diffusion tensor imaging of frontal white matter and executive functioning in cocaine-exposed...
TRANSCRIPT

DOI: 10.1542/peds.2006-0003 2006;118;2014-2024 Pediatrics
Stephen J. Blackband Christiana Leonard, Wei Hou, Cynthia Wilson Garvan, Ilona M. Schmalfuss and Tamara Duckworth Warner, Marylou Behnke, Fonda Davis Eyler, Kyle Padgett,
Cocaine-Exposed ChildrenDiffusion Tensor Imaging of Frontal White Matter and Executive Functioning in
http://www.pediatrics.org/cgi/content/full/118/5/2014located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2006 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from

ARTICLE
Diffusion Tensor Imaging of Frontal White Matterand Executive Functioning in Cocaine-ExposedChildrenTamara Duckworth Warner, PhDa, Marylou Behnke, MDa, Fonda Davis Eyler, PhDa, Kyle Padgett, PhDb, Christiana Leonard, PhDc,
Wei Hou, PhDd, Cynthia Wilson Garvan, PhDd, Ilona M. Schmalfuss, MDe,f, Stephen J. Blackband, PhDc,g
Departments of aPediatrics, cNeuroscience, dEpidemiology and Health Policy Research, and eRadiology, College of Medicine, University of Florida, Gainesville, Florida;bDepartment of Radiology, School of Medicine, University of Miami, Miami, Florida; fMalcolm Randall VA Medical Center, Gainesville, Florida; gNational High MagneticField Laboratory, Tallahassee, Florida
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
BACKGROUND. Although animal studies have demonstrated frontal white matter andbehavioral changes resulting from prenatal cocaine exposure, no human studieshave associated neuropsychological deficits in attention and inhibition with brainstructure. We used diffusion tensor imaging to investigate frontal white matterintegrity and executive functioning in cocaine-exposed children.
METHODS. Six direction diffusion tensor images were acquired using a Siemens 3Tscanner with a spin-echo echo-planar imaging pulse sequence on right-handedcocaine-exposed (n � 28) and sociodemographically similar non-exposed children(n � 25; mean age: 10.6 years) drawn from a prospective, longitudinal study.Average diffusion and fractional anisotropy were measured in the left and rightfrontal callosal and frontal projection fibers. Executive functioning was assessedusing two well-validated neuropsychological tests (Stroop color-word test andTrail Making Test).
RESULTS.Cocaine-exposed children showed significantly higher average diffusion inthe left frontal callosal and right frontal projection fibers. Cocaine-exposed chil-dren were also significantly slower on a visual-motor set-shifting task with a trendtoward lower scores on a verbal inhibition task. Controlling for gender andintelligence, average diffusion in the left frontal callosal fibers was related toprenatal exposure to alcohol and marijuana and an interaction between cocaineand marijuana exposure. Performance on the visual-motor set-shifting task wasrelated to prenatal cocaine exposure and an interaction between cocaine andtobacco exposure. Significant correlations were found between test performanceand fractional anisotropy in areas of the frontal white matter.
CONCLUSIONS. Prenatal cocaine exposure, alone and in combination with exposure toother drugs, is associated with slightly poorer executive functioning and subtlemicrostructural changes suggesting less mature development of frontal whitematter pathways. The relative contribution of postnatal environmental factors,including characteristics of the caregiving environment and stressors associatedwith poverty and out-of-home placement, on brain development and behavioralfunctioning in polydrug-exposed children awaits further research.
www.pediatrics.org/cgi/doi/10.1542/peds.2006-0003
doi:10.1542/peds.2006-0003
KeyWordsprenatal exposure, cocaine infants,neuroimaging, cognitive function,neuropsychology
AbbreviationsPCE—prenatal cocaine exposureIQ—intelligence quotientROI—regions of interestDTI—diffusion tensor neuroimagingDav—average diffusionFA—fractional anisotropySES—socioeconomic statusTMT—Trail Making Testdf—degrees of freedom
Accepted for publication Jul 5, 2006
Address correspondence to Tamara D. Warner,PhD, University of Florida, Department ofPediatrics, PO Box 100296, Gainesville, FL32610-0296. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005;Online, 1098-4275). Copyright © 2006 by theAmerican Academy of Pediatrics
2014 WARNER et al at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from

AS COCAINE-EXPOSED CHILDREN reach school age andapproach puberty, many questions remain about
the effects of prenatal cocaine exposure (PCE) on braindevelopment and cognition. In well-controlled prospec-tive studies, subtle deficits among cocaine-exposed chil-dren during the neonatal period and infancy and duringearly childhood have been reported: deficits that couldhave implications for behavioral and academic function-ing. In the first weeks and months of life, slight difficul-ties with attention, arousal, and state regulation werefound in cohorts of children with prenatal exposure tococaine and other drugs.1 In early childhood, cocaine-exposed children have demonstrated problems with vi-sual attention and impulsivity using several differenttesting paradigms including computer-administeredcontinuous performance tasks.2–7 However, with a fewexceptions, most studies examining broad cognitiveskills as measured by standardized intelligence quotient(IQ) tests have revealed no significant negative effects ofPCE.8–12
Problems related to cognition and daily functioningcould emerge as cocaine-exposed children grow olderand have more demands placed on them in school andother settings. A likely domain for later-emerging prob-lems is executive functioning, a diverse set of skillsneeded to engage in independent, purposeful, goal-di-rected behavior.13 Executive functioning includes super-visory and self-regulatory skills that organize, direct, andmanage more basic cognitive, emotional, and behavioralfunctions, especially during active, novel problem solv-ing.14 Specific executive functioning skills include atten-tion control, initiation, inhibition, and shifting betweencognitive tasks. Pathologic and neuroimaging studiessuggest that the underlying neural substrate for execu-tive functions is the prefrontal cortex and its subcorticalconnections.15,16
Animal studies indicate that PCE can result in abnor-mal white matter development. Altered glial morphol-ogy, inappropriate positioning of neurons in white mat-ter areas, and a 100% increase in white matter neuronsin granule and pyramidal cells at postnatal year 3 havebeen demonstrated in nonhuman primate studies ofPCE.17 Investigations using rodents have shown de-creased astroglial proliferation and increased density ofless mature radial glial cells.18
The possibility of white matter abnormalities in co-caine-exposed children has been suggested by 2 well-controlled physiologic studies of brain development inprospectively enrolled samples. One study using quanti-tative electroencephalographic sleep recordings foundthat PCE was associated with lower spectral correlationsbetween homologous brain regions at birth and lowerspectral power values at birth and 1 year, suggestingfewer interhemispheric neuronal connections or delayeddevelopment of these connections.19 Another study us-ing auditory brainstem response measures revealed that
heavy PCE was associated with prolonged interpeak la-tencies, indicating slower neural transmission and de-layed brain maturation.20
To date, very little neuroimaging has been conductedwith cocaine-exposed children. One study21 using pro-ton magnetic resonance spectroscopy (N � 26) found nogross structural abnormalities, no volumetric differencesfor the whole brain and 7 regions of interest (ROIs), andno differences for 4 of 5 metabolite concentrations mea-sured in the frontal lobe and striatum. Cocaine-exposedchildren did, however, show a 13% increase in frontalwhite matter creatine levels with trends for decreasedmidbrain volume bilaterally and a decreased ratio ofcholine-containing compounds to creatine in frontalwhite matter.21
Diffusion tensor neuroimaging (DTI), a noninvasiveprocedure that uses MRI to investigate white mattermicrostructure, has ushered in a new era for the study ofbrain development. In simple terms, DTI involves mea-suring the movement (diffusion) of water molecules intissues and determining the extent to which the diffu-sion is directionally independent (isotropic) and direc-tionally dependent (anisotropic). Diffusion is moreanisotropic in white matter than gray matter because themovement of water molecules is restricted by cell mem-branes and the myelin sheaths surrounding axons. Inaddition, water molecules are thought to move fasterand longer distances along the white matter fibers ratherthan perpendicular to them. Water diffusion is repre-sented quantitatively by the average diffusion (Dav) co-efficient, which provides a measure of isotropic diffu-sion, as well as by a number of measures of anisotropicdiffusion, such as fractional anisotropy (FA). The FAindex provides a scale- and orientation-independentmeasure of diffusion with values ranging from 0 (isotro-pic) to 1 (completely anisotropic).22 More detailed re-views of the technical aspects of DTI can be found else-where.23–26
Maturation of white matter tracts in children can betraced by examining changes in Dav and anisotropicdiffusion over time or in different age groups. A numberof investigators have demonstrated convincingly in lon-gitudinal and cross-sectional designs that DTI can be apowerful tool for evaluating white matter developmentin normally developing children27–36 and children withproblems ranging from leukodystrophy37 to prematuri-ty38 to developmental delay.39 In the brain as a whole,Dav has been shown to decrease significantly during thefirst year of life, reaching adult levels by age 7 years,whereas measures of anisotropy increase significantlywith development. Changes in white matter anisotropytake place in different regions of the brain at differentrates with, for example, posterior areas (visual cortexand posterior limb of the internal capsule) maturingbefore anterior areas (anterior limb of the internal cap-sule).40 Anisotropic diffusion changes reflect maturation
PEDIATRICS Volume 118, Number 5, November 2006 2015 at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from

of white matter microstructure but cannot be inter-preted solely as the result of increased myelination be-cause changes in anisotropy have been found in theabsence of myelin.23,40
Using DTI to explore relationships between cognitiveabilities and white matter microstructure in children andadolescents is still in its nascent stages, particularly incomparison to volumetric studies.41 A review by Moseleyet al42 revealed that the majority of DTI studies examin-ing cognitive performance have used adults and focusedon aging or disease-related cognitive decline (eg, multi-ple sclerosis). Two DTI studies have found that perfor-mance on reading and related measures is correlatedwith anisotropy measures in the left temporoparietalregion in both children43 and adults.44 A study of 8- to18-year-olds combining DTI and functional MRI foundsignificant correlations between FA in frontoparietalwhite matter and brain activity in the superior frontalsulcus and inferior parietal lobe during a working mem-ory task.45 In terms of executive functioning, a numberof functional MRI studies have found significant age-related differences among children, adolescents, andadults using a variety of tasks41; however, no DTI studiesrelating white matter development and executive func-tioning could be found in the extant literature.
The threefold purpose of the current study was: (1) tocompare cocaine-exposed and nonexposed children onDTI measures of frontal white matter development andon measures of executive functioning; (2) to determinewhether there are significant associations between fron-tal white matter development and executive function-ing; and (3) to test for the effects of PCE, both alone andin combination with other prenatal drug exposures, onfrontal white matter development and on executivefunctioning. We hypothesized that cocaine-exposedchildren would show significantly less mature frontalwhite development (indicated by higher Dav and lowerFA values) and significantly poorer performance on ex-ecutive functioning measures (as indicated by slowertime to completion and fewer items completed) thannonexposed children. We also expected to find signifi-cant correlations between frontal white matter DTI mea-sures and executive functioning test performance.
METHODS
ProceduresStudy approval was granted by the University of FloridaInstitutional Review Board, and a federal Certificate ofConfidentiality protects the confidentiality of the data.Participants (N � 53) were drawn from a prospective,longitudinal study on the developmental effects of PCEthat began in 1991. A separate informed consent fromthe child’s primary caregiver and assent by the childwere obtained before the current study. Detailed infor-mation about the enrollment of the participants in the
larger longitudinal study has been published previous-ly.46 Briefly, pregnant women with no chronic illnessthat might affect pregnancy outcome or fetal develop-ment were recruited for the longitudinal study whenthey first entered prenatal care or, in the case of noprenatal care, at delivery. Women who admitted use ortested urine-positive for illegal drugs other than cocaineor marijuana were excluded from the study. A total of308 women (154 cocaine users and 154 nonusers)matched on race, parity, socioeconomic status (SES)(A.B. Hollingshead, PhD, Four-Factor Index of Social Status,unpublished manual, 1975), and location of prenatalcare (which was related to prenatal risk factors) wereenrolled in the parent study. Cocaine users were identi-fied by private, structured interviews conducted by ex-perienced female research staff and/or positive urinescreens confirmed by gas chromatography/mass spec-trometry. Executive functioning measures were col-lected during the 10-year follow-up evaluation by aschool psychologist blinded to the children’s drug expo-sure status.
ParticipantsOf the surviving 296 children, 263 (89%) participated inthe 10-year follow-up assessment and completed all ofthe outcome measures. Families who lived within 2hours of the study site, which reflects the area fromwhich the original sample was drawn, were recruited bya brochure describing the study followed by a telephonecall, when possible. Left-handed children and menstru-ating girls were excluded from the study. Of the 78families who were contacted by telephone and met cri-teria, 18 were not willing or able to participate. Of the 60children enrolled, 53 had data that could be analyzed forthe purposes of this study. The MRI studies of the re-maining 7 children were incomplete or collected usingdifferent imaging parameters.
Descriptive data for the participants (cocaine-ex-posed: n � 28; nonexposed: n � 25) are shown in Table1. The current sample closely resembles the full cohortoriginally enrolled in the longitudinal study. Maternalcharacteristics for the cocaine-exposed and comparisonchildren in the current study did not differ on the 4matching variables used to select the original cohort(race, parity, SES, and location of prenatal care). Vari-ables that differed significantly in the originally enrolledcohort but did not in the current sample (although Pvalues were � .10) were mean maternal age at delivery,week that the mothers entered prenatal care, and HobelPrenatal Risk scores. As in the original cohort, cocaine-exposed children were exposed to much greateramounts of tobacco, alcohol, and marijuana.
In terms of birth outcome measures, the children inthe current study were, on average, term infants withbirth weights and head circumferences within normallimits. None was small for gestational age at birth, had a
2016 WARNER et al at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from
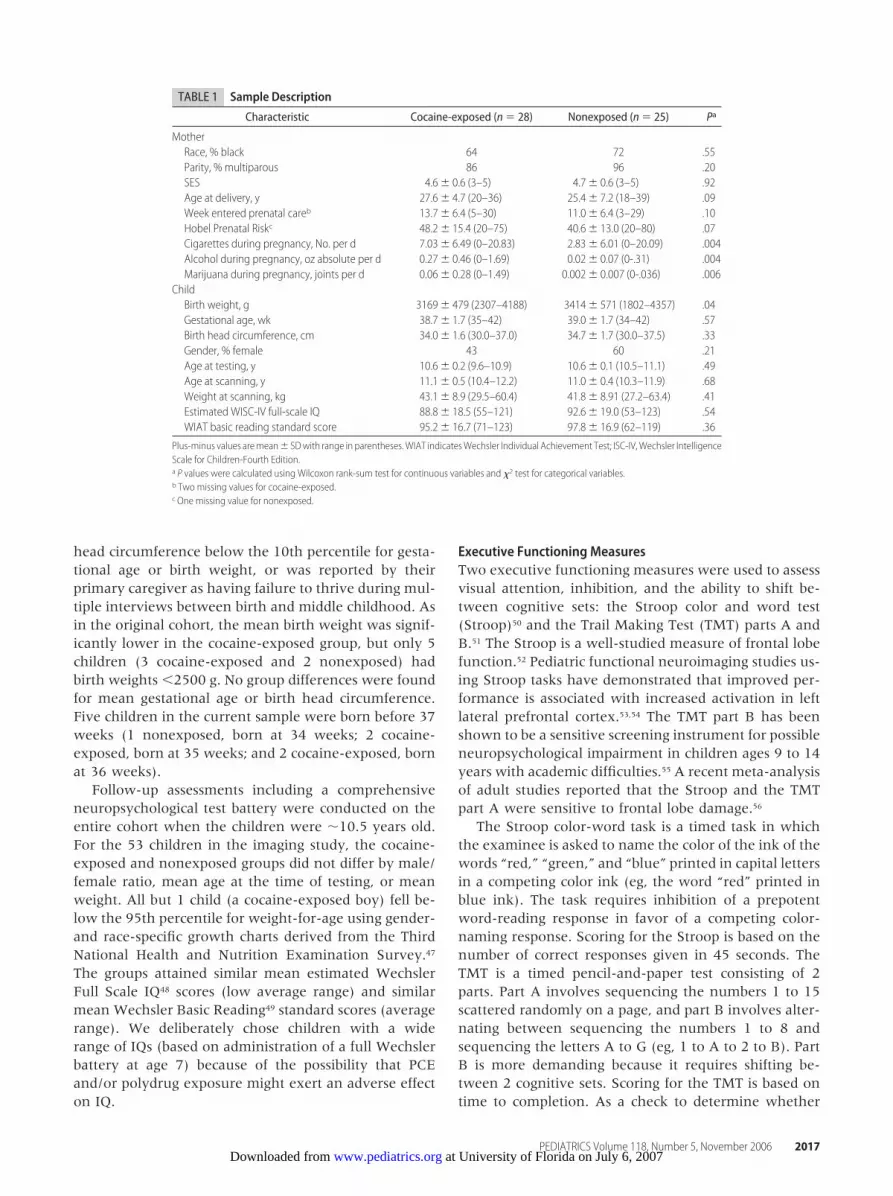
head circumference below the 10th percentile for gesta-tional age or birth weight, or was reported by theirprimary caregiver as having failure to thrive during mul-tiple interviews between birth and middle childhood. Asin the original cohort, the mean birth weight was signif-icantly lower in the cocaine-exposed group, but only 5children (3 cocaine-exposed and 2 nonexposed) hadbirth weights �2500 g. No group differences were foundfor mean gestational age or birth head circumference.Five children in the current sample were born before 37weeks (1 nonexposed, born at 34 weeks; 2 cocaine-exposed, born at 35 weeks; and 2 cocaine-exposed, bornat 36 weeks).
Follow-up assessments including a comprehensiveneuropsychological test battery were conducted on theentire cohort when the children were �10.5 years old.For the 53 children in the imaging study, the cocaine-exposed and nonexposed groups did not differ by male/female ratio, mean age at the time of testing, or meanweight. All but 1 child (a cocaine-exposed boy) fell be-low the 95th percentile for weight-for-age using gender-and race-specific growth charts derived from the ThirdNational Health and Nutrition Examination Survey.47
The groups attained similar mean estimated WechslerFull Scale IQ48 scores (low average range) and similarmean Wechsler Basic Reading49 standard scores (averagerange). We deliberately chose children with a widerange of IQs (based on administration of a full Wechslerbattery at age 7) because of the possibility that PCEand/or polydrug exposure might exert an adverse effecton IQ.
Executive Functioning MeasuresTwo executive functioning measures were used to assessvisual attention, inhibition, and the ability to shift be-tween cognitive sets: the Stroop color and word test(Stroop)50 and the Trail Making Test (TMT) parts A andB.51 The Stroop is a well-studied measure of frontal lobefunction.52 Pediatric functional neuroimaging studies us-ing Stroop tasks have demonstrated that improved per-formance is associated with increased activation in leftlateral prefrontal cortex.53,54 The TMT part B has beenshown to be a sensitive screening instrument for possibleneuropsychological impairment in children ages 9 to 14years with academic difficulties.55 A recent meta-analysisof adult studies reported that the Stroop and the TMTpart A were sensitive to frontal lobe damage.56
The Stroop color-word task is a timed task in whichthe examinee is asked to name the color of the ink of thewords “red,” “green,” and “blue” printed in capital lettersin a competing color ink (eg, the word “red” printed inblue ink). The task requires inhibition of a prepotentword-reading response in favor of a competing color-naming response. Scoring for the Stroop is based on thenumber of correct responses given in 45 seconds. TheTMT is a timed pencil-and-paper test consisting of 2parts. Part A involves sequencing the numbers 1 to 15scattered randomly on a page, and part B involves alter-nating between sequencing the numbers 1 to 8 andsequencing the letters A to G (eg, 1 to A to 2 to B). PartB is more demanding because it requires shifting be-tween 2 cognitive sets. Scoring for the TMT is based ontime to completion. As a check to determine whether
TABLE 1 Sample Description
Characteristic Cocaine-exposed (n � 28) Nonexposed (n � 25) Pa
MotherRace, % black 64 72 .55Parity, % multiparous 86 96 .20SES 4.6� 0.6 (3–5) 4.7� 0.6 (3–5) .92Age at delivery, y 27.6� 4.7 (20–36) 25.4� 7.2 (18–39) .09Week entered prenatal careb 13.7� 6.4 (5–30) 11.0� 6.4 (3–29) .10Hobel Prenatal Riskc 48.2� 15.4 (20–75) 40.6� 13.0 (20–80) .07Cigarettes during pregnancy, No. per d 7.03� 6.49 (0–20.83) 2.83� 6.01 (0–20.09) .004Alcohol during pregnancy, oz absolute per d 0.27� 0.46 (0–1.69) 0.02� 0.07 (0-.31) .004Marijuana during pregnancy, joints per d 0.06� 0.28 (0–1.49) 0.002� 0.007 (0-.036) .006
ChildBirth weight, g 3169� 479 (2307–4188) 3414� 571 (1802–4357) .04Gestational age, wk 38.7� 1.7 (35–42) 39.0� 1.7 (34–42) .57Birth head circumference, cm 34.0� 1.6 (30.0–37.0) 34.7� 1.7 (30.0–37.5) .33Gender, % female 43 60 .21Age at testing, y 10.6� 0.2 (9.6–10.9) 10.6� 0.1 (10.5–11.1) .49Age at scanning, y 11.1� 0.5 (10.4–12.2) 11.0� 0.4 (10.3–11.9) .68Weight at scanning, kg 43.1� 8.9 (29.5–60.4) 41.8� 8.91 (27.2–63.4) .41Estimated WISC-IV full-scale IQ 88.8� 18.5 (55–121) 92.6� 19.0 (53–123) .54WIAT basic reading standard score 95.2� 16.7 (71–123) 97.8� 16.9 (62–119) .36
Plus-minus values aremean� SDwith range in parentheses.WIAT indicatesWechsler Individual Achievement Test; ISC-IV,Wechsler IntelligenceScale for Children-Fourth Edition.a P values were calculated using Wilcoxon rank-sum test for continuous variables and �2 test for categorical variables.b Two missing values for cocaine-exposed.c One missing value for nonexposed.
PEDIATRICS Volume 118, Number 5, November 2006 2017 at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from

the Stroop and TMT were tapping similar aspects ofexecutive functioning, we examined correlations be-tween the 2 measures. As expected, a significant linearrelationship was found between the TMT part B and theStroop color-word score (r � �.30; P � .03).
Imaging Data CollectionImaging data were collected when the children werebetween 10 and 12 years old (mean: 11.0 � .4 years;range: 10.3–12.2 years). There was no significant differ-ence in age at the time of scanning between the 2 groups(Table 1). Imaging was performed using a Siemens 3TAllegra MRI scanner (Siemens, Iselin, NJ). ConventionalMRI sequences (axial fluid-attenuated inversion recov-ery and volumetric T1-weighted images) were obtainedto detect possible confounding pathology. DTI acquisi-tion used a spin-echo diffusion-weighted echo planarimaging pulse sequence with � values of 0, 250, and1000 seconds/mm2, 3.5-mm slice thickness, 210 � 210cm field of view, 128 � 128 matrix, 4200-ms repetitiontime, 90-ms echo time, and 4 excitations. Total acquisi-tion time was 4 minutes.
Image ProcessingConventional images were assessed for the presence ofabnormal anatomy and signal intensities by a board-certified radiologist who holds an additional certificate ofqualification in neuroradiology (I.M.S.). Dav and FAmaps were generated using in-house software.57 ROIswere measured using a semiautomated segmentationmethod, which involves hand drawing an ROI aroundthe target anatomic structure, then applying a pixel-based threshold to shrink the boundaries of the region.This method has been described in detail elsewhere andhas been shown to have high interrater and intraraterreliability.58
Two separate fiber pathways, medial and lateral fibersextending anteriorly into the frontal lobe white matter,could be discerned on the axial DTI sections. We termedthe medial fibers the “frontal callosal fibers” and thelateral fibers the “frontal projection fibers.” The frontalcallosal fibers project to the opposite hemispherethrough the corpus callosum. The frontal projection fi-bers contain afferent and efferent fibers that projectbetween a number of frontal and subcortical areas, in-cluding the dorsolateral prefrontal cortex (which is as-sociated with executive functioning), caudate, dorsome-dial nucleus of the thalamus, and reticular formation.The longer frontal projection fibers course through theinternal capsule and the cerebral peduncles. Measure-ments were made on the axial section that showed bothpathways. Figure 1 shows a sample image with an out-line of the white matter ROIs.
Statistical AnalysesSAS 8.2 (SAS Inc, Cary, NC) was used to conduct datascreening and all of the statistical analyses. Group com-parisons were made using the Wilcoxon rank-sum testfor continuous data and the �2 statistic for categoricaldata. Correlation coefficients were computed usingSpearman’s r. Multiple regression analyses were con-ducted to assess the unique contribution of PCE aloneand in combination with other variables. The criterionfor significance tests was set at � � .05, 2-tailed. Becauseneuroimaging in cocaine-exposed children represents anew area of inquiry, trends toward significance (� � .10)are reported, as well as results that meet the conven-tional criterion.
RESULTSTo evaluate the hypothesis that cocaine-exposed chil-dren would demonstrate diffusion measures associatedwith less optimal white matter integrity, the mean Dav
and FA of the groups were compared. As shown in Table2, the cocaine-exposed children had significantly higherDav in the left frontal callosal fibers (P � .02) and rightfrontal projection fibers (P � .03). The cocaine-exposedchildren also had higher Dav in the right frontal callosalfibers, but the difference from the comparison group (P� .09) did not meet the conventional criterion for sig-nificance.
FIGURE 1Axial image showingwhitematter ROIs. RFP indicates right frontal projection fibers; RFC,right frontal callosal fibers; LFC, left frontal callosal fibers; LFP, left frontal projection fibers.
2018 WARNER et al at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from
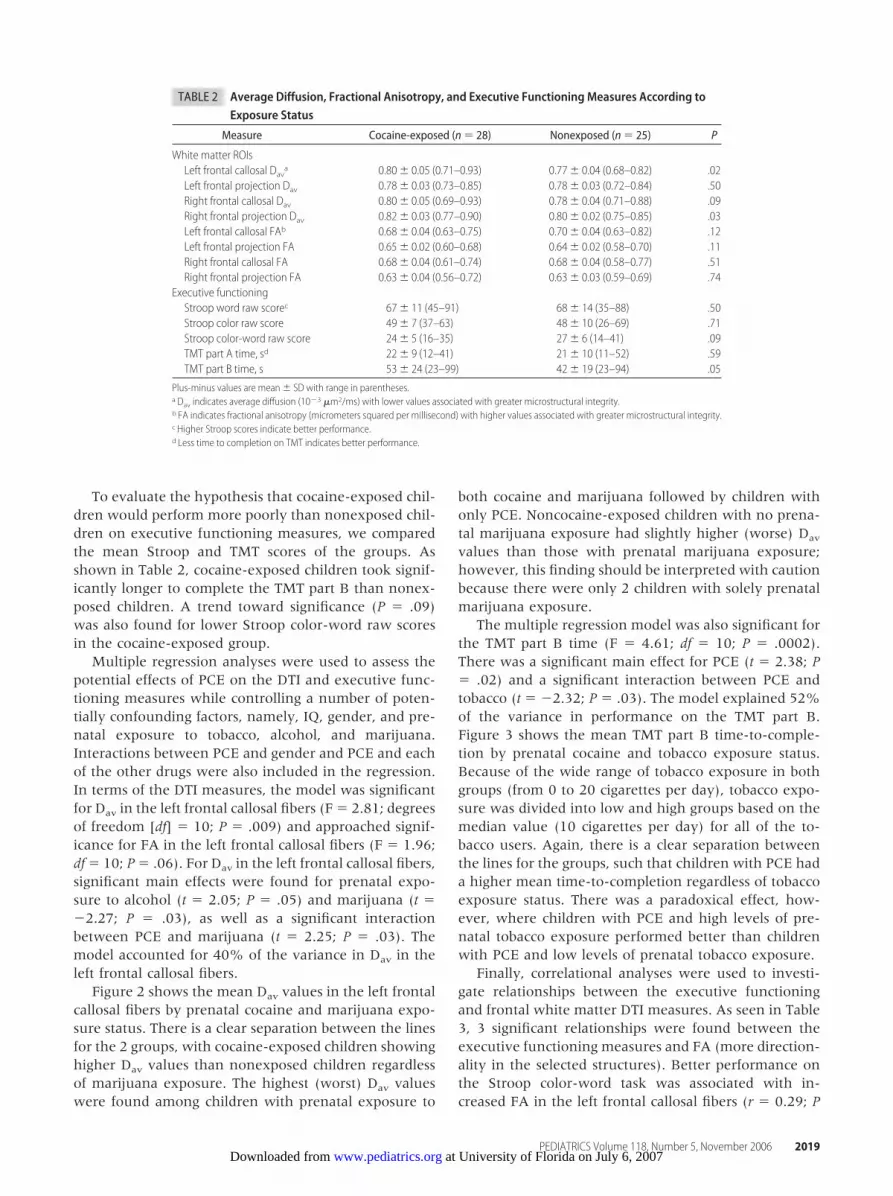
To evaluate the hypothesis that cocaine-exposed chil-dren would perform more poorly than nonexposed chil-dren on executive functioning measures, we comparedthe mean Stroop and TMT scores of the groups. Asshown in Table 2, cocaine-exposed children took signif-icantly longer to complete the TMT part B than nonex-posed children. A trend toward significance (P � .09)was also found for lower Stroop color-word raw scoresin the cocaine-exposed group.
Multiple regression analyses were used to assess thepotential effects of PCE on the DTI and executive func-tioning measures while controlling a number of poten-tially confounding factors, namely, IQ, gender, and pre-natal exposure to tobacco, alcohol, and marijuana.Interactions between PCE and gender and PCE and eachof the other drugs were also included in the regression.In terms of the DTI measures, the model was significantfor Dav in the left frontal callosal fibers (F � 2.81; degreesof freedom [df] � 10; P � .009) and approached signif-icance for FA in the left frontal callosal fibers (F � 1.96;df � 10; P � .06). For Dav in the left frontal callosal fibers,significant main effects were found for prenatal expo-sure to alcohol (t � 2.05; P � .05) and marijuana (t ��2.27; P � .03), as well as a significant interactionbetween PCE and marijuana (t � 2.25; P � .03). Themodel accounted for 40% of the variance in Dav in theleft frontal callosal fibers.
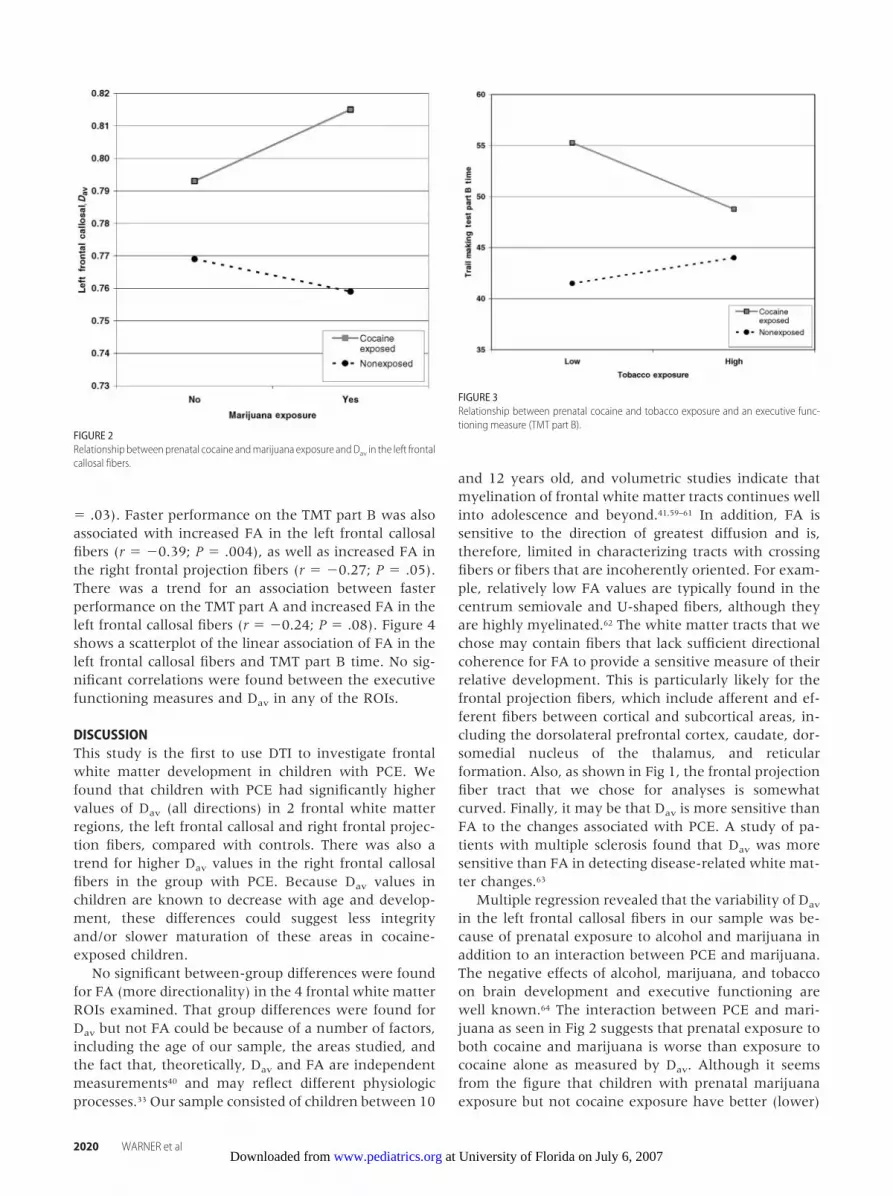
Figure 2 shows the mean Dav values in the left frontalcallosal fibers by prenatal cocaine and marijuana expo-sure status. There is a clear separation between the linesfor the 2 groups, with cocaine-exposed children showinghigher Dav values than nonexposed children regardlessof marijuana exposure. The highest (worst) Dav valueswere found among children with prenatal exposure to
both cocaine and marijuana followed by children withonly PCE. Noncocaine-exposed children with no prena-tal marijuana exposure had slightly higher (worse) Dav
values than those with prenatal marijuana exposure;however, this finding should be interpreted with cautionbecause there were only 2 children with solely prenatalmarijuana exposure.
The multiple regression model was also significant forthe TMT part B time (F � 4.61; df � 10; P � .0002).There was a significant main effect for PCE (t � 2.38; P� .02) and a significant interaction between PCE andtobacco (t � �2.32; P � .03). The model explained 52%of the variance in performance on the TMT part B.Figure 3 shows the mean TMT part B time-to-comple-tion by prenatal cocaine and tobacco exposure status.Because of the wide range of tobacco exposure in bothgroups (from 0 to 20 cigarettes per day), tobacco expo-sure was divided into low and high groups based on themedian value (10 cigarettes per day) for all of the to-bacco users. Again, there is a clear separation betweenthe lines for the groups, such that children with PCE hada higher mean time-to-completion regardless of tobaccoexposure status. There was a paradoxical effect, how-ever, where children with PCE and high levels of pre-natal tobacco exposure performed better than childrenwith PCE and low levels of prenatal tobacco exposure.
Finally, correlational analyses were used to investi-gate relationships between the executive functioningand frontal white matter DTI measures. As seen in Table3, 3 significant relationships were found between theexecutive functioning measures and FA (more direction-ality in the selected structures). Better performance onthe Stroop color-word task was associated with in-creased FA in the left frontal callosal fibers (r � 0.29; P
TABLE 2 Average Diffusion, Fractional Anisotropy, and Executive Functioning Measures According toExposure Status
Measure Cocaine-exposed (n � 28) Nonexposed (n � 25) P
White matter ROIsLeft frontal callosal Dava 0.80� 0.05 (0.71–0.93) 0.77� 0.04 (0.68–0.82) .02Left frontal projection Dav 0.78� 0.03 (0.73–0.85) 0.78� 0.03 (0.72–0.84) .50Right frontal callosal Dav 0.80� 0.05 (0.69–0.93) 0.78� 0.04 (0.71–0.88) .09Right frontal projection Dav 0.82� 0.03 (0.77–0.90) 0.80� 0.02 (0.75–0.85) .03Left frontal callosal FAb 0.68� 0.04 (0.63–0.75) 0.70� 0.04 (0.63–0.82) .12Left frontal projection FA 0.65� 0.02 (0.60–0.68) 0.64� 0.02 (0.58–0.70) .11Right frontal callosal FA 0.68� 0.04 (0.61–0.74) 0.68� 0.04 (0.58–0.77) .51Right frontal projection FA 0.63� 0.04 (0.56–0.72) 0.63� 0.03 (0.59–0.69) .74
Executive functioningStroop word raw scorec 67� 11 (45–91) 68� 14 (35–88) .50Stroop color raw score 49� 7 (37–63) 48� 10 (26–69) .71Stroop color-word raw score 24� 5 (16–35) 27� 6 (14–41) .09TMT part A time, sd 22� 9 (12–41) 21� 10 (11–52) .59TMT part B time, s 53� 24 (23–99) 42� 19 (23–94) .05
Plus-minus values are mean � SD with range in parentheses.a Dav indicates average diffusion (10�3 �m2/ms) with lower values associated with greater microstructural integrity.b FA indicates fractional anisotropy (micrometers squared per millisecond) with higher values associated with greater microstructural integrity.c Higher Stroop scores indicate better performance.d Less time to completion on TMT indicates better performance.
PEDIATRICS Volume 118, Number 5, November 2006 2019 at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from
� .03). Faster performance on the TMT part B was alsoassociated with increased FA in the left frontal callosalfibers (r � �0.39; P � .004), as well as increased FA inthe right frontal projection fibers (r � �0.27; P � .05).There was a trend for an association between fasterperformance on the TMT part A and increased FA in theleft frontal callosal fibers (r � �0.24; P � .08). Figure 4shows a scatterplot of the linear association of FA in theleft frontal callosal fibers and TMT part B time. No sig-nificant correlations were found between the executivefunctioning measures and Dav in any of the ROIs.
DISCUSSIONThis study is the first to use DTI to investigate frontalwhite matter development in children with PCE. Wefound that children with PCE had significantly highervalues of Dav (all directions) in 2 frontal white matterregions, the left frontal callosal and right frontal projec-tion fibers, compared with controls. There was also atrend for higher Dav values in the right frontal callosalfibers in the group with PCE. Because Dav values inchildren are known to decrease with age and develop-ment, these differences could suggest less integrityand/or slower maturation of these areas in cocaine-exposed children.
No significant between-group differences were foundfor FA (more directionality) in the 4 frontal white matterROIs examined. That group differences were found forDav but not FA could be because of a number of factors,including the age of our sample, the areas studied, andthe fact that, theoretically, Dav and FA are independentmeasurements40 and may reflect different physiologicprocesses.33 Our sample consisted of children between 10
and 12 years old, and volumetric studies indicate thatmyelination of frontal white matter tracts continues wellinto adolescence and beyond.41,59–61 In addition, FA issensitive to the direction of greatest diffusion and is,therefore, limited in characterizing tracts with crossingfibers or fibers that are incoherently oriented. For exam-ple, relatively low FA values are typically found in thecentrum semiovale and U-shaped fibers, although theyare highly myelinated.62 The white matter tracts that wechose may contain fibers that lack sufficient directionalcoherence for FA to provide a sensitive measure of theirrelative development. This is particularly likely for thefrontal projection fibers, which include afferent and ef-ferent fibers between cortical and subcortical areas, in-cluding the dorsolateral prefrontal cortex, caudate, dor-somedial nucleus of the thalamus, and reticularformation. Also, as shown in Fig 1, the frontal projectionfiber tract that we chose for analyses is somewhatcurved. Finally, it may be that Dav is more sensitive thanFA to the changes associated with PCE. A study of pa-tients with multiple sclerosis found that Dav was moresensitive than FA in detecting disease-related white mat-ter changes.63
Multiple regression revealed that the variability of Dav
in the left frontal callosal fibers in our sample was be-cause of prenatal exposure to alcohol and marijuana inaddition to an interaction between PCE and marijuana.The negative effects of alcohol, marijuana, and tobaccoon brain development and executive functioning arewell known.64 The interaction between PCE and mari-juana as seen in Fig 2 suggests that prenatal exposure toboth cocaine and marijuana is worse than exposure tococaine alone as measured by Dav. Although it seemsfrom the figure that children with prenatal marijuanaexposure but not cocaine exposure have better (lower)
FIGURE 2Relationship betweenprenatal cocaine andmarijuana exposure andDav in the left frontalcallosal fibers.
FIGURE 3Relationship between prenatal cocaine and tobacco exposure and an executive func-tioning measure (TMT part B).
2020 WARNER et al at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from

Dav, there were only 2 children in this group, castingdoubt on the reliability of this finding.
This study also examined performance on 2 executivefunctioning measures in children with PCE. We foundthat the cocaine-exposed group was significantly sloweron average than nonexposed children in completing atimed task that involves shifting between sequencingnumbers and sequencing letters (TMT part B). Cocaine-exposed children also performed more poorly, althoughnot significantly, on a timed task that requires inhibitionof reading a color word in favor of naming the compet-ing color ink in which the word is printed (Stroop color-word task). Poorer executive functioning in the cocaine-exposed children is consistent with other reports in theliterature of visual attention and motor inhibition diffi-culties in this population.2–7 A multiple regression anal-ysis showed that performance on the TMT part B wassignificantly predicted by PCE and an interaction withPCE and prenatal tobacco exposure. Paradoxically, how-ever, children with PCE and higher levels of prenataltobacco exposure were faster rather than slower at com-
pleting the task than children with PCE and lower levelsof tobacco exposure.
Finally, this study demonstrates a brain-behavior re-lationship between frontal white matter anisotropy andexecutive functioning performance. In the sample as awhole, better performance on both executive function-ing measures was associated with greater anisotropicdiffusion (FA) in the left frontal callosal fibers. Fasterperformance on the set-shifting task (TMT part B) wasalso associated with greater anisotropic diffusion (FA) inthe right frontal projection fibers.
The association between Stroop color-word scoresand FA in left frontal callosal fibers may be related to theverbal nature of the test and the fact that children mayrequire bilateral hemispheric coordination to completethe task. Adleman et al53 showed that developmentallyspecific Stroop-related activation of the left prefrontalcortex begins in adolescence and increases through earlyadulthood. The immature left hemisphere specializationin children could also explain why no association wasfound between Stroop performance and FA in the leftfrontal projection fibers that emanate from the prefron-tal cortex. The association between the TMT part B per-formance and left frontal callosal FA may also be relatedto the language demands of the task (interpreting lettersand numbers), whereas the association between TMTpart B performance and right frontal projection FA maybe because of the visual-spatial nature of the task (draw-ing lines to sequence symbols scattered randomly on apage). Functional MRI studies that evaluate activationpatterns associated with the various task components ofthe TMT could further elucidate these brain-behaviorrelationships.
The significant correlations between one of the exec-utive functioning measures and FA but not Dav is notunexpected. The few studies that have correlated cogni-tive performance with DTI measures have only usedanisotropy measures.42 Use of anisotropy measures islogical as a marker of myelination and axonal thickness,particularly in adults for whom brain maturation is con-sidered complete. Notably, the single DTI study of cog-
TABLE 3 Correlations Between Frontal White Matter Diffusion and Executive Functioning Measures(N � 53)
Variable Stroop Color-Word Raw Score TMT Part A Time, s TMT Part B Time, s
Left frontal callosal Dav �0.11 �0.16 �0.16Left frontal projection Dav �0.05 �0.14 0.05Right frontal callosal Dav �0.03 �0.13 �0.07Right frontal projection Dav 0.06 0.10 0.10Left frontal callosal FA 0.29b �0.24c �0.39a
Left frontal projection FA �0.09 0.11 �0.01Right frontal callosal FA 0.10 �0.19 �0.20Right frontal projection FA 0.14 �0.19 �0.27b
Dav indicates average diffusion (micrometers squared per millisecond); FA, fractional anisotropy (micrometers squared per millisecond).a P � .01.b P � .05.c P � .10.
FIGURE 4Scatterplot and regression line showing the significant correlation between an executivefunctioning measure (TMT part B time) and FA in the left frontal callosal fibers.
PEDIATRICS Volume 118, Number 5, November 2006 2021 at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from

nitive performance in children ages 7 to 13 years foundsignificant correlations with FA in a temporoparietalarea but not in a frontal area. We chose to examinepossible correlations with Dav in part because there areso few data on the association between DTI and cogni-tion in children and none in children with PCE. Inaddition, we thought that Dav may provide as useful anindex of frontal lobe white matter development as FA inour sample of 10.5-year-olds, whose frontal lobes areexpected to be less myelinated relative posterior corticalareas.
The study findings are presented as the first pieces ofa puzzle designed to elucidate the effects of PCE on thedeveloping brain. Many questions remain unanswered.For example, it is curious to us that the between-groupdifferences were found for Dav in the left frontal callosaland right projection fibers but the significant correlationsbetween one of the executive functioning measures waswith FA for these same 2 structures. Also, the state of thescience does not allow us to speculate as to laterality ofthe group differences in Dav (ie, higher Dav in callosalfibers on the left and the projection fibers on the right inthe cocaine-exposed group). In addition, the paradoxicalfinding that PCE in combination with higher levels ofprenatal tobacco exposure was associated with betterexecutive functioning warrants further investigation andreplication.
In future studies, we would like to evaluate the rel-ative contribution of postnatal environmental factors onbrain development and cognitive functioning in cocaine-exposed children. Environmental factors have beenfound to influence the development of executive func-tioning in typically developing children65 and the devel-opment of dopaminergic innervation of the prefrontalcortex in laboratory animals.66,67 The deleterious effectsof trauma, maltreatment, and abuse on brain develop-ment have been shown in terms of total cerebral volumeand changes in evoked related potentials and electroen-cephalogram studies.68 For children with PCE, a numberof studies have indicated that postnatal environmentalfactors, such as maternal psychological functioning, thecaregiving environment, and early intervention, mayhave effects that are equal to, if not more importantthan, prenatal drug exposure on child function-ing.9,10,69–71 The possible effects on brain development ofstressors associated with poverty and out-of-homeplacement early in life for the children with PCE in ourcohort72 merit close consideration as well.
CONCLUSIONTo better understand the outcomes of cocaine-exposedchildren, investigations will need to account for the ter-atogenic effects of multiple prenatal drug exposures andtheir possible interactions in the context of a variety ofother environmental risk factors.
ACKNOWLEDGMENTSFinancial support was provided by National Institutes ofHealth grants R01-DA05854 (to Drs Eyler and Behnke),R01-NF36992 (Dr Blackband), and the National HighMagnetic Field Laboratory. MRI data were obtained atthe Advanced Magnetic Resonance Imaging and Spec-troscopy facility in the McKnight Brain Institute of theUniversity of Florida.
We acknowledge the assistance of Ann Welch forcoordination of the project, Vijay Komaragiri for datamanagement, Kenneth Crandall for manual anatomicaltracing, and Eric Corpus for article preparation.
REFERENCES1. Eyler FD, Behnke M. Early development of infants exposed to
drugs prenatally. Clin. Perinatol. 1999;26:107–1502. Bandstra ES, Morrow CE, Anthony JC, Accornero VH, Fried
PA. Longitudinal investigation of task persistence and sus-tained attention in children with prenatal cocaine exposure.Neurotoxicol Teratol. 2001;23:545–559
3. Bendersky M, Gambini G, Lastella A, Bennett DS, Lewis M.Inhibitory motor control at five years as a function of prenatalcocaine exposure. J Dev Behav Pediatr. 2003;24:345–351
4. Leech SL, Richardson GA, Goldschmidt L, Day NL. Prenatalsubstance exposure: effects on attention and impulsivity of6-year olds. Neurotoxicol Teratol. 1999;21:109–118
5. Noland JS, Singer LT, Short EJ, et al. Prenatal drug exposureand selective attention in preschoolers. Neurotoxicol Teratol.2005;27:429–438
6. Richardson GA, Conroy ML, Day NL. Prenatal cocaineexposure: Effects on the development of school-age children.Neurotoxicol Teratol. 1996;18:627–634
7. Savage J, Brodsky NL, Malmud E, Giannetta JM, Hurt H.Attentional functioning and impulse control in cocaine-exposed and control children at age ten years. J Dev BehavPediatr. 2005;26:42–47
8. Frank DA, Augustyn M, Knight WG, Pell T, Zuckerman B.Growth, development, and behavior in early childhood follow-ing prenatal cocaine exposure: A systematic review. JAMA.2001;285:1613–1625
9. Bennett DS, Bendersky M, Lewis M. Children’s intellectual andemotional-behavioral adjustment at 4 years as a function ofcocaine exposure, maternal characteristics, and environmentalrisk. Dev Psychol. 2002;38:648–658
10. Arendt RE, Short EJ, Singer LT, et al. Children prenatallyexposed to cocaine: Developmental outcomes and environ-mental risks at seven years of age. J Dev Behav Pediatr. 2004;25:83–90
11. Singer LT, Minnes S, Short E, et al. Cognitive outcomes ofpreschool children with prenatal cocaine exposure. JAMA.2004;291:2448–2456
12. Frank DA, Rose-Jacobs R, Beeghly M, Wilbur M, Bellinger D,Cabral H. Level of prenatal cocaine exposure and 48-month IQ:Importance of preschool enrichment. Neurotoxicol Teratol. 2005;27:15–28
13. Lezak MD, Howieson DB, Loring DW. Neuropsychological Assess-ment. 4th ed. New York, NY: Oxford University Press; 2004
14. Gioia GA, Isquith PK, Kenworthy L, Barton RM. Profiles ofeveryday executive function in acquired and developmentaldisorders. Child Neuropsychol. 2002;8:121–137
15. Cabeza R, Nyberg L. Imaging cognition II: An empirical reviewof 275 PET and fMRI studies. J Cogn Neurosci. 2000;12:1–47
16. Fuster JM. The Prefrontal Cortex: Anatomy, Physiology, and Neu-ropsychology of the Frontal Lobe. New York, NY: Raven; 1997
2022 WARNER et al at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from

17. Lidow MS. Consequences of prenatal cocaine exposure in non-human primates. Dev Brain Res. 2003;147:23–36
18. Whitaker-Azmitia PM. Role of the neurotrophic properties ofserotonin in the delay of brain maturation induced by cocaine.Ann N Y Acad Sci. 1998;846:158–164
19. Scher MS, Richardson GA, Day NL. Effects of prenatal cocaine/crack and other drug exposure on electroencephalographicsleep studies at birth and one year. Pediatrics. 2000;105:39–48
20. Lester BM, Lagasse L, Seifer R, et al. The Maternal LifestyleStudy (MLS): effects of prenatal cocaine and/or opiate expo-sure on auditory brain response at one month. J Pediatr. 2003;142:279–285
21. Smith LM, Chang L, Yonekura ML, et al. Brain proton mag-netic resonance spectroscopy and imaging in children exposedto cocaine in utero. Pediatrics. 2001;107:227–231
22. Ulug AM, Van Zijl PCM. Orientation-independent diffusionimaging without tensor diagonalization: Anisotropy definitionsbased on physical attributes of the diffusion ellipsoid. J MagnReson Imag. 1999;9:804–813
23. Beaulieu C. The basis of anisotropic water diffusion in thenervous system - A technical review. NMR Biomed. 2002;15:435–455
24. Basser PJ, Jones DK. Diffusion-tensor MRI: Theory, experi-mental design and data analysis - A technical review. NMRBiomed. 2002;15:456–467
25. Le Bihan D, Mangin JF, Poupon C, et al. Diffusion tensorimaging: concepts and applications. J Magn Reson Imag. 2001;13:534–546
26. Watts R, Liston C, Niogi S, Ulug AM. Fiber tracking usingmagnetic resonance diffusion tensor imaging and its applica-tions to human brain development. Ment Retard Dev Disabil ResRev. 2003;9:168–177
27. Li TQ, Noseworthy MD. Mapping the development of whitematter tracts with diffusion tensor imaging. Dev Sci. 2002;5:293–300
28. McGraw P, Liang L, Provenzale JM. Evaluation of normalage-related changes in anisotropy during infancy and child-hood as shown by diffusion tensor imaging. AJR Am J Roentge-nol. 2002;179:1515–1522
29. Morriss MC, Zimmerman RA, Bilaniuk LT, Hunter JV, Hasel-grove JC. Changes in brain water diffusion during childhood.Neuroradiology. 1999;41:929–934
30. Mukherjee P, Miller JH, Shimony JS, et al. Normal brainmaturation during childhood: developmental trends character-ized with diffusion-tensor MR imaging. Radiology. 2001;221:349–358
31. Mukherjee P, Miller JH, Shimony JS, et al. Diffusion-tensorMR imaging of gray and white matter development duringnormal human brain maturation. Am J Neuroradiol. 2002;23:1445–1456
32. Neil JJ, Shiran SI, McKinstry RC, et al. Normal brain in humannewborns: apparent diffusion coefficient and diffusion anisot-ropy measured by using diffusion tensor MR imaging. Radiol-ogy. 1998;209:57–66
33. Schmithorst VJ, Wilke M, Dardzinski BJ, Holland SK. Correla-tion of white matter diffusivity and anisotropy with age duringchildhood and adolescence: a cross-sectional diffusion-tensorMR imaging study. Radiology. 2002;222:212–218
34. Schneider JF, Il’yasov KA, Hennig J, Martin E. Fast quantita-tive diffusion-tensor imaging of cerebral white matter from theneonatal period to adolescence. Neuroradiology. 2004;46:258–266
35. Ulug AM. Monitoring brain development with quantitativediffusion tensor imaging. Dev Sci. 2002;5:286–292
36. Zhang L, Thomas KM, Davidson MC, Casey BJ, Heier LA, UlugAM. MR Quantitation of volume and diffusion changes in thedeveloping brain. Am J Neuroradiol. 2005;26:45–49
37. Engelbrecht V, Scherer A, Rassek M, Witsack HJ, Modder U.Diffusion-weighted MR imaging in the brain in children: Find-ings in the normal brain and in the brain with white matterdiseases. Radiology. 2002;222:410–418
38. Nagy Z, Westerberg H, Skare S, et al. Preterm children havedisturbances of white matter at 11 years of age as shown bydiffusion tensor imaging. Pediatr Res. 2003;54:672–679
39. Filippi CG, Lin DD, Tsiouris AJ, et al. Diffusion-tensor MRimaging in children with developmental delay: preliminaryfindings. Radiology. 2003;229:44–50
40. Neil J, Miller J, Mukherjee P, Huppi PS. Diffusion tensor im-aging of normal and injured developing human brain - Atechnical review. NMR Biomed. 2002;15:543–552
41. Paus T. Mapping brain maturation and cognitive developmentduring adolescence. Trends Cogn Sci. 2005;9:60–68
42. Moseley M, Bammer R, Illes J. Diffusion-tensor imaging ofcognitive performance. Brain Cogn. 2002;50:396–413
43. Deutsch GK, Dougherty RF, Bammer R, Siok WT, Gabrieli JD,Wandell B. Children’s reading performance is correlated withwhite matter structure measured by diffusion tensor imaging.Cortex. 2005;41:354–363
44. Klingberg T, Hedehus M, Temple E, et al. Microstructure oftemporo-parietal white matter as a basis for reading ability:Evidence from diffusion tensor magnetic resonance imaging.Neuron. 2000;25:493–500
45. Olesen PJ, Nagy Z, Westerberg H, Klingberg T. Combined anal-ysis of DTI and fMRI data reveals a joint maturation of whiteand grey matter in a fronto-parietal network. Cogn Brain Res.2003;18:48–57
46. Eyler FD, Behnke M, Conlon M, Woods NS, Wobie K. Birthoutcome from a prospective, matched study of prenatal crack/cocaine use: I. Interactive and dose effects on health andgrowth. Pediatrics. 1998;101:229–236
47. Halls SB, Hanson J Child growth charts for height, weight, andbody mass index. Available at: www.halls.md/chart/child-growth/pediatric.htm. Accessed March 9, 2006
48. Wechsler D. Manual for the Wechsler Intelligence Scale for Children.3rd ed. San Antonio, TX: The Psychological Corporation; 1991
49. Wechsler D. Manual for the Wechsler Individual Achievement Test.San Antonio, TX: The Psychological Corporation; 1992
50. Golden CJ, Freshwater SM, Golden Z. Stroop Color and Word TestChildren’s Version for Ages 5–14: A Manual for Clinical and Exper-imental Uses. Wood Dale, IL: Stoelting Company; 2003
51. Reitan RM. Trail Making Test results for normal and brain-damaged children. Percept Mot Skills. 1971;33:575–581
52. MacLeod CM. Half a century of research on the Stroop effect:An integrative review. Psychol Bull. 1991;109:163–203
53. Adleman NE, Menon V, Blasey CM, et al. A developmentalfMRI study of the Stroop color-word task. NeuroImage. 2002;16:61–75
54. Schroeter ML, Zysset S, Wahl M, von Cramon DY. Prefrontalactivation due to Stroop interference increases duringdevelopment–an event-related fNIRS study. NeuroImage. 2004;23:1317–1325
55. Reitan RM, Wolfson D. The Trail Making Test as an initialscreening procedure for neuropsychological impairment inolder children. Arch Clin Neuropsychol. 2004;19:281–288
56. Demakis GJ. Frontal lobe damage and tests of executiveprocessing: A meta-analysis of the Category Test, Stroop Test,and Trail-Making Test. J Clin Exp Neuropsychol. 2004;26:441–450
57. Ozarslan E, Mareci TH. Generalized diffusion tensor imagingand analytical relationships between diffusion tensor imagingand high angular resolution diffusion imaging. Magnet ResonMed. 2003;50:955–965
58. Padgett KR. Optimizing High Field T1 and Diffusion Tensor Struc-tural Magnetic Resonance Imaging [dissertation]. Gainesville, FL:University of Florida; 2005
PEDIATRICS Volume 118, Number 5, November 2006 2023 at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from

59. Giedd JN, Blumenthal J, Jeffries NO, et al. Brain developmentduring childhood and adolescence: A longitudinal MRI study.Nat Neurosci. 1999;2:861–863
60. Sowell ER, Thompson PM, Holmes CJ, Jernigan TL, Toga AW.In vivo evidence for post-adolescent brain maturation in fron-tal and striatal regions. Nat Neurosci. 1999;2:859–861
61. Spear LP. The adolescent brain and age-related behavioralmanifestations. Neurosci Biobehav Rev. 2000;24:417–463
62. Pierpaoli C, Basser PJ. Toward a quantitative assessment ofdiffusion anisotropy. Magnet Reson Med. 1996;36:893–906
63. Castriota-Scanderbeg A, Fasano F, Hagberg G, Nocentini U,Filippi M, Caltagirone C. Coefficient Dav is more sensitive thanfractional anisotropy in monitoring progression of irreversibletissue damage in focal nonactive multiple sclerosis lesions.Am J Neuroradiol. 2003;24:663–670
64. Huizink AC, Mulder EJ. Maternal smoking, drinking or can-nabis use during pregnancy and neurobehavioral and cognitivefunctioning in human offspring. Neurosci Biobehav Rev. 2006;30:24–41
65. Klenberg L, Korkman M, Lahti-Nuuttila P. Differential devel-opment of attention and executive functions in 3- to 12-year-old Finnish children. Dev Neuropsychol. 2001;20:407–428
66. Neddens J, Brandenburg K, Teuchert-Noodt G, Dawirs RR.Differential environment alters ontogeny of dopamine inner-
vation of the orbital prefrontal cortex in gerbils. J Neurosci Res.2001;63:209–213
67. Winterfeld KT, Teuchert-Noodt G, Dawirs RR. Social environ-ment alters both ontogeny of dopamine innervation of themedial prefrontal cortex and maturation of working memoryin gerbils (Meriones unguiculatus). J Neurosci Res. 1998;52:201–209
68. Glaser D. Child abuse and neglect and the brain–a review.J Child Psychol Psychiatry. 2000;41:97–116
69. Accornero VH, Morrow CE, Bandstra ES, Johnson AL, An-thony JC. Behavioral outcome of preschoolers exposed prena-tally to cocaine: role of maternal behavioral health. J PediatrPsychol. 2002;27:259–269
70. Frank DA, Jacobs RR, Beeghly M, et al. Level of prenatalcocaine exposure and scores on the Bayley Scales of InfantDevelopment: modifying effects of caregiver, early interven-tion, and birth weight. Pediatrics. 2002;110:1143–1152
71. Johnson HL, Nusbaum BJ, Bejarano A, Rosen TS. An ecologicalapproach to development in children with prenatal drug ex-posure. Am J Orthopsychiat. 1999;69:448–456
72. Wobie K, Eyler FD, Garvan CW, Hou W, Behnke M. Prenatalcocaine exposure: an examination of out-of-home placementduring the first year of life. J Drug Issues. 2004;34:77–94
PEDIATRICS
“. . .encourages investigators to register their clinical trials in a public trialsregistry. The members of the International Committee of Medical JournalEditors plan to consider clinical trials for publication only if they have beenregistered. . . . The National Library of Medicine’s www.clinicaltrials.gov is afree registry, open to all investigators, that meets the committee’s require-ments.”
N Engl J Med. 354;24, June 15, 2006Noted by JFL, MD
2024 WARNER et al at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from

DOI: 10.1542/peds.2006-0003 2006;118;2014-2024 Pediatrics
Stephen J. Blackband Christiana Leonard, Wei Hou, Cynthia Wilson Garvan, Ilona M. Schmalfuss and Tamara Duckworth Warner, Marylou Behnke, Fonda Davis Eyler, Kyle Padgett,
Cocaine-Exposed ChildrenDiffusion Tensor Imaging of Frontal White Matter and Executive Functioning in
& ServicesUpdated Information
http://www.pediatrics.org/cgi/content/full/118/5/2014including high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/118/5/2014#BIBLat: This article cites 65 articles, 18 of which you can access for free
Subspecialty Collections
tryhttp://www.pediatrics.org/cgi/collection/neurology_and_psychia
Neurology & Psychiatryfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
at University of Florida on July 6, 2007 www.pediatrics.orgDownloaded from