowitz S, et al. Histologic inflammation isa risk factor for progression to colorectal neoplasia in ulcerativecolitis: a cohort study. Gastroenterology 2007;133(4):1099-105;quiz 1340-1.
34. Kim B, Barnett JL, Kleer CG, Appelman HD. Endoscopic andhistological patchiness in treated ulcerative colitis. Am. J.Gastroenterol. 1999;94(11):3258-62.
35. Markowitz J, Kahn E, Grancher K, Hyams J, Treem W, Daum F.Atypical rectosigmoid histology in children with newly diagnosedulcerative colitis. Am. J. Gastroenterol. 1993;88(12):2034-7.
36. Byeon JS, Yang SK, Myung SJ, et al. Clinical course of distalulcerative colitis in relation to appendiceal orifice inflammationstatus. Inflamm. Bowel Dis. 2005;11(4):366-71.
37. Haskell H, Andrews CW, Jr., Reddy SI, et al. Pathologic featuresand clinical significance of "backwash" ileitis in ulcerative colitis.Am. J. Surg. Pathol. 2005;29(11):1472-81.
38. Jenkins D, Balsitis M, Gallivan S, et al. Guidelines for the initialbiopsy diagnosis of suspected chronic idiopathic inflammatorybowel disease. The British Society of Gastroenterology Initiative. J.Clin. Pathol. 1997;50(2):93-105.
39. Seldenrijk CA, Morson BC, Meuwissen SG, Schipper NW,Lindeman J, Meijer CJ. Histopathological evaluation of colonicmucosal biopsy specimens in chronic inflammatory bowel disease:diagnostic implications. Gut 1991;32(12):1514-20.
40. Kleer CG, Appelman HD. Ulcerative colitis: patterns of involvementin colorectal biopsies and changes with time. Am. J. Surg. Pathol.1998;22(8):983-9.
41. Geboes K, Riddell R, Ost A, Jensfelt B, Persson T, Lofberg R. Areproducible grading scale for histological assessment ofinflammation in ulcerative colitis. Gut 2000;47(3):404-9.
CARL ERIKSSON Inflammatory Bowel Disease 75
42. Mosli MH, Parker CE, Nelson SA, et al. Histologic scoring indices for evaluation of disease activity in ulcerative colitis. Cochrane Database of Systematic Reviews 2017(5).
43. Gomes P, du Boulay C, Smith CL, Holdstock G. Relationship between disease activity indices and colonoscopic findings in patients with colonic inflammatory bowel disease. Gut 1986;27(1):92-5.
44. Novak G, Parker CE, Pai RK, et al. Histologic scoring indices for evaluation of disease activity in Crohn’s disease. Cochrane Database of Systematic Reviews 2017(7).
45. Sawczenko A, Sandhu BK. Presenting features of inflammatory bowel disease in Great Britain and Ireland. Arch. Dis. Child. 2003;88(11):995-1000.
46. Mekhjian HS, Switz DM, Melnyk CS, Rankin GB, Brooks RK. Clinical features and natural history of Crohn's disease. Gastroenterology 1979;77(4 Pt 2):898-906.
47. Burgmann T, Clara I, Graff L, et al. The Manitoba Inflammatory Bowel Disease Cohort Study: prolonged symptoms before diagnosis--how much is irritable bowel syndrome? Clin. Gastroenterol. Hepatol. 2006;4(5):614-20.
48. Thjodleifsson B, Sigthorsson G, Cariglia N, et al. Subclinical intestinal inflammation: an inherited abnormality in Crohn's disease relatives? Gastroenterology 2003;124(7):1728-37.
49. Pimentel M, Chang M, Chow EJ, et al. Identification of a prodromal period in Crohn's disease but not ulcerative colitis. Am. J. Gastroenterol. 2000;95(12):3458-62.
50. Bernstein CN, Blanchard JF, Rawsthorne P, Yu N. The prevalence of extraintestinal diseases in inflammatory bowel disease: a population-based study. Am. J. Gastroenterol. 2001;96(4):1116-22.
51. Vavricka SR, Brun L, Ballabeni P, et al. Frequency and risk factors for extraintestinal manifestations in the Swiss inflammatory bowel disease cohort. Am. J. Gastroenterol. 2011;106(1):110-9.
52. Gasche C, Lomer MC, Cavill I, Weiss G. Iron, anaemia, and inflammatory bowel diseases. Gut 2004;53(8):1190-7.
53. Kulnigg S, Gasche C. Systematic review: managing anaemia in Crohn's disease. Aliment. Pharmacol. Ther. 2006;24(11-12):1507-23.
54. Hoivik ML, Reinisch W, Cvancarova M, Moum B. Anaemia in inflammatory bowel disease: a population-based 10-year follow-up. Aliment. Pharmacol. Ther. 2014;39(1):69-76.
76 CARL ERIKSSON Inflammatory Bowel Disease
55. Ott C, Liebold A, Takses A, Strauch UG, Obermeier F. Highprevalence but insufficient treatment of iron-deficiency anemia inpatients with inflammatory bowel disease: results of a population-based cohort. Gastroenterology research and practice2012;2012:595970.
56. Rejler M, Tholstrup J, Andersson-Gare B, Spangeus A. Lowprevalence of anemia in inflammatory bowel disease: a population-based study in Sweden. Scand. J. Gastroenterol. 2012;47(8-9):937-42.
57. Sjoberg D, Holmstrom T, Larsson M, Nielsen AL, Holmquist L,Ronnblom A. Anemia in a population-based IBD cohort (ICURE):still high prevalence after 1 year, especially among pediatricpatients. Inflamm. Bowel Dis. 2014;20(12):2266-70.
58. Solberg IC, Lygren I, Jahnsen J, et al. Clinical course during the first10 years of ulcerative colitis: results from a population-basedinception cohort (IBSEN Study). Scand. J. Gastroenterol.2009;44(4):431-40.
59. Solberg IC, Vatn MH, Hoie O, et al. Clinical course in Crohn'sdisease: results of a Norwegian population-based ten-year follow-upstudy. Clin. Gastroenterol. Hepatol. 2007;5(12):1430-8.
60. Hoivik ML, Moum B, Solberg IC, et al. Health-related quality oflife in patients with ulcerative colitis after a 10-year disease course:results from the IBSEN study. Inflamm. Bowel Dis.2012;18(8):1540-9.
61. Hoivik ML, Bernklev T, Solberg IC, et al. Patients with Crohn'sdisease experience reduced general health and vitality in the chronicstage: ten-year results from the IBSEN study. Journal of Crohn's &colitis 2012;6(4):441-53.
62. Louis E, Collard A, Oger AF, Degroote E, Aboul Nasr El Yafi FA,Belaiche J. Behaviour of Crohn's disease according to the Viennaclassification: changing pattern over the course of the disease. Gut2001;49(6):777-82.
63. Cosnes J, Cattan S, Blain A, et al. Long-term evolution of diseasebehavior of Crohn's disease. Inflamm. Bowel Dis. 2002;8(4):244-50.
64. Bewtra M, Kaiser LM, TenHave T, Lewis JD. Crohn's disease andulcerative colitis are associated with elevated standardized mortalityratios: a meta-analysis. Inflamm. Bowel Dis. 2013;19(3):599-613.
65. Kassam Z, Belga S, Roifman I, et al. Inflammatory bowel diseasecause-specific mortality: a primer for clinicians. Inflamm. BowelDis. 2014;20(12):2483-92.
CARL ERIKSSON Inflammatory Bowel Disease 77
66. Jussila A, Virta LJ, Pukkala E, Farkkila MA. Mortality and causes of death in patients with inflammatory bowel disease: a nationwide register study in Finland. Journal of Crohn's & colitis 2014;8(9):1088-96.
67. Jess T, Frisch M, Simonsen J. Trends in overall and cause-specific mortality among patients with inflammatory bowel disease from 1982 to 2010. Clin. Gastroenterol. Hepatol. 2013;11(1):43-8.
68. Eaden JA, Abrams KR, Mayberry JF. The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut 2001;48(4):526-35.
69. Jess T, Gamborg M, Matzen P, Munkholm P, Sorensen TI. Increased risk of intestinal cancer in Crohn's disease: a meta-analysis of population-based cohort studies. Am. J. Gastroenterol. 2005;100(12):2724-9.
70. Frolkis AD, Dykeman J, Negron ME, et al. Risk of surgery for inflammatory bowel diseases has decreased over time: a systematic review and meta-analysis of population-based studies. Gastroenterology 2013;145(5):996-1006.
71. Sica GS, Biancone L. Surgery for inflammatory bowel disease in the era of laparoscopy. World J. Gastroenterol. 2013;19(16):2445-8.
72. Jess T, Riis L, Vind I, et al. Changes in clinical characteristics, course, and prognosis of inflammatory bowel disease during the last 5 decades: a population-based study from Copenhagen, Denmark. Inflamm. Bowel Dis. 2007;13(4):481-9.
73. Kaplan GG, Seow CH, Ghosh S, et al. Decreasing colectomy rates for ulcerative colitis: a population-based time trend study. Am. J. Gastroenterol. 2012;107(12):1879-87.
74. Ramadas AV, Gunesh S, Thomas GA, Williams GT, Hawthorne AB. Natural history of Crohn's disease in a population-based cohort from Cardiff (1986-2003): a study of changes in medical treatment and surgical resection rates. Gut 2010;59(9):1200-6.
75. Samuel S, Ingle SB, Dhillon S, et al. Cumulative incidence and risk factors for hospitalization and surgery in a population-based cohort of ulcerative colitis. Inflamm. Bowel Dis. 2013;19(9):1858-66.
76. Vester-Andersen MK, Prosberg MV, Jess T, et al. Disease course and surgery rates in inflammatory bowel disease: a population-based, 7-year follow-up study in the era of immunomodulating therapy. Am. J. Gastroenterol. 2014;109(5):705-14.
77. Zhulina Y, Udumyan R, Tysk C, Montgomery S, Halfvarson J. The changing face of Crohn's disease: a population-based study of the natural history of Crohn's disease in Orebro, Sweden 1963-2005. Scand. J. Gastroenterol. 2016;51(3):304-13.

78 CARL ERIKSSON Inflammatory Bowel Disease
78. Henriksen M, Jahnsen J, Lygren I, et al. Clinical course in Crohn'sdisease: results of a five-year population-based follow-up study (theIBSEN study). Scand. J. Gastroenterol. 2007;42(5):602-10.
79. Henriksen M, Jahnsen J, Lygren I, et al. Ulcerative colitis andclinical course: results of a 5-year population-based follow-up study(the IBSEN study). Inflamm. Bowel Dis. 2006;12(7):543-50.
80. Peyrin-Biroulet L, Sandborn W, Sands BE, et al. SelectingTherapeutic Targets in Inflammatory Bowel Disease (STRIDE):Determining Therapeutic Goals for Treat-to-Target. The AmericanJournal Of Gastroenterology 2015;110:1324.
81. Panes J, Su C, Bushmakin AG, Cappelleri JC, Mamolo C, Healey P.Randomized trial of tofacitinib in active ulcerative colitis: analysisof efficacy based on patient-reported outcomes. BMCGastroenterol. 2015;15:14.
82. Feagan BG, Hanauer SB, Coteur G, Schreiber S. Evaluation of adaily practice composite score for the assessment of Crohn'sdisease: the treatment impact of certolizumab pegol. Aliment.Pharmacol. Ther. 2011;33(10):1143-51.
83. Higgins PD, Schwartz M, Mapili J, Zimmermann EM. Is endoscopynecessary for the measurement of disease activity in ulcerativecolitis? Am. J. Gastroenterol. 2005;100(2):355-61.
84. Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenanceinfliximab for Crohn's disease: the ACCENT I randomised trial.Lancet 2002;359(9317):1541-9.
85. Peyrin-Biroulet L, Reinisch W, Colombel JF, et al. Clinical diseaseactivity, C-reactive protein normalisation and mucosal healing inCrohn's disease in the SONIC trial. Gut 2014;63(1):88-95.
86. Colombel JF, Rutgeerts P, Reinisch W, et al. Early mucosal healingwith infliximab is associated with improved long-term clinicaloutcomes in ulcerative colitis. Gastroenterology 2011;141(4):1194-201.
87. Rutgeerts P, Van Assche G, Sandborn WJ, et al. Adalimumabinduces and maintains mucosal healing in patients with Crohn'sdisease: data from the EXTEND trial. Gastroenterology2012;142(5):1102-1111.e2.
88. Mohammed Vashist N, Samaan M, Mosli MH, et al. Endoscopicscoring indices for evaluation of disease activity in ulcerative colitis.Cochrane Database of Systematic Reviews 2018(1).
89. Khanna R, Nelson SA, Feagan BG, et al. Endoscopic scoring indicesfor evaluation of disease activity in Crohn’s disease. CochraneDatabase of Systematic Reviews 2016(8).
90. Truelove SC, Witts LJ. Cortisone in ulcerative colitis; final reporton a therapeutic trial. Br. Med. J. 1955;2(4947):1041-8.
CARL ERIKSSON Inflammatory Bowel Disease 79
91. D'Haens G, Sandborn WJ, Feagan BG, et al. A review of activity indices and efficacy end points for clinical trials of medical therapy in adults with ulcerative colitis. Gastroenterology 2007;132(2):763-86.
92. Sandborn WJ, Feagan BG, Hanauer SB, et al. A review of activity indices and efficacy endpoints for clinical trials of medical therapy in adults with Crohn's disease. Gastroenterology 2002;122(2):512-30.
93. Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N. Engl. J. Med. 1987;317(26):1625-9.
94. Best WR, Becktel JM, Singleton JW, Kern F, Jr. Development of a Crohn's disease activity index. National Cooperative Crohn's Disease Study. Gastroenterology 1976;70(3):439-44.
95. Jones J, Loftus EV, Jr., Panaccione R, et al. Relationships between disease activity and serum and fecal biomarkers in patients with Crohn's disease. Clin. Gastroenterol. Hepatol. 2008;6(11):1218-24.
96. Cellier C, Sahmoud T, Froguel E, et al. Correlations between clinical activity, endoscopic severity, and biological parameters in colonic or ileocolonic Crohn's disease. A prospective multicentre study of 121 cases. The Groupe d'Etudes Therapeutiques des Affections Inflammatoires Digestives. Gut 1994;35(2):231-5.
97. Harvey RF, Bradshaw JM. A simple index of Crohn's-disease activity. Lancet 1980;1(8167):514.
98. Vermeire S, Schreiber S, Sandborn WJ, Dubois C, Rutgeerts P. Correlation between the Crohn's disease activity and Harvey-Bradshaw indices in assessing Crohn's disease severity. Clin. Gastroenterol. Hepatol. 2010;8(4):357-63.
99. Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2005;353(23):2462-76.
100. Bennebroek Evertsz F, Hoeks CC, Nieuwkerk PT, et al. Development of the patient Harvey Bradshaw index and a comparison with a clinician-based Harvey Bradshaw index assessment of Crohn's disease activity. J. Clin. Gastroenterol. 2013;47(10):850-6.
101. Bennebroek Evertsz F, Nieuwkerk PT, Stokkers PC, et al. The patient simple clinical colitis activity index (P-SCCAI) can detect ulcerative colitis (UC) disease activity in remission: a comparison of the P-SCCAI with clinician-based SCCAI and biological markers. Journal of Crohn's & colitis 2013;7(11):890-900.
80 CARL ERIKSSON Inflammatory Bowel Disease
102. Sands BE. Biomarkers of Inflammation in Inflammatory BowelDisease. Gastroenterology 2015;149(5):1275-1285.e2.
103. Tillett WS, Francis T. SEROLOGICAL REACTIONS INPNEUMONIA WITH A NON-PROTEIN SOMATIC FRACTIONOF PNEUMOCOCCUS. J. Exp. Med. 1930;52(4):561-71.
104. Shine B, Berghouse L, Jones JE, Landon J. C-reactive protein as anaid in the differentiation of functional and inflammatory boweldisorders. Clin. Chim. Acta 1985;148(2):105-9.
105. Poullis AP, Zar S, Sundaram KK, et al. A new, highly sensitive assayfor C-reactive protein can aid the differentiation of inflammatorybowel disorders from constipation- and diarrhoea-predominantfunctional bowel disorders. Eur. J. Gastroenterol. Hepatol.2002;14(4):409-12.
106. Beattie RM, Walker-Smith JA, Murch SH. Indications forinvestigation of chronic gastrointestinal symptoms. Arch. Dis.Child. 1995;73(4):354-5.
107. Kathiresan S, Larson MG, Vasan RS, et al. Contribution of clinicalcorrelates and 13 C-reactive protein gene polymorphisms tointerindividual variability in serum C-reactive protein level.Circulation 2006;113(11):1415-23.
108. Mosli MH, Zou G, Garg SK, et al. C-Reactive Protein, FecalCalprotectin, and Stool Lactoferrin for Detection of EndoscopicActivity in Symptomatic Inflammatory Bowel Disease Patients: ASystematic Review and Meta-Analysis. Am. J. Gastroenterol.2015;110(6):802-19; quiz 820.
109. Siemons L, Ten Klooster PM, Vonkeman HE, van Riel PL, GlasCA, van de Laar MA. How age and sex affect the erythrocytesedimentation rate and C-reactive protein in early rheumatoidarthritis. BMC Musculoskelet. Disord. 2014;15:368.
110. Dale I, Fagerhol MK, Naesgaard I. Purification and partialcharacterization of a highly immunogenic human leukocyte protein,the L1 antigen. Eur. J. Biochem. 1983;134(1):1-6.
111. Hajat C. An introduction to epidemiology. Methods Mol. Biol.2011;713:27-39.
112. Allchin WH. A Discussion on "Ulcerative Colitis.": IntroductoryAddress. Proc. R. Soc. Med. 1909;2(Med Sect):59-75.
113. Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence andprevalence of the inflammatory bowel diseases with time, based onsystematic review. Gastroenterology 2012;142(1):46-54.e42; quize30.
114. Bjornsson S. Inflammatory bowel disease in Iceland during a 30-year period, 1950-1979. Scand. J. Gastroenterol. Suppl.1989;170:47-9; discussion 50-5.
CARL ERIKSSON Inflammatory Bowel Disease 81
115. Lindberg E, Jornerot G. The incidence of Crohn's disease is not decreasing in Sweden. Scand. J. Gastroenterol. 1991;26(5):495-500.
116. Moller C, Linden G. Ulcerative colitis in Finland. I. Cases treated at central hospitals, 1956-1967. Dis. Colon Rectum 1971;14(4):259-63.
117. Myren J, Gjone E, Hertzberg JN, Rygvold O, Semb LS, Fretheim B. Epidemiology of ulcerative colitis and regional enterocolitis (Crohn's disease) in Norway. Scand. J. Gastroenterol. 1971;6(6):511-4.
118. Ronnblom A, Samuelsson SM, Ekbom A. Ulcerative colitis in the county of Uppsala 1945-2007: incidence and clinical characteristics. Journal of Crohn's & colitis 2010;4(5):532-6.
119. Tysk C, Jarnerot G. Ulcerative proctocolitis in Orebro, Sweden. A retrospective epidemiologic study, 1963-1987. Scand. J. Gastroenterol. 1992;27(11):945-50.
120. Kyle J. Crohn's disease in the northeastern and northern Isles of Scotland: an epidemiological review. Gastroenterology 1992;103(2):392-9.
121. Loftus EV, Jr., Silverstein MD, Sandborn WJ, Tremaine WJ, Harmsen WS, Zinsmeister AR. Crohn's disease in Olmsted County, Minnesota, 1940-1993: incidence, prevalence, and survival. Gastroenterology 1998;114(6):1161-8.
122. Loftus EV, Jr., Silverstein MD, Sandborn WJ, Tremaine WJ, Harmsen WS, Zinsmeister AR. Ulcerative colitis in Olmsted County, Minnesota, 1940-1993: incidence, prevalence, and survival. Gut 2000;46(3):336-43.
123. Montgomery SM, Morris DL, Thompson NP, Subhani J, Pounder RE, Wakefield AJ. Prevalence of inflammatory bowel disease in British 26 year olds: national longitudinal birth cohort. BMJ 1998;316(7137):1058-9.
124. Fireman Z, Grossman A, Lilos P, Eshchar Y, Theodor E, Gilat T. Epidemiology of Crohn's disease in the Jewish population of central Israel, 1970-1980. Am. J. Gastroenterol. 1989;84(3):255-8.
125. Odes HS, Fraser D, Krawiec J. Incidence of idiopathic ulcerative colitis in Jewish population subgroups in the Beer Sheva region of Israel. Am. J. Gastroenterol. 1987;82(9):854-8.
126. Wilson J, Hair C, Knight R, et al. High incidence of inflammatory bowel disease in Australia: a prospective population-based Australian incidence study. Inflamm. Bowel Dis. 2010;16(9):1550-6.
127. Wright JP, Marks IN, Jameson C, Garisch JA, Burns DG, Kottler RE. Inflammatory bowel disease in Cape Town, 1975-1980. Part II. Crohn's disease. S. Afr. Med. J. 1983;63(7):226-9.
82 CARL ERIKSSON Inflammatory Bowel Disease
128. Wright JP, Marks IN, Jameson C, Garisch JA, Burns DG, KottlerRE. Inflammatory bowel disease in Cape Town, 1975-1980. Part I.Ulcerative colitis. S. Afr. Med. J. 1983;63(7):223-6.
129. Lakatos L, Kiss LS, David G, et al. Incidence, disease phenotype atdiagnosis, and early disease course in inflammatory bowel diseasesin Western Hungary, 2002-2006. Inflamm. Bowel Dis.2011;17(12):2558-65.
130. Prideaux L, Kamm MA, De Cruz PP, Chan FK, Ng SC.Inflammatory bowel disease in Asia: a systematic review. J.Gastroenterol. Hepatol. 2012;27(8):1266-80.
131. Appleyard CB, Hernandez G, Rios-Bedoya CF. Basic epidemiologyof inflammatory bowel disease in Puerto Rico. Inflamm. Bowel Dis.2004;10(2):106-11.
132. Loftus CG, Loftus EV, Jr., Harmsen WS, et al. Update on theincidence and prevalence of Crohn's disease and ulcerative colitis inOlmsted County, Minnesota, 1940-2000. Inflamm. Bowel Dis.2007;13(3):254-61.
133. Logan RF. Inflammatory bowel disease incidence: up, down orunchanged? Gut 1998;42(3):309-11.
134. Hammer T, Nielsen KR, Munkholm P, Burisch J, Lynge E. TheFaroese IBD Study: Incidence of Inflammatory Bowel DiseasesAcross 54 Years of Population-based Data. Journal of Crohn's &colitis 2016;10(8):934-42.
135. Pavlovic-Calic N, Salkic NN, Gegic A, Smajic M, Alibegovic E.Crohn's disease in Tuzla region of Bosnia and Herzegovina: a 12-year study (1995-2006). Int. J. Colorectal Dis. 2008;23(10):957-64.
136. Zwi AB, Mills A. Health policy in less developed countries: pasttrends and future directions. Journal of international development1995;7(3):299-328.
137. Bernstein CN. Assessing environmental risk factors affecting theinflammatory bowel diseases: a joint workshop of the Crohn's &Colitis Foundations of Canada and the USA. Inflamm. Bowel Dis.2008;14(8):1139-46.
138. Ekbom A, Adami HO, Helmick CG, Jonzon A, Zack MM.Perinatal risk factors for inflammatory bowel disease: a case-controlstudy. Am. J. Epidemiol. 1990;132(6):1111-9.
139. Soon IS, Molodecky NA, Rabi DM, Ghali WA, Barkema HW,Kaplan GG. The relationship between urban environment and theinflammatory bowel diseases: a systematic review and meta-analysis. BMC Gastroenterol. 2012;12:51-51.
140. Strachan DP. Hay fever, hygiene, and household size. BMJ1989;299(6710):1259-60.
CARL ERIKSSON Inflammatory Bowel Disease 83
141. Sood A, Amre D, Midha V, et al. Low hygiene and exposure to infections may be associated with increased risk for ulcerative colitis in a North Indian population. Annals of gastroenterology 2014;27(3):219-223.
142. Calkins BM. A meta-analysis of the role of smoking in inflammatory bowel disease. Dig. Dis. Sci. 1989;34(12):1841-54.
143. Kaplan GG, Hubbard J, Korzenik J, et al. The inflammatory bowel diseases and ambient air pollution: a novel association. Am. J. Gastroenterol. 2010;105(11):2412-9.
144. Li X, Sundquist J, Sundquist K. Educational level and occupation as risk factors for inflammatory bowel diseases: A nationwide study based on hospitalizations in Sweden. Inflamm. Bowel Dis. 2009;15(4):608-15.
145. Roth MP, Petersen GM, McElree C, Vadheim CM, Panish JF, Rotter JI. Familial empiric risk estimates of inflammatory bowel disease in Ashkenazi Jews. Gastroenterology 1989;96(4):1016-20.
146. Yang H, McElree C, Roth MP, Shanahan F, Targan SR, Rotter JI. Familial empirical risks for inflammatory bowel disease: differences between Jews and non-Jews. Gut 1993;34(4):517-524.
147. Afzali A, Cross RK. Racial and Ethnic Minorities with Inflammatory Bowel Disease in the United States: A Systematic Review of Disease Characteristics and Differences. Inflamm. Bowel Dis. 2016;22(8):2023-40.
148. Hugot JP, Chamaillard M, Zouali H, et al. Association of NOD2 leucine-rich repeat variants with susceptibility to Crohn's disease. Nature 2001;411(6837):599-603.
149. Ogura Y, Bonen DK, Inohara N, et al. A frameshift mutation in NOD2 associated with susceptibility to Crohn's disease. Nature 2001;411(6837):603-6.
150. Pinsk V, Lemberg DA, Grewal K, Barker CC, Schreiber RA, Jacobson K. Inflammatory bowel disease in the South Asian pediatric population of British Columbia. Am. J. Gastroenterol. 2007;102(5):1077-83.
151. Probert CS, Jayanthi V, Pinder D, Wicks AC, Mayberry JF. Epidemiological study of ulcerative proctocolitis in Indian migrants and the indigenous population of Leicestershire. Gut 1992;33(5):687-693.
152. Rose JD, Roberts GM, Williams G, Mayberry JF, Rhodes J. Cardiff Crohn's disease jubilee: the incidence over 50 years. Gut 1988;29(3):346-51.
153. Srivastava ED, Mayberry JF, Morris TJ, et al. Incidence of ulcerative colitis in Cardiff over 20 years: 1968-87. Gut 1992;33(2):256-8.
84 CARL ERIKSSON Inflammatory Bowel Disease
154. Kaplan GG. The global burden of IBD: from 2015 to 2025. Nat. Rev. Gastroenterol. Hepatol. 2015;12(12):720-7.
155. Abraham C, Cho JH. Inflammatory bowel disease. N. Engl. J. Med. 2009;361(21):2066-78.
156. Harper PH, Truelove SC, Lee EC, Kettlewell MG, Jewell DP. Split ileostomy and ileocolostomy for Crohn's disease of the colon and ulcerative colitis: a 20 year survey. Gut 1983;24(2):106-13.
157. Sellon RK, Tonkonogy S, Schultz M, et al. Resident enteric bacteria are necessary for development of spontaneous colitis and immune system activation in interleukin-10-deficient mice. Infect. Immun. 1998;66(11):5224-31.
158. Brant SR. Update on the heritability of inflammatory bowel disease: the importance of twin studies. Inflamm. Bowel Dis. 2011;17(1):1-5.
159. van Dongen J, Slagboom PE, Draisma HH, Martin NG, Boomsma DI. The continuing value of twin studies in the omics era. Nature reviews. Genetics 2012;13(9):640-53.
160. Ng SC, Woodrow S, Patel N, Subhani J, Harbord M. Role of genetic and environmental factors in British twins with inflammatory bowel disease. Inflamm. Bowel Dis. 2012;18(4):725-36.
161. Halfvarson J, Bodin L, Tysk C, Lindberg E, Jarnerot G. Inflammatory bowel disease in a Swedish twin cohort: a long-term follow-up of concordance and clinical characteristics. Gastroenterology 2003;124(7):1767-73.
162. Spehlmann ME, Begun AZ, Burghardt J, Lepage P, Raedler A, Schreiber S. Epidemiology of inflammatory bowel disease in a German twin cohort: results of a nationwide study. Inflamm. Bowel Dis. 2008;14(7):968-76.
163. de Lange KM, Moutsianas L, Lee JC, et al. Genome-wide association study implicates immune activation of multiple integrin genes in inflammatory bowel disease. Nat. Genet. 2017;49(2):256-261.
164. Park JH, Wacholder S, Gail MH, et al. Estimation of effect size distribution from genome-wide association studies and implications for future discoveries. Nat. Genet. 2010;42(7):570-5.
165. Khor B, Gardet A, Xavier RJ. Genetics and pathogenesis of inflammatory bowel disease. Nature 2011;474(7351):307-17.
166. Samuelsson SM. Ulcerös kolit och proktit: Uppsala University; 1976.
167. Harries AD, Baird A, Rhodes J. Non-smoking: a feature of ulcerative colitis. Br. Med. J. (Clin. Res. Ed) 1982;284(6317):706.
CARL ERIKSSON Inflammatory Bowel Disease 85
168. Vessey M, Jewell D, Smith A, Yeates D, McPherson K. Chronic inflammatory bowel disease, cigarette smoking, and use of oral contraceptives: findings in a large cohort study of women of childbearing age. Br. Med. J. (Clin. Res. Ed) 1986;292(6528):1101-3.
169. Boyko EJ, Koepsell TD, Perera DR, Inui TS. Risk of ulcerative colitis among former and current cigarette smokers. N. Engl. J. Med. 1987;316(12):707-10.
170. Tobin MV, Logan RF, Langman MJ, McConnell RB, Gilmore IT. Cigarette smoking and inflammatory bowel disease. Gastroenterology 1987;93(2):316-21.
171. Lindberg E, Tysk C, Andersson K, Jarnerot G. Smoking and inflammatory bowel disease. A case control study. Gut 1988;29(3):352-7.
172. Boyko EJ, Perera DR, Koepsell TD, Keane EM, Inui TS. Effects of cigarette smoking on the clinical course of ulcerative colitis. Scand. J. Gastroenterol. 1988;23(9):1147-52.
173. Pullan RD, Rhodes J, Ganesh S, et al. Transdermal nicotine for active ulcerative colitis. N. Engl. J. Med. 1994;330(12):811-5.
174. Sandborn WJ, Tremaine WJ, Offord KP, et al. Transdermal nicotine for mildly to moderately active ulcerative colitis. A randomized, double-blind, placebo-controlled trial. Ann. Intern. Med. 1997;126(5):364-71.
175. Thomas GA, Rhodes J, Ragunath K, et al. Transdermal nicotine compared with oral prednisolone therapy for active ulcerative colitis. Eur. J. Gastroenterol. Hepatol. 1996;8(8):769-76.
176. Persson PG, Hellers G, Ahlbom A. Use of oral moist snuff and inflammatory bowel disease. Int. J. Epidemiol. 1993;22(6):1101-3.
177. Carlens C, Hergens MP, Grunewald J, et al. Smoking, use of moist snuff, and risk of chronic inflammatory diseases. Am. J. Respir. Crit. Care Med. 2010;181(11):1217-22.
178. Franceschi S, Panza E, La Vecchia C, Parazzini F, Decarli A, Bianchi Porro G. Nonspecific inflammatory bowel disease and smoking. Am. J. Epidemiol. 1987;125(3):445-52.
179. Kuenzig ME, Lee SM, Eksteen B, et al. Smoking influences the need for surgery in patients with the inflammatory bowel diseases: a systematic review and meta-analysis incorporating disease duration. BMC Gastroenterol. 2016;16(1):143.
180. Sutherland LR, Ramcharan S, Bryant H, Fick G. Effect of cigarette smoking on recurrence of Crohn's disease. Gastroenterology 1990;98(5 Pt 1):1123-8.
181. Sartor RB. Microbial influences in inflammatory bowel diseases. Gastroenterology 2008;134(2):577-94.
86 CARL ERIKSSON Inflammatory Bowel Disease
182. Andersson RE, Olaison G, Tysk C, Ekbom A. Appendectomy andprotection against ulcerative colitis. N. Engl. J. Med.2001;344(11):808-14.
183. Frisch M, Johansen C, Mellemkjaer L, et al. Appendectomy andsubsequent risk of inflammatory bowel diseases. Surgery2001;130(1):36-43.
184. Gent AE, Hellier MD, Grace RH, Swarbrick ET, Coggon D.Inflammatory bowel disease and domestic hygiene in infancy.Lancet 1994;343(8900):766-7.
185. Radford-Smith GL, Edwards JE, Purdie DM, et al. Protective role ofappendicectomy on onset and severity of ulcerative colitis andCrohn's disease. Gut 2002;51(6):808-13.
186. Kaplan GG, Jackson T, Sands BE, Frisch M, Andersson RE,Korzenik J. The risk of developing Crohn's disease after anappendectomy: a meta-analysis. Am. J. Gastroenterol.2008;103(11):2925-31.
187. Kaplan GG, Pedersen BV, Andersson RE, Sands BE, Korzenik J,Frisch M. The risk of developing Crohn's disease after anappendectomy: a population-based cohort study in Sweden andDenmark. Gut 2007;56(10):1387-92.
188. Roblin X, Neut C, Darfeuille-Michaud A, Colombel JF. Localappendiceal dysbiosis: the missing link between the appendix andulcerative colitis? Gut 2012;61(4):635-6.
189. Cornish JA, Tan E, Simillis C, Clark SK, Teare J, Tekkis PP. Therisk of oral contraceptives in the etiology of inflammatory boweldisease: a meta-analysis. Am. J. Gastroenterol. 2008;103(9):2394-400.
190. Khalili H, Higuchi LM, Ananthakrishnan AN, et al. Oralcontraceptives, reproductive factors and risk of inflammatory boweldisease. Gut 2013;62(8):1153-9.
191. Khalili H, Higuchi LM, Ananthakrishnan AN, et al. HormoneTherapy Increases Risk of Ulcerative Colitis but not Crohn’sDisease. Gastroenterology 2012;143(5):1199-1206.
192. Garcia Rodriguez LA, Gonzalez-Perez A, Johansson S, WallanderMA. Risk factors for inflammatory bowel disease in the generalpopulation. Aliment. Pharmacol. Ther. 2005;22(4):309-15.
193. Matuk R, Crawford J, Abreu MT, Targan SR, Vasiliauskas EA,Papadakis KA. The spectrum of gastrointestinal toxicity and effecton disease activity of selective cyclooxygenase-2 inhibitors inpatients with inflammatory bowel disease. Inflamm. Bowel Dis.2004;10(4):352-6.
CARL ERIKSSON Inflammatory Bowel Disease 87
194. Meyer AM, Ramzan NN, Heigh RI, Leighton JA. Relapse of inflammatory bowel disease associated with use of nonsteroidal anti-inflammatory drugs. Dig. Dis. Sci. 2006;51(1):168-72.
195. Takeuchi K, Smale S, Premchand P, et al. Prevalence and mechanism of nonsteroidal anti-inflammatory drug-induced clinical relapse in patients with inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2006;4(2):196-202.
196. Smecuol E, Bai JC, Sugai E, et al. Acute gastrointestinal permeability responses to different non-steroidal anti-inflammatory drugs. Gut 2001;49(5):650-5.
197. Salim SY, Soderholm JD. Importance of disrupted intestinal barrier in inflammatory bowel diseases. Inflamm. Bowel Dis. 2011;17(1):362-81.
198. Teshima CW, Dieleman LA, Meddings JB. Abnormal intestinal permeability in Crohn's disease pathogenesis. Ann. N. Y. Acad. Sci. 2012;1258:159-65.
199. Ananthakrishnan AN, Higuchi LM, Huang ES, et al. Aspirin, nonsteroidal anti-inflammatory drug use, and risk for Crohn disease and ulcerative colitis: a cohort study. Ann. Intern. Med. 2012;156(5):350-9.
200. Frank DN, St Amand AL, Feldman RA, Boedeker EC, Harpaz N, Pace NR. Molecular-phylogenetic characterization of microbial community imbalances in human inflammatory bowel diseases. Proc. Natl. Acad. Sci. U. S. A. 2007;104(34):13780-5.
201. Dave M, Higgins PD, Middha S, Rioux KP. The human gut microbiome: current knowledge, challenges, and future directions. Transl. Res. 2012;160(4):246-57.
202. O'Hara AM, Shanahan F. The gut flora as a forgotten organ. EMBO reports 2006;7(7):688-93.
203. Peterson DA, Frank DN, Pace NR, Gordon JI. Metagenomic approaches for defining the pathogenesis of inflammatory bowel diseases. Cell host & microbe 2008;3(6):417-27.
204. Eckburg PB, Bik EM, Bernstein CN, et al. Diversity of the human intestinal microbial flora. Science 2005;308(5728):1635-8.
205. Willing BP, Dicksved J, Halfvarson J, et al. A pyrosequencing study in twins shows that gastrointestinal microbial profiles vary with inflammatory bowel disease phenotypes. Gastroenterology 2010;139(6):1844-1854.e1.
206. Manichanh C, Rigottier-Gois L, Bonnaud E, et al. Reduced diversity of faecal microbiota in Crohn's disease revealed by a metagenomic approach. Gut 2006;55(2):205-11.
88 CARL ERIKSSON Inflammatory Bowel Disease
207. Rajca S, Grondin V, Louis E, et al. Alterations in the intestinal microbiome (dysbiosis) as a predictor of relapse after infliximab withdrawal in Crohn's disease. Inflamm. Bowel Dis. 2014;20(6):978-86.
208. Costello SP, Soo W, Bryant RV, Jairath V, Hart AL, Andrews JM. Systematic review with meta-analysis: faecal microbiota transplantation for the induction of remission for active ulcerative colitis. Aliment. Pharmacol. Ther. 2017;46(3):213-224.
209. Kostic AD, Xavier RJ, Gevers D. The microbiome in inflammatory bowel disease: current status and the future ahead. Gastroenterology 2014;146(6):1489-99.
210. Wurzelmann JI, Lyles CM, Sandler RS. Childhood infections and the risk of inflammatory bowel disease. Dig. Dis. Sci. 1994;39(3):555-60.
211. Gilat T, Hacohen D, Lilos P, Langman MJ. Childhood factors in ulcerative colitis and Crohn's disease. An international cooperative study. Scand. J. Gastroenterol. 1987;22(8):1009-24.
212. Ungaro R, Bernstein CN, Gearry R, et al. Antibiotics associated with increased risk of new-onset Crohn's disease but not ulcerative colitis: a meta-analysis. Am. J. Gastroenterol. 2014;109(11):1728-38.
213. Hviid A, Svanstrom H, Frisch M. Antibiotic use and inflammatory bowel diseases in childhood. Gut 2011;60(1):49-54.
214. Virta L, Auvinen A, Helenius H, Huovinen P, Kolho KL. Association of repeated exposure to antibiotics with the development of pediatric Crohn's disease--a nationwide, register-based finnish case-control study. Am. J. Epidemiol. 2012;175(8):775-84.
215. Shaw SY, Blanchard JF, Bernstein CN. Association between the use of antibiotics in the first year of life and pediatric inflammatory bowel disease. Am. J. Gastroenterol. 2010;105(12):2687-92.
216. Ng SC, Bernstein CN, Vatn MH, et al. Geographical variability and environmental risk factors in inflammatory bowel disease. Gut 2013;62(4):630-49.
217. Hou JK, Abraham B, El-Serag H. Dietary intake and risk of developing inflammatory bowel disease: a systematic review of the literature. Am. J. Gastroenterol. 2011;106(4):563-73.
218. Ananthakrishnan AN, Khalili H, Konijeti GG, et al. A prospective study of long-term intake of dietary fiber and risk of Crohn's disease and ulcerative colitis. Gastroenterology 2013;145(5):970-7.
219. Ananthakrishnan AN, Khalili H, Song M, et al. High School Diet and Risk of Crohn's Disease and Ulcerative Colitis. Inflamm. Bowel Dis. 2015;21(10):2311-9.
CARL ERIKSSON Inflammatory Bowel Disease 89
220. Ananthakrishnan AN, Khalili H, Konijeti GG, et al. Long-term intake of dietary fat and risk of ulcerative colitis and Crohn's disease. Gut 2014;63(5):776-84.
221. Jantchou P, Morois S, Clavel-Chapelon F, Boutron-Ruault MC, Carbonnel F. Animal protein intake and risk of inflammatory bowel disease: The E3N prospective study. Am. J. Gastroenterol. 2010;105(10):2195-201.
222. Tjonneland A, Overvad K, Bergmann MM, et al. Linoleic acid, a dietary n-6 polyunsaturated fatty acid, and the aetiology of ulcerative colitis: a nested case-control study within a European prospective cohort study. Gut 2009;58(12):1606-11.
223. Sharon P, Ligumsky M, Rachmilewitz D, Zor U. Role of prostaglandins in ulcerative colitis. Enhanced production during active disease and inhibition by sulfasalazine. Gastroenterology 1978;75(4):638-40.
224. De Filippo C, Cavalieri D, Di Paola M, et al. Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proc. Natl. Acad. Sci. U. S. A. 2010;107(33):14691-6.
225. Heuschkel RB, Menache CC, Megerian JT, Baird AE. Enteral nutrition and corticosteroids in the treatment of acute Crohn's disease in children. J. Pediatr. Gastroenterol. Nutr. 2000;31(1):8-15.
226. Dziechciarz P, Horvath A, Shamir R, Szajewska H. Meta-analysis: enteral nutrition in active Crohn's disease in children. Aliment. Pharmacol. Ther. 2007;26(6):795-806.
227. Zachos M, Tondeur M, Griffiths AM. Enteral nutritional therapy for induction of remission in Crohn's disease. The Cochrane database of systematic reviews 2007(1):Cd000542.
228. Svartz M. The treatment of 124 cases of ulcerative colitis with salazopyrine and attempts of desensibilization in cases of hypersensitiveness to sulfa. Acta Med. Scand. 1948;131(Suppl 206):465-72.
229. Wang Y, Parker CE, Bhanji T, Feagan BG, MacDonald JK. Oral 5-aminosalicylic acid for induction of remission in ulcerative colitis. The Cochrane database of systematic reviews 2016;4:Cd000543.
230. Wang Y, Parker CE, Feagan BG, MacDonald JK. Oral 5-aminosalicylic acid for maintenance of remission in ulcerative colitis. Cochrane Database of Systematic Reviews 2016(5).
231. Gordon M, Naidoo K, Thomas AG, Akobeng AK. Oral 5-aminosalicylic acid for maintenance of surgically-induced remission in Crohn's disease. The Cochrane database of systematic reviews 2011(1):Cd008414.
90 CARL ERIKSSON Inflammatory Bowel Disease
232. Akobeng AK, Zhang D, Gordon M, MacDonald JK. Oral 5-aminosalicylic acid for maintenance of medically-induced remissionin Crohn's disease. The Cochrane database of systematic reviews2016;9:Cd003715.
233. Ford AC, Kane SV, Khan KJ, et al. Efficacy of 5-aminosalicylates inCrohn's disease: systematic review and meta-analysis. Am. J.Gastroenterol. 2011;106(4):617-29.
234. Lim W-C, Wang Y, MacDonald JK, Hanauer S. Aminosalicylatesfor induction of remission or response in Crohn's disease. CochraneDatabase of Systematic Reviews 2016(7).
235. Hench PS, Kendall EC, et al. The effect of a hormone of the adrenalcortex (17-hydroxy-11-dehydrocorticosterone; compound E) and ofpituitary adrenocorticotropic hormone on rheumatoid arthritis.Proceedings of the staff meetings. Mayo Clinic 1949;24(8):181-97.
236. Steinhart AH, Ewe K, Griffiths AM, Modigliani R, Thomsen OO.Corticosteroids for maintenance of remission in Crohn's disease.Cochrane Database of Systematic Reviews 2003(4).
237. Ishaq S, Akobeng AK. Oral corticosteroids for induction ofremission in ulcerative colitis. Cochrane Database of SystematicReviews 2007(3).
238. Benchimol EI, Seow CH, Steinhart AH, Griffiths AM. Traditionalcorticosteroids for induction of remission in Crohn's disease.Cochrane Database of Systematic Reviews 2008(2).
239. Bean RH. The treatment of chronic ulcerative colitis with 6-mercaptopurine. Med. J. Aust. 1962;49(2):592-3.
240. Schwartz R, Stack J, Dameshek W. Effect of 6-mercaptopurine onantibody production. Proc. Soc. Exp. Biol. Med. 1958;99(1):164-7.
241. Chande N, Patton PH, Tsoulis DJ, Thomas BS, MacDonald JK.Azathioprine or 6-mercaptopurine for maintenance of remission inCrohn's disease. The Cochrane database of systematic reviews2015(10):Cd000067.
242. Gordon M, Taylor K, Akobeng AK, Thomas AG. Azathioprine and6-mercaptopurine for maintenance of surgically-induced remissionin Crohn's disease. The Cochrane database of systematic reviews2014(8):Cd010233.
243. Timmer A, Patton PH, Chande N, McDonald JW, MacDonald JK.Azathioprine and 6-mercaptopurine for maintenance of remission inulcerative colitis. The Cochrane database of systematic reviews2016(5):Cd000478.
244. Chande N, Tsoulis DJ, MacDonald JK. Azathioprine or 6-mercaptopurine for induction of remission in Crohn's disease. TheCochrane database of systematic reviews 2013(4):Cd000545.
CARL ERIKSSON Inflammatory Bowel Disease 91
245. Gisbert JP, Linares PM, McNicholl AG, Mate J, Gomollon F. Meta-analysis: the efficacy of azathioprine and mercaptopurine in ulcerative colitis. Aliment. Pharmacol. Ther. 2009;30(2):126-37.
246. Connell WR, Kamm MA, Ritchie JK, Lennard-Jones JE. Bone marrow toxicity caused by azathioprine in inflammatory bowel disease: 27 years of experience. Gut 1993;34(8):1081-5.
247. Gearry RB, Barclay ML, Burt MJ, Collett JA, Chapman BA. Thiopurine drug adverse effects in a population of New Zealand patients with inflammatory bowel disease. Pharmacoepidemiol. Drug Saf. 2004;13(8):563-7.
248. Hindorf U, Lindqvist M, Hildebrand H, Fagerberg U, Almer S. Adverse events leading to modification of therapy in a large cohort of patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2006;24(2):331-42.
249. Weinshilboum RM, Sladek SL. Mercaptopurine pharmacogenetics: monogenic inheritance of erythrocyte thiopurine methyltransferase activity. Am. J. Hum. Genet. 1980;32(5):651-62.
250. Beutler B, Milsark IW, Cerami AC. Passive immunization against cachectin/tumor necrosis factor protects mice from lethal effect of endotoxin. Science 1985;229(4716):869-71.
251. Fisher CJ, Jr., Zimmerman J, Khazaeli MB, et al. Initial evaluation of human monoclonal anti-lipid A antibody (HA-1A) in patients with sepsis syndrome. Crit. Care Med. 1990;18(12):1311-5.
252. Ziegler EJ, Fisher CJ, Jr., Sprung CL, et al. Treatment of gram-negative bacteremia and septic shock with HA-1A human monoclonal antibody against endotoxin. A randomized, double-blind, placebo-controlled trial. The HA-1A Sepsis Study Group. N. Engl. J. Med. 1991;324(7):429-36.
253. MacDonald TT, Hutchings P, Choy MY, Murch S, Cooke A. Tumour necrosis factor-alpha and interferon-gamma production measured at the single cell level in normal and inflamed human intestine. Clin. Exp. Immunol. 1990;81(2):301-305.
254. Keffer J, Probert L, Cazlaris H, et al. Transgenic mice expressing human tumour necrosis factor: a predictive genetic model of arthritis. The EMBO Journal 1991;10(13):4025-4031.
255. van Dullemen HM, van Deventer SJ, Hommes DW, et al. Treatment of Crohn's disease with anti-tumor necrosis factor chimeric monoclonal antibody (cA2). Gastroenterology 1995;109(1):129-35.
256. Behm BW, Bickston SJ. Tumor necrosis factor-alpha antibody for maintenance of remission in Crohn's disease. Cochrane Database of Systematic Reviews 2008(1).
92 CARL ERIKSSON Inflammatory Bowel Disease
257. Lawson MM, Thomas AG, Akobeng AK. Tumour necrosis factoralpha blocking agents for induction of remission in ulcerativecolitis. Cochrane Database of Systematic Reviews 2006(3).
258. Danese S, Fiorino G, Peyrin-Biroulet L, et al. Biological agents formoderately to severely active ulcerative colitis: a systematic reviewand network meta-analysis. Ann. Intern. Med. 2014;160(10):704-11.
259. Gisbert JP, Marin AC, McNicholl AG, Chaparro M. Systematicreview with meta-analysis: the efficacy of a second anti-TNF inpatients with inflammatory bowel disease whose previous anti-TNFtreatment has failed. Aliment. Pharmacol. Ther. 2015;41(7):613-23.
260. Andersen NN, Jess T. Risk of infections associated with biologicaltreatment in inflammatory bowel disease. World J. Gastroenterol.2014;20(43):16014-9.
261. Khanna D, McMahon M, Furst DE. Anti-tumor necrosis factoralpha therapy and heart failure: what have we learned and wheredo we go from here? Arthritis Rheum. 2004;50(4):1040-50.
262. Fuss IJ, Heller F, Boirivant M, et al. Nonclassical CD1d-restrictedNK T cells that produce IL-13 characterize an atypical Th2response in ulcerative colitis. J. Clin. Invest. 2004;113(10):1490-7.
263. Moćko P, Kawalec P, Smela-Lipińska B, Pilc A. Effectiveness andsafety of vedolizumab for treatment of Crohn's disease: a systematicreview and meta-analysis. Archives of Medical Science : AMS2016;12(5):1088-1096.
264. Mosli MH, MacDonald JK, Bickston SJ, et al. Vedolizumab forinduction and maintenance of remission in ulcerative colitis: aCochrane systematic review and meta-analysis. Inflamm. BowelDis. 2015;21(5):1151-9.
265. Neumann H. Treatment of Chronic Ulcerative Colitis byPneumoperitoneum. Br. Med. J. 1943;1(4278):9-10.
266. Dennis C, Eddy FD. Evaluation of vagotomy in chronic, non-specific ulcerative colitis. Proc. Soc. Exp. Biol. Med.1947;65(2):306.
267. Yeomans FC. Appendicostomy in chronic ulcerative colitis. N. Y.State J. Med. 1946;46:2269-71.
268. Garlock JH, Crohn BB, Klein SH, Yarnis H. An appraisal of thelong-term results of surgical treatment of regional ileitis.Gastroenterology 1951;19(3):414-23.
269. Brown YJ. The value of complete physiological rest of the largebowel in the treatment of ulcerative and obstructive lesions of thisorgan. Surg. Gynecol. Obstet. 1913;16(610-613).
270. Aufses AH, Kreel I. Ileostomy for granulomatous ileocolitis. Ann.Surg. 1971;173(1):91-96.
CARL ERIKSSON Inflammatory Bowel Disease 93
271. Burman JH, Thompson H, Cooke WT, Williams JA. The effects of diversion of intestinal contents on the progress of Crohn's disease of the large bowel. Gut 1971;12(1):11-15.
272. Jones JH, Lennard-Jones JE, Lockhart-Mummery HE. Experience in the treatment of Crohn's disease of the large intestine. Gut 1966;7(5):448-452.
273. McIlrath DC. Diverting ileostomy or colostomy in the management of Crohn's disease of the colon. Arch. Surg. 1971;103(2):308-10.
274. Krause U, Ejerblad S, Bergman L. Crohn's disease. A long-term study of the clinical course in 186 patients. Scand. J. Gastroenterol. 1985;20(4):516-24.
275. Softley A, Myren J, Clamp SE, Bouchier IA, Watkinson G, de Dombal FT. Factors affecting recurrence after surgery for Crohn's disease. Scand. J. Gastroenterol. Suppl. 1988;144:31-4.
276. Williams JA. The place of surgery in Crohn's disease. Gut 1971;12(9):739-49.
277. Flatmark A, Fretheim B, Gjone E. Early colectomy in severe ulcerative colitis. Scand. J. Gastroenterol. 1975;10(4):427-31.
278. Gallagher ND, Goulston SJM, Wyndham N, Morrow W. The management of fulminant ulcerative colitis. Gut 1962;3(4):306-311.
279. Wright AD. Ulcerative Colitis Complicated by Polyarthritis treated by Total Colectomy. Proc. R. Soc. Med. 1942;35(3):189-190.
280. Parks AG, Nicholls RJ. Proctocolectomy without ileostomy for ulcerative colitis. Br. Med. J. 1978;2(6130):85-88.
281. Fazio VW, Marchetti F, Church M, et al. Effect of resection margins on the recurrence of Crohn's disease in the small bowel. A randomized controlled trial. Ann. Surg. 1996;224(4):563-71; discussion 571-3.
282. Booth CC. The Metabolic Effects of Intestinal Resection in Man. Postgrad. Med. J. 1961;37(434):725-739.
283. Thompson JS, Iyer KR, DiBaise JK, Young RL, Brown CR, Langnas AN. Short bowel syndrome and Crohn's disease. J. Gastrointest. Surg. 2003;7(8):1069-72.
284. Reese GE, Purkayastha S, Tilney HS, Von Roon A, Yamamoto T, Tekkis PP. Strictureplasty vs resection in small bowel Crohn's disease: an evaluation of short-term outcomes and recurrence. Colorectal Dis. 2007;9(8):686-694.
285. Bordeianou L, Hodin RA. Expanding the role of strictureplasty: can resections be made obsolete? Inflamm. Bowel Dis. 2005;11(9):861-2.
94 CARL ERIKSSON Inflammatory Bowel Disease
286. Tichansky D, Cagir B, Yoo E, Marcus SM, Fry RD. Strictureplastyfor Crohn's disease: meta-analysis. Dis. Colon Rectum2000;43(7):911-9.
287. Statistics Sweden. Tables on the population in Sweden. In; 2017.288. Carleson R, Fristedt B, Philipson J. Ulcerative colitis; a follow-up
investigation of a 20-year primary material. Acta Med. Scand.1962;172:647-56.
289. Zhulina Y, Udumyan R, Henriksson I, Tysk C, Montgomery S,Halfvarson J. Temporal trends in non-stricturing and non-penetrating behaviour at diagnosis of Crohn's disease in Orebro,Sweden: a population-based retrospective study. Journal of Crohn's& colitis 2014;8(12):1653-60.
290. Busch K, Ludvigsson JF, Ekstrom-Smedby K, Ekbom A, Askling J,Neovius M. Nationwide prevalence of inflammatory bowel diseasein Sweden: a population-based register study. Aliment. Pharmacol.Ther. 2014;39(1):57-68.
291. Jakobsson GL, Sternegard E, Olen O, et al. Validatinginflammatory bowel disease (IBD) in the Swedish National PatientRegister and the Swedish Quality Register for IBD (SWIBREG).Scand. J. Gastroenterol. 2017;52(2):216-221.
292. Ludvigsson JF, Myrelid P. [Swibreg--a new version of national IBDregistry]. Lakartidningen 2009;106(45):3014-5.
293. Swedish Inflamatory Bowel Disease Regestry. SWIBREG. In; 2016.294. Mann HB, Whitney DR. On a Test of Whether one of Two
Random Variables is Stochastically Larger than the Other. Ann.Math. Statist. 1947;18(1):50-60.
295. Wilcoxon F. Individual Comparisons by Ranking Methods.Biometrics Bulletin 1945;1(6):80-83.
296. Dunn OJ. Multiple Comparisons among Means. Journal of theAmerican Statistical Association 1961;56(293):52-64.
297. Hornung RW, Reed LD. Estimation of Average Concentration inthe Presence of Nondetectable Values. Appl. Occup. Environ. Hyg.1990;5(1):46-51.
298. Pearson K. X. On the criterion that a given system of deviationsfrom the probable in the case of a correlated system of variables issuch that it can be reasonably supposed to have arisen from randomsampling. The London, Edinburgh, and Dublin PhilosophicalMagazine and Journal of Science 1900;50(302):157-175.
299. Fisher RA. On the Interpretation of χ<sup>2</sup> fromContingency Tables, and the Calculation of P. Journal of the RoyalStatistical Society 1922;85(1):87-94.
CARL ERIKSSON Inflammatory Bowel Disease 95
300. Kaplan EL, Meier P. Nonparametric Estimation from Incomplete Observations. Journal of the American Statistical Association 1958;53(282):457-481.
301. Mantel N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother. Rep. 1966;50(3):163-70.
302. Rhiel GS, Wilkie WC. An Investigation of the Large-Sample/Small-Sample Approach to the One-Sample Test for a Mean (Sigma Unknown). Journal of Statistics Education 1996;4(3):null-null.
303. Abramson JH. Age-standardization in epidemiological data. Int. J. Epidemiol. 1995;24(1):238-9.
304. Anderson RN, Rosenberg HM. Age standardization of death rates: implementation of the year 2000 standard. Natl. Vital Stat. Rep. 1998;47(3):1-16, 20.
305. Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008;3(1):17.
306. Cox DR. The Regression Analysis of Binary Sequences. Journal of the Royal Statistical Society. Series B (Methodological) 1958;20(2):215-242.
307. Wilks SS. The Large-Sample Distribution of the Likelihood Ratio for Testing Composite Hypotheses. Ann. Math. Statist. 1938;9(1):60-62.
308. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996;49(12):1373-9.
309. Cox DR. Regression Models and Life-Tables. Journal of the Royal Statistical Society. Series B (Methodological) 1972;34(2):187-220.
310. Hess KR. Graphical methods for assessing violations of the proportional hazards assumption in Cox regression. Stat. Med. 1995;14(15):1707-23.
311. Consul PC, Famoye F. Generalized poisson regression model. Communications in Statistics - Theory and Methods 1992;21(1):89-109.
312. Eriksson C, Cao Y, Rundquist S, et al. Changes in medical management and colectomy rates: a population-based cohort study on the epidemiology and natural history of ulcerative colitis in Orebro, Sweden, 1963-2010. Aliment. Pharmacol. Ther. 2017.
313. Fonager K, Sorensen HT, Olsen J. Change in incidence of Crohn's disease and ulcerative colitis in Denmark. A study based on the National Registry of Patients, 1981-1992. Int. J. Epidemiol. 1997;26(5):1003-8.
96 CARL ERIKSSON Inflammatory Bowel Disease
314. Molinie F, Gower-Rousseau C, Yzet T, et al. Opposite evolution in incidence of Crohn's disease and ulcerative colitis in Northern France (1988-1999). Gut 2004;53(6):843-8.
315. Romberg-Camps MJ, Hesselink-van de Kruijs MA, Schouten LJ, et al. Inflammatory Bowel Disease in South Limburg (the Netherlands) 1991-2002: Incidence, diagnostic delay, and seasonal variations in onset of symptoms. Journal of Crohn's & colitis 2009;3(2):115-24.
316. Bjornsson S, Tryggvason F, Jonasson JG, et al. Incidence of inflammatory bowel disease in Iceland 1995 - 2009. A nationwide population-based study. Scand. J. Gastroenterol. 2015;50(11):1368-75.
317. Jussila A, Virta LJ, Kautiainen H, Rekiaro M, Nieminen U, Farkkila MA. Increasing incidence of inflammatory bowel diseases between 2000 and 2007: a nationwide register study in Finland. Inflamm. Bowel Dis. 2012;18(3):555-61.
318. Sjoberg D, Holmstrom T, Larsson M, et al. Incidence and natural history of ulcerative colitis in the Uppsala Region of Sweden 2005-2009 - results from the IBD cohort of the Uppsala Region (ICURE). Journal of Crohn's & colitis 2013;7(9):e351-7.
319. Sjoberg D, Holmstrom T, Larsson M, et al. Incidence and clinical course of Crohn's disease during the first year - results from the IBD Cohort of the Uppsala Region (ICURE) of Sweden 2005-2009. Journal of Crohn's & colitis 2014;8(3):215-22.
320. Danese S, Vuitton L, Peyrin-Biroulet L. Biologic agents for IBD: practical insights. Nat. Rev. Gastroenterol. Hepatol. 2015;12(9):537-45.
321. Chan HC, Ng SC. Emerging biologics in inflammatory bowel disease. J. Gastroenterol. 2017;52(2):141-150.
322. Feagan BG, Panaccione R, Sandborn WJ, et al. Effects of adalimumab therapy on incidence of hospitalization and surgery in Crohn's disease: results from the CHARM study. Gastroenterology 2008;135(5):1493-9.
323. Dignass A, Van Assche G, Lindsay JO, et al. The second European evidence-based Consensus on the diagnosis and management of Crohn's disease: Current management. Journal of Crohn's & colitis 2010;4(1):28-62.
324. Dignass A, Lindsay JO, Sturm A, et al. Second European evidence-based consensus on the diagnosis and management of ulcerative colitis part 2: current management. Journal of Crohn's & colitis 2012;6(10):991-1030.
325. Lemann M, Mary JY, Duclos B, et al. Infliximab plus azathioprine for steroid-dependent Crohn's disease patients: a randomized placebo-controlled trial. Gastroenterology 2006;130(4):1054-61.
CARL ERIKSSON Inflammatory Bowel Disease 97
326. D'Haens G, Baert F, van Assche G, et al. Early combined immunosuppression or conventional management in patients with newly diagnosed Crohn's disease: an open randomised trial. Lancet 2008;371(9613):660-667.
327. Colombel J-F, Panaccione R, Bossuyt P, et al. Effect of tight control management on Crohn's disease (CALM): a multicentre, randomised, controlled phase 3 trial. The Lancet;390(10114):2779-2789.
328. Binder V. Clinical epidemiology--how important now? Gut 2005;54(5):574-5.
329. Ho PR, Koendgen H, Campbell N, Haddock B, Richman S, Chang I. Risk of natalizumab-associated progressive multifocal leukoencephalopathy in patients with multiple sclerosis: a retrospective analysis of data from four clinical studies. Lancet Neurol. 2017;16(11):925-933.
330. Miller DH, Khan OA, Sheremata WA, et al. A controlled trial of natalizumab for relapsing multiple sclerosis. N. Engl. J. Med. 2003;348(1):15-23.
331. Ghosh S, Goldin E, Gordon FH, et al. Natalizumab for active Crohn's disease. N. Engl. J. Med. 2003;348(1):24-32.
332. Sandborn WJ, Colombel JF, Enns R, et al. Natalizumab induction and maintenance therapy for Crohn's disease. N. Engl. J. Med. 2005;353(18):1912-25.
333. Dong-Si T, Richman S, Wattjes MP, et al. Outcome and survival of asymptomatic PML in natalizumab-treated MS patients. Annals of Clinical and Translational Neurology 2014;1(10):755-764.
334. Rungoe C, Langholz E, Andersson M, et al. Changes in medical treatment and surgery rates in inflammatory bowel disease: a nationwide cohort study 1979-2011. Gut 2014;63(10):1607-16.
335. Chhaya V, Saxena S, Cecil E, et al. The impact of timing and duration of thiopurine treatment on colectomy in ulcerative colitis: a national population-based study of incident cases between 1989-2009. Aliment. Pharmacol. Ther. 2015;41(1):87-98.
336. Gunesh S, Thomas GA, Williams GT, Roberts A, Hawthorne AB. The incidence of Crohn's disease in Cardiff over the last 75 years: an update for 1996-2005. Aliment. Pharmacol. Ther. 2008;27(3):211-9.
337. Wickbom A, Bohr J, Eriksson S, Udumyan R, Nyhlin N, Tysk C. Stable incidence of collagenous colitis and lymphocytic colitis in Orebro, Sweden, 1999-2008: a continuous epidemiologic study. Inflamm. Bowel Dis. 2013;19(11):2387-93.
98 CARL ERIKSSON Inflammatory Bowel Disease
338. Gasche C, Berstad A, Befrits R, et al. Guidelines on the diagnosisand management of iron deficiency and anemia in inflammatorybowel diseases. Inflamm. Bowel Dis. 2007;13(12):1545-53.
339. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emergingconsensus on rating quality of evidence and strength ofrecommendations. BMJ 2008;336(7650):924-6.
340. Mann CJ. Observational research methods. Research design II:cohort, cross sectional, and case-control studies. Emerg. Med. J.2003;20(1):54-60.
341. Altman DG, Bland JM. Uncertainty and sampling error. BMJ :British Medical Journal 2014;349.
342. Walter SD. Methods of reporting statistical results from medicalresearch studies. Am. J. Epidemiol. 1995;141(10):896-906.
343. Sackett DL. Bias in analytic research. J. Chronic Dis. 1979;32(1-2):51-63.
344. Zaccai JH. How to assess epidemiological studies. Postgrad. Med. J.2004;80(941):140-147.
345. Rothman KJ, Greenland S. Validity and Generalizability inEpidemiologic Studies. In: Encyclopedia of Biostatistics: John Wiley& Sons, Ltd; 2005.
346. Kaitha S, Bashir M, Ali T. Iron deficiency anemia in inflammatorybowel disease. World J. Gastrointest. Pathophysiol. 2015;6(3):62-72.
347. Jarnerot G, Hertervig E, Friis-Liby I, et al. Infliximab as rescuetherapy in severe to moderately severe ulcerative colitis: arandomized, placebo-controlled study. Gastroenterology2005;128(7):1805-11.
348. Sandborn WJ, Feagan BG, Marano C, et al. Subcutaneousgolimumab induces clinical response and remission in patients withmoderate-to-severe ulcerative colitis. Gastroenterology2014;146(1):85-95; quiz e14-5.
349. Sandborn WJ, Feagan BG, Marano C, et al. Subcutaneousgolimumab maintains clinical response in patients with moderate-to-severe ulcerative colitis. Gastroenterology 2014;146(1):96-109.e1.
350. Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumabinduces and maintains clinical remission in patients with moderate-to-severe ulcerative colitis. Gastroenterology 2012;142(2):257-65.e1-3.
351. Feagan BG, Rutgeerts P, Sands BE, et al. Vedolizumab as inductionand maintenance therapy for ulcerative colitis. N. Engl. J. Med.2013;369(8):699-710.

CARL ERIKSSON Inflammatory Bowel Disease 99
352. Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A. The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur. J. Epidemiol. 2009;24(11):659-67.

CARL ERIKSSON Inflammatory Bowel Disease 99
352. Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A.The Swedish personal identity number: possibilities and pitfalls inhealthcare and medical research. Eur. J. Epidemiol.2009;24(11):659-67.
Publications in the series
Örebro Studies in Medicine
1. Bergemalm, Per-Olof (2004). Audiologic and cognitive long-termsequelae from closed head injury.
2. Jansson, Kjell (2004). Intraperitoneal Microdialysis.Technique and Results.
3. Windahl, Torgny (2004). Clinical aspects of laser treatment oflichen sclerosus and squamous cell carcinoma of the penis.
4. Carlsson, Per-Inge (2004). Hearing impairment and deafness.Genetic and environmental factors – interactions – consequences.A clinical audiological approach.
5. Wågsäter, Dick (2005). CXCL16 and CD137 in Atherosclerosis.
6. Jatta, Ken (2006). Inflammation in Atherosclerosis.
7. Dreifaldt, Ann Charlotte (2006). Epidemiological Aspects onMalignant Diseases in Childhood.
8. Jurstrand, Margaretha (2006). Detection of Chlamydia trachomatisand Mycoplasma genitalium by genetic and serological methods.
9. Norén, Torbjörn (2006). Clostridium difficile, epidemiology andantibiotic resistance.
10. Anderzén Carlsson, Agneta (2007). Children with Cancer – Focusingon their Fear and on how their Fear is Handled.
11. Ocaya, Pauline (2007). Retinoid metabolism and signalling invascular smooth muscle cells.
12. Nilsson, Andreas (2008). Physical activity assessed by accelerometryin children.
13. Eliasson, Henrik (2008). Tularemia – epidemiological, clinical anddiagnostic aspects.
14. Walldén, Jakob (2008). The influence of opioids on gastric function:experimental and clinical studies.
15. Andrén, Ove (2008). Natural history and prognostic factors inlocalized prostate cancer.
16. Svantesson, Mia (2008). Postpone death? Nurse-physicianperspectives and ethics rounds.
17. Björk, Tabita (2008). Measuring Eating Disorder Outcome – Definitions, dropouts and patients’ perspectives.
18. Ahlsson, Anders (2008). Atrial Fibrillation in Cardiac Surgery.
19. Parihar, Vishal Singh (2008). Human Listeriosis – Sources and Routes.
20. Berglund, Carolina (2008). Molecular Epidemiology of Methicillin-Resistant Staphylococcus aureus. Epidemiological aspects of MRSA and the dissemination in the community and in hospitals.
21. Nilsagård, Ylva (2008). Walking ability, balance and accidental falls in persons with Multiple Sclerosis.
22. Johansson, Ann-Christin (2008). Psychosocial factors in patients with lumbar disc herniation: Enhancing postoperative outcome by the identification of predictive factors and optimised physiotherapy.
23. Larsson, Matz (2008). Secondary exposure to inhaled tobacco products.
24. Hahn-Strömberg, Victoria (2008). Cell adhesion proteins in different invasive patterns of colon carcinoma: A morphometric and molecular genetic study.
25. Böttiger, Anna (2008). Genetic Variation in the Folate Receptor-α and Methylenetetrahydrofolate Reductase Genes as Determinants of Plasma Homocysteine Concentrations.
26. Andersson, Gunnel (2009). Urinary incontinence. Prevalence, treatment seeking behaviour, experiences and perceptions among persons with and without urinary leakage.
27. Elfström, Peter (2009). Associated disorders in celiac disease.
28. Skårberg, Kurt (2009). Anabolic-androgenic steroid users in treatment: Social background, drug use patterns and criminality.
29. de Man Lapidoth, Joakim (2009). Binge Eating and Obesity Treatment – Prevalence, Measurement and Long-term Outcome.
30. Vumma, Ravi (2009). Functional Characterization of Tyrosine and Tryptophan Transport in Fibroblasts from Healthy Controls, Patients with Schizophrenia and Bipolar Disorder.
31. Jacobsson, Susanne (2009). Characterisation of Neisseria meningitidis from a virulence and immunogenic perspective that includes variations in novel vaccine antigens.
32. Allvin, Renée (2009). Postoperative Recovery. Development of a Multi-Dimensional Questionnaire for Assessment of Recovery.
33. Hagnelius, Nils-Olof (2009). Vascular Mechanisms in Dementia with Special Reference to Folate and Fibrinolysis.
34. Duberg, Ann-Sofi (2009). Hepatitis C virus infection. A nationwide study of assiciated morbidity and mortality.
35. Söderqvist, Fredrik (2009). Health symptoms and potential effects on the blood-brain and blood-cerebrospinal fluid barriers associated with use of wireless telephones.
36. Neander, Kerstin (2009). Indispensable Interaction. Parents’ perspectives on parent–child interaction interventions and beneficial meetings.
37. Ekwall, Eva (2009). Women’s Experiences of Gynecological Cancer and Interaction with the Health Care System through Different Phases of the Disease.
38. Thulin Hedberg, Sara (2009). Antibiotic susceptibility and resistance in Neisseria meningitidis – phenotypic and genotypic characteristics.
39. Hammer, Ann (2010). Forced use on arm function after stroke. Clinically rated and self-reported outcome and measurement during the sub-acute phase.
40. Westman, Anders (2010). Musculoskeletal pain in primary health care: A biopsychosocial perspective for assessment and treatment.
41. Gustafsson, Sanna Aila (2010). The importance of being thin – Perceived expectations from self and others and the effect on self-evaluation in girls with disordered eating.
42. Johansson, Bengt (2010). Long-term outcome research on PDR brachytherapy with focus on breast, base of tongue and lip cancer.
43. Tina, Elisabet (2010). Biological markers in breast cancer and acute leukaemia with focus on drug resistance.
44. Overmeer, Thomas (2010). Implementing psychosocial factors in physical therapy treatment for patients with musculoskeletal pain in primary care.
45. Prenkert, Malin (2010). On mechanisms of drug resistance in acute myloid leukemia.

46. de Leon, Alex (2010). Effects of Anesthesia on Esophageal Sphincters in Obese Patients.
47. Josefson, Anna (2010). Nickel allergy and hand eczema – epidemiological aspects.
48. Almon, Ricardo (2010). Lactase Persistence and Lactase Non- Persistence. Prevalence, influence on body fat, body height, and relation to the metabolic syndrome.
49. Ohlin, Andreas (2010). Aspects on early diagnosis of neonatal sepsis.
50. Oliynyk, Igor (2010). Advances in Pharmacological Treatment of Cystic Fibrosis.
51. Franzén, Karin (2011). Interventions for Urinary Incontinence in Women. Survey and effects on population and patient level.
52. Loiske, Karin (2011). Echocardiographic measurements of the heart. With focus on the right ventricle.
53. Hellmark, Bengt (2011). Genotypic and phenotypic characterisation of Staphylococcus epidermidis isolated from prosthetic joint infections.
54. Eriksson Crommert, Martin (2011). On the role of transversus abdominis in trunk motor control.
55. Ahlstrand, Rebecca (2011). Effects of Anesthesia on Esophageal Sphincters.
56. Holländare, Fredrik (2011). Managing Depression via the Internet – self-report measures, treatment & relapse prevention.
57. Johansson, Jessica (2011). Amino Acid Transport and Receptor Binding Properties in Neuropsychiatric Disorders using the Fibroblast Cell Model.
58. Vidlund, Mårten (2011). Glutamate for Metabolic Intervention in Coronary Surgery with special reference to the GLUTAMICS-trial.
59. Zakrisson, Ann-Britt (2011). Management of patients with Chronic Obstructive Pulmonary Disease in Primary Health Care. A study of a nurse-led multidisciplinary programme of pulmonary rehabilitation.
60. Lindgren, Rickard (2011). Aspects of anastomotic leakage, anorectal function and defunctioning stoma in Low Anterior Resection of the rectum for cancer.

61. Karlsson, Christina (2011). Biomarkers in non-small cell lung carcinoma. Methodological aspects and influence of gender, histology and smoking habits on estrogen receptor and epidermal growth factor family receptor signalling.
62. Varelogianni, Georgia (2011). Chloride Transport and Inflammation in Cystic Fibrosis Airways.
63. Makdoumi, Karim (2011). Ultraviolet Light A (UVA) Photoactivation of Riboflavin as a Potential Therapy for Infectious Keratitis.
64. Nordin Olsson, Inger (2012). Rational drug treatment in the elderly: ”To treat or not to treat”.
65. Fadl, Helena (2012). Gestational diabetes mellitus in Sweden: screening, outcomes, and consequences.
66. Essving, Per (2012). Local Infiltration Analgesia in Knee Arthroplasty.
67. Thuresson, Marie (2012). The Initial Phase of an Acute Coronary Syndrome. Symptoms, patients’ response to symptoms and opportunity to reduce time to seek care and to increase ambulance use.
68. Mårild, Karl (2012). Risk Factors and Associated Disorders of Celiac Disease.
69. Fant, Federica (2012). Optimization of the Perioperative Anaesthetic Care for Prostate Cancer Surgery. Clinical studies on Pain, Stress Response and Immunomodulation.
70. Almroth, Henrik (2012). Atrial Fibrillation: Inflammatory and pharmacological studies.
71. Elmabsout, Ali Ateia (2012). CYP26B1 as regulator of retinoic acid in vascular cells and atherosclerotic lesions.
72. Stenberg, Reidun (2012). Dietary antibodies and gluten related seromarkers in children and young adults with cerebral palsy.
73. Skeppner, Elisabeth (2012). Penile Carcinoma: From First Symptom to Sexual Function and Life Satisfaction. Following Organ-Sparing Laser Treatment.
74. Carlsson, Jessica (2012). Identification of miRNA expression profiles for diagnosis and prognosis of prostate cancer.
75. Gustavsson, Anders (2012): Therapy in Inflammatory Bowel Disease.
76. Paulson Karlsson, Gunilla (2012): Anorexia nervosa – treatment expectations, outcome and satisfaction.
77. Larzon, Thomas (2012): Aspects of endovascular treatment of abdominal aortic aneurysms.
78. Magnusson, Niklas (2012): Postoperative aspects of inguinal hernia surgery – pain and recurrences.
79. Khalili, Payam (2012): Risk factors for cardiovascular events and incident hospital-treated diabetes in the population.
80. Gabrielson, Marike (2013): The mitochondrial protein SLC25A43 and its possible role in HER2-positive breast cancer.
81. Falck, Eva (2013): Genomic and genetic alterations in endometrial adenocarcinoma.
82. Svensson, Maria A (2013): Assessing the ERG rearrangement for clinical use in patients with prostate cancer.
83. Lönn, Johanna (2013): The role of periodontitis and hepatocyte growth factor in systemic inflammation.
84. Kumawat, Ashok Kumar (2013): Adaptive Immune Responses in the Intestinal Mucosa of Microscopic Colitis Patients.
85. Nordenskjöld, Axel (2013): Electroconvulsive therapy for depression.
86. Davidsson, Sabina (2013): Infection induced chronic inflammation and its association with prostate cancer initiation and progression.
87. Johansson, Benny (2013): No touch vein harvesting technique in coronary by-pass surgery. Impact on patency rate, development of atherosclerosis, left ventricular function and clinical outcome during 16 years follow-up.
88. Sahdo, Berolla (2013): Inflammasomes: defense guardians in host-microbe interactions.
89. Hörer, Tal (2013): Early detection of major surgical postoperative complications evaluated by microdialysis.
90. Malakkaran Lindqvist, Breezy (2013): Biological signature of HER2-positive breast cancer.
91. Lidén, Mats (2013): The stack mode review of volumetric datasets – applications for urinary stone disease.
92. Emilsson, Louise (2013): Cardiac Complications in Celiac Disease.
93. Dreifaldt, Mats (2013): Conduits in coronary artery bypass grafting surgery: Saphenous vein, radial and internal thoracic arteries.
94. Perniola, Andrea (2013): A new technique for postoperative pain management with local anaesthetic after abdominal hysterectomy.
95. Ahlstrand, Erik (2013): Coagulase-negative Staphylococci in Hematological Malignancy.
96. Sundh, Josefin (2013): Quality of life, mortality and exacerbations in COPD.
97. Skoog, Per (2013): On the metabolic consequences of abdominal compartment syndrome.
98. Palmetun Ekbäck, Maria (2013): Hirsutism and Quality of Life with Aspects on Social Support, Anxiety and Depression.
99. Hussain, Rashida (2013): Cell Responses in Infected and Cystic Fibrosis Respiratory Epithelium.
100. Farkas, Sanja (2014): DNA methylation in the placenta and in cancer with special reference to folate transporting genes.
101. Jildenstål, Pether (2014): Influence of depth of anaesthesia on post-operative cognitive dysfunction (POCD) and inflammatory marker.
102. Söderström, Ulf (2014): Type 1 diabetes in children with non-Swedish background – epidemiology and clinical outcome
103. Wilhelmsson Göstas, Mona (2014): Psychotherapy patients in mental health care: Attachment styles, interpersonal problems and therapy experiences
104. Jarl, Gustav (2014): The Orthotics and Prosthetics Users´ Survey: Translation and validity evidence for the Swedish version
105. Demirel, Isak (2014): Uropathogenic Escherichia coli, multidrug-resistance and induction of host defense mechanisms
106. Mohseni, Shahin (2014): The role of ß-blockade and anticoagula-tion therapy in traumatic brain injury
107. Bašić, Vladimir T. (2014): Molecular mechanisms mediatingdevelopment of pulmonary cachexia in COPD
108. Kirrander, Peter (2014): Penile Cancer: Studies on Prognostic Factors
109. Törös, Bianca (2014): Genome-based characterization of Neisseriameningitidis with focus on the emergent serogroup Y disease
110. von Beckerath, Mathias (2014): Photodynamic therapy in the Headand Neck
111. Waldenborg, Micael (2014): Echocardiographic measurements atTakotsubo cardiomyopathy - transient left ventricular dysfunction.
112. Lillsunde Larsson, Gabriella (2014): Characterization of HPV-inducedvaginal and vulvar carcinoma.
113. Palm, Eleonor (2015): Inflammatory responses of gingival fibroblasts inthe interaction with the periodontal pathogen Porphyromonas gingivlis.
114. Sundin, Johanna (2015): Microbe-Host Interactions in Post-infectiousIrritable Bowel Syndrome.
115. Olsson, Lovisa (2015): Subjective well-being in old age and its associationwith biochemical and genetic biomarkers and with physical activity.
116. Klarström Engström, Kristin (2015): Platelets as immune cells in sensingbacterial infection.
117. Landström, Fredrik (2015): Curative Electrochemotherapy in the Headand Neck Area.
118. Jurcevic, Sanja (2015): MicroRNA expression profiling in endometrialadenocarcinoma.
119. Savilampi, Johanna (2015): Effects of Remifentanil on EsophagealSphincters and Swallowing Function.
120. Pelto-Piri, Veikko (2015): Ethical considerations in psychiatric inpatientcare. The ethical landscape in everyday practice as described by staff.
121. Athlin, Simon (2015): Detection of Polysaccharides and PolysaccharideAntibodies in Pneumococcal Pneumonia.
122. Evert, Jasmine (2015): Molecular Studies of Radiotheray andChemotherapy in Colorectal Cancer.
123. Göthlin-Eremo, Anna (2015): Biological profiles of endocrine breast cancer.
124. Malm, Kerstin (2015): Diagnostic strategies for blood borne infections in Sweden.
125. Kumakech, Edward (2015): Human Immunodeficiency Virus (HIV), Human Papillomavirus (HPV) and Cervical Cancer Prevention in Uganda: Prevalence, Risk factors, Benefits and Challenges of Post-Exposure Prophylaxis, Screening Integration and Vaccination.
126. Thunborg, Charlotta (2015): Exploring dementia care dyads’ person transfer situations from a behavioral medicine perspective in physiotherapy. Development of an assessmement scale.
127. Zhang, Boxi (2015): Modulaton of gene expression in human aortic smooth muscle cells by Porphyromonas gingivalis - a possible association between periodontitis and atherosclerosis.
128. Nyberg, Jan (2015): On implant integration in irradiated bone: - clinical and experimental studies.
129. Brocki, Barbara C. (2015): Physiotherapy interventions and outcomes following lung cancer surgery.
130. Ulfenborg, Benjamin (2016): Bioinformatics tools for discovery and evaluation of biomarkers. Applications in clinical assessment of cancer.
131. Lindström, Caisa (2016): Burnout in parents of chronically ill children.
132. Günaltay, Sezin (2016): Dysregulated Mucosal Immune Responses in Microscopic Colitis Patients.
133. Koskela von Sydow, Anita (2016): Regulation of fibroblast activity by kera-tinocytes, TGF-β and IL-1α –studies in two- and three dimensional in vitro models.
134. Kozlowski, Piotr (2016): Prognostic factors, treatment and outcome in adult acute lymphoblastic leukemia. Population-based studies in Sweden.
135. Darvish, Bijan (2016): Post-Dural Puncture Headache in Obstetrics. Audiological, Clinical and Epidemiological studies.
136. Sahlberg Bang, Charlotte (2016): Carbon monoxide and nitric oxide as antimicrobial agents – focus on ESBL-producing uropathogenic E. coli.
137. Alshamari, Muhammed (2016): Low-dose computed tomography of the abdomen and lumbar spine.
138. Jayaprakash, Kartheyaene (2016): Monocyte and Neutrophil Inflammatory Responses to the Periodontopathogen Porphyromonas gingivalis.
139. Elwin Marie (2016): Description and measurement of sensory symptoms in autism spectrum.
140. Östlund Lagerström, Lina (2016): ”The gut matters” - an interdisciplinary approach to health and gut function in older adults.
141. Zhulina, Yaroslava (2016): Crohn’s disease; aspects of epidemiology, clini-cal course, and fecal calprotectin.
142. Nordenskjöld, Anna (2016): Unrecognized myocardial infarction and car-diac biochemical markers in patients with stable coronary artery disease.
143. Floodeen, Hannah (2016): Defunctioning stoma in low anterior resection of the rectum for cancer: Aspects of stoma reversal, anastomotic leakage, anorectal function, and cost-effectiveness.
144. Duberg, Anna (2016): Dance Intervention for Adolescent Girls with Inter-nalizing Problems. Effects and Experiences.
145. Samano, Ninos (2016): No-Touch Saphenous Veins in Coronary Artery Bypass Grafting. Long-term Angiographic, Surgical, and Clinical Aspects.
146. Rönnberg, Ann-Kristin (2016): Gestational Weight Gain. Implications of an Antenatal Lifestyle Intervention.
147. Erik Stenberg (2016): Preventing complications in bariatric surgery.
148. Humble, Mats B. (2016): Obsessive-compulsive disorder, serotonin and oxytocin: treatment response and side effects.
149. Asfaw Idosa, Berhane (2016): Inflammasome Polymorphisms and the Inflammatory Response to Bacterial Infections.
150. Sagerfors, Marcus (2016): Total wrist arthroplasty. A clinical, radiographic and biomechanical investigation.
151. Nakka, Sravya Sowdamini (2016): Development of novel tools for prevention and diagnosis of Porphyromonas gingivalis infection and periodontitis.
152. Jorstig, Stina (2016): On the assessment of right ventricular function using cardiac magnetic resonance imaging and echocardiography.
153. Logotheti, Marianthi (2016): Integration of Functional Genomics and Data Mining Methodologies in the Study of Bipolar Disorder and Schizophrenia.
154. Paramel Varghese, Geena (2017): Innate Immunity in Human Atherosclerosis and Myocardial Infarction: Role of CARD8 and NLRP3.
155. Melinder, Carren Anyango (2017): Physical and psychological characteristics in adolescence and risk of gastrointestinal disease in adulthood.
156. Bergh, Cecilia (2017): Life-course influences on occurrence and outcome for stroke and coronary heart disease.
157. Olsson, Emma (2017): Promoting Health in Premature Infants – with special focus on skin-to-skin contact and development of valid pain assessment.
158. Rasmussen, Gunlög (2017): Staphylococcus aureus bacteremia, molecular epidemiology and host immune response.
159. Bohr Mordhorst, Louise (2017): Predictive and prognostic factors in cervical carcinomas treated with (chemo-) radiotherapy.
160. Wickbom, Anna (2017): Epidemiological aspects of Microscopic Colitis.
161. Cajander, Sara (2017): Dynamics of Human Leukocyte Antigen – D Related expression in bacteremic sepsis.
162. Zetterlund, Christina (2017): Visual, musculoskeletal and balance symptoms in people with visual impairments.
163. Sundelin, Heléne E.K. (2017): Comorbidity and Complications in Neurological Diseases.
164. Wijk, Lena (2017): Enhanced Recovery After Hysterectomy.
165. Wanjura, Viktor (2017): Register-based studies on cholecystectomy. Quality of life after cholecystec-tomy, and cholecystectomy incidence and complications after gastric bypass.
166. Kuchálik, Ján (2017): Postoperative pain, inflammation and functio-nal recovery after total hip arthroplasty. Prospective, randomized, clinical studies.
167. Ander, Fredrik (2017): Perioperative complications in obese patients. A thesis on risk reducing strategies.

168. Isaksson, Helena (2017): Clinical studies of RNA as a prognosticand diagnostic marker for disease.
169. Fengsrud, Espen (2017): Atrial Fibrillation: Endoscopic ablation andPostoperative studies.
170. Amcoff, Karin (2018): Serological and faecal biomarkers in inflam-matory bowel disease.
171. Kennedy, Beatrice (2018): Childhood bereavment, stress resilience,and cancer risk: an integrated register-based approach.
172. Andersson, Karin (2018): Metal artifacts in Computed Tomography- impact of reduction methods on image quality and radiotherapytreatment planning.
173. Calais, Fredrik (2018): Coronary artery disease and prognosis inrelation to cardiovascular risk factors, interventional techniquesand systemic atherosclerosis.
174. Meehan, Adrian (2018): Lithium-associated hyperparathyroidism:Prevalence, Pathophysiology, Management.
175. Björkenheim, Anna (2018): Catheter ablation for atrial fibrillation– effects on rhythm, symptoms and health-related quality of life.
176. Andersson, Tommy (2018): Atrial fibrillation and cause of death,sex differences in mortality, and anticoagulation treatment inlow-risk patients.
177. Christos Karefylakis (2018): Vitamin D and its role in obesity andother associated conditions.
178. Eriksson, Carl (2018): Epidemiological and therapeutic aspects ofinflammatory bowel disease.