the vulvar lichen disorders: simplex, sclerosus, planus · • brass instrument mouthpiece •...
TRANSCRIPT

The Vulvar Lichen Disorders: Simplex, Sclerosus, Planus
Paul Summers, M.D.Department of Obstetrics and GynecologyUniversity of Utah School of Medicine

Areas of Concern• 1. Dermatopathology
• 2. Spongiotic Dermatitis
• 3. Patch testing: nickel, etc
• 4. Risk for squamous cancer

Skin Flakes (lichen)• Normal healthy skin exfoliates individual
epithelial cells
• Flaking skin is common at fragile body sites
• Skin flakes are called “reactive change” when seen in the pap smear
• Skin flakes are found frequently in the saline wet prep
• Unfortunately, flakes are not yet listed as an element to evaluate in the saline wet prep

Skin Flakes in the Pap Smear• Reactive, Reparative changes are reported
in many pap smears
• Characteristic of smears with reactive/reparative changes:1. cells tend to form sheets (Alexander Meisels, Carol
Morin Cytopathology of the UterusASCP Press 1997:128)
2. spongiosis is a prominent feature if the cervix is biopsied (Yao S. Fu, Pathology of the Uterine Cervix, Vagina and Vulva Saunders 2002:281)

Skin flake typically due to a lichen skin disorder
Vulvovaginal irritant and allergic response causes the skin to flake, as is seen frequently in the saline wet prep
Skin Flakes in the Saline Wet Prep

Skin Flakes in the Wet Prep
Hyperkeratotic skin flake
Thin skin flake
Skin flake melting in KOH
Folded edge of skin flake

Flakes in the Wet Prep at the University of Utah
• 17/20 biopsy proven cases of lichen sclerosusshowed skin flakes
• 36/36 biopsy proven cases of vulvar contact dermatitis showed flakes
• 14/14 presumed by history but not confirmed cases of vulvar contact dermatitis showed flakes
Vulvovaginal Irritant and Allergic Contact Dermatitis
Lichen Simplex
What is Lichen Simplex?• Vulvar irritant or allergic contact
dermatitis• Dermatopathology shows
Spongiotic Change with or without eosinophils
• Typically secondarily infected: Staph, Strep, or Yeast

Contact Dermatitis• Affects 40% of adults continuously
• All adults will have contact dermatitis at some time
• Vulva is at special risk (fragile, increased trans epidermal water loss)
• Results in flaking skin, even in the vulvovaginal area

Irritant Contact Dermatitis
• Irritants cause immediate or delayed burning
• Typically, there is no visible skin change
• Erythema is present in severe cases
• Most commercial creams and lotions contain irritants

Allergic Contact Dermatitis • Itch-scratch cycle perpetuates the disorder
• The majority also have recurrent sinusitis, asthma, hay fever, or eczema
• Diagnosis is confirmed by hyperkeratosis, spongiosis and eosinophils on biopsy

Vulvar Susceptibility to Irritants and Allergens (Farage Arch Gynecol Obstet 2005;272;167-72)
• Relatively increased skin hydration• Significantly increased transepidermal water loss
(TEWL)• Increased penetration of irritants, especially in the
vestibule• Increased susceptibility to mechanical damage
(higher friction coefficient)
• Vulvar irritant dermatitis is often occult

Spongiotic Change with Contact Dermatitis
1. Intraepidermaledema
2. Liquifaction of dermal-epidermal interface
3. Langerhans cells—blue arrows

Severe Spongiotic Dermatitis

Fischer GO, The Commonest Causes of Symptomatic Vulvar Disease: a Dermatologist’s Perspective. Australias J Dermatol. 1996;37:12-18
• Vulvar contact dermatitis was the principal diagnosis in 54% of 141 patients referred to a dermatologist for chronic vulvovaginitis

Nardelli A, Degreff H, Goossens A. Contact Allergic Reactions of the Vulva: a 14-year Review. Dermatitis. 2004;15:131-6
• 38% of women with chronic vulvitis demonstrate an allergic or irritant response to vaginal creams and medications

Vaginal Immunology
• HIV has taught us that the lactobacillus and pH are not the protectors for the vagina
• A normal CD4 immune cell response is essential for vulvovaginal health
• The vaginal mucus contains numerous essential antimicrobial chemicals

Vulvovaginal Microbicides (Braff. J Invest Dermatol 2005;125:9-13)
Over 50 anti-microbial substances are produced by the skin (over 800 chemicals in all)
Some are innate
Some are activated by a Th1 response
A Th2 response can inhibit the release of microbicides
hBD-3 has a Minimal Inhibitory Concentration of 13.2 ug/ml against Saccharomyces cerevisiae (Garcia. Cell and Tissue Research. Published online 11 September 2001)

The Consequences of Allergic Dermatitis
• Deficient cathelicidin (LL-37) and beta defensin (hbd-2, 3) allows microbe colonization of the skin (staph, strep, yeast)
• Flaking of the stratum corneum facilitates microbe entry into the skin
• Deficient cell-mediated Th-1 response allows microbe proliferation in the skin

35 Cases of Vulvovaginal Contact Dermatitis at the University of Utah
• 25/35 have at least one yeast infection confirmed in the University clinic
• 28/31 have history of asthma, allergic rhinitis, eczema
• 23/31 have irritant reaction to creams
• 26/35 pre menopausal
• 9/35 post menopausal
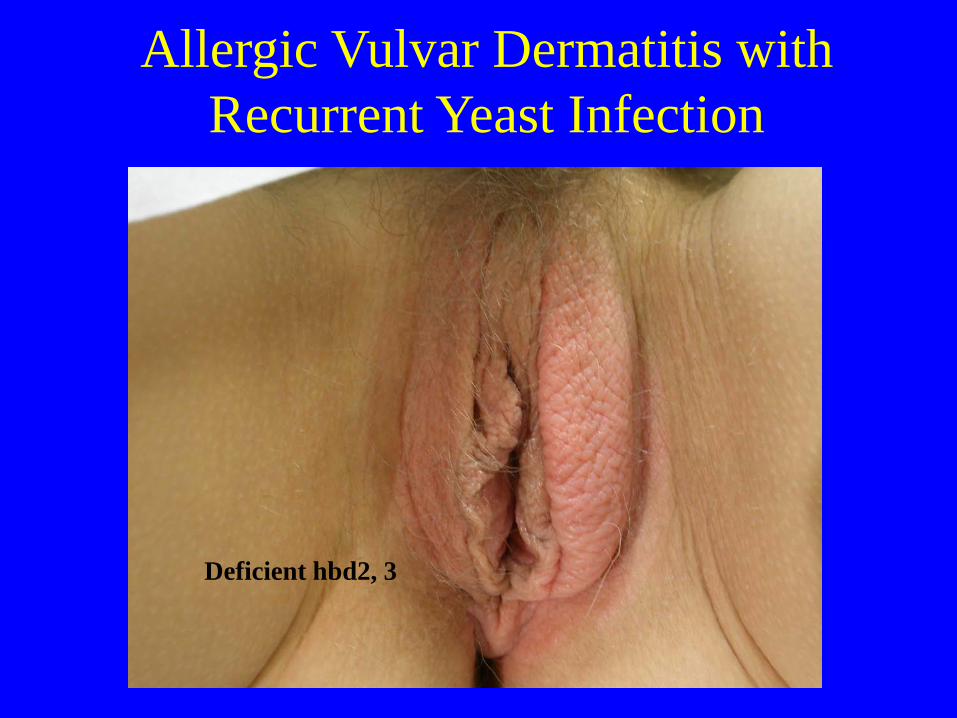
Allergic Vulvar Dermatitis with Recurrent Yeast Infection
Deficient hbd2, 3

Lichen Simplex Chronicus
Scratching here
History of asthma, hay fever, eczema, sinusitis

Vulvar MRSA

Vulvar Carcinoma
50% related to HPV, but many of the remainder are related to lichen dermatitis

Contact Dermatitis may Trigger other Disorders
• Recurrent Herpes
• Vulvar Crohns
• Behcets
• Aphthous major or minor

Primary herpes, in atopic skin with a poor Th1 response
Increased risk for recurrent HSV
Therapy for Vulvar Contact Dermatitis
• Obtain a history of products that burn to help identify Irritants to avoid
• Consider patch testing by a dermatologist
• Treat once or twice daily with a non-irritating (compounded?) steroid ointment
• Moisturize at other times with Vaseline, Crisco, or coconut oil

Therapy for Vulvar Contact Dermatitis
• Consider the long-term risk of squamous cancer
• Oral fluconazole or topical clotrimazole for yeast infection
• Treat Staph folliculitis or Strep cellulitis

What is CMC?
Processed Wood Pulp

Uses Of CMC• Industrial Grade: Oil drilling, Paper,
Paint
• Food Grade: Bread and Bakery, Ice Cream, Pudding, Beverages, Toothpaste, Cosmetics Dog and other pet foods
German patent in 1918 with increasing use after the 1940’s

Annual Production: $1.2 Billion
33% Food and Beverages

CMC is Declared safe for Human use in Europe and America
But a known skin irritant

The Rely Tampon• Carboxymethyl cellulose was used to increase
absorption of menstrual blood
• Presumed by the designer to be totally safe since CMC is a common “safe” food additive
• Around 500 million Rely Tampons produced
• Between 800 and 2000 cases of toxic shock and at least 84 deaths in 2 years of use

Rely Tampon Toxic Shock
• Vaginal Irritant reaction to CMC• (Rare) severe vaginal spongiotic
change• Proliferation of staph (strep or yeast)• 5-25% of Staph aureus can produce
TSST-1 toxic shock protein• TSST-1 is released in large amounts
after an exponential growth phase

Toxic Shock Syndrome• Eventually all adults are likely to have
antibodies against TSST-1 from low level exposure
• Mortality from Staph toxic shock is around 10%
• Mortality from Strep toxic shock is over 50%

Lessons from the Rely Tampon
• Vulvovaginal contact dermatitis is a reality
• Irritant susceptibilities are unique to the individual
• Expect consequences from secondary infection with Staph, Strep, or Yeast

Nickel Sensitivity• 11% of women and 3% of men
• Irritation from cheap jewelry (ear rings)
• Chocolate, Nuts, and bitter green vegetables have a high nickel content
• Low Nickel Diet may help decrease urinary nickel

Contact Dermatitis in Musicians• Brass instrument mouthpiece
• Exotic wood
• Varnish
• Rosin for the bow

Patch Testing by a Dermatologist• Identifies environmental irritants to
avoid
• Unfortunately, the vulva reacts to a wider range of irritants than the back
• Useful if topical steroid and moisturizers fail

(blue squares)
An Excellent Review!
*
Lichen Sclerosus• Mild lichen sclerosus is relatively common (minimal
visible skin change)
• Often hour glass-shaped rash
• Any age group
• Associated with recurrent yeast infection
• Treat any concurrent post menopausal atrophy
• Increased irritant susceptibility

Lichen Sclerosus
Complications:
1. Irritant reaction
2. Allergy, yeast infection
3. Cancer

Lichen Sclerosus Issues• Secondary development of contact
dermatitis (mixed dystrophy)
• Irritant reaction to most commercial creams
• Yeast infection
• Vulvar cancer

Lichen Sclerosus treatment• Twice daily topical steroid ointment and
moisturize with vaseline Crisco, coconut oil
• Irritant avoidance
• Treat yeast
• Biopsy lesions to exclude cancer

Autoimmune Vulvovaginitis
• Lichen Planus
• Zoon’s disorder
• Aphthous ulcer disease

Vulvovaginal Lichen Planus• Immune trigger, similar to graft vs host
reaction
• Significant vaginal pain and discharge
• Saline wet prep shows numerous WBCs, parabasal squamous cells, shift in flora

Other likely Names
• Desquamative Inflammatory Vaginitis (USA Ob-Gyn)
• Aerobic Vaginitis (“AV” in Europe and Asia)
Oral Genital Syndrome
• Simultaneous oral and vaginal lichen planus in possibly 20% of cases
• Oral Lichen Planus is treated by the dermatologist
Lichen Planus and Cancer• Oral Lichen Planus can cause aggressive
oral squamous cancer
• Associated cervical or vaginal cancer is rare but aggressive
• Plan an annual pap smear with no age limit even after hysterectomy

Parabasal cells
White blood cells
Lichen Planus, saline wet prep

Vulva, Severe Erosive Lichen Planus
Stenosis is more often in upper vagina

Chronic oral ulcer in the same patient

Same patient after 3 months of Imuran to block the excessive Th1 (autoimmune) response

Vaginal erosion
Atrophic cervix
Localized Vaginal Lichen Planus

Zoon’s disorder (vestibulitis)(Plasma cell vulvitis)
Painful erosions in the vestibule
Known Lichen Planus Triggers• Hepatitis C
• Influenza vaccine
• Contact with nickel, chemicals, pigments
• NSAIDs
• Blood pressure medications

Therapeutic possibilities for mild Lichen Planus
• Topical steroids• Topical estrogen• Clindamycin vaginal cream• Celebrex• Oral Metronidazole 500 mg BID for 30 to
60 days (Asher V. Wahba-Yahav Ideopathic lichen planus: treatment with metronidazole. J Am Acad Dermatol 1995;33(2:1):301-2
• Arzu Bueyuek Oral metronidazole treatment of lichen planus J Am AcadDermatol 2000;43:260-2)

Areas of Concern• 1. Dermatopathology
• 2. Spongiotic Dermatitis
• 3. Patch testing: nickel, etc
• 4. Risk for squamous cancer

The Skin Physiology vs. the Microbe
The End