the role of right side objects in left side neglect: a dissociation between perceptual and...
TRANSCRIPT

Nuurop\~~hok,ylu. Vol. 31. No. 8, pp. 761-773. 1993. Punted I” Great Br~lam
002X-3932.93 $6.00+0.00 c 1993 Pergamon Press Ltd
THE ROLE OF RIGHT SIDE OBJECTS IN LEFT SIDE NEGLECT: A DISSOCIATION BETWEEN PERCEPTUAL AND DIRECTIONAL
MOTOR NEGLECT
ELISABETTA LADAVAS,* CARLO UMILTA,~ PAOLA ZIANI,$ ALESSANDRA BROGI~ and MARTINA MINARINI~
*Dipartimento di Psicologia, Universita di Bologna; tDipartimento di Psicologia Generale, Universita di Padova; and $Ospedale “I Fraticini”, Firenze, Italy
(Receiced 17 September 1992; accepted 1 March 1993)
Abstract-Based on a test introduced by TEGN~R and LEVANDER, Brain 114, 1943-1951, 1991, right brain-damaged patients were assigned to a group with unilateral perceptual neglect and a group with directional motor neglect. Brain scans showed that all directional motor neglect patients had frontal lesions, whereas in perceptual neglect patients the frontal lobes were always spared. All patients were asked to execute two tasks, which were also administered to a control group. One task consisted in pointing to tokens symmetrically distributed on a display. The other task consisted in picking up the same tokens. The tasks were first executed with the aid of vision and then in a blindfolded condition. In the case of patients with perceptual neglect, performance on the left side was better in the pick-up task than in the pointing task and improved in the blindfolded condition. Neither patients with directional motor neglect nor control patients showed these effects. The results were explained in terms of the hyperattentional hypothesis of perceptual neglect, according to which, in this form of neglect, attention is captured by the objects that lie on the right side of space.
INTRODUCTION
PATIENTS with unilateral spatial neglect (neglect for short) fail to report, respond or orient to stimuli presented on the side of space ipsilateral to the lesion (see, e.g. papers in Ref. [ 161). In humans, this condition is most common after right parietal lobe injury, which results in neglect for the left side of space (see, e.g. Refs [7] and [33]).
The most widely accepted interpretation of neglect attributes it to a deficit in spatial orienting (see, e.g. papers in Ref. [16]). One possibility is that neglect patients cannot direct attention to the affected side or display a weak orienting to that side [30, 311. However, it seems clear that processes that direct attention to the intact side may also play a causal role in neglect.
KINSBOURNE [ 173 suggested that neglect could be due to the fact that the left cerebral hemisphere’s bias toward the right hemispace is released from inhibition following right hemisphere damage. In accord with this view, POSNER et al. [27, 281 showed that patients with right parietal lesions were especially impaired in responding to left side stimuli when attention had first been directed to the right side. They attributed the deficit to an impairment in disengaging attention from the right side. Subsequently, other studies provided evidence in
*Address for correspondence: Elisabetta Lgdavas, Dipartimento di Psicologia, UniversitZ di Bologna, viale Berti Pichat, 5, 40127 Bologna, Italy.
761

762 E. LADAVAS et ul.
favour of the notion that neglect patients “overattend” to the rightmost position in the display [S, 10, 14, 18, 20, 221.
In the study by LADAVAS [lS], speed and accuracy for detecting stimuli in the rightmost position in a visual display were the same when the task required neglect patients to distribute attention over the entire display or to restrict it to the rightmost position. Apparently, irrespective of task demands, neglect patients always focused attention on the rightmost position. This interpretation was corroborated by another study [20], which showed that neglect patients outperformed controls in detecting stimuli presented in the rightmost position.
It seems reasonable to argue that visual neglect arises, not because of a difficulty in directing attention to the left (i.e. the hypoattentional hypothesis), but rather because of a strong bias toward maintaining focal attention on the rightmost position (i.e. the hyperattentiona2 hypothesis). Once attention is focused on the rightmost position, neglect patients find it very difficult to disengage attention from that position, and thus are poor at exploring those positions that lie further to the left [S].
On the basis of the hyperattentional hypothesis, it can be predicted that performance of neglect patients should improve when the stimuli positioned on the right side are rendered less salient, that is less attentional attracting. This prediction was confirmed by MARK et al.
[22], who employed a modification of the classical line cancellation task. It is well known that neglect patients typically fail to cancel lines shown on the left side of a
piece of paper [l]. In the MARK et al. [22] study, besides a control condition in which patients cancelled lines by drawing over them, there was also an experimental condition in which they actually erased the lines. Omissions in the left space were much more frequent in the drawing-over condition than in erasing condition. The fact that performance on the left improved when the lines were physically removed, rather than been just marked, clearly demonstrated the attentional bias caused by the stimuli on the right. The patients performed the task by first erasing the rightmost lines, which were removed from the display. Thus, attention could gradually shift to the left, being no longer captured by the stimuli on the right.
The directional scanning was also demonstrated by other studies. ECLIN et al. [lo] measured neglect patients’ search times for predesignated targets, while varying the number of distracters to the right of the target. They found that RT increased only as a function of the number ofdistractors on the intact side (i.e. objects present on that side), showing in this way that the degree of contralateral delay increased as the attentional requirements increased on the intact side. On the contrary, search proceeded with normal latency even to the left of midline when there were no rightsided distracters.
In a study by HJALTASON and TEGNBR [14] neglect patients were required to bisect a luminous line under two conditions, that is normal illumination and darkness. As expected, the patients made large rightward errors under normal illumination. Their performance, however, greatly improved in darkness. The improved performance in darkness was likely due to the elimination of background visual stimuli from the right side of space.
Two other studies confirmed that neglect patients have a bias to look to the right, intact side of space, but also suggested that this bias may manifests itself in the absence of right-side distracters. HORNAK [lS] recorded eye movements as patients with neglect searched in a completely darkened room to detect a light stimulus. It was found that fixations were confined almost entirely to the right side of space.
BUTTER [3] tested neglect patients for line cancellation also when the lines were confined to the left half of the sheet of paper. Performance improved in the half-sheet test in comparison

THE ROLE OF RIGHT SIDE OBJECTS IN LEFT SIDE NEGLECT 763
with the whole-sheet test. The patients, however, were still impaired in the former condition. The author concluded that hyperattention to stimuli in the unneglected hemispace (the “magnet effect” in his terminology) does play a role in causing neglect but cannot be the sole factor.
Relevant evidence was provided also by GENTILINI et al. [12]; (also see Ref. [4]; but see Ref. [35], for somewhat discrepant results), who employed a modified version of Chedru test [4], in which the patients are required to press the keys of a key-board. In the control condition, the neglect patients showed a strong preference to press the keys on the right side of the key-board. This bias, however, became much less marked in the experimental condition, in which the patients were blindfolded. It can be argued that performance on the left side improved in the absence of vision because the rightmost keys no longer attracted attention.
Subsequently, CUBELLI et al. [6] reanalysed the data of GENTILINI et al. [12], and pointed out that not all patients behaved as described above. In fact, three patients were found to be impaired only when blindfolded, whereas the rest were more impaired, or exclusively impaired, when the test was performed with the assistance of vision. This may be explained by making recourse to the distinction between predominantly perceptual and predominantly directional motor forms of neglect [2, 5, 29, 321.
As said before, perceptual neglect is due an impaired ability to attend to stimuli in the contralesional hemispace. This difficulty may in turn results from either an incapacity to orient attention to the left (hypoattentional hypothesis) or to a compulsory tendency to maintain attention on the right (hyperattentional hypothesis). Although most current theories emphasize the importance of purely sensory or “input” factors in neglect, there are some impairments of goal-directed action which may accompany, or be responsible for, neglect behaviour. For example, the phenomenon of nonsensory or motor neglect has been reported in both animals [33, 361 and humans [21, 261. It involves a disturbance of spontaneous movement of the contralesional limbs in the absence of hemiplagia. This should be distinguished from direction specific impairments in the spatial extent of voluntary movements and direction specific slowness in initiating movements toward the contralateral side of space. Unlike motor neglect, these impairments are manifest in movements carried out by the ipsilesional limbs and are not necessarily restricted to movements performed in the contralateral hemispace. We will call this impairment “directional motor neglect”, which refers to a slowness in the initiation of contralesional movements [ 13, 231, reduced spatial exploration toward the contralesional side [25, 321 and insufficient amplitude of contralesional limb movements [2].
It is interesting to note that the distinction between perceptual and directional motor neglect may have also an anatomical basis. Patients with isolated posterior (very frequently, parietal) lesions show perceptual neglect [7,32,34]. In contrast, WATSON et al. [36] showed that in monkeys frontal lesions caused “intentional” (i.e. directional motor) neglect. Later, MESULAM [24] explicitly proposed that anterior lesions may be associated with intentional neglect, whereas posterior lesions typically cause attentional deficits. This notion was supported by subsequent studies that showed that directional motor neglect was associated with anterior lesions [2, 5, 321.
It would seem reasonable to predict that the procedures described above, which removed the rightmost stimuli in the display, either by erasing them [22]or by blindfolding the patient [12], should be more effective in reducing neglect when the cause of the deficit is predominantly perceptual. In contrast, one should expect much less improvement, or no improvement at all, when the origin of neglect is predominantly motoric.

764 E. LADAVAS rt al
The aim of the present study was two-fold. First, we wanted to complement the findings of MARK et al. [22] and GENTILINI er ul. [12] by combining the procedures employed in their studies. Second, and more important, we wanted to demonstrate that the improvement brought about by removing the stimuli on the right or by blindfolding the patient is limited to predominantly perceptual forms of neglect.
Crucial to the second aim of the study was, of course, the possibility of differentiating patients with perceptual neglect from patients with directional motor neglect. To this end, we employed a procedure introduced by TEGNF:R and LEVANDER [32]. Their patients performed the line cancellation task [l] under two conditions, that is with normal viewing or through a 90” angle mirror. When the patient looked at the display through the mirror, the lines that lay on the left side of the display were seen in the right half of the mirror, whereas the lines on the right side of the display were seen in the left half of the mirror. In normal viewing, 14 patients showed the typical neglect behaviour with a vertical boundary between the marked lines on the right and the unmarked lines on the left. They, however, differed in the way they behaved in the mirror condition: 10 cancelled lines in the left hemispace, whereas four cancelled lines in the right hemispace.
Those patients who cancelled lines in the right hemispace during normal viewing and lines in the left hemispace during mirror viewing were considered to show perceptual neglect. This is because they directed attention to the right in either condition. In contrast, those patients who cancelled lines in the right hemispace during both normal and mirror viewing were considered to show directional motor neglect. This is because in the mirror condition they directed attention to the left but made no movements into the left hemispace. Accordingly, in the present investigation, patients were assigned to the perceptual neglect or to the directional motor neglect group, depending on how they behaved in the mirror condition of the TEGN~R and LEVANDER test [32].
MATERIALS AND METHODS Patients
The study comprised a series of IO right brain-damaged (RBD) patients with unilateral neglect, and 5 RBD patients without neglect (all recruited from I Fraticini Hospital, Florence). All patients had unilateral lesions due to cerebrovascular events. The side and the site of lesion were confirmed by CT or MRI scans (see Table I). All were right-handed. Sex, age, length of illness, and visual field, as assessed by campimetry. are reported also in Table I. Note that only patients without field defects were included in the study.
The presence of neglect was assessed by two cancellation tests: the bell cancellation test [I I], and the letter can- cellation test [9].The RBDpatientswith unilateralneglect omitted at least 50% ofthestimuli on the left inevery test. It is worth stressing that additional RBD patients were tested for the presence of neglect, but were discarded because the deficit was not severe enough. They failed to reach the criterion of 50% left side omissions m one of the tests.
The control group was comprised of other RBD patients without neglect. For them, the difference between left side and right side omissions never exceeded IO”/0 in either direction.
Assessment c~f’perceptuui and dirrctionul motor neglrct
As said, the distinction between perceptual and directional motor neglect was based on the outcome of the mirror condition of the TEGN~R and LEVANUER test 1321. Patients were assigned to the perceptual neglect group or to the directional motor neglect group depending on whether omissions on the left side exceeded by five or more omissions on the right side (perceptual group) or vice-versa (directional motor group). This resulted in two groups of five patients each, one group with perceptual neglect and one group with directional motor neglect.
As shown in Table 1, all the patients belonging to the perceptual group had lesions to the right parietal lobe, whereas those belonging to the directional motor group had lesions that included also the right frontal lobe. The scores obtained by each of the 15 patients in the two tests for the assessment of neglect and in the TFC;N~R and LEVAWER test 1321 are reported in Table 2.

THE KOLE OF RIGHT SIDE OBJECTS IN LEFT SIDE NEGLECT 765
Table I. Summary of clinical data for the patients with perceptual neglect (PPl-PPS), directional motor neglect
(PM]-PMS), and those of the control group (PCl-PCS); R = Right, F = Frontal, P = Parietal, T = Temporal, D = Deep
Case Sex/age
Onset of illness
(months) Visual field
Locus of lesion
PPI PP2 PP3 PP4 PP5
PM1 PM2 PM3 PM4 PM5
PCI PC2 PC3 PC4 PC5
M,63 F,80 M,61 M,78 M,70
F,69 M,82 M,64 M,67 F,78
M,72 F,60 M,65 M,78 F,64
14 Normal RTPD 21 Normal RTPD
9 Normal RTP 34 Normal RP 10 Normal RTP
19 Normal RFTP 8 Normal RFTP
24 Normal RFPD 34 Normal RFTPD
8 Normal RFP
36 Norma1 RPD 12 Norma1 RTP 8 Norma1 RPD
34 Norma1 RFTPD 24 Norma1 RD
Table 2. Number of correct responses for the patients with perceptual neglect (PPI-PPS), directional motor neglect (PM 1 PM5), and those of the control group (PC1 PC2) in the clinical tests (cancellation tests and Tegner
and Levander test) as a function of Side (left and right). The number of stimuli on each side was 5 I for the letter cancellation task, I7 for the bell
cancellation task, and 20 for the Tenger and Levander test
Cancellation tests Tegntr and Levander’s test Letters Bells Normal view Mirrow view
Case L R L R L R L R
PPI PP2 PP3 PP4 PP5
PM1 PM2 PM3 PM4 PM5
PC1 PC2 PC3 PC4 PC5
0 42 0 15 5 20 5 0 0 39 0 5 15 20 5 0 0 10 0 4 0 18 13 4 0 28 0 I4 16 20 13 5
IO 25 0 10 15 20 15 6
0 7 0 17 4 15 0 6 0 19 0 2 I6 20 5 I3 0 25 0 10 I5 20 3 15
IO 25 0 5 I5 20 0 14 0 39 0 15 16 20 5 13
50 51 16 17 20 20 16 15 45 40 12 11 20 20 13 13 50 53 16 16 20 20 I5 I6 45 41 11 11 20 20 16 15 48 47 14 I4 20 20 I5 15
766 E. LADAVAS et al
Experimental phase
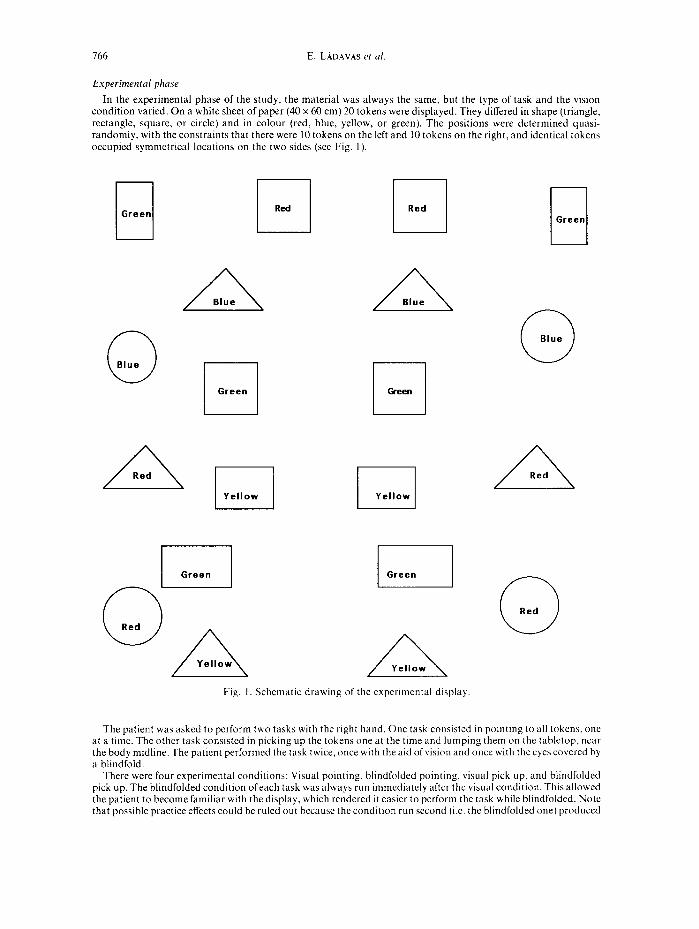
In the experimental phase of the study, the material was always the same, but the type of task and the vision condition varied. On a white sheet of paper (40 x 60 cm) 20 tokens were displayed. They differed in shape (triangle, rectangle, square, or circle) and in colour (red, blue, yellow, or green). The positions were determined quasi- randomly, with the constraints that there were 10 tokens on the left and 10 tokens on the right, and identical tokens occupied symmetrical locations on the two sides (see Fig. I)
rl Green r Red
1 I
I k-l I I
A Blue
0 Blue
A Red
A BIUI?
0 Green
r Yellow
Fig. I Schematic drawing of the experimental display
0 Green
0 Blue
A Red
0 Red
The patient was asked to perform two tasks with the right hand. One task consisted in pointing to all tokens, one at a time. The other task consisted in picking up the tokens one at the time and lumping them on the tabletop, near the body midline. The patient performed the task twice, once with the aid of vision and once with the eyes covered by a blindfold.
There were four experimental conditions: Visual pointing, blindfolded pointing, visual pick up, and blindfolded pick up. The blindfolded condition ofeach task was always run immediately after the visual condition. This allowed the patient to become familiar with the display, which rendered it easier to perform the task while blindfolded. Note that possible practice effects could be ruled out because the condition run second (i.e. the blindfolded one) produced

THE ROLE OF RIGHT SIDE OBJEC’TS IN LEFT SIDE NEGLECT 167
a better performance in one group but not in the other two groups (see results below). Half of the subjects in each group began with the pointing task and half with the pick-up task.
In the visual condition the subject was instructed to point to or pick up all the tokens that were present in the display. In either the visual or blindfolded condition, a trial was considered to be valid onlv if the token was touched (pointing task) or picked up (pick up task). The patients were not explicitly informed as to-the number and nature of the tokens.
There was no time limit and every experimental condition continued until the patient declared that he/she had pointed to or picked up all the tokens. If the patient did not point or pick up a token in either condition, the experimenter did not call his/her attention to the omission. In performing the pick-up task while blindfolded, the patients sometimes knocked against other tokens, thus obtaining additional tactile information. This might account for a better performance in the blindfolded condition. However, this possibility could also be ruled out because only one group of patients showed an advantage for the blindfolded condition (see Results below).
RESULTS
As will be seen, the results showed that, for patients with perceptual neglect, performance on the left side was better in the pick-up than in the pointing task. In addition, in either task performance improved when the patients were blindfolded. In contrast, patients with directional motor neglect and control patients did not show either the advantage of the pick- up task over the pointing task or the advantage of the blindfolded condition over the visual condition.
The dependent variable was number of omissions. The scores obtained by each patient in the four experimental conditions on the two sides of space were submitted to an overall analysis of variance, with one between-subjects factor, i.e. Group (RBD patients with perceptual neglect, RBD patients with directional motor neglect, or RBD patients without neglect), and three within-subjects factors, i.e. type of Task (pointing or pick up), Vision condition (with or without vision), and Side of space (left or right).
A number of sources were significant (all Ps < 0.01 or less): The main effects Task, Vision, and Side, and the interactions Group x Vision, Group x Side, Task x Side, Group x Task x Vision, Group x Task x Side, and Task x Vision x Side. Considering that the four-way
interaction Group x Task x Vision x Side was also highly significant [F (2, 12) = 11.03, P-c 0.0021 additional analyses of variance were performed, separately, for each group. They had the same three within-subjects factors used in the overall analysis. Besides these analyses of variance, pairwise comparisons using the Newman-Keuls method were conducted whenever necessary. The level of significance was always set at 0.05.
Perceptual group
The main effects Task and Side were significant: [F (1,4)= 1000.00, P<O.OOOOl] and [F (1, 4) = 450.78, P < O.OOOOl], respectively. Also significant were the interactions Task x Vision [F (1,4)= 11.61, P-cO.031, Task x Side [F(l, 4)=49.23, P-cO.0031 and Task x Vision x Side [F (1,4) = 24.68, P< O.OOS].
Omissions were more frequent on the left than the right side (46 vs 10%) and in the pointing task than in the pick-up task (41 vs 16%). With the aid of vision, pointing was much less accurate than pick up (50 vs lo%), whereas the two tasks did not differ in the blindfolded condition (32 vs 22%). For both tasks, performance was less accurate on the left than the right side, but the difference was larger for pointing (69 vs 13%) than for pick up (24 vs 8%).
The most interesting source of variance was no doubt the three-way interaction. It showed that on the right side omissions did not depend on either type of task or vision condition: 10% for normal pointing, 6% for normal pick up, 16% for blindfolded pointing, and 10% for
768
100
so
60
70
60
50
40
30
20
10
0
n left space
m right space
normal normal pointing pick up
blindfolded pointing
blindfolded Dick UP
60
50
40
30
20
10
0 normal pointing
normal pick up
blindfolded pointing
blindfolded pick up
50
40
30
20
10
normal pointing
normal pick up
blindfolded pointing
blindfolded pick up
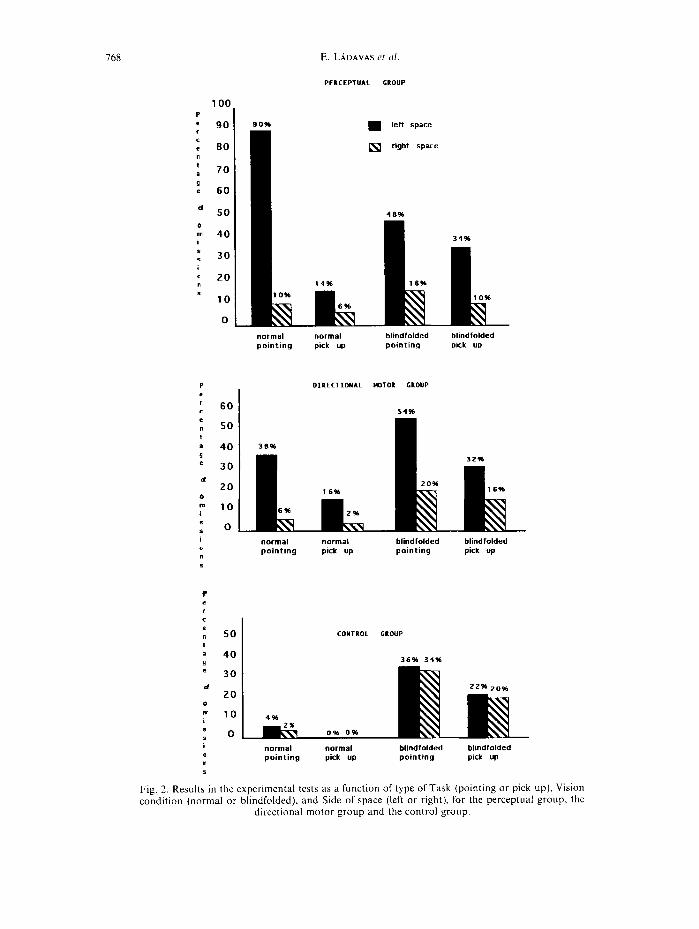
Fig. 2. Results in the experimental tests as a function of type of Task (pointing or pick up), Vision condition (normal or blindfolded), and Side of space (left or right). for the perceptual group, the
directional motor group and the control group.
THE ROLE OF RIGHT SIDE OBJECTS IN LEFT SIDE NEGLECT 769
blindfolded pick up. In contrast, on the left side performance was worse for pointing than pick up, but the difference decreased in the blindfolded condition: 90% for normal pointing, 14% for normal pick up, 48% for blindfolded pointing, and 34% for blindfolded pick up (see Fig. 2). Alternatively, one can say that, on the left side, pointing performance was better in the blindfolded condition, whereas pick up performance was better with the aid of vision.
Directional motor group
The only significant source of variance was the main effect Side [F (1,4) = 8.8 1, P -=c 0.051. As expected, performance was poorer on the left than the right side (35 vs 11%).
Because the power of the statistical test was very low, also sources not too far from the conventional level of significance are worth noting. These were Task [F (1,4) =4.40, P<O.ll], Vision [F(l, 4)=7.66, P<O.O6] and Task x Side [F(l, 47)=4.87, P<O.l]. Omissions were more numerous for pointing than pick up (30 vs 17%) and in the blindfolded than in the normal condition (3 1 vs 16%). There was a tendency for the difference between pointing and pick up to be larger on the left side (46 vs 24%) than on the right side (13 vs 9%).
The three-way interaction, however, did not even approach significance. On the right side, omissions in the four experimental conditions were the following: 6% for normal pointing, 2% for normal pick up, 2% for blindfolded pointing, and 16% for blindfolded pick up. On the left side, the corresponding figures were 38, 16, 54, and 32% (see Fig. 2).
Control group
The only significant source of variance was the main effect Vision [F (1,4)= 17.67, P<O.O2]. It showed that these patients made more omissions in the blindfolded than in the normal condition (28 vs 2%). No other sources approached statistical significance.
Performance in the four experimental conditions was as follows. On the right side: 2% for normal pointing, 0% for normal pick up, 34% for blindfolded pointing, and 20% for blindfolded pick up. On the left side, the corresponding figures were 4,0, 36 and 22% (see Fig. 2).
DISCUSSION
The discussion will be concerned with the results that are relevant for the hypothesis put forward in the introduction. We will not dwell on the difference in accuracy between left and right sides of space, which were observed for the experimental groups. More omissions on the left than the right side were only to be expected, because the experimental groups were comprised of patients with left side neglect.
As said, evidence in support of the hyperattentional hypothesis was provided, among others [3, 8, 10, 14, 15, 18,201, by MARK et al. [22], who showed that on the affected side, neglect patient made more omissions in a drawing-over task than in a equivalent erasing task, and by GENTILINI et al. 1123, who showed that, at least in some cases, omissions on the left side diminished when the eyes were covered.
Considering that neglect manifests itself in either a perceptual or a directional motor form, we reasoned that the improvement in performance on the affected side, caused by the
110 E. LADAVAS et cd.
disappearance of the stimuli on the intact side, should occur only in the case of perceptual neglect. This is because directional motor neglect is mainly due to the exploratory-motor component of the task and the role played by the attentional bias toward right side stimuli should be less prominent than it is in perceptual neglect.
The results of the present study confirmed the findings of MARK et al. [22] and GENTILINI
et al. [12], but also supported the prediction of a dissociation between perceptual and directional motor neglect. When the eyes were open, the performance of patients with perceptual neglect was better in the task in which the objects were removed from the display (i.e. the pick up task) than in the task in which all objects were always present (i.e. the pointing task).
In the pick up task, the patients started removing the objects from the right side [3,22] and this apparently allowed a better exploration of the left side. In contrast, in the pointing task attention could not be moved from the right side because the objects remained there. This interpretation is corroborated by the finding that the difference between the two tasks was much smaller in the blindfolded condition, that is when removing the objects on the right side did not affect the number of visible, attention-attracting stimuli.
The blindfolded condition, however, did produce some interesting differences. In the pointing task, performance on the affected side was better without than with the aid ofvision. This finding is even more striking if one considers that pointing should normally be easier when guided by vision, as shown by control patients and by patients with directional motor neglect. It would appear that, as suggested by GENTILINI et ul. [12], in the blindfolded condition the attentional bias toward the stimuli on the right, which now are no longer visible, becomes weaker.
The advantage in favour of the blindfolded condition was not found in the pick up task. Based on what we have said so far, one would have predicted an identical trend for both tasks. In fact, if anything, performance was worse without the aid of vision. Likely, vision is more important for a task that requires grasping an object than just pointing in its direction. Thus, in the blindfolded condition, the negative effect of lack of visual guidance might have overcompensated the positive effect produced by less salient right side objects.
Not surprisingly, on the right side the pattern that emerged from testing patients with perceptual neglect was entirely different: No differences were found between the two types of task and between the two vision conditions. Omissions were very few and their number was nearly identical when patients were asked to point to the objects or to pick them up. Similarly, very few omissions were committed either with or without the aid of vision.
Also in the case of patients with directional motor neglect, on the left side performance was worse in the pointing task than in the pick up task. This difference, however, was small and nonsignificant. Furthermore, unlike patients with perceptual neglect, patients with directional motor neglect performed nearly identically in the two tasks, with or without the aid of vision. The nonsignificant difference found in the pointing task was in the opposite direction as compared to the difference found for patients with perceptual neglect. Patients with perceptual neglect committed more omissions with the aid of vision, whereas patients with directional motor neglect committed more omissions in the blindfolded condition. The performance of patients with directional motor neglect, like that of controls, may merely reflects the fact that the task becomes more difficult when vision is excluded.
In conclusion, it would seem fair to say that the overall pattern of results upheld the hypothesis that had motivated this study. As observed by previous studies [3, 12, 14, 221, performance of neglect patients on the left side improved when the stimuli on the right were

THE ROLE OF RIGHT SIDE OBJECTS IN LEFT SIDE NEGLECT 771
rendered less salient, either by removing them from the display (i.e. the pick up task) or by excluding vision (i.e. the blindfolded condition). It is also clear, however, that the improvement occurred mainly, if not exclusively, for patients with perceptual neglect. As argued before, this pattern of results is in favour of the hyperattentional hypothesis, but limits its validity to the perceptual form of neglect.
Perhaps, the present results could also be explained in terms of the disengage hypothesis [27, 281, by arguing that once the right side objects were removed (or became less salient), attention was no longer engaged in this location. The hypothesis does not explain, however, why attention should initially be preferentially engaged on the right side. The weak left side orienting hypothesis [30,31], instead, has great difficulties in explaining the present results, unless the post-hoc assumption is made that left side orienting became stronger when the objects on the right side were removed or became less salient. In addition, neither of these alternative hypotheses explains why neglect patients can outperform controls in detecting stimuli shown on the right side [20].
This study produced also two other interesting results. The first was an anatomical dissociation between the site of the lesion in perceptual neglect and directional motor neglect. As shown in Table 1, all cases of perceptual neglect had lesions confined to the parietal lobe, whereas all cases of directional motor neglect had lesions that involved both the parietal and the frontal lobes. It seems, thus, the latter form of neglect is attributable to a disruption of the mechanisms of the right frontal lobe. It is not clear, however, why lesions involving both the parietal and the frontal lobes do not produce both perceptual and directional motor forms of neglect, rather than only directional motor neglect.
Second, the fact that performance of patients with perceptual neglect improved in the pointing task in the blindfolded condition might indicate a difference between visual percepts and visual images. In the blindfolded condition the patients could perform the task only by forming a visual image of the display they had just inspected in the normal vision condition. If the visual image and the visual percept ofthe display were identical, one would not predict an improvement when the patients performed the pointing task on an imagined display in comparison to when the display was actually perceived. However, such an improvement did occur. It would seem, thus, that the spatial features of a mental representation are different from those of a perceptual representation, and/or attention is shifted differently in these two types of representation. Perhaps, the stimuli on the right side are less salient in a mental representation than in a perceptual representation, and because of this attention was less strongly captured by the rightmost stimuli in a mental than in a perceptual representation.
Finally, it is worth noting that there was a striking similarity between the performance of the perceptual and directional motor neglect groups in the blindfolded condition. In contrast, the performance of the two groups differed in the normal vision condition. This might be taken as further evidence in support of a functional difference between images (i.e. the blindfolded condition) and percepts (i.e. the normal vision condition). Alternatively, one might suggest that, by blindfolding the patient, the motor component was unmasked also in the case of a predominantly perceptual neglect. The latter explanation assumes, of course, that in perceptual neglect patients the deficit had two components, one perceptual and one motoric, but, under normal viewing conditions, the perceptual component was the dominant one.
Acknowledyements-E.L. and C.U. were supported by grants from MURST, C.U. was also supported by a grant from CNR (contract 9200184.PF41).
172 E. LADAVAS rt al
REFERENCES I. ALBERT, M. L. A simple test of visual neglect. Nrurolo~/y 23, 658 664, 1973. 2. BISIACH, E., GEMINIAN], G., BERTI, A. and Rcsco~~, M. L. Perceptual and premotor factors ofunilateral neglect.
Neuroloy) 40, 1278~ I28 I, 1990. 3. BUTTER, C. M. Effect of stimuli in right hemispace on left-sided neglect. Nrurop,sl.c,ho/oc/ia 30, 859 864. 1992. 4. CHEDRU. F. Space representation in unilateral spatial neglect. J. Neural. Neurosurfl. Psychiat. 39, 1057-1061,
1976. 5. COSLETT, H. B., BOWL-RS, D., FITZPA~KI~K, E., HAWS, B. and H~ILMAN, K. M. Directional hypokinesia and
hemispatial inattention in neglect. Bruin 113, 457 486, 1990. 6. CUBELLI, R., NICHELLI, P., BONITO, V.. DF TAKTI, A. and INZAGHI, M. G. Different patterns of dissociation in
unilateral spatial neglect. Brain Cm/nit. 15, 139-159, 1991. 7. DE RENZI, E. Disorders c!f Spucr E~plorution and Coynition. Wiley, London. 1982. 8. DE RENZI, E., GEYTILINI. M.. FAC;LIONI, P. and BARBIERI, C. Attentional shift towards the righmost stimuli in
patients with left visual neglect. C‘ortru 25, 231 237, 1989. 9. DILLER, L. and WEINHEKC;. J. Hemi-inattention in rehabilitation: The evolution of a rational remediation
program. In Herni-inattention and Hemispheric Specializc~tron, Adounces in Neuroloyy, E. A. WEINS~~IV and R. P. FKIEULAND (Editors). Vol. 18. pp. 63 82. Raven Press. New York, 1977.
IO. EOLI~. M., ROBFKSON. L. C. and KNIGHT. R. T. Visual search performance in the neglect syndrome. J. Cm/nit. Nrurosci. 1, 372-385. 1989.
I I. GAIJTHIER. L., DFHAIJT, F. and JOA~ETT, J. The bells test: A quantitative and qualitative test for visual neglect. ht. J. din. h’rurop.s~cho/. 11, 49-54, 1989.
12. GENTILINI. M., BARBIEKI. C., DE RENLI. E. and FAC~LIONI, P. Space exploration with and without the aid of vision in patients with unilateral brain damage. Cortrlc 25, 643- 651, 1989.
13. HEILMAN, K. M., BOWERS. D.. COSL~TT. H. B.. WHELAN, H. and WATSON, R. T. Directional hypokinesia: Prolonged reaction times for leftward movements in patients with right hemisphere lesions and neglect. Neurokxqy 35, 855 X59. 1985.
14. HJALTASON, H. and T%N~~K. R. Darkness improves line bisection in unilateral spatial neglect. Carter 28, 353 358, 1992.
15. HOKNAK, J. Ocular exploration in the dark by patients with visual neglect. Nru~op,s~~ho/r,Miu 30,547 552, 1992. 16. JEANNEKOU, M. (Editor) Nruroph~sio/o(li~cl/ und Neu,op.s?cholor/i~ul Mechunisnu o$Sptrtitr/ Ncylrct. Elsevier,
Amsterdam, 1987. 17. KIF*‘SHOUKN~, M. Mechanisms of unilateral neglect. In IYruroph~.\io/oyi~u/ cd Neurops!,cho/oyi~u/ ,Mrc~hu~~ism.s
cfSputia/ Negqlect, M. JEAKNFKOI) (Editor). pp. 69 86. Elsevier, Amsterdam, 1987. 18. LAUAVAS, E. Selective spatial attention in patients with visual extinction. Bruin 113, 1527 1538. 1990. 19. LADAVAS, E. Spatial dimensions of automatic and voluntary orienting components of attention. In L’nilututrl
Neglect: Cliniwl uml E.~prrimrnttrl Studicx I. H. ROHFRSON and J. C. MAKSHALL (Editors). Taylor & Francis. London, 1992.
20. L~I~AVAS, E.. PTTKONIO, A. and UMILT~~, C. The deployment of attention m the intact field of hemineglect patients. Cortru 26, 307 317, 1990.
21. LAPLANI:. D. and Dtc;os. J. D. Motor neglect. .I. Nrurol. Neurosurq. Psyhitrt. 46, I52 158. 1983. 22. MAKK, V. W., KOOIS~KA, C. A. and HTILMAN, K. M. Hcmispatial neglect allected by non-neglected stirnull.
Nuuro/o<q_v 38, I207 12 I I. 198X. 23. M~ADOK, K. F., WATSON. R. T., BO~LKS, D. and HLILMAN. K. M. Hypomctria with hemlspatial and limb motor
neglect. Bruin 109, 293 305, 19X6. 24. MESIJLAM, M. M. A cortical network for directed attention and unilateral neglect. ilnn. Nrurol. IO, 309 325,
1981. 25. MIJOVI~, D. Mechanisms of visual spatial neglect. Absence of directional hypoktnesia in spatial exploration.
Brain 114, 1575 1593, 1991. 26. Oc;l,r~, J. A. Onset of motor neglect following a right parletal infarct and its recovery conscqucnt on the
removal of a right frontal mcningioma. N. Z. J. Pgchol. 17, 24- 31. 1988. 27. POSNEK. M. 1.. COHI.N, Y. and RAI.AL, R. D. Neural system control of spatial orienting. Phil. Trunr. K. SM.
London B298, I87 198. 1982. 28. POSNEK. M. 1. WALKEK. J. A.. F’KIF-t)KI(.H, F. A. and RA~AL. R. D. How do the parietal lobes direct covert
attention? Neurop.s~~ko/o~~iu 25, I35 145, 1987. 29. RFIJTEK-LOKENZ, P. A. and POSU~R, M. 1. Components of neglect from right-hemisphere damage: An analysis of
line bisection. Nrurops~rho/o(litr 28, 327 333, 1990. 30. RI~I>o~H. M. J. and HuMPtrKr:YS, G. W. (19X3). The effect ofculng on unilateral neglect. ,Yuuropa~~holociu 21,
5x9 -599, 1983. 31. SEKON, X., COYI:T-~~. F. and BKI.YI:K, R. Ipsilateral influcnccs on contralatcral processing in neglect patients
(b<qnit. Neurop.s!“,l”‘/. 6, 475 49X. 1989. 32. TT~N~K. R. and LEVANDLK, M. Through a looking glass. A new technique to demonstrate directional
hypokinesia in unilateral neglect. Bruirl 114, 1943 1951. 1991.
THE KOLE OF KIGHT SIDE OBJECTS IN LEFT SIDE NEGLECT 173
33. VALENSTEIN, E., HEILMAN, K. M., WATSON, R. T. and VAN DEK CON, J. J. Nonsensory neglect from parietotemporal lesions in monkeys. Neuro/oy~ 32, 1198-1201, 1982.
34. VALLAR. G. and PERANI, D. The anatomy of unilateral neglect after right hemisphere stroke lesions. A clinical CT/Scan correlation study in man. Neuropsychologiu 24, 609-622, 1986.
35. VALLAR. G., RUS~ONI, M. L., GEMIXIANI, G., BERTI, A. and CAPPA, S. F. Visual and nonvisual neglect after unilateral brain lesions: Modulation by visual input. Int. J. Neurosci. 61, 229-239, 1991.
36. WATSON, R. T., MILLER, B. D. and HEILMAN, K. M. Nonsensory neglect. Ann. Neural. 3, 505 -508, 1978.