dcoe_ops_tbi_webinar_14aug_presentation_v2-1_2014-08-14 final
TRANSCRIPT

Breaking the Code: ICD-9-Clinical Modification
Diagnosis Coding for Traumatic Brain Injury
Aug. 14, 2014, 1-2:30 p.m. (EDT)
Presenter: Amy Waller, CPC, CPMA, CPCO AHIMA Approved ICD-10-CM/PCS Trainer/Ambassador
Senior ICD-10 Trainer
Contractor, Team: Dynamics Research Corporation/Standard Technology, INC.
Arlington, Va./Bethesda, Md.
Moderator: Sherray L. Holland, PA-C TBI Clinical Educator
Contract support to Defense and Veterans Brain Injury Center
Silver Spring, Md.

Webinar Details
2
Live closed captioning is available through Federal Relay
Conference Captioning (see the “Closed Captioning” box)
Webinar audio is not provided through Adobe Connect or
Defense Connect Online
- Dial: CONUS 888-877-0398; International 210-234-5878
- Use participant pass code: 3938468
Question-and-answer (Q&A) session
- Submit questions via the Q&A box

Resources Available for Download
3
Today’s presentation and resources are available for
download in the “Files” box on the screen, or visit
dvbic.dcoe.mil/online-education

Continuing Education Details
4
DCoE’s awarding of continuing education (CE) credit is limited in
scope to health care providers who actively provide psychological
health and traumatic brain injury care to active-duty U.S. service
members, reservists, National Guardsmen, military veterans
and/or their families.
The authority for training of contractors is at the discretion of the
chief contracting official. Currently, only those contractors with scope of work or with commensurate
contract language are permitted in this training.
All who registered prior to the deadline on Thursday, Aug. 14,
2014, at 3 p.m. (EDT) and meet eligibility requirements stated
above are eligible to receive CE credit or a certificate of
attendance.

Continuing Education Details (continued)
5
If you pre-registered for this webinar and want to obtain
a CE certificate or a certificate of attendance, you must
complete the online CE evaluation and post-test.
After the webinar, visit
http://continuingeducation.dcri.duke.edu to complete the
online CE evaluation and post-test, and download your
CE certificate/certificate of attendance.
The Duke Medicine website online CE evaluation and
post-test will be open through Thursday, Aug. 21, 2014,
until 11:59 p.m. (EDT).

Continuing Education Details (continued)
Credit Designation – The Duke University School of Medicine
designates this live webinar for:
1.5 AMA PRA Category 1 Credit(s)
Additional Credit Designation includes:
1.5 ANCC nursing contact hours
0.15 IACET continuing education credit
1.5 NBCC contact hours credit commensurate to the length of the
program
1.5 contact hours from the North Carolina Psychology Board
1.5 NASW contact hours commensurate to the length of the program for
those who attend 100% of the program
6

Continuing Education Details (continued)
ACCME Accredited Provider Statement – The Duke University School of Medicine is accredited by the
Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
ANCC Accredited Provider Statement – Duke University Health System Department of Clinical Education &
Professional Development is accredited as a provider of continuing nursing education by the American Nurses Credentialing
Center’s (ANCC’s) Commission on Accreditation. 1.50 ANCC nursing contact hours are provided for participation in this
educational activity. In order to receive full contact-hour credit for this activity, you must attend the entire activity, participate
in individual or group activities such as exercises or pre/post-tests, and complete the evaluation and verification of
attendance forms at the conclusion of the activity.
IACET Authorized Provider Statement – Duke University Health System Clinical Education & Professional
Development is authorized by the International Association for Continuing Education and Training (IACET) to offer 0.15
continuing education credit to participants who meet all criteria for successful completion of authorized educational
activities. Successful completion is defined as (but may not be limited to) 100% attendance, full participation and
satisfactory completion of all related activities, and completion and return of evaluation at conclusion of the educational
activity. Partial credit is not awarded.
Duke University Health System Clinical Education & Professional Development has been approved as an Authorized
Provider by the International Association for Continuing Education &Training (IACET), 1760 Old Meadow Road, Suite 500,
McLean, VA 22102. In obtaining this approval, Duke University Health System Clinical Education & Professional
Development has demonstrated that it complies with the ANSI/IACET 1-2007 Standard, which is widely recognized as the
standard of best practice in continuing education internationally. As a result of Authorized Provider status, Duke University
Health System Clinical Education & Professional Development is authorized to offer IACET CEU’s for its programs that
qualify under the ANSI/IACET 1-2007 Standard.
7

Continuing Education Details (continued)
NBCC: Southern Regional Area Health Education Center (AHEC) is a National Board for Certified Counselors and
Affiliates, Inc.(NBCC)-Approved Continuing Education Provider (ACEPTM) and a cosponsor of this event/program. Southern
Regional AHEC may award NBCC-approved clock hours for events or programs that meet NBCC requirements. The ACEP
maintains responsibility for the content of this event. Contact hours credit commensurate to the length of the program will be
awarded to participants who attend 100% of the program.
Psychology: This activity complies with all of the Continuing Education Criteria identified through the North Carolina
Psychology Board's Continuing Education Requirements (21 NCAC 54.2104). Learners may take the certificate to their
respective State Boards to determine credit eligibility for contact hours.
NASW: National Association of Social Workers (NASW), North Carolina Chapter: Southern Regional AHEC will award
contact hours commensurate to the length of the program to participants who attend 100% of the program.
8

Questions and Chat
9
Throughout the webinar, you are welcome to submit technical
or content-related questions via the Q&A pod located on the
screen. Please do not submit technical or content-related
questions via the chat pod.
The Q&A pod is monitored during the webinar; questions will
be forwarded to presenters for response during the Q&A
session.
Participants may chat with one another during the webinar
using the chat pod.
The chat function will remain open 10 minutes after the
conclusion of the webinar.

Webinar Overview
10
The Defense and Veterans Brain Injury Center (DVBIC) reports an increase in traumatic brain
injuries (TBIs) in Defense Department numbers worldwide over the past two quarters.
All TBIs are to be documented or classified to a code from ICD-9-Clinical Modification. Proper
coding provides a detailed picture of a patient population, contributes to quality outcomes and
standards of care, permits correct reimbursements for clinical services and helps anticipate
demand for future services.
Medical coding professionals consider TBI coding to be “specialty” coding. Most lack experience
and clinical knowledge to code TBIs without guidance from coding specialists and clinical
colleagues.
Special rules apply to coding brain injuries in the Defense Department. Appendix G of the Military
Health System Coding Guidance: Professional Services and Specialty Coding Guidelines Version
3.6 contains rules that apply to coding brain injuries for both deployed and non-deployed settings.
These rules take precedence over any other coding guidance.
At the conclusion of the webinar, participants will be able to: Discuss definitions, medical terms and basic brain anatomy specific to TBI.
Articulate the importance of correct documentation for TBI and correct ICD-9-CM coding and compliance.
Analyze initial and subsequent TBI encounter documentation and validate and/or identify appropriate ICD-9-
CM codes.

Presenter: Amy Waller, CPC, CPMA, CPCO
More than 20 years experience in health care
coding, auditing, consulting, compliance, billing and
management in both civilian and military settings
Certified Professional Coder, Certified Professional
Medical Auditor and Certified Professional
Compliance Officer
AHIMA Approved ICD-10-CM/PCS Trainer/
Ambassador
Currently responsible for the ICD-10-CM/PCS
Training Program for the Army
Has trained more than 2,000 providers, coders and
administrators on ICD-10-CM/PCS
11
Amy Waller, CPC, CPMA, CPCO

Disclosures
12
The views expressed in this presentation are those
of the presenter and do not reflect the official policy
of the Defense Department (DoD) or the U.S.
Government.
The presenter does not intend to discuss the off-
label/investigative (unapproved) use of commercial
products or devices.

Breaking the Code: ICD-9-Clinical Modification (CM)
Diagnosis Coding for Traumatic
Brain Injury

Polling Question
How are you involved with TBI at your Military
Treatment Facility (MTF)?
A. Medical Doctor (MD)
B. Doctor of Osteopathic Medicine (DO)
C. Physical Therapist (PT)
D. Occupational Therapist (OT )
E. Speech-Language Pathologist (SLP)
F. Registered Nurse (RN)
G. Nurse Practitioner (NP)/Physician Assistant (PA)
H. Social Worker (SW)
I. Case Manager
J. Inpatient Coder
K. Outpatient Coder
J. Other
14
What is ICD-9-CM?
The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) is based on the World
Health Organization's Ninth Revision, International Classification of Diseases (ICD-9). ICD-9-CM is the official U.S. system of assigning codes to diagnoses and inpatient
procedures.
The National Center for Health Statistics (NCHS) and the Centers for Medicare & Medicaid Services (CMS) are the U.S. government agencies responsible for overseeing all
changes and modifications to ICD-9-CM.
15
History and Purpose
• ICD-9-CM has been in use since 1979.
• Statistical tracking of diseases was the intended
purpose of ICD-9-CM diagnosis codes (Volume 1
and 2).
• ICD-9-CM codes are used in the U.S. by payers for
billing and reimbursement purposes, not just for
epidemiological use.
Using a clinical system as a billing and reimbursement system has
many challenges. Many diagnoses do not have specific ICD-9-CM
codes. Changing to ICD-10-CM will alleviate some of these current
challenges, but it will add new ones as well, mainly for providers. 16

ICD-9-CM Classification
ICD-9-CM consists of three
volumes:
• Volume 1
• Tabular list containing a numerical list of the disease code numbers in tabular form
• Volume 2
• Alphabetical index to the disease entries
• Volume 3
• Classification system for surgical, diagnostic and therapeutic procedures (alphabetic index and tabular list)
17

ICD-10 Breakout
ICD-10-CM
• International
Classification of
Diseases 10th Revision,
Clinical Modification
– ALL Inpatient and
Outpatient Diagnosis
Codes
ICD-10-PCS
• International
Classification of
Diseases, 10th Revision,
Procedure Classification
System
– Inpatient Procedure
Codes ONLY
18

ICD-10-CM Facts
• Final rule for ICD-10-CM was implemented by the United States Department of Health and Human Services and published by CMS.
Who:
• ICD‐10-CM will replace ICD-9CM Vol. 1 & 2.
• ICD-10PCS will replace ICD-9CM Vol. 3.
• Both of these code sets will be unique to the U.S.
What:
• ALL healthcare organizations within the U.S. must make the transition.
• Workers Compensation Claims and Auto Accidents are exempt.
Where:
• Currently, the new ICD-10-CM compliance date is October 1, 2015. When:
19

TBI Definition Centers for Disease Control and Prevention
A TBI is caused by a bump, blow or jolt to the head or a penetrating head injury that disrupts the normal function of the brain.
• Not all blows or jolts to the head result in a TBI.
• Severity of a TBI may range from “mild” (i.e., a brief change in mental status or consciousness) to “severe” (i.e., an extended period of unconsciousness or memory loss after the injury).
• Most TBIs that occur each year are mild, commonly called concussions.
(Centers for Disease Control and Prevention, 2003) 20
TBI Definition Department of Defense (DoD)
A traumatically induced structural injury and/or physiological disruption of brain function as a result of external force that is indicated by new onset or worsening of at least one of the following clinical signs, immediately following the event:
• Any period of loss of or a decreased level of consciousness
• Any loss of memory for events immediately before or after the injury
• Any alteration in mental state at the time of the injury (confusion, disorientation, slowed thinking, etc.)
• Neurological deficits (weakness, loss of balance, change in vision, praxis, paresis/plegia, sensory loss, aphasia, etc.) that may or may not be transient
• Intracranial lesion
(Department of Defense, 2007)
21

External Forces
• External forces may include any of the following events:
– Head being struck by an object
– Head striking an object
– Brain undergoing an acceleration/deceleration movement
without direct external trauma to the head
– Foreign body penetrating the brain
– Forces generated from events such as a blast or
explosion, or other force yet to be defined
22 (Department of Defense, 2007)
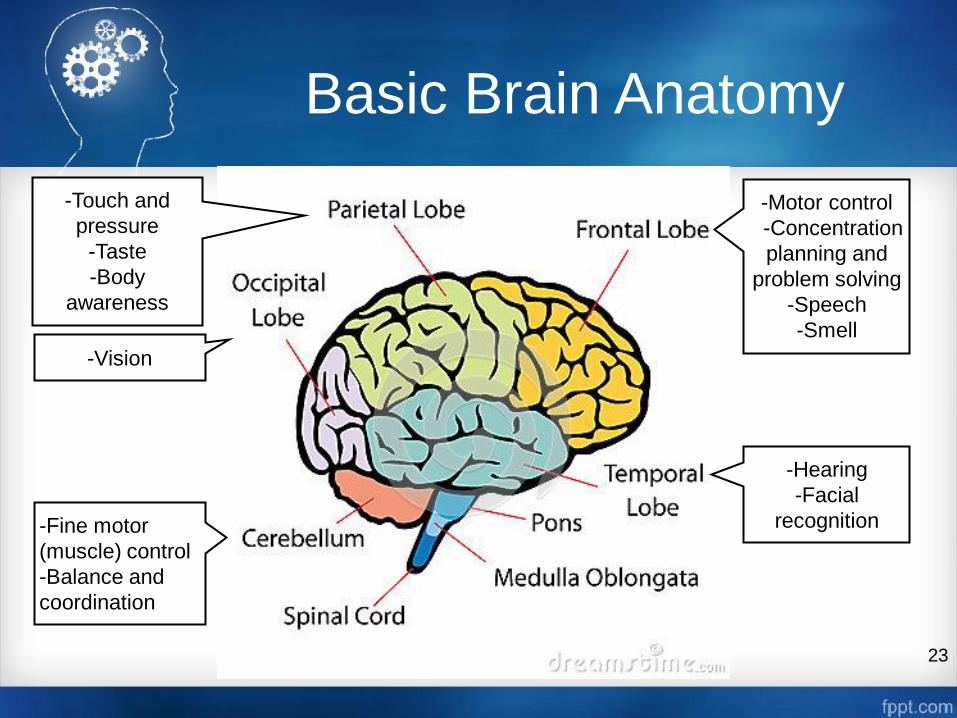
Basic Brain Anatomy
-Motor control
-Concentration
planning and
problem solving
-Speech
-Smell
-Hearing
-Facial
recognition
-Touch and
pressure
-Taste
-Body
awareness
-Vision
-Fine motor
(muscle) control
-Balance and
coordination
23

Brain Viewed from Above
Right Side Left Side
Judging the position of things in space
Knowing body position
Understanding and remembering things we do and see
Putting bits of information together to make an entire picture
Controls the left side of the body
Understanding and use of language (listening, reading, speaking and writing)
Memory for spoken and written messages
Detailed analysis of information
Controls the right side of the body
24
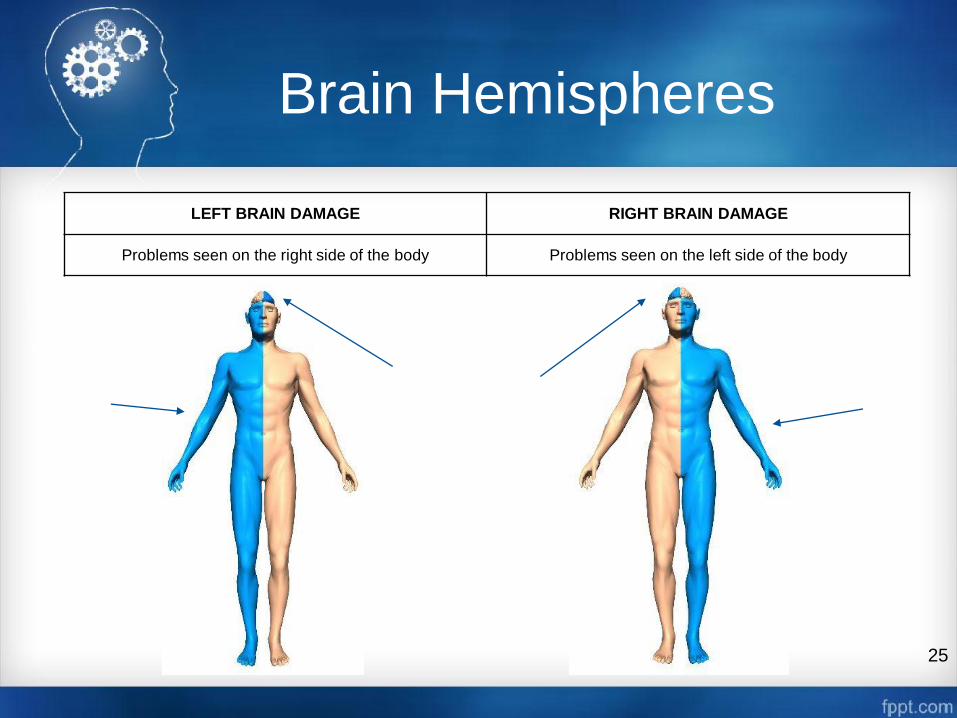
Brain Hemispheres
LEFT BRAIN DAMAGE RIGHT BRAIN DAMAGE
Problems seen on the right side of the body Problems seen on the left side of the body
25

TBI in Action
26 Coup Countercoup Injury

Polling Question
A TBI is defined as:
A. A traumatically-induced structural injury and/or physiological
disruption of brain function as a result of external force that is
indicated by new onset or worsening of at least one of the following
clinical signs, immediately following the event.
B. A TBI is caused by a bump, blow, or jolt to the head or a
penetrating head injury that disrupts the normal function of the
brain.
C. Both A and B
D. Neither A nor B
27
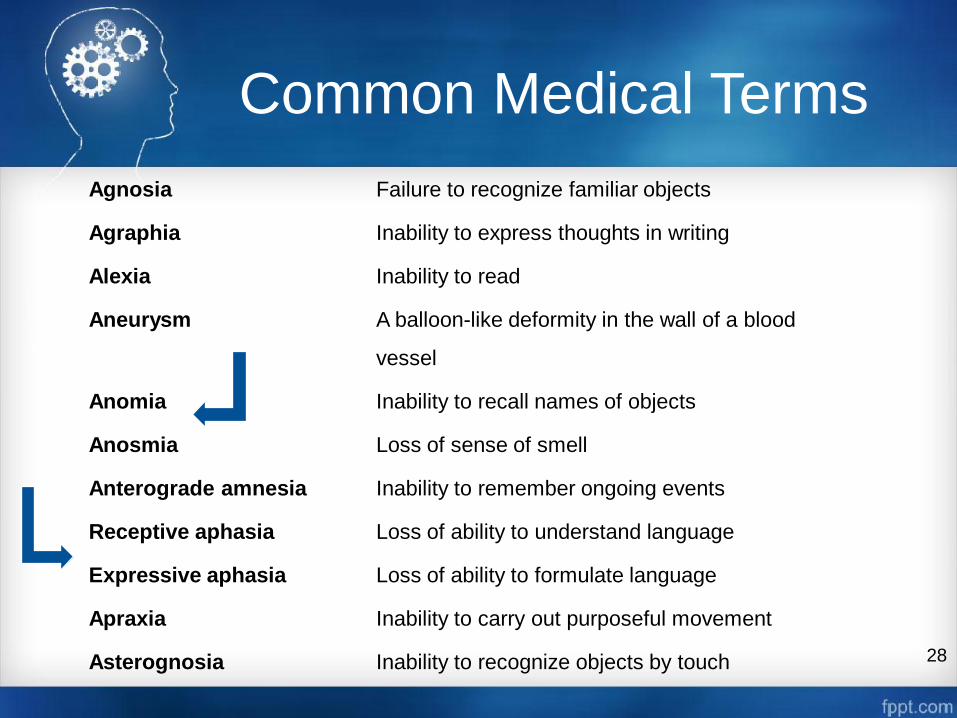
Common Medical Terms
Agnosia Failure to recognize familiar objects
Agraphia Inability to express thoughts in writing
Alexia Inability to read
Aneurysm A balloon-like deformity in the wall of a blood
vessel
Anomia Inability to recall names of objects
Anosmia Loss of sense of smell
Anterograde amnesia Inability to remember ongoing events
Receptive aphasia Loss of ability to understand language
Expressive aphasia Loss of ability to formulate language
Apraxia Inability to carry out purposeful movement
Asterognosia Inability to recognize objects by touch
28
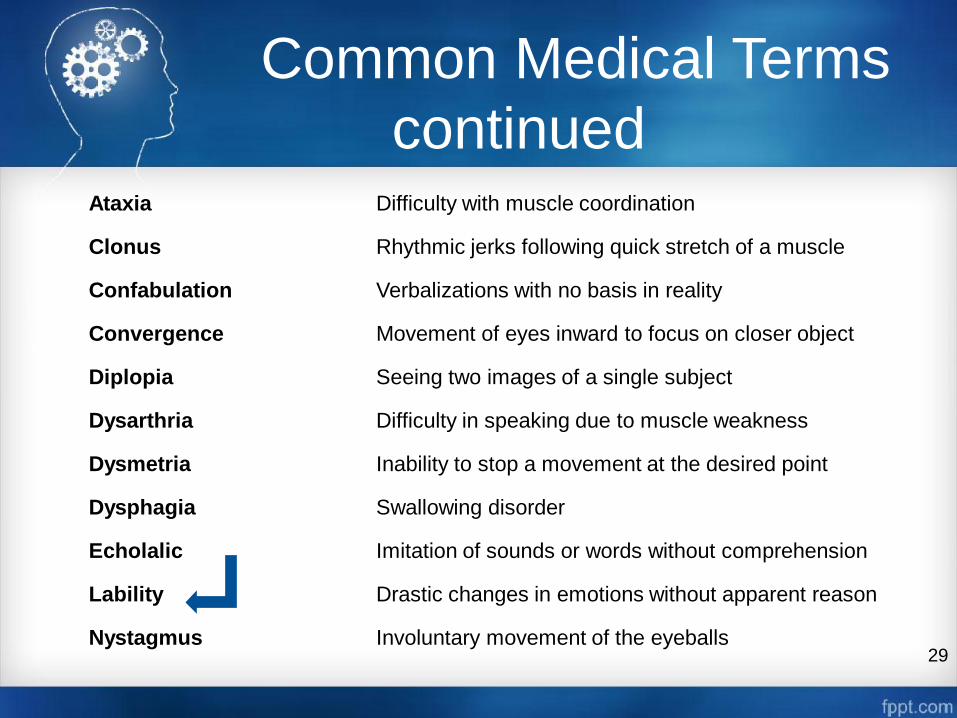
Common Medical Terms
continued Ataxia Difficulty with muscle coordination
Clonus Rhythmic jerks following quick stretch of a muscle
Confabulation Verbalizations with no basis in reality
Convergence Movement of eyes inward to focus on closer object
Diplopia Seeing two images of a single subject
Dysarthria Difficulty in speaking due to muscle weakness
Dysmetria Inability to stop a movement at the desired point
Dysphagia Swallowing disorder
Echolalic Imitation of sounds or words without comprehension
Lability Drastic changes in emotions without apparent reason
Nystagmus Involuntary movement of the eyeballs 29

TBI Acronyms
• GCS - Glasgow Coma Scale
• HI - Head Injury
• ICP - Intracranial Pressure
• IED - Improvised Explosive Device
• JPTA - Joint Patient Tracking
Application
• LOC - Loss of Consciousness
• LRMC - Landstuhl Regional Medical
Center
• MACE - Military Acute Concussion
Evaluation
• MEDEVAC - Medical Evacuation
• MRI - Magnetic Resonance Imaging
• mTBI - mild Traumatic Brain
Injury/concussion
• NICoE - National Intrepid Center of
Excellence
• PDHA - Post Deployment Health
Assessment
• PDHRA - Post Deployment Health Re-
Assessment
• PDS - Pre-deployment screening
• PM&R - Physical Medicine and
Rehabilitation
• PTSD - Post-Traumatic Stress
Disorder
• PTA - Post-Traumatic Amnesia
• RCC - Regional Care Coordinator
• REC - Regional Education Coordinator
• RPG - Rocket Propelled Grenade
• SRC - Soldier Readiness Center
• SRP - Soldier Readiness Process
• TBI - Traumatic Brain Injury
• VTC - Video Tele-Conference 30

Documentation
The ICD-9-CM and ICD-10-CM Official Guidelines for
Coding and Reporting state:
“The importance of consistent,
complete documentation in the
medical record cannot be
overemphasized..”
31 (Centers for Medicare & Medicaid Services, 2014)

Documentation Basics
Examples of clinical
documentation for outpatient
coding:
• An authenticated physician order for services
• Clinician visit notes
• A diagnosis or the reason the service was ordered
• Test results
• Therapies
• A problem list
• Medication list
32
NOTE: Coders should not be coding from all test results in the outpatient
setting; they are allowed to code from test reports that have a physician
interpretation and are authenticated by the attending physician.
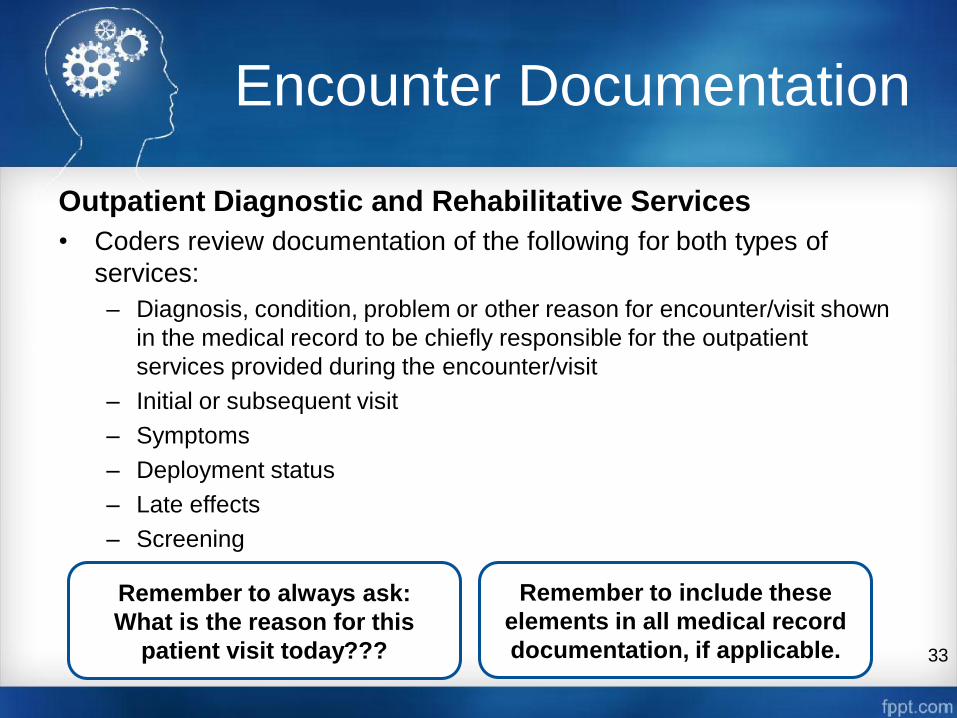
Encounter Documentation
Outpatient Diagnostic and Rehabilitative Services
• Coders review documentation of the following for both types of
services:
– Diagnosis, condition, problem or other reason for encounter/visit shown
in the medical record to be chiefly responsible for the outpatient
services provided during the encounter/visit
– Initial or subsequent visit
– Symptoms
– Deployment status
– Late effects
– Screening
33
Remember to always ask:
What is the reason for this
patient visit today???
Remember to include these
elements in all medical record
documentation, if applicable.

Other & Unspecified Codes
Other and unspecified codes are NOT the same!
“Other” Codes
– Codes titled “other” or “other specified”
• Usually a code with a 4th digit “8” or 5th digit “9” for diagnosis codes
• Use when the information in the medical record provides detail for
which a specific code does not exist
• Represent specific disease entities for which no specific code exists
so the term is included within an “other” code designation
“Unspecified” Codes
– Codes titled “un-specified”
• Usually a code with a 4th digit “9” or 5th digit “0” for diagnosis codes
• Use when the information in the medical record is insufficient to
assign a more specific code 34

TBI Level of Severity
35
The level of injury is based on observable signs at the time of injury.
Severity of injury does not predict functional or rehabilitative outcome of
the patient.
Mild Moderate Severe
Normal structural imaging Normal or abnormal
structural imaging
Normal or abnormal structural
imaging
LOC = 0 – 30 min LOC >30 min and <24 hours LOC >24 hours
AOC = a moment up to 24
hours AOC >24 hours. Severity based on other criteria
PTA = 0 – 1 day PTA >1 and <7 days PTA >7 days
AOC – Alteration of consciousness/mental state
PTA – Post-traumatic amnesia
LOC – Loss of consciousness
(Department of Defense, 2007)

Two Types of Encounters
Diagnostic Encounter
• ONLY medical providers can
diagnose a TBI.
• Initial or subsequent
• Codes types used:
– TBI diagnostic codes
– TBI V-codes
– Primary symptom codes
– Deployment status codes
– TBI screening code
– E-codes
– Other symptom codes
– Late effect codes
Rehabilitative Encounter
• Other privileged providers
MUST HAVE a medical
provider referral to treat.
• Initial or subsequent
• Code types used:
– Primary symptom code
– TBI V-code
– Late effect code
– Deployment status code
– Other symptom code
– Reason for visit code
36

Provider Visit Differences
Medical Provider
TBI Visits
• TBI screening, V80.01
Special screening for TBI:
– First positive screen:
• Initial encounter
– Seen again with
symptoms:
• Subsequent
encounter
Other Provider
TBI Visits
• Definitive TBI diagnosis by
Medical Provider:
– Receives referral:
• Initial encounter
– Seen again for e.g.,
therapy:
• Subsequent
encounter
37
Polling Question
Which of the following statement(s) is/are true?
A. When other and other specified appear in a code description, the
codes are assigned when patient record documentation provides
detail for which a specific code does not exist in ICD-9-CM.
B. Unspecified codes are assigned because patient record
documentation is insufficient to assign a more specific code.
C. Both A and B
D. Neither A nor B
38

TBI Diagnosis Codes (850 Code Series)
39
TBI Diagnosis Codes (850 Code Series)
Concussion
4th Digit: presence of loss of consciousness (LOC) 5th Digit: duration of LOC (if present)
0 No LOC 0 Unspecified state of consciousness
1 Brief LOC (requires 5th digit) 1 LOC of 30 minutes or less
2 Moderate LOC (1-24 hours) 2 LOC of 31 to 59 minutes
3 Prolonged LOC and return to pre-existing condition
4 Prolonged LOC without return to pre-existing condition
850.12 Concussion with loss of consciousness from 31 to 59 minutes
NOTE: TBI DIAGNOSIS CODES MAY ONLY BE USED BY A
MEDICAL PROVIDER
TBI Diagnosis Codes (851 Code Series)
40
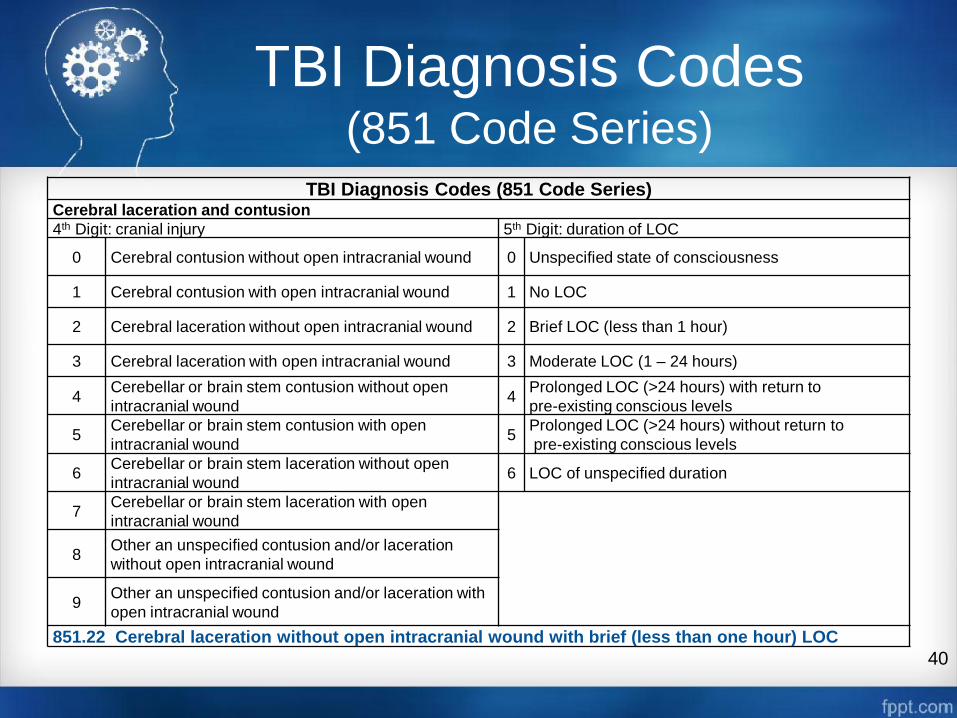
TBI Diagnosis Codes (851 Code Series) Cerebral laceration and contusion
4th Digit: cranial injury 5th Digit: duration of LOC
0 Cerebral contusion without open intracranial wound 0 Unspecified state of consciousness
1 Cerebral contusion with open intracranial wound 1 No LOC
2 Cerebral laceration without open intracranial wound 2 Brief LOC (less than 1 hour)
3 Cerebral laceration with open intracranial wound 3 Moderate LOC (1 – 24 hours)
4 Cerebellar or brain stem contusion without open
intracranial wound 4
Prolonged LOC (>24 hours) with return to
pre-existing conscious levels
5 Cerebellar or brain stem contusion with open
intracranial wound 5
Prolonged LOC (>24 hours) without return to
pre-existing conscious levels
6 Cerebellar or brain stem laceration without open
intracranial wound 6 LOC of unspecified duration
7 Cerebellar or brain stem laceration with open
intracranial wound
8 Other an unspecified contusion and/or laceration
without open intracranial wound
9 Other an unspecified contusion and/or laceration with
open intracranial wound
851.22 Cerebral laceration without open intracranial wound with brief (less than one hour) LOC

TBI Diagnosis Codes (852 Code Series)
41
TBI Diagnosis Codes (852 Code Series) Subarachnoid, subdural or extradural hemorrhage following injury
4th Digit: cranial injury 5th Digit: duration of LOC
0 Subarachnoid hemorrhage without open intracranial
wound 0 Unspecified state of consciousness
1 Subarachnoid hemorrhage with open intracranial
wound 1 No LOC
2 Subdural hemorrhage without open intracranial
wound 2 Brief LOC (less than 1 hour)
3 Subdural hemorrhage with open intracranial wound 3 Moderate LOC (1 – 24 hours)
4 Extradural hemorrhage without open intracranial
wound 4
Prolonged LOC (>24 hours) with return to pre-existing
conscious levels
5 Extradural hemorrhage with open intracranial wound 5 Prolonged LOC (>24 hours) without return to pre-existing
conscious levels
6 LOC of unspecified duration
Example: 852.33 Subdural hemorrhage with open intracranial wound and moderate LOC (1 – 24
hours)
TBI Diagnosis Codes (800-804 & 853-854 Code Series)
42
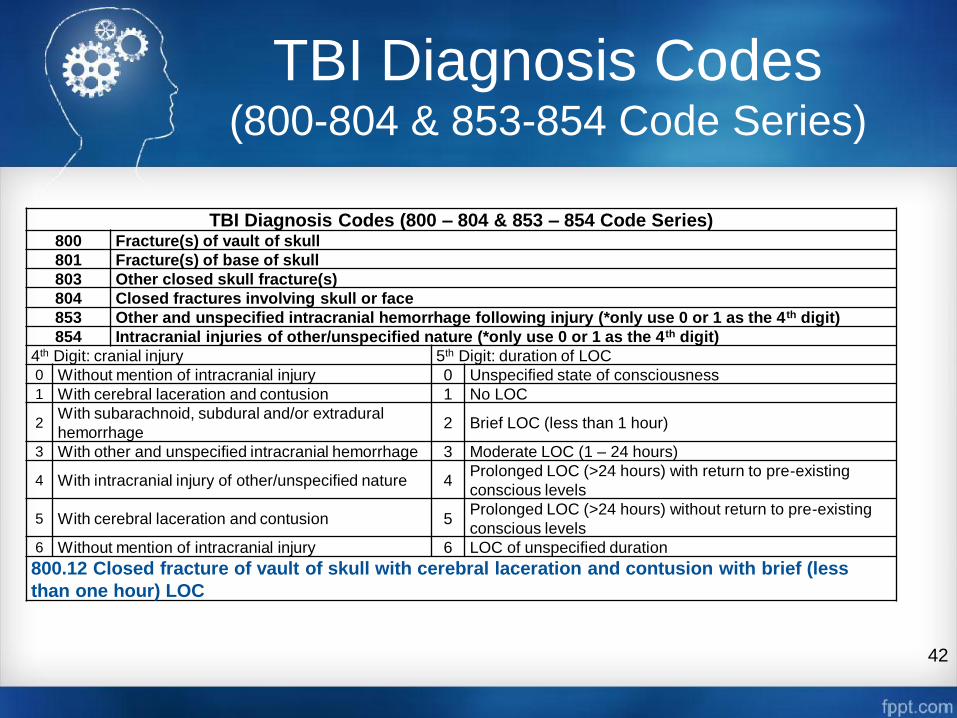
TBI Diagnosis Codes (800 – 804 & 853 – 854 Code Series) 800 Fracture(s) of vault of skull
801 Fracture(s) of base of skull
803 Other closed skull fracture(s)
804 Closed fractures involving skull or face
853 Other and unspecified intracranial hemorrhage following injury (*only use 0 or 1 as the 4th digit)
854 Intracranial injuries of other/unspecified nature (*only use 0 or 1 as the 4th digit)
4th Digit: cranial injury 5th Digit: duration of LOC 0 Without mention of intracranial injury 0 Unspecified state of consciousness 1 With cerebral laceration and contusion 1 No LOC
2 With subarachnoid, subdural and/or extradural
hemorrhage 2 Brief LOC (less than 1 hour)
3 With other and unspecified intracranial hemorrhage 3 Moderate LOC (1 – 24 hours)
4 With intracranial injury of other/unspecified nature 4 Prolonged LOC (>24 hours) with return to pre-existing
conscious levels
5 With cerebral laceration and contusion 5 Prolonged LOC (>24 hours) without return to pre-existing
conscious levels 6 Without mention of intracranial injury 6 LOC of unspecified duration
800.12 Closed fracture of vault of skull with cerebral laceration and contusion with brief (less
than one hour) LOC

V-code Definition
43
• Encounters for circumstances other than disease or injury
• V-codes (codes V01–V91) are used to describe encounters with circumstances other than disease or injury
• V-codes are used either as a first listed (primary) or contributing (secondary) code depending on the situation
V-Code Definition:
Index entries for V-codes are included in the
main Alphabetic Index in ICD-9-CM Volume 2.
DoD TBI Extender Codes
Some ICD-9-CM codes have been modified by the DoD to meet the needs of the Services.
One-character extender is paired with a specific ICD-9-CM code to acquire a unique meaning.
• Physicals
• Asthma
• Hepatitis
• Abortion
• Bacterial disease
• Gulf War-related diagnoses
Used to address a number of specific reporting requirements
44

DoD TBI V-code Usage
If an extender has been established in accordance with specificity guidelines, the root code is no longer valid for use without an
extender code.
This is crucial for TBI surveillance purposes.
Personal history of TBI codes (V15.52_x) must be used with any diagnosed TBI encounter, initial or follow-up.
45

TBI V-codes
46
V-Code (must be used with all TBI
encounters)
Injury related to Global War on
Terrorism
Level of Severity
Unknown Mild Moderate Severe Penetrating
V15.52_0 Personal history of traumatic brain injury NOT otherwise specified
V15.52_1 Yes X
V15.52_2 Yes X
V15.52_3 Yes X
V15.52_4 Yes X
V15.52_5 Yes X
V15.52_6 No X
V15.52_7 No X
V15.52_8 No X
V15.52_9 No X
V15.52_A No X
V15.52_B Unknown X
V15.52_C Unknown X
V15.52_D Unknown X
V15.52_E Unknown X
V15.52_F Unknown X

Polling Question
Severity of injury can sometimes predict
functional or rehabilitative outcome of the
patient.
A. True
B. False
47

Coding Symptoms
• Code symptoms when:
• Cases for which no more specific diagnosis can be made even after all facts bearing on the case have been investigated
• Signs or symptoms existing at the time of initial encounter that proved to be transient and whose causes could not be determined
• Provisional diagnoses in a patient who failed to return for further investigation or care
• Cases referred elsewhere for investigation or treatment before the diagnosis was made
• Cases in which a more precise diagnosis was not available for any other reason
• Certain symptoms which represent important problems in medical care and which it might be desired to classify in addition to a known cause
Codes that describe
symptoms and signs, as opposed to diagnoses, are
acceptable for reporting purposes
when an established
diagnosis has not been diagnosed (or confirmed) by the
physician.
48
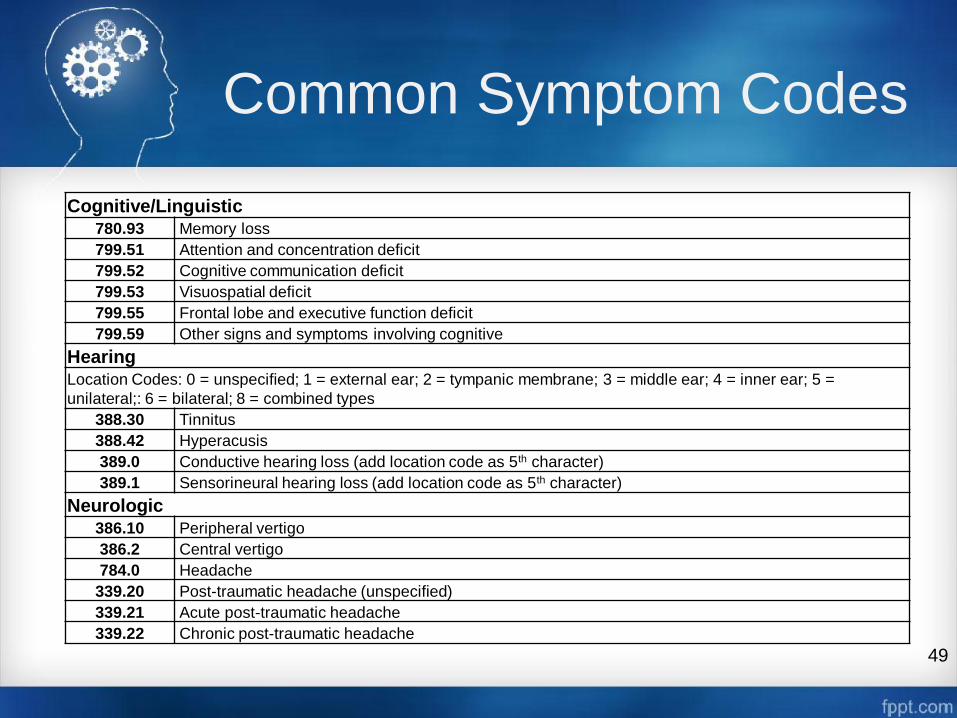
Common Symptom Codes
49
Cognitive/Linguistic 780.93 Memory loss
799.51 Attention and concentration deficit
799.52 Cognitive communication deficit
799.53 Visuospatial deficit
799.55 Frontal lobe and executive function deficit
799.59 Other signs and symptoms involving cognitive
Hearing
Location Codes: 0 = unspecified; 1 = external ear; 2 = tympanic membrane; 3 = middle ear; 4 = inner ear; 5 =
unilateral;: 6 = bilateral; 8 = combined types
388.30 Tinnitus
388.42 Hyperacusis
389.0 Conductive hearing loss (add location code as 5th character)
389.1 Sensorineural hearing loss (add location code as 5th character)
Neurologic
386.10 Peripheral vertigo
386.2 Central vertigo
784.0 Headache
339.20 Post-traumatic headache (unspecified)
339.21 Acute post-traumatic headache
339.22 Chronic post-traumatic headache

More Symptom Codes
50
Emotional/Behavioral
799.21 Nervousness
799.22 Irritability
799.23 Impulsiveness
799.24 Emotional lability
799.25 Demoralization and apathy
799.29 Other signs and symptoms involving emotional state
308.9 Acute stress reaction, unspecified
300 Anxiety/irritability
311 Depression
Sleep
780.52 Insomnia
327.23 Obstructive sleep apnea
327.3 Circadian rhythm sleep disorder: delayed type (327.31) or advanced type (327.32)
780.5 Sleep disturbance
Vision
368.13 Visual discomfort (e.g., photophobia)
368.8 Other specified visual disturbance

Late Effects
A late effect is the residual effect (condition produced) after the acute phase of an illness or injury has terminated.
• Acute phase is not defined and is left to clinical judgment
• No time limit on when a late effect code can be used
• Residual effect may be apparent early or it may occur months or years later
• Cerebrovascular accident
• Previous injury
• Never use the acute illness or injury code that led to the late effect with a late effect code.
51
Late Effect Codes
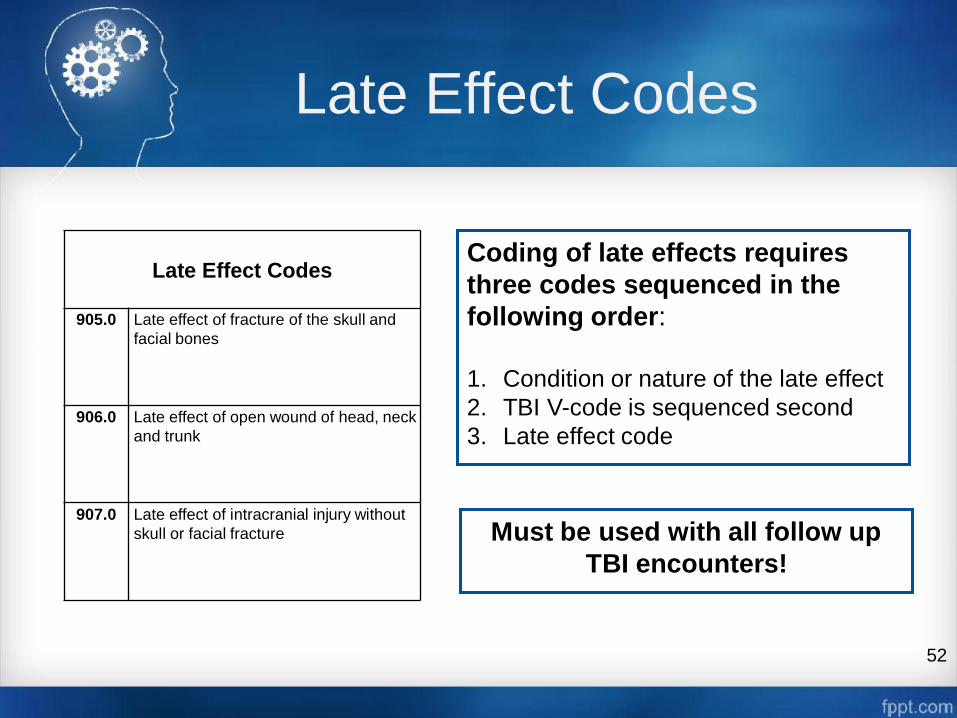
52
Late Effect Codes
905.0 Late effect of fracture of the skull and
facial bones
906.0 Late effect of open wound of head, neck
and trunk
907.0 Late effect of intracranial injury without
skull or facial fracture
Coding of late effects requires
three codes sequenced in the
following order:
1. Condition or nature of the late effect
2. TBI V-code is sequenced second
3. Late effect code
Must be used with all follow up
TBI encounters!
Polling Question
Codes that describe symptoms and signs, as
opposed to diagnoses, are never acceptable
for reporting purposes even when an
established diagnosis has not been diagnosed
(or confirmed) by the physician.
A. True
B. False
53

Deployment Codes
54
Deployment Status V-codes
V70.5_4
Pre-deployment encounter: Encounter related to a projected deployment. Could
include family members experiencing a condition related to the projected
deployment of the sponsor or other family member.
V70.5_5
During deployment encounter: Any deployment-related encounter performed while
individual (active duty [AD], contractor, etc.) is deployed. Could include family
members experiencing a condition related to the deployment of the sponsor or
other family member.
V70.5_6
Post-deployment encounter: Specifically performed because an individual was
deployed. Could include family members experiencing a condition related to a
prior deployment of the sponsor or other family member.

E-codes
• E-codes are supplemental codes that capture the external cause of
injury or poisoning, the intent and the place where the event
occurred.
• E-codes are intended to provide data for injury research and
prevention strategies.
• E-codes are never to be used as a primary diagnosis code.
55
E-codes
E979.2 Terrorism involving other explosions/fragments
E999 Late effects of injury due to war operations and terrorism
E993.3 Injury due to war operations by person-borne Improvised Explosive Device (IED)
E991.6 Injury due to war operations by vehicle-borne IED
E991.7 Injury due to war operations by other IED
Reason for Visit Codes
56
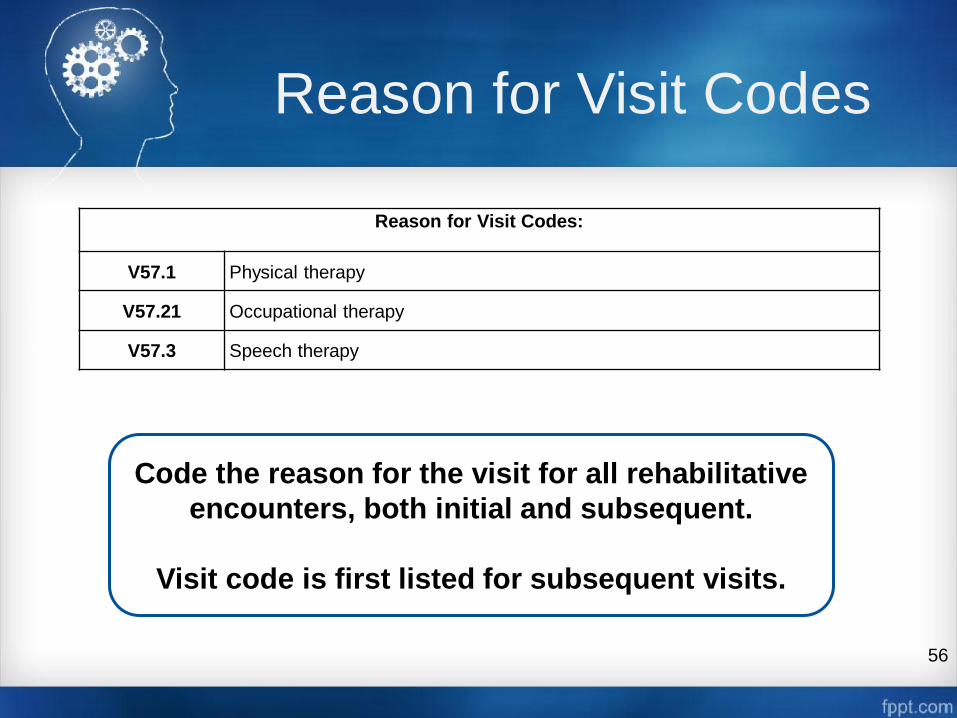
Reason for Visit Codes:
V57.1 Physical therapy
V57.21 Occupational therapy
V57.3 Speech therapy
Code the reason for the visit for all rehabilitative
encounters, both initial and subsequent.
Visit code is first listed for subsequent visits.

Code Sequencing Medical Provider – Initial
57
Order Description Code Example
1 Primary TBI Diagnosis Code 8XX.XX
2 TBI V-code V15.52_X
3 Primary symptom code 780.93
4 Deployment code, if applicable V70.5_X
5 TBI screening code V80.01
6 Other symptom codes, if applicable 784.0
7 E-code, if applicable E999
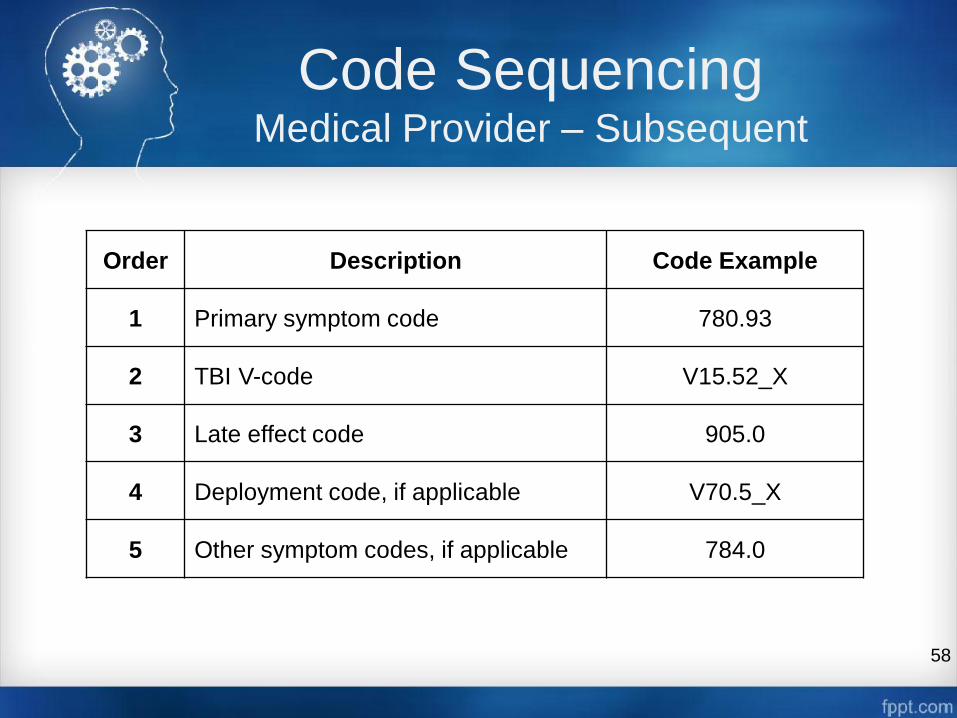
Code Sequencing Medical Provider – Subsequent
58
Order Description Code Example
1 Primary symptom code 780.93
2 TBI V-code V15.52_X
3 Late effect code 905.0
4 Deployment code, if applicable V70.5_X
5 Other symptom codes, if applicable 784.0
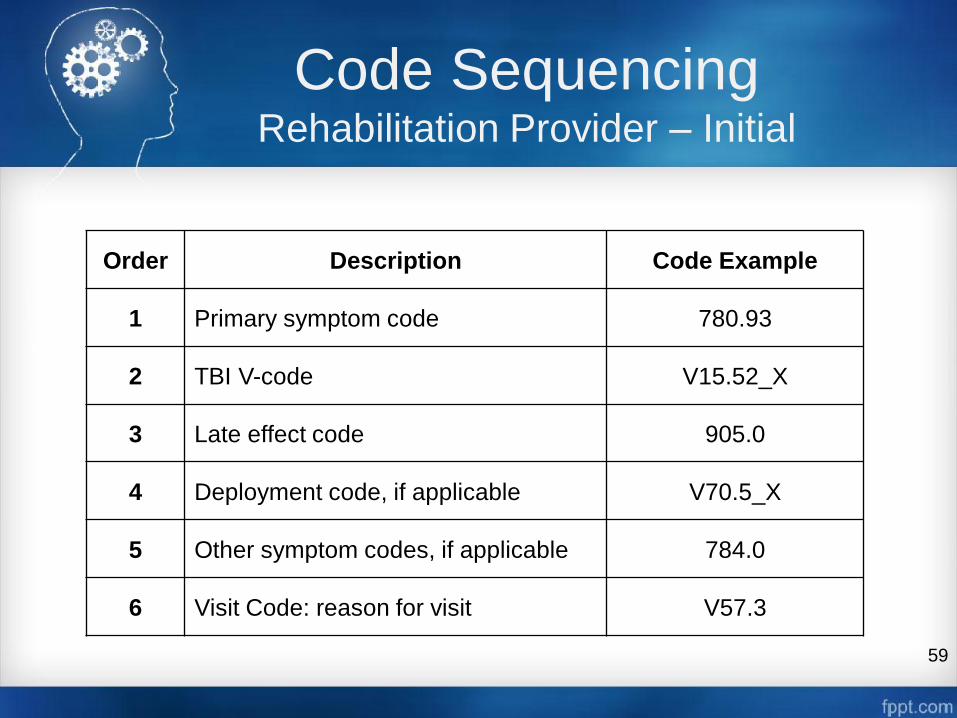
Code Sequencing Rehabilitation Provider – Initial
59
Order Description Code Example
1 Primary symptom code 780.93
2 TBI V-code V15.52_X
3 Late effect code 905.0
4 Deployment code, if applicable V70.5_X
5 Other symptom codes, if applicable 784.0
6 Visit Code: reason for visit V57.3

Code Sequencing Rehabilitation Provider – Subsequent
60
Order Description Code Example
1 Visit Code: reason for visit V57.3
2 TBI V-code V15.52_X
3 Late effect code 905.0
4 Deployment code, if applicable V70.5_X
5 Symptom codes, if applicable 780.52

Polling Question
Reason for visit codes must be used on all TBI
encounters.
A. True
B. False
61
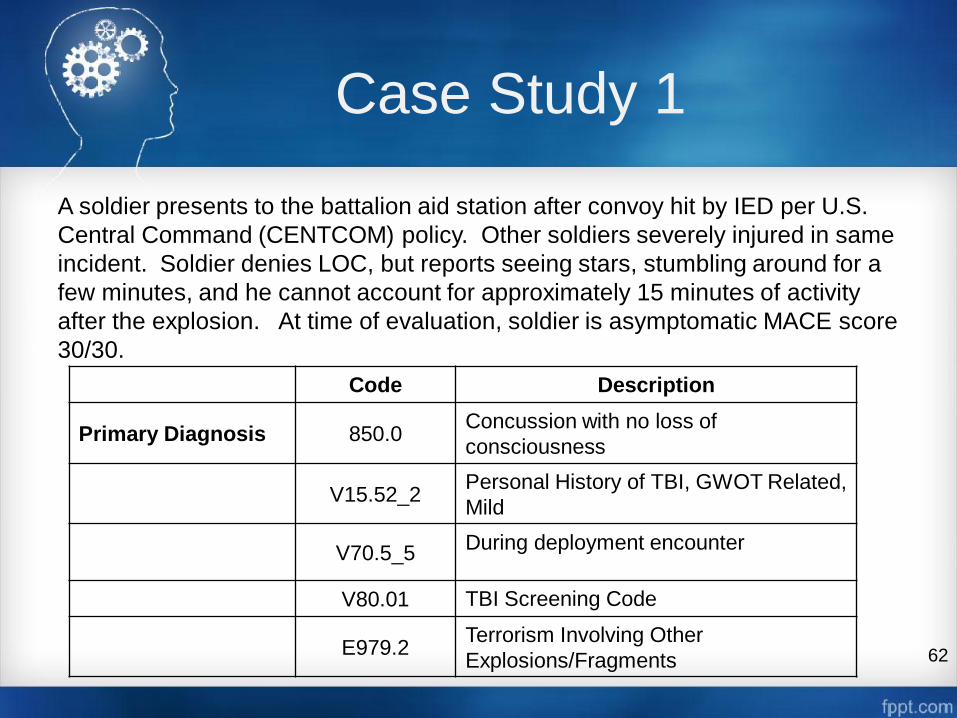
Case Study 1
A soldier presents to the battalion aid station after convoy hit by IED per U.S.
Central Command (CENTCOM) policy. Other soldiers severely injured in same
incident. Soldier denies LOC, but reports seeing stars, stumbling around for a
few minutes, and he cannot account for approximately 15 minutes of activity
after the explosion. At time of evaluation, soldier is asymptomatic MACE score
30/30.
62
Code Description
Primary Diagnosis 850.0 Concussion with no loss of
consciousness
V15.52_2 Personal History of TBI, GWOT Related,
Mild
V70.5_5 During deployment encounter
V80.01 TBI Screening Code
E979.2 Terrorism Involving Other
Explosions/Fragments

Case Study 2
A soldier presents to the MTF stating she is suffering from headaches
which date back to an explosion occurring in Iraq two weeks ago.
Provider reviews AHLTA (electronic health record) notes and finds a
note written immediately after the injury that document the injury event
associated with an alteration of consciousness coded with 850.0. The
provider determines that the complaints are acute.
NOTE: V15.52_x associates the acute symptom (headache) with TBI.
63
Code Description
Primary Diagnosis 784.0 Headache
Secondary
Diagnosis V15.52_2
Personal History of TBI, GWOT Related,
Mild
V70.5_6 Post deployment encounter

Case Study 3
A soldier presents to the clinic for evaluation of persistent headaches after she
answered yes to one of the TBI questions on the PDHA. Review of her AHLTA
notes reveals post-motor vehicle collision evaluation in theater with
documentation of right arm fracture and facial contusions six months ago, but
no documentation of TBI evaluation, no MACE, and no TBI diagnoses coded.
Follow up visits indicate complaint of headaches, but no documentation of
treatment. Patient interview reveals a history of headaches, tinnitus, intermittent
dizziness, and blurred vision since the accident. She also had grogginess and
poor recall of events for a few hours after the crash.
64
Code Description
Primary Diagnosis 850.0 Concussion with no LOC
V15.52_2 Personal History of TBI, GWOT Related,
Mild
784.0 Headache
V70.5_6 Post deployment encounter
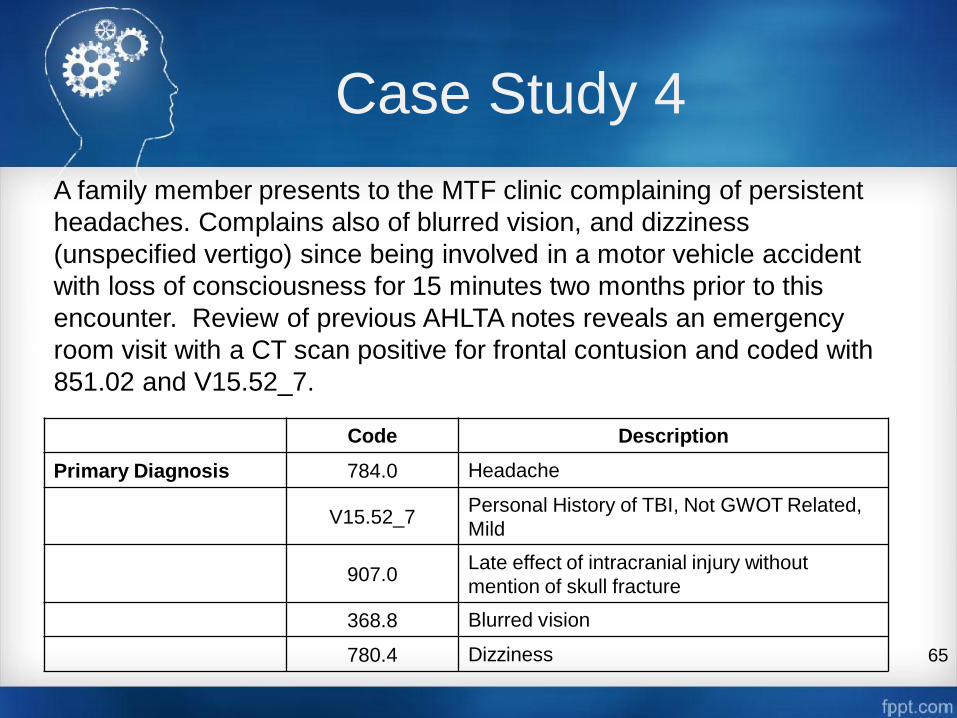
Case Study 4
A family member presents to the MTF clinic complaining of persistent
headaches. Complains also of blurred vision, and dizziness
(unspecified vertigo) since being involved in a motor vehicle accident
with loss of consciousness for 15 minutes two months prior to this
encounter. Review of previous AHLTA notes reveals an emergency
room visit with a CT scan positive for frontal contusion and coded with
851.02 and V15.52_7.
65
Code Description
Primary Diagnosis 784.0 Headache
V15.52_7 Personal History of TBI, Not GWOT Related,
Mild
907.0 Late effect of intracranial injury without
mention of skull fracture
368.8 Blurred vision
780.4 Dizziness

Accurately document
traumatic brain injury
encounters with current
Defense Department codes
Department of Defense ICD-9
Coding Guidance for
Traumatic Brain Injury
To order hard copies or download
electronic copies, visit dcoe.mil
References
Centers for Disease Control and Prevention. International Classification of Diseases, 9th Revision, Clinical Modification
(ICD-9-CM). Retrieved July 31, 2014, from http://www.cdc.gov/nchs/icd/icd9cm.htm
Center for Disease Control and Prevention, National Center for Injury Prevention and Control. (2003). Report to
Congress on mild traumatic brain injury in the United States: Steps to prevent a serious public health problem.
Retrieved from http://www.cdc.gov/traumaticbraininjury/pdf/mtbireport-a.pdf
Centers for Medicare & Medicaid Services. Coding. Retrieved July 31, 2014, from
http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalAcqCond/Coding.html
Centers for Medicare & Medicaid Services. International Classification of Diseases, 9th Revision, Clinical Modification
(ICD-9-CM). Retrieved July 31, 2014, from http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/codes.html
Centers for Medicare & Medicaid Services. International Classification of Diseases, 10th Revision, Clinical Modification
(ICD-10-CM). Retrieved July 31, 2014, from http://www.cms.gov/Medicare/Coding/ICD10/2014-ICD-10-CM-and-GEMs.html
U.S. Department of Defense, Defense Health Agency, Unified Biostatistical Utility. (2014). Military Health System coding guidance:
Professional services and specialty coding guidelines (Version 3.6). Retrieved from
http://www.tricare.mil/ocfo/bea/ubu/coding_guidelines.cfm
U.S. Department of Defense, Health Affairs. (2007). Memorandum from the Assistant Secretary of Defense S. Ward Casscells, M.D.
Retrieved from http://www.health.mil/~/media/MHS/Policy%20Files/Import/07-030.ashx
67

Access training materials, quick reference cards, patient self-report
measures and patient educational materials at dvbic.dcoe.mil
Learn how to evaluate and manage sleep
disturbances associated with a mild traumatic brain injury

Questions?
Submit questions via the
Q&A box located on the
screen.
The Q&A box is monitored
and questions will be
forwarded to our
presenters for response.
We will respond to as
many questions as time
permits.
69

Continuing Education Details
70
If you pre-registered for this webinar and want to obtain a
CE certificate or a certificate of attendance, you must
complete the online CE evaluation and post-test.
After the webinar, please visit
http://continuingeducation.dcri.duke.edu to complete the
online CE evaluation and post-test and download your CE
certificate/certificate of attendance.
The Duke Medicine website online CE evaluation and
post-test will be open through Thursday, Aug. 21, 2014,
until 11:59 p.m. (EDT).
Webinar Evaluation/Feedback
We want your feedback!
Please complete the Interactive Customer Evaluation
which will open in a new browser window after the
webinar, or visit:
https://ice.disa.mil/index.cfm?fa=card&sp=131517&s=10
19&dep=*DoD&sc=11
Or send comments to usarmy.ncr.medcom-usamrmc-
71
Chat and Networking
Chat function will remain open 10 minutes after the
conclusion of the webinar to permit webinar attendees to
continue to network with each other.
72


Save the Date
Next DCoE Psychological Health Webinar:
A Population Approach to Treatment
Engagement in Behavioral Health Care
Aug. 28, 2014
1-2:30 p.m. (EDT)
Next DCoE TBI Webinar:
Gender Differences and TBI
Oct. 9, 2014
1-2:30 p.m. (EDT)