therapeutic monitoring of tacrolimus concentrations in blood of renal and liver transplant...
TRANSCRIPT

TRE
I
TtltpdnelTeptz
0d
9
herapeutic Monitoring of Tacrolimus Concentrations in Blood ofenal and Liver Transplant Recipients: Comparison of Microparticlenzyme Immunoassay and Enzyme Multiplied Immunoassay Methods
. Bartlomiejczyk, D. Zochowska, J. Sanko-Resmer, D. Matuszewicz, and L. Paczek
ABSTRACT
Monitoring of tacrolimus blood concentrations is of utmost importance in themanagement of organ transplant recipients due to narrow therapeutic index of thedrug and its considerable interpatient variability in pharmacokinetics. Thus therapeu-tic monitoring of tacrolimus plays a crucial role not only in the evaluation of the drugefficacy but also in the control of possible side effects. We compared immunoassay-based methods, quantitative enzyme multiplied immunoassay (EMIT) with quantita-tive microparticle enzyme immunoassay (MEIA), using blood samples from renal andliver transplant recipients (n � 40) treated with tacrolimus. Blood samples wereobtained for diagnostic routine measurements. The tacrolimus concentrations mea-sured by EMIT for all the transplant patient samples were higher (2.8 to 28.5 ng/mL)than results obtained in MEIA (3.0 to 25.0 ng/mL). The mean difference expressed inpercentage was 13.94% and correlation coefficient EMIT versus MEIA was 0.97. Thetacrolimus concentrations measured by EMIT for renal graft recipients (n � 8) werehigher (6.0 to 13.3 ng/mL) than those measured by MEIA (6.1 to 12.2 ng/mL), meandifference expressed in percentage was 14.1% and correlation coefficient was 0.85. Thetacrolimus concentrations for liver transplant recipients (n � 32) measured by EMIT(2.8 to 28.5 ng/mL) were higher than results obtained in MEIA (3.0 to 25.0 ng/mL), themean difference expressed in percentage was 13.89%, and the correlation coefficientwas 0.98. The results obtained in the study show an insignificant difference in specificityof both methods used to determine the concentration of an active drug. Thus both
methods, EMIT and MEIA, seem to have similar diagnostic value.M
Ttytpp
oLJ
oM
ACROLIMUS IS A DRUG used in immunosuppres-sive treatment in patients after organ transplanta-
ion, including kidney and liver. Tacrolimus is a macro-ide, characterized by narrow scope of efficient and safeherapy and by considerable individual variability ofharmacokinetic features.1 Implementation of wrongrug dose may cause graft rejection or, when overdosed,ephrotoxicity, neurotoxicity, and many other adverseffects. Monitored therapy plays a crucial role in control-ing of treatment efficacy and possible adverse effects.he aim of the study is to compare two methods ofstimating tacrolimus trough levels in full blood ofatients after organ transplantation: EMIT enzyme mul-iplied immunoassay (EMIT) versus microparticle en-
yme immunoassay (MEIA). l041-1345/06/$–see front matteroi:10.1016/j.transproceed.2005.12.042
4
ATERIALS AND METHODS
he study was performed in a group of patients after kidney and liverransplantation (n � 40), aged from 21 to 71 years (age mean: 43.9ears) in different stages after organ transplantation. The blood wasaken routinely, for diagnostic purposes, without additional burden foratients. Patient blood samples were taken into test tubes containingotassium salt of versenianic acid. Estimations of tacrolimus trough
From the Transplantation Institute, Department of Immunol-gy, Transplantology and Internal Diseases (I.B., D.Z., J.S.-R.,.P.), Warsaw Medical University, Warsaw, Poland, and Infantesus University Hospital (D.M.), Warsaw, Poland.Address reprint requests to Irena Bartlomiejczyk, Department
f Immunology, Transplantology and Internal Diseases, Warsawedical University, ul. Nowogrodzka 59, 02-006 Warsaw, Po-
and. E-mail: [email protected]
© 2006 by Elsevier Inc. All rights reserved.360 Park Avenue South, New York, NY 10010-1710
Transplantation Proceedings, 38, 94–96 (2006)
ltoDaactc
Uni
hsptV
Tsu(
PoB
FMtlpt
MONITORING TACROLIMUS CONCENTRATIONS IN BLOOD 95
evel were performed on the day of samples collection with the use ofhe EMIT and MEIA methods at Independent Analytical Laboratoryf Department of Immunology, Transplant Medicine and Internaliseases. The EMIT 2000 Tacrolimus Test (Dade-Behring) presumestechnique of homogeneous immunoenzymatic tests for tacrolimus
nalysis in full blood. The test estimates quantitatively tacrolimusoncentrations ranging from 2 to 30 ng/mL. Analytic sensitivity of theest amounts to 1.2 ng/mL, whereas its functional sensitivity at 20%oefficient of variance (CV) amounts to 3.0 ng/mL.2
The IMx Tacrolimus II Test (Abbott Laboratories, Abbott Park, Ill,SA) is based upon a microparticle immunoenzymatic MEIA tech-
ique. Analytical sensitivity of the test amounts to 1.5 ng/mL, whereasts functional sensitivity at 20% CV amounts to 4.1 ng/mL.3
Full blood samples before implementation of the EMIT method
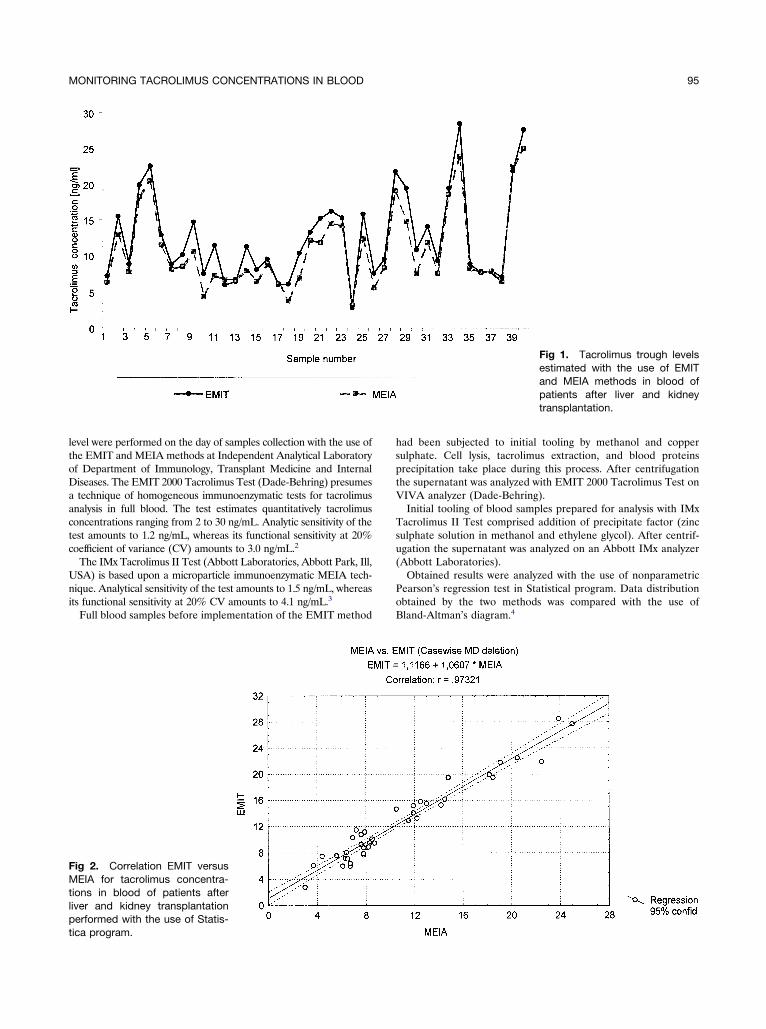
ig 2. Correlation EMIT versusEIA for tacrolimus concentra-
ions in blood of patients afteriver and kidney transplantationerformed with the use of Statis-
ica program.
ad been subjected to initial tooling by methanol and copperulphate. Cell lysis, tacrolimus extraction, and blood proteinsrecipitation take place during this process. After centrifugationhe supernatant was analyzed with EMIT 2000 Tacrolimus Test onIVA analyzer (Dade-Behring).Initial tooling of blood samples prepared for analysis with IMx
acrolimus II Test comprised addition of precipitate factor (zinculphate solution in methanol and ethylene glycol). After centrif-gation the supernatant was analyzed on an Abbott IMx analyzerAbbott Laboratories).
Obtained results were analyzed with the use of nonparametricearson’s regression test in Statistical program. Data distributionbtained by the two methods was compared with the use ofland-Altman’s diagram.4
Fig 1. Tacrolimus trough levelsestimated with the use of EMITand MEIA methods in blood ofpatients after liver and kidneytransplantation.

R
Bphaw(tagdt(wnwEgrtnasr
D
Mtf
itpMsbtApTiEmm
R
m1
L
C
a1
nbp
Fskotiem
96 BARTLOMIEJCZYK, ZOCHOWSKA, SANKO-RESMER ET AL
ESULTS
lood trough levels of patients after kidney and liver trans-lantation (n � 40) obtained by the EMIT method wereigher in comparison to the MEIA method: 2.8 to 28.5 ng/mLnd 3.0 to 25.0 ng/mL, respectively (Fig 1). Regression curveas as follows: EMIT � 1.0607 � MEIA � 1.1166; r � .97
Fig 2). The average difference between all samples amountedo 13.94%. Results distribution obtained with the use of EMITnd MEIA methods was visualized with Bland-Altman’sraph, where average difference amounted to 1.77, and stan-ard deviation amounted to 1.5 (Fig 3). Similarly, tacrolimusrough levels in blood of patients after kidney transplantationn � 8) obtained by the EMIT method (6.0 to 13.3 ng/mL)ere higher in comparison to the MEIA method (6.1 to 12.2g/mL); the average difference amounted to 1.45 ng/mL,hich constituted 14.1%. Regression curve was as follows:MIT � 0.9901 � MEIA � 1.4907; r � .88. Parallel to theroup of patients after liver transplantation (n � 32), theesults obtained by the EMIT method were higher comparingo the MEIA method: 2.8 to 28.5 ng/mL versus 3.0 to 25.0g/mL, respectively. Average difference between samplesmounted to 1.85 ng/mL, which constituted 13.89%. Regres-ion curve was as follows: EMIT � 1.065 � MEIA � 1.1315;� .98.
ISCUSSION
onitored therapy plays a crucial role in controlling efficacy ofreatment and observing its potential adverse effects. There-
ig 3. Bland-Altman’s graph foramples of patients after liver andidney transplantation. Continu-us line, average difference be-ween EMIT and MEIA methods;nterrupted line, average differ-nce between EMIT and MEIAethods � 2 SD.
ore compatibility and stability of methods of estimation ofET
mmunosuppressive drugs concentrations is of a major impor-ance. Two methods of tacrolimus estimation in full blood ofatients after kidney and liver transplantation (EMIT andEIA) were compared in our study. The data obtained
howed statistically insignificant difference in specificity ofoth methods toward active drug. Correlation ratio amountedo .97. Comparable data were obtained by Hesse et al5 andkbas et al.6 The MEIA method is more time-consuming;erformance of a series of 24 probes takes around 2 hours.he EMIT method uses continuous probing course; however,
t requires more frequent calibrations. Our data suggest thatMIT and MEIA tests are equally useful and may be imple-ented alternatively in everyday clinical practice in order toonitor the appropriate blood drug trough level.
EFERENCES
1. Oellerich M, Armstrong VW, Schutz LM: Therapeutic drugonitoring of cyclosporine and tacrolimus. Clin Biochem 31:309,
9982. IMx Tacrolimus II [package insert]: Abbott Park, Ill: Abbott
aboratories, 19983. EMIT 2000 Tacrolimus Assay [package insert]: Cupertino,
alif: Dade-Behring Syva, 20004. Bland JM, Altman DG: Statistical methods for assessing
greement between two methods of clinical measurement. Lancet:307, 19865. Hesse CJ, Baan CC, Balk AHMM, et al: Evaluation of the
ew EMIT enzyme immunoassay for the determination of whole-lood tacrolimus concentration in kidney, heart, and liver trans-lant recipients. Transplant Proc 34:2988, 20026. Akbas SH, Yavuz A, Tuncer M, et al: Evaluation of the new
MIT tacrolimus assay in kidney and liver transplant recipients.ransplant Proc 36:86, 2004