to download the may/jun issue
TRANSCRIPT

THE FLAGSHIP PUBLICATION OF THE SINGHEALTH DUKE-NUS ACADEMIC MEDICAL CENTREMCI (P) 071/05/2015
WWW.SGH.COM.SG | WWW.SINGHEALTH.COM.SG
MAYJUN2016
AWARD OFEXCELLENCE
APEX AWARDS 2015
BEST HEALTHCARE/MEDICAL PUBLICATION
FINALISTCONTENT MARKETING
AWARDS 2015
不胖、不喝酒的年轻人为何
有脂肪肝P25
YOUNG, NON-DRINKERS AND NOT OBESE, BUT
WITH FATTY LIVER DISEASE
P3
PHO
TO: A
LVIN
N L
IM
05
26在观明综合医院留医的中风病人现可 通过新计划接受跟进评估及测试
06
A new two-drug treatment offers fresh hope when lymphoma relapses
Palm tocotrienol being tested to see if it works to protect against Parkinson’s
10Routine screening of pregnant women for gestational diabetes mellitus
20Useful home devices to help the elderly live safely and easily
SINGAPORE HEALTH MAY– JUN 201602
All rights reserved. Copyright by SGH (registration no: 198703907Z). Opinions expressed in Singapore Health are solely those of the writers and are not necessarily endorsed by SGH, SingHealth Group and/or SPH Magazines Pte Ltd (registration no: 196900476M) and their related companies. They are not responsible or liable in any way for the contents of any of the advertisements, articles, photographs or illustrations contained in this publication. Editorial enquiries should be directed to the Editor, Singapore Health, 168 Jalan Bukit Merah, #13-01 Surbana One, Singapore 150168. Tel:+65 6222-3322. E-mail: [email protected]. Unsolicited material will not be returned unless accompanied by a self-addressed envelope and sufficient return postage. While every reasonable care will be taken by the Editor, no responsibility is assumed for the return of unsolicited material. ALL INFORMATION CORRECT AT TIME OF PRINTING. MCI (P) 071/05/2015. Printed in Singapore by Singapore Press Holdings Limited (registration no: 198402868E).
For advertising enquiries, please call 6319-3022 or e-mail [email protected]
For editorial enquiries, please e-mail [email protected]
GROUP EDITOR-IN-CHIEFCaroline NguiGROUP EDITOR Joanna Lee-Miller
EDITORIAL & CREATIVESENIOR EDITOR Dora TayEDITOR Serene FooSUB-EDITOR Annabelle Bok
ASSOCIATE CREATIVE DIRECTOR Jayson Ong ART DIRECTORGeoffrey Lim
GRAPHIC DESIGNERHuy Pham
MANAGING DIRECTOR Dennis PuaGENERAL MANAGER Christopher Chan
SALES & CLIENT MANAGEMENTACCOUNT MANAGER, ADVERTISING SALESLin Mi’er SENIOR EXECUTIVECLIENT MANAGEMENTJanice Low
PUBLISHING SERVICESSENIOR EXECUTIVELin Feng
PUBLISHING AGENT
CONTENT ADVISOR Tan-Huang Shuo MeiGroup Director, Communications & Service Quality, SingHealth
EDITORIAL TEAMAngela Ng (SGH)Lim Mui Khi (SGH) Ann Peters (SingHealth) Deborah Moh (SGH)
Read Singapore Health online atwww.sgh.com.sg/singaporehealth
PUBLISHERS
CO-PUBLISHERS
®

NEWS 03MAY– JUN 2016 SINGAPORE HEALTH
> Continued on page 4 (华文版本请翻阅至27页)
What’s wrong with my liver? They are young, hardly touch alcohol, and are neither obese nor diabetic, but still diagnosed with fatty liver disease. What is happening? By Low Shi Ping
N ON-ALCOHOLIC fatty liver disease has lately become a cause for con-cern in the medical community
here because of the rising incidence and changing demographics.
In the last decade, the incidence has risen to almost 50 per cent of the adult population. Those diagnosed with fatty liver disease do not fit the usual profile of patients who have known risk factors – heavy alcohol drinkers, or those who are obese or diabetic.
New data shows that people with-out these conditions are now develop-ing the disease. Some are in their 20s and of average weight and appearance, and have one common characteristic – they either drink very little alcohol or none at all. “It’s difficult to know who has this disease without scanning their
liver,” said Professor Pierce Chow, Senior Consultant, Division of Surgical Oncology, National Cancer Centre Singapore (NCCS), who has been leading research on the disease and its relationship to liver cancer.
Fatty liver is defined as a liver with at least 5 per cent fat in its cell content, which can be detected through a biopsy or by MRI, CT or ultrasound scan. How-ever, an ultrasound scan can only pick up a fatty liver when the liver has at least 30 per cent fat.
If caught early, and before the inflamed liver has developed scarring or cirrhosis, the disease can be reversed. But once it becomes cirrhotic, the dis-ease is irreversible because liver cells have been replaced by scar tissue, making the organ progressively dysfunc-
tional. Cirrhosis of the liver also puts a person at risk of developing liver cancer.
Another concern is that the simple form of the disease can progress to non-alcoholic steatohepatitis, a more severe and complicated form of fatty liver.
An even more troubling trend has emerged, said Prof Chow. Patients with non-alcoholic fatty liver disease are increasingly observed to bypass this non-alcoholic steatohepatitis stage and cirrhosis, and develop liver cancer.
“This has been noted by a number of international centres, including NCCS, and we are increasingly concerned about it. Global statistics project that in the next 10 to 15 years, non-alcoholic fatty liver disease will be the main cause of liver cancer around the world, surpass-ing even Hepatitis B and C, which are
Professor Pierce Chow (extreme left) teaching medical students about fatty liver disease. Global statistics project that in the next 10 to 15 years, non-alcoholic fatty liver disease will be the main cause of liver cancer around the world, surpassing even Hepatitis B and C, which are currently the number one causes.
PHO
TOS:
ALV
INN
LIM
/ 12
3RF
WHAT IS CAUSING IT?
Although the jury is still out on what causes non-alcoholic fatty liver disease, the medical community has a few tentative leads, according to Prof Chow. The causes could be due to many factors.
Genetic predispositionOne hypothesis is that people whose ancestors are genetically well-adapted to cyclical famine have bodies that are particularly efficient at storing consumed calories. With improved standards of living and increased consumption of food, especially carbohydrates, the body is predisposed to a condition called metabolic syndrome, which increases the risk of diabetes and non-alcoholic liver disease.
Industrial fructoseAnother theory, which is slightly more controversial, is related to changes in the food chain. There is a belief that the epidemic started in the 1970s because of the introduction of industrially manufactured sugar, specifically artificial fructose, into the manufacturing of foods such as biscuits, instant noodles and soft drinks. Fructose has a chemical structure that predisposes people to developing a fatty liver.
Change in intestinal bacteriaA third theory is linked to changes in bacteria in the intestine. Animal studies have shown that when sugar in the diet is modified during digestion, it affects bacteria in the gut. The bacteria interact with receptors in the cells of the intestine known as peroxisome proliferator-activated receptors (PPARs), which give off a cascade of messages and signals to the rest of the body to change its metabolism. This might instruct certain organs, the liver for instance, to store fat, leading to fatty liver disease.

04 NEWS
> Continued from page 3
What’s wrong with my liver?
SINGAPORE HEALTH MAY– JUN 2016
data is strong but the mechanisms are unclear,” said Prof Chow.
The high incidence rate here was detected by one of Prof Chow’s medical students, Mr Kevin Khaw from Duke-NUS Medical School.
“While attached to the ward and clinic, he noticed from looking at scans that a
Patients in the early stages of fatty liver disease usually display no symptoms. However, as it develops, tiredness, a sensation of bloating, loss of appetite and pain in the right upper abdomen might occur. Should this progress to the non-alcoholic steatohepatitis stage or become cirrhotic, signs will include nausea, jaundice, a swollen abdomen and poor concentration.
If identified early, the disease can be successfully treated so that the liver returns to its non-fatty state.
“It is potentially reversible until it
currently the number one causes,” he said.
The rising incidence of non-alcoholic fatty liver disease in Singapore is consis-tent with the rest of the developed world. In the US, non-alcoholic steatohepatitis is the second cause of patients needing a liver transplant. “The epidemiological
becomes cirrhotic,” said Prof Chow. He advises patients who have the
disease to lose about 10 per cent of their body weight through lifestyle changes, as clinical studies have shown that this consistently reverses fatty liver. One way to do this is to decrease intake of carbohydrates, especially refined sugars. Exercise is useful too, but to be effective it must be very intensive.
Prof Chow said it is a common misunderstanding among his patients that removing fat from their diet will keep the disease at bay.
CATCH IT EARLY“Unfortunately it is not so simple. The
good news is you can still manage it through lifestyle adjustments.”
At NCCS, animal studies are being done and there are plans to follow up with a prospective population study. “Not all patients with fatty liver disease will get cancer. We do not know enough, so research is important to allow us to understand who the high risk patients are.
“We want to be able to identify such patients so that we can inter-vene now to prevent cancer in the future,” said Prof Chow.
significant number of patients admitted for gallbladder surgery had non-alco-holic fatty liver disease. He realised that the incidence was higher than expected, so he did a comparison study,” said Prof Chow. The results (which won Mr Khaw a prize at a scientific conference) were staggering. Between 2000 and 2003, only
30 per cent of patients with gallstone dis-ease had concomitant fatty liver disease. A decade later, between 2010 and 2013, the figure was 50 per cent.
“These are patients who came to con-sult me for gallstone disease, not liver disease, but our routine scans showed they also had fatty liver,” said Prof Chow.
As fatty liver disease develops, tiredness, a sensation of bloating, loss of appetite and pain in the right upper abdomen might occur.
28 新闻 2015年9– 10月刊
> Continued from page 27 (失智症?我还很年轻)
看护者与患者• 接受检查:由于青年型失智症的症状不同和模拟两可,鼓励家人接受检查。让医生进行检查和评估,如家庭病史、认知评估、血检或脑部扫描等,可帮助排除可逆性的原因
• 做好准备:若家人被确诊患上失智症,你和家里的其他成员的支持至关重要。所以多了解病症和掌握患者的病情,可帮助你们对抗病症
• 保持关系良好:如果你和患者之间关系不好,那么试着修补并重新建立友好关系因为可以避
在本地,那哥安丹副教授也正在进行类似,但针对亚洲人的研究,成为东南亚首个与失智症基因有关课题的研究。这个涉及超过300名患者的研究将由国家医学研究理事会资助。
他说:“我们打算利用先进的神经成像技术进行基因分析,来找出亚洲人可能共有和独有的基因。我们也会邀请患者的家属参与这项研究,以确认家庭中的基因继承模式。”
如何应付家中失智症患若 您 家 中 有 青 年 型 失 智 症 患者,不管是生活琐事或情绪上都会影响家庭的所有成员。
免发生负面情绪反应• 规划未来:照料一名失智患者的花费不少。你应该未雨绸缪,替患者规划未来可能需要的资源,包括财务、产业、治疗和护理等事宜,别等到病情恶化时才来操心
• 学会休息:照顾患者可以是非常耗精力的事。当你感到疲惫时,找个机会休息一下充个电,无须感到内疚。在这期间可以将患者暂时托付给日间看护所或雇用家庭护理员等服务
国立脑神经医学院(NNI)神经内科心理学家伊芙琳席尔瓦(EvelineSilva)提供
孩子、看护者以及患者• 坦白以对:不要对孩子隐瞒家中有人患有青年型失智症的事实。如果觉得很难解释,可以请专业人士,或了解失智症的人
帮忙• 参与看护:让孩子们示意鼓励患者玩一些可以激发认知能力的游戏,如挑竹签和填字游戏
• 避免自责:让孩子们知道患病原因不是由他们引起的
• 照顾自己:看护者必须保持身心健康,才能全心全意地照顾患者。如果发现孩子应付不来,你可以帮助他们或让他们向别人求助
• 分享心情:多与孩子们互相分享心情或沟通,对彼此抒发或减轻疲劳或压力很有帮助
摘录自《失智症:理不清的大脑》
《失智症:理不清的大脑》,由脑神经医学院脑神经科资深临床护士林丽云撰写,是一本关于青年型失智症和其相关课题。内容丰富、简单易懂,适合青少年和年轻人阅读并从中获
益。这本书将会在不久后正式发行。
招募志愿者参与临床试验为了进一步了解失智症(阿尔茨海默氏症)和其相关课题,我们正在招募志愿者参与一项研究。若您或您有认识45岁或以上的人士,近期发现自己无论在行为、语言和记忆力上有任何异常表现或改变,请通过电子邮址 [email protected] 与脑神经医学院的临床试验研究部联络。您的参与或许能带来突破。
31新闻2014年9–10月刊
专家解答
烟霾使哮喘病加剧最近的烟霾使我的哮喘病病情恶化,经常发作。我该怎么做?在哮喘病发作时,患者的呼吸道会收窄,导致呼吸困难。如果没有适当地控制病情,让呼吸道受到环境的触发因素所刺激,病情很容易就会发作。要减少哮喘病发作,就必须控制好病情。因此,患者可能需要服用适量的控制性药物。
哮喘病的吸入性药物可被分为两大种类: 控制性药物:治疗肺炎,同时降低肺部对于触发因素,如烟霾这种环境污染物的敏感度,从而减轻敏感反应。
缓解性药物:在哮喘病发作时,舒缓并扩张已收缩的气管。在阴霾笼罩时,病情一般受到控制
的哮喘病患者可能会觉得病情转坏,并需要服用控制性药物。至于已在服药的患者,则可能需要医生调整药物剂量。
所有的哮喘病患者都应该有一份列明指示的哮喘病控制行动计划:识别早期症状,以便采取适当的措施,预防发作程度恶化;发作时需要采取的步骤;以及如何辨别发作程度是否严重到需要紧急救护治疗。
无论病情是否已受到良好的控制,所有哮喘病患者都应该随身携带一个吸入器,预防哮喘病随时发作。
新加坡保健服务集团综合诊疗所家庭内科顾问医生黄忠伟
我患上抑郁症了吗?我经常感到情绪低落,对任何东西都不感兴趣。这是不是抑郁症的征兆?月经来潮之前感到忧郁消沉是正常的吗? 月经来潮的前两周,有些妇女可能会感到情绪低落是因为黄体酮(一种会导致情绪消沉的荷尔蒙)一直在体内不断地增加所引起,又或者因为月经而必须避免进行某些活动,例如游泳/水上运动、穿紧身或浅色衣服,甚至性行为,而感到沮丧。
至于抑郁症,它主要的症状是情绪低落和意志消沉,或对任何东西失去兴趣和无法透过任何事物感到欢愉。其他症状还包括: 失眠(尤其是在凌晨醒来) 食欲不振和消瘦(或爆食和发胖)
无法集中精神或健忘 失去正能量或动力、无精打采(或容易激动和焦躁不安)
意志消极、过度内疚、绝望感,以及有自杀倾向。但如果以上症状连续出现超过两
周,并引起重大的痛苦或影响个人的日常生活能力时,那可能就是抑郁症了。
竹脚妇幼医院心理医学科主管及高级顾问医生陳瑜
近视可以治疗吗?我其中一名孩子患有近视。请问有什么方法治疗吗?如何预防近视度继续加深?另外,我也开始限制小儿子使用电脑和电子产品的时间。我是否过度反应了?遗传和环境因素会导致近视。如果你有近视,你孩子患上近视的几率会更高。此外,我们目前的生活模式也过份偏重于室内工作和近距离聚精会神。
为了减轻以上因素,保健促进局推行了一个计划,支持孩子多到户外活动,避免长时间留在室内。你也应该限制孩子玩电脑游戏和看电视的时间,并让他多到户外玩耍。
如果近视持续加深,我们可以通过其他方法来控制它,例如配戴特制
眼镜或隐形眼镜和使用阿托品滴眼剂(Atropine Eye Drop)。眼镜和隐形眼镜的治疗效果因人而异,一般成功率从零至30%不等。如果选用隐形眼镜来治疗,家长必须加倍小心护理,以确保孩子的眼睛不会受到感染和威胁到视力健康。
阿托品滴眼剂是一种能够减缓近视恶化的有效药剂,控制效率可达50%至80%。不过,不同浓度的滴眼剂可能会造成瞳孔放大和近距离视力模糊。
副作用较轻的较低浓度滴眼剂去年上市,给使用者更多样化的选择。如果你希望知道自己的孩子是否适合接受以上治疗,请咨询你的医生。
新加坡全国眼科中心及竹脚妇幼医院幼儿眼科与斜视治疗组高级顾问医生谢玮玲
Singapore Health is the official publication of Singapore General Hospital and SingHealth Group, the largest health care group in Singapore. Published bimonthly in a handy tabloid size, the newspaper aims to raise the health literacy level of Singaporeans. Singapore Health is available at Singapore General Hospital, KK Women’s and Children’s Hospital, Changi General Hospital, national speciality centres, and polyclinics under the SingHealth umbrella. It is also available at high-traffic points within the CBD area.
Singapore Health ensures your message gets across to your target audience.
Wide circulation that reaches over 160,000 readers Available at strategic locations
Contains authoritative health care news and information
For advertising enquiries, e-mail Lin Mi’er at [email protected]
31 CHI-HEX V3_R.indd 31 18/8/14 3:13 PM
Singapore Health is the official publication of Singapore General Hospital and SingHealth Group, the largest health-care group in Singapore. Published bimonthly in a handy tabloid size, the newspaper aims to raise the health literacy level of Singaporeans. Singapore Health is available at Singapore General Hospital, KK Women’s and Children’s Hospital, national specialit y centres, and polyclinic s under the SingHealth umbrella. It is also available at high-traffic points within the CBD area.
Singapore Health ensures your message gets across to your target audience.

Mr Ho Gim Bu (centre) participated in Dr Darryl Tan (left) and Associate Professor Goh Yeow Tee’s (right) PTCL trial after his disease returned. Six months before, he had undergone conventional treatment, including chemotherapy and autologous stem cell transplant.
For patients suffering from PTCL, a rare type of lymphoma that starts in the lymphatic system, a relapse almost always has a grim prognosis.
Test treatment lifts survival odds whenlymphoma relapses
FOR PATIENTS suf fe r ing f rom peripheral T-cell lymphoma or PTCL, a rare type of the cancer that starts
in the lymphatic system, a relapse almost always has a grim prognosis.
However, a multicentre phase II trial led by Singapore General Hospital (SGH) that uses a combination of two drugs not usually prescribed for PTCL is offering these patients fresh hope.
“We decided to combine panobinostat and bortezomib to treat this group of patients as studies have suggested that both drugs work very well together,” said Associate Professor Goh Yeow Tee, Senior Consultant, Department of Haematology, SGH, and senior author of the study.
Usually, when PTCL recurs, the stan-dard treatment is to prescribe one of several approved chemotherapy drugs. But, few patients respond to the treat-ment as their tumours did not shrink by at least half.
“The response rate of patients with relapsed PTCL is extremely poor – a very modest 25-29 per cent,” said Dr Darryl Tan, lead author of the study and Visiting Consultant, Department of Haematology, SGH.
But with the trial treatment, over 40 per cent of the PTCL patients involved responded to the panobinostat and bor-tezomib drug combination. More signifi-
More peripheral T-cell lymphoma patients respond to two-drug treatment, while a number had the rare cancer eradicated in multicentre trial. By Thava Rani
NEW FRONTIERS 05MAY– JUN 2016 SINGAPORE HEALTH
cantly, half of them no longer had signs of cancer after the treatment.
“This is the first time that a two non-chemotherapy drug combina-tion has been shown to be useful in treating this very difficult dis-ease,” said Dr Tan, who is in private practice.
T h e s t u d y w a s done at f ive ter t iar y hospitals in Singapore, Malaysia and South Korea between 2009 and 2013, with 25 par ticipants aged 35 to 79.
PHO
TO: 1
23RF
/ ALV
INN
LIM
THIS IS THE FIRST TIME THAT A TWO NON-CHEMOTHERAPY DRUG COMBINATION HAS BEEN SHOWN TO BE USEFUL IN TREATING THIS VERY DIFFICULT DISEASE.DR DARRYL TAN, LEAD AUTHOR OF THE STUDY AND VISITING CONSULTANT, DEPARTMENT OF HAEMATOLOGY, SGH
binations, as well as dosages, with the aim of making treatment more tolerable and durable.
At the same time, biomarker samples from the trial will be analysed to find out, if any, their correlation with the clinical responses.
Lymphoma, in its many forms, occurs most often in people in their 60s or older. PTCL accounts for 10-15 per cent of all non-Hodgkin lymphomas worldwide.
But in some parts of Asia, the inci-dence of this rare and aggressive cancer is a higher 20-25 per cent. In Singapore, close to 700 people are diagnosed with lymphoma each year.
New drugs have improved the survival prospects of lymphoma patients in gen-eral, but not for PTCL patients who often don’t respond to conventional treatment after a relapse.
For patients who undergo conven-tional treatment for the disease, includ-ing chemotherapy and stem cell trans-plant, less than 30 per cent are alive three years after. And at the 10-year mark, the survival rate is under 10 per cent.
Most were in stage III or IV of the disease and were no longer respond-ing to current standards of care. The small number of par ticipants was due in part to the rarity of the dis-ease. Many also could not start treat-ment because they had become too sick.
At the time of the trial, bortezomib was an approved drug used to treat mul-tiple myeloma, another type of cancer, but not PTCL. Panobinostat, meanwhile, was a new drug that had yet to receive the approval of the US Food and Drug Administration (FDA).
Not only did more patients respond to the treatment, they also survived longer. This allowed five of them to undergo “curative stem-cell transplant, which was not an option for them previously,” said Prof Goh.
The trial found that patients had a prolonged survival of 10 months on aver-age, and that progression of the disease was delayed by about three months.
The drugs did bring on side effects such as dehydration, fatigue and diarrhoea. “But those side effects were nowhere as severe as those experienced when undergoing chemotherapy, and are tolerable even for older patients,” said Prof Goh, noting that their oldest patient was nearly 80.
The findings of the study were pub-lished in the prestigious medical journal The Lancet last July, and presented at a meeting of the American Society of Hematology (ASH).
Because many newer drugs and agents have become available since the trial started in 2008, the team is planning to look at other drugs and drug com-

When a brain cell is exposed to a toxic substance, it starts dying a programmed death by shutting down in stages. Palm tocotrienol prevents this shutdown process and protects the brain.
06 SINGAPORE HEALTH MAY– JUN 2016
A pill for Parkinson’s?
T HE NATIONAL NEUROSCIENCE Institute (NNI) is testing the substance, which is currently
already available in a pill form. NNI signed a Memorandum of Under-standing (MOU) with Malaysian pharma-ceutical company Hovid Berhad to test whether palm tocotrienol – extracted from crude palm oil – works in exper-imental models of Parkinson’s dis-ease. Clinical studies will be carried out subsequently.
“Our short- to mid-term plan is to come up with a drug to delay the onset of Parkinson’s for those at risk of the dis-ease,” said Professor Tan Eng King, NNI’s Director of Research.
A naturally existing compound, palm tocotrienol, which promises to protect against Parkinson’s and other neurological diseases, is being tested here now. By Low Shi Ping
NEW FRONTIERS
PHO
TOS:
ALV
INN
LIM
/ 12
3RF
He said clinical trials can begin sooner than usual because NNI already has an existing method of testing tocotrienol’s efficacy.
Mr David Ho, Managing Director, Hovid Berhad, explained how the compound works: “When a brain cell is exposed to a toxic substance, it starts dying a pro-grammed death by shutting down in stages. Palm tocotrienol prevents this shutdown process and protects the brain.”
He said that tocotrienol comes from the vitamin E family. Though from the same family, tocotrienols are very dif-ferent from the more commonly known tocopherol. The differences are not only in chemical structure, but also in bio-logical functions. For example, tocotrie-nols have been found to protect brain cells against cell death where tocoph-erols have been observed to not have this effect. Hovid currently sells a pat-
The signing of the MOU between Professor Tan Eng King (left), NNI, and Mr David Ho, Managing Director, Hovid Berhad to test whether palm tocotrienol works in experimental models of Parkinson’s disease.
ented formula (with Suprabio™ system) to increase tocotrienol absorption by up to 300 per cent.
Other studies on tocotrienol have yielded positive results, especially in con-nection with stroke.
One human trial conducted in Univer-siti Sains Malaysia involved more than 120 people with white matter lesions in the brain (dead cells that group together in the white matter of the brain and are typically a sign of degeneration, possibly leading to stroke). They were given either the compound or a placebo, and moni-tored through MRIs and blood chemistry tests.
Those who took tocotrienol showed no growth in white matter lesions, said Professor Yuen Kah Hay from Universiti Sains Malaysia, who worked on the human trial, and has led tocotrienol research for more than two decades.
Prof Tan said he was attracted to this project by the evidence of these studies and Hovid’s patented product, which is a natural product. “This collaboration has vast potential and brings together NNI’s focus on ageing and neurological diseases, and what Hovid has to offer. We can move forward as we have shared ideals. This is only a stepping stone. We have many plans in place,” said Prof Tan.
Associate Professor Ng Wai Hoe, Medical Director, NNI, said this advance-ment will benefit the ageing population. “The impact of neurodegenerative dis-eases extends not just to Parkinson’s. I am certain this can bring forth many more studies into other neurological dis-eases of significant global impact.”

Physiotherapist relieves pressure at A&E
NEWS 07MAY– JUN 2016 SINGAPORE HEALTH
Having a physiotherapist at A&E prevents unnecessary admission for some patients and allows doctors to focus on those in more critical condition. By Suki Lor
NOT EVERYONE WHO IS SEEN for emergency treatment needs to be admitted to hospital. Many
who are afflicted by sudden back pain and the like may only need some form of physiotherapy before being discharged from the A&E (accident and emergency department).
Not only will these patients with no other complications avoid having to be admitted or to return for an appointment to see a specialist first and a physiother-apy referral after, but expediting their care at that point also allows emergency medicine doctors to devote time to those with more serious conditions.
With that in mind, a physiotherapist has been attached to the Singapore General Hospital’s (SGH) Department of Emergency Medicine since February 2012. The service is available every day between 9am and 6pm.
PHO
TO: A
LVIN
N L
IMWE CAN’T ELIMINATE ALL READMISSIONS, BUT WE PLAY A ROLE IN THOSE CASES WHERE WE CAN HELP AND MAKE A DIFFERENCE THROUGH FASTER ACCESS TO PHYSIOTHERAPY.MS JENNIFER LIAW, SENIOR PRINCIPAL PHYSIOTHERAPIST, SGH
The A&E physiotherapist manages patients found to have no serious injury after initial investigations to determine the nature of their emergency.
These are patients with minor ortho-paedic problems such as back, neck and-knee pain, and don’t need surgery or to be seen immediately by an orthopae-dic specialist; the elderly with a fracture or other complications following a fall; and those with vertigo, especially benign paroxysmal positional vertigo (sudden sensation of spinning). The last group is seen together with the otolaryngol-ogy team that deals with ear, nose and throat conditions.
Patients who need further attention are given appointments to be seen at the Physiotherapy Department within a week – unlike before when the pro-cess could take months. While waiting for his appointment, a patient might suffer
After a physiotherapist was stationed at the A&E, the number of emergency referrals for physiotherapy increased by more than a third to 2,472 in 2014 from 1,836 in 2013. Most of these referrals – 54 per cent – were for patients with back pain.
another fall, requiring another visit to the A&E, said Ms Jennifer Liaw, Senior Principal Physiotherapist, SGH.
“We can’t eliminate all readmis-sions, but we play a role in those cases where we can help and make a differ-ence through faster access to physio-therapy,” said Ms Liaw, the coordinator of the multi-disciplinary Early and Direct to Physiotherapy (ED-PT) project. The team included Professor Celia Tan, Group Director, Allied Health, SingHealth, and Associate Professor Mark Leong, Senior Consultant, Department of Emergency Medicine, SGH.
After a physiotherapist was stationed at the A&E, the number of emergency referrals for physiotherapy increased by more than a third to 2,472 in 2014 from 1,836 in 2013. Most of these referrals – 54 per cent – were for patients with back pain. Patients requiring further investiga-tion at the A&E’s Emergency Observation Ward and were seen by a physiotherapist also increased, to 816 in 2014 from 303 in 2013. Again, the majority of these cases were those with back pain (70 per cent). More than four-fifths of the Observation Ward patients seen by a physiotherapist were discharged, with just 17 per cent admitted to hospital ultimately.
Only experienced physiotherapists with at least five years on the job are scheduled for the service, as “the patients that we see in A&E are likely to be in acute pain, while geriatric and vestibular prob-lems can be quite complex”, said Ms Liaw.
“We want to ensure that we provide spe-cialist care, the higher level of care, to this group of patients,” she added.
Currently, an A&E physiotherapist sees between four and 14 cases a day. Because the person at the A&E must be able to manage a spectrum of conditions, the ED-PT team had to undergo training from their colleagues in other specialities to ensure they are up-to-date in areas such as geriatrics, and neurological and vestibular rehabilitation.
The ED-PT project won the Ground- breaking, Effective and Momentous (GEM) Award at the SingHealth Allied Health Innovative Practice Awards 2015, a rec-ognition of the team’s positive impact as reflected by increased referrals from doctors, said Ms Liaw.
Physiotherapists involved in the multi-disciplinary A&E project have to undergo training from their colleagues in other specialities to ensure they are up-to-date in areas such as geriatrics, and neurological and vestibular rehabilitation, said project coordinator Ms Jennifer Liaw (seated, fifth from left).
The project doesn’t stop there. The team is looking at whether nurses can play a role in helping patients with minor pain so that they can be discharged when a physiotherapist isn’t on duty in the evening. Another plan is to study which groups of patients with lower back pain
– comprising a good percentage of A&E patients – may benefit from early phys-iotherapy, and if early interventions by physiotherapists will help to reduce read-mission to the A&E and follow-up atten-dances at the orthopaedic specialist clinic.

08 NEWS SINGAPORE HEALTH MAY– JUN 2016
Less light, more sleep
A team of nurses have come up with an innovative idea to help patients get more sleep at night.
WHEN NURSES FROM THE National Heart Centre Singa-pore (NHCS) discovered that
two-thirds of their warded patients were not getting enough sleep at night, they decided to look into the matter.
Their sur vey of 50 patient s revealed that the main disturbances were noise and glare from lights at night. About 70 per cent of those who took part cited these as the main rea-sons they did not get uninterrupted sleep while in hospital.
The survey revealed that the dis-turbances took place when nurses came into the wards to carry out pro-cedures such as taking blood sam-ples (twice a night), doing electrocar-diograms (to measure heart activity), turning immobile patients, and check-ing blood glucose levels.
The noise and glare coming through the curtains would keep patients in adjacent beds awake. Added to this were the unfamiliar hos-pital setting and anxiety over upcom-ing medical procedures that some patients experienced.
“We found that patients in adja-cent beds were affected by the light coming through the curtains, but it is impossible for nurses to work under dimmer lighting condi-tions as that will compromise patient safety,” said Ms Wu Wing Yin, Nurse Clinician, Coronar y Care Unit,
NHCS, and the team leader behind this project.
To resolve the issue, the nurses came up with the innovative idea of attaching a battery-powered, flexi-ble, portable torchlight to the “Com-puter on Wheels” – a laptop mounted on a wheeled platform (pictured). It is standard protocol for nurses to push a Computer on Wheels along whenever they take blood samples from patients.
At just three watts, the low inten-sity torch is bright enough to allow nurses to safely take blood samples from patients at night without dis-turbing other patients nearby. The team also worked with in-house engi-neers to enhance the torch so that it has a USB connection, and can run on batteries instead of being attached by a wire.
The nurses also introduced changes to the night shift nursing routine. Instead of doing individual checks and procedures, screenings are streamlined to allow two nurses to do two check-ups at the same time. This gives patients longer periods of uninterrupted sleep, which helps in their recovery.
After implementing these mea-sures and with noise and glare sig-nificantly reduced, another survey showed that 79 per cent of patients now have sufficient sleep at night, compared to 30 per cent previously.
PHO
TO: J
UST
IN L
OH

NEWS 09MAY– JUN 2016 SINGAPORE HEALTH
HIS KIDNEY DISEASE had reached the stage where he had to undergo dialysis. Yet, Mr Lai Saik Ling was
reluctant to agree to the treatment. A lorry driver till about 20 years ago, the single, elderly man had little savings and was afraid he wouldn’t be able to pay for dialysis.
“His doctor told him that he had to do it, or he would die. But he refused because he felt that it was too expen-sive,” said his sister, Mdm Lai Feng Jiao, 64, in Mandarin.
Someone who needs haemodialy-sis – which involves diverting blood into a machine to be filtered before it is returned to the body – must undergo the procedure several times a week. At a private haemodialysis centre, Mr Lai can expect to pay an average of $200 per dial-ysis session. The 78-year-old is required to undergo three sessions of haemodial-ysis per week.
When his doctors at Singapore General Hospital (SGH) found out the reason for his reluctance, they referred him to the hospital’s Medical Social Services. Mr Clinton Shi, Medical Social Worker, SGH, helped him to apply to a VWO (voluntary welfare organisation) for subsidised haemodialysis, as well as to the hospital’s Needy Patients Fund for help to pay for dialysis at a private centre in the meantime.
“Generally, VWOs have long waiting
A bridge of hope When a little help is needed when a chronic or terminal illness strikes, the Needy Patients Fund can offer patients short-term funding for treatment, equipment and medications. By Desmond Ng
lists, so patients may have to wait three to six months before they are placed at one of their haemodialysis centres for subsidised treatment,” said Mr Shi. “During the interim period, patients like Mr Lai have to undergo dialysis at private centres.”
To tide Mr Lai over this period, Mr Shi was able to get the Needy Patients Fund to pay for his dialysis for the first two months, and another charitable fund for the remaining months.
“The SGH Needy Patients Fund pro-vides short-term financial assistance for patients who have been assessed to be financially needy,” said Mr Shi.
With dialysis, Mr Lai’s quality of life has improved significantly. He no longer feels the terrible tiredness and breathlessness from carrying a lot of fluid and waste in his system. Each time Mr Lai completes dialysis, he feels able to breathe properly again.
Being able to enjoy simple yet mean-ingful activities like doing volunteer work, singing in a Cantonese clan associ-ation music group, or just spending time with his siblings has given Mr Lai a new lease of life, said his sister.
“We don’t have to worry about money too much now. We also have our own families to take care of,” said Mdm Lai, adding that her brother and their family are very thankful for the financial aid to help him start dialysis.
PHO
TO: A
LVIN
N L
IM
Just as the plight of mothers and their sick children sleeping on the floors of overcrowded wards at the Singapore General Hospital (SGH) moved the late Mr Navroji Mistri to donate to the hos-pital in the 1950s, so did a talk about needy patients strike a similar chord with his nephew, Mr Noshir H Mistri.
The presentation to Rotary Club of Singapore members on how the SGH Needy Patients Fund is able to help many low-income families moved Mr Noshir Mistri so much that he decided to donate to the fund more regularly.
“After we attended the talk, we decided to give from time to time. We have donated for the past two years,” said Mr Mistri.
“The decision was also influ-enced by my uncle. My family has always been involved in social and charity work.”
Some SGH Needy Patients Fund recipients include sole breadwinners who support young children and elderly family members on a low income.
Mr Mistri’s uncle was a well-known Indian entrepreneur and philanthro-pist who donated $950,000 in 1953 – a huge amount in those days – to build Singapore’s first paediatrics ward, known as the Mistri Wing, in 1955. The building now houses SGH’s Diabetes and Metabolism Centre.
He was best known for his soda drinks business in Singapore and Mistri Road, near Shenton Way, which was named in his honour.
The couple is continuing the legacy of their late uncle who died of diabetes in late 1953. Mr Mistri said: “I have toured the Mistri Wing and I felt very proud to be associated with it.”
Mr Clinton Shi tapped on the SGH Needy Patients Fund to help pay for Mr Lai Saik Ling’s haemodialysis at a private centre while the latter’s application for subsidised treatment was being processed.
By contributing to the SGH Needy Patients Fund, Mr and Mrs Noshir H Mistri are continuing their late uncle’s philanthrophic legacy. The late Mr Navroji Mistri gave a substantial sum of money to build Singapore’s first paediatrics ward, known as the Mistri Wing, in 1955.
Bringing sunshine into the lives of the needy
• For more information about the SGH Needy Patients Fund, go to
www.sgh.com.sg/subsites/ fundraising/Pages/HomePage.aspx• Donations can be made online through
the website, by mailing a completed donation form (downloaded from the website), cheque or credit card details to
Singapore General Hospital c/o Development Office 167 Jalan Bukit Merah Tower 5, #03-11 Singapore 150167

10 NEWS SINGAPORE HEALTH MAY– JUN 2016
Screen to be safe Screening all pregnant women for gestational diabetes mellitus means early treatment, which reduces the risk to mother and child. By Desmond Ng
SINCE THE BEGINNING OF THIS YEAR, KK Women’s and Children’s Hospital (KKH) and Singapore
General Hospital have been offering routine screening for gestational diabe-tes mellitus for all its pregnant patients at 24 to 28 weeks, as part of a six-month pilot project.
The women are screened with an oral glucose tolerance test (OGTT) using a fla-voured sweet drink. Two blood samples are taken, one before they drink it and one after. The samples are then tested for the level of glucose in their blood.
The screening, while routine, is not mandatory and is aimed at earlier detec-tion and intervention.
Gestational diabetes mellitus is a condition in which the body does not produce enough of the hormone insulin to control sugar levels during pregnancy. This puts both mother and child at risk.
The baby can have excessive weight gain, get hypoglycaemia after birth, develop fetal abnormalities, and even succumb to sudden fetal death. The mother can get high blood pressure and eclampsia while pregnant, give birth pre-maturely and run the risk of getting Type 2 diabetes in the future.
WITH INCREASING GESTATION, BLOOD SUGAR LEVELS MAY RISE. IN MOST CASES, THE CONDITION DISAPPEARS AFTER DELIVERY, BUT IN SOME WOMEN, IT MAY PERSIST AND THEY WILL NEED LONG-TERM FOLLOW-UP AND TREATMENT. PROFESSOR TAN KOK HIAN, SENIOR CONSULTANT AND HEAD, PERINATAL AUDIT AND EPIDEMIOLOGY UNIT, DIVISION OF OBSTETRICS AND GYNAECOLOGY, KKH
The test was offered at KKH after the hospital and Duke-NUS Medical School did a study comparing the benefits of the routine oral glucose tolerance test with targeted screening or no screening at all.
The researchers found that preg-nant women benefit most from routine screening with the OGTT. It allows for timely intervention and brings about health benefits that far outweigh the cost. It is a more cost effective approach to reduce complications of the condi-tion in Singapore, compared to targeted screening or no screening.
According to Professor Tan Kok Hian, Senior Consultant and Head, Perinatal Audit and Epidemiology Unit, Division of Obstetrics and Gynaecology, KKH, who led the study, a previous local study had shown that the previous practice of tar-geted screening (screening only high risk cases) failed to identify more than 25 per cent of mothers with gestational diabetes. Previously, only pregnant women over 35 years old, or those with a high body mass index, or those who have relatives with diabetes, were screened for this condition.
He said that even if there is no family history of diabetes, a pregnant woman can develop gestational diabetes mel-
litus. “With increasing gestation, blood sugar levels may rise. In most cases, the condition disappears after delivery, but in some women, it may persist and they will need long-term follow-up and treat-ment.”
Prof Tan said screening is the most effective way to avoid under-diagnosing the condition, and to detect and manage it early. Pregnant women with the con-dition show no symptoms, although some may experience increased thirst, urination, appetite, and fatigue. Their raised blood sugar levels are likely to be discovered during a routine antenatal check-up with an OGTT.
Why some develop the condition is unclear although one local study found that Asians were more at risk of it than Caucasians. In Singapore, KKH sees about 12,000 births a year on average, and about 15 per cent of those pregnant women develop the condition.
Prof Tan said the condition is respon-sible for about 5 per cent of stillbirths in KKH. Such cases usually involve preg-nant women with diabetes who were initially not seen at KKH and only went to the hospital later for delivery. Others were detected late because they either went to KKH in late pregnancy, or missed follow-ups and necessary medical inter-ventions. Treatment includes dietary counselling or insulin treatment, depend-ing on the severity of the condition.
PHO
TO: A
LVIN
N L
IM /
123R
F
Professor Tan Kok Hian said screening is the most effective way to avoid under-diagnosing gestational diabetes mellitus, and to detect and manage it early. Pregnant women are screened with an oral glucose tolerance test using a flavoured sweet drink as shown here.

11UPCLOSEMAY– JUN 2016 SINGAPORE HEALTH
TEXT BY LOW SHI PING Source: www.hsa.gov.sg, www.redcross.sg
ILLU
STRA
TIO
NS:
123
RF
BLOOD TIES
Mark World Blood Donor Day on June 14 by donating blood to save
lives. With an ageing population, Singapore will see an increasing
need for blood.
General Surgery
54%
WHAT THE BLOOD WAS
USED FOR (2015)
General Medicine
31%
Haematology
9%
Accident & Emergency
6%
HOW TO DONATE• Donate at the blood
banks at places such as Health Sciences Authority, Woodlands, Dhoby Ghaut or Westgate Tower. For more details, visit www.redcross.sg.
• The donation process involves 6 simple steps over 45 minutes.
• During a donation, a unit of 350-450ml of blood is drawn. The donated blood volume will be replaced in just 3 days.
DEMAND • 112,713 units: Amount
of whole blood donations in 2015, which fell short of needs.
• 3-5%: The rate at which the demand for blood has been increasing annually in Singapore.
• 220,000 units per year: By 2030, the demand for blood is expected to double. (On average, 1 unit can help 3 people.)
120,000units of blood are needed in Singapore every year
BLOOD NEEDED• The Singapore Red
Cross and Health Sciences Authority want young people to become lifelong donors.
• The number of young donors has increased by 27%, from 16,091 in 2001 to 20,452 in 2014, since the National Blood Programme was set up in 2001.
40% regular donors
28% first-timers
28% young people
DONOR DETAILS71,277 people donated blood in 2015, representating 1.8% of Singapore’s population
male62%
female38%

Nursing, to Ms Dezarae Ang, doesn’t really feel like a job because she deals with people and every day is different.
SINGAPORE HEALTH MAY– JUN 201612 PEOPLE
SHE DIDN’T WANT a run-of-the-mill job writing repor t s and the like, but one where she
could interact with people, and which offered her challenges and meaning in life. She had been going on medical- related missions to countries like Cambodia since her early teens, so when it was time to decide after junior college, it was nursing hands down.
“I have always wanted to do some-thing related to health care. Nursing to me doesn’t really feel like a job because you deal with people and every day is different. I don’t think I could work in a nine-to-five office job. I would feel quite bored,” said Ms Dezarae Ang, Staff Nurse, Singapore General Hospital (SGH).
Ms Ang received her nursing degree in Melbourne, and since graduation, has been working at SGH’s Ward 48 for cancer patients. Again, it was her search for challenges that led her to become an oncology nurse.
“I didn’t have a specific reason for choosing oncology. I think I just wanted a more challenging environment, one where I could really talk to the patients. A lot of them are quite sick, so it’s import-ant to know how to respond to critical sit-uations. I thought it would be meaningful in a sense,” she said.
While many of the ward’s patients do well after treatment, some don’t.
Seeking a connection
HER PASSING LEFT A DEEP IMPRESSION ON ME BECAUSE I SAW THE FRAGILITY OF LIFE. IT REMINDED ME TO TREASURE THE IMPORTANT THINGS IN MY LIFE, AND PEOPLE WHO MATTER.MS DEZARAE ANG, STAFF NURSE, SGH
“Her passing left a deep impression on me because I saw the fragility of life. It reminded me to treasure the important things in my life, and people who matter,” said Ms Ang, who was only able to get over the patient’s death after attend-ing her wake. Generally, though, Ms Ang copes well with death. “I realise there are things I cannot change and I have to accept them,” she said.
Being a friend to her patients is important for her. “If you don’t establish a connection, the relationship you have with the patient is a very professional one – I give you medicine, and you take it. Talking to them about their families makes a difference to me, and I think to the patients as well. They feel more com-fortable and (perhaps that helps them respond better to treatment),” she said.
Their conditions can deteriorate very rapidly. “That came as a bit of a shock to me because at that time, I was still new to nursing. I think the hardest part is when sometimes, the patients treat you like family,” Ms Ang said.
The death of one patient hit her a little harder than others. “I had the privilege of caring for her from the start of her admis-sion until her eventual demise. When she first came in, she was very mobile and we spoke a fair bit about her life and her family,” said Ms Ang.
As a relative newbie, the 24-year-old’s priority is to settle into her job before furthering her career. She wants to take an advanced diploma in oncology as it would let her work more independently, doing things like giving chemotherapy and taking blood cultures, which are only done by doctors and resident nurses. It would also give her a chance at a management role, but she hopes to be a resident nurse to contribute to other areas of clinical care.
PHO
TO: A
LVIN
N L
IM
Ms Dezarae Ang thinks it is important for her to have a relationship with her patients, even if it’s for a brief moment. By Sol E Solomon

A S A YOUNG DOCTOR, Dr Bok Chek Wai worked with a senior r e h a b i l i t a t i o n m e d i c i n e
specialist who would become his mentor and inspiration to enter the field.
Today, Dr Bok hopes he too can spark a similar desire among his juniors to enter the field.
Noting that rehab medicine is a speciality that is little known, he wants to get the message out that it is
“an important part of the whole med-ical spectrum”, said Dr Bok, Senior Consultant and Head, Department of Rehabilitation Medicine, Singapore General Hospital (SGH). And in view of Singapore’s ageing population and a
PEOPLE 13MAY– JUN 2016 SINGAPORE HEALTH
corresponding rise in chronic diseases, rehab medicine will play an “increasingly important” role in health care, he added.
Rehab medicine deals very much with how a patient’s daily functions, strength and mobility are affected after suffering a debilitating disease such as stroke or an accident. Rehab medicine specialists try to get patients back on their feet and into society at large.
Seeing his patients recover well and being happy makes him feel good about going to work every day – “it sounds very cliched but it’s true” – but he also recognises that rehab med isn’t a bed of roses.
“Trying to help patients and their families figure out the best way forward,
getting to grips with their illness and how to cope can be stressful for both patients and health care professionals. Sometimes, they direct their anger (over the situation) at us,” Dr Bok said.
“We have to face such situations and deal with them. We understand that they’ve just had a very severe illness and are trying to cope with it.”
Doctors must offer hope to patients and their families, but they also have to provide “a healthy dose of reality”. “It won’t help patients if you are just a cheer-
Helping patients back on their feet
Rehabilitation is key to getting those who are left with physical impairments or disabilities following severe illness back on their feet and into society. By Sol E Solomon
Doctors should not just offer hope to patients and their families, they must also temper that hope with a dose of reality, says Dr Bok Chek Wai.
leader, saying yes, yes, you can do better, everything is good, without telling them what they should expect, what they can and cannot do,” he said.
He tries to emulate his mentor, Associate Professor Peter Lim, a senior consultant and member of his team.
“When I accompanied him on ward rounds as a young trainee, I saw the way he treated patients and their family mem-bers,” said Dr Bok. Prof Lim was always kind and thoughtful towards patients and staff alike, offering help in a quiet, humble manner, he added.
Dr Bok is also Programme Director for SingHealth’s S enior Resident Rehabilitation Programme, teaches at the NUS Yong Loo Lin School of Medicine and Duke-NUS Medical School, and sits on planning committees for the future Sengkang Hospital and SGH’s Outram Community Hospital.
Despite his busy schedule, he still finds time a couple of times a week to run for fun and to relax.
A friendly man with a self-deprecating sense of humour, Dr Bok enjoys playing video games and cooking – albeit for him-self for now.
“I tell my friends my cooking isn’t ready for prime time yet!” he said.
PHO
TO: A
LVIN
N L
IM
C
M
Y
CM
MY
CY
CMY
K

Q: What additional benefits does MediShield Life offer compared with MediShield?
MediShield Life provides basic health insurance coverage for subsidised treatment in public hospitals for all Singaporeans and permanent residents, regardless of age or pre-existing medical conditions.
Before, coverage ended at age 92 years but MediShield Life covers for life. Policyholders previously also could not claim for certain conditions they were already suffering from or were at risk of when they first signed up. These included heart disease, cancer and organ failure. But this is no longer true as MediShield Life provides protection for all, including those with serious medical conditions.
In addition, because of higher claim limits and lower co-insurance rates, MediShield Life payouts are higher than under MediShield. So, patients on MediShield Life pay less Medisave and/or cash.
Q: Does MediShield Life cover all medical conditions and treatments?
MediShield Life covers all medical condi-tions but it is designed as a basic health
14 MONEY SINGAPORE HEALTH MAY– JUN 2016
Is MediShield Life a better deal?MediShield Life, which replaces MediShield, offers several enhancements over the latter. What exactly are those benefits? By Thava Rani
insurance plan to help with large inpa-tient costs. That is why some procedures like cosmetic surgery, treatment for drug addiction or alcoholism, vaccinations and overseas medical treatment are excluded from coverage. MediShield sim-ilarly had exclusions.
However, unlike MediShield, all pre-existing medical conditions are covered under MediShield Life. Those with less serious or well-managed pre- existing conditions, such as well- controlled diabetes, or hypertension with no complications, osteoarthritis, pre-cancers, fibroids or cysts, will be unconditionally insured by MediShield Life. Similarly, those who are hospital-ised because of a one-off event such as an accident or dengue fever will also be covered.
Q: What about more serious conditions that were not cov-ered under MediShield?
In the case of more serious conditions such as cancer, kidney diseases, immune system disorders or illnesses requiring intensive medical treatment, or which have a high risk of complications requir-ing prolonged treatment, the patient will still be covered by MediShield Life.
They may, however, be asked to pay additional premiums.
Additional premiums are 30 per cent more than the standard rate and have to be paid over 10 years to reflect the higher risk. After this period, the patient will go back to paying the standard rate as the rest in their age group.
To f ind out which condit ions may require additional premiums, go to w w w.moh.gov.sg and click on
“MediShield Life” and select “Coverage for Pre-Existing Conditions” under “About MediShield Life”.
Q: Is there a dif ference between their claim limits?The amount that can be claimed
depends on the claim limit for each type of expense. While some claim limits, such as those for implants or kidney dialy-sis, remain the same, most claim limits are now higher under MediShield Life. For instance, the claim limit for daily ward charges in a normal ward is $700 per day versus the $450 per day under MediShield.
MediShield also imposed a maxi-mum claim limit of $70,000 per policy year and a lifetime limit of $300,000. With MediShield Life, patients can claim up to $100,000 per year and enjoy unlimited lifetime claims.
Q: Does MediShield Life also include features such as a deductible and co-insurance?
Yes. The deductible is a fixed amount that the patient pays before the MediShield Life payout kicks in. It sieves out small claims, which can be paid using Medisave and/or cash, and helps to keep premiums affordable. The deductible is payable only once a year through Medisave or cash.
The amount of the deductible has not changed under MediShield Life. For patients aged 80 and below, the deduct-ible is $1,500 for stays in subsidised C wards, and $2,000 if they choose to stay in B2 and higher wards. For those over 80 years old, the deductible is $2,000 (C wards) and $3,000 (B2 class and higher).
In addition to the deduc tible, the patient also pays a por tion of the claimable amount – or the
PHO
TO: 1
23RF
The second of a series on MediShield Life, adapted from the Ministry of Health website. For more information, go to www.moh.gov.sg/content/moh_web/medishield-life.html
co-insurance. The larger the bill, the lower the co-insurance rates.
The co-insurance rate ranged from 20‒10 per cent as the bill size increased under MediShield, but now ranges from 10‒3 per cent as the bill size increases under MediShield Life. This means patients will pay less co-insurance and MediShield Life will cover more.
Q: Are premiums higher given the many benefits? Are rebates or subsidies given?
While MediShield Life comes with higher premiums, policyholders will be eligible for rebates and subsidies of various kinds.
U n d e r b o t h M e d i S h i e l d a n d MediShield Life, Singapore residents pay more premiums while they are working, so that premiums rise less steeply in old age. The additional amounts paid during working age are set aside in a pool in the MediShield Life Fund, which individuals and others in the same generation can tap on to receive premium rebates when they are older.
Premium rebates are given to every-one from age 66 for those born in or after 1950, and from age 71 if born before 1950, provided they took up the scheme within the eligible entry age band. The rebate amount increases every few years until age 90, after which no more premium payments are required.
To phase in the impact of the pre-mium increases, all Singaporeans will receive a transitional subsidy for the first four years of MediShield Life. Addi-tionally, subsidies of up to 50 per cent of premiums are given to lower- and mid-dle-income Singapore residents, with permanent residents receiving half the applicable rate for citizens.
The Pioneer Generation also receives subsidies and Medisave top-ups ranging from 40‒60 per cent and up to $800 a year respectively, which will mean lower MediShield Life premiums than before.
$
The Pioneer Generation receives subsidies and Medisave top-ups ranging from 40-60 per cent and up to $800 a year respectively, which will mean lower MediShield Life premiums than before.

15MAY– JUN 2016 SINGAPORE HEALTH
VENETRIMThe Ultimate
LEG LOVE CREAM
WITNESS THE MAGIC
Also great for:
Soothe Tired LegsReduce Varicose Veins &
Plaza Singapura
Available at:
www.thehealthyeverythingstore.comwww.audreychristian.com
Online:
As Seen in:
Before & after sports
Review For Varicose Veins Review For Tired Legs
A day on your feet or sitting long hours
Travelling
Adv_Venetrim.indd 1 12/4/16 12:01 pm
HEALTH XCHANGE Our experts answer all your questions about health
16 SINGAPORE HEALTH MAY– JUN 2016
Is my son too chubby?
I often have hiccups. What causes it? And will drinking water or holding my breath make it go away?A hiccup is a sudden, repetitive and involuntary contraction of the diaphragm. A sudden and strong contraction of this breathing muscle rapidly sucks in air, which closes the voice box, creating
Make my hiccups go away
Dealing with hypoglycaemiaI am diabetic and recently experienced dizziness, which my doctor said was due to hypoglycaemia. What causes it and what should I do if it happens again?If you have diabetes, you don’t just have to watch out for high blood sugar. You must look out for low blood sugar as well. Diabetes develops when there is too much sugar (glucose) in the blood: the blood sugar level drops below 70 mg/dl (milligrams per decilitre) or 4 mmol/L (millimoles per litre) because the body doesn’t produce enough insulin or can’t use insulin properly.
Insulin converts carbohydrates into energy. Excess insulin relative to carbohydrate intake can lead to low blood sugar or hypoglycaemia, which is a potential medical emergency,
as it can lead to a seizure, loss of consciousness and even death. Blood sugar levels can fall suddenly because of diet, exercise and diabetic medication. If you experience low blood sugar symptoms such as dizziness, blurred vision, shaking or trembling, hunger, muscle weakness and confusion, stop any physical activity immediately. Check your blood sugar level to confirm that it is low. Even if you are unable to check, it is reasonable to assume that you are hypoglycaemic when you have those symptoms. You should quickly take a sweet food or beverage, or over-the-counter glucose tablets to raise your blood sugar level. Do not take your diabetes medication until your blood sugar level is normal.
Check your blood sugar level 15 to 20 minutes after eating to make sure it is back to normal. Eat or drink something sweet again if the first snack or drink does not bring it up sufficiently. You can resume your regular activities if you no longer have low blood sugar. Carry sweets, fruit juice or glucose tablets with you at all times, in case of hypoglycaemia.
If you experience hypoglycaemia repeatedly, promptly consult your doctor for a review of your diet, lifestyle and medication. People with diabetes should always carry some form of diabetes identification in case of an emergency.
Dr Teh Ming MingConsultantDepartment of EndocrinologySingapore General Hospital
Please visit our website to see the topics for discussion in May-Jun 2016.These articles are from www.healthxchange.com.sg,
Singapore’s first interactive health and lifestyle portal.
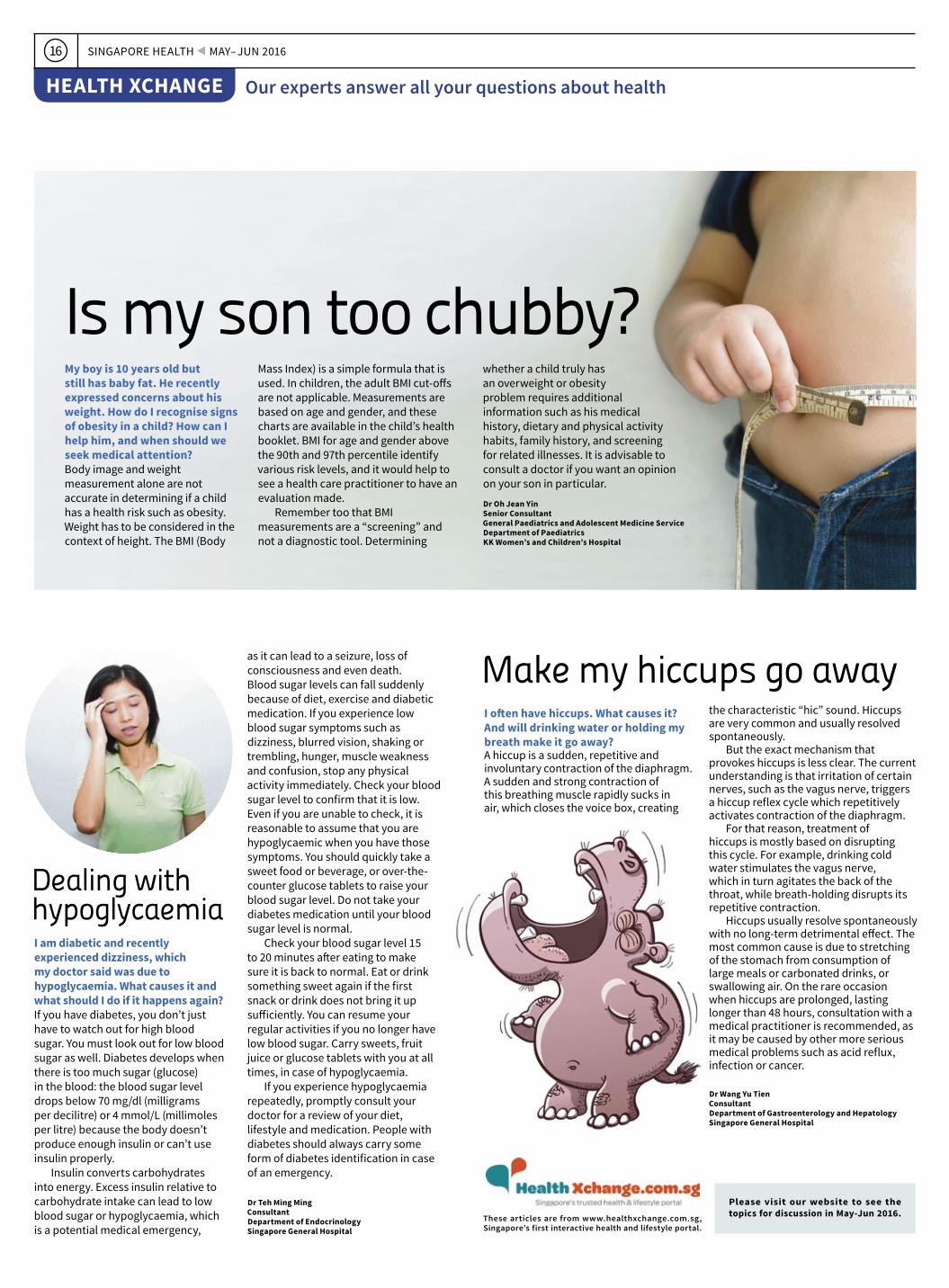
My boy is 10 years old but still has baby fat. He recently expressed concerns about his weight. How do I recognise signs of obesity in a child? How can I help him, and when should we seek medical attention?Body image and weight measurement alone are not accurate in determining if a child has a health risk such as obesity. Weight has to be considered in the context of height. The BMI (Body
the characteristic “hic” sound. Hiccups are very common and usually resolved spontaneously.
But the exact mechanism that provokes hiccups is less clear. The current understanding is that irritation of certain nerves, such as the vagus nerve, triggers a hiccup reflex cycle which repetitively activates contraction of the diaphragm.
For that reason, treatment of hiccups is mostly based on disrupting this cycle. For example, drinking cold water stimulates the vagus nerve, which in turn agitates the back of the throat, while breath-holding disrupts its repetitive contraction.
Hiccups usually resolve spontaneously with no long-term detrimental effect. The most common cause is due to stretching of the stomach from consumption of large meals or carbonated drinks, or swallowing air. On the rare occasion when hiccups are prolonged, lasting longer than 48 hours, consultation with a medical practitioner is recommended, as it may be caused by other more serious medical problems such as acid reflux, infection or cancer.
Dr Wang Yu TienConsultantDepartment of Gastroenterology and HepatologySingapore General Hospital
Mass Index) is a simple formula that is used. In children, the adult BMI cut-offs are not applicable. Measurements are based on age and gender, and these charts are available in the child’s health booklet. BMI for age and gender above the 90th and 97th percentile identify various risk levels, and it would help to see a health care practitioner to have an evaluation made.
Remember too that BMI measurements are a “screening” and not a diagnostic tool. Determining
whether a child truly has an overweight or obesity problem requires additional information such as his medical history, dietary and physical activity habits, family history, and screening for related illnesses. It is advisable to consult a doctor if you want an opinion on your son in particular.
Dr Oh Jean YinSenior ConsultantGeneral Paediatrics and Adolescent Medicine ServiceDepartment of Paediatrics KK Women’s and Children’s Hospital

17MAY– JUN 2016 SINGAPORE HEALTH
Does the doctor have the final say when acting in the best interest of the patient regarding Advance Care Planning (ACP), Advance Medical Directive (AMD) or Lasting Power of Attorney (LPA)? Is it all right for a doctor to go ahead with medical intervention when the patient’s ACP states that he does not want it? And vice versa
– what if the patient wants full treatment, but the doctor recommends no intervention?Before answering this question, it is important for readers to understand that ACP, AMD and LPA only operate once the patient loses the capacity to make specific decisions when they need to be made. If the capacity to make these decisions is still there, the health care team will continue to communicate with the patient.
If someone has made an AMD under the Advance Medical Directive Act, the doctor must carry it out if the conditions are met. These conditions are that the patient is terminally ill; three doctors have certified this; and the patient faces imminent death, and extraordinary life-sustaining treatment would only prolong the dying process. The doctor cannot “override” such a directive.
The doctor would normally have to respect the patient’s decision in an ACP. Once the patient loses the capacity to make his own serious medical
decisions, the doctor would only override the patient’s wishes if there are very good reasons for doing so. For example, if there is a new proven treatment that can now cure a patient, when there wasn’t one at the time the patient made the ACP, then the doctor may conclude that it is in the patient’s best interests to give the patient the drug.
Under an LPA, an appointed personal welfare donee is authorised to make health care decisions not related to life-sustaining treatment or treatment to prevent a serious deterioration in the patient’s health. Therefore, the doctor, and not the donee, will make serious medical decisions on behalf of the patient.
However, the doctor must consider the patient’s past and present wishes (ACP); the views of his family members, loved ones and caregivers; and any other relevant information, including clinical indications, in making a decision that is in the patient’s best interests.
A patient can request for a treatment but cannot demand it. The doctor is not obliged to provide treatment that is not clinically indicated and not in the patient’s best interests.
Assistant Professor David Sim, Consultant, Department of Cardiology, Director, Heart Failure Programme, National Heart Centre Singapore & Ms Sumytra Menon, Senior Assistant Director, Centre for Biomedical Ethics, NUS YLL School of Medicine.
I found Acting in your capacity (on page 18 of the Jan-Feb 2016 issue) very useful, as the information can help us to prepare for any illness to come. Listing down our preferences formally can help our loved ones avoid having to make difficult health care decisions for us. Thank you for the article.Mr David J Pattiselanno
This letter wins a set of Plant Placenta with Vitamin C (2X60 tablets) worth $199.80,sponsored by VitaHealth Asia Pacific (S) Pte Ltd.
Article useful for preparation
ABOUT YOUR HEALTH EXPERIENCE AND WIN A PRIZE FOR BEST LETTER
Letters must include your full name, address and phone number. Singapore Health reserves the right to edit letters and not all letters will be published. Write to [email protected] or The Editor, Singapore Health, Singapore General Hospital, Communications Department, Outram Road, Singapore 169608, or talk to us on Facebook.
The winner will receive two bottles of Genacol Derma Caps (120 capsules each), worth $116, which are sponsored by Medica Solutions Pte Ltd. www.genacolderma.sg
Who has the final say?

SINGAPORE HEALTH MAY– JUN 201618 FYI
EVENT CALENDAR
Visit www.singhealth.com.sg/events or the websites of respective institutions for any changes, more information and other listings.
▲
Healthy Breastfed Baby Contest 2016 (Assessment day)DATE June 18, SaturdayTIME 9am-6pmVENUE KKH Training Centre, Level 1, Women’s Tower, KK Women’s and Children’s HospitalFEE $20 (KK Junior Club Member), $30 (non-KK Junior Club member)REGISTRATION Call 6394-1268 (Monday-Friday, 9.30am-5.30pm) for more information.
If you have been breastfeeding your baby, sign your child up for this contest to win attractive prizes. Each baby’s photo will be posted on the KK Women’s and Children’s Hospital Facebook page and the KK Juniors Club Facebook Group.
Cancerwise Workshop: Coping With Fear Of RecurrenceDATE May 14, SaturdayTIME 1.30-3.30pm (English), 1.30-2.45pm (Mandarin)VENUE Level 4, National Cancer Centre SingaporeFEE FreeREGISTRATION Call 6225-5655 (Monday-Friday, 8.30am-5.30pm)
Among the biggest fears that plague cancer survivors is that it will rear its head again. This workshop will provide tips and tools on how to manage those emotions, and prevent them from taking over your life.
▲
Understanding Diabetes And Its ControlDATE May 5, 12, 19, 26, WednesdayTIME 6.30-8.30pmVENUE DSS@Bedok, #01-1529, Blk 141 Bedok Reservoir RoadFEE $21 for 4 sessionsREGISTRATION Call 6842-3382 for more information.
Organised by the Diabetes Society of Singapore, this four-session self-care management workshop is conducted in Malay, and covers topics such as guidelines on how to look after yourself if you have diabetes, understanding medication and nutrition.
▲
Are You Ready For Heart-Smart Eating?DATE May 18, WednesdayTIME 2-3.15pmVENUE SHF-Life Insurance Association Heart Health Hub, 190 Middle Road, #04-34 FEE FreeREGISTRATION Call 6336 9337 for reservations.
Join nutritionist Lim Kiat from the Singapore Heart Foundation as he talks about how to reduce high blood lipids with the help of a sensible diet. He will also cover myths and facts about nutrition, and discuss ideal cholesterol levels.
▲
Include your name, age, gender, address and telephone number. Winners will be notified via phone or e-mail. Incomplete or multiple entries will not be considered.
E-MAIL [email protected] POST The Editor, Singapore Health, Singapore General Hospital, Communications Department, #13-01 Surbana One, Blk 168, Jalan Bukit Merah, Singapore 150168
Winners of Contest 39: Each will receive a tubeof Joint Health Optimal Micellar Glucosaminecream (with Chondroitin) worth $39.50,sponsored by Urah Transdermal Pte Ltd. Prizes must be claimed by June 1, 2016.1. Bun Swee Lay 2. Marie Chan Mei Yi3. Ismail Mohamed Ariff 4. Lim Siew Keow5. Victoria Reberia
CONTEST
Source: Time
A healthy heart may improve cognitive function, according to a study published in
the Journal of the American Heart Association. More than 1,000 men and women above
age 40 underwent brain tests to assess their memory and processing abilities, and
the speed at which they could perform a task. They were tested again six years later.
Researchers found that a healthy heart – markers include not smoking, maintaining a healthy weight, and keeping blood pressure
and cholesterol in check – was associated with better brain function and processing
abilities, and less decline in functions such as memory and focus.
PHO
TOS:
123
RF
Adults deprived of sleep tend to eat more and less healthily. These were the findings published in the journal Sleep by researchers from the University of
Chicago, Universite Libre de Bruxelles and the Medical College of Wisconsin. When allowed only 4½ hours
of sleep (per night) over four nights, test subjects showed greater concentrations of 2AG, a type of endocannabinoid that is linked to appetite
regulation. This seemed to make them hungry easily and to eat unhealthy snacks.
Sleep to prevent snacking
Source: CNN
Hearthelps head
50 shades of grey
Source: The Age
An international study led by University College London has identified a gene that is associated with greying. Called IRF4, the gene regulates melanin (the pigment responsible for the colour of hair, skin and eyes). Other factors, such as stress, can also ignite the process. Next steps in the research include developing a treatment to prevent or reverse greying.
A study published in Annals of Internal Medicine has shown that going cold turkey is the best way to give up smoking. Funded by the British Heart Foundation, it surveyed 700 volunteers in the UK who were told to quit either gradually or immediately. Those who quit decisively were 25 per cent more likely to abstain from smoking six months after. Factors that help to strengthen this resolve include picking a convenient date to quit, sticking to it, and seeing a general practitioner for professional support and advice.
Stub it out
Source: BBC
1. Name one possible cause of fatty liver disease.
2. Which story in this issue did you find the most informative?
Closing date: June 1, 2016Send in your answers and stand to win either a bottle of Kyäni Sunrise (worth $85.75) or Kyäni Sunset (worth $79.25). The products are sponsored by Kyäni Singapore Pte Ltd.
A common condition, pneumonia can turn deadly for the elderly and those with weakened immune systems. By Desmond Ng
Pneumonia is No. 2 killer
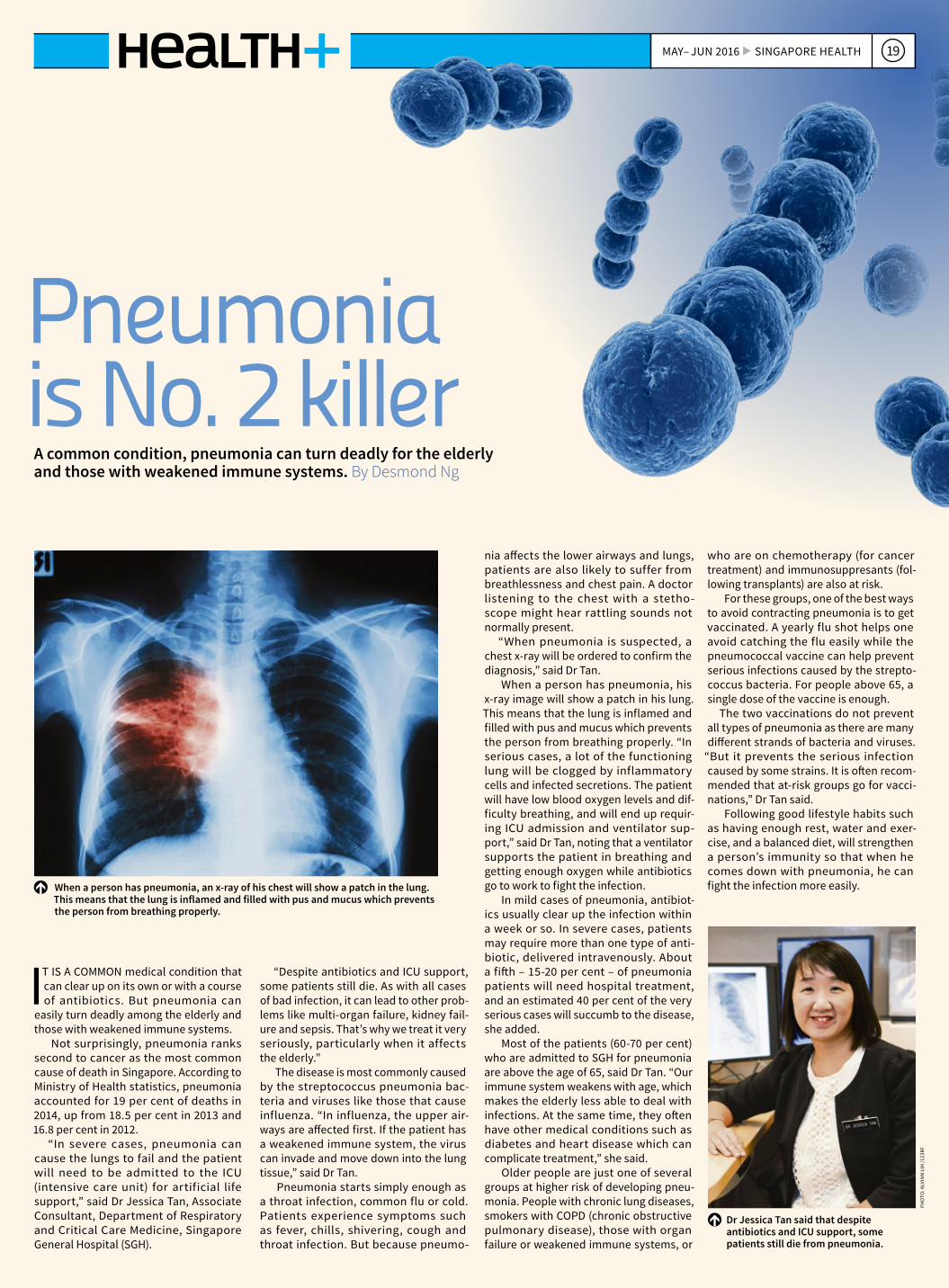
When a person has pneumonia, an x-ray of his chest will show a patch in the lung. This means that the lung is inflamed and filled with pus and mucus which prevents the person from breathing properly.
Dr Jessica Tan said that despite antibiotics and ICU support, some patients still die from pneumonia.
19MAY– JUN 2016 SINGAPORE HEALTH
I T IS A COMMON medical condition that can clear up on its own or with a course of antibiotics. But pneumonia can
easily turn deadly among the elderly and those with weakened immune systems.
Not surprisingly, pneumonia ranks second to cancer as the most common cause of death in Singapore. According to Ministry of Health statistics, pneumonia accounted for 19 per cent of deaths in 2014, up from 18.5 per cent in 2013 and 16.8 per cent in 2012.
“In severe cases, pneumonia can cause the lungs to fail and the patient will need to be admitted to the ICU (intensive care unit) for artificial life support,” said Dr Jessica Tan, Associate Consultant, Department of Respiratory and Critical Care Medicine, Singapore General Hospital (SGH).
“Despite antibiotics and ICU support, some patients still die. As with all cases of bad infection, it can lead to other prob-lems like multi-organ failure, kidney fail-ure and sepsis. That’s why we treat it very seriously, particularly when it affects the elderly.”
The disease is most commonly caused by the streptococcus pneumonia bac-teria and viruses like those that cause influenza. “In influenza, the upper air-ways are affected first. If the patient has a weakened immune system, the virus can invade and move down into the lung tissue,” said Dr Tan.
Pneumonia starts simply enough as a throat infection, common flu or cold. Patients experience symptoms such as fever, chills, shivering, cough and throat infection. But because pneumo-
nia affects the lower airways and lungs, patients are also likely to suffer from breathlessness and chest pain. A doctor listening to the chest with a stetho-scope might hear rattling sounds not normally present.
“When pneumonia is suspected, a chest x-ray will be ordered to confirm the diagnosis,” said Dr Tan.
When a person has pneumonia, his x-ray image will show a patch in his lung. This means that the lung is inflamed and filled with pus and mucus which prevents the person from breathing properly. “In serious cases, a lot of the functioning lung will be clogged by inflammatory cells and infected secretions. The patient will have low blood oxygen levels and dif-ficulty breathing, and will end up requir-ing ICU admission and ventilator sup-port,” said Dr Tan, noting that a ventilator supports the patient in breathing and getting enough oxygen while antibiotics go to work to fight the infection.
In mild cases of pneumonia, antibiot-ics usually clear up the infection within a week or so. In severe cases, patients may require more than one type of anti-biotic, delivered intravenously. About a fifth – 15-20 per cent – of pneumonia patients will need hospital treatment, and an estimated 40 per cent of the very serious cases will succumb to the disease, she added.
Most of the patients (60-70 per cent) who are admitted to SGH for pneumonia are above the age of 65, said Dr Tan. “Our immune system weakens with age, which makes the elderly less able to deal with infections. At the same time, they often have other medical conditions such as diabetes and heart disease which can complicate treatment,” she said.
Older people are just one of several groups at higher risk of developing pneu-monia. People with chronic lung diseases, smokers with COPD (chronic obstructive pulmonary disease), those with organ failure or weakened immune systems, or
who are on chemotherapy (for cancer treatment) and immunosuppresants (fol-lowing transplants) are also at risk.
For these groups, one of the best ways to avoid contracting pneumonia is to get vaccinated. A yearly flu shot helps one avoid catching the flu easily while the pneumococcal vaccine can help prevent serious infections caused by the strepto-coccus bacteria. For people above 65, a single dose of the vaccine is enough.
The two vaccinations do not prevent all types of pneumonia as there are many different strands of bacteria and viruses.
“But it prevents the serious infection caused by some strains. It is often recom-mended that at-risk groups go for vacci-nations,” Dr Tan said.
Following good lifestyle habits such as having enough rest, water and exer-cise, and a balanced diet, will strengthen a person’s immunity so that when he comes down with pneumonia, he can fight the infection more easily.
PHO
TO: A
LVIN
N L
IM /1
23RF
T HE BEGINNING OF OLD AGE – or even middle age – can bring on niggling problems like poor eye-
sight and creaky joints. Depending on the severity of those
problems, day-to-day living can be a her-culean effort. But according to occupa-tional therapists at Singapore General Hospital (SGH), there is a range of devices that people can use to make living with these problems less of an effort. Don’t die because of HIV
SINGAPORE HEALTH NOV– DEC 2015 24 SINGAPORE HEALTH MAY– JUN 2016 20
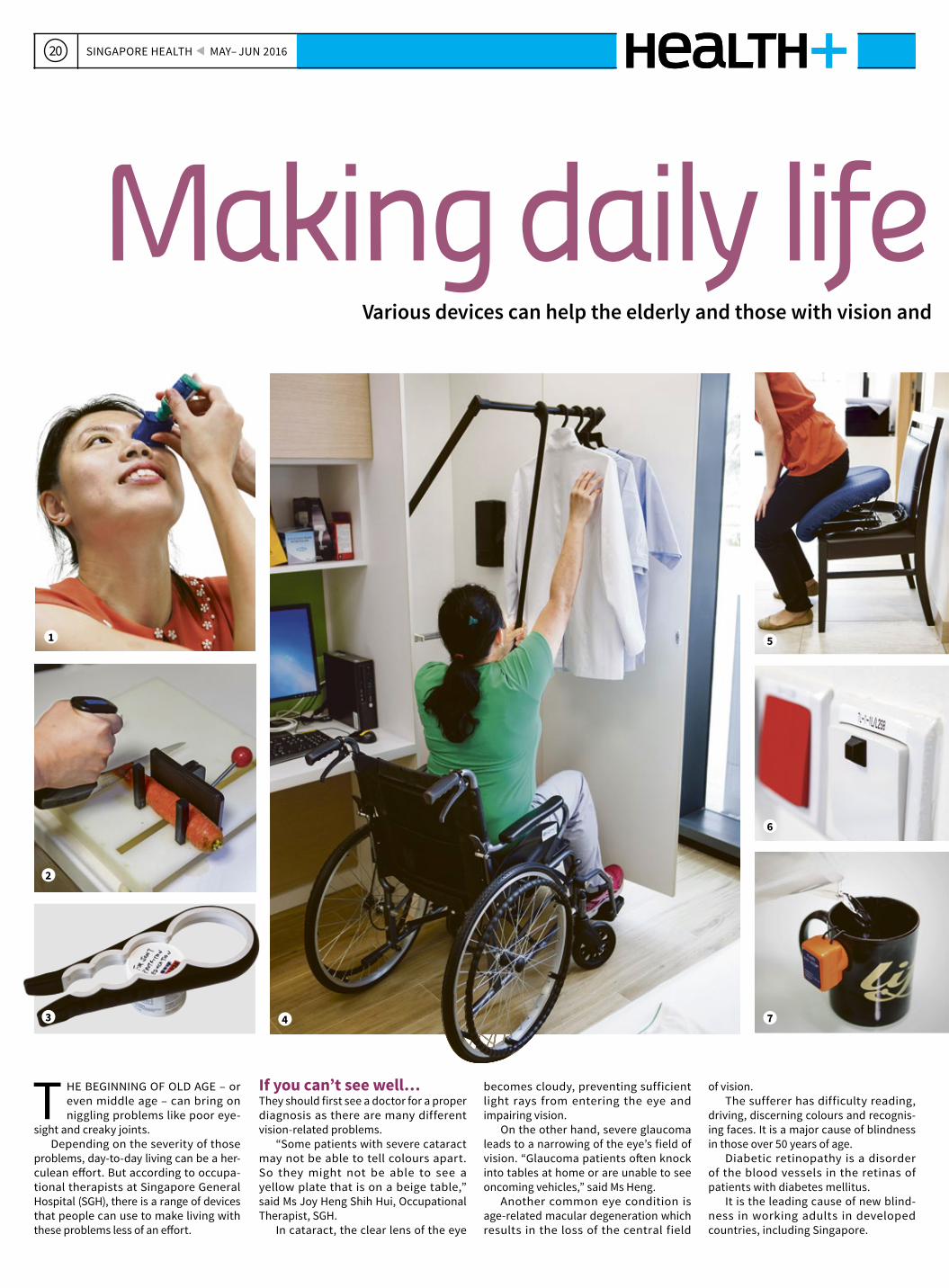
Making daily life more accessibleVarious devices can help the elderly and those with vision and other problems live safely and more easily at home. By Audrina Gan
If you can’t see well…They should first see a doctor for a proper diagnosis as there are many different vision-related problems.
“Some patients with severe cataract may not be able to tell colours apart. So they might not be able to see a yellow plate that is on a beige table,” said Ms Joy Heng Shih Hui, Occupational Therapist, SGH.
In cataract, the clear lens of the eye
becomes cloudy, preventing sufficient light rays from entering the eye and impairing vision.
On the other hand, severe glaucoma leads to a narrowing of the eye’s field of vision. “Glaucoma patients often knock into tables at home or are unable to see oncoming vehicles,” said Ms Heng.
Another common eye condition is age-related macular degeneration which results in the loss of the central field
of vision. The sufferer has difficulty reading,
driving, discerning colours and recognis-ing faces. It is a major cause of blindness in those over 50 years of age.
Diabetic retinopathy is a disorder of the blood vessels in the retinas of patients with diabetes mellitus.
It is the leading cause of new blind-ness in working adults in developed countries, including Singapore.
1
2
4
5
6
73

PHO
TOS:
ALV
INN
LIM
21MAY– JUN 2016 SINGAPORE HEALTH
Making daily life more accessibleVarious devices can help the elderly and those with vision and other problems live safely and more easily at home. By Audrina Gan
If you have stiff joints…Wear and tear, or some form of arthri-tis, can lead to stiff joints and pain, or more debilitating symptoms such as loss of flexibility. Opening bottles and jars, wringing towels, holding a knife, or carry-ing heavy objects becomes difficult.
Making basic changes around the house can help, said Ms Lin Yingying, Senior Occupational Therapist, SGH. For instance, using microfibre cloth or
thinner rags is easier on the hands when washing and wringing them out.
Devices to help open cans or bottles can be found at the household sections of department stores and even “two-dol-lar” shops.
Ms Lin has one piece of advice though. “When getting a home aid, the device should be easy to use. Get the shop assis-tant to show you how to use the device properly,” said Ms Lin.
If you can’t move about easily…The elderly and those with limited mobil-ity are prone to falls. Installing a bedrail can prevent them from falling out of bed, and also provide support when getting in and out of bed. For larger home devices, questions about what the equipment is to be used for, the amount of space it will take, its weight, portability, maintenance and installation should be considered before purchase.
10 11
8
9
1 Auto eye dropsThis device helps people with vision problems to accurately and easily dispense medicated and other eye drops.
2 Adapted cutting boardCutting and slicing is no longer a pain for people with arthritis or weak hand grip when vegetables, bread or other food is clamped onto this special cutting board.
3 Opening bottles, jars and cansThis multi-sized opener gives arthritic hands a stronger grip when twisting open bottle or jar caps. Not shown is a crochet hook-like device for lifting ring pulls of cans.
4 Lift/pull-down wardrobe railA pull-down wardrobe rail keeps clothes within easy reach of wheelchair users.
5 Assist seat cushionEssentially, this is a seat cushion with a hydraulic spring that helps those with weak leg muscles to get up easily from their seats.
6 Tactile markerPasting a tactile marker onto switches, door knobs and other objects helps the visually impaired locate things around the house easily.
7 Sounding an alertClipped onto a cup or glass, this device sounds an alert when it senses that liquid being poured in is near the top. Not shown are larger-than-normal numbers on calculators, clocks and thermometers, or those that read out the time and numbers can also help the visually impaired. 8 Teapot tipper
This device allows the lifting of heavy objects with little effort. Secure a teapot in the tipper, and the pot is then easily lifted for pouring.
9 MagnifierClipping a magnifier onto a medication bottle ensures the visually impaired take their medicines correctly. Other types of magnifiers help in reading the fine print in newspapers and books.
10 Palm peelerWearing a peeler around the finger won’t stress arthritic joints when peeling carrots and other vegetables. 11 Long-handled bath spongeAttaching a bath sponge to this long, curved handle will help those with stiff joints to scrub their backs.

SINGAPORE HEALTH MAY– JUN 201622
Stroke patients must get to the hospital as early as possible for effective treatment and a chance of a better recovery. A new treatment offers an alternative way to limit damage to the brain. By Suki Lor
When a stroke strikes
Associate Professor Deidre Anne De Silva describes the new endovascular treatment as a monumental and revolutionary development.
SINCE 1995, patients who get to the hospital within four and a half hours of a stroke can be considered for
treatment with a clot-busting drug (tPA or tissue plasminogen activator) given via an intravenous infusion. This gives them the best chance of recovery. Any later than four and a half hours from the onset of symptoms, and it becomes too risky to administer the drug.
Since last year, doctors have been able to offer patients a new minimally invasive treatment called endovascular treatment, which can be rendered in a slightly longer time window – six to eight hours after a stroke strikes.
The treatment involves restoring blood supply by mechanically pulling the clot that is blocking the blood vessel.
Doctors use a special device to stent the vessel, then pull the clot out, retriev-ing the stent at the end of the procedure.
Associate Professor Deidre Anne De Silva, Senior Consultant, Department of Neurology, National Neuroscience Institute, describes the new treatment as a monumental and revolutionary devel-opment. “For something like 20 years, we have not had any new treatment in acute stroke care. Endovascular treatment offers more patients the hope of reducing disability and improving the likelihood of independence following an ischaemic stroke, which is caused by a blockage in a blood vessel that stops blood flow and starves the brain of oxygen.”
Prof De Silva said strokes are common, can strike at any age, and have significant consequences. In Singapore,
9,000 new strokes occur each year. It is a leading cause of death and the No. 1 cause of adult disability, with six in 10 patients suffering long-term disabil-ity. Statistics show that 85 per cent of strokes are ischaemic and the rest due to primary bleeding in the brain.
Prof De Silva said that an additional one patient will be functionally inde-pendent for every three to five patients managed with this new endovascular treatment, compared to those who do not receive it. Endovascular treatment following clot-busting treatment also has greater benefits than treatment with the clot-busting agent alone.
Previously, endovascular treatment was used infrequently and could only be offered on a rescue basis to selected patients. But last year, several interna-tional randomised clinical trials revealed clear evidence for its benefit over stan-dard treatment.
“It is now a licensed, guideline-based therapy. So it is a routine practice, rather than given just on a ad-hoc rescue basis,” said Prof De Silva.
But it is still not for everyone. Six out of 10 people who get to a hospital in time are suitable either for endovascular treatment, the clot-busting drug, or both. After running scans and tests, doctors will decide whether patients are suitable for treatment and which would be best for each patient. Endovascular treatment may be given in cases when it is too late or not suitable for patients to get the clot-busting treatment, or it may also be given after the clot-busting treatment.
Move FASTTo recognise stroke symptoms remember the acronym FAST (Face, Arm, Speech and Time).
Call 995 for the emergency ambulance service operated by the Singapore Civil Defence Force to get the patient to the nearest hospital quickly. Paramedics will screen patients and notify hospitals if they suspect a stroke, so that medical teams can be ready for them.
Hurry to hospital A stroke is as much of an emer-gency as a heart attack, said Prof De Silva, who is also President of the Singapore National Stroke Association. “The earlier we can treat patients, the greater the benefit. With every minute that passes, more tissue goes from salvageable to dead.”
She said doctors who treat stroke patients use a tagline –
“time is brain” – to emphasise how important it is to get treatment in time. “So, it is alarming that only about 30 per cent of stroke
FACE Is the face drooping on one side?
ARM Can the person lift both arms?
SPEECH Does the speech sound slurred or strange?
TIMEIf you see any of the above signs, it is time to call 995 for an ambulance.
victims in Singapore get to the hos-pital in time to be even considered for acute treatment.”
She said about 20 per cent of people get strokes in their sleep, and while not much can be done to get them to hospital in time, many others can get there earlier. People must learn to recognise symptoms of stroke and come quickly to hos-pital via ambulance. “Even if these symptoms are resolved, it does not mean one need not call an ambu-lance, because they could be a har-binger of stroke.”
PHO
TOS:
ALV
INN
LIM
/123
RF/S
ING
APO
RE N
ATIO
NAL
STR
OKE
ASS
OCI
ATIO
N

Take heart
Taking care of the heart is vital if problems are to be avoided when older. By Jessica Leow
23MAY– JUN 2016 SINGAPORE HEALTH
Heart problems often plague the middle-aged and elderly, but this does not have to be the case.
Heeding the health of the heart – even in childhood – can mean less heartache in later years.
“Factors beyond our control include age, gender, and family history. But take heart – there are many factors we can control,” said Dr Lim Choon Pin, Consultant, Department of Cardiology, National Heart Centre Singapore (NHCS).
Here, he describes the heart at different stages in life and what people can do early to prevent problems later.
Dr Lim Choon Pin cited studies showing that an increased risk of developing coronary artery diseases starts at an average age of 45 for men, and 55 for women.
PHO
TO: A
LVIN
N L
IM /
123
RF
If they are prudent with their lifestyles and dietary habits, we can expect the majority of the population to have good and strong hearts at this time of their
lives. “While it is normal to have a healthy, unblocked heart, it is becoming increas-ingly less common,” said Dr Lim.
The main problem now is ischaemic heart disease: “Patients show up with more symptoms of blockages in the arteries and heart attacks. As a result, many may develop weak heart function, resulting in heart failure.”
Good lifestyle and dietary habits may help maintain a strong heart, but age is an inher-ent risk factor. Dr Lim cited studies showing that an increased risk of developing coronary artery diseases starts at an average age of 45 for men, and 55 for women. The cardiologist said the later onset age for women is likely due to the protective effect of oestrogen prior
to menopause. It protects against atherosclerosis, a disease of the arteries character-ised by the deposition of fatty material on the inner walls of arteries.
Dr Lim’s advice: Go for regular checks for diabetes, high cholesterol and high blood pressure. “Diabetes, high cholestrol and high blood pressure
can cause damage to blood vessel walls, make them more prone to injury, and increase the risk of blockage.”
Tests that can screen for the presence or probability of cor-onary artery disease – each with its advantages and risks – include the treadmill stress test and the high-sensitivity C-reactive protein test.
Even those who have laid the groundwork early in life, and have relatively fewer coronary issues and no blockages in their heart
arteries, may still develop some physiological stiffening of heart muscles due to the wear and tear of ageing, or diseases such as high
blood pressure. As a result, breathlessness or swelling in the lower limbs may occur. People in this age group are also at a higher risk of developing
abnormal heart rhythms, often due to blockages in the heart arteries or fibrosis of the nerve conduction in the heart. This can result in very slow heart rates requiring pacemaker implantation, or irregu-lar heart rhythm, called atrial fibrillation, which puts them at risk
of stroke. Heart valves may also degenerate over time. Some patients
may encounter stiffening or leaking of their heart valves, leading to the need for valve surgery or valve procedures.
Advances in minimally invasive procedures have made it possible for even the very elderly to
undergo cardiac procedures at low risk.Barring a family history or childhood incidence of heart disease, at this age the heart
is generally healthy, and free of blockage and plaque. But how it fares two decades later depends on how it is cared for now. “Take care of your heart early in life, and you will reap the
rewards as you age. Generally speaking, if you do, you can expect your heart to remain healthy and strong for most of your life,” said Dr Lim.
He said that cholesterol plaques may start forming in blood vessels at this stage. Life-style habits can impact the heart and result in cardiovascular-related risk factors such as
diabetes, high blood pressure and high cholesterol. However, unless you show cardiac symptoms or have significant cardiovascular risk factors, there is gen-
erally no need for routine cardiac imaging or stress tests. But the young should not take things for granted. Dr Lim’s advice: Do 30 minutes of moderate-
intensity exercise such as brisk walking, cycling, dancing and gardening five times weekly, or 25 minutes of high-intensity exercise such as jogging, running, swimming laps or playing tennis three times a week. Maintain a balanced diet that is rich in vegetables, fruits, whole grains and fish (rich in omega-3 fatty acids). Keep Body Mass Index (BMI) between 18.3 and 23. Do not smoke, and ensure moderate alcohol intake.
Also, get at least six hours of sleep daily. Lack of sleep has been linked to increased insu-lin resistance, diabetes and heart disease. A review of multiple studies involving almost 500,000 people revealed that those who did not get adequate sleep had an almost 48 per cent chance of dying from heart disease and a 15 per cent greater risk of stroke when followed up 25
years later. At this stage of life, it is important to start looking at one’s global cardiovascular risk. This
means that we should start calculating our individual risk of cardiovascular events over a 10-year period, and to keep these risk factors in check if the risk scores increase. To cal-
culate your risk, use the Health Promotion Board’s risk calculator: www.hpb.gov.sg/HOPPortal/dandc-article/10030.
40s-60sPROCEED WITH CARE
70s-80s WEAR & TEAR
20s-30s LAYING THE GROUNDWORK

160318-TSC-Singhealth-winter-colourproof.indd 1 21/4/2016 11:33:30 AM

25新闻新加坡中央医院与新加坡保健服务集团的双月刊 2016年5–6月刊
在过去十年,患上非酒精性脂肪肝病的人士有逐渐上升的趋势。近年来的发病率更是
达到约50%的成人人口,引起了本地医学界的特别关注。
这些患者大多数都是20多岁,拥有中等身材和体重,少喝酒或滴酒不沾的年轻人。他们也丝毫不符合一般脂肪肝的致病因素,即酗酒、过度肥胖或糖尿病。
“要是没做肝脏扫描,是很难诊断出非酒精性脂肪肝病的。”一直主力研究
我怎么可能得脂肪肝?不胖、不喝酒、无糖尿病的年轻人为何也有脂肪肝。原文 Low Shi Ping
脂肪肝病与肝癌课题,新加坡国立癌症中心肿瘤外科高级顾问医生周嘉豪教授说。肝细胞内只要积聚5%的脂肪就算是脂肪肝。一般可以通过活检、磁共振成像(MRI)、断层 X 光(CT)或超声波扫描出来。
周教 授补充说,脂肪肝 是可 逆性 疾病。若能及早确诊和治疗,通常都能让肝功能恢复正常。但如果一旦恶化为更严重和复杂的脂肪肝疾病,如肝硬化、非酒精性脂肪肝炎或肝癌,届时疾病就不容逆转了。依全球统计预测,非酒
PHO
TO: A
LVIN
N L
IM
新加坡国立癌症中心肿瘤外科高级顾问医生周嘉豪教授(左一)教导医学生有关脂肪肝病的知识。依全球统计预测,非酒精性脂肪肝病将会在未来的10到15年内取代乙型和丙型肝炎成为世界头号肝癌的主要成因。
病因是什么?
虽然专家们目前还在研究非酒精性脂肪肝病的成因,不过医学界也捕捉了一些可能造成疾病的线索,包括: 遗传倾向假设人们遗传到祖先们优良的适应周期性饥荒的基因,而促使人体特别容易摄取和存储热量。随着生活水准提升,饮食量增加,尤其是碳水化合物,人体很容易患上“代谢综合症”,使得糖尿病和非酒精性肝病发病的风险提高。
工业果糖这是具有争议性的理论。果糖的化学结构使人们容易患上脂肪肝病。有人相信脂肪肝病之所以在上世纪70年代开始盛行,是因为当时市场在制造饼干、快熟面、汽水等食物时开始引入工业化生产的制糖,特别是人工果糖。
肠道细菌的变化这是与肠道细菌的变化有关的理论。 从动物试验结果表明,当它们饮食中的糖分在消化过程中被改变时,它们肠道内的细菌也会受到影响。当细菌与肠道细胞的过氧化物酶体增殖物激活受体
(peroxisome proliferator-activated receptors, PPARs)接触时,后者会发出信息和信号给体内其他器官,通知器官改变新陈代谢的运作。这可能会导致某些器官如肝脏存储脂肪,促成 脂肪肝。
及早诊断早期的非酒精性脂肪肝病一般不会表现出任何症状。
但是随着病情演变,患者可能会有疲倦感、腹胀感、食欲不振、右上腹疼痛等症状。如果病情发展至非酒精性脂肪肝炎或肝硬化,其他症
精性脂肪肝病将会在未来的10到15年内取代乙型和丙型肝炎成为世界头号 肝癌的主要成因。
在美国,非酒精性脂肪肝炎是导致肝脏移植的第二大原因。在本地,非酒精性脂肪肝病的发病率也有上升的趋势。发现这个趋势的正是就读于杜克-国大医学院,也是周教授的其中一名 医学生,许明臻先生。
当时 还 在中央 医 院实习的 他,从 扫描影像观察到有不少入院接受胆囊手术的病人都患有非酒精性脂肪肝病,
状如恶心、黄疸、注意力涣散等也会陆续显现。
不过,不是所有脂肪肝病患者都会患上肝癌。周教授说,“及时诊断和治疗还是可以将病情逆转的。”
虽然有许 多病人常误以为只要
避免摄取脂肪,就可以预防患上脂肪肝病,其实不然。临床研究显示, 改变生活方式,加强运动量,减少 摄取碳水化合物和精制糖,减轻10%的体重才是逆转病情关键。
国立癌症中心目前正在进行相关
的动物试验,并有计划在未来进行 人口研究。
“目前为止,我们所知不足,所以 必须继续进行研究,希望通过识别潜在的高风险患者,尽快进行干预以 预防癌症的发生,”周教授说。
而且发病率还比预期高,所以才激起 许明臻着手进行对比研究。
结果显示,在2000年至2003年期间,伴有脂肪肝病的胆结石病患者有30%,十年后,即2010年至2013年期间,此比率已攀升至50%。
周教授说,“虽然前来接受治疗的是胆结石病患者,不过从常规扫描来看,这群患者的确是有脂肪肝问题。目前发病机制尚未清晰,可是在流行病学上的数据却已清楚明示,所以不能掉以轻心。”

PHO
TOS:
ALV
INN
LIM
/ GE
TTY
IMAG
ES /
123R
F
26 健康 2016年5– 6月刊
位于后港观明综合医院复健病房留医的新加坡中央医院中风病人,可能不知道他们
已在一个名为“中风康复之路”(stroke rehabilitation pathway)的计划下接受护理和治疗。
这个计划确保患者都能获得全面评估,并给予最适当的照顾。
中 央 医 院 康 复 医 学 科 高 级 顾 问 吴宜善医生说:“计划旨在确保每个 病人都能获得同等高标准的治疗和康复 护理。”
在这之前,评估、治疗和护理都是以个别不同学科的基准来进行。计划实施后,多学科小组便携手合作,按照同一套全面性的护理治疗评估表,替病人 进行评估。
参与计划的多学科医护专业人员有多达10科,其中不单只有医生及护士,也有物理治疗师、职能治疗师、足病治疗师、音乐治疗师、营养师以及药剂师,以确保病人得到全面的照顾。举个例子,当病患情绪低落时,唱歌或弹奏乐器
在观明综合医院留医的中风病人现可通过新计划接受跟进评估及测试。原文 Desmond Ng
中风病人的康复护理蓝图
整合所有治疗程序让其标准化能让医护人员更容易跟进病人的进度,也可以用来培训新人员。日后也可将成果作为基础研究,进而改良现有程序的 不足。新加坡中央医院康复医学科顾问拉力克医生
训练身体再次动起来在中风后,康复中的病人所面对的最大挑战之一是如何运用体力及适当的控制来再次站起。
有证据显示,四肢越早能够动起来可以提高康复的机会。治疗师可以利用设备来选择性地让病人开始运动。举个例子,病人可以在步态 训练机的帮助下站立起来,接着该机械可以帮助身体的其他部分活动。
过去,康复的重点是放在强健肌肉,但现在的重点是功能。与其让 病人在病床上踢脚,更好的方法是利用步态训练机帮助他站立及做 运动。病人的站姿是很重要的,它可以帮助他们重新恢复活动能力。
其他设备包括:Amadeo帮助手指失去能力的病人以及Arjo Sara Plus -另一个让病人在物理治疗时可以从坐姿转变为站姿的机械。
来自多个医学科的医疗小组利用步态训练机帮病人站起及运动。这是观明综合医院的最新设备之一。
Amadeo是一个手部康复仪器,它可以帮助手指失去活动能力的病人重新活动手指。
不但能使病人开朗起来,也能帮助带动 迈向康复之路。中央医院康复医学科 顾问拉力克(Ashfaq Ahmed Larik) 医生说:“整合所有治疗程序让其标准化能让医护人员更容易跟进病人的进度,也可以用来培训新人员。日后也可将成果作为基础研究,进而改良现有程序的
不足。”在中央医院接受中风治疗的 病人在病情稳定下来后,可以转往观明综合医院接受康复治疗。该卫星康复病房有54张病床,中风病人就占用一半。
中风是因血流中断导致脑细胞死亡,而中风的病人可能突然失去说话的能力或一边的身体瘫痪。物理治疗是中风病
人康复护理的重要一环,因为长期卧床会导致肌肉乏力。
拉力克医生说:“为提高物理治疗师的工作效率,医院增添新的先进复健机械有助于支撑中风以及脊椎损伤的 病人,让他们感受卧床已久后重新站立的感觉。”
在物理治疗时,Arjo Sara Plus站立升降机可以帮助病人由坐姿转变为直立站姿。

27健康2016年5– 6月刊
在市场上售卖的牙膏会导致过敏吗?会。牙膏的味道或香气可能会导致过敏, 像肉桂醛(肉桂的味道)、留兰香、薄荷、 香芹酮(葛缕籽的油份)及茴香醚(八角、 茴香及茴芹的香味)。
刷牙时需要多少牙膏? 牙膏含有很多化学磨料会引起不必要的磨损及敏感,不是用得多效果就会更好。所以豌豆大小就够了。
把盐涂在牙齿上可以防止蛀牙吗?不会。这只是因为旧年代没有先进的 牙科用品,一般人爱用的传统方法而已。事实上,把盐涂在牙齿上会导致牙齿 表面磨损。
我们是否真的需要每6个月看牙医一次?为什么是6个月?为什么不可以是一年或其他时间间隔? 这将视乎个人的牙齿健康或病况而定。如果你可以把牙齿健康维持良好,或那些有伴随其他疾病(像心脏病及糖尿病)的人士能把病况控制得很好,可以每6个月至1年看牙医一次。
口腔健康欠佳、患有口腔疾病如龋齿(蛀牙)或牙周病的人士则需要每3至6个月看牙医一次,让口腔疾病能及早得到治疗和控制,避免因牙周骨质流失而必须进行更复杂且昂贵的治疗。
那些病情控制不良的人士如糖尿病患者,应该 每2至4个月到牙医诊所一次以避免引发牙周病。因为牙周病会使血糖更难受控制而且还会提高糖尿病 并发症的风险,例如肾功能衰竭和视网膜病变。
患有多种疾病及服用多种药物的老年人,也应该每2至4个月到牙医诊所一次。因为药物的副作用会令唾液减少,导致口腔干燥症(口干),提高龋齿的 风险。
总的来说,单靠刷牙、使用牙线或漱口液是无法 彻底清除所有的牙斑和牙垢。所以您应该按期看 牙医来维持口腔健康,和避免疾病的发生。
长远来说,根管治疗或把牙齿拔掉,哪个 比较好?如果可以的话,保留牙齿永远都是最佳的选择。但在牙髓发炎或感染而无法康复的情况下, 根管治疗是唯一可以保存牙齿的方法。经过 根管治疗后,牙齿会补上填充物或牙冠来修复。
但当牙齿的结构由于大幅损害或蛀蚀而无法 支持牙齿修复,我们可能会建议病人把牙齿拔掉。
为什么有些人在睡觉时会磨牙或咬紧牙齿?这个情况危险吗?可以预防吗?磨牙及咬牙的起因还未有证实。可是,它们通常是与生活压力、习惯或睡眠不好有关。
长期及严重磨牙或咬牙会导致牙齿损毁;可能是轻微的牙釉质脱落或甚至牙齿纵向断裂。它也可以导致咀嚼肌疼痛及颌骨损耗较快。
预防磨牙的治疗方法包括心理辅导、按摩 治疗及有规律的睡眠模式。为减低磨牙带来的伤害,牙医通常建议睡觉时戴上牙胶。
牙刷放在厕所符合卫生吗?牙刷放在厕所问题不大,只要把它们分开放在清洁及干爽的地方,以避免受到细菌交叉污染。
有人说最重要是一天漱口几次,是真的吗?当不方便刷牙时,漱口可以把残留在口腔的食物渣宰清除。但如果你勤用牙线及用正确的方法一天刷牙两次,你根本不需要漱口液。但如果你生口疮或患有牙龈病像牙龈炎或牙周病,配方漱口液能帮助减少 牙龈流血及发炎。
我们应该早上一起来就刷牙或者是等吃完早餐才刷牙?两者都可以。如果您习惯餐后刷牙,最好隔20-30分钟后才刷。因为食物会减少口腔的酸碱值(pH),削弱牙齿的保护层使牙齿更脆弱。
您有问题想问牙医但总是找不到机会?让新加坡全国牙科中心的专家为您解答一些常见的问题。
原文 Satish Cheney
问问牙医
与其把牙齿拔掉,根管治疗是另一个可行的选择。在牙髓发炎或感染而无法康复的情况下,根管治疗是唯一可以保存牙齿的方法。新加坡全国牙医中心修复牙齿部门根管治疗科高级 顾问医生雷珍妮
专家解答
儿童的眼部护理长时间使用平板电脑和笔记型电脑玩网络游戏是否会逐渐导致孩子的眼睛疲劳?患有飞蚊症的孩子在长大后情况会不会好转,有没有 治疗方法呢?此外,眼部按摩器是否能够帮助孩子拥有健康的眼睛?研究结果显示,近距离工作或玩电脑游戏与患上近视大有关联。无论 孩子在近距离进行的是什么活动,即使是阅读,打字或观看视频,都必须在30到40分钟的连续近距离活动后,让眼睛休息一下。
飞蚊症可能是因为玻璃体后脱离、视网膜撕裂或脱离造成,而很少是 由于玻璃体或视网膜的炎性病症。对于儿童而言,上述的症状更为 罕见。不过,建议患有飞蚊症的儿童进行全面的眼科检查,以排除 以上症状。治疗方法主要视飞蚊症的病因而定。
眼部按摩器还未获得科学证明,对减少近视进展,或眼部的 健康有所帮助。
新加坡全国眼科中心小儿眼科与成人斜视眼科部
确诊患上疝气最近我发现我的腹股沟上有肿块,而且站着比坐着还明显。诊断结果证实那是疝气。可是我并不觉得有任何不适或疼痛。是什么原因导致疝气的呢?疝气的产生是由于一些引起腹压的动作,例如提重物、 排便或咳嗽过度用力以及肥胖,造成腹壁薄弱,使腹内的脂肪组织或器官,如肠道突出腹壁并在皮肤底下形成包块。
无痛的疝气一般不怎么严重。但如果肠道被绞窄或堵塞,又或者肠道或其他器官的血液供应被切断导致坏疽,那么就得必须马上动手术,将腹壁疝切除和修复损坏的肠道。
虽然早期阶段的腹壁疝一般不会引起不适,不过它会逐渐变大。如果发现腹壁疝有增长现象,腹股沟和腹部感到疼痛以及其他不适,譬如恶心、呕吐及血便,请立即求医。
新加坡中央医院普通外科部

28 2016年5– 6月刊
ADVERTORIAL