cpap-1
TRANSCRIPT
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 1/80
Virginia Beach EMS
Oxy-PEEP C-PAPEric de Forest, NREMT-P
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 2/80
C-PAP Overview
?Applies continuous pressure to airways
to improve oxygenation.
?Bridge device to improve oxygenationuntil underlying cause of the respiratory
distress can be treated.

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 3/80
With any new subject, you’ve got
to learn the lingo
? NIPPV
? NIPSV
? C-PAP
? Bi-PAP
? I-PAP
? E-PAP? PEEP
? FiO2

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 4/80
With any new subject, you’ve got
to learn the lingo
? NIPPV Non-invasive positive pressure
ventilation
? NIPSV Non-invasive pressure supportventilation
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 5/80
With any new subject, you’ve got
to learn the lingo
? C-PAP Continuous positive airway pressure
? Bi-PAP Bi-level positive airway pressure
? I-PAP Inspiratory positive airway pressure
? E-PAP Expiratory positive airway pressure
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 6/80
With any new subject, you’ve got
to learn the lingo
? PEEP Positive end-expiratory pressure
? FiO2 Fraction of inspired air

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 7/80
C-PAP vs. PEEP
? C-PAP non-invasive
? PEEP for intubated
patients
? Terms usedinterchangeably
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 8/80
C-PAP vs. Bi-PAP
? C-PAP
– Continuous pressure
– 5-20 cm H2O
? Bi-PAP
– Alternating pressure
– More with inspiration
10 cm H2O
– Less with expiration5 cm H2O

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 9/80
Upper Airway?Mouth/Nose
?Oro/Nasopharynx
? Pharynx
? Epiglottis

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 10/80
Lower Airway? Larynx
? Trachea
?Main Bronchi (R/L)
? Bronchioles
? Alveoli
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 11/80
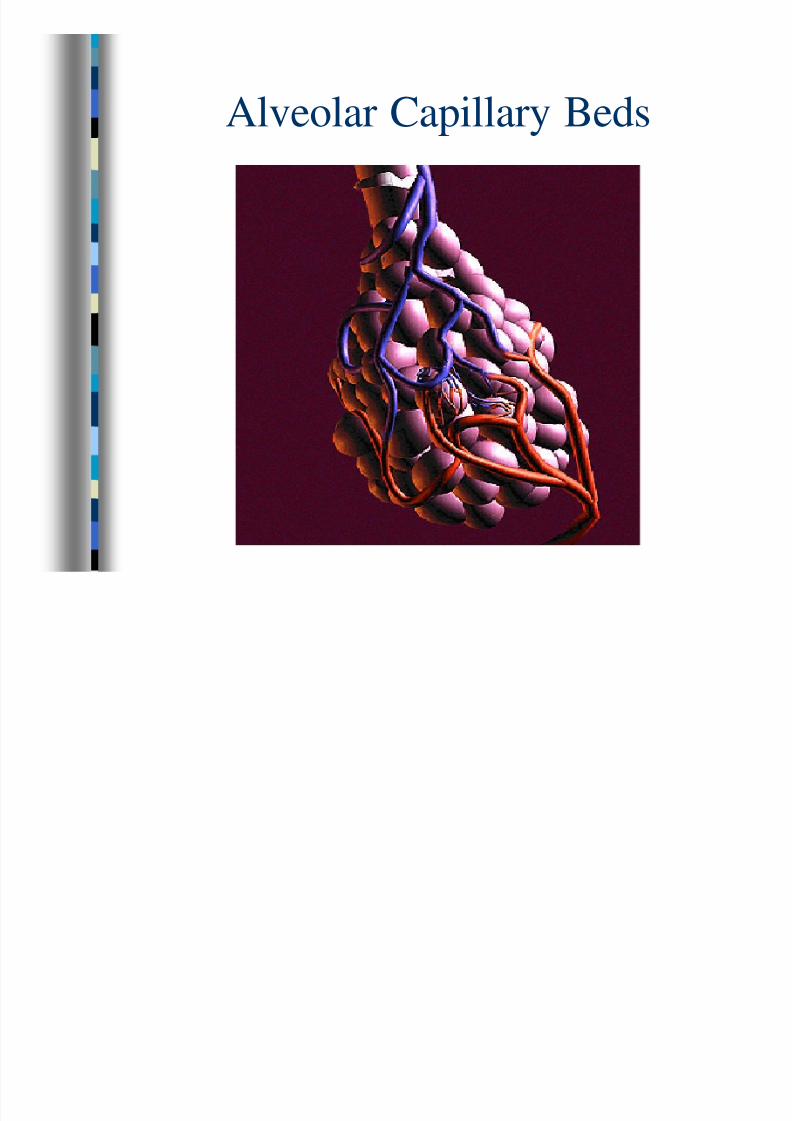
Alveolar Capillary Beds
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 12/80
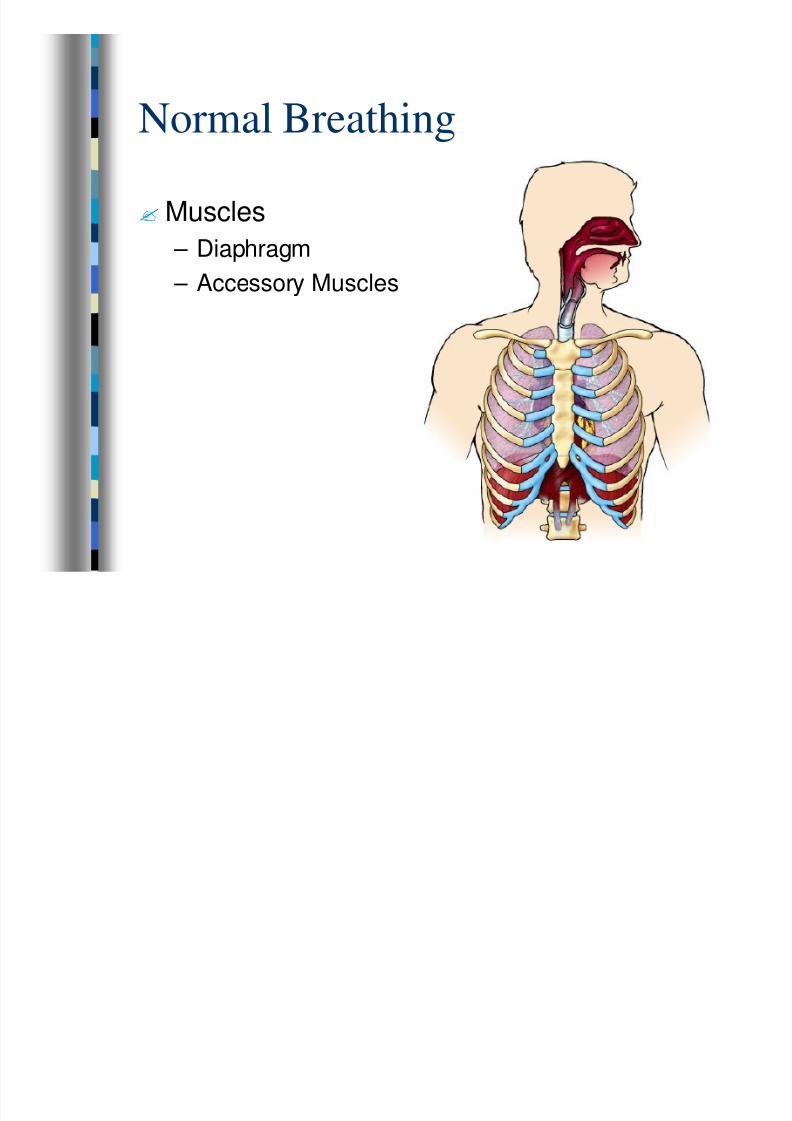
Normal Breathing
?Muscles
– Diaphragm
– Accessory Muscles

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 13/80
Inspiration
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 14/80
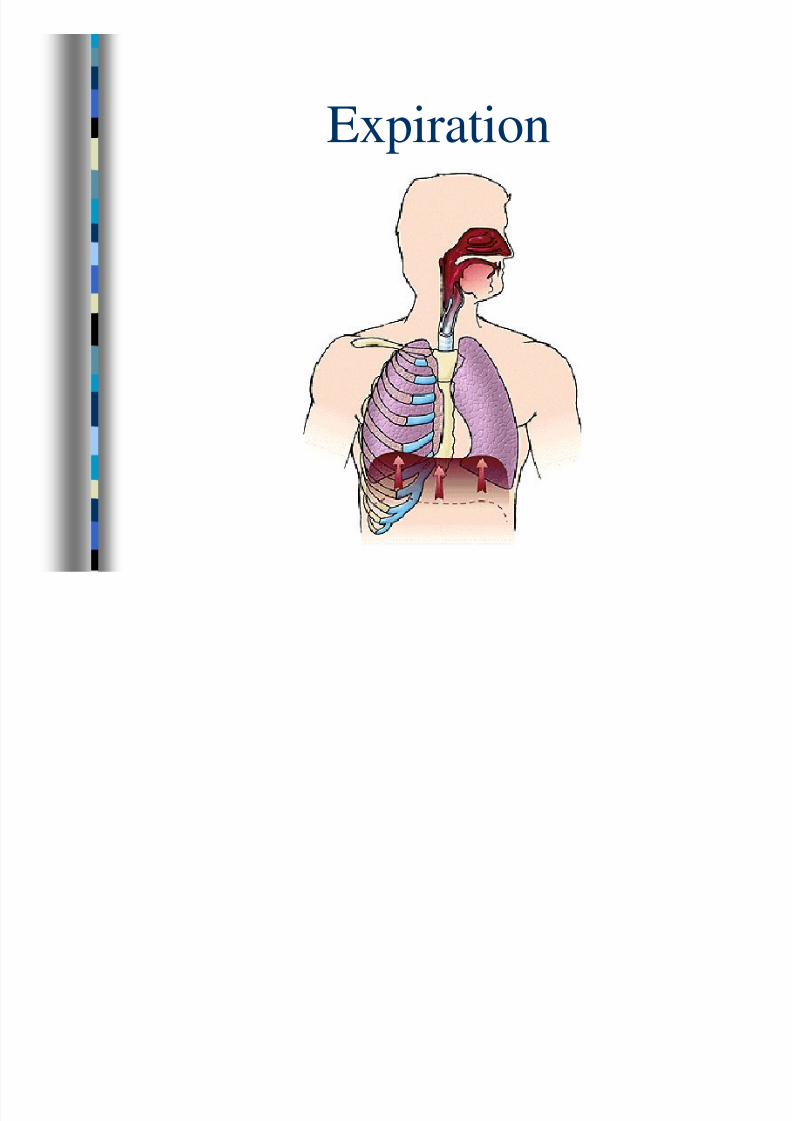
Expiration

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 15/80
Control of Breathing
? CO2 Level in
Arterial Blood
? Hypoxic Drive

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 16/80
Gas Exchange
?Ventilation
?Diffusion
?Perfusion

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 17/80
Ventilation
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 18/80
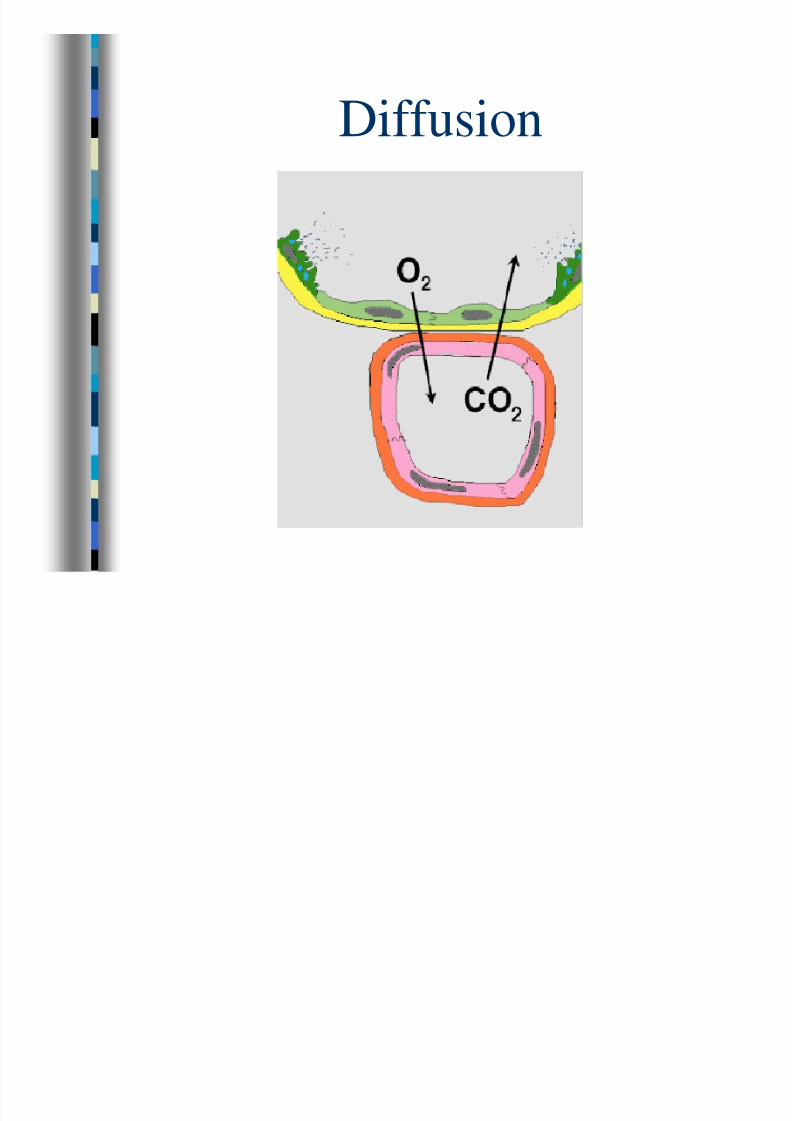
Diffusion
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 19/80
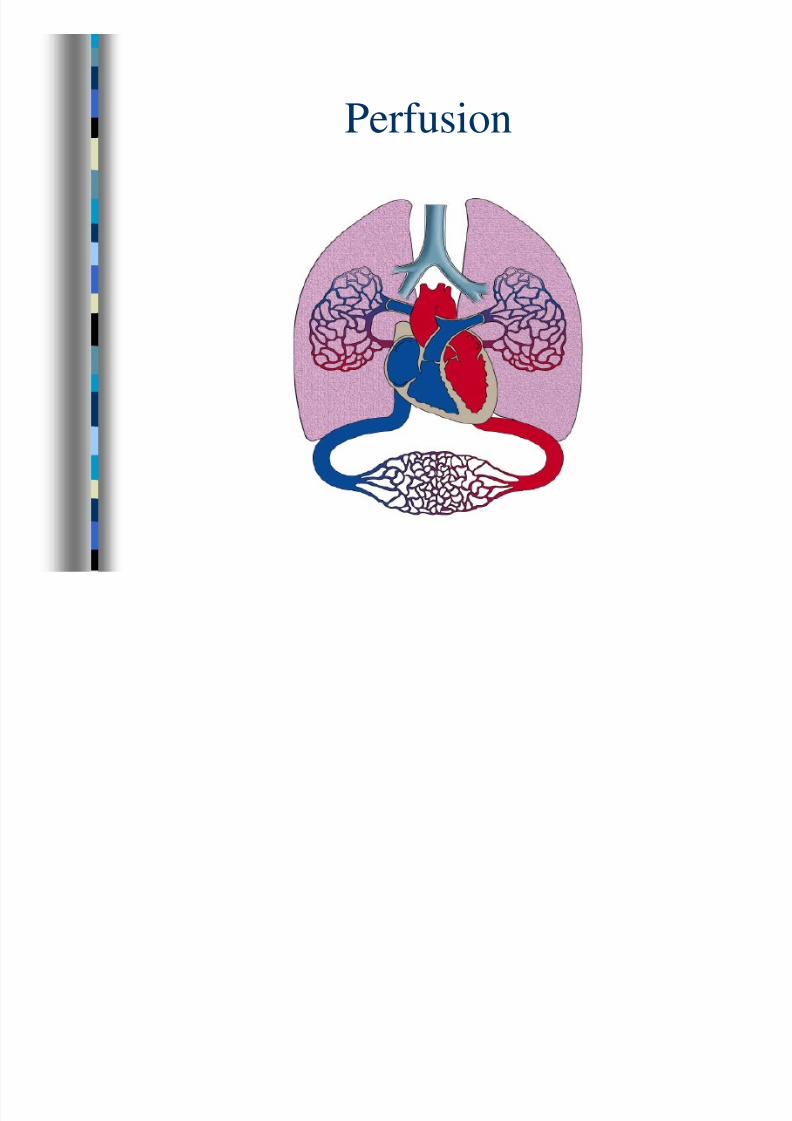
Perfusion

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 20/80
Congestive Heart Failure
? Left Ventricular
failure causes blood
to back up – Pulmonary
circulation (capillarybeds)
– Interstitial tissues – Alveoli
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 21/80
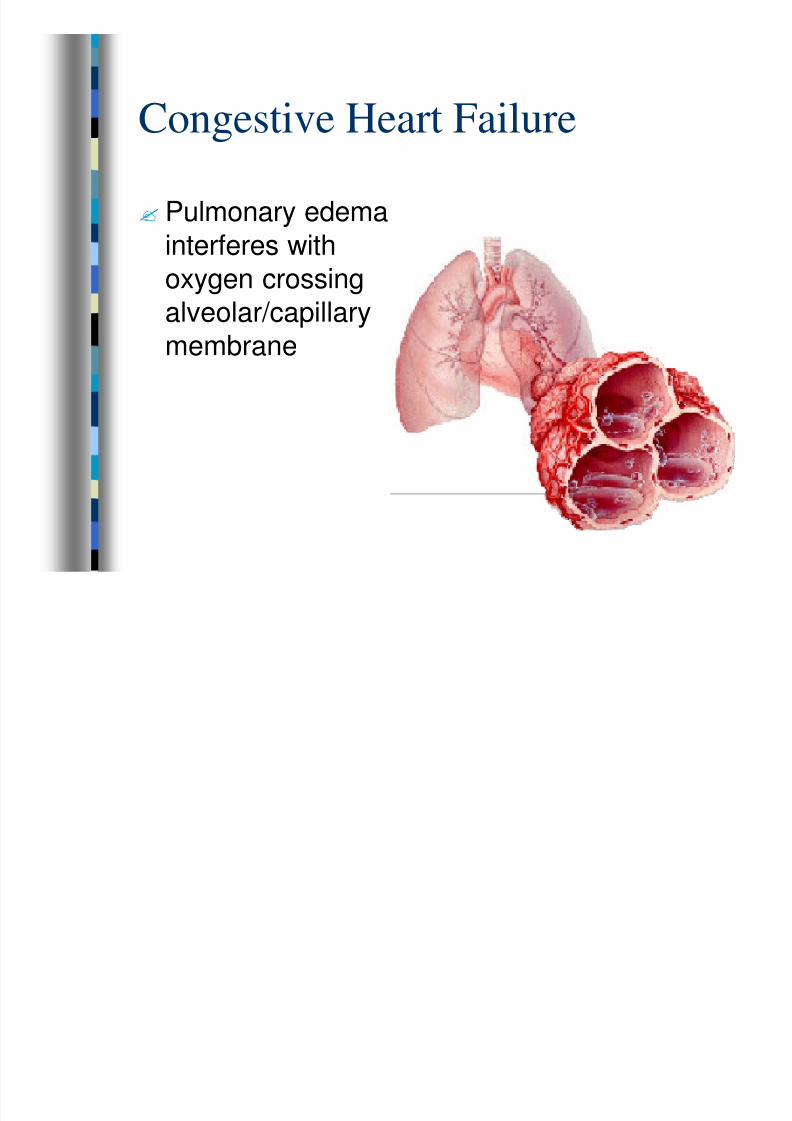
Congestive Heart Failure
? Pulmonary edema
interferes with
oxygen crossingalveolar/capillary
membrane
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 22/80
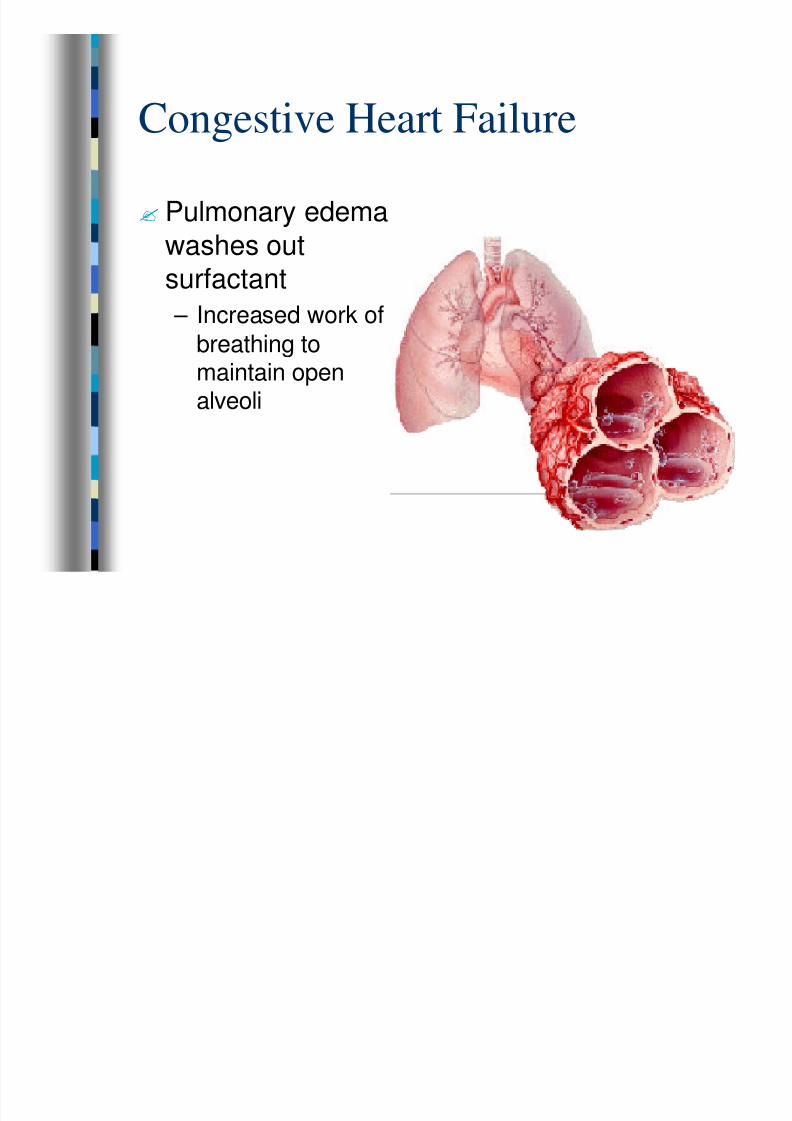
Congestive Heart Failure? Pulmonary edema
washes out
surfactant – Increased work of
breathing tomaintain openalveoli

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 23/80
CHF Infection? Bilateral rales or
crackles
? Clear or pinksputum
? Uni-lateral rales or
crackles
? Fever
? Productive coughwith green/yellow
sputum
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 24/80
COPD
?Chronic Obstructive Pulmonary Disease
– Emphysema
– Chronic Bronchitis
– Asthma
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 25/80
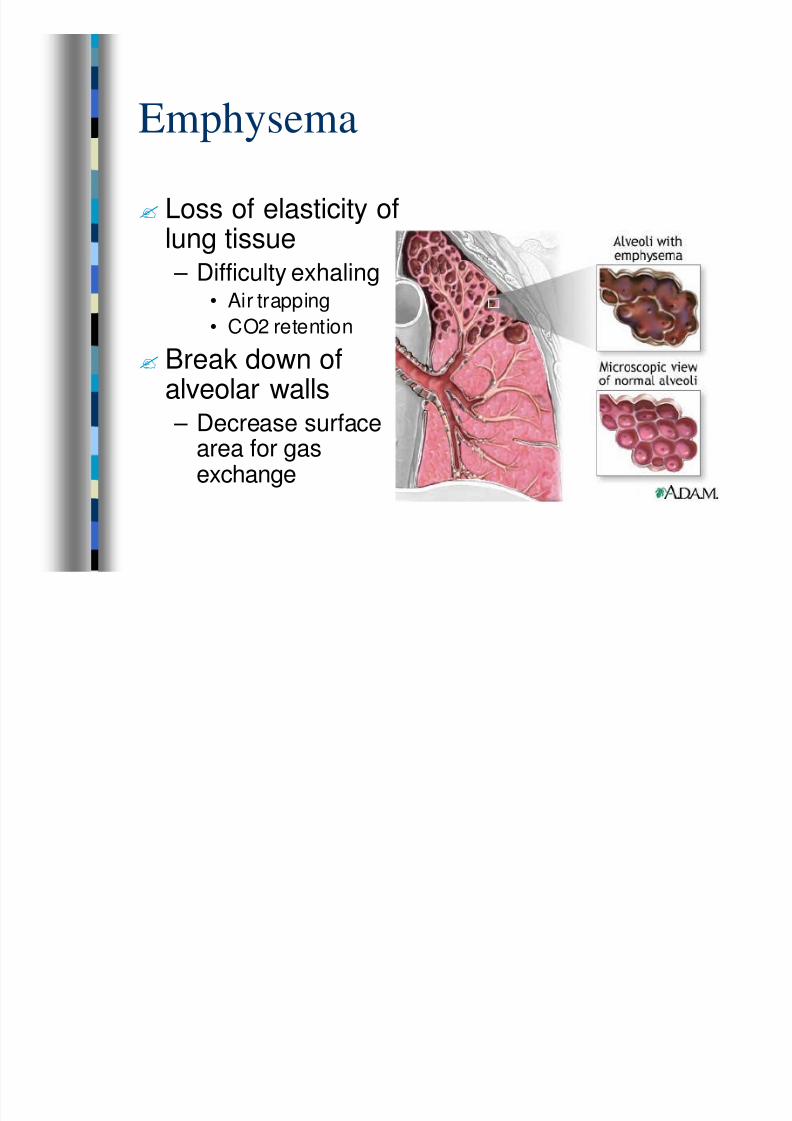
Emphysema? Loss of elasticity of
lung tissue
– Difficulty exhaling• Air trapping
• CO2 retention
? Break down ofalveolar walls
– Decrease surfacearea for gasexchange
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 26/80
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 27/80
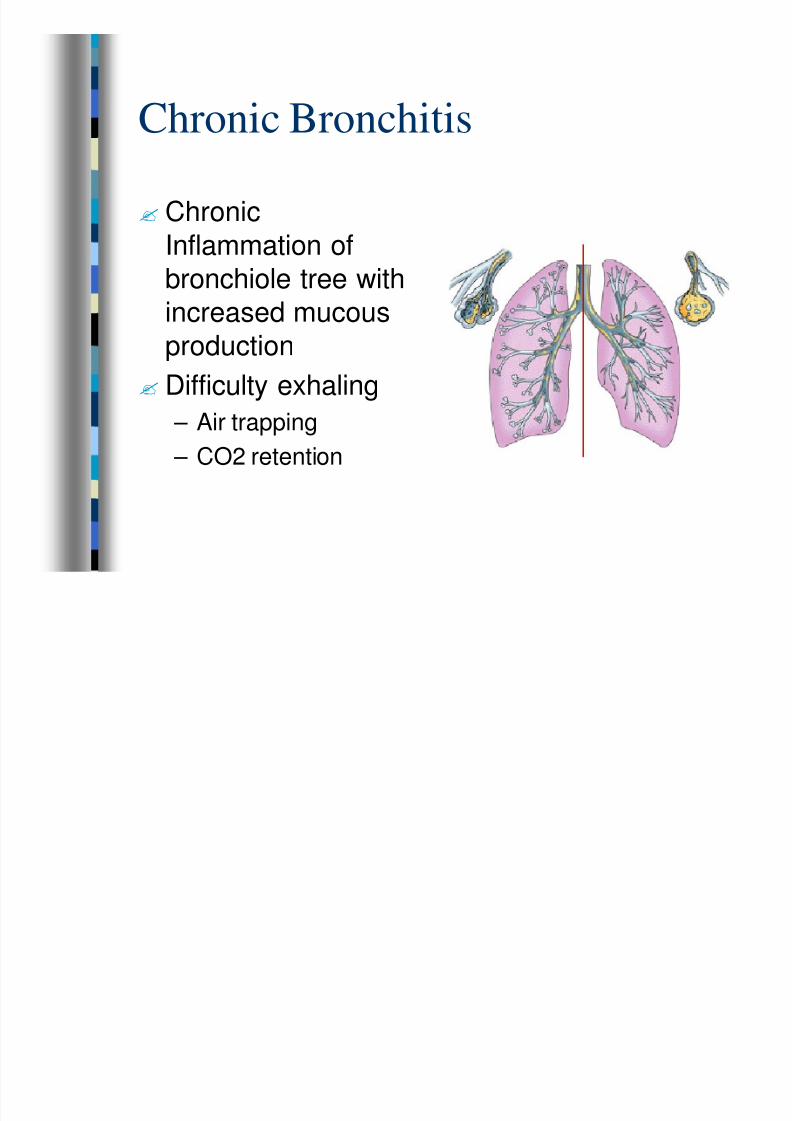
Chronic Bronchitis
? Chronic
Inflammation of
bronchiole tree withincreased mucous
production
? Difficulty exhaling
– Air trapping – CO2 retention
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 28/80
Asthma
? Intermittent
Bronchoconstriction
? Difficulty exhaling – Air trapping
– CO2 retention

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 29/80
Physiological Benefits of C-PAP
? Increase in alveolar pressure
– Stop fluid movement into alveoli
– Improves gas distribution
– Prevents alveolar collapse
– Improves re-expansion of alveoli
?Reduces work of breathing?Reduces respiratory muscle fatigue

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 30/80
Physiological Benefits of C-PAP
? Increases intrathoracic pressure
– Improves cardiac output to a point
– Too much PEEP decreases cardiac output
?Decreases need for intubation and
associated complications

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 31/80
Hazards/Complications of C-PAP
?Airway
– Mask impairs access to patient’s airway
– C-PAP does not ventilate the patient
– Gastric distension / vomiting
• Aerophagia (swallowing air) sensitive patients
– Gastric stapling
– Upper GI surgery
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 32/80
Hazards/Complications of C-PAP
?Hypoxia
– Loss of oxygen supply
• Empty oxygen tank
• Disconnection of Oxy-PEEP from oxygensource
– Mask Leak
– Rebound hypoxia may be more severethan initial hypoxia
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 33/80
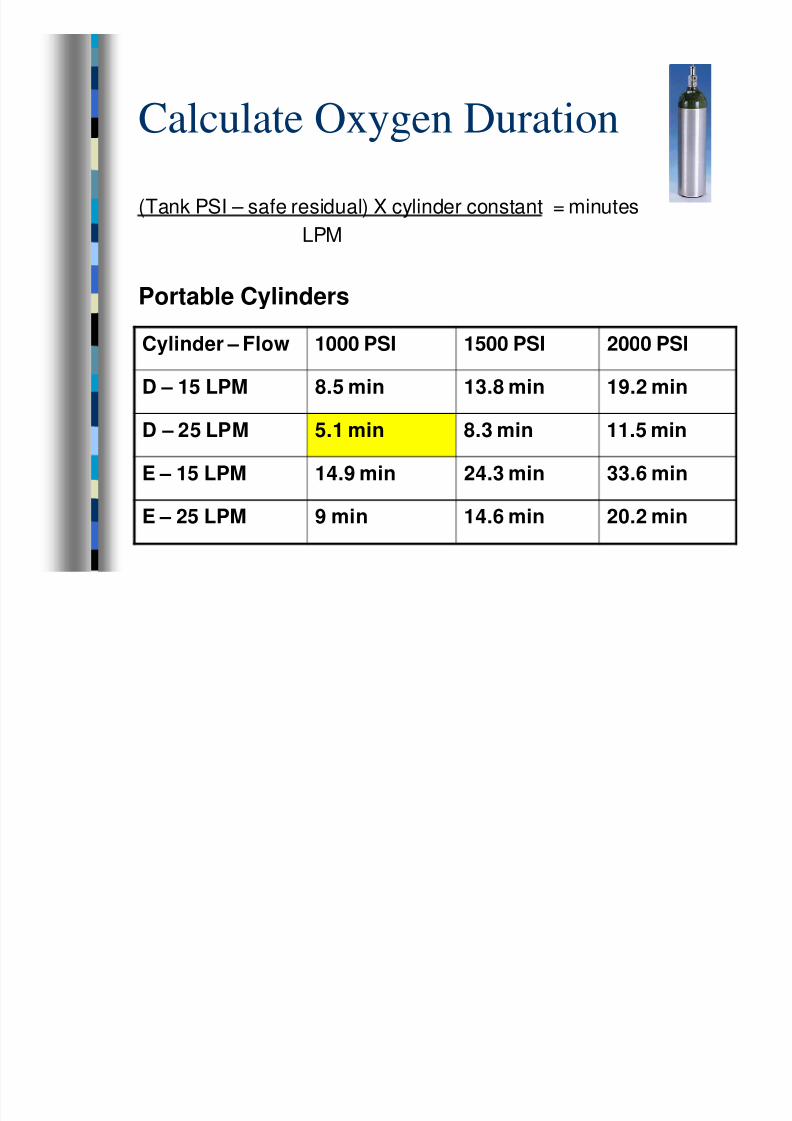
Calculate Oxygen Duration
(Tank PSI – safe residual) X cylinder constant = minutes
LPM
Portable Cylinders
Cylinder – Flow 1000 PSI 1500 PSI 2000 PSI
D – 15 LPM 8.5 min 13.8 min 19.2 min
D – 25 LPM 5.1 min 8.3 min 11.5 min
E – 15 LPM 14.9 min 24.3 min 33.6 min
E – 25 LPM 9 min 14.6 min 20.2 min
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 34/80
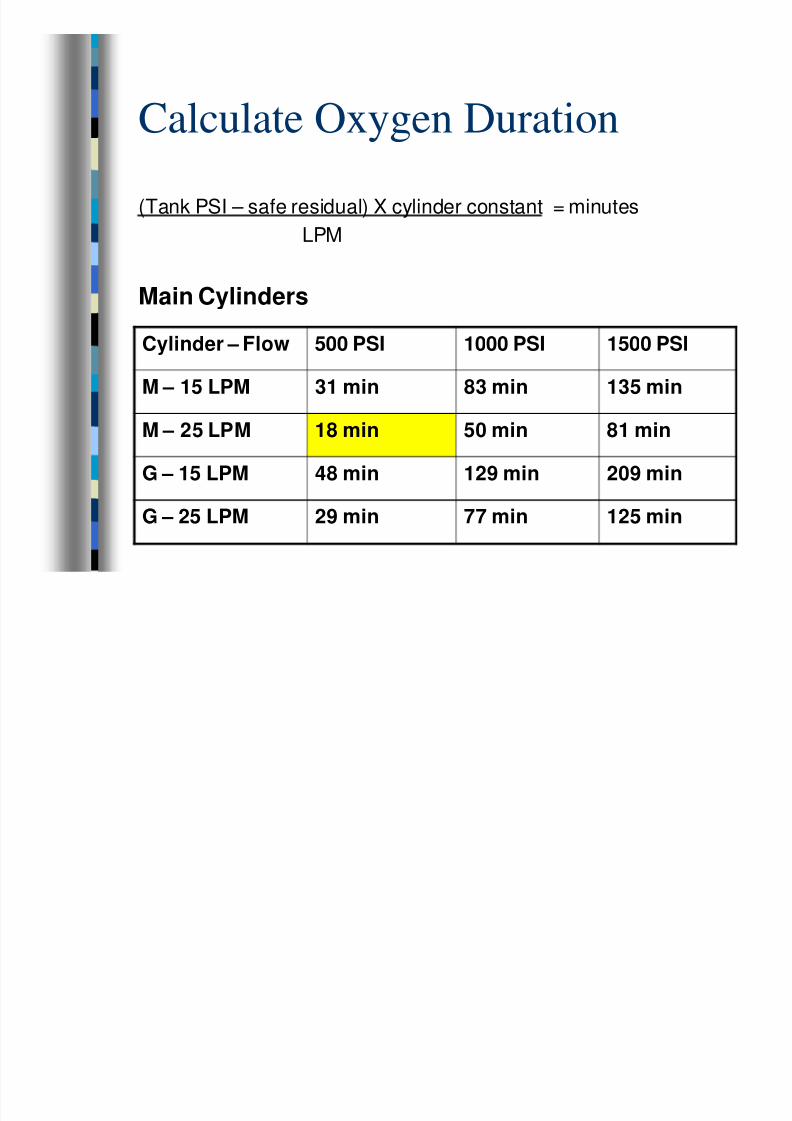
Calculate Oxygen Duration
(Tank PSI – safe residual) X cylinder constant = minutes
LPM
Main Cylinders
Cylinder – Flow 500 PSI 1000 PSI 1500 PSI
M – 15 LPM 31 min 83 min 135 min
M – 25 LPM 18 min 50 min 81 min
G – 15 LPM 48 min 129 min 209 min
G – 25 LPM 29 min 77 min 125 min
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 35/80
Hazards/Complications of C-PAP
?Hypotension
– Increased intrathoracic pressure causes
• Decreased venous return
• Decreased cardiac output
– Increased pulmonary pressure causes
• Decreased blood flow through pulmonaryvessels
• Decreased cardiac output
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 36/80
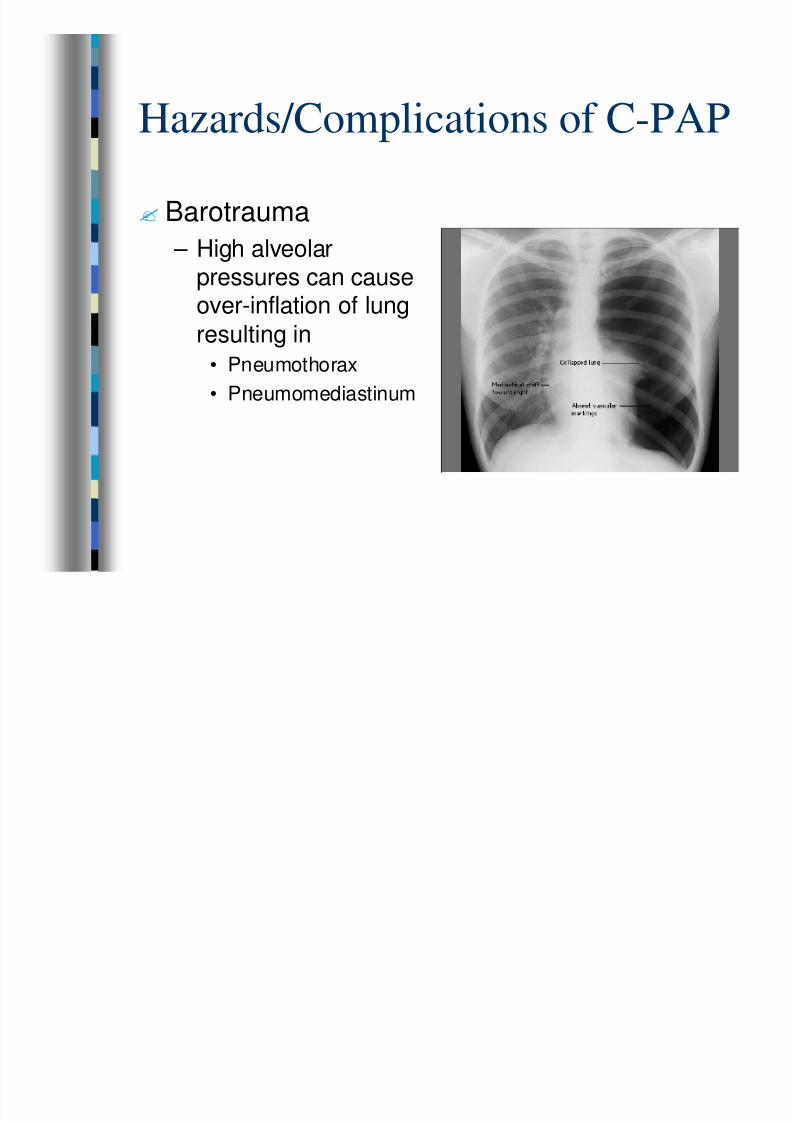
Hazards/Complications of C-PAP
? Barotrauma
– High alveolar
pressures can causeover-inflation of lung
resulting in
• Pneumothorax
• Pneumomediastinum
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 37/80
Concerns using C-PAP with
COPD? Increased Air
Trapping
? Hypotension? Barotrauma

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 38/80
Hazards/Complications of C-PAP
?More PEEP is NOT necessarily better
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 39/80
Hazards/Complications of C-PAP
?More PEEP is NOT necessarily better
– If 5 cm H2O PEEP is good it DOES NOT mean
that 10 cm H2O is better!!!
– Most patients will respond to 5 cm H2O PEEP

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 40/80
Hazards/Complications of C-PAP
?Patient Discomfort
– Requires patient cooperation to tolerate a
tightly fitting mask• Sensation of smothering or claustrophobia
– Use trial to introduce patient to device prior
to securing head strap
– Consider sedation for extreme anxiety withorders from Medical Control

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 41/80
Oxy-PEEP C-PAP
? Equipment
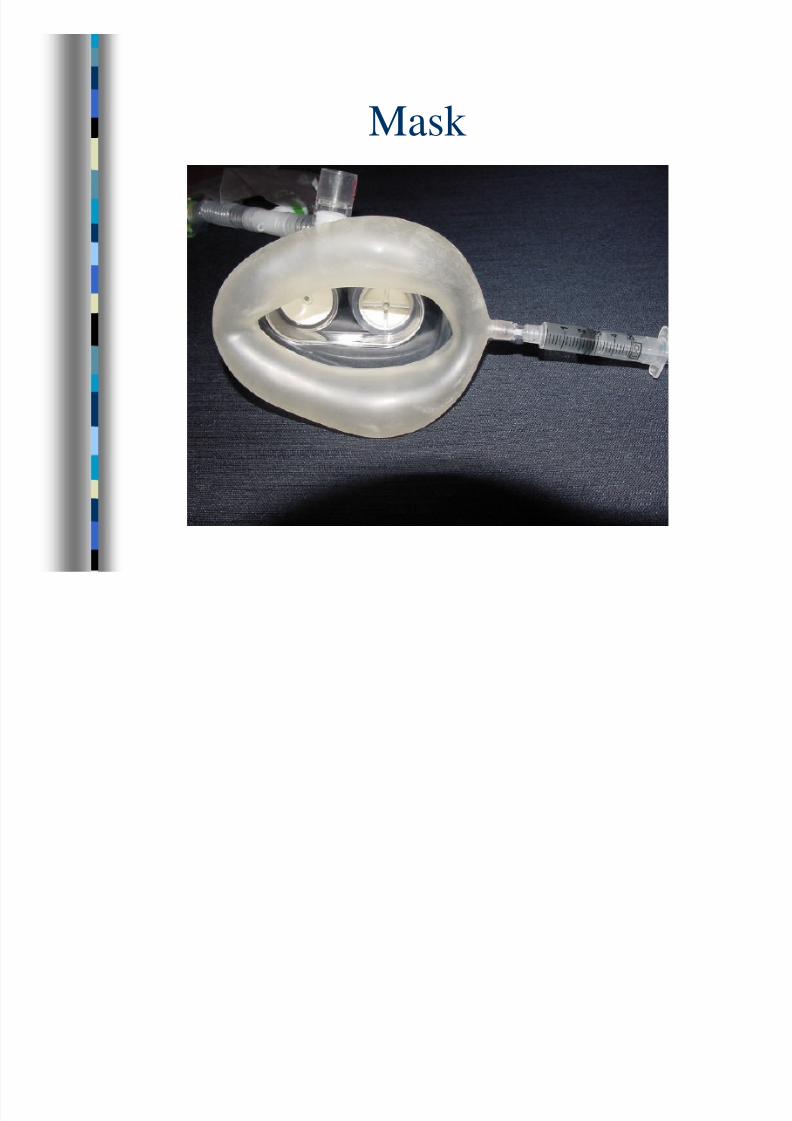
– Mask
– FiO2 dial – Reservoir bag
– Air intake valve
– PEEP valve
– Head strap
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 42/80
Mask

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 43/80
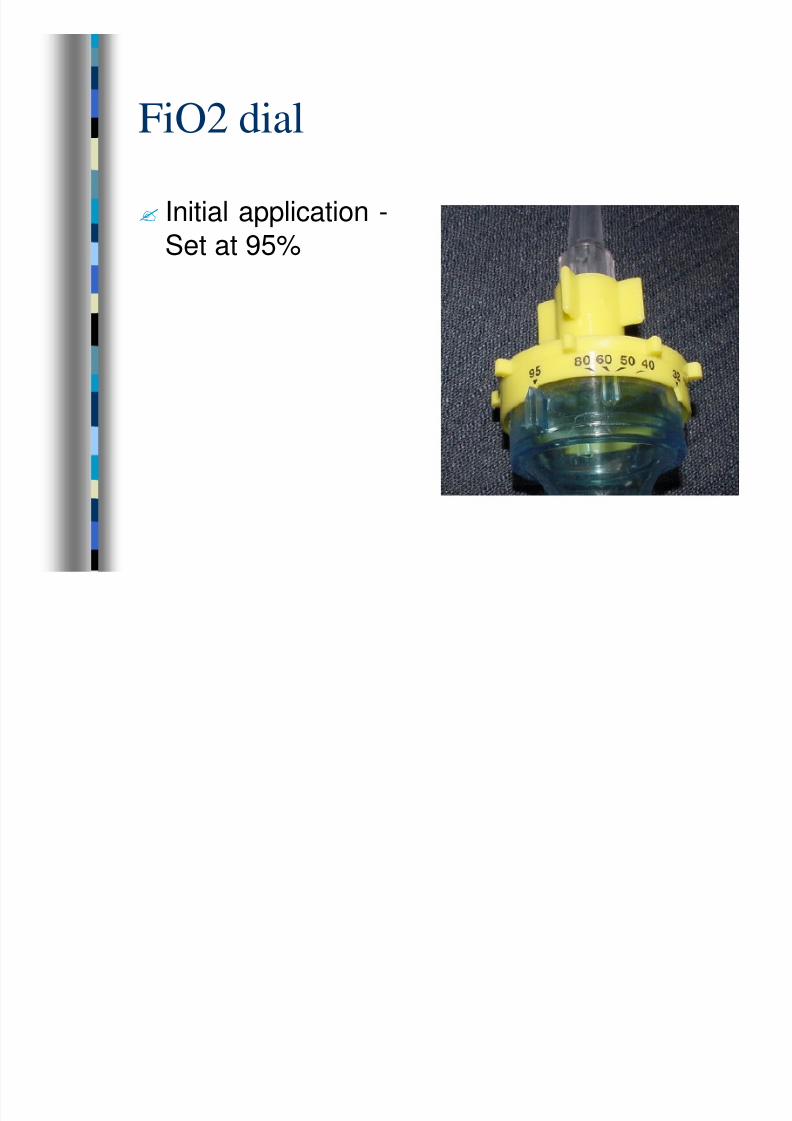
FiO2 Dial
? Range 32-95%
? LPM
– Minimum 15 LPM
– Maximum: flush
(25 LPM)
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 44/80
FiO2 dial
? Initial application -
Set at 95%
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 45/80
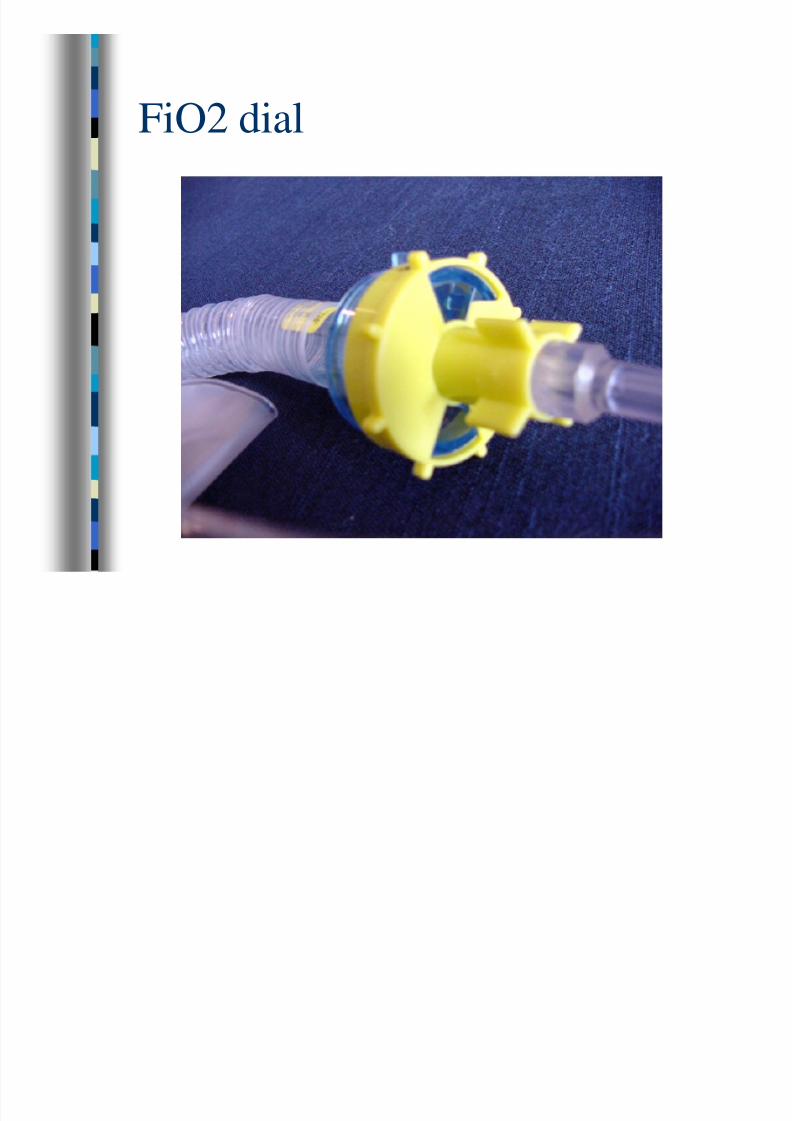
FiO2 dial

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 46/80
Reservoir Bag
? Fill before applying
C-PAP to patient
? Self-fills at FiO295%
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 47/80
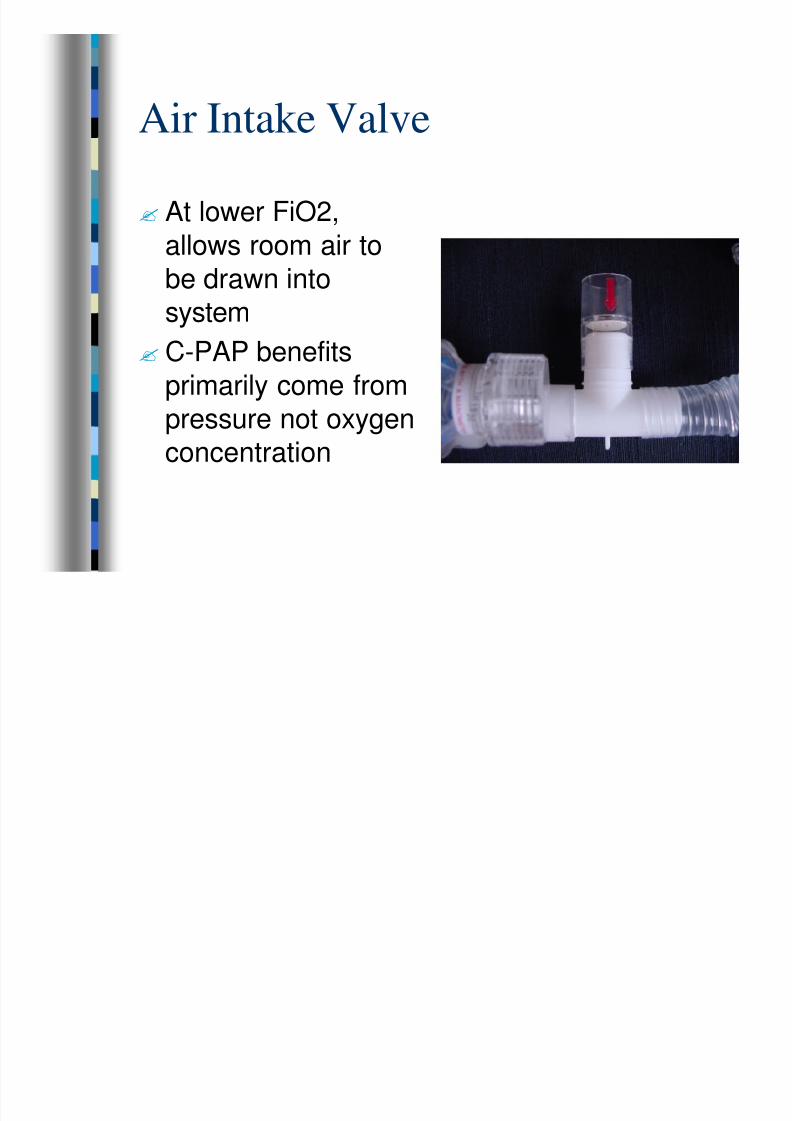
Air Intake Valve
? At lower FiO2,
allows room air to
be drawn intosystem
? C-PAP benefits
primarily come from
pressure not oxygenconcentration
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 48/80
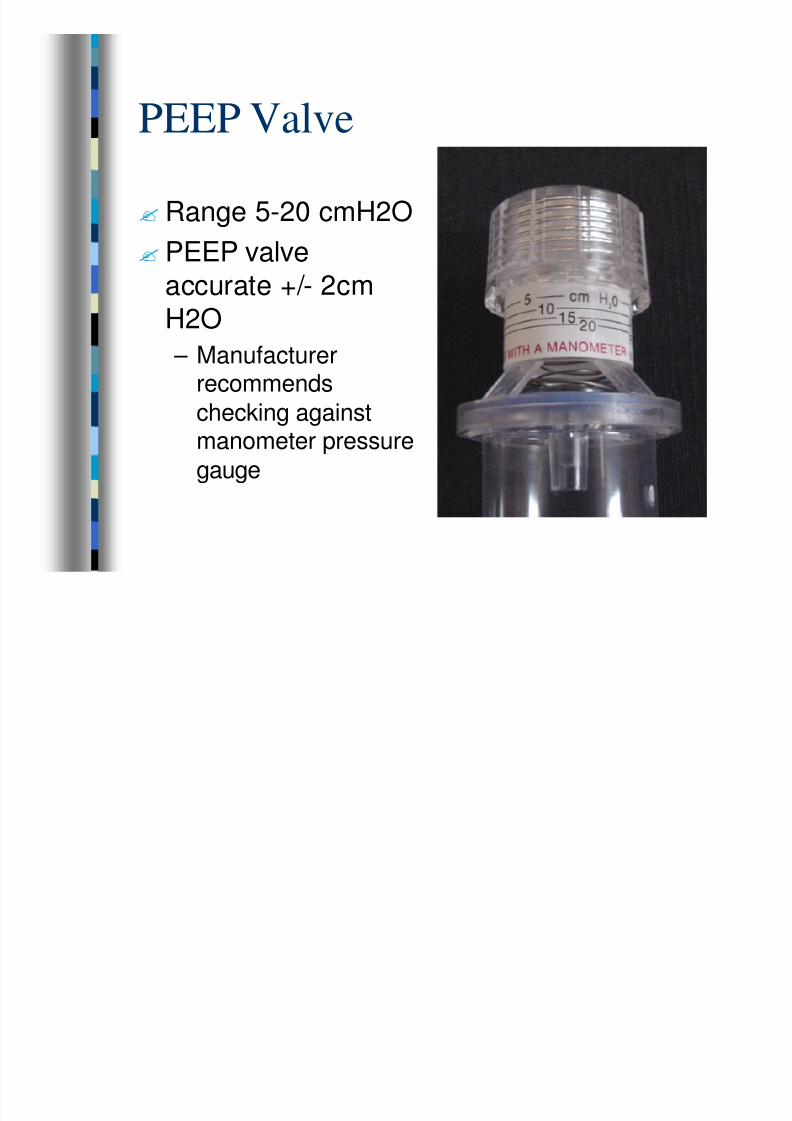
PEEP Valve
? Range 5-20 cmH2O
? PEEP valve
accurate +/- 2cmH2O
– Manufacturerrecommends
checking againstmanometer pressure
gauge
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 49/80
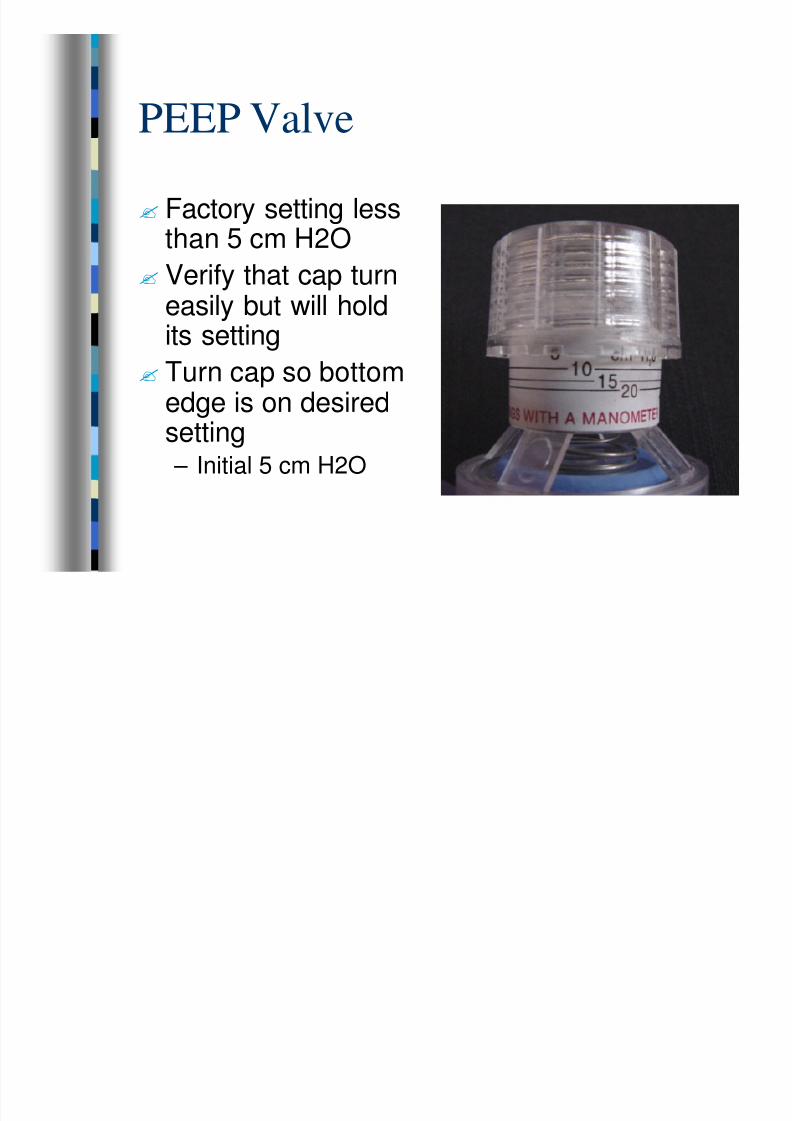
PEEP Valve
? Factory setting lessthan 5 cm H2O
? Verify that cap turneasily but will holdits setting
? Turn cap so bottomedge is on desiredsetting – Initial 5 cm H2O

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 50/80
Head Strap
? Apply to patient’s
head after patient
accepts C-PAP

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 51/80
Patient Criteria to Use Oxy-PEEP
?Old enough to get adequate mask seal
– Recommended for patients 18 years or
older
?Alert with intact airway and ventilatory
drive
?Systolic BP at least 90 mmHg
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 52/80
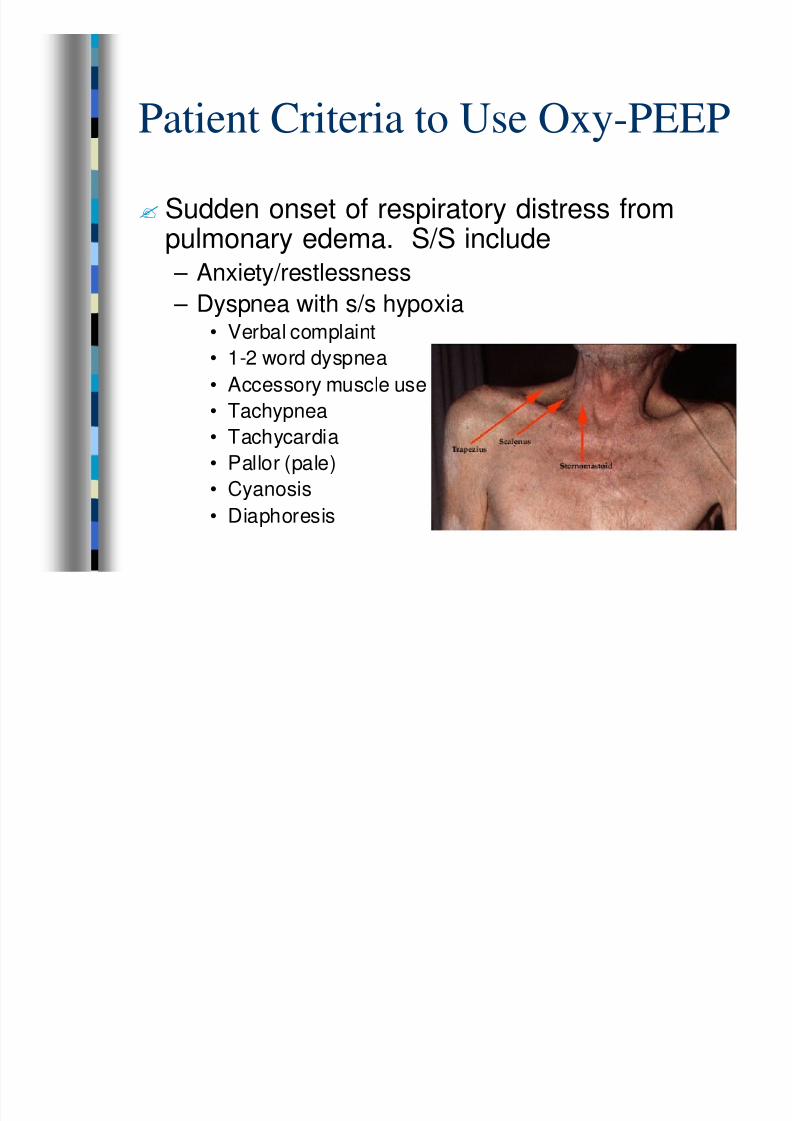
Patient Criteria to Use Oxy-PEEP
? Sudden onset of respiratory distress frompulmonary edema. S/S include
– Anxiety/restlessness – Dyspnea with s/s hypoxia• Verbal complaint
• 1-2 word dyspnea
• Accessory muscle use
• Tachypnea
• Tachycardia
• Pallor (pale)
• Cyanosis
• Diaphoresis
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 53/80
Patient Criteria to Use Oxy-PEEP
?Frothy sputum (may be pink)
?Room air SpO2 < 94%
?Bilateral crackles / rales
?Peripheral edema
?Chest pain
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 54/80
Absolute Contraindications
? Inadequate airway
or respiratory drive

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 55/80
Absolute Contraindications
? Need for immediate
airway control
(intubation)
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 56/80
Absolute Contraindications
? Hemodynamic
instability
– Systolic BP <90 mmHg
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 57/80
Absolute Contraindications
? Aspiration risk
– Vomiting or severe
nausea

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 58/80
Relative Contraindications
? Upper airway or
facial abnormalities
or trauma thatinterfere with mask
seal

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 59/80
Relative Contraindications
? Uncooperative
patient

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 60/80
Relative Contraindications
?Respiratory distress caused by
– Aspiration
– Asthma (requires MD orders)
– COPD (requires MD orders)
– Pneumonia
– Pneumothorax
– Anaphylaxis – Pulmonary embolism
– Respiratory Burns

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 61/80
Procedure
?Assess patient for S/S pulmonary
edema
?Room Air SpO2 < 94%
?Systolic BP at least 90 mmHg

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 62/80
Procedure
? Implement CHF branch of Difficulty Breathingprotocol
?May be done simultaneously with application
of C-PAP – High flow O2 via NRB until C-PAP applied
– Monitor / IV
– Nitroglycerin 0.4 mg SL X3• Once C-PAP applied, unfasten mask to administer Ntg
– Lasix 40 mg IV – Albuterol HHN if wheezing
– Morphine 2-4 mg slow IV every 5 minutes up to10 mg total

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 63/80
Procedure
?Prepare C-PAP Equipment
– Adjust FiO2 to 95%
– Set PEEP at 5 cm H2O
– Set O2 flow at flush (minimum 15 LPM)
– Fill reservoir bag
– Prepare intubation equipment – Ensure adequate supply of oxygen (main
and portable)

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 64/80
Procedure
?Prepare Patient
– Position Stretcher at 45 degrees or higher
– Inform patient of procedure
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 65/80
Procedure
?Mask Application – Trial to introduce device
• Explain patient will feel positive oxygenpressure
– Hold mask gently on patient’s faceensuring good seal
– Once patient accepts mask, secure maskwith straps
– Deflate mask as needed to get good seal

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 66/80
Procedure
?On-Going Care / Monitoring – Reassess at least every 5 minutes
• Patient’s impression of difficulty breathing• Vital signs
• Lung sounds
• SpO2
– Observe for complications• Hypotension
• Barotrauma
• Worsening dyspnea

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 67/80
Procedure
? If patient continues to have severe
difficulty breathing after 5 minutes,
consider increasing PEEP to 10 cmH2O
– Systolic BP must be at least 90 mmHg
– CAREFULLY watch for complications ofincreased PEEP

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 68/80
Procedure
?On-Going Care / Monitoring
– Oxygen conservation
• If patient is improved with C-PAP – SpO2 > 94%
– Work of breathing improved
• Consider decreasing LPM to 15
• Make sure reservoir bag remains full• Carefully monitor patient status including SpO2

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 69/80
Discontinuing C-PAP
?C-PAP usually is not discontinued in the
field
?High PEEP level may require weaning
?Rebound hypoxia can be worse thaninitial hypoxia

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 70/80
Discontinuing C-PAP
?Patient requires BVM or intubation
– Remove C-PAP, ventilate and intubate
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 71/80
Discontinuing C-PAP
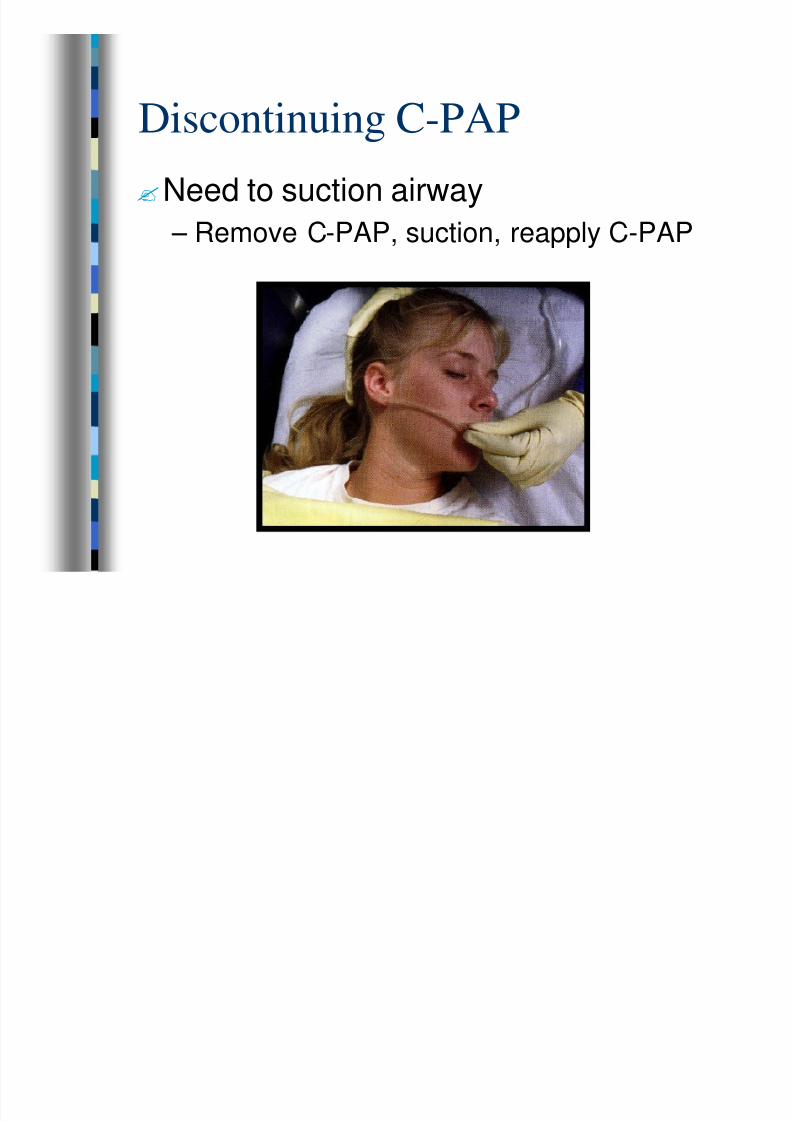
?Need to suction airway
– Remove C-PAP, suction, reapply C-PAP

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 72/80
Discontinuing C-PAP
?BP drops below 90 mmHG
– Contact Medical Control
– Is High PEEP worsening patient’s
condition? OR
– Is the underlying pathology causing the
deterioration?
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 73/80
Discontinuing C-PAP
?Consider decreasing PEEP with ordersfrom Medical Control – Patient hemodynamically stable at 5 cm
H2O PEEP
– PEEP increased to 10 cm H2O and BPdropped
– Is High PEEP worsening patient’s condition
or is the underlying pathology causinghypotension?
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 74/80
Protocol Use
? Included in A/O/V and Difficulty
Breathing Protocols
?Standing order for CT/I/P to use forCHF induced pulmonary edema

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 75/80
Protocol Use
? Initial PEEP 5 cm H2O
?FiO2 95%
?Standing order to increase to 10 cm
H2O if patient in severe distress and notimproving after 5 minutes
– Most patients will respond to 5 cm H2OPEEP

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 76/80
Documentation – It IS Your Job
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 77/80
Documentation
? Document Use under “Other”
– Not positive pressure ventilation

7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 78/80
Documentation - Narrative
? Patient’s S/S including SpO2
? S/S indicating CHF vs. COPD to rule inC-PAP use
– C-PAP use for COPD requires orders fromMedical Control
? C-PAP settings – FiO2
– PEEP
– O2 LPM
– Any changes in settings and why
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 79/80
Documentation
? Treatments to correct underlying pathology
? Patient’s response to C-PAP and other
treatments
7/31/2019 CPAP-1
http://slidepdf.com/reader/full/cpap-1 80/80
Questions????
- D. Brennaman: Initial Author