the learning health system in 5 chapters - guest speaker, william a. yasnoff
Upload: department-of-learning-health-sciences-university-of-michigan-medical-school
Post on 18-Jul-2015
544 views
TRANSCRIPT
1 © 2015
N H I I
ADVISORS
The Evolution of the Learning Health System in Five Chapters
William A. Yasnoff, MD, PhD, FACMI Managing Partner, NHII Advisors
Adjunct Professor, Division of Health Sciences Informatics,
Johns Hopkins University
University of Michigan February 10, 2015
© 2015
N H I I
ADVISORS

2 © 2015
N H I I
ADVISORS
LHS Evolution in Five Chapters 1. In the Beginning … [1970s] 2. Hints of a New Approach [1980s] 3. Foundations of the LHS [1990s]
● EMRs ● Registries ● Decision Support
4. Informed Care: The Health Information Infrastructure (HII) Vision [2000s] 5. Building HII for LHS [2010s]
3 © 2015
N H I I
ADVISORS
Chapter 1: In the Beginning . . . [70s]
■ Patient care ● Incomplete paper records ● Knowledge in clinician’s head
■ Research ● Clinical trials & case reports ● Published literature ● Dissemination dependent on
– Clinician education (journals, conferences)
– Clinician memory
4 © 2015
N H I I
ADVISORS
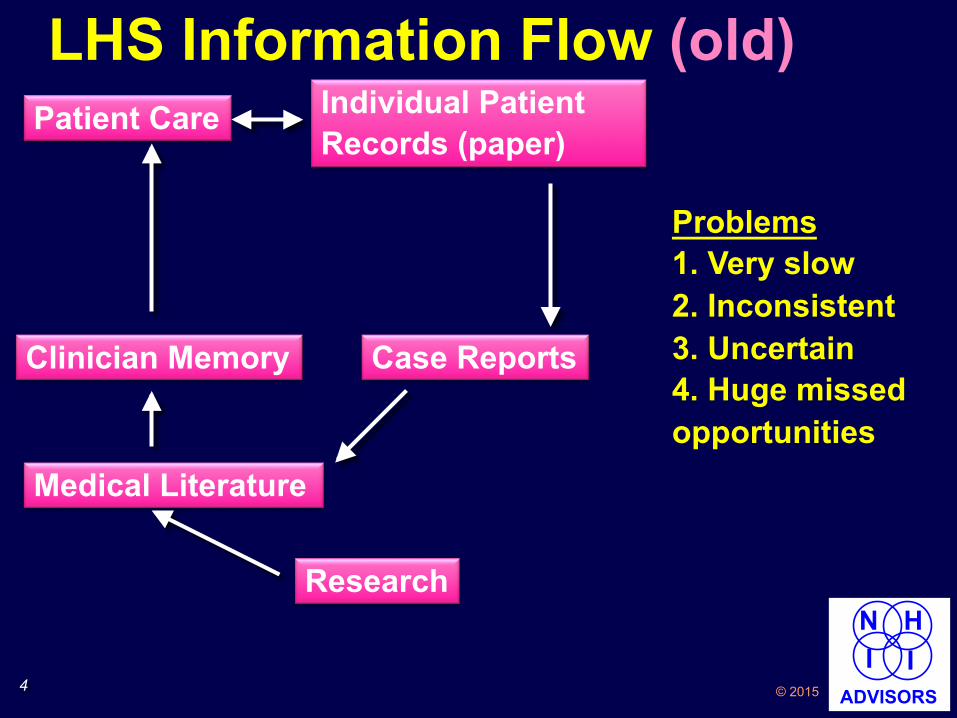
LHS Information Flow (old) Patient Care Individual Patient
Records (paper)
Clinician Memory
Research
Medical Literature
Case Reports
Problems 1. Very slow 2. Inconsistent 3. Uncertain 4. Huge missed opportunities

5 © 2015
N H I I
ADVISORS
LHS Report Card: Chapter 1
LHS Component 70s 80s 90s 00s 10s
Individual patient records D
Searchable records for other patients
Outcomes Data
Knowledge/Tools D
Publications C
Key Factors: Availability, Completeness, Speed
6 © 2015
N H I I
ADVISORS
Chapter 2: Hints of a New Approach [80s] ■ Medical College of Ohio Cardiology
Database ● Inspired by Duke Databank for
Cardiovascular Disease – Started ~1965 for CCU patients – One of earliest medical databases – Today has comprehensive records
on 200K patients ■ AMA/Net
● First comprehensive online information network for physicians
7 © 2015
N H I I
ADVISORS
MCO Cardiology Database* ■ Relational database with clinical
information about cardiology cases ■ Information entered manually ■ Outcomes data solicited by mail from
prior patients, added when received ■ Designed to answer the question,
“What happened to prior patients like this one?”
■ Used in clinical conferences to evaluate treatment options in complex cases w/o clear literature guidance
*Yasnoff WA, Brewster PS, Demain-McGreevey K, Leighton RF, and Fraker Jr TD: A Database System for Research, Teaching, and Clinical Decision Making in Cardiology. In Proceedings of Computers in Cardiology, IEEE Press, pp. 77-82, 1984

8 © 2015
N H I I
ADVISORS
AMA/Net – Faster Dissemination ■ Online information service for physicians
sponsored by AMA (late 1980s)* ■ Services
● News ● Literature (including clipping service) ● Drug Interactions ● Diagnostic Assistance – DxPlain ● Therapeutic Assistance – Hypertension
Advisor ■ Dial-up, character based interface ■ 40,000 subscribers at its peak
*Yasnoff WA: Electronic Information for Physicians: A New Dimension in Solving Traditional Problems. Pennsylvania Medicine 92:48-50, March, 1989.
9 © 2015
N H I I
ADVISORS
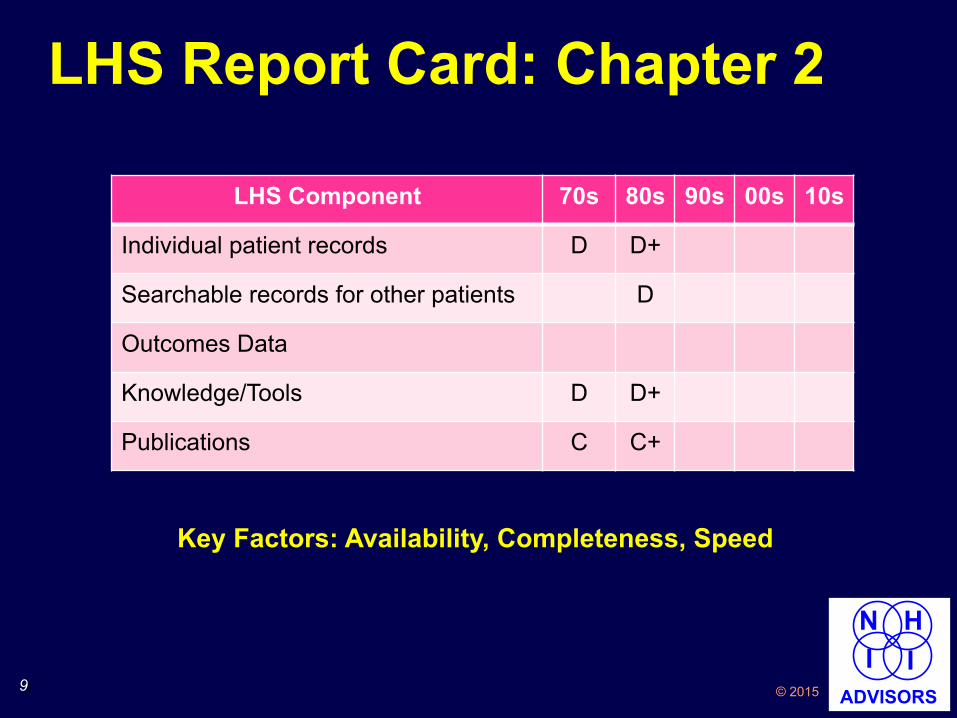
LHS Report Card: Chapter 2
LHS Component 70s 80s 90s 00s 10s
Individual patient records D D+
Searchable records for other patients D
Outcomes Data
Knowledge/Tools D D+
Publications C C+
Key Factors: Availability, Completeness, Speed

10 © 2015
N H I I
ADVISORS
Chapter 3: Foundations of the LHS [90s] ■ IOM Reports
● EHR reports (1991 & 97) – “The Computer-Based Patient Record” – “… an essential technology for
healthcare …” – Revised & updated in 1997
● “To Err is Human” (1999) – 44-98K unnecessary hospital deaths – Errors “systemic”
■ Immunization Registries ■ Decision Support

11 © 2015
N H I I
ADVISORS
Immunization Registries ■ Developed in response to 1989-91 measles
outbreaks ■ RWJ Foundation funded early efforts ($25M)
followed by CDC ($250M) ■ Oregon “Immunization Alert” was first
successful statewide registry (1996) ● Special bar coded forms collected data ● Decision support* ● Financially sustainable based on
reducing duplicate immunizations ■ Still operating successfully
*Miller PL, Frawley SJ, Sayward FG, Yasnoff WA, Duncan L, Fleming DW: Combining Tabular, Rule-Based, and Procedural Knowledge in Computer-Based Guidelines for Childhood Immunization. Computers and Biomed Res 30:211-31, 1997.

12 © 2015
N H I I
ADVISORS
Decision Support ■ CDC Guidelines for Targeted TB
Testing and Rx of Latent TB ● Encoded guidelines in computable
form (Arden syntax) ● Designed for integration with EMRs ● Can produce clinician reminders
■ CDC Prevention Guidelines* ● 360/1,069 (34%) of guidelines could
result in clinical reminders ● Potential for integration into EMRs
*Garrett NY and Yasnoff WA: Disseminating Public Health Practice Guidelines in Electronic Medical Record (EMR) Systems. J Public Health Management and Practice 8(3):1-10, 2002
13 © 2015
N H I I
ADVISORS
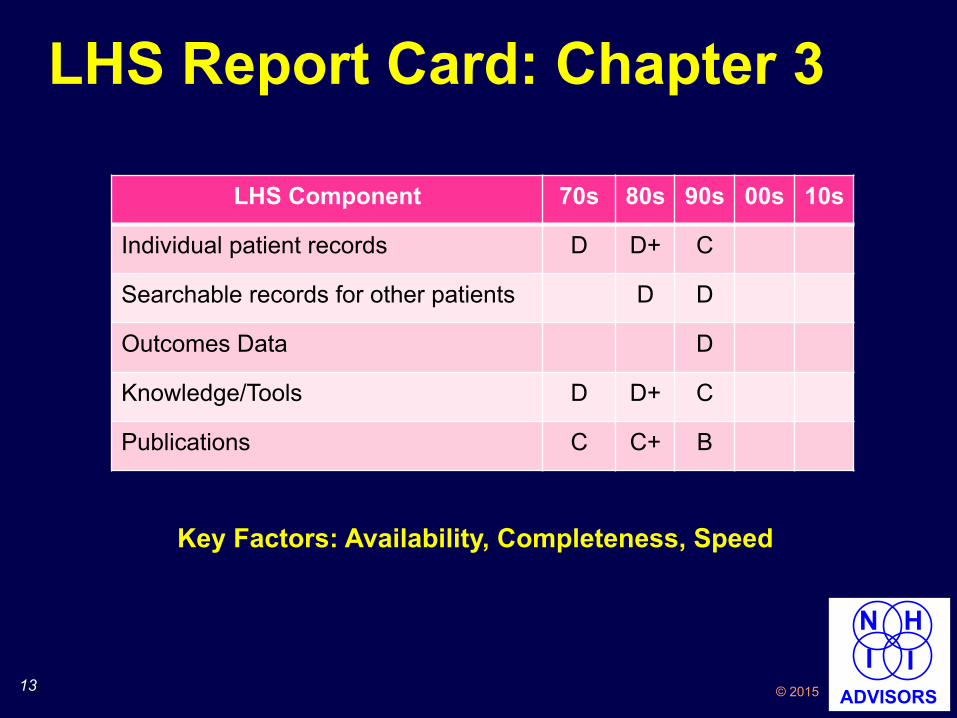
LHS Report Card: Chapter 3
LHS Component 70s 80s 90s 00s 10s
Individual patient records D D+ C
Searchable records for other patients D D
Outcomes Data D
Knowledge/Tools D D+ C
Publications C C+ B
Key Factors: Availability, Completeness, Speed
14 © 2015
N H I I
ADVISORS
Chapter 4: Informed Care: The Health Info Infrastructure Vision [00s]
■ NCVHS Report (2001) ■ Development of DHHS Office of the
National Coordinator for Health IT [ONC] (2002-4)
■ HII Progress Measures (2006-7) ■ LHS Vision from IOM (2007) ■ HITECH (2009)

15 © 2015
N H I I
ADVISORS
NCVHS* “Information for Health” ■ NCVHS/Workgroup Chair: John Lumpkin, MD
● Workgroup Member: Ted Shortliffe, MD, PhD ■ Coined the term “National Health Information
Infrastructure” ● “A comprehensive knowledge-based system capable of
providing information to all who need it to make sound decisions about health” to “support all facets of individual health, health care, and public health”
● “… implementation of the NHII will have a dramatic impact on the effectiveness, efficiency, and overall quality of health and health care in the U.S.”
■ Recommended $14 B budget over 10 years ■ Resulted in work leading to ONC
*National Committee on Vital and Health Statistics

16 © 2015
N H I I
ADVISORS
Development of ONC 2002-4 ■ 9/02: WAY assigned to HHS ■ 7/03: First-ever NHII conference developed
national consensus agenda* ● 600 attendees ● HHS Secretary announces SNOMED
licensing for entire U.S. à standing ovation
■ White House becomes interested in NHII ■ 1/04: Electronic records in State of the Union ■ 4/04: President signs Executive Order
creating ONC *Yasnoff WA, Humphreys BL, Overhage JM, Detmer DE, Brennan PF, Morris RW, Middleton B, Bates DW, Fanning JP: A Consensus Action Agenda for Achieving the National Health Information Infrastructure. J Am Med Informatics Assoc 11(4):332-338, 2004.
17 © 2015
N H I I
ADVISORS
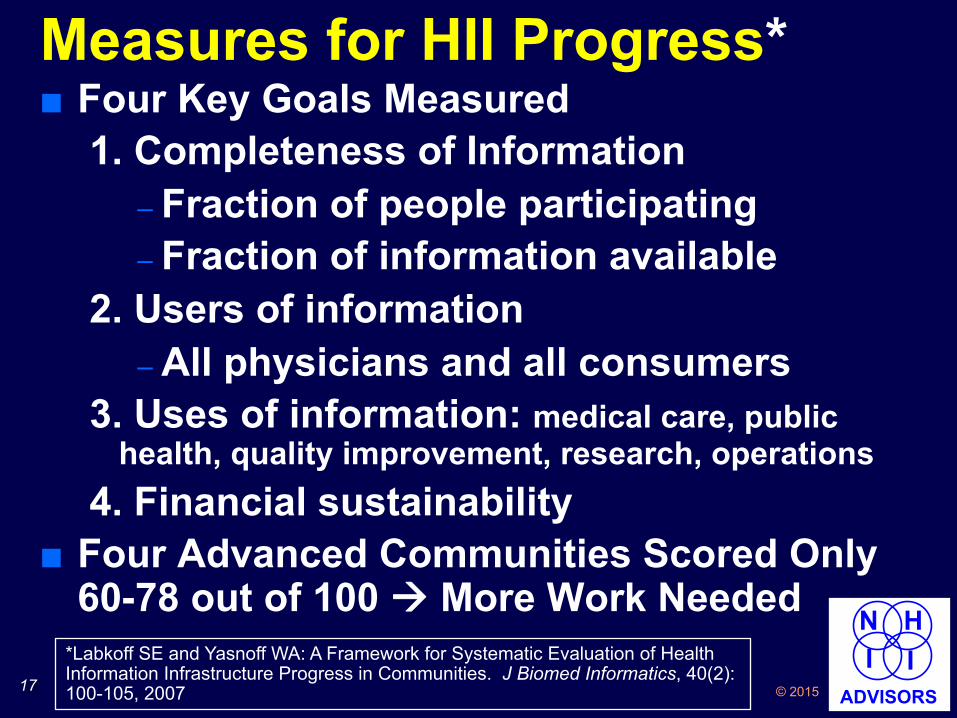
Measures for HII Progress* ■ Four Key Goals Measured
1. Completeness of Information – Fraction of people participating – Fraction of information available
2. Users of information – All physicians and all consumers
3. Uses of information: medical care, public health, quality improvement, research, operations
4. Financial sustainability ■ Four Advanced Communities Scored Only
60-78 out of 100 à More Work Needed *Labkoff SE and Yasnoff WA: A Framework for Systematic Evaluation of Health Information Infrastructure Progress in Communities. J Biomed Informatics, 40(2):100-105, 2007
18 © 2015
N H I I
ADVISORS
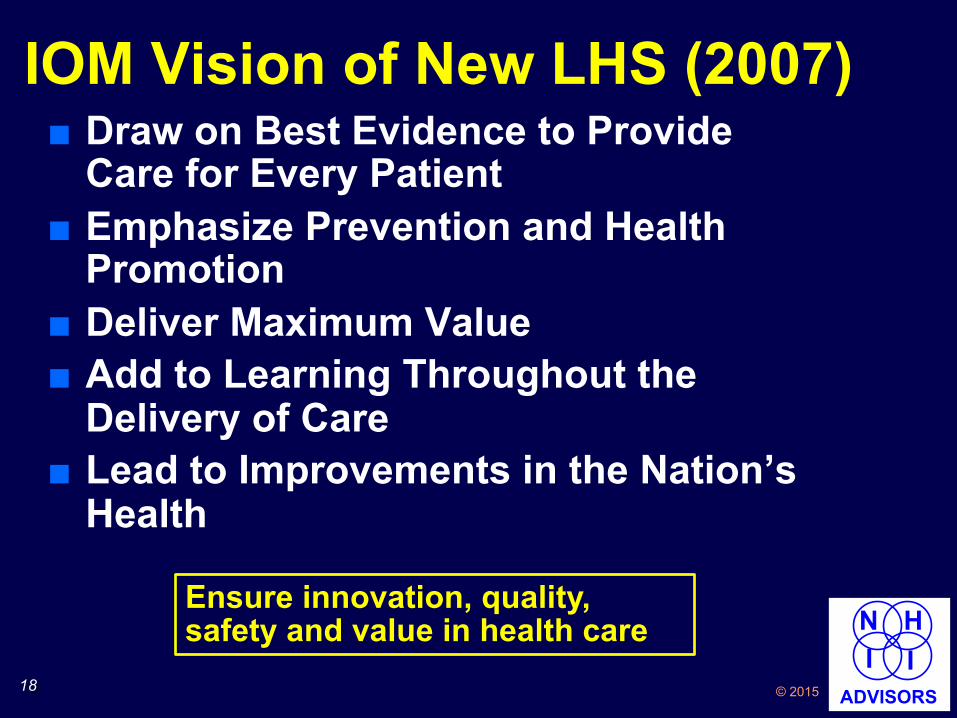
IOM Vision of New LHS (2007) ■ Draw on Best Evidence to Provide
Care for Every Patient ■ Emphasize Prevention and Health
Promotion ■ Deliver Maximum Value ■ Add to Learning Throughout the
Delivery of Care ■ Lead to Improvements in the Nation’s
Health
Ensure innovation, quality, safety and value in health care

19 © 2015
N H I I
ADVISORS
HITECH - 2009 ■ Accelerating EHR Adoption
● Provider payments for EHR “Meaningful Use”
● $44K-64K over 5 years ■ Funding State Health Info Exchanges
● $564 M (4 years) ● Increasing state matching funds ● Goal: “Facilitate and expand the secure electronic
movement and use of health information among organizations according to nationally recognized standards”
● More Useful Goal: “Facilitate the availability of comprehensive electronic records for every patient”
“The utilization of an electronic health record for each person in the U.S by 2014” – ONC Objective per HITECH
20 © 2015
N H I I
ADVISORS
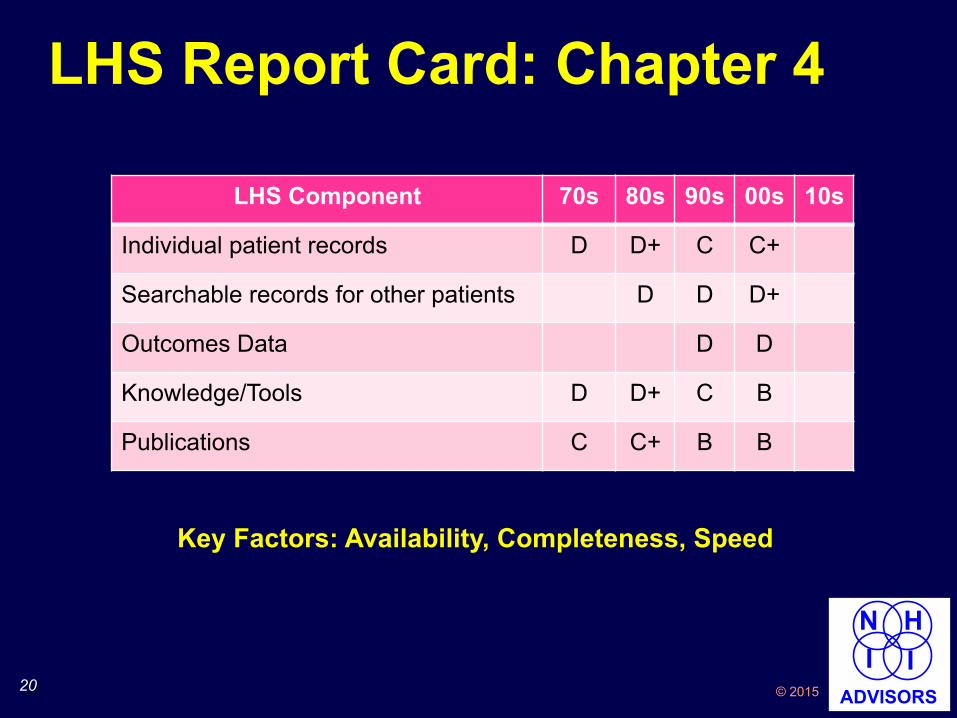
LHS Report Card: Chapter 4
LHS Component 70s 80s 90s 00s 10s
Individual patient records D D+ C C+
Searchable records for other patients D D D+
Outcomes Data D D
Knowledge/Tools D D+ C B
Publications C C+ B B
Key Factors: Availability, Completeness, Speed
21 © 2015
N H I I
ADVISORS
Chapter 5: Building HII for LHS [10s]
22 © 2015
N H I I
ADVISORS
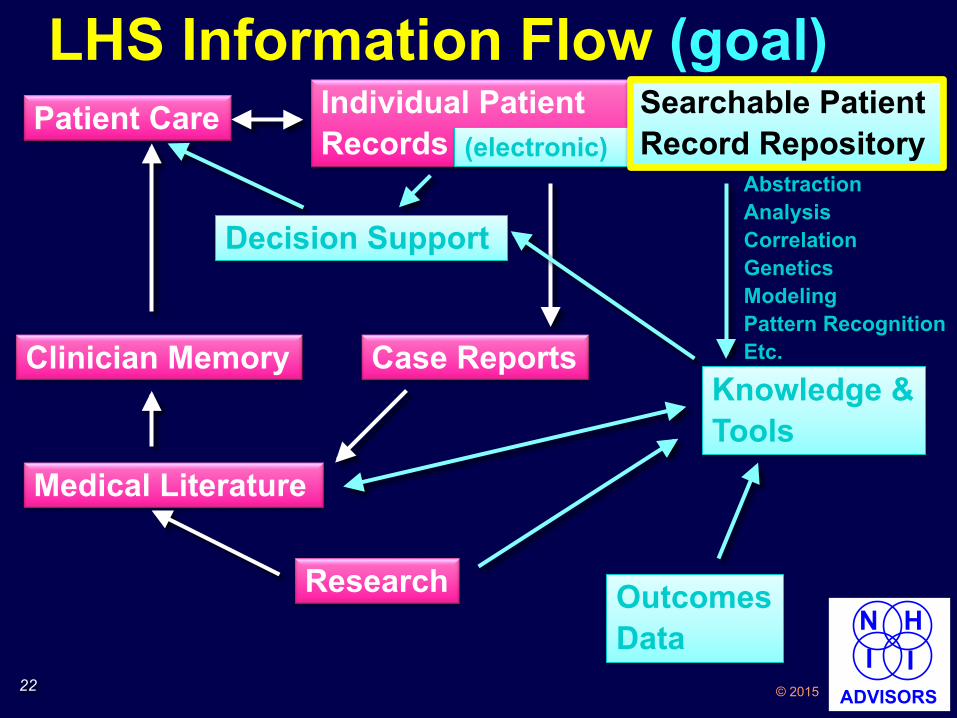
LHS Information Flow (goal) Patient Care Individual Patient
Records (paper)
Clinician Memory
Research
Medical Literature
Case Reports
Searchable Patient Record Repository
Knowledge & Tools
Decision Support
Abstraction Analysis Correlation Genetics Modeling Pattern Recognition Etc.
Outcomes Data
(electronic) Searchable Patient Record Repository
23 © 2015
N H I I
ADVISORS
HII Goals ■ Comprehensive electronic patient records
when & where needed ● Individual (patient care) ● Aggregate (research, population health)
■ Basic Requirements ● All information must be electronic à all
providers must use EHRs ● Mechanism to bring together scattered
information for each person (“Health Information Exchange” or HIE)

24 © 2015
N H I I
ADVISORS
HII Challenges 1. Privacy
● Authorized access only ● Authorized by whom?
2. Stakeholder Cooperation ● All providers must submit records
3. All Digital Records ● Paper records won’t do
4. Financial Sustainability 5. Security
● Minimize hacking vulnerability

25 © 2015
N H I I
ADVISORS
Case Study, Part 1
Diane, age 69
26 © 2015
N H I I
ADVISORS
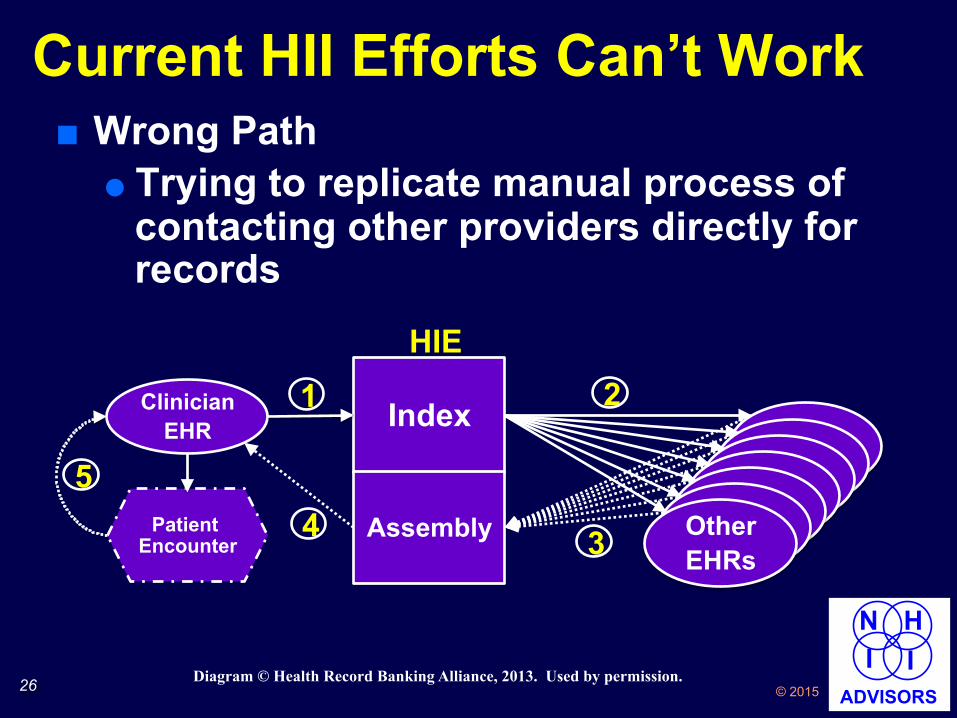
■ Wrong Path ● Trying to replicate manual process of
contacting other providers directly for records
Current HII Efforts Can’t Work
HIE
Index
Other EHRs
Assembly
Clinician EHR
Patient Encounter
5 4 3
2 1
Diagram © Health Record Banking Alliance, 2013. Used by permission.

27 © 2015
N H I I
ADVISORS
■ Complex and Expensive ● All EHRs must be online 24/7 to
respond to queries ● Real-time reconciliation of records ● Requires unique patient identifier
– Politically impractical – Privacy threat
● Must have expensive 24/7 network operations center to monitor all contributing EHRs
Current Efforts Can’t Work (continued)
28 © 2015
N H I I
ADVISORS
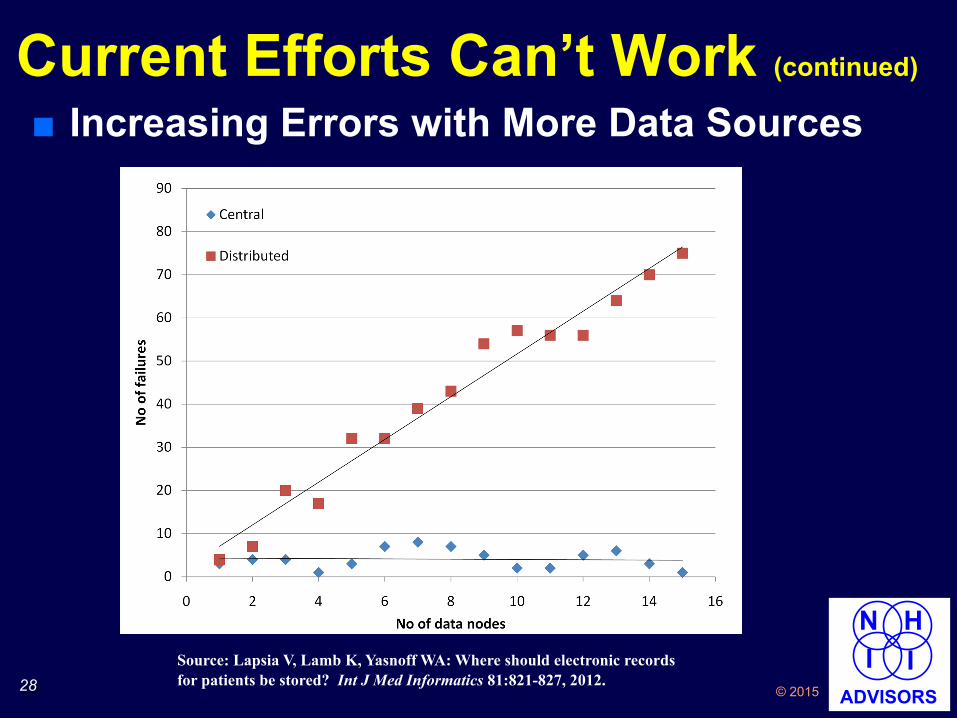
■ Increasing Errors with More Data Sources Current Efforts Can’t Work (continued)
Source: Lapsia V, Lamb K, Yasnoff WA: Where should electronic records for patients be stored? Int J Med Informatics 81:821-827, 2012.
29 © 2015
N H I I
ADVISORS
■ Unable to Facilitate Robust Data Searching ● Distributed records à sequential
search ● Sequential search is too slow to be
practical
Current Efforts Can’t Work (continued)
30 © 2015
N H I I
ADVISORS
Solution: Health Record Bank (HRB) ■ Secure community-based repository
of complete health records ■ Access to records completely
controlled by patients (or designee) ■ “Electronic safe deposit boxes” ■ Information about care deposited
once when created ● Required by HIPAA
■ Allows EHR incentives to physicians to make outpatient records electronic
■ Operation simple and inexpensive

31 © 2015
N H I I
ADVISORS
http://www.healthbanking.org/video1.html
What is a Health Record Bank?

32 © 2015
N H I I
ADVISORS
HRB Architecture
Patient Records
Clinician EHR
Patient Encounter
HRB 1
3
2
Diagram © Health Record Banking Alliance, 2013. Used by permission.

33 © 2015
N H I I
ADVISORS
HRB Rationale ■ Operationally simple
● Records immediately available ● Deposit new records when created ● Enables value-added services ● Enables research queries
■ Patient control ● Trust & privacy ● Stakeholder cooperation (HIPAA)
■ Low cost facilitates business model ● Can fund EHR incentive options
– Pay for deposits – Provide Internet-accessible EHRs

34 © 2015
N H I I
ADVISORS
© Schattauer 2014 Methods Inf Med 2/2014
1Focus Theme – Original Articles
Lessons Learned from a Health Record Bank Start-upW. A. Yasnoff1; E. H. Shortliffe2
1President, Health Record Banking Alliance (Arlington, VA); Managing Partner, National Health Information Infra -structure (NHII) Advisors (Arlington, VA); Adjunct Professor, Division of Health Sciences Informatics, Johns Hopkins University (Baltimore, MD); 2Chair, Advisory Board, Health Record Banking Alliance (Arlington, VA); Professor and Senior Advisor, College of Health Solutions, Arizona State University (Phoenix, AZ); Adjunct Professor, Columbia University (Biomedical In-formatics) and Weill Cornell Medical College (Division of Quality and Medical Informatics, Department of Public Health); Scholar in Residence, New York Academy of Medicine (New York, NY)
KeywordsHealth record bank, health information infra-structure, health information exchange, per-sonal health records, electronic health rec-ords, business model, clinical system imple-mentation
SummaryBackground: In late summer 2010, an or-ganization was formed in greater Phoenix, Arizona (USA), to introduce a health record bank (HRB) in that community. The effort was initiated after market research and was aimed at engaging 200,000 individuals as members in the first year (5% of the popu-lation). It was also intended to evaluate a business model that was based on early adoption by consumers and physicians fol-lowed by additional revenue streams related to incremental services and secondary uses of clinical data, always with specific per-mission from individual members, each of whom controlled all access to his or her own data. Objectives: To report on the details of the HRB experience in Phoenix, to describe the
sources of problems that were experienced, and to identify lessons that need to be con-sidered in future HRB ventures.Methods: We describe staffing for the HRB effort, the computational platform that was developed, the approach to marketing, the engagement of practicing physicians, and the governance model that was developed to guide the HRB design and implementation.Results: Despite efforts to engage the phy -sician community, limited consumer advertis-ing, and a carefully considered financial strategy, the experiment failed due to insuffi-cient enrollment of individual members. It was discontinued in April 2011.Conclusions: Although the major problem with this HRB project was undercapitaliza -tion, we believe this effort demonstrated that basic HRB accounts should be free for members and that physician engagement and participation are key elements in con-structing an effective marketing channel. Local community governance is essential for trust, and the included population must be large enough to provide sufficient revenues to sustain the resource in the long term.
Correspondence to:William A. Yasnoff 1854 Clarendon Blvd. Arlington, VA 22201-2914 USA E-mail: [email protected]
Methods Inf Med 2014; 53: ■–■doi: 10.3414/ME13-02-0030received: August 31, 2013accepted: November 28, 2013prepublished: ■■■
1. Background 1.1 Rationale for HRBsEstablishing a health information infra-structure (HII) that assures the availability of comprehensive electronic patient rec-
ords when and where needed has proven to be a challenging problem. Several key ob-stacles have been identified: 1) privacy – the privacy of each individual’s medical records must be protected; 2) stakeholder cooperation – physicians, hospitals, labora-
tories, pharmacies, imaging centers, etc., must all contribute their patient records; 3) incomplete information – all the records must be electronic in order to facilitate or-ganizing and delivering comprehensive records for each patient; and 4) financial sustainability – operational funding must be available on an ongoing basis [1]. In a recent report, 75% of HII projects in the U.S. reported this latter issue as an es-pecially critical obstacle [2].
Health record banks (HRBs) have been defined as “independent organizations that provide a secure electronic repository for storing and maintaining an individual’s lifetime health and medical records from multiple sources and assure that the indi-vidual always has complete control over who accesses their information” [3]. Since the concept was originally described by Szolovits [4] and first called a “health infor-mation bank” a few years later by Dodd [5], it has been studied and cited worldwide [6–13]. Recently, health record banks have been proposed as a solution to the health information infrastructure problems noted above [14]. In contrast to the commonly used distributed architecture for managing electronic health records, where each pa-tient’s records remain where they are cre-ated and are assembled in real time only when needed, the centralized HRB ap-proach has been shown in simulations to be much more efficient and less prone to error [15]. It also supports efficient, pa-tient-approved use of health records for research and policy purposes.
In an HRB, privacy is protected because individuals control access to their own rec-ords, thereby setting their own custom-tailored privacy policy. Stakeholder co -
© Schattauer 2014 Methods Inf Med 2/2014
1Focus Theme – Original Articles
Lessons Learned from a Health Record Bank Start-upW. A. Yasnoff1; E. H. Shortliffe2
1President, Health Record Banking Alliance (Arlington, VA); Managing Partner, National Health Information Infra -structure (NHII) Advisors (Arlington, VA); Adjunct Professor, Division of Health Sciences Informatics, Johns Hopkins University (Baltimore, MD); 2Chair, Advisory Board, Health Record Banking Alliance (Arlington, VA); Professor and Senior Advisor, College of Health Solutions, Arizona State University (Phoenix, AZ); Adjunct Professor, Columbia University (Biomedical In-formatics) and Weill Cornell Medical College (Division of Quality and Medical Informatics, Department of Public Health); Scholar in Residence, New York Academy of Medicine (New York, NY)
KeywordsHealth record bank, health information infra-structure, health information exchange, per-sonal health records, electronic health rec-ords, business model, clinical system imple-mentation
SummaryBackground: In late summer 2010, an or-ganization was formed in greater Phoenix, Arizona (USA), to introduce a health record bank (HRB) in that community. The effort was initiated after market research and was aimed at engaging 200,000 individuals as members in the first year (5% of the popu-lation). It was also intended to evaluate a business model that was based on early adoption by consumers and physicians fol-lowed by additional revenue streams related to incremental services and secondary uses of clinical data, always with specific per-mission from individual members, each of whom controlled all access to his or her own data. Objectives: To report on the details of the HRB experience in Phoenix, to describe the
sources of problems that were experienced, and to identify lessons that need to be con-sidered in future HRB ventures.Methods: We describe staffing for the HRB effort, the computational platform that was developed, the approach to marketing, the engagement of practicing physicians, and the governance model that was developed to guide the HRB design and implementation.Results: Despite efforts to engage the phy -sician community, limited consumer advertis-ing, and a carefully considered financial strategy, the experiment failed due to insuffi-cient enrollment of individual members. It was discontinued in April 2011.Conclusions: Although the major problem with this HRB project was undercapitaliza -tion, we believe this effort demonstrated that basic HRB accounts should be free for members and that physician engagement and participation are key elements in con-structing an effective marketing channel. Local community governance is essential for trust, and the included population must be large enough to provide sufficient revenues to sustain the resource in the long term.
Correspondence to:William A. Yasnoff 1854 Clarendon Blvd. Arlington, VA 22201-2914 USA E-mail: [email protected]
Methods Inf Med 2014; 53: ■–■doi: 10.3414/ME13-02-0030received: August 31, 2013accepted: November 28, 2013prepublished: ■■■
1. Background 1.1 Rationale for HRBsEstablishing a health information infra-structure (HII) that assures the availability of comprehensive electronic patient rec-
ords when and where needed has proven to be a challenging problem. Several key ob-stacles have been identified: 1) privacy – the privacy of each individual’s medical records must be protected; 2) stakeholder cooperation – physicians, hospitals, labora-
tories, pharmacies, imaging centers, etc., must all contribute their patient records; 3) incomplete information – all the records must be electronic in order to facilitate or-ganizing and delivering comprehensive records for each patient; and 4) financial sustainability – operational funding must be available on an ongoing basis [1]. In a recent report, 75% of HII projects in the U.S. reported this latter issue as an es-pecially critical obstacle [2].
Health record banks (HRBs) have been defined as “independent organizations that provide a secure electronic repository for storing and maintaining an individual’s lifetime health and medical records from multiple sources and assure that the indi-vidual always has complete control over who accesses their information” [3]. Since the concept was originally described by Szolovits [4] and first called a “health infor-mation bank” a few years later by Dodd [5], it has been studied and cited worldwide [6–13]. Recently, health record banks have been proposed as a solution to the health information infrastructure problems noted above [14]. In contrast to the commonly used distributed architecture for managing electronic health records, where each pa-tient’s records remain where they are cre-ated and are assembled in real time only when needed, the centralized HRB ap-proach has been shown in simulations to be much more efficient and less prone to error [15]. It also supports efficient, pa-tient-approved use of health records for research and policy purposes.
In an HRB, privacy is protected because individuals control access to their own rec-ords, thereby setting their own custom-tailored privacy policy. Stakeholder co -

35 © 2015
N H I I
ADVISORS
How HRBs Create Value Health Record Bank including free/subsidized EHRs for physicians
More complete electronic health record information Enables delivery of
optional services with compelling value
Patients sign up for HRB accounts (recommended by physicians)
Enables physicians to provide better patient care
$

36 © 2015
N H I I
ADVISORS
HRB Business Model ■ Costs (with 1,000,000 subscribers)
● Operations: $6/person/year ● EHR incentives: $10/person/year
■ Revenue ● Advertising: ~$3/person/year (option to
opt out for small fee) ● Reminders & Alerts: >= $18/person/year
(30% penetration x $60/year) – “Peace of mind” alerts ($20/year) – Preventive care reminders ($20/year) – Medication reminders ($20/year)
● Queries: >$3/person/year ■ No need to assume/capture any health
care cost savings (!!)

37 © 2015
N H I I
ADVISORS
Pro Forma Example (Houston)
($1,000)
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47
"Expenses ($K)"
"Revenue ($K)"
"Net ($K)"
Month
Initial Capital: $4.4 MM Breakeven: 16 months EBITDA Year 4: $41 MM+

38 © 2015
N H I I
ADVISORS
Prevention & Population Health ■ Challenges
● New activity – Providers do not do this now – Must hire staff & establish
procedures ● Inefficient for each provider
– More costly per capita to focus on limited populations
● Benefit externalities – Member “churn” limits ROI for
prevention – No incentive for long-term
prevention investments

39 © 2015
N H I I
ADVISORS
Prevention & Population Health ■ Potential Solution: Collaborative
Community Prevention Organization ● All providers pool resources ● Community organization does
prevention & population health for all ■ Issues
● Ongoing funding ● Continuous provider cooperation
– Initial capitalization – Annual operational funding
● Incentives good but not compelling ● Need comprehensive patient info

40 © 2015
N H I I
ADVISORS
Point of View
A Proposal for Financially SustainablePopulation Health Organizations
William A. Yasnoff, MD, PhD,1 Edward H. Shortliffe, MD, PhD,2
and Stephen M. Shortell PhD, MPH, MBA3
Reconfiguring our health delivery sector to providesafe and effective care, improve health, and simulta-
neously reduce costs requires both efficient, high-qualitymedical services and community-wide population health andprevention activities, supported by the immediate availabilityof comprehensive electronic patient information.1 Given thevarious health care stakeholders in our communities, whooften have divergent interests and incentives, how can weestablish and sustain organizations that can simultaneouslyachieve all of these goals?
Shortell2,3 has proposed entities that might be calledpopulation health organizations (PHOs) and that wouldfocus on addressing all of the determinants of health in acommunity, integrating the medical, public health, andcommunity/social service sectors. These coordinating or-ganizations would assume responsibility and accountabilityfor a defined community-wide geographic population thatwould extend beyond any individual Accountable CareOrganization’s (ACO’s) or integrated delivery system’s owngroup of patients. They would engage leaders in health caredelivery, public health, education, housing, labor, and re-lated sectors to develop effective cross-cutting services tomeet the health needs of the entire community. Targetingthe entire population would ensure that long-term preven-tion projects are included because all stakeholders wouldbenefit, regardless of ongoing and inevitable shifts in theorganizational affiliations of individuals in the community.Difficult, multifaceted problems with broad impact can beaddressed, such as obesity, diabetes, and coronary arterydisease. Risk-adjusted global or capitated payments fromMedicare, Medicaid, and commercial carriers would createbudgets tied to achieving predefined quality and cost-performance metrics.
Two key prerequisites for the success of PHOs are in-formation systems that can provide comprehensive electronicmedical information for every individual (to support target-ing of interventions) and ongoing funding sufficient tomaintain and enhance both the information infrastructure andprevention activities over time. Yasnoff et al4 have proposedhealth record banks (HRBs) as an effective mechanism forassuring the availability of comprehensive electronic patientinformation in communities. HRBs are trusted community
organizations that serve as custodians of a comprehensiveintegrated copy of each member’s personal, private healthinformation, including both medical records and personaldata that the patient may opt to add. They also could includecommunity-wide environmental health, housing, labor, andrelated human services data. The patient explicitly controlswho may access which parts of the information in his or herindividual account.5,6 When patients seek care, they givepermission to their health care providers to access some orall of their up-to-date health records available through theHRB. At the patient’s request, when care is complete, thenew records from that visit or hospitalization are securelydeposited into the HRB and made available for future use.This approach solves the problems of privacy (through pa-tient control), stakeholder cooperation (because the patientsrequest their own records, the Health Insurance Portabilityand Accountability Act [HIPAA] regulations require everystakeholder to provide them electronically if they are avail-able in that form), and financial sustainability (with revenuefrom optional applications, or ‘‘apps,’’ for use by patients aswell as use of their data for research purposes, but only withtheir permission), and it coexists with providers keeping theirown local copies of records.
HRBs can promote greater availability of electronic in-formation by subsidizing electronic health records (EHRs)for outpatient physicians, thereby assuring much higherlevels of adoption resulting in more complete information foreach patient. They also can generate substantial net revenuefrom apps, advertising, and fees for data access for researchor other purposes (with patient permission) above and be-yond their own costs of operation. For example, a ‘‘peace ofmind’’ app that automatically notifies loved ones when anemergency physician accesses HRB records (meaning thatthe person is undergoing emergency treatment) is a com-pelling value to consumers and their families for which theylikely would be willing to pay a modest fee. With consumerpermission, HRBs could readily identify eligible patients forclinical trials as well as provide data for use by researchersand policy makers. By sharing part of the revenue generatedfrom these research applications on a pro rata basis withaccount holders, consumers also would have an incentive toallow their data to be used for these purposes. The HRB
1NHII Advisors, Arlington, VA, and Division of Health Sciences Informatics, Johns Hopkins University, Baltimore, MD.2College of Health Solutions, Arizona State University, Phoenix, AZ.3Division of Health Policy and Management, School of Public Health, University of California, Berkeley.
POPULATION HEALTH MANAGEMENTVolume 17, Number 5, 2014ª Mary Ann Liebert, Inc.DOI: 10.1089/pop.2014.0060
255
A Population Health Solution

41 © 2015
N H I I
ADVISORS
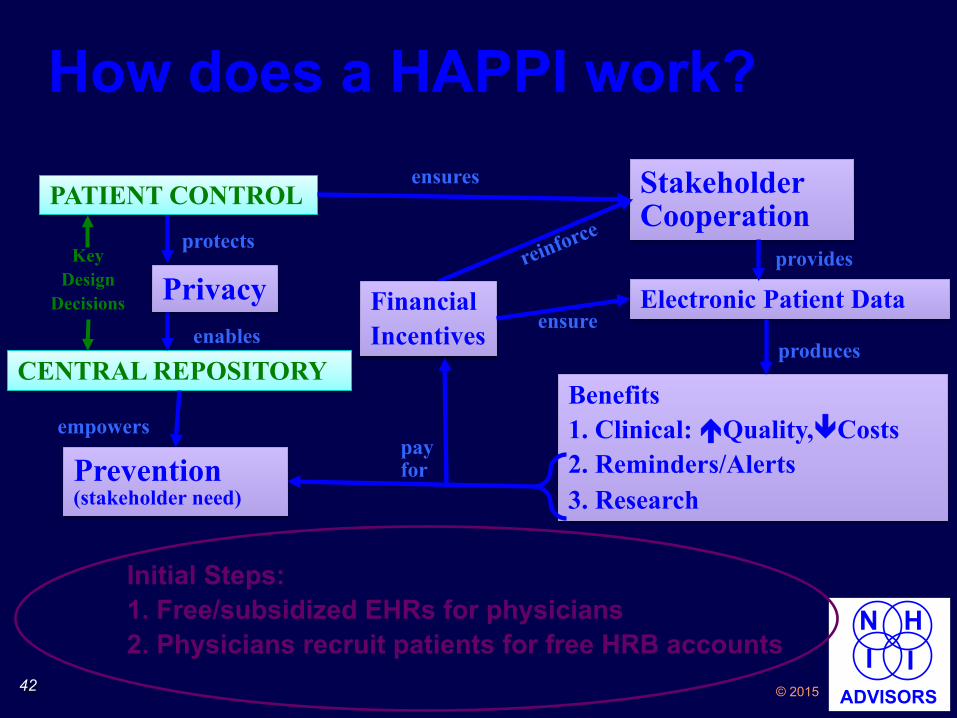
Health and Prevention Promotion Initiative (HAPPI) ■ Combine Community Prevention
Organization with Health Record Bank ■ Health Record Bank
● Provides needed information – Ensures all-electronic records
● Generates revenue (apps, ads, data) ● Provides funds for itself and more
■ Excess Funds from HRB Pay for Prevention and Population Health
■ Aligns All Stakeholder Interests
42 © 2015
N H I I
ADVISORS
How does a HAPPI work?
PATIENT CONTROL
CENTRAL REPOSITORY
Stakeholder Cooperation
ensures
Electronic Patient Data provides
Benefits 1. Clinical: éQuality,êCosts 2. Reminders/Alerts 3. Research
produces
pay for
enables
Prevention (stakeholder need)
empowers
Privacy protects
Financial Incentives ensure
Key Design
Decisions
Initial Steps: 1. Free/subsidized EHRs for physicians 2. Physicians recruit patients for free HRB accounts
43 © 2015
N H I I
ADVISORS
HRB Security Challenge ■ Centralized data best way to ensure security*
● Distributed data less secure: multiple transmission for each use
■ Inherent vulnerability of central database ● Single point of access to all data ● Potential loss of all data in one incident
■ Multiple security breaches à widespread belief that nothing is secure ● Perception is now reality
■ Challenge: Efficient search without central database
*Turn R, Shapiro NZ, Juncosa ML. Privacy and Security in Centralized vs. Decentralized Database Systems. Policy Sciences 1976;7:17-29.

44 © 2015
N H I I
ADVISORS
Avoiding Total Data Loss ■ Each patient’s data
stored in central location ● Separate database
for each patient ● Separate encryption
■ Pro: no single point of access to all data
■ Con: Sequential searching
Pt record 1* Pt record 2
Pt record N
.
.
.
*each record stored and encrypted separately

45 © 2015
N H I I
ADVISORS
Searching Separate Records
Pt record 1* Pt record 2
Pt record N
.
.
.
i ß 1
Retrieve record i
Decrypt record i
Search record i
i ß i+1
yes no *each record stored and encrypted separately i > N? END
START
Requires N iterations

46 © 2015
N H I I
ADVISORS
Searching: 2 Processors
Pt record 1* Pt record 2
Pt record N
.
.
.
i ß 1
Retrieve record i
Decrypt record i
Search record i
i ß i+2
yes no *each record stored and encrypted separately i>(N-1)? END
START
Requires N/2 iterations
Retrieve record i+1
Decrypt record i+1
Search record i+1
47 © 2015
N H I I
ADVISORS
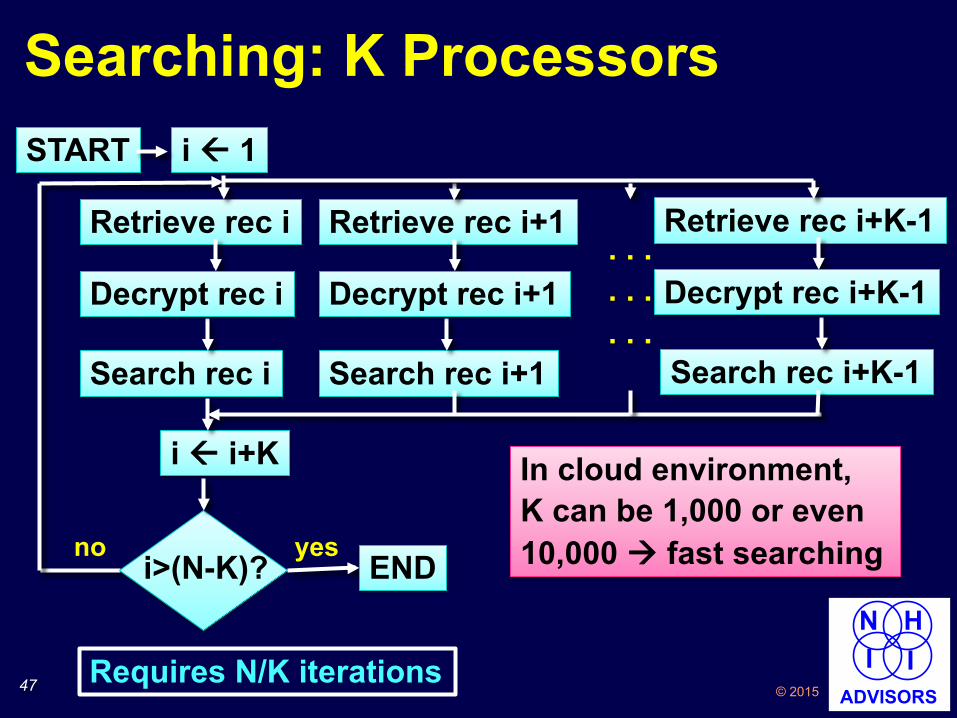
Searching: K Processors i ß 1
i ß i+K
no i>(N-K)?
yes END
START
Requires N/K iterations
Retrieve rec i Retrieve rec i+1 Retrieve rec i+K-1
Search rec i Search rec i+1 Search rec i+K-1
Decrypt rec i Decrypt rec i+1 Decrypt rec i+K-1 . . . . . . . . .
In cloud environment, K can be 1,000 or even 10,000 à fast searching
48 © 2015
N H I I
ADVISORS
Personal Health Grid™ (PHG)* ■ Each patient’s record stored in
separate database with separate encryption
■ Efficient massively parallel searching using virtual processors in cloud and/or network (which may include mobile phones)
■ No access point for all patients’ data – even for operator of service ● Eliminates “database in the sky”
security vulnerability
*patent pending (January, 2015)

49 © 2015
N H I I
ADVISORS
HRB + HAPPI + PHG = HII Solution 1. Privacy – patient control 2. Stakeholder cooperation – patient
control and ongoing incentives 3. All digital information – ongoing
incentives 4. Financial sustainability
● Apps for patients ● Apps for other stakeholders
5. Security – Personal Health Grid™ avoids potential for loss of all data
Anticipate rapid progress in HRB development

50 © 2015
N H I I
ADVISORS
Case Study, Part 2
Diane, age 69
51 © 2015
N H I I
ADVISORS
SUMMARY ■ LHS Used to be Publications and
Slow Manual Dissemination ■ New LHS Vision: Every Patient
Benefits from and Contributes to an Accessible Experience Base
■ Current LHS Vision Requires Health Information Infrastructure (HII)
■ HII Requires HRBs, HAPPI, & PHG ● Solves five key HII challenges
■ Anticipated Results ● A Real Learning Health System ● Successful Pursuit of Triple Aim

52 © 2015
N H I I
ADVISORS
LHS Report Card: Chapter 5
LHS Component 70s 80s 90s 00s 10s
Individual patient records D D+ C C+ ?
Searchable records for other patients D D D+ ?
Outcomes Data D D ?
Knowledge/Tools D D+ C B ?
Publications C C+ B B ?
Key Factors: Availability, Completeness, Speed

53 © 2015
N H I I
ADVISORS
Questions?
William A. Yasnoff, MD, PhD, FACMI [email protected] 703/527-5678

54 © 2015
N H I I
ADVISORS
Commercial Interest None No unlabeled/unapproved uses of drugs or products
William A. Yasnoff, MD, PhD

55 © 2015
N H I I
ADVISORS
LEARNING OBJECTIVES 1. Explain the differences between how learning in the
health system occurs now vs. what is envisioned in the Learning Health System
2. Name the four basic functions of the Learning Health System
3. Explain why an effective health information infrastructure is an essential component of the Learning Health System
4. Name four key challenges to the development of health information infrastructure and how a health record bank architecture addresses each one