contrast-enhanced ultrasound and prostate cancer; a multicentre european research coordination...
TRANSCRIPT

Review – Prostate Cancer
Contrast-Enhanced Ultrasound and Prostate Cancer;A Multicentre European Research Coordination Project
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3
avai lable at www.sc iencedi rect .com
journal homepage: www.europeanurology.com
Margot Wink a, Ferdinand Frauscher c, David Cosgrove b, Jean-Yves Chapelon d,Leo Palwein c, Michael Mitterberger c, Chris Harvey b, Olivier Rouviere d,Jean de la Rosette a, Hessel Wijkstra a,*aDepartment of Urology, Academic Medical Centre, University of Amsterdam, Amsterdam, The NetherlandsbDepartment of Radiology, Imperial College, London, United KingdomcDepartment of Uro-Radiology, University Hospital, Innsbruck, Austriad INSERM U556, Lyon, France
Article info
Article history:Accepted June 12, 2008Published online ahead ofprint on June 20, 2008
Keywords:Prostate carcinomaMicrobubblesUltrasound
Abstract
Context: Contrast-enhanced ultrasound is a real-time imaging technique withthe capability of visualizing perfusion patterns. Since tumour growth is asso-ciated with changes in vascularisation, this modality is under research forimaging of various tumour types. Studies have shown promising results forthe diagnosis of prostate cancer for various imaging techniques; however, theexact value of each technique is still unclear.Objective: To determine the value of contrast-enhanced ultrasound (CEUS) in thedetection, localisation, and follow-up of treatment for prostate cancer.Evidence acquisition: In the period 2002–2006, research in four European centresregarding CEUS of the prostate was coordinated in a combined program. Thispaper describes and combines the results of these studies.Evidence synthesis: Various techniques were developed and researched duringthe period of this program. Studies showed that prostate cancer could be visua-lized and localized in up to 78%. Visualization of the tumour enabled betterdetection; targeted biopsies lead to fewer biopsies per session without loss ofdetection rate. A combined approach offered the highest detection rate. CEUScould be used to visualize the effects of high-intensity focussed ultrasound andhormonal therapy for prostate cancer with success, and identified patients withan early relapse. Unfortunately, pretreatment evaluation could not identify the
nonresponders beforehand.search project was a first step towards routine use of CEUS inion and follow-up of prostate cancer; and new combined
Conclusions: This rethe clinical detect
d.sociation of Urology. Published by Elsevier B.V. All rights reserved.
studies are initiate# 2008 European As
* Corresponding author. Academic Medical Centre, University of Amsterdam, Departmentof Urology, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands. Tel. +31205666030;Fax: +31205669585.E-mail address: [email protected] (H. Wijkstra).
0302-2838/$ – see back matter # 2008 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2008.06.057

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3 983
1. Introduction
1.1. Diagnosis
The diagnosis of prostate cancer (PCa) is far fromoptimal [1]. Currently, at least 10 biopsy cores arerecommended for routine use in the PCa guidelinesprovided by the European Association of Urology [2].The positive predictive value of biopsies based onprostate-specific antigen (PSA), digital rectal exam-ination (DRE), and transrectal ultrasound (TRUS) islow and many unnecessary biopsies are performed[3]. Moreover, even in patients with low PSA values asignificant number of PCa cases are found [4,5].Therefore, the search for improvement of diagnostictechniques is a necessity.
Several different approaches to improve detec-tion are studied. Regarding tumour markers, theoptimal cut-off value of PSA is still under investiga-tion. Novel tumour markers in blood and urine havebeen researched, but no highly accurate andsensitive markers to replace PSA have been identi-fied until now. A recent review concludes thatvarious biomarkers under investigation are promis-ing, but all still have to be validated [6,7]. Whenvisualization of PCa is improved, the biopsy needlecan be targeted to the centre of the tumour. This willlead to a change in biopsy strategies, and possiblybetter grading. Furthermore, better visibility ofmalignant tissue will probably also improve staging.If the exact location and volume of the tumour isknown, treatment can be improved. Moreover,follow-up can be optimized if imaging can localizerecurrence of malignant tissue.
Detection and localisation of prostate tumoursusing greyscale ultrasound is poor, and TRUS ismainly used to guide systematic biopsies. In ascreening program, it is stated that TRUS can besafely omitted as screening tool [8]. MR, PET-CT, andnuclear imaging modalities have been reported tohave diagnostic value in local staging and detectionof the tumour.
1.2. Background
Tumour growth induces neovascularization [9], andan increased microvessel density is associated withthe prognosis and progression of PCa, in terms ofmetastases, stage of disease, and disease-specificsurvival [10–12]. Therefore, visualization of theinduced altered perfusion patterns may improvedetection of cancer.
Contrast-enhanced ultrasound imaging (CEUS)was developed to image perfusion [13,14]. Because ofthe high spatial and temporal resolution of ultra-
sound, detailed and real-time perfusion imagingbecame possible. Ultrasound contrast agents consistof small encapsulated gas bubbles that are adminis-tered intravenously and remain intravascular. Add-ing microbubbles as additional reflectors into thebloodstream increases the sensitivity of colour (CD)and power Doppler (PD) imaging. However, thesetechniques use relatively high US energy levels and,as a result, a large proportion of the microbubblesare destroyed as they are imaged [15]. During the lastyears, new imaging techniques have been developedthat enable sensitive microbubble imaging even inthe microvasculature, with lower destruction rates(Low mechanical index imaging). Nowadays, a longlist of CEUS techniques is available, from harmonicimaging, using the nonlinear behaviour of micro-bubbles in an ultrasound beam, via pulse inversiontechniques, using various pulses to isolate thenonlinear reflections, to even more specific imagingtechniques that provide selective imaging of thesignals reflected by the bubbles, cancelling out mostof the tissue reflections.
During the last decade, mainly European researchgroups have published promising results of CEUS forthe diagnosis of PCa and for guiding biopsies. In2000, a project was defined to coordinate singleinstitute efforts on a European level. The goal was toimprove diagnosis and treatment of PCa by coordi-nation of the research. A project proposal wassubmitted for funding in the European Community’sSixth Framework Programme (FP6), and, in 2002, theproject ‘CONTRAST’, QLRT-2001-2174: ‘‘Contrast-enhanced ultrasound imaging in the diagnosis andtreatment of prostate cancer’’ was granted. Thismanuscript reviews the achieved results of thisEuropean Community project in comparison topublished data outside this research group. Basedon this, a critical evaluation of CEUS is presentedand the expectations for the future are discussed.
2. Methods
The project was active during the period 2002–2006. The
project leaders are coauthoring this paper.
There were four main project objectives:
� A
chieve a critical mass by coordinating research efforts andpooling data
� C
oordinate transrectal CEUS research in Europe� D
isseminate results� S
et up continuation of research after the end of the project.The project consisted of eight work packages (WP) as
described in Table 1 and coordinated as shown in Table 2.
During the course of the project, newer techniques were
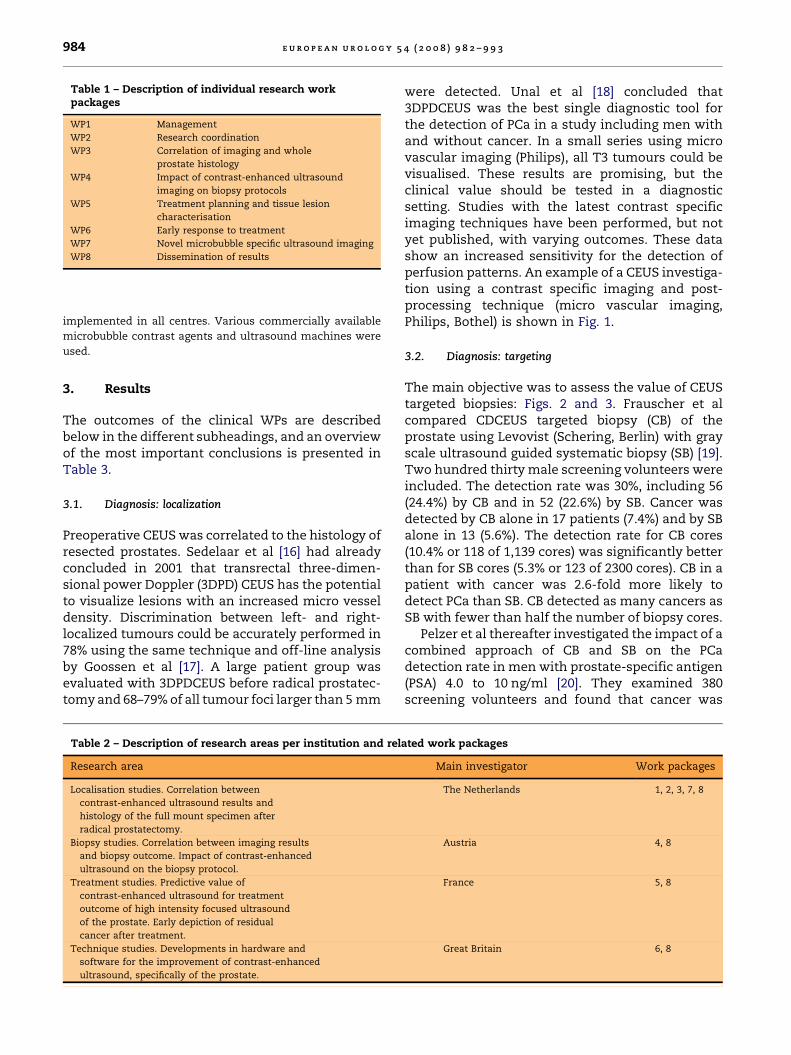
Table 1 – Description of individual research workpackages
WP1 Management
WP2 Research coordination
WP3 Correlation of imaging and whole
prostate histology
WP4 Impact of contrast-enhanced ultrasound
imaging on biopsy protocols
WP5 Treatment planning and tissue lesion
characterisation
WP6 Early response to treatment
WP7 Novel microbubble specific ultrasound imaging
WP8 Dissemination of results
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3984
implemented in all centres. Various commercially available
microbubble contrast agents and ultrasound machines were
used.
3. Results
The outcomes of the clinical WPs are describedbelow in the different subheadings, and an overviewof the most important conclusions is presented inTable 3.
3.1. Diagnosis: localization
Preoperative CEUS was correlated to the histology ofresected prostates. Sedelaar et al [16] had alreadyconcluded in 2001 that transrectal three-dimen-sional power Doppler (3DPD) CEUS has the potentialto visualize lesions with an increased micro vesseldensity. Discrimination between left- and right-localized tumours could be accurately performed in78% using the same technique and off-line analysisby Goossen et al [17]. A large patient group wasevaluated with 3DPDCEUS before radical prostatec-tomy and 68–79% of all tumour foci larger than 5 mm
Table 2 – Description of research areas per institution and rel
Research area
Localisation studies. Correlation between
contrast-enhanced ultrasound results and
histology of the full mount specimen after
radical prostatectomy.
Biopsy studies. Correlation between imaging results
and biopsy outcome. Impact of contrast-enhanced
ultrasound on the biopsy protocol.
Treatment studies. Predictive value of
contrast-enhanced ultrasound for treatment
outcome of high intensity focused ultrasound
of the prostate. Early depiction of residual
cancer after treatment.
Technique studies. Developments in hardware and
software for the improvement of contrast-enhanced
ultrasound, specifically of the prostate.
were detected. Unal et al [18] concluded that3DPDCEUS was the best single diagnostic tool forthe detection of PCa in a study including men withand without cancer. In a small series using microvascular imaging (Philips), all T3 tumours could bevisualised. These results are promising, but theclinical value should be tested in a diagnosticsetting. Studies with the latest contrast specificimaging techniques have been performed, but notyet published, with varying outcomes. These datashow an increased sensitivity for the detection ofperfusion patterns. An example of a CEUS investiga-tion using a contrast specific imaging and post-processing technique (micro vascular imaging,Philips, Bothel) is shown in Fig. 1.
3.2. Diagnosis: targeting
The main objective was to assess the value of CEUStargeted biopsies: Figs. 2 and 3. Frauscher et alcompared CDCEUS targeted biopsy (CB) of theprostate using Levovist (Schering, Berlin) with grayscale ultrasound guided systematic biopsy (SB) [19].Two hundred thirty male screening volunteers wereincluded. The detection rate was 30%, including 56(24.4%) by CB and in 52 (22.6%) by SB. Cancer wasdetected by CB alone in 17 patients (7.4%) and by SBalone in 13 (5.6%). The detection rate for CB cores(10.4% or 118 of 1,139 cores) was significantly betterthan for SB cores (5.3% or 123 of 2300 cores). CB in apatient with cancer was 2.6-fold more likely todetect PCa than SB. CB detected as many cancers asSB with fewer than half the number of biopsy cores.
Pelzer et al thereafter investigated the impact of acombined approach of CB and SB on the PCadetection rate in men with prostate-specific antigen(PSA) 4.0 to 10 ng/ml [20]. They examined 380screening volunteers and found that cancer was
ated work packages
Main investigator Work packages
The Netherlands 1, 2, 3, 7, 8
Austria 4, 8
France 5, 8
Great Britain 6, 8
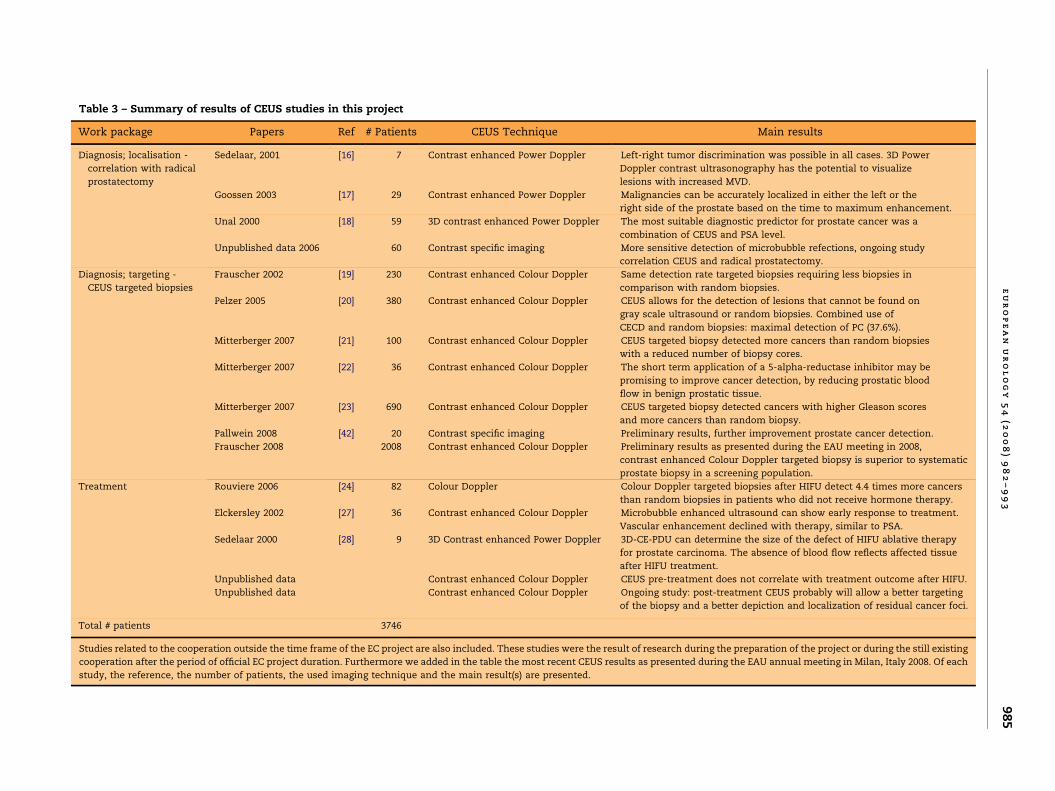
Table 3 – Summary of results of CEUS studies in this project
Work package Papers Ref # Patients CEUS Technique Main results
Diagnosis; localisation -
correlation with radical
prostatectomy
Sedelaar, 2001 [16] 7 Contrast enhanced Power Doppler Left-right tumor discrimination was possible in all cases. 3D Power
Doppler contrast ultrasonography has the potential to visualize
lesions with increased MVD.
Goossen 2003 [17] 29 Contrast enhanced Power Doppler Malignancies can be accurately localized in either the left or the
right side of the prostate based on the time to maximum enhancement.
Unal 2000 [18] 59 3D contrast enhanced Power Doppler The most suitable diagnostic predictor for prostate cancer was a
combination of CEUS and PSA level.
Unpublished data 2006 60 Contrast specific imaging More sensitive detection of microbubble refections, ongoing study
correlation CEUS and radical prostatectomy.
Diagnosis; targeting -
CEUS targeted biopsies
Frauscher 2002 [19] 230 Contrast enhanced Colour Doppler Same detection rate targeted biopsies requiring less biopsies in
comparison with random biopsies.
Pelzer 2005 [20] 380 Contrast enhanced Colour Doppler CEUS allows for the detection of lesions that cannot be found on
gray scale ultrasound or random biopsies. Combined use of
CECD and random biopsies: maximal detection of PC (37.6%).
Mitterberger 2007 [21] 100 Contrast enhanced Colour Doppler CEUS targeted biopsy detected more cancers than random biopsies
with a reduced number of biopsy cores.
Mitterberger 2007 [22] 36 Contrast enhanced Colour Doppler The short term application of a 5-alpha-reductase inhibitor may be
promising to improve cancer detection, by reducing prostatic blood
flow in benign prostatic tissue.
Mitterberger 2007 [23] 690 Contrast enhanced Colour Doppler CEUS targeted biopsy detected cancers with higher Gleason scores
and more cancers than random biopsy.
Pallwein 2008 [42] 20 Contrast specific imaging Preliminary results, further improvement prostate cancer detection.
Frauscher 2008 2008 Contrast enhanced Colour Doppler Preliminary results as presented during the EAU meeting in 2008,
contrast enhanced Colour Doppler targeted biopsy is superior to systematic
prostate biopsy in a screening population.
Treatment Rouviere 2006 [24] 82 Colour Doppler Colour Doppler targeted biopsies after HIFU detect 4.4 times more cancers
than random biopsies in patients who did not receive hormone therapy.
Elckersley 2002 [27] 36 Contrast enhanced Colour Doppler Microbubble enhanced ultrasound can show early response to treatment.
Vascular enhancement declined with therapy, similar to PSA.
Sedelaar 2000 [28] 9 3D Contrast enhanced Power Doppler 3D-CE-PDU can determine the size of the defect of HIFU ablative therapy
for prostate carcinoma. The absence of blood flow reflects affected tissue
after HIFU treatment.
Unpublished data Contrast enhanced Colour Doppler CEUS pre-treatment does not correlate with treatment outcome after HIFU.
Unpublished data Contrast enhanced Colour Doppler Ongoing study: post-treatment CEUS probably will allow a better targeting
of the biopsy and a better depiction and localization of residual cancer foci.
Total # patients 3746
Studies related to the cooperation outside the time frame of the EC project are also included. These studies were the result of research during the preparation of the project or during the still existing
cooperation after the period of official EC project duration. Furthermore we added in the table the most recent CEUS results as presented during the EAU annual meeting in Milan, Italy 2008. Of each
study, the reference, the number of patients, the used imaging technique and the main result(s) are presented.
eu
ro
pe
an
ur
ol
og
y5
4(2
00
8)
98
2–
99
39
85
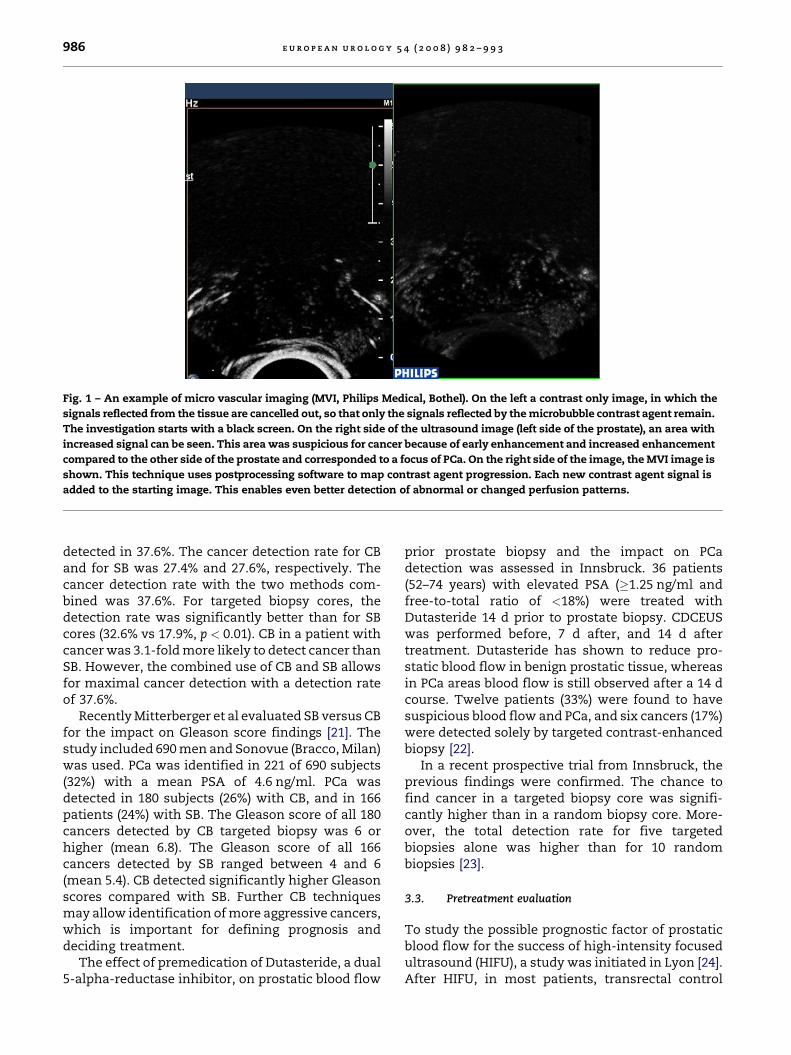
Fig. 1 – An example of micro vascular imaging (MVI, Philips Medical, Bothel). On the left a contrast only image, in which the
signals reflected from the tissue are cancelled out, so that only the signals reflected by the microbubble contrast agent remain.
The investigation starts with a black screen. On the right side of the ultrasound image (left side of the prostate), an area with
increased signal can be seen. This area was suspicious for cancer because of early enhancement and increased enhancement
compared to the other side of the prostate and corresponded to a focus of PCa. On the right side of the image, the MVI image is
shown. This technique uses postprocessing software to map contrast agent progression. Each new contrast agent signal is
added to the starting image. This enables even better detection of abnormal or changed perfusion patterns.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3986
detected in 37.6%. The cancer detection rate for CBand for SB was 27.4% and 27.6%, respectively. Thecancer detection rate with the two methods com-bined was 37.6%. For targeted biopsy cores, thedetection rate was significantly better than for SBcores (32.6% vs 17.9%, p < 0.01). CB in a patient withcancer was 3.1-fold more likely to detect cancer thanSB. However, the combined use of CB and SB allowsfor maximal cancer detection with a detection rateof 37.6%.
Recently Mitterberger et al evaluated SB versus CBfor the impact on Gleason score findings [21]. Thestudy included 690 men and Sonovue (Bracco, Milan)was used. PCa was identified in 221 of 690 subjects(32%) with a mean PSA of 4.6 ng/ml. PCa wasdetected in 180 subjects (26%) with CB, and in 166patients (24%) with SB. The Gleason score of all 180cancers detected by CB targeted biopsy was 6 orhigher (mean 6.8). The Gleason score of all 166cancers detected by SB ranged between 4 and 6(mean 5.4). CB detected significantly higher Gleasonscores compared with SB. Further CB techniquesmay allow identification of more aggressive cancers,which is important for defining prognosis anddeciding treatment.
The effect of premedication of Dutasteride, a dual5-alpha-reductase inhibitor, on prostatic blood flow
prior prostate biopsy and the impact on PCadetection was assessed in Innsbruck. 36 patients(52–74 years) with elevated PSA (�1.25 ng/ml andfree-to-total ratio of <18%) were treated withDutasteride 14 d prior to prostate biopsy. CDCEUSwas performed before, 7 d after, and 14 d aftertreatment. Dutasteride has shown to reduce pro-static blood flow in benign prostatic tissue, whereasin PCa areas blood flow is still observed after a 14 dcourse. Twelve patients (33%) were found to havesuspicious blood flow and PCa, and six cancers (17%)were detected solely by targeted contrast-enhancedbiopsy [22].
In a recent prospective trial from Innsbruck, theprevious findings were confirmed. The chance tofind cancer in a targeted biopsy core was signifi-cantly higher than in a random biopsy core. More-over, the total detection rate for five targetedbiopsies alone was higher than for 10 randombiopsies [23].
3.3. Pretreatment evaluation
To study the possible prognostic factor of prostaticblood flow for the success of high-intensity focusedultrasound (HIFU), a study was initiated in Lyon [24].After HIFU, in most patients, transrectal control
Fig. 2 – A 55-year-old man with prostate-specific antigen of
3.6 and Gleason 7 cancer in the left base of the prostate,
only found by contrast-enhanced targeted biopsy.
A. Conventional gray scale transverse image does not
show any suspicious lesion. B. Only contrast-enhanced
colour Doppler transverse image shows increased flow
associated with the cancer.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3 987
biopsy obtained 3–6 mo after treatment showsuniform tissue destruction throughout the gland.However, in some patients, incomplete tissuedestruction with unaffected islets of viable cells(whether normal or tumoural) are found. Differ-ences in local blood flow might explain thesedifferences in individual responses to the treatment(heat sink effect) [25,26]. Thirty-five patients
Fig. 3 – A 61-year-old man with prostate-specific antigen of 4.2
A. Conventional gray scale transverse image shows no focal lesi
shows increased flow in the left base, corresponding to the can
image shows increased flow corresponding to the cancer.
planned for a transrectal HIFU ablation of PCa wereincluded in the study. They all underwent apreoperative CDCEUS examination before and aftercontrast injection (Levovist, Schering, Berlin). Dedi-cated software (PixelFlux, Chameleon-software,Germany) was used to calculate the colour pixeldensity and the mean velocity within the peripheralzone, the transitional zone, and the periprostatictissues. Six mo after HIFU treatment, randomultrasound-guided control biopsies were obtainedin 31 patients. The uniformity of the tissue destruc-tion observed on each sextant control biopsy wasassessed with a three point scale. This tissuedestruction score was then compared to the pre-operative CDCEUS data. In the 182 sextants, tissuedestruction score was 0 in 111, 1 in 27, and 2 in 44.Unfortunately, this score did not correlate with thepreoperative CD findings in any region of interest,either before or after contrast injection.
3.4. Treatment effect
Because of the possibility of detailed imaging ofperfusion, CEUS was investigated for the follow-upof minimally invasive and medical treatmentmodalities that influence the perfusion of theprostate. In 2002 CEUS monitoring of hormonaltreatment was described in a combined study(London, Nijmegen). Thirty-six men with PCa werestudied at baseline and at intervals during treatmentusing Levovist (Schering, Berlin) enhanced DopplerCEUS imaging. Quantitative analysis demonstrateda decrease in CEUS signal over time and a strongcorrelation with changes in the mean PSA (r = 0.95,p < 0.001) was found. In four patients, Dopplerindices did not fall with PSA: Two patients withthe most marked discrepancy relapsed at 6 mo [27].
Before the start of this project, the effects of HIFUcould be visualized in a study in which patientsunderwent a radical prostatectomy after HIFUtreatment. The areas without perfusion could be
and Gleason 8 cancer in the left base.
on. B. Contrast-enhanced colour Doppler transverse image
cer. C. Also contrast-enhanced power Doppler transverse

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3988
demarcated and treatment effects correlated withthree-dimensional PDCEUS findings [28].
The presence of residual cancer after HIFUablation of the prostate is usually diagnosed byrandom prostate biopsy taken routinely and in theevent of significantly increased PSA [29,30]. How-ever, since residual cancer can be efficiently treatedby a second HIFU application or by radiationtherapy, there is a need for an early diagnosis andlocalisation of residual tumour foci. In a studypublished in 2004, CD-guided sextant biopsies wereobtained in 82 patients who had undergone prostateHIFU ablation for cancer, 24 of whom had hormonetherapy before, CD findings were compared withbiopsy results. Results showed that CD was asignificant independent predictor of the biopsyresults in patients without history of hormonetherapy, with CD-positive sites being 4.4 times morelikely to contain cancer at biopsy than CD-negativesites. However, CD was inaccurate in patients whohad previously received hormone therapy. More-over, CD sensitivity remained low in the overallstudy population, with only 38% of the sites withresidual cancer showing positive CD findings [31].These studies were performed without contrastmedia; a new study, described in the discussion, hasstarted using CDCEUS.
4. Discussion
4.1. Localisation and detection
Correlation between histology and CEUS regardingtumour localisation is promising, and improvementof techniques led to increase of detection. Stroh-meyer et al have published comparable results to theones presented here regarding CEUS correlationwith radical prostatectomy specimens [32]. Halpernet al also correlated the CEUS findings using aharmonic imaging method to histology and foundfive more foci of cancer in addition to the eight out of30 that were found using noncontrast ultrasound.However, seven false positive foci were detected[33]. Moerkerk et al used an automated 3D CDCEUScalculation and found a 65% correlation between theprocessed images and presence of malignancy. Theyconclude that the used ‘‘clustering analysis’’ can beof value in biopsy sessions [34].
Other imaging techniques under investigation forvisualisation of PCa are MRI, PET/CT, and elasto-graphy ultrasound. A recent review concluded thatno PET or PET/CT studies with a large number ofpatients and tissue confirmation exist and thusfurther investigations are required [35]. Regarding
MRI more data are available. Especially functionalMRI techniques are promising in the local staging[36,37]. A large meta-analysis found a maximumjoint sensitivity and specificity for the detection ofextracapsular extension of 64% [38]. However, alarge heterogenicity exists in the available MRIliterature, with sensitivity for detection varyingbetween 37–90% [39]. Furthermore, a recent reportshows that detection of tumour recurrence ispossible using dynamic contrast-enhanced MRI[40]. Kim et al recently concluded in a review paperthat 3 Tesla MR is not expected to substantiallyimprove PCa localisation. However, the addition ofspecific techniques, such as spectroscopy, to con-ventional sequences at 3 T might improve diagnosticaccuracy [41]. The main advantage of ultrasound isthe easy accessibility and the possibility to takebiopsies during the investigation. Elastography wasable to detect 88% of the cancer foci in a study thatcorrelated ultrasound results to radical prostatec-tomy specimens. Elastography guided biopsiesshowed a 2.9-fold higher detection rate than randombiopsies in a group of 230 screening volunteers [42].
The effect of CEUS on the prostate biopsy protocoland detection rate was extensively investigated.From our studies, we concluded that a clear associa-tion between contrast enhancement in the prostateandthediagnosis ofclinically significant PCa exists. Itwas shown that the sensitivity for PCa diagnosis isincreased by CEUS targeted biopsy. Fewer biopsiesare needed to accomplish the same detection rate.These findings were confirmed by the results of Royet al, who found an increase in sensitivity for thedetection of cancer using CDCEUS [43]. The Halperngroup used various greyscale and harmonic CEUStechniques. A study comprising 301 patients found asignificantly higher detection rate in CEUS targetedbiopsies than in random biopsies [44]. Finally,combined results of 2008 men from the screeninggroup in Innsbruck as presented at the EAU meetingin March 2008 clearly confirm earlier data [45].Prostatitis and benign hyperplasia may cause false-positive foci of enhancement [33]. Therefore, basedon our preliminary experiences, the short-termapplication of a 5-alpha-reductase inhibitor may bepromising to improve PCa detection, by reducingprostatic blood flow in benign prostatic tissue.
The sensitivity and specificity for the detection ofthe reflections of the microbubbles increased duringthe development of CEUS. Newer, contrast-specifictechniques were implemented in all centres. Pre-liminary results presented by Pallwein et al show afurther increase in cancer detection rate using oneof the recently developed contrast specific imagingtechniques, contrast pulse sequence imaging [42].
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3 989
Improved visualisation of the tumour may notonly lead to increased detection, but also to betterGleason grading and staging. One could imagine thata higher detection rate might lead to a higherpercentage of clinically insignificant cancers; how-ever, our results show that cancers found by meansof targeted biopsy have a higher mean Gleason scorethan the ones found by random biopsies.
4.2. Follow-up
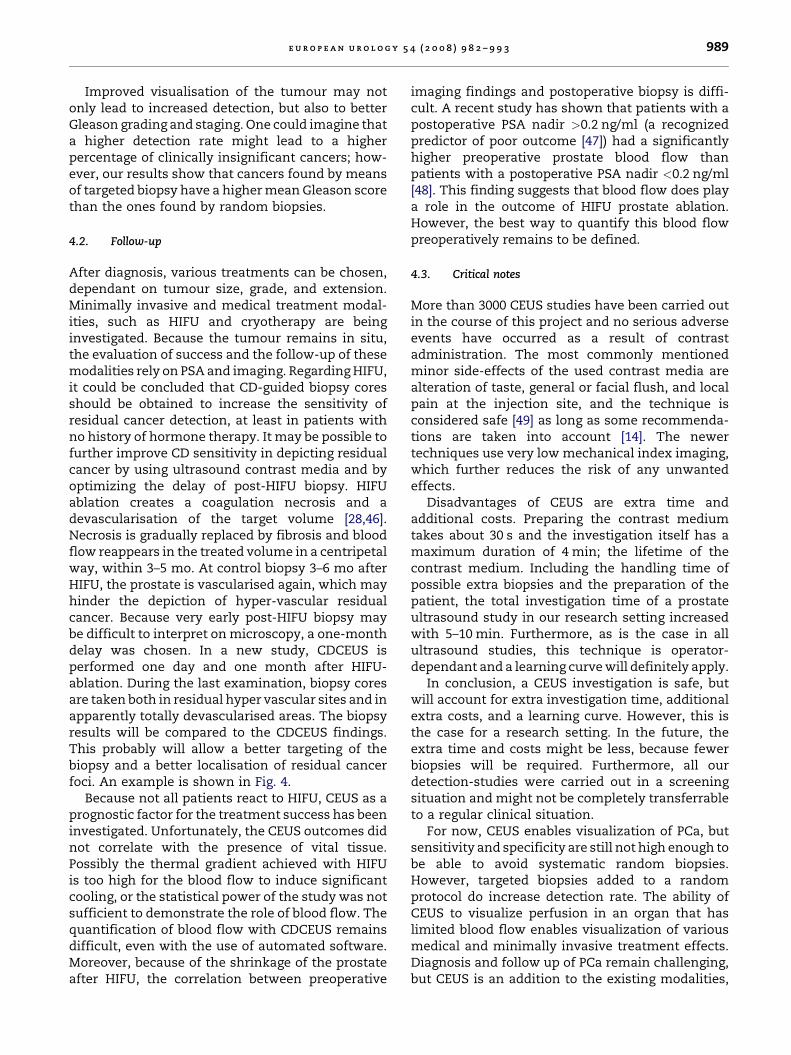
After diagnosis, various treatments can be chosen,dependant on tumour size, grade, and extension.Minimally invasive and medical treatment modal-ities, such as HIFU and cryotherapy are beinginvestigated. Because the tumour remains in situ,the evaluation of success and the follow-up of thesemodalities rely on PSA and imaging. Regarding HIFU,it could be concluded that CD-guided biopsy coresshould be obtained to increase the sensitivity ofresidual cancer detection, at least in patients withno history of hormone therapy. It may be possible tofurther improve CD sensitivity in depicting residualcancer by using ultrasound contrast media and byoptimizing the delay of post-HIFU biopsy. HIFUablation creates a coagulation necrosis and adevascularisation of the target volume [28,46].Necrosis is gradually replaced by fibrosis and bloodflow reappears in the treated volume in a centripetalway, within 3–5 mo. At control biopsy 3–6 mo afterHIFU, the prostate is vascularised again, which mayhinder the depiction of hyper-vascular residualcancer. Because very early post-HIFU biopsy maybe difficult to interpret on microscopy, a one-monthdelay was chosen. In a new study, CDCEUS isperformed one day and one month after HIFU-ablation. During the last examination, biopsy coresare taken both in residual hyper vascular sites and inapparently totally devascularised areas. The biopsyresults will be compared to the CDCEUS findings.This probably will allow a better targeting of thebiopsy and a better localisation of residual cancerfoci. An example is shown in Fig. 4.
Because not all patients react to HIFU, CEUS as aprognostic factor for the treatment success has beeninvestigated. Unfortunately, the CEUS outcomes didnot correlate with the presence of vital tissue.Possibly the thermal gradient achieved with HIFUis too high for the blood flow to induce significantcooling, or the statistical power of the study was notsufficient to demonstrate the role of blood flow. Thequantification of blood flow with CDCEUS remainsdifficult, even with the use of automated software.Moreover, because of the shrinkage of the prostateafter HIFU, the correlation between preoperative
imaging findings and postoperative biopsy is diffi-cult. A recent study has shown that patients with apostoperative PSA nadir >0.2 ng/ml (a recognizedpredictor of poor outcome [47]) had a significantlyhigher preoperative prostate blood flow thanpatients with a postoperative PSA nadir <0.2 ng/ml[48]. This finding suggests that blood flow does playa role in the outcome of HIFU prostate ablation.However, the best way to quantify this blood flowpreoperatively remains to be defined.
4.3. Critical notes
More than 3000 CEUS studies have been carried outin the course of this project and no serious adverseevents have occurred as a result of contrastadministration. The most commonly mentionedminor side-effects of the used contrast media arealteration of taste, general or facial flush, and localpain at the injection site, and the technique isconsidered safe [49] as long as some recommenda-tions are taken into account [14]. The newertechniques use very low mechanical index imaging,which further reduces the risk of any unwantedeffects.
Disadvantages of CEUS are extra time andadditional costs. Preparing the contrast mediumtakes about 30 s and the investigation itself has amaximum duration of 4 min; the lifetime of thecontrast medium. Including the handling time ofpossible extra biopsies and the preparation of thepatient, the total investigation time of a prostateultrasound study in our research setting increasedwith 5–10 min. Furthermore, as is the case in allultrasound studies, this technique is operator-dependant and a learning curve will definitely apply.
In conclusion, a CEUS investigation is safe, butwill account for extra investigation time, additionalextra costs, and a learning curve. However, this isthe case for a research setting. In the future, theextra time and costs might be less, because fewerbiopsies will be required. Furthermore, all ourdetection-studies were carried out in a screeningsituation and might not be completely transferrableto a regular clinical situation.
For now, CEUS enables visualization of PCa, butsensitivity and specificity are still not high enough tobe able to avoid systematic random biopsies.However, targeted biopsies added to a randomprotocol do increase detection rate. The ability ofCEUS to visualize perfusion in an organ that haslimited blood flow enables visualization of variousmedical and minimally invasive treatment effects.Diagnosis and follow up of PCa remain challenging,but CEUS is an addition to the existing modalities,
Fig. 4 – Transrectal ultrasound images obtained in a 74 year-old patient with local recurrence of prostate cancer after
radiation therapy. This local recurrence had been treated by HIFU ablation one month before. A. Power Doppler image
showed limited blood flux in the central gland of the prostate (arrow), suggesting that this area had not been totally
destroyed by the HIFU ablation. B. Simultaneous acquisition of a low mechanical index ultrasound image (right side of the
screen) and of a contrast ultrasound image (left side of the screen) 30 sec after bolus injection of 4.8 ml of Sonovue. The
HIFU-induced coagulation necrosis was clearly seen as a devascularized area with no contrast enhancement (straight
arrows). The anterior part of the left lobe showed intense enhancement on contrast image (arrowheads), suggesting it had
not been destroyed by HIFU. Obtaining biopsy from that anterior territory might increase the sensitivity of residual cancer
detection. Note that the devascularized area extended into the periprostatic tissues (curved arrow).
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3990
which deserves a role in PCa management and stillneeds further investigation.
Based on the goals written down in the originalproject plan, one could state that these were notachieved. During the project duration, no largemulticentre studies were initiated, and at the endof the project period, CEUS does not yet have anyrole in the routine clinical practice. However, webelieve that we made a first step. Together with the
partners involved in this project, and together withmajor ultrasound and contrast companies in thisfield at his moment, initiatives are implementedwhich will make a difference in the nearby future.
What can we expect in the near future? Manystudies are still ongoing in each of the involvedcentres and new results will soon be available.A large prospective multicentre study will beinitiated. The goal is to prove that currently available
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3 991
CEUS techniques can be used to diagnose PCa andthat CEUS targeted biopsies are superior as com-pared to systematic biopsies and therefore diagnosiswill improve with fewer biopsy cores.
Companies and research groups are developingnew CEUS techniques, which have the potential tofurther improve CEUS. Furthermore, a new genera-tion of microbubbles is under investigation andespecially targeted microbubbles seem promisingfor the future. And, last but not least, drug and genedelivery with the help of microbubbles is underinvestigation in several research centres.
We believe that CEUS in potential offers addedvalue to the entire PCa care cycle, by adding asensitive imaging modality. For now, however, theadditional value has not yet been established. Ifmulticentre approaches confirm the availableresults, diagnosis but also choice of treatment andfollow-up of PCa could improve.
Author contributions: Hessel Wijkstra had full access to all the
data in the study and takes responsibility for the integrity of
the data and the accuracy of the data analysis.
Study concept and design: Wink, Wijkstra.
Acquisition of data: Wink, Pallwein, Mitterberger, Harvey,
Rouviere.
Analysis and interpretation of data: Wink, Pallwein, Mitterberger,
Harvey, Rouviere, Frauscher, Cosgrove, Chapelon, Wijkstra.
Drafting of the manuscript: Wink, Wijkstra, Chapelon, Cosgrove,
Frauscher.
Critical revision of the manuscript for important intellectual content:
Wijkstra,Chapelon, Cosgrove, Frauscher, de la Rosette.
Statistical analysis: None.
Obtaining funding: Wijkstra, Cosgrove, Frauscher, Chapelon.
Administrative, technical, or material support: None.
Supervision: Wijkstra.
Other (specify): None.
Financial disclosures: I certify that all conflicts of interest,
including specific financial interests and relationships and
affiliations relevant to the subject matter or materials
discussed in the manuscript (eg, employment/ affiliation,
grants or funding, consultancies, honoraria, stock ownership
or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: This study was
funded by the European Community’s Sixth Framework
Programme (FP6).
Funding/Support and role of the sponsor: Design and conduct of
the study.
References
[1] Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer
statistics, 2007. CA Cancer J Clin 2007;57:43–66.
[2] Heidenreich A, Aus G, Bolla M, et al. EAU guidelines on
prostate cancer. Eur Urol 2008;53:68–80.
[3] Norberg M, Egevad L, Holmberg L, Sparen P, Norlen BJ,
Busch C. The sextant protocol for ultrasound-guided core
biopsies of the prostate underestimates the presence of
cancer. Urology 1997;50:562–6.
[4] Raaijmakers R, Blijenberg BG, Finlay JA, et al. Prostate
cancer detection in the prostate specific antigen range
of 2.0 to 3.9 ng/ml: value of percent free prostate specific
antigen on tumor detection and tumor aggressiveness.
J Urol 2004;171:2245–9.
[5] Thompson IM, Pauler DK, Goodman PJ, et al. Prevalence of
prostate cancer among men with a prostate-specific anti-
gen level < or = 4.0 ng per millilitre. N Engl J Med
2004;350:2239–46.
[6] Schiffer E. Biomarkers for prostate cancer. World J Urol
2007;25:557–62.
[7] Parekh DJ, Ankerst DP, Troyer D, Srivastava S, Thompson
IM. Biomarkers for prostate cancer detection. J Urol
2007;178:2252–9.
[8] Beemsterboer PM, Kranse R, de Koning HJ, Habbema JD,
Schroder FH. Changing role of 3 screening modalities in
the European randomized study of screening for prostate
cancer (Rotterdam). Int J Cancer 1999;84:437–41.
[9] Charlesworth PJ, Harris AL. Mechanisms of disease: angio-
genesis in urologic malignancies. Nat Clin Pract Urol
2006;3:157–69.
[10] Weidner N, Carroll PR, Flax J, Blumenfeld W, Folkman J.
Tumour angiogenesis correlates with metastasis in inva-
sive prostate carcinoma. Am J Pathol 1993;143:401–9.
[11] Borre M, Offersen BV, Nerstrom B, Overgaard J. Microves-
sel density predicts survival in prostate cancer patients
subjected to watchful waiting. Br J Cancer 1998;78:940–4.
[12] Brawer MK. Quantitative microvessel density. A staging
and prognostic marker for human prostatic carcinoma.
Cancer 1996;78:345–9.
[13] Feinstein SB. The powerful microbubble: from bench to
bedside, from intravascular indicator to therapeutic deliv-
ery system, and beyond. Am J Physiol Heart Circ Physiol
2004;287:H450–7.
[14] Albrecht T, Blomley M, Bolondi L, et al. Guidelines for the
use of contrast agents in ultrasound. Ultraschall Med
2004;25:249–56.
[15] De Jong N. Mechanical index. Eur J Echocardiogr 2002;
3:73–4.
[16] Sedelaar JP, van Leenders GJ, Hulsbergen-van de Kaa CA,
et al. Microvessel density: correlation between contrast
ultrasonography and histology of prostate cancer. Eur
Urol 2001;40:285–93.
[17] Goossen TEB, de la Rosette JJMCH, Hulsbergen-van de Kaa
CA, van Leenders GJLH, Wijkstra H. The value of dynamic
contrast enhanced power Doppler ultrasound imaging in
the localization of prostate cancer. Eur Urol 2003;43:124–31.
[18] Unal D, Sedelaar JP, Aarnink RG, et al. Three-dimensional
contrast-enhanced power Doppler ultrasonography and
conventional examination methods: the value of diagnos-
tic predictors of prostate cancer. BJU Int 2000;86:58–64.
[19] Frauscher F, Klauser A, Volgger H, et al. Comparison of
contrast enhanced color Doppler targeted biopsy with
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3992
conventional systematic biopsy: impact on prostate can-
cer detection. J Urol 2002;167:1648–52.
[20] Pelzer A, Bektic J, Berger AP, et al. Prostate cancer detec-
tion in men with prostate specific antigen 4 to 10 ng/ml
using a combined approach of contrast enhanced color
Doppler targeted and systematic biopsy. J Urol 2005;173:
1926–9.
[21] Mitterberger M, Pinggera GM, Horninger W, et al. Com-
parison of contrast enhanced color Doppler targeted
biopsy to conventional systematic biopsy: impact on
Gleason score. J Urol 2007;178:464–8.
[22] Mitterberger M, Pinggera G, Horninger W, et al. Dutasteride
prior to contrast-enhanced colour Doppler ultrasound
prostate biopsy increases prostate cancer detection. Eur
Urol 2008;53:112–7.
[23] Mitterberger M, Horninger W, Pelzer A, et al. A prospective
randomized trial comparing contrast-enhanced targeted
versus systematic ultrasound guided biopsies: impact on
prostate cancer detection. Prostate 2007;67:1537–42.
[24] Rouviere O, Curiel L, Chapelon JY, et al. Can color Doppler
predict the uniformity of HIFU-induced prostate tissue
destruction? Prostate 2004;60:289–97.
[25] Lyons BE, Samulski TV, Cox RS, Fessenden P. Heat loss
and blood flow during hyperthermia in normal canine
brain. I: Empirical study and analysis. Int J Hyperthermia
1989;5:225–47.
[26] Tilly W, Wust P, Rau B, et al. Temperature data and
specific absorption rates in pelvic tumours: predictive
factors and correlations. Int J Hyperthermia 2001;
17:172–88.
[27] Eckersley RJ, Sedelaar JP, Blomley MJ, et al. Quantitative
microbubble enhanced transrectal ultrasound as a tool
for monitoring hormonal treatment of prostate carci-
noma. Prostate 2002;51:256–67.
[28] Sedelaar JP, Aarnink RG, van Leenders GJ, et al. The
application of three-dimensional contrast-enhanced
ultrasound to measure volume of affected tissue after
HIFU treatment for localized prostate cancer. Eur Urol
2000;37:559–68.
[29] Blana A, Walter B, Rogenhofer S, Wieland WF. High-inten-
sity focused ultrasound for the treatment of localized
prostate cancer: 5-year experience. Urology 2004;63:297–
300.
[30] Gelet A, Chapelon JY, Bouvier R, Rouviere O, Lyonnet D,
Dubernard JM. Transrectal high intensity focused ultra-
sound for the treatment of localized prostate cancer:
factors influencing the outcome. Eur Urol 2001;40:
124–9.
[31] Rouviere O, Mege-Lechevallier F, Chapelon J-Y, et al. Eva-
luation of color Doppler in guiding prostate biopsy after
HIFU ablation. Eur Urol 2006;50:490–7.
[32] Strohmeyer D, Frauscher F, Klauser A, et al. Contrast-
enhanced transrectal color Doppler ultrasonography
(TRCDUS) for assessment of angiogenesis in prostate
cancer. Anticancer Res 2001;21:2907–13.
[33] Halpern EJ, McCue PA, Aksnes AK, Hagen EK, Frauscher F,
Gomella LG. Contrast-enhanced US of the prostate with
Sonazoid: comparison with whole-mount prostatectomy
specimens in 12 patients. Radiology 2002;222:361–6.
[34] van Moerkerk H, Heijmink SWTPJ, Hulsbergen-v.d. Kaa
CA, Barentsz JO, Witjes JA. Computerized three-dimen-
sional localization of prostate cancer using contrast-
enhanced power Doppler and clustering analysis. Eur Urol
2006;50:762–9.
[35] Takahashi N, Inoue T, Lee J, Yamaguchi T, Shizukuishi K.
The roles of PET and PET/CT in the diagnosis and manage-
ment of prostate cancer. Oncology 2007;72:226–33.
[36] Alonzi R, Padhani AR, Allen C. Dynamic contrast enhanced
MRI in prostate cancer. Eur J Radiol 2007;63:335–50.
[37] Futterer JJ. MR imaging in local staging of prostate cancer.
Eur J Radiol 2007;63:328–34.
[38] Engelbrecht MR, Jager GJ, Laheij RJ, Verbeek ALM, van Lier
HJ, Barentsz JO. Local staging of prostate cancer using
magnetic resonance imaging: a meta-analysis. European
Radiology 2002;12:2294–302.
[39] Kirkham APS, Emberton M, Allen C. How good is MRI at
detecting and characterising cancer within the prostate?
Eur Urol 2006;50:1163–75.
[40] Sciarra A, Panebianco V, Salciccia S, et al. Role of dynamic
contrast-enhanced magnetic resonance (MR) imaging and
proton MR spectroscopic imaging in the detection of local
recurrence after radical prostatectomy for prostate can-
cer. Eur Urol 2008;54:589–600.
[41] Kim CK, Park BK. Update of prostate magnetic resonance
imaging at 3 T. J Comput Assist Tomogr 2008;32:163–72.
[42] Pallwein L, Mitterberger M, Pelzer A, et al. Ultrasound of
prostate cancer: recent advances. Eur Radiol 2008;18:
707–15.
[43] Roy C, Buy X, Lang H, Saussine C, Jacqmin D. Contrast
enhanced color Doppler endorectal sonography of pros-
tate: efficiency for detecting peripheral zone tumours and
role for biopsy procedure. J Urol 2003;170:69–72.
[44] Halpern EJ, Ramey JR, Strup SE, Frauscher F, McCue P,
Gomella LG. Detection of prostate carcinoma with con-
trast-enhanced sonography using intermittent harmonic
imaging. Cancer 2005;104:2373–83.
[45] Mitterberger M, Colleselli D, Pelzer A, et al. Contrast
enhanced colour Doppler targeted biopsy for prostate
cancer detection: results of 2008 men. Eur Urol Suppl
2008;7:75.
[46] Rouviere O, Lyonnet D, Raudrant A, et al. MRI appearance
of prostate following transrectal HIFU ablation of loca-
lized cancer. Eur Urol 2001;40:265–74.
[47] Uchida T, Ohkusa H, Nagata Y, Hyodo T, Satoh T, Irie A.
Treatment of localized prostate cancer using high-inten-
sity focused ultrasound. BJU Int 2006;97:56–61.
[48] Wiart M, Curiel L, Gelet A, Lyonnet D, Chapelon JY, Rou-
viere O. Influence of perfusion on high-intensity focused
ultrasound prostate ablation: a first-pass MRI study. Magn
Reson Med 2007;58:119–27.
[49] Wink MH, Wijkstra H, de la Rosette JJ, Grimbergen CA.
Ultrasound imaging and contrast agents: a safe alterna-
tive to MRI? Minim Invasive Ther Allied Technol
2006;15:93–100.

Editorial Comment on: Contrast-EnhancedUltrasound and Prostate Cancer; A MulticentreEuropean Research Coordination ProjectAnurag K. SinghUniversity at Buffalo School of Medicine,Department of Radiation Medicine,Roswell Park Cancer Institute, Elm and Carlton Streets,Buffalo, NY 14263, United [email protected]
Prostate-specific antigen testing has allowed forthe detection of clinically insignificant prostatecancers that are unlikely to progress [1]. Detection,regardless of clinical significance, usually leads toaggressive treatment [2]. Since aggressive therapycarries attendant morbidity [3,4], it is critical to (1)determine which men are unlikely to progress toclinical significance and (2) evaluate methods toreduce treatment-related toxicity and/or toimprove efficacy.
Improved imaging that distinguishes benignfrom malignant prostate tissue would greatlyadvance both of these critical aims.
Despite the potential of imaging, routinelyemployed imaging technologies (computed tomo-graphy, positron emission tomography, ultra-sound, and magnetic resonance imaging) are notconsistently able to differentiate benign frommalignant tissues within the prostate. Develop-ment of methods to enhance standard imaging hasbeen impeded by limitations of research fundingand appropriate patients available for study. Amulti-institutional design, while increasing thepotential number of patients, is complicated by amultitude of factors including funding, initialperiods of operator dependence, intellectual prop-erty rights, data sharing, continuing evolution ofthe technology during the study period, andparochial interests such as institutional prestigeor individual career advancement.
In the context of such impediments, Wink et al[5] are to be lauded for their efforts to accumulatedata on contrast-enhanced ultrasound (CEUS) in aconcerted, multi-institutional manner. Theseefforts produced several publications, as refer-enced in the paper, from individual institutions. Inaddition, the pooled analysis provides valuablesafety, operator dependence, and time/cost dataderived from a remarkable number (>3000) CEUSstudies.
Ultimately, the authors concede they have notyet met their stated goal of bringing CEUS intoroutine practice. Although the ultimate utility ofCEUS in routine practice remains unknown, thisproject may serve as a model of multi-institutionalcollaboration to advance prostate imaging.
References
[1] Klotz L. Active surveillance for prostate cancer: for
whom? J Clin Oncol 2005;23:8165–9.
[2] Cooperberg MR, Broering JM, Kantoff PW, et al. Contem-
porary trends in low risk prostate cancer: risk assess-
ment and treatment. J Urol 2007;178:S14–9.
[3] Van Tol-Geerdink JJ, Stalmeier PF, Pasker-de Jong PC,
et al. Systematic review of the effect of radiation dose on
tumor control and morbidity in the treatment of pros-
tate cancer by 3D-CRT. Int J Radiat Oncol Biol Phys
2006;64:534–43.
[4] Hu JC, Elkin EP, Pasta DJ, et al. Predicting quality of life
after radical prostatectomy: results from CaPSURE. J Urol
2004;171:703–7, discussion 707–8.
[5] Wink M, Frauscher F, Cosgrove D, et al. Contrast-
enhanced ultrasound and prostate cancer; a multicentre
European research coordination project. Eur Urol 2008;
54:982–93.
DOI: 10.1016/j.eururo.2008.06.058
DOI of original article: 10.1016/j.eururo.2008.06.057
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 8 2 – 9 9 3 993