a meta-analysis of etidronate for the treatment of postmenopausal osteoporosis
TRANSCRIPT
Original Article
A Meta-analysis of Etidronate for the Treatment of PostmenopausalOsteoporosis
A. Cranney1, G. Guyatt2, N. Krolicki2, V. Welch1, L. Griffith2, J. D. Adachi1, B. Shea1, P. Tugwell1,G. Wells1 and the Osteoporosis Research Advisory Group (ORAG)*1Departments of Medicine and Clinical Epidemiology, Loeb Research Institute, University of Ottawa; and 2Departments ofMedicine and Clinical Epidemiology and Biostatistics, McMaster University, Ottawa, Canada
Abstract. The aim of the study was to review the effectof etidronate on bone density and fractures in post-menopausal women. We searched MEDLINE from 1966to 1998, examined citations of relevant articles, and theproceedings of international osteoporosis meetings. Wecontacted osteoporosis investigators to identify addi-tional studies, primary authors, and pharmaceuticalindustry sources for unpublished data. We included 13trials that randomized women to etidronate or analternative (placebo or calcium and/or vitamin D) andmeasured bone density for at least 1 year. For each trial,three independent reviewers assessed the methodologicquality and abstracted data. The data suggested areduction in vertebral fractures with a pooled relativerisk of 0.63 (95% CI 0.44 to 0.92). There was no effecton nonvertebral fractures (relative risk 0.99, (95% CI0.69 to 1.42). Etidronate, relative to control, increasedbone density after 1–3 years of treatment in the lumbarspine by 4.06% (95% CI 3.12 to 5.00), in the femoralneck by 2.35% (95% CI 1.66 to 3.04) and in the totalbody by 0.97% (95% CI 0.39 to 1.55). Effects werelarger at 4 years, though the number of patients followedmuch smaller. Etidronate increases bone density in thelumbar spine and femoral neck for up to 4 years. Thepooled estimates of fracture reduction with etidronatesuggest a reduction in vertebral fractures, but no effecton nonvertebral fractures.
Keywords: Bisphosphonates; Bone density; Etidronate;Fractures; Meta-analysis; Osteoporosis; Systematic re-views
Background
Osteoporosis is a clinical syndrome of reduced bonemass resulting in increased fragility fractures. Using adefinition of bone mass >2.5 standard deviations lowerthan that in young women, as many as 30% ofpostmenopausal women suffer from osteoporosis [1].Up to 70% of hip fractures may be attributable toosteoporosis [2] and the mortality associated with hipfracture ranges from 12% to 20%. A recent estimatepredicts an exponential increase in hip fracture incidenceup to the year 2041 [3].Treatment guidelines present a framework for the
management of osteoporosis [4,5], and include a numberof treatment options that may decrease fracture risk,including bisphosphonates. Etidronate is a first-genera-tion bisphosphonate that inhibits osteoclastic resorption[6]. Etidronate is given on a cyclical schedule every 3months because of its potential to inhibit mineralizationand cause osteomalacia.A recent meta-analysis by Cardona and Pastor [7]
suggested that etidronate may decrease the risk ofvertebral fractures. However, this meta-analysis omitteda number of potentially relevant trials, failed to contactoriginal investigators to ensure data completeness andaccuracy, and made no attempt to address the impact of
Osteoporos Int (2001) 12:140–151� 2001 International Osteoporosis Foundation and National Osteoporosis Foundation Osteoporosis
International
*The ORAG consists of Clifford Rosen, MD, John Bilezikian, MD,Lorraine Fitzpatrick, MD, M. J. Favus, MD, Douglas P. Kiel, MD,Robert Marcus, Eric Orwoll, MD, Thomas Schnitzer and DennisBlack, PhD.Correspondence and offprint requests to: Dr A. Cranney, MD,FRCPC, MSc, Division of Rheumatology, Ottawa Hospital, 737Parkdale, Room 460, Ottawa, Ontario Canada K1Y 1J8.

etidronate on nonvertebral fractures. We thereforeconducted a systematic review and meta-analysis ofthe efficacy of etidronate on bone density and fractures.Our goals included considering all published andunpublished randomized control trials (RCTs), estimat-ing effects on vertebral and nonvertebral fractures, anddetermining the consistency of etidronate effect acrossdifferent treatment groups.
Methods
We followed the procedures defined by the CochraneCollaboration for conducting a systematic review [8].
Eligibility Criteria
Trials satisfied the following criteria: (1) RCTs of atleast 1 year’s duration comparing etidronate therapy withplacebo or with calcium and/or vitamin D, (2) outcomesincluded fracture incidence or bone density and (3)participants were postmenopausal women. Eligible trialsused the intermittent cyclical method of administrationof etidronate at 400 mg per day for 14-20 days followedby 56–91 days of calcium and/or vitamin D.
Search and Selection
Our search strategies included electronic searches ofMEDLINE from 1966 to 1998, including CurrentContents for the previous 6 months using a modifiedversion of the search strategy outlined by Haynes et al.[9]. We hand-searched conference abstract books(Osteoporosis International, Journal of Bone andMineral Research) and contacted content experts toidentify unpublished studies. MeSH terms used in thedatabase search included: etidronate, didronel, coherencetherapy, osteoporosis, postmenopausal, diphosphonates,bisphosphonates, randomized controlled trial. Wesearched reference lists for other relevant RCTs.Two reviewers (A.C., V.W.) examined all potentially
relevant trials. For abstracts consistent with studyeligibility, we obtained the full text. For issues ofeligibility, as well as methodologic quality (see below),reviewers resolved disagreements by consensus.
Methodologic Quality
Three reviewers (A.C., V.W., N.K.) independentlyevaluated each trial for four characteristics: conceal-ment, intention-to-treat analysis, masking, and thecompleteness of follow-up.
Data Collection
Three reviewers (A.C., N.K., V.W.) independentlyextracted all data, including study population character-istics, treatment duration, baseline demographic data andthe baseline and end of study outcomes. When the articlepresented inadequate or unclear data, we contacted theauthors for additional information. The reviewersresolved differences in data extraction by referringback to the original article and establishing a consensus.A fourth reviewer was consulted to help resolvedifferences (B.S.). We did not include data from thehormone replacement therapy (HRT) arm or combinedHRT/etidronate arm of Wimalawansa 1995 and 1998[10,11].
A Priori Hypotheses Regarding Heterogeneity
We developed prior to the examination and pooling ofstudies, hypotheses that might explain the heterogeneityof study results. Specifically we compared groupsaccording to: (1) prevention versus treatment, (2) theconcurrent treatments including total calcium intake (atleast 1250 mg of total calcium intake on average forparticipants versus less than 1250 mg), phosphate andvitamin D, (3) year of publication (1995 or prior or after1995), (4) individual components of the qualityassessment, including concealed randomization,double-masking, loss to follow-up (less that 20%versus greater) and intention-to-treat analysis.Prior to the pooling of studies, we used a hierarchy to
define prevention versus treatment according to whetherinformation was available. When studies providedbaseline bone density, we classified studies as treatmentif they included women with lumbar spine bone density>2 standard deviations (SDs) below peak bone mass. Wechose this definition of 72.0 SD since it seemed areasonable cut-point to separate prevention (studies ofwomen without pre-existing fractures in whom the intentwas to increase bone mineral density) from treatmentstudies in which the intent was to prevent fractures. Ifthis information was unavailable we classified studies astreatment if the prevalence of vertebral fracture atbaseline was greater than 20%. If these data were notavailable we considered studies in which average agewas above 62 years as treatment.The methods of densitometry trials included: (1) dual
photon absorptiometry (DPA), (2) dual-energy X-rayabsorptiometry (DXA), (3) quantitative computed tomo-graphy (QCT) and (4) single photon absorptiometry(SPA). The precision error of QCT is not as good as thatof DXA of the posterior/anterior spine. QCT provides ameasure of volumetric density and higher rates of bonechange have been reported with QCT. Thus, we decidedto pool all measures but QCT.To detect whether there was evidence of publication
bias in our review we conducted a visual examination ofthe funnel plots, which relate the magnitude of thetreatment effect to the sample size [12–14] .
A Meta-analysis of Etidronate for Postmenopausal Osteoporosis 141
Analysis
We chose a random effects model that includesdifferences between studies in calculating the varianceestimate for all final analyses, whether of fractures orbone density [15].We conducted separate analyses for each bone density
site (total body, lumbar spine, combined forearm andfemoral neck). We began by constructing regressionmodels in which we considered data from all years. Theindependent variable in the models was the yearsassociated with each comparison, and the dependentvariable the effect size. In this regression we were able totake into account the covariance between time pointsintroduced by using data on the same subjects at multipletimes. We used a prior study to help us estimate thecorrelation between the change in bone density fromyear to year [16]. As a sensitivity analysis of therobustness of our model, we chose to use the smallestand largest correlation provided for each site varyingbetween 0.45 and 0.78 and pooled only when justifiedusing both the extreme correlations.We used our regression model to guide us in
combining data from different years of follow-up(Table 1). We began with a model that included aparameter for every time. We constructed additionalmodels. For each new model, we included one fewertime parameter – that is, we combined data acrossdifferent years of follow-up. We sought the mostparsimonious model, rejecting models if there was astatistically significant (p<0.05) reduction in fit in amodel with fewer parameters. In other words, for eachnew model with one fewer parameter we tested whetherwe had lost predictive power relative to the previousmodel, and if we had not we chose the model with fewerparameters. When the model showed we could pool dataacross years, we used the longest follow-up available foreach study (for instance, if we could pool across years 1to 3, we used 3-year data if available).To calculate the weighted mean percent difference in
bone density between treatment and control groups weused the percentage change from baseline in the twogroups and the associated standard deviations (SDs).When the SDs were not reported directly, we obtained
the results from the authors or trials’ sponsor.Heterogeneity between studies was calculated using atest based on the chi square distribution with N 71degrees of freedom where N is the number of studies[15]. Irrespective of the results of the test ofheterogeneity, we divided the studies into two groupsaccording to the a priori hypotheses. We then testedwhether the weighted mean percent differences weredifferent in the two groups according to the a priorihypotheses. For the hip, we pooled data across differentsites using one measure from each trial. If a trial reportedmore than one hip site, our order of preference was totalhip, femoral neck and trochanter. When we foundstatistically significant heterogeneity for the combinedhip bone density endpoint, we examined site ofmeasurement as one of the possible explanation forheterogeneity. For the forearm, we similarly pooled datawith the order of preference being 1/3 distal radius andulna and then 1/3 distal radius.For fractures, we determined a weighted average of
the relative risk. We constructed 2 6 2 tables forvertebral and nonvertebral fractures in each study forwhich the data were available and calculated theassociated relative risk. In analyzing the relative risks0.5 was added to each cell of the 2 6 2 table to adjustfor zero cells [17]. For pooling of the risk ratios, wechose a random effects model in which both within-study and between-study variability are considered inproducing a weighted mean of the individual studyestimates, with weights being inversely proportional tothe sampling variances. Heterogeneity was tested using achi-square procedure. We tested all our a priorihypotheses as for bone mineral density. Analyses werebased on intention-to-treat data from the individualclinical trials.
Results
Trial characteristics
We identified 358 articles by the electronic searchstrategy and 6 from hand-searching the reference lists,and retrieved 29 for closer examination. Sixteen were
Table 1. Summary of regression analysis to determine a parsimonious summary of etidronate data
Site Parameters Chi-square p value
Simpler model More complex model
Lumbar Spine No year parameters 1, 2, 3, 4 years 39.24 <0.0011, 2, [3, 4] years 1, 2, 3, 4 years 30.79 <0.0011, [2, 3], 4 years 1, 2, 3, 4 years 0.27 <0.61[1, 2, 3], 4 years 1, [2, 3], 4 years 1.98 <0.16
Model chosen: [1, 2, 3], 4 years
Femoral neck No year parameters 1, 2, 3, 4 years 33.84 <0.0011, 2, [3, 4] years 1, 2, 3, 4 years 24.86 <0.0011, [2, 3], 4 years 1, 2, 3, 4 years 0.19 <0.67[1, 2, 3], 4 years 1, [2, 3], 4 years 1.98 <0.16
Model chosen: [1, 2, 3], 4 years
142 A. Cranney et al.
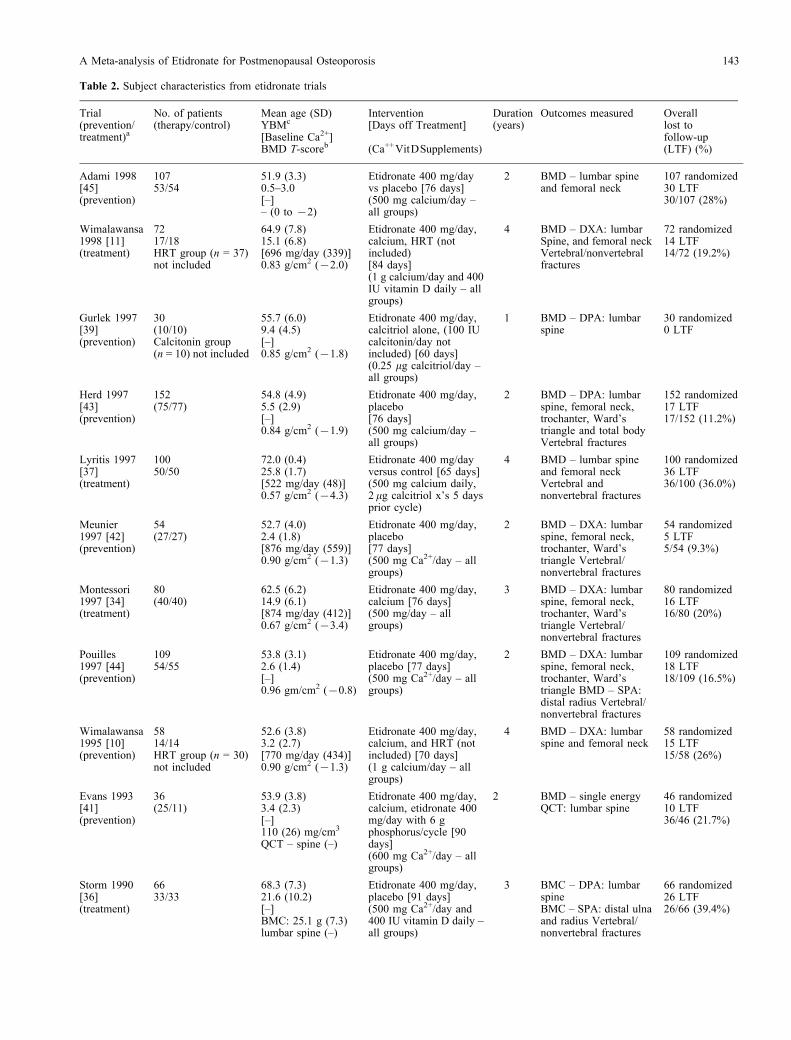
Table 2. Subject characteristics from etidronate trials
Trial(prevention/treatment)a
No. of patients(therapy/control)
Mean age (SD)YBMc
[Baseline Ca2+]BMD T-scoreb
Intervention[Days off Treatment]
(Ca++VitDSupplements)
Duration(years)
Outcomes measured Overalllost tofollow-up(LTF) (%)
Adami 1998[45](prevention)
10753/54
51.9 (3.3)0.5–3.0[–]– (0 to 72)
Etidronate 400 mg/dayvs placebo [76 days](500 mg calcium/day –all groups)
2 BMD – lumbar spineand femoral neck
107 randomized30 LTF30/107 (28%)
Wimalawansa1998 [11](treatment)
7217/18HRT group (n = 37)not included
64.9 (7.8)15.1 (6.8)[696 mg/day (339)]0.83 g/cm2 (72.0)
Etidronate 400 mg/day,calcium, HRT (notincluded)[84 days](1 g calcium/day and 400IU vitamin D daily – allgroups)
4 BMD – DXA: lumbarSpine, and femoral neckVertebral/nonvertebralfractures
72 randomized14 LTF14/72 (19.2%)
Gurlek 1997[39](prevention)
30(10/10)Calcitonin group(n = 10) not included
55.7 (6.0)9.4 (4.5)[–]0.85 g/cm2 (71.8)
Etidronate 400 mg/day,calcitriol alone, (100 IUcalcitonin/day notincluded) [60 days](0.25 mg calcitriol/day –all groups)
1 BMD – DPA: lumbarspine
30 randomized0 LTF
Herd 1997[43](prevention)
152(75/77)
54.8 (4.9)5.5 (2.9)[–]0.84 g/cm2 (71.9)
Etidronate 400 mg/day,placebo[76 days](500 mg calcium/day –all groups)
2 BMD – DPA: lumbarspine, femoral neck,trochanter, Ward’striangle and total bodyVertebral fractures
152 randomized17 LTF17/152 (11.2%)
Lyritis 1997[37](treatment)
10050/50
72.0 (0.4)25.8 (1.7)[522 mg/day (48)]0.57 g/cm2 (74.3)
Etidronate 400 mg/dayversus control [65 days](500 mg calcium daily,2 mg calcitriol x’s 5 daysprior cycle)
4 BMD – lumbar spineand femoral neckVertebral andnonvertebral fractures
100 randomized36 LTF36/100 (36.0%)
Meunier1997 [42](prevention)
54(27/27)
52.7 (4.0)2.4 (1.8)[876 mg/day (559)]0.90 g/cm2 (71.3)
Etidronate 400 mg/day,placebo[77 days](500 mg Ca2+/day – allgroups)
2 BMD – DXA: lumbarspine, femoral neck,trochanter, Ward’striangle Vertebral/nonvertebral fractures
54 randomized5 LTF5/54 (9.3%)
Montessori1997 [34](treatment)
80(40/40)
62.5 (6.2)14.9 (6.1)[874 mg/day (412)]0.67 g/cm2 (73.4)
Etidronate 400 mg/day,calcium [76 days](500 mg/day – allgroups)
3 BMD – DXA: lumbarspine, femoral neck,trochanter, Ward’striangle Vertebral/nonvertebral fractures
80 randomized16 LTF16/80 (20%)
Pouilles1997 [44](prevention)
10954/55
53.8 (3.1)2.6 (1.4)[–]0.96 gm/cm2 (70.8)
Etidronate 400 mg/day,placebo [77 days](500 mg Ca2+/day – allgroups)
2 BMD – DXA: lumbarspine, femoral neck,trochanter, Ward’striangle BMD – SPA:distal radius Vertebral/nonvertebral fractures
109 randomized18 LTF18/109 (16.5%)
Wimalawansa1995 [10](prevention)
5814/14HRT group (n = 30)not included
52.6 (3.8)3.2 (2.7)[770 mg/day (434)]0.90 g/cm2 (71.3)
Etidronate 400 mg/day,calcium, and HRT (notincluded) [70 days](1 g calcium/day – allgroups)
4 BMD – DXA: lumbarspine and femoral neck
58 randomized15 LTF15/58 (26%)
Evans 1993[41](prevention)
36(25/11)
53.9 (3.8)3.4 (2.3)[–]110 (26) mg/cm3
QCT – spine (–)
Etidronate 400 mg/day,calcium, etidronate 400mg/day with 6 gphosphorus/cycle [90days](600 mg Ca2+/day – allgroups)
2 BMD – single energyQCT: lumbar spine
46 randomized10 LTF36/46 (21.7%)
Storm 1990[36](treatment)
6633/33
68.3 (7.3)21.6 (10.2)[–]BMC: 25.1 g (7.3)lumbar spine (–)
Etidronate 400 mg/day,placebo [91 days](500 mg Ca2+/day and400 IU vitamin D daily –all groups)
3 BMC – DPA: lumbarspineBMC – SPA: distal ulnaand radius Vertebral/nonvertebral fractures
66 randomized26 LTF26/66 (39.4%)
A Meta-analysis of Etidronate for Postmenopausal Osteoporosis 143

excluded due to: lack of appropriate control group(eight trials) [18–25], lack of randomization (7 trials)[26–32] and duration of less than 1 year (1 trial) [33].Table 2 presents the characteristics of the 13 studies,including a total of 1267 women, that met the inclusioncriteria. Five trials included women with establishedosteoporosis and were classified as treatment [11,34–37]. Eight trials were classified as prevention studies[10,38–45]. The study by Watts et al. [38,40] includedfour treatment groups, two of which were placebogroups. Therefore, this study was analyzed as twoseparate studies (A and B): (A) cyclical etidronate andphosphate versus placebo and phosphate, and (B)cyclical etidronate versus placebo.All studies ensure concealed randomization and all but
one trial used an intention-to-treat analysis [37]. Sixtrials were described as double-masked, and 7 were notmasked. One trial had a loss to follow-up of less than1%, 5 trials from 5% to 20%, and the remaining 7 trialsover 20%.Eight of the investigators responded to our request and
provided additional data [10,11,34,36–39,44]. Oneauthor was unable to provide additional data [35], andwe were unable to contact four authors [41–43,45].Procter and Gamble, the manufacturer of etidronate, alsoresponded to our request for additional data.
Fractures
Nine trials (n = 1076) reported vertebral fractures[11,34–38,42–44] (Table 3). One trial reported that nofractures occurred in either treatment group [43]. Of the9 trials that reported fractures, all 6 that described themethods used to assess vertebral fractures (3 did not)used a semiquantitative rating by an experiencedradiologist to assess incident fractures [11,34–38]. Thepooled estimate of the relative risk of vertebral fracturesfrom 9 trials, 0.63 (95% CI: 0.44 to 0.92, p=0.02,heterogeneity p value 0.87), showed a fracture riskreduction with etidronate, with results very consistentacross studies (Fig. 1). Of the a priori hypotheses, noneshowed statistically significant differences betweensubgroups.Table 3 demonstrates a lack of effect of etidronate on
nonvertebral fractures (Fig. 2). The confidence intervalsaround the estimate for all nonvertebral fractures is wide(consistent with a relative risk reduction of approxi-mately 31% and a relative risk increase of 42%) and theresults are once again very consistent across studies,reflected in the heterogeneity p-value of 0.94. Theproportion of wrist fractures was 14.43% and of hipfractures 9.3%. The funnel plots showed no suggestionof publication bias.
Table 2. (Continued)
Trial(prevention/treatment)a
No. of patients(therapy/control)
Mean age (SD)YBMc
[Baseline Ca2+]BMD T-scoreb
Intervention[Days off Treatment]
(Ca++VitDSupplements)
Duration(years)
Outcomes measured Overalllost tofollow-up(LTF) (%)
Watts 1990[38](prevention)
423212/211
65.1 (13)17.9 (16.5)[746 mg/day (782)]0.86 g/cm2 (71.7)
Etidronate 400 mg/day,placebo, etidronate 400mg/day with 3 gphosphorus, placebo with3 g phosphorus [91 days](500 mg Ca2+/day – allgroups)
2 BMD – DPA: lumbarspine, femoral neck,trochanter, ward’striangle BMD – SPA:distal radius Vertebral/nonvertebral fractures
423 randomized60 LTF60/423 (14.2%)
Pacifici 1988[35](treatment)
9330/27HRT group (n = 36)not included
61 (7.8)13.8 (9.5)[875 mg/day (406)]79.1 mg/cm3 QCT –spine (–)
Etidronate 400 mg/daywith 7.5 g K phosphate/cycle, calcium, (HRT notincluded) [56 days](1 g Ca2+/day – allgroups)
2 BMD – QCT: spineBMD – SPA – nucleardata: distal andproximal radiusVertebral fractures
93 randomized42 LTF42/93 (45%)
–, data not available.a.Refer to a priori hypothesis defining prevention and treatment.b.T-score calculated using the lumbar spine BMD [(LS BMD –1.047)/0.110].c.YSM = years post menopausal.
Table 3. Weighted relative risk with 95% CI after the final year of treatment with cyclical 400 mg etidronate
Fracture sites No. oftrials
No. ofsubjects
Relative risk(95% CI)
Relative riskp value
Heterogeneityp value
Vertebral 9 1076 0.63 (0.44, 0.92) 0.02 0.87All nonvertebral 7 867 0.99 (0.69, 1.42) 0.97 0.94
We interpreted a heterogeneity p value 40.05 as indicating important between-study differences in results.
144 A. Cranney et al.
Fig. 1. Weighted relative risk for vertebral fractures: osteoporotic and non-osteoporotic populations. (The primary prevention trials of Herd,Meunier and Pouilles (n = 315) were not included due to the low incidence of fractures.) *Treatment and control groups received phosphate.
Fig. 2. Weighted relative risk for nonvertebral fractures: osteoporotic and non-osteoporotic populations. *Montessori trial (n = 80) not includeddue to zero nonvertebral fractures occurring. **Treatment and control groups received phosphate.
A Meta-analysis of Etidronate for Postmenopausal Osteoporosis 145

Bone Density
The dominant parsimonious models for each bonedensity site proved as follows: pool data from years 1to 3 for all sites measured (total body, lumbar spine,combined forearm and femoral neck), leaving year 4separate. Table 1 describes the process we used to arriveat the model for lumbar spine; this was similar for othersites.In our initial analysis we found statistically significant
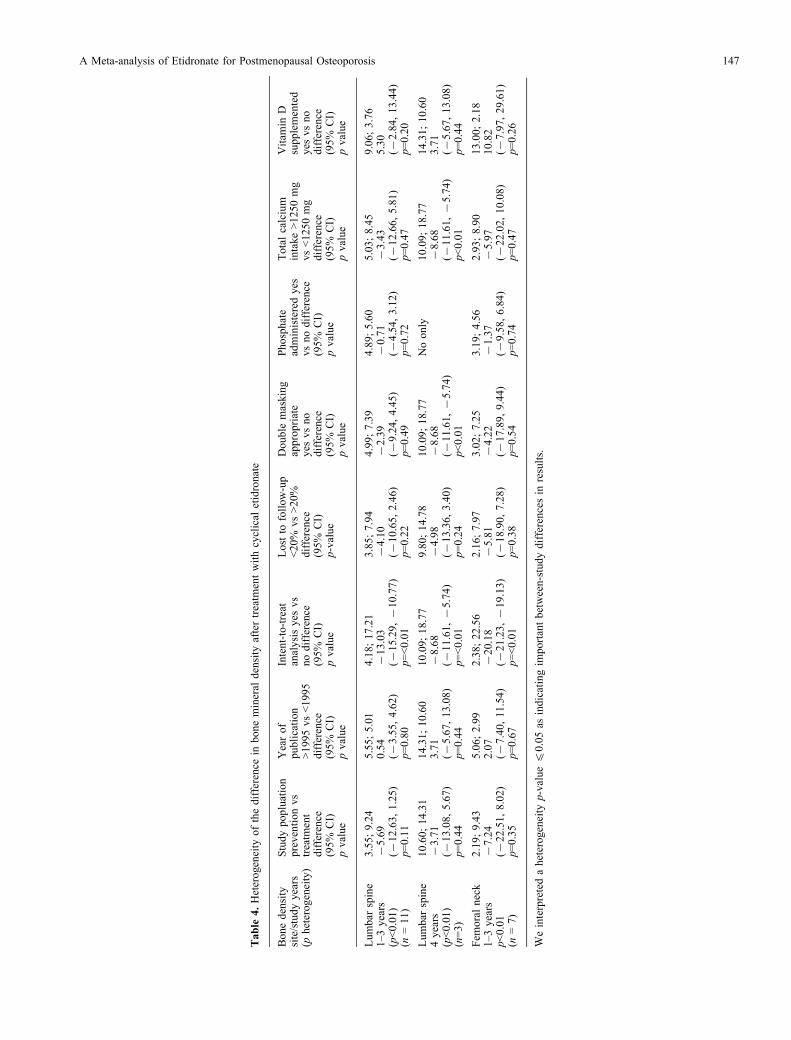
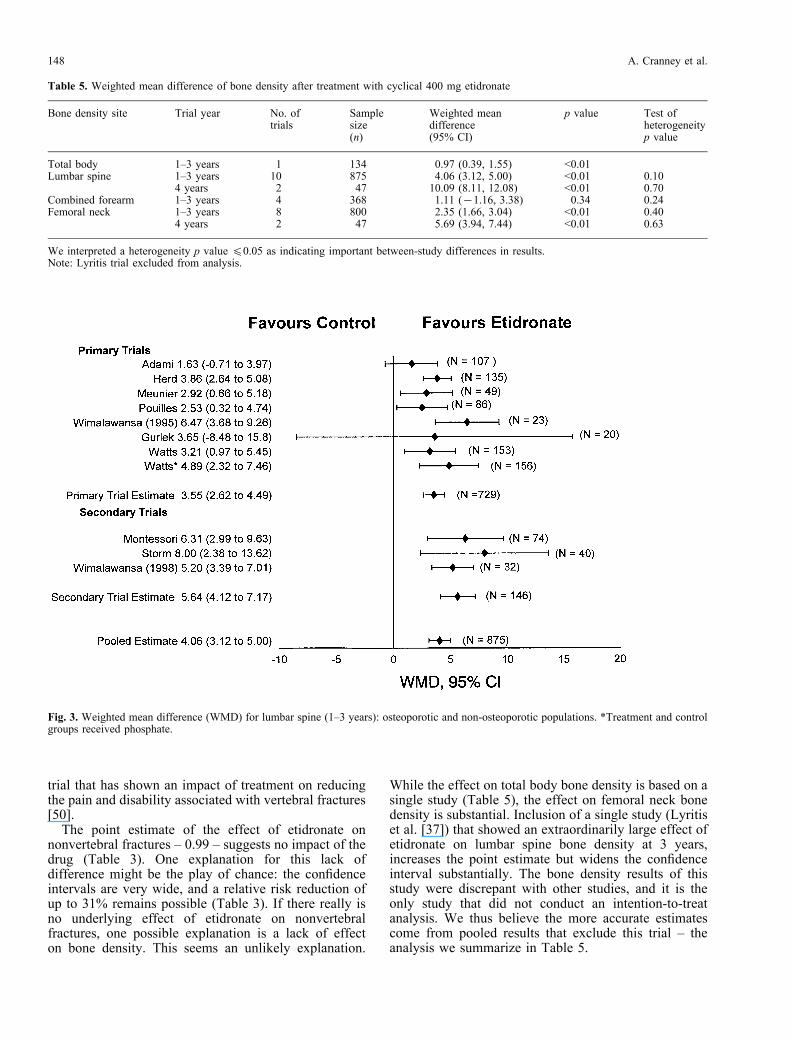
heterogeneity across studies in etidronate’s effect onbone density in the lumbar spine and femoral neck(p<0.01). When we explored sources of heterogeneity,we found one striking explanation: the one study (Lyritiset al. [37]) that did not use an intention-to-treat analysisshowed a much larger treatment effect than the otherstudies (Table 4). When we repeated our analysesexcluding this trial, we found results relatively consistentresults across studies, with no significant tests ofheterogeneity (Table 5). Because these findings suggestthat the extraordinary treatment effects in the one studythat failed to use an intention-to-treat analysis are due tobias, we will focus on the results excluding this study,and present these results in our bone density summarytable (Table 5).Table 5 shows moderate to large, statistically high
increases in bone density with etidronate therapy in thelumbar spine at 3 years, with larger changes at 4 years.The results were consistent across studies, both for the1–3 year data (Fig. 3) and for the 4-year data – bothreflected in a nonsignificant test of heterogeneity.However, the 4-year results were based on only 2 trials[10,11] with a sample size of 47. Furthermore, theeffects at 1–3 years were larger in the 3 studies thatfollowed patients for 4 years than those that did not,raising questions about the interpretation of thedifference at 4 years. These considerations suggest thatthe much larger changes in spine BMD in year 4 versusyears 1–3 may be artifactual.Inclusion of the Lyritis data increased the magnitude
of the mean effect, and widened the confidence interval,both for the 1–3 year results (point estimate 5.54%, 95%CI 2.94 to 8.13) and the 4-year estimate (13.11%, 95%CI 6.95 to 19.28) for the lumbar spine.A single study suggests etidronate increases total body
density at 3 years (Table 5). The combined forearm datashowed a relatively weak, nonsignificant trend in favorof etidronate (Table 5). The femoral neck data showed alarge, statistically significant difference in favor ofetidronate at 1–3 years. Four-year femoral neck datashowed a similar, somewhat larger effect (Table 5).Including the Lyritis data increased the magnitude of theapparent effect over the first 3 years of treatment, andwidened the confidence interval (point estimate 2.76%,95% CI 1.59 to 3.94). In the 4-year pooled estimates,inclusion of the Lyritis data increased the point estimatewithout widening the confidence interval (6.75%, 95%CI 6.07 to 7.42).There were a total of only 83 patients at 1 year and 57
at 2 years for whom QCT measurements at the lumbar
spine were available. As a result, although there was atrend in favor of etidronate, the confidence intervalswere very wide and the effects were not statisticallysignificant.Funnel plots of lumbar spine BMD, femoral neck,
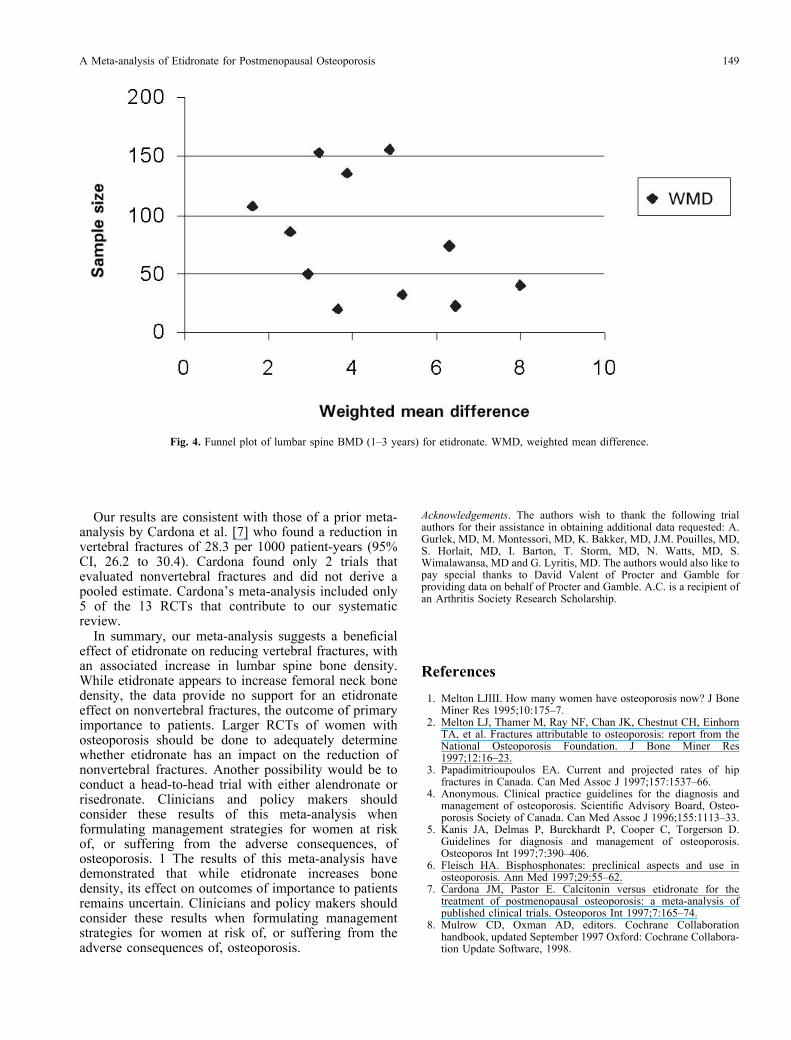
forearm and non-vertebral fractures suggested thepossibility of publication bias whereas, a funnel plot ofvertebral fractures did not. Fig. 4, presents a funnel plotof the lumbar spine BMD results. The figure demon-strates that there were four small studies of under 100patients suggesting treatment effects greater than that ofapproximately 4% than the largest studies suggest. Thecorresponding small studies showing treatment effects ofsubstantially less than 4% that one would expect aremissing. This results in a funnel with the left lowerquadrant missing and suggests the possibility that small‘‘negatives’’ trials were unreported, while small positivetrials appeared in the literature.
Toxicity and Withdrawals
Dropouts and withdrawals were available for 8 studies.The pooled estimate showed no statistical differencebetween placebo and etidronate for the risk of with-drawal due to side effects (0.93, 95% CI 0.70 to 1.23,p=0.59, heterogeneity p value 0.68) or for dropoutsoverall (1.30, 95% CI 0.58 to 2.93, p=0.53, hetero-geneity p value 0.68).
Discussion
In this meta-analysis we performed a comprehensiveliterature search, specified inclusion and exclusioncriteria, and conducted a rigorous data analysis. Wemade a systematic effort to obtain complete data from allpublished trials. To calculate summary estimates oftreatment we used a random effects model that providesa conservative estimate of treatment effect. The resultsof a meta-analysis are, however, only as strong as theprimary studies. In this case, the main limitations inquality of the studies are lack of masking and large lossto follow-up (Table 2). An additional limitation of thebone density results is the possibility of publication bias(Fig. 4).Our pooled analysis suggests that etidronate reduces
the relative risk of vertebral fractures by 37% (Table 3).The 95% confidence interval around this estimate isrelatively wide, and the boundary representing thesmallest effect consistent with the data shows a relativerisk reduction of only 8%.Reducing vertebral fractures is important if it is
associated with reduction in pain and associatedfunctional disability. Numerous observational studieshave suggested an association between fractures andpain [46–49]. There remains only a single randomized
146 A. Cranney et al.
Table
4.Heterogeneity
ofthedifference
inbonemineraldensity
aftertreatmentwithcyclicaletidronate
Bonedensity
site/studyyears
(pheterogeneity)
Studypopluation
preventionvs
treatment
difference
(95%
CI)
pvalue
Yearof
publication
>1995vs<1995
difference
(95%
CI)
pvalue
Intent-to-treat
analysisyes
vs
nodifference
(95%
CI)
pvalue
Lostto
follow-up
<20%
vs>20%
difference
(95%
CI)
p-value
Doublemasking
appropriate
yes
vsno
difference
(95%
CI)
pvalue
Phosphate
administeredyes
vsnodifference
(95%
CI)
pvalue
Totalcalcium
intake>1250mg
vs<1250mg
difference
(95%
CI)
pvalue
Vitam
inD
supplemented
yes
vsno
difference
(95%
CI)
pvalue
Lumbar
spine
1–3years
(p<0.01)
(n=11)
3.55;9.24
75.69
(712.63,1.25)
p=0.11
5.55;5.01
0.54
(73.55,4.62)
p=0.80
4.18;17.21
713.03
(715.29,710.77)
p=<0.01
3.85;7.94
74.10
(710.65,2.46)
p=0.22
4.99;7.39
72.39
(79.24,4.45)
p=0.49
4.89;5.60
70.71
(74.54,3.12)
p=0.72
5.03;8.45
73.43
(712.66,5.81)
p=0.47
9.06;3.76
5.30
(72.84,13.44)
p=0.20
Lumbar
spine
4years
(p<0.01)
(n=3)
10.60;14.31
73.71
(713.08,5.67)
p=0.44
14.31;10.60
3.71
(75.67,13.08)
p=0.44
10.09;18.77
78.68
(711.61,75.74)
p=<0.01
9.80;14.78
74.98
(713.36,3.40)
p=0.24
10.09;18.77
78.68
(711.61,75.74)
p<0.01
Noonly
10.09;18.77
78.68
(711.61,75.74)
p<0.01
14.31;10.60
3.71
(75.67,13.08)
p=0.44
Fem
oralneck
1–3years
p<0.01
(n=7)
2.19;9.43
77.24
(722.51,8.02)
p=0.35
5.06;2.99
2.07
(77.40,11.54)
p=0.67
2.38;22.56
720.18
(721.23,719.13)
p=<0.01
2.16;7.97
75.81
(718.90,7.28)
p=0.38
3.02;7.25
74.22
(717.89,9.44)
p=0.54
3.19;4.56
71.37
(79.58,6.84)
p=0.74
2.93;8.90
75.97
(722.02,10.08)
p=0.47
13.00;2.18
10.82
(77.97,29.61)
p=0.26
Weinterpretedaheterogeneityp-value40.05as
indicatingimportantbetween-studydifferencesin
results.
A Meta-analysis of Etidronate for Postmenopausal Osteoporosis 147
trial that has shown an impact of treatment on reducingthe pain and disability associated with vertebral fractures[50].The point estimate of the effect of etidronate on
nonvertebral fractures – 0.99 – suggests no impact of thedrug (Table 3). One explanation for this lack ofdifference might be the play of chance: the confidenceintervals are very wide, and a relative risk reduction ofup to 31% remains possible (Table 3). If there really isno underlying effect of etidronate on nonvertebralfractures, one possible explanation is a lack of effecton bone density. This seems an unlikely explanation.
While the effect on total body bone density is based on asingle study (Table 5), the effect on femoral neck bonedensity is substantial. Inclusion of a single study (Lyritiset al. [37]) that showed an extraordinarily large effect ofetidronate on lumbar spine bone density at 3 years,increases the point estimate but widens the confidenceinterval substantially. The bone density results of thisstudy were discrepant with other studies, and it is theonly study that did not conduct an intention-to-treatanalysis. We thus believe the more accurate estimatescome from pooled results that exclude this trial – theanalysis we summarize in Table 5.
Table 5. Weighted mean difference of bone density after treatment with cyclical 400 mg etidronate
Bone density site Trial year No. oftrials
Samplesize(n)
Weighted meandifference(95% CI)
p value Test ofheterogeneityp value
Total body 1–3 years 1 134 0.97 (0.39, 1.55) <0.01Lumbar spine 1–3 years 10 875 4.06 (3.12, 5.00) <0.01 0.10
4 years 2 47 10.09 (8.11, 12.08) <0.01 0.70Combined forearm 1–3 years 4 368 1.11 (71.16, 3.38) <0.34 0.24Femoral neck 1–3 years 8 800 2.35 (1.66, 3.04) <0.01 0.40
4 years 2 47 5.69 (3.94, 7.44) <0.01 0.63
We interpreted a heterogeneity p value 40.05 as indicating important between-study differences in results.Note: Lyritis trial excluded from analysis.
Fig. 3. Weighted mean difference (WMD) for lumbar spine (1–3 years): osteoporotic and non-osteoporotic populations. *Treatment and controlgroups received phosphate.
148 A. Cranney et al.
Our results are consistent with those of a prior meta-analysis by Cardona et al. [7] who found a reduction invertebral fractures of 28.3 per 1000 patient-years (95%CI, 26.2 to 30.4). Cardona found only 2 trials thatevaluated nonvertebral fractures and did not derive apooled estimate. Cardona’s meta-analysis included only5 of the 13 RCTs that contribute to our systematicreview.In summary, our meta-analysis suggests a beneficial
effect of etidronate on reducing vertebral fractures, withan associated increase in lumbar spine bone density.While etidronate appears to increase femoral neck bonedensity, the data provide no support for an etidronateeffect on nonvertebral fractures, the outcome of primaryimportance to patients. Larger RCTs of women withosteoporosis should be done to adequately determinewhether etidronate has an impact on the reduction ofnonvertebral fractures. Another possibility would be toconduct a head-to-head trial with either alendronate orrisedronate. Clinicians and policy makers shouldconsider these results of this meta-analysis whenformulating management strategies for women at riskof, or suffering from the adverse consequences, ofosteoporosis. 1 The results of this meta-analysis havedemonstrated that while etidronate increases bonedensity, its effect on outcomes of importance to patientsremains uncertain. Clinicians and policy makers shouldconsider these results when formulating managementstrategies for women at risk of, or suffering from theadverse consequences of, osteoporosis.
Acknowledgements. The authors wish to thank the following trialauthors for their assistance in obtaining additional data requested: A.Gurlek, MD, M. Montessori, MD, K. Bakker, MD, J.M. Pouilles, MD,S. Horlait, MD, I. Barton, T. Storm, MD, N. Watts, MD, S.Wimalawansa, MD and G. Lyritis, MD. The authors would also like topay special thanks to David Valent of Procter and Gamble forproviding data on behalf of Procter and Gamble. A.C. is a recipient ofan Arthritis Society Research Scholarship.
References
1. Melton LJIII. How many women have osteoporosis now? J BoneMiner Res 1995;10:175–7.
2. Melton LJ, Thamer M, Ray NF, Chan JK, Chestnut CH, EinhornTA, et al. Fractures attributable to osteoporosis: report from theNational Osteoporosis Foundation. J Bone Miner Res1997;12:16–23.
3. Papadimitrioupoulos EA. Current and projected rates of hipfractures in Canada. Can Med Assoc J 1997;157:1537–66.
4. Anonymous. Clinical practice guidelines for the diagnosis andmanagement of osteoporosis. Scientific Advisory Board, Osteo-porosis Society of Canada. Can Med Assoc J 1996;155:1113–33.
5. Kanis JA, Delmas P, Burckhardt P, Cooper C, Torgerson D.Guidelines for diagnosis and management of osteoporosis.Osteoporos Int 1997;7:390–406.
6. Fleisch HA. Bisphosphonates: preclinical aspects and use inosteoporosis. Ann Med 1997;29:55–62.
7. Cardona JM, Pastor E. Calcitonin versus etidronate for thetreatment of postmenopausal osteoporosis: a meta-analysis ofpublished clinical trials. Osteoporos Int 1997;7:165–74.
8. Mulrow CD, Oxman AD, editors. Cochrane Collaborationhandbook, updated September 1997 Oxford: Cochrane Collabora-tion Update Software, 1998.
Fig. 4. Funnel plot of lumbar spine BMD (1–3 years) for etidronate. WMD, weighted mean difference.
A Meta-analysis of Etidronate for Postmenopausal Osteoporosis 149
9. Haynes R, Wilczynski N, McKibbon KA, Walker CJ, Sinclair JC.Developing optimal search strategies for detecting clinicallysound studies in MEDLINE. J Am Med Info Assoc 1994;1:447–58.
10. Wimalawansa SJ. Combined therapy with estrogen and etidronatehas an additive effect on bone mineral density in the hip andvertebrae: four-year randomized study. Am J Med 1995;99:36–42.
11. Wimalawansa SJ. A four-year randomized controlled trial ofhormone replacement and bisphosphonate, alone or in combina-tion, in women with postmenopausal osteoporosis. Am J Med1998;104:219–26.
12. Montori VM, Smieja M, Guyatt GH. Publication bias: a briefreview for clinicians. Mayo Clin Proc 2000;75(12):1284–8.
13. Sutton AJ, Duval SJ, Tweedie RL, Abrams KR, Jones DR.Empirical assessment of effect of publication bias on meta-analyses. BMJ 2000;320:1574–77.
14. Begg CB. Publication bias. In: Cooper H, Hedges LV, editors.The handbook of research synthesis. New York: Russell SageFoundation, 1994:399–409.
15. Fleiss JL. The statistical basis of meta-analysis. Stat MethodsMed Res 1993;2:121–45.
16. Black DM, Cummings SR, Karpf DB, et al. Randomized trial ofeffect of alendronate on risk of fracture in women with existingvertebral fractures. Fracture Intervention Trial Research Group.Lancet 1996;348:1535–41.
17. Naylor AF. Small sample considerations in combining 2 6 2tables. Biometrics 1967;23:349–56.
18. Anderson C, Cape RDT, Crilly RGAB, Hodsman AB, WolfeBMJ. Preliminary observations of a form of coherence therapy forosteoporosis. Calcif Tissue Int 1984;36:341–3.
19. Steiniche T, Hasling C, Charles P, Eriksen EF, Melsen F,Mosekilde L. The effects of etidronate on trabecular boneremodeling in postmenopausal spinal osteoporosis: a randomizedstudy comparing intermittent treatment and an ADFR regime.Bone 1991;12:155–63.
20. Hesch RD, Heck J, Delling G, Keck E, Reeve J, Canzler H, et al.Results of a stimulatory therapy of low bone metabolism inosteoporosis with (1-38)hPTH and disphosphonate EHDP:Protocol of Study I, Osteoporosis Trial Hannover. KlinWochenschr 1988;66:976–84.
21. Hodsman AB. Effects of cyclical therapy for osteoporosis usingan oral regimen of inorganic phosphate and sodium etidronate: aclinical and bone histomorphometric study. Bone Miner1989;5:201–12.
22. Jowsey J, Riggs BL, Kelly PJ, Hoffman DL, Bordier P. Thetreatment of osteoporosis with disodium ethane-1-hydroxy-1,1-diphosphonate. J Lab Clin Med 1971;78:574–84.
23. Hasling C, Charles P, Jensen FT, Mosekilde L. A comparison ofthe effects of oestrogen/progestogen, high-dose oral calcium,intermittent cyclic etidronate and an ADFR regime on calciumkinetics and bone mass in postmenopausal women with spinalosteoporosis. Osteoporos Int 1994;4:191–203.
24. Miller PD, Brown JB, Siris ES, Hoseyni MS, Axelrod DS, BekkerPJ. A randomized, double-blind comparison of residronate andetidronate in the treatment of Paget’s disease of bone. Paget’sResidronate/Etidronate Study Group. Am J Med 1999;106:513–20.
25. Masud T, Mulcahy B, Thompson AV, Donnelly S, Keen RW,Doyle DV, et al. Effects of cyclical etidronate combined withcalcitriol versus cyclical etidronate alone on spine and femoralneck bone mineral density in postmenopausal osteoporoticwomen. Ann Rheum Dis 1998:57:346–49.
26. Ott SM, Woodson GC, Huffer WE, Miller PD, Watts NB. Bonehistomorphometric changes after cyclic therapy with phosphateand etidronate disodium in women with postmenopausalosteoporosis. J Clin Endocrinol Metab 1994;78:968–72.
27. Ryan PJ, Fogelman I. Clinical experience with etidronate inosteoporosis. Clin Rheumatol 1994;13:455–58.
28. Storm T, Kollerup G, Thamsborg G, Genant HK, Sorensen OH.Five years of clinical experience with intermittent cyclicaletidronate for postmenopausal osteoporosis. J Rheumatol1996;23:1560–64.
29. Orme SM, Simpson M, Stewart SP, Oldroyd B, Westmacott CF,Smith MA, et al. Comparison of changes in bone mineral inidiopathic and secondary osteoporosis following therapy withcyclical disodium etidronate and high dose calcium supplementa-tion. Clin Endocrinol 1994;41:245–50.
30. Mallette LE, LeBlanc AD, Pool JL, Mechanick JI. Cyclic therapyof osteoporosis with neutral phosphate and brief, high-dose pulsesof etidronate. J Bone Miner Res 1989;4:143–8.
31. Smith ML, Fogelman I, Hart DM, Bevan J, Leggate I. Effect ofetidronate disodium on bone turnover following surgicalmenopause. Calcif Tissue Int 1989;44:74–9.
32. Miller PD, Watts NB, Licata AA, et al. Cyclical etidronate in thetreatment of postmenopausal osteoporosis: efficacy and safetyafter seven years of treatment. Am J Med 1997;103:468–76.
33. Heaney RP, Saville PD. Etidronate disodium in postmenopausalosteoporosis. Clin Pharmacol Ther 1976;20:593–604.
34. Montessori ML, Scheele WH, Netelenbos JC, Kerkhoff JF,Bakker K. The use of etidronate and calcium versus calciumalone in the treatment of postmenopausal osteopenia: results ofthree years of treatment. Osteoporos Int 1997;7:52–8.
35. Pacifici R, McMurtry C, Vered I, Rupich R, Avioli LV, PacificiR, et al. Coherence therapy does not prevent axial bone loss inosteoporotic women: a preliminary comparative study. J ClinEndocrinol Metab 1988;66:747–53.
36. Storm T, Thamsborg G, Steiniche T, Genant HK, Sorenson OH.Effect of intermittent cyclic etidronate therapy on bone mass andfracture rate in women with postmenopausal osteoporosis. N EnglJ Med 1990;322:1265–71.
37. Lyritis GP, Tsakalakos N, Paspati I, Skarantavos GR, Galanos A,Androulakis C. The effect of a modified etidronate cyclicalregimen on postmenopausal osteoporosis: a four-year study. ClinRheumatol 1997;16:354–60.
38. Watts NB, Harris ST, Genant HK, Wasnich RD, Miller PD,Jackson RD, et al. Intermittent cyclical etidronate treatment ofpostmenopausal osteoporosis. N Engl J Med 1990;323;:73–9.
39. Gurlek A, Bayraktar M, Gedik O. Comparison of calcitrioltreatment with etidronate–calcitriol and calcitonin–calcitriolcombinations in Turkish women with postmenopausal osteoporo-sis: a prospective study. Calcif Tissue Int 1997;61:39–43.
40. Harris ST, Watts NB, Jackson JD, Genant HK, Wasnich RD, RossP, et al. Four-year study of intermittent cyclic etidronatetreatment of postmenopausal osteoporosis: three years of blindedtherapy followed by one year open therapy. Am J Med1993;95;:557–67.
41. Evans RA, Somers NM, Dunstan CR, Royle H, Kos S. The effectof low-dose cyclical etidronate and calcium on bone mass in earlypostmenopausal women. Osteoporos Int 1993;3:71–5.
42. Meunier PJ, Confavreux E, Tupinon I, Hardouin C, Delmas PD,Balena R. Prevention of early postmenopausal bone loss withcyclical etidronate therapy (a double-blind, placebo- controlledstudy and 1-year follow-up). J Clin Endocrinol Metab1997;82:84–91.
43. Herd RJ, Balena R, Blake GM, Ryan PJ, Fogelman I. Theprevention of early postmenopausal bone loss by cyclicaletidronate therapy: a 2-year, double-blind, placebo- controlledstudy. Am J Med 1997;103:92–9.
44. Pouilles JM, Tremollieres F, Roux C, Sebert JL, Alexandre C,Goldberg D, et al. Effects of cyclical etidronate therapy on boneloss in early postmenopausal women who are not undergoinghormonal replacement therapy. Osteoporos Int 1997;7:213–8.
45. Adami S, Orranell S, Lombardi P, Campagnoli C, Ferrari A,Marchesoni D, et al. Prevention of early postmenopausal boneloss with cyclical etidronate: a double-blind, placebo-controlledstudy. Poster F294, IBMS Second Meeting, San Francisco,California, December 1998.
46. Ettinger B, Black DM, Nevitt MC, Rundle AC, Cauley JA,Cummings SR, Genant K, and The Study of OsteoporoticFractures Research Group. Contribution of vertebral deformitiesto chronic back pain. J Bone Miner Res 1992;7:449–55.
47. Ross PD, Davis JW, Epstein RS, Wasnich RD. Pain and disabilityassociated with new vertebral fractures and other spinalconditions. J Clin Epidemiol 1994;47:231–9.
150 A. Cranney et al.

48. Oleksik A, Shen W, Dawson A, Minshal M, Lips P. The impact ofincident vertebral fractures on health-related quality of life inwomen with prevalent fractures [abstract]. J Bone Miner Res1999;14(Suppl 1):S262.
49. Silverman SL, Minshall ME, Shen W, Harper KD, Xie S. Theimpact of incident vertebral fracture of health related quality oflife in established postmenopausal osteoporosis: results from the
Multiple Outcomes of Raloxifene Evaluation Study. J BoneMiner Res 1999;14(Suppl 1):S262.
50. Nevitt MC, Thompson DE, Black DM, Rubin Sr, Ensrud K, YatesAJ, Cummings SR. Effect of alendronate on limited-activity daysand bed-disability days caused by back pain in postmenopausalwomen with existing vertebral fractures. Fracture InterventionTrial Research Group. Arch Intern Med 2000;160:77–85.
Received for publication 25 February 2000Accepted in revised form 8 August 2000
A Meta-analysis of Etidronate for Postmenopausal Osteoporosis 151