1 to establish peterborough final draft may 2009 peterborough transition plan commercial in...
Post on 19-Dec-2015
213 views
TRANSCRIPT
1
To establish
Peterborough Final DraftMay 2009
Peterborough Transition
Plan
COMMERCIAL IN CONFIDENCE
2
CONTENTS
Page
A. Foreword 3B. Executive Summary 4C. Our Transition Plan 6 D. Our Plans for Commissioning
Community Services 11
E. Our Journey so far 26F. Our Integrated Business Plan 31
1. Executive Summary 312. Profile 323. Strategy 334. Market Assessment 365. Service Development Plans
406. Financial Plans 447. Risks 498. Leadership and Workforce 519. Governance 53
G. Conclusion 57
Peterborough Community Services Transition Project Initiation Document (PID)
PCS Transition Action Plan NHS Peterborough “Living
longer, living well” 5 Year Strategic Plan 2009-2014
NHS Peterborough Operational Plan 2009/10
Next Steps Project PID Moving Forward Project PID Diagnostic and audit reports E&Y Reports on Service
Reviews Core Service Review Time to Care Priority Based Service
Reviews Reports on District Nursing &
Health Visiting Reviews Service Line Management
Project PID Next Steps Consultation
Document NHS Peterborough Business
Case recommending the future organisational model for Peterborough community services, ,November 2008
Capacity for Change Project proposal
PCS Annual Plan 2009/2010 PCS Financial Plan 2009/2010 Draft Care Strategy Section 75 Partnership
Agreement
Supporting Documents:Available on request
3
We are both pleased to introduce this joint Transition Plan.
NHS Peterborough and Peterborough Community Services (PCS) are committed to ensuring there is a strong community provider that ensures that the ‘unique’ integration of health and social care is sustained. There is a shared belief that full separation and ultimate Community Foundation Trust (CFT) status will benefit the people served by NHS Peterborough and PCS by providing a solid platform from which to maintain a balanced portfolio of the highest quality and most cost effective health and social care community services delivering maximum public value
.
The assessment process for CFT status, including strict scrutiny of the governance and financial systems, will provide NHS Peterborough with assurance that PCS has the qualities to remain a major provider of community services in Peterborough.
Contestability of community services will be an ‘ongoing’ process. The Transition Plan outlines a plan for ensuring that contestability and choice is at the heart of community services provision, ensuring continuous improvement in both the quality of services and a continued emphasis on supporting personalisation, choice and control to meet local peoples needs. It is critical to ensure that we can best meet the aspirations of our population with viable providers that can deliver high quality care closer to home and where appropriate in peoples homes.
To conclude, NHSP is committed to supporting PCS achieve CFT status in the full belief that this is the best model for the future delivery of our integrated health and adult social care community services. A great deal of progress has already been made to transform the PCS into a World Class Provider and the PCT into a World Class Commissioner. This Transition Plan outlines the next steps in that journey. We are jointly committed to ensuring this is successfully delivered for the people of Peterborough by achieving strong, vibrant and viable community services for the future.
Angela Bailey Robert Ferris
Chief Executive Managing DirectorNHS Peterborough Peterborough Community Services
FOREWORD
4
EXECUTIVESUMMARY
‘Our Organisation is unique. We commission and provide both health
and adult social care services to the people of Peterborough.’
Our Peterborough Transition Plan describes the journey we are taking to establish our directly managed primary and community services as a separate, viable, independent organisation, offering high quality services to meet the needs of our local community. It is the joint plan of NHS Peterborough and Peterborough Community Services and forms part of the PCT’s World Class Commissioning Development Plan.
Our journey to separation started in 2006, when Peterborough PCT was established following the publicationof ‘Commissioning a Patient Led NHS’ (CPLNHS) in August 2005. CPLNHS proposed that, to allow PCTs tofocus on their commissioning role, they should consider divesting themselves of their directly managed provider services. Our journey is likely to continue to 2012 and beyond.
We have acted on CPLNHS recommendations by assessing all of the options open to our community services, identifying our preferred model and separating our provider services into an Arms Length Trading Organisation(ALTO). We have determined that the best future organisational model for Peterborough Community Services is that of a community foundation trust (CFT). This is the only model that appears to be acceptable to Our key stakeholders mainly because, as a CFT and a statutory organisation, we could continue to provide the integrated health and adult social care services which are so important to us in Peterborough. We also believe that the process of preparing to become a CFT will ensure that our community services are delivered in the most effective and efficient way possible.
Our Transition Plan describes our journey so far and the journey we still have to make to reach our desired destination. We have already made significant progress and are aware that we still have a great deal to do to transform PCS into an organisation fit to be a CFT. The time line shown below sets out this journey. We have estimated the time we will need based on the experience of foundation trusts and the pilot community foundation trust who have advised us that the process is long and the time line is likely to change frequently.
NHSP established Next Steps/Moving PCS established PCS on FT pipeline Service transformation Apply to PeterboroughSeparate Provider Forward Projects as an ALTO and established & business readiness SoS & Monitor establishedDirectorate CFT Model confirmed as an APO for CFT status as a CFT?
2006 2007 2008 2009 2010 2011 2012

5
EXECUTIVE SUMMARY
NHS East of England have asked that our Transition plan responds to the following questions: How our plans for provider unit separation will lead to contestability and competition for community services; How we will strengthen our commissioning of these services to ensure commissioner-led redesign of services Staff and stakeholder engagement plan and communications strategy Provider separation arrangements Identification of organisational models and their appraisal leading to preferred selection Development of robust business plans for preferred model(s) and their evaluation for appropriateness,
viability and sustainability Business continuity plans for the period of development Development and training plan for skills and competencies to assist providers make successful transition to
new forms Risk assessment, mitigation and management plan A timeline with key milestones identified Transitional costs
We have set out our plan in four main chapters to cover these questions. These are:Our Transition Plan This chapter introduces the transition plan and describes the context, principles and approach to our plan. It
also covers the timeline and estimated transition costs.
Our Plans for Commissioning Community Services
This chapter sets out our vision for commissioning community services and describes how we will assess the market, strengthen our commissioning and support PCS through our contestability and procurement plans. It outlines our strategic and operational plans and identifies our key developments together with our commissioning timeline.
Our Journey so far Our journey so far describes the process we used to separate PCS into an ALTO and the transformation work we have already undertaken to change and develop our services. It also explains the process we used and the reasons for deciding on our preferred organisational model for PCS of a Community Foundation Trust.
Our Integrated Business Plan
This section includes PCS’s first draft Integrated Business Plan (IBP). It is set out in the format recommended by Monitor and covers a profile of our services, our vision and strategy. It outlines market assessment, our rationale for becoming a CFT, our service development plans and our financial projections and risks. It also includes our stakeholder engagement plans, development and training plan, continuity plan and governance arrangements. The IBP contains commercially sensitive information and is at a very early stage of development. It will continue to be developed over the next months and years.
6
OUR TRANSITION
PLAN
‘Peterborough Community Services is aspiring to perform as a World Class provider and
operate as a Community Foundation Trust’
NHS Peterborough (NHSP) has decided to separate the
services it directly provides, known as Peterborough
Community Services (PCS), into an autonomous
organisation and ideally establish it as a Community
Foundation Trust (CFT) for Peterborough.
Our Transition Plan describes our journey from the
beginning when we were established as Peterborough
PCT in 2006 (we are now called NHS Peterborough) and
separated our provider services into one directorate.
It covers the progress we have made by separating our
provider services into an Arms Length Trading
Organisation (ALTO), agreeing our preferred long term
organisational models for our different service groups
and confirming our commissioning plans for community
services which include how we will develop the market
for community services and ensure contestability.
It includes work we have already started to become
an Autonomous Provider Organisation (APO) and
transform our services by understanding our
services better and identifying areas where we can
improve.
Our transition plan then moves on to set out a
challenging programme to change our services and
business infrastructure to ensure that PCS can
operate as an independent viable organisation
delivering high quality services which respond to
our commissioners' requirements and meet the
needs of our local community. We have described
our future plans in the section on our Integrated
Business Plan.
Our plan forms part of our World Class
Commissioning Development Plan and is a joint plan
between NHSP and PCS.2006 2007 2008 2009 2010 2011 2012
NHSP established Next Steps/Moving PCS established PCS on FT pipeline Service transformation Apply to PeterboroughSeparate Provider Forward Projects as an ALTO and established & business readiness SoS & Monitor establishedDirectorate CFT Model confirmed as an APO for CFT status as a CFT?

7
OUR TRANSITION PLAN: Guiding Principles
‘Transforming Community Services’ sets out a number of guiding principles which have been used to underpin our transition plan and associated programmes and projects.
They are summarised as follows: Interests of patients and carers are paramount Quality is the organising principle There is a clear commissioning strategy Proposals must deliver value for money Decisions about services should be made locally and include consultation Services should be designed to meet local need Staff, unions and stakeholders must be involved in decisions High standards of human resource management Processes must be clear, robust and transparent Proposals must enable integrated care, with Local Authorities, World Class Commissioning and patient choice Proposals must fit DH principles and rules for cooperation and competition Options are equality impact assessed Service continuity, assets and staff pensions must be safeguarded
The Transition Plan has been prepared in the context of the following National, regional and local policy, guidance and requirements:
Commissioning a Patient Led NHS’, August 2005, Our Health; Our Care; Our Say, 2006, Every Child Matters, 2003Putting People First, October 2007 High Quality Care for All, June 2008, The NHS Operating Framework, 2009/20010 Transforming Community Services: Enabling new patterns of provision’ 2009 Improving Lives; Saving Lives, NHS East of England, 2007 Towards the Best, Together, NHS East of England Peterborough PCT Strategic Service Development Plan, 2007- 2012 Joint Strategic Needs Assessment for Peterborough, 2007Section 75 Partnership Agreement for adult social care services with Peterborough City Council NHS Peterborough 5 year Strategy ‘Living Longer, Living Well’ 2009 Annual Accountability Agreement 2009-2010 with Peterborough City Council
The Next Stage Review, High Quality Care for All, identified a number of objectives to achieve the vision for community services. These have been taken into account in our transition plan.
They are:
Make quality our organising principle Empower staff to improve patient care and focus on quality Enable World Class Commissioning Provide direction and strengthen leadership Promote patient choice Foster appropriate competition to drive better service quality and value for money Protect assets and the interests of taxpayers and ensure flexibility Ensure the provision of safe, fit for purpose buildings
Context ObjectivesPrinciples
8
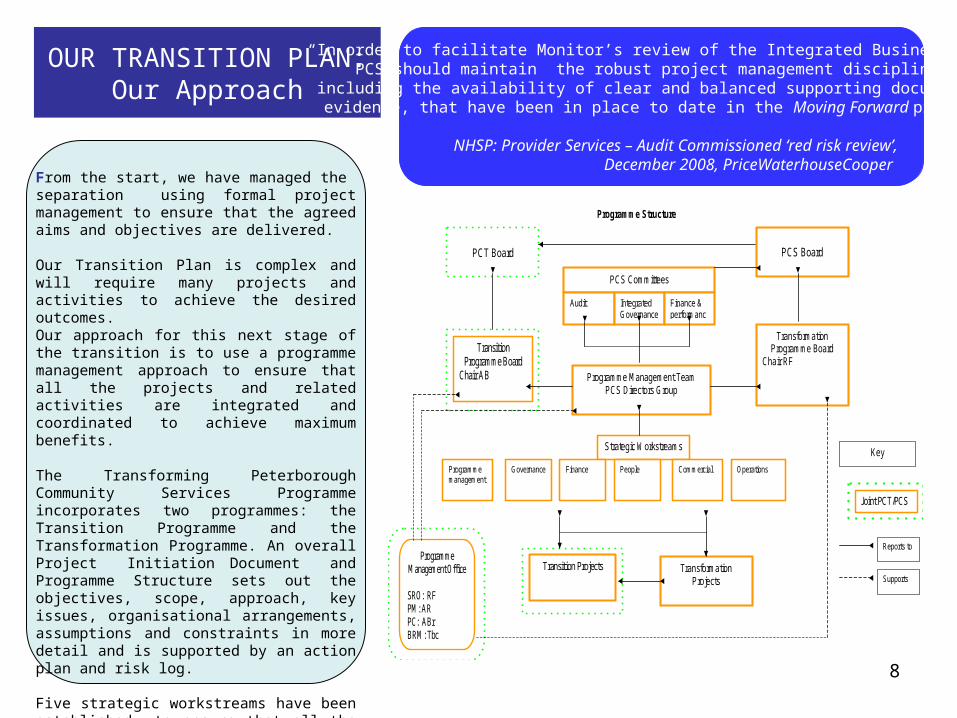
OUR TRANSITION PLAN:Our Approach
Programme Structure
PCT Board
PCS Board
PCS Committees
Audit Integrated Governance
Finance & performance
Transition Programme Board
Chair AB
Transformation Programme Board
Chair RF
Programme Management Team PCS Directors Group
Programme
Management Office
SRO: RF PM: AR PC: ABr BRM: Tbc
Key
Joint PCT/PCS
Reports to
Supports
Strategic Workstreams
Operations Governance Finance People Commercial Programme management
Transition Projects
Transformation Projects
“In order to facilitate Monitor’s review of the Integrated Business Plan, PCS should maintain the robust project management disciplines,
including the availability of clear and balanced supporting documentary evidence, that have been in place to date in the Moving Forward project.”
NHSP: Provider Services – Audit Commissioned ‘red risk review’, December 2008, PriceWaterhouseCooper
From the start, we have managed the separation using formal project management to ensure that the agreed aims and objectives are delivered.
Our Transition Plan is complex and will require many projects and activities to achieve the desired outcomes. Our approach for this next stage of the transition is to use a programme management approach to ensure that all the projects and related activities are integrated and coordinated to achieve maximum benefits.
The Transforming Peterborough Community Services Programme incorporates two programmes: the Transition Programme and the Transformation Programme. An overall Project Initiation Document and Programme Structure sets out the objectives, scope, approach, key issues, organisational arrangements, assumptions and constraints in more detail and is supported by an action plan and risk log.
Five strategic workstreams have been established to ensure that all the objectives are achieved and the resulting changes are embedded throughout the organisation. They are: Governance, Finance, People, Commercial and Operations.

9
OUR TRANSITION PLAN: Costs and Assurance
Will delivery of the plan lead to the formal transition to ALTO being completed by April 2009
Yes: ALTO status achieved in April 2008. ALTO checklist completed with evidence available. Full “business readiness for PCT provision check list (by DH) completed and all tasks due to be completed or have been achieved. All others are in progress and on time. Our Annual Plan has been submitted to EoE PDB
How the Provider will identify the core services that it will be responsible for providing?
Yes: We have carried out a core service review and clarified our core services. We carried out a Time to Care exercise and have a clear view on current productivity and competitiveness levels of our services following a market analysis, a costing exercise and improved data collection and analysis.
Does the plan indicate how the PCT will develop a clear view on which organisational form to adopt?
Yes: Our Transition Plan describes the consultation, option appraisal and business case produced to confirm our preferred organisational model. Risks, costs, timescales and draft Integrated Business Plan are covered.
Does the plan outline how the PCT will establish robust governance arrangements for the transition?
Yes: Our Integrated Business Plans includes both the governance arrangements specific to the Transition Programme and the arrangements in place or being established to ensure the organisation is well governed. These include our Board appointments and development programme, BAF and use of Performance Accelerator
Does the plan ensure that the Provider has the capability and capacity to operate as an ALTO?
Yes: the Plan demonstrates that not only can we operate as an ALTO, we are making fast progress towards APO status. Where we have identified shortfalls in capacity an capability, we have engaged external support, such as Deloitte to carry out the market analysis and E&Y to support some of our Transformation Programmes. We have proposed a new Executive structure and are implementing Service Line Management and service redesign to maximise capacity
Is the Provider engaging all relevant stakeholders in developing the transition plan?
Yes: all relevant stakeholders have been and will be engaged throughout the transition process, including recent involvement in developing our Care Strategy. We have a Communication Plan, and are in the process of producing our Transition Engagement and Communication Plan. Out transition plan builds on a number of plans and projects which have been developed with our stakeholders. Our Board includes lay members and the LA.
OUR ASSURANCEThe SHA have asked six questions to provide assurance that the Transition Plan will lead to the required standards for provider separation.
We believe that our plan, together with other supporting evidence, demonstrates that we have fully achieved all the requirements and, in many cases, exceed them. Under the RAG rating, we have scored ourselves ‘green’
Our Transition CostsUsing a recognised formula applied to organisational changes we have estimated a total transition cost equivalent to approximately 2% of turnover spent over a three year period. Assuming an amended recurring income of £69m our transition costs will be £1.3m. We can expect to spend approximately 50% of this in the first year with reducing amounts in the subsequent two years. An additional 2% efficiency each year for three years would generate the equivalent of 6% or £4.1m. In addition, it has been estimated that approximately £0.6m will be required for non-recurring transitional costs. NHSP has agreed in principle that there is a need to recognise the cost of transition and will address this as part of its overall financial plan for 2009/10 and beyond. The Business Case agreed by the PCT Board estimated additional recurrent revenue costs of £1.3m to operate PCS as a CFT. Transition costs cover three areas: Additional Capacity associated with being a fit for purpose organisation, Transformational Costs associated with building a sustainable future, Additional Costs associated with being a separate organisation e.g. external audit.
10
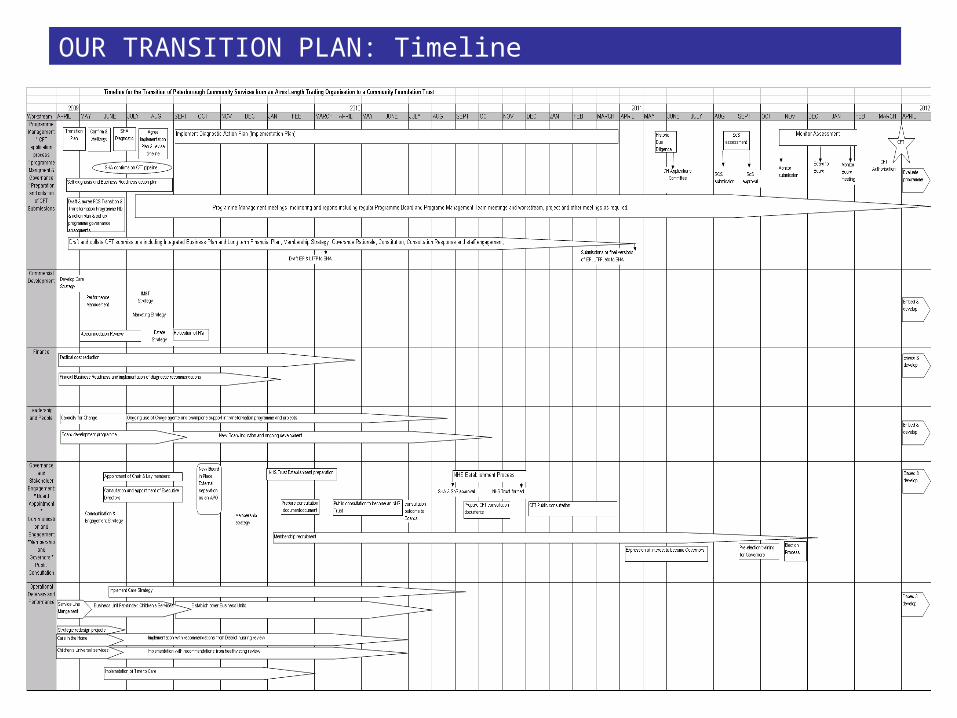
OUR TRANSITION PLAN: Timeline
11
Our Plans for Commissioning Community Services: Vision for community services
‘The future focus will be on moving care into the community, the
home, and other primary care settings ‘
The challenge of enabling 21st century health and adult social care services in Peterborough is both ambitious and
formidable. With the new City Care Centre opening in 2009, a new hospital, new mental health facilities, and with
more accessible services planned in its neighbourhoods, the ambition to ensure 21st century care has started well.
However, some of Peterborough’s population still have poorer health outcomes, shorter life expectancy and a higher
burden of disease than their neighbours. Consequently as the local leaders of the National Health Service, we are
determined to see that picture change. NHS Peterborough takes very seriously the responsibility of working with
organisational partners and listening and working with local people to change the patterns of the past to deliver a
better future for the health and well being of the people of Peterborough.
With the current economic outlook the underlying theme is that service change and improvement must be
undertaken through redesign, modernisation and improved efficiency of existing services. A key focus will be to use
hospital services for the more complex and specialist care, whilst continuing a comprehensive programme to
increasingly support care delivery within the home and other community and primary care based settings; this will
be achieved through creating financial flexibility by disinvestment in outmoded or outdated services and detailed
robust service specification leading to (re) investment in new 21st century services that meet the needs of
individual patients and service users in Peterborough.
Our Strategic Plan “Living longer, Living Well” and the directly related 2009/10 Operational Plan are the outcomes
of key planning processes within NHS Peterborough which are derived from extensive engagement with partners via
the Sustainable Community Strategy and Local Area Agreement and most importantly, are underpinned by listening
carefully to the views of local people.
The ongoing strategy of shifting care (outpatient, minor and routine surgery, some invasive procedures) away from
hospitals into a community setting has and will continue, to present opportunities for community providers including
Peterborough Community Services, to grow their businesses.
Our planning processes and commissioning intentions have informed the parallel business planning and related
processes of PCS contained within this Transition plan. We are confident that our strategic aims have been
communicated effectively and are at the centre of PCS’s mission to provide cost effective, high quality services
which meet specified outcomes.
12
Our Plans for Commissioning Community Services: Vision for community services (Continued)
‘PCS’ vision is to provide competitive, integrated health and social care services which contribute to individual well-being.’
Driven by the action plans emanating from the current Organisation Development Plan process, NHS
Peterborough’s enhanced world class commissioning (WCC) approach (throughout the whole of the commissioning
cycle) will, over the next two to three years or so, undertake a market segmentation analysis in relation to
community services. Where appropriate and possible this will lead to market stimulation and lead to enhanced
choice for service users and patients and value for money.
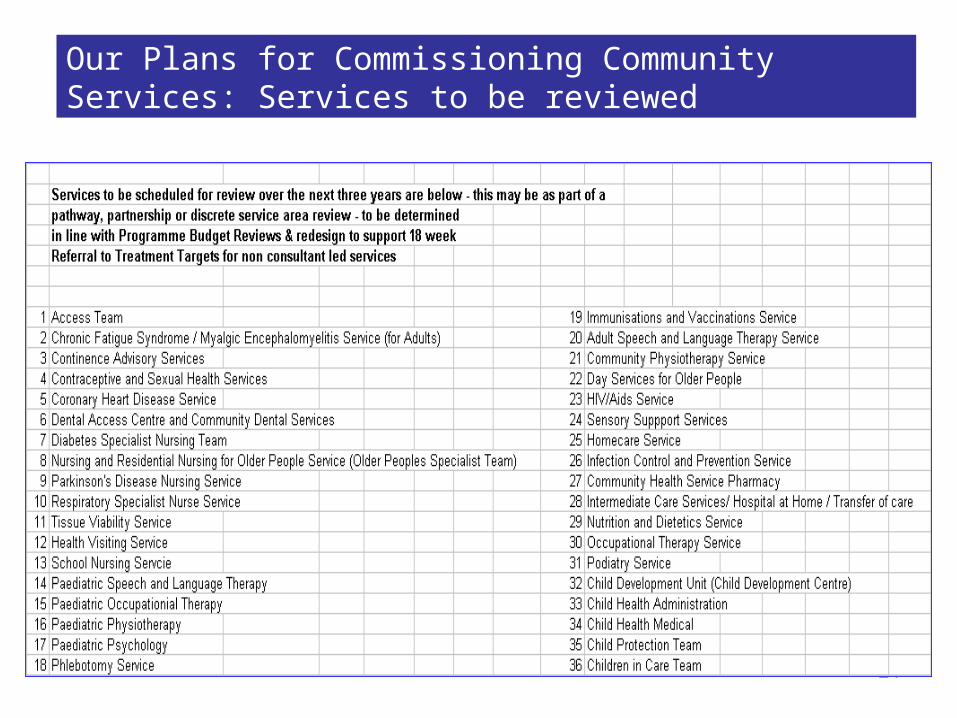
Concurrent with the segmentation of the community services health and social care markets, reviews of PCS
services within those market segments will be undertaken. Each service or set of related services along a current
or proposed future pathway or pathway redesign will then be robustly examined and analysed as to their current
and future fitness for purpose. It is envisaged that all services provided by PCS will be reviewed in the next three
years.
Where redesign or re-specification is sought the NHS Peterborough Principles of Contestability will be used to
determine whether PCS services will be subject to full contestability within the market place or that the qualifying
conditions for ‘non contestability’ apply and a collaborative commissioner led redesign approach will be undertaken
with Peterborough Community Services and other providers if applicable. (i.e. GPs and Peterborough and Stamford
Hospitals Foundation Trust)
NHS Peterborough is committed to ensuring that over the next two to three years, through the series of robust
reviews outlined that PCS will be perfectly placed as a strong provider with a portfolio of high quality, outcome
based, value for money community services.
This will be coupled with a drive to ensure that the market for services is stimulated, developed and managed so
that, where appropriate and right, services that may currently be provided by PCS are provided by other
organisations in order to best serve the individual preferences and needs of the population of Peterborough. The
corollary of this is that PCS will also be able as a strong provider to grow its business in ‘core areas’ where it is
strongest and that best fit its own strategic direction as a provider in a timed and managed way.
Thus there will be a strong and sustainable platform to move from being an Arms Length Trading Organisation
(ALTO) to an independent Community Foundation Trust (CFT) .

13
Our Plans for Commissioning Community Services: Market Development
As part of our Organisation Development we will manage and develop the market to give a clear approach to addressing the
market development issues of a) segmenting the market through client groups, care pathways and geographical areas b)
identification of gaps in the market and attraction of new providers and c) a greater understanding of provider economics and
quality will emerge.
Following on from the regionally led Health Market Analysis Project 2008 which NHS Peterborough Commissioner’s took part in,
the methodology undertaken will form a basis for the type of approach that NHS Peterborough will take for Health and Adult Social
Care market development.
The Methodology of the 7 step approach to Market Development is broadly as follows:
1. Segmentation - an initial approach to common segmentation informing data collection to support economic analysis
2. Demand Forecasts – demand modelling focusing on utilisation by disease category
3. Service Analysis – aspects of service quality analysed using common metrics across the EoE region, similar PCT comparators
and the national average.
4. Economic Attributes – economic structure of services in EoE analysed using data on expenditure, providers and contracting
5. Priorities – prioritised services for further review following demand, service and economic analysis
6. Options – market development options pursued for the prioritised services
7. Road Map – showing the way forward to the creation of a more diverse and vibrant market for community services.
‘Understanding the developing market is a key focus for NHSP and PCS'
14
Our Plans for Commissioning Community Services:NHS Peterborough Strategic and Operational Planning
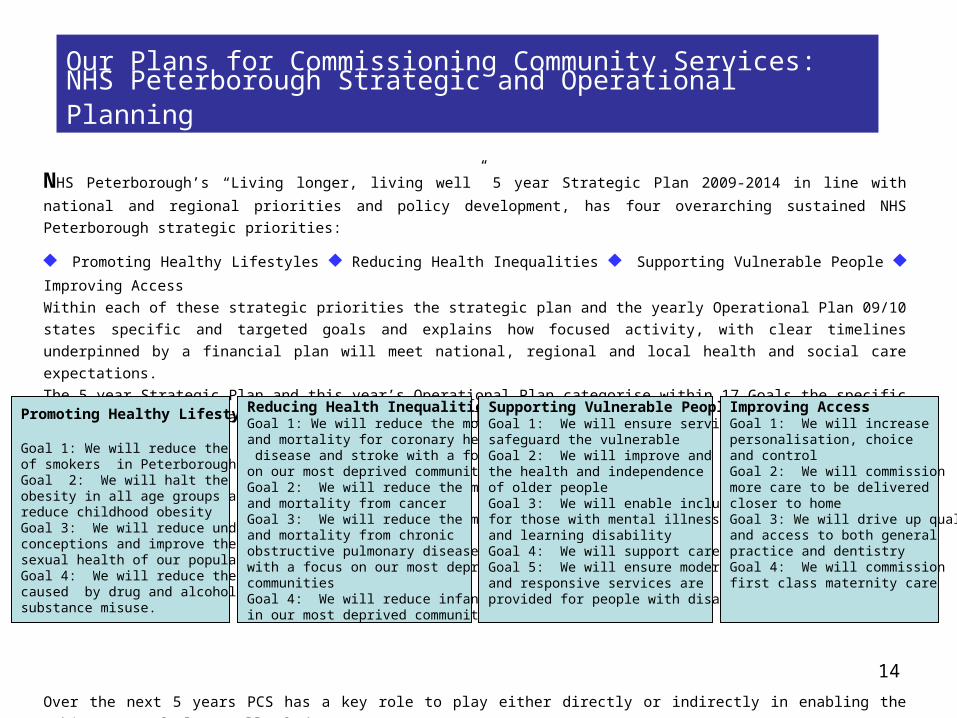
NHS Peterborough’s “Living longer, living well” 5 year Strategic Plan 2009-2014 in line with national and regional
priorities and policy development, has four overarching sustained NHS Peterborough strategic priorities:
♦ Promoting Healthy Lifestyles ♦ Reducing Health Inequalities ♦ Supporting Vulnerable People ♦ Improving
Access
Within each of these strategic priorities the strategic plan and the yearly Operational Plan 09/10 states specific and
targeted goals and explains how focused activity, with clear timelines underpinned by a financial plan will meet
national, regional and local health and social care expectations.
The 5 year Strategic Plan and this year’s Operational Plan categorise within 17 Goals the specific areas for action
and achievement. They are as follows
Over the next 5 years PCS has a key role to play either directly or indirectly in enabling the achievement of almost
all of the
strategic goals of NHS Peterborough.
Promoting Healthy Lifestyles Goal 1: We will reduce the number of smokers in Peterborough Goal 2: We will halt the rise in obesity in all age groups and reduce childhood obesity Goal 3: We will reduce under 18 conceptions and improve the sexual health of our population Goal 4: We will reduce the harm caused by drug and alcohol substance misuse.
Reducing Health Inequalities Goal 1: We will reduce the morbidity and mortality for coronary heart disease and stroke with a focus on our most deprived communitiesGoal 2: We will reduce the morbidity and mortality from cancerGoal 3: We will reduce the morbidity and mortality from chronic obstructive pulmonary disease, with a focus on our most deprived communitiesGoal 4: We will reduce infant mortality in our most deprived communities
Supporting Vulnerable People Goal 1: We will ensure services safeguard the vulnerable Goal 2: We will improve and maintain the health and independence of older people Goal 3: We will enable inclusion for those with mental illness and learning disability Goal 4: We will support carersGoal 5: We will ensure modern and responsive services are provided for people with disabilities
Improving Access Goal 1: We will increase personalisation, choice and control Goal 2: We will commission more care to be delivered closer to home Goal 3: We will drive up quality and access to both general practice and dentistry Goal 4: We will commission first class maternity care

15
Our Plans for Commissioning Community Services: The evolution of Peterborough Community Services via strengthened commissioning and contestability
‘Contestability will be the key to
competitive, high quality,
best value services'
Both commissioners within NHS Peterborough and providers within PCS hold a shared vision of what full
separation and ultimate Community Foundation Trust (CFT) status would mean for patients and social care
service users.
CFT status would provide a solid platform from which to maintain and where prudent enhance a balanced
portfolio of the highest quality and most cost effective health and social care community services.
Peterborough is a pioneer in the integration of health and social care services. A pooled budget and annual
accountability agreement with Peterborough City Council, through a Section 75 Partnership Agreement for
adult social care services with Peterborough City Council, enables NHS Peterborough to commission via
Peterborough Community Services a full range of integrated health and social care services for adults and
older people in a variety of settings (e.g. A Healthy Living Centre and imminently a new City Care Centre).
The integrated nature of health and social care services within PCS provides a high degree of assurance to
the PCT as commissioner that service delivery will be maintained throughout the process of transformation.
Through the careful and robust implementation of key principles of contestability outlined below a balanced
and planned approach to testing contestability is already well underway in relation to the services provided by
Peterborough Community Services. Over the next two to three years all of the services provided by PCS will be
part of a robust and comprehensive set of service reviews and mutually sequenced and coordinated
Programme Budget Reviews.
16
Our Plans for Commissioning Community Services: Principles of Contestability
‘Through a managed market process, we will ensure our community receives
the best service available, with minimal disruption to their care’
NHS Peterborough recognises that it has a leadership role in the development, stewardship and management
of the local health and social care provider market. In doing this NHS Peterborough recognises the contribution
and expertise of the local authority, the third sector, the independent sector and other NHS partners in
developing a successful world class contestability and robust market management approach.
The probability of risk of service disruption through ‘rushed’ procurement is mitigated if not eliminated by NHS
Peterborough systematically and robustly undergoing a cycle of commissioning/contestability and the specific
implementation of the principles of contestability.
Contestability is best achieved through a managed market process where the risks and rewards to patients and
service users, providers and NHS Peterborough are thoroughly and consistently appraised and acted upon. This
sometimes subtle balance between risks and rewards needs to be under-pinned by a
commissioning/procurement implementation plan which provides insight, research and full comprehension of
supply sectors and providers, their motivations and behaviours and economic/cost environment.
Over the next three years all of PCS’s services will be reviewed. Following the review of each service three
principles of contestation (which are logically derived from the strategic context and theoretical framework
outlined above.) will be applied to determine whether or not formal ‘contestation’ will be carried out or not.
17
Our Plans for Commissioning Community Services:
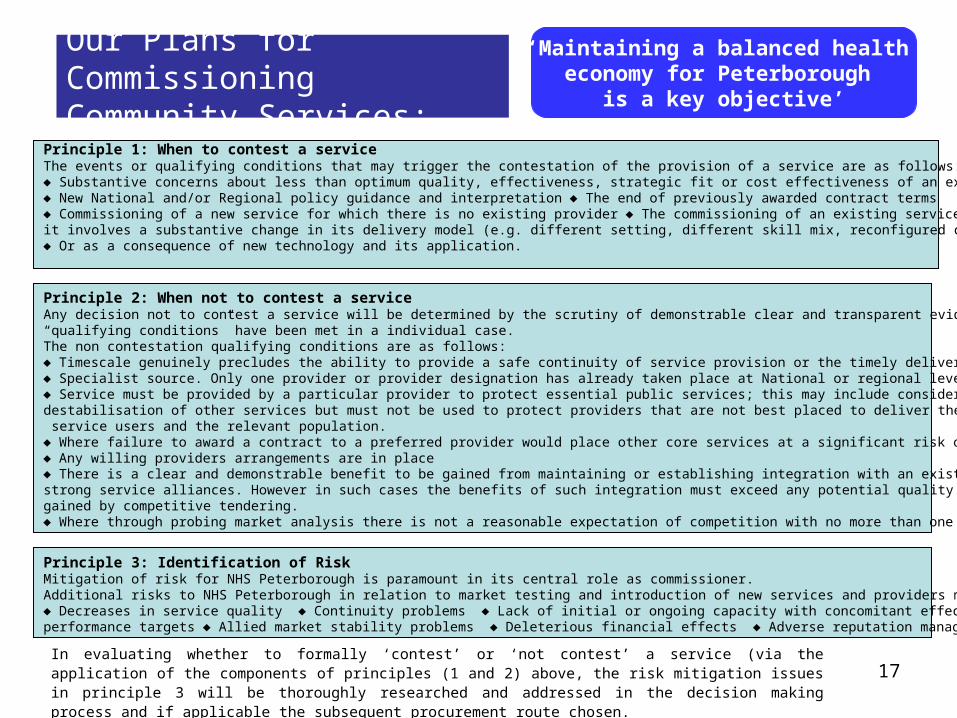
‘Maintaining a balanced health economy for Peterborough
is a key objective’
Principle 1: When to contest a service The events or qualifying conditions that may trigger the contestation of the provision of a service are as follows: ♦ Substantive concerns about less than optimum quality, effectiveness, strategic fit or cost effectiveness of an existing service ♦ New National and/or Regional policy guidance and interpretation ♦ The end of previously awarded contract terms ♦ Commissioning of a new service for which there is no existing provider ♦ The commissioning of an existing service when it involves a substantive change in its delivery model (e.g. different setting, different skill mix, reconfigured care pathway) ♦ Or as a consequence of new technology and its application.
Principle 2: When not to contest a service Any decision not to contest a service will be determined by the scrutiny of demonstrable clear and transparent evidence as to which of the “qualifying conditions” have been met in a individual case. The non contestation qualifying conditions are as follows: ♦ Timescale genuinely precludes the ability to provide a safe continuity of service provision or the timely delivery of a new required service. ♦ Specialist source. Only one provider or provider designation has already taken place at National or regional level . ♦ Service must be provided by a particular provider to protect essential public services; this may include consideration of the potential destabilisation of other services but must not be used to protect providers that are not best placed to deliver the needs of their patients and service users and the relevant population. ♦ Where failure to award a contract to a preferred provider would place other core services at a significant risk of destabilisation♦ Any willing providers arrangements are in place ♦ There is a clear and demonstrable benefit to be gained from maintaining or establishing integration with an existing service due to very strong service alliances. However in such cases the benefits of such integration must exceed any potential quality or financial advantage to be gained by competitive tendering.♦ Where through probing market analysis there is not a reasonable expectation of competition with no more than one provider coming forward
Principle 3: Identification of Risk Mitigation of risk for NHS Peterborough is paramount in its central role as commissioner. Additional risks to NHS Peterborough in relation to market testing and introduction of new services and providers may include: ♦ Decreases in service quality ♦ Continuity problems ♦ Lack of initial or ongoing capacity with concomitant effects on performance targets ♦ Allied market stability problems ♦ Deleterious financial effects ♦ Adverse reputation management
In evaluating whether to formally ‘contest’ or ‘not contest’ a service (via the application of the components of principles (1 and 2) above, the risk mitigation issues in principle 3 will be thoroughly researched and addressed in the decision making process and if applicable the subsequent procurement route chosen.

18
Our Plans for Commissioning Community Services: Strengthening of Commissioning
‘NHSP and PCS were part of the national testing process for the new NHS
Community Contract, giving us a shared insight into the benefits of the new contract’
The commissioning of community services is being strengthened through formal monitoring of the new NHS
Contract for Community Services by a Contract and Performance Group and the management at a strategic
level of in year developments by a Strategic Development Group coupled with an ongoing review of services
within an overall Programme Budget approach.
The NHS Contract for Community Services NHS Peterborough has utilised the National NHS Contract for Community Services as a SLA so as to be able to
facilitate the use of the format in its full legal sense at the point that Peterborough Community Services
becomes an Autonomous Provider Organisation. The NHS Peterborough / PCS Community NHS contract was
successfully agreed on schedule for 2009/2010.
A formal set of two interlocking PCS/PCT commissioner forums each with their own specific focus has been
established. The Contract and Performance Group (CPG) was established in April 2009 with membership from
the PCT, PCS and associate commissioners from neighbouring PCT areas. Its remit is to review progress against
existing SLAs between PCS, NHSP and other associate PCTs. NHS Peterborough PCT will be the lead
Commissioner for those neighbouring PCTs who wish to be involved, so forming a multilateral contract with PCS
at the point it becomes an Autonomous Provider Organisation (APO).
The Strategic Development Group (SDG) has been established between PCS and the PCT, in the first instance,
with a joint chairing arrangement between NHS Peterborough Commissioners and PCS to project manage an in-
year Work Development Programme for 2009/10.
Both the Contract and Performance Group (CPG) and Strategic Development Group (SDG) will meet monthly.
19
Our Plans for Commissioning Community Services: Strengthening of Commissioning
‘The information collected and reported by PCS is continually improving to provide accurate,
timely and useful performance reports to both the PCS and PCT Executive and Boards’
The CPG will use key available metrics to monitor performance against agreed specifications, the overall
financial quantum of the contract and to review the performance of the contract to ensure that all national
targets and milestones, together with any locally agreed targets, are met within the agreed plans, and that
effective steps are taken to resolve issues which may adversely impact on the delivery of these targets. In
addition consideration will be made of any capacity issues that may arise during the course of the contract
period initiating the appropriate review to support the effective delivery of services.
As part of the NHS Contract for Community Services a CQUIN incentive scheme payment of 0.5% of the NHS
contract value has been agreed. This provides an incentive for PCS to provide specified quality data in a timely
manner in the following areas:
Maximum 18 Week Referral to Treatment Targets for non consultant led targets with key quality markers to
aid responsive
deliveryMinimum Data sets across all services within the year for ten key items of data (e.g. postcode, date of birth) Financial information Pilot CQUIN (prior to national implementation) in terms of Safety, Effectiveness and service users across 4
services.
Establishing, maintaining and regularly reporting on the clear links between the 5 year Strategic Plan, the
yearly Operational Plan, the NHS Standard Community Contract and the in year Work Development Plan will
ensure progress across the commissioning cycle within a demonstrably robust WCC framework. Relevant and
appropriate performance software will be utilised to enable this process.
NHS Peterborough is confident that the appropriate level of capability and capacity that is required by the
commissioners to complete fully the key tasks of managing and monitoring the contract with PCS and therefore
providing support and assurance to the transition process will be in place.

20
Our Plans for Commissioning
Community Services: Strengthening of
Commissioning
‘Balancing investment and disinvestment in specific
Service areas will be crucial’
Programme Budget Reviews
Delivery of the Strategic Plan is based upon recognition of the need to change the way services are
delivered if financial balance is to be achieved. This will involve investing in some areas and disinvesting in
other areas. A programme of service reviews, managed by a board convened by NHS Peterborough, will be
implemented. It will use Programme Budget and Health Outcome data to review 100% of the expenditure
and identify areas where outcome is poor and/or expenditure is high. This will instigate service redesign to
meet the strategic objectives, generate financial efficiencies and release resources for reinvestment.
The comparative work has highlighted a number of areas that may require changes in services and service
models currently provided by PCS including:
Learning Disability Respiratory Musculoskeletal System problems Adult Social Care

21
Our Plans for Commissioning Community Services: 2009/10 key developments
Outlined below are some of the key planned and ongoing developments within 2009/10 which will have major
direct or indirect impacts on PCS activity.
NHSP and PCS will work together to review, redesign
and develop services
Chronic Obstructive Pulmonary Disease Currently in conjunction with the East of England SHA a COPD Care Pathway is being redesigned to the Gold standard (2008). This includes aspects of prevention and public awareness through to clinical intervention and spans primary care, secondary care and rehabilitation. A community based pulmonary rehabilitation service which will lead to positive outcomes for service users is planned to be established within the Healthy Living Centre by December 2010. There is a potential impact on PCS as it currently provides part of the current arrangements through respiratory nurse staff and the reconfiguration of the COPD rehabilitation pathway will provide for a shift of activity within it through a contestable procurement process.
Chronic Heart Disease By December 2010 NHS Peterborough will re-commission comprehensive cardiac rehabilitation services with a clear methodology for identifying, treating and following up those patients post myocardial infarction (MI) with extension of this to all those manifesting with CHD symptoms by 2011. A regional Cardiac Rehabilitation service specification is currently being used as a template to inform the design of a local template. There is expected to be a move away from the ‘sequential phases’ of the current ‘heart manual’ approach to a menu driven approach. There is a potential impact on PCS as it currently provides part of the current cardiac rehabilitation approach and the reconfiguration of the CHD rehabilitation pathway will provide for a shift of activity within it through a contestable procurement process.
Musculoskeletal Assessment and Treatment Service (MATS) The existing musculoskeletal system in NHS Peterborough has used a Musculoskeletal Assessment and Treatment Service (MATS) since October 2007 to assess and triage the majority of GP referrals into the local system. The main purpose of that system is to improve the quality of referrals reaching its main provider of secondary care, Peterborough and Stamford Hospitals Foundation Trust (PSHFT). The service is currently being reviewed and proposals for redesign and re-specification will be developed by May 2009 with the scope to consider wider integration with Pain Management Services.
Learning Disability A Priority Based Review of Learning Disability services is currently being undertaken. This review will include all learning disability services commissioned by NHS Peterborough. The current level/model of service will be defined as a baseline against which alternative levels of service can be developed. The service and financial impact taking into account risks, quality and benefit will then be developed for a variety of option levels – minimum, intermediate, current and enhanced. Service users will take part throughout the process assisted where appropriate by their advocates. When a preferred option is selected then it is envisaged elements of the learning disability service will be redesigned and potentially tendered for.
22
Self Directed Support
Self directed support (SDS) incorporating individual budgets (IB) in social care commissioning are a key to developing
choice for service users. The development of an Independent Living Support Services Access and Information Centre
(ILSS AIC) is central to the success of ensuring contestability within the Self Directed Service program. An Independent
organisation, providing advice and guidance to service users, carers, or their representatives and general members of
the public will promote the development of the service user driven market, and allow real choice in service provision.
The AIC is currently in the procurement phase and is anticipated to commence operation on the 1st October 2009. The
operator of the AIC will not be allowed to provide services. Once fully operational it is anticipated that the AIC will
become the information centre for all of the population of Peterborough who require Adult Social Care Services, care
and housing support, advice or assessment.
The ability of individuals to direct their own individual social care budgets to their preferred provider and the move
away from block or ‘purchasing intention’ contracts to “any willing provider” status will ensure over time a far more
competitive market place.
Older Peoples Accommodation Strategy
Six Peterborough City Council Older Peoples Homes are managed and staffed by Peterborough Community Services. In
June 2009 PCC Cabinet members will finalise agreement for a substantive redesign programme for this provision to
include potentially extra care housing, respite facilities, health and well being and dementia resources. Procurement of
these services will be undertaken in line with key principles of contestability over the next two years.
There are additional developments already at the implementation stage which are offering new ongoing developments
for PCS in 2009/10 for instance:
A Stroke Coordinator with specific DH Social Care funding for two years is to be recruited and employed by PCS to
support patients, carers and organisations across Peterborough to enable more effective and efficient working along
the stroke pathway.
An Integrated Diabetes service within the Healthy Living Centre facilitated by PCS has been in operation from April
2009.
Our Plans for Commissioning Community Services: 2009/2010 Key Developments continued
23
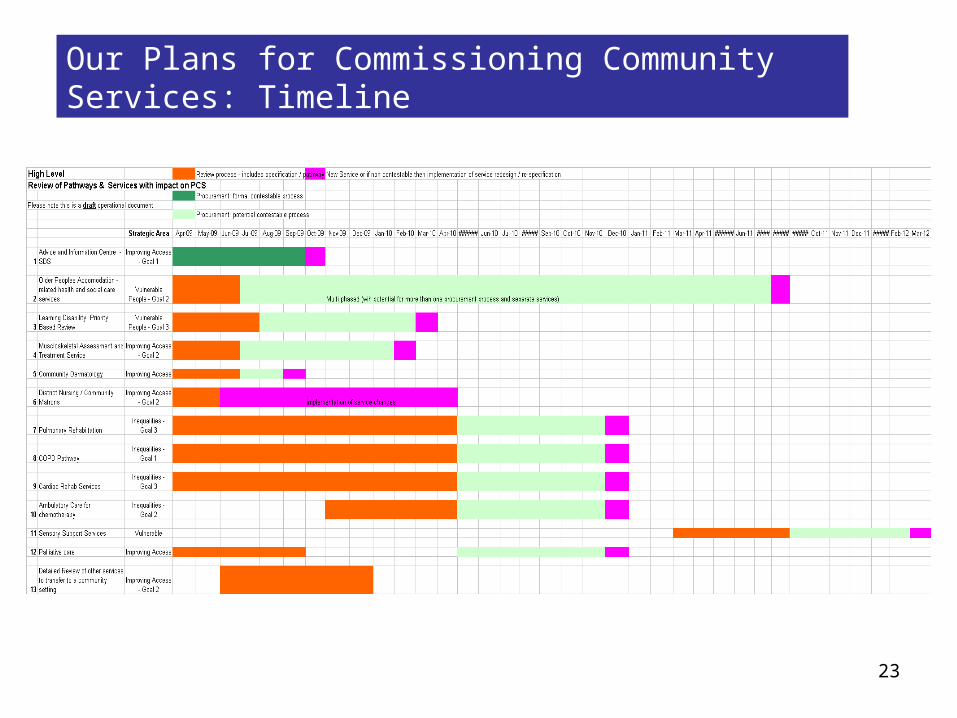
Our Plans for Commissioning Community Services: Timeline
24
Our Plans for Commissioning Community Services: Services to be reviewed

25
Our Plans for Commissioning Community Services: Conclusion
‘We have a clear strategy and timeline to achieve the successful
development of PCS as a CFT'
The strategy outlined above will be further formalised and supported by a NHS Peterborough Procurement Plan
in line with the October 2009 timetable set out in Transforming Community Services: Enabling new Patterns of
provision.
This procurement plan with its time-line informed at a summary level by the “Review of Community Services
2009-2012 Timeline” will be organised in four thematic areas:
The assessment of relevant markets (including the need for services, market structure, competition, capacity
and innovation)
The evaluation of existing contracts (measured by their performance, efficiency, demand and fitness for
purpose)
The evaluation of procurement options (by outcomes, attractiveness and whether in lots or a whole and/or from
a single or multi source)
The evaluation of procurement routes (e.g. EU part A or B options)
NHS Peterborough commissioners and PCS are confident that with a clear strategy and timeline of
commissioning developments and reviews, a well defined and increasingly robust contract relationship and a
transparent, objective, relevant and fair view of contestability, that the road from ALTO to CFT will be
achievable within the timescale outlined.
Reports used:
NHS Peterborough “Living longer, living well” 5 Year Strategic Plan 2009-2014 NHS Peterborough Operational Plan 2009/10 Transforming Community Services PPCT working paper entitled “Programme Based Budgeting for Health – Summary of 2006/7 data. Programme Budgeting Report Peterborough PCT – Eastern Region Public Health Observatory Community Services – Separation – Tool 1 – Implementation Planning – Deloittes – East of England – January 2009 – V1.0
26
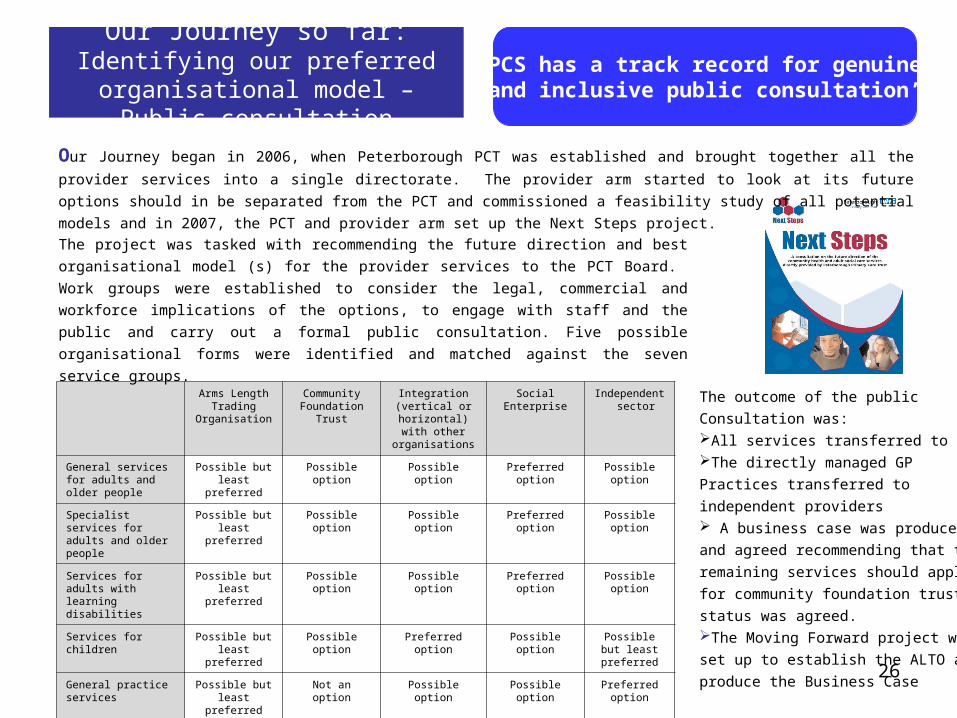
Our Journey so far: Identifying our preferred organisational model – Public consultation
‘PCS has a track record for genuine and inclusive public consultation’
Arms Length Trading
Organisation
Community Foundation Trust
Integration (vertical or horizontal) with other organisations
Social Enterprise Independent sector
General services for adults and older people
Possible but least preferred
Possible option Possible option Preferredoption
Possible option
Specialist services for adults and older people
Possible but least preferred
Possible option Possible option Preferredoption
Possible option
Services for adults with learning disabilities
Possible but least preferred
Possible option Possible option Preferredoption
Possible option
Services for children Possible but least preferred
Possible option Preferred option Possible option Possible but least preferred
General practice services Possible but least preferred
Not an option Possible option Possible option Preferredoption
Dental services Possible but least preferred
Possible option Possible option Possible option Possible option
Unplanned Care services Possible but least preferred
Possible option Possible option Possible option Possible option
The project was tasked with recommending the future direction and best
organisational model (s) for the provider services to the PCT Board. Work groups
were established to consider the legal, commercial and workforce implications of the
options, to engage with staff and the public and carry out a formal public
consultation. Five possible organisational forms were identified and matched against
the seven service groups.
The outcome of the public
Consultation was:All services transferred to an ALTOThe directly managed GP
Practices transferred to
independent providers A business case was produced
and agreed recommending that the
remaining services should apply
for community foundation trust
status was agreed. The Moving Forward project was
set up to establish the ALTO and
produce the Business Case
Our Journey began in 2006, when Peterborough PCT was established and brought together all the provider services
into a single directorate. The provider arm started to look at its future options should in be separated from the PCT
and commissioned a feasibility study of all potential models and in 2007, the PCT and provider arm set up the Next
Steps project.
27
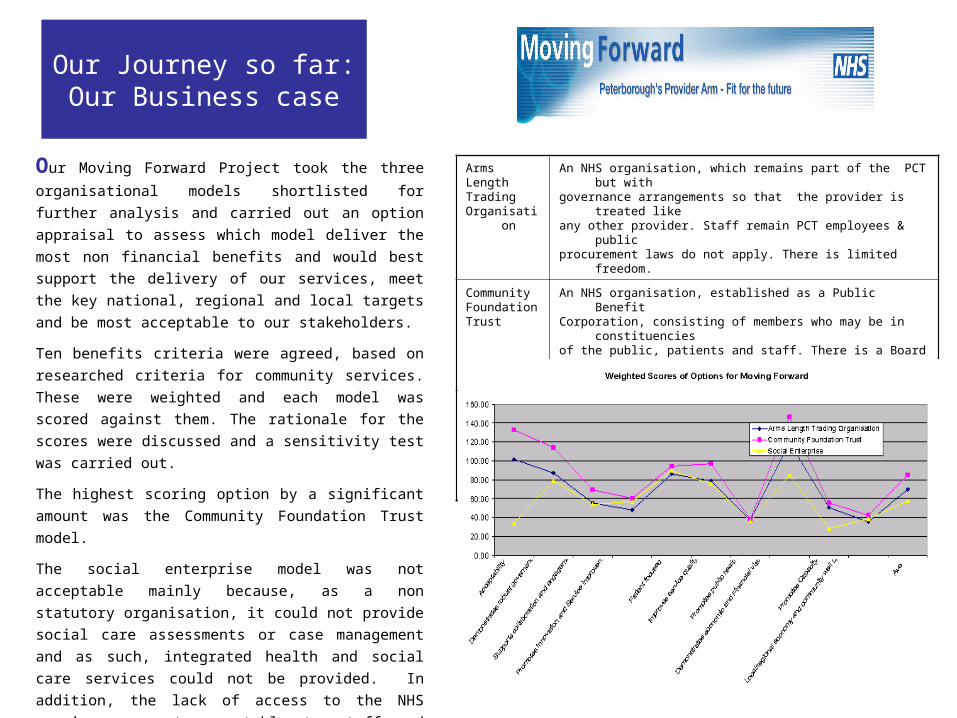
Our Journey so far:Our Business case
Arms Length TradingOrganisatio
n
An NHS organisation, which remains part of the PCT but with governance arrangements so that the provider is treated
like any other provider. Staff remain PCT employees & public procurement laws do not apply. There is limited freedom.
Community Foundation Trust
An NHS organisation, established as a Public Benefit Corporation, consisting of members who may be in
constituencies of the public, patients and staff. There is a Board of
Governors and a Board of Directors.
Social Enterprise
A business which has defined social or environmental objectives. A
Community Interest Company limited by guarantee or shares,
designed for SEs that want to use profits and assets for the public
good
Our Moving Forward Project took the three
organisational models shortlisted for further
analysis and carried out an option appraisal to
assess which model deliver the most non financial
benefits and would best support the delivery of our
services, meet the key national, regional and local
targets and be most acceptable to our stakeholders.
Ten benefits criteria were agreed, based on
researched criteria for community services. These
were weighted and each model was scored against
them. The rationale for the scores were discussed
and a sensitivity test was carried out.
The highest scoring option by a significant amount
was the Community Foundation Trust model.
The social enterprise model was not acceptable
mainly because, as a non statutory organisation, it
could not provide social care assessments or case
management and as such, integrated health and
social care services could not be provided. In
addition, the lack of access to the NHS pension was
not acceptable to staff and could have limited the
organisation’s ability to recruit staff.
Separate financial, economic and commercial cases
also ranked the CFT model as highest. Due diligence
was carried out by KPMG and supported the
findings.
28
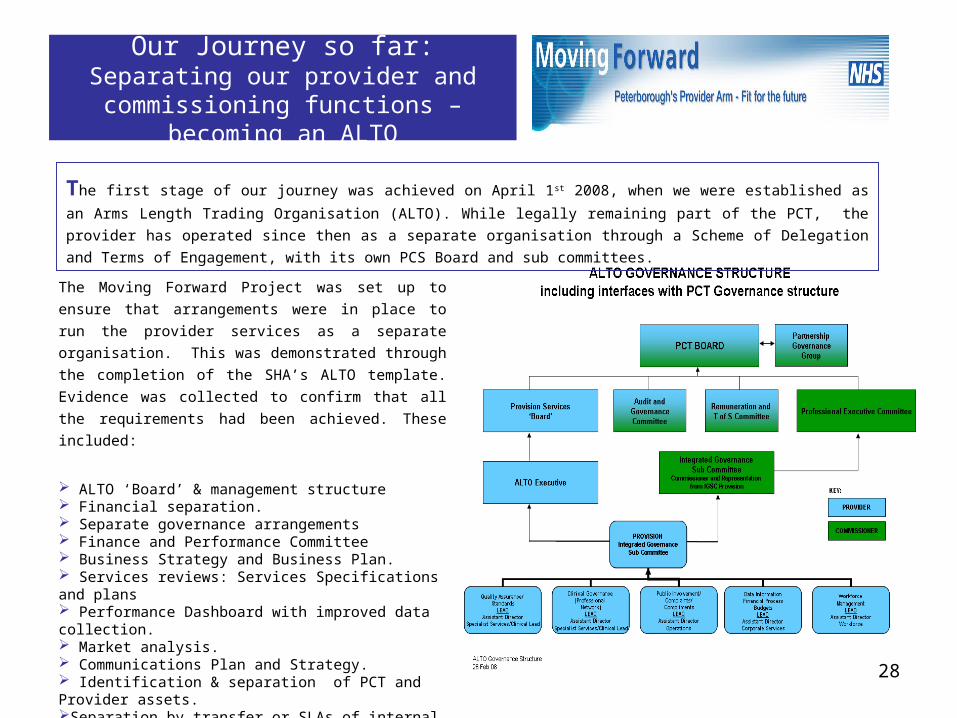
Our Journey so far: Separating our provider and commissioning
functions – becoming an ALTO
The Moving Forward Project was set up to ensure that
arrangements were in place to run the provider services as
a separate organisation. This was demonstrated through
the completion of the SHA’s ALTO template. Evidence was
collected to confirm that all the requirements had been
achieved. These included:
ALTO ‘Board’ & management structure Financial separation. Separate governance arrangements Finance and Performance Committee Business Strategy and Business Plan. Services reviews: Services Specifications and plans Performance Dashboard with improved data collection. Market analysis. Communications Plan and Strategy. Identification & separation of PCT and Provider assets.Separation by transfer or SLAs of internal support teams Workforce and Organisation Development Plan
The first stage of our journey was achieved on April 1st 2008, when we were established as an Arms Length Trading
Organisation (ALTO). While legally remaining part of the PCT, the provider has operated since then as a separate
organisation through a Scheme of Delegation and Terms of Engagement, with its own PCS Board and sub committees.
29
Our Journey so far: Separating our
provider and commissioning functions – from ALTO TO APO
PCS has a track record for laying good foundations
for future development
During 2008, a number of audits and diagnostics were carried out to confirm our ALTO status. All the audits confirmed that we were working well as an ALTO, had set up the appropriate arrangements and were progressing to APO.
The audits and diagnostics were carried out by:PriceWaterhouseCoopers for the Audit CommissionErnst & Young audit of Finance & Governance The East of England Health Authority diagnosticWe have also carried out self diagnostics using the Department of Health Business Readiness template and have completed 98% of the requirements.
We have produced an action plan which brings all the recommendations from the audits and diagnostics together with other business readiness tools and CFT requirements.
The audits and diagnostics confirmed that we understand the journey we still need to undertake to become a CFT. We have started on that journey but know we have a long way to go.
We have improved our Business infrastructure with: The development of a commercial team including a
contracts and bidding team and an Information
Management teamThe implementation of a bespoke IT system to ensure
we collect robust activity data from all our services while
STPP, the national community system, is being rolled out.Financial recovery plan resulting in 6% efficiency
savingsTactical cost reduction programme identifying over
£400k to improve the 2008/09 financial position.Performance Accelerator has been implemented to
support risk and performance management.Increased and strengthened our Finance TeamAgreed to increase the establishment of our
communications team
We commissioned Deloittes to carry out a detailed
market analysis
We have established our Transformation Programme:
‘Building a Sustainable Future’ and through it carried out
a number of reviews to inform future service
development
Since becoming an ALTO, we have continued to review, improve and develop our services and infrastructure in preparation for becoming and Autonomous Provider Organisation (APO).

30
Our Journey so far: Separating our provider and commissioning functions
‘’Really understanding our services will enable us to maximise our
Patient focus’
PROGRESS TOWARDS APPLYING TO BECOME A COMMUNITY FOUNDATION TRUST
Directory of Services Access Database
Example of Time to Care findings
Transforming Community Services – Building a Sustainable Future
Our transformation programme has progressed in a number of stages.
We have started by carrying out a number of service reviews, which
together with the market analysis, will inform the transformation work that
is required to before we can apply to become a CFT.
Ernst & Young have supported the following projects: A Core Business Review covering all the services provided by PCS.
The review included the production of a Directory of Services and
identified over 150 service redesign opportunities and areas for cost
reduction. The Time to Care tool was used to analyse the working practices of the
nursing profession across PCS and will be used to improve workforce
productivity and identify opportunities for improvement and efficiency. For
example, the time spent on administration and travel varies widely
between teams. We will identify best practice and extend to all teams.A Priority Based Service Review has been carried out of all Home Care
Services, covering Hospital at Home, Intermediate Care and Home Care.
Alternative service models have been developed and assessed using
quality scores. Tactical Cost reduction programme identified over £400k to improve
the financial position of 2008/2009.
We had commissioned two external reviews on our health visiting and
district nursing services. The findings and recommendations have been
included in the Priority based service reviews described in our service
development plans

31
OUR INTEGRATED BUSINESS PLAN: Executive Summary
‘Our Integrated Business Plan will deliver our vision and our
Business and Care Strategies’
Our Integrated Business Plan (IBP) will be our main submission in our application to be a Community Foundation Trust. The
IBP in this section of our Transition Plan is the first, high level draft of our IBP. Over the next few months, we will continue to
populate the plan in more detail with information we have already collected and further information as it is agreed. We will
engage and consult with our staff and other key stakeholders in the production of the plan. We anticipate that over the next two
years, our plan will be redrafted many times to reflect our progress towards our long term destination, using all the feedback
from our service development plans, business units and updated market analysis.
As our IBP evolves, this chapter will provide a high-level overview of PCS, our vision, our performance, the market in which we operate, why we wish to become a CFT and the benefits it will bring to our local community.
Our vision isto provide competitive, integrated health and social care services
Which contribute to individual
well-being.
Excellent Services
Improved Customer Satisfaction
Safe effective and
efficient
Modern sustaina
ble business
STRENGTHS WEAKNESSES
OPPORTUNITIES THREATS
•Integrated health and social care provision•Strong clinical skill base•Gold Star services•Strong partnerships•Good reputation •Dedicated and committed workforce• Diverse group of services
•Disparate IT systems
•Poor perceived reputation with some GPs
•Poor access to quality management information•Limited commercial experience/expertise
•Separate silos and associated behaviour
•Repatriate out of area placements
•Build on successes i.e. grow dental access centre
•Develop service to provide 24 hour support
•Develop services to accept self referrals into prevention and enablement care group
•Large number of independent and voluntary sector players
•Other NHS providers
•Difficult recruitment market
•Individual budgets
•Economic climate

32
OUR INTEGRATED BUSINESS PLAN: Profile ‘We are a strong, vibrant, viable provider of community services’
Peterborough Community Services is the Arms Length Trading Organisation of NHS Peterborough. We provide integrated
community health and adult social care services across Peterborough. We also provide specialist community health services to
parts of Cambridgeshire, Lincolnshire and Northamptonshire. Adult social care services are provided through a Section 75
Partnership Agreement between NHS Peterborough and Peterborough City Council. As a provider of integrated services, we are in
a unique position to develop and support individualised self directed health and social care.
Our population base is around 250,000 people of which about
163,000 people live in the Peterborough City Council boundary. We employ around 1400 staff (1036 w.t.e)We provide approximately fifty different, high quality services.Services are delivered in a wide range of settings including
community clinics and health centres, GP practices, people’s
homes, schools and nurseries as well as into the Peterborough
and Stamford hospitals. Our annual turnover is in the region of £82million A significant number of our services have received national
and regional recognition.We have mapped all our services to produce a service
directory including a description of the service, where it is
provided and who it is provided by, for use of our
commissioners, referrers and ourselves
Functional Department
Service Description
Service Name SettingLocality
Staff Involved
NHS East of England PledgesDarzi
Pathway LAA Social Indicators
The geographic area currently receiving PCS services
33
OUR INTEGRATED BUSINESS PLAN: Strategy
‘Our vision will inform ourStrategic direction’
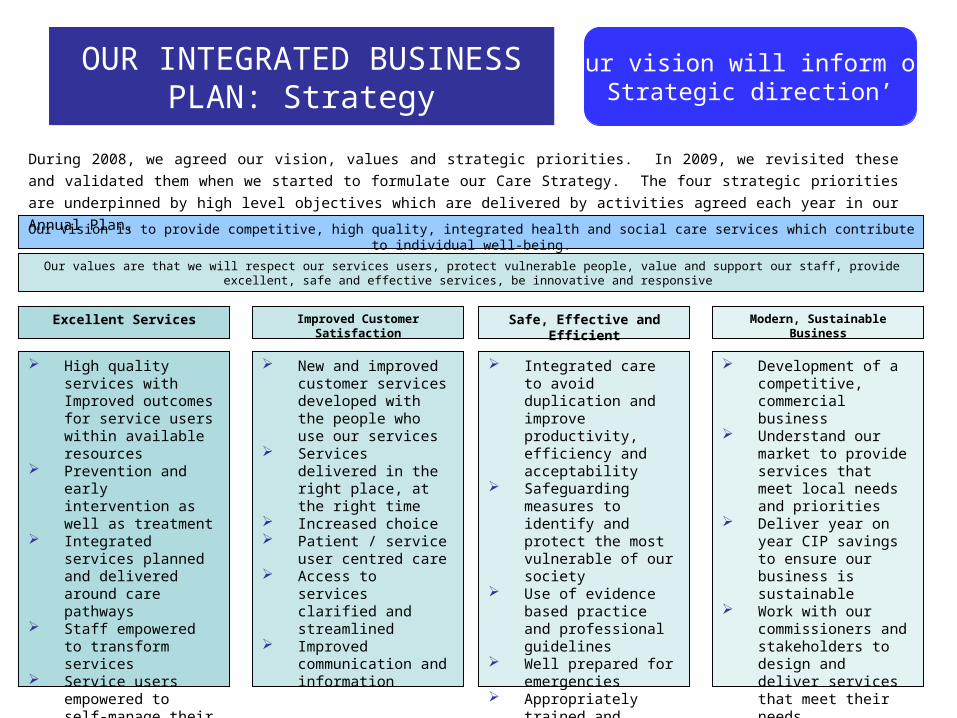
Our Vision is to provide competitive, high quality, integrated health and social care services which contribute to individual well-being.
Our values are that we will respect our services users, protect vulnerable people, value and support our staff, provide excellent, safe and effective services, be innovative and responsive
Excellent Services
During 2008, we agreed our vision, values and strategic priorities. In 2009, we revisited these and validated them when we started to
formulate our Care Strategy. The four strategic priorities are underpinned by high level objectives which are delivered by activities
agreed each year in our Annual Plan.
Improved Customer Satisfaction Safe, Effective and Efficient Modern, Sustainable Business
High quality services with Improved outcomes for service users within available resources
Prevention and early intervention as well as treatment
Integrated services planned and delivered around care pathways
Staff empowered to transform services
Service users empowered to self-manage their own care
New and improved customer services developed with the people who use our services
Services delivered in the right place, at the right time
Increased choice Patient / service user
centred care Access to services
clarified and streamlined
Improved communication and information
Integrated care to avoid duplication and improve productivity, efficiency and acceptability
Safeguarding measures to identify and protect the most vulnerable of our society
Use of evidence based practice and professional guidelines
Well prepared for emergencies
Appropriately trained and supported workforce
Development of a competitive, commercial business
Understand our market to provide services that meet local needs and priorities
Deliver year on year CIP savings to ensure our business is sustainable
Work with our commissioners and stakeholders to design and deliver services that meet their needs
34
OUR INTEGRATED BUSINESS PLAN: Strategy
‘Through careful planning and a systematic, supportive approach
we will change our culture, develop and empower our staff and restructure our
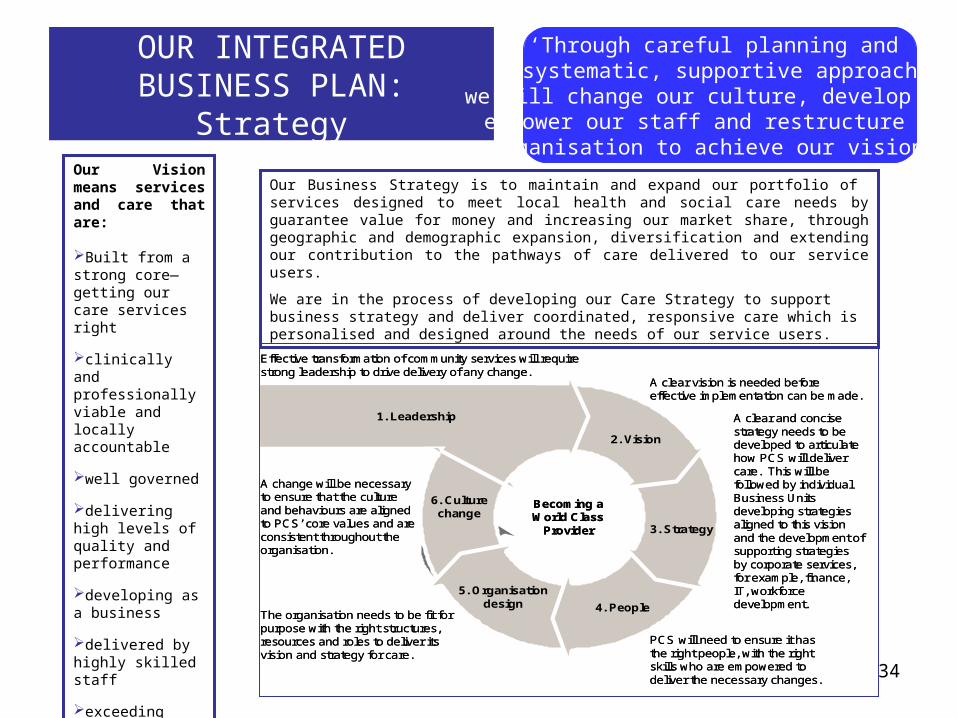
organisation to achieve our vision’ Our Vision means services and care that are:
Built from a strong core—getting our care services right
clinically and professionally viable and locally accountable
well governed
delivering high levels of quality and performance
developing as a business
delivered by highly skilled staff
exceeding customer expectations
financially viable
1. Leadership
2. Vision
3. Strategy
4. People
5. Organisationdesign
6. Culturechange
Becoming a World Class
Provider
Effective transformation of community services will require strong leadership to drive delivery of any change.
A change will be necessary to ensure that the cultureand behaviours are aligned to PCS’ core values and are consistent throughout the organisation.
The organisation needs to be fit for purpose with the right structures, resources and roles to deliver its vision and strategy for care.
PCS will need to ensure it has the right people, with the right skills who are empowered to deliver the necessary changes.
A clear and concise strategy needs to be developed to articulate how PCS will deliver care. This will be followed by individual Business Units developing strategies aligned to this vision and the development of supporting strategies by corporate services, for example, finance, IT, workforce development.
A clear vision is needed before effective implementation can be made.
1. Leadership
2. Vision
3. Strategy
4. People
5. Organisationdesign
6. Culturechange
Becoming a World Class
Provider
Effective transformation of community services will require strong leadership to drive delivery of any change.
A change will be necessary to ensure that the cultureand behaviours are aligned to PCS’ core values and are consistent throughout the organisation.
The organisation needs to be fit for purpose with the right structures, resources and roles to deliver its vision and strategy for care.
PCS will need to ensure it has the right people, with the right skills who are empowered to deliver the necessary changes.
A clear and concise strategy needs to be developed to articulate how PCS will deliver care. This will be followed by individual Business Units developing strategies aligned to this vision and the development of supporting strategies by corporate services, for example, finance, IT, workforce development.
A clear vision is needed before effective implementation can be made.
Our Business Strategy is to maintain and expand our portfolio of services designed to meet local health and social care needs by guarantee value for money and increasing our market share, through geographic and demographic expansion, diversification and extending our contribution to the pathways of care delivered to our service users.
We are in the process of developing our Care Strategy to support business strategy and deliver coordinated, responsive care which is personalised and designed around the needs of our service users.

35
OUR INTEGRATED BUSINESS PLAN: Strategy
‘Only the CFT model will support us fully in our aspiration to be a
world class provider of community services
The Rationale for Community Foundation Status
We believe that the Community Foundation Model is the best organisational form for PCS because as a CFT we would :
Be able to continue to provide integrated adult health and social care services Statutory Social Care assessment and
care
management functions can only be delegated to a statutory organisation. Through a governance framework which is robust and demonstrates clear public involvement, be able,, to fully
engage with
and involve our local community and membership in the development and delivery of services. Have a solid framework from which to maintain and enhance a balanced portfolio of the highest quality and most cost
effective health and social care community services. Have freedoms to access capital on the basis of affordability instead of the current system of centrally controlled allocations Have freedom to invest surpluses in developing new services for local people Have freedom of local flexibility to tailor new governance arrangements to the individual circumstances of their community Retain the NHS identity and brand, which is trusted by staff and the people who use our services. Have continued access to the NHS pension for both existing and new staff Be in a better position to respond to market forces than other organisational forms
In addition, an independent review carried out by the Healthcare Commission has shown that NHS Foundation Trusts are
making good progress in developing new innovative approaches to providing better quality healthcare services for the benefit of
NHS patients, and improving accountability to their local populations. While there are currently no CFT to review, our
experience so far, of preparing to be a CFT, leads us to believe that the freedoms available as a CFT combined
with the rigorous requirements of Monitor, will encourage and enable us to become a world class provider of
community services.

36
OUR INTEGRATED BUSINESS PLAN: Market Assessment
‘
We are operating in an increasingly competitive market. Understanding our market will help
us to ensure that we are the preferred provider of community services
In 2008, we commissioned Deloittes to carry out an independent
analysis of the local health care market. The purpose of the analysis
was to assist us in understanding our local health economy, increase
our knowledge of our competitors and the threats they may pose, to
understand our position in the market and our opportunity to increase
our current market share and future market growth. We used eight care
groups selected to capture the key services areas of PCS and to
broadly follow the Transforming Community Services framework. The
care groups we used were:
Integrated Health and Social Care; Treatment and Procedures Out of Hospital; Unplanned Care; Children’s
Services; Long Term Conditions; Prevention and Enablement; Learning Disabilities and End of Life Care.
The outcome of the analysis has helped us to develop our strategy for
service delivery and business development over the next 5 years. It
has helped us to identify the main risks to our future and the service
development plans we need to put in place to ensure that we are
preferred provider of community health and social care services.
Key issues from our market assessment are summarised in this draft of
our IBP and will be covered in more detail in the next draft. We intend to
repeat the analysis on a regular basis to ensure that our information
remains up-to-date and that we adjust our plans accordingly.
Our Local Health Economy
Our Local Health Economy (LHE) consists of all the
organisations who commission or provide health and
social care services across East Anglia. This includes
organisations which form part of NHS East of England,
the local authority, voluntary and private sector. PCS
covers Peterborough, parts of Cambridgeshire,
Northamptonshire and Lincolnshire.
The city of Peterborough is a heavily urban area but the
surrounding areas are largely rural with some suburban
areas.
There are four PCTs which border the PCS area, these
are Cambridgeshire PCT, Lincolnshire TPCT,
Leicestershire County and Rutland PCT and
Northamptonshire TPCT. All these PCTs except
Cambridgeshire PCT sit in the East Midlands SHA.
Peterborough PCT, Peterborough & Stamford
Hospitals NHS Foundation
Trust, Cambridgeshire PCT,
Cambridgeshire & Peterborough
NHS Foundation Trust .
can be considered key
parts of the Local Health
and Social Care Economy.
37
OUR INTEGRATED BUSINESS PLAN
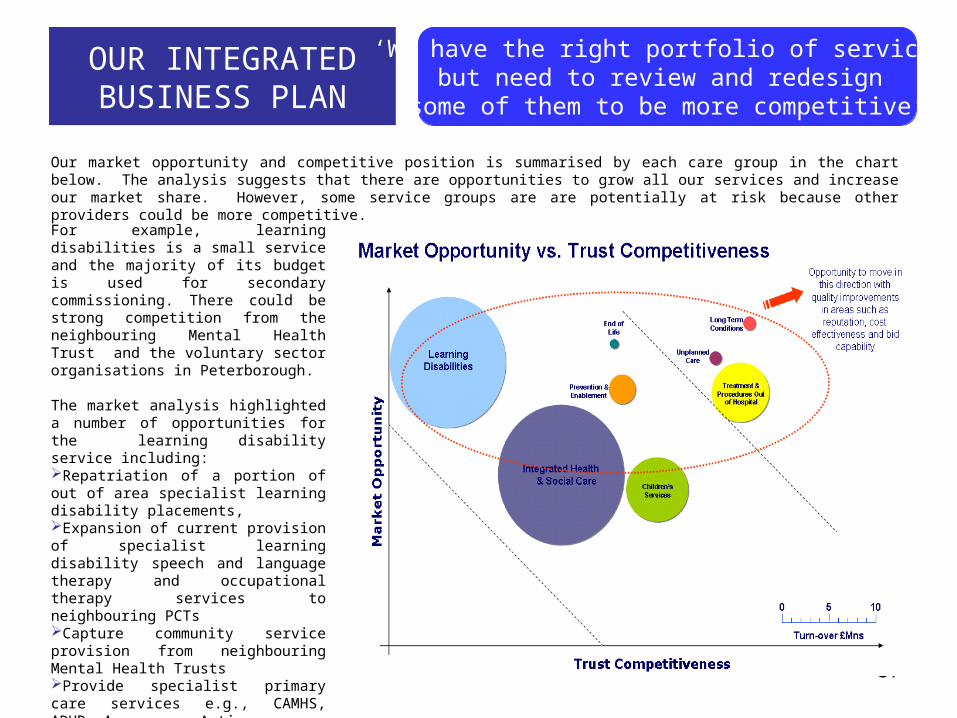
‘We have the right portfolio of services but need to review and redesign
some of them to be more competitive’
Our market opportunity and competitive position is summarised by each care group in the chart below. The analysis suggests that there are opportunities to grow all our services and increase our market share. However, some service groups are are potentially at risk because other providers could be more competitive.
For example, learning disabilities is a small service and the majority of its budget is used for secondary commissioning. There could be strong competition from the neighbouring Mental Health Trust and the voluntary sector organisations in Peterborough.
The market analysis highlighted a number of opportunities for the learning disability service including: Repatriation of a portion of out of area specialist learning disability placements,Expansion of current provision of specialist learning disability speech and language therapy and occupational therapy services to neighbouring PCTsCapture community service provision from neighbouring Mental Health TrustsProvide specialist primary care services e.g., CAMHS, ADHD, Aspergers, Autism Provide day services.
NHS P and PCS have prioritised learning disability services and are carrying out a priority based service review.
38
OUR INTEGRATED BUSINESS PLAN: Market Assessment
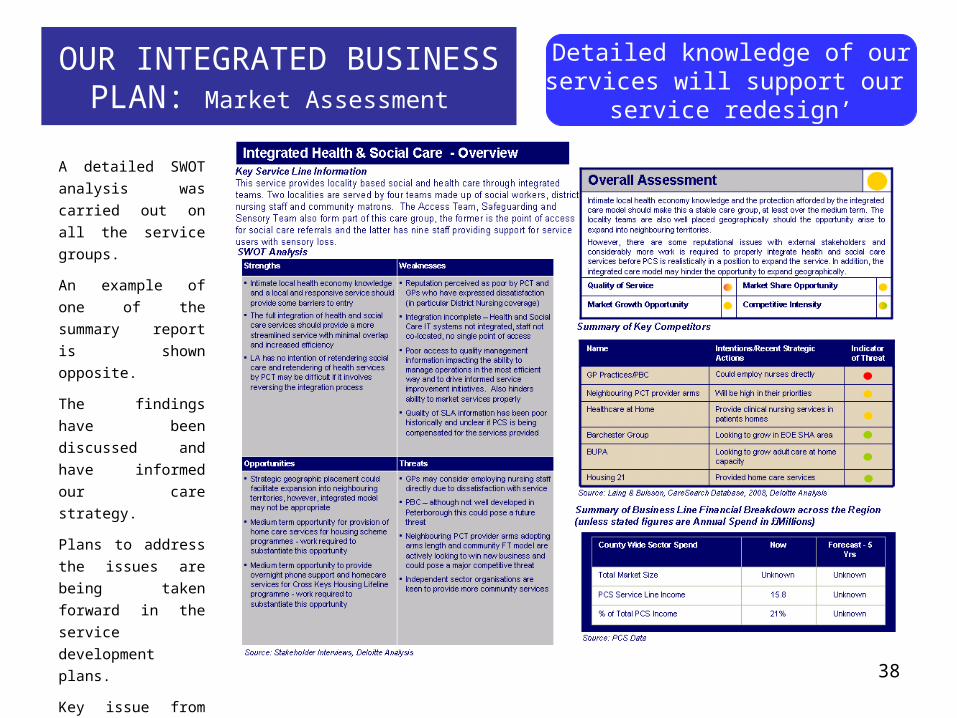
‘Detailed knowledge of our services will support our
service redesign’
A detailed SWOT
analysis was carried
out on all the service
groups.
An example of one of
the summary report is
shown opposite.
The findings have
been discussed and
have informed our
care strategy.
Plans to address the
issues are being taken
forward in the service
development plans.
Key issue from the
SWOTs include
demographic changes
and the drive to move
services out of
hospital.

39
OUR INTEGRATED BUSINESS PLAN: Market Analysis
A PEST analysis was also carried out and provides a summary of the external environment in which we operate and confirms if future initiatives and service development plans are in line with issues, trends and developments at both the local and national level
40
OUR INTEGRATED BUSINESS PLAN Service Development Plans
Our service development plans are designed to transform our services so that they deliver our vision, strategic priorities and Business and Care Strategies. They are designed to respond to our commissioners requirements identified through Practice Based Commissioning and NHSP’s Strategic Plan. They are also designed to maximise our strengths, reduce our weaknesses and respond to our opportunities and threats.
Our transformation programme includes a number of projects which will have a significant impact on our future success. Four of these service development projects are described below. As these are successfully completed and embedded across the organisation, others will be introduced.
Case management and Care Planning
The majority of our resources are currently focused on providing care to a small group of people with complex
health and social needs. We need to ensure that our services are designed around their needs and wants.
We will achieve this by: Risk stratification and management: understanding the different groups within our population and how our
response and input into these different groups needs to vary.Case management and care planning: we see case management as the thread that will run through the
services we provide. Providing our users with individualised, live care plans will become the tenet of how we
deliver services.Supporting independent living: empowering individuals to take control of their care and conditions through
education, support and other mechanisms such as telehealth.
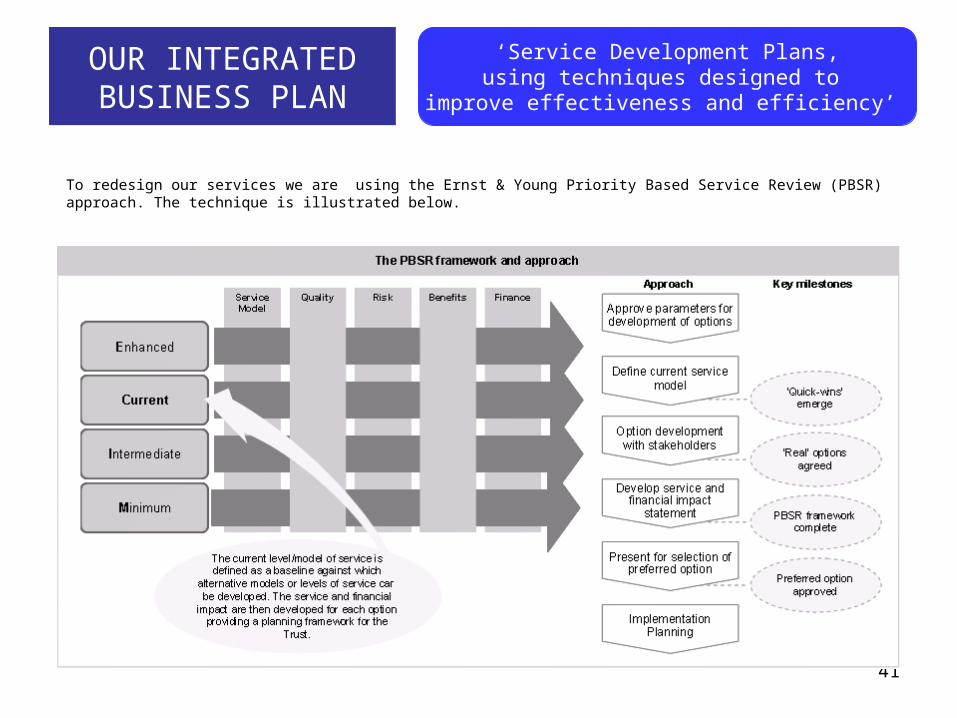
41
OUR INTEGRATED BUSINESS PLAN
‘Service Development Plans,using techniques designed to
improve effectiveness and efficiency’
To redesign our services we are using the Ernst & Young Priority Based Service Review (PBSR) approach. The technique is illustrated below.
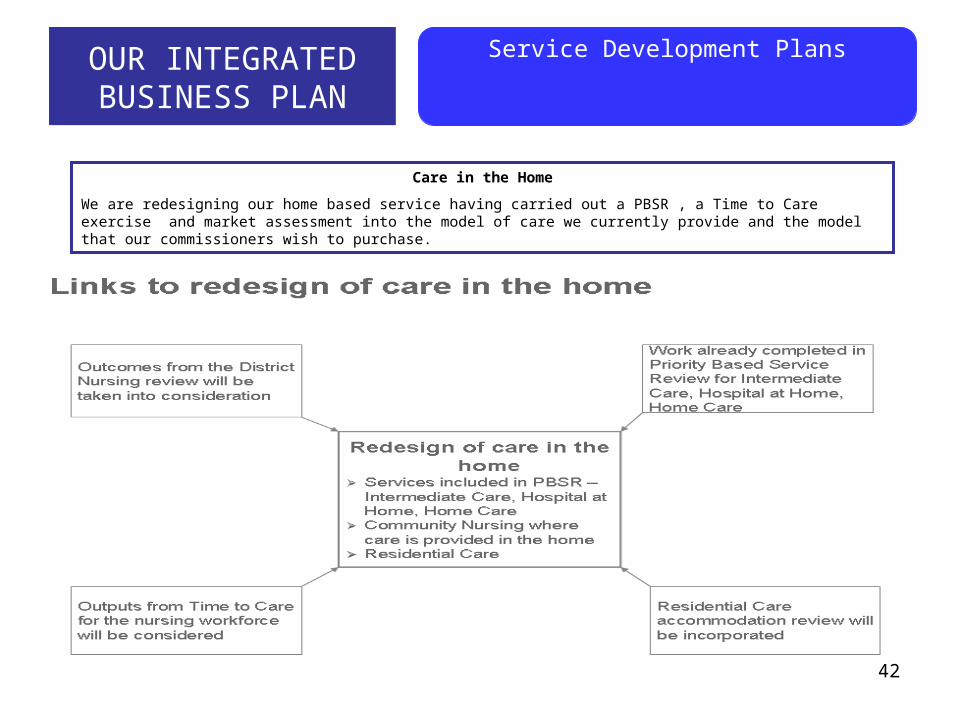
42
OUR INTEGRATED BUSINESS PLAN
Service Development Plans
Care in the Home
We are redesigning our home based service having carried out a PBSR , a Time to Care exercise and market assessment into the model of care we currently provide and the model that our commissioners wish to purchase.
43
OUR INTEGRATED BUSINESS PLAN
Service Development Plans
Priority Based Services Review of Learning Disability Services
PCS and NHS Peterborough are reviewing Learning Disability Services using PBSR to ensure more personalised services
which deliver more choice and control including individual budgets, while focusing attention on current service provision and
future requirements to ensure that our Learning Disability services are professionally and financially viable for patients and
services users in the future.
Nationally there is pressure within Learning Disability Services for a number of different reasons including a significant
increase in the number of people, with learning disabilities, surviving into adulthood with major disabilities and complex needs,
adults with learning disabilities are living longer and surviving into older age, limited capacity of family carers to care for the
extent and diversity of needs and significant increases in costs of specialised services for people with high dependency,
complex needs and challenging behaviours.
Early intervention Services For Children
We are reviewing our current model of care for our universal children’s services (school nursing and health visiting) to redesign a service which will stream line care and remove duplication.
Our project will build on the health visiting review and Time to Care information and involve detailed process mapping and significant redesign of service delivery.
44
OUR INTEGRATED BUSINESS PLAN: Financial Plan - Overview
This summary plan has been developed using the MONITOR 5 year EBITDA
pro formas and has been completed as best as we can at this time.
Financial Planning and reporting will continue to be developed and refined as
supporting systems (e.g. performance management) and skill sets are
developed and a full IBP is produced.
The Summary plan shows the following:
The actual position for 2008/2009 (subject to audit). Although shown as a rounded break even in the summary, there was actually a small under spend of £36k with a £2k closing cash balance.
The original plan for 2009/2010 as approved by the PCS Board. Details of the movements between 2008/2009 and 2009/2010 and assumptions are given below.
Projection for 2010/2011 based upon an net uplift of 1.5% and estimated cost increases for infrastructure costs.
Projection for 2011/2012 based upon a net uplift of 1% and including an increased efficiency requirement to address anticipated reductions in health spending increases and full year impacts of infrastructure costs.
The plan does not include service developments/changes that may occur in
future years nor funding streams that may be associated with them. We
accept that there will be changes and are planning on the basis of no overall
change to income levels though sources may change. Excess costs will be
shed as appropriate.
We are currently engaged, with Ernst & Young and staff in service reviews
leading to changes in how services are delivered in order to ensure we provide
cost effective services, competitive quality value for money services.
Earnings before Interest, Depreciation, Tax and Amortisation is a measure used to highlight surpluses generated by business actives and is a measure of viability and success. Whilst PCS needs to plan to generate a surplus each year for investment in its services the reality is that whilst we are fundedunder block contracts the surplus is dependant upon entirely newbusiness from non NHS sources or achieving efficiencies and relies upon Commissioner agreement to retain such savings as opposed to reinvesting in additional services activity at no cost to the Commissioner. In the light of current efficiency savings we have not set a surplus target.The measure, as currently used by MONITOR uses expenditure categories that are not currently relevant to ALTO. The first is Depreciation which presumes a fixed asset base. initial agreement was reached with NHS Peterborough over which assets would transfer to PCS. Following the Transforming Community Services guidance this isto be reviewed before any physical transfer takes place. For most, if not all, of the premises PCS operates in they will be owned by either NHS Peterborough or the City Council with PCSas effective tenants.NHS Peterborough will also own the IT networks and recordssystem that PCS would use. PCS may own some small pieces of equipment .As an ALTO within a PCT, PCS remains bound by various rules and regulations that apply to PCTs. For example we cannot invest surplus funds to generate interest and we are not subject to taxation on "profits/losses". Similarly we do not pay a PDC dividend.As we don't own the assets we can't profit from sales.The result of this is that the EBITDA as defined by MONITOR only really revolves around generating a surplus or a deficit andthe model would therefore generate a low score. The SHA has been considering this.
EBITDA

45
OUR INTEGRATED BUSINESS PLAN
Financial Plan:Overview
In 2009/2010 our main commissioner is funding a level of recurrent
and non recurrent costs associated with our move to APO status and
discussions are ongoing regarding longer term funding. This plan
assumes a need to achieve an additional level of efficiency to order to
cover recurrent costs. We have already achieved some efficiency
which are funding part of the infrastructure changes.
Peterborough City Council and NHS Peterborough are seeking to
action a number of savings initiatives, which it has already ‘top sliced
from the contract with us’. There is acceptance by the Commissioner
that achievement of the savings requires a commonly agreed
implementation plan which is currently being developed in conjunction
with them. This is over and above the baseline efficiency requirements
and represents a significant risk to PCS achieving financial balance in
2009/2010. In partial recognition of this, NHS Peterborough has
deferred part of the saving requirement to 2010/2011 if it is not
achieved.
The plan recognises the current economic climate and that there will be
a requirement for more cost effective services and future projection
rates reflect this.
NHS Peterborough is currently publishing its strategic plan and we will
work with them, and other commissioners, to develop responsive
services for the future. The projections therefore do not include overall
future growth at this time.
There are two underlying issues to be resolved in 2009/2010 that are currently shown as an efficiency requirement.
Full year effect of 2008/2009 client placementsLearning Disability Services where a full service review is underway led by NHS Peterborough
Pending final agreement with NHS Peterborough, the plan does not include a PCS share of the PCT's central corporate costs. These are currently estimated at £2.8m and include such things as accommodation costs, and support services. PCS currently receives the vast majority of its income under block contract arrangements. Work to develop currencies, costs and prices will be developed with NHS Peterborough during 2009/2010 and as the performance management infrastructure comes on line.

46
OUR INTEGRATED BUSINESS PLAN: Financial Plan - Summary

47
Our Integrated Business Plan: Financial Plan
48
Our Integrated Business Plan: Financial Plan
Service Line Management and ReportingOur services are currently managed in three directorates in professional groups or specialist services. The services are supported by corporate services managed in three specialist directorates. Care delivery is structured around the professional groups rather than our service users which often results in duplication and multiple touch points for service users, particularly those with complex needs. There can be lack of coordination and clarity for service users and for PCS, inefficiency in ways of working.
We have agreed that to improve service integration and customer experience, we need to redesign the way our services are structured around care groups and care pathways. The most appropriate model for us appears to be Service Line Management (SLM), supported by Service Line Reporting.
SLM is a robust approach that combines trusted management techniques and effective business planning in an NHS setting. By identifying specialist areas and managing them as distinct operational units, it enables NHS Foundation Trusts to understand their performance and organise their services in a way which benefits patients and delivers efficiencies for the Trust. It also provides a structure within which clinicians can take the lead on service development, resulting in better patient care.
A project plan has been agreed that will see the development of SLM across PCS over the next year or so. This will help business management and assist in our preparation for Community Foundation Trust status. Children’s Service has been agreed as a Pathfinder to develop SLM. It will be one of a few key Strategic Business Units in PCS and its preparation for SLM will be managed and monitored during 2009 to assist in rolling out SLM to the other business units. This will change the we manage our services by professional service groups to managing them by service pathway / service lines. We will improve our costing, information and management and clinical leadership of these service and as a result, will develop more patient focused efficient and effective services that respond better to our customer needs.
49
OUR INTEGRATED BUSINESS PLAN
Risks
In 2008, PCS produced its own Board Assurance Framework (BAF). The BAF reports against the four PCS key priorities and the objectives. We have recently purchased Performance Accelerator as the software tool to support risk management across PCS. This is currently being populated with the BAF risks, the key performance Indicators and national and local targets. It will also be used to monitor the risks associated with the transition and transformation programmes and the Annual and Integrated Business Plans.
We have identified five key risks for transition and plans for mitigating these risks. These and other risks are include in the programme’s risk log and will be managed by the Directors responsible for each workstreams area. A detailed risk and mitigation plan is included in our 2009/2010 Annual and Financial Plans.
Risk Mitigation
Affordability: Failure to achieve financial balance through
loss of income or inability to achieve Planned savings in
the current economic climate.
We will plan for better and worse financial positions as well as
status quo,
Skills and capacity: ensuring we have sufficient skills
and capacity to transform our culture and our services.
We have established a Capacity for Change programme
Stakeholder engagement: Stakeholders may not be
interested in or willing to engage in discussions on
service changes and may loose interest if the Transition
takes too long.
We are developing a comprehensive Stakeholder engagement
and communication plan covering both internal and external
stakeholders.
Demographic Growth: The population of Peterborough is
predicted to grow to over 200,000 people by 2021, an
increase of over 20% on the 2006 figure.
We are working closely with all our commissioners to plan for
this increase in population
50
OUR INTEGRATED BUSINESS PLAN: Risks
It is crucial to effectively manage the transition period activities and maintain the continuity of our core business activities. The service business continuity
plans will ensure that essential services are maintained whatever the disruption and other services are restored according to their assessed priority
Business Continuity
Business Continuity is a major risk during transition. Business Continuity Management (BCM) is a statutory requirement for both
NHS Peterborough and Peterborough Community Services. The Civil Contingencies Act 2004 and the NHS Emergency Planning
Guidance 2005 require both organisations to have a Business Continuity Management Policy (BCMP) with robust procedures
and plans in place to ensure that, in the event of a significant service interruption, critical day-to-day functions can be maintained.
Timely recovery and restoration of key services, systems and processes must also be achieved.
The Business Continuity Management Policy and Procedure for both NHS P and PCS has been drafted and is being circulated
for discussion. The organisations’ approach to determining its Business Continuity Management arrangements is to: Implement appropriate measures to reduce the likelihood and impact from identified risks Provide continuity for key or critical activities during and following an incident Review Recovery Time Objective following a period of disruption Understand the costs of implementing strategy and plans Understand the costs and consequences of inaction
PCS is updating the business continuity plans for all its services using Shadow planner software. Services are carrying out
business impact analyses to identify and prioritise critical services which have to be maintained, the likelihood of disruption to the
services and the impact, the point at which the situation becomes critical, the time in which they have to be restored and the
basic resources needed to maintain and restore the services.
Business continuity is about safeguarding critical work. If an incident occurs it is important to know which critical work priorities
need to be urgently continued, and the likely impact if they are affected the order of priority to restore all services to normality.
The transition programme is not a critical service which needs to be maintained. However, there are risks associated with the
transition which could impact on services and in extreme cases, could disrupt services. These risks have been identified in the
section on risk and will be included in the risk register and inform business continuity planning.
51
OUR INTEGRATED BUSINESS PLAN
Leadership and Workforce
To become a world class provider, change the way services are delivered and managed and achieve CFT status, we need to
ensure that new way of working are embedded through strategic organisational design, change management and culture
change. Staff need to be equipped with the appropriate skills and support to perform well in the new environment. The change
needs to be led from top-down. Training and development needs to be provided to the whole organisation.
Our training and development will be co-ordinated through a comprehensive organisational development programme, led by
the PCS workforce development team with support from Ernst Young and other external consultants.
The skills which need to be developed are being identified through the Service Line Management project, other projects, Board
assessments, the diagnostics and services and staff reviews.
For example, our Leadership Development Programme will include:One to one leadership development coachingBoard development workshopsChange management competency framework against which existing skills can be assessedLeadership of change survey undertaken with key senior individualsDevelopment sessions to address gaps in change management capabilityBuddy system instigated to create a community of individuals to sustain development and changeChange management toolkit developed to provide ongoing support and training for staff
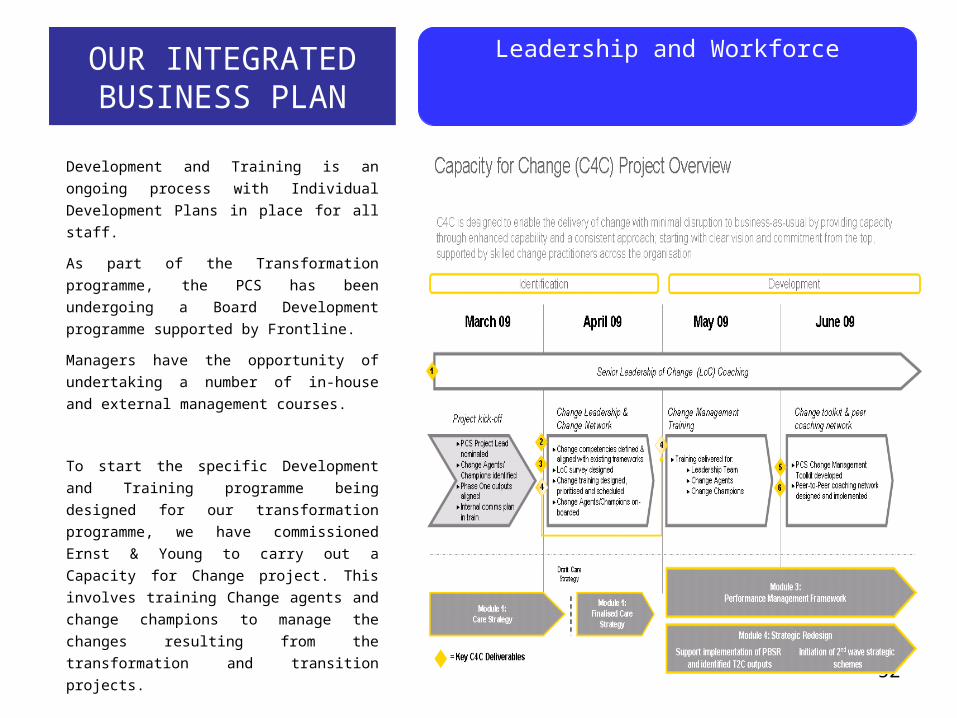
52
OUR INTEGRATED BUSINESS PLAN
Leadership and Workforce
Development and Training is an ongoing
process with Individual Development Plans in
place for all staff.
As part of the Transformation programme, the
PCS has been undergoing a Board
Development programme supported by
Frontline.
Managers have the opportunity of undertaking a
number of in-house and external management
courses.
To start the specific Development and Training
programme being designed for our
transformation programme, we have
commissioned Ernst & Young to carry out a
Capacity for Change project. This involves
training Change agents and change champions
to manage the changes resulting from the
transformation and transition projects.

53
OUR INTEGRATED BUSINESS PLANGovernance
Governance for the CFT
We are building on the governance arrangement we put
in place as an ALTO and developing them in line with
Monitor's requirements for foundation trusts.
This will include: A Governance Strategy and framework
A membership Strategy The establishment of a membership and Board
of Directors Appointment of a Board of Directors through the
Appointments Commission. The PCT has agreed the appointment of a Chair
and up to five Consultant Advisors to the Board, to
act as lay members on the PCS Board. Formal
appointments as Non Executive Directors will be
made when we are established as a CFThe Executive team is being restructured and a
proposal to create five Directors posts will go to
the PCS Board and internal consultation shortly.
Appointments to these posts will be made by the
Chair and Managing Director when the Chair has
been appointed. A constitution will be produced in line with the model
constitution for FTs. The subcommittees to the Board will be reviewed to
ensure that they cover all the areas necessary to provide
the Board with assurance that the organisation is well
governed.
Governance for the Transition
We are putting in place comprehensive governance
arrangements for managing the separation process and
the transition from ALTO to APO and on to CFT.
The Governance Framework will help to:Clarify leadership roles and responsibilitiesSupport the decision making process including sign off
arrangementsProvide assurance to the PCS and PCT Boards and
the SHAEnable monitoring of progressEnsure staff and stakeholder engagementEnsure the changes are fully embedded in the
organisationEnsure co-ordination and cohesionMake best use of resources avoiding duplication of timeAlign organisational agendas and prioritiesIdentify and mange riskIdentify and manage benefitsCreate a culture of mutual respect and trust

54
OUR INTEGRATED BUSINESS PLAN
Governance:Stakeholder Engagement and Communication
THE TRANSITION ENGAGEMENT PLAN AND COMMUNICATION STRATEGY
We are committed to engaging with all the staff and other key stakeholders throughout the transition process. To date, a
significant amount of communication, consultation and engagement has been carried out by both the PCT and PCS around the
separation to ALTO status and the decision to apply to become a CFT. In 2007, a Communications and Consultation Workgroup was set up as part of the Next Steps Project. The workgroup carried
out a stakeholder mapping exercise and produced and implemented a Communications and Involvement Strategy. The group
ensured that all key stakeholders were engaged in the debate on the future direction and organisational model for the provider
services through a series of events, workshops, communication material and a formal public consultation. Following the establishment of PCS as an ALTO in April 2007, PCS has established direct links with many of the stakeholders
and an Internal Communication Strategy was agreed. The PCT and PCS are now developing an engagement plan and a communication strategy focused specifically on the
transition to a CFT and the transformation of PCS and the services it provides to support the transition and the Transforming
Community Services agenda. The PCT and PCS, supported by the National Centre for Involvement are reviewing the existing PCT Public and Patient
Involvement (PPI) arrangements and establishing separate arrangements for PCS. Producing a membership Strategy and recruiting the membership for the aspiring CFT is also an essential part of the
engagement plan and Transition arrangements for the aspiring CFT.
Until April 2009, our communication support was provided by the PCT Communication Team. From April 1st
2009, we have our own Communications Manager who will take forward the Internal Engagement and
Communication Plans. The Internal Communication Strategy previously agreed has been updated and will be
reviewed further as part of the Transition and Transformation Programmes.
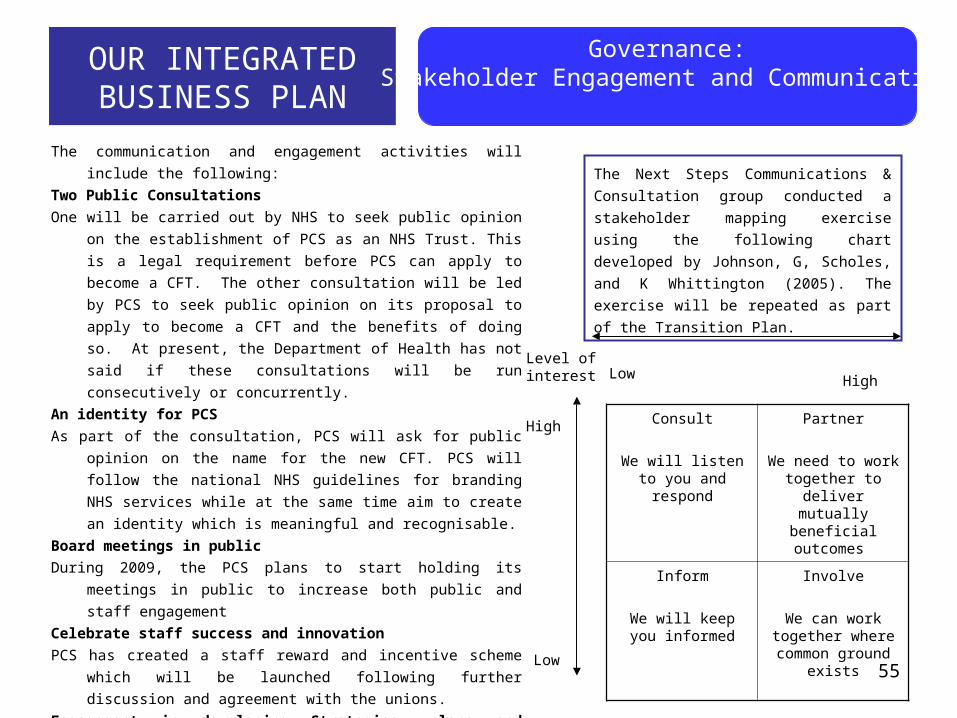
55
The communication and engagement activities will include the following:
Two Public Consultations
One will be carried out by NHS to seek public opinion on the
establishment of PCS as an NHS Trust. This is a legal requirement
before PCS can apply to become a CFT. The other consultation
will be led by PCS to seek public opinion on its proposal to apply to
become a CFT and the benefits of doing so. At present, the
Department of Health has not said if these consultations will be run
consecutively or concurrently.
An identity for PCS
As part of the consultation, PCS will ask for public opinion on the name
for the new CFT. PCS will follow the national NHS guidelines for
branding NHS services while at the same time aim to create an
identity which is meaningful and recognisable.
Board meetings in public
During 2009, the PCS plans to start holding its meetings in public to
increase both public and staff engagement
Celebrate staff success and innovation
PCS has created a staff reward and incentive scheme which will be
launched following further discussion and agreement with the
unions.
Engagement in developing Strategies, plans and services
We wish to engage with our staff and stakeholders on the way we
transform our services
Consult
We will listen to you and respond
Partner
We need to work together to deliver mutually beneficial
outcomes
Inform
We will keep you informed
Involve
We can work together where
common ground exists
Level of interest
High
Low
Low High
OUR INTEGRATED BUSINESS PLAN
Governance:Stakeholder Engagement and Communication
The Next Steps Communications &
Consultation group conducted a stakeholder
mapping exercise using the following chart
developed by Johnson, G, Scholes, and K
Whittington (2005). The exercise will be
repeated as part of the Transition Plan.
56
Our Stakeholder Engagement and Communication Plans are designed to ensure that: key stakeholders, partners, and staff are kept fully up-to-date and have the opportunity to be involved in informing the future
direction of the community health and adult social care services directly provided by Peterborough PCT, Maintain staff morale through regular communications and ensure staff have the opportunity to influence decisions taken
through consultation, as well as undertaking a formal staff consultation. To manage, through engagement, expectations of stakeholders, partners and staff in the relation to future health and social
care services. To reduce the risk of misinformation.
OUR INTEGRATED BUSINESS PLAN
Governance:Stakeholder Engagement and Communication
Formal responsibility for external relationships has previously been with NHS P. During 2008, PCS developed its own
relationship with its commissioners, partners and other key stakeholders, establishing itself as full partner in the local economy.
The Managing Director now has a place on or attends a number of Local Health Economy forums. Regular meetings are held
with commissioners and relationships with other key stakeholders are being developed.
Examples of the evolving external relationships are:
The Managing Director and the Chairman of PCS are full members of the CEO and Chairman meeting for the Peterborough
Health System.
The Managing Director represents PCS on the Children’s Trust Board and the Greater Peterborough Partnership.
The Managing Director attends the Health Overview and Scrutiny Committee on a regular basis.
PCS Chair and Managing Director meet regularly with the Chair and Chief Executive of the PCT.
PCS has actively started to develop relationships with the Practice Based Commissioning Consortium and to meet with the
PEC Chair.
PCS now links directly with the portfolio holder for Adult Social Care.
57
CONCLUSION
PCS has achieved the business readiness requirements for ALTO status and is continuing to transform and develop its
services and infrastructure to achieve the level of business readiness required to become a community foundation trust.
PCS has developed a detailed plan for transforming community services, which prioritises services for improvement and
development which will enhance individual choice, control and personalisation and continue to drive up service quality and
value for money
PCS has carried out a core service review and a market analysis and is working to wards a position when it can
demonstrate contestability and be able to respond proactively to the commissioners’ 5-year Strategic Commissioning Plan.
NHS P and PCS have reviewed the options for most appropriate organisational forms that best suit local need and
circumstances and declared an interest in establishing a Community Foundation Trust to deliver Peterborough Community
Services
NHS P and PCS have moved into a contractual relationship, using the new NHS Community Contract.
PCS has a plan in place supported by formal programme management for moving towards the preferred end state of
becoming a community foundation trust. This plan will be updated following a formal diagnostic by the SHA and on an
ongoing basis to take account of changes in the local and national environment.
NHSP has agreed the principles for the future ownership of the assets used by PCS and will agree with their SHAs a robust
strategy for the future of the community estate.
'NHSP is committed to ensuring that PCS emerges as a strong provider and has our support in its ambition
to become a CFT. PCS is committed to transforming itself to achieve the
high standards required to become a CFT as it believes this is the best organisational form
from which to deliver the community services its community needs and deserves.‘