can electronic medical records enable knowledge asset dynamics in hospitals? emerging strategies for...
TRANSCRIPT

1
Can Electronic Medical Records Enable Knowledge Asset Dynamics in Hospitals? Emerging Strategies for Effectively Balancing Knowledge Exploration and Knowledge Exploitation
Luca Gastaldi* Department of Management, Economics and Industrial Engineering Politecnico di Milano Via Lambruschi 4b, 20156 Milan (Italy) E-mail: [email protected]
* Corresponding author
Emanuele Lettieri Department of Management, Economics and Industrial Engineering Politecnico di Milano Via Lambruschi 4b, 20156 Milan (Italy) E-mail: [email protected]
Mariano Corso Department of Management, Economics and Industrial Engineering Politecnico di Milano Via Lambruschi 4b, 20156 Milan (Italy) E-mail: [email protected]
Cristina Masella Department of Management, Economics and Industrial Engineering Politecnico di Milano Via Lambruschi 4b, 20156 Milan (Italy) E-mail: [email protected]
Structured Abstract
Purpose — This study offers new insights to our understanding about how to solve the quest for systematically improving hospital performance by enhancing and balancing knowledge exploration and knowledge exploitation capabilities through the development of an EMR. Two research questions grounded the investigation. Which strategies and leverages are emerging in hospitals for improving their performances by unfolding EMR capability to advance both knowledge exploration and knowledge exploitation? Why the-se strategies and leverages have to be preferred to others?

2
Design/methodology/approach — This study has an interpretative, inductive perspective,
based on multiple and embedded case studies. Three large-sized Italian hospitals have been
considered on the basis of their strategies for improving healthcare performance through the
development of an EMR by leveraging on their knowledge exploration and knowledge ex-ploitation capabilities. The three hospitals are similar in terms of beds, employees, and ICT
budget, but they adopted distinct strategies for the development of their EMRs. Originality/value — Most of the literature on EMR is focused on the benefits, the barriers
and the determinants of the adoption of this ICT-based solution. Little is understood about
how healthcare practitioners can manage EMRs to ambidextrously combine knowledge ex-ploration and knowledge exploitation, and increase hospitals performance. This exploratory
research sheds a first light on the topic—identifying a set of actionable-oriented propositions
and three emergent strategies of EMR development. Practical implications — The paper provides healthcare practitioners with clear guide-lines to balance knowledge exploration and knowledge exploitation through the develop-ment of an EMR, and, thus, increase hospital performances—both in terms of cost reduc-tion as well as quality improvement. Keywords — Knowledge exploration, Knowledge exploitation, Healthcare, Information and Communication Technology (ICT), Electronic Medical Record (EMR) Paper type — Academic Research Paper 1 Introduction
Despite increasing investments (WHO, 2010), many change efforts within the healthcare
industry are neither sustainable nor successful (Agarwal et al., 2010). Most of the
healthcare systems are criticised as being poorly prepared to meet the changing needs of
their population (Finchman et al., 2011). Current limitations result in unexplained prac-
tice variation, gaps between evidence and practice, inequitable pattern of utilisation, poor
safety and unaffordable cost increases (Kopach-Konrad et al., 2007).
This set of challenges is increasingly forcing hospitals to leverage their knowledge as-
sets in order to increase their performance (Ford and Angermeier, 2004; Peng et al.,
2007). More specifically, knowledge management research (Oshri et al., 2004; Durcikova
et al., 2011; Schiuma, 2011) suggests that the capacity of an hospital to create sustainable
organizational value resides not only in the ownership of knowledge assets guaranteeing
the present competitive advantage (knowledge exploitation), but also in the ability to un-
derstand and govern the continuous development of knowledge assets necessary to renew
its organizational capabilities (knowledge exploration).

3
From this viewpoint, scholars (Deveraj and Kohli, 2003; Kane and Alavi, 2007; Corso
et al., 2009; Joshi et al., 2010) are increasingly recognizing the role that Information and
Communication Technologies (ICTs) might play. ICTs are critical not only for supporting
knowledge management initiatives and nurturing innovation (Alavi and Leidner, 2001;
Tantiverdi, 2005), but also to augment firms’ knowledge capabilities (Sambamurthy and
Subramani, 2005; Davenport et al., 2008) and offer opportunities to conciliate the capa-
bility to exploit the current knowledge with the capability to explore new and better ways
of creating knowledge (Joshi et al., 2010). The end result is an overall improvement in
both cost rationalisation and quality enhancement (Mithas et al., 2011).
Electronic Medical Record (EMR) has emerged as one of the most promising ICT-
based solutions to unfold this potential within the healthcare domain (Jha et al., 2006). An
EMR is a digital repository of patient data that is shareable within a hospital (Jha et al.,
2009). Typical EMR systems incorporate features such as a clinical data repository, com-
puterised patient records, decision support applications, integration with other systems,
and transaction processing capabilities (Angst et al., 2010). Although there is a growing
awareness of the potential benefits associated with EMRs (Bates et al., 2003), results are often
well under expectations (Simon et al., 2007). As a matter of fact, most of hospitals:
• Continues to barely give EMR (as well as to other ICT-based solutions) a second thought
as a source of innovation (Simon et al., 2007; Brynjolfsson and Saunders, 2009); and
• Does not adequately analyse the organizational changes required to make all the bene-
fits associated to EMR become a reality (Bates et al., 2003; Adler-Milstein, 2009).
Thus, instead of being considered strategic resources, EMRs are often simply con-
fused with other healthcare technologies (Chaudry et al., 2006), and generalized as one of
the drivers in the rising of healthcare costs (Hartley and Jones, 2005; Corso et al., 2010).
In fact, the results of their development are tremendously variable (Angst el al., 2010),
and hospital managers are still debating which EMR development strategies might be pre-
ferred to achieve an effective balance between knowledge exploration and knowledge ex-
ploitation (IHCO, 2009; Angst et al., 2010). Literature, in fact, does not provide them
with a clear guidance, since previous contributions on EMR focused on benefits (Bates et
al., 2003), barriers (Simon et al., 2007), and determinants of adoption (Miller and Tucker,
2009). Very little is known about how EMR is developed, and how this development
might contribute in increasing both knowledge exploration and knowledge exploitation
capabilities, and, thus, in improving healthcare performance.
4
2 Research Questions and Methodology
Based on this background, this study offers new insights to our understanding about how
to solve the quest for systematically improving healthcare performance by enhancing and
balancing knowledge exploration and knowledge exploitation capabilities through the de-
velopment of an EMR. Two research questions grounded the investigation:
• RQ1: Which strategies and leverages are emerging in hospitals for improving their
performances by unfolding EMR capability to advance both knowledge exploration
and knowledge exploitation?
• RQ2: Why these strategies and leverages have to be preferred to others?
In order to answer to these questions, an interpretative, inductive perspective (Eisen-
hardt, 1989b), based on multiple and embedded case studies (Eisenhardt, 1989a), has
been considered appropriated. The interpretative, inductive perspective is useful because
the research questions aim to better understand the complex knowledge-assets dynamics
underlying EMR development—retaining «the holistic and meaningful characteristics of
real-life events» (Yin, 2003). The paper relies on multiple case studies because they tend
to yield to more generalizable, robust, parsimonious results than single cases (Eisenhardt
and Graebner, 2007). The embedded unit of analysis has been selected not only to better
measure the performance of the EMR implementation strategy, but also to diminish the
probabilities of conducting the research at an abstract level (Martin and Eisenhardt, 2010).
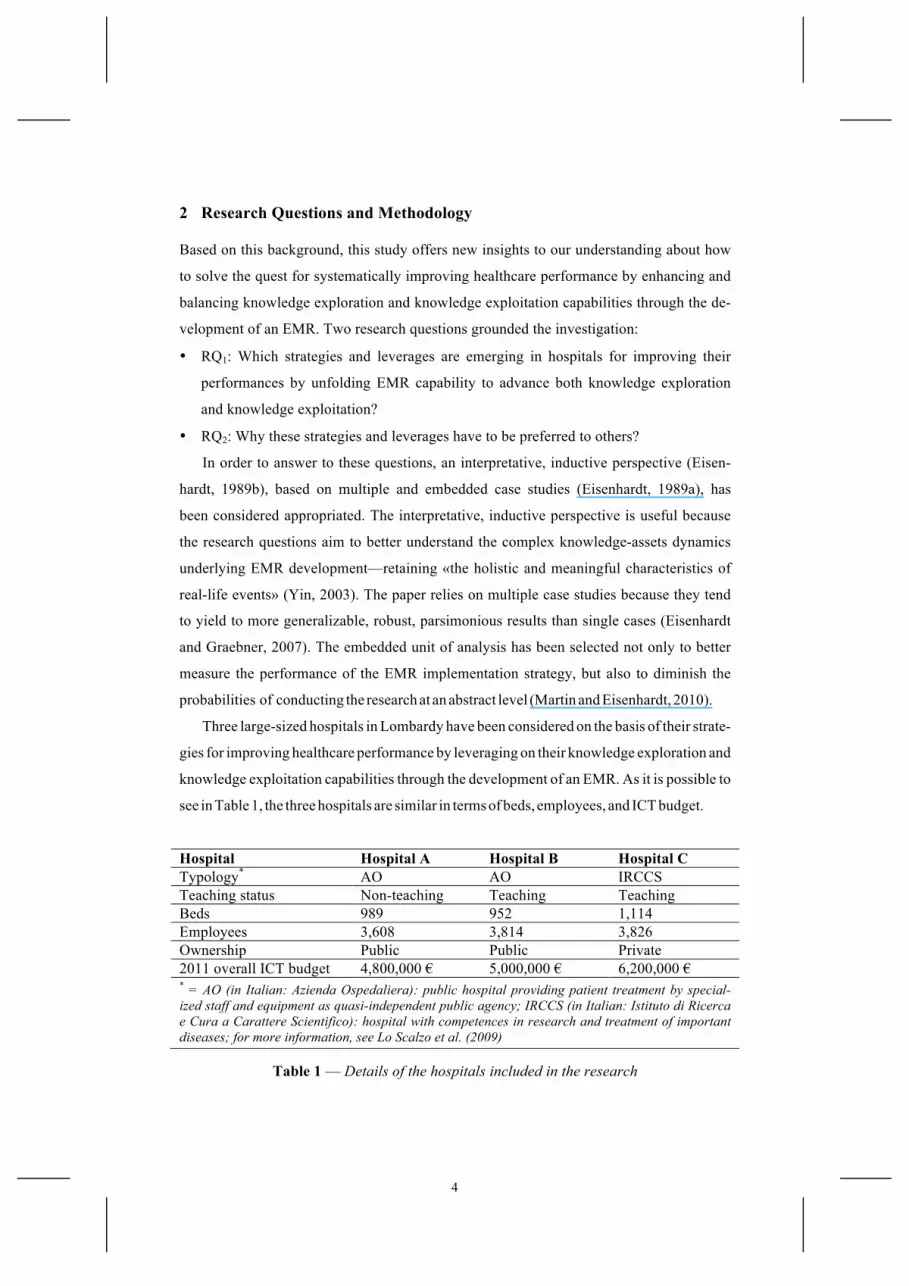
Three large-sized hospitals in Lombardy have been considered on the basis of their strate-
gies for improving healthcare performance by leveraging on their knowledge exploration and
knowledge exploitation capabilities through the development of an EMR. As it is possible to
see in Table 1, the three hospitals are similar in terms of beds, employees, and ICT budget.
Hospital Hospital A Hospital B Hospital C Typology* AO AO IRCCS Teaching status Non-teaching Teaching Teaching Beds 989 952 1,114 Employees 3,608 3,814 3,826 Ownership Public Public Private 2011 overall ICT budget 4,800,000 € 5,000,000 € 6,200,000 €
* = AO (in Italian: Azienda Ospedaliera): public hospital providing patient treatment by special-ized staff and equipment as quasi-independent public agency; IRCCS (in Italian: Istituto di Ricerca e Cura a Carattere Scientifico): hospital with competences in research and treatment of important diseases; for more information, see Lo Scalzo et al. (2009)
Table 1 — Details of the hospitals included in the research
5
According to Yin (2003), a major step in designing and conducting a case-based re-
search is defining the unit of analysis (or the case itself). Starting from the research ques-
tions, as well as from the analysis of the literature, the focus on EMR innovation process
as a first unit of analysis was chosen. By «EMR innovation process» the paper means the
set of activities and users involved in the adoption, the usage and the improvement of an
EMR. This unit of analysis provides a privileged viewpoint to understand the support de-
livered to the exploratory and exploitatory activities of the hospital.
In order to improve the likelihood of rich, accurate theory (Martin and Eisenhardt,
2010) we considered the hospital as a second unit of analysis, and the Lombardy
healthcare system as the context in which to perform the cases (Yin, 2003)1.
As suggested by literature (e.g. Martin and Eisenhardt, 2010), the research relied on sev-
eral data sources: face-to-face interviews, phone conversations, follow-up emails, and ar-
chival data such as internal documents, press releases, websites, and news articles. In order to
maximise the benefits from these sources of evidence, and better deal with the construct valid-
ity and reliability issues, two recommendations suggested by Yin (2003) have been followed:
the triangulation of data sources (Jick, 1979; Anand et al., 2007), and their organisation in an
electronic and navigable case study database (Miles and Huberman, 1994; Darke et al., 1998).
The primary data source is composed of 27 semi-structured interviews conducted over
three years with the Chief Information Officers (CIOs), at least one of the other C-levels2,
and—through a snowball technique (Patton, 2002)—other knowledgeable informants in-
volved in the EMR innovation process. Within each firm, the authors continued recruiting
informants until additional interviews failed to dispute existing, or reveal new, categories
or relationships—that is, until theoretical saturation (Strauss and Corbin, 1990) was
achieved. Table 2 summarises the informants involved into the research.
The interviews have been designed on a common protocol that evolved systematically
during the research. A key advantage of the study is its three waves of longitudinal data
collection (Glaser and Strauss 1967; Ozcan and Eisenhardt, 2009). In the first wave a fo-
cus has been put on the different ICT-based solutions present inside the hospitals. The
main information achieved are synthesised in Table 4. In the second and in the third
1 Italy’s healthcare system is a regionally-based national health care service. Lombardy is the most populous and richest region in the country, and its regional healthcare system is considered the most efficient and effective in delivering treatments and healthcare services (Lo Scalzo et al., 2009). The Lombard context is particularly ap-propriate to study EMR development and adoption because Lombardy is the Italian region investing more in ICT-driven innovation (Lo Scalzo et al., 2009). 2 The Chief Executive Officer (CEO), the Chief Financial Officer (CFO) and the Chief Medical Officer (CMO).

6
waves of interviews a focus has been put on the knowledge assets strategies followed in
each hospital, and—as data collection and analysis unfolded—the interviews became in-
creasingly focused (Andriopoulos and Lewis, 2009) on the activities and the users involved in
the adoption, the usage and the improvement of their EMR.
Hospital Hospital A Hospital B Hospital C Total Number of interviews* 8 10 9 27 Interviews to the CIO 3 4 3 12 Interviews to the CEO 2 2 3 7 Interviews to the CFO 1 2 3 Interviews to the CMO 1 1 2 Interviews to physicians and/or nurses 2 2 1 5
* = Each interview lasted approximately 1.5 hours
Table 2 — Informants involved into the research
Potential informant bias has been addressed in several ways. First, the interviews col-
lected both real-time and retrospective longitudinal data in several waves over three
years. According to Ozcan and Eisenhardt (2009) this kind of data collection is ideal be-
cause retrospective data enable efficient collection of more observations (thus enabling
better grounding), while real-time data mitigate retrospective bias (Leonard-Barton,
1990). Second, anonymity has been promised to companies and informants. According to
Eisenhardt (1989a; 1989b) this decision encourages candour. Third, the interviews have
been complemented with wide-ranging archival and observational data, as suggested by
Bingham and Eisenhardt (2011). Fourth, open-ended questioning has been used to give
the informants wide scope to relate the concept as they chose. According to Koriat and
Goldsmith (2000) this helps in addressing potential informant bias. Fifth, informants not
only from multiple levels of hierarchy, but also with different perspectives have been
considered during the interviews. If one considers that these informants were also highly
interested in the solution under exam, the accuracy of the interpretations increases (Ku-
mar et al., 1993; Ozcan and Eisenhardt, 2009). Finally, interview techniques like court-
room questioning, event tracking, and nondirective questioning (Martin and Eisenhardt,
2010) have been used to yield accurate information (Eisenhardt, 1989a; 1989b).
Following recommendations for multiple case theory building (Eisenhardt, 1989b; Eisen-
hardt and Graebner, 2007), within- and cross-case analyses have been performed with no a pri-
7
ori hypotheses. The corresponding author built a first draft of individual write-ups that triangu-
lated all of the data to emphasize themes that were supported by different data collection meth-
ods and confirmed by several informants (Jick, 1979). The other authors integrated the first
draft with their comments, and highlighted missing details that have been successively filled
with calls and emails (Ozcan and Eisenhardt, 2009). Once the write-ups were consolidated,
each author read them to form an independent view (Yin, 2003) and develop preliminary con-
cepts and rough theoretical explanations (Bingham and Eisenhardt, 2011). Finally, a cross-
case analysis has been done—using replication logic across the cases—to probe for alterna-
tive theoretical relationships and constructs that might fit the data better than the initial emer-
gent theory (Gilbert, 2005). Tables and other cell designs have been used to compare several
possible constructs at once (Miles and Huberman, 1994). From the emerging constructs and
themes, tentative relationships between constructs were formed. Then these initial relation-
ships were refined via replication logic—frequently revising each case to compare and verify
occurrence of specific construct, relationships, and logics (Ozcan and Eisenhardt, 2009).
Once the cross-case analysis was underway, the researchers cycled among the emergent
theory, case data, and literature to refine further the emerging construct definitions, abstrac-
tion levels, construct measures, and theoretical relationships (Eisenhardt, 1989a; Gilbert,
2005). The cycles continued until a strong match between the cases and the emergent theory
was achieved (Ozcan and Eisenhardt, 2009). To converge on a parsimonious set of constructs,
the researchers focused only on the most robust findings (Andriopoulos and Lewis, 2009),
asking the informants of the three hospitals to review them in order to solve discrepancies.
3 Findings
The findings are organised in three sections. The first one analyses if EMR can be con-
sidered trigger and an enabler of improved knowledge assets dynamics in hospitals. The
second one outlines three strategies for making EMR able to impact knowledge assets
dynamics. The last one considers the efforts that a hospital has to put out in overcoming
the dichotomy between knowledge exploration and knowledge exploitation.
3.1 EMR as Trigger and Enabler of Improved Knowledge Assets Dynamics
Knowledge assets dynamics are conducive of performance improvement (Schiuma, 2011).
This outcome requires an organisation to overcome the dichotomy between knowledge ex-
ploration and knowledge exploitation (e.g. Bierly and Daly, 2007; Cegarra-Navarro and

8
Dewhurst, 2007) by ambidextrously combining (i) search, variation, risk-taking, experimen-
tation, play, flexibility, discovery and innovation on the one hand, with (ii) refinement,
choice, production, efficiency, selection, implementation and execution on the other.
Durcikova et al. (2011) argue that this ambidextrous capability can lead to better organisa-
tional performances. The reason is that the organisation maintains a paradoxical focus on both
current (knowledge exploitatory efforts) as well as future (knowledge exploratory efforts)
processes of value generation—going through positive reinforcing cycles (Lewis, 2000) that
progressively solve the multiple and interrelated tensions underlying the divergence present
not only between knowledge exploration and knowledge exploitation (Andriopoulos and
Lewis, 2009; 2010), but also between the related outcomes of cost reduction and quality im-
provement (Smith and Lewis, 2011; Agarwal et al., 2010; Corso and Gastaldi, 2010).
A first element emerging from all the three cases is that—focusing on producing, finding,
analysing and sharing information through digital media (Freeman, 2007)—EMR manifests
its ambidextrous potential in triggering and enabling augmented capabilities in knowledge
exploration and knowledge exploitation by increasing the coordination among hospital
processes. For instance, the CEO of hospital A stated that: «I’ve always thought at ICT as
a lever to cut costs. As a matter of fact, there are tremendous benefits also in terms of
quality improvement: once you connect the different departments, you discover new and
better ways to provide healthcare services and have an impact on patients’ outcome».
The literature about paradoxical thinking provides three reasons supporting this claim.
First, the more the clinical processes within a hospital are coordinated through an EMR,
the easier the discovery of the specific underlying tensions explaining the dichotomy between
knowledge exploration and knowledge exploitation. In fact, there are many interrelated ten-
sions causing knowledge exploration and knowledge exploitation to diverge (Andriopolous
and Lewis, 2009), and one of the key issues that a hospital faces is the identification and the
representations of these tensions (Lewis, 2000). The fact that the tensions are entangled with
organisational processes (Smith and Lewis, 2011) makes the latter a central component for
rendering each tension as salient. As a consequence, the more the hospital processes are coor-
dinated, the more opportunities are made available for the identification and the representa-
tion of the intricate set of tensions explaining the dichotomy between knowledge exploration
and knowledge exploitation, and, ultimately, to the effective utilisation of knowledge assets.
The cases show that by leveraging on process coordination, EMR increases the possibilities to
effectively balance knowledge exploration and knowledge exploitation.

9
The second reason is linked to the first one. The more EMR connects hospital processes,
the more hospital has opportunities to develop and experience the capabilities to address the
paradoxical nature of knowledge exploration and knowledge exploitation (Andriopoulos and
Lewis, 2009). For example, in hospitals A and C the coordination of the clinical processes re-
alised through the EMR has allowed to connect Radiology and the Laboratory departments,
with the end results of quicker as well as better diagnoses that, before the development of the
EMR, were considered impossible to be performed. Moreover, the more the processes are co-
ordinated, the quicker the latent tensions derived by the inertial forces expressed by hospital’s
employees are rendered salient. In other terms, process coordination accelerates the speed of
the reinforcing cycles through which the tensions among knowledge exploration and
knowledge exploitation are progressively solved within the hospital. For instance, at the end
of the development of the EMR, the CMO of hospital C registered «a reduction in the time to
achieve a complete effective diagnosis by roughly a 30%».
Finally, process coordination favours both the differentiation (e.g. Lavie et al., 2011) as
well as integration (e.g. Eisenhardt et al., 2010) approaches used to overcome the dichotomy
between knowledge exploration and knowledge exploitation. In fact, the former and the latter
highly benefit from the coordination among organisational processes. On the one hand, de-
veloping separate contexts for knowledge exploration and knowledge exploitation, differen-
tiation approaches necessitate a recombination and a synthesis of the dichotomous efforts,
which are sped up by the ICT-driven process coordination realised through the EMR. For ex-
ample, hospital B has started the development of its EMR by digitalising all the processes of
its paediatric intensive care department. While new diagnoses were explored within this de-
partment, the other healthcare units continued to exploit their traditional ways of diagnose.
Once process digitalisation was accomplished within the paediatric intensive care, the exten-
sion of the relative benefits to the rest of the hospital has been simplified by the presence of a
digital backbone connecting the healthcare units. On the other hand, the effectiveness of inte-
gration approaches is linked to their pervasiveness, which in turn can be enhanced through a
stronger coordination among hospital processes, and, thus, through the development of an
EMR. For example, the cross-unit collaboration on clinical pathways that has been spontane-
ously developed by the healthcare units of hospital A was fostered by the digital integration of
inter-departmental processes realised through the EMR.
In all hospitals the EMR has enabled better knowledge assets dynamics, which have al-
lowed to: (i) improve the overall organisational capabilities to explore and exploit, (ii) better

10
balance knowledge exploration and knowledge exploitation at different levels (mainly the
departments and the whole hospital), and (iii) achieve better performances in terms of both cost
rationalisation and quality improvement. This evidence leads to the following proposition:
Proposition 1A: The ICT-driven coordination of the processes of the
healthcare units realised through the development of an EMR positively
affects the capability of a hospital to effectively overcome the dichotomy
between knowledge exploration and knowledge exploitation.
The cross-case analysis showed that the level of digitalisation previously accomplished
by the hospital is a key factor in explaining EMR effectiveness. In fact, all the three hospitals
had high percentages (higher than 40%) of clinical documentation already digitalised when
they started the implementation of their EMR. The CIO of hospital C remarked that EMR is
«a natural prerequisite that simply the current evolution of information systems makes im-
possible to avoid». All informants agreed on the fact that EMR is, in fact, the natural “next
step” to be accomplished after having digitalised most of hospital units. Experienced the
actual benefits of the digital integration among the resources within a generic healthcare
unit (e.g. the better diagnoses provided thanks to the digital connection of computer to-
mography and a magnetic resonance imaging devices in the radiology department), the
basic idea, followed by the three hospitals, is trying to achieve these benefits at an organi-
sational level as well—through the integration of the processes transversal the different
units. In the words of the CEO of hospital A: «We’re simply doing what we have done
within each department; but on a bigger scale. Information has to be available ubiqui-
tously to actually achieve all the benefits associated to ICT». Overall, it is thus possible to
complement the previous proposition with the following one:
Proposition 1B: The level of digitalisation accomplished within the main
hospital units moderates the capability of EMR to effectively overcome the
dichotomy between knowledge exploration and knowledge exploration.
3.2 Strategies for Making EMR Able to Impact Knowledge Assets Dynamics
One of the greatest limits of the current literature on EMRs resides in the lack of actionable
knowledge explaining how these ICT-based solutions can be adopted, used and improved
(Jha et al., 2009). Recently, Angst et al. (2010) have analysed the diffusion of EMR. However,
their «social contagion» lens does not provide actionable knowledge for the practitioners aim-

11
ing to develop this ICT-based solution, but only interesting implications for the policy makers
who want to increase the EMR adoption rate among the hospitals in a given region or country.
This study offers a complementary perspective—starting to focus on the strategies
that healthcare CIOs can follow in order to introduce an EMR. Table 8, Table 9 and Table
10 summarise the main findings achieved from this point of view. For each case, the
tables report: (i) the stimuli that have led to the decision of investing in an EMR solution,
(ii) the problems faced during its adoption, (iii) the impacts produced on knowledge ex-
ploration, knowledge exploitation and on the performances of the health care organisa-
tion, (iv) the approaches used to balance the knowledge exploratory and the knowledge
exploitatory activities related to (or enabled by) the EMR, (v) the challenges and the is-
sues faced during its usage and/or improvement, (vi) the next steps to be accomplished
according to the informants interviewed, and (vii) some of their quotes that are repre-
sentative of the elements depicted in the tables. To complement the analysis, it is useful to
refer to Table 5 for an overview of the other ICT-based solutions already present in the
three analysed hospitals when they have decided to start the development of their EMR.
The cross-analysis of the cases has highlighted the presence of multiple strategies to de-
velop an EMR, and multiple combinations of knowledge exploration and knowledge exploi-
tation characterising these strategies. In fact, an evidence that has strongly emerged from all
the cases is that, rather than a whole standalone project of EMR development, it is more com-
mon to proceed with a combination of knowledge exploratory and knowledge exploitatory
investments—realised through both radical and incremental innovations.
Interestingly, in all the three cases the stimuli that led to invest in the EMR are similar, and
refer to the desire of (i) improving the effectiveness of the clinical processes, (ii) reducing their
inefficiency, and (iii) effectively responding to external pressures related to the development
of an Electronic Health Record (EHR)1. These objectives have different relative relevance in
the three cases because of peculiar contextual conditions surrounding the development of the
EMRs, and tend to be reached after at least three years of progressive ICT-based integration.
If the first noticeable effects on hospital performance are produced after consistent time
lags, initially the focus is put on what the CIO of hospital B has called «protected niches»: de-
partments and/or EMR functionalities mostly detached by the core services offered by the
hospital, in which progressively experiment the ICT-based process integration potential of
the EMR. These protected niches allow not only to «achieve in short time lags tangible results
1 An EHR is a network information system embedding the EMRs of different healthcare organisations.

12
to be shown to both the strategic board as well as to the users, but also to avoid the over-
complications associated to the development of a pervasive solution such as the EMR—at
least in the initial stages of its development» (CIO of hospital A). Moreover, the remain of the
hospital can continue along its paths to overcome the dichotomy between knowledge explora-
tion and knowledge exploitation—making their ambidextrous balance easily achievable. The
aforementioned decision of hospital B to start the development of its EMR in the paediatric in-
tensive care department is oriented in reducing the initial interdependencies among the pro-
cesses to be integrated and the processes that are adopted in other departments to effectively
leverage on knowledge assets. Similarly, hospital A has focused on a specific EMR function-
ality, namely therapy management, in order to initially concentrate its efforts on a set of inter-
departmental processes which ICT-based integration is not particularly critical in the delivery
of healthcare service. Overall, the following proposition is suggested:
Proposition 2A: The first effective investments in the development of an
EMR support intra- or inter-departmental integration among the pro-
cesses of protected functional niches.
According the informants, the integration of clinical processes (e.g. the management of
the admissions, demission and transfer activities in hospital B) brings higher possibilities to
leverage on knowledge assets than the integration of administrative processes (e.g. the man-
agement of the informal consent in hospital B). This explains why, during the initial phases of
EMR development, CIOs tend to focus on clinical processes rather than administrative pro-
cesses. If all the informants underlined the higher value associated to the integration of the
former in comparison to the latter, they have also emphasised the higher difficulties in ac-
complishing the integration of clinical processes due both to their pervasiveness as well as to
their centrality in the creation of value for the hospital. In fact, all the analysed hospital have
accomplished administrative integration to collect what informants have called «quick wins»
between large waves of clinical integration. In the words of the CFO of hospital C: «The bene-
fits of an EMR are undoubtedly present. However they’re diluted throughout the entire hospi-
tal. Sometimes it’s better to focus on administrative processes. They won’t save lives, but their
automation provides quick wins». Overall, the following proposition is proposed:
Proposition 2B: The integration of clinical processes is more likely to al-
low EMR to effectively balance knowledge exploration and knowledge
exploitation than the integration of administrative processes.
13
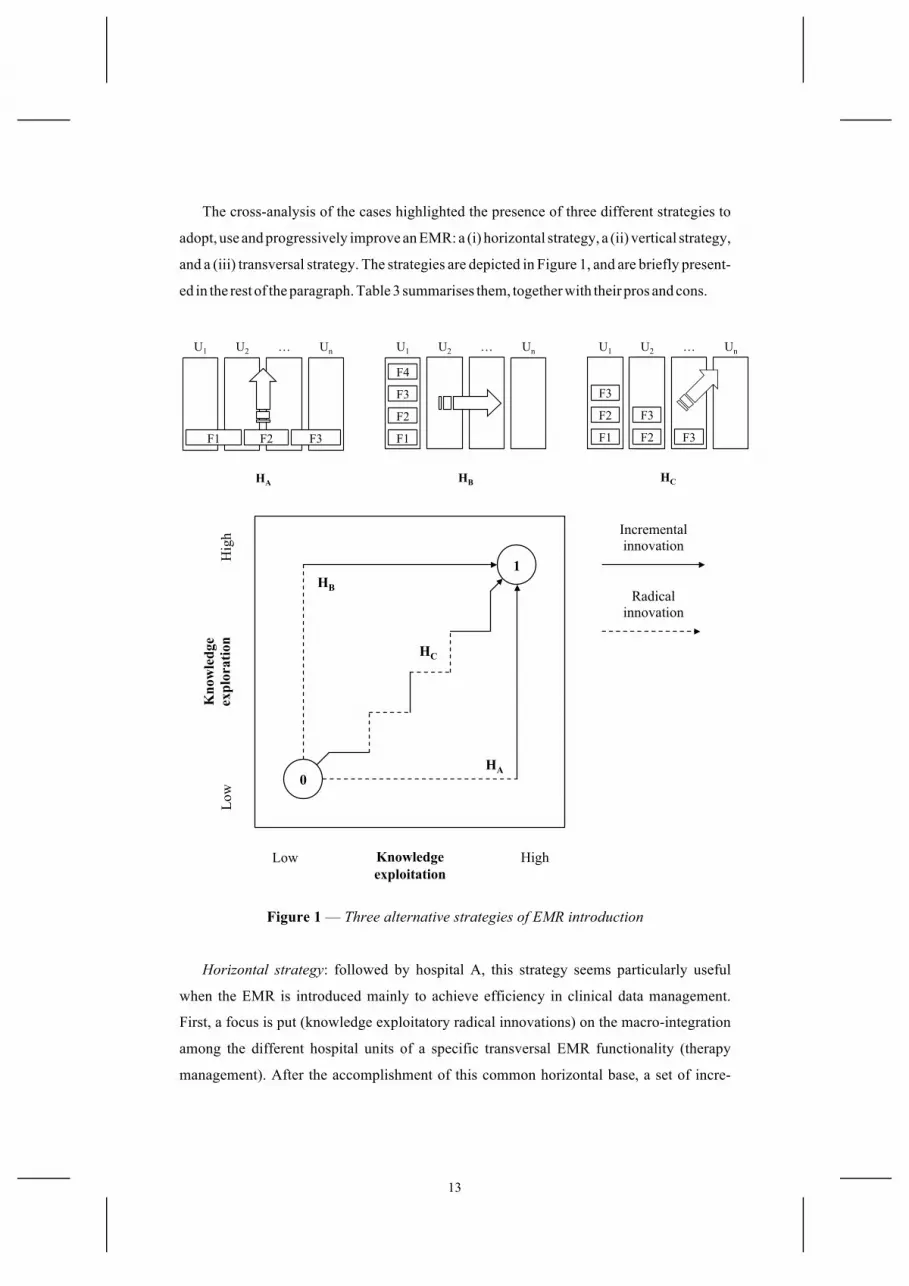
The cross-analysis of the cases highlighted the presence of three different strategies to
adopt, use and progressively improve an EMR: a (i) horizontal strategy, a (ii) vertical strategy,
and a (iii) transversal strategy. The strategies are depicted in Figure 1, and are briefly present-
ed in the rest of the paragraph. Table 3 summarises them, together with their pros and cons.
Figure 1 — Three alternative strategies of EMR introduction
Horizontal strategy: followed by hospital A, this strategy seems particularly useful
when the EMR is introduced mainly to achieve efficiency in clinical data management.
First, a focus is put (knowledge exploitatory radical innovations) on the macro-integration
among the different hospital units of a specific transversal EMR functionality (therapy
management). After the accomplishment of this common horizontal base, a set of incre-
HB HA HC
U2
F3
F2
U1
F3
F2
F1
Un …
F3
U2 U1 Un …
F2 F1 F3
U2 U1
F4
F3
F2
F1
Un …
Radical innovation
Incremental innovation
HB
HA
HC
0
1
Knowledge exploitation
Kno
wle
dge
ex
plor
atio
n
High
Low
Hig
h
Low

14
mental projects in each hospital unit is accomplished to explore new and better ways of
using the shared data. Then, the hospital focuses on a new functionality—the one relative
to the management of outpatients—and the cycle starts over from the macro-integration
of the relative processes. This typology of EMR introduction tends to privilege system in-
tegration to the meeting of physician customisation requirements.
Vertical strategy: followed by hospital B, this strategy seems particularly useful when
the EMR is introduced mainly to achieve effectiveness in clinical data management. The
focus is put on one hospital unit at a time (paediatric intensive care, cardiology, neurolo-
gy, oncology, emergency department, etc.)—exploring radical new and better ways to de-
liver its services through the ICT-based integration of its processes. After the accom-
plishment of this phase, the benefits achieved (new diagnoses and/or treatments) are
shared with the other hospital units through a set of knowledge exploitation incremental
projects. Then, the hospital focuses on another unit, and the cycle starts over from the in-
tegration of its processes. This typology of EMR introduction tends to privilege the meet-
ing of physician customisation requirements to system integration.
Transversal strategy: followed by hospital C, this strategy seems particularly useful when
the EMR is introduced to simultaneously achieve effectiveness and efficiency in clinical data
management. To combine these objectives, knowledge exploratory and knowledge exploita-
tory investments are alternated, and each time a focus is put on the most critical hospital units
(e.g. the emergency department) and/or EMR functionalities (e.g. in the diagnostic area).
Through a combination of incremental and radical innovations, the “integrated base” is pro-
gressively enlarged to more hospital units (the laboratory, the radiology department, etc.)
and EMR functionalities (e.g. therapy management, outpatient management, etc.). This ty-
pology of EMR introduction tends to balance physician customisation requirements with sys-
tem integration, by also to request high levels of organisational engagement (especially in the
strategic board), economical resources, and project management capabilities.
3.3 Innovation Stickiness in Leveraging on Knowledge Assets
A last set of considerations deals with the efforts that a hospital has to put out in over-
coming the dichotomy between knowledge exploration and knowledge exploitation. The
literature (Smith and Lewis, 2011) suggests that the progressive rendering of the underly-
ing tensions between knowledge exploration and knowledge exploitation provides oppor-
tunities to tackle deeper interrelated tensions—otherwise latent or not yet present—which
are more difficult to be solved (Smith and Lewis, 2011; Boumgarden et al., 2012).

15
Path Horizontal Vertical Transversal
Step 1
Macro-integration among inter-departmental processes (knowledge exploitatory radical innovation)
Integration of the intra-departmental process-es—one dept. at a time (knowledge exploratory radical innovation)
Alternate knowledge exploratory and knowledge exploitatory investments, focusing on the most critical depts. and functionalities
Step 2
Management of a set of projects in each unit to use the shared data (knowledge exploratory incremental innovation)
Extension of the achieved benefits to the other departments. with the integration of inter-departmental processes (knowledge exploitatory incremental innovation)
Progressive enlargement
of the operational base to more functionalities and departments (combinations of incremental and radical innovations)
Pros System integration
Physicians acceptance
System integration and physicians acceptance
Cons Physicians resistance
“Patchwork” development
Strong efforts and financial exposition
Table 3 — The three strategies to develop EMR emerged from the cases
In fact, organisations emerge as leaders respond to foundational questions—
constructing boundaries that foster distinctions and dichotomies (Ford and Backoff,
1988). These tensions, emanated through the act of strategizing, persist entangled in the
organisational processes because of the complex and adaptive nature of knowledge and or-
ganisational systems (Cyert and March, 1963), and becomes progressively interrelated and
difficulty solvable (Lewis, 2000; Andriopoulos and Lewis, 2009).
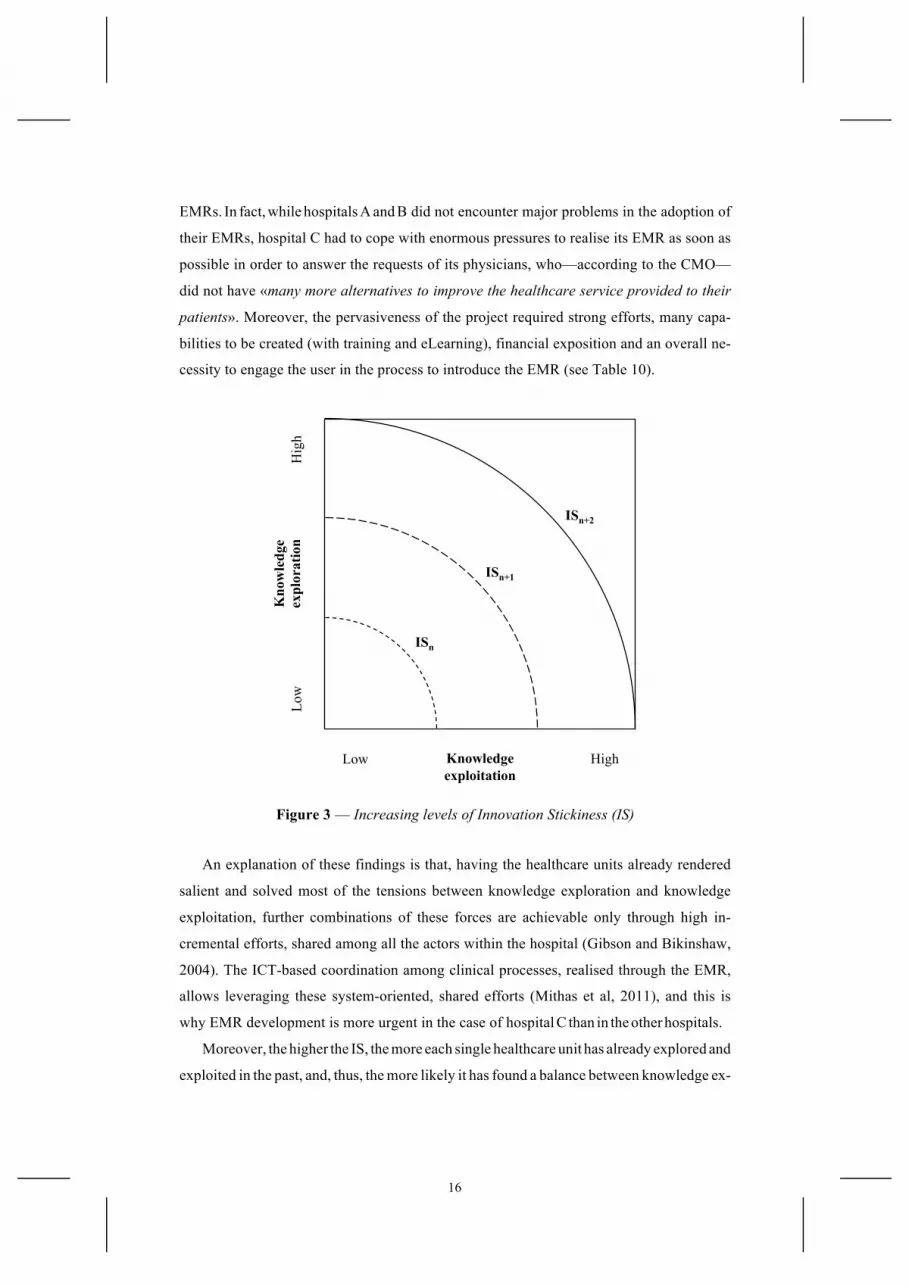
To generalise this idea it is possible to introduce the concept of Innovation Stickiness (IS).
As depicted in Figure 3, IS represents the incremental efforts to render salient and solve the ten-
sions between knowledge exploration and knowledge exploitation. When IS is low (ISn), the
opportunities to overcome the dichotomy between knowledge exploration and knowledge ex-
ploitation are greater. When IS increases (ISn+1 and ISn+2), further effective combinations of
knowledge exploration and knowledge exploitation are not easily achievable.
With respect to the case analysed, hospital C has showed a high level of IS. As de-
scribed by Lo Scalzo et al. (2009), IRCCSs do not only have certified competences in the
research and the treatment of important diseases (operating at high levels of knowledge
exploration), but also a double control—by the regional healthcare council and the Italian
Ministry of Health—over their expenditures (high level of knowledge exploitation).
The comparison between hospital C and hospital A and B suggests that the higher the IS,
the more urgent and complex the investments in the ICT-based integration realised through
16
EMRs. In fact, while hospitals A and B did not encounter major problems in the adoption of
their EMRs, hospital C had to cope with enormous pressures to realise its EMR as soon as
possible in order to answer the requests of its physicians, who—according to the CMO—
did not have «many more alternatives to improve the healthcare service provided to their
patients». Moreover, the pervasiveness of the project required strong efforts, many capa-
bilities to be created (with training and eLearning), financial exposition and an overall ne-
cessity to engage the user in the process to introduce the EMR (see Table 10).
Figure 3 — Increasing levels of Innovation Stickiness (IS)
An explanation of these findings is that, having the healthcare units already rendered
salient and solved most of the tensions between knowledge exploration and knowledge
exploitation, further combinations of these forces are achievable only through high in-
cremental efforts, shared among all the actors within the hospital (Gibson and Bikinshaw,
2004). The ICT-based coordination among clinical processes, realised through the EMR,
allows leveraging these system-oriented, shared efforts (Mithas et al, 2011), and this is
why EMR development is more urgent in the case of hospital C than in the other hospitals.
Moreover, the higher the IS, the more each single healthcare unit has already explored and
exploited in the past, and, thus, the more likely it has found a balance between knowledge ex-
Knowledge exploitation
Kno
wle
dge
ex
plor
atio
n
High
Low
Hig
h
Low
ISn
ISn+1
ISn+2

17
ploration and knowledge exploitation. In the words of the CEO of hospital C: «The ICT-
driven integration forces the unit to reconsider [this balance]—altering equilibriums devel-
oped in, and maintained through years of experience». This is why the ICT-based integration
realised through the EMR is more complex. This summary suggests that:
Proposition 3: The higher the IS, the more urgent and complex the ICT-
based coordination of the clinical processes realised through the devel-
opment of an EMR within a hospital.
In other terms, a hospital has to invest in the development of an EMR as soon as possible.
In fact, the higher the exploration and the exploitation already performed on knowledge as-
sets, the higher the IS, and, thus, the more urgent but also complex the accomplishment of any
of the three strategies outlined in the previous paragraph. On the other side, the sooner the
strategy is implemented, the weaker the pressures that will be perceived during the implemen-
tation of an EMR, and the simpler the processes through which this ICT-based solution will al-
low to overcome the dichotomy between knowledge exploration and knowledge exploitation.
4 Conclusions
Knowledge assets are relevant for improving the performance in hospitals since
healthcare is a knowledge-intensive industry, and hospital professionals have to systemat-
ically leverage on their and on others’ knowledge in order to design and implement al-
ways different and personalized pathways of care. EMR is a solution that, if well man-
aged within a hospital, allows not only the exploitation of current knowledge and the ex-
ploration of new knowledge, but also the achievement of tangible improvements in hospi-
tal performance. However, the results of EMR development are tremendously variable,
and hospital managers experience pitfalls and shortcomings in their implementation.
This study offers new elements to further the ongoing debate about the capability of
EMR to enable knowledge assets dynamics—leading to more efficient and high-quality
healthcare services. In particular, Table 4 outlines the main contributions of the achieved
finding, which are relevant from a theoretical as well as an empirical viewpoint.
The results at this stage are still preliminary, and the results of the paper need to be
further refined. However, the work represents a good starting point to frame the potential
research that could be interesting to perform in the future. In fact, as the present work rep-

18
resents an exploratory research approach rather than a confirmatory or prescriptive one,
many of the findings and propositions that have been proposed can be further investigated
and developed in the future. Considering the listed so far, the remain of the paragraph fo-
cuses on the main limitations of the paper, to propose some further research develop-
ments that the author has already planned to accomplish.
Id Proposition Theoretical contribution
Empirical contribution
1
A. The ICT-driven coordination of the processes of the healthcare units realised through the development of an EMR positively affects the capability of a hospital to effectively overcome the dichotomy between knowledge exploration and exploitation
EMR allows to balance knowledge
exploration and knowledge exploitation
The balance between knowledge
exploration and knowledge
exploitation realised through the EMR allows to increase
hospital performance
B. The level of digitalisation accomplished within the main hospital units moderated the capability of EMR to effectively overcome the dichotomy between knowledge exploration and knowledge exploration
Boundary conditions moderate EMR effectiveness in
balancing knowledge exploration and
knowledge exploitation
EMR development has to start only after a specific maturity in the digitalisation of
hospital processes
2
A. The first effective investments in the development of an EMR support intra- or inter- departmental integration among the processes of protected functional niches
Outlined three alternative strategies for EMR development
Introduced a first preliminary description of the contingent elements affecting
the choice of one strategy over the others
B. The integration of clinical processes is more likely to allow EMR to effectively balance knowledge exploration and
knowledge exploitation than the integration of administrative processes
3
The higher the IS, the more urgent and complex the ICT-based coordination of the clinical processes realised through the development of an EMR within a hospital
Introduction of the IS construct
Hospitals have to invest in the devel-opment of an EMR as soon as possible
Table 4 — Theoretical and empirical contributions of the findings

19
The main problem of the findings achieved by this work concern their generalizabil-
ity. The focus on a specific lever (EMR), on a specific industry (healthcare) and on a spe-
cific context (Lombardy), combined with the extensive use of an interpretative study risk
to produce «very idiosyncratic phenomena» (Eisenhardt, 1989b)—difficultly generaliza-
ble to other context. There are two further developments already planned to be accom-
plished in order to fill this gap. First, it would be extremely useful to combine the inter-
pretative-oriented collaborative methodology used in this work with a more inductive and
quantitative-oriented set of vertical researches that could formally test the effectiveness of
the proposed contributions in all their details. The second one is a progressive extension
of the research context to the other healthcare systems—both Italian as well as Europe-
an—in order to test the effectiveness of the models and the propositions emerged during
the empirical analysis, and see how the considerations achieved change according to the
different contingent contexts of analysis tackled.
The second main limitation is related to the operationalisation of the constructs. The
solution of the dichotomy between knowledge exploration and knowledge exploitation
necessitates of multidimensional concepts able to discern between knowledge exploratory
and knowledge exploitatory efforts. However, the cases have showed that is not so simple
to completely separate these forces. Each operationalisation has its pros and cons to be
taken into account, and there are still many biases affecting the results and their interpre-
tation. The further developments that have been planned, from this viewpoint, are mainly
related to the usage of variables that are: (i) independent by informants’ perceptions, (ii)
able to precisely measure the level of knowledge exploration and knowledge exploitation
accomplished within a healthcare unit and/or hospital, the performances achieved through
their ambidextrous balance, and the impact that ICT plays over the achieved results.
The third main limitation of this work concerns the issue of its locus of innovation.
The technology base of the healthcare industry is both complex and expanding, and the
sources of expertise are widely dispersed. According to Powel et al. (1996), in these con-
texts the locus of innovation is found in the network, rather than in individual firms. Fol-
lowing their perspective, many healthcare stakeholders have been only marginally con-
sidered by this study: the regions, the providers of ICT-based solutions, the physicians
working in primary care, and the patients—just to name the main ones. ICT-based solu-
tions such as EMRs are developed, maintained and innovated by a complex ecology of
multiple agents that share knowledge (as well as other resources) in often previously un-

20
known interaction paths (Anderson, 1999). If, as a result of this complex process, ICT-
driven innovations emerge almost unpredictably over considerable time periods—as vari-
ous agents in the ecology interact with and react to the actions of others—their govern-
ance is naturally characterized by a shared and multilevel nature (Dougherty and Dunne,
2011), which this paper has not explored in detail. In order to fill this gap further research
developments will place greater effort in understanding how to foster the necessary col-
laboration among many healthcare stakeholders over long and uncertain time periods,
while, at the same time, continuing to develop ICT-based solutions such as EMRs able to
respond to the specific necessities of the hospitals’ different lines of business.
5 References
Adler-Milstein, J. (2009) “Health Care Requires Big Changes to Complement New IT”, Harvard Business Review, Vol. 86, No. 4, p. 20.
Agarwal, R., Gao, G., DesRoches, C., and Jha, A.K. (2010) “The Digital Transformation of Healthcare”, Information Systems Research, Vol. 21, No. 4, pp. 796–809.
Alavi, M. and Leidner, D.E. (2001) “Knowledge Management and Knowledge Management Systems: Conceptual Foundations and Research Issues”, MIS Quarterly, Vol. 25, No. 1, pp. 107–136.
Anand, N., Gardner, H.K. and Morris, T. (2007) “Knowledge-based Innovation: Emergence and Embedding of New Practice Areas in Management Consulting Firms”, Academy of Manage-ment Journal, Vol. 50, No. 4, pp. 406–428.
Anderson, P. (1999) “Complexity Theory and Organization Science”, Organization Science, Vol. 10, No. 3, pp. 216–232.
Andriopoulos, C. and Lewis M.W. (2009) “Exploration-Exploitation Tensions and Organizational Ambidexterity”, Organization Science, Vol. 56, No. 8, pp. 1219–1241.
Andriopoulos, C. and Lewis, M.W (2010) “Managing Innovation Paradoxes: Ambidexterity Lessons
from Leading Product Design Companies”, Long Range Planning, Vol. 43, No. 1, pp. 104–122. Angst, C.M., Agarwal, R., Sambamurthy, V. and Kelly, K. (2010) “Social Contagion and Infor-
mation Technology Diffusion: The Adoption of Electronic Medical Records in U.S. Hospi-tals”, Management Science, Vol. 56, No. 8, pp. 1219–1241.
Bates, D., Ebell, M., Gotlieb, E., Zapp, J. and Mullins, H.C. (2003) “A Proposal for Electronic Medical Records in U.S. Primary Care”, Journal of American Medical Informatics Associa-tion, Vol. 10, No. 1, pp. 1–10.
Bingham, C.B. and Eisenhardt, K.M. (2011) “Rational Heuristics: The ‘Simple Rules’ that Strate-gist Learn from Process Experience”, Strategic Management Journal, Vol. 32, No. 13, pp. 1437–1464.
Boumgarden, P., Nicherson, J. and Zenger, T.R. (2012) “Sailing into the Wind: Exploring the Rela-tionships among Ambidexterity, Vacillation, and Organizational Performance”, Strategic Management Journal, Vol. 33, No. 6, pp. 587–610.
Brynjolfsson, E. and Saunders, A (2009) Wired for Innovation: How Information Technology is Reshaping the Economy, The MIT Press, London (UK).
Chaudry, B., Wang, J., Wu, S., Maglione, M., Mojica, W., Roth, E. Morton, S.C. and Shekelle, P.G. (2006) “Systematic Review: Impact of Health Information Technology on Quality, Efficiency, and Costs of Medical Care”, Annals of Internal Medicine, Vol. 144, No. 1, pp. E12–E22.

21
Corso, M. and Gastaldi, L. (2010) “Managing ICT-Driven Innovation to Overcome the Exploita-tion-Exploration Trade-Off: A Multiple and Collaborative Research Methodology in the Italian Health Care Industry”, 11th CINet Conference, Zürich (CH), Sep., 5–7, pp. 274–289.
Corso, M., Gastaldi, L. and Locatelli, P. (2010) “Enhancing the Diffusion of Electronic Medical Record and Electronic Health Record: Evidence from an Empirical Study in Italy”, 16th Con-gress of International Federation of Health Records Organizations (IFHRO) “Better Infor-mation for Better Health”, Milan (IT), November, 15–19, pp. 1–4.
Corso, M., Martini, A. and Pellegrini, A. (2009) “Innovation at the Intersection Between Explora-tion, Exploitation and Discontinuity”, International Journal of Learning and Intellectual Capi-tal, Vol. 6, No. 4, pp. 324–340.
Cyert, R.M. and March, J.G. (1963) A Behavioral Theory of the Firm, Prentice-Hall, Englewood-Cliffs (NJ).
Darke, P., Shanks, G. and Broadbent, M. (1998) “Successful Completing Case Study Research: Combining Rigour, Relevance and Pragmatism”, Information Systems Journal, Vol. 8, No. 4, pp. 273–289.
Davenport, T.H., Prusak L., Strong B. (2008) “Putting Ideas to Work: Knowledge Management Can Make a Difference—But It Needs to Be More Pragmatic”, MIT Sloan Management Review, Vol. 47, No. 3, pp. 1–12.
Deveraj, S. and Kohli, R. (2003) “Performance Impacts of Information Technology: Is Actual Us-age the Missing Link?”, Management Science, Vol. 16, No. 4, pp. 273–289.
Dougherty, D. and Dunne, D.D. (2011) “Organizing Ecologies of Complex Innovation”, Organiza-tion Science, Vol. 22, No. 5, pp. 1214–1223.
Durcikova, A., Fadel, K.J., Butler, B.S. and Galletta, D.F. (2011) “Knowledge Exploration and Ex-ploitation: The Impacts of Psychological Climate and Knowledge Management System Ac-cess”, Information Systems Research, Vol. 22, No. 4, pp. 855–866.
Eisenhardt, K.M. (1989a) “Building Theory from Case Study Research”, Academy of Management Review, Vol. 14, No. 4, pp. 532–549.
Eisenhardt, K.M. (1989b) “Making Fast Strategic Decisions in High-velocity Environments”, Academy of Management Journal, Vol. 32, No. 3, pp. 543–576.
Eisenhardt, K.M., Furr, N.R., Bingham, C.B. (2010) “Micro-foundations of Performance: Balanc-ing Efficiency and Flexibility in Dynamic Environments”, Organization Science, Vol. 21, No. 6, pp. 1263–1273.
Eisenhardt, K.M. and Graebner, M.E. (2007) “Theory Building form Cases: Opportunities and Challenges”, Academy of Management Journal, Vol. 50, No. 1, pp. 25–32.
Finchman, R.G., Kohli, R. and Krishnan, R. (2011) “Editorial Review—The Role of Information Systems in Healthcare: Current Research and Future Trends”, Information Systems Research, Vol. 22, No. 3, pp. 419–428.
Ford, J. and Backoff, R. (1988) “Organizational Change In and Out of Dualities and Paradox”, in Quinn, R. and Cameron K. (Eds.) Paradox and Transformations: Toward a Theory of Change in Organization and Management, Ballinger, Cambridge (MA).
Ford, R. and Angermeier, I. (2004) “Managing the Knowledge Environment: A Case Study from Healthcare”, Knowledge Management Research and Practice, Vol. 2, No. 3, pp. 131–146.
Freeman, C. (2007) “The ICT Paradigm”, in Mansell, R., Avgerou, C., Quah, D. and Silverstone, R. (Eds.) The Oxford Handbook of Information and Communication Technologies, Oxford Uni-versity Press, Oxford (UK).
Glaser, B.G. and Strauss A.L. (1967) The Discovery of Grounded Theory: Strategies for Qualitative Research, Aldine, Chicago (IL).
Gibson, C.B. and Birkinshaw, J. (2004) “The Antecedents, Consequences and Mediating Role of Organizational Ambidexterity”, Academy of Management Journal, Vol. 47, No. 2, pp. 209–226.

22
Gilbert, C.G. (2005) “Unbundling the Structure of Inertia: Resource versus Rigidity”, Academy of Management Journal, Vol. 48, No. 5, pp. 741–763.
Hartley, C. and Jones, E. (2005) EHR Implementation: A Step-By-Step Guide for the Medical Prac-tice, American Medical Association, Chicago (IL).
IHCO, ICT in Health Care Observatory (2009) “Electronic Medical Record: Toward an Integrated Support to the Clinical Processes”, Politecnico di Milano, www.osservatori.net, in Italian.
Jha, A.K., Ferris, T.G., Donelan, K., DesRoches, C., Shields, A., Rosenbaum, S. and Blumenthal, D. (2006) “How Common are Electronic Health Records in the United States? A Summary of Evidence”, Health Affairs, Vol. 25, No. 6, pp. 496–507.
Jha, A.K., DesRoches, C.M., Campbell, E.G., Donelan K., Rao, S.R., Ferris, T.G., Shields, A., Ros-enbaum, S. and Blumenthal D. (2009) “Use of Electronic Medical Records in U.S. Hospitals”, New England Journal of Medicine, 360(12): 1628–1638.
Jick, T.D. (1979) “Mixing Qualitative and Quantitative Methods: Triangulation in Action”, Admin-istrative Science Quarterly, Vol. 24, No. 3, pp. 602–611.
Joshi, K.D., Chi, L., Datta, A. and Han, S. (2010) “Changing the Competitive Landscape: Continu-ous Innovation Through IT-Enabled Knowledge Capabilities”, Information Systems Research, Vol. 22, No. 5, pp. 472–495.
Kane, G.C. and Alavi, M. (2007) “Information Technology and Organizational Learning: An Inves-tigation of Exploration and Exploitation Processes”, Org. Science, Vol. 18, No. 5, pp. 796–812.
Kopach-Konrad, R., Lawley, M., Criswell, M., Hasan, I., Chkraborty, S. and Pekny J. (2007) “Ap-plying Systems Engineering Principles in Improving Health Care Delivery”, Journal of Gen-eral Internal Medicine, Vol. 22, No. 3, pp. 431–437.
Koriat, A. and Goldsmith, M. (2000) “Toward a Psychology of Memory Accuracy”, in Fiske, S.T., Shcacter, D.L. and Zahn-Wexler, C. (Eds.) Annual Review of Psychology (Vol. 51), Berrethh-Koehler, Palo Alto (CA).
Kumar, N., Stern, L.W. and Anderson, J.C. (1993) “Conducting Interorganizational Research Using Key Informants”, Academy of Management Journal, Vol. 36, No. 6, pp. 1633–1651.
Lavie, D., Kang, J. and Rosenkpf, L. (2011) “Balance Within and Across Domains: The Perfor-mance Implications of Exploration and Exploitation in Alliances”, Organization Science, Vol. 22, No. 6, pp. 1517–1538.
Leonard-Barton, D. (1990) “A Dual Methodology for Case Studies: Synergistic Use of Longitudinal Single Site with Replicated Multiple Sites”, Organization Science, Vol. 1, No. 3, pp. 248–266.
Lewis, M.W. (2000) “Exploring Paradox: Toward a More Comprehensive Guide”, Academy of Management Review, Vol. 25, No. 4, pp. 760–776.
Lo Scalzo, A., Donatini, A., Orzella, L., Cicchetti, A., Profili, S. (2009) “Italy: Health System Re-view”, Health Systems in Transitions, Vol. 11, No. 6, pp. 1–243.
Martin, J.A. and Eisenhardt, K.M. (2010) “Rewiring: Cross-business-units Collaboration in Multi-business Organizations”, Academy of Management Journal, Vol. 53, No. 2, pp. 265–301.
Miles, M.B. and Huberman, A.M. (1994) Qualitative Data-analysis: An Expanded Source-book, Sage, Thousand Oaks (CA).
Miller, A.R. and Tucker, C. (2009) “Privacy Protection and Technology Diffusion: The Case of Electronic Medical Records”, Management Science, Vol. 55, No. 7, pp. 1077–1093.
Mithas, S., Ramasubbu, N. and Sambamurthy, V. (2011) “How Information Management Capabil-ity Influences Firm Performance”, MIS Quarterly, Vol. 35, No. 1, pp. 237–256.
Oshri, I., Pan, S.L. and Newell, S. (2004) “Trade-offs Between Knowledge Exploitation and Explo-ration Activities”, Knowledge Management Research and Practice, Vol. 3, No. 1, pp. 10–23.
Ozcan, P. and Eisenhardt, K.M. (2009) “Origin of Alliance Portfolios: Entrepreneurs, Network Strat-egies, and Firm Performance”, Academy of Management Journal, Vol. 52, No. 2, pp. 246–279.
Patton M.Q. (2002) Qualitative Research and Evaluation Methods, Sage, Thousand Oaks (CA).

23
Peng, A, Pike S. and Roos, G. (2007) “Intellectual Capital and Performance Indicators: Taiwanese Healthcare Sector”, Journal of Intellectual Capital, Vol. 8, No. 3, pp. 538–556.
Powel, W.W., Koput, K.W. and Smith-Doerr, L. (1996) “Interorganizational Collaboration and the Locus of Innovation”, Administrative Science Quarterly, Vol. 41, No. 1, pp. 116–145.
Sambamurthy, V. and Subramani, M.R. (2005) “Special Issue on Information Technologies and Knowledge Management”, MIS Quarterly, Vol 29, No. 1, pp. 1–7.
Schiuma, G. (2011) “Managing and Measuring Knowledge Assets Dynamics for Business Value Crea-tion in Organizations”, in: Managing Knowledge Assets and business Value Creation in Or-ganizations: Measures and Dynamics, ed. G. Schiuma, Business Science Reference, Hershey.
Simon, S.R., Kaushal, R., Cleary, P.D., Jenter, C.A., Volk, L.A., Poon, E.G., Orav, E.J., Lo, H.G., Williams, D.H. and Bates, D.W. (2007) “Correlates of Electronic Health Record Adoption in Office Practices”, J. of American Medical Informatics Association, Vol. 4, No. 1, pp. 110–117.
Smith, W.K. Lewis, M.W. (2011) “Toward a Theory of Paradox: A Dynamic Equilibrium Model of Organizing”, Academy of Management Review, Vol. 36, No. 2, pp. 381–461.
Straus, A.L. and Corbin, J. (1990) Basic of Qualitative Research, Sage, Newbury Park (CA). Tantiverdi, H (2005) “Information Technology Relatedness, Knowledge Management Capability,
and Performance of Multibusines Firms”, MIS Quarterly, Vol. 29, No. 2, pp. 311–334. Yin, R.K. (2003) Case Study Research: Design and Methods (3rd Ed.), Thousand Oaks (CA): Sage. WHO, World Health Organization (2010) The World Health Report 2010: Health Systems Financ-
ing—The Path to Universal Coverage, www.who.int/whr/2010/en/index.html.
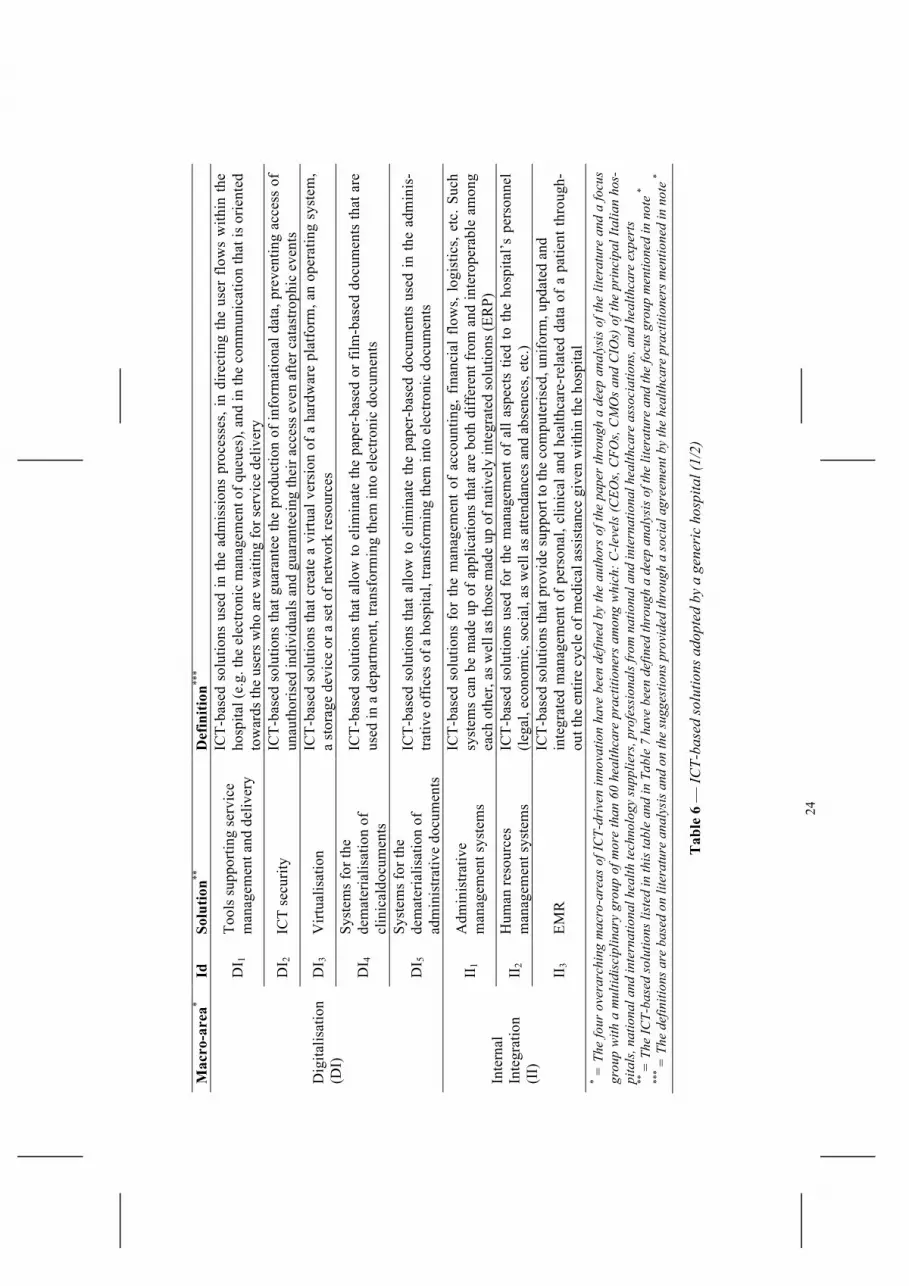
6 Appendix
Macro-area* Solution** Hospital A*** Hospital B*** Hospital C***
Digitalisation (DI)
DI1 DI2 C C C DI3 D DI4 C C C DI5 C C C
Internal Integration (II)
II1 F C C II2 C II3 D D D
External Integration (EE)
EI1 F F EI2 EI3 F F D
Analytics (AN) AN1 AN2 F AN3 F
* = The four overarching macro-areas of ICT-driven innovation have been defined by the authors of the paper through a deep analysis of the literature and a focus group with a multidisciplinary group of more than 60 healthcare practitioners among which: C-levels (CEOs, CFOs, CMOs and CIOs) of the principal Italian hospitals, national and international health technology suppliers, professionals from national and international healthcare associations, and healthcare experts **
= Refer to Table 6 and Table 7 for the definitions of all the ICT-based solutions listed in this table *** = C means «present at January 2009»; D means «under development in the period from Janu-ary 2009 to December 2011»; F means «development starting before the end of 2012»
Table 5 — ICT-based solutions in the three studied hospitals
24
Mac
ro-a
rea*
Id
Solu
tion**
D
efin
ition
***
Dig
italis
atio
n (D
I)
DI 1
To
ols
supp
ortin
g se
rvic
e m
anag
emen
t and
del
iver
y
ICT-
base
d so
lutio
ns u
sed
in th
e ad
mis
sion
s pr
oces
ses,
in d
irect
ing
the
user
flo
ws
with
in th
e ho
spita
l (e.
g. th
e el
ectro
nic
man
agem
ent o
f que
ues)
, and
in th
e co
mm
unic
atio
n th
at is
orie
nted
to
war
ds th
e us
ers
who
are
wai
ting
for s
ervi
ce d
eliv
ery
DI 2
IC
T se
curit
y IC
T-ba
sed
solu
tions
that
gua
rant
ee th
e pr
oduc
tion
of in
form
atio
nal d
ata,
pre
vent
ing
acce
ss o
f un
auth
oris
ed in
divi
dual
s an
d gu
aran
teei
ng th
eir a
cces
s ev
en a
fter c
atas
troph
ic e
vent
s
DI 3
V
irtua
lisat
ion
ICT-
base
d so
lutio
ns th
at c
reat
e a
virtu
al v
ersi
on o
f a h
ardw
are
plat
form
, an
oper
atin
g sy
stem
, a
stor
age
devi
ce o
r a s
et o
f net
wor
k re
sour
ces
DI 4
Sy
stem
s fo
r the
de
mat
eria
lisat
ion
of
clin
ical
docu
men
ts
ICT-
base
d so
lutio
ns th
at a
llow
to e
limin
ate
the
pape
r-ba
sed
or fi
lm-b
ased
doc
umen
ts th
at a
re
used
in a
dep
artm
ent,
trans
form
ing
them
into
ele
ctro
nic
docu
men
ts
DI 5
Sy
stem
s fo
r the
de
mat
eria
lisat
ion
of
adm
inis
trativ
e do
cum
ents
ICT-
base
d so
lutio
ns th
at a
llow
to e
limin
ate
the
pape
r-ba
sed
docu
men
ts u
sed
in th
e ad
min
is-
trativ
e of
fices
of a
hos
pita
l, tra
nsfo
rmin
g th
em in
to e
lect
roni
c do
cum
ents
Inte
rnal
In
tegr
atio
n (I
I)
II1
Adm
inis
trativ
e m
anag
emen
t sys
tem
s
ICT-
base
d so
lutio
ns f
or t
he m
anag
emen
t of
acc
ount
ing,
fin
anci
al f
low
s, l
ogis
tics,
etc
. Suc
h sy
stem
s ca
n be
mad
e up
of a
pplic
atio
ns th
at a
re b
oth
diff
eren
t fro
m a
nd in
tero
pera
ble
amon
g ea
ch o
ther
, as
wel
l as
thos
e m
ade
up o
f nat
ivel
y in
tegr
ated
sol
utio
ns (E
RP)
II2
Hum
an re
sour
ces
man
agem
ent s
yste
ms
ICT-
base
d so
lutio
ns u
sed
for
the
man
agem
ent
of a
ll as
pect
s tie
d to
the
hos
pita
l’s p
erso
nnel
(le
gal,
econ
omic
, soc
ial,
as w
ell a
s atte
ndan
ces
and
abse
nces
, etc
.)
II3
EMR
IC
T-ba
sed
solu
tions
that
pro
vide
sup
port
to th
e co
mpu
teris
ed, u
nifo
rm, u
pdat
ed a
nd
inte
grat
ed m
anag
emen
t of
pers
onal
, clin
ical
and
hea
lthca
re-r
elat
ed d
ata
of a
pat
ient
thro
ugh-
out t
he e
ntire
cyc
le o
f med
ical
ass
ista
nce
give
n w
ithin
the
hosp
ital
* = T
he fo
ur o
vera
rchi
ng m
acro
-are
as o
f IC
T-dr
iven
inno
vatio
n ha
ve b
een
defin
ed b
y th
e au
thor
s of
the
pape
r th
roug
h a
deep
ana
lysi
s of
the
liter
atur
e an
d a
focu
s gr
oup
with
a m
ultid
isci
plin
ary
grou
p of
mor
e th
an 6
0 he
alth
care
pra
ctiti
oner
s am
ong
whi
ch: C
-leve
ls (C
EOs,
CFO
s, C
MO
s an
d C
IOs)
of t
he p
rinc
ipal
Ital
ian
hos-
pita
ls, n
atio
nal a
nd in
tern
atio
nal h
ealth
tech
nolo
gy su
pplie
rs, p
rofe
ssio
nals
from
nat
iona
l and
inte
rnat
iona
l hea
lthca
re a
ssoc
iatio
ns, a
nd h
ealth
care
exp
erts
**
= T
he IC
T-ba
sed
solu
tions
list
ed in
this
tabl
e an
d in
Tab
le 7
hav
e be
en d
efin
ed th
roug
h a
deep
ana
lysi
s of t
he li
tera
ture
and
the
focu
s gro
up m
entio
ned
in n
ote
* **
* = T
he d
efin
ition
s are
bas
ed o
n lit
erat
ure
anal
ysis
and
on
the
sugg
estio
ns p
rovi
ded
thro
ugh
a so
cial
agr
eem
ent b
y th
e he
alth
care
pra
ctiti
oner
s men
tione
d in
not
e *
Tab
le 6
— IC
T-ba
sed
solu
tions
ado
pted
by
a ge
neri
c ho
spita
l (1/
2)

25
Mac
ro-a
rea*
Id
Solu
tion**
D
efin
ition
***
Exte
rnal
In
tegr
atio
n (E
E)
EI1
Dig
ital s
ervi
ces
to th
e pa
tient
s
ICT-
base
d so
lutio
n to
del
iver
ser
vice
s to
the
patie
nts
thro
ugh
digi
tal c
hann
els
(e.g
. pub
lic w
eb
site
); In
clud
ed in
this
cat
egor
y it
is p
ossi
ble
to f
ind
the
com
mun
icat
ion
serv
ices
(in
form
atio
n on
the
heal
thca
re o
rgan
isat
ion,
etc
.), th
ose
for
patie
nt a
cces
s of
clin
ical
info
rmat
ion
(clin
ical
da
ta, r
epor
ts, e
tc.),
thos
e su
ppor
ting
the
use
of h
ealth
care
res
ourc
es (
onlin
e re
serv
atio
ns a
nd
paym
ent f
or v
isits
, etc
.), C
RM
ser
vice
s (p
roac
tive
man
agem
ent o
f th
e re
latio
ns w
ith th
e pa
-tie
nt, d
eadl
ine
notif
icat
ion,
etc
.), a
nd s
ervi
ces
to s
uppo
rt th
e in
tera
ctio
n am
ong
patie
nts
(cha
ts,
foru
ms,
blo
gs, s
ocia
l net
wor
ks, e
tc.)
EI2
Reg
iona
l med
icin
e an
d ho
me
heal
th a
ssis
tanc
e IC
T-ba
sed
solu
tions
that
resp
ond
to th
e ai
ms
of c
reat
ing
inte
grat
ion
betw
een
the
hosp
ital,
the
dist
rict s
ervi
ces
and
fam
ily d
octo
rs, w
ith th
e in
volv
emen
t of l
ocal
com
mun
ities
of i
nter
est
EI3
Inte
grat
ion
with
the
EHR
ICT-
base
d so
lutio
ns u
sed
to c
reat
e in
tegr
atio
n w
ith th
e pl
atfo
rms
for
Elec
troni
c H
ealth
Rec
-or
ds (
EHR
s), d
efin
ed a
s th
e re
cord
for
mat
for
hea
lthca
re d
ata
com
ing
from
var
ious
peo
ple
in
char
ge o
f tre
atm
ent o
pera
tions
, mor
e fr
eque
ntly
—bu
t not
exc
lusi
vely
—in
the
sam
e te
rrito
rial
area
(e.g
. hos
pita
ls a
nd p
rivat
e cl
inic
al la
bora
torie
s op
erat
ing
in th
e sa
me
regi
onal
are
a)
Ana
lytic
s (A
N)
AN
1 C
ompu
teris
ed d
rug
man
agem
ent s
yste
ms
ICT-
base
d so
lutio
ns to
sup
port
drug
pre
scrip
tion,
pre
para
tion
and
adm
inis
tratio
n
AN
2 C
linic
al
Gov
erna
nce
tool
s
ICT-
base
d so
lutio
ns th
at s
uppo
rt cl
inic
al d
ecis
ions
with
the
obje
ctiv
e of
impr
ovin
g th
e qu
ality
of
ser
vice
s of
fere
d, a
nd re
achi
ng/m
aint
aini
ng e
leva
ted
heal
thca
re s
tand
ards
. Exa
mpl
es a
re th
e sy
stem
s to
def
ine
diag
nost
ic p
aths
, to
cont
rol a
ppro
pria
tene
ss, t
o re
port
inci
dent
s, to
attr
ibut
e D
RG
, to
verif
y Pa
tient
Dis
char
ge F
iles
(PD
Fs),
etc.
AN
3 G
over
nanc
e da
shbo
ards
ICT-
base
d so
lutio
ns th
at s
uppo
rt th
e go
vern
ance
and
adm
inis
trativ
e de
cisi
ons
with
the
obje
c-tiv
e of
impr
ovin
g th
e qu
ality
of
the
adm
inis
trativ
e pr
oces
ses.
Exa
mpl
es a
re b
usin
ess
inte
lli-
genc
e to
ols
adop
ted
to b
alan
ce th
e se
rvic
e pe
aks
of d
eman
d w
ithin
the
hosp
ital
* = T
he fo
ur o
vera
rchi
ng m
acro
-are
as o
f IC
T-dr
iven
inno
vatio
n ha
ve b
een
defin
ed b
y th
e au
thor
s of
the
pape
r th
roug
h a
deep
ana
lysi
s of
the
liter
atur
e an
d a
focu
s gr
oup
with
a m
ultid
isci
plin
ary
grou
p of
mor
e th
an 6
0 he
alth
care
pra
ctiti
oner
s am
ong
whi
ch: C
-leve
ls (C
EOs,
CFO
s, C
MO
s an
d C
IOs)
of t
he p
rinc
ipal
Ital
ian
hos-
pita
ls, n
atio
nal a
nd in
tern
atio
nal h
ealth
tech
nolo
gy su
pplie
rs, p
rofe
ssio
nals
from
nat
iona
l and
inte
rnat
iona
l hea
lthca
re a
ssoc
iatio
ns, a
nd h
ealth
care
exp
erts
**
= T
he IC
T-ba
sed
solu
tions
list
ed in
this
tabl
e an
d in
Tab
le 6
hav
e be
en d
efin
ed th
roug
h a
deep
ana
lysi
s of t
he li
tera
ture
and
the
focu
s gro
up m
entio
ned
in n
ote
* **
* = T
he d
efin
ition
s are
bas
ed o
n lit
erat
ure
anal
ysis
and
on
the
sugg
estio
ns p
rovi
ded
thro
ugh
a so
cial
agr
eem
ent b
y th
e he
alth
care
pra
ctiti
oner
s men
tione
d in
not
e *
Tab
le 7
— IC
T-ba
sed
solu
tions
ado
pted
by
a ge
neri
c ho
spita
l (2/
2)

26
Ado
ptio
n U
sage
Im
prov
emen
t R
epre
sent
ativ
e in
form
ants
quo
tes
Stim
ulus
:*
• R
educ
ing
the
inef
ficie
ncie
s
in c
linic
al d
ata
man
agem
ent
• Ex
tern
al p
ress
ures
(E
HR
inte
grat
ion)
•
Impr
ovin
g th
e ef
fect
iven
ess
of th
e tre
atm
ents
Pr
oble
ms:
•
Min
or: i
nitia
l tec
hnol
ogic
al
resi
stan
ce o
f the
phy
sici
ans
(use
d to
wor
k ac
cord
ing
to
own
wor
kflo
ws)
•
Min
or: t
ende
r writ
ing
(pre
visi
ons
of th
e m
odul
ar
ex
tens
ions
; will
ingn
ess
to
av
oid
pure
cos
t-orie
nted
ve
ndor
s)
Impa
ct o
n kn
owle
dge
expl
ora-
tion
and
know
ledg
e exp
loita
tion:
•
Step
1: m
acro
-inte
grat
ion
amon
g in
ter-
depa
rtmen
tal
proc
esse
s (k
now
ledg
e ex
ploi
tato
ry ra
dica
l in
nova
tion)
•
Step
2: m
anag
emen
t of a
set
of
pro
ject
s in
eac
h un
it to
use
the
shar
ed d
ata
(kno
wle
dge
expl
orat
ory
incr
emen
tal
inno
vatio
n)
Am
bide
xtro
us a
ppro
ach:
•
Dep
artm
enta
l lev
el:
ICT-
driv
en p
roce
ss
inte
grat
ion
• O
rgan
isat
iona
l lev
el:
tem
pora
l diff
eren
tiatio
n
an
d ad
min
iste
red
inte
grat
ion
Perf
orm
ance
impa
ct:
• In
itial
: cos
t rat
iona
lisat
ion
• Fi
nal:
initi
al +
qua
lity
impr
ovem
ent
Cha
lleng
es/is
sues
: •
Bal
anci
ng s
tand
ardi
satio
n re
quire
men
ts w
ith
prac
titio
ners
’ cu
stom
isat
ion
need
s •
Man
agin
g us
er re
sist
ance
N
ext s
teps
: •
Maj
or: c
ontin
uing
the
deve
lopm
ent o
f the
EM
R
• M
inor
: bet
ter i
nteg
ratin
g w
ith
th
e re
gion
al E
HR
(not
onl
y th
e m
anda
tory
dat
a)
• M
inor
: dev
elop
ing
an
adm
inis
trativ
e m
anag
emen
t
sy
stem
• M
y id
eas a
re p
retty
cle
ar. I
kno
w
exac
tly w
hat I
wan
t fro
m a
n EM
R an
d w
here
we’
ll en
d. H
owev
er, I
hav
e to
ta
ke in
to a
ccou
nt th
e an
nual
reso
urce
s in
my
hand
s. Th
is so
lutio
n is
the
best
co
mpr
omis
e I’
ve fo
und…
—C
IO
• …
and
this
«te
chni
cian
» co
mes
to
tell
you
that
you
hav
e to
cha
nge
a de
cenn
ial,
effe
ctiv
e w
ay o
f w
orki
ng! —
Phys
icia
n •
This
yea
r [20
09]
we
inte
grat
e; th
e ne
xt
one
[201
0] w
e’ll
star
t a v
ertic
alis
atio
n in
eac
h de
part
men
t to
see
how
we
can
use
the
shar
ed d
ata.
The
n w
e’ll
rest
art
the
proc
ess o
f int
egra
tion…
and
so o
n an
d so
fort
h —
CIO
•
Our
mai
n fo
cus w
as c
ost r
atio
nalis
a-tio
n, b
ut w
e en
ded
also
with
a b
ette
r se
rvic
e —
CM
O
• EM
R is
on
the
agen
da a
lso
for
the
year
201
2 —
CE
O
* = T
he a
ltern
ativ
es a
re li
sted
in th
e or
der o
f im
port
ance
spec
ified
by
the
info
rman
ts
Tab
le 8
— M
ain
findi
ngs o
f the
inte
rvie
ws p
erfo
rmed
on
the
hosp
ital A

27
Ado
ptio
n U
sage
Im
prov
emen
t R
epre
sent
ativ
e in
form
ants
quo
tes
Stim
ulus
:*
• Im
prov
ing
the
effe
ctiv
enes
s of
the
treat
men
t •
Exte
rnal
pre
ssur
es
(EH
R in
tegr
atio
n)
• R
educ
ing
the
inef
ficie
ncie
s in
clin
ical
dat
a m
anag
emen
t Pr
oble
ms:
•
Min
or: d
ecis
ion
from
whi
ch
depa
rtmen
t to
star
t (e
ffic
ienc
y vs
. pot
entia
l pe
rvas
iven
ess)
•
Min
or: c
lear
ly u
nder
stan
d th
e ne
cess
ities
of t
he p
hysi
cian
s •
Min
or: t
echn
ical
pro
blem
s lin
ked
to th
e cu
stom
isat
ion
of
the
EMR
to th
e w
orkf
low
s of
th
e pi
lot d
epar
tmen
t and
to
inte
rope
rabi
lity
issu
es
Impa
ct o
n kn
owle
dge e
xplo
ra-
tion
and
know
ledg
e exp
loita
tion:
•
Step
1: i
nteg
ratio
n of
the
in
tra-d
epar
tmen
tal p
roce
sses
—
one
depa
rtmen
t at a
tim
e (k
now
ledg
e ex
plor
ator
y ra
dica
l inn
ovat
ion)
•
Step
2: e
xten
sion
of t
he
achi
eved
ben
efits
to th
e ot
her d
epar
tmen
ts w
ith th
e in
tegr
atio
n of
inte
r-de
partm
enta
l pro
cess
es
(kno
wle
dge
expl
oita
tory
in
crem
enta
l inn
ovat
ion)
A
mbi
dext
rous
app
roac
h:
• D
epar
tmen
t lev
el: I
CT-
driv
en
proc
ess
inte
grat
ion
• O
rgan
isat
iona
l lev
el:
tem
pora
l diff
eren
tiatio
n an
d em
erge
nt in
tegr
atio
n Pe
rfor
man
ce im
pact
: •
Initi
al: q
ualit
y im
prov
emen
t •
Fina
l: in
itial
+ c
ost
ratio
nalis
atio
n
Cha
lleng
es/is
sues
: •
Bal
anci
ng p
ract
ition
ers’
cu
stom
isat
ion
need
s w
ith
stan
dard
isat
ion
requ
irem
ents
•
Hom
ogen
isin
g th
e di
ffer
ent
sect
ions
of t
he E
MR
N
ext s
teps
: •
Maj
or: b
ette
r int
egra
ting
the
patie
nts
to th
e he
alth
care
pr
oces
ses—
offe
ring
digi
tal
serv
ices
thro
ugh
the
site
of
the
hosp
ital
• M
ajor
: dev
elop
ing
a cl
inic
al
gove
rnan
ce s
uppo
rt sy
stem
(e
xtra
ctin
g va
lue
from
the
digi
tal d
ata)
•
Min
or: c
ontin
uing
the
deve
lopm
ent o
f the
EM
R
• O
ne b
y on
e w
e m
ake
all o
f the
m h
appy
! Se
riou
sly:
a fo
cus o
n ea
ch d
epar
tmen
t—co
mbi
ned
with
a g
ood
over
all d
esig
n—al
low
s us t
o un
ders
tand
and
bet
ter
mee
t the
dem
ands
from
the
lines
of
busi
ness
—C
IO
• W
e ar
e si
mpl
y do
ing
wha
t we
have
do
ne w
ithin
eac
h de
part
men
t. Bu
t on
a b
igge
r sca
le. I
nfor
mat
ion
has
to b
e av
aila
ble
ever
ywhe
re if
you
w
ant t
o tr
uly
achi
eve
the
rela
tive
bene
fits —
CE
O
• St
anda
rdis
atio
n? It
was
a b
lood
bath
, bu
t it w
as w
orth
it —
CIO
•
The
end
resu
lts?
Bette
r tre
atm
ent,
quic
ker d
iagn
oses
, and
bra
nd n
ew
re
sear
ch fi
elds
read
y on
the
shel
f w
aitin
g fo
r us —
Phys
icia
n •
The
risk
is to
cre
ate
a se
t of f
anta
stic
is
land
s with
kilo
met
res o
f sea
se
para
ting
them
—C
MO
•
The
uniq
ue re
ject
ion
issu
es a
re
enco
unte
red
once
you
try
to e
xten
d th
e “t
ailo
red”
feat
ure
to o
ther
de
part
men
ts. I
n th
ese
case
s, so
me
revi
sion
s are
nec
essa
ry —
CIO
•
The
next
pie
ce in
this
jigs
aw is
the
patie
nt —
CE
O
* =
The
alte
rnat
ives
are
list
ed in
the
orde
r of i
mpo
rtan
ce sp
ecifi
ed b
y th
e in
form
ants
Tab
le 9
— M
ain
findi
ngs o
f the
inte
rvie
ws p
erfo
rmed
on
the
hosp
ital B
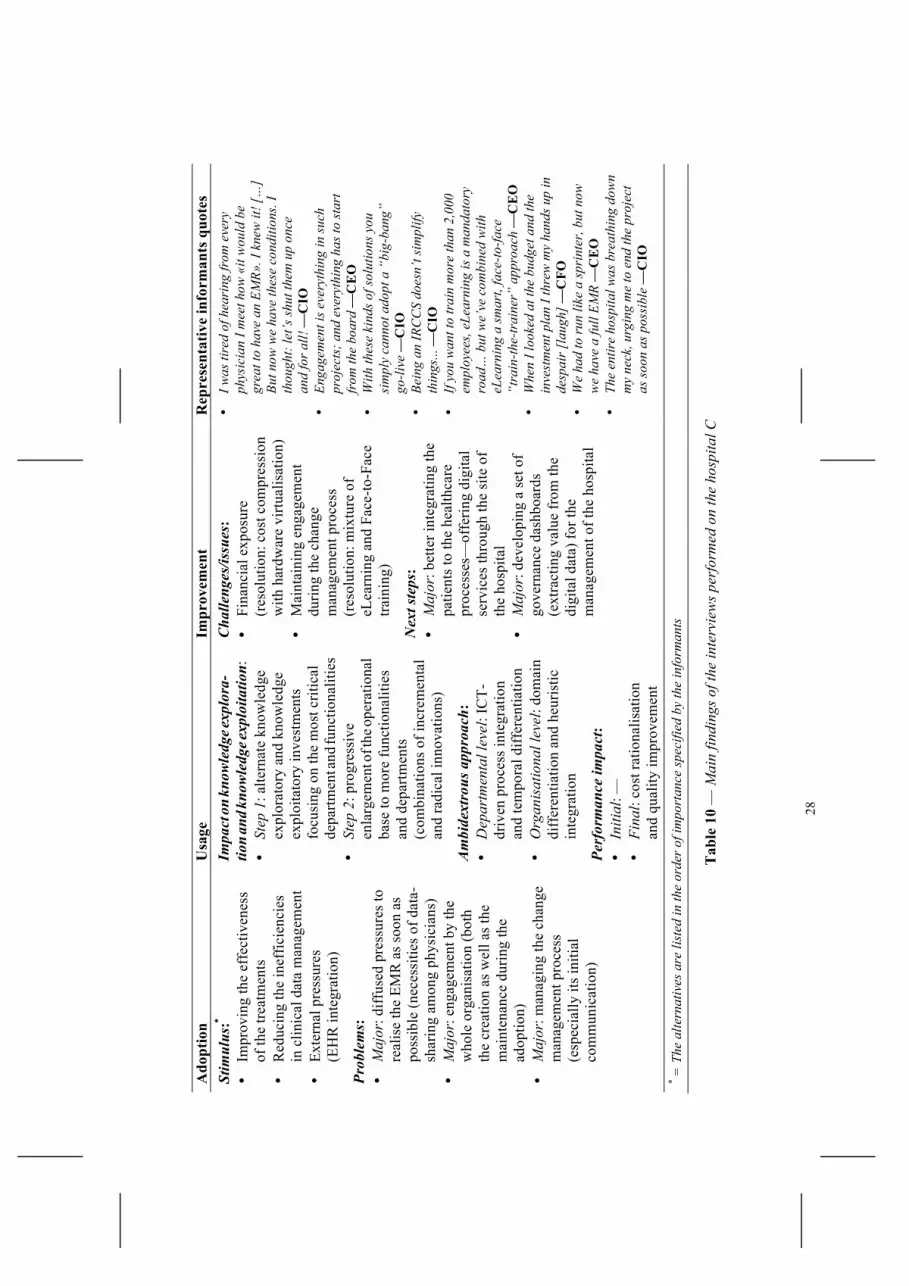
28
Ado
ptio
n U
sage
Im
prov
emen
t R
epre
sent
ativ
e in
form
ants
quo
tes
Stim
ulus
:*
• Im
prov
ing
the
effe
ctiv
enes
s of
the
treat
men
ts
• R
educ
ing
the
inef
ficie
ncie
s in
clin
ical
dat
a m
anag
emen
t •
Exte
rnal
pre
ssur
es
(EH
R in
tegr
atio
n)
Prob
lem
s:
• M
ajor
: diff
used
pre
ssur
es to
re
alis
e th
e EM
R a
s so
on a
s po
ssib
le (n
eces
sitie
s of
dat
a-sh
arin
g am
ong
phys
icia
ns)
• M
ajor
: eng
agem
ent b
y th
e w
hole
org
anis
atio
n (b
oth
the
crea
tion
as w
ell a
s th
e m
aint
enan
ce d
urin
g th
e ad
optio
n)
• M
ajor
: man
agin
g th
e ch
ange
m
anag
emen
t pro
cess
(e
spec
ially
its
initi
al
com
mun
icat
ion)
Impa
ct o
n kn
owle
dge e
xplo
ra-
tion
and
know
ledg
e exp
loita
tion:
•
Step
1: a
ltern
ate
know
ledg
e ex
plor
ator
y an
d kn
owle
dge
expl
oita
tory
inve
stm
ents
fo
cusi
ng o
n th
e m
ost c
ritic
al
depa
rtmen
t and
func
tiona
litie
s •
Step
2: p
rogr
essi
ve
enla
rgem
ent o
f the
oper
atio
nal
base
to m
ore
func
tiona
litie
s an
d de
partm
ents
(c
ombi
natio
ns o
f inc
rem
enta
l an
d ra
dica
l inn
ovat
ions
) A
mbi
dext
rous
app
roac
h:
• D
epar
tmen
tal l
evel
: IC
T-dr
iven
pro
cess
inte
grat
ion
and
tem
pora
l diff
eren
tiatio
n •
Org
anis
atio
nal l
evel
: dom
ain
diff
eren
tiatio
n an
d he
uris
tic
inte
grat
ion
Perf
orm
ance
impa
ct:
• In
itial
: —
• Fi
nal:
cost
ratio
nalis
atio
n an
d qu
ality
impr
ovem
ent
Cha
lleng
es/is
sues
: •
Fina
ncia
l exp
osur
e (r
esol
utio
n: c
ost c
ompr
essi
on
with
har
dwar
e vi
rtual
isat
ion)
•
Mai
ntai
ning
eng
agem
ent
durin
g th
e ch
ange
m
anag
emen
t pro
cess
(r
esol
utio
n: m
ixtu
re o
f eL
earn
ing
and
Face
-to-F
ace
train
ing)
N
ext s
teps
: •
Maj
or: b
ette
r int
egra
ting
the
patie
nts
to th
e he
alth
care
pr
oces
ses—
offe
ring
digi
tal
serv
ices
thro
ugh
the
site
of
the
hosp
ital
• M
ajor
: dev
elop
ing
a se
t of
gove
rnan
ce d
ashb
oard
s (e
xtra
ctin
g va
lue
from
the
digi
tal d
ata)
for t
he
man
agem
ent o
f the
hos
pita
l
• I w
as ti
red
of h
eari
ng fr
om e
very
ph
ysic
ian
I mee
t how
«it
wou
ld b
e gr
eat t
o ha
ve a
n EM
R». I
kne
w it
! […
] Bu
t now
we
have
thes
e co
nditi
ons.
I th
ough
t: le
t’s sh
ut th
em u
p on
ce
and
for a
ll! —
CIO
•
Enga
gem
ent i
s eve
ryth
ing
in su
ch
proj
ects
; and
eve
ryth
ing
has t
o st
art
from
the
boar
d —
CE
O
• W
ith th
ese
kind
s of s
olut
ions
you
si
mpl
y ca
nnot
ado
pt a
“bi
g-ba
ng”
go-li
ve —
CIO
•
Bein
g an
IRC
CS
does
n’t s
impl
ify
thin
gs...
—C
IO
• If
you
wan
t to
trai
n m
ore
than
2,0
00
empl
oyee
s, eL
earn
ing
is a
man
dato
ry
road
… b
ut w
e’ve
com
bine
d w
ith
eL
earn
ing
a sm
art,
face
-to-fa
ce
“tra
in-th
e-tr
aine
r” a
ppro
ach
—C
EO
•
Whe
n I l
ooke
d at
the
budg
et a
nd th
e
inve
stm
ent p
lan
I thr
ew m
y ha
nds u
p in
de
spai
r [la
ugh]
—C
FO
• W
e ha
d to
run
like
a sp
rint
er, b
ut n
ow
we
have
a fu
ll EM
R —
CE
O
• Th
e en
tire
hosp
ital w
as b
reat
hing
dow
n m
y ne
ck, u
rgin
g m
e to
end
the
proj
ect
as so
on a
s pos
sibl
e —
CIO
* = T
he a
ltern
ativ
es a
re li
sted
in th
e or
der o
f im
port
ance
spec
ified
by
the
info
rman
ts
Tab
le 1
0 —
Mai
n fin
ding
s of t
he in
terv
iew
s per
form
ed o
n th
e ho
spita
l C