pyogenic infections meningococcus h. influenzae pneumococcus s.aureus gas
TRANSCRIPT

Pyogenic infections
• Meningococcus
• H. influenzae
• Pneumococcus
• S.aureus
• GAS

N. meningitidis infections
BACTEREMIA WITHOUT SEPSIS SEPSIS WITHOUT MENINGITIS
MENINGITIS WITH OR WITHOUT BACEREMIA MENINGOENCEPHALITIS
INFECTIONS OF SPECIFIC ORGANS Endocarditis Pericarditis Myocarditis Pneumonia
Arthritis Osteomyelitis
Endophthalmitis Mesenterial lymphadenitis
Sinusitis Otitis media
Periorbial cellulitis

CLINICAL MANIFESTATIONS
of Str. pneumoniae infections __________________________________________________________ PNEUMONIA OTITIS MEDIA SINUSITIS LARYNGOTRACHEOBRONCHITIS PERITONITIS BACTEREMIA MENINGITIS ENDOCARDITIS PERICRDITIS ENDOPHTHALMITIS SEPTIC ARTHRITIS OSTEOMYELITIS CONJUNCTIVITIS PERIORBTAL CELLULITIS

Pneumococcus - microbiology
Gram-positiveLancet-shaped diplococcusα-hemolysisCatalase negativeProduces H2O2
Lysed by bile saltsDelicate bacteria
Pneumococcus - Surface constituents Capsular polysaccharide
Serotyping ( 90 serotypes) Quellung reaction Pathogenicity and virulence Inhibition of phagocytosis C-substance Theichoic acid (phosphocholin and galactosamine-6-phosphate
Reacts with C-reactive protein (CRP) Species specific PBP
"Lobar pneumonia must remain one of our best examples of the truththat anatomical and histological changes must be grasped thoroughlybefore the mind is allowed to wonder away over what are often thequicksands and shifting shoals of the immunologist."
W. Boyd: Pathology for the Physician (1958)
Pneumococcal pneumonia - Pathologic sequence
Engorgement (reactive edema) serum, bacteria
Red hepatization serum, bacteria, PMN, fibrin, vvt
Grey hepatization PMN, macrophages, fibrin deposition of fibrin over the pleural surface
Resolution macrophages, dead PMN, fibrin threads

Pneumococcus infections in the normal host• Infancy
• Elderly
• Recent viral infection
• Malnutrition
• Vitamin A deficiency
• „Polvere fa danno” (Leonardo da Vinci)

Pneumococcus infections in IDs• B cell defects
• Complement deficiency
• Congenital asplenia
• Hyposplenia
• Neutropenia
• AED-ID
• NEMO/IB deficiency
• IL-1R-associated kinase-4 (IRAK-4)deficiency

Arthritis of the right hip – 2.5 yr
• We: 75 mm/h, CRP: 193 mg/l
• RBC: 3.30 T/l, Hgb: 70.0 g/l
• WBC: 4700 /mm3, PMNL: 2300 /mm3
• Culture of hip joint fluid: S. pneumoniae, serotype 14
• Treatment: ceftriaxon,12 days; clindamycin,10 days
• Two episodes of low-grade fewer (< 38 OC)
Meningitis – 5½ yr
• Moderate headache, vomitus, subfebrility
• We: 40 mm/hr, CRP: 8.1 mg/l 87 mg/l
• RBC: 4.02 T/l, Hgb: 94.0 g/l
• WBC: 4800 /mm3, PMNL: 56%
• Culture of CSF: S. pneumoniae, serotype 14
• Treatment: cefotaxim, 12 days; AMX, 4 weeks
• Three episodes of low-grade fewer (< 38 OC)
• IVIG monthly

SPAD: Selective anti-Polysaccharide Antibody
Deficiency
1. Invasive disease by encapsulated bacteria
2. Poor Ab response to polysaccharide Ag
3. Normal levels of Ig and IgG subclasses
4. Intact responses to protein antigens

IRAK-4 deficiency
1. Recurrent, invasive infections caused by S. pneumoniae
2. No characteristic findings on physical exam
3. No developmental abnormalities such as ED
4. Febrile and inflammatory responses are minimal or delayed

Therapy
• IVIG substitution
• AB prophylaxis
• Vaccination with both conjugated and non-conjugated capsular vaccines

Staphylococcus aureus
Multiple strains
Localizing strains Toxin-producing strains
Coagulase TSST-1 Enterotoxin Exfoliation
Clumping factor
Protein A Toxic shock Food Scalded skin
syndrome poisoning syndrome
Bacteremia Focal infection
Abscess
Disseminated Sinusitis
Infection Boil

Diagnostic criteria of Staphylococcus TSS
MAJOR CRITERIA (ALL REQUIRED)Acute fever; temperature >38,80 CHypotension (orthostatic, shock; below age-appropriate norms)Rash (erythrodema with late desquamation)
MINOR CRITERIA (ANY 3)Mucous membrane inflammationVomiting, diarrheaLiver abnormalitiesRenal abnormalitiesMuscle abnormalitiesCentral nervous system abnormalitiesThrombocytopenia
EXCLUSIONARY CRITERIAAbsence of another explanationNegative blood cultures (except occasionally for S. aureus)
Infections by group A streptococci
__________________________________________________________RESPIRATORY TRACT INFECTIONS
SKIN INFECTIONSBACTEREMIA
VAGINITISSCARLET FEVER
RHEUMATIC FEVER__________________________________________________________

3 - Scarlet fever

Acute Rheumatic Fever (ARF)
Major manifestations1) Carditis
In 40-80% of Pts with ARF -- PancarditisValvular insufficiency -- Stenosis ("fishmouth")Arrythmia -- Cardiomegaly -- Congestive heart failure
2) PolyarthritisOccurs frequently (the most confusing)Exquisitely tender, red, warm, swollen Does not result in chronic joint diseaseDisappears in 12-24 h after therapy -- Migratory -- Affects large jointsA given joint will remain inflamed for <1 weekOccur within 5 weeks from the time of pharyngitisVirtually always associated with positive group A Strept. serology
3) ChoreaOccurs later than other manifestationsPurposless, involuntary, rapid movementsMuscle weakness -- May begin subtly (deterioration of handwriting)Behavioral abnormalities!! can be seen in SLE and Wilson,s disease!! can be confused with ticks and athetosis
4) Erythema marginatumOccurs infrequently -- evanescent, pink eruption with pale center andserpiginous marginsOccurs on the trunk and proximal extremities (never on face!)May be induced by the application of heat -- Diff. dg: Lyme disease
5) Subcutaneous nodulesOccurs infrequently -- Firm, non-tender, pea-sized nodulesOver bony prominencies (spine, olecranon, patella, ulnar and radial styloids)Correlates with the presence and severity of carditis

Acute Rheumatic Fever (ARF) Minor manifestations (4) 1) High fever (39 oC or more) 2) Arthralgia 3) Elevated ESR, CRP 4) PR prolongation * can occure in other inflammatory processes

DIAGNOSIS OF ARF Diagnostic criteria, Duckett Jones, 1944; Revised by the AHA, 1992 MAJOR MINOR 1) Carditis 1) Fever 2) Polyarthritis 2) Arthralgia 3) Chorea 3) Elevated ESR, CRP 4) Erythema marginatum 4) PR prolongation 5) Subcutan nodules PLUS: Serologic or microbiologic evidence of antecedent GAS infection!!!

INCIDENCE OF ARF
* 3% regardless of age, race, ethnic group* children between 6-10 yr of age appear to be the most susceptible* rare under 5 yr of age* decreased over 30 years before 1985/1986 to 0.5/100 000 (USA)* increased up to 18/100 000 in 1985/1986 (USA)

ARF and GAS
50 % of pts with ARF have positive throat culture for GAS
the severity of pharyngitis correlates to some degree with the attack rate
a few M serotypes of GAS appear to be rheumatogenic
a mucoid M type 18 strain was implicated in the Salt Lake City outbreak
ASO titer is the most widely used anti-Str.serologic test
20% of normal school age children have an increased ASO titer
20% of patients with ARF (especially with chorea) borderline ASO titer

THERAPY OF ARF: a subject of controversy
ANTIBIOTIC THERAPY * Penicillin 600 000 - 900 000 U as a single i.m. inj. or 200 000 - 250 000 U 2-4x per day p. os. OR * Erythromycin 30-40 mg/kg/d p.os; 10-20 mg/kg/d i.v.
ANTIINFLAMMATORY THERAPY o Salycilates o Corticosteroids
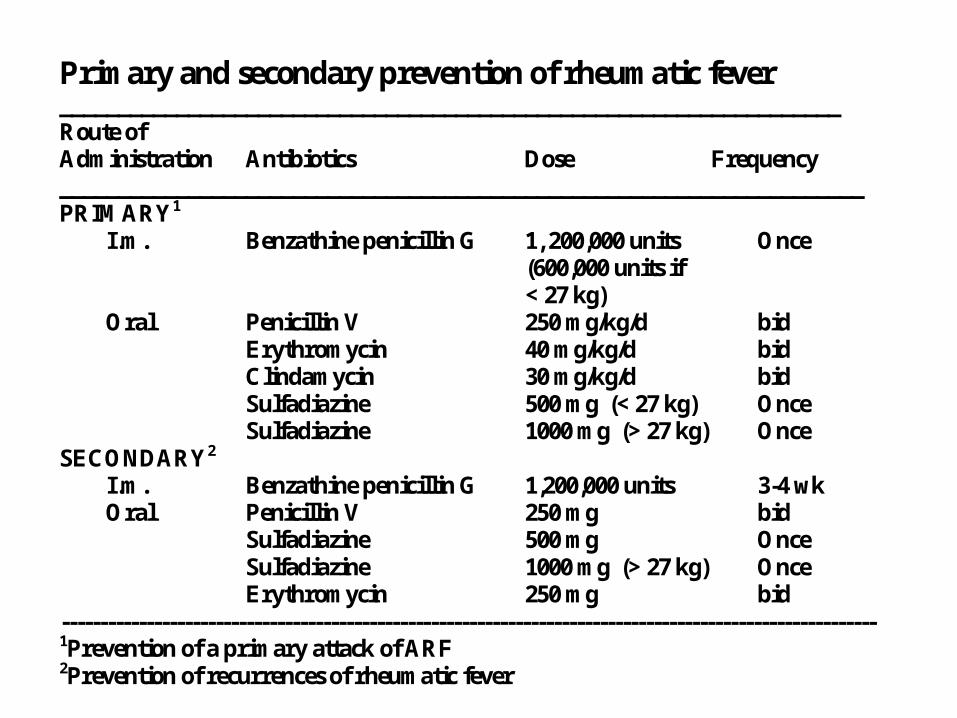
Primary and secondary prevention of rheumatic fever ___________________________________________________________________ Route of Administration Antibiotics Dose Frequency _____________________________________________________________________ PRIMARY1 I.m. Benzathine penicillin G 1, 200,000 units Once (600,000 units if < 27 kg) Oral Penicillin V 250 mg/kg/d bid Erythromycin 40 mg/kg/d bid Clindamycin 30 mg/kg/d bid Sulfadiazine 500 mg (< 27 kg) Once Sulfadiazine 1000 mg (> 27 kg) Once SECONDARY2 I.m. Benzathine penicillin G 1,200,000 units 3-4 wk Oral Penicillin V 250 mg bid Sulfadiazine 500 mg Once Sulfadiazine 1000 mg (> 27 kg) Once Erythromycin 250 mg bid ---------------------------------------------------------------------------------------------------------- 1Prevention of a primary attack of ARF 2Prevention of recurrences of rheumatic fever

3-year-old girl• Fever (38.8 C)
• Right periorbital edema
• Conjunctivitis
• 3x3 cm erythematous area over the right eye
• Intact extraocular eye movements
• No evidence of chemosis or proptosis
• Supple neck
• Diagnosis?
• Therapy?
Diagnosis
• Orbital osteomyelitis
• Orbital cellulitis
• Periorbital cellulitis
• Preseptal cellulitis

Presenting findings in periorbital cellulitis
• Redness (color)• Swelling (rubor)• Tenderness (dolor)• Normal eye movements• Fever• Leukocytosis • Chemosis• Conjunctivitis• Blue-purple hue (Hib)

Characteristic findings in orbital cellulitis
• Impairment of eye movements• Pain in the eye• Progress rapidly to
– cavernous sinus thrombosis– meningitis– brain abscess
The best choice of treatment
• Penicillin
• Ampicillin
• Cefuroxime
• Cefotaxime
• Erythromycin
Pathogens causing periorbital cellulitis
• S. aureus
• GAS
• H. influenzae
• Str. pneumoniae
• Gram- organisms
• Anaerob bacteria

Pathogenesis of periorbital cellulitis
• Infection due to – contiguous skin infection
– sinusitis
– trauma

6-year-old boy
• Fever (38.8 C) for 3 days
• Purulent nasal discharge
• Bilateral otorrhea
• Cough
• Frontal headache
• URTI ten days ago
• Therapy?
The best choice of treatment
• i.m. ceftriaxone
• i.v. cefotaxime
• p. os cephalexin
• p. os erythromycin
• p. os amoxicillin

Bacteria causing mild or moderately severe RTI
• Str. pneumoniae
• H. influenzae
• M. catarrhalis
• S. aureus (rarely)

6-year-old girl
• No fever
• Healing varicella lesions
• Rapidly enlarging skin lesion– 3x4 cm area– erythema– tenderness– Gram+ cocci in clusters (Gram stain)
• Other lesions are scabbed and dry

The best choice of treatment
• penicillin G
• ampicillin
• nafcillin
• ceftriaxone
• vancomycin