attending unintended transformations of health care infrastructure
TRANSCRIPT

1This article is published in a peer reviewed section of the International Journal of Integrated Care
International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
Research and Theory
Attending unintended transformations of health careinfrastructure
Helle Wentzer, Department of Communication and Psychology, Virtual Center for Health Informatics, http://www.v-chi.dk/english/index.htm, Aalborg University, Denmark, http://www.kommunikation.aau.dk/index.uk.html
Ann Bygholm, Department of Communication and Psychology, Virtual Center for Health Informatics, Aalborg University,Denmark
Correspondence to: Helle Wentzer, Department of Communication and Psychology, Aalborg University, Kroghstraede 1,DK-9220 Aalborg OE, Denmark, E-mail: [email protected]
AbstractIntroduction: Western health care is under pressure from growing demands on quality and efficiency. The development andimplementation of information technology, IT is a key mean of health care authorities to improve on health care infrastructure.
Theory and methods: Against a background of theories on human-computer interaction and IT-mediated communication, differentempirical studies of IT implementation in health care are analyzed. The outcome is an analytical discernment between differentrelations of communication and levels of interaction with IT in health care infrastructure. These relations and levels are synthesizedinto a framework for identifying tensions and potential problems in the mediation of health care with the IT system. These problemsare also known as unexpected adverse consequences, UACs, from IT implementation into clinical health care practices.
Results: This paper develops a conceptual framework for addressing transformations of communication and workflow in health careas a result of implementing IT.
Conclusion and discussion: The purpose of the conceptual framework is to support the attention to and continuous screening forerrors and unintended consequences of IT implementation into health care practices and outcomes.
Keywordshuman-computer interaction, socio-technical, infrastructure, communication, information technology
Introduction
Like many other Western countries, Danish society isfacing new challenges in organizing its health care.An ageing population, rising demands and possibilitiesin treatment and care, and a lack of clinical staff are,among other issues, pressing new national policies onhealth care practice, management and organization.In responding to such pressures, information technol-ogy (IT) is given a central role as a change agent ofhealth care infrastructure to support more quality,safety and continuity in and across healthcare set-tings. This paper, however, questions the nature of anIT infrastructure as some ‘thing’ that can be deliber-ately planned for by authorities and vendors w1–8x,since the unfulfilled hopes in IT strategies on healthcare so far w5x, and the contingent nature of healthand disease, leaves much open for further learning,negotiation and design.
IT systems in health care have often failed to fulfill thedesired outcomes for which they were designed, soleaving health care organizations with systems thatnobody uses at great financial expense. For example,health care institutions have often developed capitalprojects to support an ongoing process of IT imple-mentation and customization. Such projects not onlyhave to train the many users in clinical settings in thefunctionalities of a specific IT system, but also mustoffer continuous support (on both system and userdemands) on a 24 hours a day, 7 days a week,365 days a year basis. The effectiveness of the ‘work-ing relationship’ w9x between IT users and the ITsystem depends highly on the degree of stability,usability and utility of the system in the specific caredomain and practice. What this means is that theevolution of an IT system from an infrastructure to aneffectively implemented product is an unpredictableprocess requiring risk management w10x that puts

International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
2This article is published in a peer reviewed section of the International Journal of Integrated Care
emphasis on screening, evaluation and learning fromthe unintended consequences of implementing IT sys-tems into care practices. The organizers of any ITproject in health care thus face additional implemen-tation challenges beyond the purely technical. Beingaware of new kinds of possible ‘errors’ arising fromputting IT systems into clinical or practical use areimportant considerations w11x. Or as phrased in aviewpoint paper on computerized order entry systems,CPOE: ‘‘Attention to detail is critical to provide appro-priate support to clinicians’ work flows w...x. Duringsuch complex implementations, institutions mustremain cognizant of, and carefully monitor, errors thatthese systems can cause as well as the errors thatthey prevent’’ w12 p.27x.
This paper poses health care managers, IT implemen-ters and developers to draw attention to inadequacies1
of communication and interaction from IT implemen-tation in order to secure changes of health careinfrastructures in a direction that, for the benefit of thepatients, support the optimal use of technical andhuman resources. Discontinuities in communicationand workflow counteract ‘integrated care’—both interms of patient safety, patient centeredness andcoherence of care paths—as higher demands are puton cliniciansyhuman resources, compensating forinsufficient technology tools.
Methods and materials
The conceptual framework presented in the followingpaper aims to facilitate how organizations that facethe implementation of an IT project can identify, artic-ulate and negotiate across any undesirable conse-quences of new health care infrastructures w13x.
The conceptual framework is developed against thebackground of theoretical studies on infrastructure andcommunication, and empirical evaluation studies ofhuman-computer interactions in health care. Evalua-tion research is, in ‘Methods of Information in Medi-cine’, considered ‘‘a key in identifying how people,organizational, and social issues—all crucial to systemdesign, development and implementation, and use—interplay with informatics projects’’ w14 p.215x. Further,‘‘the study of failures, partial successes, and changesin project definition or outcome’’ are recommended forfuture research wibidx. Ammerwerth et al. confirm mat-uration in evaluation research in medical informatics
‘‘From the phenomenological position, attention is not primarily a focus1
on something, but a perspective from turning points, where the in-between ofrelationships can be experienced. In this sense, attention shows itself asalertness for the coming to be and the realm of transitions’’. Schuback, MSC.The knowledge of attention. International Journal of Qualitative Studies onHealth and Well-being 2006 Sep;1(3):133-40. Available from: http:yywww.tandf.noyqhw.’’
as studies of more technical aspects of implementa-tion have declined and shifted to an increase in studieson the quality of care processes and patient outcomesw15 p.55x. Leroy and Beuscart advocate the impor-tance of usability evaluation by including final users inreal settings in order to detect severe usability prob-lems w16x. Classen et al. confirm that evaluation of ITimplementation in individual health care organizationsis more pressing than ever w17 p.51x. ‘‘All organiza-tions will need to perform ongoing evaluation of theirCPOE applications and their EHR wElectronic HealthRecordx if the potential benefits of these technologiesare to be actually realized’’ w17 p.53x. Gross et al.oblige leading clinicians to participate by taking proac-tive responsibility and by making iterative improve-ments w12x. ‘‘Those implementing systems mustmonitor them for adverse effects on both patient careand on caregivers’ workflows. Similar monitoring mustoccur to ensure that desired goals are achieved.Continuous refinement based on ongoing end-userfeedback must guide progress’’ w12 p.26x. In otherwords, the current research literature calls for moredetailed knowledge of end-users’ experiences, moreresponsibilities of the organizations and proactivemethods for dealing with the consequences of ITsystems on the health care processes and outcomes.
This paper’s object of study is to evaluate IT in healthcare infrastructure, and how to study and grasp trans-formation of infrastructure. Qualitative methods areused in order to collect and reflect highly contextualdata. Research in telemedicine w18 p.529x shows thatthis area, at the end of the 1990s, was plagued bythe difficulties of generalization since research wascharacterized by confusing definitions, the use of smallsample sizes, and primarily new and evolving ITinnovations. Nonetheless, opportunities for studiesemploying qualitative methodologies enable a closeexamination of the phenomenon and help researchersbetter understand any emerging environment w19–21x.Qualitative methods are therefore central to evaluationstudies as well as the prevalence of in-depth analysisof local experiences and settings w22x, in order tograsp and fixate the contextual dimensions of healthcare services, as processes enacted and located inconcrete temporal and spatial settings w23x.
This paper attempts to illustrate organizational andinterpersonal processes of health care by undertakingan analysis across three recently completed qualitativestudies of IT implementation. Firstly, the theoreticalassumptions are outlined on how to understand ‘infra-structure’ and the role of information technology here-in. Secondly, the evaluation studies refer to the resultsof two major, international qualitative studies on UACand to three minor, Danish qualitative studies on the

International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
3This article is published in a peer reviewed section of the International Journal of Integrated Care
use of IT for communication in three different healthcare organizational settings. The analysis of theDanish studies are reflected and discussed in relationto the results of the international evaluation studieson unintended consequences. Thirdly, the methods ofthe three Danish case studies are presented and thecases are subsequently analyzed according to thequestions on infrastructural transformations and prob-lems of UAC from IT implementation. Fourthly, thedetermined relations of communication and levels ofinteracting with IT are synthesized into a conceptualframework that seeks to capture transformations ofhealth care infrastructures from human-computerinteraction.
What is an infrastructure?
The traditional concept of an infrastructure is some-thing that is just there, ready to use, completelytransparent and not open to question (for example,water or electricity supplies, the railway, the roadsystem, telecommunication, the mail service, or theInternet). Under this concept there is a tendency toperceive infrastructure as ‘hardware’ – something thatis built and maintained and then sinks into the invisiblebackground, and which is noticed only when it breaksdown. But as Edwards w24x points out, infrastructureis socio-technical in nature, meaning that infrastructureis not only based on the hardware of an organization,but also ‘software’ such as socially-communicatedbackground knowledge, general acceptance and reli-ance, and near ubiquitous accessibility.
According to the online Open Content dictionary Wik-tionary (http:yyen.wiktionary.org), infrastructure means‘‘an underlying base or foundation especially for anorganization or system’’ and ‘‘the basic facilities, serv-ices and installations needed for the functioning of acommunity or society’’. The definition provided herepoints to the fact that equally important for the under-standing of infrastructure is the development or evo-lution of ways to communicate or interface with theunderlying base. For example, telephony is possiblenot only because signals over a distance can betransmitted using electromagnetic waves via electronictransmitters, but also because of the invention of anappropriate appliance – the telephone – which canbe used for the purpose. Importantly, the system isnot successful solely because the technology works,but because enough people want to use, own andpay for a phone with which to communicate withothers. It works because the whole service is highlyorganized, making sure that it is possible to makecalls to the people you want to talk to. Furthermore, itis difficult to separate the development of the ‘base’infrastructure from the development of services and
regulations that support its functionality. It is difficult,for example, to separate the development of thetransmission of signals (base) from the developmentof phones and the other services and installationneeded to make the phone system function as aninfrastructure. As Latour demonstratively put it:‘‘Boeing-747s do not fly, airlines fly’’ w25 p.46x. Infra-structures, therefore, include technologies that aresocially co-defined by their use and are always underthe process of development or change; they growthrough their use, and it is their use that defineswhether or not something becomes an infrastructure.
Star & Ruhleder w9x and Hanseth w10x (among others)discuss the infrastructural aspects of IT systems. Theyboth suggest different dimensions to characterize aninfrastructure. While focusing on use and use practice,Star and Ruhleder mention the following character-istics:
● embeddedness (integrated in social structures andpractices),
● transparency (can be used without removing focusfrom the task),
● reach or scope (goes beyond individual tasks orprocesses),
● learned as part of membership (an inherent part ofan organization),
● links with conventions of practice (shapes and isshaped by practice),
● embodiment of standards (builds on standards andconventions),
● built on an installed base (must relate to existingtechnologies), and
● visible upon breakdown (loses transparency and isdrawn into focus when it breaks down).
Very much in line with this, but with slightly moreemphasis on the necessary technical prerequisites foran infrastructure to function, Hanseth w10x suggeststhat an infrastructure is an evolving (evolves continu-ously), shared (must function as a shared resourceor foundation for a community), open (lack of bordersin how many elements it may include, how manyusers may be using it and also in the sense that thereare no limits to who might contribute to its design anddeployment and that the development time has nobeginning and no ending), heterogeneous (includingsub-infrastructures based on different versions of thesame standard or different standards covering thesame functionality) installed base (backward compat-ibility which also means that the existing heavilyinfluences how the new can be designed and thatinfrastructures are considered as existing already,never developed from scratch).

International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
4This article is published in a peer reviewed section of the International Journal of Integrated Care
Studying infrastructure from ITimplementation
These dimensions suggest ‘‘an infrastructure, whichis without absolute boundary on a priory definition’’w9x and also points to the fact that infrastructurescannot be understood independently of the work theyafford. An IT system, then, becomes an infrastructurein relation to the involved technical and social elemen-ts of the organized practices within which it functions.Furthermore, the IT system evolves over time, doesnot have a fixed group of users or use practices, andis a dynamic ongoing process with no fixed center ofcontrol. IT implementation, therefore, also becomes apoint of departure for studying infrastructure as the‘embeddedness’, ‘transparency’, ‘embodiment of con-ventions’ and ‘scope’ only become ‘visible upon break-down’, which let the technology and ‘base’ in questionbecome a negotiable part of a ‘shared’, ‘open’ ‘hetero-geneous’ and ‘evolving’ infrastructure. The followingempirical studies are evaluations of the implement-ation of different IT systems into health care, primarilycomputerized order entry systems, CPOEs, in differentsettings that enlighten infrastructural issues.
Understanding IT infrastructureand implementation issues inhealth care from qualitative stud-ies of unintended consequences
Cambell, Sittig, Ash, Guappone and Dykstra identifynine types of unintended adverse consequences relat-ed to CPOE w11x. The types are the outcome of amajor qualitative study over 9 months; 390 hours ofobservation, 43 hours of interview, transcripts and fieldnotes of approximately 1900 pages at five US hospi-tals, using either home grown or vendor built CPOEsystems. The nine major categories are in order ofdecreasing frequency: 1) moreynew work for clin-icians; 2) unfavorable workflow issues; 3) never end-ing system demands; 4) problems related to paperpersistence; 5) untoward changes in communicationpatterns and practices; 6) negative emotions; 7) gen-eration of new kinds of errors; 8) unexpected changesof power structure; and 9) overdependence on thetechnology. In the viewpoint paper by Ash, Berg andCoiera w4x, the processes of generating errors arereflected and categorized. The categorization drawsfrom cross-Atlantic experiences with CPOE systemsin health care delivery settings. The American, Austra-lian and Dutch data are generated from qualitativestudies of ethnographic observation and semi-struc-tured interviews with professionals w4x. The overall
purpose of the CPOE systems is to prevent medicalerrors. The studies confirm, though, that CPOE sys-tems are not as successful in preventing errors as isgenerally hoped for, but that they could actually gen-erate new errors w4 p.105x. Ash et al. categorize theerrors within two ‘main categories’; firstly, the processof ‘entering and receiving messages in and from thesystem’ w4 p.106x, and secondly, the ‘communicationand coordination processes’ that the system is sup-posed to support w4 p.107x. These categories of errorscan be reinterpreted within the research tradition ofhuman-computer interaction as referring to the ‘usa-bility’ and the ‘utility’ of the system w26x. The usabilityof the system is determined by the direct interactionbetween the user and the user interface of the system,i.e. in health care delivery settings the usability of thesystem for ‘entering and receiving of messages’. The‘communication and coordination process’ w4 p.107xis concerned with the utility of the system in mediatingthe users’ collaboration on clinical tasks across differ-ent tempo-spatial locations. The three Danish imple-mentation studies presented in the followingparagraphs are examples of IT implementations tosupport and mediate the collaboration:
– across different health care institutions,– across different wards at a university hospital, and– across different user-groups in two wards of inter-
nal medicine with different professions and loginrights.
Additionally, Star and Ruhleder’s ‘Steps to an ecologyof infrastructure’ points to a third category or ‘step’ inhuman-computer interaction. Drawing on cyberneticsand the communication theory of Gregory Bateson,Star & Ruhleder understand infrastructural changesas the outcome of paradoxes between the organiza-tional purpose of the system and the utility in use w9x,also termed ‘trans-contextual syndrome’ or ‘doublebind’ w27x. Systemic experiences of ‘double binds’, i.e.bindings between what a user is expected to use thesystem for and what the system can be used for, andagain double bindings between what the system isdesigned for and what it actually does, point to ‘socio-technical problems’ in the evolving infrastructure.These problems need further attention and articulationin order to redesign the system and the work practicein question to a more deliberate and ecological‘healthy’ fit. We shall refer to such socio-technicaltensions as ‘paradoxes’ between the purposes ofimplementing the system and the actual effect. Withincultural psychology w28x and the cultural–historicaltradition of activity theory, ‘contradictions’ between theuser’s culture and tools relate to ‘the motive of theactivity’ w29x. A cultural and historical motive of west-ern health care is, for example, to prevent illness and

International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
5This article is published in a peer reviewed section of the International Journal of Integrated Care
suffering w30x. These motives and goals of health caretechniques are again, within an Aristotelian tradition,related to ethical values and collective understandingof living a ‘good life’ w31–36x. These categories andanalytical levels of understanding the development oftechnology in health care are summed up in Table 1.
The three following case studies point to such mis-apprehensions between intentions and actual use ofIT for organizing health care. The studies are qualita-tive studies conducted independently of each otherw37–42x, but analyzed according to the three analyticallevels of Table 1. Subsequently, a synthesis of thestudies is made in order to support the attention toturning points in the relationships of humans and ITwfootnote 1x w43x and the possible articulation of futureIT-related communication problems w13x.
Three minor Danish case studiesof IT implementation acrossinstitutions, hospital wards anddifferent user-groups
The objects and methods of the three case studiescan be summed up as follows. The case study on thecommunication across different health care institutionsfocused on the implementation of an information sys-tem to support the communication between the localhospital and the municipality. The implementation wasmonitored by interviews with four central figures; intotal twelve hours of interviews were conducted duringthe project. Besides diary notes, meeting minutes fromthe implementation process, and an internal evaluationreport done by the responsible organization at the endof the project also entered into the material analyzed.Further description can be found in Bygholm w37x.
The two other studies concerned the implementationof a vendor built CPOE in a university hospital, andat two wards of internal medicine at another hospitalin the same county. The CPOE system at this stageof development is only handling ‘the bookkeeping’ ofmedication. It is not offering any decision support, andis developed by a professional vendor (SystematicSoftware Inc, Aarhus, DK) in close cooperation withthe responsible Health Management Organization ofAarhus County, Denmark, who has supplied cliniciansto the development project. The county is the hospitalowner and is, according to the Danish Law on PatientSafety 2004 w44x, collecting and reviewing unintendedadverse consequences, UACs w45x, in relation to usingthe CPOE w40x. Within a period of 6 months, cliniciansin the five hospitals of the county reported 754 UACsin total, of which 97 UACs happened at the universityhospital. These 97 UACs are further categorized in
the Audit Report of the County w40x as 45 UACs dueto ‘organizational errors’, and 52 UACs caused by‘technical errors’. These organizational and technicalcircumstances of the UACs were further elaboratedon by the use of qualitative methods for richness anddetails. Some empirical examples of ‘organizationalerrors’ and ‘technical errors’ were unfolded in a lectureand discussion between researchers and students inhealth informatics held at Ballerup, Aalborg Universityin Copenhagen, 21 April 2006. These examples werecontextualized even further by two hours of interviewwith the responsible implementer at the universityhospital, retelling her experiences with concreteinstances that produced UACs.
The clinical use of the CPOE system at two internalmedical wards builds on 48 hours of observation, sixinterviews with primary users, two physicians and fournurses, and an analysis of the user interface of theCPOE and of other documents. At the time of thestudy, the CPOE had been in use for eight months.Based on the observations, three use-scenarios forcentral events in the medication process were con-structed (prescription, requisition, and considerationsof continuation of treatment). The use-scenarios wereintroduced to the interviewees for four reasons: tocondense, verify and generalize the observations andto trigger the memory of the interviewees.
The following three paragraphs will present the indi-vidual cases and analyze them according to the threeanalytical levels of interacting with IT in health careinfrastructure in Table 1.
IT communication across institutions:municipality and hospital
The Municipality of Aalborg’s Department of Care forthe Elderly and Disabled decided to implement elec-tronic exchange of information between on the onehand the municipality and the hospital, and on theother hand between the municipality and the generalpracticing doctors. The idea behind the project wasthat switching from communicating through telephoneand letters to electronic information exchange wouldmean a more correct exchange of information andalso a faster and more holistic treatment of the citizeninvolved. A well-known standard, EDI messages byway of Vans technology, was chosen for exchange ofinformation involving an extension of the standard, butfrom a technical point of view it should not be toodifficult to make the involved partners’ systems com-municate. Still, numerous problems were encounteredin the implementation and use of electronic exchangefor communication and coordination of work withsenior citizens between the partners.

International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
6This article is published in a peer reviewed section of the International Journal of Integrated Care
This case focuses on the exchange of informationbetween municipality and hospital. It illustrates thetangled nature of the problems experienced in theattempts to fit in use of a new infrastructure in thework practices of the hospital staff.
Initially, there were two issues hindering the electronicexchange of information between hospital and munic-ipality, as seen from the perspective of the hospitalstaff. First, the hospital used an old-fashioned patientadministration system and second, the involved staff(at seven medical wards) had no experience of usingICT in their work. Thus, training of the staff (approxi-mately 300 persons) was needed. For each of theseven wards involved, about four persons were trainedfor one day. The staff participating in the training wassupposed to teach the others in the wards they camefrom, thus functioning as super users. The problemwas not that the trained staff could not use the system,but more that it was an extremely time-consumingtask to send messages, the patient administrationsystem operating with many different types of screensthat should be accessed in a certain order and beingdifficult to navigate around. For an inexperienced user,it could take around an hour to send a message anddemonstrating the process for another nurse couldeasily take one and a half to two hours.
Apart from training, there was also a need for agree-ments between the municipality and the hospital toensure that messages sent were actually received atthe municipality within an acceptable time limit. Abasic guideline in the set of agreements was thedivision of messages into two categories: emergentand non-emergent messages. Emergent messageswere messages that had to be acted upon within24 hours and those had to be phoned to make surethey were received and understood by the right per-sons. An un-emergent message, which is a messagenot needing action within 24 hours, could be sent
electronically. Compared to the expectationsexpressed in the project application concerning ‘‘...amore quick and effective way of communication ... ’’by using ICT for communication this was unexpected.As for the whole set of agreements it turned out that,due to many different interpretations of the agree-ments, they got increasingly more and more detailed,which in turn made them less accessible for the staff.Thus, instead of one infrastructure for exchange ofinformation between the institutions they now had twoand double communication became a result of this,i.e. in many cases they used both the phone and thesystem to communicate the same information just tobe sure that messages were actually received.
To send more detailed information on patientsbetween the partners, personal consent was neededfor each message. In practice this was not alwaysdoable and one of the solutions that was examinedand discussed with the legal authorities was thepossibility of a general consent from each citizenreceiving care. This was, however, considered abreach of the law, thus information could only beexchanged if consent was given for each message.There was nothing new in the law; the same conditionscount when information is exchanged between twopersons by telephone. Use of electronic communica-tion, however, changes and broadens the context forinformation exchange; what can be said in an oralphone conversation between two people is not neces-sarily suitable for wider distribution in a writing-basedmedia.
This study shows the complexity of the many issuesinvolved in the attempt to change from one infrastruc-ture to another. Some of the problems were due tothe complicated interaction style demanded by the oldsystem and to computer inexperience among the staff.The fact that it was such a time-demanding task tosend and receive messages and the doubtfulness
International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
7This article is published in a peer reviewed section of the International Journal of Integrated Care
concerning the rules for exchange of information tosome extent questioned the rationale of using thesystem, seen from the point of view of the hospitalstaff. The agreements that should solve the problemsgot rather complicated in order to cover all situations.The necessity of operating with two different lines ofcommunication did not afford the work practice at alland results of problems were in many cases doublecommunication, i.e. more work instead of less workfor the staff. Adding to this, and coming from societalcontext, was the legal issue of patient consent by theexchange of patient information, which questioned thelegality of the basic intensions and goals behind theproject.
Unintended transformation of the communica-tion between the municipality and hospitalwith the edifact-systemThe study showed the complexity of the problemsrelated to achieving the aims of implementation of anew infrastructure. Doubtfulness and double commu-nication were some of the unintended consequencesand the findings of the study can be summed up atthe following levels of interaction:
1. Level of interaction: the communication betweenmunicipality and hospital were interrupted, as theirexisting Patient Administration System was difficultand time-consuming to use.
2. Level of IT-mediated interaction among users: theusers needed to establish new procedures forsending and receiving messages to each other,dividing them into urgentycomplicated messagesand non-urgent messages where only the lattercould be sent electronically, and to set rules forwho was responsible for reading and acting uponthe electronic information.
3. Infrastructural level: in contrast to the expectedvision of optimizing communication the informationexchange expanded, double communicationincluding IT and telephone were necessary tosecure quality of collaboration. The exchange ofelectronic patient data also collided with the lawon data security, whereby a whole new infrastruc-tural problem arose at a national level .2
IT communication across wards in auniversity hospital
The project organization of a university hospital isimplementing electronic order entry systems, CPOE.The aims of the system are, among others, to improvepatient safety and continuity of patient treatment and
October 2006: The Minister of Health and Internal Public Affairs made a2
suggestion for a new law on data security, which is now at hearing in theDanish Parliament to be negotiated.
care. In relation to a new Danish Health Law w44x,clinicians have been reporting on unintended conse-quences in clinical work. Within a period of 6 months,97 unintended consequences from using the CPOEsystem in the University Hospital have been reportedto the county, the hospital’s owners. These are in anAudit Report from the county w40x, categorized as 45unintended consequences of a technical nature, dueto an unstable system and inadequate user interface,and 52 unintended consequences of an organizationalnature, expressed by a lack of correspondencebetween electronic documentation of medication andother registration of data. The responsible implemen-ter of the project organization experienced though,that the technical errors and the organizational errorswere related. The following two stories show, theyeven feed each other in practice and affect the infra-structure of health care as well.
‘Technical error’ of patient safetyAn example of unintended consequences caused bytechnical inadequacies of an order entry system,CPOE, is that on some screen dumps the wrongpatient identification number is showing. Leaders ofhospital and project organization were to decide quick-ly on how to warn the end-users. But here the imple-menters face a new problem of a social origin: ‘‘Buthow do you communicate to 3000 users? w...x. Warn-ings on the screen are simply clicked away’’. Closingthe system down was an equally bad possibility: ‘‘they(the clinicians, HW) are totally depending on it’’. As asolution, a telephone-chain was started in which onehospital ward after the other should pass on themessage about the wrong patient identification num-bers in the CPOE to the next ward. The morning after,a follow-up call was made to make sure the chainwent through. The person calling the emergency wardof internal medicine recalls: ‘‘I phoned the ward topass on the warning. They were receiving patientswith heart attacks, so she just answered ‘yes, yes,yes’—and hung up. She just wanted me to get off thephone. The systems should probably have beenclosed down’’. The chain went through wards withfewer emergency cases. A control call was made tothe last ward in the telephone-chain. They neverreceived the message.
The so-called technical error becomes a story of newcommunication problems in the organization relatedto CPOE, as well as a reminder that for clinicians insitu, life and death issues take priority over technicalerrors, even though in a further prospect new, unin-tended consequences might silently come into being,as in this case of the broken telephone-chain.

International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
8This article is published in a peer reviewed section of the International Journal of Integrated Care
‘Organizational error’ of patient continuityacross wards‘Missing documentation’ or ‘double registrations of thesame patient information’ are examples of unintendedconsequences, UCs, of an organizational nature. Thisseemingly human factor had a technical side as well.Often patients move from an internal medicine wardto surgery and from surgery to intensive care, butafter implementation of the CPOE, intensive carelacked information on the patients coming from sur-gery. This gives a gap in the patients’ electronicdocumentation of medication. Though, as understoodand widely accepted in the organization, the surgeryward has no direct need of CPOE in their work, whilethe doctors, as well as the nurses, in intensive caredo. They need the information to control and confirmthe patient’s medication in the CPOE when admittinghim or her to intensive care. The responsible imple-menter of the CPOE reflects: ‘‘How do you make workprocesses to fit this problem, and who gets the job todo so? It almost turned into a war, and I was sittingin trench warfare. It is a whole new problem that wehave never had before. Previously we would just havereceived the papers from the record passing through.’’
This story is not just about inadequate collaborationbetween wards, but also that the CPOE creates newproblems for the wards and the clinicians to securethe patient continuity. This conflict was traded off asthe doctor’s secretary in the surgery ward was pointedout to enter all patient data in the CPOE.
The infrastructural changes expressed in these twostories show that the visions and expectations of morepatient safety and continuity from implementing CPOEinto health care practice are not automatically fulfilled,but require attention to new, socio-technical problemsand work on communication.
Transformation of communication with ITacross wards in a university hospitalThe study showed that IT implementation producesnew communication problems in the health careorganization, and thus the intentions of more patientsafety and fewer continuity problems are not auto-matically a result of a CPOE system, but a newchallenge for health care and project organizationsthat cannot be reduced to either technical or organi-zational errors. The two examples of a so-called‘technically’ caused UAC and organizational groundsfor UACs can be summed up as problems at thefollowing levels of interacting with IT.
Organizational aspects of the ‘technical error’ ofpatient safety
1. Level of interaction: the technical error in theCPOE system of showing wrong patient identifi-
cation numbers interrupted the patient safetythroughout the organization.
2. Level of mediated interaction: discontinuity in com-municating the technical error to all end-usersthrough a telephone-chain is collectively makingthe clinical collaboration more risky for patients aswell as for users.
3. Infrastructural level points to socio-technical prob-lems in taking responsibility for patient safety as aclinical user, and as responsible manager of thereliability of the system.
Technical aspects of ‘organizational error’ of patientcontinuity across wards
1. Level of interacting: the ward of intensive carelacks information in the CPOE on patients receivedfrom the ward of surgery.
2. Level of IT mediated interaction between thewards: as the surgeons do not need the CPOE fortheir work discontinuity appeared in the collab-oration between the wards with the replacementof paper with the CPOE.
3. At the infrastructural level the problem of recreat-ing patient continuity between the wards withCPOE became a new socio-technical problem,also posing the question: ‘‘Who is responsible forthings to flow?’’
Communication on medicationbetween clinicians using CPOE in twomedical wards
The study w36,37x points to the central situation ofenacting medication with CPOE at two internal medi-cal wards in a middle-sized Danish hospital. Theprogramme of action for medication consists of aminimum of seven core acts or ‘subprogrammes ofaction’: 1) the indication of treatment, initiated by thepatient’s problemydiagnosis, 2) the ‘prescription’ (rec-ommendation of treatment and patient’s consent ofchoice), 3) ‘drug order’, i.e. registration of order inCPOE system, 4) ‘dosage’, i.e. making the drug readyfor consumption, 5) ‘administration’ (the patient isgiven the drug), 6) ‘assessment’ of the drug’s effecton the patient, and 7) ‘considerations on how toproceed’, i.e. whether to continue or withdraw thedrug. This process takes place within a differenttemporal rhythm, and located at different places, forexample at the patient’s bedside, in the hallway, indifferent offices and the drug storage room. Globalaccess from other wards or institutions is possible.The CPOE interacted with four of the seven subpro-grammes in the medication process, 2) the prescrip-tion, 3) the order entry, 4) dosage and 7) withdrawalor continuity of treatment. The following situations of

International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
9This article is published in a peer reviewed section of the International Journal of Integrated Care
use point to transformation of ordination with theCPOE, of the registration of clinical collaboration andpossibly transformation of patient trajectories withCPOE.
Transformation of ordination with CPOEOn the doctors’ rounds, when the physician shouldorder the patient-consented prescription, a detouroccurred. The physician would not consult and orderdrugs for one patient at a time. Instead he wouldmemorize three or four patients at a time before hewould first dictate diagnosis and order to the patientrecord and then order the prescription in the CPOE.This detour in the medication safety of the individualpatient was not only caused by a clumsy PC tablethat made it too troublesome to take the CPOE lap-top along on patient rounds, but the digitalized dicta-phone for dictating to the patients’ medical recordsprior to the order entry is placed on the wall in thehallway, additionally making a long walking distancefrom the patient’s bed.
Transformation of user rights and clinicalteamworkThe work divisions inscribed in the user rights of theCPOE adhere to the certification rights of physiciansand nurses. In practice, though, the clinical teamworkrelated to ‘drug order’ and ‘dosage’ varies from theformal certification rights and duties. The inflexibleuser rights and time-consuming login to the CPOE,along with too few computers and computers placedfar away from drug storage, made the clinical collab-oration spread out in time and space, subsequentlyleading to more coordination work on medication. Acounteraction of the clinical team was to bypass theuser rights by working under the same login of a userwith physicians’ rights. This meant that the virtualmedication work registered under a specific user nameand login does not necessarily correspond to anindividual person, but might cover an empirical workteam of clinicians.
Possible transformation of patient trajectorieswith CPOEThe continuity of the patients’ medication transformedwith the CPOE. This is also part of the vision ofelectronic, instead of paper-documented, medication.CPOE gives ‘global accesses’ to the medication dataof patients, not only from all hospital wards, but alsofrom other health care institutions that might beinvolved in the future health care trajectory of thepatient. The global access and continuity aspects ofelectronic communication gave a new problem whendrug orders were withdrawn and when patients weredischarged from the hospital ward. The CPOE systemreplaced a paper medication scheme containing drug
orders for seven days at a time. After seven days thenurse on nightshift would copy the drug orders to becontinued on to a new scheme, and leave out thosethat were withdrawn in the meantime. This ‘procedureof cleaning up’ the registered drug orders were leftout of the CPOE, as the system does not run out of‘writing space’ every seventh day. Additionally, itwould be extra work for the physicians (having theuser rights to do so) to log on to the CPOE everytime they have withdrawn an order. Leaving out the‘cleaning procedure’, on the other hand, means thatdrug orders stay active in the system after the end ofhospitalization. This adds new risks to the patients’safety. In a possible future when a patient is readmit-ted into the hospital or enters another health careinstitution, the information in the CPOE might misleadthe users, and foster a wrong understanding of thepatient’s medication profile and history.
Infrastructural transformation of medicalhealth care practiceThe study points out that more ‘global access’ topatients’ medication data with the CPOE system mightlocally give more difficult access. New physical andsocial distances of prescribing and coordinating med-ication work with the CPOE have arisen, alongsidenew tasks and divisions of work.
Transformation of ordination with CPOE
1. Level of interaction: the physical distance betweenthe patient’s bed, the CPOE and other artefactsinterrupts the physician’s prescription and requisi-tion of drugs in the CPOE on doctors’ rounds.
2. Level of IT-mediated interaction: the physicianwould reduce the walking by memorizing three orfour patients at a time and order their prescriptionsin the CPOE after dictating to the patient record inthe hallway.
3. Level of infrastructure: a socio-technical paradoxarose as the doctor–patient relationship trans-formed into collective e-patient, when entering‘mass-orders’ several patients at a time. Cognitivepressure is put on the individual doctor in ordernot to mix up the patients, the patients’ prescrip-tions and orders with each other. Mistakes arelikely to be difficult to trace in the CPOE as theyhappen before the orders are prescribed.
Transformation of user rights and clinical teamwork
1. Level of interaction: the users are interrupted intheir workflow by an inflexible system for enteringand retrieving information.
2. Level of IT-mediated interaction: discontinuitybetween the rationality of medication workinscribed in the software, the number and location
International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
10This article is published in a peer reviewed section of the International Journal of Integrated Care
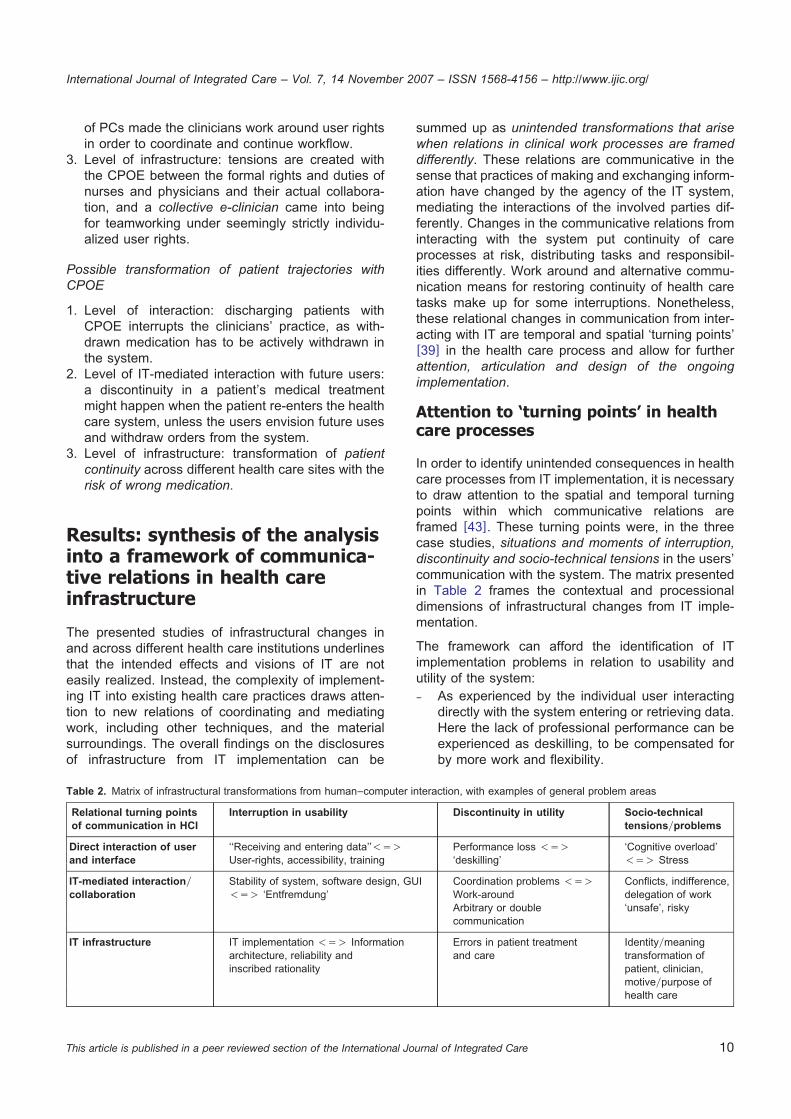
Table 2. Matrix of infrastructural transformations from human–computer interaction, with examples of general problem areas
Relational turning points Interruption in usability Discontinuity in utility Socio-technicalof communication in HCI tensionsyproblems
Direct interaction of user ‘‘Receiving and entering data’’-s) Performance loss -s) ‘Cognitive overload’and interface User-rights, accessibility, training ‘deskilling’ -s) Stress
IT-mediated interactiony Stability of system, software design, GUI Coordination problems -s) Conflicts, indifference,collaboration -s) ‘Entfremdung’ Work-around delegation of work
Arbitrary or double ‘unsafe’, riskycommunication
IT infrastructure IT implementation -s) Information Errors in patient treatment Identityymeaningarchitecture, reliability and and care transformation ofinscribed rationality patient, clinician,
motiveypurpose ofhealth care
of PCs made the clinicians work around user rightsin order to coordinate and continue workflow.
3. Level of infrastructure: tensions are created withthe CPOE between the formal rights and duties ofnurses and physicians and their actual collabora-tion, and a collective e-clinician came into beingfor teamworking under seemingly strictly individu-alized user rights.
Possible transformation of patient trajectories withCPOE
1. Level of interaction: discharging patients withCPOE interrupts the clinicians’ practice, as with-drawn medication has to be actively withdrawn inthe system.
2. Level of IT-mediated interaction with future users:a discontinuity in a patient’s medical treatmentmight happen when the patient re-enters the healthcare system, unless the users envision future usesand withdraw orders from the system.
3. Level of infrastructure: transformation of patientcontinuity across different health care sites with therisk of wrong medication.
Results: synthesis of the analysisinto a framework of communica-tive relations in health careinfrastructure
The presented studies of infrastructural changes inand across different health care institutions underlinesthat the intended effects and visions of IT are noteasily realized. Instead, the complexity of implement-ing IT into existing health care practices draws atten-tion to new relations of coordinating and mediatingwork, including other techniques, and the materialsurroundings. The overall findings on the disclosuresof infrastructure from IT implementation can be
summed up as unintended transformations that arisewhen relations in clinical work processes are frameddifferently. These relations are communicative in thesense that practices of making and exchanging inform-ation have changed by the agency of the IT system,mediating the interactions of the involved parties dif-ferently. Changes in the communicative relations frominteracting with the system put continuity of careprocesses at risk, distributing tasks and responsibil-ities differently. Work around and alternative commu-nication means for restoring continuity of health caretasks make up for some interruptions. Nonetheless,these relational changes in communication from inter-acting with IT are temporal and spatial ‘turning points’w39x in the health care process and allow for furtherattention, articulation and design of the ongoingimplementation.
Attention to ‘turning points’ in healthcare processes
In order to identify unintended consequences in healthcare processes from IT implementation, it is necessaryto draw attention to the spatial and temporal turningpoints within which communicative relations areframed w43x. These turning points were, in the threecase studies, situations and moments of interruption,discontinuity and socio-technical tensions in the users’communication with the system. The matrix presentedin Table 2 frames the contextual and processionaldimensions of infrastructural changes from IT imple-mentation.
The framework can afford the identification of ITimplementation problems in relation to usability andutility of the system:– As experienced by the individual user interacting
directly with the system entering or retrieving data.Here the lack of professional performance can beexperienced as deskilling, to be compensated forby more work and flexibility.

International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
11This article is published in a peer reviewed section of the International Journal of Integrated Care
Table 3. Types of UAC from health care infrastructures with CPOE, ranged by frequency
Relational turning points Interruption in usability Discontinuity in utility Socio-technicalof communication in HCI tensions/problems
Direct interaction of ‘Negative emotions’ (6) ‘Problems related to paper ‘Moreynew work for clinicians’ (1)user and interface persistence’ (4)
IT-mediated interactiony ‘Never ending system ‘Unfavorable workflow Untoward changes in communication patternscollaboration demands’ (3) issues’ (2) and practices (5)
Infrastructures ‘Over dependency of ‘Generation of new ‘Unexpected changes in power structure’ (8)the technology’ (9) kinds of errors’ (7)
– From experiencing the social collaboration in medi-ating clinical tasks with IT, and how these workrelations and clinical tasks are cultivated by the ITsystem.
– Again, how the purpose and identities of theinvolved participants are co-configured by theinfrastructural transformation.
Articulation of infrastructural transfor-mations as unintended consequences
The conceptual framework presented above drawsattention to determining relations of communicatingand interacting with IT in health care processes. Anydisturbances and interruptions in these ongoing pro-cesses produce contingencies that will need renewedattention and possible articulation in order to be dealtwith accordingly to ensure more deliberate and desir-able outcomes. The presented qualitative evaluationstudies of IT implementations are identifications andarticulations of such transformations in health care asunintended consequences. Furthermore, putting thenine types of UAC w11x back into context by theconceptual framework of infrastructural transformationfrom IT implementation gives the ‘picture’ as present-ed in Table 3.
Such unintended consequences of IT implementationon health care infrastructure open up for renewalreflection on IT strategies in health care, and add onto the many tasks of the capital projects implementingthe systems.
Discussion: supporting articula-tion work for redesigning IT inhealth care processes
Finally, due to its integrated nature, infrastructure isonly visible upon breakdown. Unintended conse-quences from IT implementations can therefore alsobe interpreted as disclosure of infrastructure, framingthe communicative relations, spatial and temporal,
differently. The conceptual framework for drawingattention to relational turning points for communicationand interacting with IT in health care processesintends to support the articulation work and negotiationof health care infrastructure. The identification of userexperiences of interruptions, discontinuities and socio-technical problems are of central value to the overallpatient safety and professional dependability of ITsystems in health care. The screening for errors andarticulation of unintended consequences deliveressential feedback to the implementers for customiz-ation of the system. Furthermore, the results andresearch purpose of this paper are not to generalizeinfrastructural changes a priori to positive or negativeoutcomes, but to develop a language to address futureinfrastructural changes as situations and moments thatare sensitive to adjustments and renegotiation of theIT system and the work practices in question.
Conclusion
The pervasive role of IT systems as change agents inDanish health care can therefore be seen as paradox-ical. IT implementation not only implies potential forchange of the existing infrastructure, but also forundesired changes in the practices of the involvedparticipants with consequences for the understandingof health care as such. Technology infrastructure istherefore not only a point a departure for furtherlearning w46x, but also a quest for what Marc Berghas called politics of design w47x. These politics ofdesign question and negotiate the disclosed infrastruc-ture and its more or less intended transformation ofhumans as well as the techniques within. Because ofthis entangled nature of humans and techniques,Latour poses a ‘parliament of things’ w48x. Institution-alizing the negotiating and redesign of the evolvinginfrastructure from IT implementation with the clinicalusers would clearly add on to the capital project’stasks of customization. In other words, the westernneed of transforming health care infrastructures with
International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
12This article is published in a peer reviewed section of the International Journal of Integrated Care
IT can also be elaborated further from the followingquestion: to what extent are the health care organi-zations and capital projects ready to democratize w49xthe technological infrastructure with the clinical end-users, and what are the organizational means neces-sary to do so apart from project organizations’ ongoingscreening for errors?
Reviewers
Claus Bossen, Associate Professor Aarhus University,The Faculty of Humanities, Institute of Information andMedia Studies, Denmark
One anonymous reviewer
References
1. National IT-strategi for sundhedsvæsnet 2003–2007 wNational IT-strategy for Health Carex. Indenrigs- og Sundhedsmin-isteriet; 2003 May. Available from: http:yywww.sst.dkyuploadynat_itstrategi03_07.pdf. win Danishx.
2. Olesen F. Kommunikation og teknologisk mediering wCommunication and technological mediationx. In: Elsass P, OlesenF, Henriksen S, editors. Kommunikation og forstaelse. Kvalitative studier af formidling og fortolkning i sundhedssektoren.Arhus (Denmark): Philosophia; 1997. p. 143–68. win Danishx.
3. Berg M, Langenberg C, Berg I, Kwakkernaat J. Considerations for sociotechnical design: experiences with an electronicpatient record in a clinical context. International Journal of Medical Informatics 1998 Oct–Dec;52(1–3):243–51.
4. Ash JS, Berg M, Coiera E. Some unintended consequences of information technology in health care: the natureof patient care information system-related errors. Journal of the American Medical Informatics Association 2004Mar–Apr;11(2):104–12.
5. Wears RL, Berg M. Computer technology and clinical work: still waiting for Godot. The Journal of the American MedicalAssociation 2005 Mar 9;293(10):1261–3.
6. Shortliffe EH. CPOE and the facilitation of medication errors weditorialx. Journal of Biomedical Informatics 2005Aug;38(4):257–8.
7. Horsky J, Zhang J, Patel VL. To err is not entirely human: complex technology and user cognition. Journal of BiomedicalInformatics 2005 Aug;38(4):264–6.
8. Koppel R, Localio AR, Cohen A, Strom B. Neither panacea nor black box: responding to three Journal of BiomedicalInformatics papers on computerized physician order entry systems. Commentary. Journal of Biomedical Informatics 2005Aug;38(4):267–9.
9. Star SL, Ruhleder K. Steps toward an ecology of infrastructure: design and access for large information spaces.Information Systems Research 1996 Mar;7:111–34.
10. Hanseth O. The economics of standards. In: Ciborra CU, Braa K, Cordella A, Dahlbom B, Failla A, Hanseth O, et al.,editors. From control to drift: the dynamics of corporate information infrastructures. New York: Oxford University Press;2000. p. 56–70.
11. Cambell EM, Sittig, DF, Ash JS, Guappone KP, Dykstra RH. Types of unintended consequences related to computerizedprovider order entry. Journal of the American Medical Informatics Association 2006 Sep–Oct;13(5):547–56.
12. Gross PA, Bates DW. A pragmatic approach to implementing best practices for clinical decision support systems incomputerized provider order entry systems. Journal of the American Medical Informatics Association 2007 Jan–Feb;14(1):25–8.
13. Star SL, Strauss A. Layers of silence, arenas of voice: the ecology of visible and invisible work. Computer supportedcooperative work (CSCW) 1999 Mar;8(1–2):9–30.
14. Kaplan B, Shaw NT. Future directions in evaluation research: people, organizational and social issues. Methods ofInformation in Medicine 2004;43(3):215–31.
15. Ammenwerth E, de Keizer D. An inventory of evaluation studies of information technology in health care trends inevaluation research 1982–2002. Methods of Information in Medicine 2005;44(1):44–56.
16. Leroy N, Beuscart MC. Consequence of including final users in a usability evaluation: a case study with a CPOE. In:Bertelsen P, Elkin PL, Madsen I, Nøhr C, editors. Human factors engineering in health informatics. Proceedings of thesecond HFE conference; 2007 Jun 7–8; Aarhus University Hospital, Skejby, Denmark. Aalborg (Denmark): Virtual Centrefor Health Informatics; 2007. p. 24–25. Available from: http:yywww.hfeinhi2007.orgy.
17. Classen DC, Avery AJ, Bates DW. Evaluation and certification of computerized provider order entry systems. Journal ofthe American Medical Informatics Association 2007 Jan–Feb;14(1):48–55.
18. Turner JW. Telemedicine: expanding health care into virtual environments. In: Thompson T, Dorsey A, Miller K, ParrotR, editors. Handbook of health communication. New Jersey: Lawrence Erlbaum Associates; 2003. p. 515–35.
19. Yin RK. Case study research: design and methods. 2nd ed. Thousand Oaks: Sage Publication Inc; 1994.20. Kvale S. InterViews: an introduction to qualitative research interviewing. Thousand Oaks California: Sage Publications
Inc; 1996.21. Kristiansen S, Kroghstrup HK. Deltagende observation: introduktion til en samfundsvidenskabelig metode wParticipant
Observationx. Copenhagen (Denmark): Hans Reitzel Forlag; 2005. wIn Danishx.
International Journal of Integrated Care – Vol. 7, 14 November 2007 – ISSN 1568-4156 – http://www.ijic.org/
13This article is published in a peer reviewed section of the International Journal of Integrated Care
22. Westbrook J. Georgiou A. Multi-method evaluation of the impact of clinical information systems. In: Hejlesen O, Nøhr C,editors. SHI 2005, Proceedings of the 3rd Scandinavian Conference on Health Informatics; 2005 August 25–26; AalborgUniversity, Denmark. Aalborg (Denmark): Virtual Centre for Health Informatics; 2005. p. 81.
23. Mol A. The body multiple: ontology in medical practice. Durham (NC): Duke University Press; 2002. (Science and CulturalTheory).
24. Edwards PN. Infrastructure and modernity: force, time, and social organization in the history of sociotechnical systems.In: Misa TJ, Brey P, Feenberg A, editors. Modernity and technology. Cambridge, MA: MIT Press; 2003. p. 187–225.
25. Latour B. On technical mediation—philosophy, sociology, genealogy. Common Knowledge 1994;3(2):29–64.26. Nielsen J. Usability engineering. Boston: Academic Press Professional; 1993.27. Bateson G. Steps to an ecology of mind. Chicago, London: The University of Chicago Press; 2000.28. Cole M, Engestrom E. A cultural-historical approach. In: Salomon G, editor. Distributed cognitions. Cambridge (UK):
Cambridge University Press; 1993. p. 1–46.29. Kuutti K. Activity theory as a potential framework for human computer interaction. In: Nardi BA, editor. Context and
consciousness. Cambridge: MIT Press, 1995. p. 17–44. Available from: http:yywww.dwr.bth.seykari_kuutti%20Nardi_book.pdf.
30. ‘‘The Oath’’. In: Lloyd GER, editor. Hippographic writings. London: Penguin Books; 1983. p. 67.31. Arendt H. The human condition. Chigago, London: The University of Chicago Press; 1998.32. Dunne J. Back to the rough ground: practical judgement and the lure of technique. Indiana: Notre Dame Press; 1993.33. Nussbaum M. The fragility of goodness. New York, Cambridge: Cambridge University Press; 1986.34. Polkinghorne D. Practice and the human sciences: the case for a judgment-based practice of care. New York: State
University of New York Press; 2004. (SUNY series in the philosophy of the social sciences).35. Toulmin S. Introduction. In: Toulmin S, Gustavsen B, editors. Beyond theory: changing organisations through participation.
AmsterdamyPhiladelphia: John Benjamins Publishing Company; 1996. p. 1–4.36. Wentzer H, Bygholm A. IT-implementering som læreproces wIT-implementation as learning processesx. Aalborg (Denmark):
Aalborg University; 2001. (V-CHI tech report 01-1). win Danishx.37. Bygholm A. Communicating across sectors in health care: a case of establishing new infrastructure. In: Kanstrup AM,
Nyvang T, Sørensen EM, editors. Digital governing. Aalborg (Denmark): Aalborg University Press; 2007. p. 171–92.38. Bygholm A, Boisen E. Implementering og informatisering wImplementation and Informatingx. In: Dirckinck-Holmfeld L,
Dalum B, Ulrich J, Boisen B, editors. Det Digitale Nordjylland—IKT og omstilling til netværkssamfundet wDigital NorthDenmark—ICT and change to network societyx. Aalborg (Denmark): Aalborg Universitetsforlag; 2004. p. 209–44. winDanishx.
39. Wentzer H, Bygholm A. Disclosure of infrastructure in health care. In: Hejlesen O, et al. editors. SHI2006, Proceedingsof the 4th Scandinavian Conference on Health Informatics; Aalborg University; August 24–26, 2006. Aalborg (Denmark):Virtual Centre for Health Informatics; 2006. p. 74.
40. Indberetning af utilsigtede hændelser relateret til EPJ. Arhus Amts auditrapport, wIncident reporting of unintendedconsequences in the electronic patient record. Audit-report of Hospital Owners in Aarhus Countyx. Aarhus (Denmark):Aarhus Amt; Mar 21 2005. win Danishx.
41. Bottger U. Medicinmodulet i medicineringsprocessen wCPOE in the Medication Processx. wthesisx. Aalborg (Denmark):Aalborg University; 2005. Available from: http:yyprojekter.aau.dkyprojekteryresearchymedicinmodulet_og_medicineringsprocessen(6979138)y. win Danishx.
42. Wentzer H, Bottger U, Boye N. A socio-technical study of a ubiquitous CPOE-system in local use. In: Ubiquity:technologies for better health in aging societies: Proceedings of MIE2006, Medical Informatics of Europe. Amsterdam:IOS Press; 2006. p. 326–32. (Technology and Informatics; 124).
43. Schuback, MSC. The knowledge of attention. International Journal of Qualitative Studies on Health and Well-being 2006Sep;1(3):133–40. Available from: http:yywww.tandf.noyqhw.
44. BEK Nr. 116 af 23y02y2004, § 1, stk. 3, og § 4, stk. 2, i lov nr. 429 af 10. juni 2003 om patientsikkerhed isundhedsvæsenet wDeclaration 116, in the Danish Law, no. 429, June 10 2003, §1,3 and §4,2 on Patient Safetyx.Available from: http:yywww.retsinfo.dkyDELFINyHTMLyB2003y0101805.htm. win Danishx.
45. Arsrapport 2006—DPSD Dansk PatientSikkerhedsDatabase wYearly report from the Danish Patient Security Databasex.Copenhagen (Denmark); Sundhedsstyrelsen; Mar 2007. Available from: http:yywww.sst.dkypublyPubl2007yEFTyDPSD_aarsrapportyDSPDaarsrap2006.pdf. win Danishx.
46. Engestrom Y. Developmental work research as educational research: looking ten years back and into the zone ofproximal development. Nordisk Pedagogik: Journal of Nordic Educational Research 1996;16(3):131–43.
47. Berg M. The politics of technology: on bringing social theory into technological design. Science, Technology and HumanValues 1998;23(4):456–90.
48. Latour B. We have never been modern. Cambridge (MA): Harvard University Press; 1993.49. Ehn P. Work-oriented design of computer artifacts. Falkoping, Sweden: Arbejdsliv Centrum, Hillsdale, NJ: Lawrence
Erlbaum Associates;1988.