certolizumab pegol therapy of rheumatoid arthritis: overview
TRANSCRIPT
DRUG DEVELOPMENT RESEARCH 72 : 603–614 (2011)
Clinical Research
Certolizumab Pegol Therapy of RheumatoidArthritis: Overview
Ines Zidi,1,2� Wissem Mnif,1 Aicha Bouaziz,1,3 and Nidhal Ben Amor1,2
1Laboratory of Biochemistry, Research Unit 02/UR/09-01, Higher Institute of Biotechnology, BP74, Avenue Tahar Haddad, Monastir 5000, Tunisia
2Department of Biology, Sciences College, King Faisal University, P.O. Box 1759, 31982 Al-Ahsa,Saudi Arabia
3Laboratory of Basic Health Group, 4002 Sousse, Tunisia
Strategy, Management and Health Policy
Enabling
Technology,
Genomics,
Proteomics
Preclinical
Research
Preclinical Development
Toxicology, Formulation
Drug Delivery,
Pharmacokinetics
Clinical Development
Phases I-III
Regulatory, Quality,
Manufacturing
Postmarketing
Phase IV
ABSTRACT First-line treatment for moderate to severe rheumatoid arthritis (RA) has been the use ofdisease-modifying anti-rheumatic drugs (DMARDs), e.g., methotrexate. Because of the cases of failurereported to respond to available treatments, newer RA drugs including tumor necrosis factor (TNF-a) blockershave emerged. Certolizumab pegol (CZP) is a unique polyethylene glycolated (PEG) humanized monoclonalantibody designed specifically to target TNF-a pro-inflammatory cytokine. Given that its properties closelyreflect its PEG fragment, CZP has demonstrated a clear efficiency. Pharmacokinetics and pharmacodynamicsof CZP are described together with Phase II and III CZP clinical studies focused on CZP efficiency and safety.We also discuss the future of CZP and new clinical studies that might help physicians in their choice of CZPamong available TNF-a blockers. Drug Dev Res 72:603–614, 2011. r 2011 Wiley Periodicals, Inc.
Key words: Certolizumab pegol; TNF-a; inhibitors; rheumatoid arthritis; autoimmune disease
INTRODUCTION
Rheumatoid arthritis (RA) is the most commoninflammatory arthritis affecting the small joints of thehands and feet [Lee and Weinblatt, 2001; Scott et al.,2010]. Without treatment, RA becomes more aggres-sive, leading to pronounced disability and a reductionof quality of life, as well as loss of work [Pincus andSokka, 2001]. The main societal consequence is thehigh economic burden [Kavanaugh et al., 2009].
The etiology of RA is unknown, but it is classiedas an autoimmune disease [Wordsworth and Holden,2005]. Accumulating evidence indicates that bothinnate and acquired immunity are involved in RA.Clinically, inflammatory immune cells including lym-phocytes and macrophages occur in the joints andother tissues [Bugatti et al., 2007; MaciejewskaRodrigues et al., 2009]. Moreover, the presence of
autoantibodies reactive with cyclic citrullinated pep-tides (CCP), vimentin, decorin, enolase, aldolaseA, and type II collagen has been demonstrated[Maciejewska Rodrigues et al., 2009; Scott et al., 2010].
There is consistent evidence that tumor necrosisfactor (TNF-a), a pro-inflammatory cytokine, isrelevant to the pathogenesis of RA. TNF-a is foundin high concentrations in the joints [Brennan et al.,1989]. Its effects are mediated, at least in part,by the synthesis of pro-inflammatory cytokines, theinterleukins IL-1 and IL-6, and growth factors, e.g.,
DDR
Published online in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ddr.20470
�Correspondence to: Ines Zidi, Laboratory of Biochemistry,Research Unit 02/UR/09-01, Higher Institute of Biotechnology, BP74, Avenue Tahar Haddad, Monastir 5000, Tunisia.E-mail: [email protected]
�c 2011 Wiley Periodicals, Inc.

granulocyte-colony stimulating factor (GCS-F) andgranulocyte macrophage-colony stimulating factor(GM-CSF) [Barnes and Moots, 2007; Zidi et al.,2010; Scott et al., 2010]. TNF-a is involved in theoverproduction of prostaglandins, platelet activatingfactor, and nitric oxide [Food and Drug Administration,2009].
Several biochemical markers can be used topredict the stage of the disease, including markers forjoint disease (e.g., rheumatoid factor, anti-CCP anti-bodies), for bone turnover (bone formation or boneresorption), for cartilage turnover, and lastly, formarkers of synovitis and inflammation [Ehlers andLeary, 2008].
First-line treatment of RA involves the use bydisease-modifying antirheumatic drugs (DMARDs) incombination with corticosteroids and/or nonsteroidalanti-inflammatory drugs (NSAIDs) as an alternative tomonotherapy [Wilke and Clough, 1991]. Methotrexate(MTX) is the most commonly used DMARD for RAtreatment [Scott et al., 2010].
In addition, several biologic agents have beenproposed to treat RA that may target differentmediators of the disease. Abatacept (cytotoxicT-lymphocyte-associated antigen 4-immunoglobulin,Belatacept), a soluble recombinant protein, inhibitsT-cell function through CTLA-4 blockade that mimicsand competes with the co-stimulatory molecule CD28of regulatory T cells [Senolt et al., 2009; Boissier et al.,2010]. Rituximab (Mabthera, Rituxan), a chimeric anti-CD20 monoclonal antibody, can also be used in RAtherapy. It targets CD20 on B-cell lymphocytes,inducing their depletion [Yen, 2006; Senolt et al.,2009]. This impairs production of autoantibodies (e.g.,rheumatoid factor, anti-CCP antibodies), as well as theproduction of different growth and differentiationfactors that play key roles in the synovial microenvir-onment [Boissier et al., 2010].
Currently used biologic therapies for RAinclude IL-1 (Anakinra, Kineret) and IL-6 inhibitors(Tocilizumab, Actemra) [Senolt et al., 2009; Boissieret al., 2010]. Another class of biologic used to treat RAis the TNF-a blockers that include monoclonalantibodies and fusion proteins. TNF-a blockers areeffective in the treatment of moderate to severe activeRA, specifically inhibiting TNF-a in both its mem-brane-attached and soluble forms. TNF-a blockersinclude TNF-a antibodies, e.g., infliximab (Remicade),adalimumab (Humira), golimumab (Simponi), andcertolizumab pegol (CZP) (Cimzia). Decoy receptorsinclude etanercept (TNR-001, Enbrel).
Infliximab is the only chimeric antibody asso-ciated with high levels of reactive antibodies inclu-ding anti-drug antibodies (ADA; e.g., anti-infliximab
antibodies) and autoantibodies. However, TNF-ahumanized blockers are associated with decreasedproduction of the previously detected antibodies. Thisgroup of blockers also includes the polyethyleneglycolated antibody, CZP.
The focus of this review is on literature relating toCZP, including clinical trials reporting its efficiency,safety, and potential adverse events and comorbidities.The significant body of data identifying the propertiesof CZP associated with its polyethylene glycol (PEG)fragment is also reviewed. Furthermore, we discussand propose some ideas that may be useful in thedesign of future studies required for resolving thedebated side effects and associated complications ofCZP, and for exploiting its advantageous properties.
Pharmacology of Certolizumab Pegol
Description
CZP is a recombinant humanized monoclonalunivalent antibody with an approximate molecularweight of 91 KD [Food and Drug Administration,2009]. It is composed of the fragment antigen-bindingdomain (Fab0) that targets TNF-a conjugated via amaleimide linkage to a PEG fragment (2� 20 KD,PEG2MAL40K) [Barnes and Moots, 2007; Shealy andVisvanathan, 2008; Food and Drug Administration,2009] (Table 1).
TABLE 1. Certolizumab Pegol Characteristics
Commercialname Cimzias
Other names CDP 870Description Humanized polyethylene-glycolated (PEG) Fab0
fragment of anti-tumor necrosis factorProducer UCBTotal size (kDa) �91 kDaPEG fragment size(kDa)
40 kDa (2�20 kDa)
Initial dose 400 mg (two SC injections of 200 mg) at weeks 0,2, and 4; followed by 200 mg every other week
Maintenancedose
400 mg every 4 weeks
FDA approval May 2009 for RA therapy (treatment of adults withmoderately to severely active RA)April 2008 for CD therapy (treatment of adultswith moderately to severely active CD withinadequate response to other treatments)
EMG approval October 2009 for RA therapy (treatment of adultswith moderately to severe active RA when theresponse to DMARDs including methotrexate, hasbeen inadequate)
CD, Crohn’s disease; DMARDs, disease-modifying antirheumaticdrugs; EMG, European Medicines Agency; FDA, Food and DrugAdministration; RA, rheumatoid arthritis; SC, subcutaneous.
604 ZIDI ET AL.
Drug Dev. Res.

The Fab0 fragment manufactured in Escherichiacoli is composed of a light chain with 214 amino acids(AA) and a heavy chain with 229 AA [Food and DrugAdministration, 2009]. The PEG fragment, a hydro-philic polymer, consists of repeated ethylene glycolsubunits [Alexis et al., 2008].
The lack of toxicity of CZP led to its approval bythe FDA [Monfardini and Veronese, 1998] for thetreatment of adults suffering from moderate to severeactive RA, and also for the treatment Crohn’s disease.Nevertheless, the European Medicines Agency has sofar approved its use only for RA (Table 1).
CZP is used by the subcutaneous route (s.c.) andhas similar effects intravenously (i.v.) [Kaushik andMoots, 2005; Barnes and Moots, 2007]. CZP can beadministrated as monotherapy or in combination withMTX to improve disease outcomes [Furst et al., 2011].The recommended dose for patients with RA is 400 mgat weeks 0, 2, and 4; followed by 200 mg every otherweek (Table 1) (see other recommendations of CZP use[Ding et al., 2010]). The maintenance dose was 400 mgevery 4 weeks [Food and Drug Administration, 2009].Using a pharmacodynamic-Markov mixed-effectsmodel of simulation of the American College ofRheumatology (ACR) 20 measure, Lacroix et al.[2009] supported CZP dosing, while reporting analternative maintenance regimen of 400 mg once amonth. In the study conducted by Kaushik et al.[2005], the optimal IV dose of CZP in RA patients was5 mg/kg/month [Kaushik and Moots, 2005; Shealy andVisvanathan, 2008]. The peak plasma CZP concentra-tion, linear with dosing, occurs at the end of theinfusion and declined thereafter [Choy et al., 2002;Shealy and Visvanathan, 2008].
The PEG fragment role has been extensivelyinvestigated and has been found to be effective inreducing immunogenicity in DZP. PEGylation alsoincreases the half-life of CZP to 13–14 days. WithoutPEG, the biological half-life is 0.3–0.8 days [Chameset al., 2009]. This decreases the distribution volumeand injection frequency (single s.c. injection once amonth) [Barnes and Moots, 2007; Pisal, Kosloski andBalu-Iyer, 2010]. PEGylation also decreases urinaryclearance and proteolysis by trypsin and chymotrypsin[Lu et al., 2008; Pisal et al., 2010; Singh, 2011] andenhances the solubility and stability of proteins bymasking their hydrophobic sites involved in aggrega-tion, nonfunctionality, and immunogenicity [Lu et al.,2008; Pisal et al., 2010; Singh, 2011].
Pharmacodynamics
CZP, like other TNF-ablockers, specifically tar-gets TNF-a, inhibiting its function. CZP can inhibitboth membrane-associated and soluble TNF-a. CZP
does not bind TNF-b (lymphotoxin a). TNF-a inhibi-tion by CZP proves that the crystallizable fragment(Fc) is not essential for this function [Scott and Cope,2009]. Fossati and Nesbitt [2011a] demonstratedin vitro that CZP 90% inhibitory concentration (IC90)neutralization activity is observed at 2.5 ng/ml. This isclose to the IC90 of etanercept (0.3 ng/ml) and belowthe IC90 values of infliximab and adalimumab (20 ng/mland 15 ng/ml, respectively). CZP was the most potentinhibitor of LPS-driven IL-1b secretion as comparedwith all reported TNF antibodies. However, no knownfunction has been ascribed to the latter observation[Fossati and Nesbitt, 2011a].
Administration of intact and large antibodies(constituted from two Fab fragments and one Fcfragment) is associated with frequent disadvantagesthat include immunogenicity, difficulty of diffusion, aswell as poor tissue penetration [Elbakri et al., 2010].The reduced size of CZP is thus advantageous,exhibiting better penetration into arthritic tissues andreduced immunogenicity [Taylor, 2010; Nesbitt et al.,2008]. Indeed, CZP does not contain the Fc fragmentinvolved in complement activation and in antibody-dependent cell-mediated cytotoxicity in vitro [Foodand Drug Administration, 2009].
The univalent structure of CZP is also advanta-geous because of the small immune complexes formedwith TNF-a, low passage through the placenta, and lessaccumulation in milk as compared with other IgG1anti-TNF-a antibodies [Nesbitt et al., 2008]. Moreover,CZP does not stimulate apoptosis in vitro in monocytesor lymphocytes [Fossati and Nesbitt, 2011a] and doesnot cause neutrophil necrosis [Fossati and Nesbitt,2011a].
CZP has reduced opsonization properties [Alexiset al., 2008], especially a reduced mononuclearphagocyte system rate [Li and Huang, 2008]. CZP isthe only TNF-a blocker that does not induceneutrophil degranulation in vitro [Food and DrugAdministration, 2009]. Indeed, Fossati and Nesbitt[2011b] found that the PEG fragment associated withFab0 in CZP inhibited Ca21 flux in cellular systems(IC50 �10 mg/ml) explaining the very low incidence ofCZP injection site pain in clinical studies.
Pharmacokinetics
The pharmacokinetic properties of CZP closelyrelate to its PEG fragment. Increased vascular perme-ability and retention are examples of the biologicalrelevance of PEGylation [Palframan et al., 2009]. Usingbiofluorescence imaging, CZP has enhanced penetra-tion in inflamed arthritic paws as compared with theTNF-a blockers adalimumab and infliximab [Palframanet al., 2009]. The steady-state volume of distribution
605CERTOLIZUMAB IN RHEUMATOID ARTHRITIS
Drug Dev. Res.
was estimated at 6-8L in RA patients [Food and DrugAdministration, 2009]. In addition, this antibodyremains for prolonged periods in inflamed tissuesversus normal ones, and accumulates to higher tissuelevels as compared with adalimumab and infliximab[Palframan et al., 2009].
In addition to its lack of toxicity, low immuno-genicity, and reduced clearance, the PEG fragment isassociated with favorable excretion kinetics withoutfurther metabolism [Monfardini and Veronese, 1998;Food and Drug Administration, 2009]. Followingsubcutaneous injection of CZP in RA patients theclearance rate is estimated at 21 mL/h (with 30.8%inter-subject variability and 16% inter-occasion varia-bility) [Food and Drug Administration, 2009].
Clinical Studies Using Certolizumab Pegol
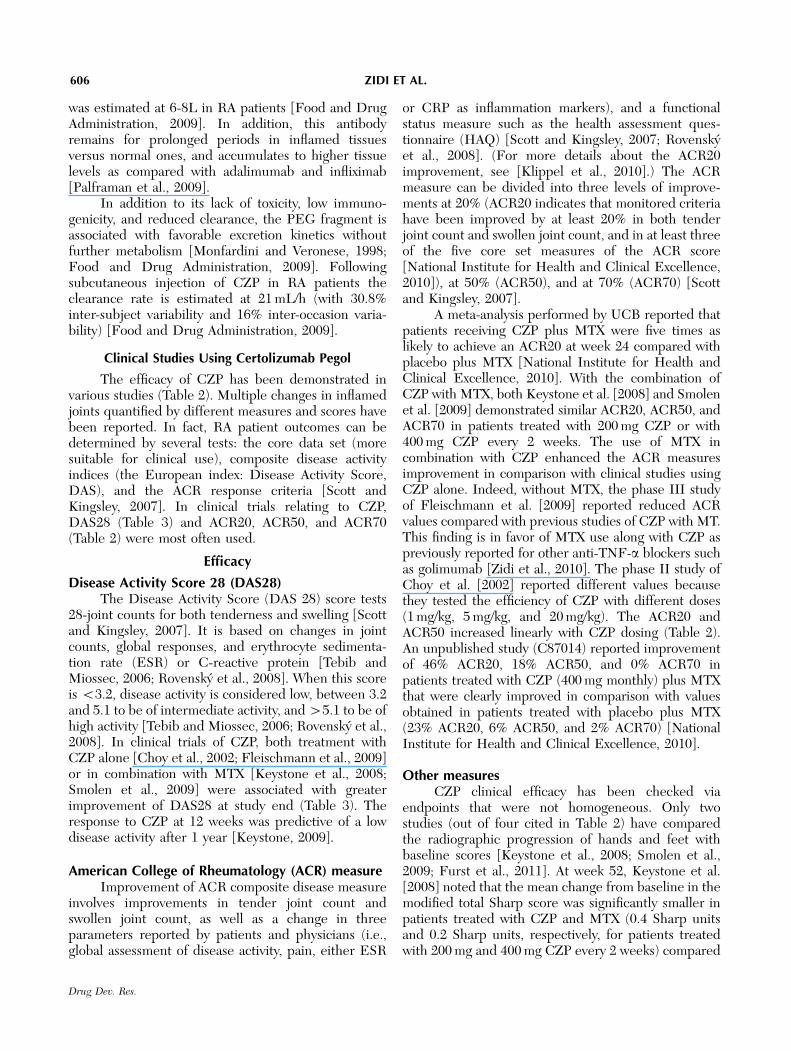
The efficacy of CZP has been demonstrated invarious studies (Table 2). Multiple changes in inflamedjoints quantified by different measures and scores havebeen reported. In fact, RA patient outcomes can bedetermined by several tests: the core data set (moresuitable for clinical use), composite disease activityindices (the European index: Disease Activity Score,DAS), and the ACR response criteria [Scott andKingsley, 2007]. In clinical trials relating to CZP,DAS28 (Table 3) and ACR20, ACR50, and ACR70(Table 2) were most often used.
Efficacy
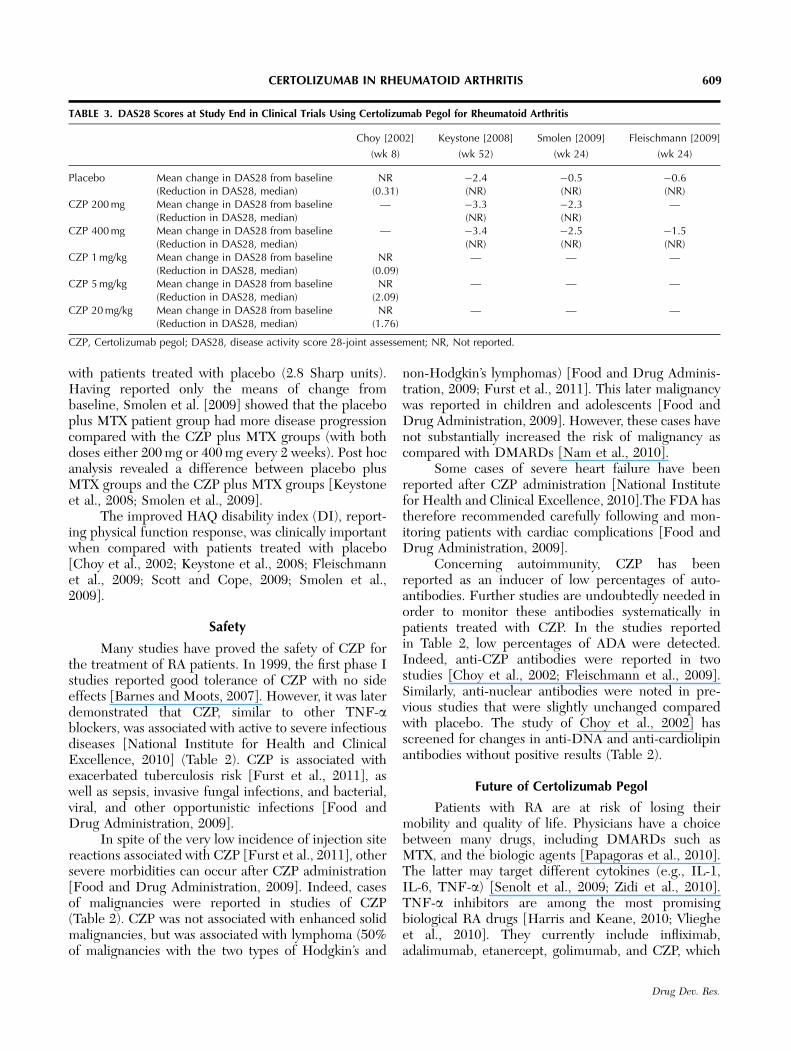
Disease Activity Score 28 (DAS28)The Disease Activity Score (DAS 28) score tests
28-joint counts for both tenderness and swelling [Scottand Kingsley, 2007]. It is based on changes in jointcounts, global responses, and erythrocyte sedimenta-tion rate (ESR) or C-reactive protein [Tebib andMiossec, 2006; Rovensky et al., 2008]. When this scoreis o3.2, disease activity is considered low, between 3.2and 5.1 to be of intermediate activity, and 45.1 to be ofhigh activity [Tebib and Miossec, 2006; Rovensky et al.,2008]. In clinical trials of CZP, both treatment withCZP alone [Choy et al., 2002; Fleischmann et al., 2009]or in combination with MTX [Keystone et al., 2008;Smolen et al., 2009] were associated with greaterimprovement of DAS28 at study end (Table 3). Theresponse to CZP at 12 weeks was predictive of a lowdisease activity after 1 year [Keystone, 2009].
American College of Rheumatology (ACR) measureImprovement of ACR composite disease measure
involves improvements in tender joint count andswollen joint count, as well as a change in threeparameters reported by patients and physicians (i.e.,global assessment of disease activity, pain, either ESR
or CRP as inflammation markers), and a functionalstatus measure such as the health assessment ques-tionnaire (HAQ) [Scott and Kingsley, 2007; Rovenskyet al., 2008]. (For more details about the ACR20improvement, see [Klippel et al., 2010].) The ACRmeasure can be divided into three levels of improve-ments at 20% (ACR20 indicates that monitored criteriahave been improved by at least 20% in both tenderjoint count and swollen joint count, and in at least threeof the five core set measures of the ACR score[National Institute for Health and Clinical Excellence,2010]), at 50% (ACR50), and at 70% (ACR70) [Scottand Kingsley, 2007].
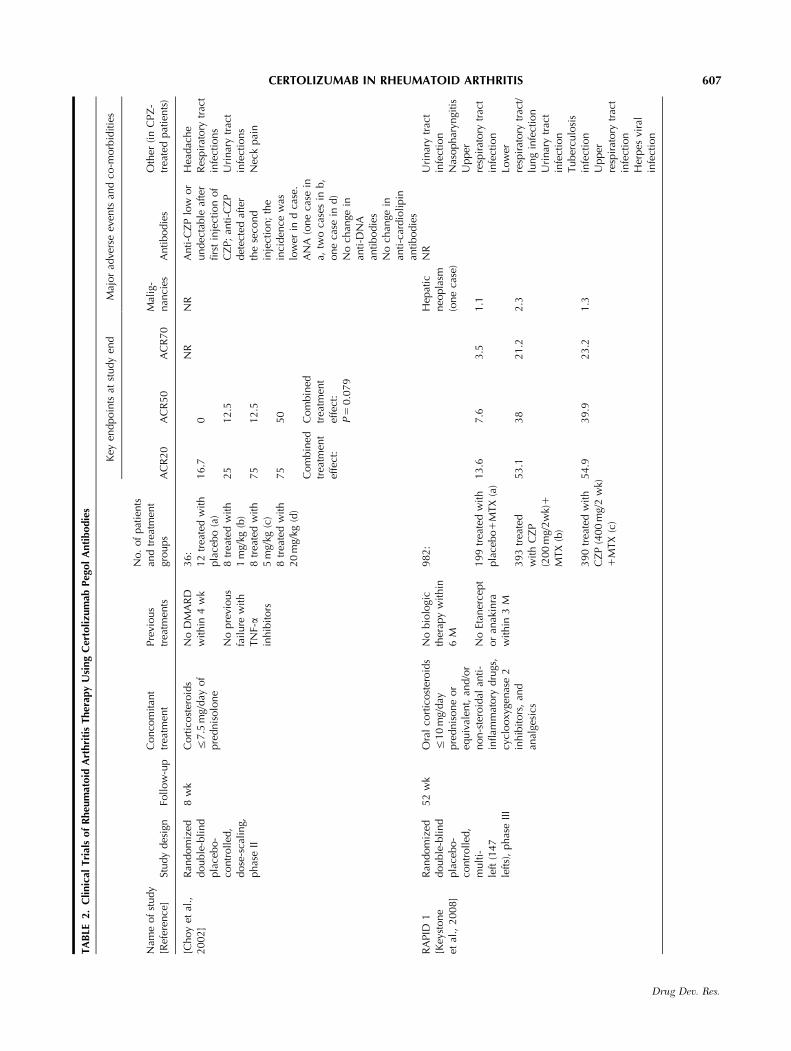
A meta-analysis performed by UCB reported thatpatients receiving CZP plus MTX were five times aslikely to achieve an ACR20 at week 24 compared withplacebo plus MTX [National Institute for Health andClinical Excellence, 2010]. With the combination ofCZP with MTX, both Keystone et al. [2008] and Smolenet al. [2009] demonstrated similar ACR20, ACR50, andACR70 in patients treated with 200 mg CZP or with400 mg CZP every 2 weeks. The use of MTX incombination with CZP enhanced the ACR measuresimprovement in comparison with clinical studies usingCZP alone. Indeed, without MTX, the phase III studyof Fleischmann et al. [2009] reported reduced ACRvalues compared with previous studies of CZP with MT.This finding is in favor of MTX use along with CZP aspreviously reported for other anti-TNF-a blockers suchas golimumab [Zidi et al., 2010]. The phase II study ofChoy et al. [2002] reported different values becausethey tested the efficiency of CZP with different doses(1 mg/kg, 5 mg/kg, and 20 mg/kg). The ACR20 andACR50 increased linearly with CZP dosing (Table 2).An unpublished study (C87014) reported improvementof 46% ACR20, 18% ACR50, and 0% ACR70 inpatients treated with CZP (400 mg monthly) plus MTXthat were clearly improved in comparison with valuesobtained in patients treated with placebo plus MTX(23% ACR20, 6% ACR50, and 2% ACR70) [NationalInstitute for Health and Clinical Excellence, 2010].
Other measuresCZP clinical efficacy has been checked via
endpoints that were not homogeneous. Only twostudies (out of four cited in Table 2) have comparedthe radiographic progression of hands and feet withbaseline scores [Keystone et al., 2008; Smolen et al.,2009; Furst et al., 2011]. At week 52, Keystone et al.[2008] noted that the mean change from baseline in themodified total Sharp score was significantly smaller inpatients treated with CZP and MTX (0.4 Sharp unitsand 0.2 Sharp units, respectively, for patients treatedwith 200 mg and 400 mg CZP every 2 weeks) compared
606 ZIDI ET AL.
Drug Dev. Res.
TA
BLE
2.
Clinic
alTri
als
of
Rheu
mat
oid
Art
hri
tis
Ther
apy
Usi
ng
Cer
toli
zum
abPeg
ol
Anti
bodie
s
Key
endpoin
tsat
study
end
Maj
or
adve
rse
even
tsan
dco
-morb
iditie
s
Nam
eof
study
[Ref
eren
ce]
Study
des
ign
Foll
ow
-up
Conco
mit
ant
trea
tmen
tPre
vious
trea
tmen
ts
No.
of
pat
ients
and
trea
tmen
tgr
oups
AC
R20
AC
R50
AC
R70
Mal
ig-
nan
cies
Anti
bodie
sO
ther
(in
CPZ
-tr
eate
dpat
ients
)
[Choy
etal
.,2002]
Ran
dom
ized
double
-bli
nd
pla
cebo-
contr
olled
,dose
-sca
ling,
phas
eII
8w
kC
ort
icost
eroid
sr
7.5
mg/
day
of
pre
dnis
olo
ne
No
DM
AR
Dw
ithin
4w
k
No
pre
vious
fail
ure
with
TN
F-a
inhib
itors
36:
12
trea
ted
wit
hpla
cebo
(a)
8tr
eate
dw
ith
1m
g/kg
(b)
8tr
eate
dw
ith
5m
g/kg
(c)
8tr
eate
dw
ith
20
mg/
kg(d
)
16.7
25
75
75
Com
bin
edtr
eatm
ent
effe
ct:�
0 12.5
12.5
50
Com
bin
edtr
eatm
ent
effe
ct:
P5
0.0
79
NR
NR
Anti-C
ZP
low
or
undec
table
afte
rfirs
tin
ject
ion
of
CZ
P;
anti
-CZ
Pdet
ecte
daf
ter
the
seco
nd
inje
ctio
n;
the
inci
den
cew
aslo
wer
ind
case
.A
NA
(one
case
ina,
two
case
sin
b,
one
case
ind)
No
chan
gein
anti
-DN
Aan
tibodie
sN
och
ange
inan
ti-c
ardio
lipin
anti
bodie
s
Hea
dac
he
Res
pir
atory
trac
tin
fect
ions
Uri
nar
ytr
act
infe
ctio
ns
Nec
kpai
n
RA
PID
1[K
eyst
one
etal
.,2008]
Ran
dom
ized
double
-bli
nd
pla
cebo-
contr
olled
,m
ult
i-le
ft(1
47
left
s),
phas
eII
I
52
wk
Ora
lco
rtic
ost
eroid
sr
10
mg/
day
pre
dnis
one
or
equiv
alen
t,an
d/o
rnon-s
tero
idal
anti
-in
flam
mat
ory
dru
gs,
cycl
ooxy
genas
e2
inhib
itors
,an
dan
alge
sics
No
bio
logi
cth
erap
yw
ithin
6M
No
Etan
erce
pt
or
anak
inra
wit
hin
3M
982:
199
trea
ted
wit
hpla
cebo
1M
TX
(a)
393
trea
ted
wit
hC
ZP
(200
mg/
2w
k)1
MTX
(b)
390
trea
ted
wit
hC
ZP
(400
mg/
2w
k)1
MTX
(c)
13.6
53.1���
54.9���
7.6
38���
39.9���
3.5
21.2���
23.2���
Hep
atic
neo
pla
sm(o
ne
case
)
1.1
2.3
1.3
NR
Uri
nar
ytr
act
infe
ctio
nN
asophar
yngi
tis
Upper
resp
irat
ory
trac
tin
fect
ion
Low
erre
spir
atory
trac
t/lu
ng
infe
ctio
nU
rinar
ytr
act
infe
ctio
nTuber
culo
sis
infe
ctio
nU
pper
resp
irat
ory
trac
tin
fect
ion
Her
pes
vira
lin
fect
ion
607CERTOLIZUMAB IN RHEUMATOID ARTHRITIS
Drug Dev. Res.
TA
BLE
2.
Cli
nic
alTri
als
of
Rheu
mat
oid
Art
hri
tis
Ther
apy
Usi
ng
Cer
toli
zum
abPeg
ol
Anti
bodie
s(C
onti
nued
)
Key
endpoin
tsat
study
end
Maj
or
adve
rse
even
tsan
dco
-morb
iditie
s
Nam
eof
study
[Ref
eren
ce]
Study
des
ign
Foll
ow
-up
Conco
mit
ant
trea
tmen
tPre
vious
trea
tmen
ts
No.
of
pat
ients
and
trea
tmen
tgr
oups
AC
R20
AC
R50
AC
R70
Mal
ig-
nan
cies
Antibodie
sO
ther
(in
CPZ
-tr
eate
dpat
ients
)
RA
PID
2[S
mole
net
al.,
2009]
Ran
dom
ized
double
-bli
nd
pla
cebo-
contr
olled
,m
ult
ilef
t(7
6le
fts)
,phas
eII
I
24
wk
Ora
lco
rtic
ost
eroid
sr
10
mg/
day
pre
dnis
one
or
equiv
alen
t,an
dnonst
eroid
alan
ti-
inflam
mat
ory
dru
gs,
cycl
ooxy
genas
e2
inhib
itors
(if
stab
lew
ithin
28
and
14
day
sre
spec
tive
ly)
No
bio
logi
cth
erap
yw
ithin
6M
No
Etan
erce
pt
or
anak
inra
within
3M
619:
127
trea
ted
wit
hpla
cebo
1M
TX
(a)
246
trea
ted
wit
hC
ZP
(200
mg/
2w
k)1
MTX
(b)
246
trea
ted
wit
hC
ZP
(400
mg/
2w
k)1
MTX
(c)
8.7
57.3���
57.6���
3.1
32.5���
33.1���
0.8
15.9��
10.6��
One
case
of
bla
dder
cance
rO
ne
case
of
test
icula
rca
nce
rO
ne
case
of
colo
nca
nce
r
Anti-C
ZP
in5.1
%of
pat
ients
rece
iv-
ing
CZ
P1
MTX
Neu
tral
isin
gan
tibodie
s:2%
(b),
1.6
%(c
)
Uri
nar
ytr
act
infe
ctio
nU
pper
resp
irat
ory
trac
tin
fect
ion
Hea
dac
he
Bac
teri
uri
aN
asophar
yngi
tis
Rheu
mat
oid
arth
riti
sH
yper
tensi
on
Hem
aturi
aH
epat
icen
zym
ein
crea
sed
AST
incr
ease
dA
LTin
crea
sed
FAST
4W
AR
D[F
leis
chm
ann
etal
.,2009]
Ran
dom
ized
double
-bli
nd
pla
cebo-
contr
olled
,m
ult
ilef
t(3
6le
fts)
,phas
eII
I
24
wk
Ora
lco
rtic
ost
eroid
sr
10
mg/
day
pre
dnis
one
equiv
alen
tst
able
for
Z4
wk
bef
ore
enro
llm
ent
and
duri
ng
the
study,
and
nonst
eroid
alan
ti-i
nflam
mat
ory
dru
gs,
anal
gesi
cs.
No
bio
logi
cth
erap
yw
ithin
6M
220:
109
trea
ted
wit
hpla
cebo
(a)
111
trea
ted
wit
hC
ZP
(400
mg/
4w
k)(b
)
9.3
45.5���
3.7
22.7���
0 5.5�
0 One
case
of
ute
rine
fibro
ids,
one
case
of
beg
nin
par
a-th
yroid
tum
or
Anti-C
ZP
Neu
tral
isin
gan
tibodie
s(b
,8.1
%)
AN
A:
a,11%
/b,
17%
Bac
teri
alar
thri
tis
Salm
onel
laar
thri
tis
Incr
ease
dblo
od
crea
tinin
e/in
crea
sed
blo
od
ure
aIs
chem
icst
roke
Men
orr
hag
ia
No
intr
a-ar
ticu
lar,
per
iart
icula
r,in
tram
usc
ula
r,an
din
trav
enous
cort
icost
eroid
s.
AC
R,
Am
eric
anC
oll
ege
of
Rheu
mat
olo
gy;
ALT
,al
anin
eam
inotr
ansf
eras
e;A
NA
;an
ti-n
ucl
ear
anti
bodie
s;A
ST,
aspar
tate
amin
otr
ansf
eras
e;C
ZP,
Cer
toli
zum
abpeg
ol;
DM
AR
D,
dis
ease
-m
odif
ying
anti
rheu
mat
icdru
gs;FA
ST4W
AR
D,ef
ficA
cyan
dSa
fety
ofce
rToli
zum
abpeg
ol,
4W
eekl
ydosA
gein
Rheu
mat
oiD
arth
riti
s,M
,m
onth
,M
TX
,m
ethotr
exat
e,N
R,notre
port
ed,R
APID
,R
heu
mat
oid
Art
hri
tis
Pre
venti
on
of
stru
ctura
lD
amag
e;w
k,w
eek.� P
r0.0
5;��
Pr
0.0
1;��� P
o0.0
01.
608 ZIDI ET AL.
Drug Dev. Res.
with patients treated with placebo (2.8 Sharp units).Having reported only the means of change frombaseline, Smolen et al. [2009] showed that the placeboplus MTX patient group had more disease progressioncompared with the CZP plus MTX groups (with bothdoses either 200 mg or 400 mg every 2 weeks). Post hocanalysis revealed a difference between placebo plusMTX groups and the CZP plus MTX groups [Keystoneet al., 2008; Smolen et al., 2009].
The improved HAQ disability index (DI), report-ing physical function response, was clinically importantwhen compared with patients treated with placebo[Choy et al., 2002; Keystone et al., 2008; Fleischmannet al., 2009; Scott and Cope, 2009; Smolen et al.,2009].
Safety
Many studies have proved the safety of CZP forthe treatment of RA patients. In 1999, the first phase Istudies reported good tolerance of CZP with no sideeffects [Barnes and Moots, 2007]. However, it was laterdemonstrated that CZP, similar to other TNF-ablockers, was associated with active to severe infectiousdiseases [National Institute for Health and ClinicalExcellence, 2010] (Table 2). CZP is associated withexacerbated tuberculosis risk [Furst et al., 2011], aswell as sepsis, invasive fungal infections, and bacterial,viral, and other opportunistic infections [Food andDrug Administration, 2009].
In spite of the very low incidence of injection sitereactions associated with CZP [Furst et al., 2011], othersevere morbidities can occur after CZP administration[Food and Drug Administration, 2009]. Indeed, casesof malignancies were reported in studies of CZP(Table 2). CZP was not associated with enhanced solidmalignancies, but was associated with lymphoma (50%of malignancies with the two types of Hodgkin’s and
non-Hodgkin’s lymphomas) [Food and Drug Adminis-tration, 2009; Furst et al., 2011]. This later malignancywas reported in children and adolescents [Food andDrug Administration, 2009]. However, these cases havenot substantially increased the risk of malignancy ascompared with DMARDs [Nam et al., 2010].
Some cases of severe heart failure have beenreported after CZP administration [National Institutefor Health and Clinical Excellence, 2010].The FDA hastherefore recommended carefully following and mon-itoring patients with cardiac complications [Food andDrug Administration, 2009].
Concerning autoimmunity, CZP has beenreported as an inducer of low percentages of auto-antibodies. Further studies are undoubtedly needed inorder to monitor these antibodies systematically inpatients treated with CZP. In the studies reportedin Table 2, low percentages of ADA were detected.Indeed, anti-CZP antibodies were reported in twostudies [Choy et al., 2002; Fleischmann et al., 2009].Similarly, anti-nuclear antibodies were noted in pre-vious studies that were slightly unchanged comparedwith placebo. The study of Choy et al., 2002] hasscreened for changes in anti-DNA and anti-cardiolipinantibodies without positive results (Table 2).
Future of Certolizumab Pegol
Patients with RA are at risk of losing theirmobility and quality of life. Physicians have a choicebetween many drugs, including DMARDs such asMTX, and the biologic agents [Papagoras et al., 2010].The latter may target different cytokines (e.g., IL-1,IL-6, TNF-a) [Senolt et al., 2009; Zidi et al., 2010].TNF-a inhibitors are among the most promisingbiological RA drugs [Harris and Keane, 2010; Vliegheet al., 2010]. They currently include infliximab,adalimumab, etanercept, golimumab, and CZP, which
TABLE 3. DAS28 Scores at Study End in Clinical Trials Using Certolizumab Pegol for Rheumatoid Arthritis
Choy [2002] Keystone [2008] Smolen [2009] Fleischmann [2009]
(wk 8) (wk 52) (wk 24) (wk 24)
Placebo Mean change in DAS28 from baseline NR �2.4 �0.5 �0.6(Reduction in DAS28, median) (0.31) (NR) (NR) (NR)
CZP 200 mg Mean change in DAS28 from baseline — �3.3 �2.3 —(Reduction in DAS28, median) (NR) (NR)
CZP 400 mg Mean change in DAS28 from baseline — �3.4 �2.5 �1.5(Reduction in DAS28, median) (NR) (NR) (NR)
CZP 1 mg/kg Mean change in DAS28 from baseline NR — — —(Reduction in DAS28, median) (0.09)
CZP 5 mg/kg Mean change in DAS28 from baseline NR — — —(Reduction in DAS28, median) (2.09)
CZP 20 mg/kg Mean change in DAS28 from baseline NR — — —(Reduction in DAS28, median) (1.76)
CZP, Certolizumab pegol; DAS28, disease activity score 28-joint assessement; NR, Not reported.
609CERTOLIZUMAB IN RHEUMATOID ARTHRITIS
Drug Dev. Res.
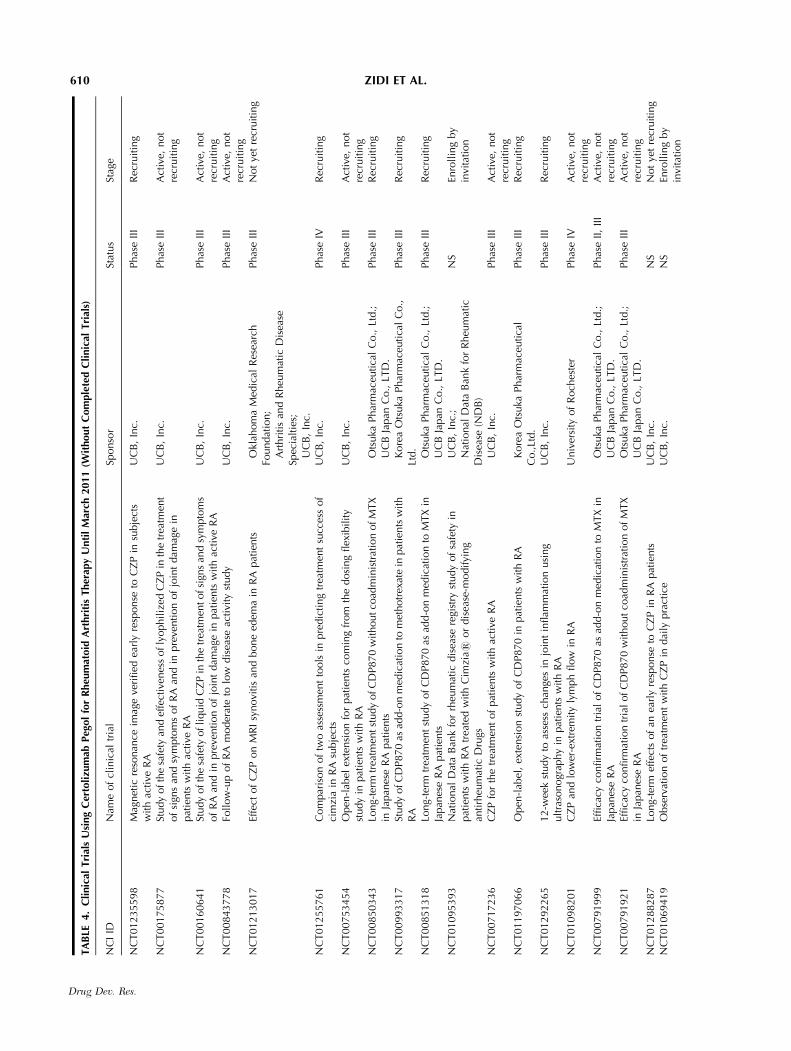
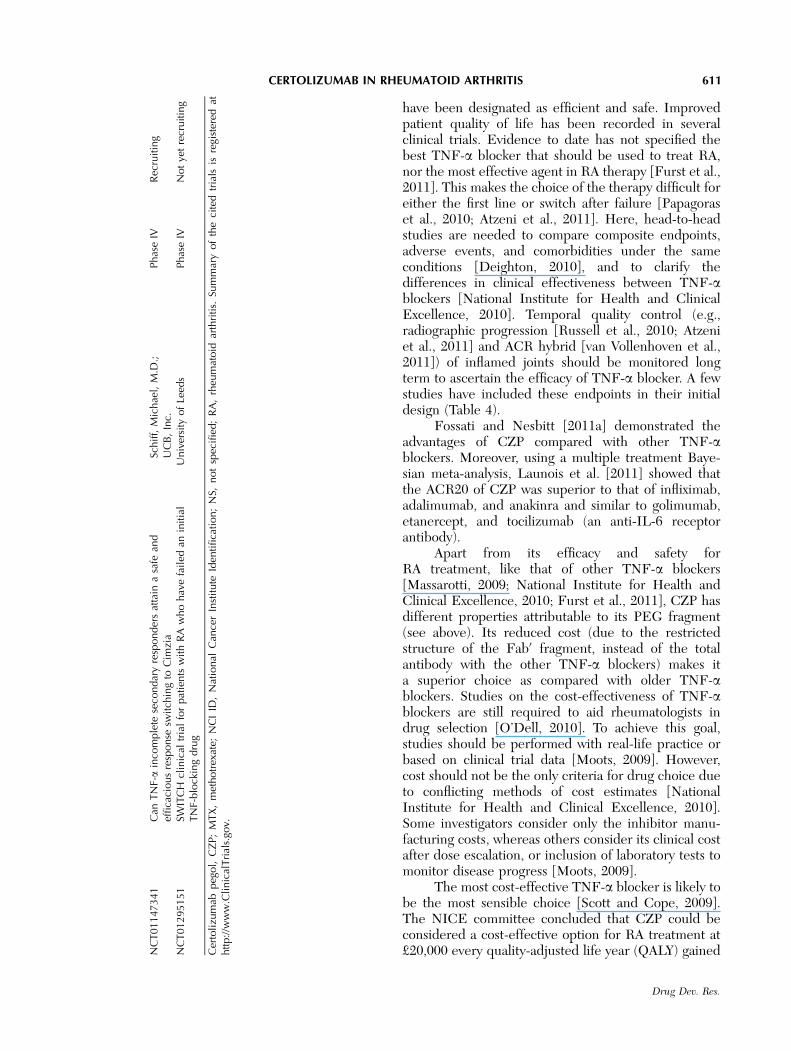
TA
BLE
4.
Cli
nic
alTri
als
Usi
ng
Cer
toli
zum
abPeg
ol
for
Rheu
mat
oid
Art
hri
tis
Ther
apy
Unti
lM
arch
2011
(Wit
hout
Com
ple
ted
Cli
nic
alTri
als)
NC
IID
Nam
eof
clin
ical
tria
lSp
onso
rSt
atus
Stag
e
NC
T01235598
Mag
net
icre
sonan
ceim
age
veri
fied
earl
yre
sponse
toC
ZP
insu
bje
cts
wit
hac
tive
RA
UC
B,
Inc.
Phas
eII
IR
ecru
itin
g
NC
T00175877
Study
ofth
esa
fety
and
effe
ctiv
enes
sofly
ophiliz
edC
ZP
inth
etr
eatm
ent
of
sign
san
dsy
mpto
ms
of
RA
and
inpre
venti
on
of
join
tdam
age
inpat
ients
wit
hac
tive
RA
UC
B,
Inc.
Phas
eII
IA
ctiv
e,not
recr
uitin
g
NC
T00160641
Study
ofth
esa
fety
ofli
quid
CZ
Pin
the
trea
tmen
tofsi
gns
and
sym
pto
ms
of
RA
and
inpre
venti
on
of
join
tdam
age
inpat
ients
wit
hac
tive
RA
UC
B,
Inc.
Phas
eII
IA
ctiv
e,not
recr
uitin
gN
CT00843778
Foll
ow
-up
of
RA
moder
ate
tolo
wdis
ease
activi
tyst
udy
UC
B,
Inc.
Phas
eII
IA
ctiv
e,not
recr
uitin
gN
CT01213017
Effe
ctof
CZ
Pon
MR
Isy
novi
tis
and
bone
edem
ain
RA
pat
ients
�Okl
ahom
aM
edic
alR
esea
rch
Foundat
ion;
�Art
hri
tis
and
Rheu
mat
icD
isea
seSp
ecia
ltie
s;
Phas
eII
IN
ot
yet
recr
uitin
g
�UC
B,
Inc.
NC
T01255761
Com
par
ison
of
two
asse
ssm
ent
tools
inpre
dic
ting
trea
tmen
tsu
cces
sof
cim
zia
inR
Asu
bje
cts
UC
B,
Inc.
Phas
eIV
Rec
ruitin
g
NC
T00753454
Open
-lab
elex
tensi
on
for
pat
ients
com
ing
from
the
dosi
ng
flex
ibilit
yst
udy
inpat
ients
wit
hR
AU
CB
,In
c.Phas
eII
IA
ctiv
e,not
recr
uitin
gN
CT00850343
Long-
term
trea
tmen
tst
udy
ofC
DP870
wit
houtco
adm
inis
trat
ion
ofM
TX
inJa
pan
ese
RA
pat
ients
�Ots
uka
Phar
mac
eutica
lC
o.,
Ltd.;
�UC
BJa
pan
Co.,
LTD
.Phas
eII
IR
ecru
itin
g
NC
T00993317
Study
ofC
DP870
asad
d-o
nm
edic
atio
nto
met
hotr
exat
ein
pat
ients
wit
hR
A�K
ore
aO
tsuka
Phar
mac
euti
cal
Co.,
Ltd.
Phas
eII
IR
ecru
itin
g
NC
T00851318
Long-
term
trea
tmen
tst
udy
of
CD
P870
asad
d-o
nm
edic
atio
nto
MTX
inJa
pan
ese
RA
pat
ients
�Ots
uka
Phar
mac
eutica
lC
o.,
Ltd.;
�UC
BJa
pan
Co.,
LTD
.Phas
eII
IR
ecru
itin
g
NC
T01095393
Nat
ional
Dat
aB
ank
for
rheu
mat
icdis
ease
regi
stry
study
of
safe
tyin
pat
ients
wit
hR
Atr
eate
dw
ith
Cim
zias
or
dis
ease
-modifyi
ng
anti
rheu
mat
icD
rugs
�UC
B,
Inc.
;�N
atio
nal
Dat
aB
ank
for
Rheu
mat
icD
isea
se(N
DB
)
NS
Enro
llin
gby
invi
tati
on
NC
T00717236
CZ
Pfo
rth
etr
eatm
ent
of
pat
ients
wit
hac
tive
RA
�UC
B,
Inc.
Phas
eII
IA
ctiv
e,not
recr
uitin
gN
CT01197066
Open
-lab
el,
exte
nsi
on
study
of
CD
P870
inpat
ients
wit
hR
A�K
ore
aO
tsuka
Phar
mac
euti
cal
Co.,
Ltd.
Phas
eII
IR
ecru
itin
g
NC
T01292265
12-w
eek
study
toas
sess
chan
ges
injo
int
inflam
mat
ion
usi
ng
ult
raso
nogr
aphy
inpat
ients
wit
hR
AU
CB
,In
c.Phas
eII
IR
ecru
itin
g
NC
T01098201
CZ
Pan
dlo
wer
-ext
rem
ity
lym
ph
flow
inR
AU
niv
ersi
tyof
Roch
este
rPhas
eIV
Act
ive,
not
recr
uitin
gN
CT00791999
Effica
cyco
nfirm
atio
ntr
ial
of
CD
P870
asad
d-o
nm
edic
atio
nto
MTX
inJa
pan
ese
RA
�Ots
uka
Phar
mac
eutica
lC
o.,
Ltd.;
�UC
BJa
pan
Co.,
LTD
.Phas
eII
,II
IA
ctiv
e,not
recr
uitin
gN
CT00791921
Effica
cyco
nfirm
atio
ntr
ial
of
CD
P870
wit
hout
coad
min
istr
atio
nof
MTX
inJa
pan
ese
RA
�Ots
uka
Phar
mac
eutica
lC
o.,
Ltd.;
�UC
BJa
pan
Co.,
LTD
.Phas
eII
IA
ctiv
e,not
recr
uitin
gN
CT01288287
Long-
term
effe
cts
of
anea
rly
resp
onse
toC
ZP
inR
Apat
ients
UC
B,
Inc.
NS
Not
yet
recr
uitin
gN
CT01069419
Obse
rvat
ion
of
trea
tmen
tw
ith
CZ
Pin
dai
lypra
ctic
eU
CB
,In
c.N
SEn
roll
ing
by
invi
tati
on
610 ZIDI ET AL.
Drug Dev. Res.
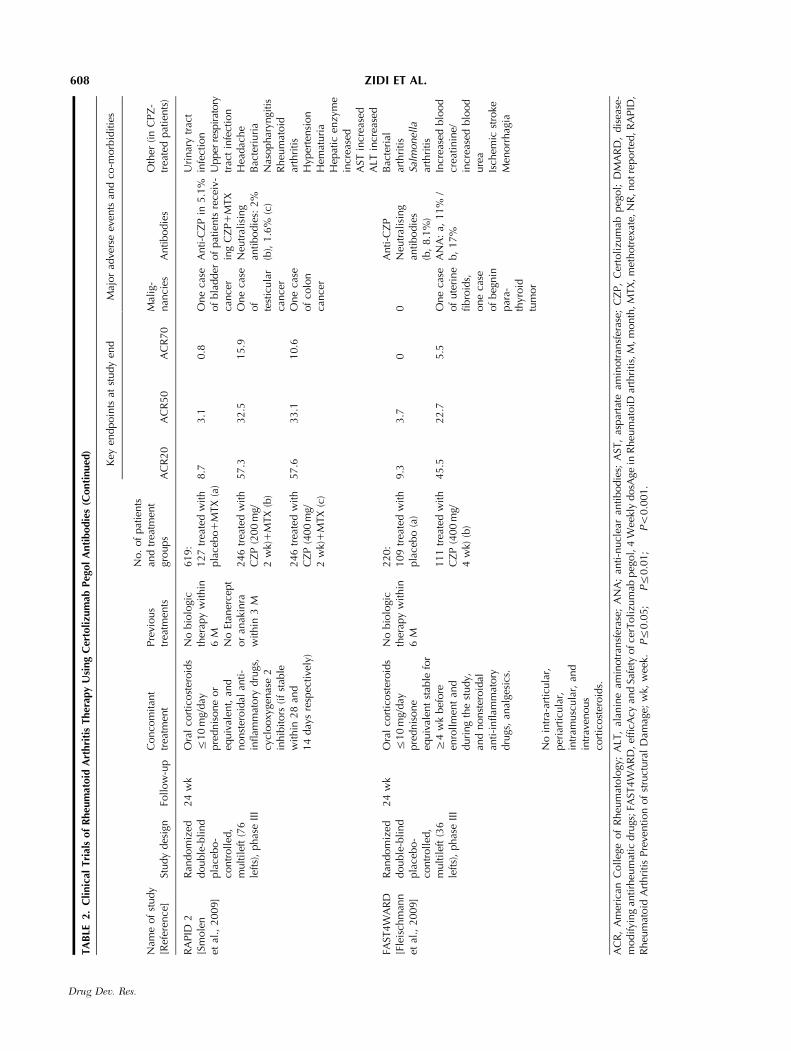
have been designated as efficient and safe. Improvedpatient quality of life has been recorded in severalclinical trials. Evidence to date has not specified thebest TNF-a blocker that should be used to treat RA,nor the most effective agent in RA therapy [Furst et al.,2011]. This makes the choice of the therapy difficult foreither the first line or switch after failure [Papagoraset al., 2010; Atzeni et al., 2011]. Here, head-to-headstudies are needed to compare composite endpoints,adverse events, and comorbidities under the sameconditions [Deighton, 2010], and to clarify thedifferences in clinical effectiveness between TNF-ablockers [National Institute for Health and ClinicalExcellence, 2010]. Temporal quality control (e.g.,radiographic progression [Russell et al., 2010; Atzeniet al., 2011] and ACR hybrid [van Vollenhoven et al.,2011]) of inflamed joints should be monitored longterm to ascertain the efficacy of TNF-a blocker. A fewstudies have included these endpoints in their initialdesign (Table 4).
Fossati and Nesbitt [2011a] demonstrated theadvantages of CZP compared with other TNF-ablockers. Moreover, using a multiple treatment Baye-sian meta-analysis, Launois et al. [2011] showed thatthe ACR20 of CZP was superior to that of infliximab,adalimumab, and anakinra and similar to golimumab,etanercept, and tocilizumab (an anti-IL-6 receptorantibody).
Apart from its efficacy and safety forRA treatment, like that of other TNF-a blockers[Massarotti, 2009; National Institute for Health andClinical Excellence, 2010; Furst et al., 2011], CZP hasdifferent properties attributable to its PEG fragment(see above). Its reduced cost (due to the restrictedstructure of the Fab0 fragment, instead of the totalantibody with the other TNF-a blockers) makes ita superior choice as compared with older TNF-ablockers. Studies on the cost-effectiveness of TNF-ablockers are still required to aid rheumatologists indrug selection [O’Dell, 2010]. To achieve this goal,studies should be performed with real-life practice orbased on clinical trial data [Moots, 2009]. However,cost should not be the only criteria for drug choice dueto conflicting methods of cost estimates [NationalInstitute for Health and Clinical Excellence, 2010].Some investigators consider only the inhibitor manu-facturing costs, whereas others consider its clinical costafter dose escalation, or inclusion of laboratory tests tomonitor disease progress [Moots, 2009].
The most cost-effective TNF-a blocker is likely tobe the most sensible choice [Scott and Cope, 2009].The NICE committee concluded that CZP could beconsidered a cost-effective option for RA treatment at£20,000 every quality-adjusted life year (QALY) gainedN
CT01147341
Can
TN
F-a
inco
mple
tese
condar
yre
sponder
sat
tain
asa
fean
def
fica
cious
resp
onse
swit
chin
gto
Cim
zia
�Sch
iff,
Mic
hae
l,M
.D.;
�UC
B,
Inc.
Phas
eIV
Rec
ruitin
g
NC
T01295151
SWIT
CH
clin
ical
tria
lfo
rpat
ients
wit
hR
Aw
ho
hav
efa
iled
anin
itia
lTN
F-blo
ckin
gdru
gU
niv
ersi
tyof
Leed
sPhas
eIV
Not
yet
recr
uitin
g
Cer
tolizu
mab
peg
ol,
CZ
P;
MTX
,m
ethotr
exat
e;N
CI
ID,
Nat
ional
Can
cer
Inst
itute
Iden
tifica
tion;
NS,
not
spec
ified
;R
A,
rheu
mat
oid
arth
riti
s.Su
mm
ary
of
the
cite
dtr
ials
isre
gist
ered
athttp:/
/ww
w.C
linic
alTri
als.
gov.
611CERTOLIZUMAB IN RHEUMATOID ARTHRITIS
Drug Dev. Res.
[National Institute for Health and Clinical Excellence,2010]. This committee reported that CZP plus MTXwas the least costly TNF-a with a more enhancedQALY when compared with adalimumab and inflix-imab. The opposite was observed for CZP comparedwith etanercept [National Institute for Health andClinical Excellence, 2010].
CZP has demonstrated a considerable indirectcost gain, as it has shown improved productivity andsocial activities in RA patients [Kavanaugh et al., 2009].These results were consolidated by Strand et al. [2009],who reported that the treatment of RA patients withCZP plus MTX was associated with significantimprovements in health-related quality of life (HRQoL)and in physical function at the first week, as well asreductions in fatigue, disease activity, and pain.
Because of its smaller structure CZP has reducedimmunogenicity. Indeed, some clinical trials havereported low anti-CZP antibodies (Table 2). Eventualimmunogenicity might be ascribed to other factors,including product-related factors, patient-relatedfactors, and treatment-related factors [Singh, 2011].
The rationale for the use of PEG fragment indrugs is well established. PEG is also a part ofpegsunercept, a soluble TNF receptor type I antibody[Furst et al., 2005]. Both CZP and pegsunercept havedemonstrated efficacy in RA [Furst et al., 2005;Bingham, 2008]. However, care must be taken withPEGylated drugs [Constantinou et al., 2010]. Anti-bodies against the PEG fragment moiety have beenfound after CZP treatment [Veronese and Pasut, 2008].Additionally, PEG fragments accumulate in rat kidney[Bendele et al., 1998; Singh, 2011]. Some reduction ofthe intended drug–target activity has also been noted[Pisal et al., 2010] and explained by an alteration in thebalance between the pharmacodynamic and pharma-cokinetic properties of CZP [Fishburn, 2008]. Con-cerns about the safety of PEG fragment-containingdrugs must be resolved with further studies.
Targeting TNF-a continues to be a major ther-apeutic opportunity in RA. Having demonstrated itsefficacy and safety as favorable properties deriving fromPEGylation, CZP is a new treatment option for RA.Recent advances and current clinical studies (Table 4)provide additional data on CZP for rheumatologists.
CONFLICT OF INTEREST
The authors declare having no conflict of interest.
REFERENCES
Alexis F, Pridgen E, Molnar LK, Farokhzad OC. 2008. Factorsaffecting the clearance and biodistribution of polymeric nano-particles. Mol Pharm 5:505–515.
Atzeni F, Sarzi-Puttini P, Gorla R, Marchesoni A, Caporali R. 2011.Switching rheumatoid arthritis treatments: an update. Autoim-mun Rev 10:397–403.
Barnes T, Moots R. 2007. Targeting nanomedicines in the treatmentof rheumatoid arthritis: focus on certolizumab pegol. IntJ Nanomed 2:3–7.
Bendele A, Seely J, Richey C, Sennello G, Shopp G. 1998. Renaltubular vacuolation in animals treated with polyethylene-glycol-conjugated proteins. Toxicol Sci 42:152–157.
Bingham CO. 2008. Emerging therapeutics for rheumatoid arthritis.Bull NYU Hosp Jt Dis 66:210–215.
Boissier MC, Assier E, Denys A. 2010. Les cibles therapeutiquesdes rhumatismes inflammatoires. In: Boissier MC, editor.Biotherapies en rhumatologie. Paris: Springer-Verlag. p 7–19.
Brennan FM, Chantry D, Jackson A, Maini R, Feldmann M. 1989.Inhibitory effect of TNF alpha antibodies on synovial cellinterleukin-1 production in rheumatoid arthritis. Lancet2:244–247.
Bugatti S, Codullo V, Caporali R, Montecucco C. 2007. B cells inrheumatoid arthritis. Autoimmun Rev 7:137–142.
Chames P, Van Regenmortel M, Weiss E, Baty D. 2009. Therapeuticantibodies: successes, limitations and hopes for the future. BrJ Pharmacol 157:220–233.
Choy EH, Hazleman B, Smith M, Moss K, Lisi L, Scott DG, Patel J,Sopwith M, Isenberg DA. 2002. Efficacy of a novel PEGylatedhumanized anti-TNF fragment (CDP870) in patients withrheumatoid arthritis: a phase II double-blinded, randomized,dose-escalating trial. Rheumatology (Oxf) 41:1133–1137.
Constantinou A, Chen C, Deonarain MP. 2010. Modulating thepharmacokinetics of therapeutic antibodies. Biotechnol Lett32:609–622.
Deighton C. 2010. If it works why can’t we have it? Sequential anti-TNF therapy in the UK. Rheumatology (Oxf) 49:2235–2236.
Ding T, Ledingham J, Luqmani R, Westlake S, Hyrich K, Lunt M,Kiely P, Bukhari M, Abernethy R, Bosworth A, et al., StandardsAaGWGoBCAC, BHPR. 2010. BSR and BHPR rheumatoidarthritis guidelines on safety of anti-TNF therapies. Rheumatology(Oxf) 49:2217–2219.
Ehlers MR, Leary ET. 2008. Biochemical markers of rheumatoidarthritis and osteoarthritis: clinical utility and practical considera-tions. In: Reid DM, Miller CG, editors. Clinical trials inrheumatoid arthritis and osteoarthritis. London, UK: Springer-Verlag. p 151–169.
Elbakri A, Nelson PN, Abu Odeh RO. 2010. The state of antibodytherapy. Hum Immunol 71:1243–1250.
Fishburn CS. 2008. The pharmacology of PEGylation: balancing PDwith PK to generate novel therapeutics. J Pharm Sci 97:4167–4183.
Fleischmann R, Vencovsky J, van Vollenhoven RF, Borenstein D,Box J, Coteur G, Goel N, Brezinschek HP, Innes A, Strand V.2009. Efficacy and safety of certolizumab pegol monotherapyevery 4 weeks in patients with rheumatoid arthritis failingprevious disease-modifying antirheumatic therapy: the FAST4-WARD study. Ann Rheum Dis 68:805–811.
Food and Drug Administration. 2009. FDA labeling information.FDA web site on line ohttp://www.accessdata.fda.gov/drugsatf-da_docs/label/2009/125160s092lbl.pdf4.
Fossati G, Nesbitt A. 2011a. Certolizumab Pegol has a differentprofile from other anti-TNFs, including Golimumab, in a varietyof in vitro assays. Ann Rheum Dis 70:A1–A94.
612 ZIDI ET AL.
Drug Dev. Res.
Fossati G, Nesbitt A. 2011b. Effect of the PEG component ofCertolizumab pegol on calcium flux in cellular systems. AnnRheum Dis 70:A1–A94.
Furst DE, Fleischmann R, Kopp E, Schiff M, Edwards CR,Solinger A, Macri M, Group S. 2005. A phase 2 dose-finding studyof PEGylated recombinant methionyl human soluble tumornecrosis factor type I in patients with rheumatoid arthritis.J Rheumatol 32:2303–2310.
Furst DE, Keystone EC, Braun J, Breedveld FC, Burmester GR,De Benedetti F, Dorner T, Emery P, Fleischmann R, Gibofsky A,et al. 2011. Updated consensus statement on biological agents forthe treatment of rheumatic diseases, 2010. Ann Rheum Dis70:i2–i36.
Harris J, Keane J. 2010. How tumour necrosis factor blockersinterfere with tuberculosis immunity. Clin Exp Immunol 161:1–9.
Kaushik VV, Moots RJ. 2005. CDP-870 (certolizumab) inrheumatoid arthritis. Expert Opin Biol Ther 5:601–606.
Kavanaugh A, Smolen JS, Emery P, Purcaru O, Keystone E,Richard L, Strand V, van Vollenhoven RF. 2009. Effect ofcertolizumab pegol with methotrexate on home and workplace productivity and social activities in patients with activerheumatoid arthritis. Arthritis Rheum 61:1592–1600.
Keystone E, Heijde D, Mason DJ, Landewe R, Vollenhoven RV,Combe B, Emery P, Strand V, Mease P, Desai C, Pavelka K. 2008.Certolizumab pegol plus methotrexate is significantly moreeffective than placebo plus methotrexate in active rheumatoidarthritis: findings of a fifty-two-week, phase III, multicenter,randomized, double-blind, placebo-controlled, parallel-groupstudy. Arthritis Rheum 58:3319–3329.
Keystone EC. 2009. Biologics: rapid control of symptoms inrheumatoid arthritis. In: Satellites: biologics and beyond: under-standing and meeting the needs of people with rheumatoidarthritis. London, UK: BMJ. p 2–4.
Klippel JH, Stone JH, Crofford LJ, White PH. 2010. Rheumatoidarthritis. In: Klippel JH, Stone JH, Crofford LJ, White PH,editors. The pocket primer on the rheumatic diseases. London,UK: Springer-Verlag. p 59–66.
Lacroix BD, Lovern MR, Stockis A, Sargentini-Maier ML,Karlsson MO, Friberg LE. 2009. A pharmacodynamic Markovmixed-effects model for determining the effect of exposure tocertolizumab pegol on the ACR20 score in patients withrheumatoid arthritis. Clin Pharmacol Ther 86:387–395.
Launois R, Avouac B, Berenbaum F, Blin O, Bru I, Fautrel B,Joubert JM, Sibilia J, Combe B. 2011. Comparison of certolizu-mab pegol with other anticytokine agents for treatment ofrheumatoid arthritis: a multiple-treatment Bayesian metaanalysis.J Rheumatol. 38:835–845.
Lee DM, Weinblatt ME. 2001. Rheumatoid arthritis. Lancet358:903–911.
Li SD, Huang L. 2008. Pharmacokinetics and biodistribution ofnanoparticles. Mol Pharm 5:496–504.
Lu Y, Harding SE, Turner A, Smith B, Athwal DS, Grossmann JG,Davis KG, Rowe AJ. 2008. Effect of PEGylation on thesolution conformation of antibody fragments. J Pharm Sci97:2062–2079.
Maciejewska Rodrigues H, Jungel A, Gay RE, Gay S. 2009. Innateimmunity, epigenetics and autoimmunity in rheumatoid arthritis.Mol Immunol 47:12–18.
Massarotti EM. 2009. FAST4WARD: implications for the clinician.Int J Clin Pract 63:986–988.
Monfardini C, Veronese FM. 1998. Stabilization of substances incirculation. Bioconjug Chem 9:418–450.
Moots RJ. 2009. Real life usage of biologics. In: Satellites: advancesin the management of rheumatoid arthritis. Proceedings of twoCPD-accredited satellite symposia supported by Wyeth atEULAR, 11 and 13 June 2008. London, UK: BMJ. p 22–25.
Nam JL, Winthrop KL, van Vollenhoven RF, Pavelka K, Valesini G,Hensor EM, Worthy G, Landewe R, Smolen JS, Emery P,Buch MH. 2010. Current evidence for the management ofrheumatoid arthritis with biological disease-modifying antirheu-matic drugs: a systematic literature review informing the EULARrecommendations for the management of RA. Ann Rheum Dis69:976–986.
National Institute for Health and Clinical Excellence. 2010. TA186Rheumatoid arthritis—certolizumab pegol: guidance. NICE website on line ohttp://www.nice.org.uk/nicemedia/live/12808/47544/47544.pdf4.
Nesbitt A, Fossati G, Brown D, Henry A, Palframan R, Stephens S.2008. Differences in the function and mode of action ofcertolizumab pegol and conventional anti-TNFs. Ann RheumDis 67:A49.
O’Dell JR. 2010. Pharmacotherapy: concepts of pathogenesis andemerging treatments. Challenges in clinical trial design ininflammatory arthritis. Best Pract Res Clin Rheumatol24:457–461.
Palframan R, Airey M, Moore A, Vugler A, Nesbitt A. 2009. Use ofbiofluorescence imaging to compare the distribution of certolizu-mab pegol, adalimumab, and infliximab in the inflamed paws ofmice with collagen-induced arthritis. J Immunol Methods348:36–41.
Papagoras C, Voulgari PV, Drosos AA. 2010. Strategies after thefailure of the first anti-tumor necrosis factor alpha agent inrheumatoid arthritis. Autoimmun Rev 9:574–582.
Pincus T, Sokka T. 2001. How can the risk of long-termconsequences of rheumatoid arthritis be reduced? Best PractRes Clin Rheumatol 15:139–170.
Pisal DS, Kosloski MP, Balu-Iyer SV. 2010. Delivery of therapeuticproteins. J Pharm Sci 99:2557–2575.
Rovensky J, Pavelka K, Bauerova K, Kucharska J. 2008. Rheumatoidarthritis. In: Gvozdjakova A, editor. Mitochondrial medicine:mitochondrial metabolism, diseases, diagnosis and therapy.Springer-Verlag. p 201–246.
Russell AS, Olszynski WP, Davison KS, Koehn C, Haraoui B. 2010.Leveling the field in the treatment of rheumatoid arthritis withbiologic therapies: equal access for equal efficacy. Clin Rheumatol29:233–239.
Scott DL, Cope A. 2009. New tumour necrosis factor inhibitors forrheumatoid arthritis: are there benefits from extending choice?Ann Rheum Dis 68:767–769.
Scott DL, Kingsley GH. 2007. Rheumatoid arthritis. In: Scott DL,Kingsley GH, editors. Inflammatory arthritis in clinical practice.London, UK: Springer-Verlag. p 1–31.
Scott DL, Wolfe F, Huizinga TW. 2010. Rheumatoid arthritis.Lancet 376:1094–1108.
Senolt L, Vencovsky J, Pavelka K, Ospelt C, Gay S. 2009.Prospective new biological therapies for rheumatoid arthritis.Autoimmun Rev 9:102–107.
Shealy DJ, Visvanathan S. 2008. Anti-TNF Antibodies: lessons fromthe past, roadmap for the future. In: Chernajovsky Y, Nissim A,
613CERTOLIZUMAB IN RHEUMATOID ARTHRITIS
Drug Dev. Res.

editors. Therapeutic antibodies. Handbook of experimentalpharmacology. Berlin: Springer-Verlag. p 101–130.
Singh SK. 2011. Impact of product-related factors on immunogeni-city of biotherapeutics. J Pharm Sci 100:354–387.
Smolen J, Landewe RB, Mease P, Brzezicki J, Mason D, Luijtens K,van Vollenhoven RF, Kavanaugh A, Schiff M, Burmester GR,et al. 2009. Efficacy and safety of certolizumab pegol plusmethotrexate in active rheumatoid arthritis: the RAPID 2 study. Arandomised controlled trial. Ann Rheum Dis 68:797–804.
Strand V, Mease P, Burmester GR, Nikaı E, Coteur G,van Vollenhoven R, Combe B, Keystone EC, Kavanaugh A.2009. Rapid and sustained improvements in health-related qualityof life, fatigue, and other patient-reported outcomes in rheuma-toid arthritis patients treated with certolizumab pegol plusmethotrexate over 1 year: results from the RAPID 1 randomizedcontrolled trial. Arthritis Res Ther 11:R170.
Taylor PC. 2010. Pharmacology of TNF blockade in rheumatoidarthritis and other chronic inflammatory diseases. Curr OpinPharmacol 10:308–315.
Tebib JG, Miossec P. 2006. Management of the patient withrheumatoid arthritis. In: Bouysset M, Tourne Y, Tillmann K,editors. Foot and ankle in rheumatoid arthritis. Paris:Springer-Verlag. p 97–109.
van Vollenhoven RF, Felson D, Strand V, Weinblatt ME, Luijtens K,Keystone E. 2011. American College of Rheumatology hybridanalysis of certolizumab pegol plus methotrexate in patients withactive rheumatoid arthritis: data from a 52-week phase III trial.Arthritis Care Res 63:128–134.
Veronese FM, Pasut G. 2008. PEGylation: posttranslationalbioengineering of protein biotherapeutics. Drug Discov TodayTechnol 5:e57–e64.
Vlieghe P, Lisowski V, Martinez J, Khrestchatisky M. 2010. Synthetictherapeutic peptides: science and market. Drug Discov Today15:40–56.
Wilke WS, Clough JD. 1991. Therapy for rheumatoid arthritis:combinations of disease-modifying drugs and new paradigms oftreatment. Semin Arthritis Rheum 21:21–34.
Wordsworth P, Holden W. 2005. Rheumatoid arthritis.In: eLS. John Wiley & Sons, Ltd: Chichester http://www.els.net/[doi:10.1038/npg.els.0006101].
Yen JH. 2006. Treatment of early rheumatoid arthritis in developingcountries. Biologics or disease-modifying anti-rheumatic drugs?Biomed Pharmacother 60:688–692.
Zidi I, Bouaziz A, Mnif W, Bartegi A, Al-Hizab FA, Amor NB. 2010.Golimumab therapy of rheumatoid arthritis: an overview. Scand JImmunol 72:75–85.
614 ZIDI ET AL.
Drug Dev. Res.