peripheral vascular diseases howard sacher, d.o long island cardiology and internal medicine
TRANSCRIPT

Peripheral Vascular DiseasesPeripheral Vascular Diseases
Howard Sacher, D.OLong Island Cardiology and Internal Medicine

Significance of Peripheral Vascular Significance of Peripheral Vascular DiseaseDisease
Recognition and management of diseases of the peripheral arteries and veins should be a legitimate part of cardiovascular practice
These disorders so commonly coexist with, occur as complications of, and at times are the presenting clinical manifestation of cardiac disease.
In our aging population, atherosclerotic occlusive peripheral arterial disease (OPAD) is common.

OPAD is present to some degree in at least half of patients with coronary artery disease.
When symptomatic, chronic OPAD presents with intermittent claudication.
With progression of occlusive arterial disease and the development of more severe ischemia, there is pain at rest—'ischemic rest pain.'

Physically Examining the Physically Examining the PatientPatient
Pulsation Bruits Elevation-Dependency Tests Ischemic Ulceration present?

Pulsation Pulsation
Examination should include palpation and characterization of the pulsation of the upper and lower extremity arteries and the cervical carotid.
One of the best clinical criteria indicative of OPAD is an absent posterior tibial artery pulse. For illustrations of examination methods



Allen Test to asses Patency Allen Test to asses Patency

To detect Subclavian Steal To detect Subclavian Steal

BruitsBruits
Most often, bruits due to occlusive arterial disease are systolic in timing.
Useful bedside point: a bruit that extends a bruit that extends into diastole indicates a stenosis severe into diastole indicates a stenosis severe enough (usually 80% or greater) to enough (usually 80% or greater) to produce a gradient in diastoleproduce a gradient in diastole

Elevation-Dependency Tests Elevation-Dependency Tests
Elevation-dependency tests are also useful in evaluating the person with occlusive peripheral arterial disease



Presence of Ischemic UlcersPresence of Ischemic Ulcers
Ischemic ulcers are extremely painful, are located most often on the toes or heel, can occur at any site of trauma to an ischemic limb, and can usually be readily distinguished from other leg and foot ulcers



Noninvasive EvaluationNoninvasive Evaluation
Ankle:Brachial index Duplex scan with color flow DopplerMagnetic Resonance Angiography

But Invasive test is the Gold But Invasive test is the Gold StandardStandard
ArteriographyArteriography remains the best means of evaluating OPAD when restoration of pulsatile flow is being considered

ABI Pre and Post ExerciseABI Pre and Post Exercise

MRA gives us a good view of vasculature with the use of gadalidium contrast
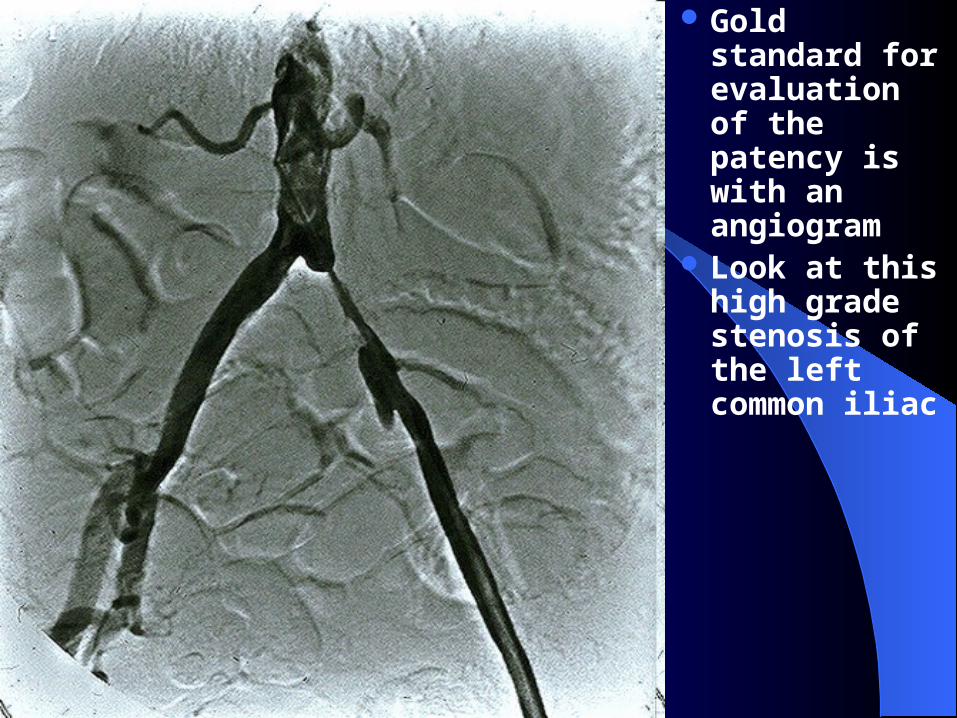
Gold standard for evaluation of the patency is with an angiogram
Look at this high grade stenosis of the left common iliac

Along with with an angiogram, the interventionalist can also perform a Percutanous Transluminal Angioplasty (PTA) using a balloon and and a stent

Post PTA, look at that left common iliac again



Superficial thrombophibitisSuperficial thrombophibitis


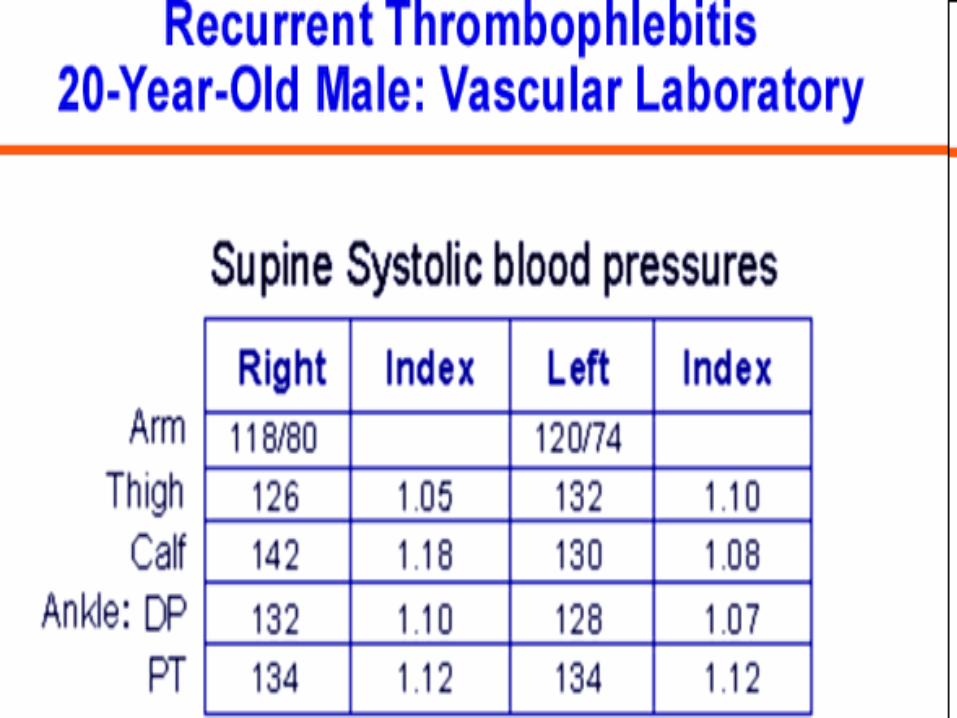


Any body wants to venture Any body wants to venture into the Dx?into the Dx?

Thromboangitis ObliteransThromboangitis Obliterans
Burger’s DiseasePrimarily effects smokersComplete obliteration of the small to
medium size vesselsPx is poor Tx is to stop smoking


Acute Peripheral Arterial Acute Peripheral Arterial OcclusionOcclusion
Classic Occlusion – Acute peripheral arterial occlusion may present
classically with the 5 Ps PainPain PallorPallor ParesthesiaParesthesia ParalysisParalysis PulselessnessPulselessness
Or may be more subtle.



Case 2Case 2

Aortagram shows a complete occlusion of Aortagram shows a complete occlusion of
the left subclavian in the thoracic outlet –the left subclavian in the thoracic outlet – Thoracic Outlet CompressionThoracic Outlet Compression

Raynaud’s PhenomenonRaynaud’s Phenomenon is also is also associated with ispilateral thoracic associated with ispilateral thoracic
compressioncompression



Livido ReticularisLivido Reticularis

Atheroembolism Atheroembolism
Management includes removal of the source of the debris. Anticoagulant therapy with either heparin or warfarin and thrombolytic therapy should be avoided, while treatment with aspirin and/or dipyridamole has been reported to improve a limited number of patients.
ErgotismErgotism
The manifestations of ergotism are usually symmetric and vary from Raynaud's phenomenon to claudication or even acute arterial occlusion.
Treatment with intravenous sodium nitroprusside in addition to discontinuing ergot preparation will relieve the arterial insufficiency

Aneurysmal DiseaseAneurysmal Disease Arterial aneurysms are more common in males 60 years of
age or older Coronary and cerebral arterial disease are frequent
comorbid conditions Abdominal Aortic Aneurysm (AAA) needs to be kept in
mind as a possible cause of unexplained abdominal, flank, or back pain in a man with an elevated sedimentation rate, a tender pulsatile abdominal mass, and rarely, weight loss or ureteral obstruction.
CT and MRI are useful to differentiate a leaking aneurysm from inflammatory AAA.

Most thoracic aortic aneurysms today are atherosclerotic
But other causes such as sudden deceleration are also important.
Given findings consistent with incomplete aortic rupture, aortography is indicated.
Surgical repair is indicated in the case of incomplete rupture or post-traumatic aneurysm in persons who are suitable surgical candidates.

Ultrasound is a reliable diagnostic technique for abdominal aortic aneurysm
Screening of elderly patients during echocardiography has a significant yield in discovering occult abdominal aortic aneurysm
In a good-risk patient, elective surgical treatment is advisable for aneurysms more than 4.5 cm in diameter
Because of the continued high mortality of ruptured abdominal aortic aneurysm, an aggressive approach to diagnosis and treatment is appropriate

Aneurysm of the Ascending AoAneurysm of the Ascending Ao

CT scan of the same patientCT scan of the same patient

Descending AorticDescending Aortic Aneurysms will usually manifest with JVDAneurysms will usually manifest with JVD

Descending Ao Descending Ao AneurysmAneurysm

Popliteal Aneurysm Popliteal Aneurysm

Palpating for an aneurysm Palpating for an aneurysm

Many times a skin Many times a skin infarctions is a infarctions is a complication of complication of PoplitealPopliteal
AneurysmsAneurysms

Or one may see Thrombosis Or one may see Thrombosis

Marfan’s Syndrome Marfan’s Syndrome
As well other connective tissue disorders has a higher propensity for aneurismal disease
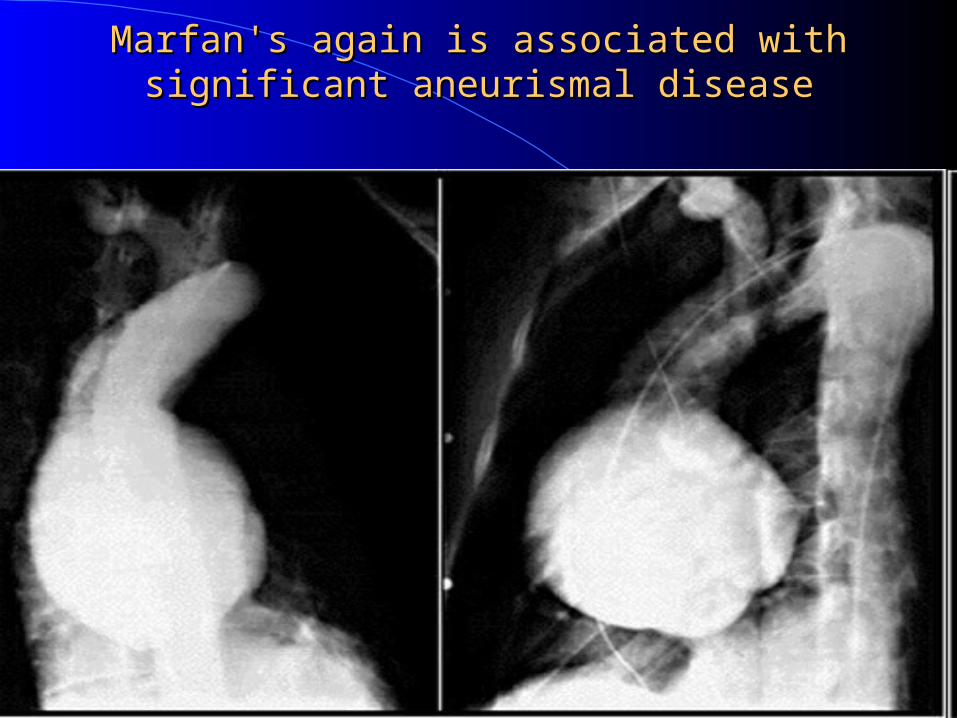
Marfan's again is associated with significant aneurismal Marfan's again is associated with significant aneurismal diseasedisease

Note the increased diameter Ao in this Pt with AAANote the increased diameter Ao in this Pt with AAA
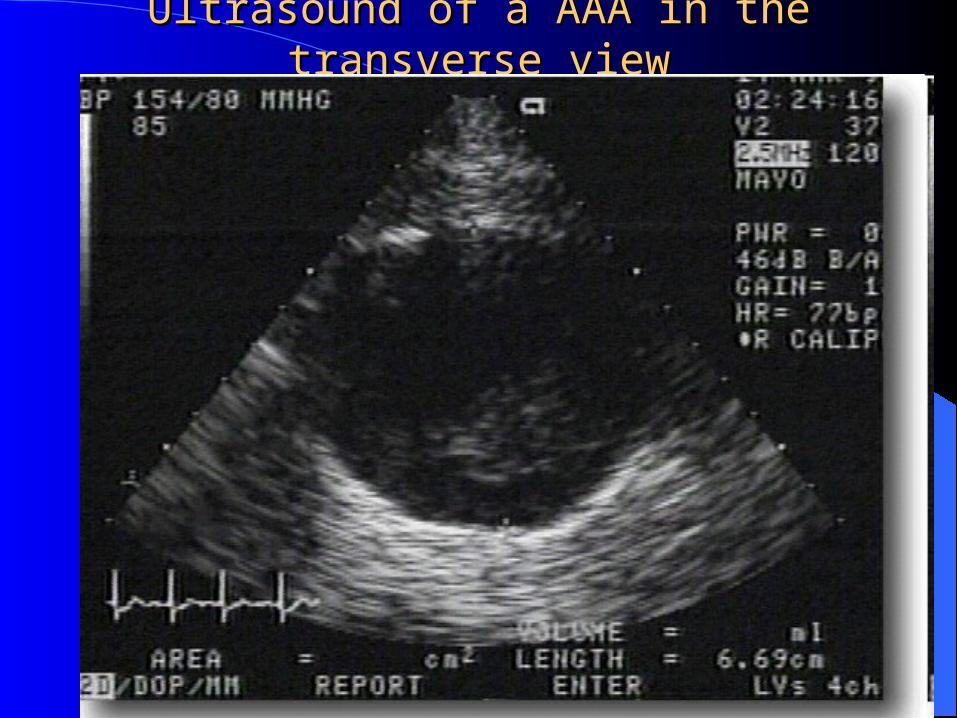
Ultrasound of a AAA in the transverse viewUltrasound of a AAA in the transverse view

In the Anteroposterior plane the AAA reveals a diameter In the Anteroposterior plane the AAA reveals a diameter of 7.7cmof 7.7cm

Only in Surgery can we get a true Only in Surgery can we get a true measurement with calipersmeasurement with calipers
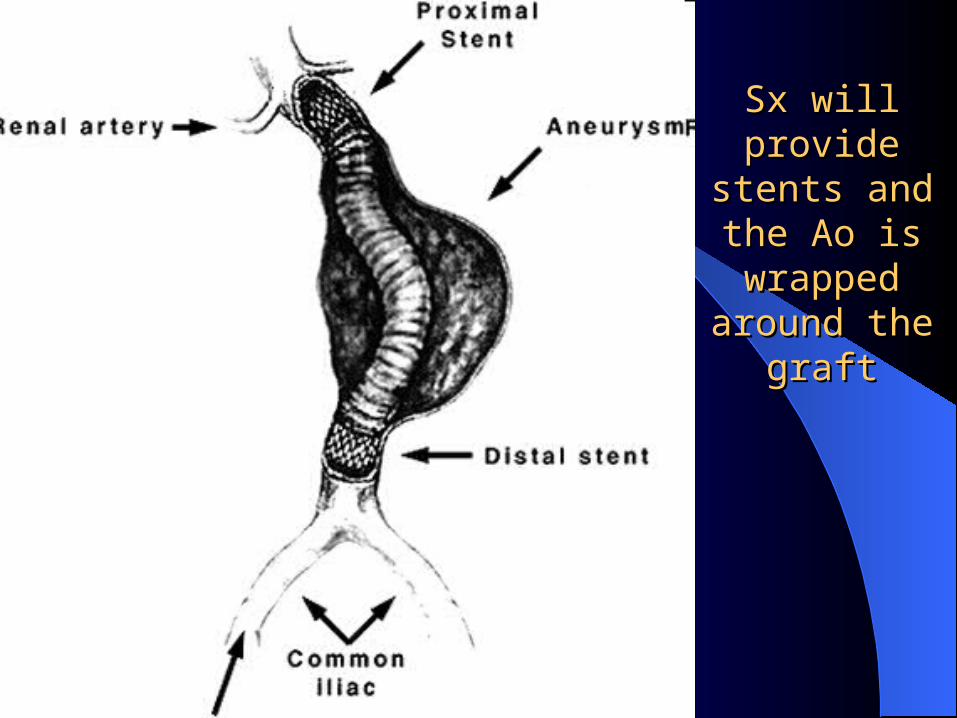
Sx will provide Sx will provide stents and the stents and the Ao is wrapped Ao is wrapped
around the around the graftgraft

In this MRA we see a Pt with bilateral RAS secondary to In this MRA we see a Pt with bilateral RAS secondary to bilateral Ileac Artery Stenoisbilateral Ileac Artery Stenois


Types of Ao DissectionTypes of Ao Dissection
Type IType IIType III
Most common presentation:– older patients, usually hypertensive, whose
abrupt chest pain or upper back pain

Echocardiography is the preferred screening procedure. Note that a normal chest roentgenogram does not exclude acute aortic dissection. Acute aortic dissection is correctly diagnosed only about half the time
Emergent pharmacological therapy to control any hypertension is indicated while the diagnosis is being confirmed
Appropriate management calls for localizing the primary tear, delineating the extent of the dissection, and demonstrating any major arterial obstruction or aortic regurgitation.

Careful control of any hypertension with beta blockade is essential.
Significant late complications of surgically repaired or medically managed aortic dissection
This may be asymptomatic but warrant surgical repair– these are pseudoaneurysms, chronic dissection
of the aorta proximal to the graft, and aortic valve insufficiency.



Atherosclerotic Ulcer of the Ao as seen on this AortogramAtherosclerotic Ulcer of the Ao as seen on this Aortogram

Severe Giant Cell Arteritis can Severe Giant Cell Arteritis can present with bilateral arm present with bilateral arm claudication secondary to claudication secondary to stenosis of the subclavian stenosis of the subclavian artery artery


Vasospastic DisordersVasospastic Disorders
The vasospastic disorders, the most common of which is Raynaud's phenomenon
Hallmarked by changes of skin color rather than intermittent claudication.
These disorders frequently are a manifestation of, or even a clue to, a variety of other disorders


In a person with Raynaud's phenomenon, it is important to learn which fingers are involved and whether the toes are also involved.
Making the differentiation between primary and secondary RP allows the physician to assure the person with primary Raynaud's disease that it is benign and to seek the underlying cause in cases of secondary Raynaud's phenomenon


Carotid Artery Duplex Carotid Artery Duplex UltrasoundUltrasound
Relevant Trial Results of Relevant Trial Results of Carotid diseaseCarotid disease
The ACAS Trial found that patients with asymptomatic carotid artery stenosis of 60% or greater whose general health makes them good candidates for elective surgery will have a reduced 5-year risk of ipsilateral stroke with carotid endarterectomy plus aggressive management of modifiable risk factors.

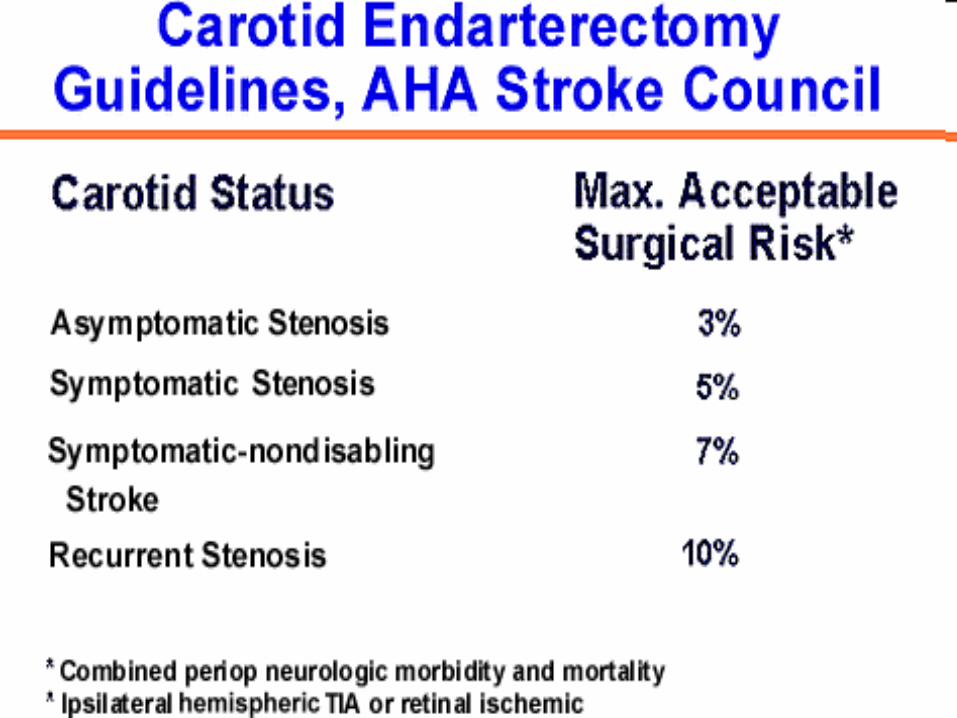
• The ECST and NASCET trials both reported benefit from carotid endarterectomy for patients with recent focal cerebral (carotid territory) or transient retinal ischemic attacks or nondisabling stroke and ipsilateral high-grade (70% to 99%) stenosis of the carotid artery.

Comorbidity Comorbidity Patient with both significant carotid and coronary
artery disease;– a carotid endarterectomy at the time of coronary artery
bypass surgery resulted in a lower stroke rate than when the carotid endarterectomy was delayed and performed within 2 weeks after the coronary artery surgery. For completed stroke
– unless there is a cardiac source of embolus, anticoagulant therapy is not indicated. Carotid endarterectomy is a consideration if the neurologic deficit is minimal and a high-grade stenosis of the ipsilateral internal carotid artery is present

Carotid Artery Dissection Carotid Artery Dissection
Spontaneous dissection of the cervical cephalic arteries is uncommon but important for two reasons – Hemicrania with Oculosympathetic paresis– Hemicrania with delayed focal cerebral
ischemic symptoms
The prognosis is good for recovery and recurrences are rare






Deep venous Deep venous obstruction not only obstruction not only
causes varicose veins causes varicose veins but also Baker’s cysts but also Baker’s cysts
(popliteal cysts)(popliteal cysts)

Arthrogram depicting Baker’s cystsArthrogram depicting Baker’s cysts

Progression of deep venous Progression of deep venous obstruction obstruction

Lipodermatosclerosis – Lipodermatosclerosis – chronic indurated cellulitischronic indurated cellulitis

Venous Stasis UlcerVenous Stasis Ulcer


Overall with DVT treatmentOverall with DVT treatment
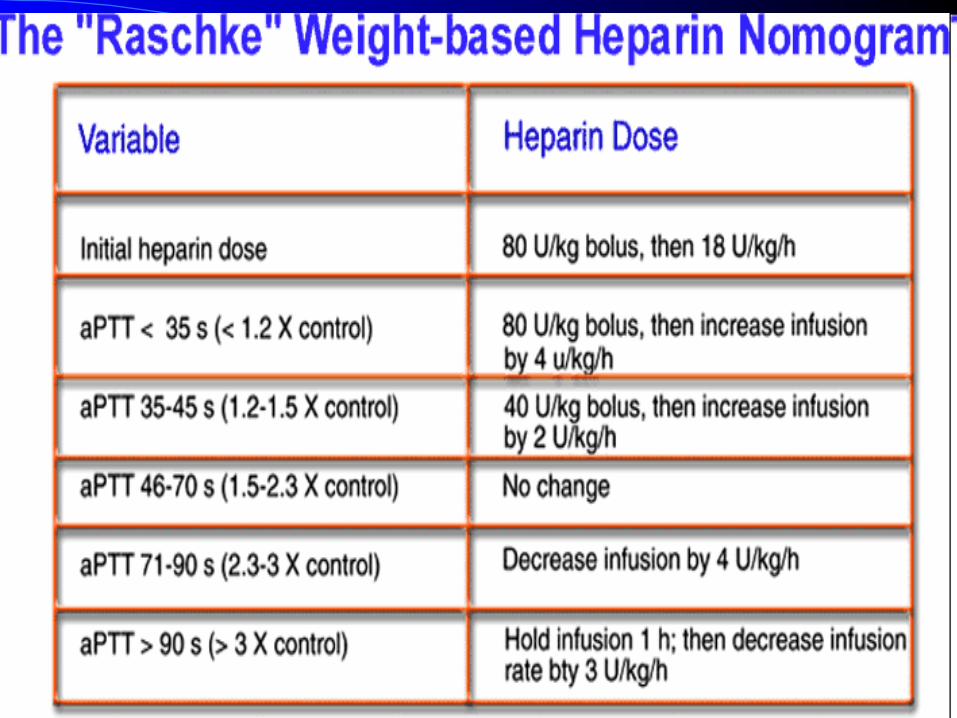
Therapy for deep vein thrombosis is heparin followed by oral anticoagulation preferably for 6 months, maintaining INR 2 to 3
Thrombolytic therapy is reserved for acute, extensive deep venous thrombosis, particularly in otherwise healthy young persons.

Thrombolysis must be followed promptly by anticoagulant therapy to prevent rethrombosis
With heparin of any type, baseline and daily platelet counts are essential because of the occurrence of heparin-induced thrombocytopenia, which warrants initiation of warfarin therapy once the diagnosis of acute deep vein thrombosis and/or pulmonary embolism is established, so that the prothrombin time reaches therapeutic range in 4 to 5 days.

Keep in the back of your mindKeep in the back of your mind
With true recurrence of deep vein thrombosis in the face of adequate anticoagulant effect, an underlying cause, often neoplastic, must be suspected
Postphlebitic changes lead to the complications of chronic venous insufficiency in most patients, unless adequate elastic support is used