warwick web view3.plenary session translating the written word into actions ... red blood cells and...
TRANSCRIPT

Warwick Medical School
MB ChB Phase I
Essentials of Clinical Medicine
Essentials of Clinical Medicine Module 1

Essentials of Clinical Medicine
Module Leader
Module Leader Dr Alex Conner – Assistant [email protected] Medical School
Co- Module Lead – Dr David Tweedie - Clinical Tutor for [email protected]
Contact details for all the lecturers in this module are contained at the top of their session pages.
2 Essentials of Clinical Medicine

Introduction
The module Essentials of Clinical Medicine is designed to underpin the MBChB course by providing an introduction to major topics that feature in the integrated curriculum that occur in Phase I, such as, the nervous system and neurobiology, musculoskeletal system, infection and immunity, the respiratory and cardiovascular systems. This module will also introduce generic subjects such as anatomical terminology, medical imaging, histology, metabolism (nutrition), early embryonic development, and pathology. It will also provide the essential basic understanding to support student’s knowledge base as they move through Phase I modules.
Aim
The aims of the module are to enable students to
Provide an understanding of major topics that will feature in the integrated curriculum undertaken in Phase I.
Address the essential components of basic body system ‘ultra’ and ‘gross’
structure in order to be able to evaluate and understand the complexities arising across subsequent modules.
Promote a conceptual and information based understanding of body systems and pathology.
Broaden students knowledge base of basic principles and skills relevant to the core modules in Phase I
Pre-requisites
Before each lecture and group work, students should read the relevant section of the handbook and web pages, download any necessary handouts from the web and examine any appropriate text to support their understanding of the topic(s) to be addressed.
Summary of Intended Learning Outcomes
It should be noted specific detailed learning outcomes will also be addressed within the specific topics. Overall on completion of this module, students should be able to:
Use and understand appropriate basic terminology across body systems (Gastrointestinal tract, cardiovascular system, Nervous System, Respiratory) in the description of both normal and pathological conditions
Describe and understand the fundamentals of normal function of cellular systems and pathogenic consequences
Understand basic medical terminology for use in anatomy, medical imaging, histology and immunity and infection.
Essentials of Clinical Medicine 3

Explain the fundamentals of the organisation of organ systems in health (Cardiovascular system, Nervous System, Respiratory system). This would include an ability to describe the basic histology of epithelia, connective tissue and mucosa.
Outline the basic pathology of organ damage
Describe mechanisms responsible for intracellular regulation and homeostasis in health and disease.
Explain the medical basis of pathological conditions and influences on health to identify better models of patient care and clinical perspectives.
Describe normal neo-natal development and metabolism and evaluate the consequences for pre-term nutrition
Understand the fundamentals of drug interaction and the consequences for prescribing
Sessional Structure & Teaching Methods
Sessions will contain a mixture of lectures and group-work based sessions. A typical session will comprise of a lecture followed by group work. The lecturing staff will provide the relevant case histories or associated questions related to the specific sessions, with students expected to act as discussants. Teaching staff will guide and moderate subsequent discussion as and when deemed appropriate to the session.
Assessment
Material from this module will be included in the End of Semester (ESA) written assessments and Objective Structured Clinical Examinations (OSCE) and may be included in all subsequent assessments in Phase I.
Suggested Reading
Clinical MedicineBy P Kumar, M Clark, and W.B SaundersEdition: 6 illustrated, Published by Elsevier Saunders UK, 2006 ISBN: 0702027634
Clinically Oriented Anatomy: Student CD-ROM [CD-ROM].By K.L. Moore, A.F Dalley, A.M.R Agur.Edition: 5, illustrated.Published by Lippincott Williams & Wilkins UK, 2006ISBN 0781736390, 9780781736398
Illustrated Clinical Anatomy. By P Abrahams, J. Craven and J LumleyEdition: 1, illustrated 4 Essentials of Clinical Medicine

Published by Hodder Arnold UK, 2005. ISBN 0340807431
Human Physiology: The Basis of Medicine, By G Pocock and C.D Richards, Edition: 3, illustrated.Published by: Oxford University Press UK, 2006ISBN 0198568789
Introduction to Clinical ExaminationBy M.J Ford, I Hennessy, A Japp Elsevier 2005
Pathophysiology of Heart DiseaseBy L.S Lily Edition: 4Published by Lippincott, Williams & Wilkins UK, 2006ISBN 0781763215
Pathology. By A. Stevens and J LoweEdition: 2Publisher: Mosby UK, 2000 ISBN 0-723432007
Essentials of Clinical Medicine 5

Sessions during Induction Week
All sessions will take place in the MTC Lecture Theatre
DATE SESSSION TITLE LECTURER
7 September 1
2
Introduction to Essentials of Clinical Medicine1.45 – 2.15pm
Introduction to the Terminology of Medicine2.15 – 5.00pm
Dr Alex Conner and Dr David Tweedie
Professor Peter Abrahams
8 September 3
4
Embryology9.00am – 12.15pm
Introduction to Molecules1.45 – 4.00pm
Dr Carolyn Rodgers
Dr Sinclair Steele
9 September 5
6
Introduction to Pathology9.00am – 12.15pm
Histology, chemical pathology, haematology and microbiology1.45 – 5.00pm
Dr Paul Matthews
Dr Paul Matthews
10 September 7
8
Introduction to Clinical Skills: What is a sign – The Physical Examination9.00am – 12.15pm
Integrated Learning Session – Putting the week together1.45 – 5.00pm
Dr Linda Maxwell
The Clinical Education Fellows
6 Essentials of Clinical Medicine

Semester 1 Timetable
All sessions are on Tuesday afternoons in the MTC LT 1.45 – 5.00pm
DATE SESSION TITLE LECTURER
14 September 9Introduction to Clinical Scenarios and Evidence Based Medicine
Dr Jeremy Shearman
21 September 10 Introduction to Physiology Dr David Tweedie and Dr Barney Ward
28 September 11 Introduction to Molecules Dr Sinclair Steele
5 October 12 Respiratory & Cardiovascular Anatomy Dr David Tweedie
12 October 13 Cell Physiology Dr Alex Conner
19 October 14 Introduction to Neurobiology Dr Dawn Collins
26 October 15 Introduction to Imaging Techniques Dr Fraser Millard
2 November 16 Molecules in the Human Body Dr Graham Ladds
9 November 17 Homoestatis Professor Peter Stanfield
16 November 18 Integrated Session* Clinical Education Fellows
23 November 19 Clinical Skills 1MedLine Training Samantha Johnson
30 November 20Clinical Skills 1Evidence Based Medicine Training
Samantha Johnson
Students to meet in LT at 1.45pm for briefing by CEFS. Break into groups and go with an identified CEF to work on an area covered by EoCM. Students to have e-mailed in advance if they want a particular area covered.
Essentials of Clinical Medicine 7

Session 1 Date: 7 September 2010Introduction to the moduleModule Leaders: Dr Alex Conner – Assistant Professor
Dr David Tweedie – Clinical Tutor WMSEmail: [email protected]
OverviewThis module was started in 2008 and is undergoing constant development. It has been changed in the light of comments from both students and staff involved in the 2009 cohort running. Your feedback throughout the running of the module is important and you do not have to wait until the end to let us know what is working really well and those areas that you feel require further attention/revision
AimsTo explain the rationale behind the planning of the module including the different educational backgrounds of students in your cohort.To encourage students with limited scientific background to understand very basic concepts.To encourage students with more substantial scientific backgrounds to help their colleagues in group work.To stress the clinical importance of this knowledge.
Intended Learning OutcomesAfter this session you should:
Appreciate the principles underlying the module Appreciate the relevance of the material to clinical medicine
8 Essentials of Clinical Medicine

Session 2Date: 7 September 2010Introduction to the Terminology of Anatomy and Anatomy Group Work
Session Leader: Professor Peter AbrahamsEmail: [email protected]
Overview A lecture will introduce about 100 common anatomical terms which form the basis of medicine. During the next three years most of you will DOUBLE your vocabulary and in this first week will use about 300 new terms. These terms are the very basis of medical practice and knowing about their origins will make it easier to work out the meaning in years to come. A special section on imaging and radiological terminology will also been provided at a future session.
Teaching Aims
To gain insight into the use of medical / anatomical terminology as used throughout your future medical practice.
Intended Learning Outcomes
By the end of the session or at least by the end of the first two weeks you should be able to: 1. “Translate” half a dozen typical case histories from medical terminology into
common language.
2. Be able to write a description of a person in a certain position or injury so that a fellow student could make themselves into that stance.
3. Be aware of the range of new terms especially prefix and suffixes that often give clues to meaning.
Structure of the Session:
1. Lectures with video clips etc. to illustrate the many terms used.
2. Group work based on “Chinese Whispers”. Pictures of anatomical odd patients which you will have to describe and pass to the next group who will then enact the position you have written down . They will do the same for you from a different set of pictures.
3. Plenary session translating the written word into actions and making “statues”.
Essentials of Clinical Medicine 9

Cross-Modular Themes
Every new term used in these sessions will be used constantly over the next 30 years of your medical career.
Suggested Reading
Any anatomy text book - the first chapter or two on terminology.
Illustrated Clinical Anatomy, ISBN 0 340 80743 1 by Abrahams Craven Lumley Hodders. This also has a website with 1000 downloadable jpeg files of anatomy and clinical medicine.
Another similar short book recommended is Essential Clinical Anatomy by Moore and Agur Williams Wilkins. An atlas is a very good way of seeing and learning anatomy and there are many on the market- some have lots of clinical cases and pictures on DVDs.
Terminology used in Anatomy is the foundation language and cornerstone of all medical practice, it is the language that one doctor uses to describe accurately a clinical situation to another person in the team.. Most average people have a normal English vocabulary of around 5000 words. Your new medical vocabulary will have doubled that figure in the next few years - so the sooner you start learning it the easier all medical subjects will seem. Learning precision in clinical medicine starts today with the anatomical words, their origins and definitions. By the end of just your first afternoon you will have gained approximately 300-400 new terms and be able to use them in a correct context. Learning this new medical language will make reading and lectures so much more comprehensible day by day so that in future you will be able to work out new terms from first principles. Many of you will feel overloaded with new facts at the end of these sessions but do not worry- it does get easier as time passes- believe me!
10 Essentials of Clinical Medicine

Group Work in Tutorial rooms
Each group of students will be given one photo with two different numbered anatomical everyday poses on it.
You will then WRITE a description of that person’s position in anatomical / medical terminology (5-10 minutes) and then pass on the written text and number to the group next door.
They will then swap with you their written descriptions of their numbered positions.
You will then take their description and work out the position of their photos (5-10 minutes). With these two positions you will then send members of your group to act out in the lecture theatre at the plenary session for all to see how accurate your interpretations are.
It is like Chinese Whispers with Medical Terminology
Essentials of Clinical Medicine 11

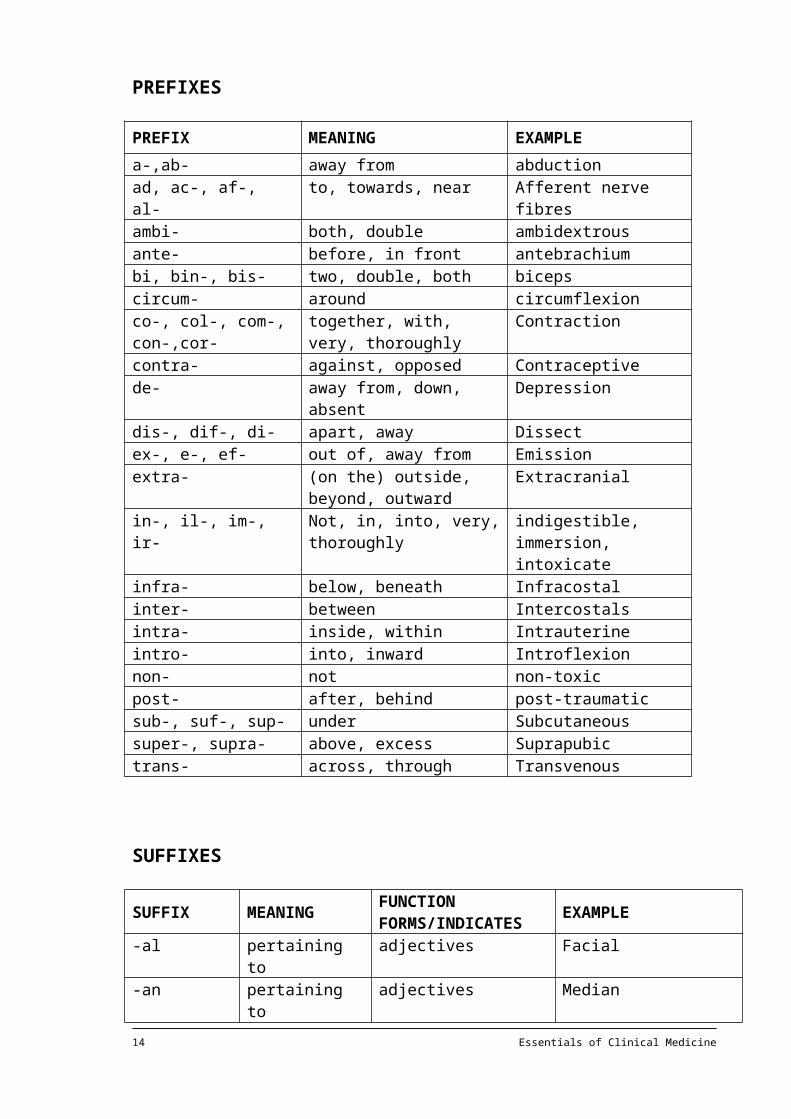
PREFIXES
PREFIX MEANING EXAMPLEa-,ab- away from abductionad, ac-, af-, al- to, towards, near Afferent nerve fibresambi- both, double ambidextrousante- before, in front antebrachiumbi, bin-, bis- two, double, both bicepscircum- around circumflexionco-, col-, com-, con-,cor-
together, with, very, thoroughly
Contraction
contra- against, opposed Contraceptivede- away from, down, absent Depressiondis-, dif-, di- apart, away Dissectex-, e-, ef- out of, away from Emissionextra- (on the) outside, beyond,
outwardExtracranial
in-, il-, im-, ir- Not, in, into, very, thoroughly
indigestible, immersion, intoxicate
infra- below, beneath Infracostalinter- between Intercostals intra- inside, within Intrauterineintro- into, inward Introflexionnon- not non-toxicpost- after, behind post-traumaticsub-, suf-, sup- under Subcutaneoussuper-, supra- above, excess Suprapubictrans- across, through Transvenous
SUFFIXES
SUFFIX MEANING FUNCTION FORMS/INDICATES EXAMPLE
-al pertaining to adjectives Facial-an pertaining to adjectives Median-ar, -ary pertaining to adjectives fibrillar, fibrillary-ation condition, state nouns (indicates
process or action)Ossification
-ion act of nouns Contraction-ive pertaining to adjectives Antitussive-ous pertaining to adjectives Pyogenous-or agent, person,
instrumentMATCH THESE
nouns Respirator
12 Essentials of Clinical Medicine

LIST A LIST B1. abduction a. concerning the area beneath the tongue2. adduct b. outside or unrelated to the bladder3. adrenal c. within the urinary bladder4. antero-inferior d. pertaining to an inward and downward position5. anterolateral e. between adjacent teeth6. bilateral f. to the left7. dextrad g. inside the heart8. dorsiduction h. indicating movement from back to front9. extracystic i. near the kidney10. extroversion j. within a joint11. interdental k. inside the mouth12. intero-inferior l. draw toward the main axis of the body13. interrenal m. turning inside out14. intra-articular n. lateral movement of the limbs away from the
median plane of the body15. intracardiac o. pertaining to two sides16. intracerebral p. located behind and at the side of a part17. intra-oral q. pertaining to posterior portion of the upper arm18. intra-osseous r. located above the kidney19. intravenous s. across or through the bladder20. intravesical t. between the kidneys21. mediolateral u. concerning the middle and side of a structure22. postbrachial v. within the main portion of the brain23. postero-anterior w. above and behind24. posterolateral x. to the right25. sinistrad y. drawing backwards26. subcutaneous z. in front and below27. sublingual aa. beneath the skin28. superoposterior bb. in front and to one side29. suprarenal cc. within the bone substance30. transvesical dd. within a vein
Essentials of Clinical Medicine 13
1. A 50-year-old man was admitted to hospital. He was is hypovolaemic (Latin: volumen: volume) shock. Haematemesis and bleeding per rectum were conditions reported by the paramedic.
On admission his haemoglobin count was found to be low, and thrombocytopenia as well as deranged clotting of blood was noticed.
In spite of being resuscitated with packed red blood cells and frozen plasma, haemorrhage and deterioration in his coagulopathy occurred (coagulation: clumping together of blood cells; clotting) the following day. An upper gastrointestinal endoscopy was performed. This revealed a large quantity of blood in the patient’s stomach and oesophagus, as well as oesophageal varices. The patient’s condition deteriorated further and he died.
A post-mortem was held. The pathologist noted in his report the body of a middle-aged man, deeply jaundiced with gynaecomastia, the abdomen markedly distended and moderate oedema. A large quantity of straw coloured fluid was present in the peritoneal cavity and numerous varices were found in the distal end of the oesophagus. Hepatic cirrhosis and splenomegaly were noticeable. Blood was found in all parts of the intestinal tract. Histology of oesophageal tissues indicated large-scale submucosal venous dilatation while the liver showed micronodular cirrhosis (cirrhosis; end-stage liver disease characterised by nodular regeneration).
2. A 70-year-old man visited his physician complaining of dysphagia and dyspnoea. He also referred to a swelling in his neck, suspecting a goitre.
After physical examination, a needle biopsy and an ultrasound scan the physician diagnosed thyroid cancer.
He recommended an immediate thyroidectomy and a dissection of the neck to search for and remove enlarged lymph nodes.
3. A 36-year-old woman visited her physician complaining about pain in the right side of her thorax and some apnoea. During the physical examination the physician observed tachypnoea and evidence of shock. He also noted varicose veins, especially in her right thigh and calf and on questioning she told him that she had had painful varicose veins in her lower limbs for some time. On cardiac examination he detected tachycardia and arrhythmia. The physician performed an ECG and also requested a pulmonary angiogram and fluoroscopy. Fluoroscopy of the patient’s lungs revealed poor or absent pulsations in the descending branch of the right pulmonary artery and relative anaemia of the right lung.
Diagnosis: a thrombus from a varicose vein in the lower limb caused pulmonary thromboembolism.
4. A markedly obese woman visited the physician for a right-sided abdominal pain. The pain dated from two years ago when, at first, intermittent episodes of epigastic pain lasting two to four hours occurred. At the time cholecystitis with cholelithiasis was diagnosed and a cholecystectomy was performed. Five large gallstones were found. Since then everything had gone well until about four months ago when right-sided pain taking a crescendo pattern started again. It did not cause nausea or emesis and there was no urge to defaecate. Apart from the cholecystectomy mentioned, her past medical history was only marked by an appendicectomy a tonsillectomy and an arthroplasty. A physical examination confirmed her
14 Essentials of Clinical Medicine

obesity. She was, anicteric. Her neck revealed no lymphadenopathy or thyromegaly. No hepato-or splenomegaly could be observed and a haemo-negative stool was registered. No oedema was apparent. Laboratory tests indicated no gastrointestinal abnormalities and the kidneys showed no signs of hydronephrosisDiagnosis: As physical examination and laboratory tests did not suggest specific abnormalities or deviations, an occult nephrolithiasis could be diagnosed.
5. Mrs Fairburn (59) was admitted to hospital complaining of severe pain in the upper right part of the abdomen. She was anorexic, febrile and nauseous. She also complained of intermittent emesis. Although her sclerae (outer layer of eyeballs) were yellow she was not particularly jaundiced. Tenderness and guarding were present in the upper quadrant of the anterior abdominal wall.
Radiological and laboratory tests were performed and cholecystits resulting from calculi in the gallbladder was diagnosed. A cholecystectomy was performed by laparoscopy and a gallstone was removed from the bile duct after choledocholithotomy
6. A 40-year-old heavy smoker visited the pulmonologist and complained about persistent tussis, thoracalgia and haemoptysis. Bronchoscopy and thoracography were requested.
A congenital lesion was revealed and after a biopsy a bronchogenic carcinoma was found in the in the apex of the lung.
7. A young woman, married to a medical student, woke up one morning not feeling well. Apart from being anorexic and lethargic, she experienced severe abdominal pain. As it was time for her menstrual period, her husband suspected probable dysmenorrhoea or even an ectopic pregnancy since she missed her last menstrual period. After she had also begun to feel febrile and nauseous, followed by emesis, so her husband took her to hospital.
During investigation the physician detected a localised myospasm in the left lower quadrant of the abdomen. A blood count indicated leukocytosis. The physician eventually diagnosed appendicitis and gave instructions for the patient to be prepared for an appendicectomy.
8. A post mortem was performed on the body of an 80-year-old woman. The patient had been admitted to hospital with severe melaena (black, tarry faeces) She required a blood transfusion. A hemicolectomy was performed but complications led to ischaemia of the colon and a colostomy also had to be established.
A week after surgery the anastomosis broke down. The patient was re-admitted with severe sepsis and faecal peritonitis. The bowel had to be reanastomosed by further surgery. A few days later, however, the patient died. At necroscopy the lungs were found to be congested and oedematous. The bowel anastomosis was still in place. Pus was found in the subphrenic spaces. Histology indicated the presence of colonic diverticula and diaphragmatic inflammation. Severe hepatic congestion was also observed.
Essentials of Clinical Medicine 15

Session 3Date: 8 September 2010 Embryology
Session Leader: Dr Carolyn RodgersE-mail: [email protected]
Overview:
An introduction to basic embryology and the events of the first three weeks of human life.
Aim:
Begin your study of embryologyOutline the early major developmental events and anatomical landmarks of a human embryoUnderstand and be able to use the terminology of early human developmentAct as an introduction to the systems embryology you will encounter in the phase one modulesBegin to identify relevance of embryology to clinical practice
Learning Outcomes:
Describe simply the processes from fertilisation to implantationDescribe simply the second week of human developmentDescribe simply the early stages of placental developmentDescribe simply the development of three germ layersDescribe simply the establishment of body axesBe able to connect some clinical problems to aberrations in the development of an early human embryo
Recommended Reading:
Langman’s Medical Embryology, by T.W.Sadler, PhD 11TH Edition 2010. Lippincott Williams and Wilkins
Embryology Colouring Book. Matsumara and England
16 Essentials of Clinical Medicine

Session 4Date: 8 September 2010Introduction to Molecules
Session Leader: Dr Sinclair SteeleEmail: [email protected]
Overview
A review of the structure and function of key biological molecules. An overview of membrane components and functions. The key principles behind signal transduction.
Teaching Aims
To introduce the basic structure and function relationships of the major biologically important molecules. To indicate the clinical significance.
To summarize the principles behind membrane function and signal transduction.
Intended Learning Outcomes
At the end of this session it is expected that you will be able to:
Briefly describe the functions of the major cellular organelles.
Understand the fragility of the human cell and be able to list injurious stimuli.
Appreciate the importance of medical genetics.
Define key genetic terminology – transcription, replication and translation.
Recognize chromosomal structure.
Have achieved an understanding of protein structure and the effects of disruption of this structure for the whole body.
Have achieved a critical understanding of the importance of the ionic balance across the cell membrane.
Appreciate the range of functions of a biological membrane.
To understand the principles of signal transduction without having memorized any one complete pathway.
Essentials of Clinical Medicine 17

Sessions 5 and 6Date: 9 September 2010Introduction to Pathology DaySession Leader: Dr Paul MatthewsTitle: Consultant Histopathologist UHCW and Honorary Associate
Professor/Phase II Co-ordinator Warwick Medical SchoolEmail: [email protected]: 024 7696 5437
Overview: What is pathology?What are its branches?How do those branches interact and provide results that drive clinical diagnosis?
Teaching Aims: The session aims to introduce the main branches of pathology, namely;
1. Histopathology2. Haematology3. Clinical Biochemistry4. Microbiology
Intended Learning Outcomes:By the end of the day the student will understand the importance of clinical pathology to patient management.
Structure of the Day:The day begins with a short introduction. There are four specialty based sessions (lecture and group work). These will be followed by a plenary session where a clinical case will be used to illustrate the importance of interaction between the specialties and ward based clinicians.
Cross-Modular Themes:See individual session outlines.
Assessment:
Material from this module will be included in the End of Semester (ESA) written assessments and Objective Structured Clinical Examinations (OSCE) and may be included in all subsequent assessments in Phase I.
18 Essentials of Clinical Medicine

Timetable
Time Topic Type Tutor in charge0900 Introduction Talk Paul Matthews
0915 Histology Lecture Paul Matthews
0945 Histology Group Work Paul Matthews
1100 Haematology Lecture Beth Harrison
1130 Haematology Group Work Beth Harrison
1345 Biochemistry Lecture Steve Smith
1415 Biochemistry Group Work Steve Smith
1515 Microbiology Lecture Peter Munthali
1545 Microbiology Group Work Peter Munthali
1630 Plenary Discussion Paul MatthewsBeth HarrisonSteve SmithPeter Munthali
Essentials of Clinical Medicine 19

Session Title: Introduction to Histopathology
Session Date: 9 September 2010, 0915-1030
Session Leader: Dr Paul MatthewsTitle: Consultant Histopathologist UHCW and Honorary Associate
Professor/Phase II Co-ordinator Warwick Medical SchoolEmail: [email protected]: 024 7696 5437
Overview: This session is intended as an introduction to those aspects of general pathology/histopathology that will help in your understanding of other Semester 1 modules. Semester 2 includes the Mechanisms of Disease Module which will look at general pathology in more detail.
Teaching Aims: The session aims to introduce the concepts of;
5. How does a histopathologist make a diagnosis?6. Inflammation and Healing7. Thrombosis and Embolism8. Atheroma9. Neoplasia
Intended Learning Outcomes:By the end of the session the student will be able to understand the very basics of;
1. How a pathologist makes a diagnosis from tissue.2. Acute Inflammation including the relevance of Latin i.e. Tumor, rubor, calor,
dolor, role of vessels and neutrophils3. Chronic Inflammation including causes, typical cells and granulomas.4. Granulation tissue and its role in healing.5. Thrombosis and embolism.6. Atheroma including the atheromatous plaque and clinical results.7. Defining the “-plasias”
a. Hyperplasiab. Metaplasiac. Dysplasia
8. Defining the “-trophies”a. Hypertrophyb. Atrophy
9. Terminology of Tumoursa. Benign and Malignant b. Invasion and Metastasisc. Clinical Effects
Structure of the Session:The session begins with a lecture. The themes will be explored further in the group work.
20 Essentials of Clinical Medicine

Cross-Modular Themes:Gastrointestinal Module; Acute and chronic inflammation of various GI organs including stomach, liver and colon. Neoplasia of GI tract. Health in the Community; Work of other healthcare professionals. Molecules; various mediators of inflammation, molecules important in cell cycle control and cellular growth which are also important in adaptation and neoplasia.
Handouts and other relevant Information:Available on-line prior to the lecture.
Required and Recommended Reading:This is an introductory talk and there is no required prior reading. However the basics of general pathology are well covered in;
General and Systematic Pathology (3rd Edition), Underwood, Churchill LivingstoneCore Pathology, Stevens and Lowe, Mosby.
These texts will be useful help in your understanding of this brief overview and
One of them is essential for the Semester 2 Mechanisms of Disease module. Have a look and choose your favourite.
Assessment:
Material from this module will be included in the End of Semester (ESA) written assessments and Objective Structured Clinical Examinations (OSCE) and may be included in all subsequent assessments in Phase I.
Essentials of Clinical Medicine 21

Group Work (Cellular Pathology)
1. Having been fascinated by the workings of the pathology department (as revealed in the Essentials of Medicine Module) you take a holiday job as a Medical Laboratory Assistant in the pathology department of your local hospital. Due to a delivery error, the samples for all the different branches of pathology have become mixed up. You are given the job of sorting out which samples need to go to which branch of pathology. E.g. a wound swab with the clinical information - (?infection) would need to go to the microbiology department. Just match up the samples to the correct branch of pathology.
The branches to choose from are;1. Histopathology/Cytopathology (Cellular pathology)2. Haematology3. Microbiology4. Clinical Biochemistry/Chemical Pathology.
The Samples: Branch of Pathology.
Bone Marrow Aspirate (Anaemia ?cause)
Blood for Troponin T (?myocardial infarct)
Blood Cultures (?septicaemia)
Colon Biopsy (diarrhoea ?cause)
Blood Film (?leukaemia)
Blood for Liver Function Tests (LFT) (?hepatitis)
Duodenal Biopsy (?coeliac disease)
Faeces (?ova/cysts/parasites)
Full Blood Count (FBC) (?anaemia)
Mid Stream Urine (MSU) ?urinary tract infection (UTI)
Swabs for Methicillin Resistant Staph.Aureus (MRSA) Screen (?carrier)
Faeces for C.Difficile Toxin (?pseudomembranous colitis)
Blood for Urea and Electolytes (U and Es) (?renal failure)
Blood for Amylase (?pancreatitis)
Lymph Node Biopsy (?tuberculosis)
22 Essentials of Clinical Medicine

2. Pick a Pathological Process
Here are some common clinical scenarios. Use your previous knowledge and any information from the lecture to identify the broad category of pathological process that is occurring.
e.g. Bernard is a 16 year old who presented to the emergency department with a 12 hour history of vague abdominal pain which has since become localised to the right lower side of his abdomen. He undergoes an operation to remove his appendix. The appendix looks red, swollen and is covered in yellow pus.
Pathological Process: This is a case of acute appendicitis and an example of acute inflammation.
Choose the pathological process in the following cases from this list.a. Cell deathb. Acute inflammation.c. Chronic inflammationd. Healing and repaire. Embolismf. Atheromag. Benign Tumourh. Malignant Tumour
Case 1
Jessie is a 32 year old with a 6 month history of diarrhoea and passing blood in the stools. She has lost weight. On examination the anus is very sore with ulceration. She has a test to look into the colon (colonoscopy). This shows ulcers in the lining of the bowel and there are narrow areas.
Pathological Process:
Case 2
Archie is 60, has had raised blood pressure for 20 years and has smoked since he was 12. Last night he felt a pain in his chest which he initially laughed off as indigestion. However the pain worsened, spread to involve his left arm and he became very sweaty. He went to casualty where the F2 doctor carried out an electrocardiogram (ECG) and sent blood for a Troponin-T level (which was raised).
Pathological Process:
Essentials of Clinical Medicine 23

Case 3
Matilda is 90 and has had an ulcer on the inner aspect of her left ankle for many months. In the past she suffered from varicous veins. The ulcer is covered by yellow dead material. A surgeon removes the dead material (debridement) and underneath is revealed red tissue which bleeds very easily.
Pathological Process:
Case 4.
Brenda found a lump in the breast. Her GP sent her to the specialist who examined her breasts and found the lump. The specialist also found a lump in the adjacent armpit and noticed tenderness over the spine when light pressure was applied.
Pathological Process:
Case 5.
Susie has just stepped off the plane from Australia. In the arrivals lounge she felt severe chest pain and became breathless.
Pathological Process:
Case 6.
Stan is 25 and has had a cough for 3 days. He is coughing up bright yellow sputum. He has felt unwell and has had a fever. He also has some sharp chest pain which is worse when he breaths in.
Pathological Process:
3. The Virtual Autopsy
Archie (whom you first met in case 2 above) does not survive the night despite all that the power of modern medicine has to offer. The relatives give permission for an autopsy to be performed. You are shown pictures of the main organs relevant to the cause of death.
For each of the photographs;a. Describe the appearance andb. Try to decide on what is wrong.
If you had to certify the cause of death what would you give as;a. The immediate cause of deathb. The underlying diseases that gave rise to a)?24 Essentials of Clinical Medicine

Heart
Description?
Problem?
Coronary Artery
Description?
Problem?
Essentials of Clinical Medicine 25

Kidney
Description?
Problem?
Cause of Death
a) …………………………………….(immediate cause)
b)……………………………………..(underling cause leading to a)
c)……………………………………..(underling cause leading to b)
d)……………………………………..(underling cause leading to c)
26 Essentials of Clinical Medicine

Session Title: An Introduction to Haematology
Date: 9 September 2010, 1100-1215
Session Leader: Dr Beth HarrisonConsultant HaematologistUniversity Hospital Coventry and Warwickshire
Email: [email protected]
Overview This session aims to introduce you to some general aspects of haematology related to red blood cells and blood coagulation and will help you in your understanding of some Semester 1 modules including respiratory and cardiovascular physiology.
Teaching Aims: To understand what blood parameters can be measured in a Haematology LaboratoryTo understand how we decide what is normal and abnormal in a blood countTo understand the work of a blood transfusion laboratoryTo understand Virchow’s Triad
Intended Learning Outcomes:
By the end of the session the student will be able to understand;What do red blood cells do?What is anaemia?What is the ABO blood group system?Why does blood clot (principles)?
Structure of the Session:
The session begins with a lecture. The themes will be explored further in the group work.
Required and Recommended Reading
This is an introductory talk and there is no required reading.
Essentials of Clinical Medicine 27

Group Work (Haematology)
Exercise 1
This is the full blood count on a young woman with longstanding tiredness. What abnormalities can you see in the results? (You have been given the reference ranges.)
Test Name Result Unit Reference RangeWBC 7.59 x10^9/l 4.00-11.00 Rbc 3.30 x10^12/l 4.10-5.10 Hb 6.3 g/dl 12.0-15.0 Hct 0.220 l/l 0.360-0.460 MCV 67.6 fl 80.0-100.0 MCHC 28.3 g/dl 31.5-34.5 Plt 571 x10^9/l 140-400 Neut 6.45 x10^9/l 2.00-7.00 Lymp 0.91 x10^9/l 1.00-3.00 Mono 0.23 x10^9/l 0.20-1.00 Eos 0.00 x10^9/l 0.02-0.50 Baso 0.00 x10^9/l 0.01-0.10 NRC 0.00 x10^9/l Comments Blood Film. Microcytosis.
Hypochromasia.
Hb=Haemoglobin; WBC=White Blood Cell Count; Rbc=Red Cell Count; MCV=Mean Cell Volume; Plt=Platelet count
Please list the abnormalities:
Can you think of anything that might be causing these abnormalities?
You may not know the names of the tests but what other pieces of information would you like to find out?
28 Essentials of Clinical Medicine

Exercise 2
A 40 year old woman has just presented to you with a swollen leg after a 10 hour coach journey down from Edinburgh to see her sister. She is on the combined oral contraceptive pill and is a life long smoker. Her BMI is 41. She had an arthroscopy on her knee 4 weeks ago to investigate pain following a twisting injury. She is concerned because her mother died following a pulmonary embolism aged 38.
List her risk factors for a venous thrombosis under the different elements of Virchow’s triad
Blood Vessel Flow
If you don’t do something about the blood clot in her leg what might happen to her?
Essentials of Clinical Medicine 29

Exercise 3
Blood Group antigens and antibodies:
Blood Group O: Red cells do not express Blood Group A or Blood Group B on their cell surfaces. Plasma contains antibodies against Blood Group A and Blood Group B (“Anti-A” and “Anti-B”). “Anti-A” and “Anti-B” lyse red cells of Blood Group A and B respectively.
Which blood (red cells) can patients of the following groups receive?
Patient is Can receive blood of group(s)Blood Group ABlood Group ABBlood Group BBlood Group O
Individuals of Blood Group ______ are known as universal donors because their blood can be given safely to patients of all blood groups.
Individuals of Blood Group ______ are known as universal recipients.
Some one of Blood Group AB can receive plasma from donors of which Blood
Group and why? A______________________________________________
30 Essentials of Clinical Medicine
Session Title: Introduction to Clinical Biochemistry
Date: 9 September 2010, 1345-1500
Session Leader: Dr Steve SmithConsultant Clinical BiochemistUniversity Hospitals of Coventry & Warwickshire
Email: [email protected]
Overview: This session is intended as an introduction to Clinical Biochemistry, its scope and terminology.
Teaching Aims: Introduction to interpretation in Clinical Biochemistry and the use of Clinical Biochemistry tests in patient diagnosis and management.
Intended Learning Outcomes: At the end of the session you will:1. Understand some of the terminology 2. Be able to describe the role of Clinical Biochemistry in the
diagnosis and management of electrolyte disorders3. Be able to describe the role of Clinical Biochemistry in the
diagnosis of diabetes4. Understand how Clinical Biochemistry supports the diagnosis
a. and management of renal disease5. Understand how Clinical Biochemistry links with the other
a. Pathology disciplines
Required and Recommended ReadingThis is an introductory session and there is no required prior reading. However the basics of Clinical Biochemistry are well covered in;
Clinical Biochemistry: An illustrated Colour Text, 4th Ed.A. Gaw, MJ Murphy, RA Cowan, DStJ O’Reilly, MJ Stewart, J. Shepherd. Churchill Livingstone.
Essentials of Clinical Medicine 31

Group Work (Clinical Biochemistry)
Case 1A 50 year old man turns up at his General Practitioner’s complaining of tiredness. The GP hasn’t seen the patient for many years and decides to do a check-up as he is significantly overweight and a known smoker?
What checks would you do and why?(The findings will be provided on the day)
What might have happened if these had not been done for a few years longer?
The GP after reviewing the findings decided to arrange for the patient to have a Glucose Tolerance Test (GTT).
What is a glucose tolerance test and what is it used for?
What preparation does the patient need to do and what should they not do during the test?
The results of the patient’s GTT were as follows:0 min Glucose = 5.8 mmol/L120 min Glucose = 12.6 mmol/L
What do these results indicate?
32 Essentials of Clinical Medicine

Case 2.65 year old male, known Type 2 diabetic attends for his annual check having had a blood test a week earlier.
What are these tests designed to indicate?
What conclusions did the GP draw from these results?
Weight 95kg Full Blood Count: No abnormalitiesBP 150/95 Urine Albumin 50mg/mmol Creatinine (<2.5)Sodium 140 mmol/L (135-143) HbA1C 8.0% (DCCT ) (6.5% -7.5%)Potassium 3.2 mmol/L (3.7-5.0) TSH 6.5 mIU/L (0.34 – 4.0)Urea 7.5 mmol/l (2.6-6.6) Glucose (Non fasting) 6.0 mmol/L (<7.8)Creatinine 105 μmol/L (59-104)eGFR 65 ml/min/1.73m2 (<60)
What would the GP’s suggestions to the patient be in the light of these results?
Case 3A 19 year old male was involved in a road traffic accident. Both femurs were fractured and his spleen was ruptured. Two days after surgery and transfusion of 16 units of blood the following results were found:
Sodium 136 mmol/L (135-143) Adjusted Calcium 2.40 mmol/L (2.22-2.58)
Potassium 6.1 mmol/L (3.7-5.0) Phosphate 2.8 mmol/l (0.75-1.40)Urea 20.9 mmol/L (2.6-6.6) Bicarbonate 17 mmol/L (22-29)Creatinine 190 μmol/l (59-104)
The patient was producing only 10 ml urine per hour and a spot urine sodium was 8mmol/L
What diagnosis pulls all this information together?
Essentials of Clinical Medicine 33

Why is no eGFR quoted?
What is an ‘adjusted’ calcium? What is it adjusted for?
What follow-up tests should be performed and how frequently?
What are the three phases of acute renal failure?
34 Essentials of Clinical Medicine

Session Title: Introduction to Microbiology
Session Date: 9 September 20101515 – 1630
Session Leader: Dr Peter Gayo MunthaliTitle: Consultant Microbiologist and Honorary Associate ProfessorDepartment: Microbiology, UHCWEmail: [email protected]: 024 7692 5472
Overview: This session is intended as an introduction to the microbiology component of the infection and immunity module. Most of the themes introduced will be covered in more detail during the immunity and infection module.
Teaching Aims: The session aims to familiarise you with the concepts of;1.What is Microbiology? What does a clinical microbiologist/Virologist do?2. Bacteria, anatomy and classification 3. Viruses and classification4. Common themes in bacterial and viral infections5. Mycology and disease6. Infection control7. Antibiotics and other anti-infectives
Intended Learning Outcomes:By the end of the session the student will be able to;
1. Describe the role of a clinical microbiologist/virologist in patient care
2. Describe the difference between bacteria and viruses.3. Distinguish between gram-positive and gram-negative
bacteria4. Describe bacteria by their shape as either cocci or rods5. Describe the relationship between viruses and cells in viral
multiplication6. Name some common bacterial and viral diseases linked to
their causative organisms7. Describe in broad terms, how antibiotics work on bacteria8. Describe the importance of infection control in health care
Essentials of Clinical Medicine 35

Structure of the Session:This is a lecture and group work in which the themes raised in the lecture will be further explored.
Cross-Modular Themes:
Infection & the Immune System: Immunology module; The anatomical organisation of the immune system and how it is adapted to resist infection, the main effector mechanisms of the immune response and how they are generated and function and the control of immune response to limit self damage.
Pathology module; understanding the function of the neutrophil and chronic inflammation including Granulomatous inflammation
Introduction to Molecules module; functions of the major cellular organelles, transcription, replication and translation and functions of a biological membrane
Handouts and other relevant Information:Available on-line prior to the lecture
Required and Recommended Reading:This is an introductory talk and prior reading is not mandatory. However those who would like prior reading, and especially those without prior biology knowledge, can read the following;
Clinical Microbiology by J. Keith Struthers; Chapter 1 and parts of Chapters 2-4
Medical Microbiology by Morag C. Timbury;Chapter 2, Bacteria-structure, growth, nutrition and geneticsChapter 20, Viruses: general properties, host response and replication
These will act as a brief introduction to basic microbiology on which you will be able to build on during the immunity and infection module and throughout your medical school training.
Assessment:
Material from this session which acts as an introduction to the subject prior to the immune and infection module may be directly or indirectly included in the End of Semester (ESA) written assessments and Objective Structured Clinical Examinations (OSCE) and may be included in all subsequent assessments in Phase I.
36 Essentials of Clinical Medicine

Group Work (Microbiology)
Case 1 1a. A 43 year old man presents with this condition, what is the diagnosis?
1b. A swab was taken from the lesion, describe what process is seen on the agar plate (choose one).
a. Gamma haemolysisb. Alpha haemolysisc. Beta haemolysis
1c. Describe the microscopic appearance of the organism
1d. What do you think is the name of the organism? (Choose one)
a. Staphylococcib. Beta haemolytic Staphylococcic. Alpha haemolytic streptococcid. Beta haemolytic streptococcie. Gamma haemolytic streptococcif. Beta haemolytic staphylococci
1e. To which antibiotics is the organism resistant?
1f. Which antibiotics would you use to treat this infection? (You can choose more than one
a. Co-trimoxazoleb. Penicillinc. Clarithromycind. Clindamycine. Linezolidf. Erythromycing. Tetracycline
Case 22a. Loveness Wariki, a 70 year old alcoholic woman presents with shortness of
breath, “the worst headache of my life” and pain when looking at lights (photophobia). A chest X-ray was done and a lumbar puncture performed. A few hours later her shortness of breath worsened and required intubation for ventilation in Intensive Care Unit. She was started on benzylpenicillin 2.4 g 4 hourly.
Describe the CXR. (Choose one)
a. Right lower zone consolidationb. Bilateral consolidationc. Left upper zone consolidationd. Right upper zone consolidatione. Right middle lobe consolidationf. Left lower zone consolidationg. Normal chest X-ray
Essentials of Clinical Medicine 37

2b. A blood culture and cerebral spinal fluid (CSF) grew this organism. Describe its cultural appearances. (Choose one)
a. Gamma haemolytic coloniesb. Alpha haemolytic coloniesc. Beta haemolytic colonies
2c. Which term best describes the organism on microscopy. (Choose one)
a. Gram-positive coccib. Gram-negative coccic. Gram-negative coccid. Gram-positive diplococcie. Gram-negative diplococci
2d. Choose the most likely name for this organism
a. Staphylococcus aureusb. Beta haemolytic Streptococcic. Streptococcus pneumoniaed. Neisseria meningitidese. Methicillin resistant Staphylococcus aureus (MRSA)
2e. What is the most appropriate diagnoses for Loveness? (You can choose more than one)
a. Atypical pneumoniab. Community acquired pneumoniac. Pneumococcal pneumoniad. Staphylococcus pneumoniae. Bacterial meningitisf. Meningitis due to Neisseria meningitidesg. Pneumococcal meningitish. Staphylococcus meningitis
Case 3 3a. This is a back of Endless Mavalas, a 13 year old girl who has been sent
back from school because she is unwell. Several other pupils have this condition.What is the most likely diagnosis?
a. Measlesb. Urticariac. Herpes simplexd. Chicken poxe. Small poxf. Rubellag. Shingles
3b. Mr Hopeful Lejend had a similar condition at 10 years of age. He is complaining of burning pain from this lesion.What is the diagnosis?
38 Essentials of Clinical Medicine

Group Work (Microbiology) Cases Pictures
Case 11a
1b
1c
1eEssentials of Clinical Medicine 39

Antibiotic Sensitivity Plate
Key for 1eS-Sensitive, R-Resistant
Zone Sizes StatusAntibiotic Code Sensitive ResistantCo-trimoxazole A ≥ 20mm ≤ 16mm RPenicillin B ≥ 20mm ≤ 19mm SClarithromycin C ≥ 22mm ≤ 19mm RClindamycin D ≥ 17mm ≤ 16mm RLinezolid E ≥ 20mm ≤ 19mm SErythromycin F ≥ 22mm ≤ 19mm RTetracycline G ≥ 20mm ≤ 19mm S
Case 2
40 Essentials of Clinical Medicine
30mm
11mm
10mm
21.5mm 23mm

2a
Loveness Wariki CXR on Admission
2b
2cEssentials of Clinical Medicine 41

Case 3
3a
Endless Mavalas’s Spots
42 Essentials of Clinical Medicine

3b
Mr. Hopeful Lejend’s Face
Essentials of Clinical Medicine 43

Session 7Date: 10 September 2010Introduction to Clinical Skills II: What is a sign – The Physical ExaminationSession Leader: Dr Linda MaxwellEmail: [email protected]
Overview
Physical examination is a different but no less exacting skill than history taking. It is art but also science. Long hours of practice, study and experience are required to learn this new art, which calls into play visual, auditory, olfactory, tactile and muscular senses.
The ability to observe is one of the marks of a fine clinician. This session will start the long process of developing your observational skills necessary for good clinical practice. It will also introduce the all important vital signs.
Objectives
After the session the student should be able to:
Define a sign
Recognise the needs, sensitivity and rights of the patient
Recognise that visual, auditory, olfactory, tactile and muscular senses are all used when examining the patient
Differentiate between the need for a comprehensive examination and a focused examination
Understand the importance of a good preparation and organisation before examining a patient
Understand the importance of observation of the whole patient first, then the detail.
Conducet a general survey of the patient
List and recognise some common signs found on general examination.
Understand the importance of and list the vital signs
Define normal temperature range and discuss different types of thermometers used to take a temperature
Attempt to palpate a pulse and measure a blood pressure
Count respiratory rate and assess the rhythm, depth and effort of breathing
Read and enter data onto an observation chart
Describe your findings with respect to the general survey and vital signs
44 Essentials of Clinical Medicine

Structure of the Session
There will be two lectures and one small group session.
Lecture 1 General aspects of physical examination and common signs
Lecture 2 Vital signs
Small Group Vital signs and Observation charts
Required and Recommended Reading1. Introduction to Clinical Examination (essential to read for CSc1)
M J Ford, I Hennessy, A Japp, Elsevier 2005
2. Clinical SkillsNLT Cox and T A RoperOxford Core Texts, Oxford University Press, 0192628747, 2005
3. Clinical Examination: A Systematic Guide to Physical DiagnosisN J Talley and S O’Connor (CD and e-text)Elsevier 2006
4. Lecture Notes on Clinical SkillsChris Hatton and Roger Blackwood4th Edition, Blackwell, 0632065117
5. Pocket to Guide to Clinical ExaminationOwen Epstein, G David Perkin, John Cookson, David P de Bono3rd Edition, Mosby, 0723425760
6. Clinical MedicinePraveen Kumar and Michael ClarkLatest Edition, W B Saunders, 0702025798
Reference book:
Color atlas of physical signs in general medicineZatouroff M Mosley
Essentials of Clinical Medicine 45

Session 8Date: 10 September 2010Integrated Learning Sessions - Putting the week together!Session Leaders: The Clinical Education Fellows (The CEFs)
OverviewInteractive session with the Clinical Education Fellows to aid understanding of how all of the concepts include in the past week can be integrated and examined.
Teaching AimsReview of the week
Introduction to Short Answer Question format
Revision session
Intended Learning OutcomesTo allow students to clarify issues arising from the first week of the Essentials of Clinical Medicine course.
To introduce students to the integrated nature of the majority of examination questions.
To emphasise the importance of group work and team working in the Medical School and NHS
46 Essentials of Clinical Medicine

Session 9Date: 14 September 2010Introduction to Clinical Scenarios and Evidence Based Medicine
Session Leader: Dr Jeremy ShearmanConsultant GastroenterologistSouth Warwickshire Foundation Trust
Email: [email protected]
OverviewA practical introduction to clinical case scenarios with some worked examples of clinical problem solving.
Teaching AimsTo illustrate some fundamental principles of history taking, physical examination and the use of investigations.
To demonstrate how technical aspects of clinical investigation are much easier if one applies basic patho-physiological principles to the history the patient has given.
To prompt a realisation that the key to clinical medicine is the ability to ask good questions.
Intended Learning OutcomesAfter this session you should:
Be able to understand why you might want to be a doctor Be keen to embark on a career in clinical medicine Be able to view the “pre-clinical” lectures in the context of the clinical course
Recommended ReadingLevel one – for everyoneEvidence based medicine: what it is and what it isn’tSackett et al BMJ 1996; 312: 71-72
Level two – for further reading for those who are interestedEvidence based medicine: How to practice and teach EBMStraus et al 2005 ElsevierISBN-10: 0-443-07444-5
Level three – for the “boffs”Clinical epidemiology – how to do clinical practice research 3rd Ed Haynes et al 2006 Lippencott Williams and WilkinsISBN-10: 0781745241
Group Work for Session 9Essentials of Clinical Medicine 47

Introduction to clinical scenarios and evidence based medicine (EBM)
In groups of three or four students the following case scenarios should be considered and discussed for no more than10mins. The groups should then discuss their responses with the other groups.
Case 2A 32 year-old plumber attends the clinic with his wife following a recent episode of rectal bleeding. He describes the blood as bright red and present predominantly on the toilet paper. His grandfather died at the age of 88 with bowel cancer.
What does the patient think is the cause of the problem?
Why has his wife come with him?
What is the most likely cause of the problem?
What other information would do need from the patient (i.e. what other
questions should you ask)?
What sort of investigation would be most worthwhile?
Case 3A 72 year-old man is referred to the clinic because of iron deficiency anaemia. He has no symptoms. He takes blood pressure medication, aspirin and clopidogrel since a coronary stent was placed 6 months ago.
What do you suspect might explain his test results?
Might there be other explanations?
What sort of investigations might the patient need?
Will those investigations seem logical to a patient with no symptoms?
How might you explain your concerns?
Case 4A 22 year-old drug user presents to the A+E department with a swollen left leg. Despite being on methadone he continues to inject heroin and the A+E department tell you that he has already attended their department 3 times that week.
Why might the patient have attended hospital?
What is the most likely cause of the swollen leg?
What sort of investigations might be useful?
What are your thoughts on treatment?
48 Essentials of Clinical Medicine

Case 5As a junior doctor you are called to a cardiac arrest.An 85 year-old man has collapsed. He had been admitted to hospital five days previously after a blackout. He is a retired public health doctor. He now lives on his own since the death of his wife 2 years previously. On admission his neighbours expressed concern about his memory. He has prostate cancer and is on hormonal therapy.By the time you arrive on the ward the nursing staff have initiated advanced life support and his ECG shows asystole (no electrical activity).
What do you think is the likely outcome?
What do you see as your priority?
To whom do you have a responsibility and why?
Essentials of Clinical Medicine 49

Session 10Date: 21 September 2010Introduction to PhysiologySession Leader: Dr David TweedieEmail: [email protected]
Overview
The session consists of two lectures and group work. The intention is to introduce some general concepts in physics and physiology.
Teaching Aims
To introduce and give insight into some general principles that will be needed in later modules.will be dealt with in greater Learning Outcomes and Reading needed
To refresh students knowledge on some basic physical principles underpinning human physiology
Intended learning outcomes
To understand some basic physical principles, and their importance in clinical practice
To understand of some of the processes in physiology and their importance in clinical practice
To prompt students to understand that physiology underpins the practice of medicine
50 Essentials of Clinical Medicine

Group work for session 10Pressure
Take each other’s blood pressure - the facilitators will show you how - and then answer the questions.
1. “You have found that the blood pressure is about ***mm Hg [mm of mercury].
2. How high would the column be if the manometer contained water?” [Hint: SG of mercury is 13.6 times that of water. Or - unscientifically, it is 13.6 times as heavy]
3. You are measuring CVP with a water manometer. You find that the pressure is 5 cm of water when the zero of the manometer is level with the heart. If someone lowers the patients bed by 10 cm without adjusting the zero, what will the new reading be?
4. When might this happen and does it matter?
Nerve, muscle & reflexes
Use the tendon hammer provided to try eliciting the knee jerk and ankle jerk reflexes.
Try the reflex with the joint as straight as possible, and at 90 degrees.
1. Which position gives a better ‘twitch’
2. Why do you think this is? (there must be tension in the muscle or tendon for demonstration of reflex)
3. Think about what this means for some of the other joint reflexes we regularly examine. (eg. for biceps reflex you may need to stretch the tendon with your finger before you can elicit reflex)
4. Try eliciting the same reflexes with your subject clenching their teeth hard.
5. Can you convince yourself of a difference? Why does this difference occur?
You will notice that it can be very difficult to be sure that a failure to elicit a reflex jerk is definitely due to decreased tone, and not operator technique! It is good technique always to compare sides but the only way to be sure is a lot of practice.
Fluid compartments
As a doctor in A&E you have to resuscitate a patient who has lost a lot of fluid. What fluid would you use – and why - if the fluid lost was a] blood because of trauma?
Essentials of Clinical Medicine 51

b] water because of e.g. severe diarrhoea?
If you had no blood what fluid would you use?
Acid / Base
Look at the following blood gas results and consider the questions below.Normal results are given below as a help.
Normal values:
pH 7.35 – 7.45 (lower = acidosis, higher = alkalosis)PO2 10 – 13 kPaPCO2 4 – 4.5 (high CO2 = resp. acidosis, low CO2 = resp alkalosis)BE -2 - +2 (negative = metab. acidosis, positive = met. Alkalosis)
1. This patient is complaining of a 12 hour history of abdominal pain.
pH 7.2pO2 13pCO2 4.0BE -8.0
On 21% oxygen.
1. Does the pH show an overall acidosis or an alkalosis?2. Is the problem respiratory or metabolic?3. What might be happening in the body tissues to cause this problem?4. What could the body do to compensate?
2. This patient is on a ventilator in the ITU
pH 7.8pO2 15pCO2 2.5BE -1.0
On 30% oxygen.
1. Does the pH show an overall acidosis or an alkalosis?2. Is the problem respiratory or metabolic?3. What do you think is causing the problem?4. What would the body do if it had control of respiration at this time?
3. This patient is on home oxygen 24% for long standing COPD.
pH 7.35
52 Essentials of Clinical Medicine

pO2 9.1pCO2 7.0BE +6.4
1. The pH appears normal, but what are the respiratory and metabolic components doing?
2. Which do you think is the underlying problem, and which is compensating?3. How long does it take for this ‘balance’ to happen?
Essentials of Clinical Medicine 53

Session 11Date: 28 September 2010Introduction to MoleculesSession Leader: Dr Graham LaddsEmail: [email protected]
Overview
This session is aim at refreshing some of the session cover in the first five weeks of the molecules module. We will cover general principles of Genetics, Membrane structure, transport of ions, receptors and cellular signalling and protein structure. A brief question and answer session will enable any problems students have had on the molecules module to be discussed.
Teaching Aims (1) To help with any difficulties that students are having with the material
covered in Molecules in the human body to date. Please let me know any topics or concepts that you want covered.
(2) Introduce a fully integrated ESA-style question, so students can see how the material from different modules fits together, and have practice doing a question.
Intended Learning Outcomes
To be able to access support for Molecules in the human body.
To gain understanding of how learning from modules is integrated within the ESA questions and practice doing a question.
Structure of the Session:
1:45 to 4:00 Revision of Molecules in the human body – Key/Difficult Issues Lecture
4:00 to 4:30 Questions using ESA format
4:30 to 5:00 Questions from students
Required and Recommended Reading
None.
However, please let us know any topics or concepts that you want covered by emailing Graham Ladds on [email protected].
54 Essentials of Clinical Medicine

Session 12Date: 5 October 2010Respiratory and Cardiovascular Anatomy
Session Leader: Dr David TweedieEmail: [email protected]
Teaching Aims
To introduce students to the anatomy of cardiovascular and respiratory systems.
Objectives Intended Learning Outcomes
After the session students should have a basic understanding of:
Basic cardiovascular physiology; to help understanding of pulsatile, one-way flow and the double circulation of blood
Structure and function of blood vessels Structure of heart Overview of vascular tree
Basic respiratory physiology; to help understanding of tidal flow of respiration Overview of respiratory system Structure of thorax Structure of airways Structure of lungs
Surface anatomy Bony landmarks; sternum, spine, ribs Heart Lungs
Essentials of Clinical Medicine 55

Session 13Date: 12 October 2010Session Leader: Dr Alex ConnerEmail: [email protected]
OverviewAll of the body’s functions are carried out by collections of cells all working together. Just like with normal physiology (understanding the parts and how they work), this session will describe the average cell and how they can specialise. There will be an emphasis on the normal functions of the cell allowing most of the body’s processes to occur. The disruption of these processes and the relevance for medicine will be discussed.
Teaching AimsThis session will describe the fundamental cell biology needed to understand how the body works at a cellular level.
The core functions of cells will be described. This will include the production of proteins from DNA, the movement of proteins around the cell and the relevance of ions for cellular function. This is key to understanding all of the processes involved in
Knowing the effects of treatments on cellular components will allow a more complete understanding of therapeutic intervention.
Intended Learning Outcomes1. To have a broad understanding of cell biology including the names, function and clinical relevance of the cell’s main constituents.
2. To understand the general physiology of cellular actions with an emphasis on cellular trafficking and signalling, neuronal transmission and muscle contraction.
56 Essentials of Clinical Medicine

Group Work:Cell Physiology
Using the model and list of terms given below correctly label the typical eukaryotic cell:
List of Terms
Ribosomes Golgi complex Cytoplasm Plasma Membrane Mitochondria Vacuole Nuclear envelope Microtubule Chromatin Nuclear pore Rough ER Smooth ERNucleolus Lysosome Microfilaments Centriole Questions:
1. Describe the contents and function of the nucleus.
2. Describe the functions of the ER
3. Outline the physiological importance of the cell membrane
4. Describe the structure and function of the mitochondria.
“The Central Dogma” is the requirement of a cell to convert DNA to mRNA to protein. The DNA is held in the nucleus and transcribed to mRNA. The mRNA is translated into protein in the cytoplasmic via the rough endoplasmic reticulum. This process is all held in place by the membrane and is provided with energy by the mitochondria.
5. Can you think of ways in which the organelles/features outlined in questions 1-4, may be involved in the onset or treatment of diseases?
i Nucleus
ii ER
iii Cell MembraneEssentials of Clinical Medicine 57

iv Mitochondria.
6. Label the cells a-f
a b c d e f
58 Essentials of Clinical Medicine

Session 14Date: 19 October 2010Session Leaders: Dr Dawn CollinsEmails: [email protected]
Overview
This session will highlight the gross structure and functions of the most fascinating system in the body. A thorough understanding of the structure and function of the nervous system is vital for understanding how the body works as the nervous system forms the hub that controls all bodily functions, from thinking and feeling to eating and reproducing. By understanding how the nervous system works and how changes in the activity within this system impacts on the other systems, you can figure out how changes and deficiencies may cause the symptoms that you associate with different diseases and disorders.
Teaching Aims
In the previous session, the cellular composition of the nervous system was discussed. This session will expand on this and discuss the gross anatomy and functioning of the nervous system and how you can relate this to the functioning of the whole body. A good understanding of how a normally functioning nervous system works will allow you to predict the outcomes and symptoms that you might observe in clinical situations when a patient has suffered damage to their nervous system.
The nervous system has been divided into many components according to structure and function. These components and how they interact to link brain to body will be discussed. The main classification of the nervous system into central and peripheral components and the relationship between the two will be discussed. A review of the gross anatomy of the central nervous system will be provided and give insight into how different areas control different functions and how this can be applied in clinical cases. The link between central and peripheral nervous system will be reviewed and the control of somatic and visceral functioning elucidated.
Intended Learning Outcomes
At the end of the session and the prescribed reading the student will be able to:
Understand the basic arrangement of the nervous system into, for example: central and peripheral, somatic and visceral components and the structures that comprise and are involved in the control of these elements
Describe the structure and functional component parts of the brain Describe the structure and function of the spinal cord State the component parts of the peripheral nervous system and understand
the signals that peripheral nerves carry Understand how the function of the nervous system can be tested in the
clinic
Essentials of Clinical Medicine 59

Structure of the Session
The structure of the session will be confirmed on the website closer to the date, but will consist of a lecture session followed by group work and/or self-directed study.
Cross-Modular Themes
No human function can be understood thoroughly without an understanding of how the nervous system operates as it is central to the control of every aspect of the body. The information discussed in this session will be utilised in every other biological module you study. Testing of the nervous system is a vital component that you will learn in Clinical Skills in semester 1; the anatomy will support your understanding of clinical conditions and the effects of lesions occurring in different regions of the CNS and will become more relevant as you move through the semesters.
Handouts and other relevant Information
The lectures will be placed on the Medical School Intranet and various materials will be handed out for the small group sessions.
Required and Recommended Reading
We recommend that you have access to a basic physiology book that details the basic anatomy and functioning of the nervous system for revision purposes, this knowledge can be expanded on as you work through Phase 1 and give you a good grounding for the Neurobiology module in Semester 3.
For lighter reading, any books by Oliver Sacks (e.g. The Man who Mistook his Wife for a Hat; An Anthropologist on Mars; Islands of the Colour Blind), will give you a fascinating insight into the life of a neurologist and the inspiring cases that you may encounter.
60 Essentials of Clinical Medicine

Group Work Questions
Q1. Indicate the cerebral regions of the following lobes and note which major function they control.
Frontal
Parietal
Temporal
Occipital
Q2. On the same figure, show the position of the central sulcus, lateral sulcus and cerebellum.
Q3. What is the precentral gyrus mainly involved in?
Q4. And the postcentral gyrus?
Q5. Regions of the brain can also be defined according to their cerebral structure, these areas have been given numbers. What are the numbers known as?
Essentials of Clinical Medicine 61

Q6. On the diagram of the brain below, indicate the areas involved with
Vision
Hearing
Motor function
Sensation
Taste
Speech
Q7. What would the effect of losing the blood supply to the areas labelled 17?
Q8. Areas 41 & 42 are also know by what name (clue: involved in language)?
Q9. Label the follow diagram (and add any other areas you know). In what plane is the figure made?
62 Essentials of Clinical Medicine

Q10. Label the following figure of the spinal cord
Q11. Label the following external view of the base of the skull
Q12. Label the following internal view of the base of the skull
Essentials of Clinical Medicine 63

Q13. Which lobe of the brain sits in the anterior fossa of the skull?
Q14. Which lobe of the brain sits in the middle cranial fossa of the skull?
Q15. Which lobe of the brain sits in the posterior cranial fossa of the skull?
Q17. Label the spinal and vertebral levels. Note how the offset between levels changes as you go down the vertebral column.64 Essentials of Clinical Medicine

Session 15
Essentials of Clinical Medicine 65

Date: 26 October 2010Introduction to Imaging TechniquesSession Leader: Dr Fraser MillardEmail: [email protected]
Overview:
What do you think is the most important scientific invention? To celebrate its centenary in 2009, the Science Museum conducted a poll to answer this question. The winner was the x-ray machine.
X-rays were discovered in 1895 by Wilhelm Röntgen who received the first Nobel Prize in Physics in 1901. Further imaging techniques are now widely available, Ultrasound, Computed Tomography (Allan Cormack and Godfrey Hounsfield, the Nobel Prize in Medicine 1979), Magnetic Resonance Imaging (Paul Lauterbur and Sir Peter Mansfield, the Nobel Prize in Medicine 2003), and Nuclear Medicine. These techniques are used to show anatomy, pathology and more recently the function of the human body in both health and disease. Technological advances have also led to the development of fine instruments and devices which may be introduced into the body to obtain images and perform interventions to treat patients. The development of the microchip and modern computing have revolutionised the amount of information obtained by these imaging techniques and how this information is stored and shared between providers of healthcare. As a result there has been a huge expansion in the role of imaging in the investigation and treatment of patients. However, as well as these benefits, imaging also has risks from the exposure to ionising radiation and magnetic fields, and complications from contrast agents such as allergic reactions and renal failure, interventional procedures, and over diagnosis and over treatment.
When you qualify as Doctors in less than four years time, these techniques will become available for you to request in your practice. How may imaging help you to manage your patients? Which is the best imaging technique to request and how will it affect your patients? How will you interpret and use the information generated? By the end of the afternoon I hope you will have tasted a flavour of this topic and whetted your appetites to find out more.
Teaching Aims and Intended Learning Outcomes:
An understanding of the role of imaging in patient management The principles of interpretation of basic radiological studies A basic understanding of the imaging techniques available and their
advantages and disadvantages An introduction to radiation protection of the patient An understanding of what the patient will experience when undergoing
investigations in the radiology department The role of the imaging department
Preparation for the Session:
66 Essentials of Clinical Medicine

To read the Introduction to Weir J, Abrahams P, Spratt J, Salkowski L.. Imaging Atlas of Human Anatomy. Mosby Elsevier 2010 Fourth Edition.See WMS library or intranet.
Recommended Reading:
Weir J, Abrahams P, Spratt J, Salkowski L. Imaging Atlas of Human Anatomy. Mosby Elsevier, 2010 Fourth Edition.See WMS library or intranet.
Patel P. Lecture Notes: Radiology. Blackwell Publishing, 2010 Third Edition.
The Royal College of Radiologists. Making the best use of clinical radiology services: referral guidelines. London: The Royal College of Radiologists, 2007.
Additional Information
Imaging Techniques - their basic principles - usages and relevance to anatomical studies and clinical medicine are only too self evident as modern medicine relies so much on exact diagnosis often confirmed by imaging. This session will introduce you to the anatomical terminology of various views and techniques of imaging. It will also show you why certain methodologies are best for certain clinical situations and how the anatomy is shown in different ways by different modalities ie ultrasound looks like a snowstorm at first but is the most reliable method to diagnose someone with abdominal pain, whereas an MR (magnetic Resonace ) imaging is the best way to see if an intervertebral disc is prolapsed and yet a crush fracture of the adjacent vertebra may be best visualised by a CT (Computerised Tomogram) scan. We will also see examples of most common modern imaging techniques and how the terminology of anatomy is used in their description of the normal and pathological conditions. All modules and all clinicians use imaging so it is important to learn the normal anatomy of most structures so as to be able to recognise pathology in a clinical setting
"ALL YOU NEED TO KNOW ABOUT MODERN IMAGING BUT NEVER DARED TO ASK"
DIAGNOSTIC X-RAY
X-rays are a form of electromagnetic radiation given off as electrons change their orbits around a nucleus; they have a wavelength and energy between low energy visible light and high energy cosmic radiation. The use of X-rays derives from their energy. The body is almost completely opaque to low energy visible light and completely transparent to high energy cosmic rays, whereas X-rays are differentially absorbed by body constituents. X-rays pass easily through air or fatty tissues (RADIO-TRANSPARENT) but substances such as bone, calcium stones or heavy metals absorb most of the X-rays (RADIO-OPAQUE).
A patient standing between an X-ray source and a photographic plate will cast a varying shadow on the plate - an X-ray photograph of the body constituents. X-ray
Essentials of Clinical Medicine 67

negatives are used. This means the less dense a material, the more X-rays will pass through onto the plate, producing a darker image.
The X-rays which do not pass on the plate release their energy inside the body, damaging the molecules they collide with. This is the mechanism by which X-rays are harmful - the effect is particularly seen on rapidly dividing cells, e.g. skin, gut, the fetus or gonadal cells.
An X-ray can be taken as a single exposure of an area of the body, i.e. a PLAIN X-RAY, but several other techniques are used.
The direction that the beam passes through the subject determines the name of the view, i.e. a postero-anterior chest X-ray is taken with the subject's back towards the beam and chest on the "cold" X-ray plate. This view is ideal for judging heart size and lungs whereas the antero-posterior chest X-ray is much better for viewing the vertebral bodies. Can you think why?
CONTRAST STUDIES
Body cavities, the lumen of vessels (e.g. arteries, veins, ureters) or viscera (e.g. bowel) can be further delineated by the use of suspensions of heavy metals or halogens.
These contrast media can be introduced in a variety of ways:
1) by direct introduction (barium enema)2) by injection (arteriograms)3) via injection or ingestion into the bloodstream and then concentration by
specific organs [e.g. intravenous urogram (kidneys), oral cholecystogram (gall bladder)].
X-ray pictures are taken before and after introduction of the contrast media and one shot converted into a positive print. When the two are superimposed any unchanging bone and soft tissue shadows will almost vanish - SUBTRACTION TECHNIQUE. This may also been performed via a computer as in DIGITAL SUBTRACTION ANGIOGRAPHY (DSA).
ANGIOGRAPHY
Access to the arterial system to produce an arteriogram (angiogram) is usually obtained by puncture and catheterisation of a femoral artery under local anaesthetic. Radiographic contrast medium is then injected into the vessel in the area under examination. If for some reason access via the femoral artery is not possible (eg. iliac occlusive disease or the presence of a graft) alternative sites such as the brachial or axillary artery can be used. Translumbar aortography (TLA), a method of arteriography involving direct percutaneous puncture of the aorta, is now less commonly employed as it does not allow selective catherisation of aortic branches and hence percutaneous interventional vascular procedures cannot be performed. The development of new technology has meant that the aorta and main upper and lower limb arteries can be visualised from an intravenous injection of contrast medium (into the brachial vein, superior vena cava or right atrium). obviating the need for arterial puncture in some patients. 68 Essentials of Clinical Medicine

This technique employs DIGITAL SUBTRACTION ANGIOGRAPHY (DSA) whereby unwanted background information is 'subtracted' leaving only an image of the blood vessels. Images of arteries obtained by injection into a vein are referred to an intravenous DSA examination (IV DSA). DSA images of arteries can, of course, be obtained by direct intra-arterial injection (IA DSA).
Manual photographic subtraction of background information can also be performed with conventional (non digital) arteriography. Subtraction, either photographic or digital, is used in cases where fine vascular detail is required and can be simply recognised by the fact that the arteries appear black as opposed to white as on an unsubtracted film. The veins may be visualised in the same way as arteries, e.g. by direct puncture and catheterisation (via the femoral vein in most instances). The veins of the upper and lower limbs are imaged by injecting contrast medium via an 18G or 20G needle placed in a peripheral vein e.g. the dorsum of the foot or hand or the cubital fossa. Alternatively if imaging from an arterial injection over a prolonged period of time, the arterial, capillary and venous phases can be recorded and venous anatomy visualised. This is a particularly useful way of imaging the portal venous system without necessitating direct trans-splenic or trans-hepatic puncture.
NUCLEAR MEDICINE - RADIONUCLIDES
Nuclear Medicine is a medical speciality concerned with the application of radionuclides to patients. Most of these applications remain within the field of diagnosis, whilst some applications of radionuclides are made for therapeutic purposes. Examples of the latter include the administration of iodine-131 for the treatment of patients suffering from hyperthyroidism or thyroid cancer, the administration of P-32 as treatment of POLYCYTHAEMIA VERA (disease of too many red cells), the intra-cavity administration of therapeutic doses of radionuclides for the treatment of malignant effusions, the intra-articular administration of radionuclides for the treatment of benign chronic arthritic effusions, and so on.
In most of the diagnostic procedures in nuclear medicine, trace amounts of suitable radionuclides linked to suitable compounds (radio-pharmaceuticals) are administered to patients in order to investigate organ or tissue function and metabolism. Indirectly, information concerning size, shape and displacement or organs can be recorded. With suitable radiation detectors (gamma cameras and scanners), often associated with computer processed information, the arrival, distribution and disappearance of a radiopharmaceutical can be monitored over a region of interest or a particular organ.
Time activity curves and/or images are often displayed in order to analyse and investigate the patient's condition. Time activity curves are used in the measurement of cerebral, hepatic or renal blood flow, whilst numerical data analysis can be applied to the investigation of myocardial perfusion, glomerular filtration, and a variety of other indices of organ physiology. The images recorded (often called scans) are frequently used to investigate the presence of primary or secondary cancer in a variety of organ systems. Tumours or metastases can be detected either as areas with increased activity ('hot spots') or as areas of reduced activity ('cold' spots). 'Hot' spot detection is used in the brain and in bone, whilst 'cold' spot detection is often used in the liver, lungs and kidneys.Essentials of Clinical Medicine 69

The most commonly used radionuclide (99M-Technetium) is linked (labelled) to compounds such as phosphates for bone scanning, chelates for brain and kidney scanning, or colloids for liver, spleen and bone marrow scanning, or to red cells for blood pool imaging.
Radiopharmaceuticals act as "magic bullets" for the localisation and lateralisation of disease. The relevant merits of these diagnostic procedures include the absence of mortality and even morbidity in all its studies, the low radiation doses delivered to patients when compared with conventional radiological techniques, the absence of side-effects or discomfort to patients and the overall economy of these investigations. Radionuclide bone scans have replaced X-ray skeletal surveys in the search for skeletal metastases – “hot spots” (frequently encountered in patients suffering from carcinoma of the breast, prostate, lungs, thyroid and kidney). Scans have considerably reduced the need for invasive angiography in the detection of embolic lung disease and reduce the need for invasive catheterisation procedures of the heart in the evaluation and follow-up of patients suffering from myocardial ischaemia. These scans can also replace contrast IVU studies in the assessment of renal function, and eliminate the need for elaborate 24 hour urine collection in measurements such as creatinine clearance. Radionuclide treatment of hyperthyroidism is today a commonly used and most effective method of controlling this disease.
COMPUTED TOMOGRAPHY
The limitation of all plain radiographic techniques is the two dimensional representation of a three dimensional structure. The linear attenuation coefficients of all the tissues in the X-ray beam form the image.
Computed tomography (CT) obtains a series of different angular X-ray projections which are processed by a computer to give a section of specified thickness. The CT image comprises a regular matrix of picture elements (pixels). All the tissues contained within the pixel attenuate the X-ray projections and result in a mean attenuation value for the pixel. This value is compared with the attenuation value of water and is displayed on a scale (the Hounsfield scale). Water is defined as 0 Hounsfield units (HU) and the scale is 2000HU wide. Air typically has a HU number of -1000; fat is approximately -100 HU; soft tissues are in the range +20 to +70 HU, and bone is greater than +400 HU.
The CT machine consists of a rigid metal frame with an X-ray tube sited opposite to a set of detectors. In early designs the tube and detectors scanned across the patient and then rotated to a different position ("translate-rotate"). Current third generation CT machines have a wider detector array and an X-ray fan beam which encompasses the whole patient. All the views per slice can be collected simultaneously so that the tube and detectors only rotate around the patient. Routine acquisition times are 2-4 seconds, though a variant of the design utilises a constantly rotating tube/detector system which permits sub-second scan times.
All CT machines, of whatever generation, share similar components. The detectors are either gas ionisation chambers, or scintillation crystals linked to photomultiplier tubes. The signal is digitised by an analogue-to-digital converter in the gantry. The digitised signal is transferred to the image processing computer 70 Essentials of Clinical Medicine

and subsequently displayed on the operators console. Images are usually photographed on medical recording film (hard copy) using optical or laser cameras. For long term storage the data is transferred to magnetic media (tape or disc) or to optical disc. These discs can then be stored in an imaging "Juke Box".No specific preparation is required for examinations of the brain, spine, musculoskeletal system and chest. Studies of the abdomen and pelvis almost always require opacification of the gastrointestinal tract using a solution of dilute contrast medium (either water soluble or a barium compound). Generally 750-1000 ml is given orally 30-60 minutes prior to imaging, with the final 300 ml taken as the patient enters the examination room. The large bowel may also be opacified by a solution of contrast medium administered rectally, either in a preparation room or on the CT table. Examinations of the female pelvis are often performed after the insertion of a vaginal tampon to facilitate interpretation.
Identification of vascular structures may be made on the basis of anatomy alone but may require the intravenous injection of water soluble contrast medium. Techniques vary accordingly to the individual case but the most common method is to inject a bolus of 50 ml followed by a rapid infusion of 50 ml using contrast medium of 300-370 mg iodine/ml. In the last few years the new generation 64 slice scans with 3D ROTATIONS have added a new dimension to anatomy learning - you will see me use these in future modules.
ULTRASOUND
In comparison with all the other images ultrasound images do not depend on the use of electromagnetic wave forms. It is the properties of high frequency sound waves (longitudinal waves) and their interaction with biological tissues that go to form these 'echograms'.
A sound wave of appropriate frequency (diagnostic range 3.5 - 10 MegaHertz) is produced by piezo-electric principles. The size and shape of the emitting crystal and its resonant frequency are important factors in determining the course of the sound beam within the tissues to be examined.
As the beam passes through tissues, two important effects determine image production:
(i) Attenuation: This is the loss of energy from the system and is a consequence of absorption and reflection, refraction and beam divergence out of the range of the receiver.
(ii) Reflection within the range of the receiver: It is the reflected sound waves (echoes) that combine to produce the image and the image texture is dependent upon differences in acoustic impedance between different tissues. Ultrasound imaging systems are sensitive to the very small changes in acoustic impedance within soft tissue structure/ranges.
In modern ultrasound imaging practice, by applying these principles, sophisticated hardware has been developed that converts the pulse-echo system, briefly described above, into a real-time tomographic image. Addition of the facility to measure movement (principally cardiac valves and flowing blood) by ultrasound
Essentials of Clinical Medicine 71

using the Doppler principle has lead to the development and wide availability of Duplex Scanners.
It is the effects of shadowing and enhancement within an ultrasound image that are of paramount importance. Systems are designed assuming an average attenuation through a depth of tissue and balanced to give an even signal intensity for deep and superficial tissues. Tissues causing shadowing are: fibrous, calcific or gaseous. Tissues causing enhancement are fluids.
The advantages of an ultrasound imaging system in clinical practice are: Non-ionising radiation is used. The safety of ultrasound at diagnostic power levels has been well proven over a long time now. Main worries were of thermal effects to local tissues and cavitation. Soft tissue images are obtained without the need for contrast agents. Equipment is relatively cheap and mobile. Ultrasound machines can be taken to the patient's bedside if necessary. Multiplanar and non-organ specific imaging is possible. Real time images allow immediate operator-patient interation to maximise the diagnostic potential of the examination and have lead to their use in guiding -interventional procedures (biopsy and drainage). Patients find the system very acceptable as it required only light pressure on the skin.
The limitations of an ultrasound imaging system are:
(i) The quality and diagnostic potential of the examination are dependent on the skill and expertise of the OPERATOR.
(ii) Ultrasound systems are unable to image tissue - gas and tissue-bone interfaces. Gas and bone containing structure cannot be imaged, and their presence obscures deeper lying tissues.
By having available a selection of different ultrasound transducers of varying frequencies and focusings, shapes and sizes, the range of imaging has been maximised:
Ultrasound imaging is a real-time, interactive process and the quality of the images is NOT best appreciated from hard-copy. (Printed format).So these are best seen on VIDEO / CDRom.
MAGNETIC RESONANCE IMAGING
MRI combines a strong magnetic field and radiofrequency energy to study the distribution and behaviour of hydrogen protons in fat and water.
The spinning proton of the hydrogen nucleus can be thought of as a tiny bar magnet, with a north and south pole. In the absence of an external magnetic field, the magnetic moments of all the protons in the body are randomly arranged. However when the patient is placed in a strong magnetic field these magnetic moments align either with or against the field lines of the magnet. There is a small excess of magnetic moments which align with the field so a net magnetic vector is established.
Radiofrequency energy is used to generate a second magnetic field, perpendicular to the static magnetic field of the machine.72 Essentials of Clinical Medicine

The result of this second magnetic field is to rotate or "flip" the protons away from the static magnetic field; the amount of rotation depends on the quantity of RF energy absorbed. Once the RF field is switched off, the protons experience only the effects of the static magnetic field and flip back to their original position. This return to the equilibrium state is called "relaxation" and during it protons emit the RF energy which they had acquired. This energy is detected by the antenna in the MRI machine, digitised, amplified, and finally spatially encoded by the array processor. The resulting images are displayed on the operator's console and can be recorded on hard copy, for viewing, or transferred to magnetic tape or optical disc, for storage.
MRI systems are graded according to the strength of the magnetic field they produce. High field systems are those capable of producing a magnetic field strength of 1-2-4-8 Tesla (10,000-20,000 Gauss), mid-field systems operate at 0.35-0.5 T and low field systems produce a field strength of less than 0.2 T. Mid and high field systems use superconducting magnets in which the coils of copper wire are kept in a superconducting state (-269°C) by being immersed in an insulated helium bath. Electromagnets are fitted in resistive systems and are limited by heating factors to 0.35 T. The third type use permanently magnetised metal cores and are of low field strength owing to the massive weight. MRI does not cause any recognised biologic hazard. Patients who have any form of pacemaker or implanted electroinductive device must NOT be examined. Other prohibited items include ferromagnetic intracranial aneurysm clips, certain types of cardiac valve replacement, and intraocular metallic foreign bodies. Generally it is safe to examine patients who have extracranial vascular clips and orthopaedic prostheses, but these may cause local artefacts. Loose metal items must be excluded from the examination room and beware of your credit cards!
The preparation for an MRI examination is simple. Patients wear metal free clothes and must answer a strict safety questionnaire.
MRI images may be obtained in ANY plane, but axial, coronal and sagittal views are the most common presented. An intravenous injection of contrast medium (a gadolinium complex) may be given to enhance tumours, inflammatory and vascular abnormalities.The next decade will see the increased use clinically of MR ANGIOGRAPHY (MRA) - where the flow of blood in vessels is picked up by the detectors without the use of contrast medium or any interventional procedure- now commonly used in assessing brain vasculature.
Essentials of Clinical Medicine 73

Session 16Date: 2 November 2010Molecules in the Human Body
Session Leader: Dr Graham LaddsEmail: [email protected]
Overview
This session is aim at refreshing some of the session cover in the first five weeks of the molecules module. We will cover general principles of Genetics, Membrane structure, transport of ions, receptors and cellular signalling and protein structure. A brief question and answer session will enable any problems students have had on the molecules module to be discussed.
Teaching Aims (3) To help with any difficulties that students are having with the material
covered in Molecules in the human body to date. Please let me know any topics or concepts that you want covered.
(4) Introduce a fully integrated ESA-style question, so students can see how the material from different modules fits together, and have practice doing a question.
Intended Learning Outcomes
To be able to access support for Molecules in the human body.
To gain understanding of how learning from modules is integrated within the ESA questions and practice doing a question.
Structure of the Session:
1:45 to 4:00 Revision of Molecules in the human body – Key/Difficult Issues Lecture
4:00 to 4:30 Questions using ESA format
4:30 to 5:00 Questions from students
Required and Recommended Reading
None.
However, please let us know any topics or concepts that you want covered by emailing Graham Ladds on [email protected].
74 Essentials of Clinical Medicine

Session 17
Date: 9 November 2010
Homeostasis
Session Leader: Professor Peter StanfieldEmail: [email protected]
OverviewClaude Bernard (1878) wrote that: ‘The constancy of the internal environment is the condition for a free and independent life’. Homeostasis is the term now used to describe this constancy and the study of the physiological mechanisms that regulate the internal environment. Both nervous and endocrine systems provide the feedback systems that perform such regulation.Teaching AimsThe session aims to introduce the concept of homeostasis as central to thinking physiologically about human function. Body fluid balance will be used as exemplar to illustrate the principles.Intended learning outcomesAt the end of the session, it is intended that learners have had the opportunity to: understand the concept of homeostasis; understand the concept of balance in body water and sodium content; understand the compartmentalisation of the fluid compartments of the body and
the equilibria that exist between them; understand in general how water intake and loss are regulated; understand the concepts of osmolality and volume as important regulated
quantities; and understand in outline the roles of the nervous system and of hormones in the
regulatory processes.
Structure of the session13.45 – 14.45 Fluid balance and the equilibria between compartments of the
body fluids (Lecture Theatre)15.00 – 16.00 Group work (Seminar Rooms)16.00 – 17.00 Homeostatic mechanisms and the regulation of body water
and extracellular fluid volume (Lecture Theatre)
Cross Modular ThemesHomeostatic mechanisms are central to understanding systemic, integrated function of the human body and these mechanisms are upset in many disease states. Body fluid regulation will be studied in more detail in the module on the urinary tract in semester 3. But the principles have relevance to many of the modules of phase I, and body fluid regulation is particularly important to the normal function of the cardiovascular system. For example, as clinicians, helping a patient manage their heart failure, you will reduce the amount of work the failing heart has to do by giving drugs – diuretics and inhibitors of aldosterone production or action - that will reduce the extracellular fluid volume.
Essentials of Clinical Medicine 75

Other relevant informationBefore the session, lectures and the group work problems will be made available by way of the medical school intranet.
Recommended readingHuman Physiology: The Basis of Medicine by G Pocock & CD Richards. 3rd edition
OUP 2006. Section 1.3: Homeostasis; Chapter 28: The regulation of body fluid volume.
76 Essentials of Clinical Medicine

Session 18Date: 16 November 2010Integrated Session
Session Leader: Dr Alex Conner/Dr David TweedieEmail: [email protected]
OverviewInteractive session with the Clinical Education Fellows and group leaders to aid understanding of previous sessions and to clarify any problems that have arisen.
Teaching AimsRevision session
Intended Learning OutcomesTo allow students to clarify issues arising from the Essentials of Clinical Medicine course. To ensure that the correct teaching is provided for these sessions, it is essential that students email the module leads in the week before this session.
Essentials of Clinical Medicine 77