blood physiology - lecture 3 immune system (is) 3_blood_2016.pdf · diapedesis - back into the...
TRANSCRIPT
Imagine just sneezing…
Blood Physiology - Lecture 3
Immune System (IS)
Dr. AM Zagrean

The Immune System
Immune organs
Central/ primary- bone marrow and
thymus- generation of lymphocytes
Peripheral/ secondary- trapping Ag+
specific (adaptive) immune responses
are initiated+ maintainance of
lymphocytes- lymph nodes, spleen,
GALT, MALT, BALT
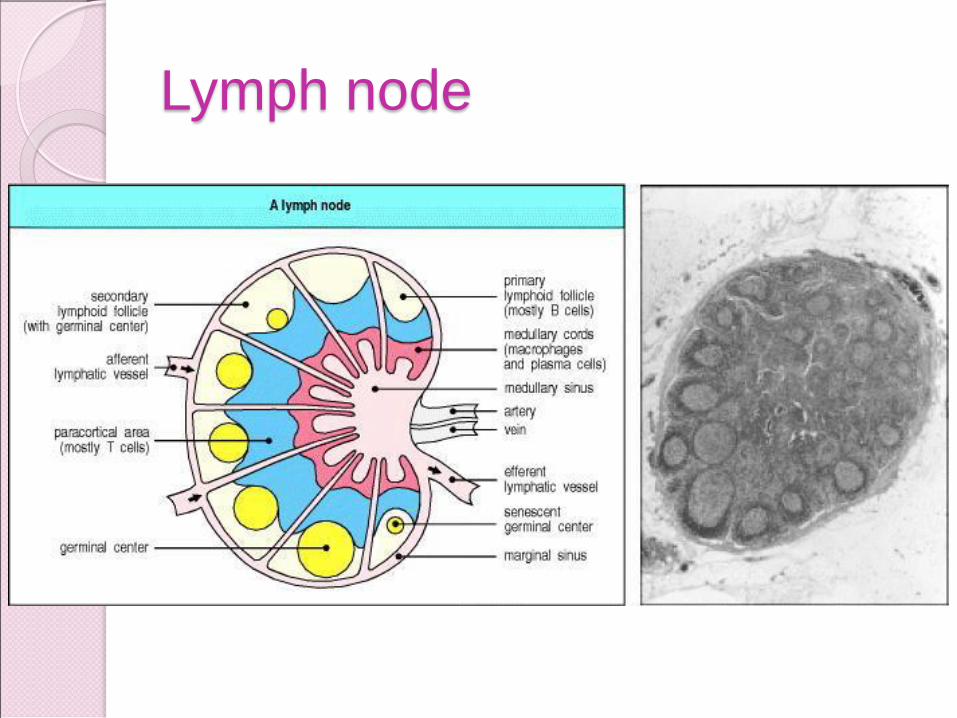
Lymph node
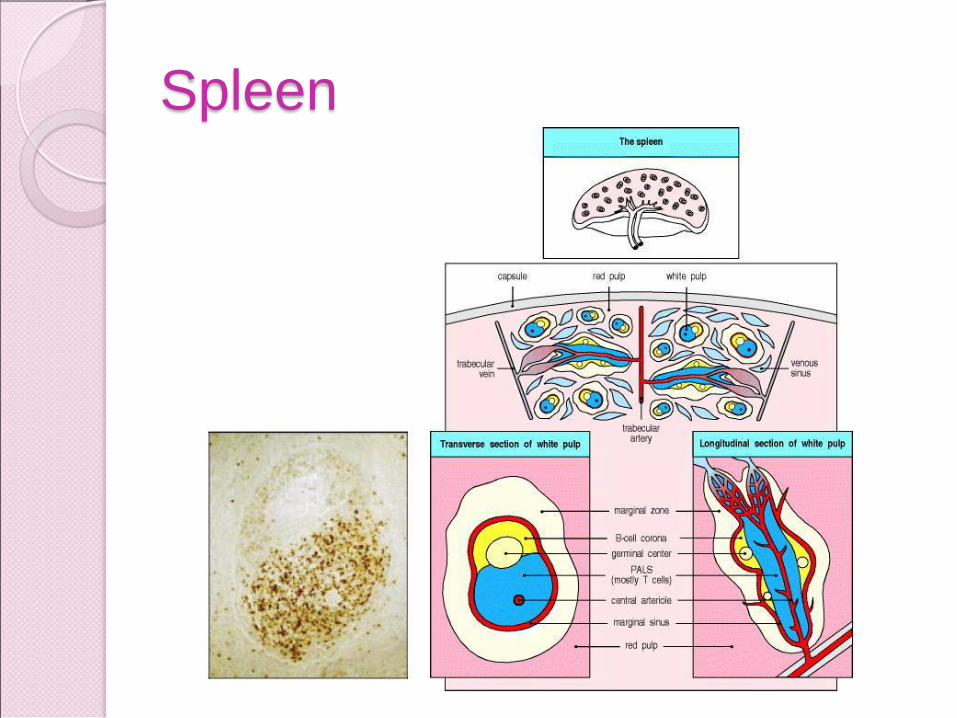
Spleen
GALT, BALT, MALT
GALT= gut-associated lymphoid
tissues- tonsils, adenoids, appendix,
Peyer’s patches (small int)
BALT= bronchial-associated lymphois
tissue
MALT= mucosal- associated lymphoid
tissue
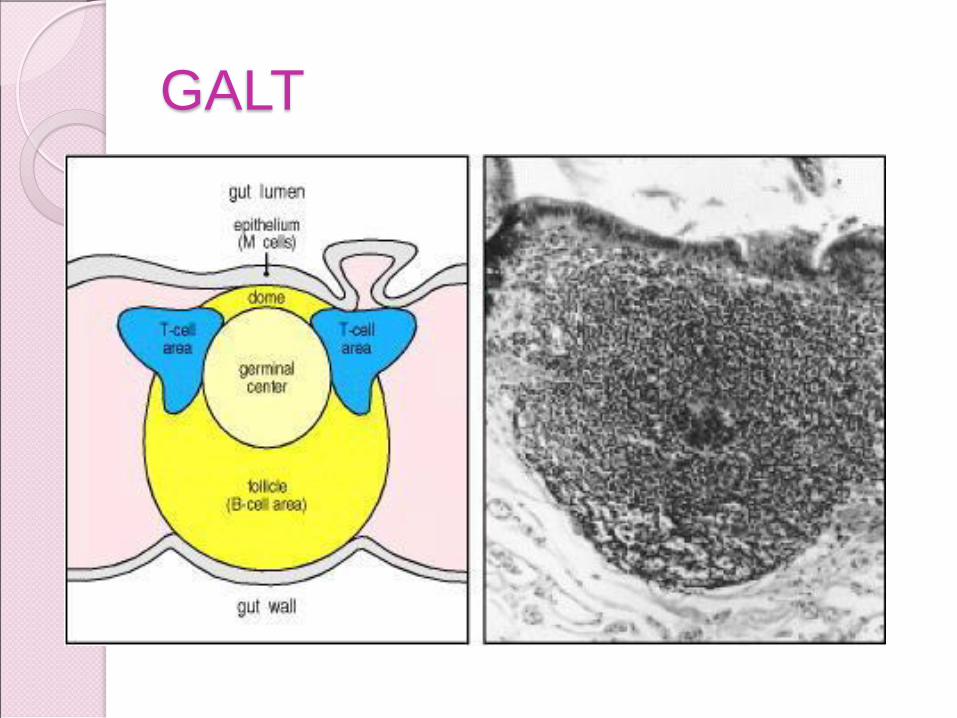
GALT

Lymph vessels
IMMUNITY
The body is continuously exposed to microorganisms (bacteria, viruses, fungi, parasites) at different levels: skin, mouth, respiratory passageways, eyes, intestinal tract, genital & urinary tracts
Immunity*: a condition of being able to resist a particular
disease especially through
preventing development of a pathogenic microorganism or
by counteracting the effects of its products
*Derives from the latin immunitas, meaning freedom from public service
(i.e., the military draft).
Overview of Immune System
In two words: specificity and memory
IS serves 3 major functions:
1. Protections from pathogens: microorganisms,
chemicals, foreign bodies – non-self, antigens
2. Removal of dead or damaged tissue and cells
3. Recognition and removal of abnormal cells
Every organism needs host defense.
Every organism needs to distinguish self from non-self.
Defense mechanisms can be toxic to self if not properly controlled.
Tolerance
Central- destruction of LT that recognize self
molecules in the thymus
Peripheral- LT that leave the thymus are relatively
safe, but not completely hypothesis
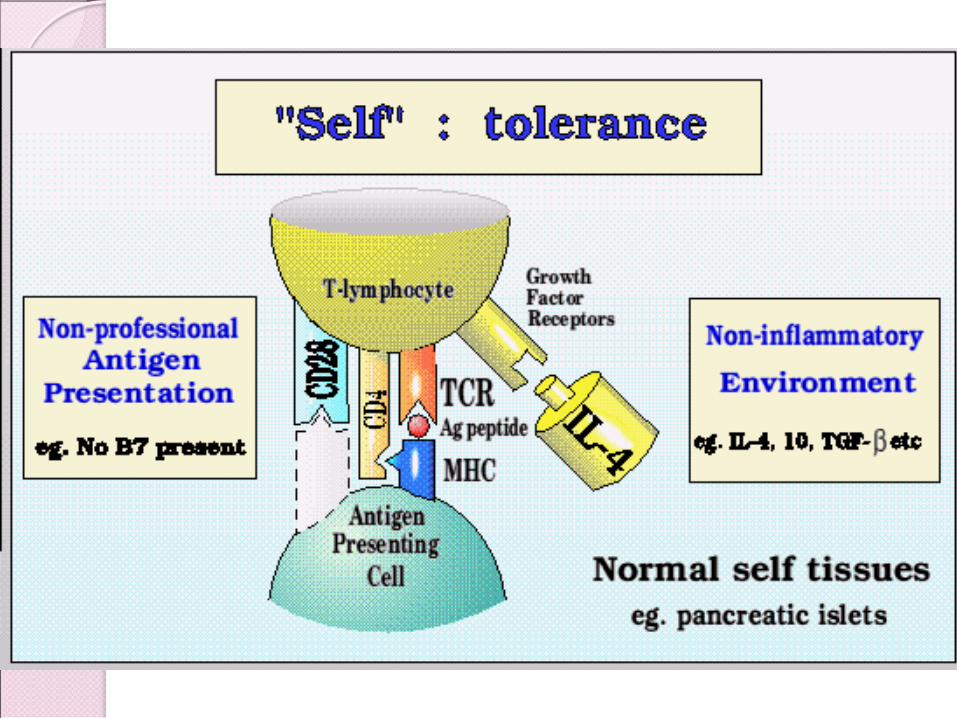
◦ Non-inflammatory environment
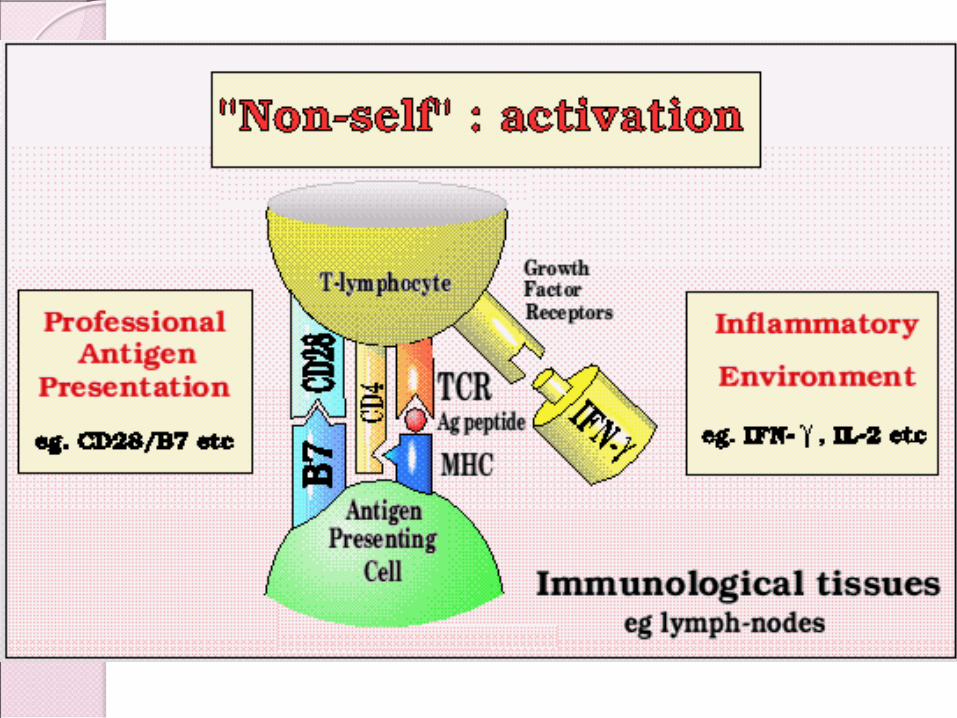
◦ Lack of costimulation- primary signal (binding to
TCR) needs a secondary signal (B7-CD28)
lack of second signal apoptosis of LT
◦ Some self molecules- hidden
◦ Death signals- Fas on LT and FasL on cells
interaction Fas-FasL death of LT
Steps in Immune System response
1. Detection & identification of non-self
2. Communication with other immune cells resulting in an
organized response
3. Recruitment of assistance and coordination of the
response among all participants
4. Destruction / suppression / removal / minimization of
spreading of the invader/non-self
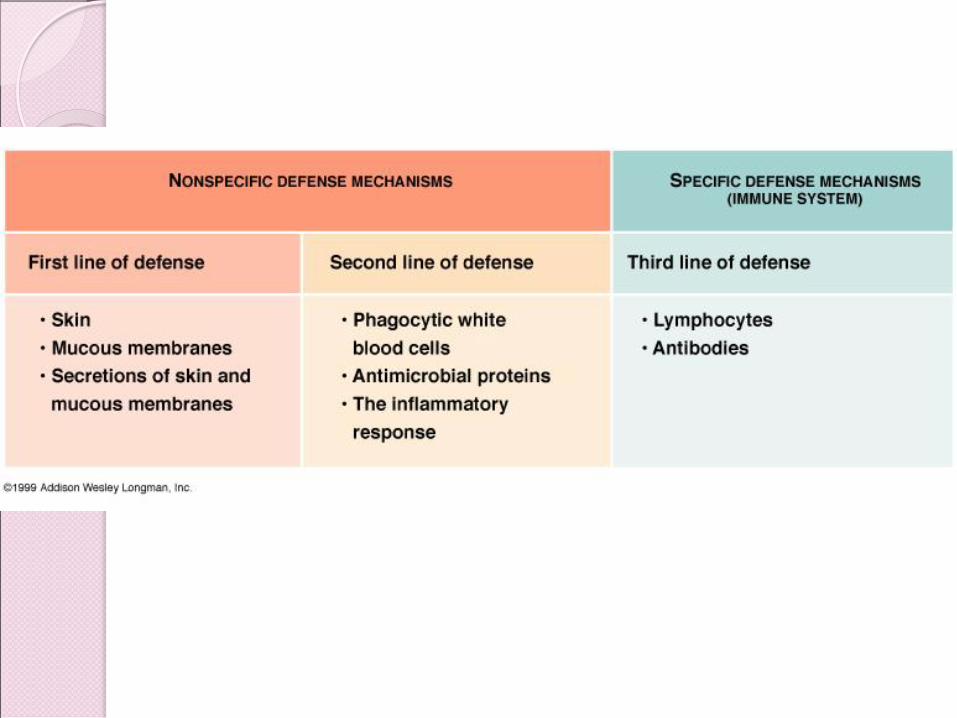
Body defense…
FIRST LINE INNATE:
Non- specific physical and chemical barriers - physical barriers: skin, mucous membranes, epithelial linings & cilia
- chemical barriers: gastric secretion, tears, saliva, urine acids / pH extremes in stomach enzymes: lysozymes (tears,saliva,milk,mucus) high salt concentrations
SECOND LINE INNATE :
Non-specific immune responses:
- monocyte/macrophage system, neutrophils, NK, eosinophils and mast cells, interferons, and complement proteins…
- inflammatory response & fever
THIRD LINE ACQUIRED
Specific immune responses – T and B lymphocytes work like a team to destroy pathogens.
17
Surface Barriers (First Line of
Defense) Skin, mucous membranes, and their
secretions make up the first line of defense
Keratin in the skin: ◦ physical barrier to most microorganisms
◦ resistant to weak acids and bases, bacterial enzymes, and toxins
Skin acidity (pH of 3 to 5) inhibits bacterial growth
Sebum contains chemicals toxic to bacteria
18
Surface Barriers
◦ Stomach mucosae secrete concentrated HCl
and protein-digesting enzymes
◦ Saliva, tears, milk, mucus contain lysozyme
◦ Mucus traps microorganisms that enter the
digestive and respiratory system
◦ Mucus-coated hairs in the nose trap inhaled
particles
◦ Mucosa of the upper respiratory tract is
ciliated- cilia sweep dust- and bacteria-laden
mucus away from lower respiratory passages
19
Nonspecific immune responses
(Second Line of Defense) The body uses nonspecific cellular and
chemical devices to protect itself
1. phagocytes
2. natural killer (NK) cells
3. inflammatory response enlists macrophages, mast cells, WBCs, and chemicals
4. antimicrobial proteins in blood and tissue fluid- interferons and complement proteins
5. fever
Harmful substances are identified by surface carbohydrates unique to infectious organisms

I. Phagocytes: Produced throughout life by the bone marrow.
Scavengers, recycling – remove dead cells, microorganisms.
(phago="eating", cyte="cell").
Granulocytes: Neutrophils polymorph
Eosinophils
Basophils tissue mast cells
Monocytes tissue macrophages
II. Immunocytes- involved in specific immune response (3rd
line)
Lymphocytes: T and B (plasma cells)
Leukocytes (WBCs): “seek out and destroy” systems
- mobile units of the body's protective immune system
- transported in the blood to different parts of the body,
mostly to areas of infection and inflammation
- Leukocytes (functional classification):

Leukocytes (morphologic classification)
Granulocytes:
Neutrophils polymorph.
Eosinophils
Basophils
Primary/azurophilic granules are common to all granulocytes, appear in the promyelocyte stage and are obscured by the appearance of specific granules in the myelocyte stage. Contain myeloperoxidase and defensins.
Secondary secretory granules appear in the myelocyte phase; contain apolactoferrin and collagenase.
All cytoplasmic granules, primary or secondary, contain biologically active substances that are involved in inflammatory and allergic reactions
Agranulocytes
Monocytes
Lymphocytes: T and B, plasma cells
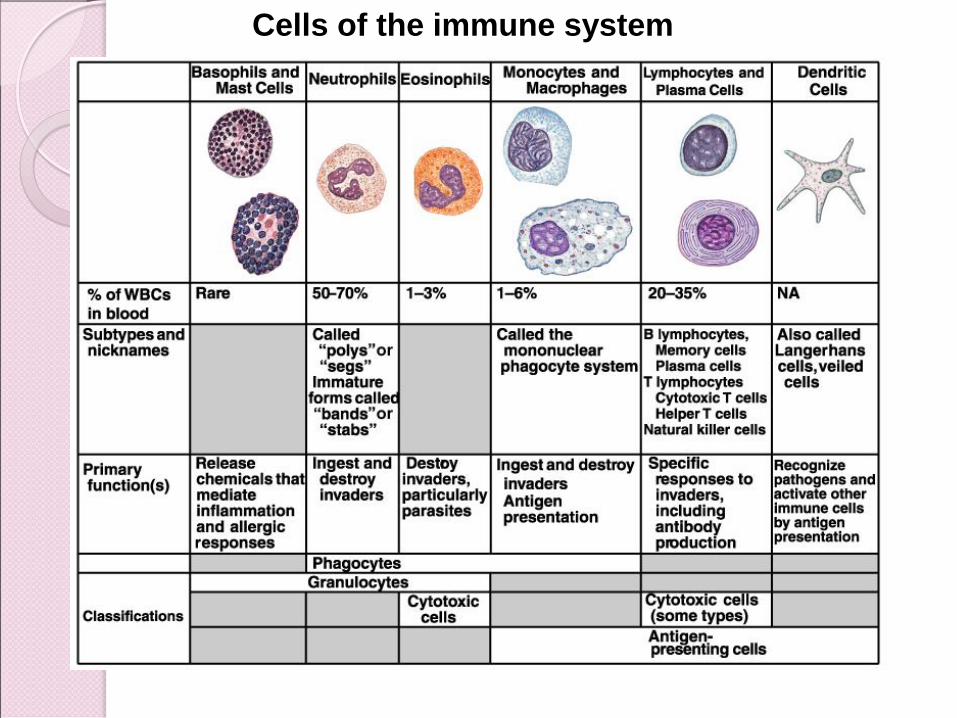
Cells of the immune system

Pluripotential
hematopoietic
stem cell
(PHSC)
PHSC
Colony
forming
unit
(CFU
GEMM)
Lymphoid
stem cell
(LSC)
CFU-B(last) CFU-E Erithrocytes
CFU-GM Granulocytes
Monocytes/Macrophages
CFU-M Megakaryocytes platelets
T Lymphocytes
B Lymphocytes
NK
Myeloid
stem
cell
(MSC)
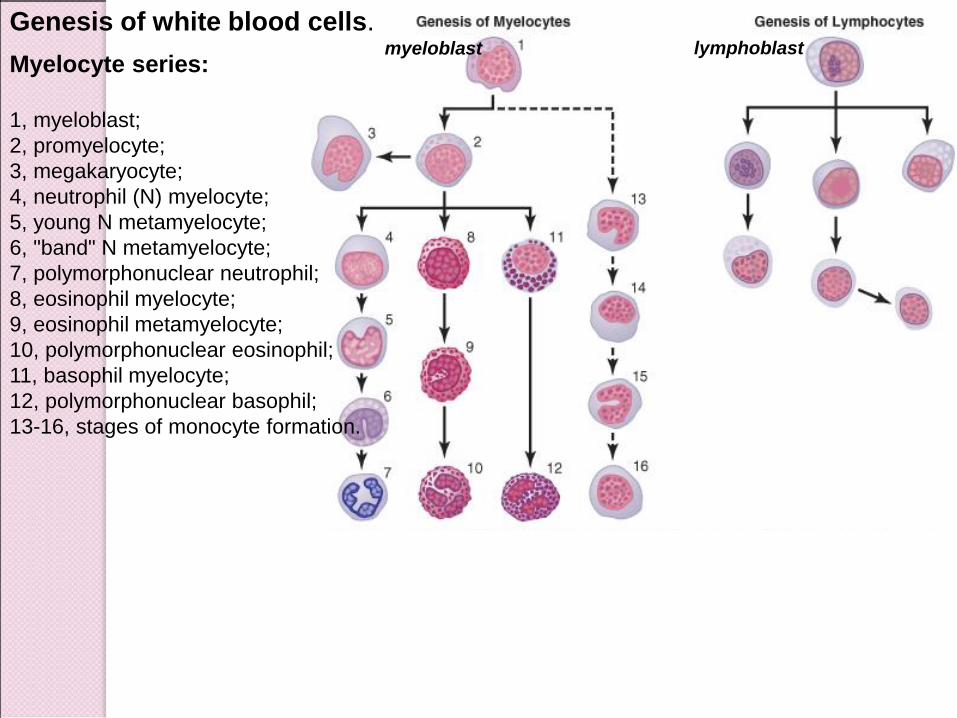
Myelocyte series:
1, myeloblast;
2, promyelocyte;
3, megakaryocyte;
4, neutrophil (N) myelocyte;
5, young N metamyelocyte;
6, "band" N metamyelocyte;
7, polymorphonuclear neutrophil;
8, eosinophil myelocyte;
9, eosinophil metamyelocyte;
10, polymorphonuclear eosinophil;
11, basophil myelocyte;
12, polymorphonuclear basophil;
13-16, stages of monocyte formation.
Genesis of white blood cells. myeloblast lymphoblast
Leukocytes:
-No: ~ 4000 - 11000 WBCs / ml of blood
-Normally, WBCs in bone marrow are ~ 3x more then in circulating
blood (~ a 6-day supply of WBCs)
Leukocyte formula
Polymorphonuclear neutrophils 62% (50-70%)
approach, ingest & kill bacteria;
see Arneth count for average age of N (nuclei lobes #)
Blood N: 50% circulating at any instant, 50% remain marginated
/sidelined on vessel walls or sequestered in closed capillaries.
Polymorphonuclear eosinophils 2.3% (1-4%)
attack parasites that are too large to be engulfed
increased in allergic disease
Polymorphonuclear basophils 0.4% (0-1%)
release histamine & other inflammatory mediators
important in immediate-type hypersensitivity reaction
Monocytes 5.3% (2-8%)
Lymphocytes 30% (20-40%)
Leukocytes life span
Granulocytes:
BM/lymphoid tissue 4-8 hrs circulating 4-5 days in tissues (less time during infections, die after digesting bacteria)
Neutrophils ‘patrol tissues’ as they squeeze out of the capillaries (diapedesis); large numbers are released during infections.
Monocytes:
BM/lymphoid tissue 10-20 hrs circulating enlarge to form tissue macrophages long-lived: months (unless destroyed while performing phagocytic functions)
Lymphocytes
lymph/lymphoid tissue (re)circulating for a few hrs. diapedesis - back into the tissues re-enter the lymph return to the blood… and so on for weeks/months
Calculations based on the blood volume and the level and half-life of blood cells in
the circulation indicate that each day an adult produces ~100 billion leukocytes. This
rate can increase by a factor of 10 or more when the demand increases.

Eosinophils (E)
2 % of all the blood leukocytes
weak phagocytes, exhibit chemotaxis, not significant in protecting against
the usual types of infection.
produced in large numbers in people with parasitic infections
eosinophils attach parasites by way of special surface molecules and
release substances that kill many of the parasites:
(1) hydrolytic enzymes from their granules, which are modified lysosomes;
(2) highly reactive forms of oxygen lethal to parasites;
(3) highly larvacidal polypeptide called major basic protein.
E collect in tissues where allergic reactions occur, migrating there because
of an eosinophil chemotactic factor released by mast cells and basophils
E detoxify some of the inflammation-inducing substances released by the
mast cells and basophils
phagocytize and destroy allergen-antibody complexes, thus preventing
excess spread of the local inflammatory process.


Basophils (B) / tissue mast cells
- release heparin (prevent blood coagulation), histamine
(vasodilator, bronchoconstrictor), smaller quantities of bradykinin
and serotonin (both are vasodilator substances) inflammation
- role in some types of allergic reactions: present membrane
receptors for immunoglobulin E (IgE, reagins or sensitizing
antibodies) binding of specific antigen for the specific IgE
attached to mast cells / basophils causes these cells to rupture
and release exceedingly large quantities of histamine, bradykinin,
serotonin, heparin, slow-reacting substance of anaphylaxis, and a
number of lysosomal enzymes local vascular and tissue
reactions that cause allergic manifestations.
Chapter 21, Immune System 30
1. Phagocytes
Macrophages are the chief phagocytic cells
Free macrophages wander throughout a region in search of cellular debris
Kupffer cells (liver) and microglia (brain) are fixed macrophages
Neutrophils become phagocytic when encountering infectious material
Eosinophils are weakly phagocytic against parasitic worms
Mast cells bind and ingest a wide range of bacteria
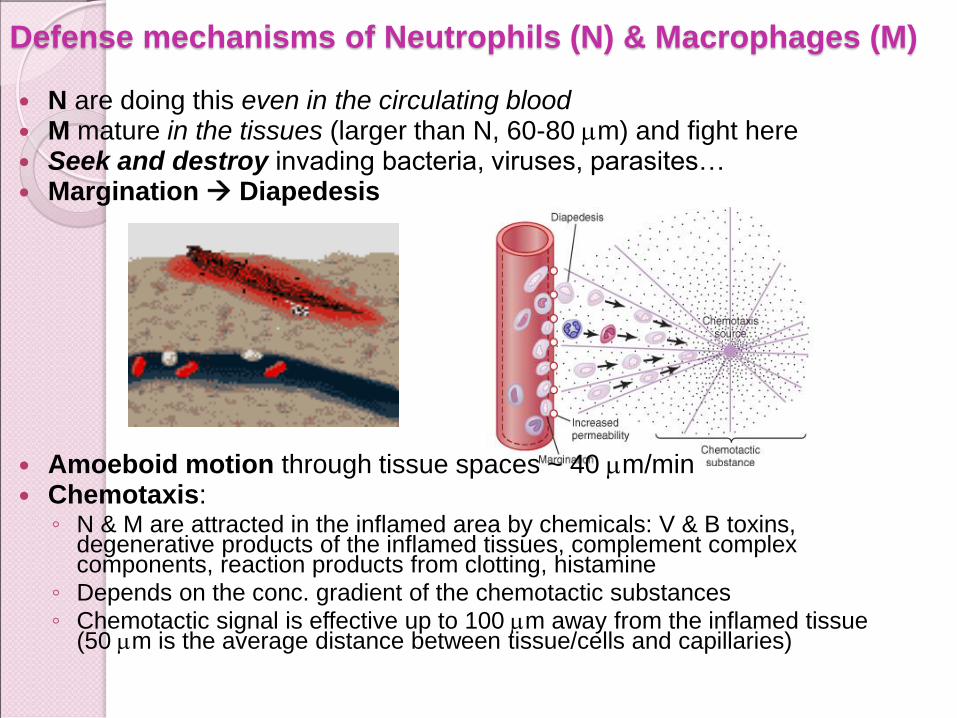
Defense mechanisms of Neutrophils (N) & Macrophages (M)
N are doing this even in the circulating blood M mature in the tissues (larger than N, 60-80 mm) and fight here Seek and destroy invading bacteria, viruses, parasites… Margination Diapedesis
Amoeboid motion through tissue spaces ~ 40 mm/min Chemotaxis:
◦ N & M are attracted in the inflamed area by chemicals: V & B toxins, degenerative products of the inflamed tissues, complement complex components, reaction products from clotting, histamine
◦ Depends on the conc. gradient of the chemotactic substances ◦ Chemotactic signal is effective up to 100 mm away from the inflamed tissue
(50 mm is the average distance between tissue/cells and capillaries)
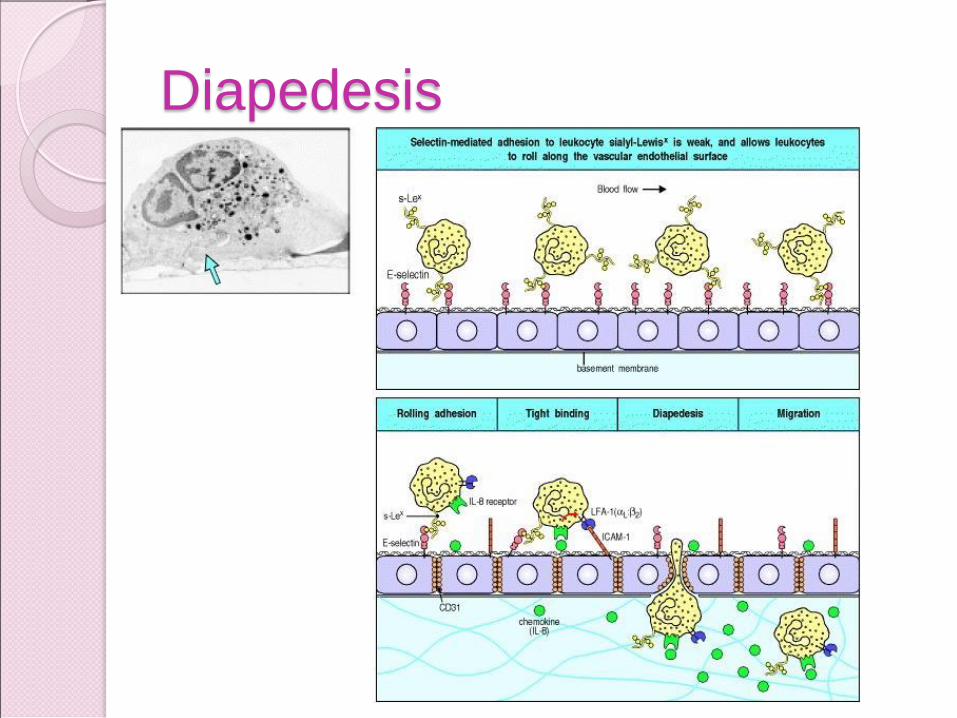
Diapedesis
Diapedesis First step- reversible binding of leukocytes
to vascular endoth- interaction SELECTIN-
sialyl-Lewisx (rolling but not anchoring)
Second step- strong interaction- induction
of ICAM-1 on the endoth interact with
integrin receptors (LFA1 and Mac-1)- due to
chemokines (IL8)
Third step- penetration
◦ Endoth junction
◦ Penetration of basement mb-
metalloproteinase
Forth step- migration through Ec matrix

Neutrophilia is caused by:
-transient - mobilization of
marginated/sequestered N
(secondary to adrenaline, exercise)
- release of stored N from BM (100 mature N
stored in the BM for every circulating N)
when stimulated by cortisol or
granulocyte-inducing factor derived from
dead leukocytes.
-stimulation of BM production
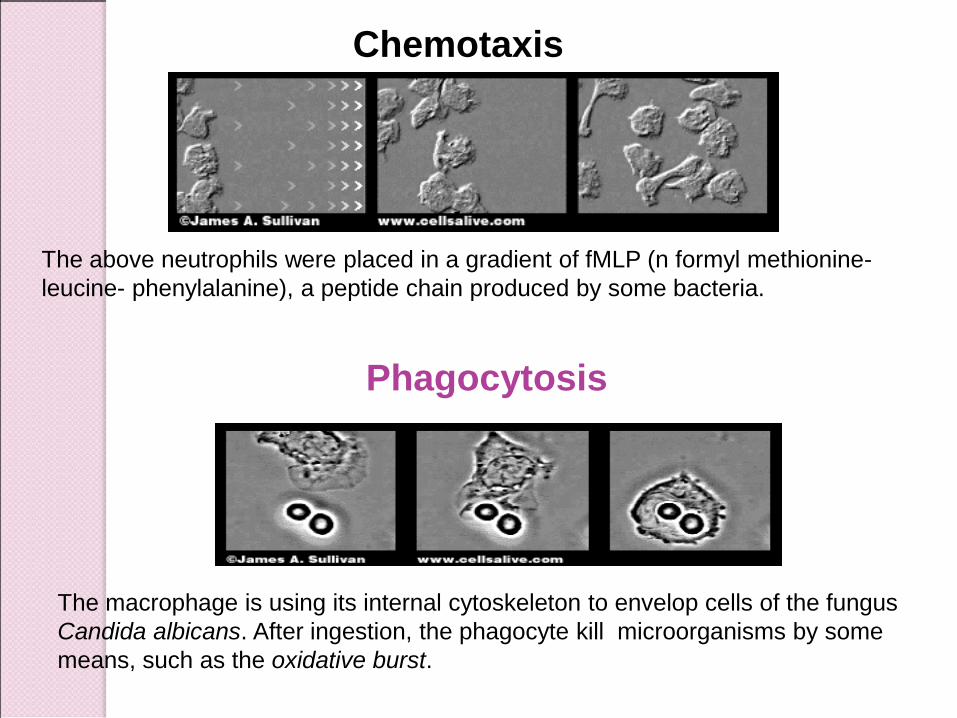
Chemotaxis
The above neutrophils were placed in a gradient of fMLP (n formyl methionine-
leucine- phenylalanine), a peptide chain produced by some bacteria.
Phagocytosis
The macrophage is using its internal cytoskeleton to envelop cells of the fungus
Candida albicans. After ingestion, the phagocyte kill microorganisms by some
means, such as the oxidative burst.
Phagocytosis Selectivity criteria:
- normal/self cells have smooth surface and protective protein coats that repel phagocytes
- through C3b molecules receptors, phagocytes (bearing ABs rec.) bind to C3b-AB complexes that coat the foreign structures (AG) = opsonization
N phagocytize 3-20 B before become inactivated/die (N attaches to B, projects pseudopodia around it fuse of pseudopodia enclosed chamber containing the phagocytized particle phagocytic vesicle inside the cytosol
M are more powerful phagocytes: engulf B and larger structures, ~ 100 /macrophage digest them and is possible to survive and function months or years after.
Phagocytic vesicles (phagosomes) fusion with lysosomes/ peroxisome/ cytoplasmic granules [contain proteolytic enzymes, lipases, bactericidal agents, oxidizing agents (O2
-, H2O2, OH-), myelo-peroxidase (form the bactericidal hypochlorite)] digestive vesicle
After ingesting a foreign invader, M “wear” pieces of it called epitops on their cell membrane receptors AG presenting cells (APC).

Opsonisation

Phagocytosis
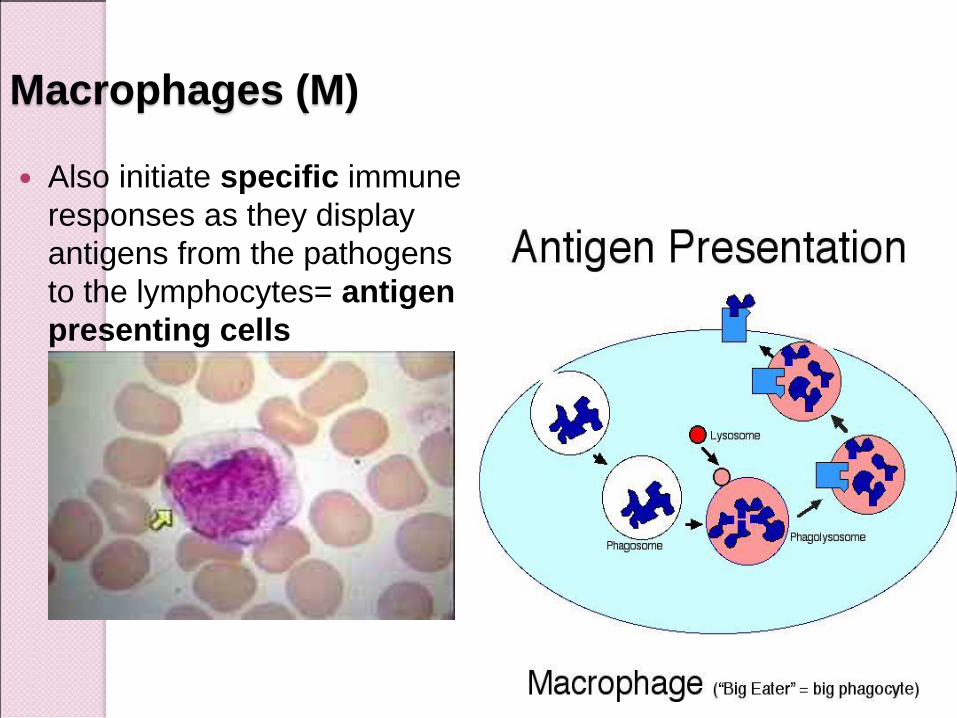
Macrophages (M)
Also initiate specific immune
responses as they display
antigens from the pathogens
to the lymphocytes= antigen
presenting cells
Monocyte-macrophage (M-M) system.
Reticuloendothelial System
Reticuloendothelial system: M-M system
Some endothelial cells from BM, spleen, lymph nodes
Monocytes (immature cells in the blood enter the tissues, begin to swell macrophages, that become attached to the tissues and remain attached for months or even years when appropriately stimulated, they detach and become mobile macrophages that respond to chemotaxis/stimuli related to the inflammatory process a widespread M-M system in the body
When infection begins in the skin and subcutaneous tissue local inflammation ensues local tissue macrophages (histiocytes) divide and form more macrophages.
Microorganisms at tissue level if not locally destroyed, enter the lymph trapped by macrophages in the lymph nodes
Alveolar M in the lungs: integral components of the alveolar walls “giant cells” capsule around not digestible particles (tuberculosis bacilli, silica dust, carbon particles).
Kupffer cells lining the liver sinusoids: filtration system for the portal blood
Microglia in the brain

Large numbers of macrophages line the lymph sinuses, and if any
particles enter the sinuses by way of the lymph, the macrophages
phagocytize them preventing general dissemination throughout the body.
Lymph nodes

Spleen capillaries are highly porous, allowing whole blood to pass out
of the capillaries into cords of red pulp. The blood then gradually
squeezes through the trabecular meshwork of these cords and
eventually returns to the circulation through the endothelial walls of the
venous sinuses. Both trabeculae of the red pulp and the venous
sinuses are lined with a large number of macrophages.
Spleen

44
2. Natural Killer (NK) Cells
~ large granular lymphocytes
Attack and kill certain tumor cells and virus-infected cells
Act more rapidly than other lymphocytes (hours from primary viral infection)
Secrete anti-viral cytokines (gamma-interferon)
Lyse virus-infected cells before the virus can replicate
Bind to cells using an antibody “bridge”, then kill it by secreting a chemical (perforin) that makes holes in the cell membrane of the target cell. With enough holes, the cell will die, because water rushing inside the cell will induce osmotic swelling
Cell lysis does not depend on binding to MHC-AG complexes

NK cells- early host response to
viral infection First wave- IFN, TNFalpha, IL12
Second wave- NK
Control viral replication
Don’t eliminate the virus
Third wave- LT
Virus elimination

Chapter 21, Immune System 46
3. Inflammation: Tissue
Response to Injury The inflammatory response is
triggered whenever body tissues are injured ◦ Prevents the spread of damaging agents
to nearby tissues
◦ Disposes of cell debris and pathogens
◦ Sets the stage for repair processes
The four cardinal signs of acute inflammation are redness, heat, swelling, and pain

Inflammation
Steps:
-vasodilation of local blood vessels excess local blood flow
-chemotaxis
-margination of N
- permeability of the capillaries … diapedesis…leakage of fluid into interstitial space, including fibrinogen
-clotting of the fluid in the interstitial spaces
-migration of large number of G & M, also fibroblasts
-swelling of the tissue cells
-release of histamine, BK, serotonin, PG, CK / lymphokines , TNF activate M-M system hours phagocytosis (in still-living cells)
‘Walling-off’ effect of inflammation tissue spaces and the lymphatics in the inflamed area are blocked by fibrinogen walling-off process delays the spread of bacteria or toxic products
Neutrophilia 25,000 /ul; increased prod of G & M in BM…
• Tissue response to injury, that helps prevent spread of pathogen and
promotes healing
Chapter 21, Immune System 48
Inflammation Response
Begins with a flood of inflammatory chemicals released into the extracellular fluid
Inflammatory mediators (chemicals) : ◦ Include kinins, prostaglandins (PGs),
complement, and cytokines
◦ Are released by injured tissue, phagocytes, lymphocytes, and mast cells
◦ Cause local small blood vessels to dilate, resulting in hyperemia
Chapter 21, Immune System 49
Inflammatory Response:
Vascular Permeability Chemicals liberated by the
inflammatory response increase the
permeability of local capillaries
Exudate (fluid containing proteins,
clotting factors, and antibodies):
◦ Seeps into tissue spaces causing local
edema (swelling), which contributes to the
sensation of pain

Chapter 21, Immune System 50
Inflammatory Response: Edema
The surge of protein-rich fluids into
tissue spaces (edema):
◦ Helps to dilute harmful substances
◦ Brings in large quantities of oxygen and
nutrients needed for repair
◦ Allows entry of clotting proteins, which
prevents the spread of bacteria= “walling
off” the AG

Chapter 21, Immune System 51
Flowchart of Events in
Inflammation
Figure 21.2
Macrophage and Neutrophil Responses During Inflammation
Tissue macrophage is a 1st line of defense against infection.
M arrive within minutes/already present in the tissue, enlarge rapidly and begin
their phagocytic actions.
Neutrophil invasion of the inflamed area is a 2nd line of defense.
Within the first hour or so after inflammation begins, large numbers of N begin
to invade the inflamed area from the blood: chemotaxis, N margination N
diapedesis, immediately begin their phagocytic actions.
Within a few hours after the onset of acute severe inflammation, the number of
neutrophils in the blood increases from 4000 - 5000 to 15,000 - 25,000 / ml
(neutrophilia), because of inflammation products that reach the bone marrow
(stored neutrophils…)
Second macrophage invasion into inflamed tissue is a 3rd line of defense.
Monocytes enter the inflamed tissue (slower process requiring several days to
become effective), then enlarge to become macrophages (~ 8 hours to enlarge
and to develop tremendous quantities of lysosomes. After days - weeks, these
M become the dominant phagocytic cells of the inflamed area.
Increased production of G & M by the BM Is a 4th line of defense resulting
from stimulation of the granulocytic and monocytic progenitor cells of the
marrow 3 - 4 days before newly formed granulocytes & monocytes mature…

Control of BM production of granulocytes and monocyte-macrophages in
response to multiple growth factors released from activated macrophages in an
inflamed tissue. G-CSF, granulocyte colony-stimulating factor; GM-CSF,
granulocyte-monocyte colony-stimulating factor; IL-1, interleukin-1; M-CSF,
monocyte colony-stimulating factor; TNF, tumor necrosis factor.

54
4. Antimicrobial Proteins
Enhance the innate defenses by:
◦ Attacking microorganisms directly
◦ Impare microorganisms’ ability to
reproduce
The most important antimicrobial
proteins are:
◦ Interferon
◦ Complement proteins
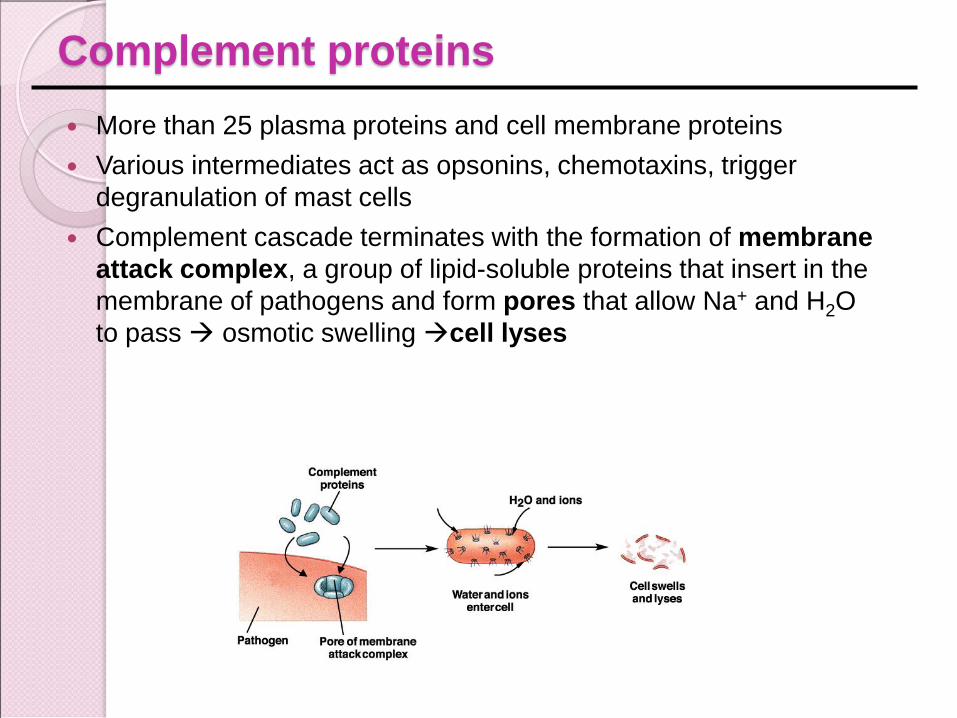
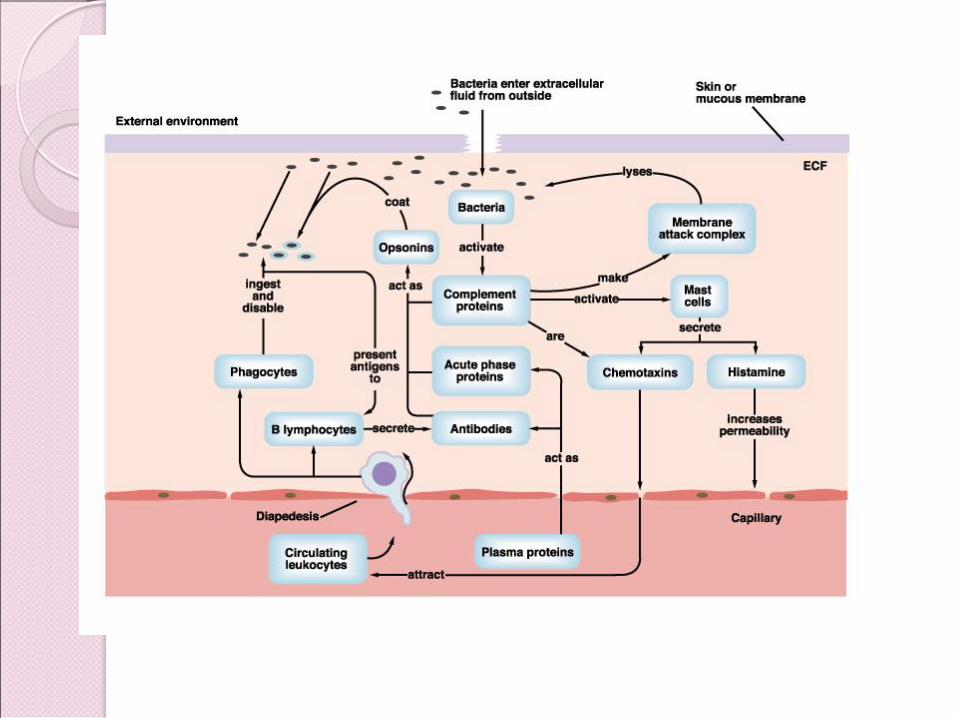
Complement proteins
More than 25 plasma proteins and cell membrane proteins
Various intermediates act as opsonins, chemotaxins, trigger
degranulation of mast cells
Complement cascade terminates with the formation of membrane
attack complex, a group of lipid-soluble proteins that insert in the
membrane of pathogens and form pores that allow Na+ and H2O
to pass osmotic swelling cell lyses
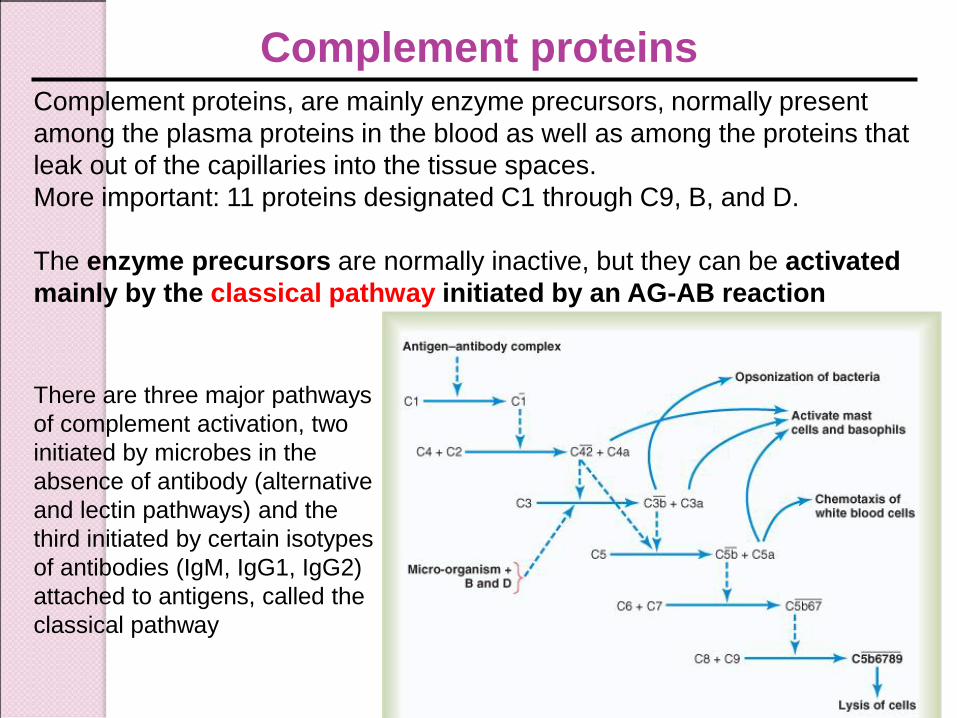
Complement proteins, are mainly enzyme precursors, normally present
among the plasma proteins in the blood as well as among the proteins that
leak out of the capillaries into the tissue spaces.
More important: 11 proteins designated C1 through C9, B, and D.
The enzyme precursors are normally inactive, but they can be activated
mainly by the classical pathway initiated by an AG-AB reaction
Complement proteins
There are three major pathways
of complement activation, two
initiated by microbes in the
absence of antibody (alternative
and lectin pathways) and the
third initiated by certain isotypes
of antibodies (IgM, IgG1, IgG2)
attached to antigens, called the
classical pathway
Effects of complement proteins/complement cascade end products
1.Opsonization and phagocytosis: C3b strongly activates phagocytosis by
both neutrophils and macrophages, causing these cells to engulf the bacteria to
which the antigen-antibody complexes are attached; enhances the number of
bacteria that can be destroyed by many hundredfold.
2.Lysis: MAC (membrane attack complex) lytic complex, a combination of
multiple complement factors designated as C5b6789, with a direct effect of
rupturing the cell membranes of bacteria or other invading organisms.
3.Agglutination: complement products change the surfaces of the invading
organisms (AGs), causing them to adhere to one another, thus promoting
phagocytosis.
4.Neutralization of viruses: complement enzymes and end products attack
the structures of some viruses.
5.Chemotaxis: fragment C5a initiates chemotaxis of neutrophils & macrophage
6. Activation of mast cells and basophils: fragments C3a, C4a, and C5a
activate mast cells and basophils release of histamine, heparin, and several
other substances into the local fluids role in inflammation and allergy.
7. Inflammatory effects: complement products contribute to local
inflammation, by increased blood flow, increased capillary leakage of proteins,
coagulation of interstitial fluid proteins walling-off effect
59
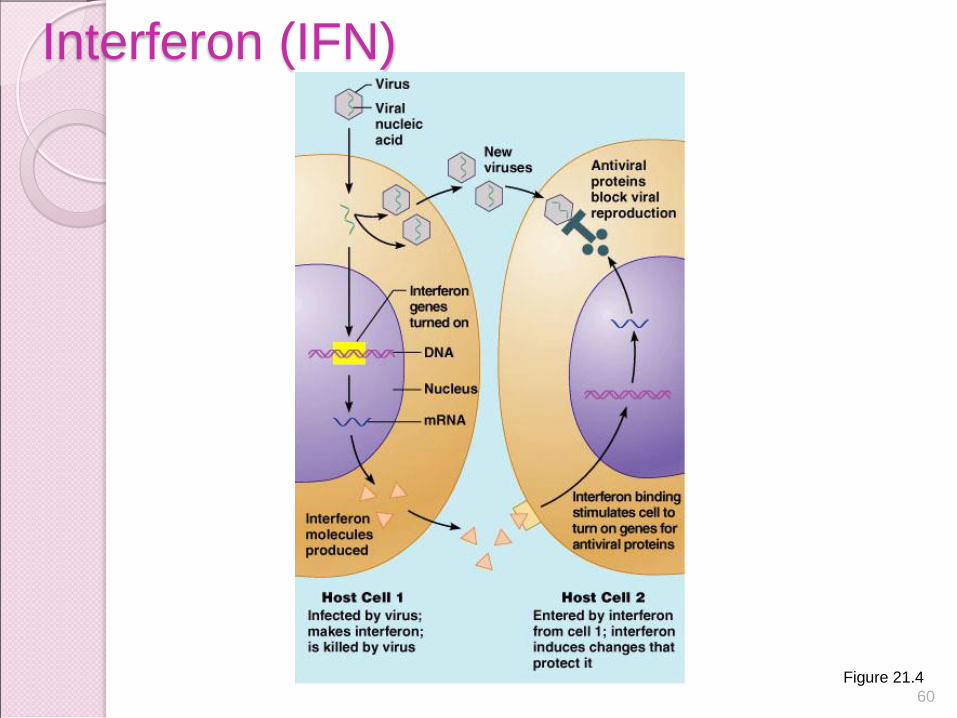
Genes that synthesize IFN are activated
when a host cell is invaded by a virus
Interferon molecules leave the infected
cell and interact with neighboring cells
Interferon stimulates the neighboring
cells to activate genes for PKR- protein
kinase R (an antiviral protein) PKR nonspecifically blocks viral replication in the
neighboring cell
Interferon (IFN)
60
Interferon (IFN)
Figure 21.4
61
Interferon Family Interferons are a family of related proteins
each with slightly different physiological effects
Lymphocytes secrete gamma () interferon, but most other WBCs secrete alpha () interferon
Fibroblasts secrete beta () interferon Interferons also activate macrophages and
mobilize NKs FDA-approved IFN is used as treatment for
different conditons
Chapter 21, Immune System 62
Abnormally high body temperature in
response to invading microorganisms
The body’s thermostat is reset
upwards in response to pyrogens,
chemicals secreted by leukocytes and
macrophages exposed to bacteria and
other foreign substances
5. Fever
POSITIVE
• indicate a reaction to infection
• stimulate phagocytosis
• slow the bacterial growth
– increases body temperature beyond the tolerance of some bacteria
NEGATIVE
• extreme heat enzyme
denaturation and
interruption of normal
biochemical reactions
> 39° C (103°F) is dangerous
> 41°C (105°F) could be fatal and
requires medical attention
Fever is induced by pyrogens:
endogenous (IL-1, IL-6, TNFa)
exogenous (bacterial lipopolysaccharide – LPS)
activ of arachidonic ac. pathway PGE2hypothalamic action
Positive/ negative effects of fever
Chapter 21, Immune System 64
The adaptive immune system is a
functional system that:
◦ Recognizes specific foreign substances
◦ Acts to immobilize, neutralize, or destroy
foreign substances
◦ Amplifies inflammatory response and
activates complement
Adaptive (Specific) Defenses (Third Line of Defense)
Chapter 21, Immune System 65
The adaptive immune system is
antigen-specific, systemic, and has
memory
It has two separate but overlapping
arms
◦ Humoral, or antibody-mediated (B Cell)
immunity
◦ Cellular, or cell-mediated (T Cell)
immunity
Adaptive Immune Defenses
Types of Specific (acquired) Immunity
I. Naturally Acquired Immunity: Obtained in the course of daily life.
A. Naturally Acquired Active Immunity:
◦ Antigens or pathogens enter body naturally.
◦ Body generates an immune response to antigens.
◦ Immunity may be lifelong (chickenpox or mumps) or temporary (influenza or intestinal infections).
B. Naturally Acquired Passive Immunity:
◦ Antibodies pass from mother to fetus via placenta or breast feeding
◦ No immune response to antigens.
◦ Immunity is usually short-lived (weeks to months).
◦ Protection until child’s immune system develops.
II. Artificially Acquired Immunity: Obtained by receiving a
vaccine or immune serum.
1. Artificially Acquired Active Immunity:
◦ Antigens are introduced in vaccines (immunization).
◦ Body generates an immune response to antigens.
◦ Immunity can be lifelong (oral polio vaccine) or temporary (tetanus toxoid).
2. Artificially Acquired Passive Immunity:
◦ Preformed antibodies (serum) are introduced into body by injection. Snake antivenom injection from horses or rabbits.
◦ Immunity is short lived (half life three weeks).
◦ Host immune system does not respond to antigens.
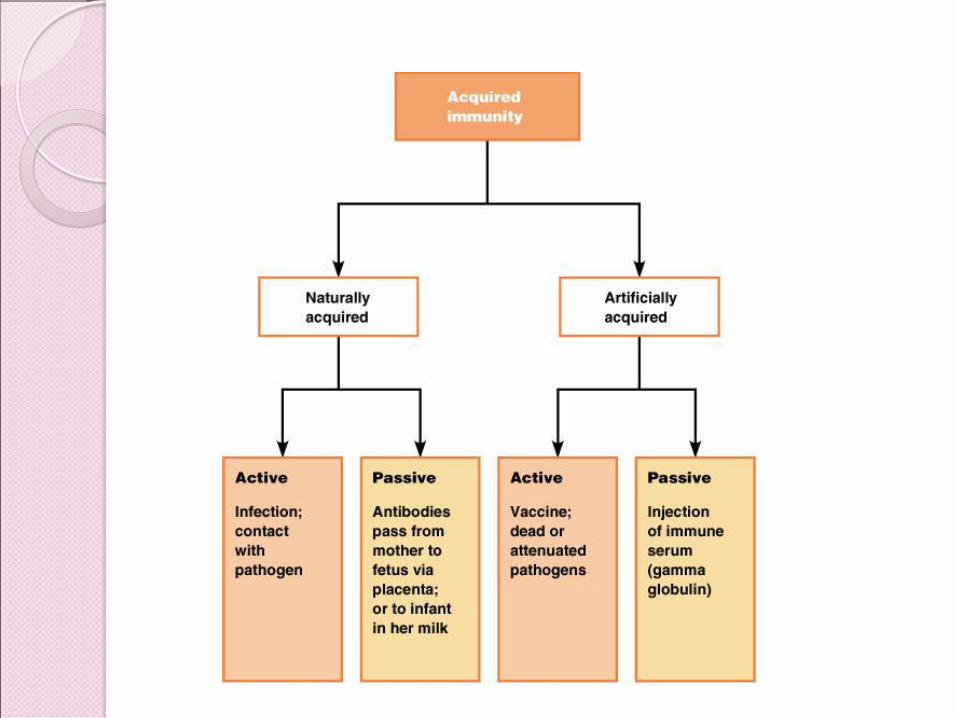

Basic Types of Acquired Immunity
Humoral immunity or B-cell immunity - develops
circulating antibodies capable of attacking the invading
agent
Cell-mediated immunity or T-cell immunity - formation of
large numbers of activated T lymphocytes that are
specifically crafted in the lymph nodes to destroy the
foreign agent
Both types of acquired immunity are initiated by
antigens

Chapter 21, Immune System 70
Two types of lymphocytes
◦ B lymphocytes – oversee humoral
immunity
◦ T lymphocytes – non-antibody-producing
cells that constitute the cell-mediated arm
of immunity
Antigen-presenting cells (APCs):
◦ Do not respond to specific antigens
◦ Play essential auxiliary roles in immunity
Cells of the Adaptive Immune System

INDUCTION OF AN IMMUNE RESPONSE
Foreign invaders - viruses, bacteria, allergens, toxins and parasites- constantly bombard our body.
Antigens (Antibody Generators…)
• Antigens are distinguished as non-self and elicit immune
responses
• For a substance to be antigenic, it usually must have a high
molecular weight, 8000 Da or greater.
• The process of antigenicity usually depends on recurrent
molecular groups, called epitopes, on the surface of the
large molecules.
• Most effective are large and complex:
• proteins
• polysaccharides
• also, glycoproteins and glycolipids

Lymphocytes (L) and Acquired Immunity (AI)
AGs diversity L specificity
L are distinguished by their specific membrane
receptors- antibodies
Each unique type of L, along with all the other
identical cells, forms a clone.
A clone of L is a group of L specific to one AG
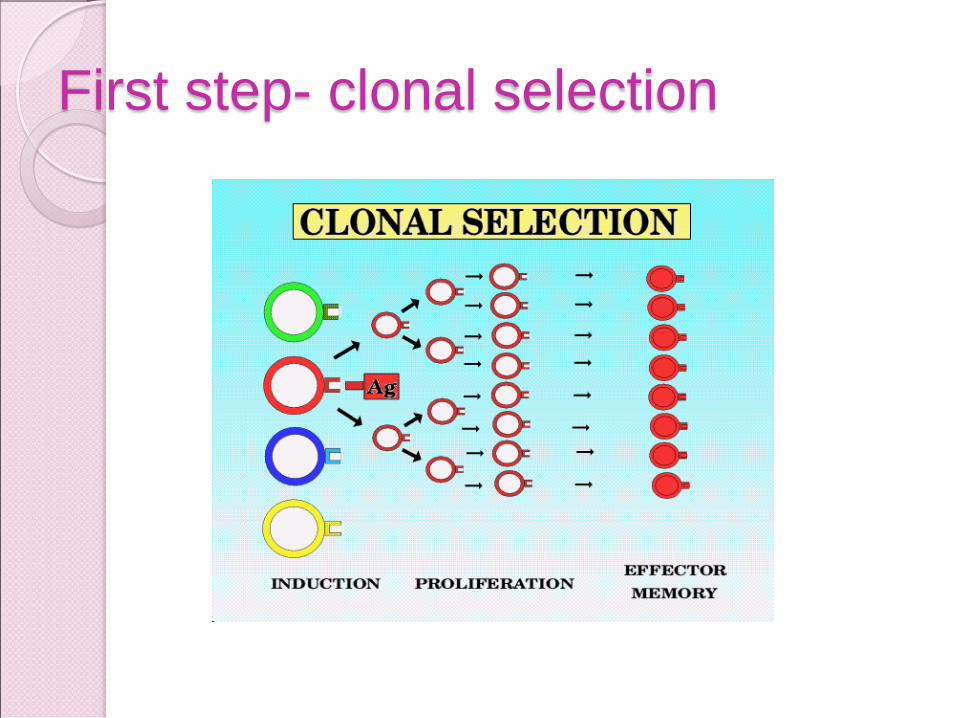
First step- clonal selection

Lymphocytes and Acquired Immunity
Initially there are only a few naïve L
Naïve L are activated after AG exposure = clonal expansion
The newly formed L in the clone differentiate into
- effector cells, short-lived cells that create the immune response
- memory cells, with longer-lives, continue to reproduce, and with a second or subsequent exposure to the same AG, activate, creating a more rapid and stronger secondary response to the AG.

Lymphocytes and Acquired Immunity
There are 3 main types of Lymphocytes:
LB (mature in bone marrow, concentrate in lymph nodes & spleen)
- secrete AB
LT (mature in thymus) – cellular immunity
B and T cells mature then circulate in the blood and lymph. Circulation
ensures they come into contact with pathogens and each other
Natural killer (NK) cells - attack & destroy infected cells

Origin of lymphocytes
Chapter 21, Immune System 77
Red bone marrow
1
2
3
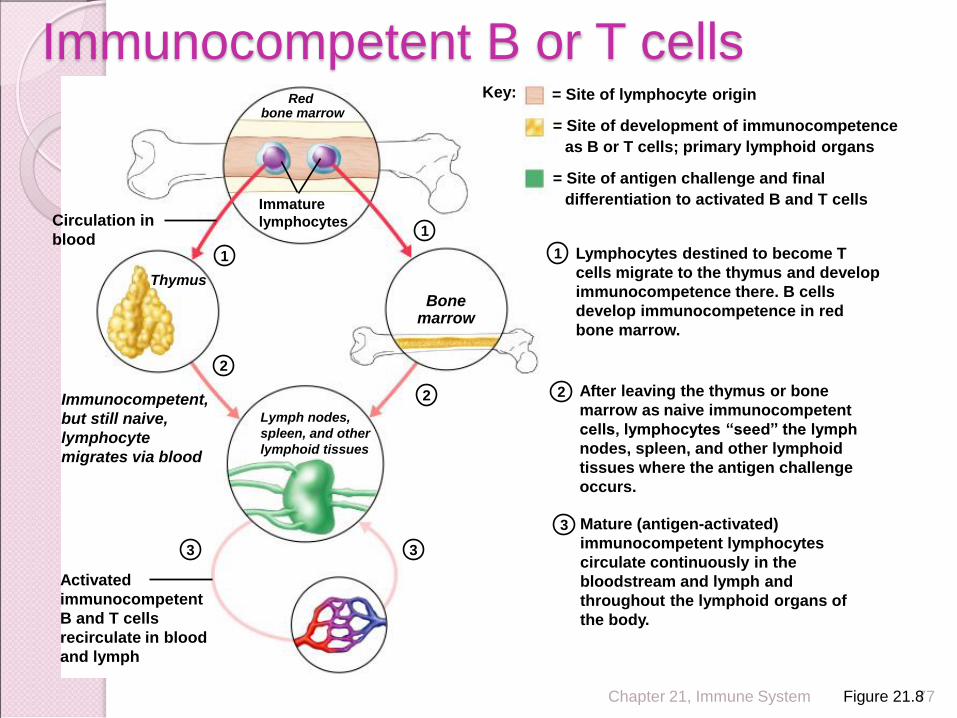
Immunocompetent,
but still naive,
lymphocyte
migrates via blood
Mature (antigen-activated)
immunocompetent lymphocytes
circulate continuously in the
bloodstream and lymph and
throughout the lymphoid organs of
the body.
Key: = Site of lymphocyte origin
= Site of development of immunocompetence
as B or T cells; primary lymphoid organs
= Site of antigen challenge and final
differentiation to activated B and T cells Immature
lymphocytes Circulation in
blood 1
1 Lymphocytes destined to become T
cells migrate to the thymus and develop
immunocompetence there. B cells
develop immunocompetence in red
bone marrow.
Thymus
Bone marrow
Lymph nodes,
spleen, and other
lymphoid tissues
2 2 After leaving the thymus or bone
marrow as naive immunocompetent
cells, lymphocytes “seed” the lymph
nodes, spleen, and other lymphoid
tissues where the antigen challenge
occurs.
3 3
Activated
immunocompetent
B and T cells
recirculate in blood
and lymph
Immunocompetent B or T cells
Figure 21.8
I. Humoral (Antibody-Mediated) Immunity
◦ Involves production of antibodies against foreign
antigens
◦ B cells that are stimulated will actively secrete
antibodies and are called plasma cells.
◦ Antibodies are found in extracellular fluids (blood
plasma, lymph, mucus, etc.) and the surface of B
cells.
◦ Defense against bacteria, bacterial toxins, and
viruses that circulate freely in body fluids, before
they enter cells.
◦ Also cause certain reactions against transplanted
tissue.
LB – B cells
Develop in BM
Secrete AB/Ig
Mature LB insert AB molecules in their membrane ABs become surface receptors mark the members of each clone ◦ There are ~10 million different B-lymphocytes, each of which make a
different antibody. The huge variety is caused by genes coding for ABs changing slightly during development.
Activation of a LB clone in response to AG exposure some cells differentiate in plasma cells =effector LB cell
- do not have AB proteins bound in their mb
- synthesize & secrete ~ 2,000 molec. of AB/sec.
memory cells of the clone remain, to respond: - rapidly and amplified to a next AG exposure (divide...)
- the enhanced secondary response is used in immunizations.
there are a small group of clones of each type of LB
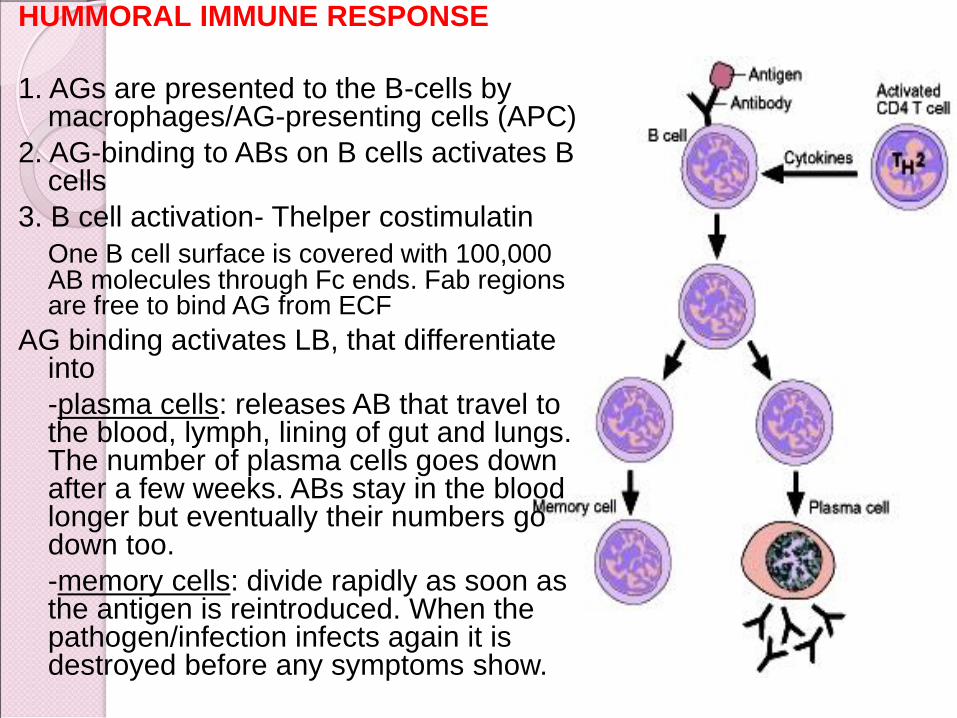
HUMMORAL IMMUNE RESPONSE
1. AGs are presented to the B-cells by macrophages/AG-presenting cells (APC)
2. AG-binding to ABs on B cells activates B cells
3. B cell activation- Thelper costimulatin
One B cell surface is covered with 100,000 AB molecules through Fc ends. Fab regions are free to bind AG from ECF
AG binding activates LB, that differentiate into
-plasma cells: releases AB that travel to the blood, lymph, lining of gut and lungs. The number of plasma cells goes down after a few weeks. ABs stay in the blood longer but eventually their numbers go down too.
-memory cells: divide rapidly as soon as the antigen is reintroduced. When the pathogen/infection infects again it is destroyed before any symptoms show.

Chapter 21, Immune System 81
Stimulated B cell growth forms clones
bearing the same antigen-specific
receptors
A naive, immunocompetent B cell is
activated when antigens bind to its
surface receptors and cross-link
adjacent receptors
These activating events, plus T cell
interactions, trigger clonal selection
Clonal Selection

Chapter 21, Immune System 82
Clonal Selection
Figure 21.9

Chapter 21, Immune System 83
Secreted antibodies:
◦ Bind to free antigens
◦ Mark the antigens for destruction by
opsonisation
Clones that do not become plasma
cells become memory cells that can
mount an immediate response to
subsequent exposures of the same
antigen
Fate of the Clones

Chapter 21, Immune System 84
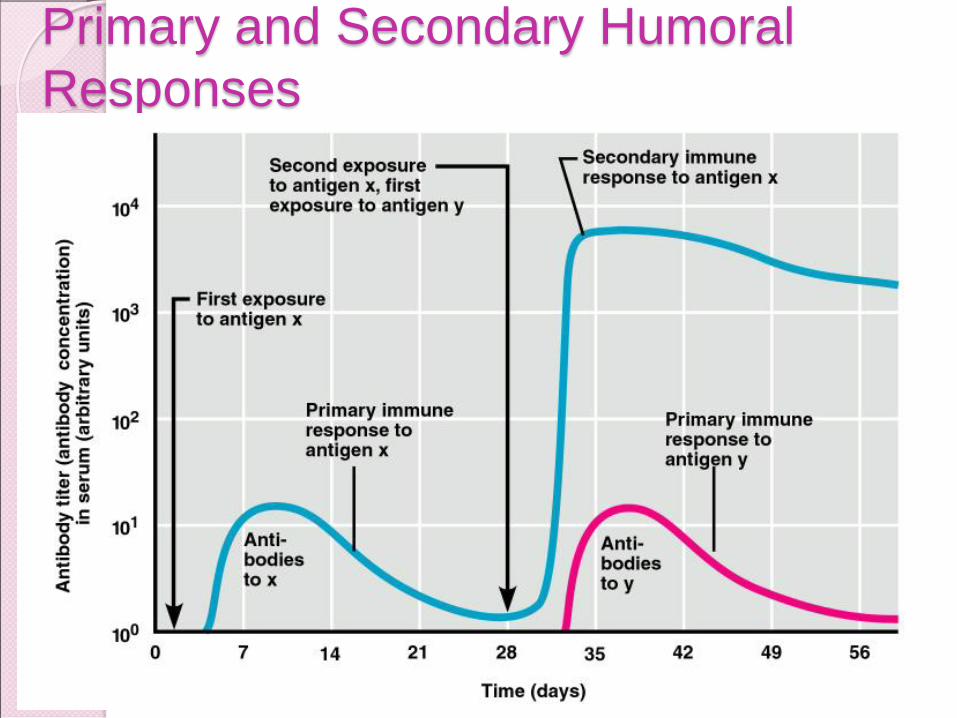
Primary immune response – cellular
differentiation and proliferation, which
occurs on the first exposure to a
specific antigen
◦ Lag period: 3 to 6 days after antigen
challenge
◦ Peak levels of plasma antibody are
achieved in 10 days
◦ Antibody levels then decline
Immunological Memory

Chapter 21, Immune System 85
Secondary immune response – re-
exposure to the same antigen
◦ Sensitized memory cells respond within
hours
◦ Antibody levels peak in 2 to 3 days at
much higher levels than in the primary
response
◦ Antibodies bind with greater affinity, and
their levels in the blood can remain high
for weeks to months
Immunological Memory
Chapter 21, Immune System 86
Primary and Secondary Humoral
Responses
Figure 21.10
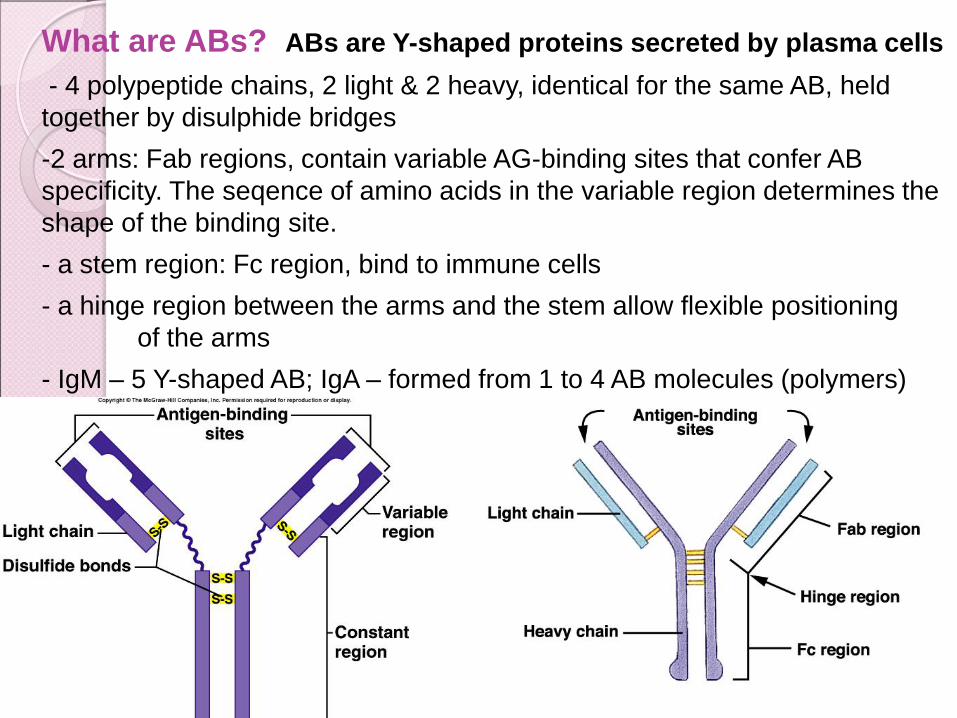
What are ABs? ABs are Y-shaped proteins secreted by plasma cells
- 4 polypeptide chains, 2 light & 2 heavy, identical for the same AB, held
together by disulphide bridges
-2 arms: Fab regions, contain variable AG-binding sites that confer AB
specificity. The seqence of amino acids in the variable region determines the
shape of the binding site.
- a stem region: Fc region, bind to immune cells
- a hinge region between the arms and the stem allow flexible positioning
of the arms
- IgM – 5 Y-shaped AB; IgA – formed from 1 to 4 AB molecules (polymers)

What are ABs?
- Immunoglobulins/globular glycoproteins secreted by plasma cells
- Separated by electrophoresis Ig G, A, E, M, D
- IgM: assoc with primary immune response
- IgG: up to 75% of adult ABs
produced in secondary immune response
maternal IgG cross placenta
- IgA: in external secretions of the body (saliva, tears, intestinal and bronchial mucus, breast milk)
disable pathogens before reaching internal environment
- IgE: assoc with allergic responses, combine with mast cells receptors and AGs to trigger mast cells degranulation

Different Immunoglobulins

How ABs work?
-opsonins (labels) to identify antigens for phagocytes
-antitoxins i.e. they block toxins for e.g. those causing
diphtheria and tetanus
-attach to bacterial flagella making them less active and easier
for phagocytes to engulf
-agglutination (clumping together) of bacteria making them
less likely to spread
-bind to and activate other immune cells; AB-bound AG is recognized by AB receptors
- AG-bound ABs activate complement, mast cells enhance inflammation
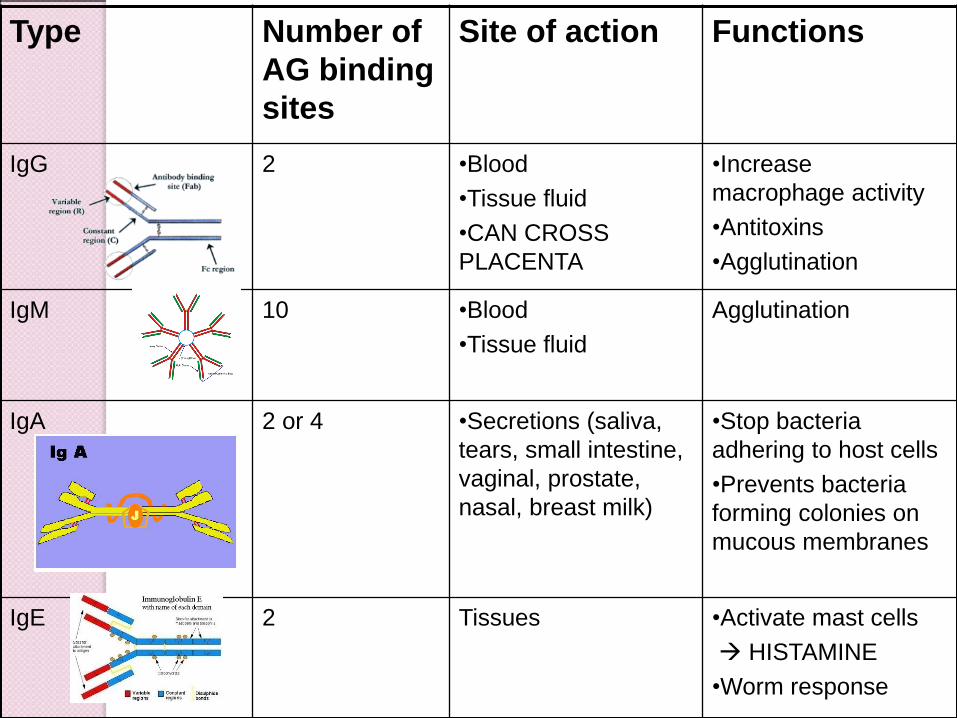
Type Number of
AG binding
sites
Site of action Functions
IgG 2 •Blood
•Tissue fluid
•CAN CROSS
PLACENTA
•Increase
macrophage activity
•Antitoxins
•Agglutination
IgM 10 •Blood
•Tissue fluid
Agglutination
IgA 2 or 4 •Secretions (saliva,
tears, small intestine,
vaginal, prostate,
nasal, breast milk)
•Stop bacteria
adhering to host cells
•Prevents bacteria
forming colonies on
mucous membranes
IgE 2 Tissues •Activate mast cells
HISTAMINE
•Worm response

Functions of antibodies
Chapter 21, Immune System 93
Since antibodies are useless against intracellular antigens, cell-mediated immunity is needed
Two major populations of T cells mediate cellular immunity
◦ CD4 cells (T4 cells) are primarily helper T cells (TH)
◦ CD8 cells (T8 cells) are cytotoxic T cells (TC) that destroy cells harboring foreign antigens
Other types of T cells are:
◦ Suppressor T cells (TS)
◦ Memory T cells
Cell-Mediated Immune Response
T Cells and Cell Mediated Immunity
Cellular Components of Immunity:
◦ T cells are key cellular component of immunity.
◦ T cells have an antigen receptor that recognizes and
reacts to a specific antigen (T cell receptor).
◦ T cell receptor only recognizes antigens combined
with major histocompatability (MHC) proteins on the
surface of cells.
MHC Class I: Found on all cells.
MHC Class II: Found on phagocytes.
◦ Clonal selection increases number of T cells.

T Cells Only Recognize Antigen Associated
with MHC Molecules on Cell Surfaces
Chapter 21, Immune System 96
T cells recognize and respond only to processed fragments of antigen displayed on the surface of body cells
T cells are best suited for cell-to-cell interactions, and target: ◦ Cells infected with viruses, bacteria, or
intracellular parasites
◦ Abnormal or cancerous cells
◦ Cells of infused or transplanted foreign tissue
Importance of Cellular Response

LT – T cells must make direct
contact with their target cells
LT differentiate in the thymus, from immature precursor cells that migrate there from the BM, into cytotoxic T cells (TC), helper T cells (TH), and suppressor T cells
LT are responsible for cell-mediated immunity
-contact with APCs, using membrane T-cell receptors
(mature T-cells have receptors which have a very similar structure to ABs and are specific to one AG).
-binding AG (from APC or invaded cell body) to T-cell receptors, activates T cell
-activated LT divide to form:
cytotoxic T cell (killer T cells) destroy AG helper T cells secretes cytokines that enhance the immune response (help B cells divide, stim macroph.)
memory T cells, remain in body
LT can not bind to free-floating AGs as LB; only bind to AGs presented as part of a membrane protein complex (MHC)
Chapter 21, Immune System 98
Major roles in immunity are: ◦ To engulf foreign particles
◦ To present fragments of antigens on their own surfaces, to be recognized by lymphocytes
◦ Secrete soluble proteins that activate T cells
Major APCs are dendritic cells (DCs), macrophages, and activated B cells
Antigen-Presenting Cells (APCs)
MHC incorporate AG fragments
Membrane protein complexes present in all nucleated
cells, are responsible for the extracellular presentation of
processed AG fragments (AG is engulfed, digested, and
their fragments are combined with an MHC complex and
inserted into cell mb by exocytosis)
2 types of MHC
MHC class I molecules – in all nucleated cells
(LT that binds to MHC class I- AG complexes kill the cell to
prevent the pathogen from reproducing)
MHC class II molecules – found primarily on APCs
Chapter 21, Immune System 100
Endogenous antigens are:
◦ Degraded by proteases and enter the
endoplasmic reticulum
◦ Transported via TAP (transporter associated
with antigen processing)
◦ Loaded onto class I MHC molecules
◦ Displayed on the cell surface in association with
a class I MHC molecule
Class I MHC Proteins

Chapter 21, Immune System 101
Class I MHC Proteins
Figure 21.15a
Chapter 21, Immune System 102
Class II MHC proteins are found only
on mature B cells, some T cells, and
antigen-presenting cells
A phagosome containing pathogens
(with exogenous antigens) merges
with a lysosome
Invariant protein prevents class II
MHC proteins from binding to peptides
in the endoplasmic reticulum
Class II MHC Proteins
Chapter 21, Immune System 103
Class II MHC proteins migrate into the
phagosomes where the antigen is
degraded and the invariant chain is
removed for peptide loading
Loaded Class II MHC molecules then
migrate to the cell membrane and
display antigenic peptide for
recognition by CD4 cells
Class II MHC Proteins

Chapter 21, Immune System 104
Class II MHC Proteins
Figure 21.15b

Chapter 21, Immune System 105
Provides the key for the immune system to
recognize the presence of intracellular
microorganisms
MHC proteins are ignored by T cells if they
are complexed with self protein fragments
Antigen Recognition

Chapter 21, Immune System 106
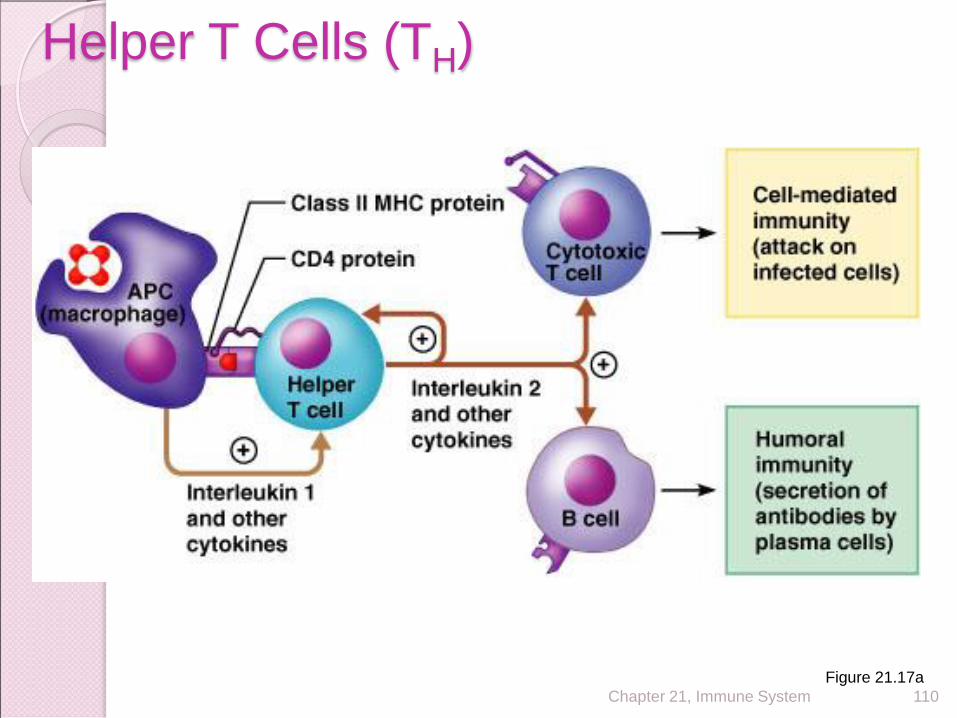
Major Types of T Cells
Figure 21.14

T Cells and Cell Mediated Immunity
Types of T cells
1. T Helper (TH) Cells: Central role in immune
response.
CD4+
Recognize antigen on the surface of antigen
presenting cells (e.g.: macrophage)+ MHCII
molecules
Activate macrophages
Induce activation of cytotoxic T cells
Stimulate B cells to produce antibodies by cytokine
production

Chapter 21, Immune System 108
TH cells interact directly with B cells that have antigen fragments on their surfaces bound to MHC II receptors
TH cells stimulate B cells to divide more rapidly and begin antibody formation
B cells may be activated without TH cells by binding to T cell–independent antigens
Most antigens, however, require TH co-stimulation to activate B cells
Cytokines released by TH amplify nonspecific defenses
Helper T Cell

Chapter 21, Immune System 109
Regulatory cells that play a central role in
the adaptive immune response
Once primed by APC presentation of
antigen, they:
◦ Chemically or directly stimulate proliferation of
other T cells
◦ Stimulate B cells
Without TH, there is no immune response
Helper T Cells (TH)
Chapter 21, Immune System 110
Helper T Cells (TH)
Figure 21.17a
Types of T cells (Continued) 2. Cytotoxic T (Tc) Cells: Destroy target cells.
CD8+
Recognize antigens on the surface of all cells, in
association with MHC I molecules:
Kill host cells that are infected with viruses or bacteria.
Recognize and kill cancer cells.
Recognize and destroy transplanted tissue.
Release protein called perforin which forms a pore
in target cell, causing lysis of infected cells.
Undergo apoptosis when stimulating antigen is
gone.

Cytotoxic T Cells Lyse Infected Cells
Chapter 21, Immune System 113
TC cells, or killer T cells, are the only T cells that can directly attack and kill other cells
They circulate throughout the body in search of body cells that display the antigen to which they have been sensitized (clone)
Their targets include:
◦ Virus-infected cells
◦ Cells with intracellular bacteria or parasites
◦ Cancer cells
◦ Foreign cells from blood transfusions or transplants
Cytotoxic T Cell (Tc)
Chapter 21, Immune System 114
In some cases, TC cells: ◦ Bind to the target cell and release perforin into
its membrane In the presence of Ca2+ perforin causes cell lysis by
creating transmembrane pores
Other TC cells induce cell death by: ◦ Secreting lymphotoxin, which fragments the
target cell’s DNA
◦ Secreting gamma interferon, which stimulates phagocytosis by macrophages
Mechanisms of Tc Action
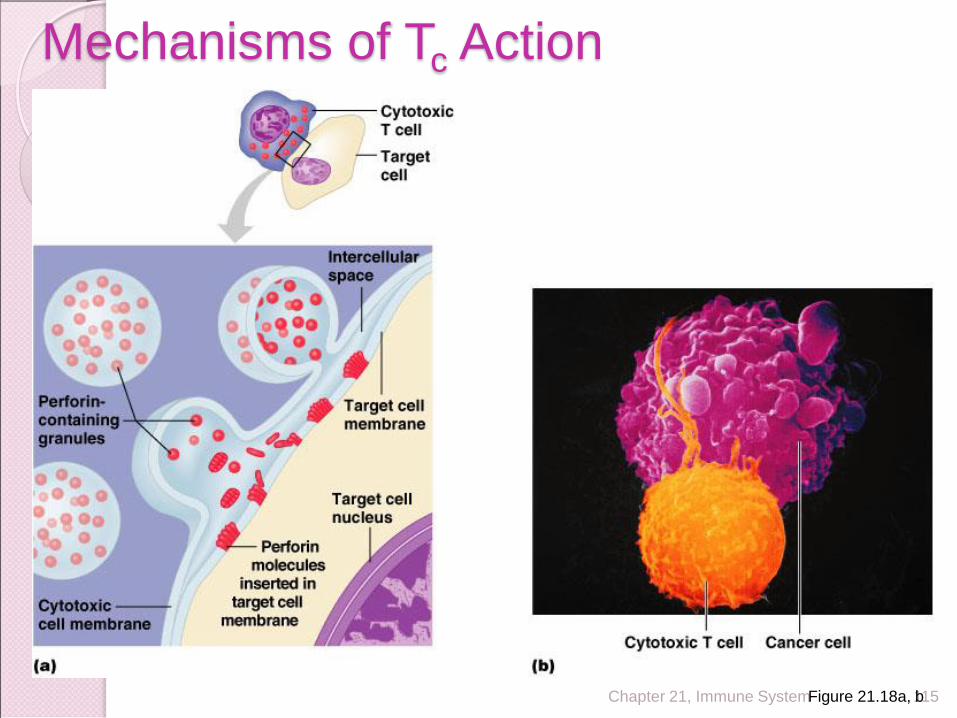
Chapter 21, Immune System 115
Mechanisms of Tc Action
Figure 21.18a, b

Chapter 21, Immune System 116
- capable of suppressing the functions of both cytotoxic and helper T cells
- prevent the cytotoxic cells from causing excessive immune reactions that might be damaging to the body's own tissues (regulatory T cells)
- plays an important role in limiting the ability of the immune system to attack a person's own body tissues, called immune tolerance
Suppessor T cell
T cells
helper T cells (TH)
◦ secrete cytokines: IL, interferons, colony-stimulating factors
cytotoxic T cells (TC)
◦ attack and destroy cells that display MHC class I-AG complexes
◦ release perforin along with granzymes apoptosis
◦ bind to ‘Fas’ receptors (death receptors) on cell surface
apoptosis
suppressor T cells
- capable of suppressing the functions of both cytotoxic and helper T
cells
- prevent the cytotoxic cells from causing excessive immune reactions
that might be damaging to the body's own tissues (regulatory T cells)
- plays an important role in limiting the ability of the immune system to
attack a person's own body tissues, called immune tolerance

Chemical signaling in immune system Antibodies: identify and target the pathogens Cytokines: communication molecules released in response to stimuli; act as
both local and long-distance signals; regulatory peptide that control cell develop, different and immune response; IL-1
Opsonins - acute phase proteins (liver proteins, act also as anti-protease molecules) - complement proteins (also cytolytic agent and mediator of inflammation) Chemotaxins Pyrogens: fever-producing substances Kinins Bradykinin (stimulates pain receptors; vasodilator) Histamine: initiate inflammation vasodilator and bronchoconstr. released by
mast cells Granzymes (cytotoxic enzymes that trigger cellular suicide) Interferons: proteins that inhibit viral reproduction; modulate immune
response Lysozyme: bactericidal enzyme MHC: membrane protein complexes used for cell recognition Membrane attack complex: a membrane pore protein made in the
complement cascade Perforin: membrane pore protein made by natural killer and cytolytic T cells T-cell rec: mb rec on LT that recognize and bind AG presented by MHC rec