dissertation on
TRANSCRIPT

1
DISSERTATION ON “A STUDY TO ASSESS THE EFFECTIVENESS OF SHORT
TERM FeSS PROTOCOL ON LEVEL OF DEPENDENCY
AMONG STROKE PATIENTS ADMITTED IN STROKE
WARD, RAJIV GANDHI GOVERNMENT GENERAL
HOSPITAL, CHENNAI-03”
M.Sc (NURSING) DEGREE EXAMINATION
BRANCH- I MEDICAL SURGICAL NURSING
COLLEGE OF NURSING
MADRAS MEDICAL COLLEGE, CHENNAI-600 003
A dissertation submitted to
THE TAMIL NADU Dr. M.G.R. MEDICAL UNIVERSITY,
CHENNAI - 600 032
In partial fulfilment of the requirement for the award of degree of
MASTER OF SCIENCE IN NURSING
OCTOBER – 2019
2
“A STUDY TO ASSESS THE EFFECTIVENESS OF SHORT
TERM FeSS PROTOCOL ON LEVEL OF DEPENDENCY
AMONG STROKE PATIENTS ADMITTED IN STROKE
WARD, RAJIV GANDHI GOVERNMENT GENERAL
HOSPITAL, CHENNAI-03”
Examination : M.Sc. (Nursing) Degree Examination
Examination Month and Year : October - 2019
Branch & Course : I – MEDICAL SURGICAL NURSING
Register Number : 301711256
Institution : COLLEGE OF NURSING,
MADRAS MEDICAL COLLEGE,
CHENNAI – 600 003.
Sd: __________________ Sd: ___________________
Internal Examiner External Examiner
Date: ____________ Date: ____________
THE TAMIL NADU Dr. M.G.R. MEDICAL UNIVERSITY,
CHENNAI - 600 032
3
CERTIFICATE
This is to certify that this dissertation titled “A STUDY TO ASSESS
THE EFFECTIVENESS OF SHORT TERM FeSS PROTOCOL ON
LEVEL OF DEPENDENCY AMONG STROKE PATIENTS ADMITTED
IN STROKE WARD, RAJIV GANDHI GOVERNMENT GENERAL
HOSPITAL, CHENNAI-03” is a bonafide work done by SOFIA
PRIYADHARSINI.S, M.Sc. (N) II year student, College of Nursing, Madras
Medical College, Chennai-03, submitted to The Tamil Nadu Dr. M.G.R
Medical University, Chennai, in partial fulfilment of the requirements for the
award of degree of Master of Science in Nursing, Branch I- MEDICAL
SURGICAL NURSING, under our guidance and supervision during the
academic period from 2017 – 2019.
Mrs.A.Thahira Begum, M.Sc(N)., MBA., M.Phil.,
Principal
College of Nursing,
Madras Medical College,
Chennai -03
Dr.R.Jayanthi, MD, FRCP(Glasg)
Dean
Madras Medical College
Chennai -03

4
“A STUDY TO ASSESS THE EFFECTIVENESS OF SHORT
TERM FeSS PROTOCOL ON LEVEL OF DEPENDENCY
AMONG STROKE PATIENTS ADMITTED IN STROKE
WARD, RAJIV GANDHI GOVERNMENT GENERAL
HOSPITAL, CHENNAI-03”
Approved by the Dissertation Committee on 24.07.2018
CLINICAL SPECIALITY GUIDE
Mrs.V.K.R.Periyar Selvi, M.Sc(N)., _____________
Reader in Medical Surgical Nursing,
College of Nursing,
Madras Medical College,
Chennai -03.
HEAD OF THE DEPARTMENT
Mrs.A.Thahira Begum, M.Sc(N)., M.B.A., M.Phil., _____________
Principal,
College of Nursing,
Madras Medical College,
Chennai-03.
DEAN
DR.R.Jayanthi, MD., FRCP (Glasg)., ___________ Dean,
Madras Medical College,
Chennai-03.
A Dissertation submitted to
THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY,
CHENNAI
In partial fulfillment of the requirement for award of the degree
MASTER OF SCIENCE IN NURSING
OCTOBER – 2019

5
ACKNOWLEDGEMENT
“I will give thanks to the lord with my whole heart; I will recount all of your wonderful deeds”
– Psalm 9:1
Gratitude calls never expressed in words but this only to deep
perceptions, which make words to flow from one‟s inner heart.
First of all, I praise God Almighty, merciful and passionate, for
providing me this opportunity and granting me the capability to
complete this study successfully. I lift up my heart in gratitude to God
Almighty, I feel the hand of God on me, leading me through thick and
thin heights of knowledge. It is he who granted me the grace and the
physical and mental strength behind all my efforts.
This dissertation appears in its current form due to the assistance
and guidance of many professionals and non-professionals. The
investigator is whole heartedly indebted to her research advisors for
their comprehensive assistance in various forms.
I express my genuine gratitude to the Institutional Ethics
Committee of Madras Medical College for giving me an approval to
conduct this study.
I wish to express my sincere thanks to Dr.R.Jayanthi, M.D.,
FRCP (Glasg), Dean, Madras Medical College, Chennai for providing
necessary facilities and extending support to conduct this study.
At the very outset, I express my whole hearted gratitude to my
esteemed guide, Mrs.A.Thahira Begum M.Sc.(N), MBA., M.Phil.,
Principal, College of Nursing, Madras Medical College, Chennai, for
her academic and professional excellence, treasured guidance, highly
instructive research mentorship, valuable suggestions, prudent guidance,

6
moral support and patience that has moulded me to conquer the spirit of
knowledge for sculpturing my manuscript into thesis.
I would like to express my deepest sense of gratitude to
Dr.R.Shankar Shanmugam, M.Sc. (N), MBA, Ph.D., Reader, H.O.D
– Department of Nursing Research, College of Nursing, Madras
Medical College, Chennai for his highly instructive research mentorship,
his hard work, efforts, interest and sincerity to mould this study in a
successful way. His easy approachability and understanding nature
inspired me to laid strong foundation in research. It is very essential to
mention his wisdom and helping nature made my research study a lively
and everlasting one.
I am grateful to Mrs.T.R.Latha M.Sc. (N), Reader, Department
of Medical Surgical Nursing, College of Nursing, Madras Medical
College, for her valuable guidance, suggestions, motivation, timely
insightful decision, and correction of the thesis with constant motivation
and timely help and support throughout the completion of this study.
I am highly indebted to Mrs.V.K.R.Periyar Selvi, M.Sc. (N),
Reader, Department of Medical Surgical Nursing, College of
Nursing, Madras Medical College, for her great support, warm
encouragement, constant guidance, thought provoking suggestions, brain
storming ideas, timely insightful decision, correction of the thesis with
constant motivation and willingness to help all the time for the fruitful
outcome of this study.
I am extremely grateful to Mrs.C.S.V.Umalakshmi, M.Sc.(N), Lecturer,
Mrs.J.Alamelumangai, M.Sc.(N), Lecturer, Mr.N.Muruganandan, M.Sc.
(N), Lecturer, Mrs.D.Anandhi, M.Sc.(N), Nursing Tutor, Department of
Medical Surgical Nursing for their encouragement, valuable suggestion,
support and advice given in the study.

7
I am grateful to Dr.G.Mala, M.Sc.(N), MBA., Ph.D., (Retd.
Nursing Tutor) and Mr.Kannan.K, M.Sc. (N), MBA, Nursing Tutor,
Department of Nursing Research, College of Nursing, Madras Medical
College, for their valuable guidance, suggestions, motivation and timely
help and support throughout the completion of this study
I am thankful to all the Faculty of College of Nursing, Madras
Medical College, for their timely advice, encouragement and support.
It‟s my duty to convey my thanks to all experts, Dr.Rama
Sambasivam, M.Sc. (N), Ph.D, Principal, Mohamed Sathak A J College
of Nursing ,Chennai; Dr.Tamilarasi, M.Sc.(N), M.Phil, Ph.D,
Principal, Madha College of Nursing, Chennai, who validated the
research tool and guided me with valuable suggestions and corrections,
constructive judgments while validating the tool.
I express my deep sense of sincere thanks to
Prof.R.Lakshminarasimhan, MD., DNB., DM., DNB., Director,
Institute of Neurology, Madras Medical College, Chennai-03, for his
valuable suggestions and kind guidance.
I have much pleasure of expressing my cordial appreciation and
thanks to all the patients who participated in the study with interest and
cooperation.
I owe my deepest sense of gratitude to Mr.A.Venkatesan, M.Sc.
(Statistics), P.G.D.C.A, Statistician for his suggestion and guidance in
statistical analysis.
I thank our librarian Mr.S.Ravi., M.L.I.S, College of Nursing,
Madras Medical College for his co-operation and assistance which built
the sound knowledge for this study.
8
I thank Dr.J.Ebenezer, B.Ed., M.Ed., and Ph.D. Headmaster,
Voorhees higher Secondary School, Vellore, for editing and providing
certificate of English editing.
I thank Mr.A.J.Theodore Rajkumar, Asst.Professor and HOD,
Department of Tamil for editing and providing certificate of Tamil
editing.
I owe my great sense of gratitude to Mr.Jas Ahamed Aslam,
Shajee computers and Mr.Ramesh, B.A., MSM Xerox for their
enthusiastic help and sincere effort in typing the manuscript with
valuable computer skills and also bringing this study into a printed form.
I extend my immense love and gratitude to my Mother
Mrs.Y.Louisa Margaret, B.Ed., for her loving support, encouragement,
earnest prayer, which enabled me to accomplish my study.
A very special thanks to my sister Ms.S.Selva Merlin, B.Sc. (N),
and my brother Mr.S.Joseph Martin, B.E, who laid the foundation of
my higher studies and for their constant support, endless patience,
unflagging love and motivation which helped me to complete my study
successfully.
I extend my heartfelt thanks to my friend Mr.S.Arun Kumar,
B.Com, for his motivation, support, patience and cooperation
throughout my study.
I would also like to thank my beloved friends Mrs.R.Revathy,
Ms.G.Priyadharshini, Mr.C.Thirupathi, Ms.S.Pabitha, Ms.A.Sandhiya,
and Ms.N.Athiba, for their constant encouragement towards the successful
completion of my study.
I take this opportunity to thank all my Colleagues, Friends,
Teaching and Non-Teaching Staff Members, of College of Nursing,

9
Madras Medical College, Chennai, for their co-operation and help
rendered in the completion of my study.
At final note, I extend my thanks to all those who have been
directly and indirectly associated with my study at various stages not
mentioned in this acknowledgement.
I thank the one above, omnipresent God, for answering my
prayers, for giving me the strength to plod on each and every phase of
my life.
10
ABSTRACT
Stroke, the sudden death of brain cells due to lack of oxygen when
the blood flow to the brain is lost by blockage or rupture of an artery to
the brain. Due to increased life expectancy and changes in lifestyle of
the population, the cerebrovascular accident (CVA) is becoming
increasingly common. In order to improve the patient‟s outcome ,
International clinical guidelines recommend early management of stroke
on arrival to the emergency department.
Optimal management of three common physiological
disturbances, namely fever, hyperglycaemia and dysphagia are the
important elements of organized stroke care with potential to
significantly influence outcomes. All three have been identified in
international guidelines, as priority care issues for inpatient stroke
management. Changing clinician practice remains a challenge. The
current study deals with nurse-initiated intervention focused on three
clinical protocols to manage fever, hyperglycaemia (Sugar)
and Swallowing dysfunction in the FeSS protocols, in the first 72 hours
of patient admission significantly decreased death and disability.
TITLE: “A study to assess the effectiveness of short term FeSS
protocol on level of dependency among stroke patients admitted in
stroke ward, Rajiv Gandhi Government General Hospital, Chennai-03”.
OBJECTIVES: To assess the pre-interventional level of
dependency among stroke patients, to determine the effectiveness of
short term FeSS protocol (post-intervention) on level of dependency
among stroke patients, to compare the pre-interventional and post-
interventional level of dependency among stroke patients and to find out

11
the association between the level of dependency after intervention of
FeSS protocol and the selected demographic variables.
METHODS AND MATERIALS: The present study was
conducted with 40 samples (patients) in quantitative approach, pre
experimental one group pre-test post-test design was used, samples were
selected by Non-probability convenient sampling technique. Pre-existing
level of dependency was assessed by using standardized tool (Barthel
Index) after the pre-test, short term FeSS protocol was implemented for
the first 72 hours following stroke unit admission, after 15 days post -test
was conducted by using the same tool.
RESULTS: The results show that in post-interventional level,
none of patients were having very severe level of dependency score,
22.5 % of patients were having severe level of dependency score, 60 %
of patients were having moderate level of dependency score, 17.5 % of
patients were having mild level of dependency score, and none of the
patients were having independent level of dependency score which is
significantly improved when compared to pre-intervention.
On an average, dependency score was improved from 8.50 to
12.15 after the administration of short term FeSS protocol. Statistical
significance was calculated by using student‟s paired „t‟test (t =12.22).
CONCLUSION: Nurses play a vital role in provding care to the
stroke patients who depend on others for their activities of daily living.
The present study confirmed that patients under FeSS protocol has
decreased level of dependency that promotes a positive stroke outcome.

12
INDEX
Chapter
No Title
Page
No
I INTRODUCTION 1
1.1 Background of the study 4
1.2 Need for the study 6
1.3 Statement of the problem 11
1.4 Objectives of the study 11
1.5 Operational Definition 11
1.6 Research Hypotheses 13
1.7 Assumption 13
1.8 De-Limitations 13
1.9 Conceptual framework 14
II REVIEW OF LITERATURE 19
III RESEARCH METHODOLOGY 35
3.1 Research Approach 35
3.2 Study Design 35
3.3 Duration of the Study 35
3.4 Study Setting 35
3.5 Study Population 36
3.6 Study Sample 36
3.7 Sample Size 36
3.8 Sample Criteria
3.8.1 Inclusion Criteria
3.8.2 Exclusion Criteria
36
3.9 Sampling Technique 37

13
Chapter
No Title
Page
No
3.10 Research Variables 37
3.11 Development and Description of Tools
3.11.1Development of Tools
3.11.2 Description of Tools
3.11.3 Scoring procedure
37
37
38
39
3.12 Content Validity 39
3.13 Reliability of Tool 39
3.14 Protection of Human Subjects 40
3.15 Pilot Study 40
3.16 Data Collection Procedure 40
3.17 Interventional Protocol 41
3.18 Data Entry and Analysis 41
IV ANALYSIS AND INTERPRETATION OF
DATA
44
V DISCUSSION 77
VI SUMMARY, IMPLICATION, LIMITATION,
RECOMMENDATION & CONCLUSION
85
6.1 Summary of the Study 85
6.2 Major findings of the Study 85
6.3 Implications of the Study 89
6.4 Limitations 92
6.5 Recommendations 92
6.6 Conclusion 93
REFERENCES
APPENDICES

14
LIST OF TABLES
Table
No Title
Page
No
3.1 Barthel index score interpretation 39
3.2 Intervention protocol 41
4.1 Distribution of demographic variables among stroke
patients.
46
4.2 Each question wise pre-interventional level of Barthel
index score among stroke patients
54
4.3 Each question wise pre-interventional percentage
Barthel index Score among stroke patients
55
4.4 Pre-interventional level of dependency score 56
4.5 Each question wise post-interventional level of Barthel
index score among stroke patients
58
4.6 Each question wise post-interventional percentage
Barthel index Score among stroke patients
59
4.7 Post- interventional level of dependency score 60
4.8 Comparison of overall dependency score before and
after short term FeSS protocol.
62
4.9 Each question wise pre-interventional and post-
interventional percentage of dependency score
64
4.10 Comparison of pre-interventional and post-
interventional level of dependency score
66
4.11 Effectiveness of short term FeSS protocol and
generalization of dependency score
68
4.12 Association between post-interventional level of
dependency score and patients’ demographic variables
69
4.13 Association between Barthel index gain score and
patients’ demographic variables
74
15
LIST OF FIGURES
Figure
No Description
1.1 Mortality rate based upon the type of stroke by 2025
1.2 Statistical rate of disability as estimated by Modified Rankins
Scale-degree
1.3 Rehabilitation Nursing Competence Model
1.4 Conceptual framework based on Weidnenbach‟s helping art
clinical nursing
3.1 Schematic representation of the Research Methodology
4.1 Cylindrical diagram shows distribution of sample age group
4.2 Pie diagram showing distribution of gender
4.3 Bar diagram shows distribution of sample according to
educational qualification.
4.4 Bar diagram shows distribution of sample according to their
occupation.
4.5 Cone diagram shows distribution of sample according to their
monthly income.
4.6 Doughnut diagram shows distribution of sample according to
their type of family.
4.7 Cylindrical diagram shows distribution of sample according to
their marital status.
4.8 Column diagram shows distribution of sample according to
language known.
4.9 Doughnut diagram shows distribution of sample according to
known case of diabetes mellitus.
4.10 Cylindrical diagram shows distribution of sample according to
the time from onset of symptoms.
4.11 Shows the pre-interventional level of dependency score among
stroke patients

16
Figure
No Description
4.12 Shows the post-interventional level of dependency score
among stroke patients.
4.13 Box plot compares pre-interventional and post-interventional
Barthel Index activities of daily living score among stroke
patients.
4.14 Multiple cylindrical diagrams show the pre-interventional and
post-interventional percentage of Barthel Index daily activity
score.
4.15 Multiple cylindrical diagrams show the pre-interventional and
post-interventional level of dependency score.
4.16 Multiple cylindrical diagrams show the association between
post-interventional level of dependency and their age.
4.17 Multiple cone diagrams shows the association between post -
interventional level of dependency and their gender.
4.18 Multiple cone diagrams show the association between post-
interventional level of dependency and their type of family.
4.19 Multiple bar diagrams show the association between stroke
patients post-interventional level of dependency score and
their diabetes status.

17
LIST OF APPENDICES
S. No Description
1. Certificate approval by Institutional Ethics Committee
2. Certificate of content validity by Experts
3. Letter seeking permission to conduct the study
4. Tool for data collection
Section A: Questionnaire regarding socio demographic
variable
Section B: FeSS Protocol that includes Fever protocol, Sugar
protocol, Swallow protocol.
Section C: Barthel Index used to assess the level of dependency
5. Informed consent form- English
6. Informed consent form- Tamil
7. Certificate of English Editing
8 Certificate of Tamil Editing
9. Certificate of Plagiarism
10. Photos
11. Handout

18
LIST OF ABBREVATION
ABBREVATION EXPANSION
RGGGH Rajiv Gandhi Government General Hospital
NS Non-Significance
P Significance
SD Standard Deviation
FeSS Fever, Sugar, Swallow
WHO World Health Organisation
CVA Cerebro Vascular Accident
ED Emergency Department
ICMR International Council of Medical Research
ADL Activities of Daily Living
QOL Quality of Life
UAS Unawareness Score
SLP Sleep Language Pathology
HRQOL Health Related Quality of Life
NIHSS National Institute of Health-Related Stroke
HR Hazard Ratio
CI Confidence Interval
DF Degree of Freedom
mRS Modified Ranking Scale
SES Socio-Economic Status
PAR Population Attributable Risk
QASC Quality in Acute Stroke Care
RCT Randomized Control Trail
US United States
SPSS Statistical Package for Social Science
ASU Acute Stroke Unit

1
CHAPTER-I
INTRODUCTION
“Start thinking wellness, not illness” -Kate Allatt
Stroke is the sudden death of some brain cells due to the lack of
oxygen when the blood flow to the brain is lost by blockage or rupture
of an artery to the brain. Due to certain changes in lifestyle of the
population, the cerebrovascular accident (CVA) is becoming commonly
increasing. According to the World Health Organization (2018) ,
cerebrovascular diseases have been the leading cause of death in the
world since the 1970s. Worldwide, in about, 33 million stroke survivors,
each year, 16.9 million, people suffer a first stroke and about 5.9 million
stroke related death make stroke the second or third most common cause
of death & one of the main causes of acquired disability among adult.
According to World Health Organization (WHO) stroke accounts
for about 10.8% mortality and 3.1% of disease burden worldwide.
Globally, 70% of strokes and 87% of both stroke-related deaths and
disability-adjusted life occurs in low- and middle-income countries.
Over the last four decades, the stroke incidence has declined by 42% in
high-income countries. Stroke mainly affect individuals who are at the
peak of their productive life. Despite its enormous impact on countries,
socio-economic development, this growing crisis has received very little
attention to date.
Developing countries like India are facing a double burden of
communicable and non-communicable diseases. Stroke is a silent killer
disease, yet it has not been given much emphasis in India as a public
health issue. Since 1990, there were totally 9.4 million deaths in India.
Out of these, 619,000 were due to stroke (73 per 100,000 population).
According to Jeyaraj Durai Pandian (2013), the India stroke factsheet

2
updated in 2012, the estimated age-adjusted prevalence rate for stroke
ranges between 84/100,000 and 262/100,000 in rural and between
334/100,000 and 424/100,000 in urban areas.
Commonly observed deficits after stroke are loss of motor control
on affected side, cognitive and perceptual dysfunction, speech and
communication problems and dependent in functional activities. CVA is
a serious public health problem in which the brain injury results in
temporary or permanent neurological deficits, of varied intensities.
Among the signs and symptoms observed after brain injury, hemiplegia
or hemiparesis stand out as the most common clinical sign of the
disease.
Despite the global decline in stroke mortality rates, the burden of
stroke (absolute numbers of people who have a stroke every year and
live with the consequences of stroke or die from their stroke) is
increasing, highlighting this, stroke is consider as the leading cause of
death and disability as a major public health issue. Populations now live
longer, with increased numbers of stroke survivors which may be due to
impressive advances in modern stroke medicine, such as introduction of
stroke care units, thrombolysis, and improved use of effective secondary
prevention therapies.
In order to improve the patient’s outcomes International clinical
guidelines, recommend early management of stroke on arrival to the
emergency department. There are certain key elements of stroke care applicable
to emergency department, which includes appropriate triage, treatment by
administration of tissue plasminogen activator (tPA) to eligible patients and
management of fever, hyperglycaemia and swallowing, followed by
prompt transfer to an acute stroke unit. Optimal management of these three
issues are pivotal for favourable patient outcome following stroke. All three
have been identified as priorities for inpatients stroke management.

3
In the early post stroke period, the elevation of both body
temperature and blood glucose is associated with significantly worsen
stroke outcomes, In the first days of an acute stroke, elevation of
temperature above 37.5°C occurs in one fifth to almost one-half of
patients and the detrimental effects of fever following stroke are
attributed to increased cerebral metabolic demands changes in the blood-
brain barrier permeability, acidosis, and an increased release of
excitatory amino acids which causes infarct expansion. There is also a
significant association between post stroke hyperglycaemia and poor
recovery. Up to 68% of all patients experience hyperglycaemia with the
first 24 hours of their acute stroke.
Hyperglycaemia following stroke has been shown to increase
infarct size and lead to poorer outcomes, independent of the patient’s
pre stroke history of diabetes. The incidence of dysphagia in the acute
post stroke period ranges from 37% to 78% and stroke patients with
dysphagia are three times more likely to develop pneumonia than those
without dysphagia.
In relation to the management of fever, hyperglycaemia and
swallowing in Australia, pre-trial data from the 2013 Stroke Foundation
National acute audit showed that only 60 % of patients received
temperature monitoring four times a day during the first 72 hours of
admission, with only 36 % of those with a fever (>37.5 °C) receiving
paracetamol within 1 hour. Less than a quarter (21 %) received four times
a day glucose monitoring in the first 72 hours of admission, and only 25 %
patients with hyperglycaemia (blood glucose >10 mmol/L) received insulin
within 1 hour. Two thirds (66 %) of patients received a swallowing screen
or assessment within 24 hours of admission, and of concern, only 52 %
received a swallow screen/assessment prior to oral intake.

4
Patients and their families are actively involved in their care and
receive consistent information and support. Stroke unit teams have
protocols for common problems and provide a training programme for
all team members. Quality in Acute Stroke Care (QASC) trial showed
that a multidisciplinary, nurse-initiated intervention focused on three
clinical protocols to manage fever, hyperglycaemia (Sugar)
and Swallowing dysfunction the FeSS protocols, in the first 72 hours of
patient following stroke unit admission which significantly decreased
death and disability.
Thus, optimal management of these three common physiological
disturbances, namely, fever, hyperglycaemia and dysphagia are
important elements of organized stroke care with potential to
significantly influence outcomes. All three have been identified in
international guidelines, as priority care issues for inpatient stroke
management. Changing clinician practice remains a challenge.
Successful translation of evidence into practice requires redress of
barriers that generally might include disagreement among experts about
best practice, attractiveness of alternative practices, inapplicability of
guidelines to certain patient subgroups, institutional inertia, vested
interests and ineffective continuing education. Production of up-to-date
evidence-based clinical guidelines without targeted implementation
strategies does not ensure practice change.
1.1 BACKGROUND OF THE STUDY
Among all the neurological disease of adult life, stroke is the one
that clearly ranks first in frequency and importance. In which, among
more than 7,00,000 people suffer from stroke each year an
approximately 2/3 of these individuals survive and require
rehabilitation. According to WHO the impact of stroke on an individual
or a population is best examined by classification of impairment,
activities and participation.

5
In 2013, stroke causes 1 of every 20 deaths in the United States.
In which on average, every 40 seconds someone affect stoke and
someone dies of approximately every 4 minutes. Approximately 10% of
all strokes occur in people 18 to 50 years of age. It also depends upon
the type of stroke in which ischemic stroke predicts to be higher in death
and dependency among stroke survivors by the year 2025.
Figure 1.1: Mortality rate based upon the type of stroke by 2025
There are well recognised gaps in the implementation of best clinical
practice in the acute stroke care. In the admission phase of acute stroke,
Hyperglycaemia, Fever and Swallowing dysfunction are poorly managed and
patient outcomes are compromised. Regarding fever 3/4th
of the patient’s
experience > 37.5 C within first few days following acute stroke attack which
leads to marked increase in morbidity & mortality. Regarding hyperglycaemia
up to 45% incidence in the first 48hours across all stroke subtypes that leads to
increased mortality & poorer functional outcome. Regarding swallowing 34.5
% failing dysphagia screening associated with poor outcome. Use of evidence-
based guidelines could improve care but have not been effectively
implemented.
Although organized stroke unit care significantly reduces death
and disability from cerebrovascular events, three physiological variables

6
are not yet universally well managed despite their importance for long-
term patient recovery. In the first days of an acute stroke, temperature
higher than 37.5°C occurs in 20–50% of patients, up to 50% become
hyperglycaemic and 37–78% have dysphagia all results in increased
morbidity and mortality. Hence, international guidelines recommend
that fever and high blood glucose concentrations be monitored and
managed proactively and that every stroke patient have their swallowing
status evaluated before receiving food, fluid, or oral medication .
1.2 NEED FOR THE STUDY
Demographic changes, urbanization and increased exposure to
major CVA risk factors will fuel the CVA burden in the future.
According to Sureshkumar Kamalakannan et al. (2017), in India, the
prevalence of stroke varies in different regions of the country and ranges
from 40 to 270 per 100000 population. Approximately 12% of all CVA
occur in the population <40 years of age. Major risk factors to CVA
identified in India are hypertension, hyperglycaemia, tobacco use and
low haemoglobin levels. CVA accounts for 2 percent of hospital
registrations, 1.5 percent of medical registrations and 9 to 30 percent of
neurological admissions in major hospitals.
The National Commission on Macroeconomics and Health , has
projected that cases of stroke would increase from 1,081,480 in 2000 to
1,667,372 in 2015. The ICMR study on Burden of Disease has estimated
that there has been an increase in the number of CVA cases in India
during the last one and a half decades by 17.5 %. Mortality due to CVA
has increased by 7.8%. The statistical rate of disability as estimated by
Modified Rankins Scale-degree among stroke survivor in India is shown
in the chart given below.

7
Figure 1.2: Statistical rate of disability as estimated by Modified
Rankins Scale degree
CVA holds the destination of being the leading cause of death in
India. Once a patient is medically stable, the focus of their recovery
shifts to rehabilitation. Some patients are transferred to in-patient
rehabilitation programs, while others may be referred to out-patient
services or home-based care. In-patient programs are usually facilitated
by an interdisciplinary team that may include a physician, nurse,
physical therapist, occupational therapist, speech and language
pathologist, psychologist and recreation therapist. The patient and their
family or caregivers also play an integral role on this team. The primary
goals of this sub-acute phase of recovery include preventing secondary
health complications, minimizing impairments and achieving functional
goals that promote independence in activities of daily living.
Correct perceptions and adequate knowledge of stroke as well as
good quality of acute stroke care have been touted as effective strategies
in improving stroke prevention and outcomes. They govern and enhance
the success of targeted interventions to control and prevent stroke and
its risk factors especially among populations at risk, through adopting
healthy lifestyles changes, improving treatment seeking behaviour and

8
adherence to medications to control medical risk factors. They also
reduce the delays in presenting to hospital in case of a stroke event. Set
protocols for acute stroke management enable early implementation of
treatment strategies to reverse abnormal physiological findings and
prevent complications
In brief, the protocols consisted of: monitoring and treatment of
temperatures > 37.5°C, treatment of major hyperglycaemia (finger prick
blood glucose levels >11 mmol/L for diabetics and >16 mmol/L for
nondiabetics) with saline initially or insulin, and nurses to undertake
swallowing screening using the Acute Dysphagia screening tool with
referral to a speech pathologist for full swallowing assessment only
when patients failed the screen. The protocols were intended to trigger
prompt nursing assessment and treatment of fever, hyperglycaemia, and
swallowing dysfunction in the first three days following admission to
hospital for stroke. A study has shown that the degree of care
dependency using the Barthel index after a stroke was higher compared
to before the stroke. However, the Barthel index contains 10 items that
are only based on physical characteristics.
Stroke is one of the principal reasons for dependency on nursing
care among adults, and the consequences result in continued care
dependency and also affects socioeconomic and cultural activities in
most patients. Care dependency in individuals is related to the fulfilment
of basic human needs such as physical, mental, emotional, cognitive,
social, economic, and environmental needs. Assessment o f the patient’s
degree of dependency is essential in determining nursing care needs,
planning nursing intervention, increase patient’s abilities, and creating
proper discharge plans. Moreover, assessing the degree of functional
limitation at admission will help nurses predict the functional outcome
after rehabilitation.

9
The Association of Rehabilitation Nurses proved a professional
Rehabilitation Nursing Competence model. The rehabilitation nursing
speciality is practiced in multiple settings across the post -care
continuum. This competency model is created to help guide, practice by
the nurses to promote rehabilitation nursing in the current health care
environment. This model developed by an evidenced based framework
to guide professional rehabilitation nursing practice. It is depicted by a
circle with role of nurse at the centre surrounded by the 4 domains and
various competencies. The broken lines illustrate the crossover of skills
& knowledge that are represented in each domain, representing a holistic
practice that rehabilitation nurses embrace.
This model is been used by the researcher in order to provide a
comprehensive care. Among those 4 domains, the researcher
incorporates the nurse-led intervention which aims to establish four sub-
categories such as
Implement Interventions based on best evidence.
Provide client & caregiver education.
Use supportive technology for improved QOL.
Deliver client & family-centered care.

10
Figure 1.3: Rehabilitation Nursing Competence Model
Thus, this model is utilized by the researcher in which, the nurse-
led interventions can be provided to the client collaboratively.
As a part of the researcher’s own clinical experience, she has been
posted in Neuro ward, there she met patients with acute onset of stroke
and they were dependent for their daily activities and more over their
dependency rate is been increased and may also lead to death after few
months to years. Nursing care was provided as per the need of the client,
but the researcher felt that there is a lack in nursing assessment at the
initial stage of stroke attack. While working on it she searched many of
the journals, articles and finally came across the study regarding FeSS
protocol which is been intervene by the nurses at acute onset of stroke
care. So, with her own interest she took this FeSS protocol as her main
study and worked on it in order to reduce the dependency rate among
stroke patients and to bring a positive stroke outcome.
11
1.3 STATEMENT OF THE PROBLEM
A study to assess the effectiveness of short term FeSS protocol on
level of dependency among stroke patients admitted in stroke ward,
Rajiv Gandhi Government General Hospital, Chennai-03.
1.4 OBJECTIVES OF THE STUDY
To assess the pre-interventional level of dependency among stroke
patients.
To determine the effectiveness of short term FeSS protocol (post-
interventional) on level of dependency among stroke patien ts.
To compare the pre-interventional and post-interventional level of
dependency among stroke patients.
To find out the association between the level of dependency after
intervention of FeSS protocol and the selected demographic
variables.
1.5 OPERATIONAL DEFINITIONS
Assess
It refers to the process of documents about the effectiveness of
FeSS protocol.
Effectiveness
It refers to the significant decrease in the level of dependency
among stroke patients.
Short Term FeSS Protocol
It refers to, the Fever, sugar, and swallow protocols were
implemented for the first 72 hours following stroke unit admission. In
brief:

12
The Fever protocol consists of monitoring the patient’s
temperature and the prompt treatment of a temperature 37.5°C or
greater in the first 72 hours, following stroke unit admission.
The Sugar protocol consists of monitoring the patient's blood
glucose levels for the first 72 hours following stroke unit
admission, and the prompt treatment of a blood glucose level
greater than 10mmols/L in the first 48 hours following stroke unit
admission.
The Swallow protocol consists of acute stroke dysphagia screen
tool to screen the patients for swallowing difficulties.
Dependency
It refers to a state of physiological reliance on someone to
perform their activities of daily living.
Level of dependency
It refers to ability of stroke patients in performing their ADLs.
Stroke
It refers to sudden death of brain cells due to lack of oxygen,
caused by blockage of blood flow or rupture of an artery to the brain.
Stroke Patients
It refers the patient with acute stroke estimated within 72 hours
onset
Stroke Ward
It refers to stroke unit which is organized in-hospital facility that
is devoted to care for patients with stroke.

13
1.6 RESEARCH HYPOTHESES
H1- There will be significant decrease in the level of dependency,
among stroke patient under FeSS protocol.
H2- There will be significant association between the level of
dependency and the selected demographic variables.
1.7 ASSUMPTIONS
The study assumes that
The stroke patients will usually depend on others to perform their
ADLs.
Intervention on FeSS protocol will enhance the stroke patients in
decreasing the level of dependency.
1.8 DE-LIMITATIONS
The study is limited to acute stroke patients.
The study is limited to 40 samples.
The study is limited up to 4 weeks of period.

14
1.9 CONCEPTUAL FRAMEWORK
BASED ON MODIFIED WEIDENBACH’S HELPING ART
CLINICAL NURSING THEORY
Conceptual framework is a theoretical approach to the study
problems that are scientifically based, which emphasizes the selection,
arrangement and classification of its concepts. It represents the
measurement on which purposes the proposed study is based.
The study is based on the concept of implementing FeSS protocol
that composed of (Fever, Sugar & Swallow protocol) among acute stroke
patients within 72 hours of stroke unit admission.
The conceptual framework used for the study was derived from
Weidnenbach’s helping art of clinical nursing theory (1964). According
to Weidnenbach’s nursing practice is an art in which the nursing action
is distinct kinds of actions. This theory views nursing as an art based on
a central purpose. This theory proposes that nursing practice has three
components such as
Identification
Ministration
Validation
This theory views nursing as an art based on a central purpose. It
consists of three factors: central purpose, prescription and realities.
Central purpose refers to the goal towards which the nurse strives. In
this study the main central purpose is to assess the effectiveness of FeSS
protocol on level of dependency among stroke patients.
The first component is to identify the demographic variables and
to assess the pre-interventional level of dependency. The researcher
observes the patient and identifies the need for help by selecting the

15
samples based on criteria for sample selection. She determines the time
of admission, the onset of symptoms and ascertains from patient’s
experience and it is evidenced through nurse-patient interaction. The
researcher notices the previous health history, whether known case of
diabetes mellitus or any other associated illness. The researcher also
assesses the level of dependency that includes their gait, speech,
swallowing ability and in performing their activities of daily living.
Finally, she validates with the patient that the health is needed.
The second component is ministration. The researcher meets the
need of the patient by ministering respective intervention.
Ministration of help needed; it has two components:
Prescription
The researcher acts by planning and implementing FeSS protocol
among acute stoke patients within 72 hours following stroke unit
admission. It composed of fever protocol – in which temperature in
monitored every 4th
hourly and treated, sugar protocol – it is done by
monitoring the patient blood glucose level every 6th
hourly and was
managed, and swallowing protocol – in which swallowing screening
done and was referred to speech pathologist. Finally, the planned
intervention is implemented to decrease the level of dependency among
stroke patient.
Realities
The realities of the situation are in which the nurse the nurse is to
provide care. It consists of all factors such as physical, physiological,
emotional and spiritual that is at play in a situation in which her action
occurs at any given moment.
16
According to Weidenbach’s she defines the five realities,
1) Agent
2) The recipient
3) Goal
4) Means
5) Framework
1. Agent
According to the theorist, the agent is the practicing nurse or the
delegates is characterized by personal attribute, capacitie s and mostly
competence in nursing
According to the researcher, this study shows that investigator is
the agent.
2. Recipient
Here the theorist, mention that the recipient is the patient or
client, which is characterized by personal attribute, problem, capacities,
aspirations and most important ability to cope with the concerns being
experienced.
In this study recipient are acute stroke patients admitted in stroke
ward.
3. Goal
The goals consist of desired outcome, the researcher or nurse
wishes to achieve. It results to be attained by nursing action.

17
4. Means
It comprises activated and device through which the practitioner
is enable to attain his/her goal. It includes skill, technique, procedure,
devices, etc.
FeSS protocol which comprises of fever protocol, sugar protocol
and swallow protocol. The researcher implements the FeSS protocol for
3 days among 40 patients.
5. Frameworks
It consists of the human environmental, professional and
organizational facilities that not only makeup the context within which
is practiced but also existing limits.
In this study, it refers to stroke ward, Rajiv Gandhi Government
General Hospital, Chennai-03.
The third component is validation. After help has been
implemented, the researcher validates that the action was indeed helpful.
Evidence must come from the patient from the purpose of the nursing
actions has been fulfilled. In validating the need for help, it was met.
The researcher validated the ministered help by comparing the pre-
interventional and post-interventional level of dependency and
associating with their selected demographic variables.

18
Central Purpose is to decrease the level of dependency among stroke patients.
Identification Validation Ministration
Demographic Variables
Age, gender, educational
qualification, occupation, monthly
income of the family, type of
family, marital status, languages
known, known case of diabetes
mellitus, time from onset of
symptoms admitted to stroke ward.
Pre-interventional assessment scale
Barthel Index is used to assess the
level of dependency in which it
about 10 activities, each carries 2
marks total 20 score.
Based upon the score obtained it is
categorized in to very severe,
severe, moderate, mild &
independent
Prescription
Implementation on
FeSS Protocol which
includes fever, sugar
& swallow protocol
within 72 hours
following stroke unit
admission to decrease
the level of
dependency among
acute stroke patients.
Along with that hand
out was issued in
imparting knowledge
regarding stroke
outcome.
REALITIES
Agent:
Investigator
Recipient: Acute
stroke patient on
admission to
stroke ward
Means: FeSS
Protocol
Framework:
Stroke ward,
Rajiv Gandhi
Government
General
Hospital,
Chennai-03
Post-interventional
level of dependency
using Barthel Index
Independent
Mild
Moderate
Severe
Very severe
Feed Back
Figure 1.1 Modified Conceptual Framework of Weidnenbach’s Helping Art of Clinical Nursing Theory

19
CHAPTER-II
REVIEW OF LITERATURE
Review of literature is a key in the research process. Review of
literature refers to an exhaustive, extensive and systematic examination
of publication relevant to the research project. Before any research can
be stated whether it is a single study or an extended project, a literature
review of previous studies and experiences related to the proposed
investigations should be done. One of the most satisfying aspects of the
literature review is the contribution it makes to the new knowledge,
insight and general scholarship of the researchers.
This section consists of four parts:
2.1. Studies related to stroke
2.2. Studies related to mortality and morbidity related to stroke
2.3. Studies related to causes of stroke
2.4. Studies related to FeSS Protocol
2.1 STUDIES RELATED TO STROKE
Gianluca Pucciarelli et al. (2019) investigated a growth mixture
longitudinal dyadic study on Quality of Life Trajectories among stroke
survivors and related changes in caregiver outcomes. The stroke
survivors (N=405, mean age=70.7y) included older adult men (52.0%),
most of whom (80.9%) had had ischemic strokes. The caregivers
(n=244, mean age=52.7y) included mostly women (65.2%), most of
whom were the survivors’ children (50.0%) or spouses (36.1%). The
longitudinal associations between the stroke survivor QOL trajectories
and the caregivers’ burden, anxiety, and depression were evaluated.
Three distinct survivor QOL trajectories were identified: high and

20
slightly improving QOL, moderate and slightly worsening QOL, and
markedly improving QOL.
Kusch M et al. (2019) conducted a study on reduced awareness
for apraxic deficits in left hemisphere stroke. The aim of the current
study was to characterize reduced awareness for apraxic as well as
aphasic deficits in patients suffering from LH stroke. After the
assessment of apraxia and aphasia, patients (n = 32) were asked to rate
their performance on a 1- to 5-point rating scale. An unawareness score
(UAS) was computed, resulting in negative scores for patients who
overestimated their performance in a given assessment, that is, exhibited
reduced awareness for their stroke-related deficits. Patients with apraxia
(n = 14) and aphasia (n = 16) significantly overestimated their
performance in the respective assessment. However, the level of
awareness was not generally related to the severity of apraxia, and there
were no group differences in other variables between patients with full
(n = 7) and reduced awareness (n = 7) for apraxic deficits.
Victoria Sherman et a. (2018) carried-out a study on screening
for dysphagia in adult patients with stroke, assessing the accuracy of
informal detection. They conducted a secondary analysis of data
captured between 2003 and 2008 from a sample of 250 adult stroke
survivors admitted to a tertiary care centre. Patient medical records were
reviewed for notation about dysphagia. To assess accuracy of notations
indicating dysphagia presence, they used speech language pathology
(SLP) assessments as the criterion reference. First notations of
swallowing by SLP were excluded. Of the remaining 170 patients, 147
(87%) had first notations (104 by nurses; 40 by physicians) within a
median of 24.3 h from admission Accuracy of detecting dysphagia from
informal notations was low, with a sensitivity of 36.7% [95% CI, 24.9,
50.1], but specificity was high (94.2% [95% CI, 86.5, 97.9]). Informal
identification methods, although timely, are suboptimal in their accuracy

21
to detect dysphagia and leave patients with stroke at risk for poor health
outcomes.
Maria van Mierlo et al. (2018) conducted a prospective cohort
study on Health-related quality of life after stroke to identify trajectories
of physical and psychosocial Health-related quality of life (HRQoL)
from two months to one-year post stroke and to determine the factors
that are associated with trajectory membership. 351 stroke patients were
followed up at 2, 6, and 12 months post stroke. Latent class growth
mixture modelling was used to determine trajectories of physical and
psychosocial HRQoL. Multinomial regression analyses were performed
to predict trajectory membership. As a result, four trajectories were
identified for both physical and psychosocial HRQoL: high, low,
recovery, and decline. Comparing the low and recovery trajectories, the
groups with low HRQoL were more likely to have higher scores for
neuroticism. Comparison of the decline and high trajectories yielded the
following predictors of physical HRQoL.
Gitta Rohweder et al. (2015) ruled-out a study on functional
outcome after common post-stroke complications occurring in the first
90 days. Patients with unselected acute stroke were included and
observed for 16 predefined complications during the first week. 50 %
(244 patients) were allocated to follow-up of 13 complications until 90
days and then assessed with the modified Rankin Scale. Ordinal logistic
regression (worsened outcome), as well as binary logistic regression for
severe dependency and death (modified Rankin Scale score>3) was
performed. Seven of the 13 complications occurred at a frequency ≥5%.
Recurrent stroke and chest infection were found to have an odds ratio
for worsened outcome of 7.45 (95% confidence interval, 2.83–20.96;
P<0.0001) and 3.28 (95% confidence interval, 1.16–9.29; P=0.025),
respectively. Active strategies for prevention and early treatment of the
first 2 complications seem advisable, patient monitoring as part of

22
comprehensive stroke unit care should ensure timely identification and
treatment of all complications.
2.2. STUDIES RELATED TO MORTALITY AND MORBIDITY
RELATED TO STROKE
Shamshirgaran SM Barzkar H et al. (2018) conducted a study on
Predictors of short-term mortality after acute stroke in East Azerbaijan
province, 2014. Study population were all patients with confirming the
diagnosis of the first-ever stroke who were hospitalized in two referral
teaching hospitals from October 2013 to March 2015. They were
followed up to 30 days after onset of stroke. Assessment
of stroke severity on admission using National Institute of
Health Stroke Scale (NIHSS), and information about risk factors and
socio-demographic factors were collected using face to face interview.
Data were analyzed using Cox proportional regression by STATA
software version 14. A total of 1036 consecutive patients with first-
ever stroke were included in this study. Of them, 228 patients (22%)
died within 30 days after stroke accordance. Advanced age was
significantly associated with a hazard for early mortality (HR=1.05 95%
CI 1.09-1.04), the inverse was true for education level, mortality
decreased as the education level increased; it was 25.7 percent among
illiterate and 14.3 among patients with higher education. Advanced
age, stroke subtype and high NIHSS score are the independent
predictors of early mortality in this study.
Tiantian Li et al. (2018) investigated a study on long-term
projections of temperature-related mortality risks for ischemic stroke,
haemorrhagic stroke, and acute ischemic heart disease under changing
climate in Beijing, China. The researcher utilized outputs from 31
downscaled climate models and two representative concentration
pathways (RCPs) for 2020s, 2050s and 2080s. This strategy was used to
estimate future net temperature along with heat and cold related deaths.

23
As a result, in 2080s, the net total number of annual tempera ture related
death exhibited a median value of 637 for ischemic stroke, 660 for
haemorrhagic stroke and 683 for ischemic heart disease. In 2080s, the
monthly death projection for haemorrhagic stroke and ischemic heart
disease showed that the largest absolute changes occurred in summer
and winter while changes for ischemic stroke occurred in summer.
Maria Schwarz et al. (2018) carried-out a retrospective cohort
study on the impact of aspiration pneumonia and nasogastric feeding on
clinical outcomes in stroke patients. To determine presence of clinical
complications related to dysphagia and to explore their operational
outcomes. A total of 110 patients presenting with an ischaemic stroke
were chart‐audited. Aspiration pneumonia post-stroke was found to be
associated with increased overall length of stay, poorer functional
outcomes post-stroke as well as being associated with a high risk of
mortality. The presence of a nasogastric tube was also assoc iated with
reduced functional outcomes post-stroke and risk of death is increased.
High prevalence and complications associated with stroke highlight the
complexity of providing nursing and allied health care to this patient
population.
Adel A Alhazzani et al. (2018), ruled-out a hospital-based follow-
up study to assess the in-hospital stroke case fatality rate, mortality rate
and explore the factors associated with in-hospital stroke mortality. First
time stroke patients admitted over one-year period were included in the
study. Data about personal characteristics, pre-stroke history, clinical
criteria, in-hospital complications and survival status were collected.
Hazard ratios (HR) and concomitant 95% confidence intervals were
computed using multivariate Cox regression survival analysis. A total of
121 in-hospital deaths out of 1249 first-time stroke patients giving on
overall case fatality rate of 9.7%. Overall, in-hospital stroke mortality
rate was 5.58 per 100,000/year. Males and elders showed a significantly

24
higher mortality rate. Multivariate Cox regression analyses revealed pre -
stroke smoking (HR=2.36), pre-stroke hypertension (HR=1.77), post-
stroke disturbed consciousness (HR=6.86), poor morbidity (HR=2.60)
and developing pulmonary embolism (HR-2.63) as significant predictors
of in-hospital strike mortality.
Karthik Mani et al. (2018) conducted a scoping review on
outcome measures used in stroke rehabilitation in India. The scoping
review framework proposed by Arksey & O’Malley in 2005 was used in
this review. Thirty-three studies identified 46 outcome measures. Most
of the outcome measures used in stroke rehabilitation research in India
was ordinal scales and body structure assessments. Reliability and
validity scores of the identified scales ranged from 0.37 – 1.00 to 0.65 –
0.96, respectively. Modified Rankin Scale and Barthel Index were the
most used outcome measures. Only two of the identified measures were
developed in India. There is a death of culturally sensitive stroke-related
outcome measures in India in all domains.
2.3 STUDIES RELATED TO CAUSES OF STROKE
Chin YY et al. (2018) investigated a study on Prevalence, risk
factors and secondary prevention of stroke recurrence in eight countries
from south, east and Southeast Asia: a scoping review. A comprehensive
search of academic journals (English) on this topic published from 2007
to 2017 was conducted. A total of 22 studies were selected from 585
studies screened from the electronic databases. First -
year stroke recurrence rates are in the range of 2.2% to 25.4%. Besides
that, modifiable risk factors are significantly associated with
pathophysiological factors (hypertension, ankle-brachial pressure index,
atherogenic dyslipidaemia, diabetes mellitus, metabolic syndrome, and
atrial fibrillation) and lifestyle factors (obesity, smoking, physical
inactivity, and high salt intake). Furthermore, age, previous history of
cerebrovascular events, and stroke subtype are also significant influence

25
risk factors for recurrence. To prevent recurrent stroke, health
intervention should be geared towards changing lifestyle to embody a
healthier approach to life.
Jeong SH et al. (2018) conducted a retrospective observational
study on enrolled consecutive cryptogenic stroke (CS) on patients who
underwent brain MRI and comprehensive cardiac evaluation. Severe
WMH was defined as Fazekas' score ≥3 and poor functional outcome as
modified Ranking Scale score ≥3 at 3 months. Long-term mortality
and causes of death were identified using national death certificates and
assessed by Kaplan-Meier method and regression analysis model.
Among 2732 patients with first-ever ischemic stroke, 599 (21.9%)
patients were classified as having CS. Severe WMH were found in 81
(34.5%) patients. After adjustments, severe WMH were an independent
predictor for poor functional outcomes at 3 months (OR 5.25, 95% CI,
2.07-13.31). Severe WMH were independently associated with short -
term functional outcomes in CS patients and independently associated
with long-term mortality in younger CS patients.
Elena Vicente et al. (2018) investigated a cross-sectional
observational study on frequency, risk factors, and prognosis of
dehydration in acute stroke the serum Urea/Creatinine ratio (U/C) was
calculated at admission and 3 days after the stroke. Dehydration was
defined as U/C>80. Patients were treated in accordance with the
standard local hydration protocol. Neurological severity was evaluated
at admission according to the NIHSS score; functional outcome was
assessed with the modified Rankin scale score (mRS) at discharge and 3
months after the stroke. 203 patients were evaluated, 78.8% presented an
ischemic stroke and 21.2% a haemorrhagic stroke. The mean age was
73.4 years ±12.9; 51.7% were men. Dehydration was detected in 18
patients (8.9%), nine patients at admission (4.5%), and nine patients
(4.5%) at 3 days after the stroke, female sex (p = 0.03) and older age

26
(p = 0.048) were associated with a higher risk of dehydration.
Dehydration was significantly associated with an unfavourable outcome
at discharge (p = 0.011), but the association was not significant at 3
months (p = 0.095).
Syed I. Khalid et al. (2017), carried-out a study on Identification
of reversible causes of minority inequity in stroke: severity related to
race and socio-economic status. The clinical and demographic data on
140 patients diagnosed with a stroke in the North Lawndale
neighbourhood of Chicago were collected prospectively over a 13-month
period and then were retrospectively analysed. Overall, haemorrhagic
stroke occurred in 31% of cases, when accounting for Socio-Economic
Status (SES), the incidence of haemorrhagic stroke in the uninsured
versus the privately or Medicaid-insured increased to 50%. Patients who
are uninsured minorities may be at an increased risk for severe strokes.
This increase in risk appears to be related to the increased incidence of
risk factors and lack of treatment.
Suresh kumar Kamalakannan et al. (2017) conducted a
population based cross-sectional studies and cohort studies on incidence
and prevalence of stroke in India. The stroke incidence rate or
cumulative stroke incidence and/or the prevalence of stroke in
participants from any age group were included. Electronic databases
(Ovid, PubMed, Medline, Embase and IndMED) were searched and
studies published during 1960 to 2015 were included. A total of 3079
independent titles were identified for screening, of which 10 population-
based cross-sectional studies were considered eligible for inclusion. The
cumulative incidence of stroke ranged from 105 to 152/100,000 persons
per year, and the crude prevalence of stroke ranged from 44.29 to
559/100,000 persons in different parts of the country during the past
decade. These values were higher than those of high-income countries.
Further investment in these studies would lead to better preventive

27
measures against stroke and better rehabilitation measures for stroke -
related disabilities in the country.
Dr.Martin et al. (2016) investigated a case-control study on
Global and regional effects of potentially modifiable risk factors
associated with acute stroke in 32 countries (INTERSTROKE). Controls
were hospital-based or community-based individuals with no history of
stroke, and were matched with cases. Odds ratios (OR) and their
population attributable risks (PARs) were calculated, with 99%
confidence intervals. Between Jan 11, 2007, and Aug 8, 2015, 26 ,919
participants were recruited from 32 countries (13,447 cases [10,388 with
ischaemic stroke and 3059 intracerebral haemorrhage] and 13 ,472
controls). Collectively, these risk factors accounted for 90·7% of the
PAR for all stroke worldwide. Hypertension was more associated with
intracerebral haemorrhage than with ischaemic stroke, whereas current
smoking, diabetes, apolipoproteins, and cardiac causes were more
associated with ischaemic stroke (p<0·0001).
B. Bonner et al. (2016) ruled-out a study on Factors predictive of
return to work after stroke in patients with mild−moderate disability in
India. Patients 18–60 years of age who were previously employed and
who had a first‐ever stroke 3 months to 2 years previously resulting in
mild to moderate disability (modified Rankin score ≤3) were recruited.
Socio‐demographic and clinical information was collected and anxiety,
depression and social support were assessed using previously validated
instruments. Of 141 patients (mean age ± SD 48 ± 8.8 years), 74
(52.5%) returned to work after stroke, younger age (OR 2.24, 95% CI
1.07–4.67) and a professional or business job (OR 3.02, 95% CI 1.44–
6.34) were significantly associated with successful return to work and
revealed that anxiety, depression and social support score did not affect
patients' decision to return to work (P = 0.17, 0.61 and 0.27,
respectively).

28
2.4 STUDIES RELATED TO FeSS PROTOCOL
Sandy Middleton et al. (2019) conducted a cluster randomized trial
on vital sign monitoring following stroke association with 90-day
independence a secondary analysis of the QASC. The Quality in Acute
Stroke Care Trial implemented nurse-initiated protocols to manage
fever, hyperglycaemia and swallowing (Fever, Sugar, Swallow clinical
protocols) achieving a 16% absolute improvement in death and dependency 90-
day post-stroke. 19 acute stroke units in New South Wales, Australia were
selected. Data from patients in the 10 intervention hospitals and the nine
control hospitals in the QASC trial post-intervention cohort was done. Of 1126
patients in the post-intervention cohort (intervention or control), 970 had both
in-hospital processes of care data and 90-day outcome data. Higher mean
temperature (P=<0.0001), finger-prick blood glucose reading ≥11/mmol/L
(P=0.0002) and when swallowing screening was performed within 24 hrs of
stroke unit admission P=0.0006).
Eric E. Smith et al. (2018) investigated a Systematic Review for
2018 Guidelines for the Early Management of Patients with Acute
Ischemic Stroke on effect of Dysphagia Screening Strategies on Clinical
Outcomes after Stroke. Dysphagia screening protocols have been
recommended to identify patients at risk for aspiration. The Medline,
Embase, and Cochrane databases were searched, to identify randomized
controlled trials (RCTs). Three RCTs were identified. Among the one
RCT found that a combined nursing quality improvement intervention
targeting fever and glucose management and dysphagia screening
reduced death and dependency. Another RCT failed to find evidence that
pneumonia rates were reduced by adding the cough reflex to routine
dysphagia screening. A smaller RCT randomly assigned two hospital
wards and found the patients on the stroke care pathway were less likely
to require intubation and mechanical ventilation

29
Alexandrov et al. (2018) carried-out an observational pilot study
to assess compliance with American guidelines for glucose and
temperature control and association with discharge outcomes in
consecutive acute stroke patients admitted to 5 US comprehensive stroke
centers. Data for the first 5 days of stroke admission were collected
from electronic medical records and entered and analyzed in SPSS using
descriptive statistics, Mann-Whitney U test, I test, and logistic
regression. A total of 1669 consecutive glucose and 3782 consecutive
temperature measurements were taken from a sample of 235 acute
stroke patients; the sample was 87% ischemic and 13% intracerebral
hemorrhage. Poor glucose control was found in 33% of patients, Poor
temperature control was noted in 10%, and 39% did not have
temperature recorded. National Institutes of Health Stroke Scale score
and well-controlled glucose were independent predictors of favorable
outcome in reperfusion patients, Nurses are well positioned to assume
leadership of glucose and temperature monitoring and treatment.
Anastasia Skafida et al. (2018) investigated a study on In-
hospital dynamics of glucose, blood pressure and temperature predict
outcome in patients with acute ischemic stroke. Serial measurements
were performed in the first seven days post-stroke and different
parameters have been estimated. Cox-proportional-hazards-model
analysis and logistic-regression analysis were applied to investigate the
association between these parameters and all-cause mortality and
functional outcome. In 1271 patients (mean age 72.3±11.2 years), after
adjusting for confounders, baseline glucose levels (p=0.017), variability
of systolic BP (SBP) as estimated by standard deviation (p=0.005), the
baseline temperature (p<0.001) were independently associated with all -
cause mortality within three months. Poor functional outcome was
associated with subject-specific baseline values of temperature
(p=0.024), the rate of SBP (p=0.004) and temperature change (p=0.018).

30
Neha Raj et al. (2018) investigated a cluster-randomized study on
development and implementation of acute stroke care pathway in a
tertiary care hospital in India. In-hospital care of stroke patients can
reduce the risk of death and disability. There is an emerging evidence
for the routine use of care pathways (CPs) for acute stroke management.
A total of 162 acute stroke patients, who were managed within 72 hours
of onset of their symptoms, were enrolled prospectively in two groups-
the stroke care pathway (CP) arm (n = 77) and the conventional care
(CC) arm (n = 85). The CP arm had a lower incidence of aspiration
pneumonia (AP) in comparison with the CC arm (6.5% vs. 15.3%, risk
ratio [RR] = 0.42, 95% confidence interval [CI] = 0.16-1.14, P = 0.062).
The CP group had a decreased risk of requirement of mechanical
ventilation (7.8% vs. 17.6%, odds ratio [OR] = 0.39, 95% CI = 0.14 -
1.07, P = 0.05).
Napon Cristian et al. (2018) conducted a prospective, cross-
sectional study on factors Associated with the Occurrence of Medical
Complications in the Acute Phase of Stroke in a Reference Hospital.
Patients admitted to hospital for stroke less than 72 hours from March
2015 to February 2016 were analyzed. A bivariate and then multivariate
analysis with logistic regression was made. The independent factors
associated with the occurrence of medical complications were, Clinical
severity of stroke (NIHSS ≥17) at admission (OR = 3.402, 95% CI 1.27-
16.46, p = 0.031); swallowing disorders at admission (OR = 10.19, 95%
CI 1.16-89.00, p = 0.000) and co-morbidities (OR = 8.72; 95% CI 1.23-
61.43, p = 0.030). The screening and appropriate management of
patients at high risk of medical complications in the acute phase of
stroke will reduce the incidence of these complications and help reduce
mortality and disability post stroke.
Sandy Middleton et al. (2017) ruled-out a Cross-Sectional Survey
following the QASC trial international uptake of a proven intervention

31
to reduce death and dependency in acute stroke to identify: (a) the
clinical discipline of healthcare professionals who downloaded the
QASC resources; (b) the purpose for downloading; (c) successful
implementation of any or all the FeSS protocols; (d) barriers to
implementation; and (e) associations with self-reported successful
implementation. Online survey of those who downloaded the QASC
resources between October 2011 and August 2013 were analysed. One-
hundred and fifty-nine people from 21 countries participated. Nurses
were the largest group to download the resources (n = 54, 38%), with
the primary purpose to inform clinical practice (n = 97, 64%). Less than
half (n = 77, 48%) downloaded, and less than a quarter (n = 38, 24%)
attempted to implement all three protocols. Of those personally involved
in implementation (n = 50) half reported doing so successfully for one
or more protocols (n =27, 54%) with 10 (20%) reporting successful
implementation of all three protocols. Higher autonomy was associated
with greater likelihood of implementation of all three protocols (p =
.038).
Kelly Coughlan et al. (2017) conducted a study on mortality
reduction for fever, hyperglycaemia, and swallowing nurse-initiated
stroke intervention QASC trial follow-up. Mortality was ascertained
using Australia’s National Death Index. Cox proportional hazards
regression compared time to death adjusting for correlation within
stroke units using the cluster sandwich method. One thousand and
seventy-six participants (intervention n=600; control n=476) were
followed for a median of 4.1 years, of whom 264 (24.5%) had died. The
QASC intervention group had improved long-term survival (>20%), but
this was only statistically significant in adjusted analyses (unadjuste d
hazard ratio [HR], 0.79; 95% confidence interval [CI], 0.58–1.07;
P=0.13; adjusted HR, 0.77; 95% CI, 0.59–0.99; P=0.045). Older age
(75–84 years; HR, 4.9; 95% CI, 2.8–8.7; P<0.001) and increasing stroke

32
severity (HR, 1.5; 95% CI, 1.3–1.9; P<0.001) were associated with
increased mortality. Results demonstrate the potential long-term and
sustained benefit of nurse-initiated multidisciplinary protocols for
management of fever, hyperglycaemia, and swallowing dysfunction.
These protocols should be a routine part of acute stroke care.
Dominique A Cadilhac et al. (2017) carried-out a Before and
after controlled design study on Improving quality and outcomes of
stroke care in hospitals: Protocol and statistical analysis plan for the
Stroke123 implementation study to determine whether an organizational
intervention can improve the quality of stroke care over usual care. To
detect an absolute 10% difference in overall performance, a minimum of
21 hospitals and 843 patients per group was determined. Primary
outcome: net change in composite score (i.e. total number of process
indicators achieved divided by the sum of eligible indicators for each
cohort). Secondary outcomes: change in individual indicators, change in
composite score comparing hospitals that did or did not develop action
plans (per-protocol analysis), impact on 90–180-day health outcomes.
Sensitivity analyses: hospital self-rated status, alternate cross-sectional
audit data (Stroke Foundation).
Anna Lydtin et al. (2016) conducted a prospective pre-
interventional/post-interventional study to embed an evidence-based
intervention to manage fever, hyperglycaemia (Sugar) and Swallowing
(the FeSS protocols) in stroke, previously demonstrated in the Quality in
Acute Stroke Care (QASC) trial to decrease 90-day death and
dependency, into all stroke services, 36 NSW stroke services. Clinical
champions attended a 1-day multidisciplinary training workshop and
received standardized educational resources and ongoing support. Using
the National Stroke Foundation audit collection tool and processes,
patient data from retrospective medical record self -reported audits for
40 consecutive patients with stroke per site pre-QASCIP were compared

33
with prospective self-reported data from 40 consecutive patients with
stroke per site post-QASCIP. Primary outcome measures: Proportion of
patients receiving care according to the FeSS protocols pre-QASCIP to
post-QASCIP. All 36 (100%) Pre-QASCIP to post-QASCIP, proportions
of patients receiving the 3 targeted clinical behaviours increased
significantly: management of fever (pre: 69%; post: 78%; p=0.003),
hyperglycaemia (pre: 23%; post: 34%; p=0.0085) and swallowing (pre:
42%; post: 51%; p=0.033).
Simeon Dale et al. (2015) revealed a Mixed Methods study on
barriers and enablers to implementing clinical treatment protocols for
fever, hyperglycaemia, and swallowing dysfunction in the quality in
acute stroke care. Pre-implementation: Workshops were held at the
intervention stroke units (n = 10). A total of 111 clinicians attended the
pre-implementation workshops, identifying 22 barriers covering four
main themes: (a) need for new policies, (b) limited workforce
(capacity), (c) lack of equipment, and (d) education and logistics of
training staff. Post-implementation, only five of the 22 barriers
identified pre-implementation were reported as actual barriers to
adoption of the FeSS protocols. As only five of the 22 barriers identified
pre-implementation were reported to be actual barriers at completion of
the trial, this suggests that barriers are often overcome whilst some are
only ever perceived rather than actual barriers.
Hilaire J. Thompson, (2015) conducted a study on Evidence-Base
for Fever Interventions Following Stroke. A comprehensive review of
the literature was conducted. The monitoring of body temperature is
considered a standard of care for stroke patients. The AHA/American
Stroke Association (ASA) guidelines specify frequency of monitoring to
be not less than every 30 minutes while in the emergency department
and every 4 hours (or as required) in the acute care setting. Fever is seen
in between 40% and 60% of patients after stroke. The most common

34
first line intervention in these protocols was acetaminophen at a dose of
650 mg. Other first-line interventions common to these protocols were
physical cooling measures, such as ice packs and fans. Use of an
indwelling catheter for temperature control has also been used to
manage fever in persons after stroke, but these systems are not viewed
as first-line therapies for management.
Sandy Middleton et al. (2014) investigated a cluster randomized
controlled trial on Implementation of evidence-based treatment
protocols to manage fever, hyperglycaemia, and swallowing dysfunction
in acute stroke (QASC). Intervention ASUs received treatment protocols
to manage fever, hyperglycaemia, and swallowing dysfunction with
multidisciplinary team building workshops to address implementation
barriers. Pre-intervention and post-intervention patient cohorts to
compare 90-day death or dependency (modified Rankin scale [mRS]
≥2), functional dependency (Barthel index), and SF-36 physical and
mental component summary scores.) 19 ASUs were randomly assigned
to intervention (n=10) or control (n=9). Of 6564 assessed for eligibility,
1696 patient’s data were obtained. Results showed that, irrespective of
stroke severity, intervention ASU patients were significantly less likely
to be dead or dependent at 90 days than control ASU patients (236
[42%] of 558 patients in the intervention group vs 259 [58%] of 449 in
the control group, p=0.002; number needed to treat 6.4, adjusted
absolute difference 15.7%.

35
CHAPTER – III
METHODOLOGY
This chapter deals with the methodology to assess the
effectiveness of short term FeSS protocol on level of dependency among
stroke patients admitted in stroke ward, Rajiv Gandhi Government
General Hospital, Chennai-03.
3.1 RESEARCH APPROACH
Quantitative research approach
3.2 STUDY DESIGN
Pre experimental one group pretest posttest design
The research design adopted for the study was pre experimental
(one group pretest posttest) with manipulation and no randomization and
no control group.
E O 1 X O2
KEY
E – Pre experimental group
O1 – Pre assessment (pre-intervention)
X – Nursing intervention (FeSS protocol)
O2 – Post assessment (post-intervention)
3.3 DURATION OF THE STUDY
4 weeks
3.4 STUDY SETTING
The study was conducted at Rajiv Gandhi Government General
Hospital, Chennai-03. It is a hospital with 3,000 beds is funded and
managed by the state government of Tamil Nadu. As of 2018, the

36
hospital receives an average of 12,000 outpatients every day. It is a
multispecialty hospital that renders its specialization in providing
comprehensive care in all specialties such as general medicine, general
surgery, cardiology, neurology, rheumatology, nephrology, orthopedics,
etc. The rationale for selecting this area is feasibility and availability of
adequate samples.
3.5 STUDY POPULATION
Target population: Acute stroke patients admitted in stroke ward,
Rajiv Gandhi Government General Hospital, Chennai-03.
Accessible population: The patients available during the study
time in stroke ward, Rajiv Gandhi Government General Hospital,
Chennai-03.
3.6 STUDY SAMPLE
The sample comprise of acute stroke patients admitted in stoke
ward within 72 hours..
3.7 SAMPLE SIZE
40 patients who met with the inclusion criteria
3.8 SAMPLE CRITERIA
3.8.1 Inclusion Criteria
Patient with acute stroke.
Age limit above 35 years of age.
Patient who understand Tamil & English.
Patient on admission to stroke ward.
37
3.8.2 Exclusion Criteria
Patient with balance disability.
Old stroke.
Severe aphasia.
Sensory disorder.
Severe cognitive impairment.
Patients who are not willing to participate.
3.9 SAMPLING TECHNIQUE
Sampling procedure is non-probability convenient sampling
technique.
3.10 RESEARCH VARIABLES
Independent Variable
Short term FeSS protocol that includes fever protocol, sugar
protocol and swallowing protocol.
Dependent Variable
Level of Dependency among stroke patients.
3.11 DEVELOPMENT AND DESCRIPTION OF TOOLS
3.11.1 Development of Tools
Standardized tool was used after in-depth review of literature;
obtain opinion and content validity from medical, nursing and statistical
experts. Construction and pretesting of tool was done during pilot study
direct assessment of patients was performed during data collection.
38
3.11.2 Discription of Tools
Section-A
Comprises a demographic variable of the patients which includes
age, gender, educational qualification, occupation, monthly income, type
of family, marital status, languages known, known case of diabetes
mellitus and time from onset of symptoms.
Section-B
Comprises of FeSS protocol that includes fever, sugar and
swallow protocol which were implemented for the first 72 hours
following stroke unit admission. In brief:
The Fever protocol consists of monitoring the patients
temperature and the prompt treatment of a temperature 37.5°C or
greater in the first 72 hours, following stroke unit admission.
The Sugar protocol consists of monitoring the patient's blood
glucose levels for the first 72 hours following stroke unit
admission, and the prompt treatment of a blood glucose level
greater than 178 mm/hg in the first 48 hours following stroke unit
admission.
The Swallow protocol consists of acute stroke dysphagia screen
tool to screen the patients for swallowing difficulties.
Section-C
Comprises of Barthel index, it is used to assess the level of
dependency in pretest and posttest among stroke patients it consists of
10 activities such as bowel, bladder, toilet use, feeding, transfer,
mobility, dressing, stairs, bathing with a total score 20.

39
3.11.3 SCORING PROCEDURE
Section-A: The demographic variables were coded to assess there
and thereby to subject it for statistical analysis.
Section-C: The standardized Barthel index tool consists of 10
activities with minimum mark 0, maximum mark 3, total score 20.
Table 3.1: Barthel Index score interpretation
Level of dependency Score
Very severe 0-4
Severe 5-9
Moderate 10-14
Mild 15-19
Independent 20
3.12 CONTENT VALIDITY
Content validity of the tool was obtained from medical and
nursing experts in the field of medical surgical nursing. They suggested
certain modification in the tool. The expert’s suggestions were
incorporated in the tool. Then the tool was finalized and used for the
main study.
3.13 RELIABILITY OF THE TOOL
Reliability of the tool was determined by test retest method. There
was a significant co-relation between the test and retest score according
to Karl Pearson’s correlation coefficient the value is 0.08 this score
indicates high co relation. Hence the tool was found to be reliable to
conduct the main study.

40
3.14 PROTECTION OF HUMAN SUBJECTS
Obtained approval from the Institutional Ethics Committee,
Madras Medical College, Director of Institute of Neurology, Rajiv
Gandhi Government General Hospital, Chennai and all respondents were
carefully informed about the purpose of the study. The students were
explained about the purpose and need of the study. They were assured
and their details and answers will be used only for research purpose and
kept confidentially. Written permission was obtained from the
participants before conducting the study.
3.15 PILOT STUDY
In order to test the feasibility, relevance of the study, a pilot study
was conducted with 10 patients. Convenient sampling technique was
used. Before and after FeSS Protocol pre and post test was conducted,
those data were analyzed to find out suitability of study. The results of
the pilot study showed that there was a positive correlation between the
level of dependency among stroke patients under FeSS protocol and the
investigator found that study was feasible.
3.16 DATA COLLECTION PROCEDURE
The study was conducted in Stroke ward, Rajiv Gandhi
Government General Hospital, Chennai-03, after obtaining permission
from the Director of Institute of Neurology. Before the data collection,
the researcher introduced herself, explained the purpose of the study to
the patients regarding short term FeSS protocol. The confidentially was
assured and consent was obtained from the participants then the patients
were interviewed and pretest was conducted. Four samples per day were
selected and assured that at any time they can withdraw from the study.
The period of study extended for four weeks; the data was collected
from Monday to Saturday between to 8am to 4pm. Using convenient

41
sampling technique 40 samples were collected who fulfilled their
selection criteria.
Pretest was conducted on the day of admission to assess the level
of dependency using Barthel index for 15 minutes; then the short term
FeSS protocol was implemented on the same day for the first 72 hours
following stroke unit admission. The patients were very cooperative and
was interested to know more about their condition. Health education was
given by issuing handouts regarding positive stroke outcomes and their
follow up.
After fifteen days of interval the post test was conducted to the
same sample for about 15-20 minutes to assess decreased level of
dependency, and evaluates the effectiveness of short term FeSS
protocol.
Table-3.2: Intervention Protocol
Place Rajiv Gandhi Government General Hospital,
Chennai-03
Intervention Short term FeSS protocol
Duration First 72 hours following stroke unit admission
Time 8am-4pm
Recipient Acute stroke patients
Administered by The investigator
3.17 DATA ENTRY AND ANALYSIS
Demographic variables in categories were given in frequencies
with their percentages.
Dependency score were given in mean and standard deviation.
Quantitative dependency score in pretest and post-interventional
were compared using student’s paired t-test.

42
Association between level of dependency score with demographic
variables are assessed using one-way ANOVA F-test and t-test.
Diagram, with regression estimate were used to represent the data.

43
FIGURE 3.1: SCHEMATIC REPRESENTATION OF
THE RESEARCH METHODOLOGY
Research Design Pre experimental one group pre-interventional and post-
interventional design
Study Setting
Stroke ward, Rajiv Gandhi Government General Hospital, Chennai-03
Target Population
Acute stroke patients
Sampling Technique
Convenient sampling technique
Sample Size
40 samples
Description of the Instrument
Standardized tool- Barthel index
Data Analysis
Descriptive and inferential statistics
Findings and Conclusion

44
CHAPTER – IV
DATA ANALYSIS AND INTERPRETATION
This chapter presents the analysis and interpretation of data
collected from 40 subjects under short term FeSS protocol to assess the
level of dependency among stroke patients using Barthel index. The data
was analyzed according to the objectives and hypothesis formulated for
purpose of the study using descriptive and inferential statistics.
Analysis is the process of organizing and synthesizing the data in
such a way that research questions can be answered and hypotheses
tested. The purpose of analysis is to reduce the data into an intelligible
and interpretable form, so that the relation of research problem can be
studied and tested.
ORGANIZATION OF DATA
Section-A: Description of frequency and percentage distribution
of demographic variables.
Section-B: Assessment of pre-interventional level of dependency
among stroke patients.
Section-C: Assessment of post-interventional level of dependency
among stroke patients.
Section-D: Comparison of pre-interventional and post-
interventional level of dependency among stroke patients and the
effectiveness of short term FeSS protocol.
Section-E: Association between the post-interventional level of
dependency among stroke patients with their selected demographic
variables

45
STATISTICAL ANALYSIS
Demographic variables in categories were given in frequencies
with their percentages.
Dependency score were given in mean and standard deviation.
Association between demographic variables and Dependency
score were analysed using Pearson chi-square test
Quantitative Dependency score in pre-interventional and post-
interventional were compared using student’s paired t-test.
Qualitative level of Dependency scores in pre-interventional and
post-interventional were compared using Stuart-Maxwell test
/extended McNemar test
Differences and generalization of Barthel Index gain score
between pre-interventional and post-interventional score was
calculated using and mean difference with 95% CI and
proportion with 95% CI.
Simple bar diagram, Pie diagram, Multiple bar diagram and Box
plot were used to represent the data.
P<0.05 was considered statistically significant. All statistical test
is two tailed tests.

46
SECTION-A: DESCRIPTION OF DEMOGRAPHIC
VARIABLES OF STUDY PARTICIPANTS.
Table 4.1: Distribution of demographic variables of stroke patients.
Demographic variables No. of
patients %
Age 35-45 years
46-55 years
Above 56 years
13
12
15
32.50%
30.00%
37.50%
Gender Male
Female
31
9
77.50%
22.50%
Educational
Qualification
Professionals 0 0.00%
Graduate or postgraduate 3 7.50%
Intermediate or post-high
school diploma 2 5.00%
High school certificate 10 25.00%
Middle school certificate 8 20.00%
Primary school certificate 10 25.00%
Illiterate 723 17.50%
Occupation Legislators, senior officials &
managers
0 0.00%
Professionals 0 0.00%
Technicians and associate
professionals
2 5.00%
Clerks 2 5.00%
Skilled workers, shop &
market scale workers
3 7.50%
Skilled agricultural & fishery
worker
3 7.50%
Craft & related trade workers 5 12.50%
Plant & machine operators &
assemblers
5 12.50%
Elementary occupation 13 32.50%
Unemployed 7 17.50

47
Demographic variables No. of
patients %
Monthly
income of the
family
Below 5,000
5,001-10,000
10,001-15,000
15,001-20,000
Above 20,000
24
10
6
0
0
60.00%
25.00%
15.00%
0.00%
0.00%
Type of
family
Joint family
Nuclear family
Extended family
23
14
3
57.50%
35.00%
7.50%
Marital status Married
Unmarried
Widow / Widower
Separated
33
2
3
2
82.50%
5.00%
7.50%
5.00%
Languages
known
Tamil
English
Both
Other language
35
0
5
0
87.50%
0.00%
12.50%
0.00%
Known case
of diabetes
mellitus
Yes
No 12
28
30.00%
70.00%
Time from
onset of
symptoms
admitted to
stroke ward
Within 4 hrs
Within 6 hrs
Within 12 hrs
After 12 hrs
8
26
5
1
20.00%
65.00%
12.50%
2.50%
Table 4.1: shows the demographic information of patients those
who were participated in this study.
Data presented in table 1 shows the following:
Regarding their Age, Maximum 37.50% of the patients belong to age
group of 35-45 years, 32.50% of the patients belong to age group of 46 – 55
years and 30.00% of the patients belong to age group of above 56 years.
Among Gender distribution, 77% of the patients were male and
23% of patients were female.

48
Regarding Educational qualification, 7.50% of the patients were
graduate or postgraduate, 5% of patients were intermediate, 25% of
patients were with high school certificate, 20% of patients were with
middle school certificate, 25% of patients were with primary school
certificate and 17.50% of patients were illiterate.
Inspite of Occupation: 5% of the patients were technicians and
associate professionals, 5% of patients were clerks, 7.50% of patients
were skilled workers, 7.50% of patients were skilled agricultural &
fishery worker, 12.50% of patients were craft & related trade workers,
32.50% of patients were elementary occupation and 17.50% of patients
were unemployed.
In related to Monthly income, 60% of patients have monthly
income of about (<5,000), 25% of patients have monthly income of
about (5,000 – 10,000) and 15% of patients have monthly income of
about (10,000 – 15,000).
Among the Type of family: 57% of the patients were joint family, 35%
of patients were nuclear family, and 8% of patients were extended family.
Regarding Marital status: 82.50% of patients were married, 5%
of patients were unmarried, 7.50% of patients were widow/widower, and
5% of patients were separated.
Based on Languages known, 87.50% of patients know Tamil and
12.50% of patients know both Tamil & English.
In related to Known case of diabetes mellitus, 70% of patients
says Yes and 30% of patients says No.
Regarding Time from onset of symptoms admitted to stroke ward,
20% of patients were within 4hrs, 65% of patients were within 6hrs, 12.5% of
patients were within 12hrs and 2.50% of patients were after12hrs.

49
Figure 4.1: Cylindrical diagram shows distribution of sample age
group
Figure 4.2: Pie diagram showing distribution of sample gender.

50
Figure 4.3: Bar diagram shows distribution of sample according to
educational qualification.
Figure 4.4: Bar diagram shows distribution of sample according to
their occupation.

51
Figure 4.5: Cone diagram shows distribution of sample according to
their monthly income.
Figure 4.6: Doughnut diagram shows distribution of sample according
to their type of family.

52
Figure 4.7: Cylindrical diagram shows distribution of sample
according to their marital status.
Figure 4.8: Column diagram shows distribution of sample according to
language known.

53
Figure 4.9: Doughnut diagram shows distribution of sample according
to known case of diabetes mellitus.
Figure 4.10: Cylindrical diagram shows distribution of sample
according to the time from onset of symptoms admitted to stroke ward
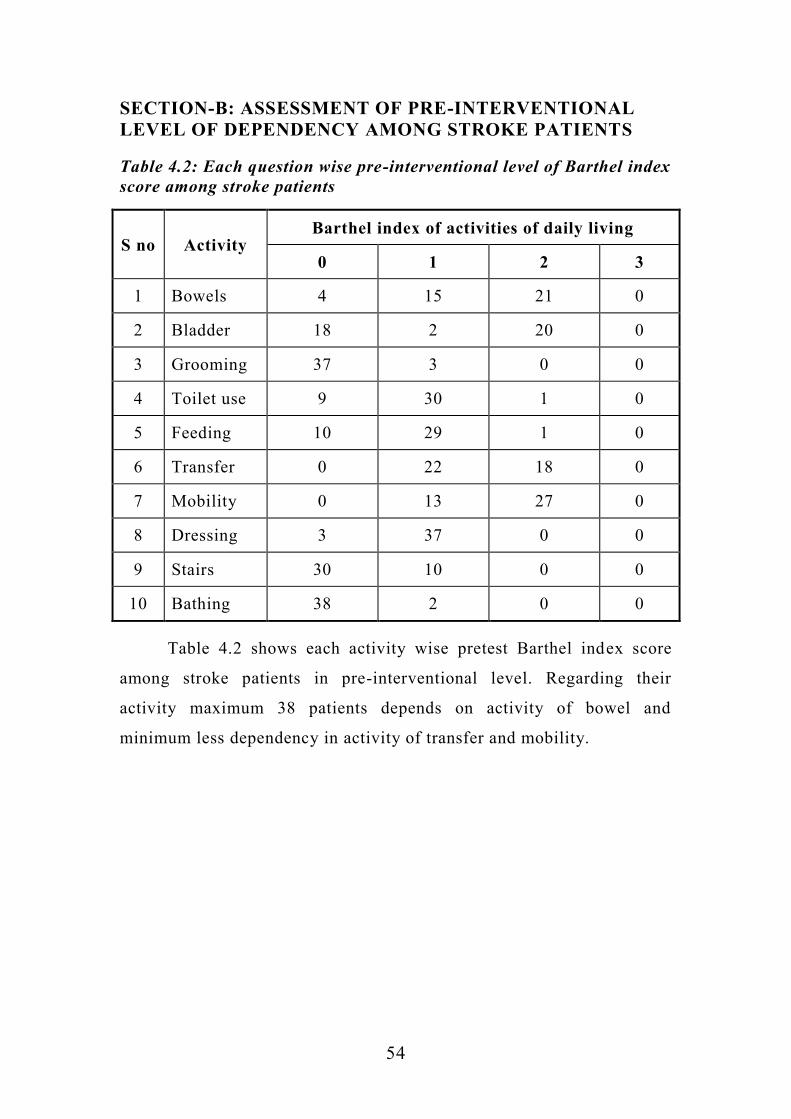
54
SECTION-B: ASSESSMENT OF PRE-INTERVENTIONAL
LEVEL OF DEPENDENCY AMONG STROKE PATIENTS
Table 4.2: Each question wise pre-interventional level of Barthel index
score among stroke patients
S no Activity Barthel index of activities of daily living
0 1 2 3
1 Bowels 4 15 21 0
2 Bladder 18 2 20 0
3 Grooming 37 3 0 0
4 Toilet use 9 30 1 0
5 Feeding 10 29 1 0
6 Transfer 0 22 18 0
7 Mobility 0 13 27 0
8 Dressing 3 37 0 0
9 Stairs 30 10 0 0
10 Bathing 38 2 0 0
Table 4.2 shows each activity wise pretest Barthel index score
among stroke patients in pre-interventional level. Regarding their
activity maximum 38 patients depends on activity of bowel and
minimum less dependency in activity of transfer and mobility.

55
Table 4.3: Each question wise pre-interventional percentage Barthel
index Score among stroke patients
S
No Activities Maximum Score Mean Sd
% mean
score
1 Bowels 2 1.42 0.68 71.00%
2 Bladder 2 1.05 0.99 52.50%
3 Grooming 1 0.08 0.27 8.00%
4 Toilet use 2 0.80 0.46 40.00%
5 Feeding 2 0.78 0.48 39.00%
6 Transfer 3 1.45 0.50 48.33%
7 Mobility 3 1.70 0.52 56.67%
8 Dressing 2 0.92 0.27 46.00%
9 Stairs 2 0.25 0.44 12.50%
10 Bathing 1 0.05 0.22 5.00%
Total 20 8.50 2.71 42.50%
Table 4.3 shows each activity wise pretest Barthel index score
among stroke patients. Regarding activity of bowels there are (71%)
maximum where as in activity of bathing there are (5%) minimum.
Overall activity percentage of score is 42.50%.

56
Table 4.4: Pre-interventional level of dependency score
Level of Dependency No. of Patients %
Very severe 4 10.00%
Severe 20 50.00%
Moderate 14 35.00%
Mild 2 5.00%
Independent 0 0.00%
Total 40 100.00%
Table 4.4: Shows 10 % of patients were having very severe level
of dependency score, 50 % of patients were having severe level of
dependency score, 35 % of patients were having moderate level of
dependency score, 5 % of patients were having mild level of dependency
score, none of the patients were independent level of dependency score.
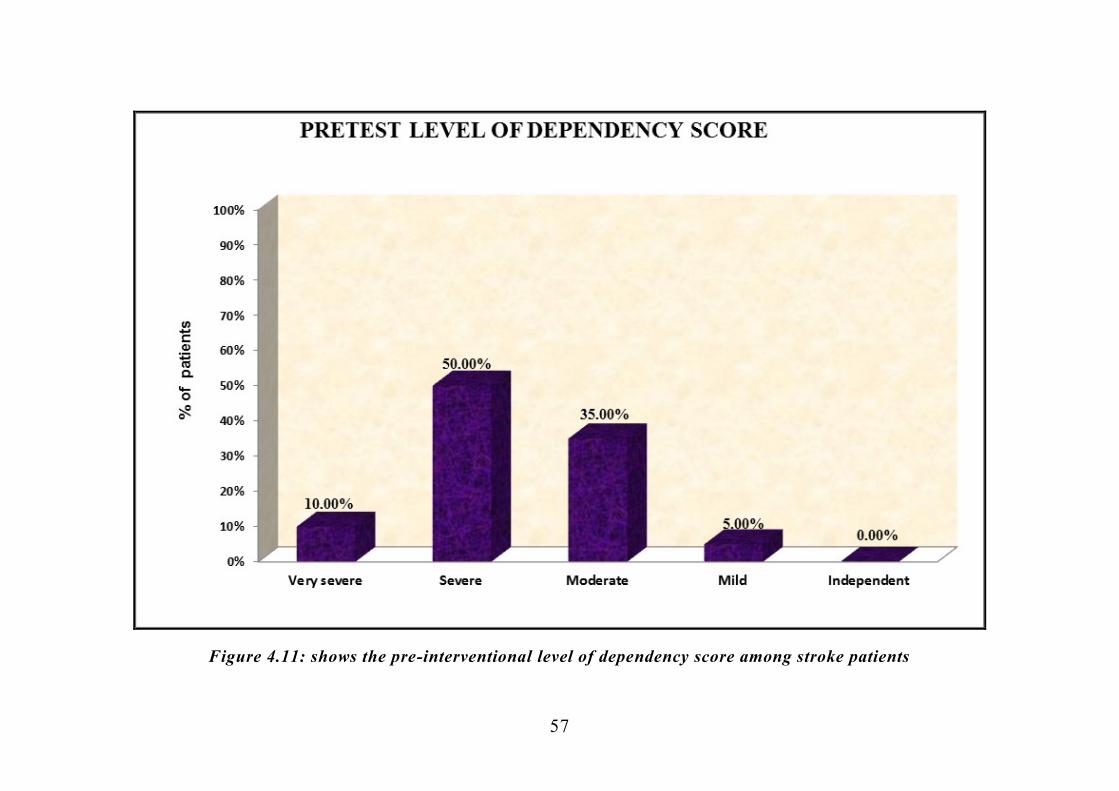
57
Figure 4.11: shows the pre-interventional level of dependency score among stroke patients

58
SECTION-C: ASSESSMENT OF POST - INTERVENTIONAL
LEVEL OF DEPENDENCY AMONG STROKE PATIENTS
Table 4.5: Each question wise post-interventional level of Barthel
index score among stroke patients
S
No Activity
Barthel index of activities of daily living
0 1 2 3
1 Bowels 1 10 29 0
2 Bladder 3 8 29 0
3 Grooming 30 10 0 0
4 Toilet use 1 31 8 0
5 Feeding 0 30 10 0
6 Transfer 0 2 34 4
7 Mobility 0 4 32 4
8 Dressing 1 35 4 0
9 Stairs 15 19 6 0
10 Bathing 31 9 0 0
Table 4.5 shows each activity wise posttest Barthel index score
among stroke patients. They were having more dependency in Bathing
and less dependency in mobility among patients.
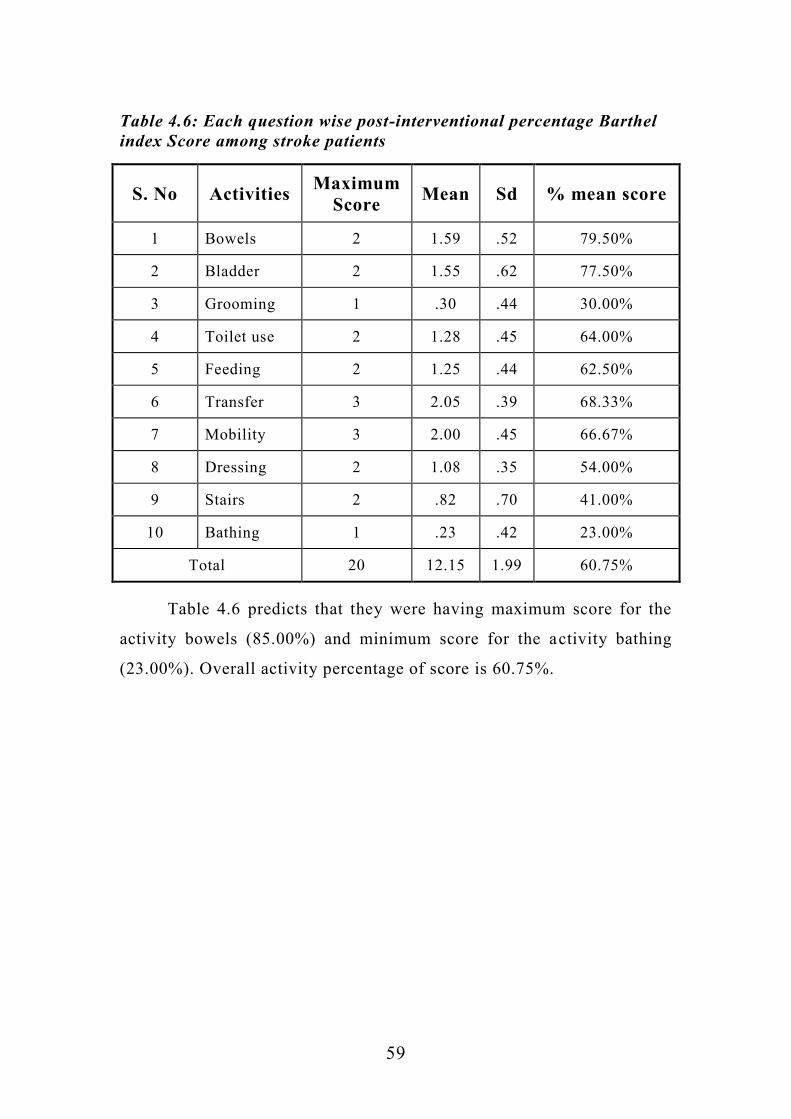
59
Table 4.6: Each question wise post-interventional percentage Barthel
index Score among stroke patients
S. No Activities Maximum
Score Mean Sd % mean score
1 Bowels 2 1.59 .52 79.50%
2 Bladder 2 1.55 .62 77.50%
3 Grooming 1 .30 .44 30.00%
4 Toilet use 2 1.28 .45 64.00%
5 Feeding 2 1.25 .44 62.50%
6 Transfer 3 2.05 .39 68.33%
7 Mobility 3 2.00 .45 66.67%
8 Dressing 2 1.08 .35 54.00%
9 Stairs 2 .82 .70 41.00%
10 Bathing 1 .23 .42 23.00%
Total 20 12.15 1.99 60.75%
Table 4.6 predicts that they were having maximum score for the
activity bowels (85.00%) and minimum score for the activity bathing
(23.00%). Overall activity percentage of score is 60.75%.

60
Table 4.7: Post-interventional level of dependency score
Level of Dependency No. of patients %
Very severe 0 0.00%
Severe 9 22.50%
Moderate 24 60.00%
Mild 7 17.50%
Independent 0 0.00%
Total 40 100.00%
Table 4.7: shows none of patients were having very severe level
of dependency score, 22.5 % of patients were having severe level of
dependency score, 60 % of patients were having moderate level of
dependency score, 17.5 % of patients were having mild level of
dependency score, and none of the patients were having independent
level of dependency score.
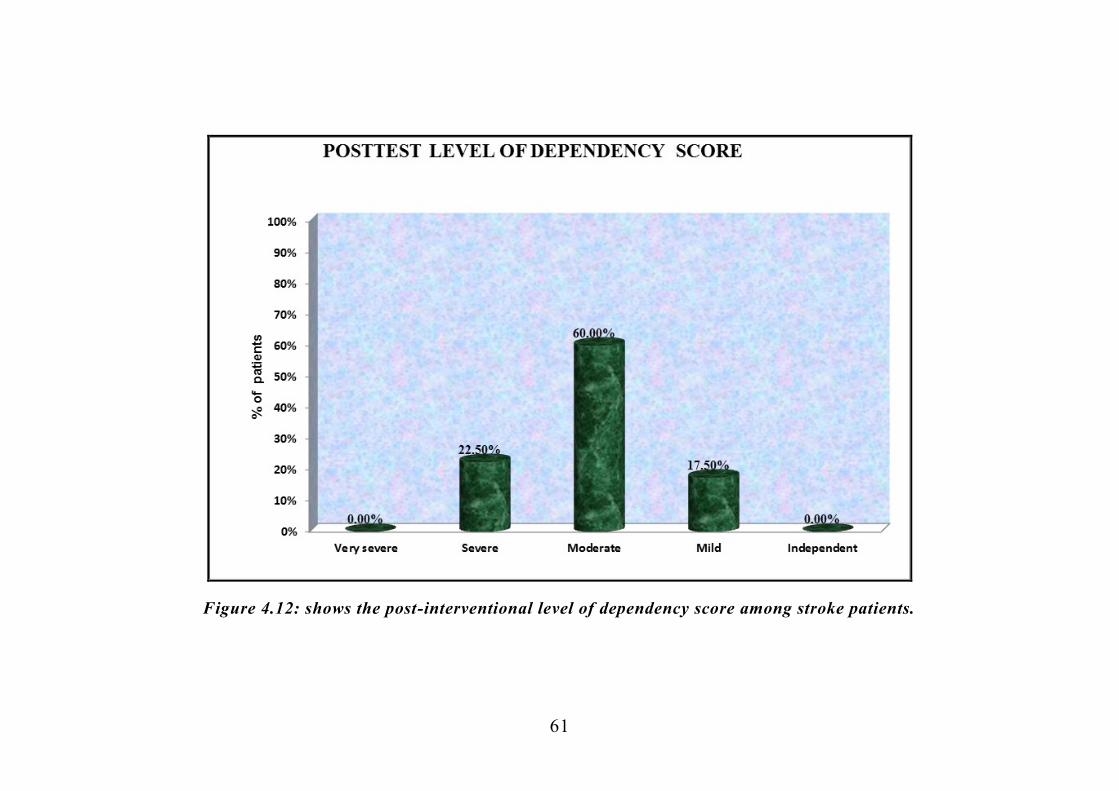
61
Figure 4.12: shows the post-interventional level of dependency score among stroke patients.

62
SECTION-D: COMPARISON OF PRE-INTERVENTIONAL AND
POST INTERVENTIONAL LEVEL OF DEPENDENCY AMONG
STROKE PATIENTS AND THE EFFECTIVENESS OF SHORT
TERM FeSS PROTOCOL
Table-4.8: Comparison of overall dependency score before and after
short term FeSS protocol.
No. of
patients
Pre-
intervention
Mean±SD
Post-
intervention
Mean±SD
Mean
difference
Mean±SD
Paired
t-test
40 8.50 ± 2.71 12.15 ± 1.99 3.65 ± 1.88
t=12.22
P=0.001***
DF = 39,
significant
*** Very high significant at P≤0.001 DF= Degrees of freedom
Table 4.8 shows the comparison of overall dependency score
between pre and post the administration of short term FeSS protocol
among stroke patients. On an average patient are improved their score
from 8.50 to 12.15 after the administration of short term FeSS protocol.
This difference is statistically significant. Statistical significance was
calculated by using student’s paired ‘t’test.

63
Figure4.13: Box Plot compares pre-interventional and post-interventional Barthel Index activities of daily living score
among stroke patients

64
Table-4.9: Each question wise pre-interventional and post-
interventional percentage of dependency score
S.NO Items
Pre-
intervention
score
Post-
intervention
score
% of gain of Barthel
index score
1 Bowels 71.00% 79.50% 8.50%
2 Bladder 52.50% 77.50% 25.00%
3 Grooming 8.00% 30.00% 22.00%
4 Toilet use 40.00% 64.00% 24.00%
5 Feeding 39.00% 62.50% 23.50%
6 Transfer 48.33% 68.33% 20.00%
7 Mobility 56.67% 66.67% 10.00%
8 Dressing 46.00% 54.00% 8.00%
9 Stairs 12.50% 41.00% 28.50%
10 Bathing 5.00% 23.00% 18.00%
Overall 42.50% 60.75% 18.25%
Table 4.9 shows each activity wise Barthel index score among the
stroke patients. On an average, in pre-intervention they are having
42.50% of score and in post-intervention they are having 60.75% of
score.

65
Figure 4.14: Multiple cylindrical diagrams show the pre-interventional and post-interventional percentage of Barthel
index daily activity score.

66
Table-4.10: Comparison of pre-interventional and post-interventional
level of dependency score
Level of Barthel
index score
Pre-
intervention
Post-
intervention Generalized
McNemar’s test
n % n %
Very severe 4 10.00% 0 0.00%
2=19.25
P=0.001***(S)
Severe 20 50.00% 9 22.50%
Moderate 14 35.00% 24 60.00%
Mild 2 5.00% 7 17.50%
Independent 0 0.00% 0 0.00%
Total 40 100.00% 40 100.00%
***significant at p≤0.001 level
Table 4.10 shows the pre-interventional and post-interventional
level of dependency score among stroke patients.
Before SHORT TERM FeSS PROTOCOL, 10 % of patients were
having very severe level of dependency score, 50 % of patients were
having severe level of dependency score, 35 % of patients were having
moderate level of dependency score, 5 % of patients were having mild
level of dependency score, and none of the patients were having
independent score.
After SHORT TERM FeSS PROTOCOL, none of patients were
having very severe level of dependency score, 22.5 % of patients were
having severe level of dependency score, 60 % of patients were having
moderate level of dependency score, 17.5 % of patients were having
mild level of dependency score, and none of the patients were having
independent score.
Level of Barthel score improvement between pretest and posttest
was calculated using Generalized McNemar’s chi-square test.

67
Figure 4.15: Multiple cylindrical diagrams show the pre-interventional and post-interventional level of
dependency score.

68
Table-4.11: Effectiveness of short term FeSS protocol and
generalization of dependency score
Max
score
Mean
score
Mean Difference of
Barthel index
score with 95%
Confidence
interval
Percentage
Difference of
Barthel index gain
score with 95%
Confidence
interval
Pretest 20 8.50 3.65(3.04 – 4.25)
18.25 %
(15.20% –21.25%) Posttest 20 12.15
Table no 4.11 shows the effectiveness of short term FeSS protocol
on level of dependency among stroke patients. On an average, after
intervention of short term FeSS protocol, patients are gained 18.25%
Barthel index score than pre-interventional score.
Differences and generalization of Barthel index gain score
between pretest and posttest score was calculated using and mean
difference with 95% CI and proportion with 95% CI.

69
SECTION-E: ASSOCIATION BETWEEN THE POST-
INTERVENTIONAL LEVEL OF DEPENDENCY AMONG
STROKE PATIENTS WITH THEIR SELECTED
DEMOGRAPHIC VARIABLES.
Table-4.12: Association between post-interventional level of
dependency score and patients’ demographic variables
Demographic
variables
Post-interventional level of Dependency score
N Chi square
test
Very
severe Severe Moderate Mild
Inde
pendent
n % n % N % n % n %
Ag
e
35-45 years 0 0.0% 3 23.0% 5 38.5% 5 38.5% 0 0% 13
2=9.35
P=0.05*(S)
46-55 years 0 0.0% 1 8.3% 9 75.0% 2 16.7% 0 0.0% 12
Above 56
years 0 0.0% 5 33.3% 10 66.7% 0 0.0% 0 0.0% 15
Gen
der
Male 0 0.0% 7 22.6% 21 67.7% 3 9.7% 0 0.0% 31 2=6.19
P=0.05*(S) Female 0 0.0% 2 22.2% 3 33.3% 4 44.4% 0 0.0% 9
Ed
uca
tio
nal
Q
ual
ific
atio
n
Professionals 0 0.0% 0 0.0% 0 0.0% 0 0.0% 0 0.0% 0
2=17.5%
P=0.06(NS)
Graduate or
postgraduate 0 0.0% 0 0.0% 1 33.3% 2 66.7% 0 0.0% 3
Intermediate
or post-high
school
diploma
0 0.0% 0 0.0% 2 100.0% 0 0.0% 0 0.0% 2
High school
certificate 0 0.0% 2 20.0% 8 80.0% 0 0.0% 0 0.0% 10
Middle
school
certificate
0 0.0% 2 25.0% 2 25.0% 4 50.0% 0 0.0% 8
Primary
school
certificate
0 0.0% 3 30.0% 6 60.0% 1 10.0% 0 0.0% 10
Illiterate 0 0.0% 2 28.6% 5 71.4% 0 0.0% 0 0.0% 7
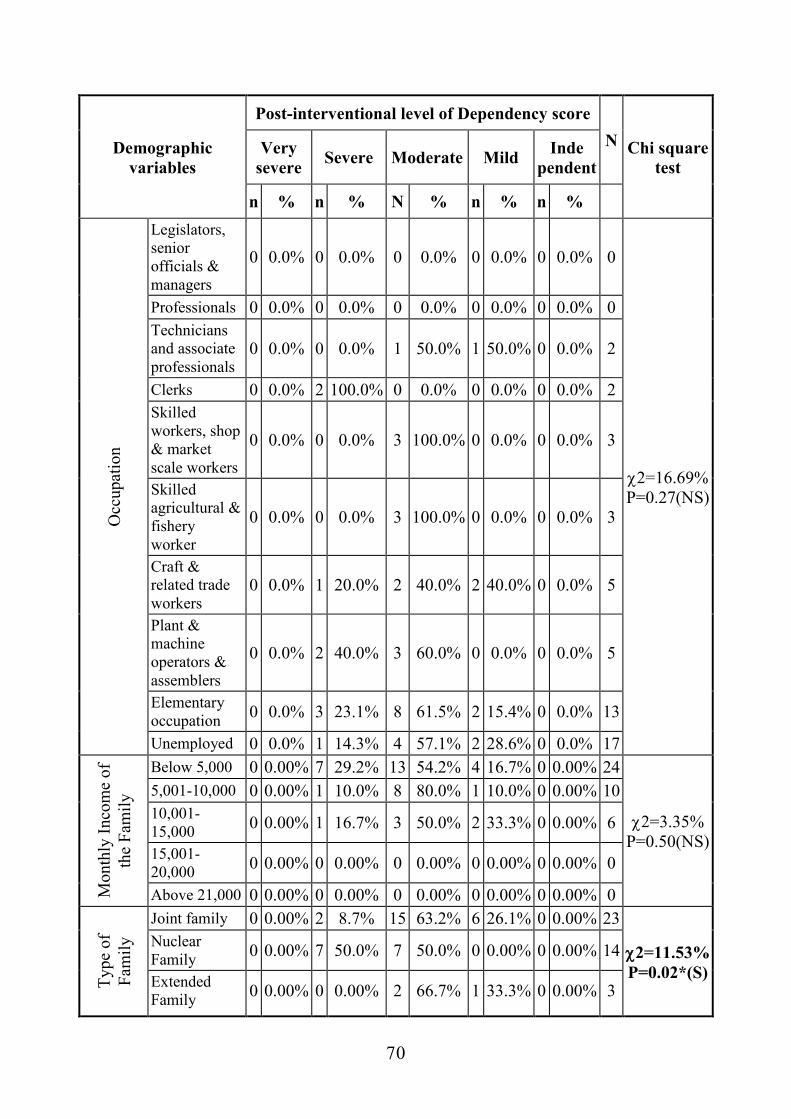
70
Demographic
variables
Post-interventional level of Dependency score
N Chi square
test
Very
severe Severe Moderate Mild
Inde
pendent
n % n % N % n % n %
Occ
up
atio
n
Legislators,
senior
officials &
managers
0 0.0% 0 0.0% 0 0.0% 0 0.0% 0 0.0% 0
2=16.69%
P=0.27(NS)
Professionals 0 0.0% 0 0.0% 0 0.0% 0 0.0% 0 0.0% 0
Technicians
and associate
professionals 0 0.0% 0 0.0% 1 50.0% 1 50.0% 0 0.0% 2
Clerks 0 0.0% 2 100.0% 0 0.0% 0 0.0% 0 0.0% 2
Skilled
workers, shop
& market
scale workers
0 0.0% 0 0.0% 3 100.0% 0 0.0% 0 0.0% 3
Skilled
agricultural &
fishery
worker
0 0.0% 0 0.0% 3 100.0% 0 0.0% 0 0.0% 3
Craft &
related trade
workers 0 0.0% 1 20.0% 2 40.0% 2 40.0% 0 0.0% 5
Plant &
machine
operators &
assemblers
0 0.0% 2 40.0% 3 60.0% 0 0.0% 0 0.0% 5
Elementary
occupation 0 0.0% 3 23.1% 8 61.5% 2 15.4% 0 0.0% 13
Unemployed 0 0.0% 1 14.3% 4 57.1% 2 28.6% 0 0.0% 17
Month
ly I
nco
me
of
the
Fam
ily
Below 5,000 0 0.00% 7 29.2% 13 54.2% 4 16.7% 0 0.00% 24
2=3.35%
P=0.50(NS)
5,001-10,000 0 0.00% 1 10.0% 8 80.0% 1 10.0% 0 0.00% 10
10,001-
15,000 0 0.00% 1 16.7% 3 50.0% 2 33.3% 0 0.00% 6
15,001-
20,000 0 0.00% 0 0.00% 0 0.00% 0 0.00% 0 0.00% 0
Above 21,000 0 0.00% 0 0.00% 0 0.00% 0 0.00% 0 0.00% 0
Ty
pe
of
Fam
ily
Joint family 0 0.00% 2 8.7% 15 63.2% 6 26.1% 0 0.00% 23
2=11.53%
P=0.02*(S)
Nuclear
Family 0 0.00% 7 50.0% 7 50.0% 0 0.00% 0 0.00% 14
Extended
Family 0 0.00% 0 0.00% 2 66.7% 1 33.3% 0 0.00% 3

71
Demographic
variables
Post-interventional level of Dependency score
N Chi square
test
Very
severe Severe Moderate Mild
Inde
pendent
n % n % N % n % n %
Mar
ital
Sta
tus
Married 0 0.00% 8 24.2% 20 60.6% 6 15.2% 0 0.00% 33
2=6.92%
P=0.32(NS)
Unmarried 0 0.00% 1 50.0% 0 0.00% 1 50.0% 0 0.00% 2
Widow/
Widower 0 0.00% 0 0.00% 3 100.0% 0 0.00% 0 0.00% 3
Separated 0 0.00% 0 0.00% 1 50.0% 1 50.0% 0 0.00% 2
Lan
gu
age
Kn
ow
n Tamil 0 0.00% 9 25.7% 21 60.0% 5 14.3% 0 0.00% 35
2=2.93%
P=0.23(NS)
English 0 0.00% 0 0.00% 0 0.00% 0 0.00% 0 0.00% 0
Both 0 0.00% 0 0.00% 3 60.0% 2 40.0% 0 0.00% 5
Other
Languages 0 0.00% 0 0.00% 0 0.00% 0 0.00% 0 0.00% 0
Kn
on
Cas
e o
f
DM
Yes 0 0.00% 5 41.7% 7 58.3% 0 0.00% 0 0.00% 12
2=5.89%
P=0.05*(S) No 0 0.00% 4 14.3% 17 60.7% 7 25.0% 0 0.00% 28
Tim
e fr
om o
nsen
t of
sym
ptom
s ad
mitt
ed to
st
roke
war
d
Within 4Hrs 0 0.00% 0 0.00% 7 87.5% 1 12.5% 0 0.00% 8
2=6.89%
P=0.33(NS)
Within 6Hrs 0 0.00% 8 30.8% 12 46.2% 6 23.1% 0 0.00% 26
Within 12Hrs 0 0.00% 1 20.0% 4 80.0% 0 0.00% 0 0.00% 5
After 12Hrs 0 0.00% 0 0.00% 1 100.0% 0 0.00% 0 0.00% 1
Table 4.12 predicts younger age patients, Female patients were
having more dependency score than others, Joint family patients and
non-diabetes patients were more score gain than others.
Statistical significance was calculated using Pearson chi square test.

72
Figure 4.16: Multiple cylindrical diagrams show the association
between post-interventional level of dependency and their age.
Figure 4.17: Multiple cone diagrams show the association between
post-interventional level of dependency and their gender.

73
Figure 4.18: Multiple cone diagrams show the association between
post-interventional level of dependency and their type of family.
Figure 4.19: Multiple Bar diagrams shows the association
between stroke patients posttest level of dependency score and their
diabetes status

74
Table 4.13: Association between Barthel index gain score and
patient’s demographic variables
Demographic
Variables
Barthel Index Gain Score
N
One-way
ANOVA F-
Test/
T-Test
Pre test Post Test
Gain
Score=
Post-Pre
Mean SD Mean SD Mean SD
Ag
e
35-45 years 7.62 3.10 12.23 2.24 4.62 1.76 13
F=5.24%
P=0.01**(S) 46-55 years 9.83 1.80 12.25 0.62 2.42 1.56 12
Above 56 years 8.20 2.70 12.00 2.54 3.80 1.78 15
Gen
der
Male 8.74 2.91 12.03 2.14 3.29 1.85 31 T=2.42%
P=0.02**(S) Female 7.67 1.73 12.56 1.42 4.89 1.54 9
Ed
uca
tio
nal
Q
ual
ific
atio
n
Professionals 0.00 0.00 0.00 0.00 0.00 0.00 0
F=1.63%
P=0.17(NS)
Graduate or
postgraduate 12.67 1.53 14.00 2.00 1.33 0.58 3
Intermediate or
post-high school
diploma
8.50 0.71 12.50 0.71 4.00 0.00 2
High school
certificate 8.50 2.68 11.90 2.23 3.40 2.01 10
Middle school
certificate 7.88 3.00 12.50 2.33 4.62 1.69 8
Primary school
certificate 8.30 2.54 11.70 2.16 3.40 1.96 10
Illiterate 7.71 2.43 11.86 1.07 4.14 1.86 7

75
Demographic
Variables
Barthel Index Gain Score
N
One-way
ANOVA F-
Test/
T-Test
Pre test Post Test
Gain
Score=
Post-Pre
Mean SD Mean SD Mean SD
Occ
up
atio
n
Legislators, senior
officials &
managers 0.00 0.00 0.00 0.00 0.00 0.00 0
F=1.00%
P=0.45(NS)
Professionals 0.00 0.00 0.00 0.00 0.00 0.00 0
Technicians and
associate
professionals 12.00 1.41 13.00 1.41 1.00 0.00 2
Clerks 5.00 1.41 10.00 1.41 5.0 0.00 2
Skilled workers,
shop & market
scale workers 9.00 1.73 12.33 0.58 3.33 2.08 3
Skilled agricultural
& fishery worker 9.67 2.52 13.33 0.58 3.67 3.06 3
Craft & related
trade workers 9.80 2.68 12.80 1.64 3.00 2.00 5
Plant & machine
operators &
assemblers 6.60 3.29 10.60 2.79 4.00 2.12 5
Elementary
occupation 8.46 2.22 12.08 2.14 3.06 1.71 13
Unemployed 8.29 2.93 12.71 1.89 4.43 1.72 7
Mon
thly
Inc
ome
of th
e
Fam
ily
Below 5,000 8.39 2.92 11.87 2.27 3.50 1.69 24 F=0.70
P=0.50(NS)
5,001-10,000 8.90 2.02 12.40 1.07 3.50 1.78 10
10,001-15,000 8.33 3.20 12.83 2.04 4.50 2.81 6
15,001-20,000 0.00 0.00 0.00 0.00 0.00 0.00 0
Above 21,000 0.00 0.00 0.00 0.00 0.00 0.00 0
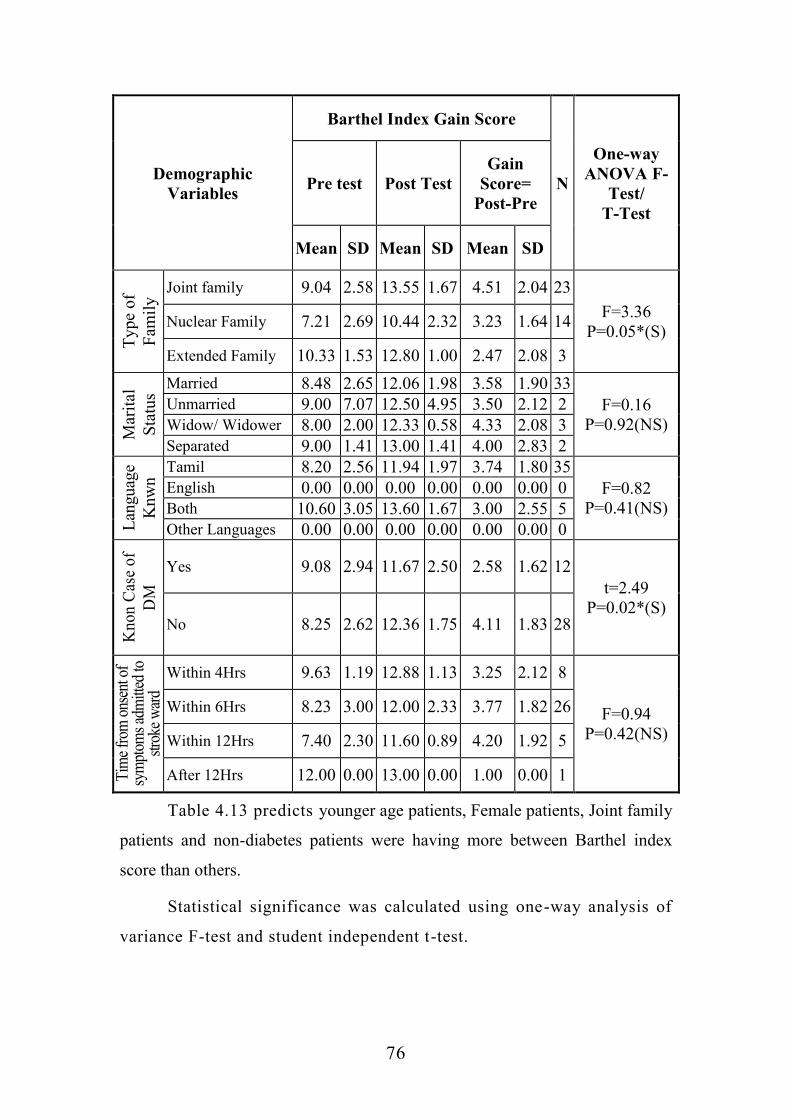
76
Demographic
Variables
Barthel Index Gain Score
N
One-way
ANOVA F-
Test/
T-Test
Pre test Post Test
Gain
Score=
Post-Pre
Mean SD Mean SD Mean SD
Ty
pe
of
Fam
ily
Joint family 9.04 2.58 13.55 1.67 4.51 2.04 23
F=3.36
P=0.05*(S) Nuclear Family 7.21 2.69 10.44 2.32 3.23 1.64 14
Extended Family 10.33 1.53 12.80 1.00 2.47 2.08 3
Mar
ital
Sta
tus
Married 8.48 2.65 12.06 1.98 3.58 1.90 33
F=0.16
P=0.92(NS)
Unmarried 9.00 7.07 12.50 4.95 3.50 2.12 2
Widow/ Widower 8.00 2.00 12.33 0.58 4.33 2.08 3
Separated 9.00 1.41 13.00 1.41 4.00 2.83 2
Lan
guag
e
Knw
n Tamil 8.20 2.56 11.94 1.97 3.74 1.80 35
F=0.82
P=0.41(NS)
English 0.00 0.00 0.00 0.00 0.00 0.00 0
Both 10.60 3.05 13.60 1.67 3.00 2.55 5
Other Languages 0.00 0.00 0.00 0.00 0.00 0.00 0
Kn
on
Cas
e o
f
DM
Yes 9.08 2.94 11.67 2.50 2.58 1.62 12
t=2.49
P=0.02*(S) No 8.25 2.62 12.36 1.75 4.11 1.83 28
Tim
e fr
om o
nsen
t of
sym
ptom
s ad
mitt
ed to
st
roke
war
d
Within 4Hrs 9.63 1.19 12.88 1.13 3.25 2.12 8
F=0.94
P=0.42(NS)
Within 6Hrs 8.23 3.00 12.00 2.33 3.77 1.82 26
Within 12Hrs 7.40 2.30 11.60 0.89 4.20 1.92 5
After 12Hrs 12.00 0.00 13.00 0.00 1.00 0.00 1
Table 4.13 predicts younger age patients, Female patients, Joint family
patients and non-diabetes patients were having more between Barthel index
score than others.
Statistical significance was calculated using one-way analysis of
variance F-test and student independent t-test.

77
CHAPTER-V
DISCUSSION
This chapter deals with the detailed discussion of the study
obtained from the results of the data analysed based on the objectives of
the study hypothesis. The purpose of the study was to assess the
effectiveness of short term FeSS protocol on level of dependency among
stroke patients admitted in stroke ward, Rajiv Gandhi Government
General Hospital, Chennai-03.
This present study was designed to evaluate the effectiveness of
short term FeSS protocol which includes Fever Protocol – monitoring of
body temperature every 4th
hourly and providing prompt management,
Sugar Protocol – management of blood glucose level within normal
range as per the protocol and Swallow protocol – swallowing screening
was done and was referred to speech pathologist. These protocols were
implemented among acute stroke patients within 72 hours following
stroke unit admission.
Totally 40 samples were included in the study. Non-probability
convenient sampling technique were used. In which pre-interventional
and post-interventional level of dependency score was assessed using
Barthel Index which comprises of around 10 activities of daily living
with a total score of 20. The intervention of the protocol by the
researcher was on the first three day following stroke unit admission and
post-intervention was conducted by the researcher after 15th
day
following implementation of FeSS protocol using Barthel Index. The
study period was for about 4 weeks.
5.1 FINDINGS BASED ON DEMOGRAPHIC VARIABLES
37.50% of the patients belong to age group of 35-45 years,
32.50% of the patients belong to age group of 46 – 55 years.

78
77% of the patients were male and 23% of patients were female.
25% of patients were with high school certificate, 20% of patients
were with middle school certificate and 25% of patients were with
primary school certificate
32.50% of patients were elementary occupation and 17.50% of
patients were unemployed.
60% of patients have monthly income of about (<5,000).
57% of the patients were joint family and 35% of patients were
nuclear family.
82.50% of patients were married.
87.50% of patients know Tamil and 12.50% of patients know both
Tamil & English.
70% of patients says Yes with known case of diabetes mellitus.
65% of patients were within 6hrs from onset of symptoms
admitted to stroke ward.
5.1. FINDINGS BASED ON OBJECTIVES
Objective-1: To assess the pre-interventional level of dependency
among stroke patients.
During pre-intervention the level of dependency among stroke
patients. They were having maximum score for the activity bowels
(71.00%) and minimum score for the activity bathing (5.00%). Overall
activity percentage of score is 42.50%.
During pre-intervention the level of dependency among stroke
patients is, 10 % of patients were having very severe level of
dependency score, 50 % of patients were having severe level of

79
dependency score, 35 % of patients were having moderate level of
dependency score, 5 % of patients were having mild level of dependency
score, none of the patients were independent level of dependency score.
The above findings were supported by Sarah Dewilde, et al,
(2019) investigated a study which aimed to assess the combined impact
of dependency on caregivers, disability & coping strategy on quality of
life after stroke, the findings reported that greater disability resulted in
large utility losses between 0.06 for mRs (modified ranking scale) 1 to
0.65 for mRs 5 (p<0.0001). Flexible Goal Adjustment (FGA) coping was
associated with additional increased in utility over and above the effect
of disability and dependency. Jose Manuel, et al, (2018), aimed a study
to investigate which factors influence caregiver strain in informal
caregivers just before the patient discharge. The results revealed that
dependency in activities of daily living scores were statistically
inversely proportional to caregiver strain. Almost 27% of total variance
of caregiver strain was due to dependency in activities of daily living.
Renata Dal -Pra Duci (2018) conducted a study to identify predictors
of dependence after middle cerebral artery (MCA) ischemic stroke, the
findings revealed that among total 144 patients, 47.2% were dependent
at 3 months after stroke. 9.17% were predictors for early dependence.
For the late dependence, 99 patients were included in which 39.4% were
dependent after 3 months.
Thus, the present study results concluded that, globally it was
observed that stroke patients dependent on others for their activities of
daily living which required prompt care.
Objective-2: To assess the effectiveness of short term FeSS protocol
(post-intervention) on level of dependency among stroke patients.
During post-intervention the level of dependency among stroke
patients. They are having maximum score for the activity bowels

80
(85.00%) and minimum score for the activity bathing (23.00%). Overall
activity percentage of score is 60.75%.
In post-interventional level of dependency, none of patients were
having very severe level of dependency score, 22.5 % of patients were
having severe level of dependency score, 60 % of patients were having
moderate level of dependency score, 17.5 % of patients were having
very severe level of dependency score, and none of the patients were
having independent level of dependency score.
The above findings were supported by Patrick Mc Elduff, (2018)
this study found the evidence of the importance of vital monitoring of
patient’s that includes temperature, blood glucose and swallowing
status. It suggested that practice of these vital monitoring in routine
nursing care can result in significant reduction in death & dependency
among stroke patient. Teresa Kenny, el al, (2015) carried-out a study on
management of fever, Hyperglycaemia & Dysphagia in an acute stroke
unit, the findings of the study suggested that care processes did not
consistently reflect best practice. 62% patient’s temperature was
monitored every 4-6th
hourly, 53% of patient’s glucose level was
monitored on admission & 83% of patients received swallow
assessment. Overall only 8 patients (26%) directly admitted to the stroke
unit received best practice assessment.
Thus, the present study findings concluded that FeSS protocols
are required to improve care quality of stroke survivors which in turn
reduces the death and dependency among stroke patients that enhance a
positive stroke outcome.

81
Objective-3: To compare the pre-interventional and post-interventional
level of dependency among stroke patients.
Comparison of overall dependency score between pre and post the
administration of short term FeSS protocol among stroke patients. On an
average patient are improved their score from 8.50 to 12.15 after the
administration of short term FeSS protocol. This difference is
statistically significant. Statistical significance was calculated by using
student’s paired ‘t’test.
Each activity wise Barthel index score among the stroke patients.
On an average, in pre-interventional they were having 42.50% of score
and in post-interventional they were having 60.75% of score.
Before SHORT TERM FeSS PROTOCOL, 10 % of patients were
having very severe level of dependency score, 50 % of patients were
having severe level of dependency score, 35 % of patients were having
moderate level of dependency score, 5 % of patients were having mild
level of dependency score, and none of the patients were having
independent score.
After SHORT TERM FeSS PROTOCOL, none of patients were
having very severe level of dependency score, 22.5 % of patients were
having severe level of dependency score, 60 % of patients were having
moderate level of dependency score, 17.5 % of patients were having
mild level of dependency score, and none of the patients were having
independent score.
Level of Barthel score improvement between pre-interventional
and post-interventional was calculated using Generalized McNemar’s
chi-square test.
The above findings were supported by Sandy Middleton, et al
(2016), proposed a study on spread of a proven intervention in acute

82
stroke. The findings of the study reveals by comparing pre & post
implementation score based on 3 targeted clinical behaviours which are
increased significantly, it shows for management of fever (pre: 96%;
post: 78%; p=0.003), hyperglycaemia (pre: 23%; post: 34%; p=0.0085)
& swallowing (pre:42%; post:51%; p=0.033). B. Furnter, et al, (2017)
conducted a study to improve post-stroke hyperglycaemia management
in clinical practice. The findings of the study states that only 11 (16%)
of patients responded to conventional treatment, whereas 58 (84%) of
patients were non-responsive. These non-responders showed a two-fold
higher risk of death or dependency at three months.
Thus, the present study findings concluded that FeSS protocol was
much effective in decreasing the level of dependency among stroke
patients. It is also effective in such way to assess the baseline data and
reduces the disability and mortality rate among stroke survivors.
Objective-4: To find out the association between the level of
dependency after intervention of FeSS protocol and the selected
demographic variables.
The demographical characteristics of 40 clients who participated
in the study includes the following
37.5% of the patient belongs to age group of 35-45 years, 32.5%
of the patients belong to age group 46-55 years and 30% of the
patients belong to age group of above 56 years.
77% of the patients were male and 23% of patients were female.
57% of patient were joint family, 35% of patient nuclear family
and 8% of patients were extended family.
70% of patients say Yes with known case of diabetes mellitus and
30% of patients says No.

83
The association between the level of dependency after
intervention of FeSS protocol and the selected demographic variables.
Younger age patients, Female patients were having more dependency
score than others, Joint family patients and non-diabetes patients have
more score gain than others. Statistical significance was calculated using
Pearson chi square test.
Younger age patients, Female patients, Joint family patients and
non-diabetes patients were having more Barthel index score than others.
Statistical significance was calculated using one-way analysis of
variance F-test and student independent t-test.
The above findings were supported by Kelly Coughlan, et al,
(2019), conducted a study on nurse-initiated stroke intervention. The
study findings predict association between the baseline demographic and
clinical characteristics, among which older age (75-84 years) &
increasing stroke severity were associated with increased mortality and
also being married was associated with increased likelihood of survival
& finally cardiovascular disease was listed either as the primary or
secondary cause of death in 80%. Neha Rai, Kameshwar, et al (2016),
conducted a cluster randomized study in development & implementation
of acute stroke care pathway. As a result, progress out of 162 patients,
the mean age was 55.7 years in which 73.5% were male which is
statistically significant (p=0.019). the outcome assessment states that,
clinical pathway showed trends towards significance when compared
with the conventional care, (i.e) there is reduction in need for
mechanical ventilation, lower the risk of aspirated pneumonia and
decreased the rate of death & dependency over 90 days outcome.
Thus, the present study result concluded that, there is a significant
association with the post-interventional level with the selected
demographic variables. The purpose of the study was to develop a

84
acceptable and evidence based acute stroke clinical protocol and also
need to implement this protocol on standard medical care.
H2-There will be significant association between the post-
interventional level of dependency and the selected demographic
variables.
The analysis revealed that there was significant association
between demographic variables such as age, gender, type of family,
known case of diabetes with the level of dependency among stroke
patients. 2=5.89 P=0.05*(S). Thus, the researcher accepts the
hypothesis.
The present study results highlight the effectiveness of short term
FeSS protocol in decreasing the level of dependency among stroke
patients. It is also evident that FeSS protocol is effective in reducing the
disability and mortality rate among stroke survivors which in turn
enhance a positive stroke outcome.

85
CHAPTER-VI
SUMMARY, IMPLICATION, RECOMMENDATION,
LIMITATION, CONCLUSION
6.1 SUMMARY OF THE STUDY
Investigator undertook the study to assess the effectiveness of
short term FeSS protocol on level of dependency among stroke patients
admitted in stroke ward, Rajiv Gandhi Government General Hospital,
Chennai-03.
The conceptual framework of the study was based on the
Modified Framework of Weidnenbach’s helping art of clinical nursing
theory. Pre experimental one group pre-interventional and post-
interventional design was used. The independent variable was short term
FeSS Protocol, dependent variable was the level of dependency among
stroke patients.
The study period was 4 weeks from 2.2.19 to 4.3.19 totally 40
patients were selected as samples using convenient sampling technique.
The data was collected using standardized tool – Barthel Index.
Intervention on short term FeSS Protocol and hand out was given. The
reliability of the tool was test retest method, the data analysis and
interpretation were done by using descriptive and inferential statistics.
6.2 MAJOR FINDINGS OF THE STUDY
6.2.1 Based on the demographic variables
Regarding their Age, Maximum 37.50% of the patients belong to age
group of 35-45 years, 32.50% of the patients belong to age group of 46 – 55
years and 30.00% of the patients belong to age group of above 56 years.
Among Gender distribution, 77% of the patients were male and
23% of patients were female.

86
Regarding Educational qualification, 7.50% of the patients were
graduate or postgraduate, 5% of patients were intermediate, 25% of
patients were with high school certificate, 20% of patients were with
middle school certificate, 25% of patients were with primary school
certificate and 17.50% of patients were illiterate.
Inspite of Occupation: 5% of the patients were technicians and
associate professionals, 5% of patients were clerks, 7.50% of patients
were skilled workers, 7.50% of patients were skilled agricultural &
fishery worker, 12.50% of patients were craft & related trade workers,
32.50% of patients were elementary occupation and 17.50% of patients
were unemployed.
In related to Monthly income, 60% of patients have monthly
income of about (<5,000), 25% of patients have monthly income of
about (5,000 – 10,000) and 15% of patients have monthly income of
about (10,000 – 15,000).
Among the Type of family: 57% of the patients were joint family, 35%
of patients were nuclear family, and 8% of patients were extended family.
Regarding Marital status: 82.50% of patients were married, 5%
of patients were unmarried, 7.50% of patients were widow/widower, and
5% of patients were separated.
Based on Languages known, 87.50% of patients know Tamil and
12.50% of patients know both Tamil & English.
In related to Known case of diabetes mellitus, 70% of patients
says Yes and 30% of patients says No.
Regarding Time from onset of symptoms admitted to stroke ward,
20% of patients were within 4hrs, 65% of patients were within 6hrs, 12.5% of
patients were within 12hrs and 2.50% of patients were after12hrs.

87
6.2.2 Based on the level of dependency before and after intervention
on FeSS Protocol:
In the pre-interventional 10 % of patients were having very
severe level of dependency score, 50 % of patients were having
severe level of dependency score, 35 % of patients were having
moderate level of dependency score, 5 % of patients were having
mild level of dependency score, none of the patients were
independent level of dependency score.
In the post-interventional none of patients were having very
severe level of dependency score, 22.5 % of patients were having
severe level of dependency score, 60 % of patients were having
moderate level of dependency score, 17.5 % of patients were
having mild level of dependency score, and none of the patients
were having independent level of dependency score.
6.2.3 Finding based on comparison of pre-interventional and post-
interventional mean knowledge score
Comparison of overall dependency score between pre and post the
administration of short term FeSS protocol among stroke patients. On an
average patient are improved their score from 8.50 to 12.15 after the
administration of short term FeSS protocol. This difference is
statistically significant. Statistical significance was calculated by using
student’s paired ‘t’test.
Each question wise pre-interventional and post-interventional
percentage of dependency score: On an average, in pre-interventional
they were having 42.50% of score and in post-interventional they were
having 60.75% of score.
6.2.4 Findings based on Comparison of pre-interventional and post-
interventional level of dependency score

88
Before SHORT TERM FeSS PROTOCOL, 10 % of patients were
having very severe level of dependency score, 50 % of patients were
having severe level of dependency score, 35 % of patients were having
moderate level of dependency score, 5 % of patients were having mild
level of dependency score, and none of the patients were having
independent level of dependency score.
After SHORT TERM FeSS PROTOCOL, none of patients were
having very severe level of dependency score, 22.5 % of patients were
having severe level of dependency score, 60 % of patients were having
moderate level of dependency score, 17.5 % of patients were having
mild level of dependency score, and none of the patients were having
independent level of dependency score. Level of Barthel score
improvement between pre-interventional and post-interventional was
calculated using Generalized McNemar’s chi-square test.
6.2.5 Findings based on Effectiveness of short term fess protocol and
generalization of dependency score
On an average, in post-interventional after intervention of short
term fess protocol, patients were gained 18.25% Barthel index score
than pre-interventional score.
Differences and generalization of Barthel index gain score
between pre-interventional and post-interventional score was calculated
using and mean difference with 95% CI and proportion with 95% CI.
6.2.6 Findings based on association between the post interventional
levels of dependency among stroke patients with their selected
demographic variables.
Younger age patients, Female patients were having more
dependency score than others, Joint family patients and non-diabetes
89
patients were more score gain than others. Statistical significance was
calculated using Pearson chi square test.
6.3 IMPLICATIONS OF THE STUDY
The findings of the study have the following implications in
different areas of nursing that is, nursing practice, nursing education,
nursing administration and nursing research. By evaluating the
effectiveness of FeSS Protocol in decreasing the level of dependency
among stroke patients. The investigator received a clear picture
regarding the different steps to be taken in different fields to improve
the same.
6.3.1. Nursing practice
This study is conducted by implementing short term FeSS
protocol to decrease the level of dependency among stroke
patients. This protocol can be utilized by the nurses in their
practice while they receive a patient with acute stroke in order to
promote a positive stroke outcome.
Ongoing in-service education programs should be designed and
implemented at stroke care units to improve nurses' knowledge
and practices on the basis of nurse's care regarding FeSS protocol.
A standardized clinical nursing FeSS protocol should be made
available in each stroke care unit.
Newly joined staff nurses in stroke care unit should also be well
oriented with the standardized clinical nursing FeSS protocol to
ensure competent nursing care in their practice.
Nurse who work in stroke care unit should follow this FeSS
protocol as a routine practice in receiving a patient with acute

90
stroke onset and promote education regarding positive stroke
outcomes.
6.3.2. Nursing Education
The practice and benefits of FeSS protocol could be introduced in
to the curriculum as a part in stroke rehabilitation to promote a
positive outcome.
The nurse educator can use this protocol in teaching the student
nurses (future nurses) to implement this into their practice.
The findings of the study will help the nurses to give more
importance for planning and organizing programme regarding
FeSS protocol, so that they can implement in the clinical practice.
Among all standardized clinical nursing protocol this FeSS
protocol must be integrated as a routine practice
Educational training programs for nurses should include following
fever protocol, sugar protocol and swallowing protocol among
stroke patient admitted to stroke unit within 72 hours onset.
The nurses should be made aware of their responsibility in the
care of stroke patients in decreasing their level of dependency.
6.3.3. Nursing Administration
Due to the technological advances and ever-growing challenges of
nursing, the nurse administrators have responsibility to provide
the nurses with substantive educational training programme.
Nursing administrator should provide necessary facilities and
opportunities for nursing students and staffs.
The nurse administrator should organize a specialized unit for
developing nurses’ knowledge & practices (training uni t).
91
The hospital administrative authority should develop up-dated
acute stroke care unit policies and procedures for nurses and
should be annually reviewed and approved by the quality
assurance committee.
Provide adequate medical and nursing supervision, guidance and
regular feedback to nurses concerning their knowledge, attitude
and performance.
Advanced booklets and electronic media regarding clinical
protocols for stroke patients should be available at each acute
stroke care unit.
Nursing administrator has more responsibility as a supervisor on
creating awareness among nurses regarding stroke rehabilitation
by facilitating free distribution of booklets, handouts, regularly in
outpatient department of hospitals, health clinics in urban and
rural.
6.3.4. Nursing Research
The findings can be utilized as evidence-based practice in clinical
practice beneficial for nurses who work in stroke care unit.
Future studies can be conducted on effect of FeSS protocol among
stroke patients for longer duration.
There is growing need for furnishing nursing research in all the
areas of care. The nurse researcher especially beginners need to
enhance their quest for knowledge and practice. The nurse
researcher may effectively use result of available patient and
recommended on the importance of application FeSS protocol.
The study findings can be a baseline for further studies to build
upon for improving the body of knowledge in nursing

92
The study findings can be effectively utilized by the emerging
researchers.
6.4. LIMITATIONS OF THE STUDY
This study is limited to stroke patients admitted in stroke ward,
Rajiv Gandhi Government General Hospital, Chennai-03.
The study is limited up to 4 weeks of period
Acute stroke patients within 72 hours onset
The investigator could get more of abroad studies than Indian
studies to support the present study
6.5. RECOMMENDATIONS
On the basis of the study the following recommendations have
been made for further study:
A similar study could be replicated on a larger sample.
A similar study could be conducted in different settings for longer
duration to find out the effectiveness of FeSS protocol.
This similar study could be replicated with a control group.
A comparative study can be conducted among stroke patients
under FeSS protocol and patients under normal routine nursing
care.
A similar study could be conducted to rule out the effectiveness of
FeSS protocol on level of dependency and mortality rate among
stroke patients.

93
6.6. CONCLUSION
Nurses must have holistic knowledge regarding use of FeSS
protocol in decreasing the level of dependency among stroke patients.
Nurses play a vital role in proving care to stroke patients who depend on
others for their activities of daily living. The present study had been
supported by a series of other studies which confirmed that patients
under FeSS protocol has decreased level of dependency that promotes a
positive stroke outcome. Data analysis and result was found that short
term FeSS protocol was an effective method in reducing the level of
dependency among stroke patients. Majority of the patients showed
decreased level of dependency after intervention of FeSS protocol. The
findings of the study were consistent with the review of literature
supports the study.

19
REFERENCES
BOOK REFERENCES
1) Anne-Marie Brady , Catherine McCabe , Margaret McCann .
Fundamentals of Medical-Surgical Nursing: A Systems Approach.
Hoboken, United States: John Wiley and Sons Ltd ; 2014
2) Dennis L. Kasper , Anthony S. Fauci , Stephen L. Hauser et al.
Harrison's Principles of Internal Medicine 19/E (Vol.1 & Vol.2).
United States: McGraw-Hill Education - Europe; 2015.
3) Douglas , Rebeiro , Waters , Crisp . Potter & Perry's
Fundamentals of Nursing - Australian Version - 5th Edition.
Marrickville, Australia: Elsevier Australia ; 2016
4) Elsevier - Health Sciences Division. Nursing Research:
Generating and Assessing Evidence for Nursing Practice. Tenth,
International Edition. Philadelphia, United States: Lippincott
Williams and Wilkins; 2016
5) Joyce M. Black, Jane Hokanson Hawks . Medical-Surgical
Nursing - Two Volume Set: Clinical Management for Positive
Outcomes, 2-Volume Set. 8th Revised edition. London, United
Kingdom: Elsevier Health Sciences; 12 May 2008
6) Kader Parahoo. Nursing Research: Principles, Process and Issues.
3rd ed. 2014. United Kingdom: MacMillan Education UK; 2014.
7) Mant J, Wade DT, Winner S. Health care needs assessment:
stroke. Health care needs assessment review, first series. 2nd edn.
Stevens A, Raftery J, Mant J, et al., editors. Oxford; Radcliffe
Medical Press : 2004. pp. 141-244.
20
8) National Institute for Health and Clinical Excellence. The
guidelines manual 2007. London: NICE; 2007.
9) O'Connell Smeltzer SC, Bare BG. Brunner and Suddarth's
Textbook of Medical-Surgical Nursing [Internet]. Philadelphia
(PA): Lippincott Williams & Wilkins; 2003.
10) Patricia L. Munhall . Nursing Research. 5th Revised edition.
Sudbury, United States: Jones and Bartlett Publishers, Inc; 2010.
11) Roller MR, Lavrakas, PJ. Applied qualitative research design: a
total quality framework approach. New York: The Gilford Press;
2015. [cited 2017 Jan 24]. Available from: Ebook Library.
12) Susan C. Dewit, Holly Stromberg , Carol Dallred . Medical-
Surgical Nursing: Concepts & Practice. 3rd Revised edition.
Philadelphia, United States: Elsevier - Health Sciences Division;
2016.
JOURNAL REFERENCES
1) Alexandrov AW, Palazzo P, Biby S, Doerr A, Dusenbury W,
Young R, Lindstrom A, Grove M, Tsivgoulis G, Middleton S,
Alexandrov AV. Back to Basics: Adherence with Guidelines for
Glucose and Temperature Control in an American Comprehensive
Stroke Center Sample. Journal of Neuroscience Nursing. 2018 Jun
1;50(3):131-7.
2) Alhazzani A, Mahfouz A, Abolyazid A, Awadalla N, Katramiz K,
Faraheen A, Khalil S, Aftab R. In Hospital Stroke Mortality:
Rates and Determinants in Southwestern Saudi Arabia.
International journal of environmental research and public health.
2018 May;15(5):927.

21
3) Bonita R, Solomon N, Broad JB. Prevalence of stroke and stroke-
related disability: estimates from the Auckland Stroke Studies.
Stroke. 1997 Oct;28(10):1898-902.
4) Bonner B, Pillai R, Sarma PS, Lipska KJ, Pandian J, Sylaja PN.
Factors predictive of return to work after stroke in patients with
mild− moderate disability in India. European journal of
neurology. 2016 Mar;23(3):548-53.
5) Chin YY, Sakinah H, Aryati A, Hassan BM. Prevalence, risk
factors and secondary prevention of stroke recurrence in eight
countries from south, east and southeast asia: a scoping review.
The Medical journal of Malaysia. 2018 Apr;73(2):90-9.
6) Cortés-Vicente E, Guisado-Alonso D, Delgado-Mederos R,
Camps-Renom P, Prats-Sánchez L, Martínez-Domeño A, Martí-
Fàbregas J. Frequency, risk factors and prognosis of dehydration
in acute stroke. Frontiers in neurology. 2019;10:305.
7) Gianluca Pucciarelli, Christopher S Lee, Karen S Lyons. Quality
of life trajectories among stroke survivors and the related changes
in caregiver outcomes. APMR (Archives of Physical Medicine and
Rehabilitation). 2019; 100(3): 401-433.
8) Harbison J, Hossain O, Jenkinson D, et al. Diagnostic accuracy of
stroke referrals from primary care, emergency room physicians,
and ambulance staff using the face arm speech test. Stroke. 2003;
34(1): 71-76.
9) Jeong SH, Ahn SS, Baik M, Kim KH, Yoo J, Kim K, Lee HS, Ha
J, Kim YD, Heo JH, Nam HS. Impact of white matter
hyperintensities on the prognosis of cryptogenic stroke patients.
PloS one. 2018 Apr 27;13(4):e0196014.

22
10) Kamalakannan S, Gudlavalleti AS, Gudlavalleti VS, Goenka S,
Kuper H. Incidence & prevalence of stroke in India: A systematic
review. The Indian journal of medical research. 2017
Aug;146(2):175.
11) Khalid SI, Carlton A, Glick RP. Identification of reversible causes
of minority inequity in stroke: severity related to race and socio-
economic status. Brain injury. 2018 Oct 15;32(12):1477-83.
12) Kidwell CS, Starkman S, Eckstein M, et al. Identifying stroke in
the field. Prospective validation of the Los Angeles pre hospital
stroke screen (LAPSS). Stroke.2003; 31(1):71-76.
13) Kothari R, Hall K, Brott T, et al.Early stroke recognition:
developing an out-of-hospital NIH Stroke Scale. Academic
Emergency Medicine. 1997; 4(10): 986-990.
14) Krishnamurthi RV, Barker-Collo S, Parag V, Parmar P, Witt E,
Jones A, Mahon S, Anderson CS, Barber PA, Feigin VL. Stroke
incidence by major pathological type and ischemic subtypes in the
Auckland regional community stroke studies: changes between
2002 and 2011. Stroke. 2018 Jan;49(1):3-10.
15) Labodi LD, Kadari C, Mahamoudou S, Judicaël KN, Cristian N,
Jean K. Factors Associated with the Occurrence of Medical
Complications in the Acute Phase of Stroke in a Reference
Hospital at Ouagadougou (Burkina Faso). Journal of Advances in
Medicine and Medical Research. 2018 Jun 13:1-4.
16) Li T, Horton RM, Bader DA, Liu F, Sun Q, Kinney PL. Long-term
projections of temperature-related mortality risks for ischemic
stroke, hemorrhagic stroke, and acute ischemic heart disease
under changing climate in Beijing, China. Environment
international. 2018 Mar 1;112:1-9.

23
17) Mani K, Sundar S. Outcome measures used in stroke
rehabilitation in India: A scoping review. The Indian Journal of
Occupational Therapy. 2018 Oct 1;50(4):111.
18) Middleton S, Bruch D, Martinez‐Garduno C, Dale S, McNamara
M. International Uptake of a Proven Intervention to Reduce Death
and Dependency in Acute Stroke: A Cross‐Sectional Survey
Following the QASC Trial. Worldviews on Evidence‐Based
Nursing. 2017 Dec;14(6):447-54.
19) Middleton S, Coughlan K, Mnatzaganian G, Low Choy N, Dale S,
Jammali-Blasi A, Levi C, Grimshaw JM, Ward J, Cadilhac DA,
McElduff P. Mortality reduction for fever, hyperglycemia, and
swallowing nurse-initiated stroke intervention: QASC Trial
(Quality in Acute Stroke Care) follow-up. Stroke. 2017
May;48(5):1331-6.
20) Middleton S, Lydtin A, Comerford D, Cadilhac DA, McElduff P,
Dale S, Hill K, Longworth M, Ward J, Cheung NW, D'Este C.
From QASC to QASCIP: successful Australian translational scale-
up and spread of a proven intervention in acute stroke using a
prospective pre-test/post-test study design. BMJ open. 2016 May
1;6(5): e011568.
21) Middleton S, McElduff P, Drury P, D’Este C, Cadilhac DA, Dale
S, Grimshaw JM, Ward J, Quinn C, Cheung NW, Levi C. Vital
sign monitoring following stroke associated with 90-day
independence: A secondary analysis of the QASC cluster
randomized trial. International journal of nursing studies. 2019
Jan 1; 89:72-9.
22) National Collaborating Centre for Chronic Conditions. Acute stroke
and TIA: guideline methodology pack. London: NCC-CC; 2006.

24
23) Nor AM, McAllister C, Louw SJ, et al. Agreement between
ambulance paramedic and physician -recorded neurological signs
with Face Arm Speech Test (FAST) in acute stroke patients.
Stroke 2004; 35(6): 1355-1359.
24) O'Donnell MJ, Chin SL, Rangarajan S, Xavier D, Liu L, Zhang H,
Rao-Melacini P, Zhang X, Pais P, Agapay S, Lopez-Jaramillo P.
Global and regional effects of potentially modifiable risk factors
associated with acute stroke in 32 countries (INTERSTROKE): a
case-control study. The lancet. 2016 Aug 20;388(10046):761-75.
25) Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM,
Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM,
Hoh B, Jauch EC. 2018 guidelines for the early management of
patients with acute ischemic stroke: a guideline for healthcare
professionals from the American Heart Association/American
Stroke Association. Stroke. 2018 Mar;49(3): e46-99.
26) Rai N, Prasad K, Bhatia R, Vibha D, Singh MB, Rai VK, Kumar
A. Development and implementation of acute stroke care pathway
in a tertiary care hospital in India: A cluster-randomized study.
Neurology India. 2016 Feb 1;64(7):39.
27) Robinson R. For Your Patients-Stroke Rehabilitation: Repetitive
Transcranial Magnetic Stimulation Improves Post-Stroke Walking
Speed. Neurology Today. 2018 Jul 5;18(13):21-3.
28) Rohweder G, Ellekjær H, Salvesen Ø, Naalsund E, Indredavik B.
Functional outcome after common poststroke complications
occurring in the first 90 days. Stroke. 2015 Jan;46(1):65-70.
29) Schwarz M, Coccetti A, Murdoch A, Cardell E. The impact of
aspiration pneumonia and nasogastric feeding on clinical

25
outcomes in stroke patients: a retrospective cohort study. Journal
of clinical nursing. 2018 Jan;27(1-2):e235-41.
30) Shamshirgaran SM, Barzkar H, Savadi-Oskouei D, Marandi MY,
Safaiyan A, Sarbazi E, Novbakht H, Gaffari S. Predictors of
short-term mortality after acute stroke in East Azerbaijan
province, 2014. Journal of cardiovascular and thoracic research.
2018;10(1):36.
31) Shiraishi A, Yoshimura Y, Wakabayashi H, Tsuji Y. Prevalence
of stroke-related sarcopenia and its association with poor oral
status in post-acute stroke patients: implications for oral
sarcopenia. Clinical Nutrition. 2018 Feb 1;37(1):204-7.
32) Simon D. Ubben, Gereon R. Fink, Stephanie Kaesberg. Deficient
allo-centric visuospatial processing contributes to apraxic deficits
in sub-acute right hemisphere stroke. J Neuropsychol. 2019;
7(3):233-5.
33) Skafida A, Mitrakou A, Georgiopoulos G, Alevizaki M, Spengos
K, Takis K, Ntaios G, Thomadakis C, Vemmos K. In-hospital
dynamics of glucose, blood pressure and temperature predict
outcome in patients with acute ischaemic stroke. European stroke
journal. 2018 Jun;3(2):174-84.
34) Van Mierlo M, van Heugten C, Post MW, Hoekstra T, Visser-
Meily A. Trajectories of health-related quality of life after stroke:
results from a one-year prospective cohort study. Disability and
rehabilitation. 2018 Apr 24;40(9):997-1006.
35) Victoria Sherman, Heather L. Flowers, Moria Kassia Kapral.
Screening for Dysphagia in Adult Patients with stroke: Assessing
the accuracy of informal detection. Dysphagia. 2018; 33:662-9.

26
NET REFERENCES
1) http//www.googlescholar.html.
2) http://www.healthline.com
3) https://en.wikipedia.org
4) https://jamanetwork.com
5) https://jamenetwork.com/journals
6) https://www.mayoclinic.org
7) https://www.pubmet.com
8) https://www.stroke.org
9) https://www.strokeassociation.org
10) https://www.webmd.com

SECTION-A
DEMOGRAPHIC VARIABLES:
1. Age
a) 35-45 years
b) 46-55 years
c) Above 56 years
2. Gender
a) Male
b) Female
3. Educational qualification
a) Professionals
b) Graduate or postgraduate
c) Intermediate or post-high school diploma
d) High school certificate
e) Middle school certificate
f) Primary school certificate
g) Illiterate
4. Occupation
a) Legislators, senior officials & managers
b) Professionals
c) Technicians and associate professionals.
d) Clerks
e) Skilled workers, shop & market scale workers
f) Skilled agricultural & fishery worker
g) Craft & related trade workers
h) Plant & machine operators & assemblers
i) Elementary occupation
j) Unemployed
5. Monthly income of the family
a) Below 5,000
b) 5,001-10,000
c) 10,001-15,000
d) 15,001-20,000
e) Above 20,001
6. Type of family
a) Joint family
b) Nuclear family
c) Extended family
7. Marital status
a) Married
b) Unmarried
c) Widow / Widower
d) Separated
8. Languages known
a) Tamil
b) English
c) Both
d) Other language.
9. Known case of diabetes mellitus
a) Yes
b) No
10. Time from onset of symptoms admitted to stroke ward
a) Within 4 hrs
b) Within 6 hrs
c) Within 12 hrs
d) After 12 hrs

SECTION-B
FeSS Fever Protocol
The QASC Fever Protocol consists of monitoring the patient’s temperature and the
prompt treatment of a temperature 37.5°C or greater in the first 72 hours using the
fever algorithm attached.
This protocol was used in conjunction with the other FeSS protocols and the FeSS
implementation strategies and not as a stand-alone protocol.
Target temperature: < 37.5°C
Record baseline temperature on admission to stroke unit and for the first 72 hours
following admission
Monitor and record temperature every four to six hours
If temperature > 37.5°C, remove blankets and any heaters
Administer oral paracetamol 1 gram then re-assess
If patient nil by mouth administer paracetamol 1gram via nasogastric tube
(NGT), per rectum (PR) or intravenously (IV) (according to hospital policy)
then re-assess
Continue to monitor and record temperature four hourly
If temperature > 38°C:
Inform medical team
Consider septic workup (as per hospital/unit policy)
-Stream Urine sample
-ray
Continue to monitor temperature four hourly
Note: Patients clinical condition should always be taken into consideration

FeSS Fever Protocol
ASU admission temperature
< 37.5o
C
Monitor
temp Q4-6H
> 37.5o
C
Remove blankets,
heaters, tepid
sponging, cold
compress
Administer
paracetamol
PO PR IV (as per
hospital policy)
Monitor
temp Q4H > 38oC
Inform medical
team & consider
septic screen as
per hospital
policy
Monitor
temp Q4H
PO = Per Oral
PR = Per Rectal
IV = Intravenous
Q4H = every four hours

FeSS Sugar Protocol
The QASC Sugar Protocol consists of monitoring the patient’s blood glucose levels
for the first 72 hours following admission to the stroke unit, and the prompt treatment
of a blood glucose level > 178 mg dl in the first 48 hours.
The QASC sugar protocol shown here has been modified slightly in response to
feedback from participating sites, and to concord with the incoming Australian
Diabetes Society Guidelines for routine glucose control in hospital.
This protocol was used in conjunction with the other FeSS protocols and the FeSS
implementation strategies and not as a stand-alone protocol

FeSS Sugar Protocol
Initial finger prick Blood Glucose Level
(BGL) on admission to stroke unit
BGL < 178 mg dl BGL > 178 mg dl
Non-diabetic
Known
Diabetes
Fasting & after meals
finger prick BGL
testing. If not eating
test BGL 6 hourly
No further
treatment
Before & after meals & bed
time finger prick BGL
testing. Continue routine
diabetes medication if
eating. Cease usual diabetes
medication if not eating and
test BGL 4-6 hourly
Insulin glucose infusion
for first 48 hours, with
hourly BGLs (reduce to
q2h if stable for 4 hours).
Suspend oral diabetic
medications. Titrate
insulin to maintain BGL
5-10 or as per local
titration algorithm
Any BGL
>178 in
first 48 hrs
go back to
red boxes
After 48 hours cease
infusion if patient stable
and tolerating oral intake.
Resume usual diabetic
medications including
insulin. Continue before
& after meals & bed time
finger prick BGL testing
Any BGL
>178 in
first 48
hrs go
back to
red boxes
Continue before
& after meals &
bed time finger
prick BGL
testing
Known
Diabetes
BGL < 178 BGL >178
Usual management
Not previously
known to be
diabetic
Seek
endocrinology
team
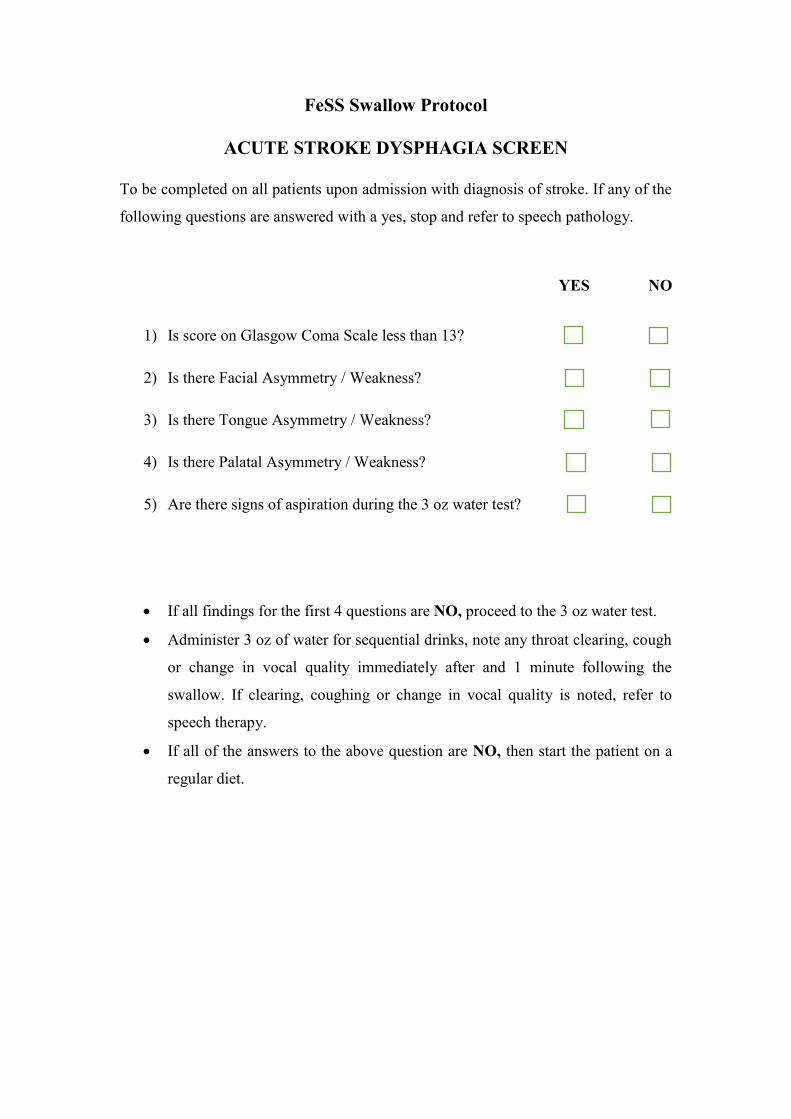
FeSS Swallow Protocol
ACUTE STROKE DYSPHAGIA SCREEN
To be completed on all patients upon admission with diagnosis of stroke. If any of the
following questions are answered with a yes, stop and refer to speech pathology.
YES NO
1) Is score on Glasgow Coma Scale less than 13?
2) Is there Facial Asymmetry / Weakness?
3) Is there Tongue Asymmetry / Weakness?
4) Is there Palatal Asymmetry / Weakness?
5) Are there signs of aspiration during the 3 oz water test?
If all findings for the first 4 questions are NO, proceed to the 3 oz water test.
Administer 3 oz of water for sequential drinks, note any throat clearing, cough
or change in vocal quality immediately after and 1 minute following the
swallow. If clearing, coughing or change in vocal quality is noted, refer to
speech therapy.
If all of the answers to the above question are NO, then start the patient on a
regular diet.



INFORMED CONSENT FORM
Title of the study: “A STUDY TO ASSESS THE EFFECTIVENESS OF SHORT TERM
FeSS PROTOCOL ON LEVEL OF DEPENDENCY AMONG STROKE PATIENTS
ADMITTED IN STROKE WARD, RAJIV GANDHI GOVERNMENT GENERAL
HOSPITAL, CHENNAI-03”.
Sample no :
Name of the participant :
Name of the principle investigator : Sofia Priyadharsini S
Whether the participant’s consent was asked; yes/no
[If the answer to the above question is yes, write the following phrase:
You agree with the manner to participate in the study].
Name and signature of/ thumb impression of the participant/ parent/guardian.
Name___________________________signature______________________
Date__________________________
Name and signature of the investigator or his representative obtaining consent:
Name____________________________signature___________________
Date _________________________

INFORMATION TO PARTICIPANTS
Title: “A STUDY TO ASSESS THE EFFECTIVENESS OF SHORT TERM FeSS
PROTOCOL ON LEVEL OF DEPENDENCY AMONG STROKE PATIENTS ADMITTED
IN STROKE WARD, RAJIV GANDHI GOVERNMENT GENERAL HOSPITAL,
CHENNAI-03”.
Investigator : Sofia Priyadharsini S
Name of the Participant :
Date :
Age/sex
You are invited to take part in this study. The information in this document is meant to help
you decide whether or not to take part. Please feel free to ask if you have any queries or
concerns.
You are being asked to Cooperative in this study being conducted in selected Institute of
mental health hospital at Chennai.
What is the Purpose of the Research (explain briefly)
This research is conducted to evaluate & to assess the effectiveness of short term fess
protocol on level of dependency among stroke patients admitted in stroke ward, Rajiv Gandhi
Government General Hospital, Chennai-03”.
We have obtained permission from the Institutional Ethics Committee.
Study Procedures
Study will be conducted after approval of ethics committee
A written formal permission will be obtained from authorities of Rajiv Gandhi
Government General Hospital at Chennai to conduct study.
The purpose of study will be explained to the participants.
The investigator will obtain informed consent.
Possible benefits to other people
The result of the research may provide benefits and also empathetic care to them by
investigator.
Confidentiality of the information obtained from you
You have the right to confidentiality regarding the privacy of your personal details. The
information from this study, if published in scientific journals or presented at scientific
meetings, will not reveal your identity.

How will your decision not to participate in the study affect you?
Your decisions not to participate in this research study will not affect your activity of
daily living, medical care or your relationship with investigator or the institution.
Can you decide to stop participating in the study once you start?
The participation in this research is purely voluntary and you have the right to
withdraw from this study at any time during course of the study without giving any reasons.
Your Privacy in the research will be maintained throughout study. In the event of any
publications or presentation resulting from the research, no personally identifiable
information will be shared.
Signature of Investigator Signature of Participants
Date Date

CERTIFICATE OF PLAGIARISM
This is to certify that the dissertation work titled, “A STUDY TO ASSESS
THE EFFECTIVENESS OF SHORT TERM FeSS PROTOCOL ON LEVEL OF
DEPENDENCY AMONG STROKE PATIENTS ADMITTED IN STROKE
WARD, RAJIV GANDHI GOVERNMENT GENERAL HOSPITAL,
CHENNAI-03” of the candidate Ms.SOFIA PRIYADHARSINI.S for the partial
fulfillment of M.Sc. Nursing Programme in the branch of MEDICAL
SURGICAL NURSING has been verified for plagiarism through relevant
plagiarism checker. We found that the uploaded thesis file from introduction to
conclusion pages and rewrite shows ______% of Plagiarism (_____%
uniqueness) in this dissertation.
CLINICAL SPECIALITY GUIDE / SUPERVISOR
Mrs.V.K.R.Periyar Selvi, M.Sc(N).,
Reader in Medical Surgical Nursing,
College of Nursing,
Madras Medical College,
Chennai -03.
PRINCIPAL
Mrs.A.Thahira Begum, M.Sc(N).,MBA., M.Phil.,
Principal,
College of Nursing,
Madras Medical College,
Chennai -03.

1
Barthel Index of Activities of Daily Living
Instructions: Choose the scoring point for the statement that most closely corresponds to the patient's current level of ability for each of the following 10 items. Record actual, not potential, functioning. Information can be obtained from the patient's self-report, from a separate party who is familiar with the patient's abilities (such as a relative), or from observation. Refer to the Guidelines section on the following page for detailed information on scoring and interpretation.
The Barthel Index Bowels 0 = incontinent (or needs to be given enemata) 1 = occasional accident (once/week) 2 = continent Patient's Score: Bladder 0 = incontinent, or catheterized and unable to manage 1 = occasional accident (max. once per 24 hours) 2 = continent (for over 7 days) Patient's Score: Grooming 0 = needs help with personal care 1 = independent face/hair/teeth/shaving (implements provided) Patient's Score: Toilet use 0 = dependent 1 = needs some help, but can do something alone 2 = independent (on and off, dressing, wiping) Patient's Score: Feeding 0 = unable 1 = needs help cutting, spreading butter, etc. 2 = independent (food provided within reach) Patient's Score:
Transfer 0 = unable – no sitting balance 1 = major help (one or two people, physical), can sit 2 = minor help (verbal or physical) 3 = independent Patient's Score: Mobility 0 = immobile 1 = wheelchair independent, including corners, etc. 2 = walks with help of one person (verbal or physical) 3 = independent (but may use any aid, e.g., stick) Patient's Score: Dressing 0 = dependent 1 = needs help, but can do about half unaided 2 = independent (including buttons, zips, laces, etc.) Patient's Score: Stairs 0 = unable 1 = needs help (verbal, physical, carrying aid) 2 = independent up and down Patient's Score: Bathing 0 = dependent 1 = independent (or in shower) Patient's Score: Total Score:
(Collin et al., 1988) Scoring: Sum the patient's scores for each item. Total possible scores range from 0 – 20, with lower scores indicating increased disability. If used to measure improvement after rehabilitation, changes of more than two points in the total score reflect a probable genuine change, and change on one item from fully dependent to independent is also likely to be reliable. Sources: • Collin C, Wade DT, Davies S, Horne V. The Barthel ADL Index: a reliability study. Int Disabil Stud. 1988;10(2):61-63. • Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65. • Wade DT, Collin C. The Barthel ADL Index: a standard measure of physical disability? Int Disabil Stud. 1988;10(2):64-67.

2
Guidelines for the Barthel Index of Activities of Daily Living General • The Index should be used as a record of what a patient does, NOT as a record of what a patient could do. • The main aim is to establish degree of independence from any help, physical or verbal, however minor and for
whatever reason. • The need for supervision renders the patient not independent. • A patient's performance should be established using the best available evidence. Asking the patient,
friends/relatives, and nurses will be the usual source, but direct observation and common sense are also important. However, direct testing is not needed.
• Usually the performance over the preceding 24 – 48 hours is important, but occasionally longer periods will be relevant.
• Unconscious patients should score '0' throughout, even if not yet incontinent. • Middle categories imply that the patient supplies over 50% of the effort. • Use of aids to be independent is allowed.
Bowels (preceding week) • If needs enema from nurse, then 'incontinent.' • 'Occasional' = once a week.
Bladder (preceding week) • 'Occasional' = less than once a day. • A catheterized patient who can completely manage the catheter alone is registered as 'continent.'
Grooming (preceding 24 – 48 hours) • Refers to personal hygiene: doing teeth, fitting false teeth, doing hair, shaving, washing face. Implements can
be provided by helper.
Toilet use • Should be able to reach toilet/commode, undress sufficiently, clean self, dress, and leave. • 'With help' = can wipe self and do some other of above.
Feeding • Able to eat any normal food (not only soft food). Food cooked and served by others, but not cut up. • 'Help' = food cut up, patient feeds self.
Transfer • From bed to chair and back. • 'Dependent' = NO sitting balance (unable to sit); two people to lift. • 'Major help' = one strong/skilled, or two normal people. Can sit up. • 'Minor help' = one person easily, OR needs any supervision for safety.
Mobility • Refers to mobility about house or ward, indoors. May use aid. If in wheelchair, must negotiate corners/doors
unaided. • 'Help' = by one untrained person, including supervision/moral support.
Dressing • Should be able to select and put on all clothes, which may be adapted. • 'Half' = help with buttons, zips, etc. (check!), but can put on some garments alone.
Stairs • Must carry any walking aid used to be independent.
Bathing • Usually the most difficult activity. • Must get in and out unsupervised, and wash self. • Independent in shower = 'independent' if unsupervised/unaided. (Collin et al., 1988)












CHAPTER-I

CHAPTER-II

CHAPTER-III

CHAPTER-IV

CHAPTER-V

CHAPTER-VI

