the pennine acute hospitals nhs · s s e management technology, ... the pennine acute hospitals nhs...
TRANSCRIPT
The Pennine Acute Hospitals NHS
A N N U A L R E P O R T 2 0 0 7 - 2 0 0 8NHS Trust

CONTENTSContacting the Trust 2
Trust Board members 3
Chairman’s report 4
Chief executive’s report 6
Infection prevention progress 9
Clinical developments and quality of care 11
Research and development 14
Governance 14
Data loss 16
Standards for Better Health/Assurance framework 16
The Trust Board 18
Improving access 22
Our growing reputation 25
Investing in our hospitals 29
Mission statement, values, strategic aims and corporate objectives 31
Future service developments 42
Patient partnerships, involvement and views 45
Investing in our staff 48
Volunteers 48
Emergency preparedness 49
Sustainable development 50
Partnership working 51
Financial report 52
Remuneration report and directors’ pay and pensions 94
Charitable funds 99
The Trust runs four main hospitals within close reach of each other, serving a population of 800,000 people living in North Manchester, Prestwich, Middleton, Heywood, Bury, Rochdale and Oldham, and the surrounding areas. The vast majority of patients are from the areas of the Trust’s four main commissioning primary care trusts - Bury, Manchester, Oldham and Heywood, Middleton and Rochdale.
North Manchester General Hospital, The Royal Oldham Hospital, Fairfield General Hospital and Rochdale Infirmary are all located within what the NHS describes as the North East Sector of Greater Manchester.
The shortest distance between the main hospitals is less than six miles (Rochdale to either Oldham or Fairfield) the furthest 12 miles (North Manchester to Rochdale). They are all well served by key roads and public transport, including a Metrolink stop near to North Manchester General Hospital, which is on the Bury-Manchester line. In addition, the Trust still has some services at the Birch Hill Hospital site near Rochdale and at the Westhulme site in Oldham.
The Trust is one of the largest in the country and employs a staff of around 10,000.
The Trust has four divisions: surgery, medicine, women and children’s and diagnostic and clinical support.
It also has directorates providing support for: human resources, facilities, modernisation and performance, planning, finance, information and
Local hospitals - supporting each other
The cover picture shows consultant breast surgeon Miss Maria Bramley (centre) and patients at the opening of the £1.3 million Victoria breast unit at The Royal Oldham Hospital, an event marked by the release of pink balloons.

1 The health issues our patients face
management technology, governance and research and development.
The Trust provides district general hospital services and a range of specialties, including the regional infectious disease unit which is based at North Manchester General Hospital.
2 Contacting the TrustThe Trust welcomes direct feedback from patients about its services. There are a number of different ways in which you can contact us or give us your views. If you have an issue which you wish to raise about your care then you should initially discuss this with ward staff.
If you wish, you can also contact the patient advice and liaison service, as follows:
• FairfieldGeneralHospital:01617782455• NorthManchesterGeneralHospital: 01617202707• TheRoyalOldhamHospital01616278678• RochdaleInfirmary:01706517354
You can also email: [email protected]
Sharing your feedbackThe Trust welcomes all comments on its services. Patients and their families can use the hospitals’ feedback sections of the NHS Choices website at www.nhs.uk, the Patient Opinion website at www.patientopinion.org.uk or the feedback sections of the Trust’s own website at www.pat.nhs.uk.
This reportIf you have any suggestions about future content for the Trust’s annual report, or its format, then please contact Fin McNicol, head of communications.Telephone01619184284.Email; [email protected] or write to:Fin McNicol, head of communicationsRoom124,HeadquartersThe Pennine Acute Hospitals NHS TrustNorth Manchester General HospitalDelaunaysRoad,ManchesterM85RB

3Trust Board members
John Jesky, Chairman
John Saxby, Chief Executive
Marian Carroll, Nursing
Robert Chadwick, Finance and IM&T
Karen James, Operations
Dr Ruth Jameson, Medical Director
Roger Pickering, Human Resources
John Wilkes, Facilities
John Battye, Non-executive
Haydn Griffith, Non-executive
Michael Holly, Non-executive
Tim Pickstone, Non-executive
Razia Shamim, Non-executive
Anne Unwin, Non-executive

4These 12 words are the Trust’s new mission statement, adopted after a lengthy Board discussion. We chose these words because Board members firmly believe that they summarise an ethos shared by all 10,000 of our staff.
Our mission statement is not simply a slogan to be displayed on posters or our website. It is a genuine statement of what our patients need, of what we want our services to be and of what our staff constantly strive to deliver.
I am pleased to say that this annual report highlights many examples of how staff are succeeding in this aim. We have had 12 months of very significant progress. The achievements of staff include providing high quality services, raising standards even further, planning for the future and gaining recognition, not just on a regional level but on the national stage.
I would like to begin this annual report by highlighting some specific achievements.
Several major initiatives were either successfully started or completed in2007-08.Wehadfinaldecisionson the public consultations, Healthy Futures and Making It Better, which set out a future vision for our services. Subsequently, work began on the implementation programme, including
Chairman’s reportthe enabling works for the new women and children’s development at North Manchester General Hospital. This development is a key part of Making It Better, not just for the Trust but for the whole of the region. It will also provide the extra capacity we need to begin to move our services to deliver the Healthy Futures vision of centres of excellence at all of our hospitals.
Progress on other key facilities included the full completion of the Trust’s central pathology laboratory. The Trust’s laundry, an essential behind-the-scenes function, received additional investment and is now modern and fit for purpose. The new breast care unit at The Royal Oldham Hospital was officially opened with a superb event devised by staff. More than 100 patients, staff and guests, including the Mayors of both Oldham and Rochdale, gathered to release balloons carrying personal thoughts and messages.
We also saw the start of other projects. Work began on installing the new state-of-the-art CT scanner at Rochdale Infirmary, and The Christie Hospital confirmed that they would be developing a radiotherapy unit at The Royal Oldham Hospital. This initiative will enable patients from across the Pennine area to receive treatment without having to travel to south Manchester.
“To provide the very best

John Jesky, Chairman
5thousands of staff saw us reduce our healthcare acquired infection rates. MRSA cases were brought down a further25%inyear,givingusaratecomparable with the national average. We also completed the deep clean of all our wards to timetable, a real achievement for a Trust of this size.
While we invested in services, and reached key performance targets, wealsoaddressedourdebtof£9.17million a full year earlier than planned. We had intended to repay this debt overtwoyears,2007-08and2008-09.Howevertheadditionalactivitywehave carried out for patients during the year, combined with strong controls on our spending, has seen us exceed our own expectations. At the end of 2007-08wehadrepaidthedebtinfull.In addition to paying off that historic debt, we also ensured that we had an appropriate level of cash to underpin our operational requirements.
We will not go into debt again. The Board believe that the Trust should continue to generate efficiencies so that surpluses can be invested in patient services. The quality of care which we all aspire to provide for our patients is underscored by solid financial foundations.
That framework also supports our future development. The Board have
done much work through the year on the strategic direction of the Trust, as we move towards our Foundation Trust application. We have already started discussions with stakeholders on the potential structure for our governors. Foundation Trust status would bring a range of benefits to patients, including giving us greater financial freedom to invest in our services.
That vision looks to the future. This report celebrates the past 12 months, and the achievements of staff. On behalf of the Board, and of all of our patients and their families, I would like to offer sincere congratulations to our staff for their successes to date, and appreciation for their efforts to come.
The Trust has previously been described by UNICEF as one of the most breast-feeding friendly in the country and this enviable status was sustained with more good news. The UNICEF Baby Friendly programme ensures that we are providing mothers with the information and support to make informed choices about breastfeeding. The results have been phenomenal. Our two fully-accredited hospitals, The Royal Oldham Hospital and North Manchester General Hospital, both doubled their breastfeeding rates through the programme. This year saw staff at The Royal Oldham Hospital successfully gain re-accreditation, while their colleagues at Fairfield General Hospital and Rochdale Infirmary both reached the first stage of the programme.
The Trust’s infant feeding co-ordinator Val Finigan, who has led our work in this programme, gained a well-deserved MBE in the New Year’s Honours list. Val is the first to say that the award reflects on the achievements of her team and the hundreds of staff who have supported new mothers. However, it is also recognition, at the highest level, of how she has shaped our approach and inspired her colleagues.
Infection prevention has been a key issue this year, and a massive effort by
care for each patient on every occasion.”

6During my first year as Chief Executive of the Trust, I have been pleased to see progress on a number of key issues, all designed to improve the quality of care provided. These include reducing hospital infections and improving access for patients. Tackling and eliminating our historic deficit also means that we can now concentrate on service developments and improvements far more than we have been able to.
The Trust is regularly the country’s top performer in the number of patients accessing our services using the Choose and Book system. We have around5,000bookingsamonth.Partof this is, naturally, down to our size, however there is more to it than that.
The NHS Choice programme encourages patients to make active decisions about which hospital they are treated in, and which NHS services they use. The latest national survey found that patients ranked hospitals using the following criteria:
• Cleanliness/infectionprevention work
• Qualityofcare
• Lengthofwaitfortreatment
• Staffattitude
• Hospitalreputation
• Hospitallocation
This report sets out how the Trust staff have performed against those standardsin2007-08.Ibelievetheyhave done extremely well, despite facing some major challenges.
Reducing MRSA infections dominated the national agenda for the NHS and our local agenda this year. I am delighted to say that this has resulted in real improvements. We made additional investment in both staff and equipment, we provided additional handwashing training for more than 4,000staff,andwesawayear-on-year25%reductioninMRSAcases.Ourrates compare well against national averages, and we intend to continue thisfocusthrough2008-09,workingtowards our target of no more than three cases per month. This figure also includes ‘community cases’, where patients are admitted with MRSA, but have it detected by our staff.
In terms of improving quality of care, we saw good progress in a vital clinical indicator. Our mortality rate has steadily reduced over recent years, and this trend continued, with our hospitals performing better than our selected peer group. This means that we have better results for patients than in comparable hospitals with a similar case mix. In comparison with the national peer group, our ratings have beenreducedfrom104in2004-05to
90in2007-08.Iamconfidentthatwewill continue to build on this progress. Our new ‘Lessons Learned’ clinical governance bulletin highlights both local and national case studies, to help us build on best practice. We joined the NHS North West Advancing Quality programme. And this year, like others, has seen an impressive list of clinical developments, some of which are detailed later in this report.
The conclusion to the public consultations Healthy Futures and Making It Better will help us guarantee the quality of our services into the future. Centres of excellence, with each hospital in the Trust supporting the others, will enable staff to ensure that they continue to meet ever-more challenging guidelines, standards and public expectations.
As a Trust we are one of the largest in England. We have the most accident and emergency attendances (nearly 257,000in2007-08),wehadthemostbirths(nearly11,000in2007-08),the fourth highest number of new outpatientreferrals(215,000)andthe third most bed days ( just over 603,000).
An important aspect of quality is timely access to our services. Patients waiting for treatment can often be in pain, or suffer anxiety or stress. Trust staff
Chief executive’s report

7have a well-deserved reputation for improving access for patients, and this againprovedthecasein2007-08.Atthe end of March 2008, the maximum waiting time for an outpatient appointment was five weeks. For those needing a diagnostic investigation just three patients were waiting more than seven weeks and for those needing surgery just three patients were waiting more than 12 weeks. The Trust also met the National 18 week Referral To Treatment target. In doing so we also reduced the number of patients on waiting lists, despite our hospitals being busier than ever. We also ensured that we maintained our standardthatinexcessof98%ofpatients attending our Accident and Emergency Departments were seen, assessed, treated and then admitted or discharged in under four hours.
What makes this success on ensuring timely access even more impressive is that this was achieved against a backdrop of some major disruption.
Following a fire safety risk assessment, some services from the Stonehill Block at Rochdale Infirmary had to be transferred to Fairfield General Hospital. The move itself was disruptive but went very smoothly and involved close working by staff at both hospitals with the PCTs and social service teams in both Rochdale and Bury. It
did however put major pressure on hospital services and I pay tribute to all of the staff for managing this imposed transfer of services in such a calm and professional way.
This winter’s diarrhoea and vomiting outbreaks were the most severe for a number of years and at the turn of the year many wards were closed to new admissions at all of our hospitals. The Royal Oldham Hospital was particularly badly affected.
In all of these cases, and in others, much less dramatic, our hospitals supported each other, using their combined resources to ensure that patients were able to continue to access services locally and in a timely manner.
The spirit of our staff in tackling issues such as these never fails to impress me and drives them in their work with patients. I regularly receive letters of praise for staff from patients, or their relatives, which emphasise this. Such letters overwhelmingly dominate my post bag rather than letters of complaint. That said, we do not always get it right and we are also committed to learning from complaints.
We have dramatically improved our performance in resolving complaints quickly. I am pleased to report that we
Chief executive, John Saxby (left) and Dr Ramesh Raja (now retired), site lead for radiology, look through the new £600,000 CT scanner at Rochdale Infirmary.

8have not only reduced the number of complaints received this year, but also the number of times when patients have felt the need to use our patient advice and liaison service.
We want to continue these improvements by making it easier for patients and service users to give us their views. This involves making sure that a wide range of communication methods are available but it also involves us taking a more proactive approach. Our Patient and Public Involvement work is one way of ensuring that we are increasingly involving patients in the planning of service development, ensuring that the patient voice is heard.
The positive feedback we receive from so many patients always reminds me that our hospitals do have good reputations for having provided the services needed by our patients for decades. I am pleased to say that their reputation is also growing across the NHS. National clinical directors have praised work carried out in our hospitals and we hosted a number of conferences which attracted delegates from across the country. The work of our staff was presented at national conferences and won national prizes.
To maintain this reputation we need to ensure that our staff have the
Promoting good health
facilities and equipment which enable them to provide the care needed. We have continued to invest in all of our hospitals. This year saw the installation of an £8.2 million system called PACS, which replaces traditional x-rays with instantly accessible digital images. A key part of the National Programme for IT, new systems were installed at The Royal Oldham and North Manchester General and upgrades to the existing equipment were made at Fairfield General and Rochdale Infirmary. This investment enables us to link to the national system, giving clinicians the ability to share images with colleagues across the country.
Patients have made it clear the criteria they will use to judge hospitals. I believe that this year has seen us deliver against these criteria, and I look forward to us building on this in the future.
John Saxby, Chief Executive
Chief executive’s report continued

9NationallytheNHSagendain2007-08was dominated by efforts to reduce the rate of healthcare associated infection (HCAI). This was mirrored by the Trust, which has this work as an absolute priority for all clinical and support staff.
The results were a reduction in the numbers of MRSA bacteraemias reported to the Health Protection Agencyfrom106in2006-07to79in2007-08;areductionofover25%.This lower figure was still above the trajectory set for the Trust. Of the 79,atotalof22werepre-48hour(or ‘community’ cases). In context,
the figure of MRSA cases per 10,000 bed days was reduced from 1.66 in 2006-07 to 1.31 in 2007-08. The Trust met its target for Clostridium Difficile (C.Diff ), with 531 cases recorded against a trajectory of 564. In context, the figure of C.Diff per 1,000 bed days was reduced from 0.93 in 2006-07 to 0.88 in 2007-08.
The Trust hosted an infection prevention summit on 30 November 2007, attended by more than 100 staff.
Professor Brian Duerden, inspector
Infection prevention progressof microbiology and infection control for the Department of Health, chaired the day and gave the keynote speech. Mary Moore, programme manager for the Department of Health’s Cleaner Hospitals Team, then outlined how their targeted support programme, which the Trust is included in, was operating. Other speakers included Dr Chris Booth, director of the Greater Manchester Health Protection Unit, and Simon Charlton, of Weightman's Solicitors, on legal perspectives. Derek Butler, chair of campaign group, MRSA Action UK, talked about the patient’s perspective.
Marian Carroll, director of nursing, took over the role of director of infection prevention from Dr Hari Panigrahi who was thanked by members of the Trust’s HCAI Improvement Board.
The Trust won a grant of more than £500,000fromtheDepartmentofHealth, which was used to support a specialist team of five senior nurses. These infection prevention sisters work across all Trust hospitals, supporting existing infection prevention staff and ward staff.
The grant also allowed for wider use of ChloraPrep, a sterilising solution used for skin preparation prior to taking blood.

✓10
Each case of MRSA is subject to a root cause analysis and is personally investigated by the chief executive and the director of nursing.
A programme was launched to provide additional handwashing training to staff, which has now been completed bymorethan50%ofstaff.Staffwhohave completed the training wear a ‘tick’ sticker on their ID badges.
A ‘bare below the elbows’ policy was introduced for staff during clinical work, making it easier for them to keep their hands clean.
Afurthergrantof£598,000supportedthe Trust’s deep clean work, and all wards had this work completed by the March 2008 deadline set by the Department of Health. A total of £97,000wasspentonnewmattresses,followinganaudit,and£13,500wasinvested in commodes.
Work continues to improve infection prevention measures, which will be assisted by a new visitor policy being introducedin2008-09.Thiswillseelimitations to existing visiting hours and other measures, making it easier to follow good hygiene guidance. The Trust will be holding a second infection prevention summit and will enter the third year of the national
Infection prevention progress continued‘Cleanyourhands’ campaign run by the National Patient Safety Agency.
In addition, we will continue to contribute to the national study to evaluate this campaign.
The Trust's five infection prevention performance sisters meet with colleagues.

11A series of clinical developments, led by our four divisions, saw us introduce new services to benefit patients, from preventative screening programmes to state-of-the-art surgical techniques.
Governance is the system which ensures the quality of an organisation’s work, highlighting areas where improvements are needed and ensuring that action is taken. The Trust saw improvements in both clinical and non-clinical governance this year, which drives up the quality of our care.
The Trust’s rate for mortality is assessed against a peer hospital group, with an index rating of 100. There was good progress in this area this year, with the Trust performing better than its peers –theratingof93inthefirstquarteroftheyearwasreducedto90inquarterfour.TheTrustindexfigureof90meansthattherateis10%lowerthanthenational rate for peer hospitals, once case mix is taken into account.
Clinical developments
Staff made significant progress in improving and developing services to patients through the year. Some of these achievements are detailed as follows:
• StafffromalloftheTrust’sclinicaldivisions, plus staff from support
directorates, contributed to the implementation workstreams of the Making It Better and Healthy Futures programmes, which aim to ensure the highest-possible quality of services for patients. The first major project was the work to develop plans for the women and children’s unit at North Manchester General Hospital. Work also began on planning for the level three neo-natal unit at The Royal Oldham Hospital, the first time this level of care has been available within the Pennine area.
• TheTrustachievedfurthersuccessin the UNICEF Baby Friendly programme, which recognises breastfeeding support for new mothers. The Royal Oldham Hospital successfully gained full re-accreditation, while Rochdale Infirmary and Fairfield General Hospital gained stage one accreditation. North Manchester General Hospital also holds full accreditation. This builds on previous work at the Trust, which has seen UNICEF describe us as ‘one of the most baby-friendly Trusts in the country’.
• A72-hourwardwasestablishedat Fairfield General Hospital in Ward2inDecember2007.Theward supports patients who can
beadmittedforlessthan72hours,if given appropriate intervention and support. Patients suitable for the ward are identified as they are admitted to the Emergency Admissions Unit, either from A&E or from GP referral. With daily consultant rounds and skilled nursing staff linking closely with occupational therapists, physiotherapists, social care staff and others, the ward was working well, with patients having an averagelengthofstayof66hours.
• TheRoyalOldhamHospital’sfirstnurse-led, transfer-of-care unit was opened this year to help ensure that patients are discharged as smoothly as possible from hospital. The16-beddedunitofferscaretopatients who no longer need to be treated in an acute ward setting but who still require nurse-led therapy. The unit, on Ward AI, benefits patients ranging from those with a newly-diagnosed illness to those adapting to new medication, or who need educating about their condition. Patients include those with deep vein thrombosis, leg ulcers and Parkinson’s Disease, as well as patients with diabetes and those requiring physiotherapy.
• InMarch2008,theTrustnominated Fairfield General
Clinical developments and quality of care

12Hospital to act as a primary stroke centre in support of the proposed hub and spoke model for Greater Manchester’s Integrated Stroke Service. The proposal, subsequently approved by the stroke network advisory group, will be supported by all stroke consultants in Pennine. The Trust views this as a chance to improve stroke services in units in all of our hospitals, and to improve outcomes for patients.
• WorkbetweentheTrust’ssurgicaland diagnostics divisions led to the introduction of a new keyhole surgery procedure which will help patients recover much more quickly. Endovascular Aneurysm Repair (EVAR) is carried out on patients who have an enlargement of their abdominal aorta (aneurysm).Morethan£150,000has been invested in new equipment to be able to carry out this procedure, which is at the leading edge of vascular surgery and interventional radiology. Previously, the only option to patients needing treatment would have been a major operation involving a large cut to the abdomen, followed by an average of 10 days’ stay in hospital, including some time in intensive care. The new procedure involves a small ‘keyhole’ incision in both groins to allow a graft to
be deployed under x-ray control to repair the aneurysm – it is suitable foraround60%ofpatients.Patients recover much quicker and are able to go home on average two days following treatment and do not usually require intensive care after the operation. This ground breaking service has come through an enthusiastic multidisciplinary team involving vascular surgeons Mr Dele Oshodi, Mr Matthew Hadfield and vascular interventional radiologist Dr Mahesh Kumar.
• FairfieldGeneralHospitalsuccessfullybecame part of the second wave bowel-cancer screening centres, as part of the national programme. The new service, which went live on 28 March 2008, is only the second of its kind in Greater Manchester and covers patients across the Pennine area. Bowel cancer is the second leading cause of cancer deaths, but regular screening can help to reduce the risk considerably – it identifies people who may be at risk but who may not have had any symptoms. To become a programme centre, the Trust had to achieve JAG (Joint Advisory Group on Gastrointestinal Endoscopy) accredita tion. Successfully gaining this involved assessment of the endoscopy pathway in all four Trust hospitals. In addition, the Trust also participated
in the national bowel cancer audit process.
• Theextracorporealshockwavelithotripsy service was established at Fairfield General Hospital in September2007,runningonedayper week. Initially it saw around four to five patients per week, but as the staff have gained experience, this has grown to eight per week. Lithotripsy is a non-invasive treatment for kidney stones and stones in the upper ureter. It means that patients who would previously have had invasive procedures do not now need surgery.
• Aspecialistpain-reliefserviceusingaprocess called cordotomy has been developed by the Trust – the largest of its kind in the north of England. The service has been developed by Dr Paul Cook, consultant in anaesthesia and palliative care at The Royal Oldham Hospital. The service assists terminally-ill patients with the asbestos-related cancer, mesothelioma. The disease can takeupto50yearstodevelopandexperts predict that cases nationally willriseto2,400ayearby2012,as the effects of exposure in the 1960sand1970sbecomeapparent.Cordotomy can help patients whose tumour is so serious that strong pain-killing drugs, such as morphine, are
Clinical developments and quality of care continued

Case study
1313poorly effective. The Oldham clinic will help meet the guidelines in the Department of Health’s Mesothelioma Framework document.
• TheNorthEastsectordrugsandtherapeutics committee was re-introduced this year. This committee is chaired by Dr Mike Finnegan, the Trust’s divisional medical director for the division of medicine. Composed of high-level representation from the Trust and the local PCTs, it is ideally placed to influence prescribing throughout the area.

The Trust’s strengths lie in cancer, infectious diseases, musculoskeletal and diabetes research and it contributes to several local and national programmes. An annual review on the Trust’s R&D activity was submitted to the Department of Health.
The Trust’s research and development (R&D) activity for the year included:
• researchprojectsinvolvingcollaborationwith12localand national universities. The Trust is actively involved in the Diabetes Local Research Network, the Stroke Local Research Network, Cancer Research Network and the Medicines for Children Network.
• DrDeepakBhatnagar,R&DDirector,wasappointedtorepresent all secondary care hospitals on the Greater Manchester Comprehensive Local Research Network.
He will also be responsible for any research infrastructure support relating to pathology matters in Greater Manchester. He continues as director of R&D at the Trust.
• asuccessfulR&Dannualprizedaywas held in October, attended by medical director Dr Ruth Jameson. Prizes were given by chief executive, John Saxby.
A number of developments took place this year to further our governance agenda, including progress on clinical and non-clinical issues.
• TheTrustestablishedanewclinicalaudit and effectiveness committee which includes both PCT and patient representation.
• Aweb-basedincidentreportingsystem was developed to simplify the reporting process thus encouraging an increase in both clinical and non-clinical incident reporting. The purpose of incident reporting is to enable the organisation to review the cause of any failings and put steps in place to ensure that they are not repeated.
• TheTrusthascontinuedtotrainstaff in the use of the National Patient Safety Agency’s Root Cause Analysis technique. This ensures that the more serious incidents are thoroughly and objectively investigated using a range of tools developed to ensure the root cause of the incident is identified and addressed.
• TheTrustgainedaLevel1ratingin the NHS Litigation Authority (NHSLA) Risk Management Standards for Acute Trusts.
GovernanceResearch and development14

15The assessment considered five standards, each containing ten criteria:
- governance- competent and capable workforce- safe environment - clinical care- learning from experience
The organisation was successful in demonstrating the Level 1 requirementsin45outof50criteria,againstapassmarkof40.
• TheTrusthasintroducedagovernance newsletter entitled ‘Lessons Learned’. Quarterly editions of the newsletter have included focus on blood transfusion, infection control and medication safety. The bulletin discusses both local and national examples of issues, with a view to promoting best clinical practice. Copies are widely circulated among clinical staff.
• FollowingaseriesofvisitsbytheHealth and Safety Executive to theTrustintheAutumnof2006,the Trust developed an action plan comprising a number of recommendations made by the inspectors. Through the year improvements made have included:
- Additional risk management training for clinical nurse managers and
directorate managers.- Trustwide security risk
assessments.- Purchase of personal security
alarms for Rochdale Infirmary A&E.- Development of a work related
stress steering group and announcement of a stress survey pilot.
- Improved capture of work related sickness and absence.
- Development of a manual handling assessment tool to prevent back injuries to staff.
- Development and roll out of a falls risk assessment.
- Improved compliance with the requirements of legionella national guidance.
With the relocation of medical beds to Fairfield from the Stonehill Block at Rochdale Infirmary, an improvement in environmental factors has been achieved, particularly relating to heating and environment.
• During2007-08itwasidentifiedthat protected teaching across the organisation needed to be co-ordinated to ensure that directorates and specialties could meet from across the Trust to work closer together developing the governance agenda. In October 2007,themedicaldirectoragreed
a set of six dates for protected teaching across the four hospital sites. Over the last few months the clinical audit department has supported the organisation of these dates and produced a generic formula for monitoring attendance, agenda setting and implementing appropriate co-ordination of support. Over the next 12 months the clinical audit department will monitor attendance and facilitate new developments during this pilot process.
• TheTrustpublishedaclinicalauditannual report which contains details of clinical audit and patient survey activity within the Trust duringtheperiod1April2006to31March2007.Clinicalauditmeasures ‘actual practice’ against ‘best practice’, highlighting improvement methods including training and education, protocols for patient treatment or other developments. The report, the third by the Trust, has a foreword by Dr Egware Odeka, clinical audit chair. The report focuses on projects completed during this period and describes any actions taken to improve patient care as a result of the audit findings.
• Thedivisionofmedicineundertooka radical review of clinical

FIG. 1 SUMMARY OF PERSONAL DATA RELATED INCIDENTS IN 2007-08
CATEGORY NATURE OF INCIDENT TOTAL
1 Loss of inadequately protected electronic equipment, devices or paper documents from secured NHS premises 9
2Loss of inadequately protected electronic equipment, devices or paper documents from outside secured NHS premises
9
3 Insecure disposal of inadequately protected electronic equipment, devices or paper documents 0
4 Unauthorised disclosure 17
5 Other 0
16governance. This involved a detailed review of each clinical directorate in turn, enabling a much clearer overview of issues within the division. Each directorate has been encouraged to develop its own risk register and was assessed on governance arrangements and reporting structure, activity, risks, training needs, audit and service developments. This cycle will be repeated from June 2008.
• TheTrustscoredaverageorbetterin18outof25categoriesin the Healthcare Commission’s maternity services survey. Our overall score was ‘fair’, but we were only marginally short of ‘better performing’. This rating is our aim for2008-9,withanaspirationof‘best performer’ by 2010.
• ThebiochemistrydepartmentatThe Royal Oldham Hospital received notification of its recommendation for accreditation by the Clinical Pathology Accreditation body (CPA). The inspection took place before the move to the central laboratory.
Personal data
The Trust takes information security very seriously, and has a series of safeguards in place.
Governance continuedThe Chief Executive of the NHS issued guidance to Trusts in relation to declaring incidents which involved the loss of potentially-identifiable personal data. Against the set criteria, none of the incidents involving Trust information were rated as being in the most serious categories – categories three to five. The Trust did have a number of incidents which were rated in the lower categories of zero to two. In line with the guidance, these are detailed in Fig.1. After each incident, processes were reviewed and action taken as required.
Standards for better health
In the declaration against the Standards for Better Health, the Trust declared thatithadmet41ofthe43corestandards for the entire year. Using
the criteria published to date by the Healthcare Commission, the Trust anticipated progress as “good” for service quality and “fair” for the use of resources.
In relation to the lapses identified in the two core standard parts not met forpartoftheyear,C14aandC14b(complaints handling), actions taken by the Trust have ensured that these have been rectified and compliance achieved within the year. Details of these standards, the nature and duration of lapses, and action plans are provided within this declaration.
The outcomes of actions taken toachievecompliancewithC14aandC14bweretestedbyanauditconducted in March 2008, and used to substantiate the declaration. In addition,theTrusthasachieved83%

17Improving the standard
17compliancewiththenational25dayscomplaints response standard during 2007-08,asignificantimprovementfrom55%complianceachievedin2006-07,andbetterthanthenationalbenchmarkof76%.
The Joint Health Overview and Scrutiny Committee, the Patient and Public Involvement Forum, the North West Strategic Health Authority and the four local Safeguarding Children Boards were invited to provide independent comment about the Trust’s performance against core standards based on evidence available to them. These comments are included verbatim on the Trust’s declaration, along with responses from the Trust.
Assurance Framework and Statement of Internal Control
The Trust continued to develop its assurance framework in order to inform the annual statement on internal control (see page 58).Non-executivedirectorsand executive directors from the Trust’s Board review the framework, which is also reviewed at the Trust Board and the governance and risk committee.

18
FIG. 1 ATTENDANCE BY BOARD MEMBERS
NON-EXECUTIVE DIRECTORS
John Jesky John Battye Tim Pickstone Haydn Griffith Michael Holly Anne Unwin Razia Shamim
11/11 8/11 10/11 10/11 11/11 9/11 7/11EXECUTIVE DIRECTORS
John Saxby* Bob Chadwick** Marian Carroll Karen James Dr Ruth Jameson Roger Pickering John Wilkes
8/9 8/8 9/11 10/11 10/11 11/11 10/11* Commenced employment 4/6/2007** On secondment – September 2007 to December 2007
The Trust BoardThe Trust Board had 11 meetings in 2007-08,withattendancebyBoardmembers as indicated in Fig. 1.
BOARD SUB-COMMITTEESIn2007-08,theTrustBoardhadsixformal sub-committees and a standing committee which has been established to take forward the FT development project. Audit committee
Chair: Michael HollyThe sub-committee:• reviewsreportsfrominternaland
external audit.• reviewscompliancewithSecretary
of State directives for countering fraud.
• reviewsthesystemofintegratedrisk, governance and internal control.
• monitorscompliancewithstandingorders and SFIs.
• receivesandapprovesannualaccounts.

releasing efficiency savings and any in-year changes made thereto, and recommends their approval to the Trust Board.
HR committee
Chair: Haydn GriffithThe sub-committee:• considersandtakesforwardHR
strategy.
Governance and risk committee
Chair: Anne UnwinThe sub-committee:• assurestheTrustBoardof
performance against governance targets.
• managestheassuranceframework,corporate risk register and governance development plan.
• considersinformationgovernance.
Remuneration committee
Chair: John JeskyThe sub-committee:• makesrecommendationstothe
Trust Board on remuneration and terms of service of executive directors and senior employees.
• reviewsarrangementsfortermination of employment and other contractual terms.
Endowment committee
Chair: John BattyeThe sub-committee:• ensuresoperationofthecharity
within the terms of its governing documents.
• reviewsandapprovescharitablefunds’ accounts for the year.
Review of the Board and its sub-committeesThe Trust Board considered a revised sub-committeestructurefor2008-09,which included a re-definition of the role of non executive directors within the structure.
Having appropriate governance arrangements for the Board and sub-committees is a key part of the process of ensuring that the mechanisms of control are fit for purpose as part of the Trust’s moves towards a future FT application. This is in line with guidance from Monitor and the experience of existing FTs.
The review indicated that it was appropriate for:• dis-establishmentofthefinanceand
human resources & organisational development sub-committees, their work being scrutinised through alternative mechanisms.
• achangeinthegovernancearrangements for risk management and clinical governance. This saw the creation of a risk management committee and clinical governance committee to replace the governance and risk committee.
The Trust Board had 11 meetings in 2007-08,withattendancebyBoardmembers as indicated in Fig. 1.
BOARD SUB-COMMITTEESIn2007-08,theTrustBoardhadsixformal sub-committees and a standing committee which has been established to take forward the FT development project. Audit committee
Chair: Michael HollyThe sub-committee:• reviewsreportsfrominternaland
external audit.• reviewscompliancewithSecretary
of State directives for countering fraud.
• reviewsthesystemofintegratedrisk, governance and internal control.
• monitorscompliancewithstandingorders and SFIs.
• receivesandapprovesannualaccounts.
Finance committee
Chair: John JeskyThe sub-committee:• monitorstheperformanceofthe
Trust through a monthly report and any other ad hoc reports considered necessary, and reports on this to the Trust Board.
• reviewsrevenuebudgetsfortheyear, including planned cash-
19

The Trust Board continuedFurther work was needed to reform the supporting infrastructure for these arrangements.
• clearertermsofreferencefortheBoard and all sub-committees, laying out membership and reporting arrangements.
The revised sub-committee structure is as follows:Audit committee
Chair: non-executive directorThe sub-committee:• reviewsreportsfrominternaland
external audit.• reviewscompliancewithSecretary
of State directives for countering fraud.
• reviewsthesystemofintegratedrisk, governance and internal control.
• monitorscompliancewithstandingorders and SFIs.
• receivesandapprovesannualaccounts.
Clinical governance committee
Chair: medical directorThe sub-committee:• givesdirectiontoandagreesclinical
governance priorities.• agreessystemsandprocessesto
ensure quality in clinical care.
Risk management committee
Chair: chief executiveThe sub-committee:• overseesthedesignandeffective
operation of risk management processes across the Trust, including the management and production of the assurance framework.
Remuneration committee
Chair: chairmanThe sub-committee:• makesrecommendationstothe
Trust Board on remuneration and terms of service of executive directors and senior employees.
• reviewsarrangementsfortermination of employment and other contractual terms.
20

Endowment committee
Chair: non-executive directorThe sub-committee:• ensuresoperationofthecharity
within the terms of its governing documents.
• reviewsandapprovescharitablefunds and accounts for the year.
Nominations committee
This sub-committee is to be established once the Trust is a FT.
21

6000700080009000
1000011000120001300014000150001600017000
Apr
-05
Jun-
05
Aug
-05
Oct
-05
Dec
-05
Feb-
06
Apr
-06
Jun-
06
Aug
-06
Oct
-06
Dec
-06
Feb-
07
Apr
-07
Jun-
07
Aug
-07
Oct
-07
Dec
-07
Feb-
08
TOTAL NUMBER OF PATIENTS WAITING FOR AN INPATIENT OR DAYCASE PROCEDURE
22Trust staff have once again delivered key access times year on year to our services, both for planned treatment and for unplanned or emergency care. They have either met or beaten national targets. Improved access has direct benefits to patients, as those waiting for procedures or treatment may be anxious, uncertain or in pain. A total of 19ofthe21accesstargetsreportedto the Trust Board were achieved in 2007-08.
This achievement comes against a rise in activity – although the number of patients using A&E was down slightly (255,234comparedwith256,332in2006-07,adropof0.4%),thenumberof admissions rose. Unplanned activity (non-electiveoremergency)was2.6%(2,516FFCEs)higherthanin2006-07,and4.6%(4,412FFCEs)abovetarget.In addition, there was more planned activity this year, both for inpatients and for outpatients. Elective activity (which includes both day case and electiveFFCEs)was6.4%(5,804FFCEs)higherthanin2006-07,and1.6%abovetarget(1 556FFCEs).Thenew outpatient target was exceeded by 4.8%(7,560attends)andwas1.4%(2,274attends)abovetarget.
Against that background, Trust staff delivered key access targets and also ensured that the Trust remains on track to achieve the 18 Week target.
Atotalof98.1%ofpatientswereable to access emergency treatment through Trust A&E departments and the local walk-in centres within the four-hour waiting standard. This passedthenationalstandardof98%.
InApril2007,morethan1,600patients were waiting more than 11 weeks for their planned treatment. By March 2008 that figure was five patients. Although not a national target, the number of patients waiting for planned treatment was reduced by 22%,from10,690to8,289.
InApril2007,morethan3,000patients were waiting more than five weeks for their outpatient appointments. By March 2008 that figure was nine patients.
Trust staff and colleagues at The ChristieHospitalensuredthat98%ofpatients received their first treatment within62daysofanurgentcancer
referral, against the national standard of95%.Duringtheyear,therewasjusta single breach of the standard of all urgent cancer referrals from GPs being seen within two weeks. All patients startedtheirtreatmentwithin31daysof the decision to treat being made, in line with the national standard.
Improving accessibility to diagnostic tests is key to improving access for treatment and Trust staff excelled in thisarea.InApril2007,atotalof2,664patients were waiting more than six weeksforthe15nationallyreportedtests, which include magnetic resonance imaging (MRI) and computerised tomography (CT) scans. By March 2008, the figure was 11 patients.
Another key point was ensuring that patients can access genito-urinary medicine (sexual health) clinics within two working days. A major investment programme saw performance increase dramatically between February and
Improving access

0200400600800
10001200140016001800
Apr
-07
May
-07
Jun-
07
Jul-0
7
Aug
-07
Sep-
07
Oct
-07
Nov
-07
Dec
-07
Jan-
08
Feb-
08
Mar
-08
0500
100015002000250030003500
Apr
-07
May
-07
Jun-
07
Jul-0
7
Aug
-07
Sep-
07
Oct
-07
Nov
-07
Dec
-07
Jan-
08
Feb-
08
Mar
-08
er ef Pat ait wee mo n ie oin
NUMBER OF PATIENTS WAITING 13 WEEKS OR MORE FOR AN INPATIENT OR DAYCASE PROCEDURE
NUMBER OF GP REFERRED PATIENTS WAITING 5 WEEKS OR MORE FOR AN OUTPATIENT APPOINTMENT
April2007.TheApril2007figureof71%wasfurtherimproved,sothatbyMarch2008,atotalof81%ofpatientswere being seen within two working days.Atotalof98%ofpatientswereoffered appointments within two working days.
The two access targets which the Trust did not meet both related to cancelled operations. Despite reducing the number of planned operations cancelledonthedayfrom1.26%foryearendingMarch2007comparedto1.03%inMarch2008,thisdidnotmeetthenationaltargetof0.8%.Improvements were undertaken which saw an improvement from January 2008, and this work will continue.
Best foot forward to improve access
23

% PATIENTS TREATED WITHIN 18 WEEKS: ADMITTED
% PATIENTS TREATED WITHIN 18 WEEKS: NON-ADMITTED
0%20%40%60%80%
100%
Apr-0
7
May
-07
Jun-
07
Jul-0
7
Aug-
07
Sep-
07
Oct-0
7
Nov
-07
Dec-
07
Jan-
0 8
Feb-
08
Mar
-08
s T eate i hin Weeks: A i
0%20%40%60%80%
100%
Apr-0
7
May
-07
Jun-
07
Jul-0
7
Aug-
07
Sep-
07
Oct-0
7
Nov
-07
Dec-
07
Jan-
08
Feb-
08
Mar
-08
24In addition, the Trust did not meet the target for the number of patients whose cancelled operations were rescheduled within 28 days. The Trust figure of 5.9%didnotmeetthenationalstandardof5.0%.Howeverthisfigurestillrepresents a significant downward trend over recent years, which saw figures as highas30%,despitefeweroperationsthen taking place.
The Trust met key milestones marking progression to meet the national standard that, by December 2008, patients will wait no more than 18 weeks from referral to the start of theirtreatment.InMarch200893%of admitted patients (elective patients whose treatment is delivered through an inpatient or day case episode) and 88%ofnon-admittedpatients(electivepatients whose treatment is delivered in outpatient appointments) began their treatment within 18 weeks of referral. The national standard of December 2008isthat90%ofadmittedpatientsand95%ofnon-admittedpatientsmustreceive treatment within 18 weeks.
Quick access to diagnostics tests are essential to facilitate the 18 week target. Through the year, the Trust’s radiology directorate reduced the waiting time fortestsfrom13weekstoamaximumof six weeks. This was achieved with the support of our hard working radiographers and radiologists who
have worked tirelessly throughout the year.Theaimfor2008-09istoreducethe waiting times to a maximum of two weeks. The radiology directorate is also developing plans throughout the coming months to extend the working day in some areas to increase convenience and choice for patients.
A major investment in the service enabled the Trust to increase the number of clinics being held, with access times improved as a result. For adults, the maximum waiting times for new routine appointments has fallen asfollowsfromDecember2007toApril 2008:• NorthManchesterGeneralHospital -36weeksto5weeks• TheRoyalOldhamHospital -13weeksto2weeks
Improving access continued
• RochdaleInfirmary -36weeksto14weeks• FairfieldGeneralHospital -27weeksto8weeks.
For children, the maximum waiting times for new routine appointments has fallen as follows from December 2007toApril2008(NorthManchesterGeneral Hospital does not currently provide children’s services):
• TheRoyalOldhamHospital -8weeksto4weeks• RochdaleInfirmary -13weeksto2weeks• FairfieldGeneralHospital -19weeksto7weeks.

Val Finigan, the Trust’s infant feeding co-ordinator
with her MBE at Buckingham Palace.
25• ImprovementsintheTrust’s
thrombolysis care was featured at the seventh Annual Spring Meeting on Cardiovascular Nursing, entitled: “Changing Practice to Improve Care”. The event, which was held at Manchester’s Bridgewater Hall, included UK and international speakers. Joanne Whitmore, thrombolysis co-ordinator at Fairfield, gave a presentation entitled ‘Co-ordinating Thrombolysis and Improving Time to Treatment’. Rochdale Infirmary and The Royal Oldham Hospital held the first and second places in terms of national performance, with North Manchester General and Fairfield showing substantial improvements. Successful development of the services across the Trust had, in part, been achieved by ensuring flexibility and using slightly different working models to ensure that each sites’ needs were met.
• DrSueRoberts,thenationalclinicaldirector for diabetes, praised the work of Trust and primary care trust staff throughout the North East Sector Diabetes Network. The network was one of just three sites selected nationally to pilot the new Diabetes Commissioning Toolkit for the NHS. The project is looking at how to ensure that diabetes
Our growing reputationPresentations at conferences of work done at the Trust, external recognition and winning awards are all signs of the growing reputation of the Trust’s hospitals. Several initiatives and achievements by the Trust’s clinical teams and individuals were marked externally in a number of ways through the year. These include:
• ValFinigan,theTrust’sinfantfeeding co-ordinator, was awarded a MBE in the New Year’s Honours list, which marked her work in successfully leading our UNICEF
Baby Friendly programme. The breastfeeding rate at both The Royal Oldham Hospital and North Manchester General Hospital doubled after they were accredited. Val has also introduced a clinic for babies suffering from ‘tongue tie’, a condition which can hinder breastfeeding. Parents from across the North West attend with their babies for the simple procedure.
• TheTrust’smidwiveswhodeveloped a pioneering service to help pregnant teenagers were commended in the Services to Disadvantaged Groups category of the All-party Parliamentary Group on Maternity. The Trust has three teenage pregnancy midwives - Pat Lowe, at Rochdale Infirmary, Deb Jones, at Fairfield, and Janine Brooks, at The Royal Oldham Hospital. The service helps around 300womenayear.
• NHSchiefexecutiveDavid Nicholson visited Fairfield’s stroke unit following the publication of the latest National Stroke Sentinel Audit, which gave it the highest rating in the North West, and the third highest nationally. All of the Trust’s units significantly improved their ratings in the audit, which was publishedinApril2007.

Dr Mahesh Kumar, clinical director for radiology, checks out the new picture archiving and communication system (PACS), which replaces traditional x-ray film with a digital image which can be viewed on computer screens. Picture: Oldham Evening Chronicle
26services meet the needs of patients, and will be used to provide a framework for other NHS diabetes services to work from.
• TheworkoftheTrust’smaternityand critical care staff in developing an Early Warning Scoring System (EWS) for maternity services was highlighted at ‘Safe Delivery – Reducing Risk in Maternity Services in a Time of Change’. This national conference was hosted by the Healthcare Commission and the National Patient Safety Agency in LondoninJune2007.ChristineO'Loughlin, senior midwife, clinical governance/contact supervisor of midwives, and Jackie Hogan, nurse consultant critical care, gave the presentation. The system was developed from an existing scheme used in general wards to highlight patients at risk of developing an acute/critical illness.
• TheRoyalOldhamHospitalwaschosen for the first time to host the Intercollegiate MRCS examination of The Royal College of Surgeons of England. The hospital hosted the third and final part of the exam – testing communication and clinical skills – for candidates who had already passed written and oral tests at The Royal College of Surgeons in London.
• Twospecialistnurseswonaprizeat an international conference for developing a new bandage policy. Nurse consultant in tissue viability, Judy Harker, is based at The Royal Oldham Hospital, while vascular nurse specialist, Debbie Ruff, is based at North Manchester General Hospital. They led work to introduce a single type of bandage for wounds across the Trust’s hospitals and improve the knowledge and skills of staff in applying them. The project won a prize at the European Wound Management Association (EWMA) conference in Glasgow, ahead of 200 other entries.
• PaulBarker,theTrust’sleadclinicalspecialist radiographer, won the Alan Nichols Memorial Award at the UK Radiological Congress for a year-long study comparing the effectiveness of carrying out ‘hot’ readings (reporting on x-ray tests when patients are still at the hospital) with that of ‘cold’ ones (when patients receive their results after being discharged). His work was subsequently presented at the Mediterranean Emergency Medicine Congress in Sorrento, Italy, which draws hundreds of delegates from hospitals across the whole of Europe.
• Morethan100doctorsandnurses from across the country attended a conference entitled ‘Paediatric Update’ which was hosted at Fairfield General Hospital inNovember2007.Thetwo-dayevent, arranged by consultant paediatrician Dr Umesh Prabhu, included a key note speech by Professor Patricia Hamilton, president of the Royal College of Paediatricians.
Our growing reputation continued

Internal awardsThe Trust runs a number of internal awards, aimed at acknowledging the contributions and success of staff from all disciplines.
Simone Gorman won the Trust’s Nurse of the Year Award. Simone works on the children’s unit at Rochdale Infirmary. She is the placement educational lead for the unit, working with student nurses as they gain experience.
Kath Sanderson, from Rochdale Infirmary, won the Midwife of the Year Award. Kath trained and worked as a general nurse before commencing
as a community midwife at Rochdale in1984.Shemorerecentlytookon additional child protection responsibilities.
Susan Brierley, labour ward practitioner at The Royal Oldham Hospital, won the Staff Innovation Award for her suggestion on how to use labels from blood product bags in patients’ notes. The suggestion was being considered as part of broader blood bank work.
The Team Innovation Award was won by 18 medical secretaries from the Trust’s four hospitals. The
medical secretaries, who all work for the division of surgery, received their award for work as professional development facilitators under the NHS Knowledge and Skills Framework.
Catherine Holt, a 21 year old student midwife at Fairfield General Hospital, won the Catherine Barrett Young Achievers’ award, her nomination citing her professionalism and motivation. The award is open to any young personagedbetween16and21whoworks for the Trust or the local PCTs.

Marking the start of endovascular aneurysm repair (EVAR) procedures at The Royal Oldham Hospital are (from the left), Mr Neil Hulton, divisional medical director for surgery; Dr Mahesh Kumar, clinical director for radiology; Mr Tim Barrett, superintendent radiographer and Mr Dele Oshodi, vascular consultant surgeon.
2828

29The Trust invests heavily in facilities and medical equipment to ensure that we can provide the highest-possible quality of care. In addition, having good working conditions helps us attract hard-to-recruit staff.This year saw the successful completion of many major projects, and the start of others.
Thenew£17.5mcentrallaboratoryatThe Royal Oldham Hospital became fully operational with the completion of offices and staff facilities. The laboratory, one of the largest in the country, will help meet the growing demand for pathology tests by hospital clinicians and GPs across the Pennine area. The NHS Medical Director, Professor Sir Bruce Keogh, officially opened the laboratory.
The£1.3mVictoriaSuiteoutpatientsunit for breast care patients opened at The Royal Oldham Hospital, with patients, staff and guests taking part in a pink balloon release. The unit creates a ‘one stop’ outpatients service for patients from Rochdale and Oldham, including the development of a herceptin service on-site. Miss Maria Bramley, a new breast surgeon who specialises in reconstructive surgery, joined the service.
Work was also completed on a centralised medical records building at
Investing in our hospitalsThe Royal Oldham Hospital, plus a new mortuary and forensic suite for use by Home Office pathologists.
The£400,000investmentinnew equipment for the Hospital Sterilisation and Disinfection Unit at The Royal Oldham Hospital ensured that the unit is well-placed to meet the rising standards demanded by EU regulations. The unit serves The Royal Oldham Hospital, plus Rochdale Infirmary, Birch Hill Hospital and community services in Oldham and Rochdale. The funding paid for state-of-the-art sterilisation and disinfection facilities, including a washer disinfector and five sterilisers. The unit sterilises clinical instruments and devices, ranging from minor operation packs used by GPs to complex orthopaedic kit used in hip surgery.
Enabling works also began on the £32millionwomenandchildren’sdevelopment at North Manchester General Hospital, a key part of the regional Making It Better programme.Rochdale Infirmary saw work begin on the installation of a new CT scanner. The£600,000machinewillbethemost powerful NHS-owned CT scanner in Greater Manchester when it begins operating in summer 2008.
Following last year’s tendering process, the Birch Hill Hospital site was
handed over to Persimmon Homes in April2007.AsmallnumberofTrustservices, including ophthalmology currently remain on the site, but will transfer in due course.
The disposal of the Westhulme site was suspended following advice from the Trust’s advisors because of conditions in the property market. While the intention remains to dispose of the site, in the short-term it will be used to help provide extra parking spaces for staff at The Royal Oldham Hospital, which has considerable pressure on its car parks.
Technological developments underpin the success of clinical advances, and this year saw the Trust invest heavily in IM&T (Information management and technology).
The main development of the year was the delivery of the National Programme for IT (NPfIT) Picture Archiving and Communication System (PACS) and the Radiology Information System (RIS). PACS replaces the traditional X-ray film with a digital image, which can be viewed on computer screens in wards and easily shared between clinicians.RIS schedules and records activity and examinations in radiology departments. Previously the Trust had four separate systems, but a single system interfaces with both PACS and the Patient

30Administration System, to link to up-to-date patient information.
The Trust invested £8.2m in the systems, which offer a range of benefits, including:• Imagemanipulationduringreading/
reporting• Theabilitytodistributeimages
more effectively and quickly, including viewing them at many locations immediately after their release, for further clinical opinion if required.
• Staffcancheckthequalityoftheimage immediately so patients do not have to be called back for a re-scan, as can happen with traditional radiology.
• PACScutsthetimeittakesfor patients to receive results, minimising concerns and improving access times. The system also means that patients do not have to carry their films around the hospitals.
Two of the Trust’s hospitals, Fairfield General Hospital and Rochdale Infirmary, had existing PACS systems, but these required upgrading to be compatible with the new national system. The system replaced x-ray films at The Royal Oldham Hospital and North Manchester General Hospital.This programme involved a major team effort for radiology and IM&T staff
across all sites. A substantial clinical engagement programme supported this work, with training also provided online. The programme is now being highlighted by NPfIT representing the successful implementation of a major scheme with clinical involvement.
Otherachievementsin2007-08include:• Provisionofaccesstoradiological
images from home for on call radiologists.
• Electroniccommunicationoftyped discharge summaries to GP practices through the introduction of a digital dictation on wards.
• DeploymentofITtosupportthemusculoskeletal clinical assessment and treatment centre at Sunnybank Health Centre in Bury.
• ImplementationoftheGPsummaryrecord at Fairfield A&E as part of the Bury PCT early adopter project.
• AwardsfromiSOFTfora‘proactiveapproach to supporting Choose and Book’ and from CHKS, highly commended for ‘data quality’.
• ImplementingNHSguidanceissuedon safeguarding personal data stored in electronic form.
Investing in our hospitals continued

31Mission statementThe Trust Board has adopted a revised mission statement to sit above the current organisational values. The mission statement and values have a longer life than the annual corporate objectives, but all three are linked. The annual corporate objectives have been cascaded throughout the organisation for interpretation at divisional, directorate, team and individual level.
The Trust Board has agreed a new mission statement, which is:
“To provide the very best care for each patient on every occasion.”
This mission statement will drive the achievement of all objectives from the corporate to the team and individual level.
Organisational values The Trust has been through an inclusive and valuable process to establish a set of organisational values. Work willacceleratein2008-09toembedthese values within the organisation in tandem with the organisational development work needed to deliver reconfiguration. The values are:
Patient care is at the centre of everything we do. We work together to deliver a high quality service to provide the best possible outcome for patients.
Mission statement, values and corporate objectivesAccountability, honesty and integrity are keys to our success both individually and across the Trust. Treating everyone with respect and promoting good working relationships will support individuals in reaching their full potential.
Strategic aims
Aspartofthediscussionsin2007-08about the development of an integrated business plan, it was agreed to adopt a set of strategic aims which would offer a framework for future business and service development.
These strategic aims are: • TheTrustisaproviderofsecondary
healthcare services.
• TheTrustprovidesanumberoftertiary (specialist) services and will continue to develop these in line with demand. The development of new specialist services will be considered depending on the financial and clinical viability of the proposal.
• TheTrustwilldevelopservicesinprimary care where this makes clinical and financial sense.
• TheTrustwillbuilduponitsbrandas a NHS provider.

1As a minimum, performance of ‘Good: Good’ in Healthcare Commission standards, including ‘Vital Signs’ and Level 3 in Auditors’ Local Evaluation (ALE)
2 Access, including 18 Weeks wait and 4 hours A&E target
3 Maintain financial strength
4 Reduction in healthcare associated infection (HCAI)
5 Improving the patient experience
6 Improving the staff experience
7 Reduction in health inequalities
8 Improve patient safety
9 A step change in the way we work, leading to a lasting improvement in the productivity and efficiency of our hospitals
10 Improve the quality of care delivered in our hospitals, including improving the patient pathway
11 Prepare for a successful Foundation Trust application
12 Deliver successful first reconfiguration moves
13 Deliver a redevelopment plan for North Manchester General Hospital
14 Commence the construction of the Christie at Pennine development
15 Build our external relationships with key stakeholders, especially GPs
TABLE 1 DELIVERY OF NATIONAL STANDARDS
DELIVERY OF LOCAL PRIORITIES
32
Corporate objectives 2008-09
The Department of Health has published guidance within ‘The OperatingFramework2008-09’,which details the national priorities the government expects the NHS to deliver next year. These are summarised into five national priority categories:
• Improvingcleanlinessandreducinghealthcare associated infections.
• Improvingaccessthroughachievement of the 18-week referral to treatment target.
• Keepingadultsandchildrenwell,improving their health and reducing health inequalities.
• Improvingpatientexperience,staffsatisfaction, and engagement; and
• Preparingforastateofemergency,such as an outbreak of pandemic flu.
The Trust’s corporate objectives for 2008-09arestructuredintotwoparts:
1 Delivery of nationally defined priorities and ‘must-dos’; and
2 Delivery of locally defined objectives, informed by local commissioning intentions and Trust priorities, as agreed by the Board.
Mission statement, values and corporate objectives continued

1As a minimum, performance of ‘Good: Good’Delivery of relevant ‘Vital Signs’Level 3 in ALE
As indicated
As indicatedAs indicated
2 Access including 18 weeks wait and 4 hours A&E target
Monthly performance trajectories met
3 Financial Strength
Breakeven taking one year with anotherAchieve External Finance LimitAchieve 3.5% return on capital employedAchieve Capital Resource Limit
4 Reduction in HCAI Monthly trajectory exceeded
5 Improving the patient experience
Improvements in annual patient satisfaction survey resultsReduction in number of complaintsReduction in delayed transfers of careReduction in operations cancelled for non-clinical reasonsReduction in outpatient appointments cancelled by hospital
6 Improving the staff experience
Improve outcomes in annual staff survey‘Delivery against Single Equality Scheme Action Plan’ Reduction in incidents of verbal, racial and physical assaultReduction in use of locum medical consultants
7 Reduction in health inequalities
Improvement in health community standardised mortality ratio Improved communication on health issues, e.g. smoking, alcohol, obesity, teenage pregnancy and cancer awarenessIncrease in organs donated for transplantation
8 Improve patient safety
Reduction in the number of patient slips, trips and fallsProvide training for Corporate Manslaughter / Homicide BillSerious untoward incidents managed appropriately according to defined timescales
9A step-change in the way we work, leading to a lasting improvement in the productivity and efficiency of our hospitals Improvement in day case rate
Improvement in theatre utilisationReduction in pre-operative bed daysReduction in Outpatient Did Not Attend rateReduction in average length of stay
TABLE 2 OBJECTIVE SUCCESS CRITERIA
3333
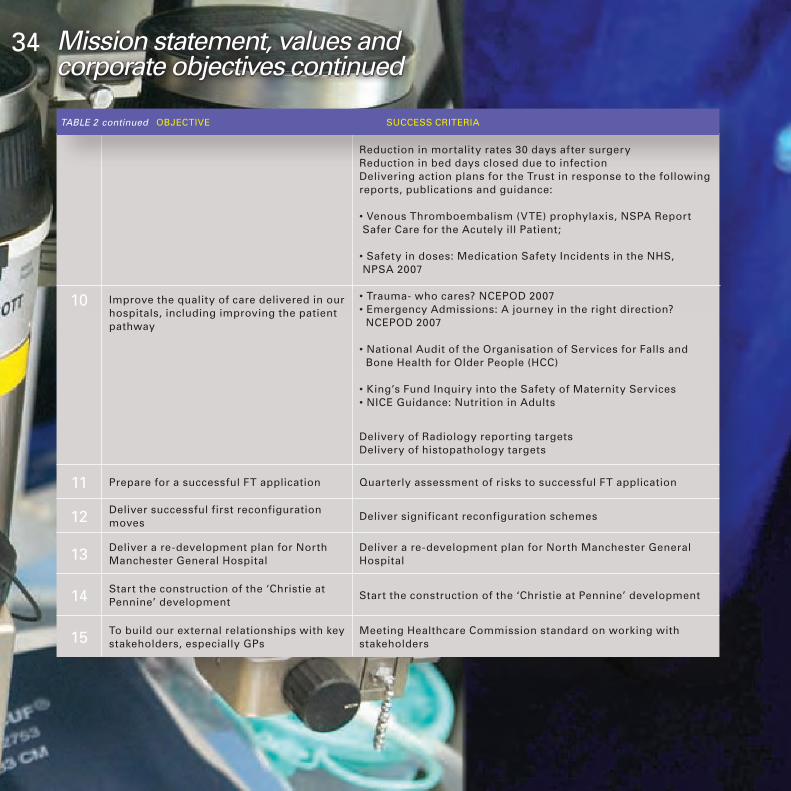
10 Improve the quality of care delivered in our hospitals, including improving the patient pathway
Reduction in mortality rates 30 days after surgeryReduction in bed days closed due to infectionDelivering action plans for the Trust in response to the following reports, publications and guidance:
• Venous Thromboembalism (VTE) prophylaxis, NSPA Report Safer Care for the Acutely ill Patient;
• Safety in doses: Medication Safety Incidents in the NHS, NPSA 2007
• Trauma- who cares? NCEPOD 2007• Emergency Admissions: A journey in the right direction? NCEPOD 2007
• National Audit of the Organisation of Services for Falls and Bone Health for Older People (HCC)
• King’s Fund Inquiry into the Safety of Maternity Services• NICE Guidance: Nutrition in Adults
Delivery of Radiology reporting targetsDelivery of histopathology targets
11 Prepare for a successful FT application Quarterly assessment of risks to successful FT application
12 Deliver successful first reconfiguration moves
Deliver significant reconfiguration schemes
13 Deliver a re-development plan for North Manchester General Hospital
Deliver a re-development plan for North Manchester General Hospital
14 Start the construction of the ‘Christie at Pennine’ development
Start the construction of the ‘Christie at Pennine’ development
15 To build our external relationships with key stakeholders, especially GPs
Meeting Healthcare Commission standard on working with stakeholders
TABLE 2 continued OBJECTIVE SUCCESS CRITERIA
3434 Mission statement, values and corporate objectives continued

35
Theannualcorporateobjectivesinthe2007-08planwerebuiltonnational and local planning and performance frameworks and linked intothedevelopmentofafive-yearintegrated business strategy.
The table shown on the following pages details how the Trust performedagainsttheseobjectives.
ObjectivesfortheTrust’sclinicaldivisions and support directorates are shaped by these strategic objectives,andcontributetotheirdelivery.
Strategic corporate objectives for 2007-08
Key Operating Parameters
• The issues the Trust faced during 2007-08 included:- Acontinuedverychallengingfinancialpositiontoachieverecurrent
financialbalancein2007-08;- DiscussionswithPCTandpracticebasedcommissionersonthe
development of service level agreements, which reflected actual activitycarriedoutandmovementtowardsdeliveryofthe18weekstarget;
- Trustresponsetothecontinueddevelopmentoftheindependentandthirdsectorprovidersandbusinessopportunitiesassociatedthereof;
- ContinuedmaintenanceofperformanceandHealthcareCommissionassessmentstandards;
- FollowingthefinaldecisiononMakingItBetterandHealthyFutures,theTrusthasnowstartedtoturnthehigh-levelplansintodetailedimplementation strategies, with milestones and risk management plans;
- Thecontinuingimplementationoforganisationaldevelopmentplans;- Continuedplanninganddecisiononthetimeframeforapplicationto
becomeaFoundationTrust;and- Continuedcapitaldevelopment,includingvacatingtheBirchHill
Hospital site, completion of the central pathology department and securing capital for the North Manchester General Hospital’s women and children’s development.
35

Excellent quality and accessible clinical care
1 We want to achieve the aims and targets of the NHS Plan and NHS Improvement Plan, including quicker and easier access to services, improved outcomes and quality of care, together with a reduction in health inequalities.
• Achievement of Healthcare Commission targets that, on average, exceed those of our competitors.
• Following the decision on “Healthy Futures” and “Making it Better”, work with our PCT partners to formulate and agree “roadmap” for implementation.
• Achievement of 2007/08 targets and LDP trajectories.
Specific progress in four key development areas:
• Tomeetlocallyagreedmilestonesto ensure that no-one waits more than 18 weeks from GP referral to hospital treatment by the end of 2008. Specific targets in-year are: (i) 85% achievement for admissions by March 2008; and (ii) 90% for those not admitted.
• Toachieveyearonyearreductionsin MRSA levels as agreed in LDPs and for locally agreed targets for CD and other infections.
• Toworkwithhealthpartnerstodeliver services that make the most progress in reducing health inequalities and promote health and well-being. A specific target is to ensure that by 2008 anyone referred to a genito-urinary medicine (GUM) clinic should have an appointment within 48 hours
It is anticipated that the Trust will improve its service quality rating from “fair” to “good”.
The “roadmap” was completed, project leads were appointed and business cases are being developed for reconfiguration process.
The Trust achieved the required level of performance for March 2008.
The Trust achieved the required level of performance for March 2008.
The Trust exceeded the target for MRSA of no more than 38 cases for the year-end; however it remained within target for C.Diff performance.
The Trust has a smoke free environment policy and continued to work with PCTs to achieve their smoking targets. With regards to obesity, healthy eating was incorporated in all hospital restaurants.The Trust met the GUM targets.
CATEGORY OF STAKEHOLDER REQUIREMENT
STRATEGIC OBJECTIVES
SUCCESS TOBE MEASURED BY:
PROGRESS TO YEAR END
36 Strategic corporate objectives for 2007-08 continued

Excellent patient experience
2 We want to be the provider of choice for secondary health care services for our local community.
• Working to ensure that every hospital appointment is booked for the convenience of the patient by 2008 (by continuing the implementation of Choose and Book) and that the Trust is the preferred option from the choice of four providers from April 2007 onwards.
• We want patients to choose Pennine Acute Trust for their care. In order to promote our services we will build on the patient survey results and other work to ensure we are delivering what patients want.
• Cancer waits – the national target was to ensure sustained delivery of a maximum waiting time of two weeks from GP urgent referral to appointment, two months from GP urgent referral to treatment and one month from diagnosis to treatment for all cancers. A specific local target is that the maximum wait for a new referral must be reduced from 14 to 9 days.
• To work with local PCTs and Practice Based Commissioners (PBC) to ensure that the Trust is providing the range of services that they wish to commission.
• To ensure complaints are dealt within Trust policy timeframes and to report performance against this standard to the Trust Board.
• To achieve improvements in patient care based on outcomes of patient satisfaction surveys.
With the exception of two weeks wait cancer appointments all services were available on the Choose and Book System.
Action plans for patient satisfaction surveys were completed.
The Trust achieved the national targets. In addition, the local target was also achieved.
Continuing.
The complaints performance improved significantly.
Action plans for patient satisfaction surveys were completed.
CATEGORY OF STAKEHOLDER REQUIREMENT
STRATEGIC OBJECTIVES
SUCCESS TOBE MEASURED BY:
PROGRESS TO YEAR END
37

3 To attract, retain and develop a diverse and talented workforce with the knowledge, skills and attitudes to deliver an excellent patient experience and become an employer of choice.
• Developing a comprehensive workforce strategy to enable the delivery of high quality patient care.
• Provide an environment in which colleagues thrive and shine.
• Promoting diversity, valuing equally the unique contribution that individual experience, knowledge and skills can bring.
• Evaluating the quality of human resource management practice to continually identify high impact service improvements.
• Having robust and effective policies that enable the Trust to achieve its strategic objectives.
Workforce plans are under development within divisions.
Policies and strategies are being produced for staff development.
A single equality scheme was launched.
An evaluation was undertaken on HR operations and key recommendations implemented.
Policies and procedures were regularly reviewed and updated.
Improving financial health and maintaining high-level cost effectiveness
4 We want to maintain the viability of the Trust by improved efficiency and effectiveness, using benchmarking and economies of scale where appropriate, and ensuring that high quality services are provided cost effectively.
• Produce plans to deliver financial stability and recurrent balance within ethos of corporate recovery.
• Integration review of financial and operational management, making financial management “everyone’s business.”
• Achieve and, where possible, exceed cost reducing efficiency savings (CRES) across the Trust. The target for 2007/08 is 2.5%.
• To ensure that the Trust signs robust service agreements based on the new NHS contract.
• To ensure that the Trust is paid for all appropriate activity under PbR and to work with PCTs to calculate ‘unbundled’ tariffs in specified HRGs.
• Build new financial systems and disciplines to manage in a working capital environment, linked to Foundation Trust development.
Completed.
Completed.
CRES achieved as per plan.
Completed: contracts signed.
Completed: ‘unbundled’ tariff included in HRG version 4.
Finance restructure completed. Objective will continue into 2008/09 and be confirmed once due diligence of FT application is undertaken.
CATEGORY OF STAKEHOLDER REQUIREMENT
STRATEGIC OBJECTIVES
SUCCESS TOBE MEASURED BY:
PROGRESS TO YEAR END
38 Strategic corporate objectives for 2007-08 continued

Dr Khalil Kawafi,
the Trust’s clinical lead for
stroke, with some
members of the
Fairfield General
Hospital stroke
team which
won the service
transformation
award at the
North West Health
and Social Care
Awards. Picture
by Bury Times
Buildings and equipment that are fit for purpose
5 We want suitable facilities, high-tech equipment and a clean hospital environment.
• Finalise estates strategy during 2007/08, including plans for the reconfiguration process.
• Continued investment in the estate to support clinical activity, capital programme in place and agreed.
• Planned annual backlog maintenance programme agreed and financed.
• Implement the cleaning service plan and improve on the current cleaning audit scores.
• Investment programme for equipment.
• Implement and achieve IM&T programmes for 2007/08.
Development of strategy continuing in line with the reconfiguration programme
Capital programme agreed
Funding agreed
Service plan agreed by the cleaning committee
Funding agreed
Achieved
CATEGORY OF STAKEHOLDER REQUIREMENT
STRATEGIC OBJECTIVES
SUCCESS TOBE MEASURED BY:
PROGRESS TO YEAR END
39
Involvement 6 We want the people we serve to feel involved in the decisions that shape our future.
• Development of a framework for patient and public involvement, recognising the FT governance framework, recruitment of governors and establishment of constituencies.
Proposals for constitution of FT council of governors were circulated to a wide range of stakeholders, and comments have been requested. This proposed a clear remit for the council in addition to a clear role description for governors.

Organisational effectiveness
7 We want an effective and responsive organisational form to prepare us to meet the future challenges of operating in a Foundation Trust environment.
• Continued work with PCTs and local communities following the consultation decisions and then implementing the reconfiguration process.
• Implement the outcomes of the Foundation Trust diagnostic exercise and develop an organisation-wide project plan for the introduction of measures to put the Trust in a position to apply for FT status no later than 2008.
• Implement the review of the organisational structure and governance arrangements in the light of a prospective FT application to ensure that they are ‘fit for purpose.’
• Start production of integrated business strategy for FT status, building on a robust understanding of our markets.
Joint working arrangements with PCTs are in place.
FT project committee met regularly and the Board received regular updates on the progress being made to develop governance structures fit for FT. A programme of Board development was commissioned and will report in summer 2008.
Review of Board structure has concluded and reported to the Board. There was a revision of Board and sub-committee structure – more details can be found on page 3.
IBP was developed to a stage where further work is now required on financial and business model. This will take place in 2008-09 once a decision on FT application is committed to.
CATEGORY OF STAKEHOLDER REQUIREMENT
STRATEGIC OBJECTIVES
SUCCESS TOBE MEASURED BY:
PROGRESS TO YEAR END
8 We want to act with probity, openness and be publicly accountable for our decisions and actions.
• Continue to ensure that all Board papers are publicly available, with particular emphasis on ensuring that web-based information is up-to-date.
• The Trust has a wide range of stakeholders and within the process of FT application we intend to ensure that they are actively engaged. This will include established fora and other systems of engagement will take place with particular emphasis on our diverse local communities. Governor membership will be representative of our communities in terms of age, disability, ethnicity, faith, sexual orientation and socio-economic groups.
Board papers were revised in line with ALE requirements. All papers now make specific reference to risk and linkages to corporate objectives. A revised external website was launched with updated links.
A large number of informal presentations were made to staff groups internally on the process of FT and external stakeholders, including MPs, were briefed on our FT aspirations. This engagement will move up a gear once FT application timeline is set.Paper on governance arrangements was sent to all stakeholders and will be further considered once responses received in.
40 Strategic corporate objectives for 2007-08 continued

Closer “cross-boundary” working
9 We want to work alongside our local partners to shape the delivery of health care in our locality.
• Clinicians and managers from all levels of the Trust regularly contribute to ‘patch-wide’ planning, modernisation and service improvement meetings.
Work-streams were identified with PCTs. A process was agreed for reconfiguration process with a Programme Board and an Assurance Board. A decision on FT application is committed to.
CATEGORY OF STAKEHOLDER REQUIREMENT
STRATEGIC OBJECTIVES
SUCCESS TOBE MEASURED BY:
PROGRESS TO YEAR END
41
Cataract patient John Tucker with Andrea Lord, ophthalmic practitioner in pre-assessment at Birch Hill Hospital in Rochdale. Andrea’s constant reassurance helped John go through with his operation.

42This year saw the conclusion of the decision-making process in two major public consultations which will shape the future development of Trust services, and those of local PCTs.The Independent Reconfiguration Panel provides advice on contested proposals for health service change in England. The panel’s reports on the Healthy Futures and Making It Better programmeswerepublishedon24August2007.
The consultants, GPs and experienced health services managers who make up the panel had endorsed a vision of high quality hospital centres of excellence developed through more than three years of pre-consultation work and formal consultation processes.They recognised that the Trust can best maintain quality of care, meet national guidance and the increasing expectations of patients, through creating centres of excellence at all of our hospitals.
In addition, they agreed that local accessibility should be ensured by moving services, where appropriate, from hospitals to community locations.The reports endorsed both of the preferred options previously approved by joint committees of local PCTs.The Secretary of State for Health endorsed the reports’ conclusions.
The next steps
The developments approved under Making It Better and Healthy Futures will take place over the next five years. The Trust, in conjunction with the local PCTs, has created the North East Sector Assurance Board to oversee this process.
Each of the PCTs will lead a clinical workstream, as follows:
Scheduled care – led by Heywood, Middleton and Rochdale PCT. Unscheduled care – led by Bury PCT. Cancer – led by Oldham PCT. Women and Children – led by Manchester PCT. Chronic Disease Management – led by Oldham PCT.
These clinical workstreams will be supported by groups covering:
• Financeandcommissioning• HRandworkforcetraining• Mediaandcommunications• Facilitiesandtransport• Informationmanagementand
technology• Estates
The Trust is committed to supporting a process which is clinically-led by the staff who will be providing the services. The consultation programme involved hundreds of clinicians and the Trust will be building on this during the implementation programme.
The first major step in the implementation programme was taken when the SHA approved the business case for the women and children’s development at North Manchester General Hospital in March 2008.
Planning permission was subsequently granted for both the enabling works and the main scheme. The enabling works will take place through summer 2008, before the main works begin.
An overview of Healthy Futures and
Making It Better
The two programmes have had a very high profile in the area through their development. The decisions create hospital centres of excellence by centralising certain types of services at specific hospitals. This will create critical masses of patients who can be treated at units which make the best use of staff skills and equipment. Each hospital will have at least one centre of excellence.
Future service developments

43The proposals were opposed by high-profile public campaigns in both Bury and Rochdale. The Trust recognises the importance of ensuring ongoing public engagement to maximise understanding of the clinical benefits of the moves. In addition, ongoing patient involvement will help ensure the best possible services.
Public focus was very heavily on the hospital services during the consultations. It is anticipated that there will be a growing awareness of community investment as LIFT centres begin to be built, and other community-based developments take place. In addition, there was little focus on services which will not change. All hospitals in the Trust will retain a range of outpatient services and day case surgery.
A summary of the Healthy Futures and Making It Better decisions is detailed below. Full information is available from www.bestforhealth.nhs.uk or by contacting the Trust’s PALS – see contact details on page 2.
The Healthy Futures decision will mean:
• A&EwillremainatTheRoyalOldham Hospital, North Manchester General Hospital and Fairfield General Hospital, Bury
• RochdaleInfirmarywillbecomea locality hospital; larger than a traditional community hospital, but smaller than a traditional district general hospital
• RochdaleInfirmary’sA&Edepartment will become an urgent care centre, caring for an estimated 85%ofexistingpatients.Theurgent care centre will not receive patients by emergency ambulance. They will be taken directly to the nearest appropriate hospital.
• AcutesurgerywillbeprovidedatNorth Manchester General Hospital and The Royal Oldham Hospital
• AcutemedicinewillbeprovidedatFairfield General Hospital, with a surgical opinion available.
The Making it Better decision will mean:
• Maternity,neonatalandinpatientpaediatric services will be centred at The Royal Oldham Hospital and North Manchester General Hospital. Ante-natal and post-natal care will continue at Fairfield Hospital and Rochdale Infirmary. Both hospitals will also retain paediatric outpatients’ services.
• Neonatalintensivecarewillbeprovided at The Royal Oldham Hospital, the first time that the area will have this service.
• Thepossibilityofstand-alonemidwife-led birth centres are being explored in Bury and Rochdale.
• Children’sobservationandassessment units will be developed at The Royal Oldham Hospital, North Manchester General Hospital and Fairfield General Hospital.
• Morecommunitychildren’snursesroles will be created, with the greatest resources in areas seeing transfer of services.

44Our NHS, Our future
The NHS next stages review is being led nationally by Professor Sir Ara Darzi and aims to set out a 10-year vision. The national programme is being supported by regional work, led by strategic health authorities. The Trust was an active participant in the regional clinical pathway groups established by NHS North West. Head of midwifery, Cathy Trinick, was a member of the maternity and newborn care group and Mr Don Mackechnie, clinical director for emergency care, was a member of the urgent care group.
The Trust supported this work through encouraging staff and patients to respond directly to the review, through information and briefing systems.The Trust also made a formal response which summarised comments from clinical teams in our divisions. The Trust’s response summarised the Healthy Futures and Making It Better decisions and noted that they shared many similar principles with ‘Our NHS, Our Future’ to date.
In addition, the Trust commented on:• Theimportanceofpreventative
work in children’s dental care.• ThevalueofincludingbothA&E
and police representatives on the mental health pathway group.
• Thebenefitsoffocusingonamorelimited number of key features in the staying healthy pathway group.
• TheimportanceofensuringthatGreater Manchester’s maternity services have large enough units to reduce the number of maternity diverts.
Further engagement work will take place following the publication of the regional vision document.
Additional major service developments
Radiotherapy service
The Christie Hospital NHS Foundation TrustconfirmedinNovember2007that it would be developing an ambulatory radiotherapy service based at The Royal Oldham Hospital. This will benefit patients not just in Oldham, but across the Pennine area, who currently have to travel across Manchester for this service.
The move is in line with the Christie’s strategy to expand radiotherapy capacity across Greater Manchester. The service will be housed in a new building at The Royal Oldham Hospital, and a multi-storey car park is planned to provide additional spaces for patients.
Foundation Trust
The Trust continued with its work
towards a Foundation Trust (FT) application.
The FT project committee has discussed proposals for a suggested future Council of Governors. These have been circulated to a wide range of stakeholders for comment. Proposals have been developed to reform the Board and sub-committee structure to align with a future FT model. A programme of Board development has commenced to consider the skill set and make recommendations on how to strengthen this in light of a future application. Detailed work is being progressed on the planning timescales for reconfiguration and the financial consequences of service moves, which will inform the development of the Trust’s long term financial plan. The Trust will pilot service line reporting in someareasduring2008-09.Anactionplan to deliver service line reporting is a requirement of FT applications.
Improving our systems
The Trust continues to recognise the opportunities and potential challenges from the increased growth of contestability in the NHS. The work tobeundertakenin2008-09tohelpfurther improve our systems, as set out in our corporate objectives, will support the efforts of staff to remain the provider of choice for local patients.
Future service developments continued

45The Trust strongly believes that involving patients and their families in discussions about our services is the best way to ensure that we can meet their needs. In addition, we also work with a range of representative groups – their role is vital in ensuring the patient voice is heard within these areas.
The work which has taken place this year included:
• Aworkshopformatfortheannualpublic meeting, which enabled patients who use a range of services to give their views to senior managers and clinical staff. Topics discussed included improving hygiene, reducing waiting times and Healthy Futures/Making It Better.
• Asimilarworkshopevent,basedon cancer services, took place at The Royal Oldham Hospital in June2007,attractingnearly100attendees. The work-shop sessions included different topics relating to cancer treatment.
• TheinvolvementofthePenninePatient User Partnership in the development of the Christie cancer service at the Trust.
• MembersofthePatients’Council,which was formed as part of the Healthy Futures programme,
have continued to support the Trust. Patients’ Council members are represented on key steering groups and committees across the organisation, including the Healthcare Associated Infection Improvement Board, the Equality and Diversity committee and the Transport Action Group.
• Workcontinuestodeveloppatientadvice and liaison service (PALS) volunteers across the organisation. PALS volunteers will be able to support patients and gather feedback, helping patients with any concerns or issues to use the service. A volunteers’ coordinator was appointed to support this development.
• Patientsupportgroupsacrosstheorganisation are still actively utilised and supported by the Trust and site-based equality and diversity groups. These groups have been established to gather both the views of the diverse local population and staff to ensure that the policies, procedures and services which the Trust provides are not discriminatory.
• TheTrust’swebsitewasre-designedand re-launched, giving greater prominence to feedback functions for patients and their families. In
addition, the Trust joined the patient opinion scheme. This independent website enables patients to give their views on services, and for the Trust to respond to them publicly.
• Withtheendofthepublicandpatient involvement forums the Trust has been working with local partners to ensure that the New Local Involvement Networks (LINks ) are supported in their development. The Trust would like to thank all forum members for their contributions to the Trust and hope these relationships continue once LINks is established.
• TheTrustregularlyhadrepresentatives at the local overview and scrutiny committees, and discussed issues as raised. This included attending both the OSC which deals specifically with the Trust and the OSCs for each of the local authorities within the Trust’s catchment area.
Comments, complaints and
compliments
The Trust values all feedback from patients, whether positive or negative, and uses this to inform development of its services. Clinicians work with PALS or complaints teams to respond to patients’ complaints or points. The Board is made aware of these issues
Patient partnerships, involvement and views

46as all final responses to complaints are signed by an executive director.
TheTrust’sperformancein2007-08saw a drop in the number of complaints received and fewer patients having to see PALS teams, despite us being busier than last year.
In addition, the number of complaints responded to within the national target has significantly improved during2007-08.Lastyear56%ofcomplaints were responded to within the25workingdaytarget.Followingthe introduction of the complaints management improvement plan in June2007theTrust’sperformancehasincreased to an end of year average of 79.5%,whichplacestheTrustamongthe top performing nationally.
Speed has not compromised the quality of responses and the Trust is pleased to see a reduction in the number of complaints being referred to the Healthcare Commission for independentreview.In2006-07atotalof26complaintswerereferredcomparedto13thisyear.InJanuary2007theHealthcareCommissionpublished Spotlight on Complaints, which described the Trust as “poorly performing” in relation to the number of complaints referred back to the Trust for further local resolution. However35ofthe38casesinthe
Patient partnerships, involvement and views continuedreport related to previous years, so did not reflect the latest improvements.
During the past year the Trust updated the complaints management policy to ensure compliance with national guidance and the NHS Litigation Authority (NHSLA) Risk Management Standards for Trusts. This policy included guidance for staff on how to resolve complaints informally and has led to a reduction in the number of formal complaints received by the Trust from685lastyearto576in2007-08.
Evidence from divisional nurse managers demonstrates that complaints are being successfully managed at ward and departmental level. This has also led to a reduction in the number of PALs contacts from 2,421in2006-07to1,866thisyear.Only7%ofcontactswentontomakea formal complaint.
In March 2008 the Trust was assessed against the NHSLA Risk Management Standards and successfully met all criteriaforstandard5,whichincludedcomplaints management. An internal audit report also provided significant assurance that the Trust is managing complaints well.
The Trust continues to learn lessons from complaints and improve systems and clinical practice. Following
concerns raised nationally and locally about the care of adults with learning disabilities in acute hospital settings the Trust has been working with the learning disabilities team to develop communication strategies,

47referral and discharge pathways and documentation and an educational toolkit, which will enable staff to better meet the needs of this very vulnerable group of patients.
The Trust is pleased to have been chosen as a project site for the Early Adopter Programme to develop an integrated complaints management system for health and social care. The coming year will see this developed
with the Department of Health and partner agencies in Oldham.
Patient surveys
Proactively gathering patients’ views through surveys is an essential component in working with patients.
In2007-08,theTrusttookpartinseveral national patient surveys. This included the national inpatient survey, the national children and young person’s survey and the national maternity survey. In addition, the Trust took part in the pilot for a national outpatient survey.
Because of the numbers of patients treated at Trust hospitals, additional local surveys are also run by the Trust throughout the year.
After consideration of results and feedback, action plans are developed in support of all of these surveys.
The Trust’s redesigned website gives patients, visitors and stakeholders a wide range of information at the touch of a button. Information about travelling to the Trust’s hospitals, the services available, career opportunities, fundraising work and media activity are just some of the features.

48Staff in the human resources and organisational development directorate successfully delivered a number of major projects, and supported delivery of many others. These included:
• Inexcessof29,000trainingepisodes utilising enhanced training methods have been delivered, specifically relating to mandatory and induction training.
• Therehasbeeninvestmentinwireless network technology to support out of hours working within clinical teams.
• Thefirstsingleequalityschemeandaction plan for the Trust has been published. Community groups and staff members consulting on the new scheme have supported this.
• Equalityimpactassessmentshavebeen completed on the majority of Trust policies.
• Equalopportunitydataincluding,ethnicity, age, gender and disability is published on the Trust website ensuring we meet legislative requirements. Analysis of this data has informed recommendations made to the Equality and Diversity Committee.
• TheTrusthasbeenre-accreditedwith the Disability Two Ticks symbol and continues to actively promote the standards this symbol represents.
• WithintheyearanextensiveHR
policy review programme has been completed, in partnership with staff-side colleagues.
• ToensuretimelyHRsupportisavailable to staff and managers, the HR helpdesk has been launched. This provides daily access to HR advice at a senior level.
• TheTrustvaluescontinuetobeimportant in influencing the way we work together in the Trust. Sessions discussing the values are delivered on every induction programme and regularly to teams.
• Amajorleadershipdevelopmentprogramme – “Developing Potential” has commenced. Over 120 of the Trust’s top leaders have enrolled for the programme that is underpinned by the NHS Leadership QualitiesFramework360degreeassessment.
• TheTrustsuccessfully“wentlive”with the electronic staff record (ESR) in October and the Oracle learning management system in January. ESR - the integrated payroll and HR system will enable more streamlined processes to be developed. The learning management system will facilitate the robust reporting of attendance and non-attendance at training events.
Investing in our staff VolunteersFrom hospital radio and supporting the chaplaincy service, to staffing reception desks and running shops, hundreds of people give up their time to volunteer in Trust hospitals each year. Their work supports that of Trust staff, and makes a real difference to patients’ time in hospital. In addition to individuals, many volunteers come through organisations including the WRVS, church groups, League of Friends, schools and colleges.
The Trust has appointed a volunteer co-ordinator, Mary Sunderland. If you wish to find out more about volunteering then please contact Mary [email protected].

The Trust is a category one responder, which means that we have specific duties under the Civil Contingencies Act during a major incident. Other category one responders include other NHS organisations, the police, the fire service and local authorities.A Trust-wide major incident plan exists, with each hospital testing their sections regularly with planning exercises. The Trust’s emergency planning committee meets monthly and members link with other local responder organisations through local resilience groups. We also liaise with the Health Protection Agency and NHS North West, and attend the Greater Manchester acute trust emergency planning meetings.Staff were also involved in a special training exercise this year, which explored how a flu pandemic would impact on the triage and treatment of patients. This was run jointly with Leicester Royal Infirmary, and included a training scenario at North Manchester GeneralHospitalinJuly2007,followedby a further exercise at Leicester in September2007.Thelessonslearnedfrom this successful project will be shared with other hospitals. A plan to respond to a flu pandemic was also developed this year.
The Trust also has continuity plans and business recovery plans.
Emergency preparedness 49

Display Energy Certificat
Energy Performance Operational Rating
How efficiently is this building b
Admin Technical information
Heating Electrical
Less energy efficient
A 0 25
B 26-50
C 51 75
D 76-100
E 101 25 108F 126-150
G Over 150
More energy efficient
100 wou
50The Trust is committed to sustainable development and has worked with the Carbon Trust to undertake energy saving audits. An action plan was put into place at The Royal Oldham Hospital and audits have been undertaken at the Trust’s three other hospitals. In addition to reducing the Trust’s carbon footprint, these action plans should help reduce both the financial and environmental costs of inefficient energy use. The reports are available on request.
Funding totalling £200,000 was provided from the Department of Health’s environment and sustainability fundin2007-08topayforenergyefficient improvements. A further £200,000 will be invested by the Trustin2008-09tocontinuethispartnership with the Carbon Trust and to implement further improvements. A two-year financial pay-back is expected, while the reduction in carbon dioxide emissions is expected to amount to more than 2,000 tonnes annually. This will enable the Trust to work towards Department of Health targets on improving energy efficiency and to play its part in the Government’s Climate Change Programme.
Sustainable developmentEnergy efficiency and sustainable development has grown into an issue of massive public interest, and a new ratings scheme will provide visible assurances of the work being done in this area. Display energy certificates are being introduced nationally from 1 October 2008, with the aim of making the public aware of buildings’ environmental impact, and encouraging greater efficiency. The certificates have to be displayed prominently in each large building. With assessments carried out annually, the certificates will indicate both current ratings and the progress over recent years.
As part of the full business case approval for the new women and children’s unit at North Manchester General Hospital, the Strategic Health Authority confirmed that it had an ‘excellent’ rating under the NHS Environmental Assessment Tool. There is a mandatory Department of Health requirement to meet the energy consumption and conservation measuresof35-55Gj/100m3.Thesenow link to more stringent building regulation approvals, and these calculations provide evidence that the building will achieve just under 38Gj/100m3,whichtheSHAdescribedas “commendable”.

te
being used?
nistrative information
0
Mar 2005
Heating
Apr 2006 Apr 2007
100
200
300
Electricity
Renewables
-50
8
uld be typical
Total CO2 Emissions
Previous Operational Ratings
Mar 2005
Apr 2006
Apr 2007
100500 150 200
108
133
15
51Joint working enables the Trust to best improve its services, and the health of local residents. The Trust is a member of a number of regional clinical networks, and also works with the multi-agency and multi-organisational local implementation teams, which exist across the four local authority areas.
In addition, the Trust promotes additional ties between our own medical staff and others.
This year saw the development of joint consultant-GP educational forums, developed by Trust medical director, Dr Ruth Jameson. These events enable hospital and community-based clinicians to come together to discuss latest clinical developments in a range of subjects. The events are held in turn at each Trust hospital and they have received positive feedback.
The Trust has also begun to support the Refugee and Asylum Seekers’ Centre for Healthcare Professionals’ Education (Reache). Based at a purpose built centre in Hope Hospital, Salford, this service supports refugee and asylum seeking healthcare professionals. Reache assists them in gaining professional registration in the UK, and in development and finding employment. Some of our staff have already provided teaching sessions at Reache, and we are supporting clinical placements within the Trust.
This works supports the ARRIVE project (Assisting the Return of Refugee Doctors Into Viable Employment). This is a joint venture by the NHS Confederation and Reache North West. This is a highly effective way to combat social and economic exclusion of some of our most challenged communities. It promotes both their success, recognises their contribution to the health service and also delivers a firm message about the valuable contribution which refugees can make to the UK.
Partnership working
An example of the information which the new display energy certificate will provide.

52Financial overview
The Trust’s audited annual accounts outline the financial performance of the Trustfor2007/08andareincluded,infull, at the end of this chapter.
The Trust has achieved a surplus of £9.472mfortheyear2007/08andin doing so repaid last year’s deficit of £9.17minfull.TheTrustwasoriginallyforecastingasurplusof£4.96mforthe year and has exceeded this by a substantial margin. This excellent result has been achieved largely because of over performance against contracts with PCTs during the year. In addition, this position would not have been possible without the financial turnaround programme launched in2006/07andthehardworkandcommitment of all staff within the Trust.
In2007/08,theTrustmetallkeyfinancial duties:• Breakeventakingoneyearwith
another• Remainwithinapprovedexternal
financinglimit(note23.3oftheaccounts)
• Maintaincapitalexpenditurewithinapprovedlimits(note23.4)
• Achievea3.5%returnoncapitalemployed(note23.2)
• Achieve95%compliancewithBetter Payments Practice Code (note7.1).
The Trust is forecasting breakeven for2008/09.Thisisaftertakinginto account forecast cost increases, changes in income due to proposed disinvestment of services by PCTs, the tariff uplift and the in year efficiency target set by the Department.
The key risk areas identified for 2008/09are:• Incomeandexpenditureto
breakeven• Cashbalancesandliquiditytobe
managed to deliver the external financing limit (EFL), capital resource limit (CRL) and public sector payment policy (PSPP)
• Capitalresourcelimitnottobeexceeded
• Deliverefficiencyprogramme• Thecontractfor2008/09includes
financial penalties to meet 18 week referral to treatment time targets and for failure to achieve reductions in the incidence of the hospital acquired infection C. Difficile.
Income and expenditure
Operating Income
Operatingincomein2007/08amountedto£499,444,000,ofwhich, income from activities was £453,642,000withotheroperatingincomeof£45,802,000.Intotal,incomehasincreasedby5.4%between years.
The vast majority of income comes from Primary Care Trusts – £420,610,000(84%).
Operating Expenditure
Operating expenses amounted to £479,175,000andthelargestelementof this is the pay bill for our staff and directorsof£317,932,000.Overall,operatingexpensesincreasedby2.2%betweenyears.In2007/08theTrustemployed,onaverage,8,872wholetime equivalent staff compared to 9,149wholetimeequivalentstheyearbefore.
Capital expenditure
In2007/08theTrustspent£26,717,000onbuildings,equipmentand information technology as shown in Table 1.
Register of declared interests
A register of declared interests is maintained by the Trust and is available for inspection on application to Mr J Saxby, chief executive. There are no company directorships held by directors of the Trust with companies who are likely to, or are seeking to, conduct business directly with the Trust.
Financial report

Medical and scientific equipment 3,798
CT scanner, Rochdale Infirmary 607
Picture Archiving Communication System (PACS) - x-ray 7,115
Information technology 1,712
Completion of central pathology laboratory, ROH 4,542
Completion of new mortuary and forensic facilities, ROH 1,887
Diabetes centre, NMGH 1,103
Medical records, ROH 948
Women & childrens development and enabling works, NMGH 1,499
Other building schemes 3,506
Future capital investment will be heavily influenced by the reconfiguration
of services over the next five years in response to the Healthy Futures and
Making It Better consultations.
TABLE1 £000
53
External auditors
The Trust’s Auditors are KPMG. The cost of work performed by the auditor inrespectofthe2007/08reportingperiodwas£319,000relatingtoauditservices and the requirements of the Audit Commission’s Code of Practice, ie the statutory audit and services carried out in relation to the statutory audit eg reports to the Department of Health.
Auditing standards require the directors to provide the external auditors with representations on certain matters material to their audit opinion. The directors have confirmed to KPMG such representations as necessary to the best of their
knowledge and belief, having made appropriate enquiries of other directors and officers of the Trust.
Statement on internal control
The Trust Board is accountable for internal control. As accountable officer, the chief executive of the Board has responsibility for maintaining a sound system of internal control that supports the achievement of the organisation’s policies, aims and objectives. The chief executive also has responsibility for safeguarding the public funds and the organisation’s assets for which he is personally responsible, as set out in the accountable officer memorandum.
As a large acute Trust with a number of constituent stakeholder organisations, various arrangements and agreements are in place through which the Trust’s performance is monitored. These are set out in the full Statement of Internal Control (included with the annual accounts) along with an explanation of the purpose of the system of internal control, information on the capacity to handle risk, the risk and control framework and review of effectiveness.
The Trust’s annual accounts for 2007/08issetoutonpages62to65.Inadditionitshouldbenotedthatto comply with legislation governing charities, a separate set of annual accounts is maintained for funds held on trust. A full set of these accounts is also available on request.
R ChadwickDirectorofFinanceandIM&T
The Pennine Acute Hospitals NHS Trust
Headquarters, North Manchester General
Hospital, Delaunays Road, Manchester
M8 5RB

54 Financial report continued
CONTENTS PAGE
Statement of directors’ responsibilities in respect of the accounts _________ 55
Independent auditor’s report to the directors of the board ________56
Statement on internal control _______58
AccountsMain Statements:Income & expenditure account _____ 62Balance sheet ____________________63Statement of total recognised gains and losses _______ 64Cash flow statement ______________ 64
ANNUAL ACCOUNTS for the Year ended 31 March 2008
Notes to the Accounts:
1 Accounting policies______________662 Segmental analysis ______________ 743 Income from activities ___________ 744 Other operating income analysis __ 745 Operating expenses analysis _____ 756 Staff costs and numbers _________ 767 Better payment practice code ____ 788Profit/(Loss)on disposal of fixed assets __________ 789 Interest payable _________________ 7810 Intangible fixed assets __________ 7911 Tangible fixed assets ___________8012 Stocks and work in progress _____ 8213 Debtors analysis _______________ 8214 Investments ___________________8315 Creditors analysis ______________8316 Provisions for liabilities and charges ___________ 8417 Movements on reserves ________8518 Notes to the cash flow statement ___________8619 Capital commitments ___________8720 Post balance sheet events ______8721 Contingencies _________________8722 Movement in public dividend capital (PDC) __________8823 Financial performance targets(breakeven,CRL,EFL) ___8824 Related party transactions ______9025 Private finance transactions _____ 9126 Pooled budget _________________ 9127 Financial instruments ___________ 9128 Third party assets ______________ 9329 Intra government and other balances _____________ 9330Lossesandspecialpayments ___ 93Finance glossary __________________98
Glossary ________________________100

55
By order of the Board
Date19June2008
Chief Executive
Date19June2008
Finance Director
Statement of directors' responsibilities in respect of the accounts
The directors are required under the NationalHealthServiceAct2006toprepare accounts for each financial year. The Secretary of State, with the approval of the Treasury, directs that these accounts give a true and fair view of the state of affairs of the trust and of the income and expenditure of the trust for that period. In preparing those accounts, the directors are required to:
• applyonaconsistentbasisaccounting policies laid down by the Secretary of State with the approval of the Treasury
• makejudgementsandestimateswhich are reasonable and prudent
• statewhetherapplicableaccountingstandards have been followed, subject to any material departures disclosed and explained in the accounts.
The directors are responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the trust and to enable them to ensure that the accounts comply with requirements outlined in the above
mentioned direction of the Secretary of State. They are also responsible for safeguarding the assets of the trust and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities.
The directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the accounts.
A flu pandemic exercise at North Manchester General Hospital

Artist Lesley Young
shows Trust chairman,
John Jesky and patient
Norman Royle one
of the new video art
installations at North
Manchester General
Hospital’s physiotherapy
department.
56Independent auditors’ report to the directors of the Board of Pennine Acute Hospitals NHS Trust
Opinion on the financial statements
We have audited the financial statements of Pennine Acute Hospitals NHSTrustfortheyearended31March2008 under the Audit Commission Act1998.ThesecomprisetheIncomeand Expenditure Account, the Balance Sheet, the Cash Flow Statement, the Statement of Total Recognised Gains and Losses and the related notes. These financial statements have been prepared under the accounting policies relevant to the National Health Service set out within them.
This report is made solely to the Board of Pennine Acute Hospitals NHS Trust, as a body, in accordance with Section 2oftheAuditCommissionAct1998.Our audit work has been undertaken so that we might state to the Board of Pennine Acute Hospitals NHS Trust, as a body, those matters which we are required to state to them in an auditor’s report and for no other purpose. To the fullest extent permitted by law, we do not accept or assume responsibility to anyone other than Pennine Acute Hospitals NHS Trust and the Board of Pennine Acute Hospitals NHS Trust, as a body, for our audit work, for this report, of for the opinions we have formed.
Respective responsibilities of Directors
and auditors
The directors’ responsibilities for preparing the financial statements in accordance with directions made by the Secretary of State are set out in the Statement of Directors’ Responsibilities.
Our responsibility is to audit the financial statements in accordance with relevant legal and regulatory requirements and International Standards on Auditing (UK and Ireland).
We report to you our opinion as to whether the financial statements give a true and fair view and whether the part of the Remuneration Report to be audited (details of senior managers’ remuneration and pensions) has been properly prepared in accordance with the accounting policies directed by the Secretary of State as being relevant to the National Health Service in England.
Financial report continued

57We review whether the directors' statement on internal control reflects compliance with the Department of Health's requirements ‘The Statement onInternalControl2003/04issuedon15September2003andfurtherguidanceissuedon7April2008. We report if it does not meet the requirements specified by the Department of Health or if the statement is misleading or inconsistent with other information we are aware of from our audit of the financial statements. We are not required to consider, nor have we considered, whether the directors' statement on internal control covers all risks and controls. We are also not required to form an opinion on the effectiveness of the Trust’s corporate governance procedures or its risk and control procedures We read other information contained in the annual report, and consider whether it is consistent with the audited financial statements. This other information comprises only the unaudited part of the remuneration report and the Operating and Financial Review. We consider the implications for our report if we become aware of any apparent misstatements or material inconsistencies with the financial statements. Our responsibilities do not extend to any other information.
Basis of audit opinion
We conducted our audit in accordance withtheAuditCommissionAct1998,the Code of Audit Practice issued by the Audit Commission and International Standards on Auditing (UK and Ireland) issued by the Auditing Practices Board. An audit includes examination, on a test basis, of evidence relevant to the amounts and disclosures in the financial statements and the part of the Remuneration Report to be audited. It also includes an assessment of the significant estimates and judgments made by the directors in the preparation of the financial statements, and of whether the accounting policies are appropriate to the Trust’s circumstances, consistently applied and adequately disclosed.
We planned and performed our audit so as to obtain all the information and explanations which we considered necessary in order to provide us with sufficient evidence to give reasonable assurance that the financial statements and the part of the remuneration report to be audited are free from material misstatement, whether caused by fraud or other irregularity or error. In forming our opinion we also evaluated the overall adequacy of the presentation of information in the financial statements and the part of the remuneration report to be audited.
Opinion
In our opinion:• thefinancialstatementsgivea
true and fair view, in accordance with the accounting policies directed by the Secretary of State as being relevant to the National Health Service in England, of the state of the Trust’s affairs as at 31 March 2008 and of its income and expenditure for the year then ended; and
• thepartoftheremunerationreport to be audited has been properly prepared in accordance with the accounting policies directed by the Secretary of State as being relevant to the National Health Service in England.
KPMG LLPManchester20 June 2008
58 Financial report continuedStatement on internal control 2007/08.
Pennine Acute HospitalsNHS Trust.
1. Scope of responsibility
The Board is accountable for internal control. As accountable officer, and chief executive of this Board, I have responsibility for maintaining a sound system of internal control that supports the achievement of the organisation’s policies, aims and objectives. I also have responsibility for safeguarding the public funds and the organisation’s assets for which I am personally responsible as set out in the accountable officer memorandum.
As a large acute Trust with a number of constituent stakeholder organisations there are a range of arrangements/agreements in place through which the Trust’s performance is monitored. These include:(i) Executive director one to one
meetings/contact with their counterparts at the Strategic Health Authority.
(ii) Performance management of the Trust overseen by Strategic Health Authority through the performance assessment framework and the organisational improvement plan. The increasing devolvement to PCTs is noted.
(iii) Overview and scrutiny committees of which there is one for each local authority and an overarching committee for the Trust.
(iv) Membership of the local authority Local Strategic Partnerships.
(v) Links with the primary care trusts through:-- the North East Sector Strategic
Board comprising of Trust chairs, chief executives, medical directors and PEC Chairs.
- monthly one to one meetings between the chief executive and PCT chief executives
- Executive Board to Board meetings quarterly with PCTs
- at chief executive level a commissioning forum comprising the acute trust and its five constituent primary care trusts.
- service level agreements and contracts detailing commissioning requirements in terms of finance, activity and performance indicators.
In addition I am supported internally by:• thegovernanceandriskcommittee,
a sub committee of the Trust Board, established as part of the overall assurance framework and the whole systems governance approach adopted by the Trust. The governance performance board provides an operational focus to governance in the organisation and
reports to the governance and risk committee
• theauditcommitteeandtheestablished arrangements for external and internal audit services. Regular reports are received by the audit committee who in turn report to the Board.
• themedicaldirectorwhohasBoardresponsibility for whole systems governance and specifically for clinical and operational risk.
• thedirectoroffinancewhohasBoard responsibility for financial management and financial risk.
• thegovernancedirectorwhohas operational responsibility for whole systems governance and the strategic development and monitoring of the organisation against its governance development plan.
2. The purpose of the system of
internal control
The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can therefore only provide reasonable and not absolute assurance of effectiveness. The system of internal control is based on an ongoing process designed to:

59• identifyandprioritisetherisks
to the achievement of the organisation’s policies, aims and objectives,
• evaluatethelikelihoodofthoserisks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically.
The system of internal control has been in place in Pennine Acute Hospitals NHS Trust for the whole year ended 31March2008anduptothedateofapproval of the annual accounts and report.
3. Capacity to handle risk
Board level responsibility for the risk management process lies with the medical director who is supported by a governance director. risk co-ordinators and health & safety advisors in turn support the governance director based on the four main hospital sites. 2007/08hasseencontinuedprogressin putting in place the key elements in the Trust’s governance development plan as evidenced by:• thecontinuedworkofthe
governance and risk sub committee of the Trust Board chaired by one of the non executive directors and the governance committees for each of the four clinical divisions of the Trust.
• thecompletionofapieceofworkto ensure that the assurance framework and corporate risk register are directly linked and the development of a top ten risk template to ensure a Board focus on the high level risks
• asuccessfulassessmentagainstthe new NHSLA Risk Management Standards Level 1
• achievementofLevel2againsttheALE assessment and progression to Level3isanticipatedinthisyear’sassessment
A standard risk assessment process is used across the Trust and training for all staff is delivered by the risk co-ordinators and health and safety advisors. As part of the Trust’s two-day general induction programme a half-day is dedicated to the governance team ensuring that risk management processes are highlighted to all new staff. The Trust has a single accident and incident reporting policy and risk management system (Ulysses). All incidents are recorded on to the system andinJune2005beganreportingpatient safety incidents to the National Patient Safety Agency (NPSA) National Reporting and Learning System (NRLS).
4. The risk and control framework
The risk and control framework is made up of the following key elements:• Thegovernancestructureoutlined
above of which risk management is an integral part.
• Theassuranceframeworkinwhichrisks are linked to the Trust’s strategic objectives.
• Divisionalriskregisterswhichareregularly reviewed at divisional governance committees
• Thegovernancedevelopmentplan which is submitted to and monitored by the Strategic Health Authority under the clinical governance reporting timetable and which now incorporates the Standards for Better Health
• TheStandardsforBetterHealthdeclaration
The Trust’s risk management strategy and policy are reviewed annually and were assessed as part of the NHSLA Risk Management Standards Level 1 assessment in March 2008. Both the strategy and the policy are circulated widely throughout the organisation and clearly describe the process for the identification of risks. A single grading process is in place throughout the Trust.

60The assurance framework was developedduring2003/04andwasreviewed, as stated above, by KPMG andinternalaudit.During2007/08asubstantial amount of work has taken place on the assurance framework with non executive directors and executive directors working in pairs to ensure it is embedded at Board level. The corporate risk register is also regularly reviewed by the executive team and has been developed to include outstanding actions. These risks are linked to the Trust’s strategic objectives. Each risk has been graded and the controls in place to minimise the risk identified. Where a significant risk remains a risk treatment plan has been identified along with timescales, resource requirements and responsibility for implementation. Each risk then has a source of review, in many cases this is external, and a residual risk rating which the organisation must consider in terms of its acceptability. Should it not be acceptable a further risk treatment plan must be developed.
Public stakeholders are involved in the following ways:
• PublicTrustBoardmeetings• Nonexecutivedirectorchairsof
the governance committee and the audit committee
• Overviewandscrutinycommittees• Patientsforums
As an employer with staff entitled to membership of the NHS Pension Scheme, control measures are in place to ensure all employer obligations contained within the Scheme regulations are complied with. This includes ensuring that deductions from salary, employers contributions and payments in to the Scheme are in accordance with Scheme rules, and that member pension scheme records are accurately updated in accordance with the time scales detailed in the regulations.
The Pennine Acute Hospitals NHS Trust is committed to protecting those individuals we hold confidential data about by putting in place measures that ensure its release to those persons who have a right to access. The arrangements in place within the trust include:• Robustarrangementsforthe
management of information governance within the trust governance framework.
Recognition of the risk which is recorded on the trust corporate risk register.
• Dedicatedinformationgovernancemanager
During2007/08• Completedandsignedinternal
assurance statements as part of the Department of Health information assurance review. Assurance statement supported by independent audit review.
• Achieved‘green’statusfortheinformation governance toolkit submission.
• Fullreviewandapprovalofinformation governance policy.
• Auditingprogrammeforinformation governance compliance recommendedfor2008/09.
• Formalreportsonprogressreinformation security to the trust boardinDecember2007andFebruary 2008.
A continual review of information security is in place with policy change and improvements recommended within the information governance structure.
Financial report continued

615. Review of effectiveness
As accountable officer, I have responsibility for reviewing the effectiveness of the system of internal control. My review is informed in a number of ways. The head of internal audit provides me with an opinion on the overall arrangements for gaining assurance through the assurance framework and on the controls reviewed as part of the internal audit work. Executive managers within the organisation who have responsibility for the development and maintenance of the system of internal control provide me with assurance. The assurance framework itself provides me with evidence that the effectiveness of controls that manage the risks to the organisation achieving its principal objectives have been reviewed. My review is also informed by the following: Standards for better health
declarations NHSLA risk management standards
assessment Data accreditation/information
governance toolkit Improving Working Lives
accreditation External audit reviews by KPMG
The Trust’s audit committee continues to work closely with the governance and risk committee to ensure that the Trust continuously improves its
management of risk. The head of internal audit in providing his opinion statement provides further assurance of the processes in place.
The Trust set a financial plan for 2007/8todeliverasurplusof£4.960mthis was to recover over a two year periodadeficitof£9.2mattheendofthefinancialyear2006/7.
The Trust is currently supported by the DoH to achieve a sustainable reduction in the number of MRSA bacteraemias. The HCAI improvement Board directs and monitors the agreed action plan through the clinical divisions. The action plan is monitored by the DoH, StHa and the commissioning PCT.
Inthe2007/08Standardsforbetterhealth declaration, the Trust Board assessedthatithadmet41ofthe43core standard parts for the entire year. Actions taken by the Trust had ensured thatcorestandardpartsC14aandC14b,althoughnotmetforpartoftheyear, had been met by the end of the year.
The Trust has continued to deliver a reduction in waiting times for patients and achieved the 18 week referral to treatment target in March. The current level of performance suggests that the Trust is on course to meet the standard required by December 2008.
An internal audit has been completed which identified that there is significant assurance that controls and monitoring arrangements are in place to meet the 18 week requirements. The report noted that there has been strong evidence of governance by the scheduled care programme board and where necessary significant issues have been raised with the Trust Board. The Trust will continue to focus on ensuring compliance with the 18 week standard.
ChiefExecutive,19June2008

Kate Gregory,
clerical officer in
health records,
introduces the new
outpatients’ check-in
screen to Phillip
Broughton at North
Manchester General
Hospital.
2007/08 2006/07
NOTE £000 £000
Income from activities 3 453,642 429,882
Other operating income 4 45,802 43,814
Total Income 499,444 473,696
Operating expenses 5 (479,175) (469,088)
OPERATINGSURPLUS/(DEFICIT) 20,269 4,608
Profit/(loss) on disposal of fixed assets 8 2,286 (181)
SURPLUS/(DEFICIT)BEFOREINTEREST 22,555 4,427
Interest receivable 1,773 834
Interest payable 9 0 0
Other finance costs - unwinding of discount 16 (214) (216)
SURPLUS/(DEFICIT)FORTHEFINANCIALYEAR 24,114 5,045
Public Dividend Capital dividends payable (14,642) (14,215)
RETAINEDSURPLUS/(DEFICIT)FORTHEYEAR 9,472 (9,170)
The notes on pages 66 to 93 form part of these accounts.All income and expenditure is derived from continuing operations.
INCOME AND EXPENDITURE ACCOUNT FOR THE YEAR ENDED 31 MARCH 2008
62 Financial report continued

31 March 31 March
2008 2007
FIXED ASSETS NOTE £000 £000
Intangible assets 10 4,578 1,666
Tangible assets 11 449,364 452,021
Investments 14.1 0 0
453,942 453,687
CURRENT ASSETS
Stocks and work in progress 12 7,707 7,253
Debtors 13 29,648 32,578
Investments 14.2 0 12
Cash at bank and in hand 18.3 6,764 1,369
44,119 41,212
CREDITORS: Amounts falling due within one year 15 (38,009) (43,707)
NETCURRENTASSETS/(LIABILITIES) 6,110 (2,495)
TOTALASSETSLESSCURRENTLIABILITIES 460,052 451,192
CREDITORS: Amounts falling due after more than one year 15 0 0
PROVISIONSFORLIABILITIESANDCHARGES 16 (12,953) (13,464)
TOTALASSETSEMPLOYED 447,099 437,728
FINANCEDBY:
TAXPAYERS’EQUITY
Public dividend capital 22 223,415 243,103
Revaluation reserve 17 185,255 188,356
Donated asset reserve 17 7,559 7,770
Government grant reserve 17 900 12
Income and expenditure reserve 17 29,970 (1,513)
TOTALTAXPAYERS’EQUITY 447,099 437,728
Signed: ……......................……………………………(Chief Executive) Date: 19 June 2008
BALANCE SHEET AS AT 31 MARCH 2008
63

2007/08 2006/07
£000 £000
Surplus/ (deficit) for the financial year before dividend payments 24,114 5,045
Fixed asset impairment losses (9,495) 0
Unrealised surplus/(deficit) on fixed asset revaluations/indexation 28,779 26,183
Increases in the donated asset and government grant reserve due to receipt of donated and government grant financed assets 938 688
TOTALRECOGNISEDGAINSANDLOSSESFORTHEFINANCIALYEAR 44,336 31,916
Prior period adjustment 0 0
TOTALGAINSANDLOSSESRECOGNISEDINTHEFINANCIALYEAR 44,336 4,427
2007/08 2006/07
OPERATING ACTIVITIES NOTE £000 £000
Net cash inflow/(outflow) from operating activities 18.1 50,397 26,506
RETURNS ON INVESTMENTS AND SERVICING OF FINANCE:
Interest received 1,725 858
Interest paid 0 0
Interest element of finance leases 0 0
Net cash inflow/(outflow) from returns on investments and servicing of finance 1,725 858
CAPITALEXPENDITURE
(Payments) to acquire tangible fixed assets (31,209) (26,964)
Receipts from sale of tangible fixed assets 18,285 10,813
(Payments) to acquire intangible assets 0 0
Receipts from sale of intangible assets 0 0
(Payments to acquire)/receipts from sale of fixed asset investments 0 0
Net cash inflow/(outflow) from capital expenditure (12,924) (16,151)
CONTINUED
STATEMENT OF TOTAL RECOGNISED GAINS AND LOSSES FOR THE YEAR ENDED 31 MARCH 2008
CASH FLOW STATEMENT FOR THE YEAR ENDED 31 MARCH 2008
64 Financial report continued

2007/08 2006/07
NOTE £000 £000
DIVIDENDS PAID (14,642) (14,215)
Net cash inflow/(outflow) before management of liquid resources and financing 24,556 (3,002)
MANAGEMENTOFLIQUIDRESOURCES
(Purchase) of investments with DH 0 0
(Purchase) of other current asset investments 0 0
Sale of investments with DH 0 0
Sale of other current asset investments 0 0
Net cash inflow/(outflow) from management of liquid resources 0 0
Net cash inflow/(outflow) before financing 24,556 (3,002)
FINANCING
Public dividend capital received 0 13,823
Public dividend capital repaid (not previously accrued) (19,688) (10,809)
LoansreceivedfromDH 0 0
Other loans received 0 0
LoansrepaidtoDH 0 0
Other loans repaid 0 0
Other capital receipts 527 0
Capital element of finance lease rental payments 0 0
Cash transferred (to)/from other NHS bodies 0 0
Net cash inflow/(outflow) from financing (19,161) 3,014
Increase/(decrease) in cash 5,395 12
CASH FLOW STATEMENT FOR THE YEAR ENDED 31 MARCH 2008 CONTINUED
65

66 Financial report - notes to the accounts1. Accounting policies
The Secretary of State for Health has directed that the financial statements of NHS trusts shall meet the accounting requirements of the NHS Trust Manual for Accounts which shall be agreed with HM Treasury. The accounting policies contained in that manual follow UK generally accepted accounting practice and HM Treasury’s Government Financial Reporting Manual to the extent that they are meaningful and appropriate to the NHS. The accounting policies have been applied consistently in dealing with items considered material in relation to the accounts.
1.1 Accounting convention
These accounts have been prepared under the historical cost convention modified to account for the revaluation of fixed assets at their value to the business by reference to their current costs. NHS Trusts are not required to provide a reconciliation between current cost and historical cost surpluses and deficits.
1.2 Acquisitions and discontinued
operations
Activities are considered to be ‘acquired’ only if they are acquired from outside the public sector.
Activities are considered to be ‘discontinued’ only if they cease entirely. They are not considered to be ‘discontinued’ if they transfer from one public sector body to another.
1.3 Income recognition
Income is accounted for applying the accruals convention. The main source of income for the Trust is from commissioners in respect of healthcare services provided under local agreements. Income is recognised in the period in which services are provided. Where income is received for a specific activity which is to be delivered in the following financial year, that income is deferred.
1.4 Intangible fixed assets
Intangible assets are capitalised when they are capable of being used in a Trust’s activities for more than one year, they can be valued and they have a cost of at least£5,000.
Intangible fixed assets held for operational use are valued at historical cost and are depreciated over the estimated life of the asset on a straight line basis, except capitalised research and development which is revalued using an appropriate index
figure. The carrying value of intangible assets is reviewed for impairment at the end of the first full year following acquisition and in other periods if events or changes in circumstances indicate the carrying value may not be recoverable.
Purchased computer software licences are capitalised as intangible fixed assets where expenditureofatleast£5,000is incurred. They are amortised over the shorter of the term of the licence and their useful economic lives.
1.5 Tangible fixed assets
Capitalisation Tangible assets are capitalised if
they are capable of being used for a period which exceeds one year and they:
• individuallyhaveacostofatleast£5,000;or
• collectivelyhaveacostofatleast£5,000andindividuallyhaveacostofmorethan£250,where the assets are functionally interdependent, they had broadly simultaneous purchase dates, are anticipated to have simultaneous disposal dates and are under single managerial control; or
• formpartoftheinitialequippingand setting-up cost of a new

67building, ward or unit irrespective of their individual or collective cost.
Valuation Tangible fixed assets are stated
at the lower of replacement cost and recoverable amount. On initial recognition they are measured at cost (for leased assets, fair value) including any costs such as installation directly attributable to bringing them into working condition. They are restated to current value each year. The carrying values of tangible fixed assets are reviewed for impairment in periods if events or changes in circumstances indicate the carrying value may not be recoverable.
All land and buildings are restated to current value using professional valuations in accordancewithFRS15everyfive years and in the intervening years by the use of indices. The buildings index is based on the All in Tender Price Index published by the Building Cost Information Service (BCIS). The land index is based on the residential building land values reported in the Property Market Report published by the Valuation Office.
Professional valuations are carried out by the District Valuers
of the Revenue and Customs Government Department. The valuations are carried out in accordance with the Royal Institute of Chartered Surveyors (RICS) Appraisal and Valuation Manual insofar as these terms are consistent with the agreed requirements of the Department of Health and HM Treasury. In accordance with the requirements of the Department of Health, the last asset valuations were undertakenin2004asattheprospective valuation date of 1 April2005andwereappliedonthe31March2005.
The valuations are carried out primarily on the basis of depreciated replacement cost for specialised operational property and existing use value for non-specialised operational property. The value of land for existing use purposes is assessed at existing use value. For non-operational properties including surplus land, the valuations are carried out at open market value.
Additional alternative open market value figures have only been supplied for operational assets scheduled for imminent closure and subsequent disposal.
All adjustments arising from indexation and five-yearly revaluations are taken to the revaluation reserve. Falls in value when newly constructed assets are brought into use are also charged there. These falls in value result from the adoption of ideal conditions as the basis for depreciated replacement cost valuations.
Assets in the course of construction are valued at current cost using the indexes as for land and buildings, as above. These assets include any existing land or buildings under the control of a contractor.
Residual interests in off-balance sheet Private Finance Initiative properties are included in tangible fixed assets as ‘assets under construction and payments on account’ where the PFI contract specifies the amount, or nil value at which the assets will be transferred to the Trust at the end of the contract. The residual interest is built up, on an actuarial basis, during the life of the contract by capitalising part of the unitary charge so that at the end of the contract the balance sheet value of the residual value plus the specified amount equal the

68 Financial report - notes to the accounts continuedexpected fair value of the residual asset at the end of the contract. The estimated fair value of the asset on reversion is determined by the district valuer based on Department of Health guidance. The district valuer should provide an estimate of the anticipated fair value of the assets on the same basis as the district valuer values the NHS Trust’s estate.
Operational equipment other than IT equipment, which is considered to have nil inflation, is valued at net current replacement cost through annual uplift by the change in the value of the GDP deflator. Equipment surplus to requirements is valued at net recoverable amount.
Depreciation, amortisation and
impairments
Tangible fixed assets are depreciated at rates calculated to write them down to estimated residual value on a straight-line basis over their estimated useful lives. No depreciation is provided on freehold land and assets surplus to requirements.
Assets in the course of construction and residual interests in off-balance sheet PFI contract assets are not depreciated until
the asset is brought into use or reverts to the Trust, respectively.
Buildings, installations and fittings are depreciated on their current value over the estimated remaining life of the asset as advised by the district valuer. Leaseholds are depreciated over the primary lease term.
Equipment is depreciated on current cost evenly over the estimated life of the asset.
Impairment losses resulting from short-term changes in price that are considered to be recoverable in the longer term are taken in full to the revaluation reserve. These include impairments resulting from the revaluation of fixed assets from their cost to their value in existing use when they become operational. This may lead to a negative revaluation reserve in certain instances.
Where, under financial reporting standard 11, a fixed asset impairment is charged to the income and expenditure account, offsetting income may be paid by the Trust’s main commissioner using funding provided by the NHS bank.
1.6 Donated fixed assets
Donated fixed assets are capitalised at their current value on receipt and this value is credited to the donated asset reserve. Donated fixed assets are valued and depreciated as described above for purchased assets. Gains and losses on revaluations are also taken to the donated asset reserve and, each year, an amount equal to the depreciation charge on the asset is released from the donated asset reserve to the income and expenditure account. Similarly, any impairment on donated assets charged to the income and expenditure account is matched by a transfer from the donated asset reserve. On sale of donated assets, the value of the sale proceeds is transferred from the donated asset reserve to the income and expenditure reserve.
1.7 Government grants
Government grants are grants from government bodies other than funds from NHS bodies or funds awarded by Parliamentary Vote. The government grants reserve is maintained at a level equal to the net book value of the assets which it has financed. Gains and losses on revaluations are also taken to the Government grant

69reserve and, each year, an amount equal to the depreciation charge on the asset is released from the Government grant reserve to the income and expenditure account. Similarly, any impairment on grant funded assets charged to the income and expenditure account is matched by a transfer from the reserve.
1.8 Private Finance Initiative (PFI)
transactions
The NHS follows HM Treasury’s technical note 1 (Revised) “How to account for PFI transactions” which provides practical guidance for the application of the applicationnoteFtoFRS5andthe guidance ‘Land and Buildings in PFI schemes Version 2’.
Where the balance of the risks and rewards of ownership of the PFI property are borne by the PFI operator, the PFI obligations are recorded as an operating expense. Where the trust has contributed assets, a prepayment for their fair value is recognised and amortised over the life of the PFI contract by charge to the income and expenditure account. Where, at the end of the PFI contract, a property reverts to the Trust, the difference between the expected fair value of the residual on
reversion and any agreed payment on reversion is built up over the life of the contract by capitalising part of the unitary charge each year, as a tangible fixed asset.
Where the balance of risks and rewards of ownership of the PFI property are borne by the Trust, it is recognised as a fixed asset along with the liability to pay for it which is accounted for as a finance lease. Contract payments are apportioned between an imputed finance lease charge and a service charge.
1.9 Stocks and work-in-progress
Stocks and work-in-progress are valued at the lower of cost and net realisable value. This is considered to be a reasonable approximation to current cost due to the high turnover of stocks. Work-in-progress comprises goods in intermediate stages of production. Partially completed contracts for patient services are not accounted for as work-in-progress.
Research and development
Expenditure on research is not capitalised. Expenditure on development is capitalised if it meets the following criteria:
• thereisaclearlydefinedproject;
• therelatedexpenditureisseparately identifiable;
• theoutcomeoftheprojecthasbeen assessed with reasonable certainty as to:
- its technical feasibility;- its resulting in a product or
service which will eventually be brought into use;
• adequateresourcesexist,orare reasonably expected to be available, to enable the project to be completed and to provide any consequential increases in working capital.
Expenditure so deferred is limited to the value of future benefits expected and is amortised through the income and expenditure account on a systematic basis over the period expected to benefit from the project. It is revalued on the basis of current cost. The amortisation charge is calculated on the same basis as used for depreciation i.e. on a quarterly basis. Expenditure which does not meet the criteria for capitalisation is treated as an operating cost in the year in which it is incurred. NHS Trusts are unable to disclose the total amount of research and development expenditure charged in the income

70and expenditure account because some research and development activity cannot be separated from patient care activity.
Fixed assets acquired for use in research and development are amortised over the life of the associated project.
1.11 Provisions
The Trust provides for legal or constructive obligations that are of uncertain timing or amount at the balance sheet date on the basis of the best estimate of the expenditure required to settle the obligation. Where the effect of the time value of money is material, the estimated risk-adjusted cash flows are discounted using the Treasury’sdiscountrateof2.2%in real terms.
Clinical negligence costs
The NHS Litigation Authority (NHSLA) operates a risk pooling scheme under which the NHS Trust pays an annual contribution to the NHSLA which in return settles all clinical negligence claims. Although the NHSLA is administratively responsible for all clinical negligence cases the legal liability remains with the Trust. The total value of clinical negligence provisions carried by
the NHSLA on behalf of the Trust isdisclosedatnote16.
Since financial responsibility for clinical negligence cases transferred to the NHSLA at 1 April 2002, the only charge to operating expenditure in relation toclinicalnegligencein2007/08relates to the Trust’s contribution to the Clinical Negligence Scheme for Trusts.
Non-clinical risk pooling
The Trust participates in the Property Expenses Scheme and the Liabilities to Third Parties Scheme. Both are risk pooling schemes under which the Trust pays an annual contribution to the NHS Litigation Authority and, in return, receives assistance with the costs of claims arising. The annual membership contributions, and any ‘excesses’ payable in respect of particular claims are charged to operating expenses as and when they become due.
1.12 Pension costs
Past and present employees are covered by the provisions of the NHS Pensions Scheme. Details of the benefits payable under these provisions can be found on the NHS Pensions website at www.pensions.nhsbsa.nhs.uk. The
Scheme is an unfunded, defined benefit scheme that covers NHS employers, General Practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying Scheme assets and liabilities. Therefore, the Scheme is accounted for as if it were a defined contribution scheme: the cost to the NHS body of participating in the Scheme is taken as equal to the contributions payable to the Scheme for the accounting period.
The Scheme is subject to a full actuarial valuation every four years(until2004,basedonafiveyearvaluationcycle),andaFRS17accounting valuation every year. An outline of these follows:
a. Full actuarial (funding) valuation
The purpose of this valuation is to assess the level of liability in respect of the benefits due under the scheme (taking into account its recent demographic experience), and to recommend the contribution rates to be paid by employers and scheme members. The last such valuation, which determined current contribution rates was
Financial report - notes to the accounts continued

71undertakenasat31March2004and covered the period from 1 April1999tothatdate.
Theconclusionfromthe2004valuation was that the Scheme had accumulated a notional deficit of £3.3billionagainstthenotionalassetsasat31March2004.However, after taking into account the changes in the benefit and contribution structure effective from 1 April 2008, the Scheme actuary reported that employer contributions could continue at the existingrateof14%ofpensionablepay. On advice from the Scheme actuary, scheme contributions may be varied from time to time to reflect changes in the scheme’s liabilities.Upto31March2008,the vast majority of employees paid contributionsattherateof6%of pensionable pay. From 1 April 2008, employees contributions areonatieredscalefrom5%upto8.5%oftheirpensionablepaydepending on total earnings.
b. FRS17 Accounting valuation
InaccordancewithFRS17,avaluation of the Scheme liability is carried out annually by the Scheme actuary as at the balance sheet date by updating the results of the full actuarial valuation.
Between the full actuarial valuations at a two-year midpoint, a full and detailed member data-set is provided to the Scheme actuary. At this point the assumptions regarding the composition of the Scheme membership are updated to allow the Scheme liability to be valued.
The valuation of the Scheme liabilityasat31March2008,isbased on detailed membership dataasat31March2006(thelatestmidpoint)updatedto31March 2008 with summary global member and accounting data.
The latest assessment of the liabilities of the Scheme is contained in the Scheme actuary report, which forms part of the annual NHS Pension Scheme (England and Wales) Resource Account, published annually. These accounts can be viewed on the NHS Pensions website. Copies can also be obtained from The Stationery Office.
Scheme provisions as at 31 March 2008
The Scheme is a “final salary” scheme. Annual pensions are normally based on 1/80th of thebestofthelast3yearspensionable pay for each year
of service. A lump sum normally equivalentto3yearspensionispayable on retirement. Annual increases are applied to pension payments at rates defined by the Pensions(Increase)Act1971,and are based on changes in retail prices in the twelve months ending30Septemberintheprevious calendar year. On death, apensionof50%ofthemember’spension is normally payable to the surviving spouse.
Early payment of a pension, with enhancement, is available to members of the Scheme who are permanently incapable of fulfilling their duties effectively through illness or infirmity. A death gratuity of twice final year’s pensionable pay for death in service, and five times their annual pension for death after retirement, less pension already paid, subject to a maximum amount equal to twice the member’s final year’s pensionable pay less their retirement lump sum for those who die after retirement, is payable.
For early retirements other than those due to ill health the additional pension liabilities are not funded by the scheme. The full amount of the liability for the

72additional costs is charged to the income and expenditure account at the time the Trust commits itself to the retirement, regardless of the method of payment.
The Scheme provides the opportunity to members to increase their benefits through money purchase additional voluntary contributions (AVCs) provided by an approved panel of life companies. Under the arrangement the employee/member can make contributions to enhance an employee’s pension benefits. The benefits payable relate directly to the value of the investments made.
Scheme provisions from 1 April 2008
From 1 April 2008 changes have been made to the NHS Pension Scheme contribution rates and benefits. Further details of these changes can be found on the NHS Pensions website www.pensions.nhsbsa.nhs.uk.
1.13Liquidresources
Deposits and other investments that are readily convertible into known amounts of cash at or close to their carrying amounts are treated as liquid resources in the cashflow statement. The Trust
does not hold any investments with maturity dates exceeding one year from the date of purchase.
1.14 Value Added Tax
Most of the activities of the Trust are outside the scope of VAT and, in general, output tax does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of fixed assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT.
1.15 Foreign Exchange
Transactions that are denominated in a foreign currency are translated into sterling at the exchange rate ruling on the dates of the transactions. Resulting exchange gains and losses are taken to the Income and Expenditure Account.
1.16 Third Party Assets
Assets belonging to third parties (such as money held on behalf of patients) are not recognised in the accounts since the Trust has no beneficial interest in them. Details of third party assets are given in Note 28 to the accounts.
1.17 Leases
Where substantially all risks and rewards of ownership of a leased asset are borne by the NHS Trust, the asset is recorded as a tangible fixed asset and a debt is recorded to the lessor of the minimum lease payments discounted by the interest rate implicit in the lease. The interest element of the finance lease payment is charged to the income and expenditure account over the period of the lease at a constant rate in relation to the balance outstanding. Other leases are regarded as operating leases and the rentals are charged to the income and expenditure account on a straight-line basis over the term of the lease.
1.18 Public Dividend Capital (PDC) and
PDC Dividend
Public dividend capital represents the outstanding public debt of an NHS Trust. At any time the Secretary of State can issue new PDC to, and require repayments of PDC from, the NHS Trust.
A charge, reflecting the forecast cost of capital utilised by the NHS Trust, is paid over as public dividend capital dividend. The charge is calculated at the real rate set by HM Treasury (currently 3 5%)ontheforecastaverage
Financial report - notes to the accounts continued

At the launch of Roch Valley Radio are station manager Bob Chadwick (seated) with (from the left) the Mayor of Rochdale, Councillor Robin Parker; BBC Radio Manchester presenter, Eamonn O’Neal, and the Mayor of Bury, Councillor Peter Ashworth.Roch Valley radio entertains patients in Rochdale Infirmary and Fairfield General Hospital
73carrying amount of all assets less liabilities, except for donated assets and cash with the Office of the Paymaster General. The average carrying amount of assets is calculated as a simple average of opening and closing relevant net assets. A note to the accounts discloses the rate that the dividend represents as a percentage of the actual average carrying amount of assets less liabilities in the year.
1.19LossesandSpecialPayments
Losses and special payments are items that Parliament would not have contemplated when it agreed funds for the health service or passed legislation. By their nature they are items that ideally should not arise. They are therefore subject to special control procedures compared with the generality of payments. They are divided into different categories, which govern the way each individual case is handled.
Losses and special payments are charged to the relevant functional headings in the income and expenditure account on an accruals basis, including losses which would have been made good through insurance cover had NHS Trusts not been bearing their own risks (with insurance
premiums then being included as normal revenue expenditure).
1.20 EU Emissions Trading Scheme
EU Emission Trading Scheme allowances are accounted for as government granted current asset investments, valued at open market value. As the Trust makes emissions a provision is recognised, with an offsetting transfer from the government
grant reserve. The provision is settled on surrender of the allowances. The current asset investment, provision and government grant reserve are valued at current market value at the balance sheet date.

£000 £000
Patient transport services 0 0
Education, training and research 18,334 16,580
Charitable and other contributions to expenditure
68 85
Transfers from donated asset reserve 635 572
Transfers from government grant reserve
0 9
Non-patient care services to other bodies 19,007 19,239
Income generation 4,888 4,665
Other income 2,870 2,664
45,802 43,814
£000 £000
Strategic Health Authorities 0 0
NHS Trusts 0 0
Primary Care Trusts* 420,610 392,778
Foundation Trusts 0 0
LocalAuthorities 20 26
Department of Health 27,567 32,354
NHS Other 0 0
Non NHS:
- Private patients 358 405
- Overseas patients (non- reciprocal) 294 296
- Injury cost recovery /Road Traffic Act 3,553 3,171 - Pharmacy 859 530
- Non English NHS bodies 215 201
- Other 166 121
453,642 429,882
*Includes£4,134,000tooffsetfixedassetimpairments charged to operating expenses.
The RTA cost recovery scheme was extended to includepersonalinjuryfromJanuary2007andisnow known as injury cost recovery.
Injury cost recovery income is subject to a provision fordoubtfuldebtsof7.8%toreflectexpectedratesof collection.
4. Other Operating Income
2007/08 2006/07 2007/08 2006/07
742. Segmental Analysis
The Pennine Acute Hospitals NHS Trust was not a lead foranyconsortiumatthebalancesheetdateof31stMarch 2008.
3. Income from Activities
Financial report - notes to the accounts continued

£000 £000
Services from other NHS Trusts 3,750 3,859
Services from PCTs 4,877 4,148
Services from other NHS bodies 4,140 4,072
Services from Foundation Trusts 847 816
Purchase of healthcare from non NHS bodies 1,858 654
Directors’ costs 1,180 1,226
Staff costs 316,752 311,381
Supplies and services - clinical 69,496 62,716
Supplies and services - general 12,745 12,498
Consultancy services 682 1,480
Establishment 5,181 5,498
Transport 1,091 1,055
Premises 14,850 15,606
Bad debts 839 48
Depreciation 21,727 17,460
Amortisation 666 499
Fixed asset impairments and reversals 4,134 12,075
Audit fees 320 317
Clinical negligence premium 7,010 6,622
Security 1,537 1,560
Interpreter fees 777 657
Clinical waste 739 625
Training 913 853
Insurance 543 574
Legalfees 491 945
Employers liability and permanent injury benefit 404 902
Other 1,626 942
479,175 469,088
5. Operating Expenses
5.1 Operating expenses comprise:
2007/08 2006/07
75

2007/08 2006/07 2007/08 2006/07
£000 £000 £000 £000
Operating leases which expire:
Within 1 year 72 61 40 44
Between 1 and 5 years 0 0 121 87
After 5 years 0 0 0 0
72 61 161 131
2007/08 2006/07
£000 £000 £000 £000
Salaries and wages 267,415 261,598 5,817 264,397
Social Security Costs 21,224 21,224 0 19,469
Employer contributions to NHS Pension Scheme 29,232 29,232 0 28,680
317,871 312,054 5,817 312,546
5.2 Operating leases
5.2/1 Operating expenses include:
£000 £000
Hire of plant and machinery 171 230
Other operating lease rentals 72 61
243 291
TOTALPERMANENTLY
EMPLOYED OTHER
Land and buildings Other leases
2007/08 2006/07
76
5.2/2 Annual commitments under non - cancellable operating leases are:
6. Staff costs and numbers
6.1 Staff costs
Financial report - notes to the accounts continued

2007/08 2006/07
Number Number Number Number
Medical and dental 1,044 1,005 39 1,037
Ambulance staff 0 0 0 0
Administration and estates 2,035 2,008 27 2,072
Healthcare assistants and other support staff 761 720 41 805
Nursing, midwifery and health visiting staff 3,944 3,922 22 4,106
Nursing, midwifery and health visiting learners 89 89 0 113
Scientific, therapeutic and technical staff 999 992 7 1,016
Total 8,872 8,736 136 9,149
TOTALPERMANENTLY
EMPLOYED OTHER
£000 £000
Management costs 15,757 16,687
Income 486,363 460,010
2007/08 2006/07
776.2 Average number of persons employed
6.3 Employee benefits
Therewerenoemployeebenefitsin2007/08or2006/07.
6.4 Management costs
Management costs are defined as those on the management costs website at www.dh.gov.uk/PolicyAndGuidance/OrganisationPolicy/FinanceAndPlanning/NHSManagementCosts/fs/en.
6.5 Retirements due to ill-health
During2007/08therewere23(2006/07,29)earlyretirementsfromtheNHS Trust on the grounds of ill-health. The estimated additional pension liabilitiesoftheseill-healthretirementswillbe£1,242,481(£1,786,854).The cost of these ill-health retirements will be borne by the NHS Business Services Authority - Pensions Division.

£000 £000
Profit on disposal of land and buildings 2,409 0
Profits on disposal of plant and equipment 8 2
(Loss)ondisposalofplantandequipment (131) (183)
2,286 (181)
Number £000
Total Non-NHS trade invoices paid in the year 128,492 136,068
Total Non NHS trade invoices paid within target 126,205 133,531
Percentage of Non-NHS trade invoices paid within target 98% 98%
Total NHS trade invoices paid in the year 5,600 36,333
Total NHS trade invoices paid within target 5,350 35,498
Percentage of NHS trade invoices paid within target 96% 98%
2007/08
2007/08 2006/07
787. Better Payment Practice Code
7.1 Better Payment Practice Code - measure of compliance
The Better Payment Practice Code requires the Trust to aim to pay all undisputedinvoicesbytheduedateorwithin30daysofreceiptofgoodsor a valid invoice, whichever is later.
7.2 TheLatePaymentofCommercialDebts(Interest)Act1998
The Trust did not incur any interest charges in relation to late payment of debtsfor2007/08or2006/07.
8. Profit/(Loss)onDisposalofFixedAssets
Profit/(loss) on the disposal of fixed assets is made up as follows:
Profit on disposal relates mainly to Birch Hill.
9. Interest Payable
TheTrustdidnotincuranyinterestpayablein2007/08or2006/07.
Financial report - notes to the accounts continued

Bio medical scientists Louise Grundy and Amina Khatum show Professor Bruce Keogh, medical director of the NHS, some of the features of the new £17.5 million pathology laboratory at The Royal Oldham Hospital.
£000
Gross cost at 1 April 2007 3,613
Indexation
Impairments 0
Reclassifications 1,429
Revaluation 0
Additions purchased 2,152
Additions donated 0
Additions government granted 0
Disposals (13)
Gross cost at 31 March 2008 7,181
Amortisation at 1 April 2007 1,947
Indexation
Impairments 0
Reversal of impairments 0
Reclassifications 0
Revaluation 0
Charged during the year 666
Disposals (10)
Amortisation at 31 March 2008 2,603
Net book value
- Purchased at 1 April 2007 1,666
- Donated at 1 April 2007 0
- Government granted at 1 April 2007 0
- Total at 1 April 2007 1,666
- Purchased at 31 March 2008 4,578
- Donated at 31 March 2008 0
- Government granted at 31 March 2008 0
- Total at 31 March 2008 4,578
10. Intangible Fixed Assets
Software licences
79
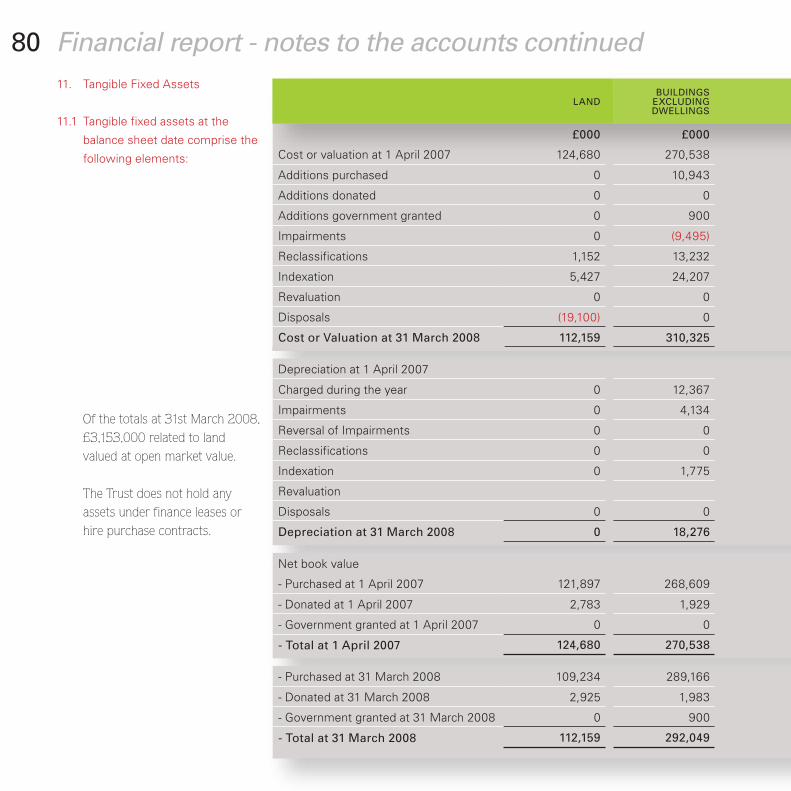
£000 £000
Cost or valuation at 1 April 2007 124,680 270,538
Additions purchased 0 10,943
Additions donated 0 0
Additions government granted 0 900
Impairments 0 (9,495)
Reclassifications 1,152 13,232
Indexation 5,427 24,207
Revaluation 0 0
Disposals (19,100) 0
Cost or Valuation at 31 March 2008 112,159 310,325
Depreciation at 1 April 2007
Charged during the year 0 12,367
Impairments 0 4,134
Reversal of Impairments 0 0
Reclassifications 0 0
Indexation 0 1,775
Revaluation
Disposals 0 0
Depreciation at 31 March 2008 0 18,276
Net book value
- Purchased at 1 April 2007 121,897 268,609
- Donated at 1 April 2007 2,783 1,929
- Government granted at 1 April 2007 0 0
- Total at 1 April 2007 124,680 270,538
- Purchased at 31 March 2008 109,234 289,166
- Donated at 31 March 2008 2,925 1,983
- Government granted at 31 March 2008 0 900
- Total at 31 March 2008 112,159 292,049
11. Tangible Fixed Assets
11.1 Tangible fixed assets at the
balance sheet date comprise the
following elements:
Ofthetotalsat31stMarch2008,£3,153,000relatedtolandvalued at open market value.
The Trust does not hold any assets under finance leases or hire purchase contracts.
LAND BUILDINGS
EXCLUDING DWELLINGS
80 Financial report - notes to the accounts continued

£000 £000 £000 £000 £000 £000 £000
586 17,120 96,107 1,655 11,881 975 523,542
0 1,816 4,088 33 6,551 196 23,627
0 0 38 0 0 0 38
0 0 0 0 0 0 900
0 0 0 0 0 0 (9,495)
(3) (16,994) 791 104 317 (28) (1,429)
52 0 1,327 25 0 21 31,059
0 0 0 0 0 0 0
0 0 (14,216) (282) 0 (35) (33,633)
635 1,942 88,135 1,535 18,749 1,129 534,609
64,496 1,118 5,442 465 71,521
19 7,099 118 1,991 133 21,727
0 0 0 0 0 0 4,134
0 0 0 0 0 0 0
0 0 0 0 0 0
3 474 9 8 2,269
0 0 0 0 0
0 (14,098) (282) 0 (26) (14,406)
22 0 57,971 963 7,433 580 85,245
586 17,120 28,591 499 6,439 510 444,251
0 0 3,020 38 0 0 7,770
0 0 0 0 0 0 0
586 17,120 31,611 537 6,439 510 452,021
613 1,942 27,556 529 11,316 549 440,905
0 0 2,608 43 0 0 7,559
0 0 0 0 0 0 900
613 1,942 30,164 572 11,316 549 449,364
DWELLINGS
ASSETS UNDER CONSTRUCTION AND PAYMENTS
ON ACCOUNT
PLANT AND MACHINERY
TRANSPORT EQUIPMENT
INFORMATION TECHNOLOGY
FURNITURE & FITTINGS TOTAL
81

11.2 The net book value of land, buildings and dwellings at 31 March 2008 comprises:
£000 £000
Freehold 404,653 395,645
Longleasehold 168 159
Short leasehold 0 0
TOTAL 404,821 395,804
12. Stocks and Work in Progress
£000 £000
Raw materials and consumables 7,707 7,253
13. Debtors
Amounts falling due within one year:£000 £000
NHS debtors 16,189 22,138
Provision for irrecoverable debts :
- Overseas visitors (428) (201)
- Other (108) (71)
Other prepayments and accrued income 1,468 1,525
VAT 1,696 914
Other debtors 2,537 3,092
Sub Total 21,354 27,397
Amounts falling due after more than one year:
Capital debtors 3,226 0
Injury cost recovery / Road Traffic Act 5,993 5,613
Provision for irrecoverable debts - Injury cost recovery (925) (432)
Sub Total 8,294 5,181
TOTAL 29,648 32,578
31 March 2008 31 March 2007
31 March 2008 31 March 2007
31 March 2008 31 March 2007
82 Financial report - notes to the accounts continued

Fairfield General Hospital hosted a top level conference on children’s healthcare. Pictured from the left: consultant paediatrician, Dr Umesh Prabhu, who organised the event; speaker Professor Patricia Hamilton, president of the Royal College of Paediatricians; Dr Ruth Jameson, the Trust’s medical director, and speaker Peter Walsh, chief executive of Action against Medical Accidents.
£000
Balance at 1 April 2007 12
Additions 0
Disposals 0
Revaluations (12)
Balance at 31 March 2008 0
14. Investments
14.1 Fixed Asset Investments
The Trust does not hold any fixed asset investments.
14.2 Current Asset Investments
15. Creditors
15.1 Creditors at the balance sheet date are made up of:
Amounts falling due within one year: £000 £000
Payments received on account 70 63
NHS creditors 3,466 2,889
Non - NHS trade creditors - revenue 2,486 2,075
Non - NHS trade creditors - capital 6,921 11,133
Tax 502 5,334
Social security costs 519 4,007
Pension creditors 4,460 4,351
Other creditors 1,228 828
Accruals and deferred income 18,357 13,027
Total 38,009 43,707
TheTrusthasnoamountsfallingdueaftermorethanoneyearineither2007/08or2006/07.
15.2Loans,otherlong-termfinancialliabilitiesandfinanceleases.-
TheTrusthadnoloans,otherlongtermfinancialliabilitiesnorfinanceleasesat31stMarch2008.
EU emissions trading scheme
31 March 2008 31 March 2007
83

Pictured at a training session for an emergency incident at Rochdale Infirmary are,
from the left: John Lindars, divisional director for women and children’s; Cathy
Trinick, head of midwifery, and Dr Egware Odeka, associate medical director for
women and children’s.
£000 £000 £000 £000 £000
At 1 April 2007 3,954 397 2,435 6,678 13,464
Arising during the year 119 166 73 1,208 1,566
Utilised during the year (286) (199) (281) (855) (1,621)
Reversed unused 0 (70) 0 (600) (670)
Unwinding of discount 87 0 54 73 214
At 31 March 2008 3,874 294 2,281 6,504 12,953
Expected timing of cashflows:Within one year 285 196 282 1,940 2,703
Between one and five years 1,139 98 1,126 1,855 4,218
After five years 2,450 0 873 2,709 6,032
Pensions relating to other staff
Legalclaims Restructurings Other Total
8416. Provisions for liabilities and charges
Other provisions relate mainly to permanent injury benefits payable, residual effects of pay banding appeals, contract issues and changes to pay.
Financial report - notes to the accounts continued
£55,777,751isincludedintheprovisionsoftheNHSLitigationAuthorityat31March2008inrespectofclinicalnegligenceliabilitiesoftheNHSTrust(31March2007£44,648,150)

£000 £000 £000 £000 £000
At 1 April 2007 as previously stated 188,356 7,770 12 (1,513) 194,625
Prior Period Adjustments 0 0 0 0 0
At 1 April 2007 as restated 188,356 7,770 12 (1,513) 194,625
Transfer from the income and expenditure account 0 0 0 9,472 9,472
Fixed asset impairments (9,495) 0 0 0 (9,495)
Surplus/(deficit) on other revaluations/indexation of fixed/current assets 28,405 386 (12) 0 28,779
Transfer of realised profits/(losses) to the income and expenditure reserve (22,011) 0 0 22,011 0
Receipt of donated/government granted assets 0 38 900 0 938
Transfers to the income and expenditure account for depreciation, impairment, and disposal of donated/government granted assets 0 (635) 0 0 (635)
At 31 March 2008 185,255 7,559 900 29,970 223,684
Revaluation Reserve
Donated Asset
Reserve
Government Grant
Reserve
Income and Expenditure
ReserveTotal
8517. Movements on Reserves
Movements on reserves in the year comprised the following:

£000 £000
Total operating surplus/(deficit) 20,269 4,608
Depreciation and amortisation charge 22,393 17,959
Fixed asset impairments and reversals 4,134 12,075
Transfer from donated asset reserve (635) (572)
Transfer from the government grant reserve 0 (9)
(Increase)/decrease in stocks (454) 554
(Increase)/decrease in debtors 5,687 (13,951)
Increase/(decrease) in creditors (272) 4,702
Increase/(decrease) in provisions (725) 1,140
Net cash inflow/(outflow) from operating activities before restructuring costs 50,397 26,506
Payments in respect of fundamental reorganisation/restructuring 0 0
Net cash inflow from operating activities 50,397 26,506
£000 £000
Increase/(decrease) in cash in the period 5,395 12
Cash (inflow) from new debt 0 0
Cash outflow from debt repaid and finance lease capital payments 0 0
Cash (inflow)/outflow from (decrease)/increase in liquid resources 0 0
Change in net debt resulting from cash flows 5,395 12
Non - cash changes in debt (12) 12
Net debt at 1 April 2007 1,381 1,357
Net debt at 31 March 2008 6,764 1,381
2007/08 2006/07
2007/08 2006/07
86 Financial report - notes to the accounts continued18. Notes to the cash flow Statement
18.1 Reconciliation of operating surplus to net cash flow from operating activities:
18.2 Reconciliation of net cash flow to movement in net debt

£000 £000 £000 £000
OPG cash at bank 1,171 5,484 6,655
Commercial cash at bank and in hand 198 (89) 109
Bank overdraft 0 0 0
LoanfromDHduewithinoneyear 0 0 0 0
Other debt due within one year 0 0 0 0
LoanfromDHdueafteroneyear 0 0 0 0
Other debt due after one year 0 0 0 0
Finance leases 0 0 0 0
Current asset investments 12 0 (12) 0
1,381 5,395 (12) 6,764
At 1 April 2007 Other cash changes in year
Non-cash changes in year
At 31 March 2008
£000 £000
Contingent liabilities* (147) (189)
2007/08 2006/07
87
*The Trust’s liability to third parties (public and employer’s) under the scheme operatedbytheNHSLAamountsto£147,470.
19. Capital Commitments
Commitmentsundercapitalexpenditurecontractsat31stMarch2008were£2,223,000(31stMarch2007£7,727,000).
20. Post Balance Sheet Events
There are no Post Balance Sheet Events which have a material effect on the accounts.
21. Contingencies
18.3 Analysis of changes in net debt

£000 £000
Public Dividend Capital as at 1 April 2007 243,103 240,089
New Public Dividend Capital received (including transfers from dissolved NHS Trusts) 0 13,823
Public Dividend Capital repaid in year (19,688) (10,809)
Public Dividend Capital as at 31 March 2008 223,415 243,103
£000 £000 £000 £000 £000
Turnover 387,225 422,704 446,095 473,696 499,444
Retained surplus/(deficit) for the year 226 1,398 56 (9,170) 9,472
Break-even in-year position 226 1,398 56 (9,170) 9,472
Break-even cumulative position 236 1,634 1,690 (7,480) 1,992
Materiality test (i.e. is it equal to or less than 0.5%):
- Break-even in-year position as a percentage of turnover 0.06% 0.33% 0.01% (1.94%) 1.90%
- Break-even cumulative position as a percentage of turnover 0.06% 0.39% 0.38% (1.58%) 0.40%
2007/08 2006/07
2003/04 2004/05 2005/06 2006/07 2007/08
88 Financial report - notes to the accounts continued
23. Financial Performance Targets
23.1 Breakeven Performance
Thetrust’sbreakevenperformancefor2007/08isasfollows:
22. Movement in Public Dividend Capital

£000 £000 £000
External financing limit (25,073) 3,014
Cash flow financing (24,556) 3,002
Finance leases taken out in the year 0 0
Other capital receipts (527) 0
External financing requirement (25,083) 3,002
Undershoot/(overshoot) 10 12
£000 £000
Gross capital expenditure 26,717 34,175
Less:bookvalueofassetsdisposedof (19,230) (10,995)
Plus: loss on disposal of donated assets 6 24
Less:capitalgrants (900) 0
Less:donationstowardstheacquisitionoffixedassets (38) (677)
Charge against the capital resource limit 6,555 22,527
Capital resource limit 6,600 22,551
(Over)/Underspend against the capital resource limit 45 24
2007/08 2006/07
2007/08 2006/07
89
23.4CapitalResourceLimit
The Trust is given a capital resource limit which it is not permitted to overspend
23.2 Capital cost absorption rate
TheTrustisrequiredtoabsorbthecostofcapitalatarateof3.5%ofaveragerelevantnet assets. The rate is calculated as the percentage that dividends paid on public dividend capital,totalling£14,642,000,bearstotheaveragerelevantnetassetsof£430,836,000,thatis3.4%.
23.3 External financing
The Trust is given an external financing limit which it is permitted to undershoot.

£000
Oldham PCT Income from activities 108,977
Manchester PCT Income from activities 65,651
Bury PCT Income from activities 80,062
Heywood, Middleton and Rochdale PCT Income from activities 103,159
EastLancashirePCT Income from activities 11,820
Salford PCT Income from activities 5,895
Tameside and Glossop PCT Income from activities 5,381
Western Cheshire PCT Income from activities 23,081
Other PCTs (less than £5m) Income from activities 22,422
Department of Health Income from activities 27,567
NHSLitigationAuthority; Annual contribution to risk pooling 7,479
NHS Purchasing and Supply Agency; Purchase of goods and services 10,543
National Blood Authority Service level agreement 4,501
NHS Pensions Agency Employer’s contributions to NHS Pension Scheme 29,232
Related Party Transaction details Amount
90 Financial report - notes to the accounts continued24. Related Party Transactions
The Pennine Acute Hospitals NHS Trust is a body corporate established by order of the Secretary of State for Health.
During the year none of the Board Members or members of the key management staff or parties related to them has undertaken any material transactions with the Pennine Acute Hospitals NHS Trust.
The Department of Health is regarded as a related party. During the year the Pennine Acute Hospitals NHS Trust has had a significant number of material transactions with the Department, and with other entities for which the Department is regarded as the parent Department. These entities are listed below:
In addition, the Trust has had a number of material transactions with other Government Departments and other central and local Government bodies. Most of these transactions have been with Bury MBC, Oldham MBC, Rochdale MBC and Manchester City Council.

9125. Private Finance Transactions
The Trust has no PFI schemes.
26. Pooled Budget
The Trust has not participated in pooled budget projectsduring2007/08.
27 Financial Instruments
FRS13,derivativesandotherfinancialinstruments,requires disclosure of the role that financial instruments have had during the period in creating or changing the risks an entity faces in undertaking its activities. Because of the continuing service provider relationship that the NHS Trust has with local primary care trusts and the way those primary care trusts are financed, the NHS Trust is not exposed to the degree of financial risk faced by business entities. Also financial instruments play a much more limited role in creating or changing risk than would be typical of the listed companies to whichFRS13mainlyapplies.TheNHSTrusthaslimitedpowers to borrow or invest surplus funds and financial assets and liabilities are generated by day-to-day operational activities rather than being held to change the risks facing the NHS Trust in undertaking its activities.
AsallowedbyFRS13,debtorsandcreditorsthataredue to mature or become payable within 12 months from the balance sheet date have been omitted from all disclosures other than the currency profile.
Liquidity risk The NHS Trust’s net operating costs are incurred
under annual service agreements with local primary care trusts, which are financed from resources voted annually by Parliament. The Trust also largely finances its capital expenditure from funds made available from Government under an agreed borrowing limit. The Pennine Acute Hospitals NHS Trust is not, therefore, exposed to significant liquidity risks.
Interest-RateRisk 100%oftheTrust’sfinancialassetsand100%ofits
financial liabilities carry nil or fixed rates of interest. The Pennine Acute Hospitals NHS Trust is not, therefore, exposed to significant interest-rate risk. The following two tables show the interest rate profiles of the Trust’s financial assets and liabilities.

Total Floating
rate Fixed rate
Non-interest bearing
Weighted average interest
rate
Weighted average
period for which
fixed
Weighted average
term
Currency £000 £000 £000 £000 % Years YearsAt 31 March 2008Sterling 6,764 6,764 0 0 0.00% 0 0
Other 0 0 0 0 0.00% 0 0
Gross financial assets 6,764 6,764 0 0
At 31 March 2007
Sterling 1,369 1,369 0 0 0.00% 0 0
Other 0 0 0 0 0.00% 0 0
Gross financial assets 1,369 1,369 0 0
Fixed rate
Non-interest bearing
£000 £000
Financial assets
Cash 6,764 6,764
Book Value Fair Value
92 Financial report - notes to the accounts continued27.1 Financial Assets
27.2FinancialLiabilities
ForFRS13purposes,theTrusthasnomaterialfinancialliabilities.
ForeignCurrencyRisk The Trust has no/negligible foreign currency income or expenditure.
27.3 Fair Values
Set out below is a comparison, by category, of book values and fair values of theNHSTrust’sfinancialassetsandliabilitiesasat31March2008.
Financialliabilities ForFRS13purposes,theTrusthasnomaterialfinancialliabilities.

£000 £000 £000 £000
Balances with other Central Government Bodies 1,983 0 6,146 0
BalanceswithLocalAuthorities 0 0 0 0
Balances with NHS Trusts and Foundation Trusts 15,441 0 2,746 0
Balances with Public Corporations and Trading Funds 12 0 55 0
Balances with bodies external to government 3,918 8,294 29,062 0
At 31 March 2008 21,354 8,294 38,009 0
Balances with other Central Government Bodies 1,181 0 14,420 0
BalanceswithLocalAuthorities 0 0 0 0
Balances with NHS Trusts and Foundation Trusts 21,388 0 2,161 0
Balances with Public Corporations and Trading Funds 92 0 0 0
Balances with bodies external to government 4,304 5,613 27,126 0
At 31 March 2007 26,965 5,613 43,707 0
Debtors: amounts falling due within one
year
Debtors: amounts falling due after more
than one year
Creditors: amounts falling due within one
year
Creditors: amounts falling due after more
than one year
9328 Third Party Assets
TheTrustheld£42,000cashatbankandinhandat31March2008(£54,000-at31March2007)whichrelatestomoniesheldbytheNHSTrustonbehalfofpatients.Thishas been excluded from cash at bank and in hand figure reported in the accounts.
29 Intra-Government and Other Balances
30 LossesandSpecialPayments
Therewere386casesoflossesandspecialpayments(2006/07:535cases)totalling£548,093(2006/07:£580,632)paidduring2007/08.
Showing their support for The Big Drink Debate, the largest ever survey of regional drinking habits, are A&E
consultant, Dr Kassim Ali and senior sister, Penny Yates, both based at Fairfield General Hospital.
94 The Remuneration ReportThe membership of our remuneration committee comprises the chairman and non-executive directors, with the chief executive attending as required. The committee makes recommendations to the Board on the remuneration and terms of service of the chief executive and executive directors, ensuring they are fairly rewarded for their contribution to the Trust.
The chairman undertook a performance assessment of the chief executive measured against achievement of the corporate objectives. The chief executive undertook similar assessments with the other executive directors.
Executives are employed on permanent contracts. The chief executive is
required to give six month’s notice of termination of employment and the executive directors three months.
There are no special guaranteed termination payments or compensation payments for early termination of executives. Executives are subject only to the same redundancy rights as all other employees of the Trust.

2007-08 2006-07
(bands of £5000) (bands of £5000)£000 £000 £000 £000 £000 £000
J Saxby, Chief Executive (from 04/06/2007) 145-150 0 3 0 0 0
C Appleby, Chief Executive (to 14/05/2006) 70-75 0 0
R Chadwick, see note 1 95-100 0 0 155-160 0 0
BLivesey,seenote2 30-35 0 0 95-100 0 0
R Jameson, Medical Director 160-165 0 0 155-160 0 0
M Carroll, Director of Nursing 100-105 0 0 100-105 0 0
R Pickering, Director of Human Resources 135-140 0 0 130-135 0 0
J Wilkes, Director of Facilities 100-105 0 0 100-105 0 0
K James, Director of Operations 110-115 0 0 105-110 0 0
J Jesky, Chairman 20-25 0 0 20-25 0 0
J Battye, Non Executive Director 5-10 0 0 5-10 0 0
TD Pickstone, Non Executive Director 5-10 0 0 5-10 0 0
R Shamim, Non Executive Director 5-10 0 0 5-10 0 0
A Unwin, Non Executive Director 5-10 0 0 5-10 0 0
H Griffith, Non Executive Director 5-10 0 0 0-5 0 0
M Holly, Non Executive Director 5-10 0 0 0-5 0 0
C Brooks, Non Executive Director (to 31/08/2006) 0-5 0 0
Prof A Rogers, Non Executive Director (to 31/12/2006) 0-5 0 0
Name and title Salary Other Remuneration
Benefits in Kind Salary Other
RemunerationBenefits
in Kind
95Salary and Pension entitlements of senior managers
A. Remuneration
Note 1: R Chadwick, Acting Chief Executive to 03/06/2007, Director of Finance and IM&T from 04/06/2007 to 07/10/2007 and from 22/12/2007 to date. Between 8/10/2007 to 21/12/2007 R Chadwick was on secondment to CTC NHS Trust, Liverpool as Chief Executive (figures not included above).
Note 2: B Livesey, Acting Director of Finance and IM&T to 03/06/2007 and from 08/10/2007 to 30/11/2007.

(bands of £2500)
£000 £000 £000
J Saxby, Chief Executive (from 04/06/2007) 5-7.5 17.5-20 65-70
R Chadwick, see note 0-2.5 5-7.5 45-50
R Jameson, Medical Director 7.5-10 27.5-30 45-50
M Carroll, Director of Nursing 0-2.5 2.5-5 45-50
R Pickering, Director of Human Resources 0-2.5 2.5-5 0-5
J Wilkes, Director of Facilities 0-2.5 0-2.5 25-30
K James, Director of Operations 2.5-5 7.5-10 30-35
Name and title
Real increase in pension
at age 60
Real increase in lump
sum at age 60
Total accrued pension at age 60 at 31 March 2008
96
As non-executive members do not receive pensionable remuneration, there will be no entries in respect of pensions for non-executive members.
A cash equivalent transfer value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time. The benefits valued are the member’s accrued benefits and any contingent spouse’s pension payable from the scheme. A CETV is a payment made by a pension scheme, or arrangement to secure pension benefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme. The pension figures shown
relate to the benefits that the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which the disclosure applies. The CETV figures, and the other pension details, include the value of any pension benefits in another scheme or arrangement which the individual has transferred to the NHS pension scheme. They also include any additional pension benefit accrued to the member as a result of their purchasing additional years of pension service in the scheme at their own cost. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries.
Real Increase in CETV - This reflects the increase in CETV effectively funded by the employer. It takes account of the increase in accrued pension due to inflation, contributions paid by the employee (including the value of any benefits transferred from another pension scheme or arrangement) and uses common market valuation factors for the start and end of the period.
Salary and Pension entitlements of senior managers
B. Pension Benefits
The Remuneration Report continued

With the new £600,000 CT scanner at Rochdale Infirmary are (from the left) consultant radiologist, Dr Kundan Shah; chief
executive, John Saxby; site lead for radiology, Dr Ramesh Raja (now retired); and consultant radiologists Dr Judith Mather
and Dr Sohail Sabir.
(bands of £5000)
£000 £000 £000 £000 £000
195-200 1,211 1,020 95 0
135-140 703 636 36 0
145-150 814 613 130 0
135-140 792 739 24 0
5-10 43 23 13 0
75-80 404 377 13 0
95-100 456 402 31 0
Lump sum at age 60 related to accrued
pension at 31 March 2008
Cash Equivalent Transfer Value at
31 March 2008
Cash Equivalent Transfer Value at
31 March 2007
Real Increase in Cash Equivalent
Transfer Value
Employers Contribution to
Stakeholder Pension
97Salary and Pension entitlements of senior managers
B. Pension Benefits

98Accruals accounting - accruals accounting recognises assets or liabilities when goods or services are provided or received - whether or not cash changes hands at the same time. Also known as 'the matching concept', this form of accounting ensures that income and expenditure is scored in the accounting period when the 'benefit' derived from services is received or when supplied goods are 'consumed', rather than when payment is made.
Amortisation - the process of charging the cost of an asset over its useful life as opposed to recording its cost as a single entry in the income and expenditure account. Usually refers to intangible assets eg computer software. Similar in effect to depreciation.
Capital (Fixed Assets) - expenditure on the acquisition of land and premises, individual works for the provision, adaptation, renewal, replacement and demolition of buildings, items or groups of equipment and vehicles, etc. In the NHS, expenditure on an item is classified as capital if it is in excess of £5,000.
Capital Charges - capital charges are a way of recognising the costs of ownership and use of capital assets and comprise depreciation and interest/target return on capital.
CapitalResourceLimit(CRL)A - control set by DoH onto NHS organisations to limit the level of capital expenditure that may be incurred in year.
Cost of Capital - a charge on the value of assets tied up in an organisation, as a measure of the cost to the economy.
Current Assets - debtors, stocks, cash or similar, whose value is either, or can be converted into cash within the next twelve months.
Depreciation - the measure of the wearing out, consumption or other loss of value of a fixed asset whether arising from use, passage of time or obsolescence through technology, and market changes.
ExternalFinancingLimits(EFLs) - the ExternalFinancingLimit(EFL)isafundamental element of the NHS trusts financial regime. It is a cash based public expenditure control set by DoH and a trust’s access to all sourcesofexternalfinance.TheEFLrepresents the excess of its approved level of capital spending over the cash a trust can generate internally (mainly surpluses and depreciation), essentially controlling the amount of “externally” generated funding.
Impairments - impairments generally relate to fixed assets and represent the loss of value of a fixed asset below that recorded in the accounts of the organisation. Impairment occurs because something has happened to a fixed asset itself or to the economic environment in which it is used.
Indexation - process of adjusting the value, normally of fixed assets, to account for inflation.
Intangible asset - software licence or some other right, which although invisible provides value to the organisation from its use. More commonly includes goodwill or brand values in the private sector.
Market Forces Factor (MFF) - MFF is a composite index of geographical cost variations in land, buildings, equipment and staff pay (including Londonweighting).MFFisexcludedfrom national tariff and paid to Trusts separately by the Department of Health. This helps to even out the purchasing power of commissioners of NHS services (mainly primary care trusts) and allows the use of a national tariff across the country.
Provisions - provisions are made when an expense is probable but there is uncertainty about how much or when payment will be required, e.g. estimates for employers or public liability. Provisions are included in the accounts to comply with the accounting principle of prudence. An estimate of the likely expense is charged to the income & expenditure account as soon as the issue comes to light, although actual cash payment may not be made for many years. The expense is matched by a balance sheet provision entry showing the potential liability of the organisation.
Prudential Borrowing Code (PBC) - a framework that allows NHS trusts to manage their capital positions within their ability to service the resulting financial obligations. The PBC is based upon a series of financial tests, which determine prudent capital positions relative to their revenues and costs.
PrudentialBorrowingLimit(PBL) - the PBLiscalculatedbyreferencetothe rules contained in the PBC and represents the total borrowing (from all sources) that an NHS trust can service based on its current financial performance.
Public Dividend Capital (PDC) - PDC is similar to company share capital. It represents the value of the assets employed by a Trust at its formation plus any further issue or repayment of capital in subsequent years from/to the Department of Health.
Tangible asset- physical visible asset.
Working Capital - working capital is the current assets and liabilities (debtors, stock, cash and creditors) required to facilitate the operation of an organisation.
Finance glossary

Donations 159,000
Legacies 249,000
Investment Income 164,000
£
99SMALLCHANGE-BIGDIFFERENCE
The Trust operates a registered charity called The Pennine Acute Hospitals Charity and other related charities (Charity Commission registration no 1050197).
People and organisations make donations to the Trust’s charity funds for many different reasons. Sometimes it is to mark gratitude for treatment, sometimes it is to support the service generally and sometimes it is to help remember a family member who worked for the Trust.
These donations range from donations of a few pounds up to six figure sums, but they are all equally welcome – and they are all put to good use. Last year thecharityspent£733,000duringthe year on patients’ amenities, staff education and welfare and research.
The charity has the Trust Board as the corporate trustee and covers all of our
hospitals – Fairfield General, Birch Hill, Rochdale Infirmary, North Manchester General and The Royal Oldham for any charitable purpose relating to the NHS.
The charity received income of £572,000intheyear2007/08comprising:
£480,000wasspentonpatients’amenities. The majority of expenditure has been on medical equipment for a range of wards and departments across all hospitals. In addition, the hospital arts project management is fundedbycharitablefunds.£145,000was spent on staff education and welfare. The majority of expenditure is on courses and conferences across arangeofdesignatedfunds.£83,000was spent on research during the year.
The trustee of the Pennine Acute Hospitals Charity would like to express their sincere thanks for all the generous donations received over the last year
and the charitable work undertaken by all individuals and organisations. Charitable donations contribute greatly enhancing the services that we are able to provide across the Trust.
More information about charitable funds and activities, as well as making donations on-line, is available on the Trust’s website at www.pat.nhs.uk by clicking on the charity’s logo. Gift Aid enables potential donors to maximise the income to the charity. The taxman adds25pinthepoundforeverypounddonated by UK taxpayers. Gift Aid information and envelopes are now available on all wards as well as the cashiers’ offices at each site.
A full copy of the charity’s annual report and accounts is on the Trust’s website.
Donations to The Pennine Acute Hospitals Charity and other related charities can be received at any of the hospitals’ cashiers’ offices or more information is available from Jan Bolton, charitable fundraising managerontel:01619084497.
Charitable Funds

100GlossaryAcute services – medical or surgical treatment usually provided in a hospital setting. The organisation running the hospital is called an acute trust, such as Pennine Acute Trust.
Board – each NHS organisation is run by a Board. The Board consists of executive directors and non-executive directors, who are members of the public.
Choose and Book/Choice – The system allowing patients to choose from a range of hospitals and a date for their first outpatient appointment. More info at www.nhs.uk
Department of Health – the Government department responsible for the NHS. More info: www.dh.gov.uk
Elective – planned hospital treatment, either with a patient being admitted from a waiting list or by a planned admission
GP – General practitioner or family doctor.
LIFT–LocalImprovementFinanceTrust is the mechanism of financing capital builds in primary care (ie new GP practices).
Healthcare Commission - The Healthcare Commission is the health watchdog for England. More info: www.healthcarecommission.org.uk
NHS – The National Health Service was set up in 1948 and is now the largest organisation in Europe. More info: www.nhs.uk/aboutnhs/howthenhsworks.
NHS Plan – the 10-year plan for investment and reform in the NHS,
published in July 2000, which contains the basis of the targets for modernisation of the NHS, to meet patients’ needs.
NICE – the National Institute for Health and Clinical Excellence (sometimes written as either NICE or NIHCE) is an independent organisation responsible for providing national guidance on promoting good health and preventing and treating ill health. More info: www.nice.org.uk
Non-elective/emergency care – unplanned hospital treatment
North East sector – north east of Greater Manchester, the area served by the Trust. Often referred to within the context of the Trust’s partnership work with the local PCTs in this area – Bury PCT (www.burypct.nhs.uk), Heywood, Middleton and Rochdale PCT (www.hmrpct.nhs.uk), Manchester PCT (www.manchester.nhs.uk) and Oldham PCT (www.oldham.nhs.uk)
NSF - National Service Frameworks are long term strategies for improving specific areas of care.
NPSA – the National Patient Safety Agency co-ordinates the reporting of patient safety incidents, and work to improve patient safety in the NHS. More info: www.npsa.nhs.uk
Patient pathway – the treatment process for the patient, taking in all contact from any clinician.
PCT – Primary care trusts are organisations which commission (ie fund) most health services for residents in their area. They also provide some community-based services directly, such as district nursing, and have public health responsibilities.
Primary care - the part of the NHS where GPs, community nurses and other healthcare professionals work.
Secondary care - specialist services, usually providing in an acute hospital setting.
SHA - the Strategic Health Authority links the Department of Health and local NHS organisations. The SHA for the North West region is called NHS North West – www.northwest.nhs.uk
Tertiary care - care of a highly-specialised nature typically provided as an inpatient in a single hospital serving one region. Referrals are normally made by clinicians at other hospitals.
The Pennine Acute Hospitals NHS Trust – the hospital Trust which runs North Manchester General Hospital, The Royal Oldham Hospital, Fairfield General Hospital in Bury, Rochdale Infirmary and has some services at the Birch Hill Hospital site near Littleborough.Providesacuteservicesto an area of around 800,000 residents across the north east of Greater Manchester. Referred to as “the Trust” through this report. More info at: www.pat.nhs.uk
Tier 2 – a system where services traditionally only available at a hospital are provided in community settings.
This report contains a number of clinical terms – plain English versions via NHS Direct www.nhsdirect.nhs.uk/encyclopaedia.

If English is not your first language and if you need help with this document please contact the Ethnic Health Team on 01616278770.
Copies of this report, including different formats, are available from:
The Pennine Acute Hospitals NHS Trust, Communications Department, Trust Headquarters, North Manchester General Hospital, Delaunays Road, Crumpsall, ManchesterM85RB. Telephone:01619184284.It is also available online at www.pat.nhs.uk
The Trust actively welcomes comments and suggestions on ways in which to develop its communications systems, both internal and external – including this annual report.
Any suggestions should be made by writing to:
Fin McNicol, head of communications, at the above address. Tel:01619184284Email:[email protected]

Designed and Produced by Niche Communications Limited. Tel: 0161 430 7771 Email: [email protected] WWW: nichecommunications.co.uk
The Pennine Acute HospitalsNHS Trust
NHS