viro finals.docx
TRANSCRIPT
HEPATITIS VIRUSES
o 5 types: A-Eo main target organ: livero differ: structure, mode of replication, course of disease, mode
of transmissiono classic signs: jaundice plus elevated liver enzymeso NB. Histopathologic lesions in the liver are identical regardless
of the virus type
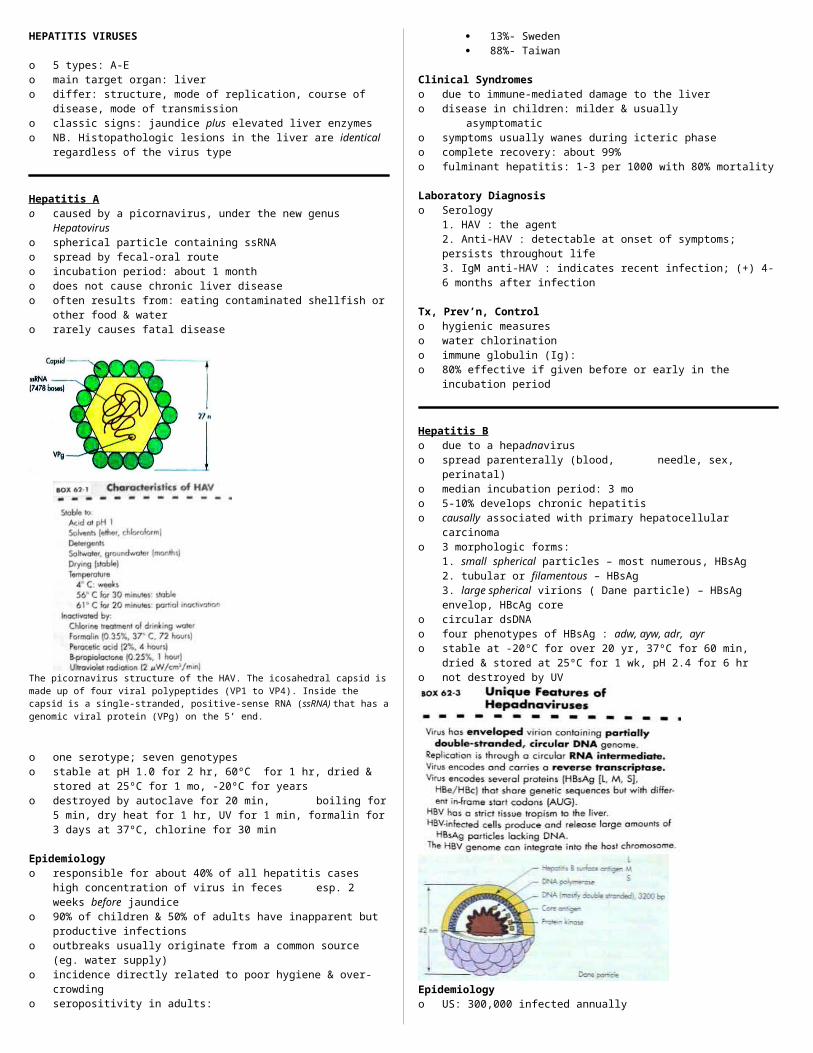
Hepatitis Ao caused by a picornavirus, under the new genus Hepatoviruso spherical particle containing ssRNA o spread by fecal-oral routeo incubation period: about 1 montho does not cause chronic liver diseaseo often results from: eating contaminated shellfish or other food
& watero rarely causes fatal disease
The picornavirus structure of the HAV. The icosahedral capsid is made up of four viral polypeptides (VP1 to VP4). Inside the capsid is a single-stranded, positive-sense RNA (ssRNA) that has a genomic viral protein (VPg) on the 5’ end.
o one serotype; seven genotypeso stable at pH 1.0 for 2 hr, 60ºC for 1 hr, dried & stored at 25ºC
for 1 mo, -20ºC for yearso destroyed by autoclave for 20 min, boiling for 5 min, dry
heat for 1 hr, UV for 1 min, formalin for 3 days at 37ºC, chlorine for 30 min
Epidemiologyo responsible for about 40% of all hepatitis cases high
concentration of virus in feces esp. 2 weeks before jaundiceo 90% of children & 50% of adults have inapparent but
productive infectionso outbreaks usually originate from a common source (eg. water
supply)o incidence directly related to poor hygiene & over-crowdingo seropositivity in adults:
13%- Sweden 88%- Taiwan
Clinical Syndromeso due to immune-mediated damage to the livero disease in children: milder & usually asymptomatico symptoms usually wanes during icteric phaseo complete recovery: about 99%o fulminant hepatitis: 1-3 per 1000 with 80% mortality
Laboratory Diagnosiso Serology
1. HAV : the agent2. Anti-HAV : detectable at onset of symptoms; persists throughout life3. IgM anti-HAV : indicates recent infection; (+) 4-6 months after infection
Tx, Prev’n, Controlo hygienic measureso water chlorinationo immune globulin (Ig): o 80% effective if given before or early in the incubation period
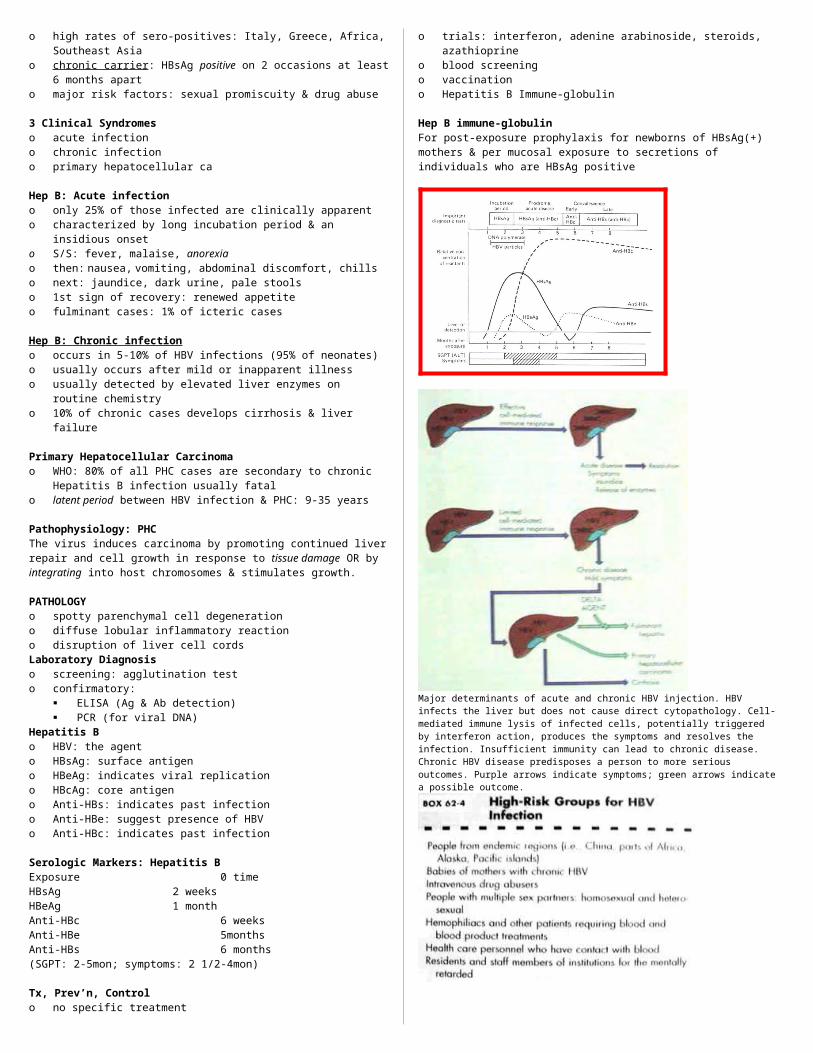
Hepatitis Bo due to a hepadnaviruso spread parenterally (blood, needle, sex, perinatal)o median incubation period: 3 moo 5-10% develops chronic hepatitiso causally associated with primary hepatocellular carcinomao 3 morphologic forms:
1. small spherical particles – most numerous, HBsAg2. tubular or filamentous – HBsAg3. large spherical virions ( Dane particle) – HBsAg envelop, HBcAg core
o circular dsDNAo four phenotypes of HBsAg : adw, ayw, adr, ayro stable at -20ºC for over 20 yr, 37ºC for 60 min, dried & stored
at 25ºC for 1 wk, pH 2.4 for 6 hro not destroyed by UV
Epidemiologyo US: 300,000 infected annuallyo high rates of sero-positives: Italy, Greece, Africa, Southeast
Asiao chronic carrier : HBsAg positive on 2 occasions at least 6
months aparto major risk factors: sexual promiscuity & drug abuse
3 Clinical Syndromeso acute infectiono chronic infectiono primary hepatocellular ca
Hep B: Acute infectiono only 25% of those infected are clinically apparento characterized by long incubation period & an insidious onseto S/S: fever, malaise, anorexiao then: nausea, vomiting, abdominal discomfort, chillso next: jaundice, dark urine, pale stoolso 1st sign of recovery: renewed appetiteo fulminant cases: 1% of icteric cases
Hep B: Chronic infection
o occurs in 5-10% of HBV infections (95% of neonates)o usually occurs after mild or inapparent illnesso usually detected by elevated liver enzymes on routine
chemistryo 10% of chronic cases develops cirrhosis & liver failure
Primary Hepatocellular Carcinomao WHO: 80% of all PHC cases are secondary to chronic Hepatitis
B infection usually fatalo latent period between HBV infection & PHC: 9-35 years
Pathophysiology: PHCThe virus induces carcinoma by promoting continued liver repair and cell growth in response to tissue damage OR by integrating into host chromosomes & stimulates growth.
PATHOLOGYo spotty parenchymal cell degenerationo diffuse lobular inflammatory reactiono disruption of liver cell cordsLaboratory Diagnosiso screening: agglutination testo confirmatory:
ELISA (Ag & Ab detection) PCR (for viral DNA)
Hepatitis Bo HBV: the agento HBsAg: surface antigeno HBeAg: indicates viral replicationo HBcAg: core antigeno Anti-HBs: indicates past infectiono Anti-HBe: suggest presence of HBVo Anti-HBc: indicates past infection
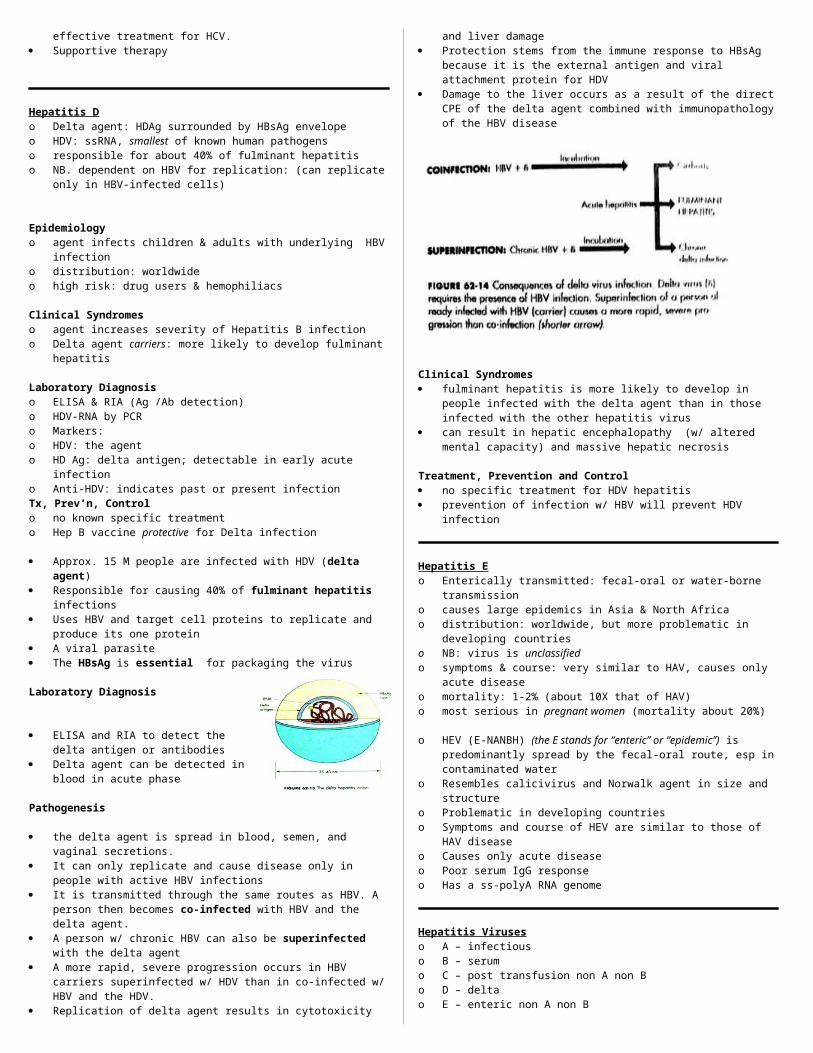
Serologic Markers: Hepatitis BExposure 0 timeHBsAg 2 weeksHBeAg 1 monthAnti-HBc 6 weeksAnti-HBe 5monthsAnti-HBs 6 months(SGPT: 2-5mon; symptoms: 2 1/2-4mon)
Tx, Prev’n, Controlo no specific treatmento trials: interferon, adenine arabinoside, steroids, azathioprineo blood screeningo vaccinationo Hepatitis B Immune-globulin
Hep B immune-globulinFor post-exposure prophylaxis for newborns of HBsAg(+) mothers & per mucosal exposure to secretions of individuals who are HBsAg positive
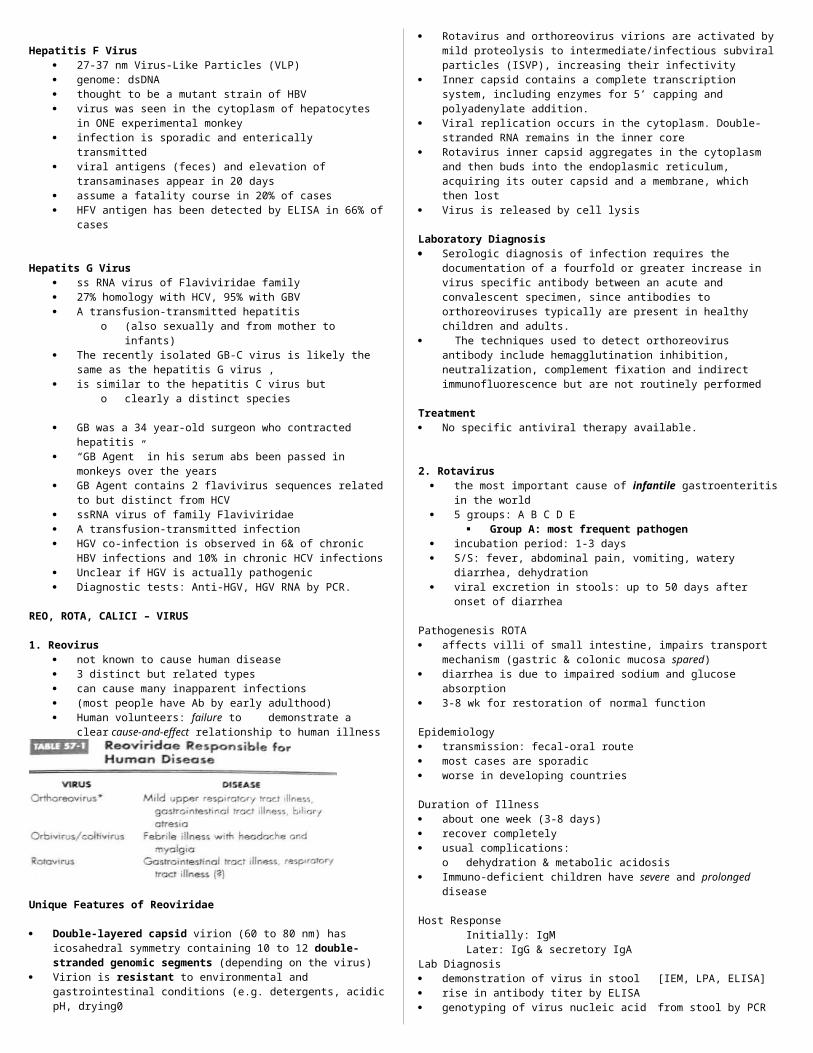
Major determinants of acute and chronic HBV injection. HBV infects the liver but does not cause direct cytopathology. Cell-mediated immune lysis of infected cells, potentially triggered by interferon action, produces the symptoms and resolves the infection. Insufficient immunity can lead to chronic disease. Chronic HBV disease predisposes a person to more serious outcomes. Purple arrows indicate symptoms; green arrows indicate a possible outcome.
(SGPT: 2-5mon; symptoms: 21/2-4mon)
Serologic events associated with the typical course of acute hepatitis B disease.
Tx, Prev’n, Control
No specific treatment Trials: interferon, adenine arabinoside, steroids, azathioprine Blood screening Vaccination Hepatitis B Immune-globulin
Hep B immune-globulin For post-exposure prophylaxis for newborns of HBsAg(+)

mothers & per mucosal exposure to secretions of individuals who are HBsAg positive
Hepatitis Co family Flaviviridae, genus Hepaciviruso positive-stranded RNA viruso 6 genotypes; >70 subtypeso accounts for about 90% of NANBH infectiono major cause of post-transfusion hepatitiso 70-90% of HCV patients develop chronic hepatitis
Epidemiologyo spread: parenteral & sexualo risk factors: IV drug users, blood recipientso suspicion: HBV-negative, post- transfusion hepatitiso occurs in 5-10% of transfusion recipients
Clinical Syndromes1. Acute Form: similar to acute Hepatitis A & B but inflammatory response is less and symptoms are milder2. Chronic Form: more prevalent than HBV, often leads to cirrhosiso Anti-HCV is not protective
Laboratory Diagnosiso ELISA (antibody detection)o RT-PCR (HCV-RNA)o markers:
1. HCV: the agent2. Anti-HCV: the antibody
Tx, Prev’n, Controlo Interferon alfa and ribavirin:o the only effective treatmento (50% response rate)o liver transplanto supportiveo blood screening
accounts for 90% of the cases of NANBH virus infection and is the major cause of posttransfusion hepatitis.
a flavivirus with a positive sense RNA genome and is enveloped.
HCV has an inclination to establish noncytolytic persistent infections and therefore chronic disease
Epidemiology of HBV, HCV, and HDV DISEASE/VIRAL FACTORS
o Enveloped virus is labile to drying. HBV is less sensitive to detergents than other enveloped viruses.
o Virus is shed during asymptomatic periods.o Virus causes chronic disease with potential shedding.
TRANSMISSIONo In blood, semen, and vaginal secretions (HBV); saliva
and mother’s milk).o Via transfusion, needlestick injury, shared drug
paraphernalia, sex, and breast-feeding.
WHO IS AT RISK?o Children: mild asymptomatic disease with
establishment of chronic infection.o Adults: insidious onset of hepatitis.o HBV-infected people co-infected or superinfected
with HDV: abrupt, more severe symptoms with possible fulminant disease.
o Adults with chronic HBV: at high risk for primary hepatocellular carcinoma.
MODES OF CONTROLo Avoidance of high-risk behavioro HBV: vaccine and screening of blood supply.
Clinical Syndrome HCV can cause acute infection but is more likely to establish
chronic infections. A viremia can be detected w/in 1-3 weeks of a transfusion of
HCV-contaminated blood
The viremia lasts 4-6 months in people with an acute infection In acute infection, it is similar to HAV and HBV but symptoms
are usually milder Chronic persistent hepatitis caused by HCV is even more
prevalent than that caused by HBV, often progressing to chronic active hepatitis, cirrhosis, and finally liver failure
Cell-mediated immunopathology is responsible mainly for producing the tissue damage.
Continual liver repair and induction of cell growth occurring during chronic HCV infection are predisposing factors in the dev of PHC.
Laboratory Diagnosis ELISA detection of Antibody Seroconversion occurs w/in 7-31 weeks of infection The presence of the virion RNA in serum I s a better indicator
of the disease RT-PCR can detect HCV RNA in seronegative people
Treatment, Prevention and Control Recombinant interferon-alpha is the only known effective
treatment for HCV. Supportive therapy
Hepatitis Do Delta agent: HDAg surrounded by HBsAg envelopeo HDV: ssRNA, smallest of known human pathogenso responsible for about 40% of fulminant hepatitiso NB. dependent on HBV for replication: (can replicate only in
HBV-infected cells)
Epidemiologyo agent infects children & adults with underlying HBV infectiono distribution: worldwideo high risk: drug users & hemophiliacs
Clinical Syndromeso agent increases severity of Hepatitis B infectiono Delta agent carriers: more likely to develop fulminant hepatitis
Laboratory Diagnosiso ELISA & RIA (Ag /Ab detection)o HDV-RNA by PCRo Markers:o HDV: the agento HD Ag: delta antigen; detectable in early acute infectiono Anti-HDV: indicates past or present infectionTx, Prev’n, Controlo no known specific treatmento Hep B vaccine protective for Delta infection
Approx. 15 M people are infected with HDV (delta agent) Responsible for causing 40% of fulminant hepatitis
infections Uses HBV and target cell proteins to replicate and produce its
one protein A viral parasite The HBsAg is essential for packaging the virus
Laboratory Diagnosis
ELISA and RIA to detect the delta antigen or antibodies
Delta agent can be detected in blood in acute phase
Pathogenesis
the delta agent is spread in blood, semen, and vaginal secretions.
It can only replicate and cause disease only in people with active HBV infections
It is transmitted through the same routes as HBV. A person then becomes co-infected with HBV and the delta agent.
A person w/ chronic HBV can also be superinfected with the
delta agent A more rapid, severe progression occurs in HBV carriers
superinfected w/ HDV than in co-infected w/ HBV and the HDV. Replication of delta agent results in cytotoxicity and liver
damage Protection stems from the immune response to HBsAg
because it is the external antigen and viral attachment protein for HDV
Damage to the liver occurs as a result of the direct CPE of the delta agent combined with immunopathology of the HBV disease
Clinical Syndromes fulminant hepatitis is more likely to develop in people infected
with the delta agent than in those infected with the other hepatitis virus
can result in hepatic encephalopathy (w/ altered mental capacity) and massive hepatic necrosis
Treatment, Prevention and Control no specific treatment for HDV hepatitis prevention of infection w/ HBV will prevent HDV infection
Hepatitis Eo Enterically transmitted: fecal-oral or water-borne transmissiono causes large epidemics in Asia & North Africao distribution: worldwide, but more problematic in developing
countrieso NB: virus is unclassifiedo symptoms & course: very similar to HAV, causes only acute
diseaseo mortality: 1-2% (about 10X that of HAV)o most serious in pregnant women (mortality about 20%)
o HEV (E-NANBH) (the E stands for “enteric” or “epidemic”) is predominantly spread by the fecal-oral route, esp in contaminated water
o Resembles calicivirus and Norwalk agent in size and structureo Problematic in developing countrieso Symptoms and course of HEV are similar to those of HAV
diseaseo Causes only acute diseaseo Poor serum IgG responseo Has a ss-polyA RNA genome
Hepatitis Viruseso A – infectiouso B – serumo C – post transfusion non A non Bo D – delta o E – enteric non A non B
Hepatitis F Virus 27-37 nm Virus-Like Particles (VLP) genome: dsDNA thought to be a mutant strain of HBV virus was seen in the cytoplasm of hepatocytes in ONE
experimental monkey infection is sporadic and enterically transmitted
viral antigens (feces) and elevation of transaminases appear in 20 days
assume a fatality course in 20% of cases HFV antigen has been detected by ELISA in 66% of cases
Hepatits G Virus ss RNA virus of Flaviviridae family 27% homology with HCV, 95% with GBV A transfusion-transmitted hepatitis
o (also sexually and from mother to infants) The recently isolated GB-C virus is likely the same as the
hepatitis G virus , is similar to the hepatitis C virus but
o clearly a distinct species
GB was a 34 year-old surgeon who contracted hepatitis “GB Agent” in his serum abs been passed in monkeys
over the years GB Agent contains 2 flavivirus sequences related to but
distinct from HCV ssRNA virus of family Flaviviridae A transfusion-transmitted infection HGV co-infection is observed in 6& of chronic HBV
infections and 10% in chronic HCV infections Unclear if HGV is actually pathogenic Diagnostic tests: Anti-HGV, HGV RNA by PCR.
REO, ROTA, CALICI – VIRUS
1. Reovirus not known to cause human disease 3 distinct but related types can cause many inapparent infections (most people have Ab by early adulthood) Human volunteers: failure to demonstrate a clear
cause-and-effect relationship to human illness
Unique Features of Reoviridae
Double-layered capsid virion (60 to 80 nm) has icosahedral symmetry containing 10 to 12 double-stranded genomic segments (depending on the virus)
Virion is resistant to environmental and gastrointestinal conditions (e.g. detergents, acidic pH, drying0
Rotavirus and orthoreovirus virions are activated by mild proteolysis to intermediate/infectious subviral particles (ISVP), increasing their infectivity
Inner capsid contains a complete transcription system, including enzymes for 5’ capping and polyadenylate addition.
Viral replication occurs in the cytoplasm. Double-stranded RNA remains in the inner core
Rotavirus inner capsid aggregates in the cytoplasm and then buds into the endoplasmic reticulum, acquiring its outer capsid and a membrane, which then lost
Virus is released by cell lysis
Laboratory Diagnosis Serologic diagnosis of infection requires the documentation of
a fourfold or greater increase in virus specific antibody between an acute and convalescent specimen, since antibodies to orthoreoviruses typically are present in healthy children and adults.
The techniques used to detect orthoreovirus antibody include hemagglutination inhibition, neutralization, complement fixation and indirect immunofluorescence but are not routinely performed
Treatment No specific antiviral therapy available.
2. Rotavirus the most important cause of infantile gastroenteritis in the
world 5 groups: A B C D E
Group A: most frequent pathogen incubation period: 1-3 days S/S: fever, abdominal pain, vomiting, watery diarrhea,
dehydration viral excretion in stools: up to 50 days after onset of
diarrhea
Pathogenesis ROTA affects villi of small intestine, impairs transport mechanism
(gastric & colonic mucosa spared) diarrhea is due to impaired sodium and glucose absorption 3-8 wk for restoration of normal function
Epidemiology transmission: fecal-oral route most cases are sporadic worse in developing countries
Duration of Illness about one week (3-8 days) recover completely usual complications:
o dehydration & metabolic acidosis Immuno-deficient children have severe and prolonged disease
Host ResponseInitially: IgM Later: IgG & secretory IgA
Lab Diagnosis demonstration of virus in stool [IEM, LPA, ELISA] rise in antibody titer by ELISA genotyping of virus nucleic acid from stool by PCR [the most sensitive method]
Treatment and Prevention supportive immunization waste water treatment sanitation
3. Calicivirus important agents of viral gastroenteritis 5 Ag types; ‘star of David’ appearance most important member: Norwalk virus incubation period: 24-48 hr characterized by: rapid onset, brief clinical course (12-60 hr) S/S: nausea, vomiting, abdominal pain, low-grade
fever, headache, malaise, diarrhea
Norwalk VirusNB. the most important cause of epidemic viral gastroenteritis in adultsCharacterized by:1. absence of bacterial pathogen2. rapid onset and recovery & relatively mild systemic signs3. a pattern that spreads rapidly with no particular age nor geographic predilection
Small, non-enveloped 27nm particle with ss-RNA genome
Self-limited gastroenteritis 1969: GE outbreak in Norwalk, Ohio Most important cause of epidemic viral gastroenteritis in
adults
Epidemiology Usually occurs in schools, recreational camps, nursing
homes Infection is mainly through food & water and person-to-
person Agent occurs worldwide & outbreaks all-year round
Clinical Infection incubation period: 24-48 hr S/S: nausea, vomiting, abdominal pain, fever, headache,
malaise, diarrhea symptoms lasts for 12-60 hours stools: non-bloody & non-mucoid
NB. About half have diarrhea
Laboratory diagnosisRT-PCR - most widely used for viral detection in feces and vomitus,
food & water ELISA - most efficient in detecting soluble & particulate antigens; antibody responsesIEM
Treatment and Control symptomatic & supportive careful disposal of stools effective hand washing careful processing of food purification of drinking water & swimming pool water no vaccine is available
RETROVIRUSES (RNA TUMOR VIRUSES)
UNIQUE CHARACTERISTICS OF RETROVIRUSES
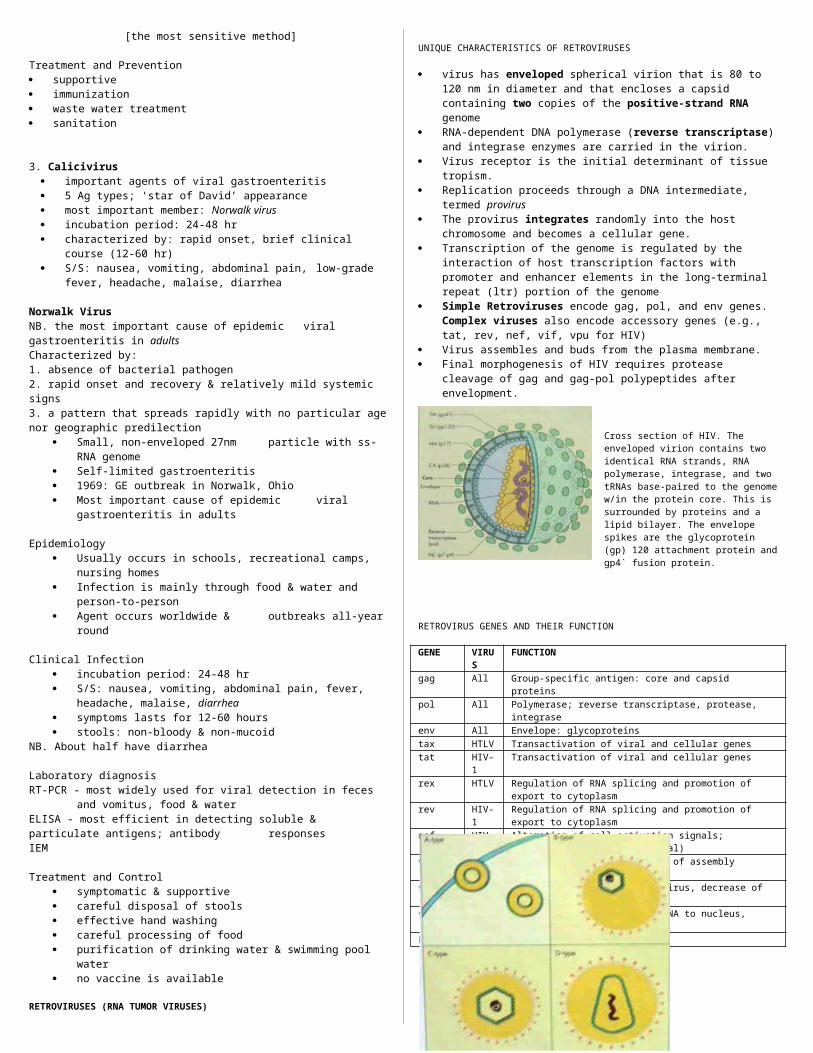
virus has enveloped spherical virion that is 80 to 120 nm in diameter and that encloses a capsid containing two copies of the positive-strand RNA genome
RNA-dependent DNA polymerase (reverse transcriptase) and integrase enzymes are carried in the virion.
Virus receptor is the initial determinant of tissue tropism. Replication proceeds through a DNA intermediate, termed
provirus The provirus integrates randomly into the host chromosome
and becomes a cellular gene. Transcription of the genome is regulated by the interaction of
host transcription factors with promoter and enhancer elements in the long-terminal repeat (ltr) portion of the genome
Simple Retroviruses encode gag, pol, and env genes. Complex viruses also encode accessory genes (e.g., tat, rev, nef, vif, vpu for HIV)
Virus assembles and buds from the plasma membrane. Final morphogenesis of HIV requires protease cleavage of gag
and gag-pol polypeptides after envelopment.
Cross section of HIV. The enveloped virion contains two identical RNA strands, RNA polymerase, integrase, and two tRNAs base-paired to the genome w/in the protein core. This is surrounded by proteins and a lipid bilayer. The envelope spikes are the glycoprotein (gp) 120 attachment protein and gp4` fusion protein.
RETROVIRUS GENES AND THEIR FUNCTION
GENE VIRUS
FUNCTION
gag All Group-specific antigen: core and capsid proteinspol All Polymerase; reverse transcriptase, protease, integraseenv All Envelope: glycoproteinstax HTLV Transactivation of viral and cellular genestat HIV-
1Transactivation of viral and cellular genes
rex HTLV Regulation of RNA splicing and promotion of export to cytoplasm
rev HIV-1
Regulation of RNA splicing and promotion of export to cytoplasm
nef HIV-1
Alteration of cell activation signals; progression to AIDS (essential)
vif HIV-1
Virus infectivity, promotion of assembly
vpu HIV-1
Facilitation of release of virus, decrease of cell surface CD4
vpr (vpx*)
HIV-1
Transport of complementary DNA to nucleus, arresting of cell growth
LTR All Promoter, enhancer elements
Morphological distinction of retrovirions. The morphology and position of the nucleocapsid core are used to classify the viruses. A-type particles are immature intracytoplasmic forms that bud through the plasma membrane into mature B-type, C-type and D-type particles.
CLASSIFICATION OF RETROVIRUSES
SUBFAMILY CHARACTERISTICS EXAMPLESOncovirinae
- B
- C
- D
Are associated with cancer and neurological disorders
Have eccentric nucleocapsid core in mature virion
Have centrally located nucleocapsid core in mature virion
Have nucleocapsid core with cylindrical form
-
Mouse mammary tumor virus
Human T-lymphotrophic virus (HTLOV-1, HTLV-2, HTLV-5), Rous sarcoma virus (chickens)
Mason-Phizer monkey virus
Lentivirinae Have slow onset of disease; casue neurological disorders and immunosuppression; are viruses with D-type, cylindrical nucleoapsid core
Human foamy virus
Spumavirinae Cause no clinical disease but characteristic vacuolated “foamy” cytopathology
Human foamy virus
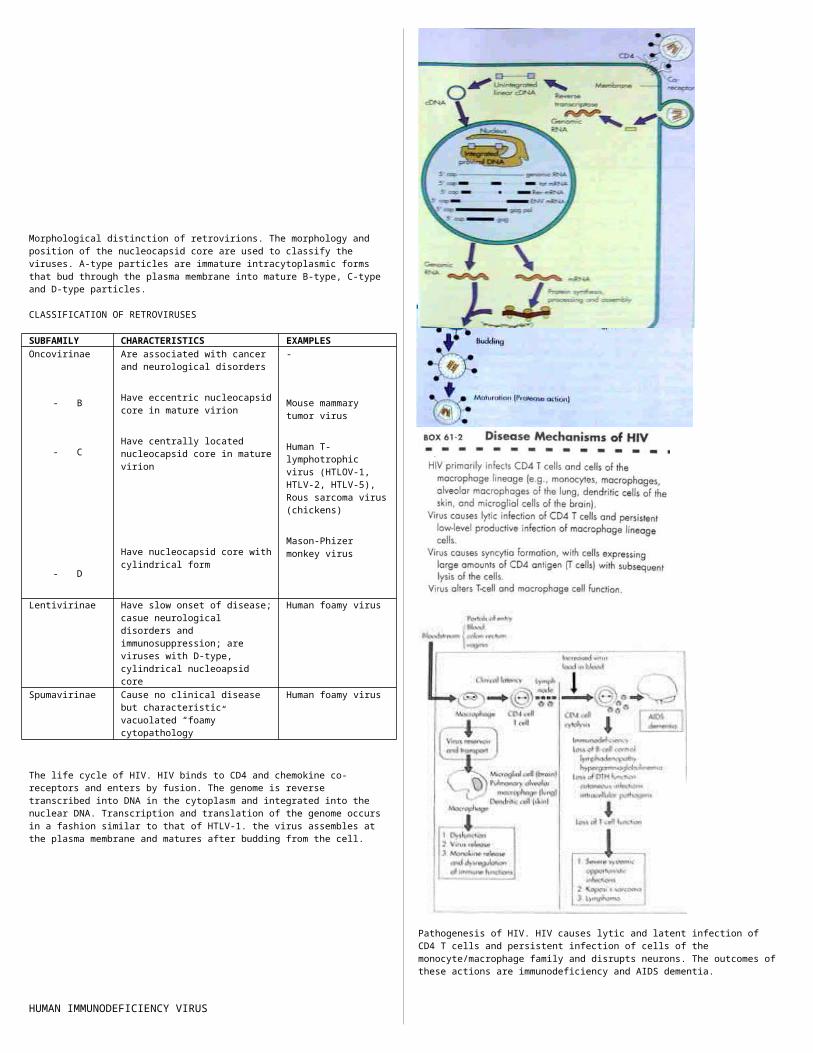
The life cycle of HIV. HIV binds to CD4 and chemokine co-receptors and enters by fusion. The genome is reverse transcribed into DNA in the cytoplasm and integrated into the nuclear DNA. Transcription and translation of the genome occurs in a fashion similar to that of HTLV-1. the virus assembles at the plasma membrane and matures after budding from the cell.
HUMAN IMMUNODEFICIENCY VIRUS
Pathogenesis of HIV. HIV causes lytic and latent infection of CD4 T cells and persistent infection of cells of the monocyte/macrophage family and disrupts neurons. The outcomes of these actions are immunodeficiency and AIDS dementia.
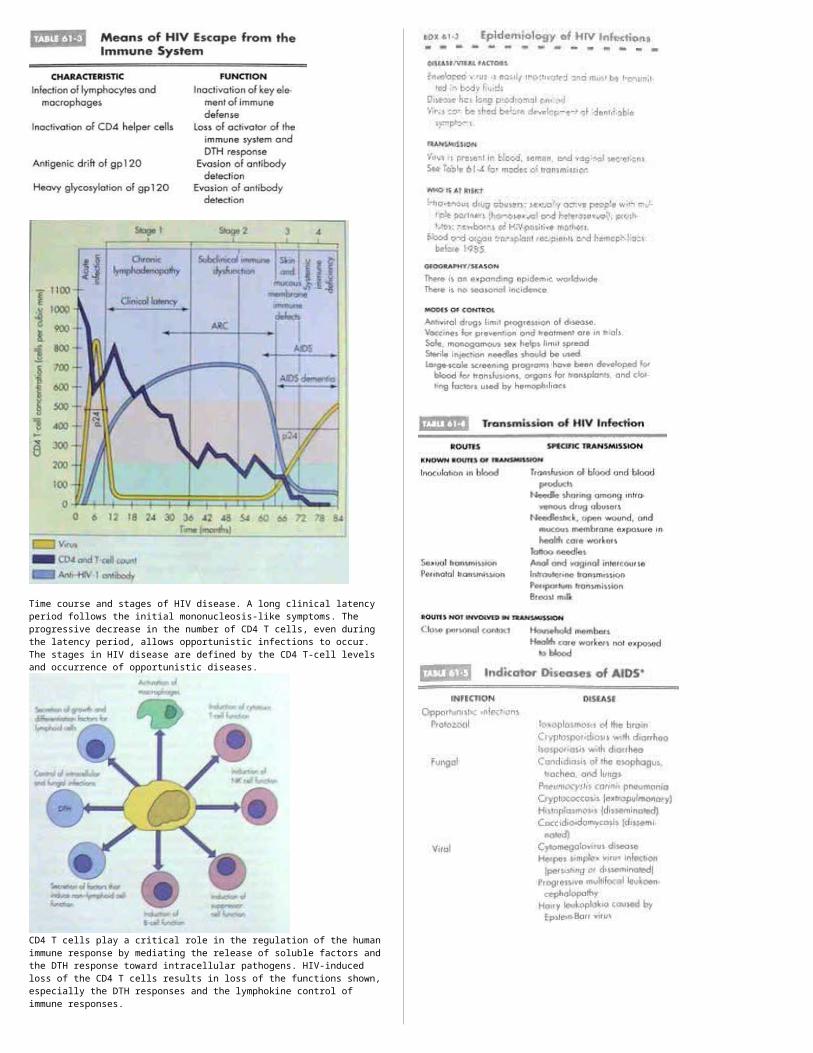
Time course and stages of HIV disease. A long clinical latency period follows the initial mononucleosis-like symptoms. The progressive decrease in the number of CD4 T cells, even during the latency period, allows opportunistic infections to occur. The stages in HIV disease are defined by the CD4 T-cell levels and occurrence of opportunistic diseases.
CD4 T cells play a critical role in the regulation of the human immune response by mediating the release of soluble factors and the DTH response toward intracellular pathogens. HIV-induced loss of the CD4 T cells results in loss of the functions shown, especially the DTH responses and the lymphokine control of immune responses.
HUMAN T-LYMPHOTROPIC VIRUS AND OTHER ONCOGENIC RETROVIRUSES
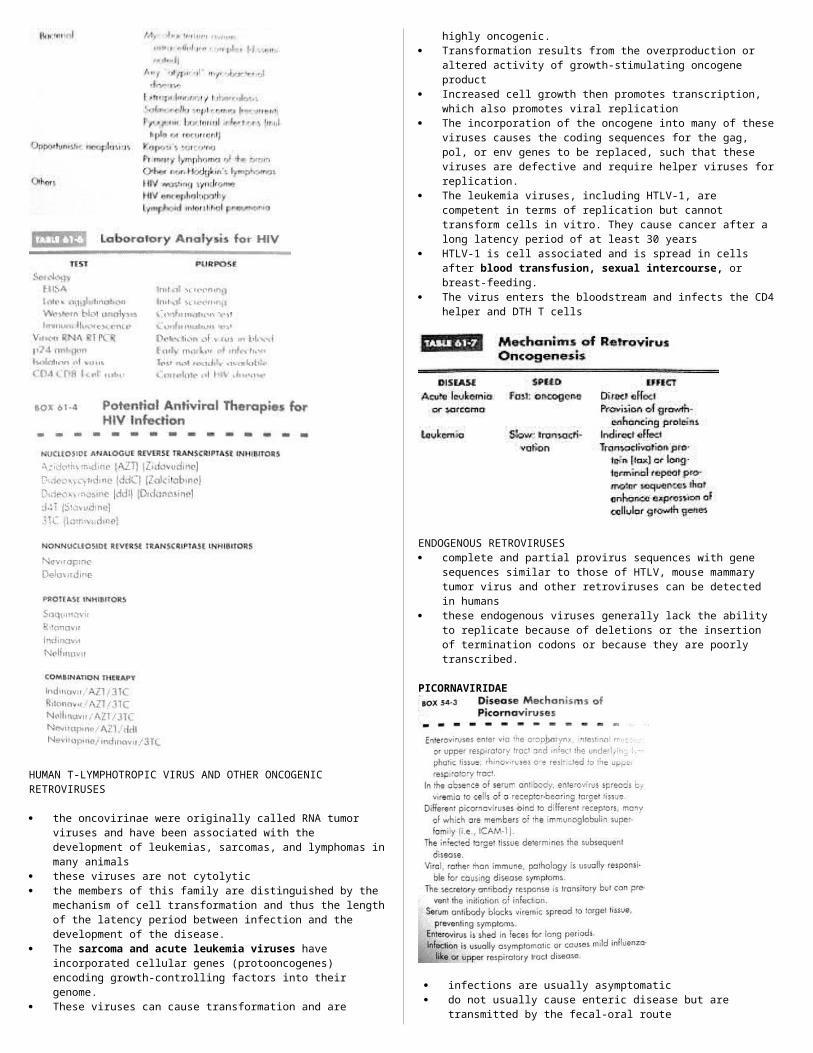
the oncovirinae were originally called RNA tumor viruses and have been associated with the development of leukemias, sarcomas, and lymphomas in many animals
these viruses are not cytolytic the members of this family are distinguished by the
mechanism of cell transformation and thus the length of the latency period between infection and the development of the disease.
The sarcoma and acute leukemia viruses have incorporated cellular genes (protooncogenes) encoding growth-controlling factors into their genome.
These viruses can cause transformation and are highly oncogenic.
Transformation results from the overproduction or altered activity of growth-stimulating oncogene product
Increased cell growth then promotes transcription, which also promotes viral replication
The incorporation of the oncogene into many of these viruses
causes the coding sequences for the gag, pol, or env genes to be replaced, such that these viruses are defective and require helper viruses for replication.
The leukemia viruses, including HTLV-1, are competent in terms of replication but cannot transform cells in vitro. They cause cancer after a long latency period of at least 30 years
HTLV-1 is cell associated and is spread in cells after blood transfusion, sexual intercourse, or breast-feeding.
The virus enters the bloodstream and infects the CD4 helper and DTH T cells
ENDOGENOUS RETROVIRUSES complete and partial provirus sequences with gene sequences
similar to those of HTLV, mouse mammary tumor virus and other retroviruses can be detected in humans
these endogenous viruses generally lack the ability to replicate because of deletions or the insertion of termination codons or because they are poorly transcribed.
PICORNAVIRIDAE
infections are usually asymptomatic do not usually cause enteric disease but are transmitted by
the fecal-oral route Poliovirus is the prototype The upper respiratory tract, oropharynx and intestinal tract
are portals of entry Virions are impervious to stomach acid, proteases and bile Replication is initiated in the mucosa and lymphoid tissue of
the tonsils and pharynx, it later infects the peyer’s patches and underlying intestinal mucosa
Primary viremia – spreats virus to receptor-bearing target tissues (where 2nd phase of replication begins)
In polioviruses – the virus must cross the blood-brain barrier or may gain access to the brain by infecting skeletal muscle and traveling up the innervating nerves to the brain
Polio virus has one of the narrowest tissue tropisms, recognizing a receptor expressed on anterior horn cells of the spinal cord, dorsal root ganglia, motor neurons, skeletal muscle cells, lymphoid cells
Coxsackieviruses and echoviruses recognize receptors expressed on more cell types and tissues
Receptors are rpesent on cells of the CNS, heart, lung, pancrease, mucosa
Most enteroviruses are cytolytic, replicating rapidly and causing direct damage to target cells
Antibody is the major protective immune response to the enteroviruses; it can prevent initial infection in the oropharynx and GIT; prevents spread to target tissue
Cell-mediated immunity is not usually involved in protection but may play a role in pathogenesis
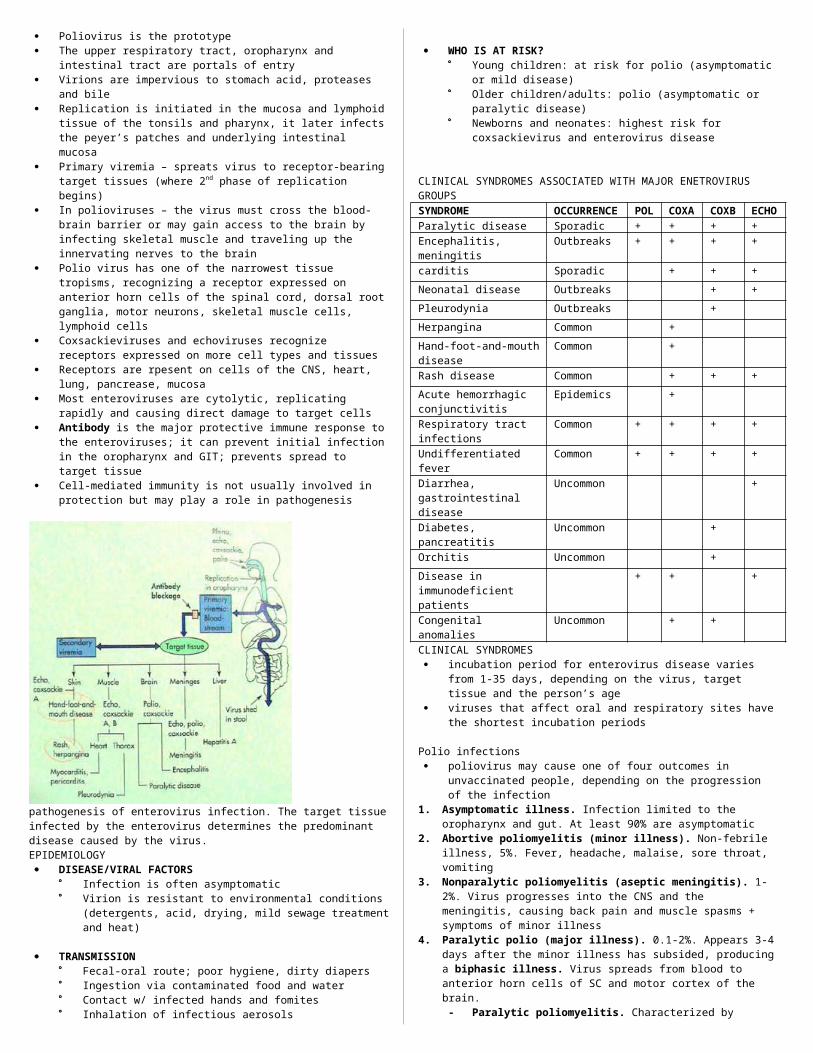
pathogenesis of enterovirus infection. The target tissue infected by the enterovirus determines the predominant disease caused by the virus.EPIDEMIOLOGY DISEASE/VIRAL FACTORS
Infection is often asymptomatic Virion is resistant to environmental conditions
(detergents, acid, drying, mild sewage treatment and heat)
TRANSMISSION Fecal-oral route; poor hygiene, dirty diapers Ingestion via contaminated food and water Contact w/ infected hands and fomites Inhalation of infectious aerosols
WHO IS AT RISK? Young children: at risk for polio (asymptomatic or mild
disease) Older children/adults: polio (asymptomatic or paralytic
disease) Newborns and neonates: highest risk for coxsackievirus
and enterovirus disease
CLINICAL SYNDROMES ASSOCIATED WITH MAJOR ENETROVIRUS GROUPSSYNDROME OCCURREN
CEPOL
COXA
COXB
ECHO
Paralytic disease Sporadic + + + +Encephalitis, meningitis
Outbreaks + + + +
carditis Sporadic + + +Neonatal disease Outbreaks + +Pleurodynia Outbreaks +Herpangina Common +Hand-foot-and-mouth disease
Common +
Rash disease Common + + +Acute hemorrhagic conjunctivitis
Epidemics +
Respiratory tract infections
Common + + + +
Undifferentiated fever Common + + + +Diarrhea, gastrointestinal
Uncommon +
diseaseDiabetes, pancreatitis Uncommon +Orchitis Uncommon +Disease in immunodeficient patients
+ + +
Congenital anomalies Uncommon + +CLINICAL SYNDROMES incubation period for enterovirus disease varies from 1-35
days, depending on the virus, target tissue and the person’s age
viruses that affect oral and respiratory sites have the shortest incubation periods
Polio infections poliovirus may cause one of four outcomes in unvaccinated
people, depending on the progression of the infection1. Asymptomatic illness. Infection limited to the oropharynx
and gut. At least 90% are asymptomatic2. Abortive poliomyelitis (minor illness). Non-febrile illness,
5%. Fever, headache, malaise, sore throat, vomiting3. Nonparalytic poliomyelitis (aseptic meningitis). 1-2%.
Virus progresses into the CNS and the meningitis, causing back pain and muscle spasms + symptoms of minor illness
4. Paralytic polio (major illness). 0.1-2%. Appears 3-4 days after the minor illness has subsided, producing a biphasic illness. Virus spreads from blood to anterior horn cells of SC and motor cortex of the brain. - Paralytic poliomyelitis. Characterized by
asymmetrical flaccid paralysis with no sensory loss.- Bulbar poliomyelitis. Involve the muscles of the
pharynx, vocal cords and respiration. Results in death of 75% of patients
- Postpolio syndrome. Sequelae of poliomyelitis that may occur much later in life (30-40 yrs)
Progression of poliovirus infection. Infection may be asymptomatic or progress to minor or major disease.
Coxsackievirus and Echovirius Infections coxsackie A viruses are assoc with diseases with vesicular
lesions (herpangina) whereas coxsackie B (b for body) are associated with myocarditis and pleurodynia.
Herpangina is casued by several types of coxsackie A virus. Fever, sore throat, pain… Classic finding is vesicular ulcerated lesions around the
soft palate and uvula Virus can be recovered from lesions or feces Requires only symptomatic management
Hand-foot-and-Mouth disease is a vesicular exanthema caused by an enterovirus usually cox A16. Lesions on hands, feet, mouth and tongue
Pleurodynia (Bornholm disease) aka devil’s grip, is a acute illness in w/c patients have sudden onset of fever and unilateral low thoracic, pleuritic chest pain
Myocardial and Pericardial infections caused by coxB. Neonates have febrile illnesses and sudden onset of unexplained heart failure Cyanosis, tachycardia, cardiomegaly and hepatomegaly
occur Acute benign pericarditis affects young adults;
symptoms resemble those of MI but fever is more severe.
Viral (aseptic) meningitis, acute febrile illness accompanied by headache and signs of meningeal irritation including nuchal rigidity. Petechiae or skin rash may occur in patients
Fever and rash may occur in Px infected with Echo and Cox. Eruptions are usually maculopapular but may occasionally be petechial or vesicular
Transmission of enteroviruses. The capsid structure is resistant to mild sewage treatment, saltwater, detergents, and temp changes, allowing these viruses to be transmitted by fecal-oral route and on hands.
LABORATORY DIAGNOSIS Clinical chemistry
CSF from poliovirus or enterovirus aseptic meningitis reveals a predominantly lymphocytic pleocytosis
In viral meningitis, the CSF glucose level is usually normal or slightly low
Culture Poliovirus may be isolated from patient’s pharynx It grows well on monkey kidney tissue culture The specific type of enterovirus can be determined by
using specific antibody and assays (IF, ELISA) Serology
Detection of IgM or finding a 4-fold increase in Ab titer bet time of acute illness and period of convalescence
TREATMENT, PREVENTION AND CONTROL no specific antiviral therapy supportive therapy 2 types of polio vaccine exist
inactivated polio vaccine (IPV) live attenuated oral polio vaccine (OPV).- both are effective but OPV is used due to its ease of
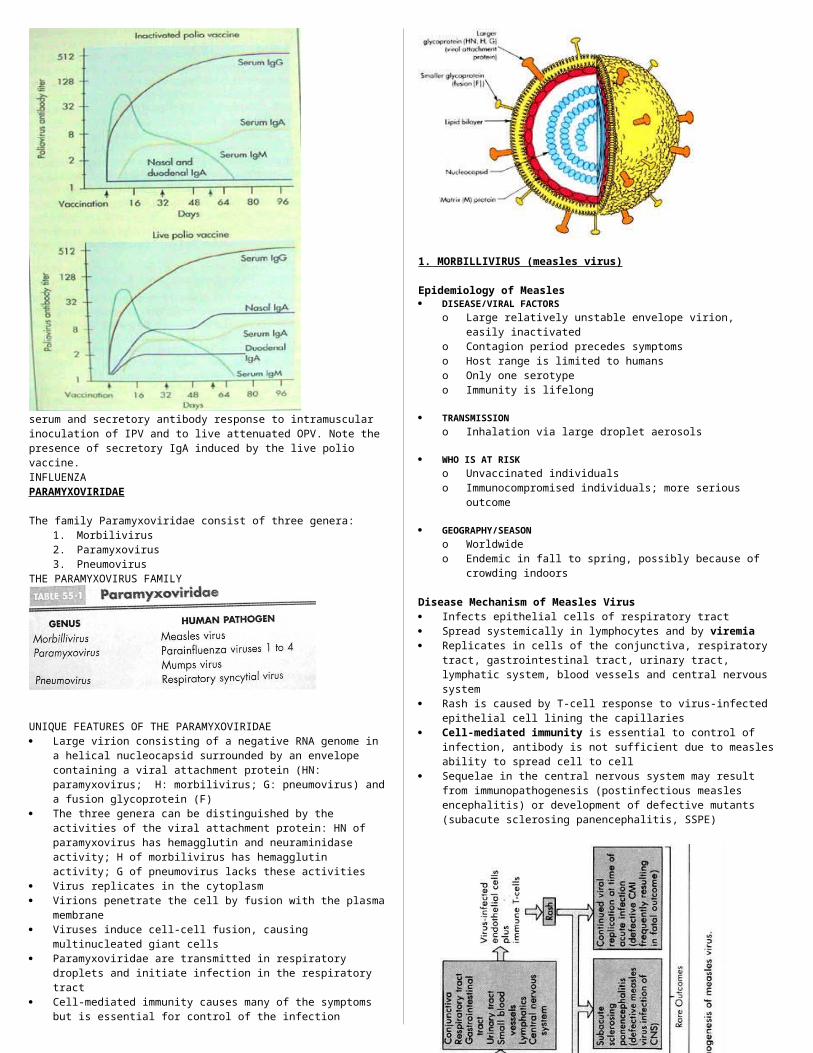
delivery and capacity to elicit a lifelong immunity
serum and secretory antibody response to intramuscular inoculation of IPV and to live attenuated OPV. Note the presence of secretory IgA induced by the live polio vaccine.INFLUENZAPARAMYXOVIRIDAE
The family Paramyxoviridae consist of three genera: 1. Morbilivirus2. Paramyxovirus3. Pneumovirus
THE PARAMYXOVIRUS FAMILY
UNIQUE FEATURES OF THE PARAMYXOVIRIDAE Large virion consisting of a negative RNA genome in a helical
nucleocapsid surrounded by an envelope containing a viral attachment protein (HN: paramyxovirus; H: morbilivirus; G: pneumovirus) and a fusion glycoprotein (F)
The three genera can be distinguished by the activities of the viral attachment protein: HN of paramyxovirus has hemagglutin and neuraminidase activity; H of morbilivirus has hemagglutin activity; G of pneumovirus lacks these activities
Virus replicates in the cytoplasm Virions penetrate the cell by fusion with the plasma
membrane Viruses induce cell-cell fusion, causing multinucleated giant
cells Paramyxoviridae are transmitted in respiratory droplets and
initiate infection in the respiratory tract Cell-mediated immunity causes many of the symptoms but is
essential for control of the infection

1. MORBILLIVIRUS (measles virus)
Epidemiology of Measles DISEASE/VIRAL FACTORS
o Large relatively unstable envelope virion, easily inactivated
o Contagion period precedes symptomso Host range is limited to humanso Only one serotypeo Immunity is lifelong
TRANSMISSIONo Inhalation via large droplet aerosols
WHO IS AT RISKo Unvaccinated individualso Immunocompromised individuals; more serious outcome
GEOGRAPHY/SEASONo Worldwide o Endemic in fall to spring, possibly because of crowding
indoors
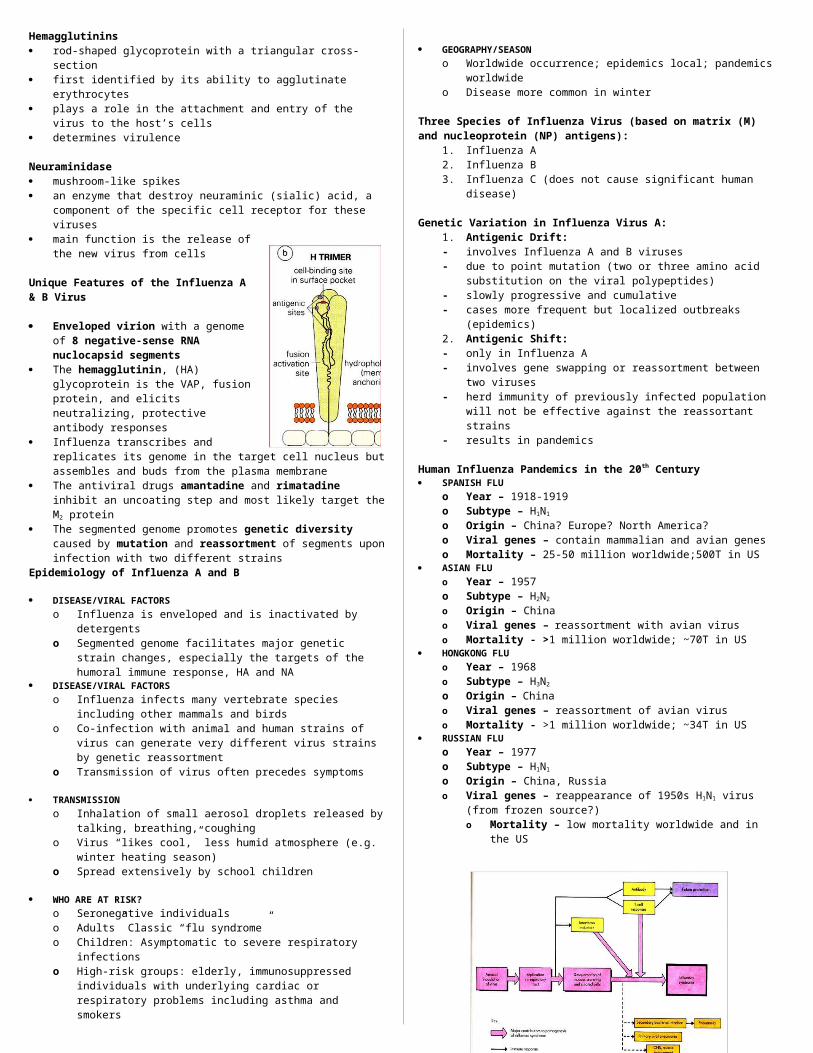
Disease Mechanism of Measles Virus Infects epithelial cells of respiratory tract Spread systemically in lymphocytes and by viremia Replicates in cells of the conjunctiva, respiratory tract,
gastrointestinal tract, urinary tract, lymphatic system, blood vessels and central nervous system
Rash is caused by T-cell response to virus-infected epithelial cell lining the capillaries
Cell-mediated immunity is essential to control of infection, antibody is not sufficient due to measles ability to spread cell to cell
Sequelae in the central nervous system may result from immunopathogenesis (postinfectious measles encephalitis) or development of defective mutants (subacute sclerosing panencephalitis, SSPE)
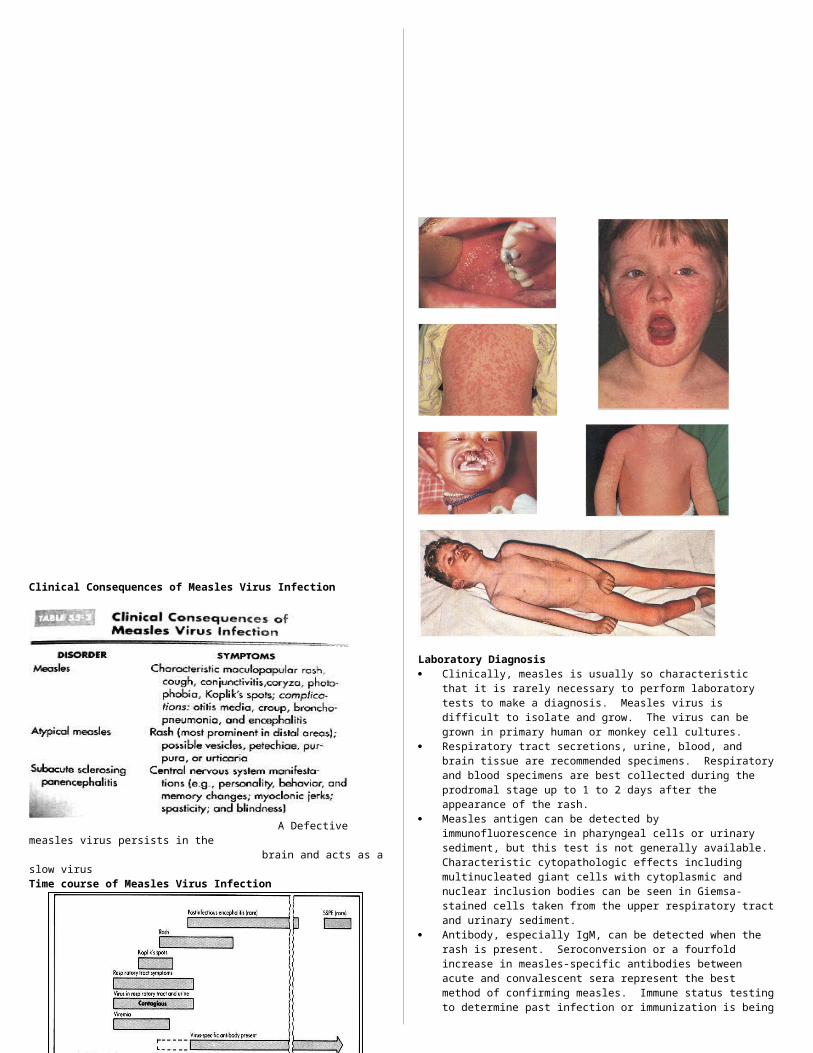
Clinical Consequences of Measles Virus Infection
A Defective measles virus persists in the
brain and acts as a slow virusTime course of Measles Virus Infection
Laboratory Diagnosis Clinically, measles is usually so characteristic that it is rarely
necessary to perform laboratory tests to make a diagnosis. Measles virus is difficult to isolate and grow. The virus can be grown in primary human or monkey cell cultures.
Respiratory tract secretions, urine, blood, and brain tissue are recommended specimens. Respiratory and blood specimens are best collected during the prodromal stage up to 1 to 2 days after the appearance of the rash.
Measles antigen can be detected by immunofluorescence in pharyngeal cells or urinary sediment, but this test is not generally available. Characteristic cytopathologic effects including multinucleated giant cells with cytoplasmic and nuclear inclusion bodies can be seen in Giemsa-stained cells taken from the upper respiratory tract and urinary sediment.
Antibody, especially IgM, can be detected when the rash is present. Seroconversion or a fourfold increase in measles-specific antibodies between acute and convalescent sera represent the best method of confirming measles. Immune status testing to determine past infection or immunization is being used to document childhood immunization.
Treatment, Prevention and Control] A live attenuated measles vaccine in use since 1963. Live
attenuated vaccine is given to all children after 6 months of age, in combination with mumps and rubella vaccine (MMR vaccine) at 15 months
Inactivated “killed” vaccines are no longer available, even for the immunocompromised, because of the subsequent effect on naturally acquired measles virus infection (atypical measles). No specific antiviral treatment is available for measles.
Exposed susceptible individuals who are immunocompromised should be given immune serum globulin to modify their measles infection. This product is most effective if given within 6 days of exposure.
2. PARAMYXOVIRUS
PARAINFLUENZA VIRUS
Epidemiology of Parainfluenza Virus Infection DISEASE/VIRAL FACTORS
o Large relatively unstable enveloped virion, easily inactivated
o Contagion period precedes symptoms and may occur in the absence of symptoms
o Host range is limited to humanso Reinfection later in life can occur
TRANSMISSIONo Inhalation of large droplet aerosols
WHO ARE AT RISK?
o Children: mild diseaae, croupo Adults: reinfection with milder symptoms
GEOGRAPHY/SEASONo Ubiquitous and worldwide
Disease Mechanism of Parainfluenza Viruses Four serotypes of viruses Infection is limited to respiratory tract, upper respiratory
tract disease is most common, but significant disease can occur upon lower respiratory tract infection
Parainfluenza viruses are not systemic and do not cause viremia
Diseases include coldlike symptoms, bronchitis (inflammation of bronchial tubes), bronchiolitis (inflammation of bronchioles), croup (laryngotracheobronchitis)
Infection induces protective immunity of short duration
Laboratory Diagnosis Parainfluenza virus isolated from nasal washings and
respiratory secretions grow well in primary monkey kidney cells. However, like the other paramyxovirus, the virions are labile during transit to the lab. Virus-infected cells in aspirates or in cell culture can be identified by immunofluorescence.
Treatment, Prevention and Control No specific antiviral agents are available. Vaccination with killed vaccines is ineffective possibly because
they fail to induce local secretory antibody and appropriate cellular immunity. No live attenuated vaccine is presently available.
a. MUMPS VIRUS
Epidemiology of Mumps Virus DISEASE/VIRAL FACTORS
o Large relatively unstable enveloped virion, easily inactivated
o Contagion period precedes symptomso May cause asymptomatic sheddingo Host range is limited to humanso Only one serotypeo Immunity is lifelong
TRANSMISSIONo Large droplet aerosols
WHO IS AT RISK?o Unvaccinated individualso Immunocompromised individuals, more serious outcome
GEOGRAPHY/SEASONo Worldwideo Endemic in late winter and early spring
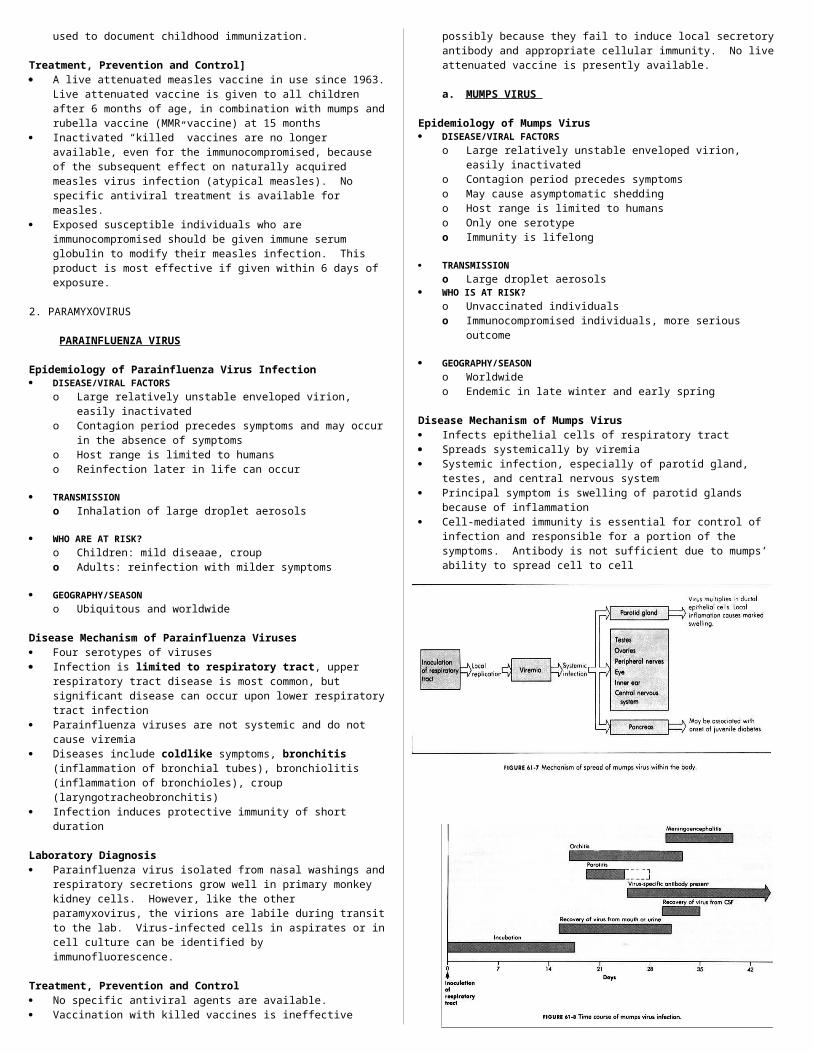
Disease Mechanism of Mumps Virus Infects epithelial cells of respiratory tract Spreads systemically by viremia Systemic infection, especially of parotid gland, testes, and
central nervous system Principal symptom is swelling of parotid glands because of
inflammation Cell-mediated immunity is essential for control of infection and
responsible for a portion of the symptoms. Antibody is not sufficient due to mumps’ ability to spread cell to cell
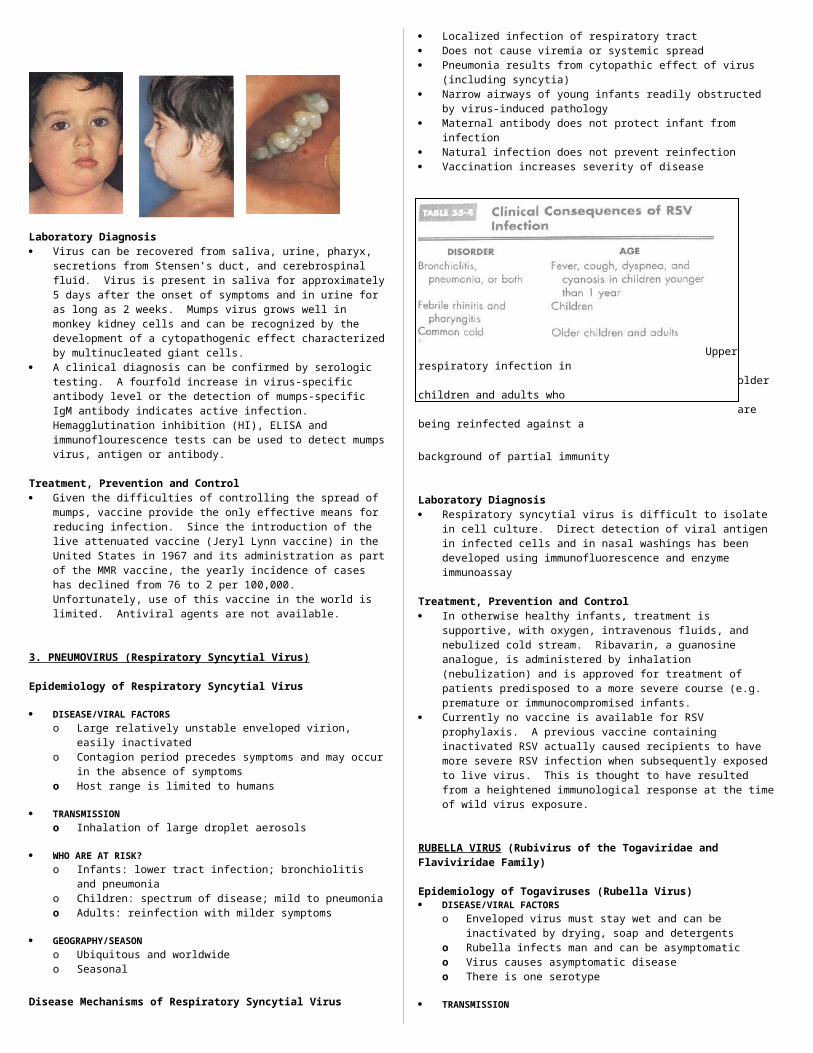
Laboratory Diagnosis Virus can be recovered from saliva, urine, pharyx, secretions
from Stensen’s duct, and cerebrospinal fluid. Virus is present in saliva for approximately 5 days after the onset of symptoms and in urine for as long as 2 weeks. Mumps virus grows well in monkey kidney cells and can be recognized by the development of a cytopathogenic effect characterized by multinucleated giant cells.
A clinical diagnosis can be confirmed by serologic testing. A fourfold increase in virus-specific antibody level or the detection of mumps-specific IgM antibody indicates active infection. Hemagglutination inhibition (HI), ELISA and immunoflourescence tests can be used to detect mumps virus, antigen or antibody.
Treatment, Prevention and Control Given the difficulties of controlling the spread of mumps,
vaccine provide the only effective means for reducing infection. Since the introduction of the live attenuated vaccine (Jeryl Lynn vaccine) in the United States in 1967 and its administration as part of the MMR vaccine, the yearly incidence of cases has declined from 76 to 2 per 100,000. Unfortunately, use of this vaccine in the world is limited. Antiviral agents are not available.
3. PNEUMOVIRUS (Respiratory Syncytial Virus)
Epidemiology of Respiratory Syncytial Virus
DISEASE/VIRAL FACTORSo Large relatively unstable enveloped virion, easily
inactivatedo Contagion period precedes symptoms and may occur in
the absence of symptomso Host range is limited to humans
TRANSMISSIONo Inhalation of large droplet aerosols
WHO ARE AT RISK?o Infants: lower tract infection; bronchiolitis and pneumoniao Children: spectrum of disease; mild to pneumoniao Adults: reinfection with milder symptoms
GEOGRAPHY/SEASONo Ubiquitous and worldwide o Seasonal
Disease Mechanisms of Respiratory Syncytial Virus
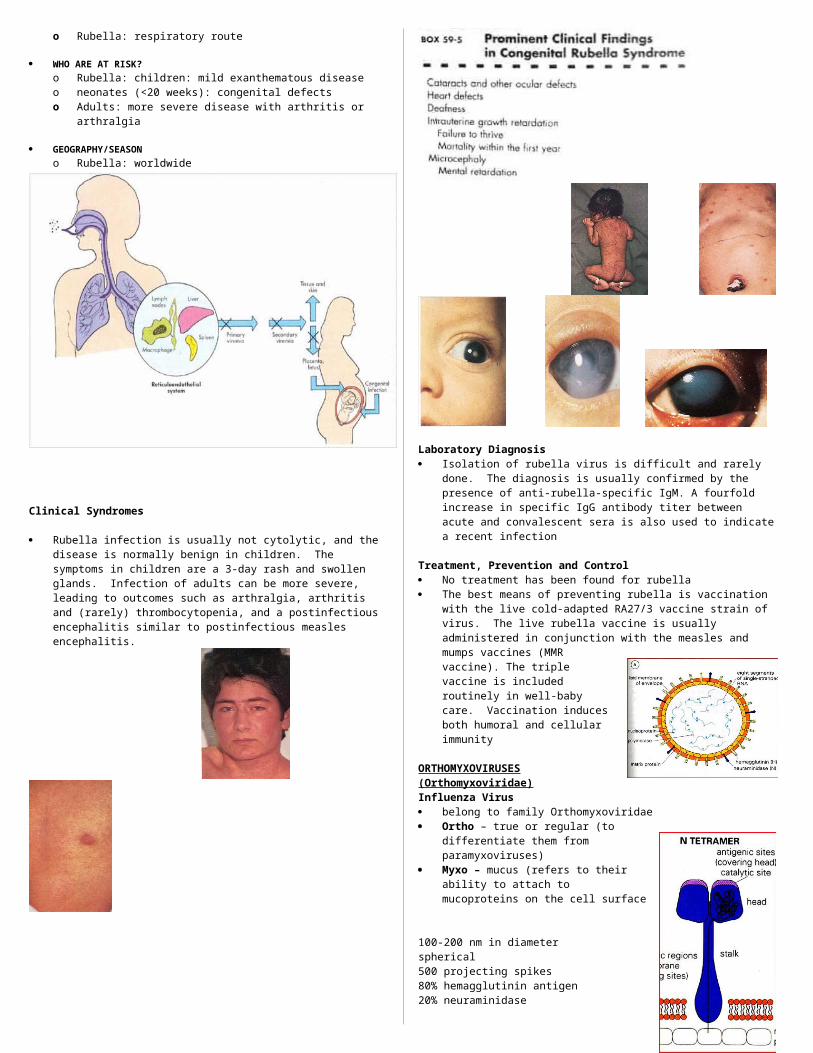
Localized infection of respiratory tract Does not cause viremia or systemic spread Pneumonia results from cytopathic effect of virus (including
syncytia) Narrow airways of young infants readily obstructed by virus-
induced pathology Maternal antibody does not protect infant from infection Natural infection does not prevent reinfection Vaccination increases severity of disease
Upper respiratory infection in older children and adults who are being reinfected against a background of partial immunity
Laboratory Diagnosis Respiratory syncytial virus is difficult to isolate in cell culture.
Direct detection of viral antigen in infected cells and in nasal washings has been developed using immunofluorescence and enzyme immunoassay
Treatment, Prevention and Control In otherwise healthy infants, treatment is supportive, with
oxygen, intravenous fluids, and nebulized cold stream. Ribavarin, a guanosine analogue, is administered by inhalation (nebulization) and is approved for treatment of patients predisposed to a more severe course (e.g. premature or immunocompromised infants.
Currently no vaccine is available for RSV prophylaxis. A previous vaccine containing inactivated RSV actually caused recipients to have more severe RSV infection when subsequently exposed to live virus. This is thought to have resulted from a heightened immunological response at the time of wild virus exposure.
RUBELLA VIRUS (Rubivirus of the Togaviridae and Flaviviridae Family)
Epidemiology of Togaviruses (Rubella Virus) DISEASE/VIRAL FACTORS
o Enveloped virus must stay wet and can be inactivated by drying, soap and detergents
o Rubella infects man and can be asymptomatico Virus causes asymptomatic diseaseo There is one serotype
TRANSMISSIONo Rubella: respiratory route
WHO ARE AT RISK?o Rubella: children: mild exanthematous diseaseo neonates (<20 weeks): congenital defectso Adults: more severe disease with arthritis or arthralgia
GEOGRAPHY/SEASONo Rubella: worldwide
Clinical Syndromes
Rubella infection is usually not cytolytic, and the disease is normally benign in children. The symptoms in children are a 3-day rash and swollen glands. Infection of adults can be more severe, leading to outcomes such as arthralgia, arthritis and (rarely) thrombocytopenia, and a postinfectious encephalitis similar to postinfectious measles encephalitis.
Laboratory Diagnosis Isolation of rubella virus is difficult and rarely done. The
diagnosis is usually confirmed by the presence of anti-rubella-specific IgM. A fourfold increase in specific IgG antibody titer between acute and convalescent sera is also used to indicate a recent infection
Treatment, Prevention and Control No treatment has been found
for rubella The best means of preventing
rubella is vaccination with the live cold-adapted RA27/3 vaccine strain of virus. The live rubella vaccine is usually administered in conjunction with the measles and mumps vaccines (MMR vaccine). The triple vaccine is included routinely in well-baby care. Vaccination induces both humoral and cellular immunity
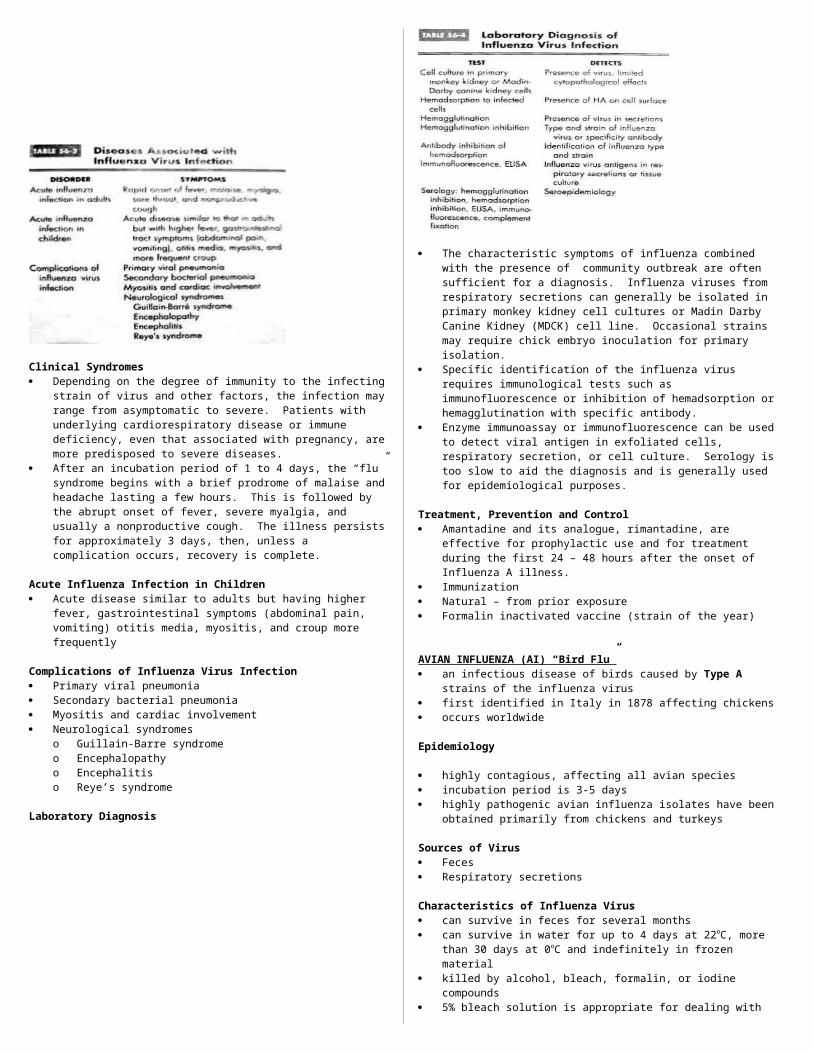
ORTHOMYXOVIRUSES (Orthomyxoviridae)Influenza Virus belong to family Orthomyxoviridae Ortho – true or regular (to differentiate them from
paramyxoviruses) Myxo – mucus (refers to their ability to attach to
mucoproteins on the cell surface
100-200 nm in diameterspherical500 projecting spikes80% hemagglutinin antigen20% neuraminidase
Hemagglutinins rod-shaped glycoprotein with a
triangular cross-section first identified by its ability to
agglutinate erythrocytes plays a role in the attachment and
entry of the virus to the host’s cells determines virulence
Neuraminidase mushroom-like spikes an enzyme that destroy neuraminic (sialic) acid, a component
of the specific cell receptor for these viruses main function is the release of the new virus from cells
Unique Features of the Influenza A & B Virus
Enveloped virion with a genome of 8 negative-sense RNA nuclocapsid segments
The hemagglutinin, (HA) glycoprotein is the VAP, fusion protein, and elicits neutralizing, protective antibody responses
Influenza transcribes and replicates its genome in the target cell nucleus but assembles and buds from the plasma membrane
The antiviral drugs amantadine and rimatadine inhibit an uncoating step and most likely target the M2 protein
The segmented genome promotes genetic diversity caused by mutation and reassortment of segments upon infection with two different strains
Epidemiology of Influenza A and B
DISEASE/VIRAL FACTORSo Influenza is enveloped and is inactivated by detergents o Segmented genome facilitates major genetic strain
changes, especially the targets of the humoral immune response, HA and NA
DISEASE/VIRAL FACTORSo Influenza infects many vertebrate species including other
mammals and birdso Co-infection with animal and human strains of virus can
generate very different virus strains by genetic reassortment
o Transmission of virus often precedes symptoms
TRANSMISSIONo Inhalation of small aerosol droplets released by talking,
breathing, coughingo Virus “likes cool,” less humid atmosphere (e.g. winter
heating season)o Spread extensively by school children
WHO ARE AT RISK?
o Seronegative individualso Adults” Classic “flu syndrome”o Children: Asymptomatic to severe respiratory infectionso High-risk groups: elderly, immunosuppressed individuals
with underlying cardiac or respiratory problems including asthma and smokers
GEOGRAPHY/SEASONo Worldwide occurrence; epidemics local; pandemics
worldwideo Disease more common in winter
Three Species of Influenza Virus (based on matrix (M) and nucleoprotein (NP) antigens):
1. Influenza A2. Influenza B3. Influenza C (does not cause significant human disease)
Genetic Variation in Influenza Virus A:1. Antigenic Drift: - involves Influenza A and B viruses- due to point mutation (two or three amino acid
substitution on the viral polypeptides)- slowly progressive and cumulative- cases more frequent but localized outbreaks (epidemics)2. Antigenic Shift: - only in Influenza A- involves gene swapping or reassortment between two
viruses- herd immunity of previously infected population will not
be effective against the reassortant strains- results in pandemics
Human Influenza Pandemics in the 20th Century SPANISH FLU
o Year – 1918-1919o Subtype – H1N1
o Origin – China? Europe? North America?o Viral genes – contain mammalian and avian geneso Mortality – 25-50 million worldwide;500T in US
ASIAN FLUo Year – 1957o Subtype – H2N2
o Origin – Chinao Viral genes – reassortment with avian viruso Mortality - >1 million worldwide; ~70T in US
HONGKONG FLUo Year – 1968o Subtype – H3N2
o Origin – Chinao Viral genes – reassortment of avian viruso Mortality - >1 million worldwide; ~34T in US
RUSSIAN FLUo Year – 1977o Subtype – H1N1
o Origin – China, Russiao Viral genes – reappearance of 1950s H1N1 virus (from
frozen source?)o Mortality – low mortality worldwide and in the US
Clinical Syndromes Depending on the degree of immunity to the infecting strain of
virus and other factors, the infection may range from asymptomatic to severe. Patients with underlying cardiorespiratory disease or immune deficiency, even that associated with pregnancy, are more predisposed to severe diseases.
After an incubation period of 1 to 4 days, the “flu” syndrome begins with a brief prodrome of malaise and headache lasting a few hours. This is followed by the abrupt onset of fever, severe myalgia, and usually a nonproductive cough. The illness persists for approximately 3 days, then, unless a complication occurs, recovery is complete.
Acute Influenza Infection in Children Acute disease similar to adults but having higher fever,
gastrointestinal symptoms (abdominal pain, vomiting) otitis media, myositis, and croup more frequently
Complications of Influenza Virus Infection Primary viral pneumonia Secondary bacterial pneumonia Myositis and cardiac involvement Neurological syndromes
o Guillain-Barre syndromeo Encephalopathyo Encephalitiso Reye’s syndrome
Laboratory Diagnosis
The characteristic symptoms of influenza combined with the presence of community outbreak are often sufficient for a diagnosis. Influenza viruses from respiratory secretions can generally be isolated in primary monkey kidney cell cultures or Madin Darby Canine Kidney (MDCK) cell line. Occasional strains may require chick embryo inoculation for primary isolation.
Specific identification of the influenza virus requires immunological tests such as immunofluorescence or inhibition of hemadsorption or hemagglutination with specific antibody.
Enzyme immunoassay or immunofluorescence can be used to detect viral antigen in exfoliated cells, respiratory secretion, or cell culture. Serology is too slow to aid the diagnosis and is generally used for epidemiological purposes.
Treatment, Prevention and Control Amantadine and its analogue, rimantadine, are effective for
prophylactic use and for treatment during the first 24 – 48 hours after the onset of Influenza A illness.
Immunization Natural – from prior exposure Formalin inactivated vaccine (strain of the year)
AVIAN INFLUENZA (AI) “Bird Flu” an infectious disease of birds caused by Type A strains of the
influenza virus first identified in Italy in 1878 affecting chickens occurs worldwide
Epidemiology
highly contagious, affecting all avian species incubation period is 3-5 days highly pathogenic avian influenza isolates have been obtained
primarily from chickens and turkeys
Sources of Virus Feces Respiratory secretions
Characteristics of Influenza Virus can survive in feces for several months can survive in water for up to 4 days at 22oC, more than 30
days at 0oC and indefinitely in frozen material killed by alcohol, bleach, formalin, or iodine compounds 5% bleach solution is appropriate for dealing with
biohazardous spillage killed by heat
Time Temperature
3 hrs 56o C30 mins
60o C
1 min 70o C
Transmission: direct contact with secretions from infected birds, especially
feces contaminated feed, water, equipment and clothing clinically normal waterfowl and sea birds may introduce the
virus into the flocks broken contaminated eggs may infect chicks in the incubator
Clinical Types1. Low Pathogenic Avian Influenza (LPAI)
- causes mild disease (decreased egg production, mild respiratory symptoms)
- as it circulate, may mutate w/in 6-9 months into a highly pathogenic strain
2. Highly Pathogenic Avian Influenza (HPAI) (Fowl Plague)- coughing, sneezing, excessive lacrimation- cyanosis of unfeathered skin- edema of the head- ruffled feathers- diarrhea- nervous system disorders- sudden death without clinical signs- due to subtypes H5 0r H7- 100% mortality
Previous Outbreaks of Highly Pathogenic Avian Influenza ITALY
o Year – 1999-2000o Domestic bird affected – turkeyo Strain – H7N1
HONGKONG (CHINA)o Year – 2002o Domestic bird affected – chickeno Strain – H5N1
CHILEo Year – 2002o Domestic bird affected – chickeno Strain – H7N3
NETHERLANDS
o Year – 2003o Domestic bird affected – chickeno Strain – H7N7
Control Measures in Outbreaks slaughtering of all birds (culling) disposal of carcasses and all animal products clearing and disinfection of poultry allow at least 21 days before restocking
Problems associated with outbreaks1. Extremely difficult to control even under favorable conditions
- 1983 Pennsylvania (USA) outbreak took 2 years to control- 1995 Mexico outbreak – H5N2 strain has never been
entirely eliminated up to the present
2. Severe Economic Loss- 1983 Pennsylvania (USA) outbreak:
o 17 million birds were destroyedo direct cost in US is $62 milliono indirect cost in US is $250 million
- 1999-2001 Italyo 13 million birds were destroyed
- 2003 Netherlands (reached Belgium and Germany)o birds destroyed:
30M in Netherlands 2.7M in Belgium 400T in Germany
3. Bird to human transmission- close human contact with live animals provides an ideal
environment for the zoonotic transfer and evolution of infectious disease agent (live animal market or wet markets)
- since 1977, 7 confirmed outbreaks of human infections with avian influenza
Clinical Features HONGKONG 1997
o influenza-like illness with pneumoniao liver dysfunction o abnormal clotting profileso gastrointestinal manifestationso renal failureo pancytopenia (hemophagocytic syndrome)
VIETNAM 2004o of the 10 patients, 9 had direct contact with poultry
(chicken or ducks)o incubation period of 2-4 days (mean 3 days)o fevero cougho diarrheao shortness of breatho lymphopeniao diffuse, multifocal, patch infiltrates or segmented/lobular
consolidationsLaboratory Diagnosis Optimal specimen for Influenza virus detection is
nasopharyngeal aspirate obtained within 3 days of the onset of symptoms, however, nasopharyngeal swabs and other specimen can be used
rapid antigen detection assay - commercially available, provides results in 15-30 minutes but not sensitive or specific
Virus cultureo Enables further antigenic and genetic characterization,
drug susceptibility and vaccine preparationo Takes 2-10 dayso Must be performed under Biosafety level 3+ laboratory
conditions Reverse Transcriptase PCR
o Detects diverse Influenza A viruses including Avian H5N1 strains
o Can be performed in standard Biosafety level 2 laboratory
Treatment, Prevention and Control Indication for laboratory testing
1. Hospitalized Patientso Radiographically confirmed pneumonia, acute respiratory
distress syndrome, or other severe respiratory illness for which an alternate diagnosis has not been established and
o History of travel to a country with documented H5N1 avian influenza within 10 days of symptom onset
2. Case to case basiso Temperature > 38°C and o One or more of the following: cough, sore throat,
shortness of breath and o History of contact with domestic poultry (eg. Visited a
poultry farm, household raising poultry, or bird market) or a known or suspected human case of influenza H5N1 -affected country within 10 days of symptom onset.
Antiviral Treatment:o Current H5N1 strains are resistant to Amantadine and
Rimantandine but sensitive to neuraminidase inhibitors (Oseltamivir and Zanamivir)
Preventive Measures:o avoid contact with poultryo thorough and frequent hand hygiene using soap and
water or alcohol - based hand rubso poultry, including eggs should be cooked thoroughly o Persons involved in outbreak eradication should use
appropriate personal protective equipment (gloves, disposable clothing, shoe covers, safety goggles, and particulate respirators.
Isolation Precautions for patients hospitalized with suspected or confirmed Avian Influenza H5N1
o Standard Precaution – strict hand hygiene before and after all patient’s contact
o Contact Precautions – use gloves and gown for all patient’s contact
o Eye Protection – wear when within 3 feet (1 m) of the patient
o Airborne Precaution – Place patient in an airborne isolation room (negative
air pressure with 6-12 air exchange per hour) Use of fit tested respirator when entering a room (N-
95 filtering facepiece respirator Vaccination
o Human Influenza Vaccine current inactivated trivalent human influenza vaccine
provides no protection against H5 and H7 avian influenza strains.
given to people at risk of avian and human influenza viruses simultaneously and to decrease the possibility of reassortment.
o H5N1 Vaccine a prototype vaccine have been developed using
plasmid-based reverse genetic technology. clinical trials and safety testing must be completed
before it can be commercially available.
RHINOVIRUS (Picornaviridae)
Characteristics Belong to family Picornaviridae More than 100 serotypes Most important cause of the common cold and upper
respiratory tract infections
Epidemiology VIRAL FACTORS
o Resistant to drying and detergento Labile at acidic pHo Optimum growth is at 33C
TRANSMISSION
o Direct contact via infected hand and fomiteso Inhalation of infected droplets
WHO ARE AT RISK?o All ages
Clinical Syndromes Most common cause of common cold – sneezing followed by
rhinorrhea then nasal obstruction Mild sore throat Headache Malaise Fever Chills
Laboratory Diagnosis Unnecessary unless the physician needs to establish which of
the many respiratory viruses cause the illness Culture Serology
Treatment, Prevention and Control Supportive No effective antiviral drug Handwashing and disinfection of contaminated objects are the
best means of preventing the spread of the virus
Viruses in GIT Infections Rotaviruses Norwalk-like agent Coronaviruses Fastidious(Enteric) Adenoviruses Astroviruses Caliciviruses others: Picorna-Parvo-like viruses
Generalities Disease is manifested mainly as diarrhea Affect all age group Sporadic or epidemic form Most cases are self-limited Infection is usually asymptomatic
1. ROTAVIRUSES (from the family Reoviridae)
Most common cause of epidemic diarrhea in infants Can also cause diarrhea in animals Genome: 11 segments of ds:RNA Groups A-F have been described Group A: most common cause of GE in children
Epidemiology Transmission: fecal-oral route Most cases are sporadic Cases are worse in developing countries
Clinical Manifestations Abrupt onset of diarrhea Usually non-bloody & non-mucoid Other S/S: fever & vomiting Most severely affected: infants 6-24 months old Incubation period: 2-5 days Duration of Illness About one week Usual complications: dehydration & metabolic acidosis Diarrhea is due to decreased absorption
Host Response Initially: IgM Followed by: IgG & secretory IgA
Diagnosis Cell culture EM, IEM, ELISA LPA, Gel Electrophoresis
Treatment & Prevention Supportive Immunization
2. NORWALK-LIKE GROUP (miscellaneous virus) Small, non-enveloped 27nm particle with ss-RNA genome Self-limited gastroenteritis 1969: GE outbreak in Norwalk, Ohio
Epidemiology Usually occurs in schools, recreational camps, nursing homes Infection is mainly through food & water and person-to-person Agent occurs worldwide & outbreaks all-year round
Clinical Infection Most have: nausea, vomiting, abdominal pain About half: diarrhea Some: chills & fever Symptoms lasts for 24 hours Stools: non-bloody & non-mucoid
Diagnosis Best: IEM & RIA RIA & ELISA: most efficient in detecting soluble & particulate
antigens
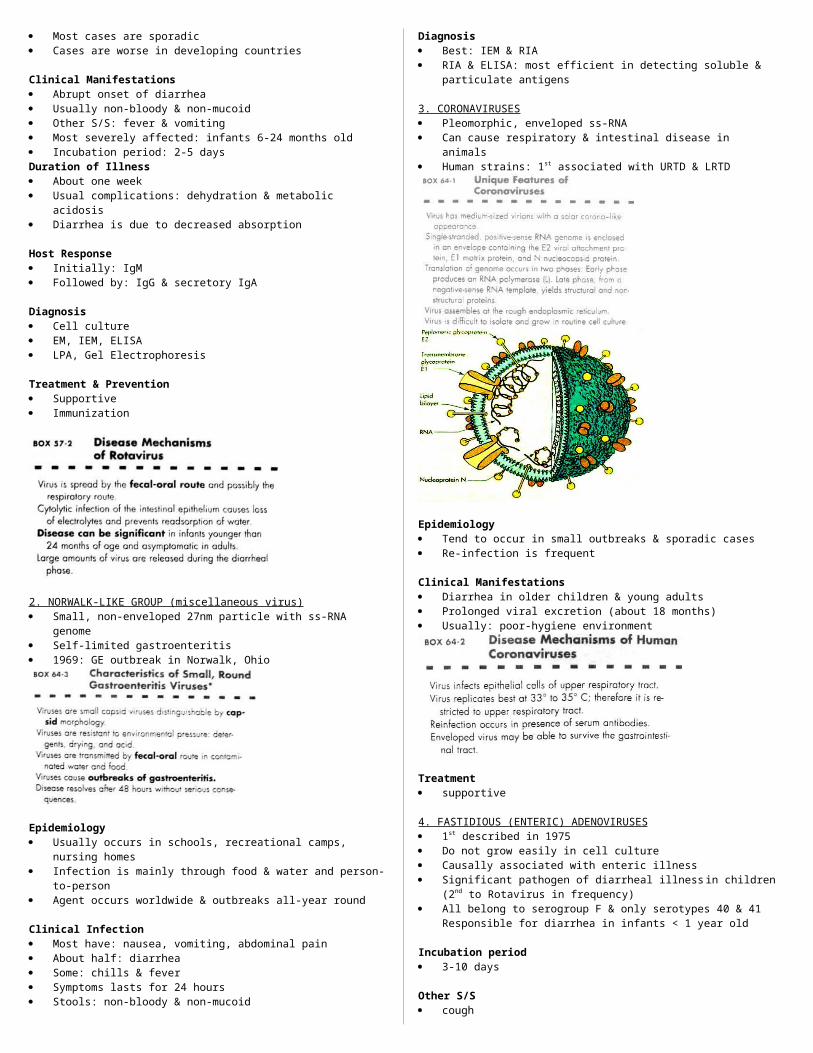
3. CORONAVIRUSES Pleomorphic, enveloped ss-RNA Can cause respiratory & intestinal disease in animals Human strains: 1st associated with URTD & LRTD
Epidemiology Tend to occur in small outbreaks & sporadic cases
Re-infection is frequent
Clinical Manifestations Diarrhea in older children & young adults Prolonged viral excretion (about 18 months) Usually: poor-hygiene environment
Treatment supportive
4. FASTIDIOUS (ENTERIC) ADENOVIRUSES 1st described in 1975 Do not grow easily in cell culture Causally associated with enteric illness Significant pathogen of diarrheal illness in children (2nd to
Rotavirus in frequency) All belong to serogroup F & only serotypes 40 & 41
Responsible for diarrhea in infants < 1 year old
Incubation period 3-10 days
Other S/S cough rhinorrhea wheezing pneumonia conjunctivitis
Duration Illness: mild to moderate, lasts 6-9 days, occurs any month of
the year
Diagnosis virus in stool (EM, ELISA, etc.)
5. ASTROVIRUSES (miscellaneous virus) Described in 1975 28-30 nm particle Shed in stools in very large numbers Present in the stools of infants with or without acute
gastroenteritis 5-to 6-pointed star-shaped particles Associated with disease in many countries: pediatric wards,
schools, nursing homes See Box 64-3
S/S Malaise low-grade fever watery diarrhea for 3 daysDiagnosis EM, IEM, IF of cell cultures
Incubation period 1-3 days
6. CALICIVIRUSES (miscellaneous virus)
35-39 nm particles ‘star of David’ appearance 5 antigenic types Almost all children are (+) for antibodies by 5 years Diarrhea & asymptomatic infections have been documented See Box 64.3
Illness similar to Rotavirus diarrhea
Transmission
Fecal-oral spread occurs, as well as food-borne
Diagnosis
EM, IEM, ELISA
7. OTHER VIRUSES
A. PICORNA-PARVOVIRUS-LIKE o have also been isolated in stools of patients with
diarrhea & asymptomatic patients
B. MINIREOVIRUS & MINIROTAVIRUS o have been visualized in stools of children with
diarrhea & in infants who have acquired diarrhea within hospital setting
RHABDOVIRUSES
PHYSIOLOGY, STRUCTURE AND REPLICATION
within the envelope, the helical nucleocapsid is coiled symmetrically into a cylindrical structure, giving the appearance of striations.
The nucleocapsid is composed of:o 1 ss (-) RNAo nucleoprotein (N) – major structural protein of the virus
maintains RNA in a configuration acceptable for transcription
protects RNA from ribonuclease digestiono large (L) proteinso nonstructural proteins (NS)
Matrix (M) protein lies between the envelope and the nucleocapsid
L and NS constitute the RNA polymerase Assembly of the virion occurs in 2 places:
o Nucleocapsid – cytoplasmo Envelopment and release – at cell plasma layer
DISEASE MECHANISMS OF RABIES VIRUSRabies is usually transmitted in saliva and is acquired from
the bite of a rabid animalRabies virus is not very cytolytic and seems to remain cell
associatedVirus replicates in the muscle at the site of the bite, with
minimal or no symptoms (incubation phase)The length of the incubation phase is determined by the
infectious dose and the proximity of the infection site to the CNS and brain.
After weeks to months, the virus infects the peripheral nerves and travels up the CNS to the brain (prodrome phase).
Infection of the brain causes classic symptoms, coma, and death (neurological phase).
During the neurological phase, the virus spreads to the glands, skin, and other body parts, including the salivary glands, from where it is transmitted.
Rabies infection does not elicit an antibody response until the late stages of the disease, when the virus has spread from the CNS to other sites.
Antibody can block the progression of the virus.The long incubation period allows active immunization as a
postexposure treatment.
PATHOGENESIS AND IMMUNITY1. virus may directly infect nerve endings by binding to
nicotinic acetylcholine receptors or muscle at the site of inoculation
2. virus remains at the site for days to months before progressing to the CNS
3. virus travels by retrograde axoplasmic transport to the dorsal root ganglia and to the spinal cord
4. affected areas include the hippocampus, BS, ganglionic cells of the pontine nuclei and purkinje cells
5. virus disseminates via afferent neurons to highly innervated sites
6. after the virus invades the brain and SC, an encephalitis develops and neurons degenerate
neutralizing antibodies are not apparent until after the clinical disease is well established
antibody can block the spread of virus to the CNS and to the brain if administered or generated during the incubation period
period is often long enough to allow generation of a therapeutic protective antibody response
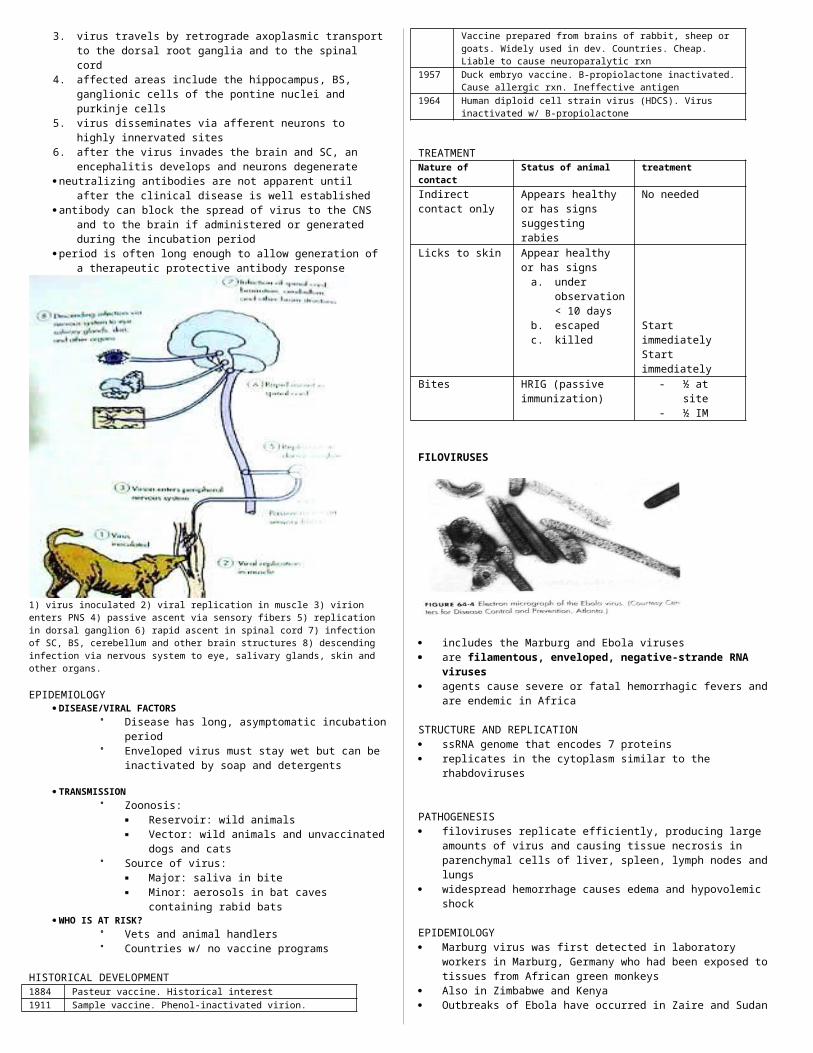
1) virus inoculated 2) viral replication in muscle 3) virion enters PNS 4) passive ascent via sensory fibers 5) replication in dorsal ganglion 6) rapid ascent in spinal cord 7) infection of SC, BS, cerebellum and other brain structures 8) descending infection via nervous system to eye, salivary glands, skin and other organs.
EPIDEMIOLOGY DISEASE/VIRAL FACTORS
Disease has long, asymptomatic incubation period
Enveloped virus must stay wet but can be inactivated by soap and detergents
TRANSMISSION Zoonosis:
Reservoir: wild animals Vector: wild animals and unvaccinated dogs
and cats Source of virus:
Major: saliva in bite Minor: aerosols in bat caves containing rabid
bats WHO IS AT RISK?
Vets and animal handlers Countries w/ no vaccine programs
HISTORICAL DEVELOPMENT1884 Pasteur vaccine. Historical interest1911 Sample vaccine. Phenol-inactivated virion. Vaccine
prepared from brains of rabbit, sheep or goats. Widely used in dev. Countries. Cheap. Liable to cause neuroparalytic rxn
1957 Duck embryo vaccine. B-propiolactone inactivated. Cause allergic rxn. Ineffective antigen
1964 Human diploid cell strain virus (HDCS). Virus inactivated w/ B-propiolactone
TREATMENTNature of contact
Status of animal treatment
Indirect contact only
Appears healthy or has signs suggesting rabies
No needed
Licks to skin Appear healthy or has signs
a. under observation < 10 days
b. escapedc. killed
Start immediatelyStart immediately
Bites HRIG (passive immunization)
- ½ at site- ½ IM
FILOVIRUSES
includes the Marburg and Ebola viruses are filamentous, enveloped, negative-strande RNA
viruses agents cause severe or fatal hemorrhagic fevers and are
endemic in Africa
STRUCTURE AND REPLICATION ssRNA genome that encodes 7 proteins replicates in the cytoplasm similar to the rhabdoviruses
PATHOGENESIS filoviruses replicate efficiently, producing large amounts of
virus and causing tissue necrosis in parenchymal cells of liver, spleen, lymph nodes and lungs
widespread hemorrhage causes edema and hypovolemic shock
EPIDEMIOLOGY Marburg virus was first detected in laboratory workers in
Marburg, Germany who had been exposed to tissues from African green monkeys
Also in Zimbabwe and Kenya Outbreaks of Ebola have occurred in Zaire and Sudan
CLINICAL SYNDROME most severe causes of viral hemorrhagic fevers begins w/ influenza-like symptoms death occurs in as many as 90% of patients w/ clinically
evident disease
LABORATORY DIAGNOSIS handling requires level 4 isolation procedures Marburg – can be grown on tissue culture Ebola – needs animal host Infected cells have large eosinophilic cytoplasmic inclusion
bodies Antigens can be detected by immunofluorescence
TREATMENT antibody-containing serum and interferon therapies
SUBACUTE SPONGIFORM ENCEPHALOPATHIES AND UNCONVENTIONAL AGENTS cause spongiform encephalopathies (slow neurodegenerative
diseases) include the human diseases kuru, Creutzfeldt-jakob disease
(CJD), Gerstmann-Straussler-Scheniker (GSS) disease, and fatal familial insomnia (FFI)
include the animal diseases scrapie, bovine spongiform encephalopathy (mad cow disease), chronic wasting disease and transmissible mink encephalopathy
it has no virion structure or genome, no immune response is elicited and agents are resistant to inactivation by heat, disinfectants and radiation
The slow virus agent appears to be a modified host protein known as a prion (a small proteinaceous infectious particle)
Long incubation period which can last 30 years in humans
STRUCTURE AND PHYSIOLOGY the slow virus agents were suspected to be viruses because
they can pass through filters that block the passage of particles greater than 100nm
the prototype of these agents is scrapie; scrapie-infected hamsters have scrapie-associated fibrils in their brain; these are infectious and contain prions
prions lack detectable nucleic acids and consists of aggregates of protease-resistant, hydrophobic glycoprotein
PATHOGENESIS
spongiform encephalopathy – characteristic degeneration of neurons and axons of the gray matter that occurs in affected patients
vacuolation of the neurons, formation of amyloid-containing plaques and fibrirls, proliferation and hypertrophy of astrocytes, fusion of neurons and adjacent glial cells
no inflammation or immune response to the agent is generated
incubation for CJD and kuru may be as long as 30 yrs but the patient dies w/in a year when symptoms become evident
EPIDEMIOLOGY DISEASE/VIRAL FACTORS
Agents are impervious to standard viral disinfection procedures
Diseases have very long incuation periods (30
yrs)
TRANSMISSION Transmission is via infected tissue, or
syndrome may be inherited Infection occurs through cuts in skin,
transplantation of contaminated medical devices and potentially through ingestion of infected tissue
WHO IS AT RISK? Women and children of the Fore tribe in New
Guinea were at risk for kuru Surgeons, transplant and brain surgery patients
CLINICAL SYNDROMEcause a progressive, degenerative neurological disease w/
long incubation period but with rapid progress to death after onset of symptoms
loss of muscle control, leading to shivering, myoclonic jerks, tremors, loss of coordination and progressive dementia
LABORATORY DIAGNOSISno methods for directly detecting virus using EM, antigen
detection or nucleic acid probes no serological tests can detect antibody diagnosis is made on clinical grounds w/ confirmation by the
characteristic histological changes in brain tissue
TREATMENT, PREVENTION, CONTROLno treatment for kuru or CJD autoclaving at 15 psi for 1 hr, treatment w/ 5% hypochlorite
solution or 1.0M sodium hydroxide
ENTEROVIRUS
infections are usually asymptomatic do not usually cause enteric disease but are transmitted by
the fecal-oral route Poliovirus is the prototype The upper respiratory tract, oropharynx and intestinal tract
are portals of entry Virions are impervious to stomach acid, proteases and bile Replication is initiated in the mucosa and lymphoid tissue of
the tonsils and pharynx, it later infects the peyer’s patches and underlying intestinal mucosa
Primary viremia – spreats virus to receptor-bearing target tissues (where 2nd phase of replication begins)
In polioviruses – the virus must cross the blood-brain barrier or may gain access to the brain by infecting skeletal muscle and traveling up the innervating nerves to the brain
Polio virus has one of the narrowest tissue tropisms, recognizing a receptor expressed on anterior horn cells of
the spinal cord, dorsal root ganglia, motor neurons, skeletal muscle cells, lymphoid cells
Coxsackieviruses and echoviruses recognize receptors expressed on more cell types and tissues
Receptors are rpesent on cells of the CNS, heart, lung, pancrease, mucosa
Most enteroviruses are cytolytic, replicating rapidly and causing direct damage to target cells
Antibody is the major protective immune response to the enteroviruses; it can prevent initial infection in the oropharynx and GIT; prevents spread to target tissue
Cell-mediated immunity is not usually involved in protection but may play a role in pathogenesis
pathogenesis of enterovirus infection. The target tissue infected by the enterovirus determines the predominant disease caused by the virus.
EPIDEMIOLOGY DISEASE/VIRAL FACTORS Infection is often asymptomatic Virion is resistant to environmental conditions
(detergents, acid, drying, mild sewage treatment and heat)
TRANSMISSION Fecal-oral route; poor hygiene, dirty diapers Ingestion via contaminated food and water Contact w/ infected hands and fomites Inhalation of infectious aerosols
WHO IS AT RISK? Young children: at risk for polio (asymptomatic or mild
disease) Older children/adults: polio (asymptomatic or paralytic
disease) Newborns and neonates: highest risk for coxsackievirus
and enterovirus disease
CLINICAL SYNDROMES ASSOCIATED WITH MAJOR ENETROVIRUS GROUPSSYNDROME OCCURREN
CEPOL
COXA
COXB
ECHO
Paralytic disease Sporadic + + + +Encephalitis, meningitis Outbreaks + + + +carditis Sporadic + + +Neonatal disease Outbreaks + +Pleurodynia Outbreaks +Herpangina Common +Hand-foot-and-mouth disease Common +Rash disease Common + + +Acute hemorrhagic conjunctivitis
Epidemics +
Respiratory tract infections Common + + + +Undifferentiated fever Common + + + +Diarrhea, gastrointestinal disease
Uncommon +
Diabetes, pancreatitis Uncommon +

Orchitis Uncommon +Disease in immunodeficient patients
+ + +
Congenital anomalies Uncommon + +CLINICAL SYNDROMES
incubation period for enterovirus disease varies from 1-35 days, depending on the virus, target tissue and the person’s age
viruses that affect oral and respiratory sites have the shortest incubation periods
poliovirus may cause one of four outcomes in unvaccinated people, depending on the progression of the infection
1. Asymptomatic illness. Infection limited to the oropharynx and gut. At least 90% are asymptomatic
2. Abortive poliomyelitis (minor illness). Non-febrile illness, 5%. Fever, headache, malaise, sore throat, vomiting
3. Nonparalytic poliomyelitis (aseptic meningitis). 1-2%. Virus progresses into the CNS and the meningitis, causing back pain and muscle spasms + symptoms of minor illness
4. Paralytic polio (major illness). 0.1-2%. Appears 3-4 days after the minor illness has subsided, producing a biphasic illness. Virus spreads from blood to anterior horn cells of SC and motor cortex of the brain. - Paralytic poliomyelitis. Characterized by
asymmetrical flaccid paralysis with no sensory loss.- Bulbar poliomyelitis. Involve the muscles of the
pharynx, vocal cords and respiration. Results in death of 75% of patients
- Postpolio syndrome. Sequelae of poliomyelitis that may occur much later in life (30-40 yrs)
Progression of poliovirus infection. Infection may be asymptomatic or progress to minor or major disease.
Coxsackievirus and Echovirius Infections
coxsackie A viruses are assoc with diseases with vesicular lesions (herpangina) whereas coxsackie B (b for body) are associated with myocarditis and pleurodynia.
Herpangina is casued by several types of coxsackie A virus. Fever, sore throat, pain…
Classic finding is vesicular ulcerated lesions around the soft palate and uvula
Virus can be recovered from lesions or feces Requires only symptomatic management
Hand-foot-and-Mouth disease is a vesicular exanthema caused by an enterovirus usually cox A16.
Lesions on hands, feet, mouth and tonguePleurodynia (Bornholm disease) aka devil’s grip, is a
acute illness in w/c patients have sudden onset of fever and unilateral low thoracic, pleuritic chest pain
Myocardial and Pericardial infections caused by coxB. Neonates have febrile illnesses and sudden onset of unexplained heart failure
Cyanosis, tachycardia, cardiomegaly and hepatomegaly occur
Acute benign pericarditis affects young adults; symptoms resemble those of MI but fever is more severe.
Viral (aseptic) meningitis, acute febrile illness accompanied by headache and signs of meningeal irritation including nuchal rigidity.
Petechiae or skin rash may occur in patients
Fever and rash may occur in Px infected with Echo and Cox. Eruptions are usually maculopapular but may occasionally be petechial or vesicular
Transmission of enteroviruses. The capsid structure is resistant to mild sewage treatment, saltwater, detergents, and temp changes, allowing these viruses to be transmitted by fecal-oral route and on hands.
LABORATORY DIAGNOSISClinical chemistry
CSF from poliovirus or enterovirus aseptic meningitis reveals a predominantly lymphocytic pleocytosis
In viral meningitis, the CSF glucose level is usually normal or slightly low
Culture Poliovirus may be isolated from patient’s
pharynx It grows well on monkey kidney tissue culture The specific type of enterovirus can be
determined by using specific antibody and assays (IF, ELISA)
Serology Detection of IgM or finding a 4-fold increase in
Ab titer bet time of acute illness and period of convalescence
TREATMENT, PREVENTION AND CONTROLno specific antiviral therapysupportive therapy
2 types of polio vaccine exist
inactivated polio
vaccine (IPV) live attenuated oral polio vaccine (OPV).
- both are effective but OPV is used due to its ease of delivery and capacity to elicit a lifelong immunity
serum and secretory antibody response to intramuscular inoculation of IPV and to live attenuated OPV. Note the presence of secretory IgA induced by the live polio vaccine.
ARBOVIRUSES The members of the Togaviridae and Flaviviridae families are
enveloped, positive, ssRNA viruses Most are transmitted by arthropods and are therefore
arboviruses (arthropod borne) The Togaviruses can be classified into three major genera
1. Alphavirus2. Rubivirus (Rubella virus)3. Arterivirus
The Flaviviridae include:1. flaviviruses2. Pestivirus3. hepatitis C and G
Alphaviruses and Flaviviruses are discussed together because of similarities in the disease they cause and their epidemiology
ALPHAVIRUSES AND FLAVIVIRUSES
Historically classified as arboviruses, because they are usually spread by arthropod vectors: arthropod-borne
Host: vertebrates & invertebrates Hepatitis C: recently classified as a Flavivirus
Epidemiology (of Togavirus and Flavivirus Infection) Both alpha- and flaviviruses are prototypical arboviruses Most common vector: mosquito Others: ticks & sandflies Usual reservoir: birds & small mammals
DISEASE/VIRAL FACTORSo Enveloped virus must stay wet and can be inactivated by
drying, soap, and detergents.o Virus can infect mammals, birds, reptiles, and insectso Asymptomatic or nonspecific (flulike fecer or chills),
encephalitis, hemorrhagic fever, or arthritis.
TRANSMISSIONo Togaviruses and flaviviruses: specific arthropods
characteristic of each virus (zoonosis: arbovirus).
WHO IS AT RISK?o People who enter ecological niche of arthropod:
arboviruses
GEOGRAPHY/SEASONo Endemic regions for each arbovirus are determined by
habitat of mosquito or other vectoro Aedes mosquito, which causes dengue and yellow fever,
is found in urband areas and in pools of water.o Culex mosquito, which causes St. Louis encephalitis, is
found in forest and urban areas.o Disease is more common in summer
MODES OF CONTROLo Mosquito breeding sites and mosquitoes should be
eliminatedo Live attenuated vaccines are available for yellow fever
virus and Japanese encephalitis virus.
Patterns of alphavirus and flavivirus transmission. The cycle of arbovirus transmission maintains and amplifies the virus in the environment. Host-vector relationships that can provide this cycle are indicated by the double arrow. “Dead-end” infections with not transmission of the virus back to the vector are indicated by the single arrow. For St. Louis encephalitis, yellow fever, and dengue viruses, humans are not dead-end hosts and support an urban cycle. The Russian spring-summer encephalitis virus can be transmitted to humans by a tick bite and in milk form from infected goats.
ALPHAVIRUSES
1. Venezuelan Equine Encephalitis2. Eastern Equine Encephalitis3. Western Equine Encephalitis4. Chikungunya5. Semliki6. Sindbis
FLAVIVIRUSES1. Dengue2. Yellow Fever3. Japanese Encephalitis4. West Nile5. St. Louis Encephalitis6. Russian spring-summer encephalitis7. Powassan
Arboviruses (main characteristics)1. Should infect both vertebrates & invertebrates2. Initiate a sufficient viremia in the vertebrate host to allow
acquisition by the invertebrate vector3. Initiate a persistent infection of the salivary gland of the
vector to provide virus for infecting other vertebrate hosts
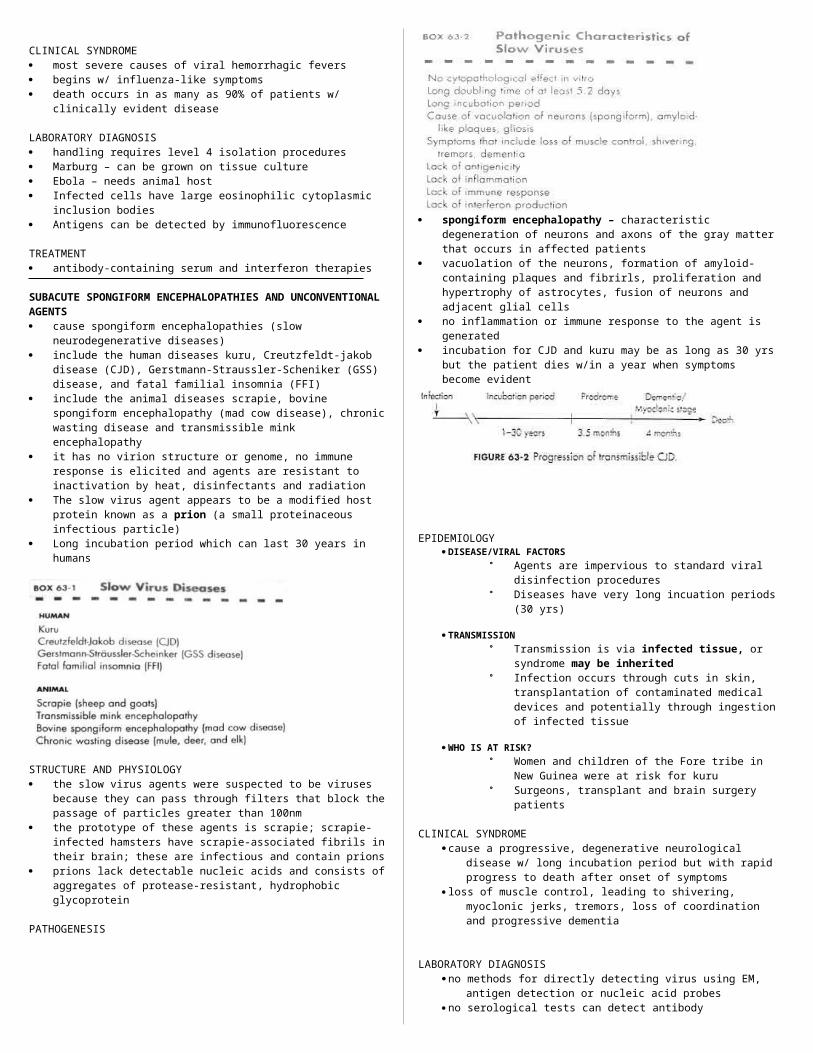
Clinical Syndromes Infection with Alphaviruses
o EEE,WEE,VEE: can progress to encephalitis in humanso S/S: chills, fever, rash, acheso Sindbis & Chikungunya: cause only systemic disease
more of a problem to livestock than to humans…
Infection with Flaviviruseso relatively benign (although encephalitis or hemorrhagic
disease can still occur)o encephalitis viruses : St. Louis, Japanese, Murray Valley,
Russian spring-summero hemorrhagic viruses : Dengue & Yellow Fever
DENGUE Usually mild & self-limited but when re-challenged with a
related strain can cause severe hemorrhagic/shock symptoms DHF/DSS: due to rupture of vasculature, internal bleeding, loss
of plasma Pathogenesis Lesions are in small blood vessels, with endothelial swelling,
perivascular edema and mononuclear infiltrates
DHF/DSS are altered manifestations of dengue, often in epidemic form Pathogenesis: not well understood, but seems to involve pre-
existing dengue antibodies DHF: abrupt course & is assoc with hypoprotenemia,
thrombocytopenia, prolonged BT, elevated PT DSS: characterized by shock & hemoconcentration
YELLOW FEVER Severe systemic disease with degeneration of liver, kidney,
heart & hemorrhage of blood vessels Lesions are due to the localization & propagation of the virus
in a particular organ Mortality: as high as 50%
Laboratory Diagnosis Cell culture (both vertebrate & invertebrate cell line) Cytopathology, IF, hemadsorption of avian erythrocytes ELISA, HI, LPA
Tx, Prev’n, Control Mainly supportive No specific treatment Vector elimination Avoidance of endemic places Vaccination: Yellow Fever, Jap enceph, EEE, WEE, Russian
spring-summer Vaccine for VEE: only for domestic animals
Disease syndromes of alphaviruses and flaviviruses. Primary viremia may be associated with mild systemic disease. Most infections are limited to this. If sufficient virus is produced during the secondary viremia to escape immune protection and to reach critical target tissue, severe systemic disease or encephalitis may result. For dengue hemorrhagic fever (DHF), which can cause dengue shock syndrome (DSS) because of the loss of luids from the vasculature.
Disease Mechanisms of Togavirus and Flavivirus Viruses are cytolytic, except for rubella. Viruses establish systemic infection and viremia. Viruses are good inducers of interferon, which can account for
the influenza-like symptoms of infection. Viruses, except rubella and hepatitis C, are arboviruses Flaviviruses infect cells of the monocyte-macrophage lineage. Non-neutralizing antibody can enhance flavivirus infection via
Fc receptors on the macrophage.
Influenza-like syndrome
Encephalitis
Hepatitis
Hemorrhage
Shock
Dengue + + + +Yellow F. + + + +St. Louis E + +Venezuelan E
+ +
Western equine E
+ +
Eastern equine E
+ +
Japanese E + +
ARENAVIRUSESGeneralities Include lymphocytic choriomenigitis(LCM) & hemorrhagic
fever viruses (Lassa fever, Junin, Machupo) Zoonoses (persistent infection of specific rodents) Virus becomes endemic in the habitat of the rodent
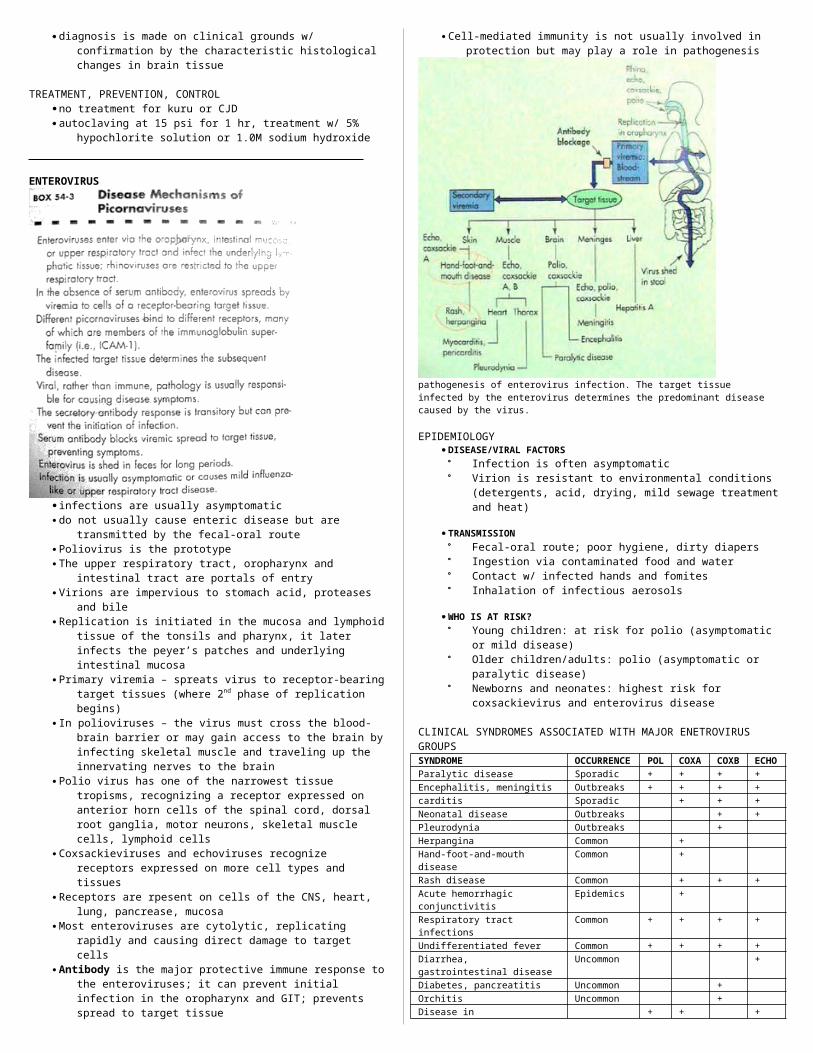
Pathogenesis Infect macrophages, cause vascular damage and tissue
destruction
Epidemiology Mainly found: tropical Africa & South America Infect specific rodents & are endemic to their habitat Infection of humans: aerosol, contamination of food or
fomites Human-to-human: Lassa fever
Clinical Manifestations Lymphocytic Choriomenigitis
o fever with myalgia occurs more often than meningitiso menigeal illness: subacute & persists for several months o brain & meninges: perivascular mononuclear infiltrates
Lassa Fever, etc.o endemic: West Africa, Argentina (Junin), Bolivia
(Machupo)o S/S: fever, coagulopathy, petechiae, occasional visceral
hemorrhages, liver & spleen necrosiso others: pharingitis, diarrhea, vomitingo Dx: recent travel to endemic areas
Laboratory Diagnosis Serology (due to the danger of routine isolation)
Tx, Prev’n, Control For Lassa fever: Ribavirin (although with limited activity) Supportive Limit contact with vectors