aplar rheumatoid arthritis treatment recommendations
TRANSCRIPT

SPECIAL EDITORIAL REVIEW
APLAR rheumatoid arthritis treatment recommendations
Chak Sing LAU,1 Faith CHIA,2 Andrew HARRISON,3 Tsu-Yi HSIEH,4 Rahul JAIN,5
Seung Min JUNG,6 Mitsumasa KISHIMOTO,7 Ashok KUMAR,8 Khai Pang LEONG,2
Zhanguo LI,9 Juan Javier LICHAUCO,10 Worawit LOUTHRENOO,11 Shue-Fen LUO,12 Peter
NASH,13 Chin Teck NG,14 Sung-Hwan PARK,6 Bagus Putu Putra SURYANA,15
Parawee SUWANNALAI,16 Linda Kurniaty WIJAYA,17 Kazuhiko YAMAMOTO,18 Yue YANG9
and Swan Sim YEAP19
1Division of Rheumatology and Clinical Immunology, Queen Mary Hospital, University of Hong Kong, Hong Kong, 2Department ofRheumatology, Allergy and Immunology, Tan Tock Seng Hospital, Singapore City, Singapore, 3Department of Medicine, University ofOtago Wellington, Wellington South, New Zealand, 4Section of Allergy, Immunology and Rheumatology, and Section of ClinicalSkills Training, Taichung Veterans General Hospital, Taichung, Taiwan, 5Narayana Hospital, Jaipur, India, 6Division ofRheumatology, Department of Internal Medicine, The Catholic University of Korea, St. Mary’s Hospital, Seoul, South Korea,7Immuno-Rheumatology Center, St Luke’s International Hospital, Tokyo, Japan, 8Department of Rheumatology, Fortis Flt. Lt RajanDhall Hospital, New Delhi, India, 9Department of Rheumatology, Peking University People’s Hospital, Beijing, China,10St. Luke’s Medical Center, Quezon City, Philippines, 11Division of Rheumatology, Department of Internal Medicine, Faculty ofMedicine, Chiang Mai University, Chiang Mai, Thailand, 12Department of Rheumatology, Allergy and Immunology, Chang GungMemorial Hospital and Chang Gung University, Tao-Yuan, Taiwan, 13Department of Medicine, University of Queensland, Brisbane,Queensland, Australia, 14Department of Rheumatology and Immunology, Singapore General Hospital, Singapore City, Singapore,15Rheumatology Division, Department of Internal Medicine, Brawijaya University, Saiful Anwar General Hospital, Malang,Indonesia, 16Allergy, Immunology and Rheumatology Division, Internal Medicine Department, Faculty of Medicine, RamathibodiHospital, Mahidol University, Bangkok, Thailand, 17Division of Rheumatology, Department of Internal Medicine, University ofIndonesia, Jakarta, Indonesia, 18Department of Allergy and Rheumatology, Graduate School of Medicine, The University of Tokyo,Tokyo, Japan, and 19Subang Jaya Medical Centre, Selangor, Malaysia
AbstractAims: Rheumatoid arthritis is a chronic inflammatory condition that affects approximately 1% of the world’s
population. There are a wide number of guidelines and recommendations available to support the treatment of
rheumatoid arthritis; however, the evidence used for these guidelines is predominantly based on studies in Cau-
casian subjects and may not be relevant for rheumatoid arthritis patients in the Asia-Pacific region. Therefore,
the Asia Pacific League of Associations for Rheumatology established a Steering Committee in 2013 to address
this issue.
Materials and methods: The AGREE II instrument and the ADAPTE Collaboration framework were applied to
systematically identify, appraise, synthesize, and adapt international rheumatoid arthritis guidelines for use in
the Asia-Pacific region.
Results: Forty rheumatoid arthritis treatment recommendations, based on evidence and expert opinion, were
drafted and are presented in this report.
Correspondence: Professor Chak Sing Lau, Division of Rheuma-tology and Clinical Immunology, Queen Mary Hospital,University of Hong Kong, Hong Kong, Hong Kong.Email: [email protected]
© 2015 Asia Pacific League of Associations for Rheumatology and Wiley Publishing Asia Pty Ltd
International Journal of Rheumatic Diseases 2015; 18: 685–713

Conclusion: The Asia Pacific of Associations for Rheumatology rheumatoid arthritis treatment recommenda-
tions are intended to serve as a reference for best practice management of rheumatoid arthritis in Asia-Pacific,
focusing on local issues to ensure the delivery of basic care for these patients, and to improve their outcomes. In
addition, the document will serve as a reference for national rheumatology associations in Asia-Pacific for devel-
oping guidelines in their respective countries.
Key words: drug treatment, rheumatoid arthritis.
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic inflammatory
autoimmune disease of unknown etiology that affects
approximately 1% of the global population.1–3 The dis-
ease is characterized by inflammation, pain, stiffness
and progressive joint destruction leading to high rates of
morbidity and mortality in the affected individuals.1–3
Furthermore, RA is associated with productivity losses
and increased financial burden, increased psychological
distress, depression and, consequently, significantly
decreased health-related quality of life.4–6
Disease-modifying antirheumatic drugs (DMARDs)
form the cornerstone of RA treatment. These agents
have the capacity to modify the disease process by
reducing or reversing signs and symptoms, disability,
impairment of quality of life, inability to work, and
progression of joint damage.7 Early and aggressive treat-
ment with DMARDs has been shown to be effective in
altering the clinical course of RA, and slowing or stop-
ping the radiographic progression. DMARDs are
broadly classified into conventional DMARDs
(cDMARDs) including synthetic chemical agents such
as methotrexate, sulfasalazine and leflunomide, and
biological DMARDs (bDMARDs), including: tumor
necrosis factor (TNF) inhibitors (adalimumab, cer-
tolizumab pegol, etanercept, golimumab and inflix-
imab); the T-cell costimulation inhibitor, abatacept; the
anti-B cell agent, rituximab; the interleukin (IL)-6 recep-
tor (IL-6R)-blocking monoclonal antibody, tocilizu-
mab; as well as the IL-1 inhibitor, anakinra. Recently,
tofacitinib, a Janus kinase (JAK) inhibitor, has also been
shown to have disease-modifying effects in RA.
NEED FOR RA RECOMMENDATIONS INTHE ASIA-PACIFIC (AP) REGION
As the evidence used in most international RA treatment
guidelines is obtained predominantly from studies in
Caucasian subjects, these guidelines may not be relevant
for RA patients in the AP countries. Data show that
there is an increased prevalence of certain infections
(e.g., tuberculosis [TB], hepatitis B and C infection,
Epstein–Barr virus infection)8,9 and malignancies (e.g.,
T-cell and natural killer-cell lymphomas,10 stomach
cancer11) in the AP region. Thus, a Steering Committee
under the auspice of the Asia Pacific League of Associa-
tions for Rheumatology (APLAR) was formed in 2013
to formulate AP region-specific treatment recommenda-
tions for RA that address AP-specific issues.
However, the AP region has vast intra-regional diver-
sity in terms of ethnicities, socioeconomic structures
and health resources; these characteristics also differ
from those in Western countries. Furthermore, the
availability and dosage of medications vary across AP
countries. Thus, it is difficult to develop RA treatment
recommendations that will be appropriate for all AP
countries. Owing to a shortage of rheumatologists, RA
patients in the region are also often managed by general
practitioners and allied health practitioners. Conse-
quently, the treatment practices are not standardized
and vary widely, even within countries. Furthermore,
there are limited data from the AP region to endorse
evidence-based recommendations that may be consid-
ered more appropriate in some countries in the region.
Nevertheless, this Steering Committee aimed to develop
recommendations that will be as evidence-based as pos-
sible and define the best practices for managing RA in
the AP region.
In addition, the Steering Committee also made rec-
ommendations based on expert opinion and consensus
so that countries with limited resources may be able to
achieve the minimum essential standard of care for
their RA patients.
TARGET AUDIENCE AND CONTENTS
The intended target audience for this document includes
rheumatologists and all practitioners who manage RA. It
focuses predominantly on recommendations for the
pharmacological treatment of RA. The document
includes 40 recommendations across the following RA
treatment domains: general RA treatment strategies; role
of non-steroidal anti-inflammatory drugs (NSAIDs),
including: cyclooxygenase-2 (COX-2) inhibitors; role of
corticosteroids; role of conventional DMARDs
686 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

(cDMARDS); and role of bDMARD agents. Specific key
questions across these key domains were identified and
recommendation statements developed accordingly
(Table 1).
This document does not include recommendations
for the diagnosis of RA, patient referral policies or
Table 1 Key questions regarding the treatment of RA in the
AP region
A. General RA treatment strategies
i. What are the goals of treatment?
ii. What are the clinical, laboratory and radiological fea-
tures and prognostic features that will guide treatment
decisions?
iii. Overall treatment strategies
1. How is treatment initiated and the goal of treatment
discussed with patients?
2. How are adjustments made based on clinical, bio-
chemical and radiological findings?
a. What are the response criteria and what should
be the frequency of monitoring?
b. What precautions are necessary for ensuring the
safety of patients on RA treatment?
3. How long should patients be maintained on
DMARD and non-DMARD treatments?
B. Role of NSAIDs including COX-2 inhibitors
i. What is the optimum dosage of NSAIDs and COX-2 inhi-
bitors?
ii. What are the side effects of NSAIDs and COX-2 inhibi-
tors?
iii. What are the associated gastrointestinal and cardiovas-
cular risks?
iv. What are the adverse events in patients with comorbidi-
ties?
v. Do NSAIDs have disease-modifying activity?
C. Role of cDMARDs
i. When are cDMARDS prescribed?
ii. Which cDMARDs should be used?
iii. What investigations are required before starting
cDMARD treatment?
iv. What is the optimal dosing for cDMARDs?
v. Which cDMARD combinations are preferred?
vi. What are the precautions when using cDMARDs?
vii. How to monitor patients on cDMARDs and what is the
frequency of assessment?
viii. How is treatment failure defined with cDMARDs?
ix. Is dose reduction or cessation possible with cDMARDs
when disease is deemed to be in remission?
D. Role of corticosteroid agents
i. What is the difference in opinions between AP and Euro-
pean/US practitioners about corticosteroid use?
ii. When should corticosteroids be prescribed?
iii. How should corticosteroids be administered?
iv. What is the optimal dosing regimen for corticosteroids?
v. When should treatment with corticosteroids be tapered
and stopped?
vi. What precautions are necessary when treating with cor-
ticosteroids?
vii. How should patients on corticosteroids be monitored?
E. Role of bDMARD agents
i. When should bDMARDs be prescribed?
1. What is the definition of inadequate response to
cDMARDs?
2. Which prognostic factors should be assessed when
prescribing bDMARDs?
ii. Which class of drugs should be used?
1. Need to discuss individual agents or class?
2. What is the algorithm for initiating and switching
treatment with bDMARDs?
iii. Should methotrexate or other cDMARDs be co-pre-
scribed with bDMARDs?
iv. Which investigations should be performed before pre-
scribing bDMARDs?
v. What is the optimal dosing strategy for different
bDMARDs?
vi. What is the therapeutic strategy for combination ther-
apy of bDMARDs with non-biologic DMARDs?
vii. What precautions should be taken when prescribing
bDMARDs?
viii. How should treatment with bDMARDs be monitored
and what should be the frequency of assessment?
ix. What are the definitions of primary and secondary treat-
ment failure with bDMARDs?
x. What is the therapeutic strategy for dose reduction or
cessation with bDMARDs when RA is deemed to be in
remission?
xi. What is the therapeutic strategy for bDMARDs in the
following special situations:
1. Infectious complications
a. TB
b. Hepatitis
c. Others
2. Autoimmunity
3. Malignancies
4. Surgery
5. Pregnancy/lactation
6. Vaccination policies
F. What is the role of complementary/unproven therapies in
the treatment of RA?
AP, Asia Pacific; bDMARD, biological DMARD; cDMARD, conven-tional DMARD; COX-2 inhibitors, cyclooxygenase-2 inhibitors;DMARD, disease-modifying antirheumatic drug; NSAID, non-steroidalanti-inflammatory drug; RA, rheumatoid arthritis; TB, tuberculosis.
Table 1 (continued)
International Journal of Rheumatic Diseases 2015; 18: 685–713 687
APLAR RA recommendations

management of comorbid conditions. Furthermore,
costs were not embedded in the discussion of the rec-
ommendations, as formal cost-effectiveness analyses
were not performed.
FUNDING AND CONFLICT OF INTEREST
The process of developing the APLAR RA treatment rec-
ommendations was funded by APLAR and was also
supported by unrestricted educational grants from the
following pharmaceutical companies: AbbVie, Janssen,
Pfizer, Roche and UCB. Relevant disclosures for the
Steering Committee members, including industry fund-
ing, consultancies and commercial interests, are
included at the end of this article.
OBJECTIVES
The primary objective was to develop a document that
would serve as a reference for best RA management
practices in the AP region, focusing on local issues in
the region. In addition, the document would also serve
as a reference for national rheumatology associations in
the region for developing RA guidelines in respective
countries.
MATERIALS AND METHODS
The ADAPTE framework was used to systematically
identify, appraise, synthesize, and adapt international
RA guidelines for use in the AP region. This was done
by following the steps outlined in the ADAPTE manual
and toolkit, and helped to expedite the process of rec-
ommendation development.12,13
Assembly of the APLAR RA RecommendationsSteering CommitteeA Steering Committee was formed by inviting 22 mem-
bers of APLAR representing 12 countries from the AP
region, as well as one RA patient for developing this set
of recommendations. The APLAR members were
rheumatology experts who had served on numerous RA
research projects and decision-making panels both
internationally and in their respective countries. All
members of the Steering Committee attended the meet-
ings, contributed to discussions and were actively
involved in every phase of recommendation develop-
ment. No representative of pharmaceutical companies
was involved in any part of recommendation
development.
Scope of the recommendationsMembers of the Steering Committee developed key
questions pertaining to RA treatment in the AP region.
These questions, developed during a face-to-face meet-
ing, addressed various domains of RA treatment, as
described earlier (Table 1).
Search criteriaThe studies included were clinical practice guidelines
and consensus statements with recommendations for
adult RA populations, and published in English
between January 2000 and December 2013. Studies
that provided evidence from the AP region to support
recommendation of RA treatment practices specific to
the region were also included. Non-English articles
were considered, provided a member of the Steering
Committee could translate them into English. Articles
were excluded if they did not address the key ques-
tions or were deemed to be of poor methodological
quality by a validated guidelines quality appraisal
instrument.14,15
Search strategyA systematic search was performed according to the
inclusion–exclusion criteria described above in Med-
line, EMBASE, Google Scholar and SCOPUS. The search
terms included RA, specific drug names for cDMARDs
and bDAMRDs, NSAIDs, corticosteroids, AP, guideli-
nes, consensus statements and recommendations. All
search results were reviewed by two independent mem-
bers. The steps involved in the systematic search are
shown in Figure 1.
Appraisal of guideline qualityThe quality of each guideline was assessed using a vali-
dated questionnaire, the Appraisal of Guidelines,
Research and Evaluation (AGREE) instrument.15 This
instrument includes 23 questions that are organized
into six domains: (i) scope and purpose; (ii) stake-
holder involvement; (iii) rigor of development; (iv)
clarity of presentation; (v) applicability; and (vi) edito-
rial independence. Each of the 23 items targets various
aspects of practice guideline quality. Each guideline was
independently assessed by two reviewers to formulate a
single-item overall assessment as ‘Recommend’, ‘Rec-
ommend with modifications’ or ‘Not recommend’.
Grading evidenceEach guideline had a different system for grading evi-
dence. To reconcile these differences, we translated each
688 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

guideline’s evidence grading system into a simplified
system as suggested by the Scottish Intercollegiate
Guideline Network (SIGN) to assign a level of evidence
and strength of recommendation for each recommen-
dation.16
Evidence synthesisWe prepared a table of included guidelines containing
descriptive characteristics, including guideline devel-
oper, country, year, summary of recommendations and
AGREE assessment, for each subsection of the guideline.
This was followed by development of evidence tables
for each question; these included guideline characteris-
tics, recommendations, summary of guideline assess-
ment (AGREE assessment) and supporting evidence
(Table 2).
Development of recommendationsMembers of the Steering Committee summarized rec-
ommendations and supporting evidence from inter-
national guidelines to address each key question. A
recommendation for the AP region was developed
by adapting and rewording the existing recommen-
dation. An emphasis was placed on recent guidelines
with strong methodological quality. Supporting evi-
dence from randomized controlled trials (RCTs) and
observational studies referenced by the guideline was
reviewed by members in detail. All members partici-
pated in developing the wording of recommenda-
tions. Consensus was achieved by using the Delphi
technique whereby members had an opportunity to
cast a vote anonymously, without getting swayed by
opinions of fellow members; disagreements were
resolved through discussions and multiple rounds of
voting. Statements were included as recommenda-
tions provided more than 80% of the members par-
ticipated in the polling and more than 50% of the
members voted in favor of the outcome. Setting the
acceptance margin to 70% resulted in exclusion of
many questions considered important during meet-
ing discussions. Thus, for the purpose of this recom-
mendation document, a majority was determined by
more than 50% of votes.
Extended reviewDraft recommendations developed by the group were
sent to Josef Smolen and Vibeke Strand for review and
comments. The draft recommendations were also pre-
sented in an open forum during the 2014 APLAR Con-
gress to seek opinions and suggestions from
participants. Feedback from the respondents was used
to finalize the recommendations and inform supporting
text. This document was developed in accordance with
the principles outlined by the AGREE II instrument and
the ADAPTE collaboration. The recommendations were
also sent for review and official endorsement by APLAR.
Figure 1 Steps in the systematic review of international guidelines and recommendations on the pharmacological managementof rheumatoid arthritis.
International Journal of Rheumatic Diseases 2015; 18: 685–713 689
APLAR RA recommendations

RESULTS
Each recommendation is presented with a level of evi-
dence and strength (Table 3) and accompanied with
supporting text which is structured as follows.
Supporting evidence
Description of the source guidelines used for adapta-
tion
Summary of evidence linked to recommendation statement
Summary of original evidence presented in source
guidelines.
Special comment/recommendation for the AP region
A special comment/expert opinion that is relevant for
the region.
RecommendationsA summary of the recommendations is presented in
Table 3. It should be noted that the recommendations
are stratified into different sections relevant to the dif-
ferent stages and groups of drugs used in the treatment
of RA. These sections may thus be referenced separately
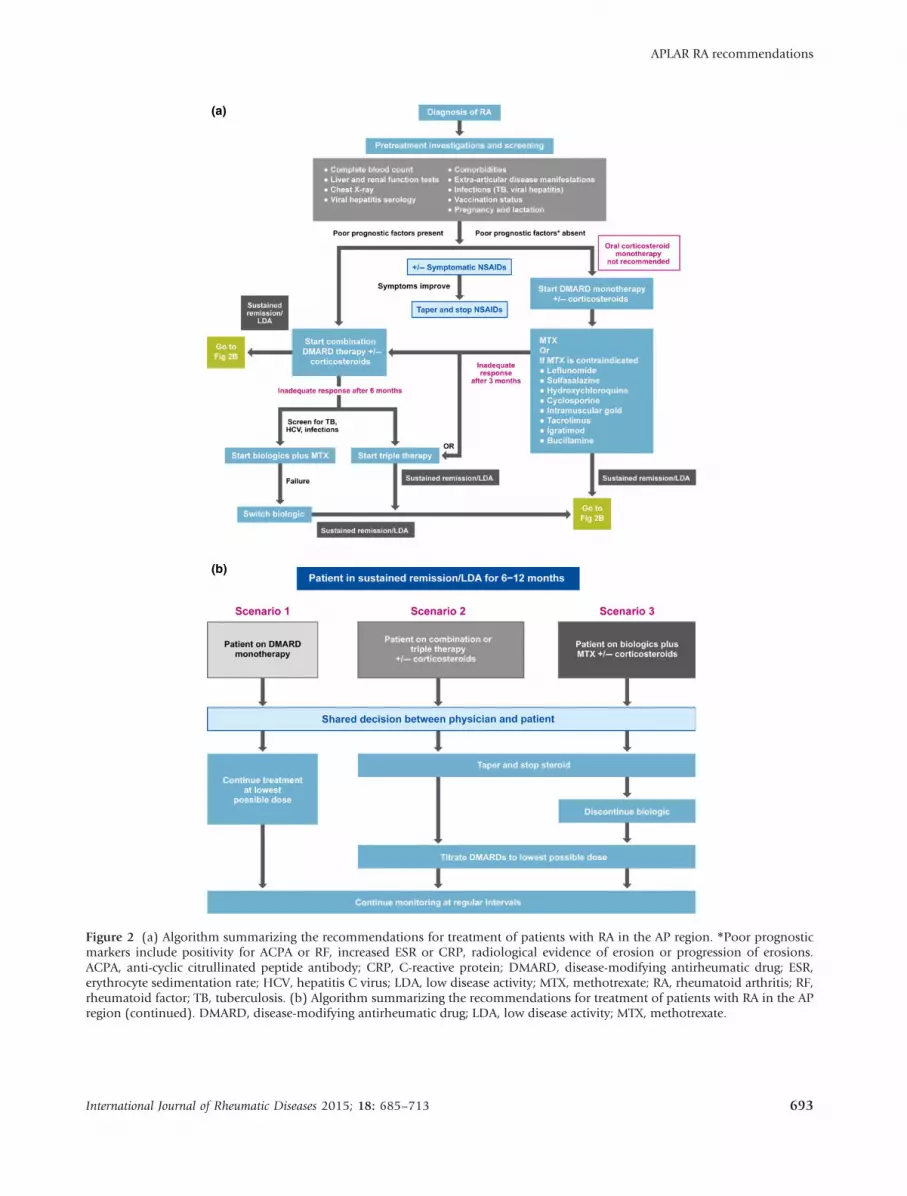
and individually. An algorithm summarizing the rec-
ommendations for treatment of patients with RA in the
AP region is presented in Figure 2.
Section 1 – General RA treatment strategies
Recommendation 1. RA treatment should be aimed atmaintaining physical functioning and good qualityof life through achieving a state of sustained remis-sion, or low disease activity when remission may notbe an achievable target. (Level II; Strength B)
Supporting evidence
References 17–29.
Summary of evidence linked to recommendation statement
It was noted that, in every patient, treatment should be
aimed at reaching a target of remission17–24 or low dis-
ease activity,17–20,24 as soon as possible25 and measur-
ing disease activity using objective parameters such as
Disease Activity Score (DAS), DAS28 (DAS of 28 joints),
Simplified Disease Activity Index (SDAI) and Clinical
Disease Activity Index (CDAI).26,27 Consequently, this
will halt joint damage, prevent disability and improve
quality of life.28,29 It should be noted that DAS28 < 2.6
is regarded by the Food and Drug Administration
(FDA) as a cut-off point for low disease activity,
whereas remission is probably better defined according
to the American College of Rheumatology–EuropeanLeague Against Rheumatism (ACR–EULAR) criteria
based on SDAI, CDAI or the Boolean criteria.30
Special comment/recommendation for the AP region
In the AP region, there may be some situations in which
remission or even low disease activity may not be possi-
ble. For example, many AP patients first present to their
clinician with advanced disease and often severe joint
deformity. For these patients to achieve remission, the
use of bDMARDs is often required but these agents are
not affordable for most of these patients. Furthermore,
many patients are engaged in work involving physical
labor which may aggravate the signs and symptoms of
RA, rendering a low disease activity state non-achiev-
able. Thus, for many RA patients in the region, we rec-
ommend counselling to ensure compliance, and an
agreement on a treatment target, maintaining symptom
control and work ability, to be reached between the
clinician and the patient.
Recommendation 2. Treatment of RA is a shared deci-sion between the clinician and patient, and should bestarted once diagnosed. (Level I; Strength A)
Supporting evidence
References 17, 19–25, 27, 29, 31, 32 and 33.
Table 2 System used for assigning level of evidence and
strength of recommendation16
Levels of evidence Strength of recommendation
I. Meta-analyses, systematic
reviews of RCTs, or
individual RCT
A. Strong recommendation:
Direct level I evidence
II. Meta-analyses, systematic
reviews of observational
studies (cohort/case
control studies), or
individual observational
studies
OR
RCT subgroup/post-hoc
analyses
B. Moderate
recommendation:
Direct level II evidence or
extrapolated level I
evidence
III. Non-analytical studies, e.g.,
case reports, case series
C. Weak recommendation:
Direct level III evidence
or extrapolated level II
evidence
IV. Expert opinion
OR
Recommendations are not
linked to evidence
D. Consensus
recommendation:
Expert opinion based on
very limited evidence
RCT, randomized controlled trial.
690 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

Table 3 APLAR treatment recommendations for the management of RA in the AP region
Recommendations Level Strength
Section 1 – General RA treatment strategies
1. RA treatment should be aimed at maintaining physical functioning and good quality of life through
achieving a state of sustained remission, or low disease activity when remission may not be an
achievable target.
II B
2. Treatment of RA is a shared decision between the clinician and patient, and should be started once
diagnosed.
I A
3. The choice of treatment is based on the findings of active disease and/or poor prognosis and
comorbidities.
II B
4. Poor prognostic factors include positivity for ACPA or RF, increased ESR or CRP, radiological evidence of
erosion or progression of erosions.
II B
5. All patients with recently diagnosed RA or active disease should be monitored for disease activity every 1
to 3 months.
I A
6. A suitable and practical standardized measure of disease activity should be routinely performed to assess
patients’ response to treatment.
I A
7. Safety monitoring while patients are on bDMARD therapy is likewise recommended. II B
8. All patients should be assessed clinically at presentation for extra-articular disease manifestations,
comorbidities, and infections such as TB and hepatitis (II). Information on vaccination status and
special situations such as pregnancy and lactation should be obtained (II).
II B
9. If patients show persistent remission for 6 months, treatment with corticosteroids and NSAIDs may be
tapered, with the aim of eventually stopping these treatments.
II B
10. If a patient is in sustained remission for more than 6 to 12 months after discontinuation of NSAIDs,
corticosteroids and bDMARDs, then a gradual reduction in cDMARDs can be attempted with caution, as
a shared decision between the patient and physician.
IV D
Section 2 – Role of NSAIDs (including COX-2 inhibitors)
11. NSAIDs and COX-2 inhibitors should be used at the lowest effective dose for the shortest possible period
of time.
IV D
Section 3 – Role of corticosteroids
12. Oral corticosteroid monotherapy is not recommended. IV D
13. Oral corticosteroids can be considered to control active RA in combination with cDMARDs. I A
14. In early RA, the addition of low-dose corticosteroids (prednisolone ≤ 7.5 mg/day) to cDMARDs leads to
a reduction in radiographic progression.
I A
15. Corticosteroids should be used in the lowest possible dose and tapered as rapidly as clinically feasible. IV D
Section 4 – Role of conventional DMARDs
16. Treatment with cDMARDs as monotherapy or in combination should be started as soon as the diagnosis
of RA is made.
I A
17. Methotrexate is the first-line cDMARD for RA patients, and is considered as the “anchor drug”. I A
18. Patients who cannot tolerate methotrexate may receive other cDMARDs such as leflunomide,
sulfasalazine and hydroxychloroquine as first-line treatments.
I A
Bucillamine, iguratimod, cyclosporin, azathioprine, IM gold or tacrolimus may also be considered in
some AP countries.
I B
19. Pretreatment investigations: complete blood count, liver function and renal function tests, viral hepatitis
serology and chest radiograph should be ordered prior to initiating methotrexate therapy.
II B
20. Combination cDMARD therapy should be considered in active RA patients, particularly those with poor
prognostic factors.
I B
21. Combination cDMARD therapy should include methotrexate as the anchor drug unless methotrexate is
contraindicated.
II B
22. Triple therapy with cDMARDs is an effective option in patients who show inadequate response to
methotrexate monotherapy.
II B
23. Patients should be assessed every 1 to 3 months after the initial treatment or change of regimen until
the disease is stabilized, in remission or in low disease activity state.
I A
24. Patients who have been stabilized or are in remission or low disease activity can be monitored every 3 to
6 months.
IV D
International Journal of Rheumatic Diseases 2015; 18: 685–713 691
APLAR RA recommendations

Summary of evidence linked to recommendation statement
Successful management of patients with RA depends
upon empowering the patients with the knowledge
about the chronic and fluctuating course of the disease,
treatment goal31 and, particularly, about the possible
evolution and prognosis,24 including side effects, costs
of the drugs and the continuous need of physiother-
apy.22 Offering verbal and written information to
Table 3 (continued)
Recommendations Level Strength
25. Definition of treatment failure: Inadequate response with cDMARDs is defined as failure to achieve
remission or low disease activity after a therapeutic trial of at least two standard cDMARDs in
combination at optimal doses for 6 months (I). One of the failed cDMARDs must be methotrexate
unless methotrexate is contraindicated (I).
I A
Section 5 – Role of bDMARDs
26. A bDMARD can be prescribed in patients who have inadequate response or intolerance to cDMARDs. I A
27. Early bDMARD use can be considered in patients who have active disease with poor prognostic factors. IV D
28. Prior to starting treatment with bDMARDs, history regarding active or current infections, comorbidities
including tumors and malignancies, vaccinations, pregnancy, and possible contraindications should be
obtained in all patients.
I A
29. All patients should be screened for TB, and HBV and HCV infections before initiating bDMARD therapy. I A
30. Live vaccines should be given at least 4 weeks prior to bDMARD administration. III–IV C–D31. Monotherapy or combination with methotrexate/cDMARDs: bDMARDs are most effective when
combined with methotrexate.
I A
32. In patients with RA who are candidates for bDMARD therapy, the therapeutic options include TNF
antagonists, abatacept, rituximab and tocilizumab.
I A
33. Patients who fail to achieve remission or low disease activity after 6 months of bDMARD therapy are
recommended to switch to another bDMARD agent.
III C
34. Dose reduction
In patients who have achieved remission, a reduction in treatment should be considered. I A
If the patient remains in extended remission (> 12 months), tapering of bDMARDs can be considered. II B
35. Infectious complications: TB
Screening for TB is recommended prior to starting bDMARD therapy. II B
All patients with latent TB infection should receive prophylactic anti-TB therapy. II B
Patients with active TB infection need to be adequately treated before consideration of bDMARD
treatment.
III C
36. Infectious complications: hepatitis
Patients should be screened for HBV and HCV infections prior to the commencement of bDMARDs. IV D
bDMARDs should be avoided in patients with active or untreated chronic HBV infection and active
HCV infection.
III C
37. Active infections
Active infections are contraindications for bDMARDs. I A
When an infection is suspected, based on clinical judgement, the bDMARD agent should be stopped
and the patient must be treated appropriately.
IV D
38. Pregnancy and lactation while on bDMARDs should only be considered after thorough assessment of
benefits and risks.
IV D
39. Vaccination
Administration of all vaccines, if indicated, should, ideally, be undertaken at least 4 weeks before
starting a bDMARD.
III–IV C–D
Concurrent administration of live, attenuated vaccines is an absolute contraindication for patients
being treated with bDMARDs.
IV D
Section 6 – Role of tofacitinib
40. Tofacitinib may be considered if a bDMARD has failed II B
ACPA, anti-citrullinated peptide antibodies; AP, Asia-Pacific; bDMARD, biological DMARD; COX-2 inhibitors, cyclooxygenase-2 inhibitors;cDMARD, conventional DMARD; CRP, C-reactive protein; DMARD, disease-modifying antirheumatic drug; ESR, erythrocyte sedimentation rate;HBV, hepatitis B virus; HCV, hepatitis C virus; IM, intramuscular; NSAID, non-steroidal anti-inflammatory drug; RA, rheumatoid arthritis; RF,rheumatoid factor; TB, tuberculosis; TNF, tumor necrosis factor.
692 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.
(a)
(b)
Figure 2 (a) Algorithm summarizing the recommendations for treatment of patients with RA in the AP region. *Poor prognosticmarkers include positivity for ACPA or RF, increased ESR or CRP, radiological evidence of erosion or progression of erosions.ACPA, anti-cyclic citrullinated peptide antibody; CRP, C-reactive protein; DMARD, disease-modifying antirheumatic drug; ESR,erythrocyte sedimentation rate; HCV, hepatitis C virus; LDA, low disease activity; MTX, methotrexate; RA, rheumatoid arthritis; RF,rheumatoid factor; TB, tuberculosis. (b) Algorithm summarizing the recommendations for treatment of patients with RA in the APregion (continued). DMARD, disease-modifying antirheumatic drug; LDA, low disease activity; MTX, methotrexate.
International Journal of Rheumatic Diseases 2015; 18: 685–713 693
APLAR RA recommendations

people with RA will improve their understanding of the
condition and its management, and counter any mis-
conceptions they may have.32
Early treatment could improve the outcome of RA.23,29
Treatment with traditional DMARDs with or without low
dose glucorticoids should be considered as soon as the
diagnosis of RA is made17,24,25,32 to increase clinical
response and decrease radiographic progression.
Special comment/recommendation for the AP region
Early treatment of RA in this region may not be possible
in some countries with poor economic status due to an
inefficient referral system and a shortage of rheumatolo-
gists. The Steering Committee would, therefore, like to
reinforce that this recommendation is aimed not only
for rheumatologists but any clinicians who participate
in the care of patients with RA. For many countries in
the AP region, improving the knowledge of general clin-
icians of RA and its treatment is of utmost importance.
Recommendation 3. The choice of treatment is basedon the findings of active disease and/or poor progno-sis and comorbidities. (Level II; Strength B)
Supporting evidence
References 17, 18, 21–24 and 27–29.
Summary of evidence linked to recommendation statement
The presence of poor prognostic features should be
assessed at baseline and considered when making treat-
ment decisions. These include high disease activity
state, (high number of swollen and tender joints, ele-
vated erythrocyte sedimentation rate [ESR] or C-reactive
protein [CRP]), rheumatoid factor (RF) positivity, anti-
cyclic citrullinated peptide antibody (ACPA) positivity,
and early presence of joint damage,17,18,21–24,28,29 extra-
articular features (e.g., presence of rheumatoid nodules,
vasculitis, Felty’s syndrome) and functional limitation
as measured by the Health Assessment Questionnaire
Disability Index (HAQ-DI).18,23,28
Special comment/recommendation for the AP region
Most RA patients in the AP region present late with it
and many would have developed erosive disease. Bas-
ing radiological erosions solely as an indication for
aggressive treatment may lead to over-treatment for
some patients. Therefore, other markers of high dis-
ease activity and poor prognosis may be more appro-
priate indications for intensive DMARD treatment.
Recommendation 4. Poor prognostic factors includepositivity for ACPA or RF, increased ESR or CRP, radi-ological evidence of erosion or progression of ero-sions. (Level II; Strength B)
Supporting evidence
References 17, 18, 21–24, 28, 29 and 34.
Summary of evidence linked to recommendation statement
Refer to Recommendation 3 above.
Special comment/recommendation for the AP region
In addition to comments made under Recommenda-
tion 3 above, clinicians should be aware of the wide-
spread misuse of corticosteroid agents, many of which
may be purchased over the counter or from a quack in
the AP region, which may mask some of these poor
prognostic factors.
Recommendation 5. All patients with recently diag-nosed RA or active disease should be monitoredfor disease activity every 1 to 3 months. (Level I;Strength A)
Supporting evidence
References 18–20, 22, 24, 28, 32–37.
Summary of evidence linked to recommendation statement
At the beginning of RA treatment, especially in patients
with high/moderate disease activity, the patient should
preferably be assessed every month.19,20,24 The fre-
quency of monitoring in patients with active RA should
be 1 to 3 months,22,28,32–37 aiming to achieve remis-
sion by 6 months33 when the interval for monitoring
may be between 3 to 6 months, depending on the
degree of disease activity.18
Special comment/recommendation for the AP region
Lack of resources in many countries in the AP region is
a major obstacle for frequent monitoring of RA disease
activity and treatment. Rheumatologists may need the
assistance of general clinicians and allied health work-
ers in the monitoring process, as well as a patient self-
reporting system. The development of a good allied
health worker and patient education program is of
utmost importance in the overall management of
patients with RA in this region.
Recommendation 6. A suitable and practical standard-ized measure of disease activity should be routinely
694 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

performed to assess patients response to treatment.(Level I; Strength A)
Supporting evidence
References 17–19, 21–24, 26–28, 32, 34–36 and 38–42.
Summary of evidence linked to recommendation statement
Most guidelines recommend the use of a validated com-
posite score such as DAS28, SDAI and CDAI for mea-
suring disease activity before starting treatment, and for
monitoring disease activity and drug response after
starting treatment.17,18,21–24,26–28,32,35,36,38–42 In addi-
tion, some guidelines recommend using the Health
Assessment Questionnaire (HAQ) for evaluating the
functional impact of the disease.21,32,36,41 The French
guidelines also recommend anteroposterior X-rays of
the hands, wrist and forefeet to monitor the course of
RA; this may be done every 6 months until the end of
the first year, then once every year until end of the third
year, and thereafter every 2 to 4 years.42
Special comment/recommendation for the AP region
Regular measurement of serum CRP may not be afford-
able in many AP countries. Rheumatologists from these
countries are recommended to use ESR instead; other-
wise, clinical activity measurement without ESR, for
example, CDAI, should be used in patient monitoring.
Recommendation 7. All patients should be assessedclinically at presentation for extra-articular diseasemanifestations, comorbidities and infections, such asTB and hepatitis (Level II; Strength B). Informationon vaccination status and special situations such aspregnancy and lactation should be obtained (Level II;Strength B)
Supporting evidence
References 18, 22–24, 29, 31, 33–35, 37, 38 and 43–59.
Summary of evidence linked to recommendation statement
Given that RA is a systemic disease accompanied with
not only joint dysfunction but also other comorbidities
(such as cardiovascular disease and osteoporosis), extra-
articular manifestations (such as pericarditis, pleuritis
and vasculitis), and an increased risk of infections,32 it is
recommended to evaluate and screen patients for these
conditions before initiating treatment with DMARDs,
NSAIDs or corticosteroids.18,22–24,29,31,33–35,37,38,43–59
As most drugs used in the treatment of RA are con-
traindicated during pregnancy and breastfeeding, it is
recommended to rule out these situations before initiat-
ing treatment.24,31,33–35,37,38,48,52–54,58 Before starting
cDMARDs or bDMARDs, patients’ vaccination status
should be assessed and updated, and all killed, recom-
binant and live attenuated vaccinations under-
taken.18,24,31,33,37,38,46,53,54,56
Special comment/recommendation for the AP region
No region-specific comments.
Recommendation 8. Safety monitoring while patientsare on bDMARD therapy is likewise recommended.(Level II; Strength B)
Supporting evidence
References 18, 22, 23, 32, 34, 35, 37, 43–47 and 60.
Summary of evidence linked to recommendation statement
Treatment with bDMARDs, particularly TNF inhibitors,
is associated with an increased risk of certain infections,
including TB, as well as that of non-Hodgkin’s lym-
phoma and congestive heart failure.43,44 Thus, many
guidelines recommend screening for active and latent
TB before starting bDMARDs,18,22,23,34–37,43–47 and per-
forming baseline hepatitis serology as well as other
investigations, including a complete blood picture, liver
function tests, serum urea and creatinine levels and
antinuclear antibody status, and to rule out presence of
active and latent infections and other comorbidities.
Furthermore, continuous monitoring for these condi-
tions and side effects is also emphasized during
bDMARD therapy.18,22,23,32,34,35,37,43–47,60
Special comment/recommendation for the AP region
It is especially important to monitor for the emergence
of infective complications. Clinicians should be on the
alert for not only TB and hepatitis infections but all
other opportunistic infections, including fungal and
parasitic infections.
Recommendation 9. Once the patient has improvedsymptomatically, treatment with corticosteroids andNSAIDs may be tapered, with the aim of eventuallystopping these treatments. (Level II; Strength B)
Supporting evidence
References 17, 21, 22, 24–26, 28, 29, 32, 55, 57, 61 and
62.
Summary of evidence linked to recommendation statement
While NSAIDs in combination with DMARDs are
effective in controlling pain and inflammation in RA,
International Journal of Rheumatic Diseases 2015; 18: 685–713 695
APLAR RA recommendations

long-term use is not recommended as these drugs are
associated with significant gastrointestinal, cardiovascu-
lar and renal adverse effects.21,22,24,55,57,61 Furthermore,
these agents have not demonstrated any efficacy in
modifying the disease course.57 Corticosteroids, in
combination with DMARDs, are effective in limiting
disease progression, and are particularly effective in
decreasing inflammation in patients with flares and
improving symptom control in those with early dis-
ease.59 However, given the toxicity with long-term use,
it is recommended to taper therapy as symptoms
improve and discontinue completely once patients
achieve remission.17,21,22,24–26,28,29,32,55,57,61,62
Special comment/recommendation for the AP region
Clinicians should be aware of over-the-counter and
quack-provided corticosteroid preparations, and their
use must be discouraged.
Recommendation 10. If a patient is in sustained remis-sion for more than 6 to 12 months after discontinua-tion of NSAIDs, corticosteroids and bDMARDs, thena gradual reduction in cDMARDs can be attemptedwith caution, as a shared decision between thepatient and physician. (Level IV; Strength D)
Supporting evidence
References 17, 21, 22, 25, 26, 28, 32 and 55.
Summary of evidence linked to recommendation statement
Duration of remission is required for more than
1 year in the Indian 2008 guidelines,22 6–12 months
in the 2013 Brazilian guidelines26 and over
6 months in the German 2013 guidelines.25 The
suggested sequence of drug withdrawal is NSAID,
corticosteroid, bDMARD and then cDMARD.26,28 The
reduction in treatment should be performed cau-
tiously, gradually and in a stepwise manner. A
shared decision must be reached between the patient
and physician in this regard.17,25,28 According to the
BeST study, sustained remission was defined as
DAS < 1.6 for more than 6 months. According to
the Indian guidelines, a minimum maintenance dose
will be required for an indefinite period.22 The Bri-
tish Society for Rheumatology and British Health
Professionals in Rheumatology (BSR-BHPR) guideli-
nes warn about the frequent association of with-
drawal with flare and disease progression.55 The
2013 Brazilian guidelines describe withdrawal of
cDMARD in exceptional situations.26
Special comment/recommendation for the AP region
Because of the poor affordability of bDMARDs for
most patients in this region, patients may rely more
on cDMARDs for disease control. Thus, we recom-
mend primarily cautious dose reduction but not
complete cessation of cDMARDs for the majority of
patients.
Section 2 – Role of NSAIDs (including cyclo-oxygenase-2
inhibitors)
Recommendation 11. NSAIDs and COX-2 inhibitorsshould be used at the lowest effective dose forthe shortest possible period of time. (Level IV;Strength D)
Supporting evidence
References 29, 32 and 55.
Summary of evidence linked to recommendation
The National Institute for Health and Care Excellence
(NICE) 2009 guidelines reviewed data from several
studies to show that NSAIDs and COX-2 inhibitors
were effective in treating the symptoms of RA and
recommended that oral NSAIDs/COX-2 inhibitors be
used in the lowest effective dose over the shortest
period of time; it is advisable to use NSAIDs as
needed.32 However, no optimum dose was proposed.
The BSR 2006 and 2009 guidelines emphasized that
long-term use of NSAIDs should be at the lowest
effective dose and are best avoided because of the
associated risks.29,55
NSAIDS and COX-2 inhibitors, undoubtedly, are effi-
cacious in controlling RA symptoms, but their gastroin-
testinal, cardiovascular and renal adverse effects are a
matter of serious concern. A balanced approach should
be undertaken whereby the benefits are weighed against
the possible adverse effects.
Special comment/recommendation for the AP region
In the AP region, there is a general lack of awareness
among patients and clinicians of the adverse effects
associated with long-term NSAID use. Since NSAID use
can mask symptoms by reducing inflammation,32,61 it
can obscure RA progression and often delays referral
from general practitioners. Availability of NSAIDs over
the counter in many Asian countries also poses a signifi-
cant challenge. Clearly, therefore, educating the public
and allied healthcare workers is an important priority
concern in this region.
696 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.
Section 3 – Role of corticosteroids
Recommendation 12. Oral corticosteroid monotherapyis not recommended. (Level IV; Strength D)
Supporting evidence
References 17, 21, 22, 25, 28, 32, 57, 62 and 63.
Summary of evidence linked to recommendation statement
Advice from a rheumatologist must be obtained before
treatment initiation with oral corticosteroids.62 The
Latin American guidelines do not recommend corticos-
teroids as a sole disease-modifying agent.57 The EULAR
2013 guidelines state that monotherapy is not specifi-
cally recommended and should only be used in excep-
tional cases when all other DMARDs are
contraindicated.17 Other guidelines advise corticos-
teroid usage in combination with DMARDs.25,62
Special comment/recommendation for the AP region
The use of corticosteroids in Asia poses particular risks.
There is a widespread practice of self-medication as a
result of ineffective control of the sales of prescription
medications, leading to inappropriate use of corticos-
teroid agents.57 Misuse of corticosteroids among clini-
cians in some AP countries is also widespread. It is,
therefore, recommended that patients with suspected
RA be assessed by a practitioner experienced in dealing
with RA and not be put on corticosteroid monotherapy
without a firm indication.
Recommendation 13. Oral corticosteroids can be con-sidered to control active RA in combination withcDMARDs. (Level I; Strength A)
Supporting evidence
References 17, 21, 22, 25, 28, 32, 57, 62 and 63.
Summary of evidence linked to recommendation
Low-dose corticosteroids can be considered as part of
the initial treatment strategy (in combination with
one or more cDMARDs) for up to 6 months, but
should be tapered as rapidly as clinically feasible.17
Short-term treatment with corticosteroids should be
offered for managing flares in patients with recent-
onset or established disease, to rapidly decrease
inflammation.28,32
For polyarticular flares, or at first presentation of the
disease, intramuscular/intra-articular, or short oral
courses of corticosteroids can decrease symptoms while
waiting for other slower-acting drugs to take effect; this
is described as “bridging therapy”.17,22,23,25,32,57,62,63
Intra-articular injections are extremely useful for treat-
ing a flare in one or only a few joints.22,28,32 Injection
into the same joint should not be repeated before
3 months, and it is advised that no more than three
injections be administered per joint per year.22
For severe extra-articular manifestations, intravenous
corticosteroids can save critical organs (e.g., eyes in scle-
ritis) or, occasionally, even life-threatening complica-
tions (e.g., severe serositis or vasculitis); however,
corticosteroids should be used in combination with
immunosuppressive agents such as cyclophos-
phamide.32
In people with established RA, only continue
long-term treatment with corticosteroids when: (a)
the long-term complications of corticosteroid therapy
have been fully discussed; and (b) all other treat-
ment options (including bDMARDs) have been
offered.32
Special comment/recommendation for the AP region
No region-specific comments.
Recommendation 14. In early RA, the addition of low-dose corticosteroids (prednisolone ≤ 7.5 mg/day) tocDMARDs leads to a reduction in radiographic pro-gression. (Level I; Strength A)
Supporting evidence
References 17, 21, 22, 25, 28, 32, 57, 62 and 63.
Summary of evidence linked to recommendation
The EULAR 2010, Latin American and NICE guidelines
discuss the evidence that low-dose prednisolone
(< 7.5 mg daily) in patients with early RA does reduce
radiographic progression over 2 years.32,57,63 According
to the European Standing Committee for International
Clinical Studies Including Therapeutics (ESCISIT) 2007
guidelines, corticosteroids are “probably effective in
slowing radiographic progression in early and estab-
lished RA”.21
Special comment/recommendation for the AP region
No region-specific comments.
Recommendation 15. Corticosteroids should be usedin the lowest possible dose and tapered as rapidly asclinically feasible. (Level IV; Strength D)
Supporting evidence
References 17, 21, 22, 25, 28, 32, 57, 62 and 63.
International Journal of Rheumatic Diseases 2015; 18: 685–713 697
APLAR RA recommendations

Summary of evidence linked to recommendation statement
It is recommended to keep the requirement for con-
tinuing corticosteroid treatment under constant
review, and titrate the dose against therapeutic
response, risk of under-treatment and development
of adverse events.17 However, the panel could not
recommend an optimal tapering strategy based on
the existing evidence. The Canadian 2012 and Ger-
man 2013 guidelines recommend that corticosteroids
should be used at the lowest possible dose and
tapered as rapidly as possible.25,28 In contrast, the
EULAR 2010 guidelines recommend slow tapering to
avoid clinical relapses.63
Special comment/recommendation for the Asia-Pacific region
This recommendation is particularly relevant in the AP
region due to the widespread misuse of corticosteroids
in some countries as stated above.
Section 4 – Role of cDMARDs
Recommendation 16. Treatment with cDMARDs asmonotherapy or in combination should be started assoon as the diagnosis of RA is made. (Level I;Strength A)
Supporting evidence
References 17, 18, 21–26, 28, 29 and 57.
Summary of evidence linked to recommendation statement
Most of the guidelines recommend starting cDMARDs
as soon as possible once the diagnosis of RA is con-
firmed;17,23,25,28,29,57 treatment should not be delayed
by more than 3 months.23 The ACR–EULAR 2010 clas-
sification criteria should be used to confirm diagnosis
of RA and facilitate early introduction of effective ther-
apy in RA. In patients with undifferentiated arthritis,
the use of cDMARDs can be considered,26 but in
patients at risk of developing persistent and/or erosive
arthritis, treatment with cDMARDs should be started as
early as possible even if they do not fulfil the diagnostic
criteria.21 In patients with early RA, cDMARD
monotherapy is recommended in low and moderate
disease activity, or high disease activity without poor
prognostic markers.
Special comment/recommendation for the AP region
Delay in initiating cDMARD treatment for patients with
RA in the AP region remains a major concern, primarily
due to delay in the diagnosis of the underlying condi-
tion. Much work is needed to enhance public and clini-
cian awareness of RA and its treatment.
Recommendation 17. Methotrexate is the first-linecDMARD for RA patients, and is considered as the an-chor drug. (Level I; Strength A)
Supporting evidence
References 17, 21–29 and 57.
Summary of evidence linked to recommendation statement
Methotrexate is the preferred cDMARD with respect
to efficacy and safety and should be the first
cDMARD used in RA unless contraindicated;17,24–26,28
it is described as the “anchor drug”21,22,27 or “drug
of choice”.24,57 DMARD-naive patients should be
started on methotrexate monotherapy, and treatment
should be given for a duration of no less than
3 months at the maximally tolerated dose.23 Choice
of the first agent is based on the risk : benefit ratio
with hydroxychloroquine an option in disease per-
ceived as mild, and methotrexate or sulfasalazine in
diseases adjudged moderate-to-severe, or likely to
progress.29
Special comment/recommendation for the AP region
Methotrexate used to be a taboo and thought to be
excessively hepatotoxic in many AP countries. However,
the efficacy and safety of this agent is now well estab-
lished and methotrexate should be used unless con-
traindicated or there is poor tolerance.
Recommendation 18. Patients who cannot toleratemethotrexate may receive other cDMARDs such asleflunomide, sulfasalazine and hydroxychloroquineas first-line treatment (Level I; Strength A). Bucil-lamine, iguratimod, cyclosporin, azathioprine, intra-muscular gold or tacrolimus may also be consideredin some AP countries. (Level I; Strength B)
Supporting evidence
References 17, 23–26, 57 and 64–68.
Summary of evidence linked to recommendation statement
Patients without poor prognostic factors (i.e., with no
erosions, are RF-negative, with low CRP levels, or with
low disease activity) or those who cannot tolerate
methotrexate may receive other cDMARDs, such as
leflunomide, sulfasalazine, hydroxychloroquine or
injectable gold.23 The antimalarials hydroxychloro-
quine and chloroquine are less effective and should be
698 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

reserved for mild disease forms and diseases with low
erosive potential.24
Special comment/recommendation for the AP region
In many Asian countries, chloroquine may be recom-
mended and is preferred to hydroxychloroquine or
other cDMARDs due to its low treatment cost and high
availability. In some AP countries, cDMARDs such as
bucillamine and iguratimod, which are not available in
Western countries, are widely used. Though these drugs
have not been thoroughly evaluated outside their coun-
tries of origin, they have undergone rigorous testing
locally and may also be the cDMARDs of choice for RA
in the respective countries. For example, the efficacy of
bucillamine can be judged within 3 months in moder-
ately active RA patients either before or after methotrex-
ate treatment.64 Iguratimod is non-inferior in active RA
patients when compared to methotrexate65 or salazo-
sulfapyridine.66 Tacrolimus improves RA symptoms in
patients with RA inadequately controlled with at least
one prior cDMARD67 and is well tolerated.68
Recommendation 19. Pre-treatment investigations:complete blood count, liver function and renal func-tion tests, viral hepatitis serology and chest radio-graph should be ordered prior to initiatingmethotrexate therapy (Level II; Strength B).
Supporting evidence
References 22, 23 and 57.
Summary of evidence linked to recommendation statement
Pre-treatment investigations prior to initiating
methotrexate should include complete blood count
(CBC), liver function test (LFT) and renal function test
(RFT), hepatitis B and C serology and chest X-
ray.22,23,57 Other guidelines also consider screening for
risk factors for cardiovascular diseases and osteoporo-
sis,23 and human immunodeficiency virus (HIV) in
high-risk patients.28 The pre-treatment investigations
for other cDMARDs are: eye examination (funduscopy
and perimetry) for antimalarials; and CBC, RFT and
LFT for leflunomide, sulfasalazine, cyclosporine, and
azathioprine. Blood pressure and serum creatinine
should also be measured prior to initiating leflunomide
and cyclosporine.22
Special comment/recommendation for the AP region
The high prevalence of hepatitis and TB in the AP
region provides the rationale for recommending the
pre-treatment investigations described above before
starting methotrexate treatment.
Recommendation 20. Combination cDMARD therapyshould be considered in patients with active RA, par-ticularly those with poor prognostic factors. (Level I;Strength B)
Supporting evidence
References 17, 18, 23–25 and 28.
Summary of evidence linked to recommendation statement
If, after 3 months of cDMARD monotherapy (in
patients without poor prognostic features), a patient
deteriorates from low to moderate/high disease activ-
ity, then methotrexate, hydroxychloroquine or
leflunomide should be added.18 A combination of
cDMARDs (including double or triple therapy) may
be considered in patients with very serious disease
and poor prognostic factors.17,18,23–25,28 Patients with
suboptimal treatment response should receive step-
up therapy with combination therapy of methotrex-
ate plus another agent (leflunomide, sulfasalazine,
hydroxychloroquine).23 Initial combination therapy
with cDMARDs may also be considered, particularly
in patients with poor prognostic features, moderate-
to-high disease activity, and patients with recent-on-
set disease.
Special comment/recommendation for the AP region
Long-term treatment compliance with mono- or combi-
nation cDMARD therapy is a challenge in many AP
countries. This may be related to the cost of treatment,
anxiety about drug side effects and the need for regular
monitoring. Patients should be educated about the dis-
ease and the need for uninterrupted treatment. Clini-
cians should explore this possibility and patients
should also be reassured of the safety of the prescribed
drugs, and encouraged to have adequate trials of
cDMARD monotherapy before escalation to combina-
tion cDMARD therapy.
Recommendation 21. Combination cDMARD therapyshould include methotrexate as the anchor drugunless methotrexate is contraindicated. (Level II;Strength B)
Supporting evidence
References 17, 18, 21–26, 28, 32 and 57.
International Journal of Rheumatic Diseases 2015; 18: 685–713 699
APLAR RA recommendations

Summary of evidence linked to recommendation statement
Most guidelines recommend methotrexate as the anchor
drug unless it is contraindicated.17,18,21–24,26,28,57
Although direct comparisons between different regimens
are lacking, combination cDMARD therapies, including
methotrexate, have been proven to be superior to
cDMARD monotherapy. Other combinations without
methotrexate are not sufficiently evaluated. On the basis
of guideline review, the panel recommends methotrexate
combination therapy in patients who have inadequate
response to methotrexate monotherapy.
The most commonly used cDMARDs in combina-
tion with methotrexate are hydroxychloroquine, sul-
fasalazine or their concurrent use. Leflunomide has
also been studied in association with methotrexate.
However, methotrexate combined with leflunomide
should be cautiously used because of higher toxic-
ity.69,70 Methotrexate-based combination therapies
with azathioprine, cyclosporine A and intramuscular
gold have been evaluated in at least one random-
ized controlled trial. The details of the regimens are
listed in the ACR 2008, NICE 2009 and EULAR
guidelines and a meta-analysis by Katchamart
et al.32,69,71–73
Special comment/recommendation for the AP region
As described above, cDMARDs available for treatment
of RA extend to bucillamine, iguratimod and tacrolimus
in certain AP countries. However, the use of these drugs
combined with methotrexate or as an anchor drug in
combination regimens has not been extensively studied
and requires further evaluation.
Recommendation 22. Triple therapy with cDMARDs isan effective option in patients who show inadequateresponse to methotrexate monotherapy. (Level II;Strength B)
Supporting evidence
References 17, 18, 21–26, 28, 32 and 57.
Summary of evidence linked to recommendation statement
All the reviewed guidelines recommend changing regi-
men in patients who fail methotrexate monother-
apy.17,18,21–26,28,32,57 The options include switching
among cDMARDs and switching from cDMARDs to
bDMARD agents. Combination cDMARD therapy can
be an effective alternative to bDMARD therapy. In
methotrexate-inadequate responders, methotrexate
combination with one or two kinds of other cDMARDs
was proven to be superior to methotrexate monother-
apy.73 More recent data showed that triple therapy with
cDMARDs had similar efficacy with bDMARD ther-
apy.74–76 Although most recommendations did not
specify the mandatory application of triple cDMARDs
after methotrexate failure, current evidence suggests that
triple therapy with cDMARDs may be able to substitute
for bDMARD therapy.
The TACIT trial, which was published since the cur-
rent consensus was reached, showed combination
methotrexate and leflunomide was an equally effective
regimen as methotrexate plus a TNF inhibitor.77 This
combination may also be considered as an alternative
for triple combination cDMARDs.
Special comment/recommendation for the AP region
Because of the high cost and limited availability of
bDMARDs in many AP countries, the panel recom-
mends triple cDMARD therapy as an effective
option for patients with inadequate response to
methotrexate.
Recommendation 23. Patients should be assessedevery 1 to 3 months after the initial treatment orchange of regimen until the disease is stabilized, inremission or in low disease activity state. (Level I;Strength A)
Supporting evidence
References 17–19, 21, 24–26, 28, 32 and 72.
Summary of evidence linked to recommendation statement
One systematic review of trials on strategy-driven
treatment approaches in RA concluded that intensive
steering (treatment target, follow up method) and
intensive medication strategies in early active RA pro-
duces a better clinical outcome, improved physical
function and less structural damage.78
Early-stage active RA can be monitored
monthly.19,24,26,31 Radiographs of joints are recom-
mended as frequently as every 6 to 12 months during
the first few years21,28 or annually19 to estimate poten-
tial progression of joint damage.
Special comment/recommendation for the AP region
The shortage of rheumatologists in many AP coun-
tries represents a major hurdle to the frequent moni-
toring of RA patients. As indicated earlier, an
effective educational program for patients and other
healthcare providers, including general practitioners
and allied health workers, is urgently needed in
many AP countries.
700 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

Recommendation 24. Patients who have been stabi-lized or are in remission or low disease activitycan be monitored every 3 to 6 months. (Level IV;Strength D)
Supporting evidence
References 17, 19, 24, 26, 28, 32 and 55.
Summary of evidence linked to recommendation statement
Most guidelines agree that monitoring can be less fre-
quent once the treatment target has been stabilized.
However, the suggested monitoring intervals are vari-
able and may only represent the compromise of
expert opinion (IV, D). According to the Canadian
guidelines, patients in remission can be monitored at
longer intervals without further specification.28 The
Brazilian guidelines suggest monitoring every
3 months for controlled disease.25,26 The treat-to-tar-
get guidelines consider less frequent monitoring such
as every 3 to 6 months for patients in sustained, low
disease activity or remission.19 The EULAR 2013
guidelines propose monitoring every 6 to 12 months
once the treatment target has been stabilized.17 The
BSR-BHPR 2009 and NICE guidelines recommend
annual review.32,55
Special comment/recommendation for the AP region
No region-specific comments.
Recommendation 25. Definition of treatment failure:inadequate response with cDMARDs is defined asfailure to achieve remission or low disease activityafter a therapeutic trial of at least two standardcDMARDs in combination at optimal doses for6 months (Level I; Strength A). One of the failedcDMARDs must be methotrexate unless methotrex-ate is contraindicated. (Level I; Strength A)Supporting evidence
References 17, 18, 21–26, 28, 32, 34, 35, 52 and 57.
Summary of evidence linked to recommendation statement
Six guidelines define treatment target as remission or
low disease activity; thus, any other status would be
inadequate response/treatment failure.18,24–26,28,57
Three guidelines define target as remission.17,21,23 The
required treatment usually includes at least methotrex-
ate monotherapy unless not tolerated;18,28,34,35 or in
combination with another cDMARD.17,18,22–
24,26,28,32,48,52 The treatment duration, at a standard tar-
get dose, may be at least 3 months18,23,28,34,35,48,57 or
6 months.17,22,23,26,31,52
Special comment/recommendation for the AP region
No region-specific comments.
Section 5 – Role of bDMARDs
Recommendation 26. A bDMARD can be prescribed inpatients who have inadequate response or intoler-ance to cDMARDs. (Level I; Strength A)
Supporting evidence
References 17, 18, 22, 23, 25, 26, 28, 31, 33–36, 38, 39,48–51, 53, 54, 56–58 and 79.
Summary of evidence linked to recommendation statement
The BSR 2010 guidelines recommend starting a TNF
inhibitor in those who have active RA and have
inadequate response to cDMARDs.39 Inadequate
response is defined as DAS28 > 3.2 with ≥ 3 tender
and swollen joint counts, and being treated with at
least two cDMARDs (one should be methotrexate
unless contraindicated) in combination over a 6-
month period, and at a standard dose for at least
2 months, unless a significant toxicity occurs and
limits the dose and duration of treatment. Rituximab
(anti-CD20) should be prescribed in a patient who
has inadequate response or intolerance to at least
one TNF inhibitor,58 and still has active disease
defined by DAS28 ≥ 3.2 or SDAI > 11 or similar
indices. Tocilizumab (anti-IL-6) is recommended for
those who have moderate or severe disease activity,
according to a validated composite measure, and
have had inadequate response or intolerance to at
least one cDMARD or TNF inhibitor. Abatacept
(CTLA-4Ig) is recommended for those who have
moderate or severe disease activity, according to a
validated composite measure, and have had inade-
quate response or intolerance to at least one
cDMARD or TNF inhibitor.
Special comment/recommendation for the AP region
As has been stated above, as a result of the high cost
and limited availability of bDMARDs in many AP coun-
tries, triple cDMARD combination therapy may be con-
sidered for patients in whom bDMARDs are indicated.
Recommendation 27. Early bDMARD use can be con-sidered in patients who have active disease with poorprognostic factors. (Level IV; Strength D)
Supporting evidence
Reference 18.
International Journal of Rheumatic Diseases 2015; 18: 685–713 701
APLAR RA recommendations

Summary of evidence linked to recommendation statement
In 2012, the ACR suggested that TNF inhibitors,
with or without methotrexate, may be considered in
patients with early RA (duration < 6 months) and
high disease activity and poor prognostic features.
This recommendation is based on expert opinion as
the data on the use of TNF inhibitors in early RA
patients with active disease and poor prognostic fac-
tors are limited.18
Special comment/recommendation for the AP region
Once again, for countries with poor socioeconomic
status and where the reimbursement system is inade-
quate, combination cDMARD therapies, including triple
therapy, may be considered for these patients instead.
Recommendation 28. Prior to starting treatment withbDMARDs, history regarding active or current infec-tions, comorbidities including tumors and malignan-cies, vaccinations, pregnancy, and possiblecontraindications should be obtained in all patients.(Level I; Strength A)
Supporting evidence
References 18, 21, 22, 24, 26, 31, 33, 35, 38, 46, 48–50,53, 54, 56 and 57.
Summary of evidence linked to recommendation statement
Reports on the risk of serious infections and the devel-
opment of malignancies in RA patients receiving
bDMARD therapy, particularly TNF inhibitors, showed
conflicting results. A meta-analysis showed the use of
TNF inhibitors is associated with increased risk of seri-
ous infections,80,81 but another meta-analysis could not
confirm this finding.82
A meta-analysis of randomized controlled trials
found that the point estimate of malignancy risk was
higher in etanercept-treated patients than in controls,83
but two recent meta-analyses failed to confirm these
findings.84,85
Regarding pregnancy, data from the BSR Biologics
Register found that the incidence of spontaneous loss
among those who were prior exposed to TNF inhibitors
was higher than in controls (17% vs. 10%), but without
risk of significant congenital abnormalities. Neverthe-
less, they recommended that pregnancy be avoided dur-
ing anti-TNF therapy.86
A study on the effect of high-dose TNF inhibitor (in-
fliximab) showed a detrimental effect on congestive
heart failure;87 however, two recent studies could not
confirm this finding.88,89
Rituximab may be used in RA patients with lym-
phoma46 and should be avoided in those with
hypogammaglobulinemia or low CD4 counts.56 Tocili-
zumab should be avoided in those with a history of
bowel perforation.24,33,48
Special comment/recommendation for the AP region
It is of particular importance that clinicians have a high
level of alertness of pre-existing infectious diseases,
including uncommon infections, and other comorbidi-
ties in AP patients receiving bDMARDs because of dif-
ferences in the pattern and frequency of occurrence of
these conditions in this region.
Recommendation 29. All patients should be screenedfor TB, and hepatitis B and C virus infections beforeinitiating bDMARD therapy. (Level I; Strength A)
Supporting evidence
References 18, 22–24, 28, 31, 33, 34, 38, 43, 46, 48–50,52–54 and 56–58.
Summary of evidence linked to recommendation statement
Overall, 22 studies recommended screening for infec-
tions that included TB, HBV and HCV infections prior
to starting bDMARD therapy.18,22–24,28,31,33,34,38,43,46,
48–50,52–54,56–58 In Japan, testing for beta D-glucan is
also recommended prior to initiating TNF inhibitors
and tocilizumab (anti-IL-6).48,49
Special comment/recommendation for the AP region
The AP region is endemic for TB. Therefore, active and
latent TB should be evaluated and treated properly,
according to each individual country guideline, prior to
commencement of bDMARDs.
Recommendation 30. Live vaccines should be given atleast 4 weeks prior to administration of bDMARDagents. (Level III–IV; Strength C–D)
Supporting Evidence
References 18, 22–24, 31, 33–35, 37, 38, 43, 46, 48, 52,55, 56 and 58.
Summary of evidence linked to recommendation statement
Patients who are immunocompromised are at risk of
disseminated infection with live attenuated vaccines.
All guidelines reviewed emphasized that concurrent
administration of live attenuated vaccines was not rec-
ommended in patients receiving bDMARDs. Most
guidelines agree that live attenuated vaccines should be,
ideally, given 4 weeks prior to initiation of bDMARDs
702 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

but the level of evidence for this remained low (Level
IV).
Patients already on bDMARDs who require live
vaccines should only receive it 6 months after the
last infusion of infliximab or 23 weeks after the last
dose of etanercept.22,46,52 There was no guidance on
how long to discontinue other bDMARD agents,
although the Canadian guidelines recommend that
the timing for withholding/restarting therapy should
be based on the pharmacokinetic properties of the
agent used.
In the rare event when a live vaccine may be required
urgently in a patient on bDMARDs (e.g., outbreak or
urgent travel), discussion about the risks and benefits
should be undertaken with the patient in consultation
with an infectious disease physician.
Special comment/recommendation for the AP region
No region-specific comments.
Recommendation 31. Monotherapy or combinationwith methotrexate/cDMARDs: bDMARDs are mosteffective when combined with methotrexate. (Level I;Strength A)
Supporting evidence
References 17–19, 21, 23–26, 28, 29, 31–33, 35, 36, 38,48, 51, 52, 56 and 57.
Summary of evidence linked to recommendation statement
The guidelines reviewed recommend the use of
methotrexate in combination with bDMARD agents.
This combination is associated with significant ben-
efits in terms of control of disease activity,
improved function and quality of life as well as
retardation of radiographic progression.17,32
Methotrexate is also believed to reduce development
of human anti-chimeric antibody (HACA) in
patients receiving infliximab.51 In the CONCERTO
trial that enrolled early RA patients receiving adali-
mumab plus methotrexate, an increasing trend of
efficacy was observed with increased doses of
methotrexate. However, the efficacy of the 10 mg
weekly dose of methotrexate was equivalent to the
20 mg weekly dose.17
In cases where methotrexate is contraindicated, sev-
eral guidelines mention that alternative cDMARDs such
as leflunomide, sulfasalazine, azathioprine and cyclos-
porine can be combined with bDMARD agents.36,56 In
addition, adalimumab, etanercept and certolizumab
have been approved as monotherapy18,25,38,56 and toci-
lizumab has, likewise, been used as monotherapy for
patients with RA.17,23,25,33,48
Special comment/recommendation for the AP region
Please refer to recommendations 18 and 21.
Recommendation 32. In patients with RA who are can-didates for bDMARD therapy, the therapeutic optionsinclude TNF inhibitors, abatacept, tocilizumab andrituximab. (Level I; Strength A)
Supporting evidence
References 17–19, 21, 23–26, 28, 29, 31–33, 35, 36, 38,48, 51, 52, 56 and 57.
Summary of evidence linked to recommendation statement
In the ACR 2012 guidelines, TNF inhibitors may be
used as initial treatment for patients with early RA
(< 6 months’ duration) who present with high dis-
ease activity and poor prognostic factors).18 TNF
inhibitors provide the most robust efficacy and
safety among all bDMARD agents for RA. However,
recent data have shown other bDMARD agents such
as abatacept and tocilizumab have sufficient and
comparable efficacy and safety data and can be con-
sidered as first-line bDMARD agents.17,25 The use of
rituximab as first-line bDMARD therapy has been
described in certain circumstances, such as in
patients with history of lymphoma, demyelinating
disease or TB which precludes the use of other
bDMARD agents.17,56
Special comment/recommendation for the AP region
Patient preference and cost of treatment should always
be considered when choosing a particular bDMARD.
Several countries may have problems in sustaining the
use of bDMARDs due to non-reimbursement.
Recommendation 33. Patients who fail to achieveremission or low disease activity after 6 months ofbDMARD therapy are recommended to switch toanother bDMARD agent. (Level III; Strength C)
Supporting evidence
References 17, 18, 23–25, 28, 29, 31, 33, 34, 36, 38, 44,52–54, 57 and 58.
Summary of evidence linked to recommendation statement
In the era of treat-to-target in RA, a significant delay
should not be allowed before switching therapy in
patients who have not achieved an adequate response.
Most guidelines suggest a timeline of 12 weeks. The
International Journal of Rheumatic Diseases 2015; 18: 685–713 703
APLAR RA recommendations

ACR guidelines separated the duration of failure with a
TNF inhibitor (3 months) and a non-TNF inhibitor
bDMARD (6 months) as it was felt that the response to
treatment to non-TNF inhibitor bDMARDs may take
longer.18
Observational studies have suggested that switching
to a second TNF inhibitor after failure of the first
may be a feasible option. There are no controlled tri-
als to compare switching to a second TNF inhibitor
or a bDMARD agent of another mode of action, so
the choice should be based on a shared decision
between the patient and the physician based on
patient’s preferences and characteristics. The EULAR
recommendations emphasize that no preference is
stated.17
Two guidelines specifically looked at switching to
another bDMARD after failure of rituximab.31,58 Early
studies suggested a numerical but not statistically sig-
nificant increase in infections with the use of TNF
inhibitors after rituximab but further follow up
showed that there was no difference in incidence of
infection. Data from registries suggest that use of
abatacept after rituximab is also safe, but further data
are needed.
Special comment/recommendation for the AP region
Biosimilars may be available in certain AP countries.
They may be considered because of their comparatively
lower cost. However, the use of these agents must also
be based on available evidence. This will be discussed
in a subsequent APLAR statement.
Recommendation 34. Dose reduction: in patients whohave achieved remission, a reduction in treatmentshould be considered. (Level I; Strength A). If thepatient remains in extended remission(> 12 months), tapering of bDMARDs can be consid-ered. (Level II; Strength B)
Supporting evidence
References 21, 28, 29, 34–37, 44 and 52.
Summary of evidence linked to recommendation statement
Of the 10 guidelines which discussed tapering of treat-
ment in the case of sustained remission, several recom-
mend that corticosteroids and/or NSAIDs should be
tapered first.28,29,34–37,44,52 Some, but not all, recom-
mend tapering of bDMARDs in patients with sustained
remission.21,29,35,37,44,52 The issue of withdrawal after
remission is reached remains inadequately researched
and is stated as an item in the ‘research agenda’ in the
EULAR 2013 guidelines.17
Special comment/recommendation for the AP region
As has been highlighted earlier, long-term bDMARDs
are not often affordable by most patients in the AP
region. They often request their clinician to taper or
even stop their treatment early. While awaiting further
data to become available, the Steering Committee rec-
ommends that tapering should only be considered if a
patient has remained in disease remission for at least
12 months.
Recommendation 35. Infectious complications: TBScreening for TB is recommended prior to startingbDMARD therapy. (Level II; Strength B) All patientswith latent TB infection (LTBI) should receive pro-phylactic anti-TB therapy. (Level II; Strength B)Patients with active TB infection need to be ade-quately treated before consideration of bDMARDtreatment. (Level III; Strength C)
Supporting evidence
References 18, 22–24, 28, 35, 37, 43, 45–47 and 48–52.
Summary of evidence linked to recommendation statement
The most common criteria for “LTBI” included a
weal > 10 mm (different guidelines/consensus/recom-
mendations suggested different cut-off values for
tuberculin skin testing [TST]; the Hong Kong recom-
mendations used 10 mm induration for immuno-
competent patients and 5 mm for patients who are
significantly immunocompromised such as those
with HIV infection; the French 2003 TNFi and Latin
American 2006 guidelines also suggested 10 mm; the
Japanese 2007 guidelines suggested 20 mm; the
French 2007, Portuguese 2011 and Brazilian 2012
guidelines used 5 mm; the Philippine 2006 guideli-
nes suggested 8 mm) or a blister in response to a
TST done more than 10 years after the last Bacille-
Calmette Guerin (BCG) vaccination, with no history
of correct treatment for active TB, or residual radio-
graphic TB lesions > 1 cm in size with no
certainty.49
TNF inhibitors, particularly the monoclonal antibod-
ies, have been found to be associated with increased
incidence of TB.90 Prophylaxis with anti-TB drugs with
an accepted regimen, such as isoniazid 300 mg/day is
recommended at least 1 month prior to starting
TNF inhibitors and other bDMARD agents and be
704 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

maintained for 9 months in RA patients with occult TB
infection.
Special comment/recommendation for the AP region
The AP region has a high prevalence of active TB infec-
tions. Thus, the proportion of patients at risk for TB
infection and re-infection during bDMARD therapy is
higher when compared with Europe and North
America.
The high cost and limited availability of interferon-
gamma release assay (IGRA) and the lack of timely
access to infectious disease specialists may be barriers to
the accurate diagnosis of latent TB infection. Neverthe-
less, a chest X-ray and TST are the minimum require-
ments for screening for LTBI.
The common practice of administration of the BCG
vaccine across many AP countries may lead to a high
false-positive rate for TST. Thus, many AP countries
have set a higher cut-off value for LTBI screening pur-
poses. Clinicians are therefore recommended to refer to
their national guidelines for their respective criteria for
LTBI based on TST results. Where such guidelines are
unavailable, the committee recommends using the
development of a weal > 10 mm following TST as the
cut-off value for LTB1 warranting the use of prophylac-
tic anti-TB antibiotics prior to bDMARD treatment.
The issue of TB infections and RA treatment will be
dealt with in a subsequent APLAR recommendation
report.
Recommendation 36. Infectious complications: Hepati-tisPatients should be screened for HBV and HCV infec-
tions prior to the commencement of bDMARDs.(Level IV; Strength D) bDMARDs should be avoidedin patients with active or untreated chronic HBV infec-tion and active HCV infection. (Level III; Strength C)
Supporting evidence
References 18, 22–24, 31, 33, 35, 37, 43, 48, 51, 52, 56and 58 addressed the topic of hepatitis-related compli-
cations associated with bDMARD use, but no evidence
was identified to support this statement.
Summary of evidence linked to recommendation
Although there was some evidence, most is in the form
of case reports, some of which are contradictory.
Special comment/recommendation for the AP region
Patients with evidence of chronic viral hepatitis B infec-
tion, including serum positivity for hepatitis B surface
antigen or anti-hepatitis core antibodies, should be
given appropriate anti-viral treatment while on
bDMARD therapies. The cost of anti-viral treatment
plus the need for regular monitoring, including blood
hepatitis B DNA detection, will further lower the afford-
ability of bDMARDs for many RA patients in this
region. While appreciating the very high cost of anti-
HCV treatments, they should be considered in HCV-in-
fected patients prior to dDMARDs.
The timely access to infectious disease and hepa-
tology specialists is not always possible in many AP
countries. Rheumatologists need to stay vigilant of
these infections when starting bDMARDs for these
patients.
Recommendation 37. Active infections are contraindi-cations for bDMARDs. (Level I; Strength A) When aninfection is suspected, based on clinical judgement,the bDMARD agent should be stopped and thepatient must be treated appropriately. (Level IV;Strength D)
Supporting evidence
References 25, 26, 35, 37, 38, 43, 48–52 and 57.
Summary of evidence linked to recommendation
Of the 48 RA management recommendation reports, 11
discussed non-TB, non-hepatitis infec-
tions.25,26,35,37,43,48–52,57 Active infections as contraindi-
cations for bDMARDs were discussed in four
recommendations.35,38,48 Besides, past history of seri-
ous infections in the last 6 months and history of pneu-
mocystis pneumonia (PCP) were identified as
contraindications for bDMARDs in four guidelines.48–50
Compared with the general population, patients with
RA have an increased risk of infection, which is nearly
twice as high as that observed in matched non-RA con-
trols.91,92 When considering serious infections, a trend
toward an increased frequency compared to cDMARDs
has been noted regarding monoclonal anti-TNF anti-
bodies,93–95 with a significant increase reported in two
previous studies with infliximab and adalimumab.96,97
These findings are consistent with the results of a meta-
analysis published in 2006 that included all random-
ized controlled trials performed with infliximab and
adalimumab.80
Special comment/recommendation for the AP region
While there is no prevalence data from the AP region of
several transmissible diseases such as leprosy, malaria,
Chagas’ disease, schistosomiasis, yellow fever, dengue
International Journal of Rheumatic Diseases 2015; 18: 685–713 705
APLAR RA recommendations

fever, filariasis and helminthic infections, we recom-
mend physicians to remain alert regarding these condi-
tions so as to allow timely diagnosis and appropriate
treatment.
Recommendation 38. Pregnancy and lactation whileon bDMARDs should only be considered after thor-ough assessment of benefits and risks. (Level IV;Strength D)
Supporting evidence
References 22, 24, 31, 33, 37, 38, 43, 48, 51, 52, 57 and
58.
Summary of evidence linked to recommendation
There is an inherent inadequacy of safety data on
bDMARD agents during pregnancy because pregnant
women as a group are excluded from the majority of
premarketing clinical trials and safety studies for ethi-
cal reasons. However, most recommendations stated
that pregnancy and lactation should be avoided while
on bDMARDs and effective contraception is strongly
recommended to prevent pregnancy in women with
childbearing potential until more safety data are
available.
Special comment/recommendation for the AP region
Earlier, the Steering Committee suggested the consider-
ation of triple combination cDMARDs as an alternative
to bDMARDs because of cost and availability concerns.
It should be noted that cDMARDs are as potentially, or
more, toxic than bDMARDs.98
Recommendation 39. Vaccination: administration ofall vaccines, if indicated, should, ideally, be under-taken at least 4 weeks before starting a bDMARD.(Level III–IV; Strength C–D) Concurrent administra-tion of live, attenuated vaccines is an absolute con-traindication for patients being treated withbDMARDs. (Level IV; Strength D)
Supporting evidence
References 18, 22–24, 31, 33–35, 37, 38, 43, 46, 48, 52,55, 56, 58.
Table 4 Research agenda for some of the 40 treatment recommendations for RA patients in the AP region
I. General RA treatment strategies
Longitudinal studies of the socioeconomic cost of RA
Prevalence of use of complementary, over-the-counter and self-medications for RA
Setting a realistic treatment target for patients from countries with low resources
Evaluation of the role of non-rheumatologists and allied health workers in RA management
II. Role of NSAIDs
The use of NSAIDs and their short- and long-term side effects (much of this has already been carried out previously)
III. Role of corticosteroids
The prevalence of corticosteroid abuse
Evaluation of the effects of long-term low-dose corticosteroids
IV. Role of cDMARDs
Do Asian patients tolerate methotrexate less well?
Efficacy of combination cDMARDs involving agents such as bucillamine, iguratimod, intramuscular gold or tacrolimus
Effects of cDMARDs on TB reactivation and novel infections
Effects of cDMARDs on chronic viral hepatitis carriers
Comparison of the efficacy of triple cDMARD combination and biologic agents
V. Role of bDMARDs
Effects of bDMARDs on TB reactivation and novel infections
Effects of bDMARDs on chronic viral hepatitis carriers
The frequency and occurrence of infective complications, including opportunistic infections associated with bDMARD use
The frequency and occurrence of malignant conditions associated with bDMARD use
Dose titration of bDMARDs
VI. Role of tofacitinib
The efficacy and long- and short-term side-effect profile of tofacitinib
The efficacy of tofacitinib in bDMARD failure patients
The possible role of tofacitinib in bDMARD-na€ıve patients
bDMARD, biological DMARD; cDMARD, conventional DMARD; DMARD, disease-modifying antirheumatic drug; NSAID, non-steroidal anti-in-flammatory drug; RA, rheumatoid arthritis; TB, tuberculosis.
706 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

Summary of evidence linked to recommendation
Overall, there is a lack of data on the safety of vaccina-
tion during treatment with most bDMARDs. Further-
more, there are not many studies on the efficacy of
vaccines during treatment with bDMARDs; a study on
pneumococcal vaccination suggested that patients on
TNF inhibitors may not respond adequately to vaccina-
tion.99 Thus, the recommendation of the Steering Com-
mittee in this regard aligns with that of most guidelines
and is predominantly based on expert opinion.
Special comment/recommendation for the AP region
No region-specific comments.
Section 6 – Role of tofacitinib
Recommendation 40: Tofacitinib may be considered if abDMARD has failed. (Level II; Strength B).Supporting evidence
This recommendation is made not based on a review
of the treatment recommendations/guidelines that the
Steering Committee had initially identified. However,
the role of tofacitinib was included in the EULAR RA
treatment recommendations 2013 update.17
Summary of evidence linked to recommendation statement
Tofacitinib, a JAK inhibitor, has been under investiga-
tion as a therapy for RA. It is not a bDMARD or a
cDMARD. In a number of placebo-controlled studies,
tofacitinib, used either as a monotherapy or in combi-
nation with a cDMARD, primarily methotrexate, was
associated with reductions in signs and symptoms of
RA and improvement in physical function in patients
with active disease despite previous treatment with
cDMARDs.100–102 In another study of active disease-pa-
tients receiving background methotrexate, tofacitinib
was found to be significantly superior to placebo and
was numerically similar to adalimumab in efficacy.103
Furthermore, in a 6-month, double-blind, parallel-
group phase 3 study involving 266 patients who were
TNF inhibitor refractory, tofacitinib use was associated
with meaningful improvements in signs and symptoms
of RA and physical function.104 However, the efficacy of
this agent in other bDMARD refractory RA patients has
not been reported.
Special comment/recommendation for the AP region
While there is evidence that tofacitinib is useful in
active RA disease patients who have failed cDMARDs,
and probably those who are refractory to TNF inhibi-
tors, more data is needed to support its use as a first-
line DMARD or after a patient has failed a bDMARD,
specifically the non-TNF inhibitors. While we await
long-term data on the efficacy and side-effect profiles,
particularly infectious disease complications, of tofaci-
tinib, the Steering Committee felt it is not yet ready
to recommend its use in DMARD-na€ıve patients. The
other consideration is to do with the possible high
financial cost of tofacitinib which is significantly
higher than that of all cDMARDs. This is an impor-
tant consideration for many AP countries where there
are financial constraints in obtaining access to expen-
sive medications. Our decision to recommend its use
in patients who have failed a bDMARD is based on
an extrapolation of the data reported by Burmester
et al.104 The Steering Committee encourages national
societies to include tofacitinib in their national drug
formulary.
DISCUSSION
These are the first RA treatment recommendations
developed by APLAR. The AP region is unique in many
ways. It accounts for 61% of the world population with
diverse ethnic, cultural and socioeconomic varia-
tions.105 The prevalence, clinical manifestations,
response to treatment and outcome of RA patients in
many Asian countries have been suggested to differ
from those reported in the West. Importantly, rheuma-
tology is still a developing medical subspecialty in the
region with a severe shortage of trained rheumatologists
in many countries.106 Not only are many RA patients in
the AP region managed by non-rheumatologists, the
lack of resources also means RA clinical studies are
sparse and that a big gap exists in the evidence-based
management of RA in this region.
The primary aim of these treatment recommenda-
tions is to provide clinicians with an evidence-based
reference for the treatment of RA in the AP region.
The Steering Committee was comprised of rheumatol-
ogists from 12 AP countries representing a diverse
spectrum of cultures and ethnicities, health economic
statuses and practises of rheumatology in the region.
A patient with RA was also invited to join the Com-
mittee so as to include patients’ perspectives on the
treatment of their condition in the recommendations.
Because of the nature of the recommendation drafting
process which required members to communicate in
English, a patient from Hong Kong who was literate
in the language was invited to join the Committee.
International Journal of Rheumatic Diseases 2015; 18: 685–713 707
APLAR RA recommendations

The Steering Committee did not perform a system-
atic review of original articles to inform recommenda-
tions. Instead, the recommendations were developed
using the ADAPTE framework12,13 appraising all
international RA practice guidelines and recommen-
dations through to December 2013. The ADAPTE
Collaboration is an international collaboration of
researchers, guideline developers and guideline
implementers who aim to promote the development
and use of clinical practice guidelines through the
adaptation of existing guidelines. Having first estab-
lished the scope and purpose of the current RA
treatment recommendations, the Steering Committee
conducted a thorough search for guidelines and rele-
vant documentations that have been previously pub-
lished. Each of these articles was then assessed for
guideline quality, currency, content, consistency and
acceptability/applicability for the AP region using the
AGREE instrument.15 Selected previous guidelines
were rigorously and systematically reviewed and dis-
cussed by members of the Steering Committee
before they were customized to create the current
adapted recommendations. The generic adaptation
process of ADAPTE has been shown to be valid and
of high quality.12,13
Based on the key questions that the Steering Com-
mittee had identified regarding the treatment of RA
in the AP region, 40 recommendations concerning
the general RA treatment strategies, and the role of
NSAIDs, corticosteroids, cDMARDs, bDMARDs and
tofacitinib have been made. Specific issues relating to
the safety and monitoring of cDMARDs and
bDMARDs are not covered in the current report.
These include screening and prophylactic treatment
for latent TB, management of patients who are
chronic viral hepatitis B/C carriers and precautions
with other regional prevalent infectious diseases.
These will be covered separately in a later instalment
of the recommendations.
The role of tofacitinib, a JAK inhibitor, in RA was not
originally included as one of the key questions. How-
ever, midway through the development of these recom-
mendations, tofacitinib became available in a number
of AP countries and a recommendation on the use of
this agent was included in the EULAR RA treatment rec-
ommendations 2013 update. The Steering Committee
therefore felt it would be appropriate to include the role
of tofacitinib in RA treatment in the current recommen-
dations.
Realizing that many Asian countries are under-re-
sourced to allow them to adhere strictly to the recom-
mendations made in this report, the Steering
Committee added comments based on expert opinions
and consensus following each recommendation in the
hope that minimum care requirement is achieved for all
RA patients in these countries. In addition, it is hoped
that some of these region-specific comments, which
may lack full evidence, may form the basis of a research
agenda, which is by no means exhaustive, for clinicians
in the AP region (Table 4).
It should be noted that the current report does not
include recommendations for physical and occupa-
tional treatment, and alternative/complementary ther-
apies which are widely practised by many patients in
the AP region. This is partly because evidence on the
role of these treatment modalities is sparse. Further-
more, in many AP countries, the physical and occu-
pational therapy disciplines are poorly developed.
However, where physical and other non-pharmaco-
logical therapies are available, clinicians should
advise RA patients about their roles in protecting nor-
mal joint function. For example, the BSR 2005 guide-
lines mentioned that patients should be informed
about alternative techniques of effective pain manage-
ment, including transcutaneous nerve stimulation
(TENS) and behavioral approaches.60 Others have
also found that physical therapy and exercise are ben-
eficial in RA patients.57 Where resources are limited
and patients are unable to afford the cost of proce-
dures such as TENS, patients may be advised to exer-
cise at home, as leisure time physical activity has
also been shown to be beneficial and should be
encouraged.22
CONCLUSION
APLAR has developed a set of general recommenda-
tions for the best practise management of RA in the
AP region. We are also hopeful that some of these
recommendations, where evidence for this region
may be lacking, may stimulate clinicians to embark
on research studies to resolve them. Specific issues
such as the prevention of reactivation or novel TB
and viral hepatitis infections will be addressed in a
second instalment.
ACKNOWLEDGEMENTS
We would like to thank the Asia Pacific League of Asso-
ciations for Rheumatology (APLAR) for funding this
project, Ms King Chu Chan for serving as a patient rep-
resentative on the Steering Committee, Dr Josef Smolen
708 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

and Dr Vibeke Strand for reviewing the recommenda-
tions, and Dr Pradnya Kulkarni and Mr Chris Facey of
MIMS (Hong Kong) Limited for providing medical writ-
ing support.
FUNDING
APLAR and unrestricted educational grants from the fol-
lowing pharmaceutical companies: AbbVie, Janssen, Pfi-
zer, Roche and UCB.
CONFLICT OF INTEREST
All authors have disclosed any conflicts of interest. The
individual declarations are summarized below. CSL has
received unrestricted educational grants from AbbVie,
Janssen-Cilag, Pfizer, Roche and UCB, and personal fees
from Abbvie, Bristol-Myers Squibb, Celltrion,
GlaxoSmithKline, Pfizer, Roche, Sanofi-Aventis and
UCB; AH has received grants from Roche, and personal
fees from Abbvie and Pfizer; MK has received personal
fees from AbbVie, Astellas, Bristol-Myers Squibb, Chu-
gai, Eisai, Janssen, Ono, Pfizer, Santen and Tanabe-Mit-
subishi; JJL has received personal fees from Janssen,
Pfizer and Roche; WL has received personal fees from
Janssen, Pfizer, Roche and Sanofi-Aventis, and investiga-
tor fees from Janssen, Pfizer and Roche; PN has received
research grants and personal fees from Pfizer; PS has
received research grants from Pfizer. All other authors
declare no conflict.
CONTRIBUTIONS
All authors were involved in performing the literature
search, appraisal of guideline quality, grading of evi-
dence, evidence synthesis, development of recommen-
dations, and writing and proofreading of recommen-
dations.
REFERENCES
1 McInnes IB, Schett G (2011) The pathogenesis of
rheumatoid arthritis. N Engl J Med 365, 2205–19.2 Turesson C, Jacobsson L, Bergstr€om U (1999) Extra-artic-
ular rheumatoid arthritis: prevalence and mortality.
Rheumatology (Oxford) 38, 668–74.3 Moreland L (2005) Unmet needs in rheumatoid arthritis.
Arthritis Res Ther 7 (Suppl. 3), S2–8.4 Salaffi F, Carotti M, Gasparini S et al. (2009) The health-
related quality of life in rheumatoid arthritis, ankylosing
spondylitis, and psoriatic arthritis: a comparison with a
selected sample of healthy people. Health Qual Life Out-
comes 7, 25.5 Filipovic I, Walker D, Forster F et al. (2011) Quantifying
the economic burden of productivity loss in rheumatoid
arthritis. Rheumatology (Oxford) 50, 1083–90.6 Gettings L (2010) Psychological well-being in rheuma-
toid arthritis: a review of the literature. Musculoskeletal
Care 8, 99–106.7 Smolen JS, Aletaha D, Koeller M et al. (2007) New thera-
pies for treatment of rheumatoid arthritis. Lancet 370(9602), 1861–74.
8 Flavell KJ, Biddulph JP, Powell JE et al. (2001) South
Asian ethnicity and material deprivation increase the risk
of Epstein-Barr virus infection in childhood Hodgkin’s
disease. Br J Cancer 85, 350–6.9 Glaser SL, Gulley ML, Clarke CA et al. (2008) Racial/eth-
nic variation in EBV-positive classical Hodgkin lym-
phoma in California populations. Int J Cancer 123,1499–507.
10 Kwong YL, Anderson BO, Advani R et al. (2009) Manage-
ment of T-cell and natural-killer-cell neoplasms in Asia:
consensus statement from the Asian Oncology Summit
2009. Lancet Oncol 10, 1093–101.11 World Cancer Research Fund International. Cancer statis-
tics, data on specific cancers: Stomach cancer. Available at
http://www.wcrf.org/int/cancer-facts-figures/data-specific-
cancers/stomach-cancer-statistics. Accessed 8 July 2015.
12 http://www.g-i-n.net/document-store/working-groups-
documents/adaptation/adapte-manual-for-guideline.pdf/
view. Accessed 8 July 2015.
13 Schieir O, Hazlewood G, Akhavan P et al. (2010) Time to
ADAPTE: a novel methodology for the development of
national clinical practice guidelines to expedite dissemi-
nation [abstract]. Ann Rheum Dis 69 (Suppl. 3), 652.
14 AGREE Collaboration (2003) Development and valida-
tion of an international appraisal instrument for assess-
ing the quality of clinical practice guidelines: the AGREE
project. Qual Saf Health Care 12 (1), 18–23.15 Brouwers MC, Kho ME, Browman GP et al. (2010)
AGREE II: advancing guideline development, report-
ing and evaluation in health care. CMAJ 182(18), E839–42.
16 Harbour R, Miller J (2001) A new system for grading rec-
ommendations in evidence based guidelines. BMJ 323(7308), 334–6.
17 Smolen JS, Landew�e R, Breedveld FC et al. (2014) EULAR
recommendations for the management of rheumatoid
arthritis with synthetic and biological disease-modifying
antirheumatic drugs: 2013 update. Ann Rheum Dis 73,492–509.
18 Singh JA, Furst DE, Bharat A et al. (2012) 2012 update of
the 2008 American College of Rheumatology recommen-
dations for the use of disease-modifying antirheumatic
drugs and biologic agents in the treatment of rheumatoid
arthritis. Arthritis Care Res (Hoboken) 64, 625–39.
International Journal of Rheumatic Diseases 2015; 18: 685–713 709
APLAR RA recommendations

19 Smolen JS, Aletaha D, Bijlsma JW et al. (2010) Treating
rheumatoid arthritis to target: recommendations of an
international task force. Ann Rheum Dis 69, 631–7.20 Schoels M, Smolen JS (2012) Treating rheumatoid arthri-
tis to target: evidence-based recommendations for
enhanced disease management. Reumatol Clin 8 (1), 1–2.21 Combe B, Landewe R, Lukas C et al. (2007) EULAR rec-
ommendations for the management of early arthritis:
report of a task force of the European Standing Commit-
tee for International Clinical Studies Including Therapeu-
tics (ESCISIT). Ann Rheum Dis 66 (1), 34–45.22 Misra R, Sharma BL, Gupta R et al. (2008) Indian
Rheumatology Association consensus statement on the
management of adults with rheumatoid arthritis. Indian J
Rheumatol 3 (Suppl. 3), 1–16.23 Mok CC, Tam LS, Chan TH et al. (2011) Management of
rheumatoid arthritis: consensus recommendations from
the Hong Kong Society of Rheumatology. Clin Rheumatol
30, 303–12.24 da Mota LM, Cruz BA, Brenol CV et al. (2012) 2012
Brazilian Society of Rheumatology Consensus for the
treatment of rheumatoid arthritis. Rev Bras Reumatol 52,152–74.
25 Albrecht K, Kr€uger K, Wollenhaupt J et al. (2014) Ger-
man guidelines for the sequential medical treatment of
rheumatoid arthritis with traditional and biologic dis-
ease-modifying antirheumatic drugs. Rheumatol Int 34(1), 1–9.
26 da Mota LM, Cruz BA, Brenol CV et al. (2013) Guidelines
for the drug treatment of rheumatoid arthritis. Rev Bras
Reumatol 53, 158–83.27 Katchamart W, Bourr�e-Tessier J, Donka T et al. (2010)
Canadian recommendations for use of methotrexate in
patients with rheumatoid arthritis. J Rheumatol 37, 1422–30.
28 Bykerk VP, Akhavan P, Hazlewood GS et al. (2012) Cana-
dian Rheumatology Association recommendations for
pharmacological management of rheumatoid arthritis
with traditional and biologic disease-modifying antirheu-
matic drugs. J Rheumatol 39, 1559–82.29 Luqmani R, Hennell S, Estrach C et al. (2006) British
Society for Rheumatology and British Health Profession-
als in Rheumatology guideline for the management of
rheumatoid arthritis (after the first 2 years). Rheumatology
(Oxford) 45, 1167–9.30 Ruyssen-Witrand A, Guernec G, Nigon D et al. (2014)
Aiming for SDAI remission versus low disease activity at
1 year after inclusion in ESPOIR cohort is associated with
better 3-year structural outcomes. Ann Rheum Dis 74,1676–83.
31 Buch MH, Smolen JS, Betteridge N et al. (2011) Updated
consensus statement on the use of rituximab in patients
with rheumatoid arthritis. Ann Rheum Dis 70, 909–20.32 The National Collaborating Centre for Chronic Condi-
tions (2009) Rheumatoid arthritis: National clinical
guidelines for management and treatment in adults.
Available at http://www.ncbi.nlm.nih.gov/pubmed-
health/PMH0009576/pdf/TOC.pdf. Accessed 8 July 2015.
33 Smolen JS, Schoels MM, Nishimoto N et al. (2013) Con-
sensus statement on blocking the effects of interleukin-6
and in particular by interleukin-6 receptor inhibition in
rheumatoid arthritis and other inflammatory conditions.
Ann Rheum Dis 72, 482–92.34 Fautrel B, Constantin A, Morel J et al. (2006) Recommen-
dations of the French Society for Rheumatology. TNFaantagonist therapy in rheumatoid arthritis. Joint Bone
Spine 73, 433–41.35 Fautrel B, Pham T, Mouterde G et al. (2007) Recommen-
dations of the French Society for Rheumatology regarding
TNFa antagonist therapy in patients with rheumatoid
arthritis. Joint Bone Spine 74, 627–37.36 Caporali R, Conti F, Alivernini S et al. (2011) Recommen-
dations for the use of biologic therapy in rheumatoid
arthritis: update from the Italian Society for Rheumatology
I. Efficacy. Clin Exp Rheumatol 29 (3 Suppl. 66), S7–14.37 Favalli EG, Caporali R, Sinigaglia L et al. (2011) Recom-
mendations for the use of biologic therapy in rheumatoid
arthritis: update from the Italian Society for Rheumatol-
ogy II. Safety. Clin Exp Rheumatol 29 (3 Suppl. 66), S15–27.
38 Fonseca JE, Bernardes M, Canh~ao H et al. (2011) Por-
tuguese guidelines for the use of biological agents in
rheumatoid arthritis – October 2011 update. Acta Reuma-
tol Port 36, 385–8.39 Deighton C, Hyrich K, Ding T et al. (2010) BSR and
BHPR rheumatoid arthritis guidelines on eligibility crite-
ria for the first biological therapy. Rheumatology (Oxford)
49, 1197–9.40 Dudler J, Finckh A, Kyburz D et al. (2010) Swiss consen-
sus statement: recommendations for optimising re-treat-
ment with MabThera (rituximab) in rheumatoid arthritis.
Swiss Med Wkly 140, w13073.41 Pham T, Gossec L, Fautrel B et al. (2005) Physical exami-
nation and laboratory tests in the management of
patients with rheumatoid arthritis: development of rec-
ommendations for clinical practice based on published
evidence and expert opinion. Joint Bone Spine 72, 222–8.42 Gossec L, Fautrel B, Pham T et al. (2005) Structural evalu-
ation in the management of patients with rheumatoid
arthritis: development of recommendations for clinical
practice based on published evidence and expert opinion.
Joint Bone Spine 72, 229–34.43 Nordgaard-Lassen I, Dahlerup JF, Belard E et al. (2012)
Guidelines for screening, prophylaxis and critical infor-
mation prior to initiating anti-TNF-alpha treatment. Dan
Med J 59 (7), C4480.
44 Valesini G, Montecucco C, Cutolo M (2006) Recommen-
dations for the use of biologic (TNF-alpha blocking)
agents in the treatment of rheumatoid arthritis in Italy.
Clin Exp Rheumatol 24, 413–23.
710 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

45 Mariette X, Salmon D (2003) French guidelines for diag-
nosis and treating latent and active tuberculosis in
patients with RA treated with TNF blockers. Ann Rheum
Dis 62, 791.46 Bombardier C, Hazlewood GS, Akhavan P et al. (2012)
Canadian Rheumatology Association recommendations
for the pharmacological management of rheumatoid
arthritis with traditional and biologic disease-modifying
antirheumatic drugs: part II safety. J Rheumatol 39, 1583–602.
47 Lichauco JJ, Tankeh-Torres SA, Navarra SV et al. (2006)
Philippine guidelines on the screening for tuberculosis
prior to the use of biologic agents. APLAR J Rheumatol 9,184–92.
48 Koike R, Harigai M, Atsumi T et al. (2009) Japan College
of Rheumatology 2009 guidelines for the use of tocilizu-
mab, a humanized anti-interleukin-6 receptor mono-
clonal antibody, in rheumatoid arthritis. Mod Rheumatol
19, 351–7.49 Miyasaka N, Takeuchi T, Eguchi K (2006) Guidelines for
the proper use of etanercept in Japan. Mod Rheumatol 16,63–7.
50 Miyasaka N, Takeuchi T, Eguchi K (2005) Official Japa-
nese guidelines for the use of infliximab for rheumatoid
arthritis. Mod Rheumatol 15, 4–8.51 Koike R, Takeuchi T, Eguchi K et al. (2007) Update on
the Japanese guidelines for the use of infliximab and
etanercept in rheumatoid arthritis. Mod Rheumatol 17,451–8.
52 Ledingham J, Deighton CBritish Society for Rheumatol-
ogy Standards, Guidelines and Audit Working Group
(2005) Update on the British Society for Rheumatology
guidelines for prescribing TNFalpha blockers in adults
with rheumatoid arthritis (update of previous guidelines
of April 2001). Rheumatology (Oxford) 44, 157–63.53 Rheumatoid Arthritis Study Group of the Portuguese
Society of Rheumatology (2007) Portuguese guidelines
for the use of biological agents in rheumatoid arthritis –December 2007 update. Acta Reumatol Port 32, 363–6.
54 Fonseca JE, Canh~ao H, Reis M et al. (2010) Portuguese
guidelines for the use of biological agents in rheumatoid
arthritis – March 2010 update. Acta Reumatol Port 35 (1),
95–8.55 Luqmani R, Hennell S, Estrach C et al. (2009) British
Society for Rheumatology and British Health Profession-
als in Rheumatology guideline for the management of
rheumatoid arthritis (after the first 2 years). Rheumatology
(Oxford) 48, 436–9.56 Bukhari M, Abernethy R, Deighton C et al. (2011) BSR
and BHPR guidelines on the use of rituximab in rheuma-
toid arthritis. Rheumatology (Oxford) 50, 2311–3.57 Cardiel MH, PANLAR group, GLADAR group (2006) First
Latin American position paper on the pharmacological
treatment of rheumatoid arthritis. Rheumatology (Oxford)
45(Suppl.2), ii7–22.
58 Smolen JS, Keystone EC, Emery P et al. (2007) Consensus
statement on the use of rituximab in patients with
rheumatoid arthritis. Ann Rheum Dis 66, 143–50.59 Salmon D, GTI group, AFSSAPS group (2002) Recom-
mendations about the prevention and management of
tuberculosis in patients taking infliximab. Joint Bone Spine
69, 170–2.60 Kennedy T, McCabe C, Struthers G et al. (2005) BSR
guidelines on standards of care for persons with rheuma-
toid arthritis. Rheumatology (Oxford) 44, 553–6.61 Emery P, Breedveld FC, Dougados M et al. (2002) Early
referral recommendation for newly diagnosed rheuma-
toid arthritis: evidence based development of a clinical
guide. Ann Rheum Dis 61, 290–7.62 Mouterde G, Dernis E, Ruyssen-Witrand A et al. (2010)
Indications of glucocorticoids in early arthritis and
rheumatoid arthritis: recommendations for clinical prac-
tice based on data from the literature and expert opinion.
Joint Bone Spine 77, 597–603.63 Gorter SL, Bijlsma JW, Cutolo M et al. (2010) Current
evidence for the management of rheumatoid arthritis
with glucocorticoids: a systematic literature review
informing the EULAR recommendations for the manage-
ment of rheumatoid arthritis. Ann Rheum Dis 69, 1010–4.64 Sekiguchi N, Kameda H, Amano K et al. (2006) Efficacy
and safety of bucillamine, a D-penicillamine analogue, in
patients with active rheumatoid arthritis. Mod Rheumatol
16, 85–91.65 Lu LJ, Bao CD, Dai M et al. (2009) Multicenter, random-
ized, double-blind, controlled trial of treatment of active
rheumatoid arthritis with T-614 compared with
methotrexate. Arthritis Rheum 61, 979–87.66 Hara M, Abe T, Sugawara S et al. (2007) Efficacy and
safety of iguratimod compared with placebo and salazo-
sulfapyridine in active rheumatoid arthritis: a controlled,
multicenter, double-blind, parallel-group study. Mod
Rheumatol 17 (1), 1–9.67 Kawai S, Takeuchi T, Yamamoto K et al. (2011) Efficacy
and safety of additional use of tacrolimus in patients with
early rheumatoid arthritis with inadequate response to
DMARDs–a multicenter, double-blind, parallel-group
trial. Mod Rheumatol 21, 458–68.68 Takeuchi T, Kawai S, Yamamoto K et al. (2014) Post-mar-
keting surveillance of the safety and effectiveness of tacro-
limus in 3,267 Japanese patients with rheumatoid
arthritis. Mod Rheumatol 24 (1), 8–16.69 Saag KG, Teng GG, Patkar NM et al. (2008) American
College of Rheumatology 2008 recommendations for the
use of nonbiologic and biologic disease-modifying anti-
rheumatic drugs in rheumatoid arthritis. Arthritis Rheum
59, 762–84.70 Visser K, Katchamart W, Loza E et al. (2009) Multina-
tional evidence-based recommendations for the use of
methotrexate in rheumatic disorders with a focus on
rheumatoid arthritis: integrating systematic literature
International Journal of Rheumatic Diseases 2015; 18: 685–713 711
APLAR RA recommendations

research and expert opinion of a broad international
panel of rheumatologists in the 3E Initiative. Ann Rheum
Dis 68, 1086–93.71 Gaujoux-Viala C, Smolen JS, Landew�e R et al. (2010)
Current evidence for the management of rheumatoid
arthritis with synthetic disease-modifying antirheumatic
drugs: a systematic literature review informing the EULAR
recommendations for the management of rheumatoid
arthritis. Ann Rheum Dis 69, 1004–9.72 Smolen JS, Landew�e R, Breedveld FC et al. (2010) EULAR
recommendations for the management of rheumatoid
arthritis with synthetic and biological disease-modifying
antirheumatic drugs. Ann Rheum Dis 69, 964–75.73 Katchamart W, Trudeau J, Phumethum V et al. (2009) Ef-
ficacy and toxicity of methotrexate (MTX) monotherapy
versus MTX combination therapy with non-biological
disease-modifying antirheumatic drugs in rheumatoid
arthritis: a systematic review and meta-analysis. Ann
Rheum Dis 68, 1105–12.74 van Vollenhoven RF, Geborek P, Forslind K et al. (2012)
Conventional combination treatment versus biological
treatment in methotrexate-refractory early rheumatoid
arthritis: 2 year follow-up of the randomised, non-
blinded, parallel-group Swefot trial. Lancet 379 (9827),
1712–20.75 Moreland LW, O’Dell JR, Paulus HE et al. (2012) A ran-
domized comparative effectiveness study of oral triple
therapy versus etanercept plus methotrexate in early
aggressive rheumatoid arthritis: the treatment of Early
Aggressive Rheumatoid Arthritis Trial. Arthritis Rheum 64,2824–35.
76 O’Dell JR, Mikuls TR, Taylor TH et al. (2013) Therapies
for active rheumatoid arthritis after methotrexate failure.
N Engl J Med 369, 307–18.77 Scott DL, Ibrahim F, Farewell V et al. (2015) Tumour
necrosis factor inhibitors versus combination intensive
therapy with conventional disease modifying anti-rheu-
matic drugs in established rheumatoid arthritis: TACIT
non-inferiority randomised controlled trial. BMJ 350,h1046.
78 Knevel R, Schoels M, Huizinga TW et al. (2010) Current
evidence for a strategic approach to the management of
rheumatoid arthritis with disease-modifying antirheu-
matic drugs: a systematic literature review informing the
EULAR recommendations for the management of
rheumatoid arthritis. Ann Rheum Dis 69, 987–94.79 Emery P, Reginster JY, Appelboom T et al. (2001) WHO
Collaborating Centre consensus meeting on anti-cytokine
therapy in rheumatoid arthritis. Rheumatology (Oxford)
40, 699–702.80 Bongartz T, Sutton AJ, Sweeting MJ et al. (2006) Anti-
TNF antibody therapy in rheumatoid arthritis and the
risk of serious infections and malignancies: systematic
review and meta-analysis of rare harmful effects in ran-
domized controlled trials. JAMA 295, 2275–85.
81 Askling J, Fored CM, Brandt L et al. (2007) Time-depen-
dent increase in risk of hospitalisation with infection
among Swedish RA patients treated with TNF antagonists.
Ann Rheum Dis 66, 1339–44.82 Thompson AE, Rieder SW, Pope JE (2011) Tumor necro-
sis factor therapy and the risk of serious infection and
malignancy in patients with early rheumatoid arthritis: a
meta-analysis of randomized controlled trials. Arthritis
Rheum 63, 1479–85.83 Bongartz T, Warren FC, Mines D et al. (2009) Etanercept
therapy in rheumatoid arthritis and the risk of malignan-
cies: a systematic review and individual patient data
meta-analysis of randomised controlled trials. Ann Rheum
Dis 68, 1177–83.84 Le Blay P, Mouterde G, Barnetche T et al. (2012) Risk of
malignancy including non-melanoma skin cancers with
anti-tumor necrosis factor therapy in patients with
rheumatoid arthritis: meta-analysis of registries and sys-
tematic review of long-term extension studies. Clin Exp
Rheumatol 30, 756–64.85 Moulis G, Sommet A, B�en�e J et al. (2012) Cancer risk of
anti-TNF-a at recommended doses in adult rheumatoid
arthritis: a meta-analysis with intention to treat and per
protocol analyses. PLoS ONE 7, e48991.86 Verstappen SM, King Y, Watson KD et al. (2011) Anti-
TNF therapies and pregnancy: outcome of 130 pregnan-
cies in the BSR Biologics Register. Ann Rheum Dis 70,823–6.
87 Chung ES, Packer M, Lo KH et al. (2003) Random-
ized, double-blind, placebo-controlled, pilot trial of
infliximab, a chimeric monoclonal antibody to tumor
necrosis factor, in patients with moderate-to-severe
heart failure: results of the anti-TNF Therapy Against
Congestive Heart Failure (ATTACH) trial. Circulation
107, 3133–40.88 Listing J, Strangfeld A, Kekow J et al. (2008) Does tumor
necrosis factor alpha inhibition promote or prevent heart
failure in patients with rheumatoid arthritis? Arthritis
Rheum 58, 667–77.89 Westlake SL, Colebatch AN, Baird J et al. (2011) Tumour
necrosis factor antagonists and the risk of cardiovascular
disease in patients with rheumatoid arthritis: a systematic
literature review. Rheumatology 50, 518–31.90 British Thoracic Society Standards of Care Committee
(2005) BTS recommendations for assessing risk and for
managing Mycobacterium tuberculosis infection and dis-
ease in patients due to start anti-TNF-alpha treatment.
Thorax 60, 800–5.91 Caporali R, Caprioli M, Bobbio-Pallavicini F et al. (2008)
DMARDS and infections in rheumatoid arthritis. Autoim-
mun Rev 8, 139–43.92 Doran MF, Crowson CS, Pond GR et al. (2002) Fre-
quency of infection in patients with rheumatoid arthritis
compared with controls: a population-based study.
Arthritis Rheum 46, 2287–93.
712 International Journal of Rheumatic Diseases 2015; 18: 685–713
C. S. Lau et al.

93 Weinblatt ME, Keystone EC, Furst DE et al. (2003) Adali-
mumab, a fully human anti-tumor necrosis factor alpha
monoclonal antibody, for the treatment of rheumatoid
arthritis in patients taking concomitant methotrexate: the
ARMADA trial. Arthritis Rheum 48 (1), 35–45.94 Lipsky PE, van der Heijde DM, St Clair EW et al. (2000)
Infliximab and methotrexate in the treatment of
rheumatoid arthritis. Anti-Tumor Necrosis Factor Trial in
Rheumatoid Arthritis with Concomitant Therapy Study
Group. N Engl J Med 343, 1594–602.95 Breedveld FC, Weisman MH, Kavanaugh AF et al. (2006)
The PREMIER study: a multicenter, randomized, double-
blind clinical trial of combination therapy with adali-
mumab plus methotrexate versus methotrexate alone or
adalimumab alone in patients with early, aggressive
rheumatoid arthritis who had not had previous
methotrexate treatment. Arthritis Rheum 54 (1), 26–37.96 Keystone EC, Kavanaugh AF, Sharp JT et al. (2004) Ra-
diographic, clinical, and functional outcomes of treat-
ment with adalimumab (a human anti-tumor necrosis
factor monoclonal antibody) in patients with active
rheumatoid arthritis receiving concomitant methotrexate
therapy: a randomized, placebo-controlled, 52-week trial.
Arthritis Rheum 50, 1400–11.97 Westhovens R, Yocum D, Han J et al. (2006) The safety
of infliximab, combined with background treatments,
among patients with rheumatoid arthritis and various
comorbidities: a large, randomized, placebo-controlled
trial. Arthritis Rheum 54, 1075–86.98 Ǿstensen M, Andreoli L, Brucato A et al. (2014) State of
the Art: reproduction and Pregnancy in Rheumatic Dis-
eases. Autoimmun Rev 14, 376–86.
99 Elkayam O, Caspi D, Reitblatt T et al. (2004) The effect
of tumor necrosis factor blockade on the response to
pneumococcal vaccination in patients with rheumatoid
arthritis and ankylosing spondylitis. Semin Arthritis
Rheum 33, 283–8.100 Fleischmann R, Kremer J, Cush J et al. (2012) Placebo-
controlled trial of tofacitinib monotherapy in rheuma-
toid arthritis. N Engl J Med 367, 495–507.101 Kremer J, Li ZG, Hall S et al. (2013) Tofacitinib in
combination with nonbiologic disease-modifying anti-
rheumatic drugs in patients with active rheumatoid
arthritis: a randomized trial. Ann Intern Med 159,253–61.
102 van der Heijde D, Tanaka Y, Fleischmann R et al. (2013)
Tofacitinib (CP-690,550) in patients with rheumatoid
arthritis receiving methotrexate: twelve-month data from
a twenty-four-month phase III randomized radiographic
study. Arthritis Rheum 65, 559–70.103 van Vollenhoven RF, Fleischmann R, Cohen S et al.
(2012) Tofacitinib or adalimumab versus placebo in
rheumatoid arthritis. N Engl J Med 367, 508–19.104 Burmester GR, Blanco R, Charles-Schoeman C et al.
(2013) Tofacitinib (CP-690,550) in combination with
methotrexate in patients with active rheumatoid arthritis
with an inadequate response to tumour necrosis factor
inhibitors: a randomised phase 3 trial. Lancet 381(9865), 451–60.
105 http://www.unescap.org/stat/data/syb2011/I-People/Pop
ulation.pdf. Accessed 8 July 2015.
106 Lau CS, Feng PH (2007) Rheumatology without borders.
Nat Clin Pract Rheumatol 3, 305.
International Journal of Rheumatic Diseases 2015; 18: 685–713 713
APLAR RA recommendations