ventricular arrhythmias of ischaemia/reperfusion; means of...
TRANSCRIPT
Ventricular arrhythmias of ischaemia/reperfusion;
Means of prevention
Cardiac electrophysiology course 2008
Rita PappPhD studentLaboratory of Haemodynamics

Background: CAD = Coronary Artery Disease (degenerative alterations in the media and intima of blood vessels, endothel damage, atheroma plaque)
"Ischo" = „retention" "haima" = „blood„ (greek)
• „Insufficient perfusion of the myocardium" (Opie)• „Lack of arterial circulation" (Jennings)• „Imbalance between demand/supply" (Schelbert)
Basic concept: Imbalance between myocardial blood demand and blood supply
The concept of myocardial ischaemia

Coronary stenosis, occlusion
blood supply ↓/blood demand↑
Physical/emotional stress
reduced perfusion
reduced heart function
metabolic alterations
electrophysiological changes,
arrhythmias
Consequences of myocardial ischaemia

Severity of ischaemia is influenced by:• physical, emotional stress (increases blood demand)• extent of blood supply reduction, which depends on:
location of stenosis extent of stenosis collateral circulation
• duration of ischaemia (<5’ occlusion is reversible, <15-20’ reversible but needs time to recover, >20-30’ irreversible)
:Ischaemic area
proximal
distal
sten
osis occlusion
goodcollateral circulation
poor collateral circulation

Normal perfusion Mild ischaemia
glucose
pyruvate
extracell. glucose glycogen
lactate
ATP
extracell. fatty acid
fatty acid
O2
O2-
F1F0CP
NAD+NADH
ADP+Pi ATP
Krebs cycle
ox. phosph.
glucose
pyruvate
extracell. glucose glycogen
lactate
ATP
extracell. fatty acid
fatty acid
O2
O2-
F1F0CP
NAD+NADH
ADP+Pi ATP
Krebs cycle
ox. phosph.

Normal perfusion Severe ischaemia
fatty acid
glucose
pyruvate
extracell. glucose glycogen
lactate
ATP
extracell. fatty acid
O2
O2-
F1F0CP
NAD+NADH
ADP+Pi ATP
Krebs cycle
ox. phosph.
-glucose
pyruvate
extracell. glucose glycogen
lactate
ATP
extracell. fatty acid
fatty acid
O2
O2-
F1F0CP
NAD+NADH
ADP+Pi ATP
Krebs cycle
ox. phosph.

0
5
10
15
20
25
30
35
40
0 5 10 15 20 25 30 35 40 45 50 55 60
Num
ber o
f ext
rasy
stol
es
Duration of ischaemia (min)
1a 1b
Arrhythmias may occur after some minutes of ischaemia already
LADLAD
LCXLCX• Canine model of ischaemia/reperfusion • Occlusion of the left anterior descendens (LAD) coronary artery• LCX: ramus circumflexus of the left coronary

nucleusnucleusSER
Lactate ↑H+ ↑ ATP ↓
pH ↓ (5.5-6!!)
ADP, Pi ↑
H+
NHE
Na+ ↑
3 Na+
NCX
Ca2+↑
Cellular background of 1a arrhythmias: rapid formation of ionic imbalance
K+↓
K+ ↑
Cl- ↑
IK1IKATP
H2O
• H+, Na+i, Ca2+
i ↑, K+ loss
• Lactate, H+, Na+, ADP, Pi: water influx, oedema

• Increased Ca2+i: diastolic relaxation ↓,
→ end-diastolic pressure, preload ↑
• Low ATP: contraction force weakens, hybernation, reversible (rapidly recovers following reperfusion)
Effects on heart function and ST segmentHeart function:
++
occlusion
++++++++
++++----------
current++
• KK++ efflux in the ischaemic area: it becomes efflux in the ischaemic area: it becomes positively chargedpositively charged→ injury current flows here from normal areas→ injury current flows here from normal areas• visible on the ECG, ST-elevationvisible on the ECG, ST-elevation
• Appears within Appears within minutes, minutes, correlates with correlates with ischaemia severityischaemia severity
ST segment:

Electrophysiological consequences
• pOpO22, K, K++, pH gradients, pH gradients• Changes are most severe in Changes are most severe in the ischaemic centrum and the ischaemic centrum and usually in the endocardium usually in the endocardium → → slow conduction, blocksslow conduction, blocks• Border of the ischaemic and Border of the ischaemic and the normal zone: heterogenous the normal zone: heterogenous → → favors arrhythmogenesisfavors arrhythmogenesis
AP
• depolarization, resting membrane potential ↓• Na+ channel inactivation, slow AP upstroke, both AP duration and amplitude ↓• slow and discontinuous impulse propagation, conduction blocks

Ventricular arrhythmias Extrasystole (ES)blood pressure
left ventricular pressure
LV contractility (+/-dP/dt)
inhomogeneity of activation
epicardial ECG 1-2 ↕
coronary flow
limb ECG, lead II
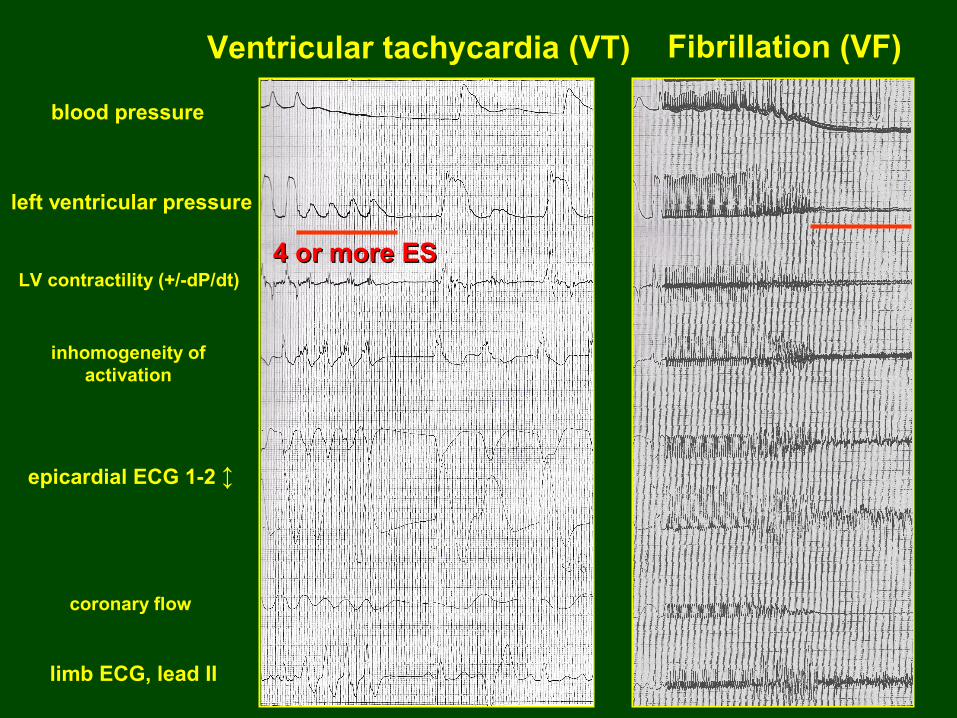
Ventricular tachycardia (VT) Fibrillation (VF)
blood pressure
left ventricular pressure
LV contractility (+/-dP/dt)
inhomogeneity of activation
epicardial ECG 1-2 ↕
coronary flow
limb ECG, lead II
4 or more ES4 or more ES
1
2
3
4
1
2
34
Ref.
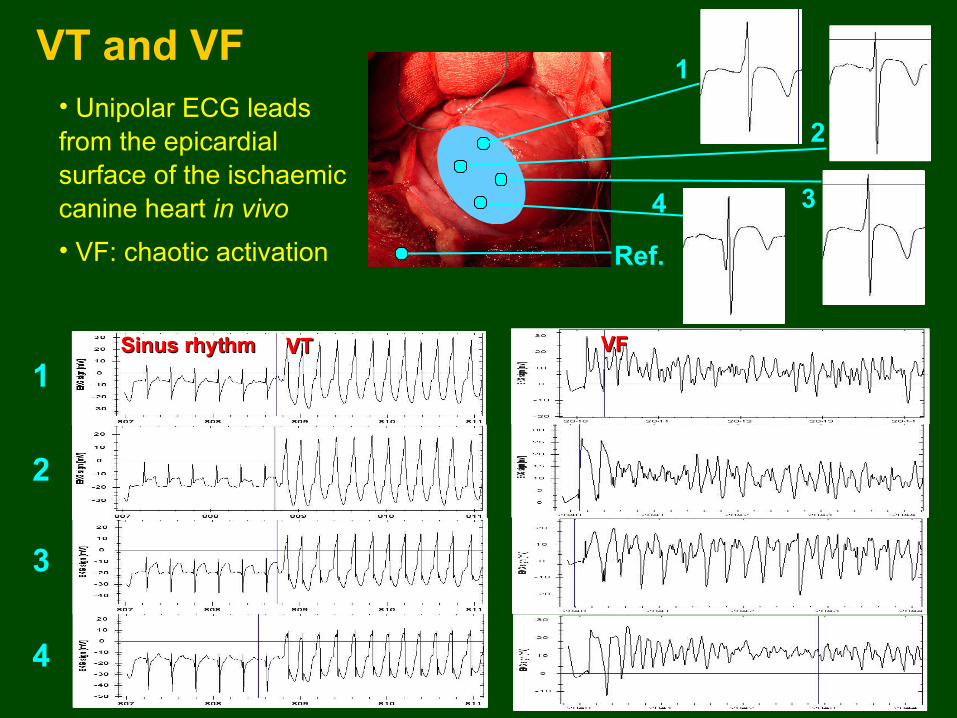
Sinus rhythmSinus rhythm VTVT VFVF
VT and VF• Unipolar ECG leads from the epicardial surface of the ischaemic canine heart in vivo• VF: chaotic activation

Mechanism of 1a arrhythmiasReentryReentryCause: conduction block, inhomogenous reftractoriness→ the activation wave turns back
→ → splitting of the reentry splitting of the reentry circuit into multiple circuit into multiple wavelets: fibrillationwavelets: fibrillation
Reentry in 2D:Reentry in 2D:(Activation map from the epicardium (Activation map from the epicardium of an isolated mouse heart)of an isolated mouse heart)Normal beat ↓
Reentry →

1a arrhythmias are followed by a short arrhythmia free period, then a new arrhythmia phase appearsESES
Time (min)
• 3-8th min of ischaemia• Less severe arrhythmias• Less characterized in human
• 15-25th min of ischaemia• Severe arrhythmias, great mortality, also in human!
0
5
10
15
20
25
30
35
40
0 5 10 15 20 25 30 35 40 45 50 55 60
1a 1b

The 1b phase of arrhythmias is more severe than 1a
123456
1011121314151617181920
789
5 10 15 20 25
ES VT VF
Duration of ischaemia (min)
Model: anaestetised dog, Model: anaestetised dog, LAD occlusionLAD occlusion
↕ 1a ↕ 1b

Causes and mechanism of 1b arrhythmias
sejtmagsejtmagSER
ATP Ø
Na+ ↑
3 Na+
NCX
Ca2+↑
K+ ↑Na+-K+ pump
Membrane Ca2+ ATPase
SERCA
β-ARNA, A
pH ↓
Closure of gap junctions
ATP is lost, ATP-ases stop, catecholamine- release: Ca2+
i ↑
Delayed afterdepolarization (DAD), if threshold (TP) is reached,
focal arrhythmias occur
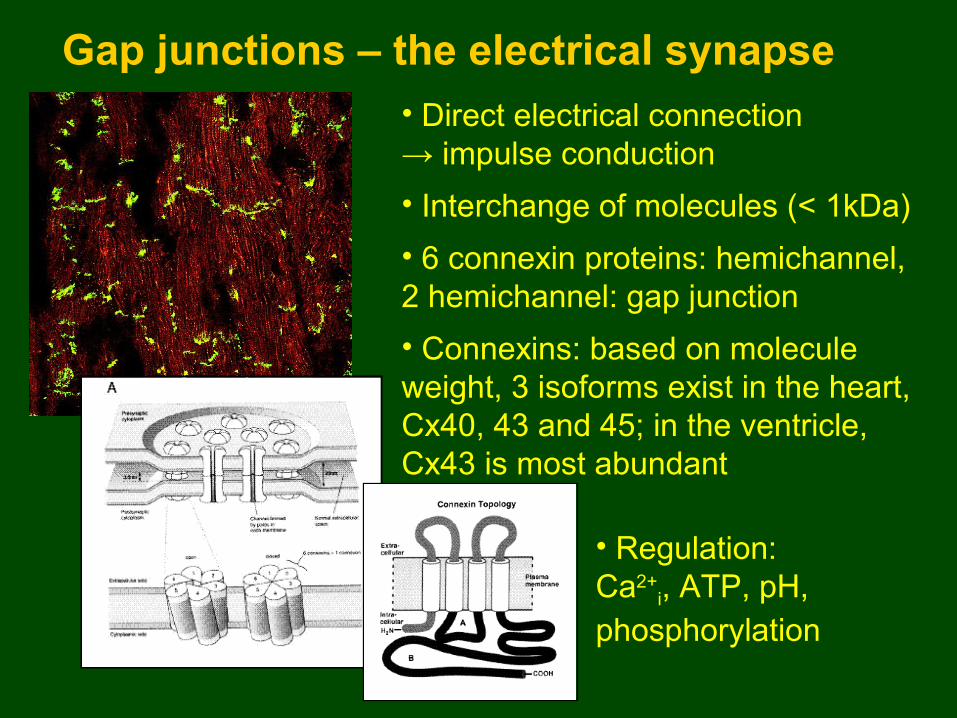
Gap junctions – the electrical synapse• Direct electrical connection → impulse conduction• Interchange of molecules (< 1kDa)• 6 connexin proteins: hemichannel, 2 hemichannel: gap junction• Connexins: based on molecule weight, 3 isoforms exist in the heart, Cx40, 43 and 45; in the ventricle, Cx43 is most abundant
• Regulation: Ca2+
i, ATP, pH, phosphorylation

Closure of gap junctions (uncoupling) due to high Ca2+
i and its measurement
Model: isolated papillary Model: isolated papillary muscle of the rabbitmuscle of the rabbit
Steep rise of Ca2+i and
uncoupling overlap in time
CaCa2+2+
uncouplinguncoupling
Measurement of uncoupling:Electrical impedance (resistivity of an AC circuit)Under-threshold current delivered to the tissue – Voltage is measured
U/I: tissue resistivityU/I: tissue resistivity
Phase delay due to Phase delay due to membranes, proportional membranes, proportional to the extent of uncouplingto the extent of uncoupling

1b arrhythmias coincide with uncoupling in the in vivo canine heart
Time (min)
Number of ES/min
Tissue resistivity (Ohm*cm)
Phase delay (Degree)
Closed GJ
Open GJ
How does uncoupling lead to arrhythmias?
Makes impulse conduction slow and inhomogenousConduction block can be formed
→ Reentry
Closed GJ
Open GJ

Further fate of the tissue:
Ischaemia continuesIschaemia continues,, subacute phase (hours - days) subacute phase (hours - days)
• few and not life-threatening arrhythmias, but:few and not life-threatening arrhythmias, but:
• more severe tissue damage (extensive cell death, both more severe tissue damage (extensive cell death, both apoptotic and necrotic, within 3 or 4 hours)apoptotic and necrotic, within 3 or 4 hours)
ReperfusionReperfusion,, if happens within 2 or 3 hours: a portion of if happens within 2 or 3 hours: a portion of dying cells, which injured reversibly and thus can be dying cells, which injured reversibly and thus can be saved, get a chance to survivesaved, get a chance to survive

Functional changes in the acute/subacute phase of ischaemia (30’– hours, days)
Ca2+↑↑Ca2+↑ nucleusnucleus
OO22--, H, H22OO22, ,
OHOH.., OONO, OONO--proteasesproteases
phospholipasephospholipase
LDH, CKEnzyme loss:
Lysis of contractile proteins
Pores on the membrane: complete ionic imbalance!!
• Free radicals, phospholipase activation Free radicals, phospholipase activation → → membrane damagemembrane damage• Ion and protein loss through the membrane poresIon and protein loss through the membrane pores• Enzyme loss: lactate dehydrogenase, creatine kinase, their levels Enzyme loss: lactate dehydrogenase, creatine kinase, their levels can be measured from the blood, infarct markers +indices of severitycan be measured from the blood, infarct markers +indices of severity• Lysis of the contractile system beginsLysis of the contractile system begins• Ends in cell death, fibrosis on the necrotized area Ends in cell death, fibrosis on the necrotized area → infarct scar→ infarct scar

Reperfusion: rapid recovery (?) of metabolism
Ca2+↑nucleusnucleus
OO22--, H, H22OO22, ,
OHOH.., OONO, OONO--
Neutrophil granulocytes: sources of free radicals!
Endothel damage: permeable, +reactive hyperaemia may absent, danger of no-reflow.
Ca2+↑↑
CaCa2+2+
3 Na3 Na++ NCXNCX
†† ††
• ECG, pH recovers rapidly (2-3 min)
• Ca2+, Na+ levels are still high
• Burst release of free radicals (peaks at 4-7 min of reperfusion)
• Sudden opening of gap junctions: death signals are forwarded to the neighbours
Xanthine oxidaseXanthine oxidase
Passage of death signals
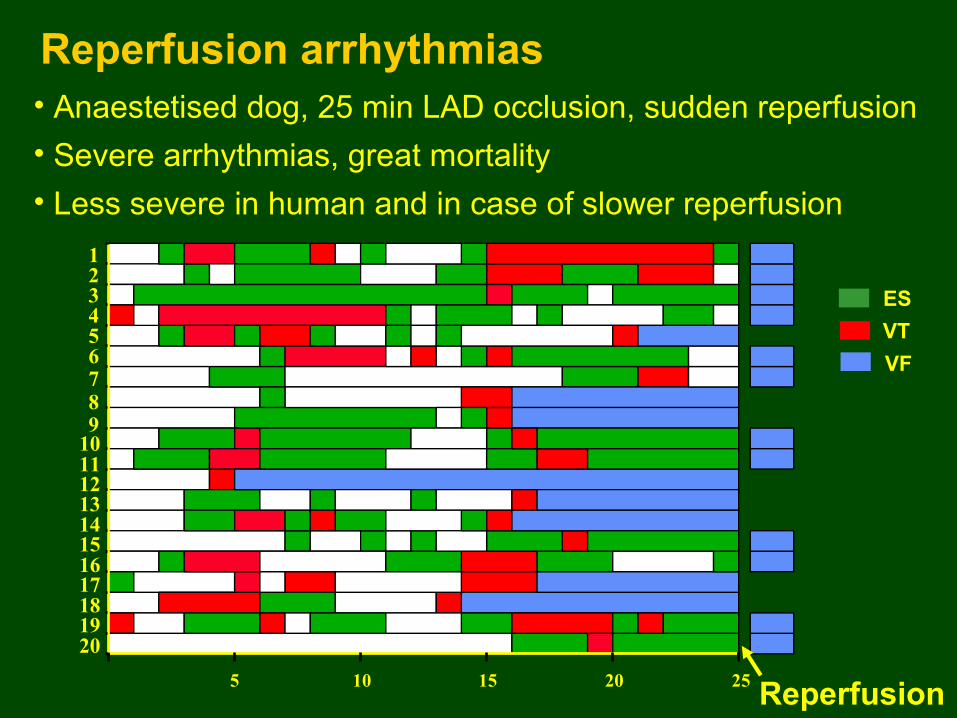
Reperfusion arrhythmias
123456
1011121314151617181920
789
5 10 15 20 25 Reperfusion
ESVTVF
• Anaestetised dog, 25 min LAD occlusion, sudden reperfusion• Severe arrhythmias, great mortality• Less severe in human and in case of slower reperfusion

Consequences of ischaemia/reperfusion• Cell death, infarct scar (fibrosis) – anatomical reentryCell death, infarct scar (fibrosis) – anatomical reentry• Stunning: (Stunning: (≠ hibernation!) ≠ hibernation!) temporary, reversible decrease in temporary, reversible decrease in
contractility in the reperfused tissue, contractility in the reperfused tissue, responds to inotropic agents, decreased Caresponds to inotropic agents, decreased Ca2+2+ sensitivity? sensitivity?
• Heart failure, atrial fibrillationHeart failure, atrial fibrillation• Sympathetic nerve endings die distal to the occlusion site – Sympathetic nerve endings die distal to the occlusion site –
ββ-AR upregulation → -AR upregulation → heterogenous, extremely heterogenous, extremely catecholamine-sensitive area, potential source of further catecholamine-sensitive area, potential source of further arrhythmiasarrhythmias
Anatomical (fix) reentryAnatomical (fix) reentryInf. Inf. scarscar

Prevention of ischaemia/reperfusion injury
1. Pharmacological prevention: improvement of heart function, cholesterol-lowering, application of antioxidants and Ca2+ antagonists during reperfusion
2. To utilize the heart’s own, endogenous adaptation mechanisms
• preconditioning
• postconditioning

Concept of preconditioning„What does not kill you, that makes you stronger” (Nietzsche)
Short, sublethal periods of ischaemia/reperfusion make the heart protected (preconditioned) against adverse outcomes of a subsequent, longer ischaemia/reperfusion insult.
Protocol of classic (ischaemic) preconditioning:
The phenomenon was described in 1986 (Murry The phenomenon was described in 1986 (Murry et alet al.)..).
„Test” ischaemia Reperfusion
Preconditioning
5 min 5 min 25 min20 min 20 min
I IIR R

REPERFUSION
123456
1011121314151617181920
789
21225 10 15 20 250Duration of ischaemia (min)
ES VT VF
Antiarrhythmic effect in the dog in vivo
→ → SurvivalSurvival
123456
1011121314151617181920
789
5 10 15 20 25
Control
Precon-ditioned
ESVTVF

Preconditioning: protection against…• Ischaemia/reperfusion induced arrhythmiasIschaemia/reperfusion induced arrhythmias• Cell death due to ischaemia/reperfusion (delays it)Cell death due to ischaemia/reperfusion (delays it)• Deterioration of heart function during ischaemia as well Deterioration of heart function during ischaemia as well as against stunning (result of ischaemia/reperfusion)as against stunning (result of ischaemia/reperfusion)
Duration of the protected status:Duration of the protected status:
• early phase: provides protection for 1-2 hours after the early phase: provides protection for 1-2 hours after the PC stimulus (signaling events)PC stimulus (signaling events)
• late phase: protection reoccurs 24-48 hour following late phase: protection reoccurs 24-48 hour following the PC stimulus (changes in gene expression)the PC stimulus (changes in gene expression)

Mechanisms of preconditioningPreconditioning stimulus: ischaemia in case of classical PC, Preconditioning stimulus: ischaemia in case of classical PC, but also can be rapid pacing, warm/cold, but also can be rapid pacing, warm/cold, physical exercisephysical exercise → anything which shifts the O→ anything which shifts the O22 demand/O demand/O22 supply balance. supply balance.
„Trigger”:• adenosine• bradikinin• endogenous opiates• NO• free radicals
Mediator:• second messengers (Ca2+)• PKC, ERK, MAPK, Akt kinases• mit. KATP channel
Effector:• NHE, NCX, L-type CaNHE, NCX, L-type Ca2+2+ ch. ch.• sarcolemmal Ksarcolemmal KATPATP channel channel
• gap junctions, mitochondriagap junctions, mitochondria
↓ O2 demand
↓ ATP loss, acidification↓ Ca2+, Na+ overloadImproved conduction
„Test” ischaemia Reperfusion
5 min 5 min 25 min20 min 20 min
I IIR R

Time (min)
Number of ES/min
Tissue resistivity
Phase delay
Preconditioning moderates gap junctional uncoupling during test ischaemia
Control PC
Closed GJ
Open GJ
Closed GJ
Open GJ

Clinical relevance of preconditioningPresent:Present:• existence of the phenomenon is verified in humanexistence of the phenomenon is verified in human• PTCA, coronary angioplasty after infarctPTCA, coronary angioplasty after infarct• heart surgery: short aorta clamping before arresting the heart surgery: short aorta clamping before arresting the heartheart• lifestyle: physical exercise can be of preconditioning effectlifestyle: physical exercise can be of preconditioning effect
Future:Future:• pharmacological preconditioning of people being at risk of pharmacological preconditioning of people being at risk of myocardial infarction, by mimicking the signalization of myocardial infarction, by mimicking the signalization of classic preconditioningclassic preconditioning→ requires exact and complete description of the → requires exact and complete description of the underlying mechanismsunderlying mechanisms
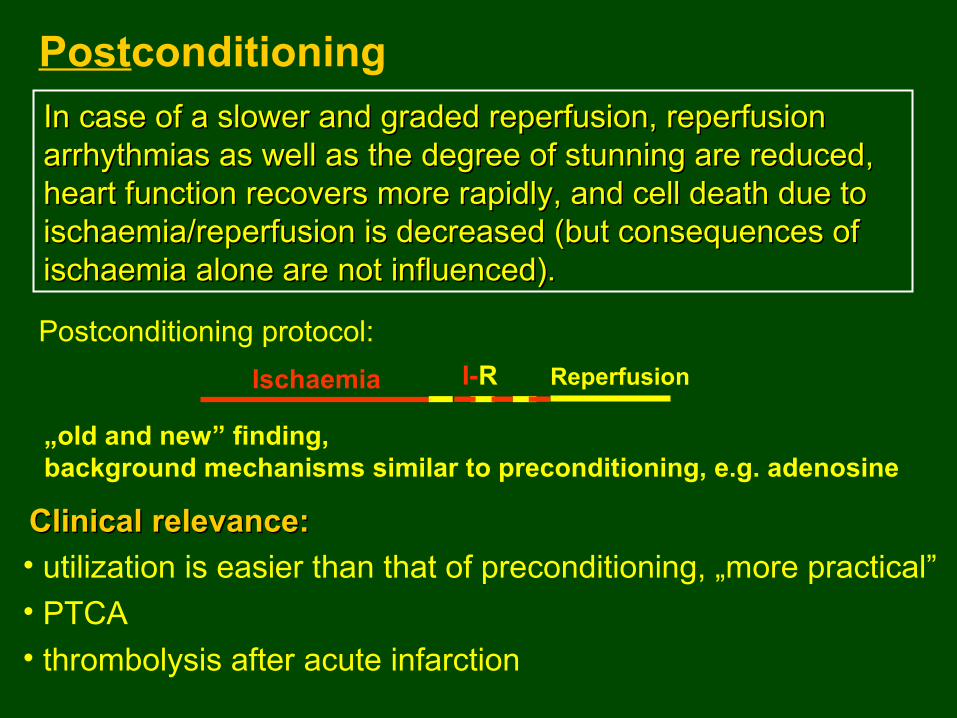
Postconditioning
„old and new” finding, background mechanisms similar to preconditioning, e.g. adenosine
In case of a slower and graded reperfusion, reperfusion In case of a slower and graded reperfusion, reperfusion arrhythmias as well as the degree of stunning are reduced, arrhythmias as well as the degree of stunning are reduced, heart function recovers more rapidly, and cell death due to heart function recovers more rapidly, and cell death due to ischaemia/reperfusion is decreased (but consequences of ischaemia/reperfusion is decreased (but consequences of ischaemia alone are not influenced).ischaemia alone are not influenced).
Clinical relevance:Clinical relevance:• utilization is easier than that of preconditioning, „more practical”• PTCA• thrombolysis after acute infarction
Postconditioning protocol:Ischaemia ReperfusionI-R

Thx
for
your
attention!