drawing perseveration in neglect: effects of target density
TRANSCRIPT
1
Journal of Neuropsychology (2012)C© 2012 The British Psychological Society
TheBritishPsychologicalSociety
www.wileyonlinelibrary.com
Drawing perseveration in neglect: Effectsof target density
Lorenzo Pia1∗, Raffaella Ricci1, Patrizia Gindri2
and Giuseppe Vallar3,4
1Psychology Department and Neuroscience Institute of Turin (NIT), University ofTurin, Italy
2Sanitary Garrison ‘San Camillo’, Turin, Italy3Department of Psychology, University of Milano-Bicocca, Milan, Italy4Neuropsychological Laboratory, IRCCS The Italian Institute for Auxology,Milan, Italy
In cancellation tasks, patients with unilateral spatial neglect typically fail to mark targetswithin the side of the sheet contralateral to the side of the lesion (contralesional).Moreover, they can show a perseverative behaviour, which consists in repeatedlycancelling stimuli, mainly in the side of the display ipsilateral to the side of the lesion(ipsilesional). We investigated in 13 right-brain-damaged patients with left spatial neglectand perseverative behaviour whether and how different densities of horizontal targetsmodulated omission and perseverative errors. We found that the density of targetsmodulated the patients’ distribution of neglect (area of omission), but not its extent,as indexed by the percentage of omissions. Specifically, the area of omissions tightenedwhen target density increased leftwards. On the other hand, target density did notaffect the distribution of perseverative behaviour (area of perseveration), as well as itsextent, as indexed by the percentage of perseverations. Correlation analyses showedthat both the extent and the distribution of omissions were positively correlated toclinical measures of spatial neglect. Conversely, perseverations did not show such acorrelation. These findings support the view that two different pathological mechanismsmight be involved in left spatial neglect and in ipsilesional perseverative behaviour.
Left unilateral spatial neglect is a neuropsychological syndrome that is usually associatedwith lesions to the right hemisphere, with the damage most frequently involvinga network including the inferior parietal lobule, the temporo-parietal junction, thedorsolateral pre-motor cortex, their white matter connections, as well as the thalamusand the basal ganglia (see Halligan, Fink, Marshall, & Vallar, 2003; Heilman, Watson,& Valenstein, 2003; Husain, 2008 for reviews). Neglect patients tend to ignore (i.e.,neither react to nor search for) stimuli within the side of space contralateral to the side
∗Correspondence should be addressed to Lorenzo Pia, Psychology Department & Neuroscience Institute of Turin (NIT), ViaPo 14, Turin 10123, Italy (e-mail: [email protected]).
DOI:10.1111/j.1748-6653.2012.02034.x

2 L. Pia et al.
of the lesion (contralesional), namely the left-hand side in right-brain-damaged patients.Accordingly, in cancellation tasks, these patients, when asked to cross out with a penciltargets printed on a sheet of paper, typically omit contralesional stimuli and mark targetslocated in the side of space ipsilateral to the side of the lesion (ipsilesional, the right-hand side in right-brain-damaged patients). In cancellation tasks, patients may also showa perseverative behaviour, namely a tendency to recancel ipsilesional targets (Bottini& Toraldo, 2003; Khurshid, Longin, Crucian, & Barrett, 2009; Kim et al., 2009; Manly,Woldt, Watson, & Warburton, 2002; Mark, Kooistra, & Heilman, 1988; Na et al., 1999;Nys, Seurinck, & Dijkerman, 2008; Nys, van Zandvoort, van der Worp, Kappelle, &de Haan, 2006; Pia, Folegatti, Guagliardo, Genero, & Gindri, 2009; Ronchi, Posteraro,Fortis, Bricolo, & Vallar, 2009; Rusconi, Maravita, Bottini, & Vallar, 2002; Toraldoet al., 2005; Vallar, Zilli, Gandola, & Bottini, 2006). These ’perseverative responses’in pencil-and-paper cancellation tasks, where, importantly, a visual feedback is presentare to be distinguished from ’re-visiting behavior’ during computerized visual searchtasks, in which no visual visible mark is available (Husain et al., 2001; Mannan et al.,2005). Additionally, perseverations cannot be traced back to a gross, general cognitiveimpairment, being virtually absent in patients with probable senile dementia of theAlzheimer type (Rusconi et al., 2002). Furthermore, in patients with left spatial neglect,perseveration is unrelated to deficits of verbal and visuo-spatial short-term memory (digitand block span), and of executive functions (Nys et al., 2006; Ronchi et al., 2009).Perseveration is considered a main ’productive’ manifestation of the neglect syndrome,distinct from the more widely investigated ’defective’ manifestations, such as omissionerrors in cancellation task (Vallar, 1998; Vallar & Mancini, 2010).
Perseverations have been reported quite frequently in concomitance with spatialneglect (ranging from 30%, Na et al., 1999, to 90%, Rusconi et al., 2002 of patients). Sofar, at least two main hypotheses have been proposed to account for the occurrenceof perseverative responses in patients with neglect. One view is that perseveration maybe integral to neglect, representing the inability to disengage spatial attention fromthe ipsilesional side (Mark et al., 1988), or related to a sort of residual processing ofcontralesional (neglected) information (Bottini & Toraldo, 2003; Manly et al., 2002;Toraldo et al., 2005). Another view is that perseverative behaviour and spatial neglect,although often associated, are functionally and anatomically independent disorders(Khurshid et al., 2009; Pia et al., 2009; Ronchi et al., 2009; Rusconi et al., 2002;Vallar et al., 2006). Specifically, perseveration would be a consequence of a pathologicalrelease of a complex motor behaviour brought about by a frontal-subcortical damage,co-occurring with, but independent of, the ipsilesional spatial bias (i.e., neglect). The’independence’ view is anatomically specified at some extent, with perseveration inneglect patients being associated with frontal-subcortical (basal ganglia) damage, andthe lack of this productive phenomenon with posterior lesions (e.g., Na et al., 1999; Nyset al., 2006; Pia et al., 2009; Rusconi et al., 2002; Vallar et al., 2006). Conversely, theview that perseveration is intrinsic to the neglect syndrome is anatomically unspecified.
Here, we aimed at further addressing the issue of the relationship between unilateralspatial neglect and perseverative behaviour in a group of right-brain-damaged patientsdisplaying both omissions and perseverations. In this retrospective study, we useda cancellation task in which target density varied across conditions. Based on thedistinction proposed by Chatterjee and co-workers (Chatterjee, Mennemeier, & Heilman,1992b, 1992c), we shall refer to the number of omission errors committed by patients asto the extent of unilateral spatial neglect, and to the neglected area as to the distributionof neglect; the same terms shall be used for perseveration errors. In this study, we

Drawing perseveration in neglect 3
aimed at investigating, first, whether and how target density affected the extent and thedistribution of the two error types (i.e., omissions and perseverations), and their spatialdistribution (i.e., the areas of omissions and of perseverations). Second, we analysedthe relationships between spatial neglect and perseverative behaviour by means ofcorrelation analyses. We predicted that if perseverations and omissions (extent and/ordistribution) are part of a single pathological mechanism, they should be modulated bythe different target densities in a similar way. On the contrary, if they are two independentdisorders, they should not be modulated in the same way by the target density.
MethodsParticipantsThirteen right-handed patients with left unilateral spatial neglect following a righthemisphere damage (4 women; mean age 70.69 years, SD = 7 years; mean educationallevel 6.77 years, SD = 4.85 years) participated in the study, after having given writteninformed consent, according to the Declaration of Helsinki. They were selected among28 neglect patients who had taken part in a previous study (Ricci, Pia, & Gindri, 2004),for showing both omissions and perseveration in cancellation tasks (dataset dates backto 2004). Contralesional somatosensory, motor, and visual field defects were assessedby a standard neurological exam (Bisiach & Faglioni, 1974). Unilateral spatial neglectwas assessed by means of a line bisection task (five 180-mm-long horizontal lines), andtwo visuo-spatial exploratory tasks: letter (Diller & Weinberg, 1977), and line (Albert,1973) cancellation. The admission criteria were at least one perseveration error (seedefinition below) in the baseline condition of the experimental task, and a score abovethe cut-off in both the letter (Vallar, Rusconi, Fontana, & Musicco, 1994), and theline cancellation tasks. The patients’ demographic, clinical, and experimental data arereported in Table 1. Neglect severity of the patients who were selected for the presentstudy did not significantly differ from that of patients who were not included in thestudy, as assessed through letter and line cancellation tasks (independent-samples t testp > .05).
Stimuli and procedureTargets consisted of 54 black ellipses with 7 × 4 mm axes, printed on an A4 whitesheet of paper. Three targets were drawn in a random vertical position along each of 18165-mm-long virtual vertical lines located parallel to the shorter side of the sheet. Thehorizontal position of the virtual vertical lines varied across conditions. In one condition(‘uniform density’), the lines were evenly spaced at a distance of 10 mm. In the twoother conditions (i.e., ‘increasing leftward density’ and ‘increasing rightward density’),they were unevenly spaced with distances progressively increasing from one side of thepage to the other (towards the right in the former, and towards the left in the latter,according to the exponential function Y = ex; x ∈ [−0.50; 1.1] in steps of 0.10; seeFigure 1).
Since the difficulty in seeing one’s own marks (they are generally more faint thanthe printed stimuli on the sheet) may lead to recancellations prompted by a lack of avisible reminder of already cancelled targets, participants were asked to cross out allthe targets once with a clearly visible mark, using a black soft pen (see discussion inManly et al., 2002). Throughout the execution of the cancellation task, the examiner

4 L. Pia et al.
Tabl
e1.
Dem
ogra
phic
,clin
ical
,and
expe
rim
enta
ldat
aof
13ri
ght-
brai
n-da
mag
edpa
tient
s
Neu
rolo
gica
lTo
tal
mea
nex
amin
atio
nLe
tter
Line
BIS
OP
Erro
rex
tent
Erro
rdi
stri
butio
n
ScLe
sion
DM
SV
O(%
)P
(%)
O(A
rea)
P(A
rea)
PtS
Y(y
)si
teE
(d)
UD
ILD
IRD
UD
ILD
IRD
UD
ILD
IRD
UD
ILD
IRD
1F
6813
PI
573–
32–
22–
25
730
.411
.67
9.67
23.1
525
16.6
715
.74
14.8
123
.15
64.2
631
.72
85.7
673
.48
67.6
389
.93
2F
574
F,P
M54
1–1
0–0
0–0
169
26.8
34.5
2.83
67.5
978
.745
.37
4.63
3.7
7.41
241.
7522
4.42
230.
3225
.89
34.5
429
.39
3M
725
icI
313–
33–
30–
012
1648
.231
.17
3.33
52.7
866
.67
53.7
6.48
1.85
10.1
917
8.7
175.
5825
2.86
33.5
313
.75
17.0
14
M62
5P
I7
3–1
3–3
2–2
252
9.4
27.8
3.6
750
.93
5053
.70
2.78
0.9
344
.93
116.
1321
8.26
21.4
04.
095
M70
5P,
TI
453–
32–
21–
226
171
14.8
31.
6727
.78
30.5
624
.07
4.63
3.7
.93
83.1
344
.98
94.7
321
.79
15.1
24
6M
775
O,T
I31
3–1
2–2
1–2
336
43.4
20.5
5.17
36.1
129
.63
48.1
58.
336.
4813
.89
185.
6745
.57
202.
7924
.08
34.7
619
.66
7M
825
F,P,
TI
583–
33–
33–
35
1880
42.1
71.
8376
.85
82.4
175
1.85
1.85
6.48
296.
4924
5.33
284.
6610
.12
18.7
035
.87
8F
715
bg,i
c,th
H2
3–3
3–1
1–1
332
−70
13.1
78.
515
.74
26.8
530
.56
21.3
18.5
27.
4150
.19.
1461
.894
.25
99.5
433
.71
9F
695
Ic,t
hI
403–
20–
01–
125
216
7.5
7.67
19.4
416
.67
5.56
12.0
419
.44
11.1
132
.82
14.3
84.
8458
.30
95.3
449
.210
M63
18P,
TH
733–
33–
3N
.A.
2518
65.2
28.6
715
57.4
142
.59
59.2
626
.85
40.7
415
.74
135.
8310
1.1
276.
2993
.64
129.
826
.67
11M
775
P,T
I11
13–
21–
10–
05
133
.4.3
34.
330
01.
858.
334.
6311
.11
00
035
.25
19.5
847
.89
12M
755
crI
363–
13–
23–
312
1248
.640
1.5
76.8
575
.93
69.4
42.
780.
934.
6325
1.9
210.
130
8.0
20.5
38.
1917
.42
13M
7613
F,P,
TI
622–
22–
22–
119
16−.
212
3.5
501.
8514
.81
4.63
9.26
5.56
156.
930
163.
824
.64
39.9
123
.43
Pt:p
atie
nt;S
:sex
,M=
mal
e,F
=fe
mal
e.Sc
:yea
rs(y
)of
scho
olin
g(fo
rmal
educ
atio
n).L
esio
nsi
te:F
=fr
onta
l,O
=oc
cipi
tal,
T=
tem
pora
l,bg
=ba
salg
angl
ia,
ic=
inte
rnal
caps
ule,
th=
thal
amus
;cr
=co
rona
radi
ata.
E:ae
tiolo
gy,H
=ha
emor
rhag
e,I=
isch
aem
ia,M
=m
enin
giom
a.D
:dur
atio
nof
dise
ase,
num
ber
ofda
ys(d
)el
apse
dbe
twee
nth
eon
set
ofth
edi
seas
ean
dth
efir
stda
yof
the
neur
opsy
chol
ogic
alas
sess
men
t.N
euro
logi
cale
xam
inat
ion:
Con
tral
esio
nalM
otor
(M),
Som
atos
enso
ry(S
),an
dV
isua
lhal
f-fiel
d(V
)ne
urol
ogic
alde
ficits
(the
two
valu
esre
fer
toth
eup
per
and
low
erlim
b/vi
sual
quad
rant
s,re
spec
tivel
y);s
core
sra
nged
from
norm
al(0
)to
seve
rede
fect
s(3
).Le
tter
:let
ter
canc
ella
tion;
left
min
usri
ght
omis
sion
s(c
ut-o
ffsc
ore
≥3).
Line
:lin
eca
ncel
latio
n;le
ftm
inus
righ
tom
issi
ons
(cut
-off
scor
e≥1
;neu
rolo
gica
llyun
impa
ired
part
icip
ants
perf
orm
this
task
with
out
erro
rs).
BIS:
line
bise
ctio
n;m
ean
line
bise
ctio
ner
ror
(mm
):po
sitiv
eva
lues
indi
cate
da
righ
twar
der
ror,
nega
tive
valu
esa
left
war
der
ror.
O:o
mis
sion
s;m
ean
num
ber
ofom
issi
ons
inth
eel
lipse
sca
ncel
latio
nta
sk(a
vera
ged
acro
ssco
nditi
ons)
.P:
pers
ever
atio
ns;m
ean
num
ber
ofpe
rsev
erat
ions
inth
eel
lipse
sca
ncel
latio
nta
sk(a
vera
ged
acro
ssth
eth
ree
cond
ition
s).E
rror
exte
nt:p
erce
nt(%
)om
issi
ons
and
perc
ent
ofpe
rsev
erat
ions
inth
eth
ree
targ
etde
nsity
cond
ition
s.Er
ror
dist
ribu
tion:
area
ofom
issi
onan
dar
eaof
pers
evea
ratio
nsin
the
thre
eta
rget
dens
ityco
nditi
ons;
UD
:uni
form
dens
ity.I
L/R
D:i
ncre
asin
gle
ftw
ard/
righ
twar
dta
rget
dens
ity.

Drawing perseveration in neglect 5
Figure 1. Stimuli used on the ellipses cancellation task in the different background conditions (‘uniformdensity’, ‘increasing leftward density’, ‘increasing rightward density’).
paid attention to the possibility that perseveration represented a defective reaching ofthe target itself. This possibility would be suggested by the behaviour of a patient whoeventually crossed out the target, after a number of crossings near it (see discussion inRusconi et al., 2002). No patient showed such a behaviour. Finally, the examiner verifiedthat no patient exhibited cancellation behaviour indicative of the presence of a reaching

6 L. Pia et al.
Figure 2. An example of the scoring procedure for the spatial distribution of errors.
deficit: for example, a target cancellation preceded by some other cancellations in theproximity of it. The sheet of paper was aligned with the mid-sagittal plane of the patient’strunk, and placed at a comfortable reading distance (about 50 cm). Each stimulus arraywas presented twice (in an A-B-C-C-B-A order) for a total of six trials.
The amount of errors was assessed by recording the number of omissions and thenumber of perseverations within each condition. Values were subsequently transformedin percent omissions ([number of omissions/number of targets] × 100), and percentperseverations ([number of perseverations/number of cancellations] × 100). A per-severation error was operationally defined as ’crossing a target with more than onedistinct mark’, with successive marks: each additional mark was scored 1 (see Ronchiet al., 2009). For discussions concerning scoring procedures for perseveration errors,see Manly et al. (2002), Na et al. (1999), Ronchi et al. (2009), Rusconi et al. (2002), andToraldo et al. (2005).
The spatial distribution of errors was assessed by computing within each conditionthe area in which patients made omissions or perseverative errors following the sameprocedure of the previous aforementioned study (Ricci et al., 2004). The area wasdelimited as follows. Proceeding from left to right (omissions) or from right to left(perseverations), straight lines interconnected all targets with each error type. Thewider polygon was drawn using such lines as sides, with the following constraints:(1) target cancelled once were not included in the polygon or touched one of its sidesand (2) lines interconnecting omissions or perseverations, which also passed throughthe space between two targets cancelled once lying on the same vertical virtual line,were disregarded. Areas (cm2) were measured using a graphic digital tablet (WacomUltrarapid) with graphical software (AutoCAD 14). An example of the procedure ispresented in Figure 2. The procedure is described in detail in Ricci et al. (2004).
Statistical analysesThe percent omission and perseveration errors and the omission and perseveration areasin the three stimulus density conditions were analysed by one-way repeated measuresanalyses of variance. Correlations between the number and area of omissions and numberand area of perseveration errors (normalized z-score), in the three stimulus density

Drawing perseveration in neglect 7
Figure 3. Ellipses cancellation task. Mean (SE) percent omissions and mean percent perseveration bybackground condition.
conditions, and between these scores and measures of spatial neglect (normalized z-score), were computed.
ResultsExtent of errorsNo differences across stimulus density conditions were found for both percent omissions,(F (2, 24) = .584, p = .564), and percent perseverations, (F (2, 24) = .042, p = .958).This indicates that the amount of errors, namely the extent of neglect and perseveration,was unaffected by the horizontal distribution of targets (see Figure 3).
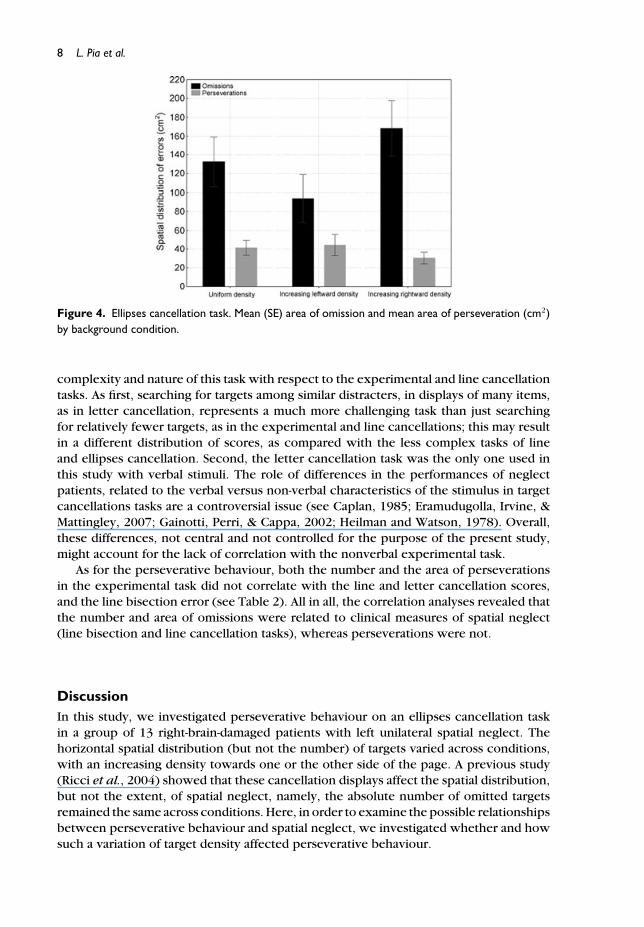
Error distributionFor area of omissions, a significant difference across stimulus density conditions wasfound (F (2, 24) = 9.886, p < .001). A Newman–Keuls post hoc analysis showed thateach comparison was significant (p < .05), with the area of omissions being largest inthe ‘increasing rightward density’ condition (mean = 168.009 cm2, SE = 29.745 cm2),intermediate in the ’uniform density’ condition (mean = 132.501 cm2, SE = 26.275 cm2),and smallest in the ‘increasing leftward density’ condition (mean = 93.727 cm2, SE =25.372 cm2). For the areas of perseverations, no significant differences were found (F(2, 24) = 1.611, p = .22). In sum, the horizontal pattern of target density affected thesize of the area of omissions, but not that of the area of perseverations (see Figure 4).
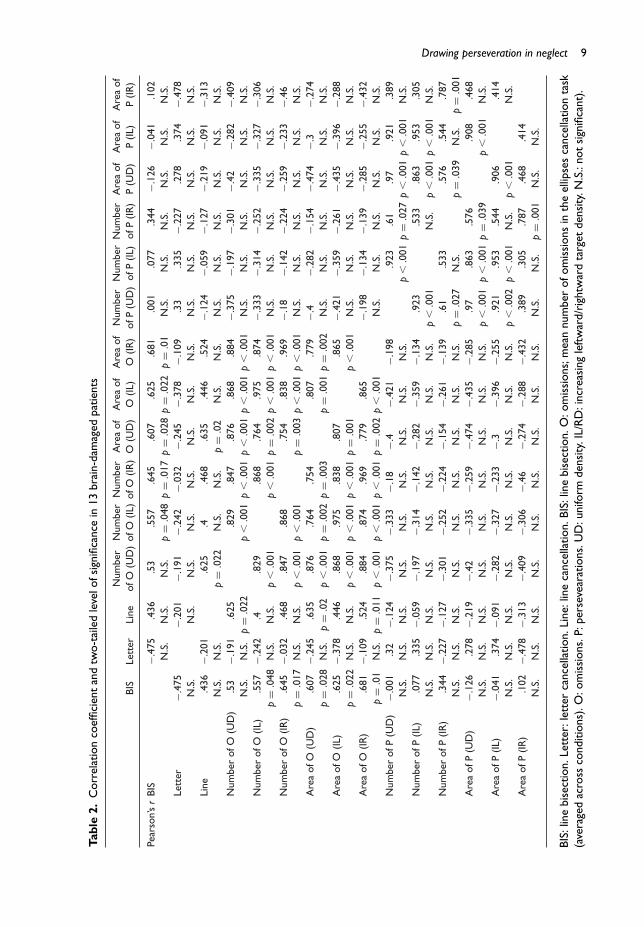
CorrelationsBoth the number and the area of omissions in each stimulus density conditions werenot correlated to the number or to the area of perseverations. However, these omissionmeasures had some positive correlations with the line cancellation, and line bisectionscores, but not to the letter cancellation score (see Table 2). The lack of significantcorrelations with the letter cancellation might be tentatively explained by the different
8 L. Pia et al.
Figure 4. Ellipses cancellation task. Mean (SE) area of omission and mean area of perseveration (cm2)by background condition.
complexity and nature of this task with respect to the experimental and line cancellationtasks. As first, searching for targets among similar distracters, in displays of many items,as in letter cancellation, represents a much more challenging task than just searchingfor relatively fewer targets, as in the experimental and line cancellations; this may resultin a different distribution of scores, as compared with the less complex tasks of lineand ellipses cancellation. Second, the letter cancellation task was the only one used inthis study with verbal stimuli. The role of differences in the performances of neglectpatients, related to the verbal versus non-verbal characteristics of the stimulus in targetcancellations tasks are a controversial issue (see Caplan, 1985; Eramudugolla, Irvine, &Mattingley, 2007; Gainotti, Perri, & Cappa, 2002; Heilman and Watson, 1978). Overall,these differences, not central and not controlled for the purpose of the present study,might account for the lack of correlation with the nonverbal experimental task.
As for the perseverative behaviour, both the number and the area of perseverationsin the experimental task did not correlate with the line and letter cancellation scores,and the line bisection error (see Table 2). All in all, the correlation analyses revealed thatthe number and area of omissions were related to clinical measures of spatial neglect(line bisection and line cancellation tasks), whereas perseverations were not.
DiscussionIn this study, we investigated perseverative behaviour on an ellipses cancellation taskin a group of 13 right-brain-damaged patients with left unilateral spatial neglect. Thehorizontal spatial distribution (but not the number) of targets varied across conditions,with an increasing density towards one or the other side of the page. A previous study(Ricci et al., 2004) showed that these cancellation displays affect the spatial distribution,but not the extent, of spatial neglect, namely, the absolute number of omitted targetsremained the same across conditions. Here, in order to examine the possible relationshipsbetween perseverative behaviour and spatial neglect, we investigated whether and howsuch a variation of target density affected perseverative behaviour.
Drawing perseveration in neglect 9
Tabl
e2.
Cor
rela
tion
coef
ficie
ntan
dtw
o-ta
iled
leve
lofs
igni
fican
cein
13br
ain-
dam
aged
patie
nts
Num
ber
Num
ber
Num
ber
Are
aof
Are
aof
Are
aof
Num
ber
Num
ber
Num
ber
Are
aof
Are
aof
Are
aof
BIS
Lett
erLi
neof
O(U
D)
ofO
(IL)
ofO
(IR)
O(U
D)
O(IL
)O
(IR)
ofP
(UD
)of
P(IL
)of
P(IR
)P
(UD
)P
(IL)
P(IR
)
Pear
son’
sr
BIS
−.47
5.4
36.5
3.5
57.6
45.6
07.6
25.6
81.0
01.0
77.3
44−.
126
−.04
1.1
02N
.S.
N.S
.N
.S.
p=
.048
p=
.017
p=
.028
p=
.022
p=
.01
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
Lett
er−.
475
−.20
1−.
191
−.24
2−.
032
−.24
5−.
378
−.10
9.3
3.3
35−.
227
.278
.374
−.47
8N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.Li
ne.4
36−.
201
.625
.4.4
68.6
35.4
46.5
24−.
124
−.05
9−.
127
−.21
9−.
091
−.31
3N
.S.
N.S
.p
=.0
22N
.S.
N.S
.p
=.0
2N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
umbe
rof
O(U
D)
.53
−.19
1.6
25.8
29.8
47.8
76.8
68.8
84−.
375
−.19
7−.
301
−.42
−.28
2−.
409
N.S
.N
.S.
p=
.022
p�
.001
p�
.001
p�
.001
p�
.001
p�
.001
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
Num
ber
ofO
(IL)
.557
−.24
2.4
.829
.868
.764
.975
.874
−.33
3−.
314
−.25
2−.
335
−.32
7−.
306
p=
.048
N.S
.N
.S.
p�
.001
p�
.001
p=
.002
p�
.001
p�
.001
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
Num
ber
ofO
(IR)
.645
−.03
2.4
68.8
47.8
68.7
54.8
38.9
69−.
18−.
142
−.22
4−.
259
−.23
3−.
46p
=.0
17N
.S.
N.S
.p
�.0
01p
�.0
01p
=.0
03p
�.0
01p
�.0
01N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.A
rea
ofO
(UD
).6
07−.
245
.635
.876
.764
.754
.807
.779
−.4
−.28
2−.
154
−.47
4−.
3−.
274
p=
.028
N.S
.p
=.0
2p
�.0
01p
=.0
02p
=.0
03p
=.0
01p
=.0
02N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.A
rea
ofO
(IL)
.625
−.37
8.4
46.8
68.9
75.8
38.8
07.8
65−.
421
−.35
9−.
261
−.43
5−.
396
−.28
8p
=.0
22N
.S.
N.S
.p
�.0
01p
�.0
01p
�.0
01p
=.0
01p
�.0
01N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.A
rea
ofO
(IR)
.681
−.10
9.5
24.8
84.8
74.9
69.7
79.8
65−.
198
−.13
4−.
139
−.28
5−.
255
−.43
2p
=.0
1N
.S.
p=
.011
p�
.001
p�
.001
p�
.001
p=
.002
p�
.001
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
Num
ber
ofP
(UD
)−.
001
.32
−.12
4−.
375
−.33
3−.
18−.
4−.
421
−.19
8.9
23.6
1.9
7.9
21.3
89N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
p�
.001
p=
.027
p�
.001
p�
.001
N.S
.N
umbe
rof
P(IL
).0
77.3
35−.
059
−.19
7−.
314
−.14
2−.
282
−.35
9−.
134
.923
.533
.863
.953
.305
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.p
�.0
01N
.S.
p�
.001
p�
.001
N.S
.N
umbe
rof
P(IR
).3
44−.
227
−.12
7−.
301
−.25
2−.
224
−.15
4−.
261
−.13
9.6
1.5
33.5
76.5
44.7
87N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
p=
.027
N.S
.p
=.0
39N
.S.
p=
.001
Are
aof
P(U
D)
−.12
6.2
78−.
219
−.42
−.33
5−.
259
−.47
4−.
435
−.28
5.9
7.8
63.5
76.9
08.4
68N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
p�
.001
p�
.001
p=
.039
p�
.001
N.S
.A
rea
ofP
(IL)
−.04
1.3
74−.
091
−.28
2−.
327
−.23
3−.
3−.
396
−.25
5.9
21.9
53.5
44.9
06.4
14N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
p�
.002
p�
.001
N.S
.p
�.0
01N
.S.
Are
aof
P(IR
).1
02−.
478
−.31
3−.
409
−.30
6−.
46−.
274
−.28
8−.
432
.389
.305
.787
.468
.414
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.N
.S.
N.S
.p
=.0
01N
.S.
N.S
.
BIS:
line
bise
ctio
n.Le
tter
:let
ter
canc
ella
tion.
Line
:lin
eca
ncel
latio
n.BI
S:lin
ebi
sect
ion.
O:o
mis
sion
s;m
ean
num
ber
ofom
issi
ons
inth
eel
lipse
sca
ncel
latio
nta
sk(a
vera
ged
acro
ssco
nditi
ons)
.O:o
mis
sion
s.P:
pers
evea
ratio
ns.U
D:u
nifo
rmde
nsity
.IL/
RD
:inc
reas
ing
left
war
d/ri
ghtw
ard
targ
etde
nsity
.N.S
.:no
tsi
gnifi
cant
).

10 L. Pia et al.
As found in the original larger group of patients, from which the participants inthis retrospective study were selected (Ricci et al., 2004), the spatial distribution ofomissions, but not its number, was modulated by the cancellation frame. In particular,the omitted area was found to be smaller when target density increased leftwards,larger when target density increased rightwards. The finding that patients cancelled acomparable number of targets across conditions could be accounted for by the factthat the number of targets did not change across conditions. Chatterjee and colleagues(Chatterjee et al., 1992a; Chatterjee, Thompson, & Ricci, 1999) have shown that thenumber of cancellations made by brain-damaged patients with spatial neglect dependsupon the number of targets and not on their density. As for perseverative behaviour,here we found that both the percent and the spatial distribution of perseverations werenot affected by variations of the horizontal density of targets. Therefore, our resultsshow a dissociation of the effects of target density on omissions and perseverations.The patients’ divide between the neglected and explored regions, namely the edgebetween left omissions and right cancellations, shifts towards the denser side. Despitethis, the area of perseverative errors does not change. The lack of association betweenperseveration behaviour and spatial neglect is further confirmed by the absence ofsignificant correlations between clinical measures of the severity of spatial neglect (i.e.,number of omissions in line cancellation and deviation in line bisection) and the numberof perseverations, which is in line with previous findings (Pia et al., 2009; Ronchi et al.,2009; Rusconi et al., 2002; Vallar et al., 2006). Conversely, omissions in the experimentaltask correlated with line bisection and line cancellation performance, but not withletter cancellation performance. Indeed, double dissociations between omissions andperseveration errors have been observed in previous group studies reporting bothpatients who show omissions without perseveration, and patients showing perseverationwithout omissions (Na et al., 1999; Nys et al., 2006; Pia et al., 2009; Ronchi et al., 2009;Rusconi et al., 2002). Additionally, treatment may ameliorate one deficit but not theother. Monocular patching of the right eye ameliorates omissions but not perseverationsin a cancellation task (Khurshid et al., 2009). In one study (Nys et al., 2008), repeatedsessions of prism adaptation improved cancellation, but perseveration errors increased,particularly contralesionally. In another study (Vallar et al., 2006), a single session ofprism adaptation improved both omission and perseveration, but the effects were foundto be unrelated. It is worth noticing that interpretations of perseveration as integral tospatial neglect (Bottini & Toraldo, 2003; Manly et al., 2002; Mark et al., 1988; Toraldoet al., 2005) predict an association between the two disorders.
Our results are in agreement with previous findings supporting the view that neglectand perseverative behaviour should be considered as separate pathological phenomenawith discrete anatomical counterparts (Khurshid et al., 2009; Pia et al., 2009; Ronchiet al., 2009; Rusconi et al., 2002; Vallar et al., 2006). Indeed, it has been proposedthat perseveration errors might be due to the pathological release of complex motorbehaviour, brought about by lesions to frontal/subcortical areas (Rusconi et al., 2002;Vallar et al., 2006). This deficit would add to, and would be triggered by, the primaryipsilesional bias. The co-occurrence of a defective monitoring of motor acts (as ina cancellation task) with the disordered representation of the working space wherethese actions are to be performed, would elicit ipsilesional perseverations. From ananatomical standpoint, such an interpretation attributes to frontal, subcortical damage(which may also disrupt connections with frontal areas), or both, a key role in givingrise to perseverative errors (Na et al., 1999; Nys et al., 2006; Pia et al., 2009; Rusconiet al., 2002; Vallar et al., 2006). In the present study, anatomical data were based on
Drawing perseveration in neglect 11
medical reports, and, therefore, no definite conclusions can be drawn (7 out of 13[53%] patients had lesions involving frontal or subcortical structures). The standardneurological exam (Bisiach & Faglioni, 1974) showed, however, that all patients hadcontralesional hemiplegia or hemiparesis, indicating anterior/subcortical damage.
To summarize, this study, using an experimental manipulation of target density inthe display, provides evidence to the effect that drawing perseveration is a distinctdeficit with respect to the core primary impairment of left spatial neglect, namelyomission errors. In visuo-motor exploratory tasks such as cancellation, in neglect patientsperseveration can result from the combined effect of: (1) a representational/attentionalrestriction of exploration to the ipsilesional portion of space, due to neglect, on the onehand; (2) impaired motor response inhibition (related to frontal-subcortical damage),on the other hand, with the ipsilesional focusing of attentional/representational spatialprocesses lateralizing perseveration behaviour towards the ipsilesional side (Rusconiet al., 2002; Vallar et al., 2006).
Finally, it is worth noticing that our conclusions are mainly based on negative findings,namely the lack of a significant statistical relationship. Hence, since the ’absence ofevidence is not evidence of absence’ (Altman & Bland, 1995), our findings shouldbe taken with caution, with further studies being needed. It should be also noted,however, that interpretations of perseveration as integral to spatial neglect cruciallypredict an association between the two disorders. The present findings do not ruleout the possibility that, at least in some patients, perseveration behaviour may becaused or influenced also by other factors, such as residual processing of contralesionalinformation (Bottini & Toraldo, 2003; Manly et al., 2002; Toraldo et al., 2005), or thesaliency of ipsilesional, non-neglected information, which modulates both omission andperseveration errors (Mark et al., 1988). Another factor to be taken into consideration is aspatial working memory deficit, which can contribute to a disproportionate revisiting ofpreviously explored targets, during computerized visual search tasks (Husain et al., 2001;Malhotra, Mannan, Driver, & Husain, 2004; Malhotra, Parton, Driver, & Husain, 2003;Mannan et al., 2005; Parton et al., 2006; Wojciulik, Husain, Clarke, & Driver, 2001).However, perseveration and revisiting are dissociable (Husain et al., 2001; Mannanet al., 2005) and spatial working memory performance is not correlated to perseverationseverity in classic pencil-and-paper cancellation tasks (Ronchi et al., 2009).
In conclusion, we show differential effects of target density on perseverationbehaviour and left unilateral spatial neglect. Future research may further elucidate thefactors modulating different types of repetitive behaviour (perseveration, revisiting) inbrain-damaged patients with spatial neglect, and their anatomical underpinnings.
AcknowledgmentsThese works was supported in part by a Compagnia di San Paolo grant (2008–2010) to L.P.,and by FAR of the University of Milano-Bicocca and Ricerca Corrente grants from the IRCCSThe Italian Institute for Auxology to G.V. The manuscript is original, not previously published,and not under concurrent consideration elsewhere. We state no conflict of interests and therespect of requirements for authorship.
ReferencesAlbert, M. L. (1973). A simple test of visual neglect. Neurology, 23(6), 658–664.

12 L. Pia et al.
Altman, D. G., & Bland, J. M. (1995). Absence of evidence is not evidence of absence. BritishMedical Journal, 311(7003), 485.
Bisiach, E., & Faglioni, P. (1974). Recognition of random shapes by patients with unilateral lesionsas a function of complexity, association value and delay. Cortex, 10(2), 101–110.
Bottini, G., & Toraldo, A. (2003). The influence of contralesional targets on the cancellation of ipsile-sional targets in unilateral neglect. Brain and Cognition, 53(2), 117–120. doi:10.1016/S0278-2626(03)00091-5
Caplan, B. (1985). Stimulus effects in unilateral neglect. Cortex, 21(1), 69–80.Chatterjee, A., Mennemeier, M., & Heilman, K. M. (1992a). A comparison of line bisection and
cancellation in unilateral neglect. Journal of Clinical and Experimental Neuropsychology,85(14), 267–274.
Chatterjee, A., Mennemeier, M., & Heilman, K. M. (1992b). Search patterns and neglect: A casestudy. Neuropsychologia, 30(7), 657–672. doi:10.1016/0028-3932(92)90070-3
Chatterjee, A., Mennemeier, M., & Heilman, K. M. (1992c). A stimulus-response relationship in uni-lateral neglect: The power function. Neuropsychologia, 30(12), 1101–1108. doi:10.1016/0028-3932(92)90101-Q
Chatterjee, A., Thompson, K. A., & Ricci, R. (1999). Quantitative analysis of cancellation tasks inneglect. Cortex, 35(2), 253–262. doi:10.1016/S0010-9452(08)70798-6
Diller, L., & Weinberg, J. (1977). Hemi-inattention in rehabilitation: The evolution of a rationalremediation program. Advances in Neurology, 18, 63–82.
Eramudugolla, R., Irvine, D. R. F., & Mattingley, J. B. (2007). Association between auditoryand visual symptoms of unilateral spatial neglect. Neuropsychologia, 45(11), 2631–2637.doi:10.1016/j.neuropsychologia.2007.03.015
Gainotti, G., Perri, R., & Cappa, A. (2002). Left hand movements and right hemisphere activationin unilateral spatial neglect: A test of the interhemispheric imbalance hypothesis. Neuropsy-chologia, 40(8), 1350–1355. doi:10.1016/S0028-3932(01)00211-1
Halligan, P. W., Fink, G. R., Marshall, J. C., & Vallar, G. (2003). Spatial cognition: Evidence fromvisual neglect. Trends in Cognitive Sciences, 7(3), 125–133.
Heilman, K. M., & Watson, R. T. (1978). Changes in the symptoms of neglect induced by changingtask strategy. Archives of Neurology, 35(1), 37–49. doi:10.1016/S1364-6613(03)00032-9
Heilman, K. M., Watson, R. T., & Valenstein, E. (2003). Neglect and related disorders. In K. M.Heilman & E. Valenstein (Eds.), Clinical neuropsychology (4th ed., pp. 296–346). New York:Oxford University Press.
Husain, M. (2008). Hemispatial neglect. In G. Goldenberg & B. Miller (Eds.), Handbook of clinicalneurology (Vol. 88, pp. 359–372). Amsterdam: Elsevier.
Husain, M., Mannan, S., Hodgson, T., Wojciulik, E., Driver, J., & Kennard, C. (2001). Impairedspatial working memory across saccades contributes to abnormal search in parietal neglect.Brain, 124(5), 941–952. doi:10.1093/brain/124.5.941
Khurshid, S., Longin, H., Crucian, G. P., & Barrett, A. M. (2009). Monocular patching af-fects inattention but not perseveration in spatial neglect. Neurocase, 15(4), 311–317.doi:10.1080/13554790902776888
Kim, E. J., Lee, B. H., Park, K. C., Suh, M. K., Ku, B. D., & Heilman, K. M. (2009). Consecutive versusreturn motor perseveration during line cancellation task in hemispatial neglect. Cognitive andBehavioral Neurology, 22(2), 122–126.
Malhotra, P., Mannan, S., Driver, J., & Husain, M. (2004). Impaired spatial working memory: Onecomponent of the visual neglect syndrome? Cortex, 40(4–5), 667–676. doi:10.1016/S0010-9452(08)70163-1
Malhotra, P., Parton, A., Driver, J., & Husain, M. (2003). A spatial memory deficit exacerbates visualneglect following stroke. Journal of Neurology, Neurosurgery and Psychiatry, 74(3), 23.
Manly, T., Woldt, K., Watson, P., & Warburton, E. (2002). Is motor perseveration in unilateralneglect ‘driven’ by the presence of neglected left-sided stimuli? Neuropsychologia, 40(11),1794–1803. doi:10.1016/S0028-3932(02)00035-0
Drawing perseveration in neglect 13
Mannan, S. K., Mort, D. J., Hodgson, T. L., Driver, J., Kennard, C., & Husain, M. (2005). Revisitingpreviously searched locations in visual neglect: Role of right parietal and frontal lesionsin misjudging old locations as new. Journal of Cognitive Neuroscience, 17(2), 340–354.doi:10.1162/0898929053124983
Mark, V. W., Kooistra, C. A., & Heilman, K. M. (1988). Hemispatial neglect affected by non-neglected stimuli. Neurology, 38(8), 1207–1211.
Na, D. L., Adair, J. C., Kang, Y., Chung, C. S., Lee, K. H., & Heilman, K. M. (1999). Motorperseverative behavior on a line cancellation task. Neurology, 52(8), 1569–1576.
Nys, G. M., Seurinck, R., & Dijkerman, H. C. (2008). Prism adaptation moves neglect-relatedperseveration to contralesional space. Cognitive and Behavioral Neurology, 21(4), 249–253.doi:10.1097/WNN.0b013e31818a5cc1
Nys, G. M., van Zandvoort, M. J., van der Worp, H. B., Kappelle, L. J., & de Haan, E. H. (2006).Neuropsychological and neuroanatomical correlates of perseverative responses in subacutestroke. Brain, 129(8), 2148–2157. doi:10.1093/brain/awl19
Parton, A., Malhotra, P., Nachev, P., Ames, D., Ball, J., & Chataway, J. (2006). Space re-exploration inhemispatial neglect. Neuroreport, 17(8), 833–836. doi:10.1097/01.wnr.0000220130.86349.a7
Pia, L., Folegatti, A., Guagliardo, M., Genero, R., & Gindri, P. (2009). Are drawing perseverationspart of the neglect syndrome? Cortex, 45(3), 293–299. doi:10.1016/j.cortex.2007.11.015
Ricci, R., Pia, L., & Gindri, P. (2004). Effects of illusory spatial anisometry in unilateral neglect.Experimental Brain Research, 154(2), 226–237. doi:10.1007/s00221-003-1650-y
Ronchi, R., Posteraro, L., Fortis, P., Bricolo, E., & Vallar, G. (2009). Perseverationin left spatial neglect: Drawing and cancellation tasks. Cortex, 45(3), 300–312.doi:10.1016/j.cortex.2008.03.012
Rusconi, M. L., Maravita, A., Bottini, G., & Vallar, G. (2002). Is the intact side really intact?Perseverative responses in patients with unilateral neglect: A productive manifestation.Neuropsychologia, 40(6), 594–604. doi:10.1016/S0028-3932(01)00160-9
Toraldo, A., Gandola, M., Loffredo, S., Rancati, A., Zanardi, G., & Bottini, G. (2005). Can-celing out both the real and the spectral lines. Brain and Cognition, 57(3), 226–235.doi:10.1016/j.bandc.2004.08.051
Vallar, G. (1998). Spatial hemineglect in humans. Trends in Cognitive Sciences, 2(3), 87–97.Vallar, G., & Mancini, F. (2010). Mapping the neglect syndrome onto neurofunctional streams.
In N. Gangopadhyay, M. Madary, & F. Spice (Eds.), Perception, action, and consciousness:Sensorimotor dynamics and two visual systems (pp. 183–215). Oxford: Oxford UniversityPress.
Vallar, G., Rusconi, M. L., Fontana, S., & Musicco, M. (1994). Tre test di esplorazione visuo-spaziale: Taratura su 212 soggetti normali [Three clinical tests for the assessment of visuo-spatial exploration. Norms from 212 normal subjects]. Archivio di Psicologia, Neurologia ePsichiatria, 55(4), 827–841.
Vallar, G., Zilli, T., Gandola, M., & Bottini, G. (2006). Productive and defective impairments inthe neglect syndrome: Graphic perseveration, drawing productions and optic prism exposure.Cortex, 42(6), 911–920. doi:10.1016/S0010-9452(08)70435-0
Wojciulik, E., Husain, M., Clarke, K., & Driver, J. (2001). Spatial working memory deficit inunilateral neglect. Neuropsychologia, 39(4), 390–396. doi:10.1016/S0028-3932(00)00131-7
Received 4 July 2011; revised version received 28 March 2012