annals of internal medicine - the medicine box | handy ... · annals of internal medicine ......
TRANSCRIPT
Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
1 of 16 20/06/2006 2:27 PM
© 1993 American College of Physicians Volume 119(9), 1 November 1993, pp 874-881Annals of Internal Medicine
The Weight-based Heparin Dosing Nomogram Compared with a "Standard Care" Nomogram:
A Randomized Controlled Trial[Articles]
Raschke, Robert A.; Reilly, Brendan M.; Guidry, James R.;Fontana, Joseph R.; Srinivas, Sandhya
From Good Samaritan Regional Medical Center, Phoenix, Arizona; the University of Rochester School of Medicine, Rochester, New York; St. Mary's Hospital, Rochester, New York.
Requests for Reprints: Robert A. Raschke, MD, Department of Medicine, Good Samaritan Regional Medical Center, 1111 E. McDowell Road, Phoenix, AZ 85006.
Abstract
Objective: To determine whether an intravenous heparin dosing nomogram based on body weight achieves therapeutic anticoagulation more rapidly than a "standard care" nomogram.
Design: Randomized controlled trial.
Setting: Two community teaching hospitals in Phoenix, Arizona, and Rochester, New York.
Participants: One hundred fifteen patients requiring intravenous heparin treatment for venous or arterial thromboembolism or for unstable angina.
Intervention: Patients were randomized to the weight-based nomogram (starting dose, 80 units/kg body weight bolus, 18 units/kg per hour infusion) or the standard care nomogram (starting dose, 5000-unit bolus, 1000 units per hour infusion). Activated partial thromboplastin time (APTT) values were monitored every 6 hours, and heparin dose adjustments were determined by the nomograms.
Measurements: Activated partial thromboplastin times were measured using a widely generalizable laboratory method. The primary outcomes were the time to exceed the therapeutic threshold (APTT > 1.5 times the control) and the time to achieve therapeutic range (APTT, 1.5 to 2.3 times the control). Bleeding complications and recurrent thromboembolism were also compared.
Results: Kaplan-Meier curves for the primary outcomes favored the weight-based nomogram (P < 0.001 for both). In the weight-based heparin group, 60 of 62 patients (97%) exceeded the therapeutic threshold within 24 hours, compared with 37 of 48 (77%) in the standard care group (P < 0.002). Only one major bleeding complication occurred (in a standard care patient). Recurrent thromboembolism was more frequent in the standard care group; relative risk, 5.0 (95% CI, 1.1 to 21.9).
Conclusions: The weight-based heparin nomogram is widely generalizable and has proved tobe effective, safe, and superior to one based on standard practice.
Heparin therapy improves clinical outcomes in patients with thromboembolic disorders [1,2,3,4], but the determination of appropriate heparin dosing is often problematic. Physicians'
dosing decisions vary widely, as do their therapeutic goals [5]. Practice audits reveal frequent
underdosing, with delays in achieving therapeutic anticoagulation leading to suboptimal clinical outcomes [6,7].
Recent research offers hope that clarification of treatment goals and specific dosing
Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
2 of 16 20/06/2006 2:27 PM
guidelines may improve outcomes. Hull and colleagues [3] reported that rapidly exceeding a
"therapeutic threshold" (activated partial thromboplastin time (APTT), 1.5 times the control) reduced the rate of recurrent thromboembolism from 25% to 2%, a finding confirmed in other studies [4,8,9,10,11,12]. In addition, a retrospective analysis suggested that an initial heparin
infusion dose of 1000 units per hour is often insufficient [13], and the most recent American
College of Chest Physicians Consensus Conference on Antithrombotic Therapy recommends an initial infusion of at least 1250 units per hour [14,15]. Finally, dosing nomograms--which specify
heparin dose adjustments in response to any given APTT level--have shown promising results [16,17].
Despite these advances, uncertainties remain. Randomized controlled studies have not compared higher initial heparin doses with 1000 units per hour, and many physicians continue to follow this clinical tradition [5]. Because the relation between bleeding complications and
"excessive" APTT values is controversial [3,10,16,18,19,20,21,22,23,24], so is the optimal upper limit
of the therapeutic range [5,14,25]. For this reason, Hull and colleagues [14] and Hirsh [25] have
recently de-emphasized the value of the therapeutic range and have stressed the need to minimize recurrent thromboembolism by rapidly exceeding the "therapeutic threshold". Measured against that standard, Hull's nomogram succeeded in 98% of patients; however, heparin infusions were routinely started at 1670 units per hour and nearly half of the patients had excessive APTT levels that persisted for 24 hours or more [16]. The generalizability of this
nomogram is limited by its dependence on an APTT test reagent that yields markedly prolonged APTTs compared with reagents commonly used in the United States [16,17,26,27]. (Activated
partial thromboplastin times vary greatly depending on laboratory method used [14,15,16,25,26,27], analogous to the variability of prothrombin times that prompted development
of the International Normalized Ratio.)
We agree with Hull and colleagues that heparin nomograms "relentlessly direct the heparin dosage and drive the APTT into the therapeutic range" [16]. We hypothesized that a
patient-specific nomogram, based on total body weight (the single best predictor of individual heparin requirements [28,29]) would achieve high success rates without the need for prescribing
excessive heparin doses.
Our study, using the most generalizable APTT test system in North America, compares the performance of our weight-based heparin nomogram with another nomogram reflecting a prevalent standard of practice. Our report is the first to describe a weight-based heparin nomogram, the first to compare two nomograms prospectively, and the first nomogram study tohave easily generalizable results.
MethodsStudy Design
In a randomized controlled trial, we compared two nomograms for intravenous heparin dosing in patients with venous thromboembolism, unstable angina, or arterial thromboembolism. During the first 48 hours of anticoagulation, the appropriate nomogram determined all dosing decisions (Tables 1, 2), and warfarin was withheld. We defined two primary outcomes. The first was the time elapsed between initiating heparin therapy and surpassing the therapeutic threshold (APTT, 1.5 times the control), considered the minimum acceptable level of anticoagulation. The second was the time elapsed before achieving therapeutic range (APTT, 1.5 to 2.3 times the control), the optimal goal for intravenous
Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
3 of 16 20/06/2006 2:27 PM
anticoagulation.
We did our study simultaneously at two community teaching hospitals: a 700-bed regional referral center in Phoenix, Arizona, and a 250-bed, inner-city hospital in Rochester, New York. Both hospitals are major teaching affiliates of university medical schools, and each maintains a large, accredited internal medicine residency program.
Patients
Patients admitted between May 1991 and January 1992 were deemed eligible if they were toreceive intravenous heparin for one of the following indications: 1) pulmonary embolism, diagnosed clinically and confirmed by a high-probability lung scan or pulmonary arteriography; 2) proximal deep vein thrombosis, confirmed by ascending venography, impedance plethysmography, or Doppler ultrasonography; 3) unstable angina, diagnosed clinically by an attending cardiologist using the Braunwald criteria [30]; or 4) acute noncoronary arterial
ischemia. Exclusion criteria included 1) anticoagulant or thrombolytic therapy in the previous 7 days, 2) active hemorrhage, 3) acute major cerebral vascular event, 4) history of heparin-induced thrombocytopenia, and 5) known allergy to heparin.
A power analysis revealed that a total study size of 100 patients would have 90% power (with a type I error of 0.05) to detect a 6-hour difference in the mean time needed to achieve the primary outcomes.
The Nomograms
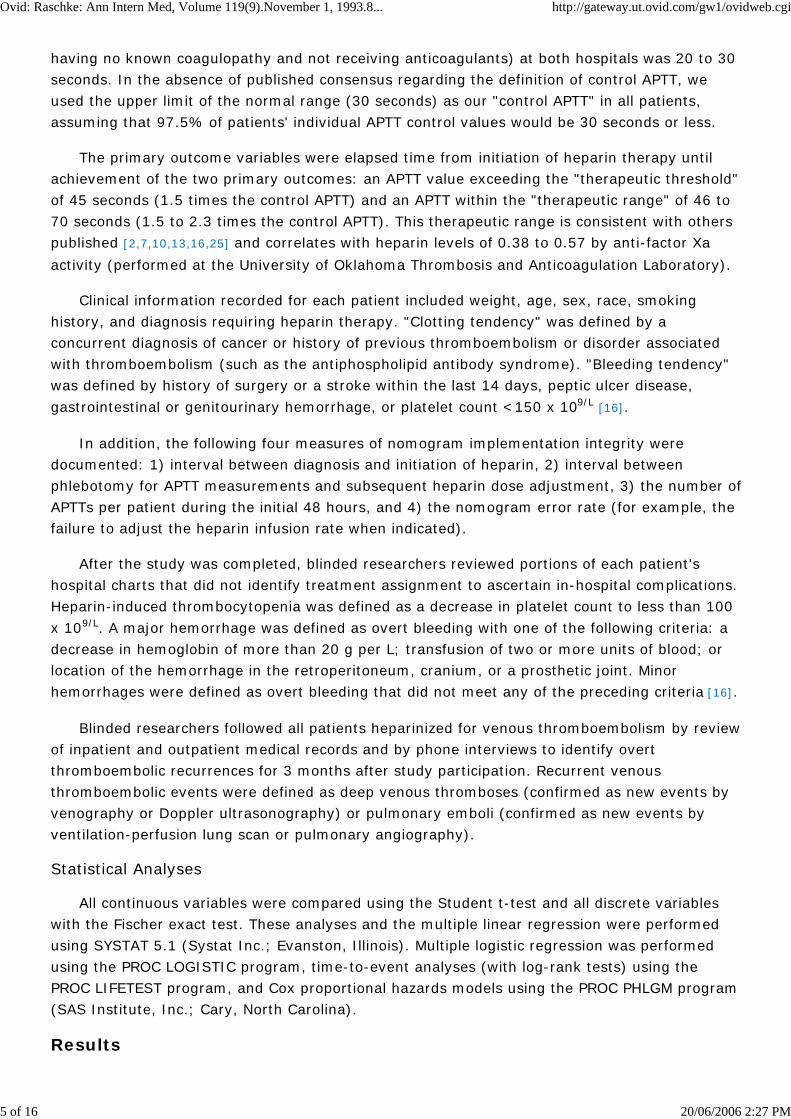
The "standard practice" nomogram Table 1 was based on the mode for each of the responses
to a survey of 61 internists at our hospitals regarding their usual practices of heparin administration [5]. The initial bolus and infusion doses were identical to those recommended by
the American College of Chest Physicians at the time the study was done [13], and dose
adjustments in response to APTT results were similar to those of subsequently published nomograms [16,17].
Table 1. Standard Care Nomogram
We constructed the weight-based nomogram Table 2 after we reviewed the literature and did
a preliminary dosing study. Many reports have described bolus doses ranging from 50 to 150 units per kg body weight and infusion doses from 15 to 25 units per kg per hour [8,28,29,31,37].
In one study, 78% of patients achieved therapeutic goals rapidly after receiving a bolus of 75

Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
4 of 16 20/06/2006 2:27 PM
units per kg and an initial infusion of 17 units per kg per hour [34]. In our preliminary dosing
study, the mean dose of heparin required to achieve two consecutive therapeutic APTT values in24 patients with unstable angina was 17.3 +- 4.0 units per kg per hour [38]. The initial heparin
doses we chose for our weight-based nomogram (bolus, 80 units per kg; infusion, 18 units per kg per hour) supplied 511 units per kg per day, consistent with reports that daily heparin requirements in venous thromboembolism range from 480 to 600 units per kg [7,39,40].
Subsequent infusion adjustments in the nomogram were designed to minimize delay in attainingthe therapeutic range. All doses in the weight-based nomogram were calculated based on actualbody weight rather than ideal weight.
Table 2. Weight-based Nomogram
Intervention
After informed consent was obtained, patients were randomized to one of the two nomograms, and preprinted orders for implementation of the appropriate nomogram were charted. Staff nurses, who were not blinded, weighed each patient, calculated doses, and adjusted the infusion rate accordingly. Although the nurses could not influence the results of APTT measurements, several indices of nomogram implementation were monitored to detect any unintended co-interventions.
Patients randomized to standard heparin therapy received a 5000-unit bolus of intravenous heparin followed by an infusion dose of 1000 units per hour. Patients in the weight-based heparin group received an intravenous bolus of 80 units per kg, followed by an infusion dose of 18 units per kg per hour. At both hospitals, heparin sodium (pork derived, Schein Pharmaceuticals Inc.; New York, New York) was diluted in 5% dextrose solution and administered with infusion pumps.
"Stat" APTT levels were drawn every 6 hours. (This interval approximates four half-lives of heparin, the time required to achieve steady-state kinetics.) When the staff nurses received the APTT results, they consulted the nomogram and adjusted the heparin dose. No adjustments were made if blood for the APTT was drawn less than 4 hours after the last heparin dose adjustment was made.
Measurements
All blood specimens for APTT were collected in siliconized Vacutainer tubes (Bectin-DickinsonCompany; Rutherford, New Jersey) containing buffered citrate. Both our hospital laboratories use plain Dade actin thromboplastin (Baxter Healthcare Corporation, Dade Division; Miami, Florida) and automated coagulation systems (MLA Electra 700 and 1000 series, Medical Laboratory Automation Inc.; Pleasantville, New York) to determine APTT values. The correlation coefficient for APTTs performed with plain Dade actin thromboplastin on these two automated systems, using mean values reported for all plasma samples in the 1992 College of American Pathologists' data [27], is 0.999. The normal range for APTT (mean APTT +- 2 SD in patients
Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
5 of 16 20/06/2006 2:27 PM
having no known coagulopathy and not receiving anticoagulants) at both hospitals was 20 to 30 seconds. In the absence of published consensus regarding the definition of control APTT, we used the upper limit of the normal range (30 seconds) as our "control APTT" in all patients, assuming that 97.5% of patients' individual APTT control values would be 30 seconds or less.
The primary outcome variables were elapsed time from initiation of heparin therapy until achievement of the two primary outcomes: an APTT value exceeding the "therapeutic threshold"of 45 seconds (1.5 times the control APTT) and an APTT within the "therapeutic range" of 46 to 70 seconds (1.5 to 2.3 times the control APTT). This therapeutic range is consistent with others published [2,7,10,13,16,25] and correlates with heparin levels of 0.38 to 0.57 by anti-factor Xa
activity (performed at the University of Oklahoma Thrombosis and Anticoagulation Laboratory).
Clinical information recorded for each patient included weight, age, sex, race, smoking history, and diagnosis requiring heparin therapy. "Clotting tendency" was defined by a concurrent diagnosis of cancer or history of previous thromboembolism or disorder associated with thromboembolism (such as the antiphospholipid antibody syndrome). "Bleeding tendency" was defined by history of surgery or a stroke within the last 14 days, peptic ulcer disease,
gastrointestinal or genitourinary hemorrhage, or platelet count <150 x 109/L [16].
In addition, the following four measures of nomogram implementation integrity were documented: 1) interval between diagnosis and initiation of heparin, 2) interval between phlebotomy for APTT measurements and subsequent heparin dose adjustment, 3) the number ofAPTTs per patient during the initial 48 hours, and 4) the nomogram error rate (for example, the failure to adjust the heparin infusion rate when indicated).
After the study was completed, blinded researchers reviewed portions of each patient's hospital charts that did not identify treatment assignment to ascertain in-hospital complications.Heparin-induced thrombocytopenia was defined as a decrease in platelet count to less than 100
x 109/L. A major hemorrhage was defined as overt bleeding with one of the following criteria: a decrease in hemoglobin of more than 20 g per L; transfusion of two or more units of blood; or location of the hemorrhage in the retroperitoneum, cranium, or a prosthetic joint. Minor hemorrhages were defined as overt bleeding that did not meet any of the preceding criteria [16].
Blinded researchers followed all patients heparinized for venous thromboembolism by reviewof inpatient and outpatient medical records and by phone interviews to identify overt thromboembolic recurrences for 3 months after study participation. Recurrent venous thromboembolic events were defined as deep venous thromboses (confirmed as new events by venography or Doppler ultrasonography) or pulmonary emboli (confirmed as new events by ventilation-perfusion lung scan or pulmonary angiography).
Statistical Analyses
All continuous variables were compared using the Student t-test and all discrete variables with the Fischer exact test. These analyses and the multiple linear regression were performed using SYSTAT 5.1 (Systat Inc.; Evanston, Illinois). Multiple logistic regression was performed using the PROC LOGISTIC program, time-to-event analyses (with log-rank tests) using the PROC LIFETEST program, and Cox proportional hazards models using the PROC PHLGM program(SAS Institute, Inc.; Cary, North Carolina).
Results

Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
6 of 16 20/06/2006 2:27 PM
Patients
Among 121 eligible patients, three were unwilling and three were unable to provide informed consent. Of 115 randomized patients, 100 received heparin for at least 48 hours. Heparin was discontinued in six patients before 48 hours when unstable angina resolved, in four patients whose initial diagnosis of deep venous thrombosis was later ruled out, in three patients who had adverse events, and in one patient whose peripheral arterial ischemia resolved. One patient was removed from the standard protocol at 23 hours by an attending physician because "it isn't working". These 15 patients were included in both time-to-event analyses.
Of the 115 patients randomized, 85 had deep venous thrombosis or pulmonary embolus, 26 had unstable angina, 2 had acute peripheral arterial ischemia, and 2 had crescendo transient ischemic attacks. Sixty-two (55% at each site) were randomized to the weight-based nomogramand 53 to the standard care nomogram. The baseline characteristics of the patients in the two groups were similar Table 3. The higher prevalence of bleeding tendency in patients in the
standard care group was caused by a disproportionate number of patients with a history of peptic ulcer disease at one hospital.
Table 3. Patient Characteristics
Primary Outcomes
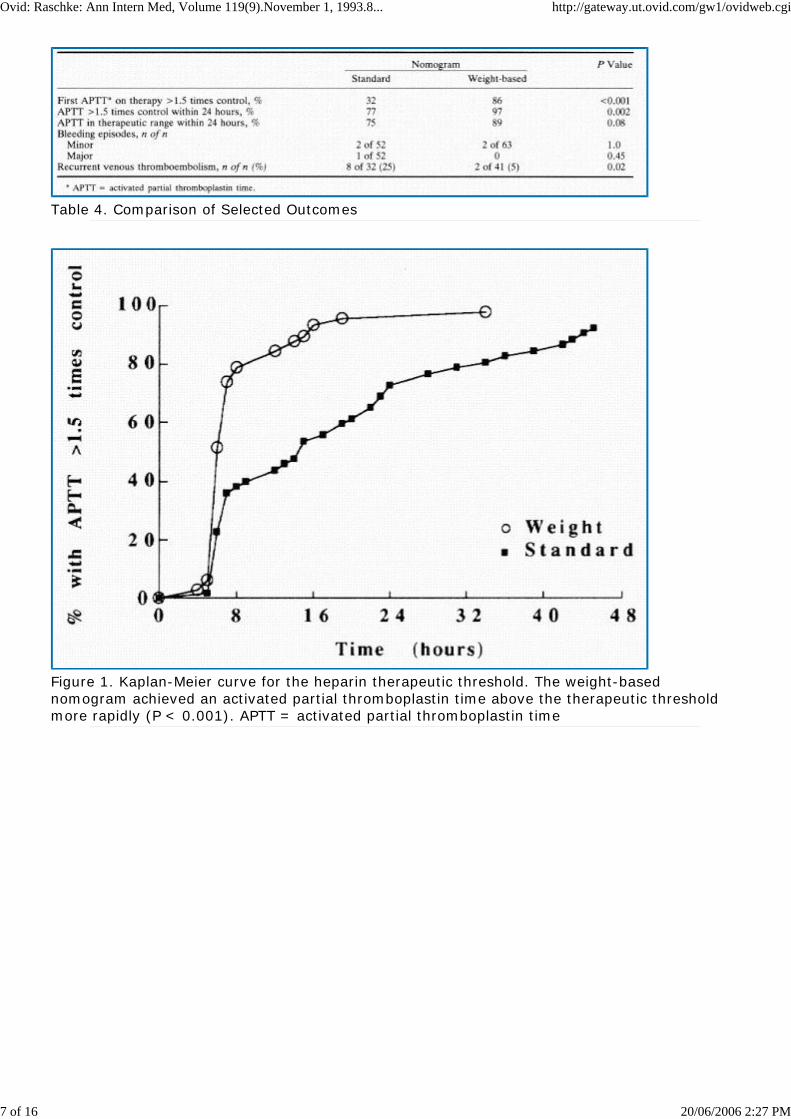
The success of the nomograms was compared using time-to-event analysis (Figures 1, 2). The weight-based nomogram achieved both primary outcomes, APTT exceeding the therapeutic threshold and APTT within the therapeutic range, more rapidly than did the standard care nomogram (P < 0.001 for both). The mean time required to exceed the therapeutic threshold was 8.2 hours in the weight-based group and 20.2 hours in the standard-care group (P < 0.001). The therapeutic threshold was achieved in 86% of the patients in the weight-based group on the first APTT drawn during therapy (compared with 32% in the standard care group, P < 0.001). By 24 hours, the proportion exceeding the therapeutic threshold was 97% in the weight-based group and 77% in the control group (P = 0.002) Table 4.
Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
7 of 16 20/06/2006 2:27 PM
Table 4. Comparison of Selected Outcomes
Figure 1. Kaplan-Meier curve for the heparin therapeutic threshold. The weight-based nomogram achieved an activated partial thromboplastin time above the therapeutic threshold more rapidly (P < 0.001). APTT = activated partial thromboplastin time
Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
8 of 16 20/06/2006 2:27 PM
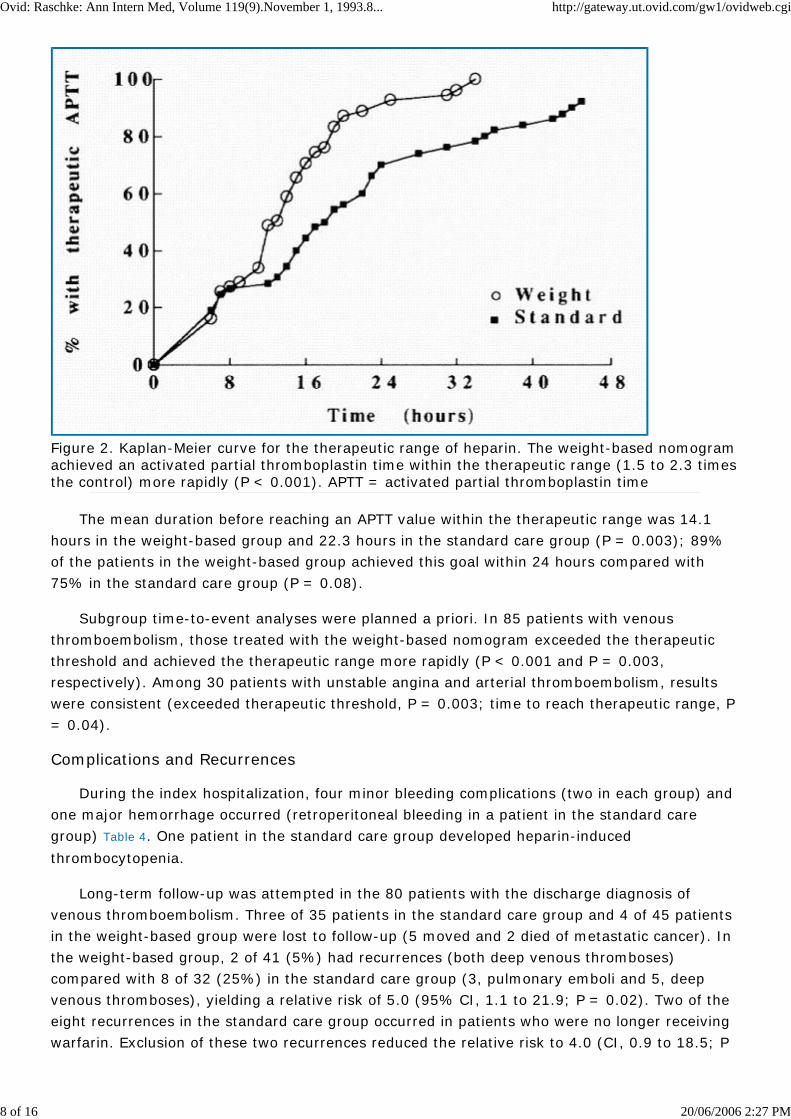
Figure 2. Kaplan-Meier curve for the therapeutic range of heparin. The weight-based nomogram achieved an activated partial thromboplastin time within the therapeutic range (1.5 to 2.3 times the control) more rapidly (P < 0.001). APTT = activated partial thromboplastin time
The mean duration before reaching an APTT value within the therapeutic range was 14.1 hours in the weight-based group and 22.3 hours in the standard care group (P = 0.003); 89% of the patients in the weight-based group achieved this goal within 24 hours compared with 75% in the standard care group (P = 0.08).
Subgroup time-to-event analyses were planned a priori. In 85 patients with venous thromboembolism, those treated with the weight-based nomogram exceeded the therapeutic threshold and achieved the therapeutic range more rapidly (P < 0.001 and P = 0.003, respectively). Among 30 patients with unstable angina and arterial thromboembolism, results were consistent (exceeded therapeutic threshold, P = 0.003; time to reach therapeutic range, P = 0.04).
Complications and Recurrences
During the index hospitalization, four minor bleeding complications (two in each group) and one major hemorrhage occurred (retroperitoneal bleeding in a patient in the standard care group) Table 4. One patient in the standard care group developed heparin-induced
thrombocytopenia.
Long-term follow-up was attempted in the 80 patients with the discharge diagnosis of venous thromboembolism. Three of 35 patients in the standard care group and 4 of 45 patients in the weight-based group were lost to follow-up (5 moved and 2 died of metastatic cancer). In the weight-based group, 2 of 41 (5%) had recurrences (both deep venous thromboses) compared with 8 of 32 (25%) in the standard care group (3, pulmonary emboli and 5, deep venous thromboses), yielding a relative risk of 5.0 (95% CI, 1.1 to 21.9; P = 0.02). Two of the eight recurrences in the standard care group occurred in patients who were no longer receiving warfarin. Exclusion of these two recurrences reduced the relative risk to 4.0 (CI, 0.9 to 18.5; P
Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
9 of 16 20/06/2006 2:27 PM
= 0.06).
Nomogram Performance and Implementation
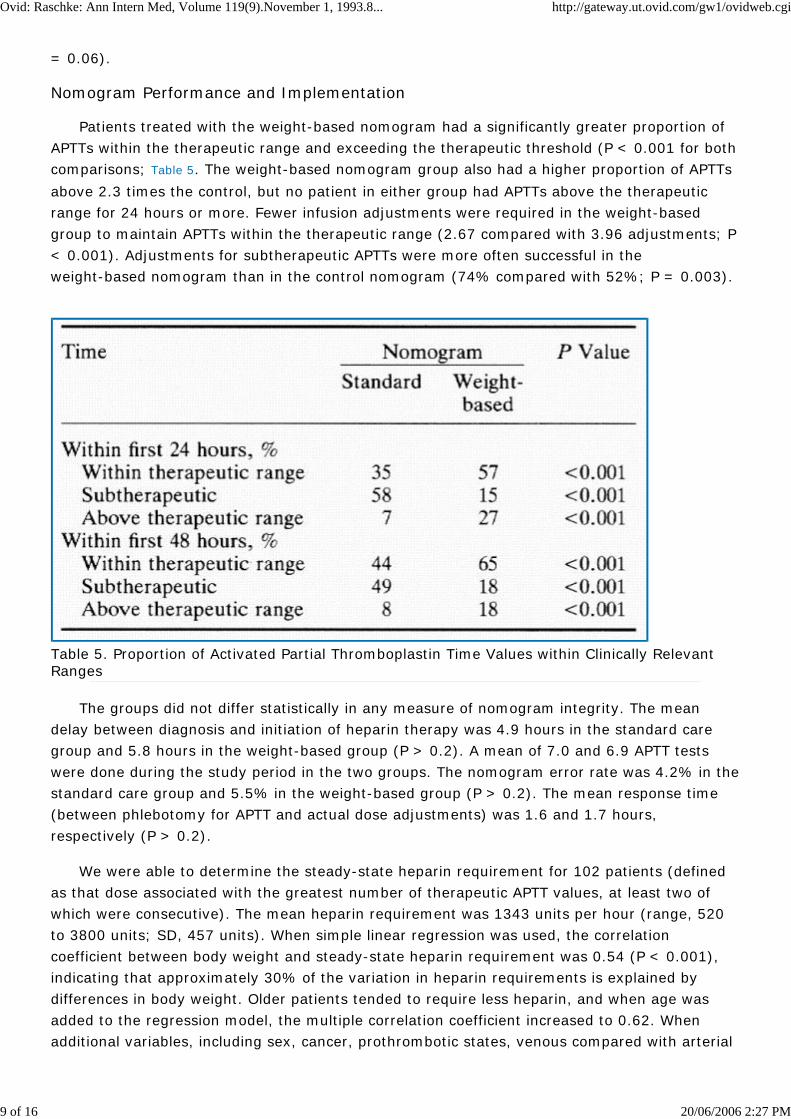
Patients treated with the weight-based nomogram had a significantly greater proportion of APTTs within the therapeutic range and exceeding the therapeutic threshold (P < 0.001 for both comparisons; Table 5. The weight-based nomogram group also had a higher proportion of APTTs
above 2.3 times the control, but no patient in either group had APTTs above the therapeutic range for 24 hours or more. Fewer infusion adjustments were required in the weight-based group to maintain APTTs within the therapeutic range (2.67 compared with 3.96 adjustments; P < 0.001). Adjustments for subtherapeutic APTTs were more often successful in the weight-based nomogram than in the control nomogram (74% compared with 52%; P = 0.003).
Table 5. Proportion of Activated Partial Thromboplastin Time Values within Clinically Relevant Ranges
The groups did not differ statistically in any measure of nomogram integrity. The mean delay between diagnosis and initiation of heparin therapy was 4.9 hours in the standard care group and 5.8 hours in the weight-based group (P > 0.2). A mean of 7.0 and 6.9 APTT tests were done during the study period in the two groups. The nomogram error rate was 4.2% in thestandard care group and 5.5% in the weight-based group (P > 0.2). The mean response time (between phlebotomy for APTT and actual dose adjustments) was 1.6 and 1.7 hours, respectively (P > 0.2).
We were able to determine the steady-state heparin requirement for 102 patients (defined as that dose associated with the greatest number of therapeutic APTT values, at least two of which were consecutive). The mean heparin requirement was 1343 units per hour (range, 520 to 3800 units; SD, 457 units). When simple linear regression was used, the correlation coefficient between body weight and steady-state heparin requirement was 0.54 (P < 0.001), indicating that approximately 30% of the variation in heparin requirements is explained by differences in body weight. Older patients tended to require less heparin, and when age was added to the regression model, the multiple correlation coefficient increased to 0.62. When additional variables, including sex, cancer, prothrombotic states, venous compared with arterial

Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
10 of 16 20/06/2006 2:27 PM
thromboembolism, and presence of pulmonary embolus, were entered in a stepwise fashion none statistically altered heparin requirements.
Nine patients treated with the weight-based nomogram weighed more than 100 kg (101 to 131 kg). Despite the fact that the initial heparin infusion rates calculated for these patients ranged as high as 2350 units per hour, all nine achieved an APTT within the therapeutic range in24 hours, and APTTs above the therapeutic range within the initial 48 hours of treatment were no more frequent than in patients who weighed less than 100 kg (1.38 compared with 1.4; P > 0.2).
The relative risk for recurrent thromboembolism in patients who failed to exceed the therapeutic threshold within 24 hours was 1.4 (P > 0.2) and in those who failed to exceed the threshold by 48 hours it was 4.5 (P = 0.08). Forced-entry multiple logistic regression showed that neither heparin requirement, age, sex, smoking history, cancer, previous deep venous thrombosis, nor the presence of pulmonary embolus explained thromboembolic recurrence (the P values for each of these variables was >0.2).
We carefully examined the possibility that the superior performance of the weight-based nomogram was simply caused by higher initial heparin infusion doses (mean, 1440 units per hour). First, the effect of the initial heparin infusion dose in absolute units and in units per body weight were examined using Cox proportional-hazards models for each of the two time-to-eventoutcomes (time to exceed the therapeutic threshold and time to achieve an APTT in the therapeutic range). Initial heparin dose per kilogram body weight was a highly significant predictor of success (P < 0.001 and P = 0.006, respectively), despite adjustment for absolute differences in initial heparin doses.
We also found that among patients in the weight-based group, success did not depend on whether they had received initial heparin infusion doses of 1250 units per hour. Twenty-one of the 22 patients who received initial doses less than 1250 units per hour exceeded the therapeutic threshold within 24 hours compared with 40 of 41 patients who received at least 1250 units per hour (P > 0.2). Thus, no advantage was apparent in initially receiving a larger heparin dose, so long as that dose was appropriate given the patient's body weight. Further, although all patients in the standard-care group initially received 1000 units per hour, the "unsuccessfully" anticoagulated patients in this group actually received lower initial heparin doses in units per kg body weight (11.9 compared with 14.7 units; P = 0.008), because their mean weight was 14 kg greater (87 compared with 73 kg; P = 0.01).
Overall, 54 of 115 patients in our study (47%) received less than 30 000 units of heparin in the first 24 hours (<1250 units per hour) after the initial bolus, yet all but one exceeded the therapeutic threshold within 24 hours. The mean weight in this group was 16 kg less than that of other patients (P = 0.04); therefore, although they received what some would consider insufficient doses of heparin, the initial dose on a per-weight basis was adequate (mean, 16.2 units per kg per hour). These analyses all suggest that initial heparin dose in units per kilogram body weight is a more powerful predictor of success than any of the absolute measures of the initial heparin dose.
Discussion
Our study showed that the weight-based heparin nomogram is effective, safe, and superior to one based on a prevalent standard of practice. This new nomogram individualizes heparin
Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
11 of 16 20/06/2006 2:27 PM
doses by patient weight and thereby rapidly achieves therapeutic goals while avoiding prolongedperiods of excessive anticoagulation. It performs well when implemented by staff nurses in community hospitals and it was developed using an APTT assay that allows wide generalizability.We propose that the weight-based nomogram be considered for adoption as the current standard of practice for hospitalized patients requiring intravenous heparin.
We agree with Hull and colleagues, Cruickshank and colleagues, and others that the use of aheparin nomogram has advantages over intuitive dosing practices [16,17]. Our own "standard
nomogram" rapidly exceeded the therapeutic threshold in three quarters of our control patients, a performance comparable to that of Cruickshank and colleagues' nomogram [17], and far
superior to practice audits and historical controls cited in other studies [6,7,29].
We believe there are two main reasons for the superior performance of the weight-based nomogram. First, it calculates patient-specific heparin doses that approximate the optimum dosefor each individual. The weight-based nomogram prescribed initial doses closer to eventual heparin requirements, drove subtherapeutic APTT results above the therapeutic threshold more rapidly, and required fewer dose adjustments to maintain APTT values within the therapeutic range. Our results confirm that body weight is the best single predictor of individual heparin requirements. Second, although it was consistent with the concurrent recommendations of the American College of Chest Physicians [13], the "standard-care" nomogram used an initial heparin
infusion dose now known to be insufficient. Nevertheless, an exhaustive analysis of our data showed that the success of the weight-based nomogram cannot be attributed to the fact that it used larger initial heparin doses. The dominant predictor of success was the administration of a heparin dose appropriate for the individual patient's body weight.
We believe that rapidly exceeding the therapeutic threshold to minimize recurrent thromboembolism is the primary goal of intravenous anticoagulation, but it is also prudent to avoid excessive anticoagulation. Hull and colleagues' nomogram exceeded the therapeutic threshold in 98% of patients within 24 hours by using large initial heparin doses, but 47% of their patients had APTTs persisting above the therapeutic range for 24 or more consecutive hours [16]. Major bleeding complications occurred in 6.5% (16 of 199) of their patients,
consistent with the 5.2% rate in a recent meta-analysis [41]. By contrast, the success of our
weight-based nomogram was equivalent to that reported by Hull and colleagues, but none of our patients had APTTs above the therapeutic range persisting for 24 hours, and none had a major hemorrhage. The boundaries of the therapeutic range in our study correlated with anti-factor Xa levels of 0.38 to 0.57 units per mL, narrower than the standard range (0.35 to 0.70 units per mL; [25]); therefore, our low bleeding rate may reflect "tight control" of
anticoagulation.
This argument assumes a relationship between APTT levels above the therapeutic range andhemorrhagic complications: a controversial issue. Bleeding is related to the dose of heparin administered and to various measures of heparin activity such as the whole blood clotting time [19,20,21,22,42], so it seems logical that it should also be related to excessive APTT values.
Although several studies have shown an increased risk for hemorrhage in patients with excessively prolonged APTTs [3,23,24], others have not [10,16,18]. Because the danger of
excessive prolongation of APTTs remains uncertain, it is almost universally recommended that heparin therapy be titrated to maintain APTTs within a therapeutic range rather than simply to exceed a therapeutic threshold [13,14,16,17,25]. This task appears to be straightforward using the
weight-based nomogram.

Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
12 of 16 20/06/2006 2:27 PM
Generalizability is a critical factor in the clinical utility of any heparin nomogram. Both previously published nomograms measured APTT values with a highly sensitive thromboplastin reagent, used by less than 10% of U.S. hospitals and yielding APTTs up to 18.6 seconds longer than more commonly used reagents [27]. In our study, the most common reagent in the United
States (plain Dade actin) was used to measure APTT on the most widely used automated anticoagulation systems. This analytic technique has intermediate sensitivity; more than 80% ofthe institutions participating in the 1992 College of American Pathologists survey use test systems yielding APTT results within 5 seconds of those used in our nomogram [27]. Thus,
institutions using plain Dade Actin, Dade-Actin, Dade-Actin FSL, or IL Test APTT reagents, or those whose mean control APTT is under 30 seconds, can currently use the APTT ranges in our nomogram without making adjustments.
Other institutions may need to customize the nomogram's APTT ranges for local use in one of two ways. Activated partial thromboplastin time values may be standardized by comparing them with other measures of heparin activity (anti-factor Xa activity or protamine titration) [17].
This method is accurate but imprecise because of wide interpatient variation in the correlation between these tests [28,43]. A more practical but less accurate alternative involves the use of
APTT ratios (actual APTT/control APTT), as shown in Table 2RF 13 *. Unfortunately, a system
analogous to the International Normalized Ratio is currently unavailable for standardizing APTT results.
Our study has several potential limitations. First, the nurses who implemented the nomograms were not blinded; however, they could not influence the primary outcome measurements, and monitoring of all steps in nomogram implementation show no unintended co-intervention. Second, some may question the design of our standard nomogram. It is difficultto model the standard of practice in heparin management; however, we feel the standard care nomogram probably overestimated the typical quality of care. Its performance is superior to that described in previous audits of intravenous anticoagulation and in the historical controls used in other studies [6,7,17,29]. Third, our study did not address the effect of simultaneous
warfarin administration on nomogram performance; Hull and colleagues' previous study addressed this issue [16].
Recurrent thromboembolism occurred significantly more frequently among standard care group patients, but we cannot attribute this finding solely to differences in nomogram performance. The recurrence rate in our standard care group (25%) is higher than that reportedby others [3,44,45,46], and we did not monitor the adequacy of outpatient anticoagulation. Two
patients in the standard care group with recurrences had discontinued warfarin prematurely; these outcomes cannot be attributed to initial heparin management.
Nevertheless, the 5% recurrence rate observed in the patients in our weight-based heparin group compares favorably with results from other studies [3,44,45,46]. The only clinical factor we
identified that predicted recurrence was failure to exceed the therapeutic threshold within 48 hours, a finding consistent with the previous observations by Hull and colleagues and by Basu and associates [3,10]. These findings raise an intriguing question. Why should the first 48 hours
of heparin therapy influence recurrences weeks or months later? We tested the alternative hypothesis--that patients destined to suffer recurrence were "heparin resistant" to begin with--and found that the steady-state heparin requirement did not differ among patients with and without recurrence (1357 compared with 1332 units per hour; P > 0.2). We agree with Hull,Hirsh, and others that rapid attainment of therapeutic APTT does indeed affect the risk for
Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
13 of 16 20/06/2006 2:27 PM
recurrent thromboembolism. It has been postulated that "protection" of clot-bound thrombin from heparin-antithrombin III complexes may play a role in this phenomenon [47,48].
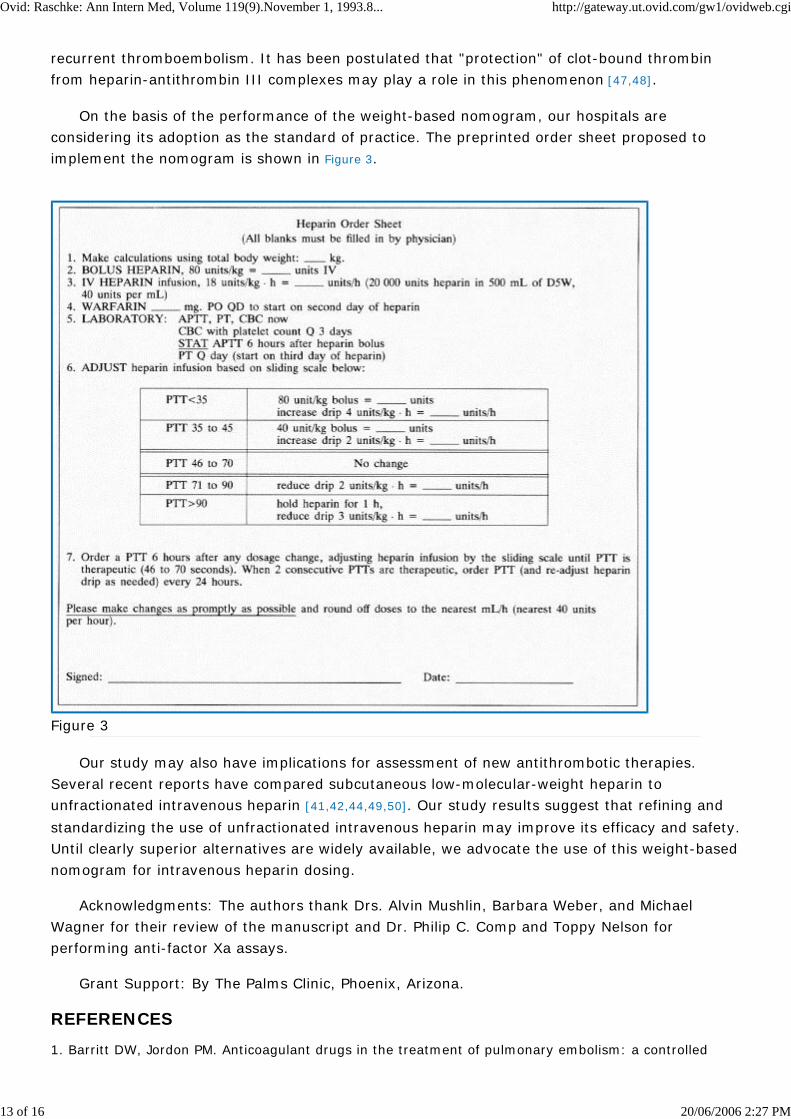
On the basis of the performance of the weight-based nomogram, our hospitals are considering its adoption as the standard of practice. The preprinted order sheet proposed to implement the nomogram is shown in Figure 3.
Figure 3
Our study may also have implications for assessment of new antithrombotic therapies. Several recent reports have compared subcutaneous low-molecular-weight heparin to unfractionated intravenous heparin [41,42,44,49,50]. Our study results suggest that refining and
standardizing the use of unfractionated intravenous heparin may improve its efficacy and safety.Until clearly superior alternatives are widely available, we advocate the use of this weight-basednomogram for intravenous heparin dosing.
Acknowledgments: The authors thank Drs. Alvin Mushlin, Barbara Weber, and Michael Wagner for their review of the manuscript and Dr. Philip C. Comp and Toppy Nelson for performing anti-factor Xa assays.
Grant Support: By The Palms Clinic, Phoenix, Arizona.
REFERENCES
1. Barritt DW, Jordon PM. Anticoagulant drugs in the treatment of pulmonary embolism: a controlled

Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
14 of 16 20/06/2006 2:27 PM
trial. Lancet. 1960;1:1309-12. Bibliographic Links Library Holdings [Context Link]
2. Theroux P, Ouimet H, McCans J, Latour JG, Joly P, Levy G, et al. Aspirin, heparin, or both to treat acute unstable angina? N Engl J Med. 1988;319:1105-11. Bibliographic Links Library Holdings [Context Link]
3. Hull RD, Raskob GE, Hirsh J, Jay RM, Leclerc JR, Geerts WH, et al. Continuous intravenous heparin compared with intermittent subcutaneous heparin in the initial treatment of proximal-vein thrombosis. N Engl J Med. 1986;315:1109-14. Bibliographic Links Library Holdings [Context Link]
4. Turpie AG, Robinson JG, Doyle DJ, Mulji AS, Mishkel GJ, Sealey BJ, et al. Comparison of high-dose with low-dose subcutaneous heparin to prevent left ventricular mural thrombosis in patients with acute transmural anterior myocardial infarction. N Engl J Med. 1989;320:352-7. Bibliographic Links Library Holdings [Context Link]
5. Reilly B, Raschke R, Sandhya S, Nieman TH. Intravenous heparin dosing: patterns and variations in internists' practices. J Gen Intern Med. (In press). [Context Link]
6. Fennerty AG, Thomas P, Backhouse G, Bentley P, Campbell IA, Routledge PA. Audit of control of heparin treatment. BMJ. 1985; 290:27-8. [Context Link]
7. Wheeler AP, Jaquiss RD, Newman JH. Physician practices in the treatment of pulmonary embolism anddeep venous thrombosis. Arch Intern Med. 1988;148:1321-5. Bibliographic Links Library Holdings[Context Link]
8. Kashtan J, Conti S, Blaisdell FW. Heparin therapy for deep venous thrombosis. Am J Surg. 1980;140:836-40. Bibliographic Links Library Holdings [Context Link]
9. Coon WW, Willis PW 3d, Symons MJ. Assessment of anticoagulant treatment of venous thromboembolism. Ann Surg. 1969;170:559-68. Bibliographic Links Library Holdings [Context Link]
10. Basu D, Gallus A, Hirsh J, Cade J. A prospective study of the value of monitoring heparin treatment with the activated partial thromboplastin time. N Engl J Med. 1972;287:324-7. Bibliographic LinksLibrary Holdings [Context Link]
11. Kaplan K, Davison R, Parker M, Mayberry B, Feiereisel P, Salinger M. Role of heparin after intravenous thrombolytic therapy for acute myocardial infarction. Am J Cardiol. 1987;59:241-4. Bibliographic Links Library Holdings [Context Link]
12. Camilleri JF, Bonnet JL, Bouvier JL, Levy G, Djiane P, Bory M, et al. Thrombolyse intraveineuse dans l'infarctus du myocarde: influence de la qualite de l'anticoagulation sur le taux de recidives precoces d'angor ou d'infarctus. Arch Mal Coeur. 1988;81:1037-41. Bibliographic Links Library Holdings[Context Link]
13. Hyers TM, Hull RD, Weg JG. Antithrombotic therapy for venous thromboembolic disease. Chest. 1989;95(Suppl):37S-51S. Bibliographic Links Library Holdings [Context Link]
14. Hyers TM, Hull RD, Weg JG. Antithrombotic therapy for venous thromboembolic disease. Chest. 1992;102(Suppl.):408S-25S. [Context Link]
15. Cairns JA, Hirsh J, Lewis HD Jr, Resnekov L, Theroux P. Antithrombotic agents in coronary artery disease. Chest. 1992; 102(Suppl.):456S-81S. [Context Link]
16. Hull RD, Raskob GE, Rosenbloom D, Lemaire J, Pineo GF, Baylis B, et al. Optimal therapeutic level of heparin therapy in patients with venous thromboembolism. Arch Intern Med. 1992;152:1589-95. [ContextLink]
17. Cruickshank MK, Levine MN, Hirsh J, Roberts R, Siguenza M. A standard heparin nomogram for the management of heparin therapy. Arch Intern Med. 1991;151:333-7. Bibliographic Links Library Holdings [Context Link]
18. Conti S, Daschbach M, Blaisdell FW. A comparison of high-dose versus conventional-dose heparin therapy for deep vein thrombosis. Surgery. 1982;92:972-7. Bibliographic Links Library Holdings[Context Link]
19. Levine MN, Hirsh J, Kelton JG. Heparin-induced bleeding. In: Lane DA, Lindahl U, eds. Heparin: Chemical and Biological Properties, Clinical Applications. London: Edward Arnold; 1989:517-32. [Context Link]

Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
15 of 16 20/06/2006 2:27 PM
20. O'Sullivan EF, Hirsh J, McCarthy RA, Gruchy GC de. Heparin in the treatment of venous thromboembolic disease: administration, control, and results. Med J Austral. 1968;2:153-9. Bibliographic Links Library Holdings [Context Link]
21. The Urokinase Pulmonary Embolism Trial. A National Cooperative Study. Circulation. 1973;47(Suppl.):1-108. [Context Link]
22. Wilson JR, Lampman J. Heparin therapy: a randomized prospective study. Am Heart J. 1979;97:155-8. Bibliographic Links Library Holdings [Context Link]
23. Norman CS, Provan JL. Control and complications of intermittent heparin therapy. Surg Gynecol Obstet. 1977;145:338-42. Bibliographic Links Library Holdings [Context Link]
24. Landefeld CS, Cook EF, Flatley M, Weisberg M, Goldman L. Identification and preliminary validation of predictors of major bleeding in hospitalized patients starting anticoagulant therapy. Am J Med. 1987;82:703-13. Bibliographic Links Library Holdings [Context Link]
25. Hirsh J. Heparin. N Engl J Med. 1991;324:1565-74. Bibliographic Links Library Holdings [Context Link]
26. Raschke R, Hertel G. Clinical use of the heparin nomogram (Letter). Arch Intern Med. 1991;151:2318-21. Bibliographic Links Library Holdings [Context Link]
27. College of American Pathologists. 1992 CAP Surveys, Set CG2-A. Northfield, Illinois: College of American Pathologists; 1992:4-8. [Context Link]
28. Cipolle R, Seifert R, Neilan B, Zaske DE, Haus E. Heparin kinetics: variables related to disposition anddosage. Clin PharmacolTher. 1981;29:387-93. [Context Link]
29. Cipolle RJ, Rodvold KA. Heparin. In: Evans WE, Schentag JJ, Jusko WJ;eds. Applied Pharmacokinetics. Spokane, Washington: Applied Therapeutics; 1986:908-42. [Context Link]
30. Braunwald E. Unstable angina-A classification. Circulation. 1989; 80:410-4. Ovid Full TextBibliographic Links Library Holdings [Context Link]
31. Guidry JR, Raschke R, Morkunas AR. Toxic effects of drugs used in the ICU. Anticoagulants and thrombolytics. Crit Care Clin. 1991;7: 533-54. Bibliographic Links Library Holdings [Context Link]
32. Handeland GF, Abildgaard U, Holm HA, Arnesen KE. Dose adjusted heparin treatment of deep venousthrombosis: a comparison of unfractionated and low molecular weight heparin. Eur J Clin Pharmacol. 1990;39:107-12. Bibliographic Links Library Holdings
33. Holm HA, Finnanger B, Hartmann A, Laerum F, Lohren O, Ruud TE, et al. Heparin treatment of deep venous thrombosis in 280 patients: symptoms related to dosage. Acta Med Scand. 1984;215: 47-53. Bibliographic Links Library Holdings
34. Talstad I. Heparin therapy adjusted for body weight. Am J Clin Pathol. 1985;83:378-81. Bibliographic Links Library Holdings [Context Link]
35. Wilson JE 3d, Bynum LJ, Parkey RW. Heparin therapy in venous thromboembolism. Am J Med. 1981;70:808-16. Bibliographic Links Library Holdings
36. Hattersley PG, Mitsuoka JC, King JH. Heparin therapy for thromboembolic disorders. JAMA. 1983;250:1413-6. Bibliographic Links Library Holdings
37. Ellison MJ, Sawyer WT, Mills TC. Calculation of heparin dosage in a morbidly obese woman. Clin Pharm. 1989;8:65-8. Bibliographic Links Library Holdings [Context Link]
38. Raschke R, Guidry J, Laufer N. Heparin-nitroglycerin interaction. (Letter). Am Heart J. 1991;121:1849. Library Holdings [Context Link]
39. Andersson G, Fagrell B, Holmgren K, Johnsson T, Ljungberg B, Nilsson E, et al. Subcutaneous administration of heparin. A randomised comparison with intravenous administration of heparin to patients with deep-vein thrombosis. Thromb Res. 1982;27:631-9. Bibliographic Links Library Holdings [Context Link]
40. Pini M, Pattacini C, Quintavalla R, Poli T, Megha A, Tegliaferri A, et al. Subcutaneous vs intravenous heparin in the treatment of deep venous thrombosis--a randomized clinical trial. Thromb Haemost.

Ovid: Raschke: Ann Intern Med, Volume 119(9).November 1, 1993.8... http://gateway.ut.ovid.com/gw1/ovidweb.cgi
16 of 16 20/06/2006 2:27 PM
1990;64:222-6. Bibliographic Links Library Holdings [Context Link]
41. Hommes DW, Bura A, Mazzolai L, Buller HR, ten Cate JW. Subcutaneous heparin compared with continuous intravenous heparin administration in the initial treatment of deep vein thrombosis. Ann Intern Med. 1992;116:279-84. Bibliographic Links Library Holdings [Context Link]
42. Nieuwenhuis HK, Albada J, Banga JD, Sixma JJ. Identification of risk factors for bleeding during treatment of acute venous thromboembolism with heparin or low molecular weight heparin. Blood. 1991;78:2337-43. Bibliographic Links Library Holdings [Context Link]
43. Whitfield LR, Levy G. Relationship between concentration and anticoagulant effect of heparin in plasma of normal subjects: magnitude and predictability of interindividual differences. Clin Pharmacol Ther. 1980;28:509-16. Bibliographic Links Library Holdings [Context Link]
44. Hull RD, Raskob GE, Pineo GF, Green D, Trowbridge AA, Elliott G, et al. Subcutaneous low-molecular-weight heparin compared with continuous intravenous heparin in the treatment of proximal-vein thrombosis. N Engl J Med. 1992;326:975-82. Bibliographic Links Library Holdings[Context Link]
45. Gallus A, Jackaman J, Tillett J, Mills W, Wycherley A. Safety and efficacy of warfarin started early after submassive venous thrombosis or pulmonary embolism. Lancet. 1986;2:1293-6. Bibliographic Links Library Holdings [Context Link]
46. Hull RD, Raskob GE, Rosenbloom D, Panju AA, Brill-Edwards P, Ginsberg JS, et al. Heparin for 5 daysas compared with 10 days in the initial treatment of proximal venous thrombosis. N Engl J Med. 1990;322:1260-4. Bibliographic Links Library Holdings [Context Link]
47. Weitz JI, Hudoba M, Massel D, Maraganore J, Hirsh J. Clot-bound thrombin is protected from inhibition by heparin-antithrombin III but is susceptible to inactivation by antithrombin-III independent inhibitors. J Clin Invest. 1990;86:385-91. Bibliographic Links Library Holdings [Context Link]
48. Hogg PJ, Jackson CM. Fibrin monomer protects thrombin from inactivation by heparin-antithrombin III: implications for heparin efficacy. Proc Natl Acad Sci USA. 1989;86:3619-23. Bibliographic LinksLibrary Holdings [Context Link]
49. Thery C, Simonneau G, Meyer G, Helenon O, Bridey F, Armagnac C, et al. Randomized trial of subcutaneous low-molecular-weight heparin CY 216 (Fraxiparine) compared with intravenous unfractionated heparin in the curative treatment of submassive pulmonary embolism. Circulation. 1992;85:1380-9. Ovid Full Text Bibliographic Links Library Holdings [Context Link]
50. Prandoni P, Lensing AW, Buller HR, Carta M, Cogo A, Vigo M, et al. Comparison of subcutaneous low-molecular-weight heparin with intravenous standard heparin in proximal deep-vein thrombosis. Lancet. 1992;339:441-5. Bibliographic Links Library Holdings [Context Link]
Accession Number: 00000605-199311010-00002
Copyright (c) 2000-2006 Ovid Technologies, Inc.Version: rel10.3.0, SourceID 1.12052.1.81