are cognitive outcome and recovery different in civilian penetrating versus non-penetrating brain...
TRANSCRIPT

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Ylioja, Shelley]On: 5 October 2010Access details: Access Details: [subscription number 927599200]Publisher Psychology PressInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
The Clinical NeuropsychologistPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713721659
Are Cognitive Outcome and Recovery Different in Civilian PenetratingVersus Non-Penetrating Brain Injuries?Shelley Yliojaa; Robin Hanksa; Anne Bairda; Scott Millisa
a University of Windsor, Ontario, Canada
First published on: 29 September 2010
To cite this Article Ylioja, Shelley , Hanks, Robin , Baird, Anne and Millis, Scott(2010) ' Are Cognitive Outcome andRecovery Different in Civilian Penetrating Versus Non-Penetrating Brain Injuries?', The Clinical Neuropsychologist, 24:7, 1097 — 1112, First published on: 29 September 2010 (iFirst)To link to this Article: DOI: 10.1080/13854046.2010.516021URL: http://dx.doi.org/10.1080/13854046.2010.516021
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

The Clinical Neuropsychologist, 24: 1097–1112, 2010
http://www.psypress.com/tcn
ISSN: 1385-4046 print/1744-4144 online
DOI: 10.1080/13854046.2010.516021
ARE COGNITIVE OUTCOME AND RECOVERYDIFFERENT IN CIVILIAN PENETRATING VERSUSNON-PENETRATING BRAIN INJURIES?
Shelley Ylioja, Robin Hanks, Anne Baird, and Scott MillisUniversity of Windsor, Ontario, Canada
The present study sought to determine whether cognitive outcome and course of recovery
in civilian penetrating brain injury due to gunshot can be distinguished from that of non-
penetrating brain injury due to motor vehicle accident. Matched survivors of penetrating
and non-penetrating brain injury were assessed with a brief neuropsychological test battery
at inpatient rehabilitation, 1 year post-injury, and 2 years post-injury. The traumatic brain
injury groups were found to have patterns of performance marked by reliably distinct
differences in isolated areas, with different cognitive predictors of brain injury type present
in early versus later recovery. The degree of recovery over the first 2 years appeared to be
quite similar for penetrating and non-penetrating injuries.
Keywords: Penetrating traumatic brain injury; Non-penetrating traumatic brain injury; Cognition.
INTRODUCTION
The nature of a traumatic brain injury (TBI), whether it is penetrating or non-penetrating, may be of importance in cognitive outcome. Whereas numerous studieshave examined cognitive outcome (e.g., Fork et al., 2005; Hellawell, Taylor, &Pentland, 1999; McKinlay & Watkiss, 1999; Salmond & Sahakian, 2005; Scheid,Walther, Guthke, Preul, & von Cramon, 2006) and course of recovery (Christensenet al., 2008; Millis et al., 2001; Schretlen & Shapiro, 2003) following non-penetratingbrain injury, research on penetrating brain injury is limited, particularly in thecivilian population. In addition, no study has directly compared cognitive outcomein these civilian TBI subtypes. The current study compared cognitive outcome andcourse of recovery in civilian survivors of penetrating TBI due to a gunshot woundand non-penetrating TBI due to a motor vehicle accident (MVA). The purpose wasto provide clinicians with knowledge of distinctions in expected cognitive outcomein these two groups.
Mechanism of injury in non-penetrating and penetrating TBI
A different mechanism of injury accounts for penetrating and non-penetratingbrain injuries; thus differing cognitive outcome might also be expected. The primary
The Clinical Neuropsychologist, 24: 1097–1112, 2010
http://www.psypress.com/tcn
ISSN: 1385-4046 print/1744-4144 online
DOI: 10.1080/13854046.2010.516021
ARE COGNITIVE OUTCOME AND RECOVERYDIFFERENT IN CIVILIAN PENETRATING VERSUSNON-PENETRATING BRAIN INJURIES?
Shelley Ylioja, Robin Hanks, Anne Baird, and Scott MillisUniversity of Windsor, Ontario, Canada
The present study sought to determine whether cognitive outcome and course of recovery
in civilian penetrating brain injury due to gunshot can be distinguished from that of non-
penetrating brain injury due to motor vehicle accident. Matched survivors of penetrating
and non-penetrating brain injury were assessed with a brief neuropsychological test battery
at inpatient rehabilitation, 1 year post-injury, and 2 years post-injury. The traumatic brain
injury groups were found to have patterns of performance marked by reliably distinct
differences in isolated areas, with different cognitive predictors of brain injury type present
in early versus later recovery. The degree of recovery over the first 2 years appeared to be
quite similar for penetrating and non-penetrating injuries.
Keywords: Penetrating traumatic brain injury; Non-penetrating traumatic brain injury; Cognition.
INTRODUCTION
The nature of a traumatic brain injury (TBI), whether it is penetrating or non-penetrating, may be of importance in cognitive outcome. Whereas numerous studieshave examined cognitive outcome (e.g., Fork et al., 2005; Hellawell, Taylor, &Pentland, 1999; McKinlay & Watkiss, 1999; Salmond & Sahakian, 2005; Scheid,Walther, Guthke, Preul, & von Cramon, 2006) and course of recovery (Christensenet al., 2008; Millis et al., 2001; Schretlen & Shapiro, 2003) following non-penetratingbrain injury, research on penetrating brain injury is limited, particularly in thecivilian population. In addition, no study has directly compared cognitive outcomein these civilian TBI subtypes. The current study compared cognitive outcome andcourse of recovery in civilian survivors of penetrating TBI due to a gunshot woundand non-penetrating TBI due to a motor vehicle accident (MVA). The purpose wasto provide clinicians with knowledge of distinctions in expected cognitive outcomein these two groups.
Mechanism of injury in non-penetrating and penetrating TBI
A different mechanism of injury accounts for penetrating and non-penetratingbrain injuries; thus differing cognitive outcome might also be expected. The primary
Address correspondence to: Shelley Ylioja, University of Windsor, Windsor, Ontario N9A 5L1,
Canada. E-mail: [email protected]
Accepted for publication: August 5, 2010. First published online: September 27, 2010
� 2010 Psychology Press, an imprint of the Taylor & Francis group, an Informa business
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

cause of moderate to severe non-penetrating TBI is MVAs and the main mechanismof injury is diffuse axonal injury (DAI), caused by axonal stretching and tearingduring acceleration, deceleration, and rotational forces on brain matter (Gaetz,2004) which initiates a series of events within axons leading to white matter damage,myelin loss, and gliosis (Povlishock, 1992). Injury is multi-focal, occurring mainly incortical gray–white matter junctions, subcortical white matter, corpus callosum, andthe brain stem (Adams, Mitchell, Graham, & Doyle, 1977; Gaetz, 2004). DAI inmoderate to severe TBI following a MVA is also often accompanied by contusion,hematoma, and hemorrhage (Smith, Meaney, & Shull, 2003).
Penetrating brain injury in civilian and military populations, on the other hand,is typically caused by gunshot wounds and the injury is more focal in nature. Injuryto the brain matter tends to involve a 2- to 4-mm radius surrounding the area ofpenetration (Oehmichen, Meissner, & Konig, 2001), with some variation dependingon mass, velocity, and shape of the object (‘‘Management and Prognosis . . . ’’,2001). Although not usually associated with penetrating TBI, evidence of some DAIin these cases has been found (Gaetz, 2004; Oehmichen et al., 2001).
Cognitive outcome in non-penetrating and penetrating TBI
No comparisons of cognitive outcome in penetrating versus non-penetratingTBI in a civilian sample have been published. Two studies using military sampleswere found (Black, 1973; Grosswasser et al., 2002). All penetrating injuries weresustained in combat in both studies. Non-penetrating injuries were from MVA orother blunt injury in Grosswasser and colleagues (2002) study, whereas the contextof non-penetrating injuries was not specified in Black’s (1973) study. Black (1973)found overall intellectual and memory functioning to be significantly better in thepenetrating TBI group at approximately 3 months post-injury. Grosswasser et al.,(2002) found no difference in general cognitive functioning between Vietnamveterans who had sustained a penetrating or a non-penetrating head injury 12 to14 years earlier. These two groups also showed a similar amount of change frompre-injury assessment. Taken together, the results of these studies may suggest thatmore global deficits are present following non-penetrating brain injury at 3 monthspost-TBI, with such a difference in general cognitive outcome no longer existingseveral years post-injury, at least in military samples. However, the similarity ofinjury severity in these two studies is unclear and neither study included scores inspecific domains of cognition.
Non-penetrating TBI. The most commonly reported cognitive deficits inmoderate to severe TBI include processing speed, attention, and some aspects ofmemory (Fork et al., 2005; Hellawell et al., 1999; Madigan, DeLuca, Diamond,Tramontano, & Averill, 2000; Mathias & Wheaton, 2007; McKinlay & Watkiss,1999; Rios, Perianez, & Munoz-Cespedes, 2004; Scheid et al., 2006; Zahn & Mirsky,1999). While some have reported evidence of impairment in complex attention andexecutive function as well (Fork et al., 2005; Mathias & Wheaton, 2007; Rios et al.,2004; Salmond & Sahakian, 2005; Scheid et al., 2006), others have argued that thesedeficits may result from underlying problems in processing speed and basicattention (Felmingham, Baguley, & Green, 2004). Whereas some studies specify that
1098 SHELLEY YLIOJA ET AL.
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010
the participants have experienced a non-penetrating injury, others do not explicitlyaddress the type of TBI. While it is thus possible that some of these investigationsmay have included both non-penetrating and penetrating brain injuries, it can beassumed that the majority of participants sustained non-penetrating injuries giventhe lower survival rate following a penetrating TBI.
Research examining time course of recovery in moderate to severe TBI hasgenerally revealed that the most rapid cognitive recovery occurs during the first5 months (Christensen et al., 2008) with recovery continuing between 6 months to2 years post-injury (Schretlen & Shapiro, 2003), and some further improvement stillseen at 5 years (Millis et al., 2001). Although recovery tends to occur in all affecteddomains of cognition, rate of recovery varies across domains, with slowerimprovement observed for more complex functioning (Kersel, Marsh, Havill, &Sleigh, 2001). Furthermore, cognitive function may never return to pre-injury levels.For example, aspects of attention, processing speed, memory, and executivefunction have still been found to be significantly lower than normal controls at10 years post-injury (Draper & Ponsford, 2008).
Penetrating TBI. Because of the high mortality rate following a penetratingbrain injury (‘‘Management and Prognosis . . . ’’, 2001) research examining cognitiveoutcome in civilian penetrating TBI is limited. It is assumed based on clinical loreand research with military survivors that the cognitive outcome followingpenetrating injuries in civilians differs from that of non-penetrating injuries.Moreover, compared to non-penetrating injuries, penetrating injuries are expectedto produce more varied outcomes across individuals. However, these expectationshave not been empirically tested in civilian populations.
Military survivors of penetrating injuries have been the main source ofcognitive outcome studies. However, large differences in mechanism and severityexist between military and civilian penetrating brain injuries, and thus it isimportant to study outcome in civilian penetrating TBI as a separate group(‘‘Management and Prognosis . . . ’’, 2001; Wertheimer, Hanks, & Hasenau, 2008).For instance, penetrating TBI in military samples tends to have a greater degree oftissue damage and worse neurologic outcome compared to civilian TBI as a result ofdifference in weapons (Tsuei et al., 2005). Other important factors that have beencited include military cases having a greater length of time before receiving medicalattention, high chance of wound infection in the field, and variable quality ofmedical treatment (Sapsford, 2003).
Studies of war veterans with penetrating brain injuries have generally foundlesion location and volume of the damaged tissue to be most predictive of cognitivedeficits. Long-term follow-up of war veterans 12 to 15 years post-injury revealedboth of these factors to be predictive of overall intelligence once pre-morbidintelligence had been controlled for (Grafman et al., 1988). Intelligence wasmeasured with the Armed Forces Qualification Test (AFQT), which includes fourmultiple-choice subtests: vocabulary, arithmetic word problems, object-functionmatching, and mental visuospatial construction. With respect to specific domains ofcognition, lesion location was a stronger predictor than lesion volume. In particular,poorer vocabulary and object–function matching were related to temporal andoccipital lobe damage. Follow-up at 30 or more years post-injury found overall
PENETRATING VS NON-PENETRATING TBI 1099
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

intelligence to be predicted by pre-morbid intelligence as well as total volume lossand specific lesion locations including the caudate nucleus, left parietal lobe,hippocampus, right amygdala, and right frontal lobe (Raymont et al., 2008). A20-year follow-up of 74 veterans with penetrating TBI by Corkin (1979) found thatgeneral intelligence was observed to be more impaired in left-hemispheric injuries,whereas performance on a visuoperception task was dependent on volume of injury,irrespective of hemisphere. Alternately, while Black (1974) also found hemisphere tobe of importance, his analysis revealed that veterans with right-hemispheric lesionshad significantly lower performance on all Wechsler Adult Intelligence Scale(WAIS) subtests compared to controls whereas those with left-hemispheric lesionswere only significantly lower than controls on three subtests. Of note, these militarystudies are all long-term follow-ups and little is known of cognitive outcome in thefirst months to years following penetrating TBI even in military samples.
Only two studies examining cognitive function in civilian penetrating braininjury were found. The first studied four adults and two children 1 year post-injury(Kaufman et al., 1985). Verbal and non-verbal long-term memory, visuospatial andvisuoconstruction ability, motor skill, somatosensory function, and overallintellectual function were examined. No statistical analysis was conducted, butthe authors concluded that location (hemisphere) of injury was related to cognitivedeficits with verbal and visuospatial impairments related to left and righthemisphere lesions, respectively. The other civilian study examined verbalmemory functioning of 10 individuals with moderate to severe penetrating braininjury within 6 months of injury (Millis & Ricker, 1995). This group demonstratedimpairment in most aspects of learning and memory alongside relatively intactstorage, with no differentiation based on hemisphere of lesion. However, theauthors hypothesized that lesion location may differentiate deficits among people ina larger sample. These two studies considered together offer no conclusionregarding the pattern of cognitive deficits observed following civilian penetratingbrain injury.
CURRENT STUDY
The Southeastern Michigan Traumatic Brain Injury System (SEMTBIS)project, which examines outcome in TBI, includes a comparatively high number ofsurvivors of brain injury due to gunshot wound, allowing a sufficient sample size ofcivilian penetrating brain injuries in which to study cognitive outcome. The currentstudy compared cognitive outcome and recovery in survivors of penetrating TBIdue to gunshot wound and non-penetrating TBI due to MVA using neuropsycho-logical test results from three time points: inpatient rehabilitation, 1 year post-injury, and 2 years post-injury. The goal was to clarify whether there are significantdifferences in cognitive outcome and course of cognitive recovery between thesesubtypes of TBI.
It was hypothesized that there would be different patterns of cognitive deficitsin penetrating and non-penetrating TBI (Hypothesis 1). The non-penetrating injurygroup was expected to show more deficits in processing speed and attentioncompared to the penetrating injury group, given that DAI is the main mechanism ofinjury. The penetrating injury group, on the other hand, was expected to have more
1100 SHELLEY YLIOJA ET AL.
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

focal deficits, given the focal nature of the injury. However, such focal deficitswould vary within the penetrating group depending on location of injury, and it wasexpected that examination of the penetrating group as a whole would fail to showa particular pattern of deficit. Thus the hypothesized group difference was that thenon-penetrating TBI group would have poorer attention and processing speed thanthe penetrating TBI group. It was further hypothesized that the groups would showa similar degree of recovery in cognitive function over time (Hypothesis 2).Recovery across the first 2 years post-injury has been demonstrated in non-penetrating TBI. No studies were found examining course of recovery in penetratingTBI, but it might be expected that recovery would occur in this group as well.
METHOD
Participants
Survivors of penetrating brain injury due to gunshot (n¼ 61) and non-penetrating brain injury due to motor vehicle accident (n¼ 61) were drawn from anarchival database composed of traumatic brain injury cases admitted to an urbanmedical center between 1992 and 2008 who had agreed to participate in themulticenter TBI Model System project funded by the National Institute onDisability and Rehabilitation Research. All penetrating TBI cases due to gunshotwound in this project database that had neuropsychological test data for one ormore of the time points of interest were included. Random case selection in SPSSwas used to choose a subset of an equal number of MVA TBI cases that did notdiffer significantly from the penetrating TBI group on age, t(120)¼ 1.08, p¼ .28,education level—categories: �8 years, 9–11 years, 12 years, some college/Associate’sdegree (13–15 years), Bachelor’s degree (16 years); �2(1,N¼ 121)¼ 4.14, p¼ .39—and injury severity as measured by post-traumatic amnesia (PTA) length,t(101)¼�0.03, p¼ .98. Given the frequency of missing or inaccurate initial GCSwith patients that are intubated and/or sedated at the accident scene (Gabbe,Cameron, & Finch, 2003) and the availability of consistent measurement of PTAlength during inpatient rehabilitation for all participants, length of PTA wasthought to be a better estimate to equate injury severity between groups. Significantdifferences were observed for race, �2(1,N¼ 122)¼ 7.29, p¼ .03, and sex,�2(1,N¼ 122)¼ 8.72, p¼ .00, with significantly more African American males inthe penetrating TBI group (Table 1). The majority of patients had sustained a severeTBI (85.2% of penetrating group, 88.5% of non-penetrating group), defined asPTA length of 7 or more days.
Cognitive data were obtained from a brief neuropsychological test batteryadministered during inpatient rehabilitation stay upon clearing PTA, at 1 year post-injury (year 1), and at 2 years post-injury (year 2). Inpatient rehabilitation staytypically occurred at 2 to 6 weeks post-injury for a period of 2 to 3 weeks. Of the122 participants, neuropsychological testing was administered to 101 participants atinpatient rehabilitation (50 non-penetrating, 82%; 51 penetrating, 84%), 59 at year1 (28 non-penetrating, 46%; 31 penetrating, 51%), and 58 at year 2 (23 non-penetrating, 38%; 35 penetrating, 57%). There was no significant difference in
PENETRATING VS NON-PENETRATING TBI 1101
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

injury severity between those who returned for testing at follow-up years and thosewho did not—year 1: t(101)¼ 0.152, p¼ .87; year 2: t(101)¼ 0.527, p¼ .60.
Measures
Neuropsychological tests included the Trail Making Test A & B (Trails A,Trails B; Reitan & Wolfson, 1985), the Symbol Digit Modalities Test written andoral (SDMT; Smith, 1991), Word Generation (CFL or FAS; Benton & Hamsher,1989), Grooved Pegboard (pegs; Matthews & Klove, 1964), and the CaliforniaVerbal Learning Test-II (CVLT-II; Delis, Kramer, Kaplan, & Ober, 2000) or ReyAuditory Verbal Learning Test (RAVLT; Schmidt, 1996). If a participant attemptedbut was unable to complete a particular test the lowest score obtained by a memberof the group plus one was assigned (Dikmen, Machamer, Winn, & Temkin, 1995),as opposed to having a missing score for that individual and potentiallyoverestimating the true ability of the group. This was done with Trails A, TrailsB, and/or pegs in 11 participants, for a total of 19 assigned scores. SDMT writtenand oral scores were averaged to create an overall SDMT score. Becauseparticipants tested prior to 2002 were administered the RAVLT and participantstested since 2002 were administered the CVLT-II, learning and memory scores were
Table 1 Demographic variables for entire sample by TBI group
Variable GSW MVA t p
Mean (SD) Mean (SD)
Age 27.57 (10.20) 29.97 (13.89) 1.085 0.280
PTA (days) 24.86 (21.28) 24.75 (18.59) �0.027 0.979
n (%) n (%) �2 p
Sex 8.72 0.003**
Male 50 (82) 35 (57.4)
Female 11 (18) 26 (42.6)
Race 7.29 0.027*
Caucasian 7 (11.5) 18 (29.5)
African American 51 (83.6) 38 (62.3)
Other 3 (4.9) 5 (8.2)
Education 4.148 0.386
�8th grade 6 (9.8) 2 (3.3)
9–11 27 (44.3) 25 (41)
12 18 (29.5) 24 (39.3)
13–15 10 (16.3) 8 (13.2)
16 0 (0) 1 (1.6)
Missing 0 (0) 1 (1.6)
Injury Severity
Mild complicated 6 (9.8) 2 (3.3)
Moderate 2 (3.3) 5 (8.2)
Severe 52 (85.2) 54 (88.5)
Missing 1 (1.6) 0 (0)
*p5 .05, **p5 .01, GSW¼ gunshot wound, MVA¼motor vehicle accident,
PTA¼ post-traumatic amnesia.
1102 SHELLEY YLIOJA ET AL.
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010
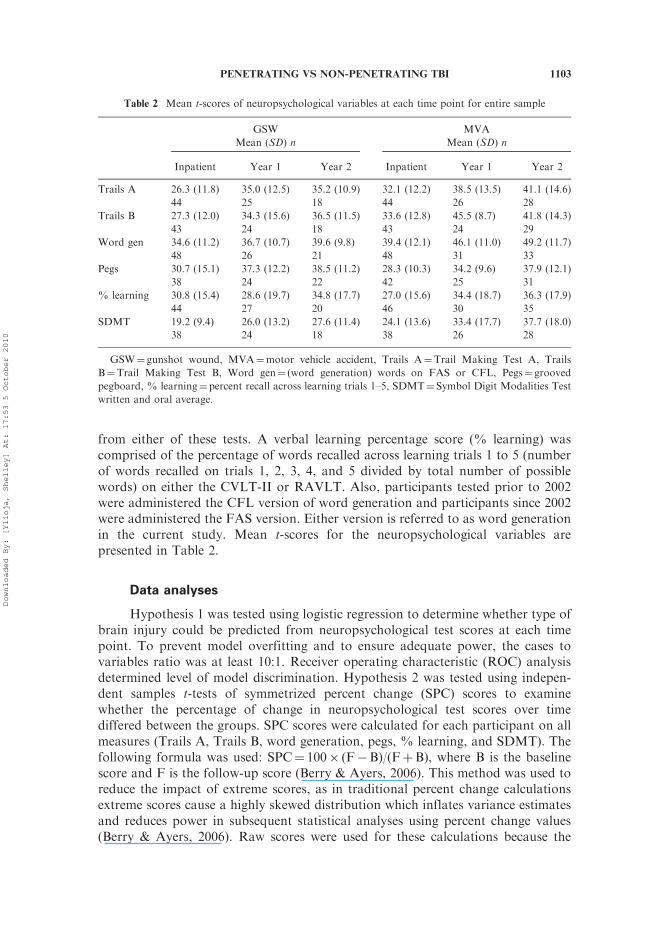
from either of these tests. A verbal learning percentage score (% learning) wascomprised of the percentage of words recalled across learning trials 1 to 5 (numberof words recalled on trials 1, 2, 3, 4, and 5 divided by total number of possiblewords) on either the CVLT-II or RAVLT. Also, participants tested prior to 2002were administered the CFL version of word generation and participants since 2002were administered the FAS version. Either version is referred to as word generationin the current study. Mean t-scores for the neuropsychological variables arepresented in Table 2.
Data analyses
Hypothesis 1 was tested using logistic regression to determine whether type ofbrain injury could be predicted from neuropsychological test scores at each timepoint. To prevent model overfitting and to ensure adequate power, the cases tovariables ratio was at least 10:1. Receiver operating characteristic (ROC) analysisdetermined level of model discrimination. Hypothesis 2 was tested using indepen-dent samples t-tests of symmetrized percent change (SPC) scores to examinewhether the percentage of change in neuropsychological test scores over timediffered between the groups. SPC scores were calculated for each participant on allmeasures (Trails A, Trails B, word generation, pegs, % learning, and SDMT). Thefollowing formula was used: SPC¼ 100� (F�B)/(FþB), where B is the baselinescore and F is the follow-up score (Berry & Ayers, 2006). This method was used toreduce the impact of extreme scores, as in traditional percent change calculationsextreme scores cause a highly skewed distribution which inflates variance estimatesand reduces power in subsequent statistical analyses using percent change values(Berry & Ayers, 2006). Raw scores were used for these calculations because the
Table 2 Mean t-scores of neuropsychological variables at each time point for entire sample
GSW
Mean (SD) n
MVA
Mean (SD) n
Inpatient Year 1 Year 2 Inpatient Year 1 Year 2
Trails A 26.3 (11.8) 35.0 (12.5) 35.2 (10.9) 32.1 (12.2) 38.5 (13.5) 41.1 (14.6)
44 25 18 44 26 28
Trails B 27.3 (12.0) 34.3 (15.6) 36.5 (11.5) 33.6 (12.8) 45.5 (8.7) 41.8 (14.3)
43 24 18 43 24 29
Word gen 34.6 (11.2) 36.7 (10.7) 39.6 (9.8) 39.4 (12.1) 46.1 (11.0) 49.2 (11.7)
48 26 21 48 31 33
Pegs 30.7 (15.1) 37.3 (12.2) 38.5 (11.2) 28.3 (10.3) 34.2 (9.6) 37.9 (12.1)
38 24 22 42 25 31
% learning 30.8 (15.4) 28.6 (19.7) 34.8 (17.7) 27.0 (15.6) 34.4 (18.7) 36.3 (17.9)
44 27 20 46 30 35
SDMT 19.2 (9.4) 26.0 (13.2) 27.6 (11.4) 24.1 (13.6) 33.4 (17.7) 37.7 (18.0)
38 24 18 38 26 28
GSW¼ gunshot wound, MVA¼motor vehicle accident, Trails A¼Trail Making Test A, Trails
B¼Trail Making Test B, Word gen¼ (word generation) words on FAS or CFL, Pegs¼ grooved
pegboard, % learning¼percent recall across learning trials 1–5, SDMT¼ Symbol Digit Modalities Test
written and oral average.
PENETRATING VS NON-PENETRATING TBI 1103
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

amount of change in scores rather than the actual neuropsychological test scores arecompared between the groups, and this type of comparison would not be affected bydemographic differences.
RESULTS
Hypothesis 1: Cognitive outcome
Logistic regression analysis was performed for each time point with injurytype (penetrating vs non-penetrating) as the outcome variable. Predictors used atinpatient rehabilitation included Trails B, word generation, pegs, % learning, andSDMT. The SDMT was removed for years 1 and 2 to keep the number of cases tovariables ratio at least 10:1, as there were fewer participants at the follow-up years.The SDMT was chosen to be removed because it has the most redundancy withanother test (Trails B) in terms of the cognitive domains being measured. All otherpredictor variables remained the same as at inpatient rehabilitation. Because ofgroup differences in gender and race, demographically adjusted t-scores were usedfor the logistic regression analyses. Demographically adjusted t-scores were basedon the Heaton norms (Heaton, Miller, Taylor, & Grant, 2004) for Trails B, wordgeneration, and pegs, and the norms available in the test manuals for the CVLT-II,RAVLT, and SDMT. A high level of collinearity was not detected. None of thepredictor variables had variance inflation factors exceeding 4, none of the conditionindexes was greater than 30, and none of the associated variance decompositionproportions was greater than .50. Examination of measures of influence revealedtwo influential cases at year 2, which were removed. This resulted in a sample sizeof 67 at inpatient rehabilitation (36 non-penetrating, 31 penetrating), 44 at year 1(22 non-penetrating, 22 penetrating), and 43 at year 2 (27 non-penetrating, 16penetrating).
Test of the full model against a constant-only model was statisticallyreliable at all time points, indicating that the full set of predictors (neuropsy-chological test scores) reliably discriminated between penetrating and non-penetrating TBI at inpatient rehabilitation (�2¼ 17.07, p¼ .00), year 1(�2¼ 20.46, p¼ .00), and year 2 (�2¼ 22.37, p¼ .00). The Hosmer-Lemeshowtest indicated that the model had acceptable calibration at all time points(inpatient rehabilitation¼ 6.24, p¼ .62; year 1¼ 7.67, p¼ .47; year 2¼ 6.83,p¼ .56). Model discrimination was acceptable for inpatient (area under the ROCcurve¼ 0.77, p¼ .00), excellent for year 1 (area under the curve¼ 0.86, p¼ .00),and excellent for year 2 (area under the curve¼ 0.85, p¼ .00) (Hosmer &Lemeshow, 2000). Regression coefficients, Wald statistics, odd ratios, and 95%confidence intervals for the odd ratios of each predictor are displayed in Table 3.Based on the Wald statistic, injury etiology was reliably predicted at inpatientrehabilitation by performance on SDMT, % learning, and pegs, and at years 1and 2 by performance on word generation and pegs. Specifically, performance ofthe penetrating TBI group was better for % learning and pegs and poorer forSDMT at inpatient rehabilitation, and better for pegs and poorer for wordgeneration at years 1 and 2.
1104 SHELLEY YLIOJA ET AL.
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

Hypothesis 2: Recovery over time
SPC scores quantified the amount of change in raw test scores betweeninpatient rehabilitation and year 1, years 1 and 2, and inpatient rehabilitation andyear 2. Because great variability existed in follow-up rate, and calculations ofchange over time must be conducted within an individual participant, a decreasedsample size was available for independent t-test calculations. However, it wasdecided that exploratory t-tests would still be conducted on the SPC scores toexamine differences in change over time between the penetrating and non-penetrating TBI groups on all tests, with the acknowledgement that non-significantresults may simply be a function of low power. With the exception of normality ofthree variables (SDMT inpatient rehabilitation & year 1, inpatient rehabilitation &year 2; pegs inpatient rehabilitation & year 2; all in the non-penetrating TBI group),all variables met the assumptions for analysis by independent t-tests. T-test analysesrevealed no significant difference in SPC scores between the groups for any of thetests at any of the time points (Table 4).
Average SPC scores revealed improved performance over time in both TBIgroups for the majority of the tests. The number of penetrating TBI participantshaving test scores for all three time points was too small to allow statisticalcomparison of degree of change between inpatient rehabilitation and year 1 tochange between year 1 and year 2. However, while statistical significance is
Table 3 Logistic regression results predicting penetrating versus non-penetrating injury
Variable b (SE) Wald (df ) Signif OR 95% CI
Inpatient
Trails B �0.003 (0.027) 0.015 (1) .903 0.997 0.945–1.051
Word gen �0.041 (0.030) 1.891 (1) .169 0.960 0.905–1.018
Pegs 0.062 (0.029) 4.756 (1) .029* 1.064 1.006–1.126
% learning 0.052 (0.022) 5.897 (1) .015* 1.054 1.010–1.099
SDMT �0.077 (0.035) 4.776 (1) .029* 0.926 0.864–0.920
Constant �0.254 (1.173) 0.047 (1) .829 0.776
Year 1
Trails B �0.060 (0.040) 2.253 (1) .133 0.941 0.870–1.019
Word gen �0.147 (0.053) 7.738 (1) .005** 0.863 0.778–0.957
Pegs 0.110 (0.048) 5.266 (1) .022* 1.116 1.016–1.226
% learning 0.001 (0.024) 0.001 (1) .969 1.001 0.954–1.050
Constant 4.594 (2.043) 5.058 (1) .025* 98.911
Year 2
Trails B �0.061 (0.055) 1.220 (1) .269 0.941 0.844–1.048
Word gen �0.210 (0.073) 8.385 (1) .004** 0.811 0.703–0.934
Pegs 0.124 (0.050) 6.043 (1) .014* 1.132 1.025–1.250
% learning �0.013 (0.026) 0.254 (1) .614 0.987 0.937–1.039
Constant 6.750 (2.728) 6.125 (1) .013* 854.229
b¼ beta weight, SE¼ standard error, Wald¼Wald statistic, signif¼ significance level, OR¼odd ratio,
CI¼ confidence interval, Trails B¼Trail Making Test B, Word gen¼ (word generation) words on FAS
or CFL, Pegs¼ grooved pegboard, % learning¼ percent recall across learning trials 1–5,
SDMT¼Symbol Digit Modalities Test written and oral average, *p5 .05, **p5 .01; sample sizes:
penetrating TBI (inpatient¼ 31, year 1¼ 22, year 2¼ 16), non-penetrating TBI (inpatient¼ 36, year
1¼ 22, year 2¼ 27).
PENETRATING VS NON-PENETRATING TBI 1105
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

unknown, average SPC scores for both TBI groups were larger for inpatient
rehabilitation to year 1 than for year 1 to year 2, indicating a larger change in testscores during the former time points.
To determine the level of impairment present in each group at each time point,the percentage having a t-score in the mild impairment range (t-score¼ 30–39) andmoderate impairment range or greater (t-score5 30) on each test was calculated for
each group (Table 5). Fewer participants have scores in the impaired range withincreasing time since injury. However, a number of participants still have at leastmild or moderate impairment at 2 years post-injury.
DISCUSSION
The current study sought to determine whether there are differences betweencivilian penetrating and non-penetrating TBI in cognitive outcome and degree of
recovery within the first 2 years following injury. Results suggest that there aresignificant differences in cognitive outcome between penetrating and non-penetrating TBI, with these differences varying across time post-injury. Comparedto non-penetrating TBI, penetrating TBI was distinguished by better verbal
learning, better fine motor dexterity, and possibly poorer attention during the firstweeks post-injury, and better fine motor dexterity and poorer verbal generativity at
Table 4 Symmetrized percent change scores and t-test results
Variable Mean (SD)/n t p Effect size
Inpatient vs year 1 GSW MVA
Trails A �16.56 (26.51)/13 �21.33 (18.98)/19 0.595 .556 0.108
Trails B �17.45 (25.40)/12 �24.71 (19.45)/17 0.873 .391 0.166
Word gen 9.49 (15.44)/17 17.89 (14.14)/22 �1.768 .085 0.279
Pegs �14.23 (21.77)/13 �14.04 (17.00)/18 �0.027 .979 0.005
% learning 1.49 (20.26)/15 8.64 (16.22)/19 �1.142 .262 0.198
SDMT 16.82 (22.91)/14 13.67 (31.91)/16 0.306 .762 0.058
Inpatient vs year 2
Trails A �23.08 (29.63)/10 �19.68 (22.25)/19 �0.349 .730 0.067
Trails B �14.42 (14.93)/10 �17.74 (25.09)/19 0.383 .705 0.074
Word gen 17.61 (28.34)/14 17.53 (18.06)/23 0.011 .991 0.002
Pegs �15.63 (18.40)/11 �12.53 (20.56)/20 �0.417 .680 0.077
% learning 7.70 (12.67)/11 9.09 (17.97)/22 �0.230 .820 0.041
SDMT 19.82 (12.63)/10 21.53 (16.74)/16 �0.276 .785 0.056
Year 1 vs 2
Trails A �3.30 (21.87)/12 �2.88 (18.36)/20 �0.058 .954 0.011
Trails B �5.36 (18.31)/11 3.13 (13.74)/19 �1.444 .160 0.263
Word gen �0.61 (13.14)/15 2.22 (14.00)/26 �0.639 .526 0.102
Pegs �3.23 (9.66)/14 �1.07 (9.11)/22 �0.677 .503 0.115
% learning 2.27 (11.78)/14 0.12 (9.32)/25 0.627 .535 0.103
SDMT 4.69 (13.59)/12 3.27 (9.03)/20 0.355 .725 0.065
GSW¼ gunshot wound, MVA¼motor vehicle accident, Trails A¼Trail Making Test A, Trails
B¼Trail Making Test B, Word gen¼ (word generation) words on FAS or CFL, Pegs¼ grooved
pegboard, % learning¼percent recall across learning trials 1–5, SDMT¼Symbol Digit Modalities Test
written and oral average.
1106 SHELLEY YLIOJA ET AL.
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

1 and 2 years post-injury. Nonetheless, the degree to which patients of these TBItypes recovered over the first 2 years post-injury appeared to be quite similar.
It was hypothesized that there would be different patterns of cognitive deficitsin penetrating and non-penetrating TBI. Specifically, it was thought that the non-penetrating injury group would show more deficits in processing speed andattention, given that DAI is the main mechanism of injury. Results indicate,however, that attention abilities may actually be poorer in the penetrating group,at least within the first few weeks post-injury, as indicated by the significantcontribution to group differentiation of the SDMT at inpatient rehabilitation.However, Trails B failed to show a similar differentiation. The SDMT and Trails Btests are highly correlated (McCaffrey, Krahula, Heimberg, Keller, & Purcell, 1988),both measuring scanning and visuomotor tracking elements of attention in additionto speeded processing (Lezak, Howieson, & Loring, 2004; Strauss, Sherman, &Spreen, 2006). Thus some aspect of the SDMT not shared by Trails B seems likelyto be contributing to the current result. One possibility is the high sensitivity ofSDMT to processing speed deficits in TBI samples (Ponsford & Kinsella, 1992).Group differentiation by the SDMT but not by Trails B could therefore be anindication of poorer processing speed in the penetrating group. The SDMT wasremoved as a predictor at years 1 and 2, therefore it is unknown if it continues todifferentiate the groups beyond the first weeks post-injury. Overall, attentionabilities at 1 and 2 years post-injury appear to be more similar between the groups
Table 5 Percentage of entire sample with impaired test scores at each time point
Inpatient Year 1 Year 2
t¼ 30–39 t5 30 n t¼ 30–39 t5 30 n t¼ 30–39 t5 30 n
Trails A
GSW 18.1 61.4 44 32.0 32.0 25 16.7 38.9 18
MVA 29.6 38.6 44 7.7 38.5 26 14.3 25.0 28
Trails B
GSW 30.2 55.8 43 16.7 45.8 24 33.3 27.8 18
MVA 30.2 41.9 43 25.0 4.2 24 23.9 17.2 29
Word gen
GSW 22.9 37.5 48 30.8 26.9 26 42.9 9.5 21
MVA 37.5 16.7 48 25.8 3.2 31 9.1 6.1 33
Pegs
GSW 34.2 47.4 38 41.7 25.0 24 31.8 27.3 22
MVA 33.4 57.1 42 40.0 32.0 25 41.9 22.6 31
% learning
GSW 27.3 47.7 44 26.0 48.1 27 10.0 50.0 20
MVA 28.3 50.0 46 26.7 40.0 30 17.1 40.0 35
SDMT
GSW 10.6 86.8 38 20.8 66.7 24 38.9 50.0 18
MVA 15.7 71.1 38 23.0 38.5 26 14.3 39.3 28
GSW¼ gunshot wound, MVA¼motor vehicle accident, t¼ 30–39¼% of sample with mild
impairment, t5 30¼% of sample with moderate impairment or greater, Trails A¼Trail Making Test
A, Trails B¼Trail Making Test B, Word gen¼ (word generation) words on FAS or CFL, Pegs¼ grooved
pegboard, % learning¼percent recall across learning trials 1–5, SDMT¼Symbol Digit Modalities
Test written and oral average.
PENETRATING VS NON-PENETRATING TBI 1107
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010
than expected, and it is unclear whether some aspect of attention is more affected inpenetrating TBI early on in recovery.
Initial learning of verbal information by the penetrating TBI group is superiorto that of the non-penetrating TBI group at baseline testing. However, close to 50%of both groups had a verbal learning score in the moderate impairment range orlower. Initial learning tends to be affected following a non-penetrating TBI(McKinlay & Watkiss, 1999; Scheid et al., 2006), and the current results suggest thatis also affected following a penetrating TBI although to a lesser extent. The presenceof impairment in verbal learning following penetrating injury is in line with thefindings of Millis and Ricker (1995) in which testing completed within 6 months ofa penetrating injury revealed substantial impairment in initial learning of verbalinformation. Absence of continuing differences between the groups at years 1 and 2suggests that better verbal learning by the penetrating TBI group is only present inthe first few months post-injury.
It appears that fine motor dexterity is more affected following non-penetratingTBI and continues to be poorer than in penetrating TBI cases even 2 years later.Impaired performance on pegs has been previously reported following mildcomplicated to severe non-penetrating TBI (Millis et al., 2001). This task requirescomplex coordinated motor skills involving sequencing and rapid integration ofinformation from several modalities (Greiffenstein, Baker, & Gola, 1996). Theseauthors speculated that the high frequency of frontal damage in TBI might accountfor complex motor skill compromise in TBI.
The penetrating TBI group was also distinguished by lower word generationat years 1 and 2 post-injury. Impaired verbal generativity has been observed in non-penetrating TBI and has been noted by Kersel et al. (2001) and by Ruff and Evans(1986) to show little improvement over time. These authors speculated that verbalgenerativity difficulties in TBI result from inflexibility of information processing,evidenced by failure to create, maintain, and/or switch strategies that are typicallyused to aid in generating more words. Although information regarding strategy wasnot available in the current study due to the archival nature of the data, the findingssuggest that this ability may show even less recovery following a penetrating TBI.
It is generally accepted that penetrating TBI results in greater variability ofcognitive outcome across survivors than does non-penetrating TBI, due to theinfluence of injury location. However, the separable patterns of test performanceobserved between the groups in the current sample suggest that those survivinga penetrating TBI share more cognitive sequelae than has been previously thought,even without accounting for injury location. Classification of the penetrating injurygroup based on pattern of neuropsychological test performance was high at alltime points (inpatient rehabilitation¼ 71.0%, year 1¼ 68.2%, year 2¼ 81.2%).Although these rates are approximately 10% lower at each time point than in thenon-penetrating TBI group, they are still quite good. Of course, it is possible thatlocation of injury in the penetrating TBI group may have dictated the pattern ofresults in the current study. However, analysis of the influence of injury locationwas precluded in the current study, due to lack of imaging data for a large portionof the group. It is recommended that future research examine this possibility.
Irrespective of differences in some aspects of cognition that exist between thegroups, results of the current study suggest that the degree to which patients recover
1108 SHELLEY YLIOJA ET AL.
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

over time within the first 2 years post-injury may be similar regardless of whetherthe injury was penetrating or non-penetrating. Improvement was evident in bothgroups between all time points for the majority of the tests. Because the t-test resultsare limited by small sample size, it is possible that the lack of statistically significantdifference in degree of recovery between the groups was simply due to low power.
Results suggest that the greatest amount of improvement in both groupsoccurs during the first year post-injury, with recovery slowing down but still presentduring the second year post-injury. This is in line with previous research in non-penetrating TBI (Christensen et al., 2008; Schretlen & Shapiro, 2003). However,although improvement is evident over time in both groups, many individuals stillshow some degree of impairment at years 1 and 2.
A major limitation of the current study was that the entire sample was not ableto be used in the logistic regression or SPC analyses because participants were notalways available for testing at all time points and those who were tested were notalways administered all of the measures. Possible reasons for participants not beingtested at all time points include being lost to follow-up due to telephone/addresschange, death, incarceration, or lack of interest in continued participation. Reasonsthat the complete battery was not always administered include motor/visual/verbalimpairments, refusal to complete certain tests, or time constraints. For the logisticregression analyses we were interested in examining performance in participantswho completed all of the measures at that time point to allow a more accuraterepresentation of cognitive outcome, resulting in smaller than expected sample sizes.Moreover, because the logistic regression analyses were not comprised of identicalparticipant samples across time points (year 1: 50% of sample same as inpatientrehabilitation; year 2: 47% same as inpatient rehabilitation, 65% same as year 1),observed differences between early and late outcome may at least partially reflectthis. In addition to the lower number of participants included in the analyses, smallsample size also limited the number of neuropsychological test variables that couldbe included as predictors in the logistic regression analyses. It is possible that therewould be differences between the groups on the other measures as well. Therelatively small battery of neuropsychological tests administered may also beregarded as a limitation, as some aspects of cognitive functioning that could be ofimportance in distinguishing the groups may not have been assessed. However,there is research to show that this brief battery is clinically useful as well aspredictive of outcome at one year post-injury (Hanks et al., 2008; Kalmar et al.,2008). SPC analyses examining change between two time points included onlyindividuals who had been tested at both times to allow a more accuraterepresentation of cognitive recovery over time. This examination of change withinindividuals rather than with group means resulted in smaller than expected samplesizes for these analyses as well. Another potential limitation is that this study wasconducted in an inner city urban rehabilitation center, with the demographics of thesample reflecting this. For example, although education level was matched betweenthe groups, the level of education in the current sample is low. Therefore the sampledemographics may limit generalization of the findings. Despite these limitations, thecurrent study is the first to do a comparison of cognitive outcome and recoveryfollowing penetrating versus non-penetrating TBI in a civilian population, and thusthe results are still quite valuable.
PENETRATING VS NON-PENETRATING TBI 1109
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

As clinical expectations regarding cognitive outcome in penetrating TBI stilltend to be based on case studies and clinical lore rather than on research, in contrastto non-penetrating TBI, the current findings begin to fill a gap in clinical literature.Using a brief neuropsychological test battery, civilians with penetrating TBI due togunshot and those with non-penetrating TBI due to MVA who underwent inpatientrehabilitation were found to have reliably distinct differences in pattern of cognitiveperformance. Furthermore, these areas of difference changed over the course ofrecovery. In contrast, the degree of recovery over the first 2 years post-injury may besimilar for penetrating and non-penetrating TBI, with the greatest amount ofrecovery occurring during the first year.
ACKNOWLEDGMENT
This project was partially supported by NIDRR grant #H133A080044-09,which funds the SEMTBIS project through the TBIModel Systemmulticenter study.
REFERENCES
Adams, J. H., Mitchell, D. E., Graham, D. I., & Doyle, D. (1977). Diffuse brain damage of
immediate impact type: Its relationship to primary brain stem damage in head injury.Brain, 100, 489–502.
Benton, A. L., & Hamsher, K. (1989).Multilingual Aphasia Examination. Iowa City, IA: AJAAssociates.
Berry, D. A., & Ayers, G. D. (2006). Symmetrized percent change for treatment comparisons.The American Statistician, 60, 27–31.
Black, F. M. (1973). Cognitive and memory performance in subjects with brain damagesecondary to penetrating missile wounds and closed head injury. Clinical Psychology, 29,141–142.
Black, F. M. (1974). Cognitive effects of unilateral brain lesions secondary to penetrating
missile wounds. Perceptual and Motor Skills, 38, 387–391.Christensen, B. K., Colella, B., Inness, E., Hebert, D., Monette, G., Bayley, M., et al. (2008).
Recovery of function after traumatic brain injury: A multilevel modeling analysis of
Canadian outcomes. Archives of Physical Medicine and Rehabilitation, 89, S3–S15.Corkin, S. (1979). Hidden-Figures-Test performance: Lasting effects of unilateral penetrating
head injury and transient effects of bilateral cingulotomy. Neuropsychologia, 17, 585–605.
Delis, D. C., Kramer, J. H., Kaplan, E., & Ober, B. A. (2000). California Verbal LearningTest – Second edition. San Antonio, TX: The Psychological Corporation.
Dikmen, S. S., Machamer, J. E., Winn, H. R., & Temkin, N. R. (1995). Neuropsychological
outcome at 1-year post head injury. Neuropsychology, 9, 80–90.
Draper, K., & Ponsford, J. (2008). Cognitive functioning ten years following traumatic brain
injury and rehabilitation. Neuropsychology, 22, 618–625.
Felmingham, K. L., Baguley, I. J., & Green, A. M. (2004). Effects of diffuse axonal injuryon speed of information processing following severe traumatic brain injury.Neuropsychology, 18, 564–571.
Fork, M., Bartels, C., Ebert, A. D., Grubich, C., Synowitz, H., & Wallesch, C. W. (2005).Neuropsychological sequelae of diffuse traumatic brain injury. Brain Injury, 19,
101–108.
1110 SHELLEY YLIOJA ET AL.
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

Gabbe, B. J., Cameron, P. A., & Finch, C. F. (2003). The status of the Glasgow Coma Scale.Emergency Medicine, 15, 353–360.
Gaetz, M. (2004). The neurophysiology of brain injury. Clinical Neurophysiology, 115, 4–18.
Grafman, J., Jonas, B. S., Martin, A., Salazar, A. M., Weingartner, H., Ludlow, C., et al.(1988). Intellectual function following penetrating head injury in Vietnam veterans.Brain, 111, 169–184.
Greiffenstein, M. F., Baker, W. J., & Gola, T. (1996). Motor dysfunction profiles in traumaticbrain injury and postconcussion syndrome. Journal of the InternationalNeuropsychological Society, 2, 477–485.
Groswasser, Z., Reider-Groswasser, I. I., Schwab, K., Ommaya, A. K., Pridgen, A.,
Brown, H. R., et al. (2002). Quantitative imaging in late TBI. Part II: Cognition andwork after closed and penetrating head injury: A report of the Vietnam head injurystudy. Brain Injury, 16, 681–690.
Hanks, R. A., Millis, S. R., Ricker, J. H., Giacino, J. T., Nakese-Richardson, R., Frol, A. B.,et al. (2008). The predictive validity of a brief inpatient neuropsychologic battery forpersons with traumatic brain injury. Archives of Physical Medicine and Rehabilitation, 89,
950–957.Heaton, R. K., Miller, S. W., Taylor, M. J., & Grant, I. (2004). Revised comprehensive norms
for an expanded Halstead-Reitan battery: Demographically adjusted neuropsychological
norms for African American and Caucasian adults. Lutz, FL: Psychological AssessmentResources.
Hellawell, D. J., Taylor, R., & Pentland, B. (1999). Cognitive and psychosocial outcomefollowing moderate or severe traumatic brain injury. Brain Injury, 13, 489–504.
Hosmer, D. W., & Lemeshow, S. (2000). Applied logistic regression (2nd ed.). New York:Wiley Interscience.
Kalmar, K., Novack, T. A., Nakase-Richardson, R., Sherer, M., Frol, A. B., Gordon, W. A.,
et al. (2008). Feasibility of a brief neuropsychologic test battery during acute inpatientrehabilitation after traumatic brain injury. Archives of Physical Medicine andRehabilitation, 89, 942–949.
Kaufman, H. H., Levin, H. S., High Jr, W. M., Childs, T. L., Wagner, K. A., &Gildenberg, P. L. (1985). Neurobehavioral outcome after gunshot wounds to the headin adult civilians and children. Neurosurgery, 16, 754–758.
Kersel, D. A., Marsh, N. V., Havill, J. H., & Sleigh, J. W. (2001). Neuropsychological
functioning during the year following severe traumatic brain injury. Brain Injury, 15,283–296.
Lezak, M. D., Howieson, D. B., & Loring, D. W. (2004). Neuropsychological assessment
(4th ed.). New York: Oxford University Press.Madigan, N. K., DeLuca, J., Diamond, B. J., Tramontano, G., & Averill, A. (2000). Speed
of information processing in traumatic brain injury: Modality-specific factors. Journal
of Head Trauma Rehabilitation, 15, 943–956.‘‘Management and prognosis of penetrating brain injury’’ [supplement issue]. (2001).
The Journal of Trauma, 51, S1–S86.
Mathias, J. L., & Wheaton, P. (2007). Changes in attention and information-processing speedfollowing severe traumatic brain injury: A meta-analytic review. Neuropsychology, 21,212–223.
Matthews, C. G., & Klove, K. (1964). Instruction manual for the adult neuropsychology test
battery. Madison, WI: University of Wisconsin Medical School.
McCaffrey, R. J., Krahula, M. M., Heimberg, R. G., Keller, K. E., & Purcell, M. J. (1988).A comparison of the Trail Making Test, Symbol Digit Modalities Test, and the HooperVisual Organization Test in an inpatient substance abuse population. Archives of Clinical
Neuropsychology, 3, 181–187.
PENETRATING VS NON-PENETRATING TBI 1111
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010

McKinlay, W., & Watkiss, A. (1999). Cognitive and behavioral effects of brain injury.In M. Rosenthal, E. Griffith, J. Kreutzer, & B. Pentland (Eds.), Rehabilitation of adultand child with traumatic brain injury (pp. 74–88). Philadelphia: F.A. Davis Company.
Millis, S. R., & Ricker, J. H. (1995). Verbal learning and memory impairment in adultcivilians following penetrating missile wounds. Brain Injury, 9, 509–515.
Millis, S. R., Rosenthal, M., Novack, T. A., Sherer, M., Nick, T. G., Kreutzer, J. S., et al.
(2001). Long-term neuropsychological outcome after traumatic brain injury. Journal ofHead Trauma Rehabilitation, 16, 343–355.
Oehmichen, M., Meissner, C., & Konig, H. G. (2001). Brain injury after survived gunshot tothe head: Reactive alterations at sites remote from the missile track. Forensic Science
International, 115, 189–197.Ponsford, J., & Kinsella, G. (1992). Attentional deficits following closed-head injury. Journal
of Clinical and Experimental Neuropsychology, 14, 822–838.
Povlishock, J. T. (1992). Traumatically induced axonal injury: Pathogenesis and pathobio-logical implications. Brain Pathology, 2, 1–12.
Raymont, V., Greathouse, A., Reding, K., Lipsky, R., Salazar, A., & Grafman, J. (2008).
Demographic, structural and genetic predictors of late cognitive decline after penetratinghead injury. Brain, 131, 543–558.
Reitan, R. M., & Wolfson, D. (1985). The Halstead-Reitan Neuropsychological Test Battery:
Theory and interpretation. Tucson, AZ: Neuropsychology Press.Rios, M., Perianez, J. A., & Munoz-Cespedes, J. M. (2004). Attentional control and slowness
of information processing after severe traumatic brain injury. Brain Injury, 18, 257–272.Ruff, R. M., & Evans, R. (1986). Impaired verbal and figural fluency after head injury.
Archives of Clinical Neuropsychology, 1, 87–101.Salmond, C. H., & Sahakian, B. J. (2005). Cognitive outcome in traumatic brain injury
survivors. Current Opinion in Critical Care, 1, 111–116.
Sapsford, W. (2003). Penetrating brain injury in military conflict: Does it merit moreresearch? Journal of the Royal Army Medical Corps, 149, 5–14.
Scheid, R., Walther, K., Guthke, T., Preul, C., & von Cramon, Y. (2006). Cognitive sequelae
of diffuse axonal injury. Archives of Neurology, 63, 418–424.Schmidt, M. (1996). Rey Auditory-Verbal Learning Test. Los Angelos, CA: Western
Psychological Services.Schretlen, D. J., & Shapiro, A. M. (2003). A quantitative review of the effects of traumatic
brain injury on cognitive functioning. International Review of Psychiatry, 15, 341–349.Smith, A. (1991). Symbol Digit Modalities Test. Los Angeles, CA: Western Psychological
Services.
Smith, D. H., Meaney, D. F., & Shull, W. H. (2003). Diffuse axonal injury in head trauma.Journal of Head Trauma Rehabilitation, 18, 307–316.
Strauss, E., Sherman, E., & Spreen, O. (2006). A compendium of neuropsychological tests:
Administration, norms, and commentary (3rd ed.). New York: Oxford University Press.Tsuei, Y. S., Sun, M. H., Lee, H. D., Chiang, M. Z., Leu, C. H., Cheng, W. Y., et al.
(2005). Civilian gunshot wounds to the brain. Journal of the Chinese Medical
Association, 68, 126–130.Wertheimer, J. C., Hanks, R. A., & Hasenau, D. L. (2008). Comparing functional status and
community integration in severe penetrating and motor vehicle-related brain injuries.Archives of Physical Medicine and Rehabilitation, 89, 1983–1990.
Zahn, T. P., & Mirsky, A. F. (1999). Reaction time indicators of attention deficits in closedhead injury. Journal of Clinical and Experimental Neuropsychology, 21, 352–367.
1112 SHELLEY YLIOJA ET AL.
Downloaded By: [Ylioja, Shelley] At: 17:53 5 October 2010