update in cardiology: evidence published in 2010 annals of internal medicine 2011
TRANSCRIPT

Update in Cardiology: Evidence Published in 2010
Annals of Internal Medicine 2011

Paper #1Statins and all-cause mortality in high-risk
primary prevention: a meta-analysis of 11 randomized controlled trials involving
65,229 participants
Cambridge, EnglandAccepted for Publication 2009
Statins and all-cause mortality in high-risk primary preventionObjectiveif statin therapy reduces all-cause mortality
among intermediate to high-risk individuals without a history of CVD

Statins and all-cause mortality in high-risk primary preventionBackgroundCV dz is the leading cause of death
worldwideStatins are one of the most commonly
prescribed meds in the US The AHA and American College of Cardiology
suggests prescribing statins to reduce LDL in ppl high risk for heart dz

Statins and all-cause mortality in high-risk primary preventionMethodssearched the databases of MEDLINE and the
Cochrane Collaboration Inclusion criteria were (1) randomized trials
of statins vs placebo/control, (2) trials that collected information on all-cause mortality, and (3) trials conducted among individuals without prevalent CVD at baseline.

Statins and all-cause mortality in high-risk primary preventionIncluded trials: the West of Scotland Coronary Prevention Study (WOSCOPS) the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart
Attack Trial (ALLHAT) Air Force/Texas Coronary Atherosclerosis Prevention Study
(AFCAPS/TexCAPS) Primary Prevention of Cardiovascular Disease with Pravastatin in Japan
(MEGA) the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) the Collaborative Atorvastatin Diabetes Study (CARDS) the Atorvastatin Study for Prevention of Coronary Heart Disease Endpoints
in Non-Insulin-Dependent Diabetes Mellitus (ASPEN) the Justification For The Use Of Statins In Prevention: An Intervention
Trial Evaluating Rosuvastatin (JUPITER) the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER) the Hypertension High Risk Management (HYRIM) trial the Prevention of Renal and Vascular Endstage Disease Intervention Trial
(PREVEND IT)

Statins and all-cause mortality in high-risk primary preventionPopulation:65,229 participants followed for approximately
244,000 person-years, during which 2793 deaths occurred.
Mean age of subjects ranged from 51 to 75 years% women: 0% to 68%% diabetes: 0% to 100%Average baseline LDL-C :138 mg/dL. Average follow-up of 3.7 years The mean LDL-C level among participants allocated
to placebo was 134 mg/dL compared with a mean of 94 mg/dL among those allocated to statins


Statins and all-cause mortality in high-risk primary preventionOutcomes32,606 participants assigned to placebo arm: 1,447
deaths 32,623 participants assigned to statin-treated arm:
1,346 deathsThe risk ratio for all-cause mortality associated with
the use of statins was 0.91 (95% CI, 0.83-1.01)No significant relationship between mean baseline
levels of LDL and the relative reduction in all-cause mortality across studies (P = .97)
No material relationship between mean LDL reduction and reduction in all-cause mortality, whether assessed in relation to absolute (P = .62) or percentage reduction in LDL-C (P = .46)

Date of download: 8/24/2013Copyright © 2012 American Medical
Association. All rights reserved.
From: Statins and All-Cause Mortality in High-Risk Primary Prevention: A Meta-analysis of 11 Randomized Controlled Trials Involving 65 229 Participants
Arch Intern Med. 2010;170(12):1024-1031. doi:10.1001/archinternmed.2010.182

Date of download: 8/24/2013Copyright © 2012 American Medical
Association. All rights reserved.

Statins and all-cause mortality in high-risk primary preventionConclusionsThe use of statin therapy did not result in
reduction in all-cause mortality There were on average an estimated 7 fewer
deaths for every 10 000 person-years of treatment, suggesting that all-cause mortality benefits are more modest in the short term, even among high-risk primary prevention populations
Further caution is needed when extrapolating the potential benefits of statins on mortality to lower-risk primary prevention populations

Statins and all-cause mortality in high-risk primary preventionCautions and future studies Is there possible benefit to long term statin use? These results should be interpreted with caution, since individual
studies varied considerably with respect to the demographic characteristics of the participants, the duration of follow-up, and the type and dose of statins used
Unable to analyze subgroups (women) How did the study define “high risk”? Lowering lipid levels in a very high-risk primary prevention population
is not likely to be harmful, but mortality benefits are likely to be modest
Drugs for asymptomatic patients for lifelong prevention should be proven to help ppl feel better or live longer; statins in asymptomatic patients without CVD does not meet this criterion
Paper #2Multiple testing, cumulative radiation dose, and clinical indications in patients
undergoing myocardial perfusion imaging
Columbia UniversityAccepted for Publication 2010

Multiple testing, cumulative radiation dose, and clinical indications in patients undergoing myocardial perfusion imaging
ObjectiveTo characterize procedure counts,
cumulative estimated effective doses of radiation, and clinical indications for patients undergoing MPI
Multiple testing, cumulative radiation dose, and clinical indications in patients undergoing myocardial perfusion imagingBackgroundThe single test with the highest radiation burden,
accounting for 22% of cumulative effective dose from medical sources, is myocardial perfusion imaging (MPI)
There has been an increase in the burden of ionizing radiation associated with imaging and the potential risks of cancer
The per capita dose of medical radiation in the United States increased nearly 6-fold from the early 1980s to 2006
No data are available characterizing total longitudinal radiation burden, or the association of radiation burden with reasons for testing

Multiple testing, cumulative radiation dose, and clinical indications in patients undergoing myocardial perfusion imagingMethodsretrospective cohort study evaluated
procedure counts, cumulative estimated effective doses of radiation, and clinical indications in a cohort of patients undergoing MPI
All inpatients and outpatients undergoing single-photon emission computed tomography MPI at CUMC/NYPH during the first 100 days of 2006; then looked back from 1988-2008 for all medical imaging

Multiple testing, cumulative radiation dose, and clinical indications in patients undergoing myocardial perfusion imagingPopulation1097 patients, including 565 women (51.5%) Mean age was 62.2 years (SD, 13.1; range, 11.6-
96.8 years)A total of 424 patients (38.7%) were Hispanic,
314 (28.6%) were white, 228 (20.8%) were black, and 131 (11.9%) were other race (eg, American Indian/Alaskan, Asian, Indian [India])
Mean (SD) income for zip code was $39.3 ($23.0) thousand (range, $14.3-$146.8 thousand)

Multiple testing, cumulative radiation dose, and clinical indications in patients undergoing myocardial perfusion imagingOutcomes Patients underwent a median of 15 procedures involving radiation exposure, of
which 4 were high-dose procedures, defined as an effective dose of at least 3 mSv, the equivalent of 1 year's natural background radiation
A total of 200 patients (18.2%) had at least 3 MPIs and 54 (4.9%) had at least 5 MPI examinations
Median cumulative estimated effective dose from MPI alone was 28.9 mSv For all medical testing, median cumulative estimated effective dose was 64.0
mSv Women underwent significantly more procedures involving exposure to ionizing
radiation than men. No significant differences were observed between black, Hispanic, and white
patients in total number of procedures No strong correlation was observed between socioeconomic status (median
income for zip code) and number of MPI examinations, number of ionizing radiation procedures, or cumulative effective dose
Patients without health insurance underwent fewer tests involving radiation and lower cumulative effective dose
There was a trend toward increased odds of undergoing multiple MPI examinations for male patients and patients of higher socioeconomic status

Date of download: 8/24/2013Copyright © 2012 American Medical
Association. All rights reserved.
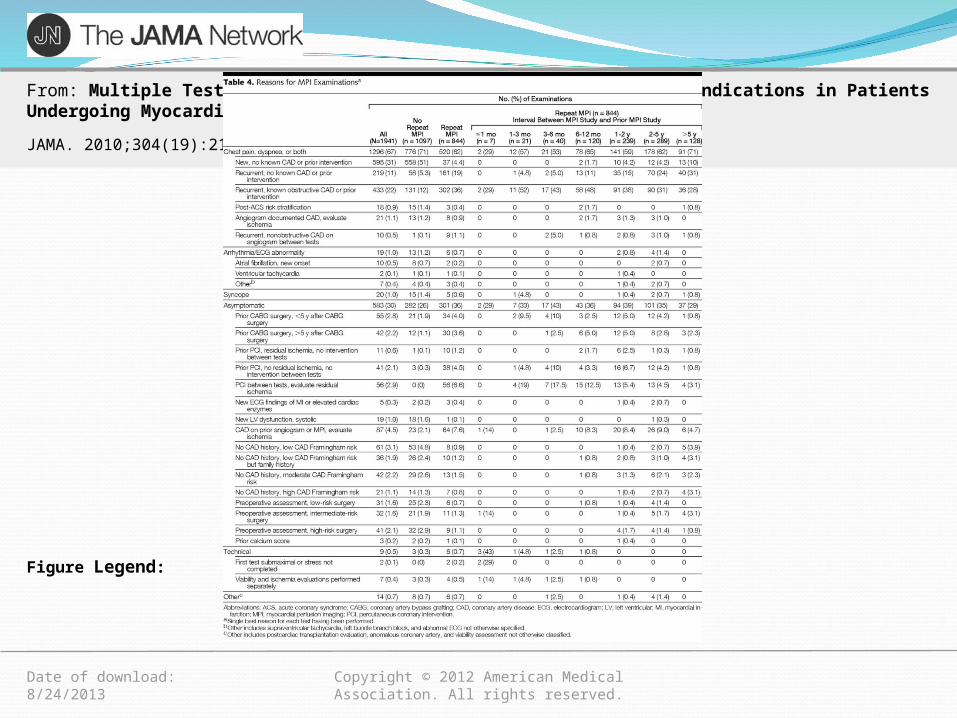
From: Multiple Testing, Cumulative Radiation Dose, and Clinical Indications in Patients Undergoing Myocardial Perfusion Imaging
JAMA. 2010;304(19):2137-2144. doi:10.1001/jama.2010.1664
The inset is the expanded y-axis from x = 100 mSv to x = 500 mSv for myocardial perfusion imaging and from x = 200 mSv to x = 1000 mSv for all procedures. All bins are of width 20 mSv.
Figure Legend:
Date of download: 8/24/2013Copyright © 2012 American Medical
Association. All rights reserved.
From: Multiple Testing, Cumulative Radiation Dose, and Clinical Indications in Patients Undergoing Myocardial Perfusion Imaging
JAMA. 2010;304(19):2137-2144. doi:10.1001/jama.2010.1664
Figure Legend:

Date of download: 8/24/2013Copyright © 2012 American Medical
Association. All rights reserved.
From: Multiple Testing, Cumulative Radiation Dose, and Clinical Indications in Patients Undergoing Myocardial Perfusion Imaging
JAMA. 2010;304(19):2137-2144. doi:10.1001/jama.2010.1664
Figure Legend: Of 1097 patients undergoing index MPI, 424 (38.6%) underwent additional MPI studies. A total of 236 patients (56%) undergoing multiple MPI examinations had 2 examinations within 2 years of each other, and 117 (28%) had 2 MPI examinations within 1 year of each other. Repeat tests were more likely to demonstrate ischemia (36% vs 24%, P < .001) or scar (25% vs 14%, P < .001) than initial tests.

Multiple testing, cumulative radiation dose, and clinical indications in patients undergoing myocardial perfusion imagingConclusionsMany patients undergoing MPI received very
high cumulative estimated effective doses More than 30% of patients received a cumulative
estimated effective dose of more than 100 mSv, a level at which there is little controversy over the potential for increased cancer risks.
The median cumulative estimated effective dose for the 39% of patients undergoing more than 1 MPI examination was 121 mSv, higher than that in the exposed (≥5 mSv) cohort in the Life Span Study of Japanese atomic bomb survivors

Multiple testing, cumulative radiation dose, and clinical indications in patients undergoing myocardial perfusion imagingCautions/future? clinical context, risk of radiation vs benefit of
studyEffective dose reflects cancer risk from
radiation, but is a population-averaged metric that does not account for individual characteristics such as age and health status
Findings represent a single hospital in NYCOne third of MPIs were performed in
asymptomatic pts and therefore not indicated and unlikely to be clinically beneficial

Paper #3Effects of intensive blood-pressure control
in type 2 diabetes mellitus
ACCORD Blood Pressure writing group- ‘Merica! and Canada
Accepted for Publication 2010

Effects of intensive blood-pressure control in type 2 diabetes mellitusObjectiveThe Action to Control Cardiovascular Risk in
Diabetes (ACCORD) blood pressure trial (ACCORD BP) evaluated the effect of targeting a systolic blood pressure of 120 mm Hg, as compared with a goal of 140 mm Hg, among patients with type 2 diabetes at high risk for cardiovascular events
Effects of intensive blood-pressure control in type 2 diabetes mellitusBackgroundDiabetes mellitus increases the risk of
cardiovascular disease 2-3x at every level of systolic blood pressure
JNC 7 recommends beginning drug treatment in diabetic patients at SBP>130 mm Hg, with a treatment goal of reducing systolic blood pressure to below 130 mm Hg
Evidence?

Effects of intensive blood-pressure control in type 2 diabetes mellitusMethodsACCORD trial: randomized trial conducted at 77 clinical
sites organized into seven networks in the United States and Canada
10,251 high-risk participants with type 2 diabetes mellitus4733 participants were randomly assigned to either
intensive or standard blood-pressure control (the ACCORD blood-pressure trial)
intensive therapy: SBP <120 mm Hgstandard therapy: SBP <140 mm HgTreatment was with standard BP meds used in clinical
practice

Effects of intensive blood-pressure control in type 2 diabetes mellitusPopulation type 2 diabetes mellitus w/ A1C of 7.5% or more and were 40
years of age or older with cardiovascular disease or 55 years of age or older with anatomical evidence of a
substantial amount of atherosclerosis, albuminuria, left ventricular hypertrophy
or at least two additional risk factors for cardiovascular disease (dyslipidemia, hypertension, smoking, or obesity)
Or SBP bt 130 and 180 mm Hg who were taking three or fewer antihypertensive medications and who had the equivalent of a 24-hour protein excretion rate of less than 1.0 g
The mean age of the participants was 62.2 years; 47.7% were women and 33.7% had cardiovascular disease at baseline.
The mean systolic and diastolic blood pressures of the participants at baseline were 139.2 mm Hg and 76.0 mm Hg, respectively.
The mean duration of follow-up for the rate of death was 5.0 years

Effects of intensive blood-pressure control in type 2 diabetes mellitusOutcomes primary outcome : first occurrence of a major cardiovascular event, which was
defined as the composite of nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death
secondary outcomes: combination of the primary outcome plus another event After the first year of therapy, the average SBP was 119.3 mm Hg in the intensive-
therapy group and 133.5 mm Hg in the standard-therapy group. The corresponding mean diastolic blood pressures were 64.4 and 70.5 respectively.
The intensive-therapy group had greater exposure to drugs from every class. The intensive-therapy group had significantly higher rates of serious adverse events
attributed to antihypertensive treatment, as well as higher rates of hypokalemia and elevations in serum creatinine level
The frequency of macroalbuminuria at the final visit was significantly lower in the intensive-therapy group than in the standard-therapy group, and there was no between-group difference in the frequency of end-stage renal disease or the need for dialysis.

Mean Systolic Blood-Pressure Levels at Each Study Visit.
The ACCORD Study Group. N Engl J Med 2010;362:1575-1585.

Effects of intensive blood-pressure control in type 2 diabetes mellitusOutcomes continuedThe primary composite outcome occurred in 445
participants The rate was 1.87% per year in the intensive-therapy
group as compared with 2.09% per year in the standard-therapy group, with no significant between-group difference
Nominally significant differences were seen in the rate of total stroke (0.32% per year in the intensive-therapy group vs. 0.53% per year in the standard-therapy group)and in the rate of nonfatal stroke

Primary and Secondary Outcomes.
The ACCORD Study Group. N Engl J Med 2010;362:1575-1585.

Effects of intensive blood-pressure control in type 2 diabetes mellitusConclusions Intensive antihypertensive therapy in the ACCORD BP trial did not significantly
reduce the primary cardiovascular outcome or the rate of death from any cause, despite the fact that there was a significant and sustained difference between the intensive-therapy group and the standard-therapy group in mean systolic blood pressure
The event rate observed in the standard-therapy group was almost 50% lower than the expected rate
Evidence of some possible harm from side effects associated with intensive blood-pressure control
? Baseline BP not high enough to see the benefits of lowering blood pressure ? 5 years is not long enough to see significant cardiac benefits from the normalization
of systolic blood pressure among persons with diabetes who have good control of glycemia, especially when other effective treatments, such as statins and aspirin, are used frequently.
Other Papers and Conclusions1. Patients’ and cardiologists’ perceptions of the benefits of
PCI for stable coronary disease-Finding: disconnect bt patient and MD perceptions of why
PCI was being performed-Conclusions: reminder that PCI is no better than optimal
medical management for prevention of MI and death, and we need better pt communication
-Cautions: recall bias

Other Papers and Conclusions2. Effects of combination lipid therapy in type 2 DM-Findings: Pts with DM did not have a reduction in the
primary outcomes of nonfatal MI, nonfatal stroke or death w/ increase in HDL or reduction in triglycerides
-Conclusions: More favorable lipid profile does not necessarily correlate with reduced cardiac events in patients with DM
-Cautions: ?benefit in subgroups (men)

Other Papers and Conclusions3. Transcatheter Aortic Valve Implantation for Aortic Stenosis-Findings: TAVI reduced mortality rate at 1 year versus
standard therapy, but had more vascular complications-Conclusions: TAVI should be considered in symptomatic
patients with severe AS-Cautions: balloon angio not prevalent anymore, little benefit.
Should have studies of TAVI vs medical management

Other Papers and Conclusions4. Multicenter validation of the diagnostic accuracy of a
blood-based gene expression test for assessing obstructive CAD in nondiabetic patients
-Findings: gene test only contributed modestly, clinical info still more diagnostic
-Conclusions: gene testing is exciting but still requires a lot of work and cannot be linked to CAD in a causal manner
-Cautions: no clinical outcomes

Other Papers and Conclusions5. Low diagnostic yield of elective coronary angiography-Findings: only 1/3 of pt’s undergoing cath/PCI had
obstructive CAD, and 1/3 of pts referred for PCI had no symptoms
-Conclusions: more ppl undergoing PCI now have normal caths than 20 years ago. We need better clinical and noninvasive risk stratification to prevent unnecessary procedures
-Cautions: unclear what testing led to cath, what “gatekeeper” testing was peformed